Fibrillatory Conduction in the Atrial Free Walls of Goats in Persistent. and Permanent Atrial Fibrillation
|
|
|
- Nelson Abner Watts
- 6 years ago
- Views:
Transcription
1 Fibrillatory Conduction in the Atrial Free Walls of Goats in Persistent and Permanent Atrial Fibrillation Running title: Verheule et al.; Conduction in persistent and permanent AF Sander Verheule PhD, Els Tuyls MSc, Arne van Hunnik BSc, Marion Kuiper BSc, Ulrich Schotten MD PhD and Maurits Allessie MD PhD Downloaded from by guest on May 11, 2018 Department of Physiology, Faculty of Medicine, Maastricht University, ity, The Netherlands Correspondence: e: Sander Verheule, e, PhD Dept of Physiology Universiteitssingel ER Maastricht, the Netherlands Tel: Fax: Journal Subject Codes: [130] Animal models of human disease; [132] Arrhythmiasbasic studies 1
2 Abstract: Background - Over a time course of months, the stability of atrial fibrillation (AF) gradually increases and the efficacy of pharmacological cardioversion declines, both in humans and animal models. Changes in fibrillatory conduction over this period are largely unexplored. Methods and Result - Goats were instrumented with an atrial endocardial pacemaker lead and a burst pacemaker. AF was maintained for 3 weeks (ST, n=10) or 6 months (LT, n=7). AF could be cardioverted pharmacologically at the early timepoint (persistent AF), but not at the later timepoint (permanent AF). At follow-up, a high-resolution mapping electrode was used to record epicardial conduction patterns in the free walls ls of the right (RA) and left atrium (LA). A new method for mapping of fibrillation ion waves was used to describe AF conduction patterns. Wavefronts propagated pagated uniformly during slow pacing in both groups, although conduction velocity was significantly lower in the LT group (LA: vs cm/s; RA: 94 8 vs cm/s). Median AF cycle length (AFCL) was not significantly different between the groups. However, the LT group showed highly complex activation patterns during AF with an increased number of simultaneously propagating waves (LT: RA: waves/afcl; LA: waves/afcl versus ST: RA: waves/afcl; LA: waves/afcl). Fibrillation waves in the LT group showed pronounced dissociation with large activation time differences. The incidence of waves newly appearing within the recording area was also increased in both atria. These alterations in conduction were accompanied by myocyte hypertrophy and increased endomysial fibrosis. Conclusions - Long term AF in goats leads to dissociated conduction in the atrial free walls that may contribute to increased AF stability. Key words: atrium, fibrillation, conduction, tissue, structure 2
3 Introduction In paroxysmal AF patients, the pulmonary veins often harbor high-frequency sources that can initiate and maintain AF episodes. 1 In chronic AF patients however, sites with a relatively high activation frequency are more widespread throughout the atria and isolation of the pulmonary vein region has a substantially lower efficacy in restoring sinus rhythm. 2, 3 This indicates that the relative contribution of the pulmonary vein region to AF stability is smaller in chronic AF and that the atrial myocardium outside this region has become a 'substrate for AF'. There is evidence that atrial conduction patterns are indeed more complex in chronic AF patients than in acute AF patients. 4-6 However, AF patients often have an advanced age or underlying heart disease, such as valvular disease and heart failure, which are known to affect the AF substrate. 7-9 Here, we have studied the process of AF substrate formation due to the arrhythmia itself in a goat model of 'lone AF'. As in many patients, 10 the stability of AF in goats gradually increases with time. 11 After 2 days, the atrial refractory period and AFCL are markedly shortened (electrical remodeling), and AF episode duration has increased to seconds or minutes. After 2-3 weeks, AF does not terminate spontaneously anymore, but it can still be converted pharmacologically (persistent AF). Over a time period of weeks to months, structural alterations gradually increase. 12 In parallel, the success rate of pharmacological cardioversion decreases, until it is no longer possible to cardiovert AF in most goats (permanent AF). 13 To investigate the transition from persistent to permanent AF, we have studied goats after 3 weeks of maintained AF (short term AF, ST) and goats after six months of AF (long term AF, LT). We have characterized conduction patterns in the 3
4 atrial free walls during pacing and AF using high-resolution epicardial mapping and a new method to describe fibrillation patterns. Compared to the ST group, the LT group showed more complex, dissociated activation patterns, i,e. the free walls were activated by higher numbers of simultaneously propagating wavefronts. Methods Instrumentation Ten ST and seven LT goats were included in this study (weight ST: 50 3 kg; LT: 49 4 kg). All animal procedures were in accordance with national and institutional itu guidelines. Anesthesia was induced with 10 mg/kg Pentobarbital bital and maintained i with 2% Isoflurane. A bipolar screw-in J-lead (Medtronic, Minneapolis, MN) was inserted through the jugular vein into the RA. The lead was connected with an Itrel pacemaker e (Medtronic, Minneapolis, MN) in a subcutaneous pocket in the neck. AF was maintained by applying a 1-second burst of 50 Hz every two seconds for 3 weeks (ST), or 6 months (LT). In the LT goats, a second RA lead was connected to a Kappa pacemaker (Medtronic Inc, Minneapolis, MN) to record a RA electrogram. Monitoring of AF stability In the LT group, AF stability was evaluated by a monthly pharmacological cardioversion experiment. An I Kur /I to blocker, AVE0118 (Sanofi-Aventis), was used in combination with an I Kr blocker, dofetilide. For determination of the AFCL from a RA electrogram, the Kappa pacemaker was interrogated telemetrically. 4
5 A continuous infusion of 10 mg/kg/h AVE0118 was given for 30 minutes followed by a combination of 10 mg/kg/h AVE0118 and 20 g/kg/h dofetilide for another 30 minutes. We have previously shown that this treatment could restore sinus rhythm in 100 % of goats after days of AF. 14 Follow-up experiments and data analysis After 3 weeks (ST) or 6 months of AF (LT), an open-chest follow-up experiment was performed. Anesthesia was induced with Nesdonal (20 mg/kg) and maintained with 2% Isoflurane. After stabilization of the anesthesia, cardiac output was determined er using thermodilution. Subsequently, the chest was opened by a left-sided thoracotomy, ot o the third and fourth ribs were removed and the pericardium was opened to expose the heart. Atrial conduction was measured using a round high density mapping electrode array a of 4 cm in diameter, consisting of 234 unipolar recording electrodes with an interelectrode distance of 2.4 mm, connected to a 256-channel amplifier (sampling rate 1 khz, filtering bandwidth Hz). Pairs of pacing electrodes were located at the sides of the recording array for bipolar pacing. After recording AF, goats were electrically cardioverted to record conduction during pacing. To analyze fibrillation patterns, a novel 'wave mapping' algorithm was used, detailed in the online supplement. Histology Endomysial fibrosis and myocyte diameter were determined from thin sections of plastic embedded atria from 4 ST and 5 LT goats, see online supplement for details. 5
6 Statistical analysis Results are expressed as mean Standard Error of the Mean (SEM). Statistical analysis was performed using one-way ANOVA with Bonferroni correction, a P-value < 0.05 was considered statistically significant. Results Progressive stabilization of AF In the LT group, AF stability was evaluated in awake goats on a monthly basis. Figure 1A shows the success rate of pharmacological cardioversion ion by AVE118 (I kur /I to - blocker) and dofetilide (I kr -blocker) at different time points. After 1 month of AF, sinus rhythm could be restored in 80% of the goats, but cardioversion efficacy gradually decreased to 50% after 3 months of AF and 0% after 4 months of AF. Over the 6-month monitoring period, the baseline AFCL calculated from the RA electrogram in awake goats did not decrease significantly (figure 1B). The AFCL measured ms after one month of AF and 92 6 ms after six months of AF. Thus, failure of pharmacological cardioversion was not attributable to a further progression of electrical remodeling. In figure 1C, the effect of AVE0118 and dofetilide on the AFCL is provided for a representative goat after one, three and six months of AF. After one month of AF, 14 minutes of AVE0118 administration increased AFCL from 96 at baseline to 128 ms before cardioversion (total dose: 140 mg/kg AVE0118). After 3 months of AF, AFCL increased from 82 ms at baseline to 130 ms after 30 minutes of AVE0118 and to 140ms after 14 minutes of combined infusion of AVE0118 and dofetilide before cardioversion 6
7 (total dose: 440 mg/kg AVE0118 and 4.7 g/kg dofetilide). After six months of AF, AFCL increased from 86 ms to 129 ms with AVE0118 alone and reached 203 ms after 30 minutes of combined infusion of AVE0118 and dofetilide (total dose: 600 mg/kg AVE0118 and 10 g/kg dofetilide). Despite exceeding the AFCL prior to cardioversion at the earlier time points, sinus rhythm was not restored. After 4 months of AF, pharmacological cardioversion failed in all LT goats. In ST goats, no spontaneous cardioversions were observed during the day prior to follow-up experiments, as determined by monitoring the surface ECG after the pacemaker was turned off. Therefore, goats in the ST and LT groups were considered to be in persistent and permanent AF, respectively, at the time of sacrifice experiments. ents. Conduction velocity and fibrillation intervals After 3 weeks (ST group, n=10) or 6 months (LT group, n=7), an open chest sacrifice experiment was performed. LT goats had a preserved cardiac output ( ml min -1 kg -1 vs in ST goats, p=ns) and did not show any clinical signs of heart failure. During sinus rhythm and slow pacing, both groups showed uniform atrial propagation. However, CV during slow pacing (BCL 400 ms) was decreased by 30% in both atria in the LT group compared to the ST group (figure 2A and B). During AF, the average of the median AFCLs in the ST group ( and ms in the RA and LA, respectively) was not significantly different from the LT group ( ms and ms for the RA and LA, respectively, figure 2C). In addition, the beat-to-beat variability in AFCL was not significantly different between the two groups for either LA or RA (figure 2D). 7
8 Conduction heterogeneity and block To quantify differences between ST and LT goats, the distribution of conduction times during AF was evaluated. The distribution in LT goats had a more pronounced tail towards long conduction times, as illustrated in figure 3A. Compared to the ST group, the average of the median conduction times in the LT group was significantly increased in the LA, but not in the RA (figure 3B). The incidence of conduction block (defined as a conduction time >12 ms) was significantly higher in the LT atria (figure 3C). Activation patterns during AF To investigate the increase in AF stability, we studied fibrillatory conduction patterns. During AF, activation patterns were more complex in LT goats than in ST goats (see supplemental videos). In figure 4, a representative example of conduction o patterns during consecutive beats of AF in the LA of an ST goat are shown. During these beats, the LA was activated by 3-5 waves. In the first beat, two waves entered the recording area from the side of the array, followed shortly by an epicardial breakthrough (asterisk) near the middle of the array. Three peripheral waves activated the area during the second beat, and four peripheral waves and a breakthrough were observed during the third beat. In the fourth beat, a broad wave activated most of the area from the periphery, with notable areas of slow conduction, followed by two late, discontinuous waves after a considerable delay (zigzag lines). As illustrated in a representative example for the LA in figure 5, more complex activation patterns were observed in the LT goats. In the four consecutive beats of AF shown here, the LA free wall was activated by waves per 8
9 beat. For example, during the second beat, a total of 7 peripheral waves entered the recording area at various timepoints. In addition, three epicardial breakthroughs waves originated away from the periphery. Finally, five discontinuous waves originated after a delay at the boundary of previous waves. The other beats show comparable, highly complex and irregular patterns. Within the areas activated by a wave, regions of slow conduction were often observed. Overall, compared to ST goats, AF in LT goats was characterized by a larger number of simultaneously propagating wavefronts that often followed a meandering trajectory. The high degree of dissociation of fibrillation waves together with numerous epicardial breakthroughs and discontinuities led to a greatly increased complexity of fibrillatory conduction. Figure 6 shows an example of the dissociated conduction patterns that were far more prominent in the LT group. Both the unipolar electrograms and the derived isochronal map shows that neighboring electrodes can be part of different dissociated, narrow fibrillation waves with large activation time differences. Figure 6 also illustrates an example of epicardial breakthroughs in the RA of a LT goat. The isochronal map shows three epicardial breakthroughs with the resulting fibrillation waves spreading away from their sites of origin and colliding near the middle of the array. Number and characteristics of fibrillation waves The activation maps in figures 3 and 4 indicate that the number of fibrillation waves per cycle is higher in the LT group than in the ST group. Indeed, as shown in figure 7A, the total number of waves was significantly increased in both atria. Comparing the ST and LT groups, the average number of waves/afcl increased from to 9
10 in the RA and from to in the LA. Thus, the number of waves per AFCL was increased by factors of 2 and 3 in the RA and LA, respectively. To further delineate the alterations in conduction pattern, the source of these fibrillation waves was investigated. We distinguished between peripheral waves, entering the recording area from the edge of the array and 'non-peripheral waves', i.e. waves newly appearing within the recording area, away from the outer edge. In comparison to the ST group, the number of peripheral waves per AFCL was significantly increased in the LT group for both atria (figure 7B). The number of 'non-peripheral waves' was also significantly increased in both atria of the LT group (figure 7C). However, the ratio between non-peripheral and peripheral waves was not significantly different fere between the ST and LT groups in either atrium (figure 7D). Structural changes Histological changes were assessed in the epicardial layer of 4 ST and 5 LT goats. No significant difference in the separation of myocyte bundles (perimysial fibrosis) or in the occurrence of larger areas of (replacement) fibrosis was observed between the groups (data not shown). However, a significant larger degree of endomysial fibrosis was present in both atria of LT goats (figure 8 A and B), leading to increased transverse myocyte-tomyocyte distances (figure 8C). In addition, myocyte diameter was significantly larger in the atria of LT goats, reflecting myocyte hypertrophy due to chronic AF (figure 8D). 10
11 Discussion In this study, we have investigated conduction patterns at two stages in the progressive stabilization of AF. We demonstrate a greatly increased complexity of fibrillatory conduction in the atrial free walls after 6 months of AF, indicating that these regions contribute more to the 'AF substrate'. Based on our previous studies, the ST group has complete electrical remodeling without significant structural changes, whereas the LT group has both complete electrical remodeling and significant structural remodeling. In the goat model, electrical remodeling is complete after 2-3 days of AF. 11 Here, we found that the AFCL was not significantly different between ST and LT goats during follow up experiments, although there was a trend toward a lower median AFCL in LT goats during anesthesia. However, median AFCL did not change over a time course of 6 months in awake LT goats. Thus, the difference in AF stability between the groups cannot n be attributed to a progression of electrical remodeling. A much slower process of 'structural remodeling' has been proposed to explain the progressive AF stabilization after the first days of AF. These slow structural changes include cellular hypertrophy and dedifferentiation, myolysis, an increased extracellular matrix volume per myocyte and 12, 15 heterogeneous connexin40 distribution. Time course of AF stabilization We have previously shown that AF stability gradually increases over a time course of months. Eijsbouts et al. showed that the cardioversion efficacy of flecainide gradually decreases from 60% after 1 month to 17% after 4 months of AF. 13 In another study, we have reported a 100% success rate of cardioversion with a combination of 11
12 AVE0118 and dofetilide in goats after 46±17 days of AF. 14 Here, we show that cardioversion efficacy of this drug combination also gradually declined to 0% after 4 months of AF. This loss of cardioversion efficacy indicates an increased AF stability, reflecting the transition from persistent to permanent AF. Changes in fibrillatory conduction The increased AF stability after six months of AF was associated with changes in the activation pattern. Overall, fibrillation patterns in the LT group were more complex, particularly in the LA. In summary, we observed the following pro-arrhythmic hm alterations in the LT group: 1) A decrease in conduction velocity; 2) Increased conduction heterogeneity and block during AF; 3) An increase in the number of simultaneously propagating fibrillation i waves; 4) An increased incidence of newly appearing waves. Ad 1) During slow pacing, macroscopic CV was 30% lower in both atria in the LT group compared to the ST group. In other large animal models of AF, such as canine models of congestive heart failure and chronic LA dilatation, no change in CV was observed. 8, 9 In these models, marked structural alterations have been observed, including relatively large areas of replacement fibrosis. In our goat model of AF, we have not observed such large fibrotic areas. However, we have previously reported a heterogeneous decrease in the expression of the gap junction protein connexin40 (which is associated with increased complexity of fibrillatory conduction in chronic AF patients 16 ) and an increase in the amount of extracellular matrix per myocyte. 15 The latter observation is confirmed in this study by the increased transverse intermyocyte distances within bundles (endomysial 12
13 fibrosis). This resembles the pattern of interstitial fibrosis ('microfibrosis') reported for human atrial trabeculae during normal aging. 17 Alterations in cellular connectivity due to microfibrosis can produce large delays during conduction perpendicular to the main fiber orientation. 17 Thus, this pattern of fibrosis may have a pronounced effect on epicardial conduction, especially during transverse conduction. Ad 2) We expect the impairment of epicardial conduction in the LT group to lead to an increased conduction heterogeneity during AF. Indeed, 6 months of AF resulted in an increased incidence of long conduction times and conduction block. In detailed activation maps, the decrease in epicardial CV was also reflected by areas of slow conduction within waves in the LT group (examples in figure 5). Furthermore, re, there was marked beat-to-beat variability ability in the location of conduction block between waves and areas of slow conduction within waves. This indicates that structural remodeling does not lead to fixed transmural obstacles to propagation, but rather to a decrease in conduction reserve due to the ubiquitous occurrence of myocyte hypertrophy and endomysial fibrosis throughout the epicardial layer. As these changes are expected to compromise transverse conduction in particular, 18 conduction disturbances may depend on the coupling interval and propagation direction. Ad 3) Using a computer model, Moe et al have demonstrated that AF can be maintained by multiple randomly propagating wavelets. 19 In a canine model of cholinergic AF, Allessie et al have shown that AF was maintained as long as a critical minimal number of 4 to 6 fibrillation waves were simultaneously present. 20 In the present study, we have found that a 10-cm 2 area of the atrial free wall in the ST group displayed an average of 4 to 5 fibrillation waves per AFCL. The observed fibrillation patterns were similar to those 13
14 in humans during acute AF. 21 In LT goats, the number of waves within this 10-cm 2 area was a factor 2-3 higher. In addition, the atria dilate due to chronic AF, 22 which will further increase the number of simultaneously propagating waves in LT goats compared to ST goats. The large number of fibrillation waves may explain why AF is sustained in the ST group and why AF stability is further increased in the LT group. Ad 4) The number of fibrillation waves appearing on the epicardial surface within the central region of the array was increased in both atria of the LT group. We have further classified these fibrillation waves into epicardial breakthroughs and discontinuous waves. Although there may be a degree of contamination between the two types of nonperipheral waves, this approach allows us to distinguish diverging patterns tern of newly appearing waves, which may have different underlying mechanisms. Epicardial breakthroughs may result either from transmural propagation from the endocardial trabecular network or from local generation of a new wave due to cellular proarrhythmic mechanisms. Discontinuous waves may result from a delay in conduction between adjacent electrodes in the epicardial plane. Spach et al have shown that myocyte hypertrophy and increased interstitial fibrosis, similar to that observed in this study, can 17, 18 lead to activation delays during transverse conduction. A major advantage of our methods of analysis is that it allows a detailed reconstruction of activation patterns during AF. Using this analysis, we have not observed sites with a rapid repetitive activation patterns acting as AF 'drivers' in the regions investigated here. Quantitatively, both the number of peripheral and non-peripheral waves (epicardial breakthroughs and discontinuous waves) was higher in LT than in ST atria. However, the ratio between nonperipheral and peripheral waves was not different between the groups. Thus, the number 14
15 of waves entering from the periphery and new waves appearing within the recording area increase in the same proportion. This indicates that the additional complexity generated within the area under observation is at least as large as that generated outside the field of view, supporting an 'anarchical' (substrate-based) rather than 'hierarchical' (driver with or without a substrate) mechanism. Interestingly, a recent study by Everett et al using simultaneous epi- and endocardial mapping indicated that fibrillation patterns in dogs after 6-8 weeks of rapid atrial pacing could be explained by multiple wavelet reentry. 23 However, our results are also compatible with high-frequency sources outside the field of view, with an increased propensity to wavebreak throughout the atrial free walls. In either case, the altered conduction properties of the free walls in LT goats are likely to increase AF stability. In most parameters investigated in this study, the LA was more severely affected than the RA. During AF, the LA may face a larger hemodynamic load and degree of stretch. However, in earlier studies we have not found systematic differences between the atria in cellular hypertrophy, ECM volume and connexin distribution. 15 Alternatively, differences in conduction during AF may reflect the interaction between structural remodeling and differences in anatomy between the atria. The overall anatomy and endocardial trabecular network differ between the atria, 24 and this is likely to influence conduction pathways during AF. 25 Overall, the factors discussed above contribute to a higher degree of complexity of fibrillatory conduction in the LT group, which is likely to increase AF stability. Our results are consistent with the assumption that structural remodeling causes a decrease in conduction reserve, leading to dissociated conduction of fibrillation waves. 15
16 Study Limitations The substrate for AF in this goat model of 'lone AF' may not be representative for all AF patients. In many patients, underlying heart disease or advanced age may lead to atrial structural changes that create a preexisting substrate for AF. In our goat model, we have studied alterations in fibrillation patterns due to AF itself. We show differences in propagation patterns associated with the transition from persistent to permanent AF in the absence of a preexisting substrate. Whether a preexisting substrate would affect propagation during AF and the time course of AF stabilization requires further investigation. We did not observe high-frequency sources driving AF. It is conceivable ceiv that such sources were located outside our recording locations, which spanned the major part of the anterior surface of the free walls. In patients with paroxysmal AF, the pulmonary vein region can display rapid ectopic activity. 1 In a sheep model of cholinergic AF 26 and a dog model of lone AF, activation frequencies were higher in the LA than in the RA. 27 In our model, the difference in AFCL between RA and LA was small, and there was no consistent gradient in activation frequency: the RA had a smaller median AFCL in 5 out of 10 ST goats and in 5 out of 7 LT goats. Nevertheless, conduction patterns in LT goats were more complex in the LA than in the RA, as evidenced by the larger number of simultaneous waves. Thus, the median AFCL does not accurately reflect the complexity of fibrillatory conduction. Overall, the complexity of conduction patterns in the free walls was markedly increased after 6 months of AF. Irrespective of the possible contribution of areas outside these recorded areas, the free walls have at that point become a substrate that is likely to increase AF stability. 16
17 Conclusion Comparison of fibrillation pattern between goats with persistent and permanent AF shows an increased dissociation of epicardial conduction, leading to an increased number of simultaneously propagating fibrillation waves. Thus, over a time course of months, AF itself causes changes in fibrillatory conduction that are likely to contribute to increased AF stability. The widespread changes in behavior of the atrial free walls may contribute significantly to the substrate of chronic AF and may help to explain the limited efficacy of targetted ablation strategies in chronic AF patients. Funding Sources: Dutch Heart Foundation grant 2001B024 (SV), Leducq Foundation grant 07CVD03 (US) and the Dutch Research Organization VIDI-grant (US) Conflict of Interest Disclosures: None References: 1. Haissaguerre M, Jais P, Shah D, Takahashi A, Hocini M, Quiniou G, Garrigue S, Le Mouroux A, Le Metayer P, Clementy J. Spontaneous initiation of atrial fibrillation by ectopic beats originating in the pulmonary veins. N Engl J Med. 1998;339: Sanders P, Berenfeld O, Hocini M, Jais P, Vaidyanathan R, Hsu LF, Garrigue S, Takahashi Y, Rotter M, Sacher F, Scavee C, Ploutz-Snyder R, Jalife J, Haissaguerre M. Spectral analysis identifies sites of high-frequency activity maintaining atrial fibrillation in humans. Circulation. 2005;112: Sanders P, Nalliah CJ, Dubois R, Takahashi Y, Hocini M, Rotter M, Rostock T, Sacher F, Hsu LF, Jonsson A, O'Neill MD, Jais P, Haissaguerre M. Frequency 17
18 mapping of the pulmonary veins in paroxysmal versus permanent atrial fibrillation. J Cardiovasc Electrophysiol. 2006;17: Ravelli F, Faes L, Sandrini L, Gaita F, Antolini R, Scaglione M, Nollo G. Wave similarity mapping shows the spatiotemporal distribution of fibrillatory wave complexity in the human right atrium during paroxysmal and chronic atrial fibrillation. J Cardiovasc Electrophysiol. 2005;16: Wu J, Estner H, Luik A, Ucer E, Reents T, Pflaumer A, Zrenner B, Hessling G, Deisenhofer I. Automatic 3D mapping of complex fractionated atrial electrograms (CFAE) in patients with paroxysmal and persistent atrial fibrillation. J Cardiovasc Electrophysiol. 2008;19: Stiles MK, Brooks AG, Kuklik P, John B, Dimitri H, Lau DH, Wilson L, Dhar S, Roberts-Thomson RL, Mackenzie L, Young GD, Sanders P. High-Density Mapping of Atrial Fibrillation in Humans. J Cardiovasc asc Electrophysiol. 2008;19: Koura T, Hara M, Takeuchi S, Ota K, Okada Y, Miyoshi S, Watanabe A, Shiraiwa K, Mitamura H, Kodama I, Ogawa S. Anisotropic conduction o properties in canine atria analyzed by high-resolution optical mapping. Circulation. 2002;105: Verheule S, Wilson E, Banthia S, Everett THt, Shanbhag S, Sih HJ, Olgin J. Direction-dependent conduction abnormalities in a canine model of atrial fibrillation due to chronic atrial dilatation. Am J Physiol Heart Circ Physiol. 2004;287:H Li D, Fareh S, Leung TK, Nattel S. Promotion of atrial fibrillation by heart failure in dogs: atrial remodeling of a different sort. Circulation. 1999;100: Kopecky SL, Gersh BJ, McGoon MD, Whisnant JP, Holmes DR, Ilstrup DM, Frye RL. The natural history of lone atrial fibrillation. A population-based study over three decades. N Engl J Med. 1987;317: Wijffels M, Kirchhof C, Dorland R, Allessie M. Atrial fibrillation begets atrial fibrillation. A study in awake chronically instrumented goats. Circulation. 1995;92:
19 12. Ausma J, Litjens N, Lenders MH, Duimel H, Mast F, Wouters L, Ramaekers F, Allessie M, Borgers M. Time course of atrial fibrillation-induced cellular structural remodeling in atria of the goat. J Mol Cell Cardiol. 2001;33: Eijsbouts S, Ausma J, Blaauw Y, Schotten U, Duytschaever M, Allessie M. Serial cardioversion by class IC Drugs during 4 months of persistent atrial fibrillation in the goat. J Cardiovasc Electrophysiol. 2006;17: Blaauw Y, Schotten U, van Hunnik A, Neuberger HR, Allessie M. Cardioversion of persistent atrial fibrillation by a combination of atrial specific and non-specific class III drugs in the goat. Cardiovasc Res. 2007;75: Ausma J, van der Velden HM, Lenders MH, van Ankeren EP, Jongsma HJ, Ramaekers F, Borgers M, Allessie M. Reverse structural and gap-junctional remodeling after prolonged atrial fibrillation in the goat. Circulation. ion. 2003;107: Kanagaratnam atnam P, Cherian A, Stanbridge RD, Glenville B, Severs NJ, Peters NS. Relationship between connexins and atrial activation during human atrial fibrillation. J Cardiovasc Electrophysiol. 2004;15: Spach MS, Boineau JP. Microfibrosis produces electrical load variations i due to loss of side-to-side cell connections. Pacing Clin Electrophysiol. 1997;20: Spach MS, Heidlage JF, Barr RC, Dolber PC. Cell size and communication: role in structural and electrical development and remodeling of the heart. Heart Rhythm. 2004;1: Moe GK, Abildskov JA. Atrial fibrillation as a self-sustaining arrhythmia independent of focal discharge. Am Heart J. 1959;58: Allessie M, Lammers W, Bonke F, Hollen J. Experimental evaluation of Moe's multiple wavelet hypothesis of atrial fibrillation. In: Cardiac Arrhythmias, eds Zipes D.P., J Jalife J Konings K, Kirchhof C, Smeets J, Wellens HJ, Penn OC, Allessie M. Highdensity mapping of electrically induced atrial fibrillation in humans. Circulation. 1994;89:
20 22. Eckstein J, Verheule S, de Groot N, Allessie M, Schotten U. Mechanisms of perpetuation of atrial fibrillation in chronically dilated atria. Prog Biophys Mol Biol. 2008;97: Everett THt, Wilson EE, Hulley GS, Olgin JE. Transmural characteristics of atrial fibrillation in canine models of structural and electrical atrial remodeling assessed by simultaneous epicardial and endocardial mapping. Heart Rhythm. 2010;7: Ho SY, Anderson RH, Sanchez-Quintana D. Atrial structure and fibres: morphologic bases of atrial conduction. Cardiovasc Res. 2002;54: Berenfeld O, Zaitsev A, Mironov S, Pertsov AM, Jalife J. Frequency-dependent breakdown of wave propagation into fibrillatory conduction across the pectinate muscle network in the isolated sheep right atrium. Circ Res. 2002;90: ;9 0: 26. Mandapati R, Skanes A, Chen J, Berenfeld O, Jalife J. Stable microreentrant sources as a mechanism of atrial fibrillation in the isolated sheep heart. Circulation. 2000;101: Everett THt, Wilson E, Verheule S, Guerra JM, Foreman S, Olgin J. Structural atrial remodeling alters the substrate and spatiotemporal organization n of atrial fibrillation. Am J Physiol Heart Circ Physiol. 2006;291:H
21 Figure Legends: Figure 1. Decreasing efficacy of pharmacological cardioversion. A) The success rate of pharmacological cardioversion (AVE dofetilide) decreased with time (white and gray bars: successful and failed cardioversion, respectively). Numbers above the bars denote the number of successful cardioversions and the number of goats tested. B) Over 6 months of AF, the baseline AFCL remained constant in awake goats. C) Representative example showing the effect of AVE0118 (10 mg/kg/h) and dofetilide (20 g/kg/h) on AFCL, gray arrows indicate cardioversion. Figure 2. Conduction velocity and AF cycle length. A) Examples of isochrone maps during pacing with a BCL of 400 ms (recorded after electrical cardioversion), illustrating the decreased CV in the LT LA. Distance between isochrones 10 ms. B) the CV at a BCL of 400 ms was significantly decreased in both atria of LT goats compared to ST goats. C) During AF, the average of the median AFCLs was not significantly different between ST and LT group for either atrium. D) The ST and LT groups did not show significant differences in beat-to-beat AFCL variability. In this and all subsequent graphs data points for the individual goats are shown (circles), along with the mean ± SEM (squares). *: P<0.05, **: P<0.01, ***: P< Figure 3. Conduction times. A) Representative examples of conduction time distributions during AF in an ST (left panel) and LT goat (right panel). In the LT goat, the distribution had a longer tail, indicating an increased incidence of long conduction 21
22 times. B) The average of the median conduction times (P50 of the distribution) was significantly increased in the LT group compared to the ST group in the LA, but not in the RA. C) The incidence of conduction block (conduction times > 12 ms) was significantly increased in the LT LA compared to the ST LA, and significantly larger in the LT RA compared to the ST RA. Figure 4. Activation patterns during AF in the LA of an ST goat. Representative example of isochronal maps recorded from the LA free wall during 4 consecutive beats of AF. In these beats, the recording area is activated by 3-5 waves, colored different shades of gray. Thin dashed lines indicate the boundaries of individual waves. White numbers indicate the starting time point of the waves. Peripheral waves are indicated by dashed arrows. Asterisks s denote epicardial breakthroughs. Discontinuous waves are indicated by a zigzag line (beat 4). Isochronal lines are separated by 5 ms. Figure 5. Activation patterns during AF in the LA of an LT goat. Representative example of isochronal maps recorded from the LA free wall during 4 consecutive beats of AF. In these beats, the recording area is activated by waves. Some discontinuous waves, indicated by white zigzag lines, are conducted from a wave in the previous beat window (e.g. the wave in the upper left quadrant in beat 2, starting at 40 ms). By contrast, a black zigzag line indicates discontinuous conduction from one wave to another within the beat shown. For further annotations see legend of figure 3. 22
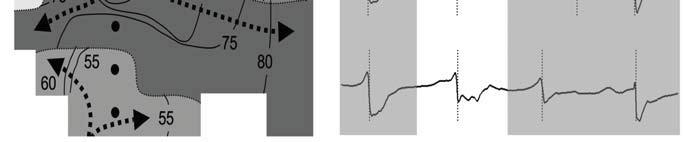
23 Figure 6. Dissociated conduction and epicardial breaktroughs in LT goats. A) Overview of waves during one beat of AF (highlighted in panel C) in the LA, for annotations see legend of figure 3. B) Detailed isochronal map of a part of the recording area (dashed box in A) illustrates dissociated conduction. This area was activated by several narrow waves propagating along various trajectories (dashed arrows) with large activation time differences between neighboring waves. The wave in the middle of this map originated as a discontinuous wave from the large epicardial breakthrough wave in the middle of the array. C) Electrograms recorded at the points indicated by black dots in B. Time points of activation are indicated by dashed vertical lines. Dissociated iate epicardial conduction is reflected in the asynchroneity of the activation timepoints. ints ts. D) In this example, the wave originating as a breakthrough on the left encounters an area of pronounced slow conduction before colliding with the wave that originated as a breakthrough on the right. A third breakthrough wave originates in the lower part of the array and collides with the other two breakthrough waves. E) Unipolar electrograms of the electrodes marked by dots in the panel D (electrograms from top to bottom correspond to dots from left to right). Figure 7. Number and types of fibrillation waves. A) The total number of fibrillation waves per AFCL was significantly higher in the LT group than in the ST group for both atria and significantly higher in the LT LA than in the LT RA. B) The number of peripheral waves was significantly increased in both atria of LT goats compared to ST goats and significantly larger in the LT LA than in the LT RA. C) The number of nonperipheral waves (i.e. waves appearing within the recording area away from the outer edge of the array) was significantly increased in both atria of the LT group. D) The ratio 23
24 between nonperipheral and peripheral waves was not significantly different between the ST and LT groups in either atrium. Figure 8. Endomysial fibrosis and myocyte hypertrophy. Examples of the epicardial side of toluidine blue stained sections of A) a ST goat, showing tightly packed myocytes, and B) a LT goat, showing increased myocyte width and endomysial fibrosis. There were significant increases in C) average myocyte-to-myocyte distance within bundles and D) Myocyte diameter (n=4 for ST LA and RA, n=5 for LT LA and RA). 24
 160 120 80 1 month 3 months 6 months 40-30 0 30 60-30 0 30 60-30 0 30 60 Time (min) Time (min) Time")
25 A C Succes Failure 120 (4/5) (2/6) Success (3/6) Failure (0/7) (0/7) (0/7) B Time (months) Time (months) AVE 0118 AVE 0118 AVE 0118 dofetilide dofetilide dofetilide 200 AFCL (ms) month 3 months 6 months Time (min) Time (min) Time (min)
 200 150 100 50 AFCL Irregularity (ms) 60 40 20 0 ST LT ST LT 0 ST LT ST LT RA LA")
26 A BB C 250 ST LA LAA AV groove LT LA B D CV (cm/s) * ** ST LT ST LT RA LA median AFCL (ms) AFCL Irregularity (ms) ST LT ST LT 0 ST LT ST LT RA LA RA LA
27 A ST LA LT LA B C Median Conduction time (ms) * ST LT ST LT Conduction Block (%) * *** ST LT ST LT RA LA RA LA
28
29




30 A B C D E

31 A Waves/ AFCL C * ** *** ST LT ST LT RA LA B D Peripheral Waves/ AFCL ** *** * ST LT ST LT RA LA Non-peripheral waves/ AFCL * *** ST LT ST LT Nonperipheral/Peripheral ST LT ST LT RA LA RA LA
 20 15 10 ST LT * * 5 0 RA LA 0")
32 A C B D 8 ST LT 25 myocyte distance (um) * * myocyte diameter (um) ST LT * * 5 0 RA LA 0 RA LA


33 Fibrillatory Conduction in the Atrial Free Walls of Goats in Persistent and Permanent Atrial Fibrillation Sander Verheule, Els Tuyls, Arne van Hunnik, Marion Kuiper, Ulrich Schotten and Maurits Allessie Circ Arrhythm Electrophysiol. published online October 11, 2010; Circulation: Arrhythmia and Electrophysiology is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX Copyright 2010 American Heart Association, Inc. All rights reserved. Print ISSN: Online ISSN: The online version of this article, along with updated information and services, is located on the World Wide Web at: Data Supplement (unedited) at: Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation: Arrhythmia and Electrophysiology can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answerdocument. Reprints: Information about reprints can be found online at: Subscriptions: Information about subscribing to Circulation: Arrhythmia and Electrophysiology is online at:
34 SUPPLEMENTAL MATERIAL Methods: Analysis of fibrillation patterns Using custom software, time points of maximum negative dv/dt were determined for each electrode to determine local activation times and construct activation time maps. Conduction velocity (CV) during pacing at a basic cycle length (BCL) of 400 ms was calculated as the average of local CVs determined by a vectorbased algorithm. For each recording location, 4-5 seconds of AF was analyzed in detail. AF cycle length (AFCL) was determined by measuring the time between consecutive activations at each electrode. The beat-to-beat variation in AFCL of successive beats were determined for each electrode. To quantify the width of the distribution of beatto-beat differences in AFCL, the range containing 60% of the AFCL variations within this distribution was denoted as the 'AFCL irregularity'. The distribution of conduction times was assessed by calculating the difference in activation time between each electrode and its neighbours. Conduction block was defined as a conduction time between adjacent electrodes >12 ms. For quantitative analysis of fibrillation patterns, activation time points were grouped into separate fibrillation waves. First, sites of earliest activation were identified that did not have preceding activation times in the immediately adjacent electrodes within 12 ms. From such a starting points of a wave, neighbouring electrodes were ascribed to that wave using an iterative procedure, by finding conduction times between adjacent electrodes 12 ms. With the interelectrode distance of 2.4 mm, this corresponds to a CV >20 cm/s. This limit of 12 ms was chosen because it represents the average value of the 95th percentile of the local
35 conduction time histogram in normal goats. Therefore, this value lies at the lower end of what can be considered activation by normal conduction. A starting point for a new wave was marked when its activation time was not preceded within 12 ms with ANY of its neighbors, making activation through normal conduction unlikely. Waves were defined as areas surrounded by lines of block (interelectrode conduction times >12 ms) or fusion (interelectrode conduction times 12 ms) everywhere along their boundaries within the recording array. Even with the complex fibrillation patterns observed in LT goats, waves were still comprised of multiple electrode positions, indicating that the interelectrode distance of 2.4 mm was sufficient to resolve individual waves. Wave maps were generated automatically by a computer algorithm applying these criteria and then independently checked and edited by two researchers. Depending on their origin, different types of fibrillation waves were distinguished: 'Peripheral waves' entering the mapping area from the outer edge of the array and 'non-peripheral waves' appearing at the epicardial surface inside the mapping area, excluding the outer edge. The non-peripheral waves were further subdivided in 'epicardial breakthroughs' and 'discontinuous waves'. An epicardial breakthrough was defined as a non-peripheral wave with a site of origin either not immediately adjacent to a previous wave or immediately adjacent to a previous waves, but with a delay larger than 50 ms. Thus, epicardial breakthroughs were characterized as the appearance of a wave in the recording area that could not be explained by propagating fibrillation waves present in the epicardial plane. 1 Discontinuous waves were defined as waves originating at the boundary of an earlier wave with a delay between 12 and 50 ms. The delay of >12 ms to the starting point of a discontinuous wave qualified as conduction block. For that reason, these events were qualified as separate fibrillation waves. Thus, discontinuous waves can be seen as a type of 'breakthrough', but one
36 that is closely linked in space and time to a previous epicardial wave. The incidence of all types of waves was normalized to the median AFCL of that AF episode. Examples of comparisons between conventional activation movies and 'waves movies' can be seen in the online supplemental movies. From such movies, consecutive time windows were selected and represented as 'wave maps', illustrating the starting points of waves within the recording array and the boundaries of these waves. In the areas within a wave boundary, activation time ischrones were drawn manually to illustrate propagation patterns of individual fibrillation waves (figures 3-5). Methods: Histology After electrophysiological studies, hearts were excised and fixed in zinc acetate buffered formalin solution (4%, ph 5.5). The fixated atria were embedded in plastic resin (Technovit 7100, Heraeus Kulzer). Transverse sections (5µm) were stained with toluidine blue. For quantitative analysis, photographs were taken at 200x magnification. The diameter of the atrial myocytes was measured in myocytes with the nucleus in plane of the section. Endomysial fibrosis was defined as connective tissue separating individual myocytes within bundles. The width of endomysial tissue septa was quantified as the distance between myocytes within bundles. Legend to Supplemental Movies. Movies showing LA fibrillation patterns in a representative ST and LT goat. The left panels show a normal activation movie, the right panels show the corresponding 'wave map'. Fibrillatory conduction was substantially more dissociated
37 in the LT LA than in the ST LA. Gray circles indicate peripheral waves, white stars represent epicardial breakthroughs and white arrows denote discontinuous waves. References 1. de Groot NMS, Houben RM, Klautz R, Braun J, Smeets JLRM, Allessie MA, Schalij MJ. Comparison of epicardial breakthrough of fibrillation waves between patients with acute and chronic atrial fibrillation. In: Thesis, Leiden University, ISBN :
Reentry in a Pulmonary Vein as a Possible Mechanism of Focal Atrial Fibrillation
 824 Reentry in a Pulmonary Vein as a Possible Mechanism of Focal Atrial Fibrillation BERNARD BELHASSEN, M.D., AHARON GLICK, M.D., and SAMI VISKIN, M.D. From the Department of Cardiology, Tel-Aviv Sourasky
824 Reentry in a Pulmonary Vein as a Possible Mechanism of Focal Atrial Fibrillation BERNARD BELHASSEN, M.D., AHARON GLICK, M.D., and SAMI VISKIN, M.D. From the Department of Cardiology, Tel-Aviv Sourasky
Electropathological Substrate of Long-Standing Persistent Atrial Fibrillation in Patients With Structural Heart Disease Longitudinal Dissociation
 Electropathological Substrate of Long-Standing Persistent Atrial Fibrillation in Patients With Structural Heart Disease Longitudinal Dissociation Maurits A. Allessie, MD, PhD; Natasja M.S. de Groot, MD,
Electropathological Substrate of Long-Standing Persistent Atrial Fibrillation in Patients With Structural Heart Disease Longitudinal Dissociation Maurits A. Allessie, MD, PhD; Natasja M.S. de Groot, MD,
PDF hosted at the Radboud Repository of the Radboud University Nijmegen
 PDF hosted at the Radboud Repository of the Radboud University Nijmegen The following full text is a publisher's version. For additional information about this publication click this link. http://hdl.handle.net/2066/88723
PDF hosted at the Radboud Repository of the Radboud University Nijmegen The following full text is a publisher's version. For additional information about this publication click this link. http://hdl.handle.net/2066/88723
Long-Standing Persistent Atrial Fibrillation: Can We Distinguish Ectopic Activity From Reentry by Epicardial Mapping?
 Long-Standing Persistent Atrial Fibrillation: Can We Distinguish Ectopic Activity From Reentry by Epicardial Mapping? Running title: de Bakker et al.; Can epicardial mapping reveal the AF mechanism? Jacques
Long-Standing Persistent Atrial Fibrillation: Can We Distinguish Ectopic Activity From Reentry by Epicardial Mapping? Running title: de Bakker et al.; Can epicardial mapping reveal the AF mechanism? Jacques
The Regional Distribution and Correlation. Complex Fractionated Atrial Electrograms and Dominant Frequency in. during Atrial Fibrillation
 Original Article Complex Fractionated Atrial Electrograms and Dominant Frequency in Acta Atrial Cardiol Fibrillation Sin 2011;27:174 81 Electrophysiology The Regional Distribution and Correlation between
Original Article Complex Fractionated Atrial Electrograms and Dominant Frequency in Acta Atrial Cardiol Fibrillation Sin 2011;27:174 81 Electrophysiology The Regional Distribution and Correlation between
FREQUENCY COHERENCE MAPPING OF CANINE ATRIAL FIBRILLATION: IMPLICATION FOR ANTI-ARRHYTHMIC DRUG-INDUCED TERMINATION
 56 Vol. 5 No. 2 April 2003 FREQUENCY COHERENCE MAPPING OF CANINE ATRIAL FIBRILLATION: IMPLICATION FOR ANTI-ARRHYTHMIC DRUG-INDUCED TERMINATION HAN-WEN TSO', TSAIR KAO', SHIH-AMN CHEN 2, CHING-TAI TAI\
56 Vol. 5 No. 2 April 2003 FREQUENCY COHERENCE MAPPING OF CANINE ATRIAL FIBRILLATION: IMPLICATION FOR ANTI-ARRHYTHMIC DRUG-INDUCED TERMINATION HAN-WEN TSO', TSAIR KAO', SHIH-AMN CHEN 2, CHING-TAI TAI\
Electrophysiologic Properties of Pulmonary Veins Assessed Using a Multielectrode Basket Catheter
 Journal of the American College of Cardiology Vol. 43, No. 12, 2004 2004 by the American College of Cardiology Foundation ISSN 0735-1097/04/$30.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2004.01.051
Journal of the American College of Cardiology Vol. 43, No. 12, 2004 2004 by the American College of Cardiology Foundation ISSN 0735-1097/04/$30.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2004.01.051
High-Densiy Mapping of Electrically Induced Atrial Fibrillation in Humans
 1665 High-Densiy Mapping of Electrically Induced Atrial Fibrillation in Humans Karen T.S. Konings, MD; Charles J.H.J. Kirchhof, MD, PhD; Joep R.L.M. Smeets, MD, PhD; Hein J.J. Wellens, MD, PhD; Olaf C.
1665 High-Densiy Mapping of Electrically Induced Atrial Fibrillation in Humans Karen T.S. Konings, MD; Charles J.H.J. Kirchhof, MD, PhD; Joep R.L.M. Smeets, MD, PhD; Hein J.J. Wellens, MD, PhD; Olaf C.
Atrial fibrillation (AF) has a progressive character, with
 has a progressive character, with") Reverse Structural and Gap-Junctional Remodeling After Prolonged Atrial Fibrillation in the Goat Jannie Ausma, PhD; Huub M.W. van der Velden, PhD; Marie-Hélène Lenders, BSc; Erwin P. van Ankeren, BSc;
Reverse Structural and Gap-Junctional Remodeling After Prolonged Atrial Fibrillation in the Goat Jannie Ausma, PhD; Huub M.W. van der Velden, PhD; Marie-Hélène Lenders, BSc; Erwin P. van Ankeren, BSc;
Mechanism of Immediate Recurrences of Atrial Fibrillation After Restoration of Sinus Rhythm
 Mechanism of Immediate Recurrences of Atrial Fibrillation After Restoration of Sinus Rhythm AMAN CHUGH, MEHMET OZAYDIN, CHRISTOPH SCHARF, STEVE W.K. LAI, BURR HALL, PETER CHEUNG, FRANK PELOSI, JR, BRADLEY
Mechanism of Immediate Recurrences of Atrial Fibrillation After Restoration of Sinus Rhythm AMAN CHUGH, MEHMET OZAYDIN, CHRISTOPH SCHARF, STEVE W.K. LAI, BURR HALL, PETER CHEUNG, FRANK PELOSI, JR, BRADLEY
Changes in the Atrial Substrate Alters the Spatiotemporal Organization and Characteristics of Atrial Fibrillation
 Changes in the Atrial Substrate Alters the Spatiotemporal Organization and Characteristics of Atrial Fibrillation 3 Thomas H. Everett Division of Cardiology, Department of Medicine, University of California
Changes in the Atrial Substrate Alters the Spatiotemporal Organization and Characteristics of Atrial Fibrillation 3 Thomas H. Everett Division of Cardiology, Department of Medicine, University of California
Influences of Anisotropic Tissue Structure on Reentrant Circuits in the Epicardial Border Zone of Subacute Canine Infarcts
 182 Influences of Anisotropic Tissue Structure on Reentrant Circuits in the Epicardial Border Zone of Subacute Canine Infarcts Stephen M. Dillon, Maurits A. Allessie, Philip C. Ursell, and Andrew L. Wit
182 Influences of Anisotropic Tissue Structure on Reentrant Circuits in the Epicardial Border Zone of Subacute Canine Infarcts Stephen M. Dillon, Maurits A. Allessie, Philip C. Ursell, and Andrew L. Wit
Wavelength and vulnerability to atrial fibrillation: Insights from a computer model of human atria
 Europace (2005) 7, S83eS92 Wavelength and vulnerability to atrial fibrillation: Insights from a computer model of human atria Vincent Jacquemet a, *, Nathalie Virag b, Lukas Kappenberger c a Signal Processing
Europace (2005) 7, S83eS92 Wavelength and vulnerability to atrial fibrillation: Insights from a computer model of human atria Vincent Jacquemet a, *, Nathalie Virag b, Lukas Kappenberger c a Signal Processing
It has been demonstrated in animal models that chronic
 Pulmonary Veins and Ligament of Marshall as Sources of Rapid Activations in a Canine Model of Sustained Atrial Fibrillation Tsu-Juey Wu, MD; James J.C. Ong, MD; Che-Ming Chang, MD; Rahul N. Doshi, MD;
Pulmonary Veins and Ligament of Marshall as Sources of Rapid Activations in a Canine Model of Sustained Atrial Fibrillation Tsu-Juey Wu, MD; James J.C. Ong, MD; Che-Ming Chang, MD; Rahul N. Doshi, MD;
Deposited on: 29 October 2009
 Workman, A.J. (2009) Mechanisms of postcardiac surgery atrial fibrillation: more pieces in a difficult puzzle. Heart Rhythm, 6 (10). pp. 1423-1424. ISSN 1547-5271 http://eprints.gla.ac.uk/7847/ Deposited
Workman, A.J. (2009) Mechanisms of postcardiac surgery atrial fibrillation: more pieces in a difficult puzzle. Heart Rhythm, 6 (10). pp. 1423-1424. ISSN 1547-5271 http://eprints.gla.ac.uk/7847/ Deposited
Original Article Structural changes in the progression of atrial fibrillation: potential role of glycogen and fibrosis as perpetuating factors
 Int J Clin Exp Pathol 2015;8(2):1712-1718 www.ijcep.com /ISSN:1936-2625/IJCEP0004433 Original Article Structural changes in the progression of atrial fibrillation: potential role of glycogen and fibrosis
Int J Clin Exp Pathol 2015;8(2):1712-1718 www.ijcep.com /ISSN:1936-2625/IJCEP0004433 Original Article Structural changes in the progression of atrial fibrillation: potential role of glycogen and fibrosis
Atrial Fibrillation: Classification and Electrophysiology. Saverio Iacopino, MD, FACC, FESC
 Atrial Fibrillation: Classification and Electrophysiology Saverio Iacopino, MD, FACC, FESC Sinus Rythm Afib (first episode) AFib Paroxistic AFib Spontaneous conversion Permanent AFib Recurrence Sinus Rythm
Atrial Fibrillation: Classification and Electrophysiology Saverio Iacopino, MD, FACC, FESC Sinus Rythm Afib (first episode) AFib Paroxistic AFib Spontaneous conversion Permanent AFib Recurrence Sinus Rythm
CARDIOLOGY GRAND ROUNDS
 CARDIOLOGY GRAND ROUNDS Title: Controversies in AF ablation, pros/cons, LT outcomes Speaker: Bruce D. Lindsay Section Head, Clinical Cardiac Electrophysiology, Vice-Chair Cardiology Cleveland Clinic Date:
CARDIOLOGY GRAND ROUNDS Title: Controversies in AF ablation, pros/cons, LT outcomes Speaker: Bruce D. Lindsay Section Head, Clinical Cardiac Electrophysiology, Vice-Chair Cardiology Cleveland Clinic Date:
State of the Art. Atrial Fibrillation: A Question of Dominance?
 State of the Art Hellenic J Cardiol 45: 345-358, 2004 Atrial Fibrillation: A Question of Dominance? JOSÉ JALIFE, OMER BERENFELD Institute for Cardiovascular Research and Department of Pharmacology, SUNY
State of the Art Hellenic J Cardiol 45: 345-358, 2004 Atrial Fibrillation: A Question of Dominance? JOSÉ JALIFE, OMER BERENFELD Institute for Cardiovascular Research and Department of Pharmacology, SUNY
Catheter ablation of AF Where do we stand, where do we go?
 Catheter ablation of AF Where do we stand, where do we go? Sébastien Knecht MD, PhD Hôpital cardiologique du Haut L Evêque, Bordeaux Declaration of conflict of interest ABLATION STRATEGIES Duration proc:
Catheter ablation of AF Where do we stand, where do we go? Sébastien Knecht MD, PhD Hôpital cardiologique du Haut L Evêque, Bordeaux Declaration of conflict of interest ABLATION STRATEGIES Duration proc:
University of Groningen. Atrial remodeling due to atrial tachycardia and heart failure Schoonderwoerd, Bas Arjan
 University of Groningen Atrial remodeling due to atrial tachycardia and heart failure Schoonderwoerd, Bas Arjan IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you
University of Groningen Atrial remodeling due to atrial tachycardia and heart failure Schoonderwoerd, Bas Arjan IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you
QUest for the Arrhythmogenic Substrate of Atrial fibrillation in Patients Undergoing Cardiac Surgery (QUASAR Study): Rationale and Design
: Rationale and Design") J. of Cardiovasc. Trans. Res. (2016) 9:194 201 DOI 10.1007/s12265-016-9685-1 METHODS PAPER QUest for the Arrhythmogenic Substrate of Atrial fibrillation in Patients Undergoing Cardiac Surgery (QUASAR Study):
J. of Cardiovasc. Trans. Res. (2016) 9:194 201 DOI 10.1007/s12265-016-9685-1 METHODS PAPER QUest for the Arrhythmogenic Substrate of Atrial fibrillation in Patients Undergoing Cardiac Surgery (QUASAR Study):
Microstructural Basis of Conduction II Introduction to Experimental Studies
 Bioeng 6460 Electrophysiology and Bioelectricity Microstructural Basis of Conduction II Introduction to Experimental Studies Frank B. Sachse fs@cvrti.utah.edu Overview Microstructural Basis of Conduction
Bioeng 6460 Electrophysiology and Bioelectricity Microstructural Basis of Conduction II Introduction to Experimental Studies Frank B. Sachse fs@cvrti.utah.edu Overview Microstructural Basis of Conduction
Characteristics of Rapid Rhythms Recorded Within Pulmonary Veins During Atrial Fibrillation
 Characteristics of Rapid Rhythms Recorded Within Pulmonary Veins During Atrial Fibrillation HIROSHI TADA, MEHMET ÖZAYDIN, HAKAN ORAL, BRADLEY P. KNIGHT, AMAN CHUGH, CHRISTOPH SCHARF, FRANK PELOSI, Jr.,
Characteristics of Rapid Rhythms Recorded Within Pulmonary Veins During Atrial Fibrillation HIROSHI TADA, MEHMET ÖZAYDIN, HAKAN ORAL, BRADLEY P. KNIGHT, AMAN CHUGH, CHRISTOPH SCHARF, FRANK PELOSI, Jr.,
AF ABLATION Concepts and Techniques
 AF ABLATION Concepts and Techniques Antony F Chu, M.D. Director of Complex Ablation Arrhythmia Services Section Division of Cardiology at the Rhode Island and Miriam Hospital HIGHLIGHTS The main indications
AF ABLATION Concepts and Techniques Antony F Chu, M.D. Director of Complex Ablation Arrhythmia Services Section Division of Cardiology at the Rhode Island and Miriam Hospital HIGHLIGHTS The main indications
Peri-Mitral Atrial Flutter with Partial Conduction Block between Left Atrium and Coronary Sinus
 Accepted Manuscript Peri-Mitral Atrial Flutter with Partial Conduction Block between Left Atrium and Coronary Sinus Ryota Isogai, MD, Seiichiro Matsuo, MD, Ryohsuke Narui, MD, Shingo Seki, MD;, Michihiro
Accepted Manuscript Peri-Mitral Atrial Flutter with Partial Conduction Block between Left Atrium and Coronary Sinus Ryota Isogai, MD, Seiichiro Matsuo, MD, Ryohsuke Narui, MD, Shingo Seki, MD;, Michihiro
From the Division of Cardiology, Department of Internal Medicine, University of Michigan Medical Center, Ann Arbor, Michigan
 118 Reprinted with permission from JOURNAL OF CARDIOVASCULAR ELECTROPHYSIOLOGY, Volume 13, No. 2, February 2002 Copyright 2002 by Futura Publishing Company, Inc., Armonk, NY 10504-0418 Differentiation
118 Reprinted with permission from JOURNAL OF CARDIOVASCULAR ELECTROPHYSIOLOGY, Volume 13, No. 2, February 2002 Copyright 2002 by Futura Publishing Company, Inc., Armonk, NY 10504-0418 Differentiation
Chapter 16: Arrhythmias and Conduction Disturbances
 Complete the following. Chapter 16: Arrhythmias and Conduction Disturbances 1. Cardiac arrhythmias result from abnormal impulse, abnormal impulse, or both mechanisms together. 2. is the ability of certain
Complete the following. Chapter 16: Arrhythmias and Conduction Disturbances 1. Cardiac arrhythmias result from abnormal impulse, abnormal impulse, or both mechanisms together. 2. is the ability of certain
CARDIOINSIGHT TM NONINVASIVE 3D MAPPING SYSTEM CLINICAL EVIDENCE SUMMARY
 CARDIOINSIGHT TM NONINVASIVE 3D MAPPING SYSTEM CLINICAL EVIDENCE SUMMARY April 2017 SUPPORTING EVIDENCE RHYTHM AF VT PUBLICATIONS Driver Domains in Persistent Atrial Fibrillation (Haissaiguerre, et al)
CARDIOINSIGHT TM NONINVASIVE 3D MAPPING SYSTEM CLINICAL EVIDENCE SUMMARY April 2017 SUPPORTING EVIDENCE RHYTHM AF VT PUBLICATIONS Driver Domains in Persistent Atrial Fibrillation (Haissaiguerre, et al)
Progression of atrial fibrillation: can we prevent it? Early catheter ablation will stop progression of atrial fibrillation pro
 Progression of atrial fibrillation: can we prevent it? Early catheter ablation will stop progression of atrial fibrillation pro Jerónimo Farré MD, Madrid, ES AF: the kingdom of wishful thinking In AF we
Progression of atrial fibrillation: can we prevent it? Early catheter ablation will stop progression of atrial fibrillation pro Jerónimo Farré MD, Madrid, ES AF: the kingdom of wishful thinking In AF we
From the Imperial College Healthcare NHS Trust, London, UK
 1224 Stimulation of the Intrinsic Cardiac Autonomic Nervous System Results in a Gradient of Fibrillatory Cycle Length Shortening Across the Atria During Atrial Fibrillation in Humans PHANG BOON LIM, M.A.,
1224 Stimulation of the Intrinsic Cardiac Autonomic Nervous System Results in a Gradient of Fibrillatory Cycle Length Shortening Across the Atria During Atrial Fibrillation in Humans PHANG BOON LIM, M.A.,
Contemporary Strategies for Catheter Ablation of Atrial Fibrillation
 Contemporary Strategies for Catheter Ablation of Atrial Fibrillation Suneet Mittal, MD Director, Electrophysiology Medical Director, Snyder Center for Atrial Fibrillation The Arrhythmia Institute at The
Contemporary Strategies for Catheter Ablation of Atrial Fibrillation Suneet Mittal, MD Director, Electrophysiology Medical Director, Snyder Center for Atrial Fibrillation The Arrhythmia Institute at The
Electrical disconnection of pulmonary vein (PV) myocardium
 myocardium") Left Atrial Appendage Activity Masquerading as Pulmonary Vein Potentials Dipen Shah, MD; Michel Haissaguerre, MD; Pierre Jais, MD; Meleze Hocini, MD; Teiichi Yamane, MD; Laurent Macle, MD; Kee Joon Choi,
Left Atrial Appendage Activity Masquerading as Pulmonary Vein Potentials Dipen Shah, MD; Michel Haissaguerre, MD; Pierre Jais, MD; Meleze Hocini, MD; Teiichi Yamane, MD; Laurent Macle, MD; Kee Joon Choi,
The role of the hyperpolarization-activated inward current f in arrhythmogenesis: a computer model study
 1 The role of the hyperpolarization-activated inward current f in arrhythmogenesis: a computer model study Nico H.L. Kuijpers, Rikkert H. Keldermann, Huub M.M. ten Eikelder, Theo Arts, and Peter A.J. Hilbers
1 The role of the hyperpolarization-activated inward current f in arrhythmogenesis: a computer model study Nico H.L. Kuijpers, Rikkert H. Keldermann, Huub M.M. ten Eikelder, Theo Arts, and Peter A.J. Hilbers
Journal of the American College of Cardiology Vol. 37, No. 5, by the American College of Cardiology ISSN /01/$20.
 Journal of the American College of Cardiology Vol. 37, No. 5, 2001 2001 by the American College of Cardiology ISSN 0735-1097/01/$20.00 Published by Elsevier Science Inc. PII S0735-1097(01)01132-9 Increased
Journal of the American College of Cardiology Vol. 37, No. 5, 2001 2001 by the American College of Cardiology ISSN 0735-1097/01/$20.00 Published by Elsevier Science Inc. PII S0735-1097(01)01132-9 Increased
Journal of the American College of Cardiology Vol. 42, No. 2, by the American College of Cardiology Foundation ISSN /03/$30.
 Journal of the American College of Cardiology Vol. 42, No. 2, 2003 2003 by the American College of Cardiology Foundation ISSN 0735-1097/03/$30.00 Published by Elsevier Inc. doi:10.1016/s0735-1097(03)00586-2
Journal of the American College of Cardiology Vol. 42, No. 2, 2003 2003 by the American College of Cardiology Foundation ISSN 0735-1097/03/$30.00 Published by Elsevier Inc. doi:10.1016/s0735-1097(03)00586-2
Arrhythmia/Electrophysiology. Remodeling of Sinus Node Function in Patients With Congestive Heart Failure. Reduction in Sinus Node Reserve
 Arrhythmia/Electrophysiology Remodeling of Sinus Node Function in Patients With Congestive Heart Failure Reduction in Sinus Node Reserve Prashanthan Sanders, MBBS, PhD; Peter M. Kistler, MBBS; Joseph B.
Arrhythmia/Electrophysiology Remodeling of Sinus Node Function in Patients With Congestive Heart Failure Reduction in Sinus Node Reserve Prashanthan Sanders, MBBS, PhD; Peter M. Kistler, MBBS; Joseph B.
How to ablate typical atrial flutter
 Europace (1999) 1, 151 155 HOW TO... SERIES How to ablate typical atrial flutter A. Takahashi, D. C. Shah, P. Jaïs and M. Haïssaguerre Electrophysiologie Cardiaque, Hopital Cardiologique du Haut-Lévêque,
Europace (1999) 1, 151 155 HOW TO... SERIES How to ablate typical atrial flutter A. Takahashi, D. C. Shah, P. Jaïs and M. Haïssaguerre Electrophysiologie Cardiaque, Hopital Cardiologique du Haut-Lévêque,
Pathogenesis of atrial fibrillation
 Chapter 2 Pathogenesis of atrial fibrillation Mechanism of atrial fibrillation The mechanism of atrial fibrillation (AF) is still debatable. Several mechanisms have been proposed and seen in a variety
Chapter 2 Pathogenesis of atrial fibrillation Mechanism of atrial fibrillation The mechanism of atrial fibrillation (AF) is still debatable. Several mechanisms have been proposed and seen in a variety
A MODEL OF GAP JUNCTION CONDUCTANCE AND VENTRICULAR TACHYARRHYTHMIA
 A MODEL OF GAP JUNCTION CONDUCTANCE AND VENTRICULAR TACHYARRHYTHMIA X. D. Wu, Y. L. Shen, J. L. Bao, C. M. Cao, W. H. Xu, Q. Xia Department of Physiology, Zhejiang University School of Medicine, Hangzhou,
A MODEL OF GAP JUNCTION CONDUCTANCE AND VENTRICULAR TACHYARRHYTHMIA X. D. Wu, Y. L. Shen, J. L. Bao, C. M. Cao, W. H. Xu, Q. Xia Department of Physiology, Zhejiang University School of Medicine, Hangzhou,
Hunter, Ross J. For additional information about this publication click this link.
 Catheter ablation of fractionated electrograms for atrial fibrillation: does it improve outcomes and can it be refined based on electrogram morphology or knowledge of the remodelling process?. Hunter,
Catheter ablation of fractionated electrograms for atrial fibrillation: does it improve outcomes and can it be refined based on electrogram morphology or knowledge of the remodelling process?. Hunter,
ECG. Prepared by: Dr.Fatima Daoud Reference: Guyton and Hall Textbook of Medical Physiology,12 th edition Chapters: 11,12,13
 ECG Prepared by: Dr.Fatima Daoud Reference: Guyton and Hall Textbook of Medical Physiology,12 th edition Chapters: 11,12,13 The Concept When the cardiac impulse passes through the heart, electrical current
ECG Prepared by: Dr.Fatima Daoud Reference: Guyton and Hall Textbook of Medical Physiology,12 th edition Chapters: 11,12,13 The Concept When the cardiac impulse passes through the heart, electrical current
Antifibrotic Therapy Delays Progression from Paroxysmal to Persistent Atrial Fibrillation
 Antifibrotic Therapy Delays Progression from Paroxysmal to Persistent Atrial Fibrillation José Jalife, M.D. Center for Arrhythmia Research University of Michigan No Disclosures The mechanisms that maintain
Antifibrotic Therapy Delays Progression from Paroxysmal to Persistent Atrial Fibrillation José Jalife, M.D. Center for Arrhythmia Research University of Michigan No Disclosures The mechanisms that maintain
Circulation: Arrhythmia and Electrophysiology CHALLENGE OF THE WEEK
 A 14-year-old girl with Wolff-Parkinson-White syndrome and recurrent paroxysmal palpitations due to atrioventricular reentry tachycardia had undergone two prior failed left lateral accessory pathway ablations
A 14-year-old girl with Wolff-Parkinson-White syndrome and recurrent paroxysmal palpitations due to atrioventricular reentry tachycardia had undergone two prior failed left lateral accessory pathway ablations
Use of Conventional Dual Chamber Pacemakers With Custom Lead Adapters to Induce Atrial Fibrillation or Heart Failure in Dogs
 Use of Conventional Dual Chamber Pacemakers With Custom Lead Adapters to Induce Atrial Fibrillation or Heart Failure in Dogs Faruk Cingoz, MD, George Yanulis, MS, Elizabeth Ching, RN, Kiyotaka Fukamachi,
Use of Conventional Dual Chamber Pacemakers With Custom Lead Adapters to Induce Atrial Fibrillation or Heart Failure in Dogs Faruk Cingoz, MD, George Yanulis, MS, Elizabeth Ching, RN, Kiyotaka Fukamachi,
Atrial fibrillation (AF) is the most common arrhythmia in
 is the most common arrhythmia in") Distinctive Electrophysiological Properties of Pulmonary Veins in Patients With Atrial Fibrillation Pierre Jaïs, MD; Mélèze Hocini, MD; Laurent Macle, MD; Kee-Joon Choi, MD; Isabel Deisenhofer, MD; Rukshen
Distinctive Electrophysiological Properties of Pulmonary Veins in Patients With Atrial Fibrillation Pierre Jaïs, MD; Mélèze Hocini, MD; Laurent Macle, MD; Kee-Joon Choi, MD; Isabel Deisenhofer, MD; Rukshen
Both atrial tachycardia and congestive heart failure (CHF)
") Contrasting Efficacy of Dofetilide in Differing Experimental Models of Atrial Fibrillation Danshi Li, MD, PhD; Agnes Bénardeau, PhD; Stanley Nattel, MD Background Rapid atrial pacing (RAP) and congestive
Contrasting Efficacy of Dofetilide in Differing Experimental Models of Atrial Fibrillation Danshi Li, MD, PhD; Agnes Bénardeau, PhD; Stanley Nattel, MD Background Rapid atrial pacing (RAP) and congestive
Use of Catheter Ablation in the Treatment of Ventricular Tachycardia Triggered by Premature Ventricular Contraction
 J Arrhythmia Vol 22 No 3 2006 Case Report Use of Catheter Ablation in the Treatment of Ventricular Tachycardia Triggered by Premature Ventricular Contraction sao Kato MD, Toru wa MD, Yasushi Suzuki MD,
J Arrhythmia Vol 22 No 3 2006 Case Report Use of Catheter Ablation in the Treatment of Ventricular Tachycardia Triggered by Premature Ventricular Contraction sao Kato MD, Toru wa MD, Yasushi Suzuki MD,
Mapping Cardiac Pacemaker Circuits: Methodological puzzles of SAN optical mapping
 Mapping Cardiac Pacemaker Circuits: Methodological puzzles of SAN optical mapping Igor R. Efimov, Vadim V. Fedorov, Boyoung Joung, and Shien-Fong Lin Journal of American College of Cardiology, 66(18):1976-86,
Mapping Cardiac Pacemaker Circuits: Methodological puzzles of SAN optical mapping Igor R. Efimov, Vadim V. Fedorov, Boyoung Joung, and Shien-Fong Lin Journal of American College of Cardiology, 66(18):1976-86,
Abrupt changes in fibrillatory wave characteristics at the termination of paroxysmal atrial fibrillation in humans
 Europace (2007) 9, 466 470 doi:10.1093/europace/eum096 Abrupt changes in fibrillatory wave characteristics at the termination of paroxysmal atrial fibrillation in humans Simona Petrutiu 1,3, Alan V. Sahakian
Europace (2007) 9, 466 470 doi:10.1093/europace/eum096 Abrupt changes in fibrillatory wave characteristics at the termination of paroxysmal atrial fibrillation in humans Simona Petrutiu 1,3, Alan V. Sahakian
A Dynamic model of Pulmonary Vein Electrophysiology. Harry Green 2 nd year Ph.D. student University of Exeter
 A Dynamic model of Pulmonary Vein Electrophysiology Harry Green 2 nd year Ph.D. student University of Exeter Background to the Project Cardiac disease is the leading cause of death in most developed countries
A Dynamic model of Pulmonary Vein Electrophysiology Harry Green 2 nd year Ph.D. student University of Exeter Background to the Project Cardiac disease is the leading cause of death in most developed countries
Catheter Ablation: Atrial fibrillation (AF) is the most common. Another Option for AF FAQ. Who performs ablation for treatment of AF?
 is the most common. Another Option for AF FAQ. Who performs ablation for treatment of AF?") : Another Option for AF Atrial fibrillation (AF) is a highly common cardiac arrhythmia and a major risk factor for stroke. In this article, Dr. Khan and Dr. Skanes detail how catheter ablation significantly
: Another Option for AF Atrial fibrillation (AF) is a highly common cardiac arrhythmia and a major risk factor for stroke. In this article, Dr. Khan and Dr. Skanes detail how catheter ablation significantly
Electrophysiology 101: What Do Surgeons Need to Know. Richard B Schuessler PhD
 Electrophysiology 101: What Do Surgeons Need to Know Richard B Schuessler PhD Disclosures Research Grant from Atricure, Inc. Arrhythmias Where The Surgical Approach Has Been Used WPW AVNRT Automatic Ectopic
Electrophysiology 101: What Do Surgeons Need to Know Richard B Schuessler PhD Disclosures Research Grant from Atricure, Inc. Arrhythmias Where The Surgical Approach Has Been Used WPW AVNRT Automatic Ectopic
480 April 2004 PACE, Vol. 27
 Incremental Value of Isolating the Right Inferior Pulmonary Vein During Pulmonary Vein Isolation Procedures in Patients With Paroxysmal Atrial Fibrillation HAKAN ORAL, AMAN CHUGH, CHRISTOPH SCHARF, BURR
Incremental Value of Isolating the Right Inferior Pulmonary Vein During Pulmonary Vein Isolation Procedures in Patients With Paroxysmal Atrial Fibrillation HAKAN ORAL, AMAN CHUGH, CHRISTOPH SCHARF, BURR
Stretching Cardiac Myocytes: A Finite Element Model of Cardiac Tissue
 Megan McCain ES240 FEM Final Project December 19, 2006 Stretching Cardiac Myocytes: A Finite Element Model of Cardiac Tissue Cardiac myocytes are the cells that constitute the working muscle of the heart.
Megan McCain ES240 FEM Final Project December 19, 2006 Stretching Cardiac Myocytes: A Finite Element Model of Cardiac Tissue Cardiac myocytes are the cells that constitute the working muscle of the heart.
Original Article The effect of ranolazine on maintaining sinus rhythm in patients with resistant atrial fibrillation
 www.ipej.org 175 Original Article The effect of ranolazine on maintaining sinus rhythm in patients with resistant atrial fibrillation David K. Murdock, MD, Naomi Overton, MD, Mary Kersten RN, Jeff Kaliebe,
www.ipej.org 175 Original Article The effect of ranolazine on maintaining sinus rhythm in patients with resistant atrial fibrillation David K. Murdock, MD, Naomi Overton, MD, Mary Kersten RN, Jeff Kaliebe,
V. TACHYCARDIAS Rapid rhythm abnormalities
 V. TACHYCARDIAS Rapid rhythm abnormalities Tachyarrhythmias currently account for up to 350,000 deaths annually in the US. In addition to these clearly dangerous rhythm disturbances, other forms of more
V. TACHYCARDIAS Rapid rhythm abnormalities Tachyarrhythmias currently account for up to 350,000 deaths annually in the US. In addition to these clearly dangerous rhythm disturbances, other forms of more
EHRA/EUROPACE 2011 Madrid, Spain June
 EHRA/EUROPACE 2011 Madrid, Spain June 26.-29.2011 Implementing modern management in atrial fibrillation patients Proceedings from the 3rd AFNet/EHRA consensus conference EHRA Special Session Different
EHRA/EUROPACE 2011 Madrid, Spain June 26.-29.2011 Implementing modern management in atrial fibrillation patients Proceedings from the 3rd AFNet/EHRA consensus conference EHRA Special Session Different
Evidence for Longitudinal and Transverse Fiber Conduction in Human Pulmonary Veins
 Evidence for Longitudinal and Transverse Fiber Conduction in Human Pulmonary Veins Relevance for Catheter Ablation Javier E. Sanchez, MD; Vance J. Plumb, MD; Andrew E. Epstein, MD; G. Neal Kay, MD Background
Evidence for Longitudinal and Transverse Fiber Conduction in Human Pulmonary Veins Relevance for Catheter Ablation Javier E. Sanchez, MD; Vance J. Plumb, MD; Andrew E. Epstein, MD; G. Neal Kay, MD Background
Ablation of persistent AF Is it different than paroxysmal?
 Ablation of persistent AF Is it different than paroxysmal? Steven J. Kalbfleisch, MD Medical Director Electrophysiology Laboratory Ohio State University Wexner Medical Center Ross Heart Hospital Columbus,
Ablation of persistent AF Is it different than paroxysmal? Steven J. Kalbfleisch, MD Medical Director Electrophysiology Laboratory Ohio State University Wexner Medical Center Ross Heart Hospital Columbus,
Tachycardia-induced heart failure - Does it exist?
 Tachycardia-induced heart failure - Does it exist? PD Dr Etienne Delacrétaz Clinique Cecil et Hôpital de Fribourg SSC Cardiology meeting 2015 Zürich Rapid atrial fibrillation is a common cause of heart
Tachycardia-induced heart failure - Does it exist? PD Dr Etienne Delacrétaz Clinique Cecil et Hôpital de Fribourg SSC Cardiology meeting 2015 Zürich Rapid atrial fibrillation is a common cause of heart
New Parameter to Predict Recurrence of Paroxysmal Atrial Fibrillation after Pulmonary Vein Isolation by the P-Wave Signal-Averaged Electrocardiogram
 Showa Univ J Med Sci 29 2, 141 150, June 2017 Original New Parameter to Predict Recurrence of Paroxysmal Atrial Fibrillation after Pulmonary Vein Isolation by the P-Wave Signal-Averaged Electrocardiogram
Showa Univ J Med Sci 29 2, 141 150, June 2017 Original New Parameter to Predict Recurrence of Paroxysmal Atrial Fibrillation after Pulmonary Vein Isolation by the P-Wave Signal-Averaged Electrocardiogram
Is cardioversion old hat? What is new in interventional treatment of AF symptoms?
 Is cardioversion old hat? What is new in interventional treatment of AF symptoms? Joseph de Bono Consultant Electrophysiologist University Hospitals Birmingham Atrial Fibrillation (AF) Affects 2% of the
Is cardioversion old hat? What is new in interventional treatment of AF symptoms? Joseph de Bono Consultant Electrophysiologist University Hospitals Birmingham Atrial Fibrillation (AF) Affects 2% of the
Mechanisms of Fractionated Electrograms Formation in the Posterior Left Atrium During Paroxysmal Atrial Fibrillation in Humans
 Journal of the American College of Cardiology Vol. 57, No. 9, 2011 2011 by the American College of Cardiology Foundation ISSN 0735-1097/$36.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2010.09.066
Journal of the American College of Cardiology Vol. 57, No. 9, 2011 2011 by the American College of Cardiology Foundation ISSN 0735-1097/$36.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2010.09.066
ANALYSIS AND VISUALIZATION OF ATRIAL FIBRILLATION ELECTROGRAMS USING CROSS-CORRELATION
 ANALYSIS AND VISUALIZATION OF ATRIAL FIBRILLATION ELECTROGRAMS USING CROSS-CORRELATION Conrad John Geibel III A thesis submitted to the faculty of the University of North Carolina at Chapel Hill in partial
ANALYSIS AND VISUALIZATION OF ATRIAL FIBRILLATION ELECTROGRAMS USING CROSS-CORRELATION Conrad John Geibel III A thesis submitted to the faculty of the University of North Carolina at Chapel Hill in partial
Role of Atrial Remodeling in Patients with Atrial Fibrillation
 REVIEW ARTICLE Role of Atrial Remodeling in Patients with Atrial Fibrillation Li-Wei Lo, Shih-Ann Chen* Division of Cardiology, Department of Medicine, Taipei Veterans General Hospital, and Institute of
REVIEW ARTICLE Role of Atrial Remodeling in Patients with Atrial Fibrillation Li-Wei Lo, Shih-Ann Chen* Division of Cardiology, Department of Medicine, Taipei Veterans General Hospital, and Institute of
Catheter ablation for atrial fibrillation (AF) was focused
 was focused") Mechanisms of Wave Fractionation at Boundaries of High-Frequency Excitation in the Posterior Left Atrium of the Isolated Sheep Heart During Atrial Fibrillation Jérôme Kalifa, MD*; Kazuhiko Tanaka, MD*;
Mechanisms of Wave Fractionation at Boundaries of High-Frequency Excitation in the Posterior Left Atrium of the Isolated Sheep Heart During Atrial Fibrillation Jérôme Kalifa, MD*; Kazuhiko Tanaka, MD*;
Research Article Characterization of Electrograms from Multipolar Diagnostic Catheters during Atrial Fibrillation
 BioMed Research International Volume 0, Article ID, pages http://dx.doi.org/./0/ Research Article Characterization of Electrograms from Multipolar Diagnostic Catheters during Atrial Fibrillation Prasanth
BioMed Research International Volume 0, Article ID, pages http://dx.doi.org/./0/ Research Article Characterization of Electrograms from Multipolar Diagnostic Catheters during Atrial Fibrillation Prasanth
Atrial fibrillation (AF) is the most common sustained
 is the most common sustained") Chronic Atrial Fibrillation in Patients With Rheumatic Heart Disease Mapping and Radiofrequency Ablation of Flutter Circuits Seen at Initiation After Cardioversion Mohan Nair, MD; Prasad Shah, MD; Ravinder
Chronic Atrial Fibrillation in Patients With Rheumatic Heart Disease Mapping and Radiofrequency Ablation of Flutter Circuits Seen at Initiation After Cardioversion Mohan Nair, MD; Prasad Shah, MD; Ravinder
AF Today: W. For the majority of patients with atrial. are the Options? Chris Case
 AF Today: W hat are the Options? Management strategies for patients with atrial fibrillation should depend on the individual patient. Treatment with medications seems adequate for most patients with atrial
AF Today: W hat are the Options? Management strategies for patients with atrial fibrillation should depend on the individual patient. Treatment with medications seems adequate for most patients with atrial
Case 1 Left Atrial Tachycardia
 Case 1 Left Atrial Tachycardia A 16 years old woman was referred to our institution because of recurrent episodes of palpitations and dizziness despite previous ablation procedure( 13 years ago) of postero-septal
Case 1 Left Atrial Tachycardia A 16 years old woman was referred to our institution because of recurrent episodes of palpitations and dizziness despite previous ablation procedure( 13 years ago) of postero-septal
The major thoracic veins, with their specific electrical
 Atrial Fibrillation Originating From Persistent Left Superior Vena Cava Li-Fern Hsu, MBBS; Pierre Jaïs, MD; David Keane, MD; J. Marcus Wharton, MD; Isabel Deisenhofer, MD; Mélèze Hocini, MD; Dipen C. Shah,
Atrial Fibrillation Originating From Persistent Left Superior Vena Cava Li-Fern Hsu, MBBS; Pierre Jaïs, MD; David Keane, MD; J. Marcus Wharton, MD; Isabel Deisenhofer, MD; Mélèze Hocini, MD; Dipen C. Shah,
PART I. Disorders of the Heart Rhythm: Basic Principles
 PART I Disorders of the Heart Rhythm: Basic Principles FET01.indd 1 1/11/06 9:53:05 AM FET01.indd 2 1/11/06 9:53:06 AM CHAPTER 1 The Cardiac Electrical System The heart spontaneously generates electrical
PART I Disorders of the Heart Rhythm: Basic Principles FET01.indd 1 1/11/06 9:53:05 AM FET01.indd 2 1/11/06 9:53:06 AM CHAPTER 1 The Cardiac Electrical System The heart spontaneously generates electrical
This presentation will deal with the basics of ECG description as well as the physiological basics of
 Snímka 1 Electrocardiography basics This presentation will deal with the basics of ECG description as well as the physiological basics of Snímka 2 Lecture overview 1. Cardiac conduction system functional
Snímka 1 Electrocardiography basics This presentation will deal with the basics of ECG description as well as the physiological basics of Snímka 2 Lecture overview 1. Cardiac conduction system functional
Mapping the Conversion of Atrial Flutter to
 882 Mapping the Conversion of Atrial Flutter to Atrial Fibrillation and Atrial Fibrillation to Atrial Flutter Insights Into Mechanisms Jose Ortiz, Shinichi Niwano, Haruhiko Abe, Yoram Rudy, Nancy J. Johnson,
882 Mapping the Conversion of Atrial Flutter to Atrial Fibrillation and Atrial Fibrillation to Atrial Flutter Insights Into Mechanisms Jose Ortiz, Shinichi Niwano, Haruhiko Abe, Yoram Rudy, Nancy J. Johnson,
KENTARO YOSHIDA, M.D., MAGNUS ULFARSSON, PH.D.,
 Complex Electrograms Within the Coronary Sinus: Time- and Frequency-Domain Characteristics, Effects of Antral Pulmonary Vein Isolation, and Relationship to Clinical Outcome in Patients with Paroxysmal
Complex Electrograms Within the Coronary Sinus: Time- and Frequency-Domain Characteristics, Effects of Antral Pulmonary Vein Isolation, and Relationship to Clinical Outcome in Patients with Paroxysmal
How to Ablate Atrial Tachycardia Mechanisms and Approach. DrJo Jo Hai
 How to Ablate Atrial Tachycardia Mechanisms and Approach DrJo Jo Hai Contents Mechanisms of focal atrial tachycardia Various mapping techniques Detailed discussion on activation sequence mapping and entrainment
How to Ablate Atrial Tachycardia Mechanisms and Approach DrJo Jo Hai Contents Mechanisms of focal atrial tachycardia Various mapping techniques Detailed discussion on activation sequence mapping and entrainment
PERMANENT PACEMAKERS AND IMPLANTABLE DEFIBRILLATORS Considerations for intensivists
 PERMANENT PACEMAKERS AND IMPLANTABLE DEFIBRILLATORS Considerations for intensivists Craig A. McPherson, MD, FACC Associate Professor of Medicine Constantine Manthous, MD, FACP, FCCP Associate Clinical
PERMANENT PACEMAKERS AND IMPLANTABLE DEFIBRILLATORS Considerations for intensivists Craig A. McPherson, MD, FACC Associate Professor of Medicine Constantine Manthous, MD, FACP, FCCP Associate Clinical
Ankara, Turkey 2 Department of Cardiology, Division of Arrhythmia and Electrophysiology, Yuksek Ihtisas
 258 Case Report Electroanatomic Mapping-Guided Radiofrequency Ablation of Adenosine Sensitive Incessant Focal Atrial Tachycardia Originating from the Non-Coronary Aortic Cusp in a Child Serhat Koca, MD
258 Case Report Electroanatomic Mapping-Guided Radiofrequency Ablation of Adenosine Sensitive Incessant Focal Atrial Tachycardia Originating from the Non-Coronary Aortic Cusp in a Child Serhat Koca, MD
A RAPID CYCLE LENGTH VARIABILITY DETECTION TECHNIQUE OF ATRIAL ELECTROGRAMS IN ATRIAL FIBRILLATION
 A RAPID CYCLE LENGTH VARIABILITY DETECTION TECHNIQUE OF ATRIAL ELECTROGRAMS IN ATRIAL FIBRILLATION by SEUNGYUP LEE Submitted in partial fulfillment of the requirements for the degree of Master of Science
A RAPID CYCLE LENGTH VARIABILITY DETECTION TECHNIQUE OF ATRIAL ELECTROGRAMS IN ATRIAL FIBRILLATION by SEUNGYUP LEE Submitted in partial fulfillment of the requirements for the degree of Master of Science
University of Groningen. Atrial remodeling due to atrial tachycardia and heart failure Schoonderwoerd, Bas Arjan
 University of Groningen Atrial remodeling due to atrial tachycardia and heart failure Schoonderwoerd, Bas Arjan IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you
University of Groningen Atrial remodeling due to atrial tachycardia and heart failure Schoonderwoerd, Bas Arjan IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you
Atrial Fibrillation: Rate vs. Rhythm. Michael Curley, MD Cardiac Electrophysiology
 Atrial Fibrillation: Rate vs. Rhythm Michael Curley, MD Cardiac Electrophysiology I have no relevant financial disclosures pertaining to this topic. A Fib Epidemiology #1 Most common heart rhythm disturbance
Atrial Fibrillation: Rate vs. Rhythm Michael Curley, MD Cardiac Electrophysiology I have no relevant financial disclosures pertaining to this topic. A Fib Epidemiology #1 Most common heart rhythm disturbance
Linear Ablation Should Not Be a Standard Part of Ablation in Persistent AF. Disclosures. LA Ablation vs. Segmental Ostial Ablation With PVI for PAF
 Linear Ablation Should Not Be a Standard Part of Ablation in Persistent AF The CA Heart Rhythm Symposium September 7, 2012 Gregory K. Feld, MD Professor of Medicine Director, Cardiac EP Program University
Linear Ablation Should Not Be a Standard Part of Ablation in Persistent AF The CA Heart Rhythm Symposium September 7, 2012 Gregory K. Feld, MD Professor of Medicine Director, Cardiac EP Program University
Στροφείς (rotors) και πραγματικότητα. Χάρης Κοσσυβάκης Επιμελητής A Καρδιολογικό Τμήμα Γ.Ν.Α. «Γ. ΓΕΝΝΗΜΑΤΑΣ»
 και πραγματικότητα. Χάρης Κοσσυβάκης Επιμελητής A Καρδιολογικό Τμήμα Γ.Ν.Α. «Γ. ΓΕΝΝΗΜΑΤΑΣ»") Στροφείς (rotors) και πραγματικότητα. Χάρης Κοσσυβάκης Επιμελητής A Καρδιολογικό Τμήμα Γ.Ν.Α. «Γ. ΓΕΝΝΗΜΑΤΑΣ» Mechanisms that sustain Atrial Fibrillation multiwavelet hypothesis, since 1964 a critical
Στροφείς (rotors) και πραγματικότητα. Χάρης Κοσσυβάκης Επιμελητής A Καρδιολογικό Τμήμα Γ.Ν.Α. «Γ. ΓΕΝΝΗΜΑΤΑΣ» Mechanisms that sustain Atrial Fibrillation multiwavelet hypothesis, since 1964 a critical
Atrial fibrillation (AF) is the most common cardiac
 is the most common cardiac") Effects of Antiarrhythmic Drugs on Fibrillation in the Remodeled Atrium Insights Into the Mechanism of the Superior Efficacy of Amiodarone Kaori Shinagawa, MD; Akiko Shiroshita-Takeshita, MD; Gernot Schram,
Effects of Antiarrhythmic Drugs on Fibrillation in the Remodeled Atrium Insights Into the Mechanism of the Superior Efficacy of Amiodarone Kaori Shinagawa, MD; Akiko Shiroshita-Takeshita, MD; Gernot Schram,
Rational Approach to Improving Cardiac Arrhythmia Therapy. Rational Approach to Improving Cardiac Arrhythmia Therapy
 Rational Approach to Improving Cardiac Arrhythmia Therapy Rational Approach to Improving Cardiac Arrhythmia Therapy Stanley Nattel, MD Stanley Nattel, MD DEDICATED TO THE MASTER OF RATIONAL THERAPEUTICS
Rational Approach to Improving Cardiac Arrhythmia Therapy Rational Approach to Improving Cardiac Arrhythmia Therapy Stanley Nattel, MD Stanley Nattel, MD DEDICATED TO THE MASTER OF RATIONAL THERAPEUTICS
University of Groningen. Atrial remodeling due to atrial tachycardia and heart failure Schoonderwoerd, Bas Arjan
 University of Groningen Atrial remodeling due to atrial tachycardia and heart failure Schoonderwoerd, Bas Arjan IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you
University of Groningen Atrial remodeling due to atrial tachycardia and heart failure Schoonderwoerd, Bas Arjan IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you
Intraoperative and Postoperative Arrhythmias: Diagnosis and Treatment
 Intraoperative and Postoperative Arrhythmias: Diagnosis and Treatment Karen L. Booth, MD, Lucile Packard Children s Hospital Arrhythmias are common after congenital heart surgery [1]. Postoperative electrolyte
Intraoperative and Postoperative Arrhythmias: Diagnosis and Treatment Karen L. Booth, MD, Lucile Packard Children s Hospital Arrhythmias are common after congenital heart surgery [1]. Postoperative electrolyte
Electrophysiological and Electroanatomic Characterization of the Atria in Sinus Node Disease. Evidence of Diffuse Atrial Remodeling
 Electrophysiological and Electroanatomic Characterization of the Atria in Sinus Node Disease Evidence of Diffuse Atrial Remodeling Prashanthan Sanders, MBBS, PhD; Joseph B. Morton, MBBS, PhD; Peter M.
Electrophysiological and Electroanatomic Characterization of the Atria in Sinus Node Disease Evidence of Diffuse Atrial Remodeling Prashanthan Sanders, MBBS, PhD; Joseph B. Morton, MBBS, PhD; Peter M.
Cardiac Arrhythmia Mapping!
 Cardiac Arrhythmia Mapping! Challenges and Opportunities" Derek J. Dosdall, Ph.D. 22 October, 2010 OUTLINE!! Historical perspective! Current mapping techniques!optical mapping!electrical mapping (Purkinje
Cardiac Arrhythmia Mapping! Challenges and Opportunities" Derek J. Dosdall, Ph.D. 22 October, 2010 OUTLINE!! Historical perspective! Current mapping techniques!optical mapping!electrical mapping (Purkinje
Medicine. Dynamic Changes of QRS Morphology of Premature Ventricular Contractions During Ablation in the Right Ventricular Outflow Tract
 Medicine CLINICAL CASE REPORT Dynamic Changes of QRS Morphology of Premature Ventricular Contractions During Ablation in the Right Ventricular Outflow Tract A Case Report Li Yue-Chun, MD, Lin Jia-Feng,
Medicine CLINICAL CASE REPORT Dynamic Changes of QRS Morphology of Premature Ventricular Contractions During Ablation in the Right Ventricular Outflow Tract A Case Report Li Yue-Chun, MD, Lin Jia-Feng,
Jurnal Teknologi FREQUENCY ESTIMATION FOR ATRIAL FIBRILLATION FROM HUMAN STUDIES. Full Paper. Anita Ahmad *
 Jurnal Teknologi FREQUENCY ESTIMATION FOR ATRIAL FIBRILLATION FROM HUMAN STUDIES Anita Ahmad * Department of Control and Mechatronics Engineering, Faculty of Electrical Engineering, Universiti Teknologi
Jurnal Teknologi FREQUENCY ESTIMATION FOR ATRIAL FIBRILLATION FROM HUMAN STUDIES Anita Ahmad * Department of Control and Mechatronics Engineering, Faculty of Electrical Engineering, Universiti Teknologi
Mechanisms of atrial fibrillation terminations in humans: insights from non-invasive cardiac mapping
 VENICE ARRHYTHMIAS, 16-18 OCTOBER, 2015 Mechanisms of atrial fibrillation terminations in humans: insights from non-invasive cardiac mapping E. Fetisova, A. Tsyganov, M. Chaykovskaya, V. Kalinin, M. Yakovleva
VENICE ARRHYTHMIAS, 16-18 OCTOBER, 2015 Mechanisms of atrial fibrillation terminations in humans: insights from non-invasive cardiac mapping E. Fetisova, A. Tsyganov, M. Chaykovskaya, V. Kalinin, M. Yakovleva
The prevalence of atrial fibrillation (AF), already the most common sustained cardiac arrhythmia,
, already the most common sustained cardiac arrhythmia,") Electrophysiology ATRIAL FIBRILLATION: CLASSIFICATION, PATHOPHYSIOLOGY, MECHANISMS AND DRUG TREATMENT See end of article for authors affiliations Correspondence to: Dr Vias Markides, Waller Cardiac Department,
Electrophysiology ATRIAL FIBRILLATION: CLASSIFICATION, PATHOPHYSIOLOGY, MECHANISMS AND DRUG TREATMENT See end of article for authors affiliations Correspondence to: Dr Vias Markides, Waller Cardiac Department,
Since pulmonary veins (PVs) have
 have") Case Report Hellenic J Cardiol 2011; 52: 371-376 Left Atrial-Pulmonary Vein Reentrant Tachycardia Following Pulmonary Vein Isolation Dionyssios Leftheriotis, Feifan Ouyang, Karl-Heinz Kuck II. Med. Abteilung,
Case Report Hellenic J Cardiol 2011; 52: 371-376 Left Atrial-Pulmonary Vein Reentrant Tachycardia Following Pulmonary Vein Isolation Dionyssios Leftheriotis, Feifan Ouyang, Karl-Heinz Kuck II. Med. Abteilung,
arxiv: v1 [q-bio.to] 29 Oct 2018
![arxiv: v1 [q-bio.to] 29 Oct 2018](/thumbs/89/99254486.jpg "arxiv: v1 [q-bio.to] 29 Oct 2018") Unified Mechanism of Atrial Fibrillation in a Simple Model Max Falkenberg 1,2,3, Andrew J. Ford 1, Anthony C. Li 1, Alberto Ciacci 1,2,3, Nicholas S. Peters 3, and Kim Christensen 1,2,3 1 Blackett Laboratory,
Unified Mechanism of Atrial Fibrillation in a Simple Model Max Falkenberg 1,2,3, Andrew J. Ford 1, Anthony C. Li 1, Alberto Ciacci 1,2,3, Nicholas S. Peters 3, and Kim Christensen 1,2,3 1 Blackett Laboratory,
Atrial fibrillation (AF) has a tendency to become more
 has a tendency to become more") Reversal of Atrial Electrical Remodeling After Cardioversion of Persistent Atrial Fibrillation in Humans W. Julian C. Hobbs, MB; Simon Fynn, MB; Derick M. Todd, MB; Peter Wolfson, MB; Mike Galloway, BS;
Reversal of Atrial Electrical Remodeling After Cardioversion of Persistent Atrial Fibrillation in Humans W. Julian C. Hobbs, MB; Simon Fynn, MB; Derick M. Todd, MB; Peter Wolfson, MB; Mike Galloway, BS;
Index. cardiology.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A AADs. See Antiarrhythmic drugs (AADs) ACE inhibitors. See Angiotensin-converting enzyme (ACE) inhibitors ACP in transseptal approach to
Index Note: Page numbers of article titles are in boldface type. A AADs. See Antiarrhythmic drugs (AADs) ACE inhibitors. See Angiotensin-converting enzyme (ACE) inhibitors ACP in transseptal approach to
Atrial Fibrillation Begets Atrial Fibrillation Autonomic Mechanism for Atrial Electrical Remodeling Induced by Short-Term Rapid Atrial Pacing
 Atrial Fibrillation Begets Atrial Fibrillation Autonomic Mechanism for Atrial Electrical Remodeling Induced by Short-Term Rapid Atrial Zhibing Lu, MD; Benjamin J. Scherlag, PhD; Jiaxiong Lin, MD; Guodong
Atrial Fibrillation Begets Atrial Fibrillation Autonomic Mechanism for Atrial Electrical Remodeling Induced by Short-Term Rapid Atrial Zhibing Lu, MD; Benjamin J. Scherlag, PhD; Jiaxiong Lin, MD; Guodong
Phase 2 Early Afterdepolarization as a Trigger of Polymorphic Ventricular Tachycardia in Acquired Long-QT Syndrome
 Phase 2 Early Afterdepolarization as a Trigger of Polymorphic Ventricular Tachycardia in Acquired Long-QT Syndrome Direct Evidence From Intracellular Recordings in the Intact Left Ventricular Wall Gan-Xin
Phase 2 Early Afterdepolarization as a Trigger of Polymorphic Ventricular Tachycardia in Acquired Long-QT Syndrome Direct Evidence From Intracellular Recordings in the Intact Left Ventricular Wall Gan-Xin