Hypertension Update 2009
|
|
|
- Ezra Chambers
- 6 years ago
- Views:
Transcription

1


2 Hypertension Update 2009 New Drugs, New Goals, New Approaches, New Lessons from Clinical Trials Timothy C Fagan, MD, FACP Professor Emeritus University of Arizona
3 New Drugs Direct Renin Inhibitors Endothelin Antagonists


4 DRI Works at the Point of Activation of the RAAS


5 Aliskiren Reduced PRA Alone and in Combination With Ramipril*


6 Aliskiren Maintained 80% SBP Reduction 4 Days After Last Dose


7 Why Use a DRI? Aliskiren and Aliskiren + HCTZ Have an Established d Safety and Tolerability Profile
8 Endothelin Antagonists Endothelin (ET) antagonists such as bosentan have been used successfully to treat pulmonary hypertension. Trials with multiple ET antagonists are under way in hypertension and CHF. The selective ET A antagonist, darusentan, may be approved by the FDA in 2009.
9 New Goals Uncomplicated Hypertension Diabetes Renal Disease Diabetes + Renal Disease Coronary Disease


10 How Low Should Blood Pressure Be Lowered?
11 New Approaches Emphasis on Cost:Benefit Emphasis on Systolic Blood Pressure Combination Therapy Emphasis on Endpoints
12 Emphasis on Cost:Benefit Many generic antihypertensive agents are now available for as little as $10/90 days. A 4 drug antihypertensive regimen utilizing diuretics, Beta blockers, ACE-Is and CCBs can be used at a cost of $162.22/year or $0.44/day

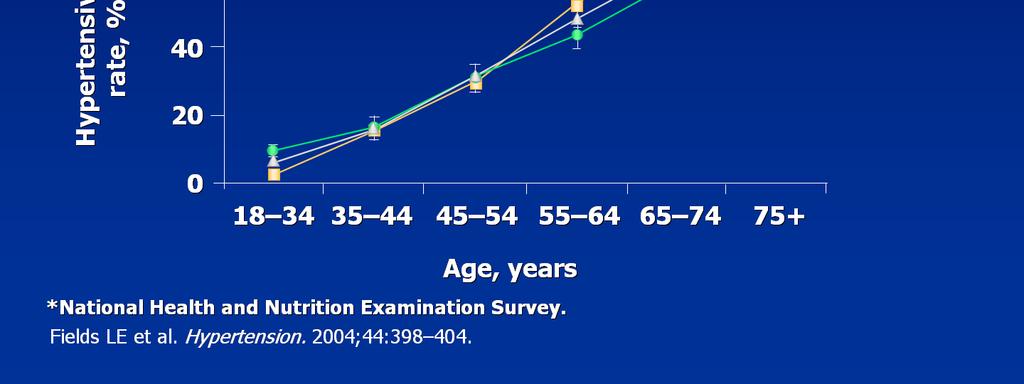
13 Prevalence of Hypertension Increases With Age


14 Isolated Systolic Hypertension Accounts for Most Uncontrolled HTN N in the Elderly


15 Relative Importance of DBP and SBP as Predictors of CHD as a Function of Age
16 Systolic vs Diastolic BP as Predictors of Outcomes in ASCOT-BPLA MI + CHD Death + Revascularization HR/1 SD P SBP 1.16 <.0001 Fatal + Nonfatal Stroke HR/1 SD P SBP 1.38 <.0001 DBP DBP PP 1.23 <.0001 PP 1.45 <.0001
17 Combination Antihypertensive Therapy Evolution and Rationale
18 Historical Evolution of Fixed- Dose Combination Agents 1960s Reserpine-hydralazine-hydrochlorothiazide (Ser-Ap-EsR) Methyldopa/thiazide diuretic 1970s Thiazide/potassium-sparing diuretic Thiazide/spironolactone β-blocker/thiazide diuretic Clonidine/thiazide diuretic 1980s Angiotensin-converting enzyme inhibitor/thiazide diuretic 1990s Low-dose β-blocker/low-dose thiazide diuretic Angiotensin-converting enzyme inhibitor/calcium antagonist Angiotensin II receptor blocker/thiazide diuretic Adapted from: Epstein M, Bakris G. Arch Intern Med. 1996;156:


19 BP Control Usually Requires Combination Therapy
20 JNC VII The initiation of therapy with more than one drug increases the likelihood of achieving BP goal in a more timely fashion. The use of fixed-dose combinations may be more convenient and simplify the treatment regimen, and may cost less than the individual components prescribed separately.
21 JNC VII The use of multidrug combinations often produces greater BP reduction at lower doses of the component agents, resulting in fewer side effects. However, caution is advised in initiating therapy with multiple agents, particularly in some older persons and in those at risk for orthostatic hypotension, such as diabetics with autonomic dysfunction.
22 Combination Antihypertensive Therapy: Potential Reductions in Dose-Related Side Effects Thiazide diuretics with potassium-sparing diuretics May reduce K+ loss and decrease the risk of hypokalemia Thiazide diuretics with ARBs or ACE inhibitors May reduce risk of hypokalemia ACE inhibitors and dihydropyridine CCBs Combinations may have less edema than seen with dihydropyridines alone Beta-adrenoreceptor-blockers and direct vasodilators or dihydropyridine CCBs Beta-blockers reduce tachycardia seen with these agents Epstein, et al. Arch Intern Med. 1996;156: Jeunemaitre, et al. Am J Cardiol. 1988; 62: Pedrinelli, et al. Hypertension. 2000; 35: Van Zwieten. Clin Investig. 1992;70(suppl 1):


23 Guideline Recommendations Regarding Initial Use of Combination TherapyT

 vs")
24 Increased Persistence* with Single-pill Combination (SPC) vs Separate Pill Therapy
25 Single Pill Combination Therapy Demonstrates Improved Compliance in Hypertensive Patients Risk ratio (95% CI) % Weight Taylor et al 0.74 (0.67, 0.81) 27.1 Dezii 0.74 (0.65, 0.84) 13.9 NDC dataset 0.81 (0.77, 0.86) 46.4 Dezii 0.71 (0.62, 0.80) 12.6 Overall (95% CI) 0.77 (0.73, 0.80) P< Risk Ratio Favors FDC Agent Retrospective Study FDC fixed dose combination Bangalore S, Am J Med 2007;120: Favors Individual Agents Given Separately

26 Potential Benefits of Single-Pill Combinations
27 Emphasis on Endpoints New Lessons from Clinical Trials Does which drugs we use matter? In moderate risk patients? In high risk patients? In very high risk patients?
28 ALLHAT Does the First Drug Matter? Moderate Risk Diuretic vs ACE-I vs CCB
29 ALLHAT Design: Double-blind, randomized, prospective Patients: 42,418, mean age 67, with HTN +1 other risk factor, controlled on no more than 2 drugs, partially treated BP 156/89 Intervention: Chlorthalidone mg vs amlodipine mg vs lisinopril mg vs doxazosin 1-8 mg Primary Endpoint: MI or CHD death
 and lisinopril (~2 mmhg) groups. Diastolic BP (mmhg) 90 85 80 75 Amlodipine Lisinopril Compared to chlorthalidone: DBP significantly lower in amlodipine group (~1 mmhg).")
30 ALLHAT Mean Systolic and Diastolic Blood Pressure During Follow-up Chlorthalidone Chlorthalidone Systolic BP (mmhg) Amlodipine Lisinopril Compared to chlorthalidone: SBP significantly higher in amlodipine (~1 mmhg) and lisinopril (~2 mmhg) groups. Diastolic BP (mmhg) Amlodipine Lisinopril Compared to chlorthalidone: DBP significantly lower in amlodipine group (~1 mmhg) Follow-up, yrs SBP=systolic blood pressure DBP=diastolic blood pressure ALLHAT Research Group. JAMA. 2002;288: org Copyright 2002, American Medical Association.

31 Cumulative Fatal CHD and Nonfatal MI event rate (%) No. at Risk Chlorthalidone Amlodipine Lisinopril ALLHAT Primary Outcome by Treatment Group Time to event, yrs Chlorthalidone Amlodipine Lisinopril ALLHAT Research Group. JAMA. 2002;288: Copyright 2002, American Medical Association org
32 ALLHAT Conclusions The doxazosin arm was stopped early for higher CHF rates. The Primary Combined Endpoint of MI + CHD Death was not different with chlorthalidone, amlodipine or lisinopril. BP was lower in the chlorthalidone group as were CVA, angina and revascularization. The long term significance of more new onset diabetes in the chlorthalidone group is unclear.
33 OnTarget Design: Double-blind, randomized, prospective Patients: 25,620 with vascular disease or DM with TOD, treated BP at baseline 142/82 Intervention: ramipril 10 mg vs telmisartan 80 mg vs the combination Primary Endpoint: MI, CVA, CV death or CHF hospitalization
34 Kaplan-Meier Curves for the Primary Outcome in the Three Study Groups The ONTARGET Investigators. N Engl J Med 2008;358:
35 Relative Risks in Prespecified Subgroups The ONTARGET Investigators. N Engl J Med 2008;358:

36 Discontinuation of Study Medications and Selected Reasons for Permanent Discontinuation The ONTARGET Investigators. N Engl J Med 2008;358:
37 OnTarget Conclusions The Primary Composite Endpoint of MI, CVA, CV Death or CHF hospitalization did not differ between ramipril, telmisartan or the combination. Telmisartan was better tolerated than ramipril and both were better tolerated than the combination. For cardioprotection in patients with vascular disease or diabetes, telmisartan is equal to ramipril and the combination of ACEI and ARB has no advantage and is less well tolerated.
38 LIFE Design: Double-blind, randomized, prospective Patients: 9,193 with HTN and LVH, mean age 67, untreated BP at baseline 174/98 Intervention: losartan mg vs atenolol mg Primary Endpoint: MI, CVA or death
39 LIFE Study Blood Pressure During Follow-up Systolic mmhg Losartan Atenolol Mean Arterial Diastolic Study Month Dahlof B, et al. Lancet. 2002;359: Reprinted with permission from Elsevier Science. org
40 Proportion of patients with first event (%) LIFE Study Primary Composite Endpoint Intention-to-treat Adjusted risk reduction 13 0%, P=0 021 Unadjusted risk reduction 14 6%, P=0 009 Atenolol Losartan Study Month Losartan (n) Atenolol (n) Dahlof B, et al. Lancet. 2002;359: Reprinted with permission from Elsevier Science. org
41 Proportion of patients with first event (%) LIFE Study Fatal and Non-Fatal Stroke Intention-to-treat Adjusted risk reduction 24 9%, P=0 001 Unadjusted risk reduction 25 8%, P= Atenolol Losartan Study Month Dahlof B, et al. Lancet. 2002;359: Reprinted with permission from Elsevier Science. org
42 LIFE Diabetes and ISH Does the First Drug Matter? Very High Risk ARB vs Beta Blocker
43 Proportion of patients with first event(%) LIFE Study Diabetes Subgroup Total Mortality Adjusted risk reduction 38 7%, P=0 002 Unadjusted risk reduction 40 1%, P=0 001 Atenolol Losartan Study Month Lindholm LH, et al. Lancet. 2002;359: Reprinted with permission from Elsevier Science. org
44 LIFE: Total Mortality Diabetes Subgroup 24 Proportion of patients (%) L H Lindholm et al. Lancet 2002;359: Atenolol Losartan 4 Adjusted Risk Reduction 38.7%, p=0 002 Unadjusted Risk Reduction 40.1%, p= Study Month
45 Endpoint rate (%) LIFE Study ISH Subgroup Total Mortality Unadjusted relative risk reduction=30%; P=0.03 Adjusted relative risk reduction=28%; P=0.046 Atenolol Losartan Study month Kjeldsen SE, et al. JAMA. 2002;228: Copyright 2002, American Medical Association. org
46 LIFE Conclusions The Primary Combined Endpoint of MI, CVA or Death, but particularly CVA, were lower with losartan than with atenolol. In the Very High Risk, Diabetes and ISH subgroups, even Total Mortality was lower with losartan. In High Risk patients with hypertension, initial therapy with ARB is superior to Beta Blocker.
47 ASCOT-BPLA Do the First and Second Drug Matter? High Risk CCB + ACEI vs Beta Blocker + diuretic
48 ASCOT-BPLA Design: Double-blind, randomized, prospective Patients: 19,257, mean age 63, with HTN + 3 other risk factors, untreated BP 165/95 Intervention: amlodipine 5-10 mg + perindopril 4-8 mg vs atenolol mg + bendroflumethiazide mg Primary Endpoint: MI (clinical or silent) or CHD death
49 ASCOT BPLA Primary Endpoint Risk Reduction Percent Non-fatal MI, fatal CHD Atenolol ± thiazide (474 events) Amlodipine ± perindopril (429 events) 1.0 HR=0.90 (95% CI, ) P= Years Number at risk Amlodipine ± perindopril Atenolol ± thiazide Dahlöf B et al. Lancet. 2005;366:
50 ASCOT BPLA Secondary Endpoints Unadjusted Hazard Ratio (95% CI) Endpoint (n amlo vs aten) Non-fatal MI* +fatal CHD (390 vs 444) Total coronary endpoint (753 vs 852) Total CV event and procedures(1362 vs 1602) All-cause mortality (738 vs 820) Cardiovascular mortality (263 vs 342) Fatal and non-fatal stroke (327 vs 422) Fatal and non-fatal heart failure (124 vs 159) P Value P = P = P < P = P = P = P = Favors amlodipine ± perindopril Favors atenolol ± thiazide The area of each square is proportional to the amount of statistical information. *Excludes silent non-fatal MI. Adapted from Dahlöf B et al. Lancet. 2005;366:
51 ASCOT-BPLA Conclusions The Primary Combined Endpoint of MI or CHD Death and most secondary endpoints, including total mortality, were lower in the amlodipineperindopril (CCB-ACEI) than in the atenololthiazide group. BP was lower in the CCB-ACEI group, but the Hazard Ratios for the Primary Endpoint and CVA were still significant when adjusted for BP. The CCB-ACEI regimen was superior to the Beta Blocker-Thiazide regimen.
52 ACCOMPLISH Does the Second Drug Matter? High Risk ACEI + CCB vs diuretic
53 ACCOMPLISH Design: Double-blind, randomized, prospective Patients: 11,506, mean age 68, with HTN and vascular disease or DM or LVH or CKD, Treated BP with a mean of 2 drugs 145/80 Intervention: benazepril mg + amlodipine 5-10 mg vs hydrochlorothiazide mg Primary Endpoint: MI, CVA, CHF, coronary intervention, resuscitated SCD or CVD death
54 160 ACCOMPLISH Blood Pressure Results Benazepril/amlodipine Benazepril/HCTZ 140 mmhg Patients, n Months Benazepril/amlodipine (N) 5,740 5,517 5,404 5,178 5,010 4,866 4,298 2,804 1,074 Benazepril/HCTZ (N) 5,757 5,537 5,408 5,222 5,033 4,825 4,299 2,529 1,042 The mean SBP/DBP following titration was 131.6/73.3 mm Hg in the benazepril/amlodipine group and 132.5/74.4 mm Hg in the benazepril/hctz group. The mean difference in SBP/DBP between the 2 groups was 0.9/1.1 mmhg (p<0.001) Jamerson K, et al. N Engl J Med. In Press
55 0.16 ACCOMPLISH Primary Endpoint Benazepril/amlodipine (552 patients with events: 9.6%) Benazepril/HCTZ (679 patients with events: 11.8%) 20% Cumulative event rate HR 0.80 (95%CI ); p< ,096 1,277 Time to first CV mortality/morbidity (days) Months Patients at risk (N) Benazepril/amlodipine 5,512 5,317 5,141 4,959 4,739 2,826 1,447 Benazepril/HCTZ 5,483 5,274 5,082 4,892 4,655 2,749 1,390 Jamerson K, et al. N Engl J Med. In Press
56 ACCOMPLISH Components of the Primary Endpoint* HR (95%CI) p-value Composite CV mortality/morbidity 0.80 ( ) <0.001 CV mortality 0.80 ( ) 0.08 MI (fatal/non-fatal) 0.78 ( ) 0.04 Stroke (fatal/non-fatal) 0.84 ( ) 0.17 Hospitalisation for unstable angina 0.75 ( ) 0.14 Coronary revascularisation procedure 0.86 ( ) 0.04 *Only the first event in an individual patient was counted in the analysis of the primary end point Jamerson K, et al. N Engl J Med. In Press Favours Benazepril /amlodipine Favours Benazepril /HCTZ
57 ACCOMPLISH Subgroup analyses for the primary endpoint Subgroups Benazepril/ amlodipine N=5744 Benazepril /HCTZ N=5762 Hazard Ratio (95% CI) p-value n(%) n(%) Sex Male 365 (10.6) 461 (13.1) 0.80 ( ) Female 187 (8.1) 218 (9.7) 0.83 ( ) 0.06 Age 65 years 70 years 386 (10.1) 260 (11.0) 474 (12.4) 323 (13.8) 0.81 ( ) 0.79 ( ) Diabetes Yes 307 (8.8) 383 (11.0) 0.79 ( ) No 245 (10.8) 296 (12.9) 0.82 ( ) 0.02
58 ACCOMPLISH Conclusions In the total cohort, as well as the 6,946 patients with diabetes, the Primary Combined Endpoint (-20%), as well as MI (-20%) and coronary revascularization (-14%), were lower in the benazeprilamlodipine than in the benazeprilhydrochlorothiazide group. When added to initial therapy with ACEI, CCB is superior to thiazide diuretic.
59 Summary: New Drugs The first Direct Renin Inhibitor, aliskiren, is effective and very well tolerated. The place of Direct Renin Inhibition in the antihypertensive armamentarium is as yet undetermined. The first selective antagonist of the endothelin A receptor, darusentan, may be approved this year for treatment of hypertension. The place of Selective Endothelin Receptor Antagonism in the antihypertensive armamentarium is as yet undetermined.
60 Summary: New Goals The goal BP for patients with low risk, uncomplicated hypertension remains unchanged at <140/90. The goal BP for patients with Diabetes, CKD, Angina or high risk of CAD is <130/80. The goal BP for patients with Diabetes + CKD is <120/70. In 2010, JNC VIII may revise these goals.
61 Summary: New Approaches I Nearly all patients with hypertension can be treated for less than $0.45 per day. Thiazide-type diuretics are superior in preventing 1 or more major forms of CVD and are less expensive. They should be preferred for first-step antihypertensive therapy. The ALLHAT authors. Adopted in JNC VII. Based upon current costs and subsequent clinical trials, this conclusion is no longer valid.
62 Summary: New Approaches II After age 55, Systolic BP is a strong predictor of CV events and Diastolic BP becomes a negative predictor. Initial treatment with combination therapy is reasonable and appropriate for patients with BP >20/10 mmhg above goal BP. Single Pill combination therapy has several advantages over Separate Pill therapy, especially better compliance.
63 Summary:Emphasis on Endpoints While BP reduction is of primary importance in treating hypertension, choice of agent is important in High Risk Patients. With different agents, at the same reduction in BP, there may be differences in MI, CVA, other CV endpoints, Total Mortality and new onset Diabetes. Multiple clinical trials support the superiority of ACE-Is, ARBs and CCBs over Beta Blockers and thiazide diuretics.

64
Treating Hypertension in Individuals with Diabetes
 Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
ALLHAT. Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic
 1 U.S. Department of Health and Human Services National Institutes of Health Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker
1 U.S. Department of Health and Human Services National Institutes of Health Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker
In the Literature 1001 BP of 1.1 mm Hg). The trial was stopped early based on prespecified stopping rules because of a significant difference in cardi
. The trial was stopped early based on prespecified stopping rules because of a significant difference in cardi") Is Choice of Antihypertensive Agent Important in Improving Cardiovascular Outcomes in High-Risk Hypertensive Patients? Commentary on Jamerson K, Weber MA, Bakris GL, et al; ACCOMPLISH Trial Investigators.
Is Choice of Antihypertensive Agent Important in Improving Cardiovascular Outcomes in High-Risk Hypertensive Patients? Commentary on Jamerson K, Weber MA, Bakris GL, et al; ACCOMPLISH Trial Investigators.
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, Financial Disclosures
 Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University
Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension
 Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension Prof. Massimo Volpe, MD, FAHA, FESC, Chair of Cardiology, Department of Clinical and Molecular Medicine
Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension Prof. Massimo Volpe, MD, FAHA, FESC, Chair of Cardiology, Department of Clinical and Molecular Medicine
Hypertension. Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute
 Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Understanding the importance of blood pressure control An overview of new guidelines: How do they impact daily current management?
 Understanding the importance of blood pressure control An overview of new guidelines: How do they impact daily current management? Slides presented during CDMC in Almaty, Kazakhstan on Saturday April 12,
Understanding the importance of blood pressure control An overview of new guidelines: How do they impact daily current management? Slides presented during CDMC in Almaty, Kazakhstan on Saturday April 12,
Hypertension Management: A Moving Target
 9:45 :30am Hypertension Management: A Moving Target SPEAKER Karol Watson, MD, PhD, FACC Presenter Disclosure Information The following relationships exist related to this presentation: Karol E. Watson,
9:45 :30am Hypertension Management: A Moving Target SPEAKER Karol Watson, MD, PhD, FACC Presenter Disclosure Information The following relationships exist related to this presentation: Karol E. Watson,
Hypertension Pharmacotherapy: A Practical Approach
 Hypertension Pharmacotherapy: A Practical Approach Ronald Victor, MD Burns & Allen Chair in Cardiology Director, The Hypertension Center Associate Director, The Heart Institute Hypertension Center 1. 2.
Hypertension Pharmacotherapy: A Practical Approach Ronald Victor, MD Burns & Allen Chair in Cardiology Director, The Hypertension Center Associate Director, The Heart Institute Hypertension Center 1. 2.
Antihypertensive Trial Design ALLHAT
 1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
JNC 8 -Controversies. Sagren Naidoo Nephrologist CMJAH
 JNC 8 -Controversies Sagren Naidoo Nephrologist CMJAH Joint National Committee (JNC) Panel appointed by the National Heart, Lung, and Blood Institute (NHLBI) First guidelines (JNC-1) published in 1977
JNC 8 -Controversies Sagren Naidoo Nephrologist CMJAH Joint National Committee (JNC) Panel appointed by the National Heart, Lung, and Blood Institute (NHLBI) First guidelines (JNC-1) published in 1977
Hypertension Update Clinical Controversies Regarding Age and Race
 Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014
 HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Causes of Poor BP control Rates
 Goals Of Hypertension Management in Clinical Practice World Hypertension League (WHL) Meeting Adel E. Berbari, MD, FAHA, FACP Professor of Medicine and Physiology Head, Division of Hypertension and Vascular
Goals Of Hypertension Management in Clinical Practice World Hypertension League (WHL) Meeting Adel E. Berbari, MD, FAHA, FACP Professor of Medicine and Physiology Head, Division of Hypertension and Vascular
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
State of the art treatment of hypertension: established and new drugs. Prof. M. Burnier Service of Nephrology and Hypertension Lausanne, Switzerland
 State of the art treatment of hypertension: established and new drugs Prof. M. Burnier Service of Nephrology and Hypertension Lausanne, Switzerland First line therapies in hypertension ACE inhibitors AT
State of the art treatment of hypertension: established and new drugs Prof. M. Burnier Service of Nephrology and Hypertension Lausanne, Switzerland First line therapies in hypertension ACE inhibitors AT
Talking about blood pressure
 Talking about blood pressure Mrs Khan 56 BP 158/99 BMI 32 Total cholesterol 5.4 (HDL 0.8) HbA1c 43 She has been promising to do more exercise and eat more healthily for the last 2 years but her weight
Talking about blood pressure Mrs Khan 56 BP 158/99 BMI 32 Total cholesterol 5.4 (HDL 0.8) HbA1c 43 She has been promising to do more exercise and eat more healthily for the last 2 years but her weight
Managing Hypertension in Diabetes Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park.
 Managing Hypertension in Diabetes 2015 Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park Case Scenario Mike M is a 59 year old man with type 2 diabetes managed
Managing Hypertension in Diabetes 2015 Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park Case Scenario Mike M is a 59 year old man with type 2 diabetes managed
Hypertension Update Warwick Jaffe Interventional Cardiologist Ascot Hospital
 Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
Preventing and Treating High Blood Pressure
 Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
Randomized Design of ALLHAT BP Trial
 Outcomes in Hypertensive Black and Nonblack Patients Treated with Chlorthalidone, Amlodipine, and Lisinopril* *Wright JT, Dunn JK, Cutler JA et al. JAMA 2005:293:1595-1608. 42,418 High-risk hypertensive
Outcomes in Hypertensive Black and Nonblack Patients Treated with Chlorthalidone, Amlodipine, and Lisinopril* *Wright JT, Dunn JK, Cutler JA et al. JAMA 2005:293:1595-1608. 42,418 High-risk hypertensive
Explore the Rationale for the Dual Mechanism CCB/ARB Approach in Hypertension Management
 Explore the Rationale for the Dual Mechanism CCB/ARB Approach in Hypertension Management Jeong Bae Park, MD,PhD Dept of Med/Cardiology, Cheil General Hospital, Kwandong University College of Medicine Apr
Explore the Rationale for the Dual Mechanism CCB/ARB Approach in Hypertension Management Jeong Bae Park, MD,PhD Dept of Med/Cardiology, Cheil General Hospital, Kwandong University College of Medicine Apr
Modern Management of Hypertension
 Modern Management of Hypertension Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Hypertension Prevalence
Modern Management of Hypertension Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Hypertension Prevalence
ALLHAT Role of Diuretics in the Prevention of Heart Failure - The Antihypertensive and Lipid- Lowering Treatment to Prevent Heart Attack Trial
 1 ALLHAT Role of Diuretics in the Prevention of Heart Failure - The Antihypertensive and Lipid- Lowering Treatment to Prevent Heart Attack Trial Davis BR, Piller LB, Cutler JA, et al. Circulation 2006.113:2201-2210.
1 ALLHAT Role of Diuretics in the Prevention of Heart Failure - The Antihypertensive and Lipid- Lowering Treatment to Prevent Heart Attack Trial Davis BR, Piller LB, Cutler JA, et al. Circulation 2006.113:2201-2210.
2/10/2014. Hypertension: Highlights of Hypertension Guidelines: Making the Most of Limited Evidence. Issues with contemporary guidelines
 Hypertension: 214 Highlights of Hypertension Guidelines: Making the Most of Limited Evidence Michael A, Weber, MD Editor-in-Chief, The Journal of Clinical Hypertension, Professor of Medicine, Division
Hypertension: 214 Highlights of Hypertension Guidelines: Making the Most of Limited Evidence Michael A, Weber, MD Editor-in-Chief, The Journal of Clinical Hypertension, Professor of Medicine, Division
VALUE OF ACEI IN THE MANAGEMENT OF HYPERTENSION
 VALUE OF ACEI IN THE MANAGEMENT OF HYPERTENSION Dr Catherine BESEME Paris 6 th December 2005 6 th International Congress of Bangladesh Society of Medicine Hypertension is a risk factor at the source, with
VALUE OF ACEI IN THE MANAGEMENT OF HYPERTENSION Dr Catherine BESEME Paris 6 th December 2005 6 th International Congress of Bangladesh Society of Medicine Hypertension is a risk factor at the source, with
Rationale for the use of Single Pill Combination (SPC) and Asian data of ARB/CCB SPC
 and Asian data of ARB/CCB SPC") Rationale for the use of Single Pill Combination (SPC) and Asian data of ARB/CCB SPC Seung Woo Park, MD Samsung Medical Center BP Control Rates in Asia BP controlled BP uncontrolled 24.3% 36.6% 19% Turkey
Rationale for the use of Single Pill Combination (SPC) and Asian data of ARB/CCB SPC Seung Woo Park, MD Samsung Medical Center BP Control Rates in Asia BP controlled BP uncontrolled 24.3% 36.6% 19% Turkey
DISCLOSURE PHARMACIST OBJECTIVES 9/30/2014 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES. I have nothing to disclose.
 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
Modern Management of Hypertension: Where Do We Draw the Line?
 Modern Management of Hypertension: Where Do We Draw the Line? Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Blood Pressure
Modern Management of Hypertension: Where Do We Draw the Line? Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Blood Pressure
APPENDIX D: PHARMACOTYHERAPY EVIDENCE
 Página 1 de 7 APPENDIX D: PHARMACOTYHERAPY EVIDENCE Table D1. Outcome Trials of Antihypertensive Agents Study Drug Regimen N Duration Primary Outcomes Remarks Antihypertensive Therapy vs Placebo SHEP 1991
Página 1 de 7 APPENDIX D: PHARMACOTYHERAPY EVIDENCE Table D1. Outcome Trials of Antihypertensive Agents Study Drug Regimen N Duration Primary Outcomes Remarks Antihypertensive Therapy vs Placebo SHEP 1991
Hypertension 2015: Recent Evidence that Will Change Your Practice
 Hypertension 2015: Recent Evidence that Will Change Your Practice Gerald W. Smetana, M.D. Division of General Medicine Beth Israel Deaconess Medical Center Professor of Medicine Harvard Medical School
Hypertension 2015: Recent Evidence that Will Change Your Practice Gerald W. Smetana, M.D. Division of General Medicine Beth Israel Deaconess Medical Center Professor of Medicine Harvard Medical School
Combination Therapy for Hypertension
 Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
Rationale for the use of Single Pill Combination. Yong Jin Kim, MD Seoul National University Hospital
 Rationale for the use of Single Pill Combination Yong Jin Kim, MD Seoul National University Hospital Unmet Need of Hypertension Treatment Hypertension # 1 Risk Factor for Global Mortality 0 1 2 3 4 5 6
Rationale for the use of Single Pill Combination Yong Jin Kim, MD Seoul National University Hospital Unmet Need of Hypertension Treatment Hypertension # 1 Risk Factor for Global Mortality 0 1 2 3 4 5 6
Hypertension and Cardiovascular Disease
 Hypertension and Cardiovascular Disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
Hypertension and Cardiovascular Disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
By Prof. Khaled El-Rabat
 What is The Optimum? By Prof. Khaled El-Rabat Professor of Cardiology - Benha Faculty of Medicine HT. Introduction Despite major worldwide efforts over recent decades directed at diagnosing and treating
What is The Optimum? By Prof. Khaled El-Rabat Professor of Cardiology - Benha Faculty of Medicine HT. Introduction Despite major worldwide efforts over recent decades directed at diagnosing and treating
Disclosures. Learning Objectives. Hypertension: a sprint to the finish Ontario Pharmacists Association 1
 Disclosures I have no current or past relationships with commercial entities I have received a speaker s fee from the Ontario Pharmacists Association for this learning activity Laura Tsang PharmD Sunnybrook
Disclosures I have no current or past relationships with commercial entities I have received a speaker s fee from the Ontario Pharmacists Association for this learning activity Laura Tsang PharmD Sunnybrook
Is there a mechanism of interaction between hypertension and dyslipidaemia?
 Is there a mechanism of interaction between hypertension and dyslipidaemia? Neil R Poulter International Centre for Circulatory Health NHLI, Imperial College London Daegu, Korea April 2005 Observational
Is there a mechanism of interaction between hypertension and dyslipidaemia? Neil R Poulter International Centre for Circulatory Health NHLI, Imperial College London Daegu, Korea April 2005 Observational
Jared Moore, MD, FACP
 Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
STANDARD treatment algorithm mmHg
 STANDARD treatment algorithm 130-140mmHg (i) At BASELINE, If AVERAGE SBP 1 > 140mmHg If on no antihypertensive drugs: Start 1 drug: If >55 years old / Afro-Caribbean: Calcium channel blocker (CCB) 2 If
STANDARD treatment algorithm 130-140mmHg (i) At BASELINE, If AVERAGE SBP 1 > 140mmHg If on no antihypertensive drugs: Start 1 drug: If >55 years old / Afro-Caribbean: Calcium channel blocker (CCB) 2 If
Hypertension (JNC-8)
") Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
Cedars Sinai Diabetes. Michael A. Weber
 Cedars Sinai Diabetes Michael A. Weber Speaker Disclosures I disclose that I am a Consultant for: Ablative Solutions, Boston Scientific, Boehringer Ingelheim, Eli Lilly, Forest, Medtronics, Novartis, ReCor
Cedars Sinai Diabetes Michael A. Weber Speaker Disclosures I disclose that I am a Consultant for: Ablative Solutions, Boston Scientific, Boehringer Ingelheim, Eli Lilly, Forest, Medtronics, Novartis, ReCor
Diagnosis and treatment of hypertension. Kari Nelson, MD MSHS Division of General Internal Medicine VA Puget Sound, University of Washington
 Diagnosis and treatment of hypertension Kari Nelson, MD MSHS Division of General Internal Medicine VA Puget Sound, University of Washington Outline Epidemiology Diagnosis Evaluation of individuals with
Diagnosis and treatment of hypertension Kari Nelson, MD MSHS Division of General Internal Medicine VA Puget Sound, University of Washington Outline Epidemiology Diagnosis Evaluation of individuals with
Hypertension Guidelines Michael A. Weber, MD Division of Cardiovascular Medicine State University of New York Downstate Medical Center
 Hypertension Guidelines 2016 Michael A. Weber, MD Division of Cardiovascular Medicine State University of New York Downstate Medical Center Speaker Disclosures I disclose that I am a Consultant for: Ablative
Hypertension Guidelines 2016 Michael A. Weber, MD Division of Cardiovascular Medicine State University of New York Downstate Medical Center Speaker Disclosures I disclose that I am a Consultant for: Ablative
BLOOD PRESSURE-LOWERING TREATMENT
 BLOOD PRESSURE-LOWERING TRIALS NUMBER OF PARTICIPANTS NUMBER OF PERCENTAGE OF MEAN AGE MEAN - (YEARS) TRIALS WITH ANALYSIS BY GENDER N, (%) 69,473 28,008 40.3% 70.2 3.2 3/5 (60%) APPENDIX 2 1 BLOOD PRESSURE-LOWERING
BLOOD PRESSURE-LOWERING TRIALS NUMBER OF PARTICIPANTS NUMBER OF PERCENTAGE OF MEAN AGE MEAN - (YEARS) TRIALS WITH ANALYSIS BY GENDER N, (%) 69,473 28,008 40.3% 70.2 3.2 3/5 (60%) APPENDIX 2 1 BLOOD PRESSURE-LOWERING
New Lipid Guidelines. PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids.
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
Hypertension in the Era of ACC/AHA: Practice Changing Evidence and Recommendations
 Hypertension in the Era of ACC/AHA: Practice Changing Evidence and Recommendations Gerald W. Smetana, M.D., MACP Division of General Medicine Beth Israel Deaconess Medical Center Professor of Medicine
Hypertension in the Era of ACC/AHA: Practice Changing Evidence and Recommendations Gerald W. Smetana, M.D., MACP Division of General Medicine Beth Israel Deaconess Medical Center Professor of Medicine
Hypertension in the Elderly. John Puxty Division of Geriatrics Center for Studies in Aging and Health, Providence Care
 Hypertension in the Elderly John Puxty Division of Geriatrics Center for Studies in Aging and Health, Providence Care Learning Objectives Review evidence for treatment of hypertension in elderly Consider
Hypertension in the Elderly John Puxty Division of Geriatrics Center for Studies in Aging and Health, Providence Care Learning Objectives Review evidence for treatment of hypertension in elderly Consider
Diabetes and Hypertension
 Diabetes and Hypertension William C. Cushman, MD, FAHA, FACP, FASH Chief, Preventive Medicine, Veterans Affairs Medical Center Professor, Preventive Medicine, Medicine, and Physiology University of Tennessee
Diabetes and Hypertension William C. Cushman, MD, FAHA, FACP, FASH Chief, Preventive Medicine, Veterans Affairs Medical Center Professor, Preventive Medicine, Medicine, and Physiology University of Tennessee
MANAGEMENT OF HYPERTENSION: TREATMENT THRESHOLDS AND MEDICATION SELECTION
 Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
Management of High Blood Pressure in Adults
 Management of High Blood Pressure in Adults Based on the Report from the Panel Members Appointed to the Eighth Joint National Committee (JNC8) James, P. A. (2014, February 05). 2014 Guideline for Management
Management of High Blood Pressure in Adults Based on the Report from the Panel Members Appointed to the Eighth Joint National Committee (JNC8) James, P. A. (2014, February 05). 2014 Guideline for Management
Clinical Updates in the Treatment of Hypertension JNC 7 vs. JNC 8. Lauren Thomas, PharmD PGY1 Pharmacy Practice Resident South Pointe Hospital
 Clinical Updates in the Treatment of Hypertension JNC 7 vs. JNC 8 Lauren Thomas, PharmD PGY1 Pharmacy Practice Resident South Pointe Hospital Objectives Review the Eighth Joint National Committee (JNC
Clinical Updates in the Treatment of Hypertension JNC 7 vs. JNC 8 Lauren Thomas, PharmD PGY1 Pharmacy Practice Resident South Pointe Hospital Objectives Review the Eighth Joint National Committee (JNC
Hypertension: What s new since JNC 7. Harold M. Szerlip, MD, FACP, FCCP, FASN, FNKF
 Hypertension: What s new since JNC 7 Harold M. Szerlip, MD, FACP, FCCP, FASN, FNKF Disclosures Spectral Diagnostics Site investigator Eli Lilly Site investigator ACP IM ITE writing committee NBME Step
Hypertension: What s new since JNC 7 Harold M. Szerlip, MD, FACP, FCCP, FASN, FNKF Disclosures Spectral Diagnostics Site investigator Eli Lilly Site investigator ACP IM ITE writing committee NBME Step
Pre-ALLHAT Drug Use. Diuretics. ß-Blockers. ACE Inhibitors. CCBs. Year. % of Treated Patients on Medication. CCBs. Beta Blockers.
 Pre- Drug Use % of Treated Patients on Medication 60 50 40 30 20 10 0 1978 Diuretics ß-Blockers ACE Inhibitors Year CCBs CCBs Beta Blockers Diuretics ACE Inhibitors 1980 1982 1984 1986 1988 1990 1992 IMS
Pre- Drug Use % of Treated Patients on Medication 60 50 40 30 20 10 0 1978 Diuretics ß-Blockers ACE Inhibitors Year CCBs CCBs Beta Blockers Diuretics ACE Inhibitors 1980 1982 1984 1986 1988 1990 1992 IMS
Reframe the Paradigm of Hypertension treatment Focus on Diabetes
 Reframe the Paradigm of Hypertension treatment Focus on Diabetes Paola Atallah, MD Lecturer of Clinical Medicine SGUMC EDL monthly meeting October 25,2016 Overview Physiopathology of hypertension Classification
Reframe the Paradigm of Hypertension treatment Focus on Diabetes Paola Atallah, MD Lecturer of Clinical Medicine SGUMC EDL monthly meeting October 25,2016 Overview Physiopathology of hypertension Classification
Combination therapy in the treatment of arterial hypertension. Franco Veglio SIIIA. UNIVERSITA degli STUDI di TORINO
 SIIIA UNIVERSITA degli STUDI di TORINO FACOLTA DI MEDICINA E CHIRURGIA DIPARTIMENTO DI MEDICINA ED ONCOLOGIA SPERIMENTALE SCU MEDICINA INTERNA CENTRO IPERTENSIONE ARTERIOSA AOU S.GIOVANNI BATTISTA TORINO
SIIIA UNIVERSITA degli STUDI di TORINO FACOLTA DI MEDICINA E CHIRURGIA DIPARTIMENTO DI MEDICINA ED ONCOLOGIA SPERIMENTALE SCU MEDICINA INTERNA CENTRO IPERTENSIONE ARTERIOSA AOU S.GIOVANNI BATTISTA TORINO
Jackson T. Wright, Jr. MD, PhD
 DIFFERENTIAL EFFECTS OF BLOOD PRESSURE MEDICATIONS IN BLACK PATIENTS Jackson T. Wright, Jr. MD, PhD Professor of Medicine Program Director, WT Dahms MD Clinical Research Unit Clinical and Translational
DIFFERENTIAL EFFECTS OF BLOOD PRESSURE MEDICATIONS IN BLACK PATIENTS Jackson T. Wright, Jr. MD, PhD Professor of Medicine Program Director, WT Dahms MD Clinical Research Unit Clinical and Translational
ALLHAT. ALLHAT Antihypertensive Trial Results by Baseline Diabetic & Fasting Glucose Status
 ALLHAT Antihypertensive Trial Results by Baseline Diabetic & Fasting Glucose Status 1 Introduction and Background Clinical trials have reported reduction in CV events with diuretics, CCBs, ACE inhibitors,
ALLHAT Antihypertensive Trial Results by Baseline Diabetic & Fasting Glucose Status 1 Introduction and Background Clinical trials have reported reduction in CV events with diuretics, CCBs, ACE inhibitors,
Managing Hypertension in 2016
 Managing Hypertension in 2016: Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
Managing Hypertension in 2016: Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
Objectives. Describe results and implications of recent landmark hypertension trials
 Hypertension Update Daniel Schwartz, MD Assistant Professor of Medicine Associate Medical Director of Heart Transplantation Temple University School of Medicine Disclosures I currently have no relationships
Hypertension Update Daniel Schwartz, MD Assistant Professor of Medicine Associate Medical Director of Heart Transplantation Temple University School of Medicine Disclosures I currently have no relationships
Update in Hypertension
 Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Hypertension in 2015: SPRINT-ing ahead of JNC-8. MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic
 Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
Metabolic Consequences of Anti Hypertensives: Is It Clinically Important?
 Metabolic Consequences of Anti Hypertensives: Is It Clinically Important?,FACA,FICA,MASH,FVBWG,MISCP CONSULTANT OF CARDIOLOGY DIRECTOR OF PORT-FOUAD HOSPITAL CCU Consideration of antihypertensive agents
Metabolic Consequences of Anti Hypertensives: Is It Clinically Important?,FACA,FICA,MASH,FVBWG,MISCP CONSULTANT OF CARDIOLOGY DIRECTOR OF PORT-FOUAD HOSPITAL CCU Consideration of antihypertensive agents
Difficult-to-Control & Resistant Hypertension. Anthony Viera, MD, MPH, FAHA Professor and Chair
 Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
Managing HTN in the Elderly: How Low to Go
 Managing HTN in the Elderly: How Low to Go Laxmi S. Mehta, MD, FACC The Ohio State University Medical Center Assistant Professor of Clinical Internal Medicine Clinical Director of the Women s Cardiovascular
Managing HTN in the Elderly: How Low to Go Laxmi S. Mehta, MD, FACC The Ohio State University Medical Center Assistant Professor of Clinical Internal Medicine Clinical Director of the Women s Cardiovascular
2014 HYPERTENSION GUIDELINES
 2014 HYPERTENSION GUIDELINES Eileen M. Twomey, Pharm.D., BCPS 1 Learning Objectives Describe specific blood pressure thresholds at which antihypertensive therapy should be initiated and blood pressure
2014 HYPERTENSION GUIDELINES Eileen M. Twomey, Pharm.D., BCPS 1 Learning Objectives Describe specific blood pressure thresholds at which antihypertensive therapy should be initiated and blood pressure
Don t let the pressure get to you:
 Balanced information for better care Don t let the pressure get to you: Current evidence-based goals for treating hypertension A cornerstone of primary care: Lowering high blood pressure prevents cardiovascular
Balanced information for better care Don t let the pressure get to you: Current evidence-based goals for treating hypertension A cornerstone of primary care: Lowering high blood pressure prevents cardiovascular
JNC Evidence-Based Guidelines for the Management of High Blood Pressure in Adults
 JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
Improvement of drug adherence using single pill combinations:
 Improvement of drug adherence using single pill combinations: what is the evidence? Prof. Michel Burnier Service of Nephrology and Hypertension, CHUV, Lausanne, Switzerland Potentialcauses of non-adherence
Improvement of drug adherence using single pill combinations: what is the evidence? Prof. Michel Burnier Service of Nephrology and Hypertension, CHUV, Lausanne, Switzerland Potentialcauses of non-adherence
Hypertension Management Controversies in the Elderly Patient
 Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Management of Lipid Disorders and Hypertension: Implications of the New Guidelines
 Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Hypertension targets: sorting out the confusion. Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town
 Hypertension targets: sorting out the confusion Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town Historical Perspective The most famous casualty of this approach was the
Hypertension targets: sorting out the confusion Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town Historical Perspective The most famous casualty of this approach was the
Masked Hypertension. Why Should We Care? Dr. Peter J. Lin Director Primary Care Initiatives - Canadian Heart Research Centre
 Masked Hypertension Why Should We Care? Dr. Peter J. Lin Director Primary Care Initiatives - Canadian Heart Research Centre PRESENTER DISCLOSURE Faculty: Dr. Peter Lin Relationships with commercial interests:
Masked Hypertension Why Should We Care? Dr. Peter J. Lin Director Primary Care Initiatives - Canadian Heart Research Centre PRESENTER DISCLOSURE Faculty: Dr. Peter Lin Relationships with commercial interests:
Management of Hypertension
 Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Blood Pressure Targets in Diabetes
 Stockholm, 29 th August 2010 ESC Meeting Blood Pressure Targets in Diabetes Peter M Nilsson, MD, PhD Department of Clinical Sciences University Hospital, Malmö Sweden Studies on BP in DM2 ADVANCE RCT (Lancet
Stockholm, 29 th August 2010 ESC Meeting Blood Pressure Targets in Diabetes Peter M Nilsson, MD, PhD Department of Clinical Sciences University Hospital, Malmö Sweden Studies on BP in DM2 ADVANCE RCT (Lancet
Treating Hypertension in 2018: What Makes the Most Sense Today?
 Treating Hypertension in 2018: What Makes the Most Sense Today? Daniel Blanchard, MD Professor of Medicine UC San Diego Cardiovascular Center La Jolla, California 1 2 Speaker Disclosures Consultant and/or
Treating Hypertension in 2018: What Makes the Most Sense Today? Daniel Blanchard, MD Professor of Medicine UC San Diego Cardiovascular Center La Jolla, California 1 2 Speaker Disclosures Consultant and/or
Abbreviations Cardiology I
 Cardiology I and Clinical Controversies Joseph J. Saseen, Pharm.D., FCCP, BCPS (AQ Cardiology) Reviewed by Stuart T. Haines, Pharm.D., FCCP, BCPS; and Michelle M. Richardson, Pharm.D., FCCP, BCPS Learning
Cardiology I and Clinical Controversies Joseph J. Saseen, Pharm.D., FCCP, BCPS (AQ Cardiology) Reviewed by Stuart T. Haines, Pharm.D., FCCP, BCPS; and Michelle M. Richardson, Pharm.D., FCCP, BCPS Learning
Should we prescribe aspirin and statins to all subjects over 65? (Or even all over 55?) Terje R.Pedersen Oslo University Hospital Oslo, Norway
 Terje R.Pedersen Oslo University Hospital Oslo, Norway") Should we prescribe aspirin and statins to all subjects over 65? (Or even all over 55?) Terje R.Pedersen Oslo University Hospital Oslo, Norway The Polypill A strategy to reduce cardiovascular disease by
Should we prescribe aspirin and statins to all subjects over 65? (Or even all over 55?) Terje R.Pedersen Oslo University Hospital Oslo, Norway The Polypill A strategy to reduce cardiovascular disease by
How clinically important are the results of the large trials in hypertension?
 How clinically important are the results of the large trials in hypertension? Stéphane LAURENT, MD, PhD, FESC Pharmacology Department and PARCC / INSERM U970 Hôpital Européen Georges Pompidou, Université
How clinically important are the results of the large trials in hypertension? Stéphane LAURENT, MD, PhD, FESC Pharmacology Department and PARCC / INSERM U970 Hôpital Européen Georges Pompidou, Université
We are delighted to have Dr. Roetzheim with us today to discuss Managing Hypertension in Older Adult Patients.
 Richard Roetzheim, MD, MSPH is Professor and Chair, Department of Family Medicine at the University of South Florida Morsani College of Medicine. Dr. Roetzheim has considerable experience leading NIH funded
Richard Roetzheim, MD, MSPH is Professor and Chair, Department of Family Medicine at the University of South Florida Morsani College of Medicine. Dr. Roetzheim has considerable experience leading NIH funded
Disclosures. Hypertension: Nationwide Dilemma. Learning Objectives. What s Currently Recommended? Specific Concerns 3/9/2012
 How Should We ACCOMPLISH Good Blood Pressure Control In Our VETS? Disclosures No conflicts of interest to disclose Updates in the Management of HypertensionIn the Elderly Antoine T. Jenkins, Pharm.D.,
How Should We ACCOMPLISH Good Blood Pressure Control In Our VETS? Disclosures No conflicts of interest to disclose Updates in the Management of HypertensionIn the Elderly Antoine T. Jenkins, Pharm.D.,
Management of The Patients with Hypertension and High Risk Cardiovascular Disease
 Management of The Patients with Hypertension and High Risk Cardiovascular Disease Songsak Kiatchoosakun, MD. Cardiology, Medicine Khon Kaen University CVD and Hypertension: Worldwide Morbidity and Mortality
Management of The Patients with Hypertension and High Risk Cardiovascular Disease Songsak Kiatchoosakun, MD. Cardiology, Medicine Khon Kaen University CVD and Hypertension: Worldwide Morbidity and Mortality
 Choice of therapy in esse... http://www.uptodate.co... Page 1 of 28 Official reprint from UpToDate www.uptodate.com Print Back Choice of therapy in essential hypertension: Recommendations Authors Norman
Choice of therapy in esse... http://www.uptodate.co... Page 1 of 28 Official reprint from UpToDate www.uptodate.com Print Back Choice of therapy in essential hypertension: Recommendations Authors Norman
Management of Hypertension in Women
 Management of Hypertension in Women Eliseo J. Pérez-Stable MD Professor of Medicine DGIM, Department of Medicine July 1, 2013 Declaration of full disclosure: No conflict of interest (I have never been
Management of Hypertension in Women Eliseo J. Pérez-Stable MD Professor of Medicine DGIM, Department of Medicine July 1, 2013 Declaration of full disclosure: No conflict of interest (I have never been
The Road to Renin System Optimization: Renin Inhibitor
 The Road to Renin System Optimization: Renin Inhibitor A New Perspective on the Renin-Angiotensin System (RAS) Yong-Jin Kim, MD Seoul National University Hospital Human and Economic Costs of Hypertension
The Road to Renin System Optimization: Renin Inhibitor A New Perspective on the Renin-Angiotensin System (RAS) Yong-Jin Kim, MD Seoul National University Hospital Human and Economic Costs of Hypertension
Difficult to Treat Hypertension
 Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets
 New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of
New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of
Impact of recent landmark clinical trials on hypertension treatment
 Review: Clinical Trial Outcomes Impact of recent landmark clinical trials on hypertension treatment Clin. Invest. (2011) 1(8), 1141 1154 High blood pressure remains an important global cause of cardiovascular
Review: Clinical Trial Outcomes Impact of recent landmark clinical trials on hypertension treatment Clin. Invest. (2011) 1(8), 1141 1154 High blood pressure remains an important global cause of cardiovascular
The State of Hypertension in NZ in 2010 personal view
 The State of Hypertension in NZ in 2010 personal view Patient referred to medical clinic Dear Dr, Please see this man with resistant hypertension 50 year old European male Blood Pressure on current meds
The State of Hypertension in NZ in 2010 personal view Patient referred to medical clinic Dear Dr, Please see this man with resistant hypertension 50 year old European male Blood Pressure on current meds
Updates in Cardiovascular Recommendations for Diabetic Patients
 Updates in Cardiovascular Recommendations for Diabetic Patients Chris Tawwater, Pharm.D., BCPS Clinical Pharmacist, Abilene Regional Medical Center Assistant Professor, Adult Medicine Division Pharmacotherapy
Updates in Cardiovascular Recommendations for Diabetic Patients Chris Tawwater, Pharm.D., BCPS Clinical Pharmacist, Abilene Regional Medical Center Assistant Professor, Adult Medicine Division Pharmacotherapy
Hypertension. Most important public health problem in developed countries
 Hypertension Strategy for Continued Success in Treatment for the 21st Century November 15, 2005 Arnold B. Meshkov, M.D. Associate Professor of Medicine Temple University School of Medicine Philadelphia,
Hypertension Strategy for Continued Success in Treatment for the 21st Century November 15, 2005 Arnold B. Meshkov, M.D. Associate Professor of Medicine Temple University School of Medicine Philadelphia,
Update sulla terapia antiipertensiva e antiaggregante nel paziente cardiometabolico
 Update sulla terapia antiipertensiva e antiaggregante nel paziente cardiometabolico G. Mazzanti UO Cardiologia Ospedale SS. Annunziata, Cento (FE) AUSL di Ferrara Antiplatelet therapy Aspirin Aspirin:
Update sulla terapia antiipertensiva e antiaggregante nel paziente cardiometabolico G. Mazzanti UO Cardiologia Ospedale SS. Annunziata, Cento (FE) AUSL di Ferrara Antiplatelet therapy Aspirin Aspirin:
Individual management of arterial hypertension. Doumas Michael, Internist Lecturer, Aristotle University, Thessaloniki
 Individual management of arterial hypertension Doumas Michael, Internist Lecturer, Aristotle University, Thessaloniki From Population to Individual Management of Arterial Hypertension Epidemiologic impact
Individual management of arterial hypertension Doumas Michael, Internist Lecturer, Aristotle University, Thessaloniki From Population to Individual Management of Arterial Hypertension Epidemiologic impact
First line treatment of primary hypertension
 First line treatment of primary hypertension Dr. Vijaya Musini Assistant Professor, Dept. Anesthesiology, Pharmacology and Therapeutics Manager, Drug Assessment Working Group Therapeutics Initiative Editor,
First line treatment of primary hypertension Dr. Vijaya Musini Assistant Professor, Dept. Anesthesiology, Pharmacology and Therapeutics Manager, Drug Assessment Working Group Therapeutics Initiative Editor,
Hypertension diagnosis (see detail document) Diabetic. Target less than 130/80mmHg
 Diabetic. Target less than 130/80mmHg") Hypertension diagnosis (see detail document) Non-diabetic Diabetic Very elderly (older than 80 years) Target less than 140/90mmHg Target less than 130/80mmHg Consider SBP target less than 150mmHg Non-diabetic
Hypertension diagnosis (see detail document) Non-diabetic Diabetic Very elderly (older than 80 years) Target less than 140/90mmHg Target less than 130/80mmHg Consider SBP target less than 150mmHg Non-diabetic
Hypertension mechanisms
 הטיפול בלחץ דם בעזרת תרופות מישלב Hypertension mechanisms ESH Task Force Document. J Hypertens 2009 The history of development of antihypertensive drugs ESH Task Force Document. J Hypertens 2009 הטיפול
הטיפול בלחץ דם בעזרת תרופות מישלב Hypertension mechanisms ESH Task Force Document. J Hypertens 2009 The history of development of antihypertensive drugs ESH Task Force Document. J Hypertens 2009 הטיפול
Amlodipine/Valsartan (Exforge ) Changing the Landscape of BP Management
 Changing the Landscape of BP Management") Amlodipine/Valsartan (Exforge ) Changing the Landscape of BP Management Bum-Kee Hong Yongdong Severance Hospital Yonsei University College of Medicine Rationale for Multiple-Mechanism Therapy Inadequacy
Amlodipine/Valsartan (Exforge ) Changing the Landscape of BP Management Bum-Kee Hong Yongdong Severance Hospital Yonsei University College of Medicine Rationale for Multiple-Mechanism Therapy Inadequacy
MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure. No relevant financial relationships. Blood Pressure and Risk
 MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
Hypertension Management Focus on new RAAS blocker. Disclosure
 Hypertension Management Focus on new RAAS blocker Rameshkumar Raman M.D Endocrine Associates of The Quad Cities Disclosure Speaker bureau Abbott, Eli Lilly, Novo Nordisk, Novartis, Takeda, Merck, Solvay
Hypertension Management Focus on new RAAS blocker Rameshkumar Raman M.D Endocrine Associates of The Quad Cities Disclosure Speaker bureau Abbott, Eli Lilly, Novo Nordisk, Novartis, Takeda, Merck, Solvay