*Core lab for numerous trials, for which I receive no direct compensation from sponsors.
|
|
|
- Asher Harris
- 6 years ago
- Views:
Transcription
1 Rebecca T. Hahn, MD, FACC, FASE Director of Interventional Echo Professor of Medicine Columbia University Company Abbott Vascular Gore&Assoc NaviGATE Medtronic Boston Scientific GE Medical Philips Healthcare Nature of Affiliation Consultant/Advisory Board Unlabeled Product Usage None Speaker None *Core lab for numerous trials, for which I receive no direct compensation from sponsors. 1
 anesthetic care or conscious sedation Imaging Advantages Standard windows for assessing")




 factors (i.e. calcific acoustic")
 and 3D imaging Probe interference with fluoroscopic Limited")

2 Parameter TTE TEE Sedation during None required (sedation for procedure General anesthesia, monitored TAVR only) anesthetic care or conscious sedation Imaging Advantages Standard windows for assessing ventricular Higher resolution with high frame rates and valvular structure & function for 2D and 3D imaging Pre-procedural imaging may avoid complications (i.e. paravalvular regurgitation, annular/aortic rupture, coronary occlusion) Immediate, accurate intra-procedural diagnosis of complications Imaging Disadvantages Image quality dependent on patient factors Special windows required for assessing (i.e. chest morphology, lung hyperinflation, ventricular and valvular structure & suboptimal patient positioning) function Procedural delay during image acquisition Image quality dependent on patient (to minimize radiation exposure to imager) factors (i.e. calcific acoustic shadowing, Non-continuous imaging during procedure cardiac position relative to esophagus Low resolution with low frame rates for 2D and stomach) and 3D imaging Probe interference with fluoroscopic Limited imaging windows for nontransfemoral access routes probe) imaging (minimized by articulation of Other Advantages Early recovery and discharge Continuous imaging throughout procedure, irrespective of access route Other Disadvantages Possible higher radiation exposure to Need for post-procedure monitoring imager (Note: may not be different than for TTE) Interference with sterile field Trauma to oropharynx, esophagus or stomach Retroflexion Anteflexion Right Flexion Left Flexion Left+Ante Right+ Ante Continuous Imaging is KEY to early detection of complications 2



3 DOI: /j.echo Figure 4 Figure 5 Pre-procedural Imaging Journal of the American Society of Echocardiography DOI: ( /j.echo ) Copyright 2017 American Society of EchocardiographyTerms and Conditions 3



4 DOI: /j.echo Post-procedural Imaging Figure 8 Figure 12 Journal of the American Society of Echocardiography DOI: ( /j.echo ) Copyright 2017 American Society of Echocardiography Terms and Conditions 4

5 DOI: /j.echo An 80-year-old female with a past medical history of Severe mitral stenosis status-post valvuloplasty in Moscow in 1963 Atrial fibrillation on Coumadin Hypertension Chronic kidney disease Complained of increased dyspnea on exertion and fatigue that started six months prior and had progressively worsened. 5


. Mitral valve area of 1.")


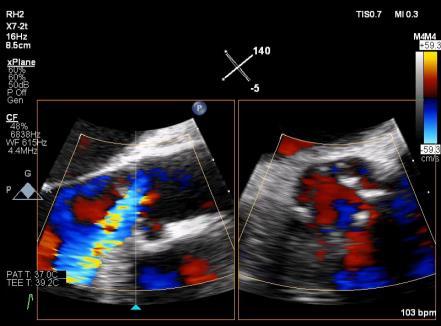
6 Pre-procedural transthoracic echocardiogram showed: Rheumatic mitral valve with stenosis and a mitral valvuloplasty score of 9 (Mobility = 2, Leaflet thickness = 2, Subvalvular thickening = 4 and Calcification = 2) Mean gradient 5 mmhg Heavily calcified aortic valve. Severe aortic stenosis Peak/mean gradients of 96.4/43.8mmHg Ejection fraction 65-70% Given the findings on transthoracic echocardiogram the plan was to perform a transcatheter aortic valve implantation (TAVI). Mitral valve area of 1.2 cm 2 by continuity equation Dense smoke in markedly dilated LAA (no MR) Intra-procedural TEE showed: Severe mitral stenosis by multiple methods Dense smoke in the LAA consistent with very slow flow but no thrombus No mitral regurgitation Mitral valve area of 1.35 cm 2 by 3D planimetry In light of TEE findings, an intra-procedural decision was made to perform a percutaneous balloon mitral valvuloplasty (PBMV) prior to TAVR 6







7 Valvuloplasty Valvuloplasty Percutaneous balloon mitral valvuloplasty was performed using a 23mm Inoue balloon. Two inflations were performed resulting in lateral commissural fracture and improved valve opening Pre-PBMV Post-PBMV Planimetered MVOA= 1.7 cm 2 Single jet of mild mitral regurgitation was seen (EROA by 3D = 13mm 2 ) Smoke resolved 7

")
")

8 Pre-PBMV Post-PBMV MG 9.1 mmhg MG 4.9 mmhg Annular perimeter = 67 mm Annulus-to-left main distance of 10.7mm and a left coronary cusp (LCC) length of 14.5 mm with a sinus of Valsalva (SOV) diameter of 2.85 cm. A 26mm Evolut-R selected Significant discordance L Main and LCC, small SOV 8



9 During BAV the left main coronary ostium was covered by the left coronary cusp (yellow arrow) on TEE with slow/faint filling was seen on contrast injection (red arrow). 20mm Z-Med II balloon 6F JL 3.5 6F Guideliner 3.5 x 15mm DES placed in mlad 9





10 Evolut-R 26mm ST elevations noted on monitor Evolut-R 26mm Marked reduced flow in LM ostium 10





11 Urgent stent deployment in LM Deployed at 12 atm ST segments rapidly resolved and no wall motion abnormalities were detected 11


12 Final AR Assessment 2+ AR No Post-dilatation was performed 83 year-old man Class III heart failure Known Severe AS for 2 years with preserved EF PV 4.5 m/s MG 43 mmhg AVA 0.7cm 2 EF 55%, Moderate MR. Mild phtn. Type II DM, CKD on HD, Morbid obesity, OSA on BiPAP TAVR/SAVR were deferred in the past since he had Stevens- Johnson syndrome when exposed to contrast dye, twice. In the past 5 months experienced increased fatigue after HD and was requiered to start on Midodrine. STS 13% 12




13 26 mm vs 29 mm valve 13


14 Trivial agitated bubbles in the LV during BAV Good Annular Sealing Aorta stretching 14



15 15
16 Trivial PVL No central Ao Regurgitation AVA 2.33 cm2 PV 1.6 m/s P/MG: 11/5 mmhg DI 0.44 Mild MR (No change during procedure) HPI: 84 y/o F with Diastolic HF (NYHAIV,EF 50%), Aortic insufficiency, ESRD(on HD MWF, LUE AV fistula;still makes some urine),copd(no intubations), HTN, hyperlipidemia, anemia, h/o GIB 2/2 to high consumption of NSAIDS(pt now reports allergy to ASA/NSAIDS Experiencing increasing episodes of SOB, resulting in increased hospitalizations, on 2/5/18 pt presented to Outside Hospital ED c/o SOB was admitted Echo showed worsening aortic regurgitation 16


17 17





18 3D EROA = 50 mm2 PISA EROA = 40 mm2 Quantitative Doppler EROA = 51 mm2 18




19 Repositioning required: Pacing used 19




20 Complete Heart Block with lower position Original Pacemaker Dislodged Removal of first Pacer 20




21 21

22 22
TAVR: Echo Measurements Pre, Post And Intra Procedure
 2017 ASE Florida, Orlando, FL October 10, 2017 8:00 8:25 AM 25 min TAVR: Echo Measurements Pre, Post And Intra Procedure Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
2017 ASE Florida, Orlando, FL October 10, 2017 8:00 8:25 AM 25 min TAVR: Echo Measurements Pre, Post And Intra Procedure Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
How Do I Evaluate a Patient Being Considered for TAVR? Sunday, February 14, :00 11:25 PM 25 min
 2016 ASE State of the Art Echocardiography Course Tucson, AZ How Do I Evaluate a Patient Being Considered for TAVR? Sunday, February 14, 2016 11:00 11:25 PM 25 min 1 M U H A M E D S A R I Ć, M D, P H D
2016 ASE State of the Art Echocardiography Course Tucson, AZ How Do I Evaluate a Patient Being Considered for TAVR? Sunday, February 14, 2016 11:00 11:25 PM 25 min 1 M U H A M E D S A R I Ć, M D, P H D
Echo Assessment Pre-TAVI
 Disclosure Statement of Financial Interest Within the past 12 months, I or my spouse/partner have had a financial Interest /arrangement or affiliation with the organization(s) listed below Echocardiographic
Disclosure Statement of Financial Interest Within the past 12 months, I or my spouse/partner have had a financial Interest /arrangement or affiliation with the organization(s) listed below Echocardiographic
MITRAL STENOSIS: MANY FLAVORS Rheumatic and Calcification. Rheumatic Mitral Stenosis 76yo male
 MITRAL STENOSIS: MANY FLAVORS Rheumatic and Calcification David S Rubenson MD FACC FASE Founding Director, Cardiac Non-Invasive Laboratory Scripps Clinic Medical Group number 1 Rheumatic Mitral Stenosis
MITRAL STENOSIS: MANY FLAVORS Rheumatic and Calcification David S Rubenson MD FACC FASE Founding Director, Cardiac Non-Invasive Laboratory Scripps Clinic Medical Group number 1 Rheumatic Mitral Stenosis
Percutaneous Therapy for Calcific Mitral Valve Disease
 31 st Annual State of the Art Echocardiography San Diego, CA February 18, 2018 5:00 5:15 PM 15 min Percutaneous Therapy for Calcific Mitral Valve Disease Muhamed Sarić MD, PhD, MPA Director of Noninvasive
31 st Annual State of the Art Echocardiography San Diego, CA February 18, 2018 5:00 5:15 PM 15 min Percutaneous Therapy for Calcific Mitral Valve Disease Muhamed Sarić MD, PhD, MPA Director of Noninvasive
New Cardiovascular Devices and Interventions: Non-Contrast MRI for TAVR Abhishek Chaturvedi Assistant Professor. Cardiothoracic Radiology
 New Cardiovascular Devices and Interventions: Non-Contrast MRI for TAVR Abhishek Chaturvedi Assistant Professor Cardiothoracic Radiology Disclosure I have no disclosure pertinent to this presentation.
New Cardiovascular Devices and Interventions: Non-Contrast MRI for TAVR Abhishek Chaturvedi Assistant Professor Cardiothoracic Radiology Disclosure I have no disclosure pertinent to this presentation.
PARAVALVULAR LEAK POST TAVR. Elements of Follow-up Post TAVR
 PARAVALVULAR LEAK POST TAVR David S Rubenson MD FACC FASE Founding Director, Cardiac Non-Invasive Laboratory Scripps Clinic Medical Group number 1 Elements of Follow-up Post TAVR JACC CV Imag 2016;9:193
PARAVALVULAR LEAK POST TAVR David S Rubenson MD FACC FASE Founding Director, Cardiac Non-Invasive Laboratory Scripps Clinic Medical Group number 1 Elements of Follow-up Post TAVR JACC CV Imag 2016;9:193
Imaging in TAVI. Jeroen J Bax Dept of Cardiology Leiden Univ Medical Center The Netherlands Davos, feb 2013
 Imaging in TAVI Jeroen J Bax Dept of Cardiology Leiden Univ Medical Center The Netherlands Davos, feb 2013 Research grants: Medtronic, Biotronik, Boston Scientific, St Jude, BMS imaging, GE Healthcare,
Imaging in TAVI Jeroen J Bax Dept of Cardiology Leiden Univ Medical Center The Netherlands Davos, feb 2013 Research grants: Medtronic, Biotronik, Boston Scientific, St Jude, BMS imaging, GE Healthcare,
What I Have Learned from 3D Imaging of Heart Valve Disease
 What I Have Learned from 3D Imaging of Heart Valve Disease Rebecca T. Hahn, MD Director of Interventional Echocardiography Columbia University Core Lab Director for multiple tricuspid device trials for
What I Have Learned from 3D Imaging of Heart Valve Disease Rebecca T. Hahn, MD Director of Interventional Echocardiography Columbia University Core Lab Director for multiple tricuspid device trials for
Comments restricted to Sapien and Corevalve 9/12/2016. Disclosures: Core Lab contracts with Edwards Lifesciences, Middlepeak, Medtronic
 Para-ValvularRegurgitation post TAVR: Predict, Prevent, Quantitate, Manage Linda D. Gillam, MD, MPH, FACC, FASE Chair, Department of Cardiovascular Medicine Morristown Medical Center/Atlantic Health System
Para-ValvularRegurgitation post TAVR: Predict, Prevent, Quantitate, Manage Linda D. Gillam, MD, MPH, FACC, FASE Chair, Department of Cardiovascular Medicine Morristown Medical Center/Atlantic Health System
Procedural Guidance of TAVR: How to Assure it Goes Right and What to Do If It Doesn t
 Procedural Guidance of TAVR: How to Assure it Goes Right and What to Do If It Doesn t James D. Thomas, M.D., F.A.C.C. Department of Cardiovascular Medicine Heart and Vascular Institute Cleveland Clinic
Procedural Guidance of TAVR: How to Assure it Goes Right and What to Do If It Doesn t James D. Thomas, M.D., F.A.C.C. Department of Cardiovascular Medicine Heart and Vascular Institute Cleveland Clinic
Stress Testing in Valvular Disease
 2017 ASE Florida Orlando, FL October 10, 2017 2:40 2:50 PM 10 min Grand Harbor Ballroom South Stress Testing in Valvular Disease Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
2017 ASE Florida Orlando, FL October 10, 2017 2:40 2:50 PM 10 min Grand Harbor Ballroom South Stress Testing in Valvular Disease Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
Optimal Imaging Technique Prior to TAVI -Echocardiography-
 2014 KSC meeting Optimal Imaging Technique Prior to TAVI -Echocardiography- Geu-Ru Hong, M.D. Ph D Associate Professor of Medicine Division of Cardiology, Severance Cardiovascular Hospital Yonsei University
2014 KSC meeting Optimal Imaging Technique Prior to TAVI -Echocardiography- Geu-Ru Hong, M.D. Ph D Associate Professor of Medicine Division of Cardiology, Severance Cardiovascular Hospital Yonsei University
HOW IMPORTANT ARE THESE ECHO MEASUREMENTS ANYWAY?
 HOW IMPORTANT ARE THESE ECHO MEASUREMENTS ANYWAY? John D. Carroll, MD Professor, Director of Interventional Cardiology and Co-Medical Director of the Cardiac and Vascular Center, University of Colorado
HOW IMPORTANT ARE THESE ECHO MEASUREMENTS ANYWAY? John D. Carroll, MD Professor, Director of Interventional Cardiology and Co-Medical Director of the Cardiac and Vascular Center, University of Colorado
DISCLOSURE. Relevant Financial Relationship(s) Off Label Usage. None. None
 Off Label Usage. None. None") Echo for TAVR Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echocardiography Associate Director, Cardiology Fellowship Mayo
Echo for TAVR Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echocardiography Associate Director, Cardiology Fellowship Mayo
Conflict of Interests
 Introduction to Interventional Echocardiography Roberto M Lang, MD Tomtec Conflict of Interests Research Grants Philips Medical Imaging Research Grants Speakers bureau Advisory bureau 1 Structural Heart
Introduction to Interventional Echocardiography Roberto M Lang, MD Tomtec Conflict of Interests Research Grants Philips Medical Imaging Research Grants Speakers bureau Advisory bureau 1 Structural Heart
Case Presentations TAVR: The Good Bad and The Ugly
 Case Presentations TAVR: The Good Bad and The Ugly Vincent J. Pompili, MD, FACC, FSCAI Professor of Internal Medicine Director of Interventional Cardiovascular Medicine and Cardiac Catheterization Laboratories
Case Presentations TAVR: The Good Bad and The Ugly Vincent J. Pompili, MD, FACC, FSCAI Professor of Internal Medicine Director of Interventional Cardiovascular Medicine and Cardiac Catheterization Laboratories
Echocardiographic Evaluation of Aortic Valve Prosthesis
 Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Co Director, Echocardiography, Director, Interventional Cardiology Research, Beaumont Health System
Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Co Director, Echocardiography, Director, Interventional Cardiology Research, Beaumont Health System
MITRAL STENOSIS. Joanne Cusack
 MITRAL STENOSIS Joanne Cusack BSE Breakdown Recognition of rheumatic mitral stenosis Qualitative description of valve and sub-valve calcification and fibrosis Measurement of orifice area by planimetry
MITRAL STENOSIS Joanne Cusack BSE Breakdown Recognition of rheumatic mitral stenosis Qualitative description of valve and sub-valve calcification and fibrosis Measurement of orifice area by planimetry
Boston, MA 2 Service Chief, Cardiovascular Imaging, Department of Radiology, Massachusetts General Hospital,
 Chapter 9: Cardiac imaging for TAVR: CTA, TTE, TEE, and valve sizing Lucy M. Safi, DO 1 ; Brian Ghoshhajra, MD, MBA 2 ; Jonathan J. Passeri, MD 3 1 Clinical and Research Fellow in Medicine, Massachusetts
Chapter 9: Cardiac imaging for TAVR: CTA, TTE, TEE, and valve sizing Lucy M. Safi, DO 1 ; Brian Ghoshhajra, MD, MBA 2 ; Jonathan J. Passeri, MD 3 1 Clinical and Research Fellow in Medicine, Massachusetts
TAVR Cases. Disclosures 2/17/2018. February 17, :15 3:30 PM 15 min
 31 st Annual State of the Art Echocardiography San Diego, CA February 17, 2018 3:15 3:30 PM 15 min TAVR Cases Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate Professor
31 st Annual State of the Art Echocardiography San Diego, CA February 17, 2018 3:15 3:30 PM 15 min TAVR Cases Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate Professor
Disclosures. ESC Munich 2012 Bernard Iung, MD Consultancy: Abbott Boehringer Ingelheim Bayer Servier Valtech
 Disclosures ESC Munich 2012 Bernard Iung, MD Consultancy: Abbott Boehringer Ingelheim Bayer Servier Valtech Speaker s fee Edwards Lifesciences Sanofi-Aventis Decision Making in Patients with Multivalvular
Disclosures ESC Munich 2012 Bernard Iung, MD Consultancy: Abbott Boehringer Ingelheim Bayer Servier Valtech Speaker s fee Edwards Lifesciences Sanofi-Aventis Decision Making in Patients with Multivalvular
Echocardiographic Evaluation of Aortic Valve Prosthesis
 Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Co-Director, Echocardiography, Director, Interventional Cardiology Research, Beaumont Health System
Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Co-Director, Echocardiography, Director, Interventional Cardiology Research, Beaumont Health System
Severity of AS Degree of AV calcification (? Bicuspid AV), annulus size, & aortic root
, annulus size, & aortic root") The role of Cardiac Imaging modalities in evaluation & selection of patients for Trans-catheter Aortic Valve Implantation Dr.Saeed AL Ahmari Consultant Cardiologist Prince Sultan Cardaic Center, Riyadh
The role of Cardiac Imaging modalities in evaluation & selection of patients for Trans-catheter Aortic Valve Implantation Dr.Saeed AL Ahmari Consultant Cardiologist Prince Sultan Cardaic Center, Riyadh
Culprit vs Multivalve Transcatheter Intervention
 Culprit vs Multivalve Transcatheter Intervention Howard C. Herrmann, MD, FACC, MSCAI John Bryfogle Professor of Cardiovascular Medicine and Surgery Health System Director for Interventional Cardiology
Culprit vs Multivalve Transcatheter Intervention Howard C. Herrmann, MD, FACC, MSCAI John Bryfogle Professor of Cardiovascular Medicine and Surgery Health System Director for Interventional Cardiology
22/06/2017. Oxford City. Transcatheter aortic valve replacement 2017 guidelines. 1. First time I have heard about it. 2.
 Oxford City Transcatheter aortic valve replacement 2017 guidelines Monday 19 th June Jim Newton Oxford Oxford University Hospitals NHS FT How familiar are you with TAVR? 1. First time I have heard about
Oxford City Transcatheter aortic valve replacement 2017 guidelines Monday 19 th June Jim Newton Oxford Oxford University Hospitals NHS FT How familiar are you with TAVR? 1. First time I have heard about
TEE guided TAVR using BASILICA technique in patient with stenotic Freestyle aortic bioprosthesis
 TEE guided TAVR using BASILICA technique in patient with stenotic Freestyle aortic bioprosthesis Zuyue Wang MD Associate professor, Georgetown University School of Medicine MedStar Heart and Vascular Institute
TEE guided TAVR using BASILICA technique in patient with stenotic Freestyle aortic bioprosthesis Zuyue Wang MD Associate professor, Georgetown University School of Medicine MedStar Heart and Vascular Institute
Aortic Stenosis and TAVR TARUN NAGRANI, MD INTERVENTIONAL AND ENDOVASCULAR CARDIOLOGIST, SOMC
 Aortic Stenosis and TAVR TARUN NAGRANI, MD INTERVENTIONAL AND ENDOVASCULAR CARDIOLOGIST, SOMC No Financial Disclosures Aortic Stenosis AS is an insidious disease with a long latency period followed by
Aortic Stenosis and TAVR TARUN NAGRANI, MD INTERVENTIONAL AND ENDOVASCULAR CARDIOLOGIST, SOMC No Financial Disclosures Aortic Stenosis AS is an insidious disease with a long latency period followed by
Bogdan A. Popescu. University of Medicine and Pharmacy Bucharest, Romania. EAE Course, Bucharest, April 2010
 Bogdan A. Popescu University of Medicine and Pharmacy Bucharest, Romania EAE Course, Bucharest, April 2010 This is how it started Mitral stenosis at a glance 2D echo narrow diastolic opening of MV leaflets
Bogdan A. Popescu University of Medicine and Pharmacy Bucharest, Romania EAE Course, Bucharest, April 2010 This is how it started Mitral stenosis at a glance 2D echo narrow diastolic opening of MV leaflets
Transcatheter Aortic Valve Implantation Management of risks and complications
 Transcatheter Aortic Valve Implantation Management of risks and complications TAVI Summit, Seoul, Korea, Spetember 3rd, 2011 Alain Cribier University of Rouen, France Complications of TAVI Depending on
Transcatheter Aortic Valve Implantation Management of risks and complications TAVI Summit, Seoul, Korea, Spetember 3rd, 2011 Alain Cribier University of Rouen, France Complications of TAVI Depending on
Successful Percutaneous Closure of Mitral Bioprosthetic Paravalvular Leak Using Figulla ASD Occluder
 Hans R. Figulla, M.D., PhD ; Ali Hamadanchi, M.D. Medicine, Pneumology Universitity Hospital, Jena, Germany Successful Percutaneous Closure of Mitral Bioprosthetic Paravalvular Leak Using Figulla ASD Occluder
Hans R. Figulla, M.D., PhD ; Ali Hamadanchi, M.D. Medicine, Pneumology Universitity Hospital, Jena, Germany Successful Percutaneous Closure of Mitral Bioprosthetic Paravalvular Leak Using Figulla ASD Occluder
Valve Replacement without a Scalpel Transcatheter Aortic Valve Replacement (TAVR) Charles T. Klodell, M.D.
 Charles T. Klodell, M.D.") Valve Replacement without a Scalpel Transcatheter Aortic Valve Replacement (TAVR) Charles T. Klodell, M.D. Professor, Thoracic and Cardiovascular Surgery University of Florida klodell@surgery.ufl.edu Disclosures
Valve Replacement without a Scalpel Transcatheter Aortic Valve Replacement (TAVR) Charles T. Klodell, M.D. Professor, Thoracic and Cardiovascular Surgery University of Florida klodell@surgery.ufl.edu Disclosures
Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know
 Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know James F. Burke, MD Program Director Cardiovascular Disease Fellowship Lankenau Medical Center Disclosure Dr. Burke has no conflicts
Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know James F. Burke, MD Program Director Cardiovascular Disease Fellowship Lankenau Medical Center Disclosure Dr. Burke has no conflicts
Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants
 Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants Martin G. Keane, MD, FASE Professor of Medicine Lewis Katz School of Medicine at Temple University Basic root structure Parasternal
Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants Martin G. Keane, MD, FASE Professor of Medicine Lewis Katz School of Medicine at Temple University Basic root structure Parasternal
TAVR SPRING 2017 The evolution of TAVR
 TAVR SPRING 2017 The evolution of TAVR Matthew Johnson, MD Disclosers None Evolution of the Balloon- Expandable Transcatheter Valves Cribier 2002 SAPIEN 2006 SAPIEN XT 2009 SAPIEN 3 2013 * Sheath compatibility
TAVR SPRING 2017 The evolution of TAVR Matthew Johnson, MD Disclosers None Evolution of the Balloon- Expandable Transcatheter Valves Cribier 2002 SAPIEN 2006 SAPIEN XT 2009 SAPIEN 3 2013 * Sheath compatibility
TRANSCATHETER AORTIC VALVE IMPLANTATION: PSCC EXPERIENCE DR HUSSEIN ALAMRI PSCC RIYADH
 TRANSCATHETER AORTIC VALVE IMPLANTATION: PSCC EXPERIENCE DR HUSSEIN ALAMRI PSCC RIYADH Available systems: Edwards (TA and TF) and Core valve. INTRODUCTION 3 4% 0f > 65 y. 30 40% of elderly denied surgery,.
TRANSCATHETER AORTIC VALVE IMPLANTATION: PSCC EXPERIENCE DR HUSSEIN ALAMRI PSCC RIYADH Available systems: Edwards (TA and TF) and Core valve. INTRODUCTION 3 4% 0f > 65 y. 30 40% of elderly denied surgery,.
Congenital. Unicuspid Bicuspid Quadricuspid
 David Letterman s Top 10 Aortic Stenosis The victim can be anyone: Echo is the question and the answer!!!! Hilton Head Island Echocardiography Conference 2012 Timothy E. Paterick, MD, JD, MBA Christopher
David Letterman s Top 10 Aortic Stenosis The victim can be anyone: Echo is the question and the answer!!!! Hilton Head Island Echocardiography Conference 2012 Timothy E. Paterick, MD, JD, MBA Christopher
Edwards Sapien. Medtronic CoreValve. Inoperable FDA approved High risk: in trials. FDA approved
 Transcatheter Aortic Valve Replacement Symptomatic Aortic Stenosis Asymptomatic Juan Crestanello, MD Interim Director, Division of Cardiac Surgery Associate Professor Division of Cardiac Surgery The Ohio
Transcatheter Aortic Valve Replacement Symptomatic Aortic Stenosis Asymptomatic Juan Crestanello, MD Interim Director, Division of Cardiac Surgery Associate Professor Division of Cardiac Surgery The Ohio
Evolut R in bicuspid valve anatomies
 Evolut R in bicuspid valve anatomies U. Gerckens MD University of Rostock, Germany Potential conflicts of interest Speaker's name: Ulrich Gerckens I have the following potential conflicts of interest to
Evolut R in bicuspid valve anatomies U. Gerckens MD University of Rostock, Germany Potential conflicts of interest Speaker's name: Ulrich Gerckens I have the following potential conflicts of interest to
Federico M Asch MD, FASE MedStar Heart and Vascular Institute Georgetown University Washington, DC
 TAVR: When Things go Wrong Federico M Asch MD, FASE MedStar Heart and Vascular Institute Georgetown University Washington, DC Disclosures Academic Echo Core Lab Abbott / St Jude Medical Edwards Medtronic
TAVR: When Things go Wrong Federico M Asch MD, FASE MedStar Heart and Vascular Institute Georgetown University Washington, DC Disclosures Academic Echo Core Lab Abbott / St Jude Medical Edwards Medtronic
CIPG Transcatheter Aortic Valve Replacement- When Is Less, More?
 CIPG 2013 Transcatheter Aortic Valve Replacement- When Is Less, More? James D. Rossen, M.D. Professor of Medicine and Neurosurgery Director, Cardiac Catheterization Laboratory and Interventional Cardiology
CIPG 2013 Transcatheter Aortic Valve Replacement- When Is Less, More? James D. Rossen, M.D. Professor of Medicine and Neurosurgery Director, Cardiac Catheterization Laboratory and Interventional Cardiology
New York Valves Patient focused evidence-based approach. New York City: 6 December Antonio Colombo
 New York Valves 2018 Patient focused evidence-based approach New York City: 6 December 2018 Antonio Colombo Speaker 7 EMO GVM Centro Cuore Columbus Milan, Italy No conflicts to report Vascular complications
New York Valves 2018 Patient focused evidence-based approach New York City: 6 December 2018 Antonio Colombo Speaker 7 EMO GVM Centro Cuore Columbus Milan, Italy No conflicts to report Vascular complications
Structural Heart Disease Transcatheter Aortic Valve Replacement (TAVR)
") Structural Heart Disease Transcatheter Aortic Valve Replacement (TAVR) Kathleen Harper DO FACC FACP 87 Chief, Cardiology Section VA Maine Healthcare Kathleen.Harper@va.gov Prevalence of Aortic Stenosis
Structural Heart Disease Transcatheter Aortic Valve Replacement (TAVR) Kathleen Harper DO FACC FACP 87 Chief, Cardiology Section VA Maine Healthcare Kathleen.Harper@va.gov Prevalence of Aortic Stenosis
Menachem M. Weiner Assistant Professor of Anesthesiology Icahn School of Medicine at Mount Sinai
 Menachem M. Weiner Assistant Professor of Anesthesiology Icahn School of Medicine at Mount Sinai Anesthetic care and considerations Intraoperative events TEE Perioperative complications Most common valvular
Menachem M. Weiner Assistant Professor of Anesthesiology Icahn School of Medicine at Mount Sinai Anesthetic care and considerations Intraoperative events TEE Perioperative complications Most common valvular
When Does 3D Echo Make A Difference?
 When Does 3D Echo Make A Difference? Wendy Tsang, MD, SM Assistant Professor, University of Toronto Toronto General Hospital, University Health Network 1 Practical Applications of 3D Echocardiography Recommended
When Does 3D Echo Make A Difference? Wendy Tsang, MD, SM Assistant Professor, University of Toronto Toronto General Hospital, University Health Network 1 Practical Applications of 3D Echocardiography Recommended
PROSTHETIC VALVE BOARD REVIEW
 PROSTHETIC VALVE BOARD REVIEW The correct answer D This two chamber view shows a porcine mitral prosthesis with the typical appearance of the struts although the leaflets are not well seen. The valve
PROSTHETIC VALVE BOARD REVIEW The correct answer D This two chamber view shows a porcine mitral prosthesis with the typical appearance of the struts although the leaflets are not well seen. The valve
Echocardiographic Evaluation of Aortic Valve Prosthesis
 Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Director, Interventional Cardiology Research, Beaumont Health System Associate Professor of Medicine,
Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Director, Interventional Cardiology Research, Beaumont Health System Associate Professor of Medicine,
ECHO HAWAII. Role of Stress Echo in Valvular Heart Disease. Not only ischemia! Cardiomyopathy. Prosthetic Valve. Diastolic Dysfunction
 Role of Stress Echo in Valvular Heart Disease ECHO HAWAII January 15 19, 2018 Kenya Kusunose, MD, PhD, FASE Tokushima University Hospital Japan Not only ischemia! Cardiomyopathy Prosthetic Valve Diastolic
Role of Stress Echo in Valvular Heart Disease ECHO HAWAII January 15 19, 2018 Kenya Kusunose, MD, PhD, FASE Tokushima University Hospital Japan Not only ischemia! Cardiomyopathy Prosthetic Valve Diastolic
13/06/2018. Rheumatic Mitral Stenosis: What does the ESC Guideline say? Mitral Stenosis: Echo Assessment. Mitral Stenosis ESC Guidance 2017
 Rheumatic Mitral Stenosis: What does the ESC Guideline say? Mitral Stenosis: Echo Assessment Dave Northridge Edinburgh Heart Centre Rheumatic mitral stenosis Prosthetic mitral dysfunction Calcific/degenerative
Rheumatic Mitral Stenosis: What does the ESC Guideline say? Mitral Stenosis: Echo Assessment Dave Northridge Edinburgh Heart Centre Rheumatic mitral stenosis Prosthetic mitral dysfunction Calcific/degenerative
Back to Basics: Common Errors In Quantitation In Everyday Practice
 Back to Basics: Common Errors In Quantitation In Everyday Practice Deborah Agler, ACS, RDCS, FASE October 9, 2017 ASE: Echo Florida Rebecca T. Hahn, MD Director of Interventional Echocardiography Professor
Back to Basics: Common Errors In Quantitation In Everyday Practice Deborah Agler, ACS, RDCS, FASE October 9, 2017 ASE: Echo Florida Rebecca T. Hahn, MD Director of Interventional Echocardiography Professor
Prosthesis-Patient Mismatch or Prosthetic Valve Stenosis?
 EuroValves 2015, Nice Prosthesis-Patient Mismatch or Prosthetic Valve Stenosis? Philippe Pibarot, DVM, PhD, FACC, FAHA, FASE FESC Canada Research Chair in Valvular Heart Diseases Université LAVAL Disclosure
EuroValves 2015, Nice Prosthesis-Patient Mismatch or Prosthetic Valve Stenosis? Philippe Pibarot, DVM, PhD, FACC, FAHA, FASE FESC Canada Research Chair in Valvular Heart Diseases Université LAVAL Disclosure
DOPPLER HEMODYNAMICS (1) QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES
 QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES") THORAXCENTRE DOPPLER HEMODYNAMICS (1) QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES J. Roelandt DOPPLER HEMODYNAMICS Intracardiac pressures and pressure gradients Volumetric measurement
THORAXCENTRE DOPPLER HEMODYNAMICS (1) QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES J. Roelandt DOPPLER HEMODYNAMICS Intracardiac pressures and pressure gradients Volumetric measurement
Διαδερμική θεραπεία των παραβαλβιδικών διαφυγών Σ.Ράμμος
 ΔΜΙΝΑΡΙΟ ΔΠΙΣΗΜΟΝΙΚΩΝ ΔΝΩΔΩΝ ΔΛΛΗΝΙΚΟΤ ΚΟΛΛΔΓΙΟΤ ΚΑΡ ΙΟΛΟΓΙΑ 2-4.10.2015 Δπιζηημονική Ένωζη Δπεμβαηικής Καρδιολογίας Βαλβιδοπάθειες, Γιαδερμικές παρεμβάζεις Διαδερμική θεραπεία των παραβαλβιδικών διαφυγών
ΔΜΙΝΑΡΙΟ ΔΠΙΣΗΜΟΝΙΚΩΝ ΔΝΩΔΩΝ ΔΛΛΗΝΙΚΟΤ ΚΟΛΛΔΓΙΟΤ ΚΑΡ ΙΟΛΟΓΙΑ 2-4.10.2015 Δπιζηημονική Ένωζη Δπεμβαηικής Καρδιολογίας Βαλβιδοπάθειες, Γιαδερμικές παρεμβάζεις Διαδερμική θεραπεία των παραβαλβιδικών διαφυγών
Image Assistance in TAVI Why CT? Won-Jang Kim, MD, PhD Clinical Assistant Professor of Medicine, Heart Institute, Asan Medical Center, Seoul, Korea
 Image Assistance in TAVI Why CT? Won-Jang Kim, MD, PhD Clinical Assistant Professor of Medicine, Heart Institute, Asan Medical Center, Seoul, Korea Major Uses of CT in TAVI Ileofemoral Patient Arterial
Image Assistance in TAVI Why CT? Won-Jang Kim, MD, PhD Clinical Assistant Professor of Medicine, Heart Institute, Asan Medical Center, Seoul, Korea Major Uses of CT in TAVI Ileofemoral Patient Arterial
ΔΙΑΔΕΡΜΙΚΗ ΑΝΣΙΚΑΣΑΣΑΗ ΑΟΡΣΙΚΗ ΒΑΛΒΙΔΑ αντιμετώπιση επιπλοκών ΠΕΣΡΟ. ΔΑΡΔΑ, MD, FESC IICE 2012
 ΔΙΑΔΕΡΜΙΚΗ ΑΝΣΙΚΑΣΑΣΑΗ ΑΟΡΣΙΚΗ ΒΑΛΒΙΔΑ αντιμετώπιση επιπλοκών ΠΕΣΡΟ. ΔΑΡΔΑ, MD, FESC IICE 2012 TAVR Technologies Current Generation Devices ~ 50,000 patients treated thru 2011 in > 500 interventional centers
ΔΙΑΔΕΡΜΙΚΗ ΑΝΣΙΚΑΣΑΣΑΗ ΑΟΡΣΙΚΗ ΒΑΛΒΙΔΑ αντιμετώπιση επιπλοκών ΠΕΣΡΟ. ΔΑΡΔΑ, MD, FESC IICE 2012 TAVR Technologies Current Generation Devices ~ 50,000 patients treated thru 2011 in > 500 interventional centers
Quantification of Aortic Regurgitation
 Quantification of Aortic Regurgitation ASE Review 2018 Boston Susan E Wiegers, MD, FASE, FACC Professor of Medicine And thanks to Dr. Roberto Lang Disclosure None related to this presentation 1 Objectives
Quantification of Aortic Regurgitation ASE Review 2018 Boston Susan E Wiegers, MD, FASE, FACC Professor of Medicine And thanks to Dr. Roberto Lang Disclosure None related to this presentation 1 Objectives
Section 1: Initial Evaluation for Valvular Heart Disease Table 1: Initial Evaluation of an Asymptomatic Patient
 Section 1: Initial Evaluation for Valvular Heart Disease Table 1: Initial Evaluation of an Asymptomatic Patient Indication 1. Unexplained murmur or abnormal heart sounds 2. Reasonable suspicion of valvular
Section 1: Initial Evaluation for Valvular Heart Disease Table 1: Initial Evaluation of an Asymptomatic Patient Indication 1. Unexplained murmur or abnormal heart sounds 2. Reasonable suspicion of valvular
Imaging Assessment of Aortic Stenosis/Aortic Regurgitation
 Imaging Assessment of Aortic Stenosis/Aortic Regurgitation Craig E Fleishman, MD FACC FASE The Heart Center at Arnold Palmer Hospital for Children, Orlando SCAI Fall Fellows Course 2014 Las Vegas Disclosure
Imaging Assessment of Aortic Stenosis/Aortic Regurgitation Craig E Fleishman, MD FACC FASE The Heart Center at Arnold Palmer Hospital for Children, Orlando SCAI Fall Fellows Course 2014 Las Vegas Disclosure
ICE: Echo Core Lab-CRF
 APPENDIX 1 ICE: Echo Core Lab-CRF Study #: - Pt Initials: 1. Date of study: / / D D M M M Y Y Y Y 2. Type of Study: TTE TEE 3. Quality of Study: Poor Moderate Excellent Ejection Fraction 4. Ejection Fraction
APPENDIX 1 ICE: Echo Core Lab-CRF Study #: - Pt Initials: 1. Date of study: / / D D M M M Y Y Y Y 2. Type of Study: TTE TEE 3. Quality of Study: Poor Moderate Excellent Ejection Fraction 4. Ejection Fraction
Aortic valve implantation using the femoral and apical access: a single center experience.
 Aortic valve implantation using the femoral and apical access: a single center experience. R. Hoffmann, K. Brehmer, R. Koos, R. Autschbach, N. Marx, G. Dohmen Rainer Hoffmann, University Aachen, Germany
Aortic valve implantation using the femoral and apical access: a single center experience. R. Hoffmann, K. Brehmer, R. Koos, R. Autschbach, N. Marx, G. Dohmen Rainer Hoffmann, University Aachen, Germany
PVL Assessment. Is paravalvular regurgitation after TAVR still an important consideration in 2018?
 Joint Meeting 1 Aortic and Mitral Club Chairpersons: S.Adamopoulos, M. Vavuranakis, L. Michalis, P. Nihoyannopoulos PVL Assessment. Is paravalvular regurgitation after TAVR still an important consideration
Joint Meeting 1 Aortic and Mitral Club Chairpersons: S.Adamopoulos, M. Vavuranakis, L. Michalis, P. Nihoyannopoulos PVL Assessment. Is paravalvular regurgitation after TAVR still an important consideration
The FORMA Early Feasibility Study: 30-Day Outcomes of Transcatheter Tricuspid Valve Therapy in Patients with Severe Secondary Tricuspid Regurgitation
 The FORMA Early Feasibility Study: 30-Day Outcomes of Transcatheter Tricuspid Valve Therapy in Patients with Severe Secondary Tricuspid Regurgitation Susheel Kodali, MD Director, Structural Heart & Valve
The FORMA Early Feasibility Study: 30-Day Outcomes of Transcatheter Tricuspid Valve Therapy in Patients with Severe Secondary Tricuspid Regurgitation Susheel Kodali, MD Director, Structural Heart & Valve
Transcatheter procedures of the future; expanding the treatment options for patients with severe aortic stenosis
 Transcatheter procedures of the future; expanding the treatment options for patients with severe aortic stenosis John Webb MD Director interventional cardiology, St Paul s Hospital McLeod Professor of
Transcatheter procedures of the future; expanding the treatment options for patients with severe aortic stenosis John Webb MD Director interventional cardiology, St Paul s Hospital McLeod Professor of
Minimalist Transcatheter Aortic Valve Replacement (MA-TAVR)
") Minimalist Transcatheter Aortic Valve Replacement (MA-TAVR) Jensen HA, Condado JF, Devireddy C, Binongo JN, Leshnower BG, Babaliaros V, Sarin EL, Lerakis S, Guyton RA, Stewart JP, Syed AQ, Mavromatis K,
Minimalist Transcatheter Aortic Valve Replacement (MA-TAVR) Jensen HA, Condado JF, Devireddy C, Binongo JN, Leshnower BG, Babaliaros V, Sarin EL, Lerakis S, Guyton RA, Stewart JP, Syed AQ, Mavromatis K,
An Update on the Edwards TAVR Results. Zvonimir Krajcer, MD Director, Peripheral Intervention Texas Heart Institute at St.
 An Update on the Edwards TAVR Results Zvonimir Krajcer, MD Director, Peripheral Intervention Texas Heart Institute at St. Luke s Hospital Disclosures On the speaker s bureau for Endologix, TriVascular,
An Update on the Edwards TAVR Results Zvonimir Krajcer, MD Director, Peripheral Intervention Texas Heart Institute at St. Luke s Hospital Disclosures On the speaker s bureau for Endologix, TriVascular,
Pre-procedural CT angiography for Transcatheter Aortic Valve Implantation: What a Radiologist Needs to Know?
 Pre-procedural CT angiography for Transcatheter Aortic Valve Implantation: What a Radiologist Needs to Know? E O Dwyer, C O Brien, I Murphy, C Shortt, O Buckley Department of Radiology, AMNCH, Dublin,
Pre-procedural CT angiography for Transcatheter Aortic Valve Implantation: What a Radiologist Needs to Know? E O Dwyer, C O Brien, I Murphy, C Shortt, O Buckley Department of Radiology, AMNCH, Dublin,
THE PERCUTANEOUS MANAGEMENT OF VALVULAR HEART DISEASE DR JOHN RAWLINS CONSULTANT INTERVENTIONAL CARDIOLOGIST UNIVERSITY HOSPITAL SOUTHAMPTON
 THE PERCUTANEOUS MANAGEMENT OF VALVULAR HEART DISEASE DR JOHN RAWLINS CONSULTANT INTERVENTIONAL CARDIOLOGIST UNIVERSITY HOSPITAL SOUTHAMPTON INTRODUCTION History of heart valve intervention Current indications
THE PERCUTANEOUS MANAGEMENT OF VALVULAR HEART DISEASE DR JOHN RAWLINS CONSULTANT INTERVENTIONAL CARDIOLOGIST UNIVERSITY HOSPITAL SOUTHAMPTON INTRODUCTION History of heart valve intervention Current indications
DISCLOSURE. Mitral ViV: why? Mitral Valve- in- Valve: Procedural Image Guidance with TEE, a Must Have or Nice to Have? UW Medicine NONE.
 Mitral Valve- in- Valve: Procedural Image Guidance with TEE, a Must Have or Nice to Have? G. Burkhard Mackensen, MD, PhD, FASE Professor & Chief, Division of Cardiothoracic Anesthesia, Department of Anesthesiology
Mitral Valve- in- Valve: Procedural Image Guidance with TEE, a Must Have or Nice to Have? G. Burkhard Mackensen, MD, PhD, FASE Professor & Chief, Division of Cardiothoracic Anesthesia, Department of Anesthesiology
Nouvelles indications/ Nouvelles valves
 Nouvelles indications/ Nouvelles valves Sadra Lotus Valve system Boston Scientific A. Tirouvanziam Institut Thorax Nantes SH-31314-AC Sept 2012 Slide 1 of 53 SH-31314-AC Sept 2012 Slide 2 of 53 Building
Nouvelles indications/ Nouvelles valves Sadra Lotus Valve system Boston Scientific A. Tirouvanziam Institut Thorax Nantes SH-31314-AC Sept 2012 Slide 1 of 53 SH-31314-AC Sept 2012 Slide 2 of 53 Building
2019 Qualified Clinical Data Registry (QCDR) Performance Measures
 Performance Measures") 2019 Qualified Clinical Data Registry (QCDR) Performance Measures Description: This document contains the 18 performance measures approved by CMS for inclusion in the 2019 Qualified Clinical Data Registry
2019 Qualified Clinical Data Registry (QCDR) Performance Measures Description: This document contains the 18 performance measures approved by CMS for inclusion in the 2019 Qualified Clinical Data Registry
Echo evaluation for TAVR. From the General Cardiologist to the Interventional Echocardiologist
 Echo evaluation for TAVR From the General Cardiologist to the Interventional Echocardiologist Disclosures Proctoring activities for Abbott Vascular I and the HYGEIA Hospital «Heart Team» have received
Echo evaluation for TAVR From the General Cardiologist to the Interventional Echocardiologist Disclosures Proctoring activities for Abbott Vascular I and the HYGEIA Hospital «Heart Team» have received
After PARTNER 2A/S3i and SURTAVI: What is the Role of Surgery in Intermediate-Risk AS Patients?
 After PARTNER 2A/S3i and SURTAVI: What is the Role of Surgery in Intermediate-Risk AS Patients? Vinod H. Thourani, MD Professor of Surgery and Medicine Emory University Disclosure Statement of Financial
After PARTNER 2A/S3i and SURTAVI: What is the Role of Surgery in Intermediate-Risk AS Patients? Vinod H. Thourani, MD Professor of Surgery and Medicine Emory University Disclosure Statement of Financial
AORTIC STENOSIS HENRY FORD HOSPITAL CENTER FOR STRUCTURAL HEART DISEASE
 AORTIC STENOSIS HENRY FORD HOSPITAL CENTER FOR STRUCTURAL HEART DISEASE WHAT IS AORTIC STENOSIS? THE AORTIC VALVE The aorta is the major vessel that carries oxygenated blood out of the left side of the
AORTIC STENOSIS HENRY FORD HOSPITAL CENTER FOR STRUCTURAL HEART DISEASE WHAT IS AORTIC STENOSIS? THE AORTIC VALVE The aorta is the major vessel that carries oxygenated blood out of the left side of the
The Role of Imaging in Transcatheter Aortic Valve Implantation
 The Role of Imaging in Transcatheter Aortic Valve Implantation Helmut Baumgartner Westfälische Wilhelms-Universität Münster Division of Adult Congenital and Valvular Heart Disease Department of Cardiovascular
The Role of Imaging in Transcatheter Aortic Valve Implantation Helmut Baumgartner Westfälische Wilhelms-Universität Münster Division of Adult Congenital and Valvular Heart Disease Department of Cardiovascular
Multicentre clinical study evaluating a novel resheatable self-expanding transcatheter aortic valve system
 Multicentre clinical study evaluating a novel resheatable self-expanding transcatheter aortic valve system Preliminary Results: Acute and 1-year Outcomes Ganesh Manoharan, MBBCh, MD, FRCP Consultant Cardiologist
Multicentre clinical study evaluating a novel resheatable self-expanding transcatheter aortic valve system Preliminary Results: Acute and 1-year Outcomes Ganesh Manoharan, MBBCh, MD, FRCP Consultant Cardiologist
Potential conflicts of interest
 Potential conflicts of interest Speaker's name: Petros Dardas MEDTRONIC proctor for TAVI Intermediate risk 83 FEMALE COAD SEVERE AS NYHA III Mean gradient 35 mmhg, AVA 0.45cm2, SVI 21ml/m2 Paradoxical
Potential conflicts of interest Speaker's name: Petros Dardas MEDTRONIC proctor for TAVI Intermediate risk 83 FEMALE COAD SEVERE AS NYHA III Mean gradient 35 mmhg, AVA 0.45cm2, SVI 21ml/m2 Paradoxical
Transcatheter Aortic Valve Replacement: Current and Future Devices: How do They Work, Eligibility, Review of Data
 Transcatheter Aortic Valve Replacement: Current and Future Devices: How do They Work, Eligibility, Review of Data Echo Florida 2013 Jonathan J. Passeri, M.D. Co-Director, Heart Valve Program Director,
Transcatheter Aortic Valve Replacement: Current and Future Devices: How do They Work, Eligibility, Review of Data Echo Florida 2013 Jonathan J. Passeri, M.D. Co-Director, Heart Valve Program Director,
Successful Transfemoral Edwards Sapien Aortic. Valve Implantation in a Patient with Previous. Mitral Valve Replacement
 Advanced Studies in Medical Sciences, Vol. 2, 2014, no. 1, 37-45 HIKARI Ltd, www.m-hikari.com http://dx.doi.org/10.12988/asms.2014.31213 Successful Transfemoral Edwards Sapien Aortic Valve Implantation
Advanced Studies in Medical Sciences, Vol. 2, 2014, no. 1, 37-45 HIKARI Ltd, www.m-hikari.com http://dx.doi.org/10.12988/asms.2014.31213 Successful Transfemoral Edwards Sapien Aortic Valve Implantation
TAVI Implantation: Rapid Pacing, Pre and Post Dilatation
 TAVI Summit 2012 Seoul, September 9, 2012 TAVI Implantation: Rapid Pacing, Pre and Post Dilatation Eberhard Grube, MD, FACC, FSCAI Medizinische i i Klinik ik und Polikinik II, University i Hospital Bonn,
TAVI Summit 2012 Seoul, September 9, 2012 TAVI Implantation: Rapid Pacing, Pre and Post Dilatation Eberhard Grube, MD, FACC, FSCAI Medizinische i i Klinik ik und Polikinik II, University i Hospital Bonn,
Disclosures Rebecca T. Hahn, MD, FASE
 The New ASE Guidelines for Native Valvular Regurgitation Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR (With caveats and comments from R. Hahn) William A. Zoghbi MD, FASE, MACC Professor
The New ASE Guidelines for Native Valvular Regurgitation Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR (With caveats and comments from R. Hahn) William A. Zoghbi MD, FASE, MACC Professor
History. 2D echo before TAVI. 88 female Hypertensive - hyperlipidemic History of LOC syncope Echo: severe AS AV gradient 90 mmhg Good LV LVH
 History 88 female Hypertensive - hyperlipidemic History of LOC syncope Echo: severe AS AV gradient 90 mmhg Good LV LVH 2D echo before TAVI LHC: Normal cors Pre severe calcification LVOT calcification
History 88 female Hypertensive - hyperlipidemic History of LOC syncope Echo: severe AS AV gradient 90 mmhg Good LV LVH 2D echo before TAVI LHC: Normal cors Pre severe calcification LVOT calcification
Andrzej Ochala, MD Medical University of Silesia, Katowice, Poland
 Andrzej Ochala, MD Medical University of Silesia, Katowice, Poland Bicuspid aortic valve o Most common congenital heart disease in adults (1% - 2%) o AS is the most common complication of BAV o Patophysiology
Andrzej Ochala, MD Medical University of Silesia, Katowice, Poland Bicuspid aortic valve o Most common congenital heart disease in adults (1% - 2%) o AS is the most common complication of BAV o Patophysiology
G. AORTIC STENOSIS (AS)
") G. AORTIC STENOSIS (AS) DEFINITION THE FACTS Aortic stenosis (AS) is a narrowing/thickening/obstruction of the aortic valve (AOV) that impedes systolic flow traveling from the left ventricle, through the
G. AORTIC STENOSIS (AS) DEFINITION THE FACTS Aortic stenosis (AS) is a narrowing/thickening/obstruction of the aortic valve (AOV) that impedes systolic flow traveling from the left ventricle, through the
Prosthetic valve dysfunction: stenosis or regurgitation
 Prosthetic valve dysfunction: stenosis or regurgitation Jean G. Dumesnil MD, FRCP(C), FACC, FASE(Hon) Quebec Heart and Lung Institute, Québec, Québec No disclosures Possible Causes of High Gradients in
Prosthetic valve dysfunction: stenosis or regurgitation Jean G. Dumesnil MD, FRCP(C), FACC, FASE(Hon) Quebec Heart and Lung Institute, Québec, Québec No disclosures Possible Causes of High Gradients in
What are the best diagnostic tools to quantify aortic regurgitation?
 What are the best diagnostic tools to quantify aortic regurgitation? Agnès Pasquet, MD, PhD Pôle de Recherche Cardiovasculaire Institut de Recherche Expérimentale et Clinique Université catholique de Louvain
What are the best diagnostic tools to quantify aortic regurgitation? Agnès Pasquet, MD, PhD Pôle de Recherche Cardiovasculaire Institut de Recherche Expérimentale et Clinique Université catholique de Louvain
MITRAL VALVE DISEASE- ASSESSMENT AND MANAGEMENT. Irene Frantzis P year, SGUL Sheba Medical Center
 MITRAL VALVE DISEASE- ASSESSMENT AND MANAGEMENT Irene Frantzis P year, SGUL Sheba Medical Center MITRAL VALVE DISEASE Mitral Valve Regurgitation Mitral Valve Stenosis Mitral Valve Prolapse MITRAL REGURGITATION
MITRAL VALVE DISEASE- ASSESSMENT AND MANAGEMENT Irene Frantzis P year, SGUL Sheba Medical Center MITRAL VALVE DISEASE Mitral Valve Regurgitation Mitral Valve Stenosis Mitral Valve Prolapse MITRAL REGURGITATION
25 different brand names >44 different models Sizes mm
 Types of Prosthetic Valves BIOLOGIC STENTED Porcine xenograft Pericardial xenograft STENTLESS Porcine xenograft Pericardial xenograft Homograft (allograft) Autograft PERCUTANEOUS MECHANICAL Bileaflet Single
Types of Prosthetic Valves BIOLOGIC STENTED Porcine xenograft Pericardial xenograft STENTLESS Porcine xenograft Pericardial xenograft Homograft (allograft) Autograft PERCUTANEOUS MECHANICAL Bileaflet Single
Assessment and Preparation of Patients with TAVI. Rob Tanzola Associate Professor, Queen s University
 Assessment and Preparation of Patients with TAVI Rob Tanzola Associate Professor, Queen s University My patient has aortic stenosis and needs non-cardiac surgery Should (s)he get a TAVI? Rob Tanzola Associate
Assessment and Preparation of Patients with TAVI Rob Tanzola Associate Professor, Queen s University My patient has aortic stenosis and needs non-cardiac surgery Should (s)he get a TAVI? Rob Tanzola Associate
The Colibri heart valve: theory and practice in the achievement of a low-profile, pre-mounted, pre-packaged TAVI valve
 INNOVATIONS / NOVEL TECHNOLOGIES The Colibri heart valve: theory and practice in the achievement of a low-profile, pre-mounted, pre-packaged TAVI valve R. David Fish 1 *, MD; David Paniagua 1, MD; Pedro
INNOVATIONS / NOVEL TECHNOLOGIES The Colibri heart valve: theory and practice in the achievement of a low-profile, pre-mounted, pre-packaged TAVI valve R. David Fish 1 *, MD; David Paniagua 1, MD; Pedro
Ian T. Meredith AM. MBBS, PhD, FRACP, FCSANZ, FACC, FAPSIC. Monash HEART, Monash Health & Monash University Melbourne, Australia
 Two-Year Outcomes With the Fully Repositionable and Retrievable Lotus Transcatheter Aortic Replacement Valve in 120 High-Risk Surgical Patients With Severe Aortic Stenosis: Results From the REPRISE II
Two-Year Outcomes With the Fully Repositionable and Retrievable Lotus Transcatheter Aortic Replacement Valve in 120 High-Risk Surgical Patients With Severe Aortic Stenosis: Results From the REPRISE II
Comprehensive Hemodynamics By Doppler Echocardiography. The Echocardiographic Swan-Ganz Catheter.
 Comprehensive Hemodynamics By Doppler Echocardiography. The Echocardiographic Swan-Ganz Catheter. Itzhak Kronzon, MD, FASE, FACC, FESC, FAHA, FACP, FCCP North Shore HS, LIJ/Lenox Hill Hospital, New York
Comprehensive Hemodynamics By Doppler Echocardiography. The Echocardiographic Swan-Ganz Catheter. Itzhak Kronzon, MD, FASE, FACC, FESC, FAHA, FACP, FCCP North Shore HS, LIJ/Lenox Hill Hospital, New York
Challenging Case. 89 year old man 5/11/2016. Prior 31 mm CoreValve NYHA III Moderately-severe PVL
 5/11/2016 Vumedi May 2016 89 year old man Challenging Case Prior 31 mm CoreValve NYHA III Moderately-severe PVL Paul Sorajja, MD Director, Center for Valve and Structural Heart Disease Minneapolis Heart
5/11/2016 Vumedi May 2016 89 year old man Challenging Case Prior 31 mm CoreValve NYHA III Moderately-severe PVL Paul Sorajja, MD Director, Center for Valve and Structural Heart Disease Minneapolis Heart
Echo Doppler Assessment of Right and Left Ventricular Hemodynamics.
 Echo Doppler Assessment of Right and Left Ventricular Hemodynamics. Itzhak Kronzon, MD, FASE, FACC, FESC, FAHA, FACP, FCCP Northwell, Lenox Hill Hospital, New York Professor of Cardiology Hofstra University
Echo Doppler Assessment of Right and Left Ventricular Hemodynamics. Itzhak Kronzon, MD, FASE, FACC, FESC, FAHA, FACP, FCCP Northwell, Lenox Hill Hospital, New York Professor of Cardiology Hofstra University
Percutaneous Valve in Native With and Without Mitral Valve Calcification: When To Go Hybrid
 Percutaneous Valve in Native With and Without Mitral Valve Calcification: When To Go Hybrid Deborah Tabachnick, MD Cardiac Surgeon The Heart Hospital Baylor Plano Baylor Scott & White Health Disclosures
Percutaneous Valve in Native With and Without Mitral Valve Calcification: When To Go Hybrid Deborah Tabachnick, MD Cardiac Surgeon The Heart Hospital Baylor Plano Baylor Scott & White Health Disclosures
Critical role of multi-modality planning in Transcatheter Mitral Valve Replacement
 Critical role of multi-modality planning in Transcatheter Mitral Valve Replacement Dee Dee Wang, MD, FACC, FASE, FSCCT Director Structural Heart Imaging Medical Director 3D Printing Henry Ford Innovations
Critical role of multi-modality planning in Transcatheter Mitral Valve Replacement Dee Dee Wang, MD, FACC, FASE, FSCCT Director Structural Heart Imaging Medical Director 3D Printing Henry Ford Innovations
Echocardiography as a diagnostic and management tool in medical emergencies
 Echocardiography as a diagnostic and management tool in medical emergencies Frank van der Heusen MD Department of Anesthesia and perioperative Care UCSF Medical Center Objective of this presentation Indications
Echocardiography as a diagnostic and management tool in medical emergencies Frank van der Heusen MD Department of Anesthesia and perioperative Care UCSF Medical Center Objective of this presentation Indications
Questions of the webinar "Imaging in TAVI procedures" Answered by Andreas Hagendorff, Victoria Delgado and Bernard Cosyns
 Questions of the webinar "Imaging in TAVI procedures" Answered by Andreas Hagendorff, Victoria Delgado and Bernard Cosyns 1. The incidence in AR I think that this question focuses on the incidence in AR
Questions of the webinar "Imaging in TAVI procedures" Answered by Andreas Hagendorff, Victoria Delgado and Bernard Cosyns 1. The incidence in AR I think that this question focuses on the incidence in AR
Preprocedural evaluation for TAVR
 KEBE 30/05/15 Preprocedural evaluation for TAVR Ioannis Iakovou, MD, PhD Interventional Cardiology Onassis Cardiac Surgery Center Athens, Greece Clinical Pathway: Developing Peri- Procedural Protocols
KEBE 30/05/15 Preprocedural evaluation for TAVR Ioannis Iakovou, MD, PhD Interventional Cardiology Onassis Cardiac Surgery Center Athens, Greece Clinical Pathway: Developing Peri- Procedural Protocols
Is TAVR the treatment of choice for high risk diabetic patients with aortic stenosis? Insights from the FRANCE2 Registry
 Is TAVR the treatment of choice for high risk diabetic patients with aortic stenosis? Insights from the FRANCE2 Registry E Van Belle, E Teiger, F Juthier, A Vincentelli, B Iung, H Eltchaninoff, J Fajadet,
Is TAVR the treatment of choice for high risk diabetic patients with aortic stenosis? Insights from the FRANCE2 Registry E Van Belle, E Teiger, F Juthier, A Vincentelli, B Iung, H Eltchaninoff, J Fajadet,
Dobutamine Stress testing In Low Flow, Low EF, Low Gradient Aortic Stenosis Case Studies
 Dobutamine Stress testing In Low Flow, Low EF, Low Gradient Aortic Stenosis Case Studies Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR William A. Zoghbi MD, FASE, MACC Professor and
Dobutamine Stress testing In Low Flow, Low EF, Low Gradient Aortic Stenosis Case Studies Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR William A. Zoghbi MD, FASE, MACC Professor and