Patient Management Code Blue in the CT Suite
|
|
|
- Shanon Rogers
- 6 years ago
- Views:
Transcription
1 Patient Management Code Blue in the CT Suite David Stultz, MD November 28, 2001
2 Case Presentation A 53-year-old woman experienced acute respiratory distress during an IV contrast enhanced CT scan of the chest, abdomen and pelvis. A code blue was signaled. Upon arrival, the patient complained of dyspnea but no chest pain.
3 Physical Examination Her examination showed: Vitals: Resps 30, Pulse 110, BP 110/60 Pulse Ox 80% on 3 L/min of O 2 Inspection of her neck showed a midline trachea Chest examination revealed cyanosis, absent left-sided breath sounds and clear right lung by auscultation Heart auscultation revealed no murmur The abdomen was distended from ascites 2+ leg edema was present
4 Differential Diagnosis Pneumothorax Anaphylaxis Pulmonary Embolism Thrombosis Air Embolism MI Cardiac Tamponade ARDS

5 Chest Xray
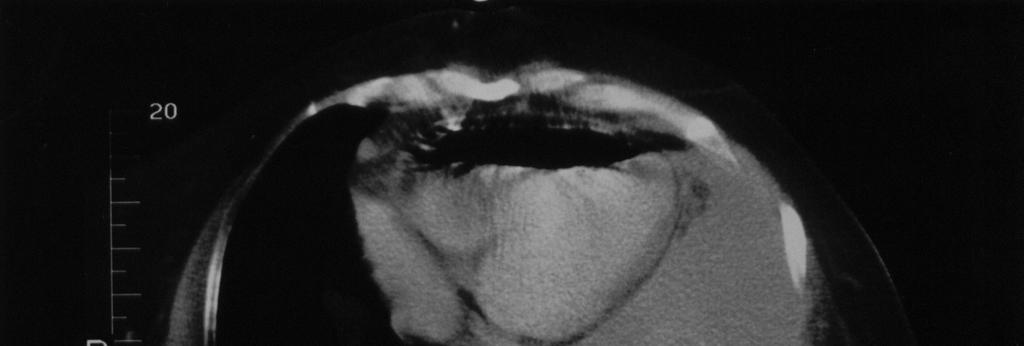
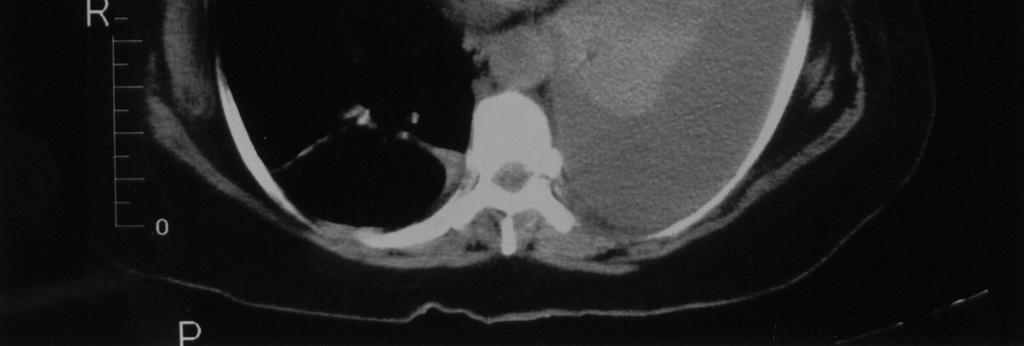
6 , David Stultz, MD Chest CT


7 , David Stultz, MD Chest CT Reviewed
8 Air Embolism Occurs when gas enters systemic venous system Gas transported to lungs through pulmonary arteries Interferes with blood transport and gas exchange Leads to cardiac arrythmia, pulmonary hypertension, right ventricular strain
9 Significance Air embolism occurs in up to 12% of patients undergoing IV contrast injection for CT scan When infused rapidly, 50 ml of intravenous air may lead to acute right heart failure and possible cardiac arrest. Larger amounts of intravascular air can be well tolerated if received at a slower rate of infusion
10 Etiology Many potential sources of air embolism Air entry favored by a pressure gradient from the superior venous sites to the right atrium Large-bore IV catheter access Neurosurgical and other surgical procedures where the patient is sitting Trauma Injury to the arms or legs may lead to venous air entry especially when the extremity is positioned superior to the right atrium or in the setting of shock
11 Diagnosis Consider in a hospitalized patient who develops rapid onset respiratory distress or cardiovascular compromise Characteristic mill-wheel murmur due to air-blood mixing within the cardiac chambers is rarely auscultated Intravascular air is best demonstrated by CT of the chest or bedside echocardiography
12 Treatment Immediate prevention of further air entry Place patient in left lateral decubitus position to minimize right ventricular air entering the pulmonary outflow tract Provide patient with 100% O 2 Placement of a central venous catheter for evacuation of the air embolism can be attempted Hyperbaric oxygen is generally not used as first line therapy, but should be considered when there are neurological symptoms or signs suggesting a paradoxical embolism.
13 Create Diffusion Gradient Providing patient with 100% FiO 2 elevates the nitrogen gradient and encourages diffusion of nitrogen from the intravascular air collection into the blood, accelerating the resolution of the air embolism
14 Hyperbaric therapy Indicated for all arterial gas emboli 100% Oxygen at pressure above atmospheric Achieves PAO 2 up to 2000 mm Hg Decreases size of gas embolism due to increased pressure Creates high diffusion gradient to promote nitrogen absorption Increases tissue oxygenation Delayed treatment may still be beneficial
15 Alternative Therapies (Generally not recommended) Maintain normovolemia via IV infusion to maintain CVP at 12 mm Hg Heparin therapy may be beneficial in arterial embolization, but not generally recommended Corticosteroids are not recommended Lidocaine bolus of 1.5 mg/kg has been beneficial in animals
16 Paradoxical Embolism Occurs when air in the venous system migrates to the arterial system Often via patent foramen ovale (30% of general population) May be due to migration of massive venous embolism Signs include end arterial organ damage Place in flat position, otherwise treated the same as venous embolism Give higher consideration to hyperbaric therapy
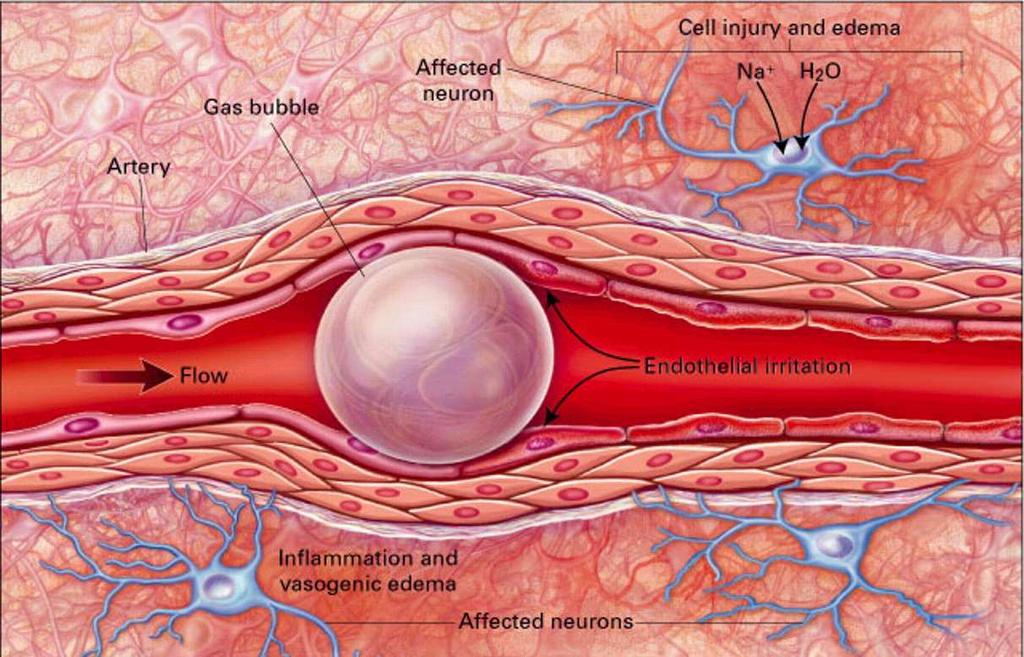
17 Arterial Embolization Concerning targets include coronary arteries and cerebral vasculature Visceral and skeletal muscles tolerate arterial emboli reasonably well Two mechanisms of damage reduced arterial perfusion and local inflammatory response to bubble
18 Arterial Embolization
19 Patient Code Blue Course The CT scan of the chest showed a large left pleural effusion and approximately 40 ml of air in the right ventricle which was inadvertently introduced during IV contrast injection. The patient was emergently intubated and mechanical ventilation was initiated with 100% O 2.
20 ICU Course She was maintained in a left lateral decubitus position. A cordis catheter was inserted into the right internal jugular vein followed by introduction of a 20 cm triple lumen catheter. Approximately 20 ml of air and frothy blood were aspirated through the triple lumen catheter.
21 ICU Course The patient remained intubated overnight. The following morning a quick-look echocardiogram revealed no evidence of air embolism. A followup chest CT also showed no residual air. She was successfully extubated 12 hours after intubation without further complication

22 Follow Up Chest CT


23 Comparison CT Before After
24 Conclusions Suspect air embolism in a patient with acute dyspnea and the right clinical setting Position patient and administer 100% Oxygen Watch for evidence of paradoxical embolism or neurological compromise and institute hyperbaric therapy if present
25 Bibliography Groell R, Schaffler GJ, Rienmueller R, et al. Vascular air embolism: location, frequency, and cause on electronbeam CT studies of the chest. Radiology 1997; 202: Muth CM, Shank ES. Gas embolism. N Engl J Med 2000; 342: Woodring JH, Fried AM. Nonfatal venous air embolism after contrast-enhanced CT. Radiology 1988; 167:
Therapeutic hypothermia
 INDUCED HYPOTHERMIA Dr. Attilla Kiss M.D. Acting Medical Director Emergency Services EMS Medical Director St. John Medical Center OBJECTIVES Define and explain Induced Hypothermia Discuss both pre-hospital
INDUCED HYPOTHERMIA Dr. Attilla Kiss M.D. Acting Medical Director Emergency Services EMS Medical Director St. John Medical Center OBJECTIVES Define and explain Induced Hypothermia Discuss both pre-hospital
Episodic Desaturation
 Episodic Desaturation James D. Flaherty, MD Assistant Professor of Medicine University, Feinberg School of Medicine Medical Director, Coronary Care Unit Memorial Hospital, Chicago April 27, 2012 Disclosures
Episodic Desaturation James D. Flaherty, MD Assistant Professor of Medicine University, Feinberg School of Medicine Medical Director, Coronary Care Unit Memorial Hospital, Chicago April 27, 2012 Disclosures
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv
 Rv") ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
Lecture Notes. Chapter 9: Smoke Inhalation Injury and Burns
 Lecture Notes Chapter 9: Smoke Inhalation Injury and Burns Objectives List the factors that influence mortality rate Describe the nature of smoke inhalation and the fire environment Recognize the pulmonary
Lecture Notes Chapter 9: Smoke Inhalation Injury and Burns Objectives List the factors that influence mortality rate Describe the nature of smoke inhalation and the fire environment Recognize the pulmonary
Canadian Trauma Trials Collaborative. Occult Pneumothorax in Critical Care (OPTICC): Standardized Data Collection Sheet
: Standardized Data Collection Sheet") Canadian Trauma Trials Collaborative STUDY CENTRE: Institution: City / Province: / Occult Pneumothorax in Critical Care (OPTICC): Standardized Sheet PATIENT DEMOGRAPHICS: First Name: Health record number
Canadian Trauma Trials Collaborative STUDY CENTRE: Institution: City / Province: / Occult Pneumothorax in Critical Care (OPTICC): Standardized Sheet PATIENT DEMOGRAPHICS: First Name: Health record number
Dr. Rami M. Adil Al-Hayali Assistant Professor in Medicine
 Dr. Rami M. Adil Al-Hayali Assistant Professor in Medicine Venous thromboembolism: pulmonary embolism (PE) deep vein thrombosis (DVT) 1% of all patients admitted to hospital 5% of in-hospital mortality
Dr. Rami M. Adil Al-Hayali Assistant Professor in Medicine Venous thromboembolism: pulmonary embolism (PE) deep vein thrombosis (DVT) 1% of all patients admitted to hospital 5% of in-hospital mortality
Echocardiography as a diagnostic and management tool in medical emergencies
 Echocardiography as a diagnostic and management tool in medical emergencies Frank van der Heusen MD Department of Anesthesia and perioperative Care UCSF Medical Center Objective of this presentation Indications
Echocardiography as a diagnostic and management tool in medical emergencies Frank van der Heusen MD Department of Anesthesia and perioperative Care UCSF Medical Center Objective of this presentation Indications
SWISS SOCIETY OF NEONATOLOGY. Potentially fatal complications of peripherally inserted central venous catheters (PICCs)
") SWISS SOCIETY OF NEONATOLOGY Potentially fatal complications of peripherally inserted central venous catheters (PICCs) October 2001 2 Berger TM, Neonatal and Pediatric Intensive Care Unit, Children s Hospital
SWISS SOCIETY OF NEONATOLOGY Potentially fatal complications of peripherally inserted central venous catheters (PICCs) October 2001 2 Berger TM, Neonatal and Pediatric Intensive Care Unit, Children s Hospital
Pulmonary Embolism. Thoracic radiologist Helena Lauri
 Pulmonary Embolism Thoracic radiologist Helena Lauri 8.5.2017 Statistics 1-2 out of 1000 adults annually are diagnosed with deep vein thrombosis (DVT) and/or pulmonary embolism (PE) About half of patients
Pulmonary Embolism Thoracic radiologist Helena Lauri 8.5.2017 Statistics 1-2 out of 1000 adults annually are diagnosed with deep vein thrombosis (DVT) and/or pulmonary embolism (PE) About half of patients
HEMODYNAMIC DISORDERS
 HEMODYNAMIC DISORDERS Normal fluid homeostasis requires vessel wall integrity as well as maintenance of intravascular pressure and osmolarity within certain physiologic ranges. Increases in vascular volume
HEMODYNAMIC DISORDERS Normal fluid homeostasis requires vessel wall integrity as well as maintenance of intravascular pressure and osmolarity within certain physiologic ranges. Increases in vascular volume
Head injuries. Severity of head injuries
 Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
Cor pulmonale. Dr hamid reza javadi
 1 Cor pulmonale Dr hamid reza javadi 2 Definition Cor pulmonale ;pulmonary heart disease; is defined as dilation and hypertrophy of the right ventricle (RV) in response to diseases of the pulmonary vasculature
1 Cor pulmonale Dr hamid reza javadi 2 Definition Cor pulmonale ;pulmonary heart disease; is defined as dilation and hypertrophy of the right ventricle (RV) in response to diseases of the pulmonary vasculature
Respiratory Emergencies. Chapter 11
 Respiratory Emergencies Chapter 11 Respiratory System Anatomy and Function of the Lung Characteristics of Adequate Breathing Normal rate and depth Regular breathing pattern Good breath sounds on both sides
Respiratory Emergencies Chapter 11 Respiratory System Anatomy and Function of the Lung Characteristics of Adequate Breathing Normal rate and depth Regular breathing pattern Good breath sounds on both sides
Thrombolysis in PE. Outline. Disclosure. Overview on Pulmonary Embolism. Hot Topics in Emergency Medicine 2012 Midyear Clinical Meeting
 Disclosure Thrombolysis in PE Daniel P. Hays, PharmD, BCPS, FASHP reports no relevant financial relationships. Daniel P. Hays, PharmD, BCPS, FASHP Outline 55 YOF presents to ED with SOB PMH of DVT + noncompliance
Disclosure Thrombolysis in PE Daniel P. Hays, PharmD, BCPS, FASHP reports no relevant financial relationships. Daniel P. Hays, PharmD, BCPS, FASHP Outline 55 YOF presents to ED with SOB PMH of DVT + noncompliance
Hemodynamic Monitoring
 Perform Procedure And Interpret Results Hemodynamic Monitoring Tracheal Tube Cuff Pressure Dean R. Hess PhD RRT FAARC Hemodynamic Monitoring Cardiac Rate and Rhythm Arterial Blood Pressure Central Venous
Perform Procedure And Interpret Results Hemodynamic Monitoring Tracheal Tube Cuff Pressure Dean R. Hess PhD RRT FAARC Hemodynamic Monitoring Cardiac Rate and Rhythm Arterial Blood Pressure Central Venous
CHEST INJURY PULMONARY CONTUSION
 CHEST INJURY PULMONARY CONTUSION Introduction Pulmonary contusion refers to blunt traumatic lung parenchymal injury which results in oedema and haemorrhaging into alveolar spaces. It may also result in
CHEST INJURY PULMONARY CONTUSION Introduction Pulmonary contusion refers to blunt traumatic lung parenchymal injury which results in oedema and haemorrhaging into alveolar spaces. It may also result in
Presenter: Steven Brust, HCS-D, HCS-H Product Manager, Home Health Coding Center
 Presenter: Steven Brust, HCS-D, HCS-H Product Manager, Home Health Coding Center Pinpoint & properly assign the appropriate heart failure codes Left- vs. Right-sided Left ventricular failure (LVF) may
Presenter: Steven Brust, HCS-D, HCS-H Product Manager, Home Health Coding Center Pinpoint & properly assign the appropriate heart failure codes Left- vs. Right-sided Left ventricular failure (LVF) may
Chapter 29 - Chest_and_Abdominal_Trauma
 Introduction to Emergency Medical Care 1 OBJECTIVES 29.1 Define key terms introduced in this chapter. Slides 11, 15, 18, 27 29.2 Describe mechanisms of injury commonly associated with chest injuries. Slides
Introduction to Emergency Medical Care 1 OBJECTIVES 29.1 Define key terms introduced in this chapter. Slides 11, 15, 18, 27 29.2 Describe mechanisms of injury commonly associated with chest injuries. Slides
A Practical Approach to Ultrasound Assessment of Respiratory Distress
 A Practical Approach to Ultrasound Assessment of Respiratory Distress Yanick Beaulieu, MD, FRCPC Director, Bedside Ultrasound Curriculum Division of Cardiology and Critical Care Hôpital du Sacré-Coeur
A Practical Approach to Ultrasound Assessment of Respiratory Distress Yanick Beaulieu, MD, FRCPC Director, Bedside Ultrasound Curriculum Division of Cardiology and Critical Care Hôpital du Sacré-Coeur
Research Article Can we predict the Position of Central Venous Catheter Tip Following Cannulation of Internal Jugular Vein?
 Cronicon OPEN ACCESS ANAESTHESIA Research Article Can we predict the Position of Central Venous Catheter Tip Following Cannulation of Internal Jugular Vein? Pradeep Marur Venkategowda 1, Surath Manimala
Cronicon OPEN ACCESS ANAESTHESIA Research Article Can we predict the Position of Central Venous Catheter Tip Following Cannulation of Internal Jugular Vein? Pradeep Marur Venkategowda 1, Surath Manimala
AORTIC DISSECTIONS Current Management. TOMAS D. MARTIN, MD, LAT Professor, TCV Surgery Director UF Health Aortic Disease Center University of Florida
 AORTIC DISSECTIONS Current Management TOMAS D. MARTIN, MD, LAT Professor, TCV Surgery Director UF Health Aortic Disease Center University of Florida DISCLOSURES Terumo Medtronic Cook Edwards Cryolife AORTIC
AORTIC DISSECTIONS Current Management TOMAS D. MARTIN, MD, LAT Professor, TCV Surgery Director UF Health Aortic Disease Center University of Florida DISCLOSURES Terumo Medtronic Cook Edwards Cryolife AORTIC
Prehospital Resuscitation for the 21 st Century Simulation Case. VF/Asystole
 Prehospital Resuscitation for the 21 st Century Simulation Case VF/Asystole Case History 1 (hypovolemic cardiac arrest secondary to massive upper GI bleed) 56 year-old male patient who fainted in the presence
Prehospital Resuscitation for the 21 st Century Simulation Case VF/Asystole Case History 1 (hypovolemic cardiac arrest secondary to massive upper GI bleed) 56 year-old male patient who fainted in the presence
Cerebral Air Embolism Following Pigtail Catheter Insertion for Pleural Fluid Drainage
 http://dx.doi.org/10.4046/trd.2013.74.6.286 ISSN: 1738-3536(Print)/2005-6184(Online) Tuberc Respir Dis 2013;74:286-290 CopyrightC2013. The Korean Academy of Tuberculosis and Respiratory Diseases. All rights
http://dx.doi.org/10.4046/trd.2013.74.6.286 ISSN: 1738-3536(Print)/2005-6184(Online) Tuberc Respir Dis 2013;74:286-290 CopyrightC2013. The Korean Academy of Tuberculosis and Respiratory Diseases. All rights
1 Chapter 13 Respiratory Emergencies 2 Respiratory Distress Patients often complain about. Shortness of breath Symptom of many different Cause can be
 1 Chapter 13 Respiratory Emergencies 2 Respiratory Distress Patients often complain about. Shortness of breath Symptom of many different Cause can be difficult to determine. Even for physician in hospital
1 Chapter 13 Respiratory Emergencies 2 Respiratory Distress Patients often complain about. Shortness of breath Symptom of many different Cause can be difficult to determine. Even for physician in hospital
Case 1. A 35-year-old male presented with fever, cough, and purulent sputum for one week. This was his CXR (Fig. 1.1). What is the diagnosis?
. What is the diagnosis?") 1 Interpreting Chest X-Rays CASE 1 Fig. 1.1 Case 1. A 35-year-old male presented with fever, cough, and purulent sputum for one week. This was his CXR (Fig. 1.1). What is the diagnosis? CASE 1 Interpreting
1 Interpreting Chest X-Rays CASE 1 Fig. 1.1 Case 1. A 35-year-old male presented with fever, cough, and purulent sputum for one week. This was his CXR (Fig. 1.1). What is the diagnosis? CASE 1 Interpreting
Tests Your Pulmonologist Might Order. Center For Cardiac Fitness Pulmonary Rehab Program The Miriam Hospital
 Tests Your Pulmonologist Might Order Center For Cardiac Fitness Pulmonary Rehab Program The Miriam Hospital BASIC ANATOMY OF THE LUNGS Lobes of Lung 3 lobes on the Right lung 2 lobes on the Left Blood
Tests Your Pulmonologist Might Order Center For Cardiac Fitness Pulmonary Rehab Program The Miriam Hospital BASIC ANATOMY OF THE LUNGS Lobes of Lung 3 lobes on the Right lung 2 lobes on the Left Blood
Describe regional differences in pulmonary blood flow in an upright person. Describe the major functions of the bronchial circulation
 OBJECTIVES Describe regional differences in pulmonary blood flow in an upright person Define zones I, II, and III in the lung, with respect to pulmonary vascular pressure and alveolar pressure Describe
OBJECTIVES Describe regional differences in pulmonary blood flow in an upright person Define zones I, II, and III in the lung, with respect to pulmonary vascular pressure and alveolar pressure Describe
European Resuscitation Council
 European Resuscitation Council Incidence of Trauma in Childhood Leading cause of death and disability in children older than one year all over the world Structured approach Primary survey and resuscitation
European Resuscitation Council Incidence of Trauma in Childhood Leading cause of death and disability in children older than one year all over the world Structured approach Primary survey and resuscitation
Topics to be Covered. Cardiac Measurements. Distribution of Blood Volume. Distribution of Pulmonary Ventilation & Blood Flow
 Topics to be Covered MODULE F HEMODYNAMIC MONITORING Cardiac Output Determinants of Stroke Volume Hemodynamic Measurements Pulmonary Artery Catheterization Control of Blood Pressure Heart Failure Cardiac
Topics to be Covered MODULE F HEMODYNAMIC MONITORING Cardiac Output Determinants of Stroke Volume Hemodynamic Measurements Pulmonary Artery Catheterization Control of Blood Pressure Heart Failure Cardiac
ITLS Pediatric Provider Course Advanced Pre-Test
 ITLS Pediatric Provider Course Advanced Pre-Test 1. You arrive at the scene of a motor vehicle crash and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
ITLS Pediatric Provider Course Advanced Pre-Test 1. You arrive at the scene of a motor vehicle crash and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
TRAINING NEONATOLOGY SILVANA PARIS
 TRAINING ON NEONATOLOGY SILVANA PARIS RESUSCITATION IN DELIVERY ROOM INTRODUCTION THE GLOBAL RESUSCITATION BURDEN IN NEWBORN 136 MILL NEWBORN BABIES EACH YEAR (WHO WORLD REPORT) 5-8 MILL NEWBORN INFANTS
TRAINING ON NEONATOLOGY SILVANA PARIS RESUSCITATION IN DELIVERY ROOM INTRODUCTION THE GLOBAL RESUSCITATION BURDEN IN NEWBORN 136 MILL NEWBORN BABIES EACH YEAR (WHO WORLD REPORT) 5-8 MILL NEWBORN INFANTS
EMT. Chapter 14 Review
 EMT Chapter 14 Review Review 1. All of the following are common signs and symptoms of cardiac ischemia, EXCEPT: A. headache. B. chest pressure. C. shortness of breath. D. anxiety or restlessness. Review
EMT Chapter 14 Review Review 1. All of the following are common signs and symptoms of cardiac ischemia, EXCEPT: A. headache. B. chest pressure. C. shortness of breath. D. anxiety or restlessness. Review
CARDIAC PROBLEMS IN PREGNANCY
 CARDIAC PROBLEMS IN PREGNANCY LAS VEGAS, NEVADA, USA 27 February 1 March 2016 SUCCESSFUL TREATMENT WITH RECOMBINANT TISSUE PLASMINOGEN ACTIVATOR OF MASSIVE PULMONARY EMBOLISM IN THE 16 TH WEEK OF PREGNANCY
CARDIAC PROBLEMS IN PREGNANCY LAS VEGAS, NEVADA, USA 27 February 1 March 2016 SUCCESSFUL TREATMENT WITH RECOMBINANT TISSUE PLASMINOGEN ACTIVATOR OF MASSIVE PULMONARY EMBOLISM IN THE 16 TH WEEK OF PREGNANCY
Extracorporeal Life Support Organization (ELSO) Guidelines for Pediatric Respiratory Failure
 Guidelines for Pediatric Respiratory Failure") Extracorporeal Life Support Organization (ELSO) Guidelines for Pediatric Respiratory Failure Introduction This pediatric respiratory failure guideline is a supplement to ELSO s General Guidelines for all
Extracorporeal Life Support Organization (ELSO) Guidelines for Pediatric Respiratory Failure Introduction This pediatric respiratory failure guideline is a supplement to ELSO s General Guidelines for all
PEMSS PROTOCOLS INVASIVE PROCEDURES
 PEMSS PROTOCOLS INVASIVE PROCEDURES Panhandle Emergency Medical Services System SURGICAL AND NEEDLE CRICOTHYROTOMY Inability to intubate is the primary indication for creating an artificial airway. Care
PEMSS PROTOCOLS INVASIVE PROCEDURES Panhandle Emergency Medical Services System SURGICAL AND NEEDLE CRICOTHYROTOMY Inability to intubate is the primary indication for creating an artificial airway. Care
A 50-Year-Old Woman With Dyspnea, Lower Extremity Edema, and Volume Loss of the Right Hemithorax. Eugene Shostak, MD; and Akmal Sarwar, MD, FCCP
 CHEST A 50-Year-Old Woman With Dyspnea, Lower Extremity Edema, and Volume Loss of the Right Hemithorax Eugene Shostak, MD; and Akmal Sarwar, MD, FCCP Postgraduate Education Corner PULMONARY AND CRITICAL
CHEST A 50-Year-Old Woman With Dyspnea, Lower Extremity Edema, and Volume Loss of the Right Hemithorax Eugene Shostak, MD; and Akmal Sarwar, MD, FCCP Postgraduate Education Corner PULMONARY AND CRITICAL
1. What additional information needs to be collected to properly treat this client?
 CASE 1 A 45-year-old male presents to the emergency department with a complaint of chest pain for the past two hours. 1. What additional information needs to be collected to properly treat this client?
CASE 1 A 45-year-old male presents to the emergency department with a complaint of chest pain for the past two hours. 1. What additional information needs to be collected to properly treat this client?
INSTITUTE FOR MEDICAL SIMULATION & EDUCATION ACLS PRACTICAL SCENARIOS
 Practical Teaching for Respiratory Arrest with a Pulse (Case 1) You are a medical officer doing a pre-operative round when 60-year old patient started coughing violently and becomes unconscious. Fortunately
Practical Teaching for Respiratory Arrest with a Pulse (Case 1) You are a medical officer doing a pre-operative round when 60-year old patient started coughing violently and becomes unconscious. Fortunately
PRE-HOSPITAL EMERGENCY CARE COURSE.
 PRE-HOSPITAL EMERGENCY CARE COURSE www.basics.org.uk Chest Assessment & Management BASICS Education March 2016 Objectives To understand the importance of oxygenation and ventilation To be able to describe
PRE-HOSPITAL EMERGENCY CARE COURSE www.basics.org.uk Chest Assessment & Management BASICS Education March 2016 Objectives To understand the importance of oxygenation and ventilation To be able to describe
Pulmonary Pathophysiology
 Pulmonary Pathophysiology 1 Reduction of Pulmonary Function 1. Inadequate blood flow to the lungs hypoperfusion 2. Inadequate air flow to the alveoli - hypoventilation 2 Signs and Symptoms of Pulmonary
Pulmonary Pathophysiology 1 Reduction of Pulmonary Function 1. Inadequate blood flow to the lungs hypoperfusion 2. Inadequate air flow to the alveoli - hypoventilation 2 Signs and Symptoms of Pulmonary
Emergency physician use of ultrasonography to evaluate hypotension: a case report
 Hong Kong Journal of Emergency Medicine Emergency physician use of ultrasonography to evaluate hypotension: a case report SSW Chan In a non-trauma patient, several conditions giving rise to hypotension
Hong Kong Journal of Emergency Medicine Emergency physician use of ultrasonography to evaluate hypotension: a case report SSW Chan In a non-trauma patient, several conditions giving rise to hypotension
IFT1 Interfacility Transfer of STEMI Patients. IFT2 Interfacility Transfer of Intubated Patients. IFT3 Interfacility Transfer of Stroke Patients
 IFT1 Interfacility Transfer of STEMI Patients IFT2 Interfacility Transfer of Intubated Patients IFT3 Interfacility Transfer of Stroke Patients Interfacility Transfer Guidelines IFT 1 TRANSFER INTERFACILITY
IFT1 Interfacility Transfer of STEMI Patients IFT2 Interfacility Transfer of Intubated Patients IFT3 Interfacility Transfer of Stroke Patients Interfacility Transfer Guidelines IFT 1 TRANSFER INTERFACILITY
Supplementary material 1. Definitions of study endpoints (extracted from the Endpoint Validation Committee Charter) 1.
 1.") Rationale, design, and baseline characteristics of the SIGNIFY trial: a randomized, double-blind, placebo-controlled trial of ivabradine in patients with stable coronary artery disease without clinical
Rationale, design, and baseline characteristics of the SIGNIFY trial: a randomized, double-blind, placebo-controlled trial of ivabradine in patients with stable coronary artery disease without clinical
Medical NREMT-PTE. NREMT Paramedic Trauma Exam.
 Medical NREMT-PTE NREMT Paramedic Trauma Exam https://killexams.com/pass4sure/exam-detail/nremt-pte Question: 41 Which of the following most accurately describes the finding of jugular venous distension
Medical NREMT-PTE NREMT Paramedic Trauma Exam https://killexams.com/pass4sure/exam-detail/nremt-pte Question: 41 Which of the following most accurately describes the finding of jugular venous distension
Can be felt where an artery passes near the skin surface and over a
 1 Chapter 14 Cardiovascular Emergencies 2 Cardiovascular Emergencies Cardiovascular disease has been leading killer of Americans since. Accounts for 1 of every 2.8 deaths Cardiovascular disease (CVD) claimed
1 Chapter 14 Cardiovascular Emergencies 2 Cardiovascular Emergencies Cardiovascular disease has been leading killer of Americans since. Accounts for 1 of every 2.8 deaths Cardiovascular disease (CVD) claimed
Background & Indications Probe Selection
 Teresa S. Wu, MD, FACEP Director, EM Ultrasound Program & Fellowship Co-Director, Simulation Based Training Program & Fellowship Associate Program Director, EM Residency Program Maricopa Medical Center
Teresa S. Wu, MD, FACEP Director, EM Ultrasound Program & Fellowship Co-Director, Simulation Based Training Program & Fellowship Associate Program Director, EM Residency Program Maricopa Medical Center
November 2012 Critical Care Case of the Month: I Just Can t Do It Captain! I Can t Get the Sats Up!
 November 2012 Critical Care Case of the Month: I Just Can t Do It Captain! I Can t Get the Sats Up! Bridgett Ronan, MD Department of Pulmonary Medicine Mayo Clinic Arizona Scottsdale, AZ History of Present
November 2012 Critical Care Case of the Month: I Just Can t Do It Captain! I Can t Get the Sats Up! Bridgett Ronan, MD Department of Pulmonary Medicine Mayo Clinic Arizona Scottsdale, AZ History of Present
Introduction and Overview of Acute Respiratory Failure
 Introduction and Overview of Acute Respiratory Failure Definition: Acute Respiratory Failure Failure to oxygenate Inadequate PaO 2 to saturate hemoglobin PaO 2 of 60 mm Hg ~ SaO 2 of 90% PaO 2 of 50 mm
Introduction and Overview of Acute Respiratory Failure Definition: Acute Respiratory Failure Failure to oxygenate Inadequate PaO 2 to saturate hemoglobin PaO 2 of 60 mm Hg ~ SaO 2 of 90% PaO 2 of 50 mm
Respiratory Disease. Dr Amal Damrah consultant Neonatologist and Paediatrician
 Respiratory Disease Dr Amal Damrah consultant Neonatologist and Paediatrician Signs and Symptoms of Respiratory Diseases Cardinal Symptoms Cough Sputum Hemoptysis Dyspnea Wheezes Chest pain Signs and Symptoms
Respiratory Disease Dr Amal Damrah consultant Neonatologist and Paediatrician Signs and Symptoms of Respiratory Diseases Cardinal Symptoms Cough Sputum Hemoptysis Dyspnea Wheezes Chest pain Signs and Symptoms
SAFE approach. Unresponsive? Shout or call for help. Open Airway. Not Breathing normally? 30 chest compressions. 2 rescue breaths
 Basic Life Support Dial 2222 Chin lift, head tilt jaw thrust Look, listen, feel For 10 seconds Rate 100/min *Lateral tilt* SAFE approach Unresponsive? Shout or call for help Open Airway Not Breathing normally?
Basic Life Support Dial 2222 Chin lift, head tilt jaw thrust Look, listen, feel For 10 seconds Rate 100/min *Lateral tilt* SAFE approach Unresponsive? Shout or call for help Open Airway Not Breathing normally?
Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition
 Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition Table of Contents Volume 1 Chapter 1: Cardiovascular Anatomy and Physiology Basic Cardiac
Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition Table of Contents Volume 1 Chapter 1: Cardiovascular Anatomy and Physiology Basic Cardiac
Chapter 14 Cardiovascular Emergencies Cardiovascular Emergencies Cardiovascular disease has been leading killer of Americans since.
 1 2 3 4 5 Chapter 14 Cardiovascular Emergencies Cardiovascular Emergencies Cardiovascular disease has been leading killer of Americans since. Accounts for 1 of every 2.8 deaths Cardiovascular disease (CVD)
1 2 3 4 5 Chapter 14 Cardiovascular Emergencies Cardiovascular Emergencies Cardiovascular disease has been leading killer of Americans since. Accounts for 1 of every 2.8 deaths Cardiovascular disease (CVD)
Shock, Monitoring Invasive Vs. Non Invasive
 Shock, Monitoring Invasive Vs. Non Invasive Paula Ferrada MD Assistant Professor Trauma, Critical Care and Emergency Surgery Virginia Commonwealth University Shock Fluid Pressors Ionotrope Intervention
Shock, Monitoring Invasive Vs. Non Invasive Paula Ferrada MD Assistant Professor Trauma, Critical Care and Emergency Surgery Virginia Commonwealth University Shock Fluid Pressors Ionotrope Intervention
HISTORY. Question: What category of heart disease is suggested by the fact that a murmur was heard at birth?
 HISTORY 23-year-old man. CHIEF COMPLAINT: Decreasing exercise tolerance of several years duration. PRESENT ILLNESS: The patient is the product of an uncomplicated term pregnancy. A heart murmur was discovered
HISTORY 23-year-old man. CHIEF COMPLAINT: Decreasing exercise tolerance of several years duration. PRESENT ILLNESS: The patient is the product of an uncomplicated term pregnancy. A heart murmur was discovered
Appendix to Gibson et al. Application of a decision rule and a D-dimer assay in the
 Appendix to Gibson et al. Application of a decision rule and a D-dimer assay in the diagnosis of pulmonary embolism (Thromb Haemost 2010; 103.4) Case 1 You are paged by an emergency room physician, who
Appendix to Gibson et al. Application of a decision rule and a D-dimer assay in the diagnosis of pulmonary embolism (Thromb Haemost 2010; 103.4) Case 1 You are paged by an emergency room physician, who
Shock. William Schecter, MD
 Shock William Schecter, MD The Cell as a furnace O 2 1 mole Glucose Cell C0 2 ATP 38 moles H 2 0 Shock = Inadequate Delivery of 02 and Glucose to the Cell 0 2 Cell ATP 2 moles Lactic Acid Treatment of
Shock William Schecter, MD The Cell as a furnace O 2 1 mole Glucose Cell C0 2 ATP 38 moles H 2 0 Shock = Inadequate Delivery of 02 and Glucose to the Cell 0 2 Cell ATP 2 moles Lactic Acid Treatment of
Case 1 Organ Set 3. Case 1 (for Organ Sets 1 3) 10/2/2015 CARIOVASCULAR II LABORATORY
 10/2/2015 CARIOVASCULAR II LABORATORY") MHD I CRIOVSCULR II LORTORY 0/5/5 Case Organ Set Organ Set 2 Organ Set 3 Case (for Organ Sets 3) 72 year old man with a history of diabetes mellitus type 2, HTN, and hyperlipidemia presents with progressive
MHD I CRIOVSCULR II LORTORY 0/5/5 Case Organ Set Organ Set 2 Organ Set 3 Case (for Organ Sets 3) 72 year old man with a history of diabetes mellitus type 2, HTN, and hyperlipidemia presents with progressive
Adult Echocardiography Examination Content Outline
 Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
Introduction. Invasive Hemodynamic Monitoring. Determinants of Cardiovascular Function. Cardiovascular System. Hemodynamic Monitoring
 Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
REPORT OF TRANSFUSION ADVERSE REACTION TO BLOOD CENTERS
 REPORT OF TRANSFUSION ADVERSE REACTION TO BLOOD CENTERS INSTRUCTIONS: Send the form to ALL blood centers that provided blood components to this patient. Timely reporting is important, so that, if appropriate,
REPORT OF TRANSFUSION ADVERSE REACTION TO BLOOD CENTERS INSTRUCTIONS: Send the form to ALL blood centers that provided blood components to this patient. Timely reporting is important, so that, if appropriate,
Cath Lab Essentials: Pericardial effusion & tamponade
 Cath Lab Essentials: Pericardial effusion & tamponade Pranav M. Patel, MD, FACC, FSCAI Chief, Division of Cardiology Director, Cardiac Cath Lab & CCU University of California, Irvine Division of Cardiology
Cath Lab Essentials: Pericardial effusion & tamponade Pranav M. Patel, MD, FACC, FSCAI Chief, Division of Cardiology Director, Cardiac Cath Lab & CCU University of California, Irvine Division of Cardiology
Postoperative chest x-ray May Mats Beckman Emergency Radiology. Shutter use!
 Postoperative chest x-ray May 2009 Mats Beckman Emergency Radiology Shutter use! 2Postoperative chest x-ray May 2009 Exposure/ window settings Quick resorption of infiltrations= water logged lung 3Postoperative
Postoperative chest x-ray May 2009 Mats Beckman Emergency Radiology Shutter use! 2Postoperative chest x-ray May 2009 Exposure/ window settings Quick resorption of infiltrations= water logged lung 3Postoperative
Expanding Horizons: AngioVac Suction Thrombectomy at UTHealth
 Expanding Horizons: AngioVac Suction Thrombectomy at UTHealth Naveed Saqib, MD Assistant Professor Department of Cardiothoracic and Vascular Surgery McGovern Medical School The University of Texas Science
Expanding Horizons: AngioVac Suction Thrombectomy at UTHealth Naveed Saqib, MD Assistant Professor Department of Cardiothoracic and Vascular Surgery McGovern Medical School The University of Texas Science
Cardiovascular and Pulmonary System
 Cardiovascular and Pulmonary System MS1 - COM 531 - Spring 2018 3/21/2018 Weeks Date Time Title Faculty Monday, 3/26/2018 8:00-9:00 am CVP Course Introduction Falck & Yarbrough Monday, 3/26/2018 9:00-10:00
Cardiovascular and Pulmonary System MS1 - COM 531 - Spring 2018 3/21/2018 Weeks Date Time Title Faculty Monday, 3/26/2018 8:00-9:00 am CVP Course Introduction Falck & Yarbrough Monday, 3/26/2018 9:00-10:00
Impedance Cardiography (ICG) Application of ICG in Intensive Care and Emergency
 Application of ICG in Intensive Care and Emergency") Impedance Cardiography (ICG) Application of ICG in Intensive Care and Emergency Aim of haemodynamic monitoring in ICU and ED Detection and therapy of insufficient organ perfusion Answers to common cardiovascular
Impedance Cardiography (ICG) Application of ICG in Intensive Care and Emergency Aim of haemodynamic monitoring in ICU and ED Detection and therapy of insufficient organ perfusion Answers to common cardiovascular
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acute coronary syndrome(s), anticoagulant therapy in, 706, 707 antiplatelet therapy in, 702 ß-blockers in, 703 cardiac biomarkers in,
Index Note: Page numbers of article titles are in boldface type. A Acute coronary syndrome(s), anticoagulant therapy in, 706, 707 antiplatelet therapy in, 702 ß-blockers in, 703 cardiac biomarkers in,
The Cardiovascular System Part I: Heart Outline of class lecture After studying part I of this chapter you should be able to:
 The Cardiovascular System Part I: Heart Outline of class lecture After studying part I of this chapter you should be able to: 1. Describe the functions of the heart 2. Describe the location of the heart,
The Cardiovascular System Part I: Heart Outline of class lecture After studying part I of this chapter you should be able to: 1. Describe the functions of the heart 2. Describe the location of the heart,
PFIZER INC. Study Center(s): A total of 6 centers took part in the study, including 2 in France and 4 in the United States.
: A total of 6 centers took part in the study, including 2 in France and 4 in the United States.") PFIZER INC. These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert. For publications based on this study, see associated bibliography.
PFIZER INC. These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert. For publications based on this study, see associated bibliography.
Chest Trauma.
 Chest Trauma www.fisiokinesiterapia.biz Objectives Anatomy of Thorax Main Causes of Chest Injuries S/S of Chest Injuries Different Types of Chest Injuries Treatments of Chest Injuries Anatomy of the chest
Chest Trauma www.fisiokinesiterapia.biz Objectives Anatomy of Thorax Main Causes of Chest Injuries S/S of Chest Injuries Different Types of Chest Injuries Treatments of Chest Injuries Anatomy of the chest
Bedside assessment of fluid status
 Bedside assessment of fluid status 2nd AKI Academy October 18 th 2014 David Treacher Guy s & St Thomas NHS Trust Assessing the circulation - the 3 key questions v Is my patient adequately filled? v What
Bedside assessment of fluid status 2nd AKI Academy October 18 th 2014 David Treacher Guy s & St Thomas NHS Trust Assessing the circulation - the 3 key questions v Is my patient adequately filled? v What
Cardiovascular Practice Quiz
 Cardiovascular Practice Quiz 1. When caring for a patient following a cardiac catheterization with coronary angiography, which of the following findings would be of most concern to the nurse? a. Swelling
Cardiovascular Practice Quiz 1. When caring for a patient following a cardiac catheterization with coronary angiography, which of the following findings would be of most concern to the nurse? a. Swelling
Cardiac Emergencies. Jim Bennett Paramedic and Clinical Education Coordinator American Medical Response Spokane, Washington
 Cardiac Emergencies Jim Bennett Paramedic and Clinical Education Coordinator American Medical Response Spokane, Washington The Heart -------Aorta Pulmonary Veins---- Superior Vena Cava------ Right Atrium-----
Cardiac Emergencies Jim Bennett Paramedic and Clinical Education Coordinator American Medical Response Spokane, Washington The Heart -------Aorta Pulmonary Veins---- Superior Vena Cava------ Right Atrium-----
ARDS Management Protocol
 ARDS Management Protocol February 2018 ARDS Criteria Onset Within 1 week of a known clinical insult or new or worsening respiratory symptoms Bilateral opacities not fully explained by effusions, lobar/lung
ARDS Management Protocol February 2018 ARDS Criteria Onset Within 1 week of a known clinical insult or new or worsening respiratory symptoms Bilateral opacities not fully explained by effusions, lobar/lung
Definition: HPS is a disease process with a triad of: 1- Liver disease. 2- Widespread intrapulmonary vasodilatation. 3- Gas exchange abnormality prese
 Hepatopulmonary syndrome (HPS) By Alaa Haseeb, MS.c Definition: HPS is a disease process with a triad of: 1- Liver disease. 2- Widespread intrapulmonary vasodilatation. 3- Gas exchange abnormality presenting
Hepatopulmonary syndrome (HPS) By Alaa Haseeb, MS.c Definition: HPS is a disease process with a triad of: 1- Liver disease. 2- Widespread intrapulmonary vasodilatation. 3- Gas exchange abnormality presenting
Case discussion Acute severe asthma during pregnancy. J.G. van der Hoeven
 Case discussion Acute severe asthma during pregnancy J.G. van der Hoeven Case (1) 32-year-old female - gravida 3 - para 2 Previous medical history - asthma Pregnant (33 w) Acute onset fever with wheezing
Case discussion Acute severe asthma during pregnancy J.G. van der Hoeven Case (1) 32-year-old female - gravida 3 - para 2 Previous medical history - asthma Pregnant (33 w) Acute onset fever with wheezing
DAY1_CARDIOVASCULAR PRACTICE QUESTIONS
 DAY1_CARDIOVASCULAR PRACTICE QUESTIONS 1 P age 1. A 59-year-old male is admitted complaining of chest pain and dyspnea. ST elevation and T-wave inversion were seen on the ECG in V2, V3, and V4. IV thrombolytic
DAY1_CARDIOVASCULAR PRACTICE QUESTIONS 1 P age 1. A 59-year-old male is admitted complaining of chest pain and dyspnea. ST elevation and T-wave inversion were seen on the ECG in V2, V3, and V4. IV thrombolytic
Cardiac Emergencies. A Review of Cardiac Compromise. Lawrence L. Lambert
 Cardiac Emergencies A Review of Cardiac Compromise Lawrence L. Lambert 1 Cardiac Emergencies Objectives: Following successful completion of this training session, the student should be able to: 1. Describe
Cardiac Emergencies A Review of Cardiac Compromise Lawrence L. Lambert 1 Cardiac Emergencies Objectives: Following successful completion of this training session, the student should be able to: 1. Describe
You Are the Emergency Medical Responder
 Lesson 32: Injuries to the Chest, Abdomen and Genitalia You Are the Emergency Medical Responder Your police unit responds to a call in a part of town plagued by violence. When you arrive, you find the
Lesson 32: Injuries to the Chest, Abdomen and Genitalia You Are the Emergency Medical Responder Your police unit responds to a call in a part of town plagued by violence. When you arrive, you find the
5. What is the cause of this patient s metabolic acidosis? LACTIC ACIDOSIS SECONDARY TO ANEMIC HYPOXIA (HIGH CO LEVEL)
") Self-Assessment RSPT 2350: Module F - ABG Analysis 1. You are called to the ER to do an ABG on a 40 year old female who is C/O dyspnea but seems confused and disoriented. The ABG on an FiO 2 of.21 show:
Self-Assessment RSPT 2350: Module F - ABG Analysis 1. You are called to the ER to do an ABG on a 40 year old female who is C/O dyspnea but seems confused and disoriented. The ABG on an FiO 2 of.21 show:
Heart Disorders. Cardiovascular Disorders (Part B-1) Module 5 -Chapter 8. Overview Heart Disorders Vascular Disorders
 Module 5 -Chapter 8. Overview Heart Disorders Vascular Disorders") Cardiovascular Disorders (Part B-1) Module 5 -Chapter 8 Overview Heart Disorders Vascular Disorders Susie Turner, MD 1/7/13 Heart Disorders Coronary Artery Disease Cardiac Arrhythmias Congestive Heart
Cardiovascular Disorders (Part B-1) Module 5 -Chapter 8 Overview Heart Disorders Vascular Disorders Susie Turner, MD 1/7/13 Heart Disorders Coronary Artery Disease Cardiac Arrhythmias Congestive Heart
Imminent Cardiac Collapse: The Catastrophe You Cannot Afford To Miss
 Imminent Cardiac Collapse: The Catastrophe You Cannot Afford To Miss Presenting Authors Ameya J Baxi, MD (baxi@uthscsa.edu) Carlos Restrepo, MD Disclaimer: We do not have any conflict of interest or financial
Imminent Cardiac Collapse: The Catastrophe You Cannot Afford To Miss Presenting Authors Ameya J Baxi, MD (baxi@uthscsa.edu) Carlos Restrepo, MD Disclaimer: We do not have any conflict of interest or financial
SHOCK. Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital
 SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
ERDHEIM-CHESTER DISEASE LUNG & HEART ISSUES
 ERDHEIM-CHESTER DISEASE LUNG & HEART ISSUES GIULIO CAVALLI, M.D. INTERNAL MEDICINE AND CLINICAL IMMUNOLOGY IRCCS SAN RAFFAELE HOSPITAL VITA-SALUTE SAN RAFFAELE UNIVERSITY MILAN, ITALY cavalli.giulio@hsr.it
ERDHEIM-CHESTER DISEASE LUNG & HEART ISSUES GIULIO CAVALLI, M.D. INTERNAL MEDICINE AND CLINICAL IMMUNOLOGY IRCCS SAN RAFFAELE HOSPITAL VITA-SALUTE SAN RAFFAELE UNIVERSITY MILAN, ITALY cavalli.giulio@hsr.it
Carry this card with you at all times. Show this card to any medical professional treating you. Patient Implant Card. Option ELITE Vena Cava Filter.
 Patient Guide A Safe Option for a Healthier You! P/N: P-2017-0175-00 Rev B 1. Static magnetic field of 3 Tesla or less. 2. Spatial gradient magnetic field of 720 Gauss/cm or less. 3. Maximum whole body
Patient Guide A Safe Option for a Healthier You! P/N: P-2017-0175-00 Rev B 1. Static magnetic field of 3 Tesla or less. 2. Spatial gradient magnetic field of 720 Gauss/cm or less. 3. Maximum whole body
Syncope Due to Intracavitary Left Ventricular Obstruction Secondary to Giant Esophageal Hiatus Hernia
 American Journal of Medical Case Reports, 2017, Vol. 5, No. 4, 89-93 Available online at http://pubs.sciepub.com/ajmcr/5/4/4 Science and Education Publishing DOI:10.12691/ajmcr-5-4-4 Syncope Due to Intracavitary
American Journal of Medical Case Reports, 2017, Vol. 5, No. 4, 89-93 Available online at http://pubs.sciepub.com/ajmcr/5/4/4 Science and Education Publishing DOI:10.12691/ajmcr-5-4-4 Syncope Due to Intracavitary
Looking Outside the Box: Incidental Extracardiac Finding in Echo
 Looking Outside the Box: Incidental Extracardiac Finding in Echo Dr. Aijaz Shah Head of Division, Adult Echocardiography Laboratory Prince Sultan Cardiac Centre Riyadh Case 1 17 year old boy presented
Looking Outside the Box: Incidental Extracardiac Finding in Echo Dr. Aijaz Shah Head of Division, Adult Echocardiography Laboratory Prince Sultan Cardiac Centre Riyadh Case 1 17 year old boy presented
Mary Lou Garey MSN EMT-P MedFlight of Ohio
 Mary Lou Garey MSN EMT-P MedFlight of Ohio Function Prolonged and frequent access to venous circulation Allows for patient to carry on normal life; decrease number of needle sticks Medications, parenteral
Mary Lou Garey MSN EMT-P MedFlight of Ohio Function Prolonged and frequent access to venous circulation Allows for patient to carry on normal life; decrease number of needle sticks Medications, parenteral
Lines and tubes. 1 Nasogastric tubes Endotracheal tubes Central lines Permanent pacemakers Chest drains...
 Lines and tubes 1 Nasogastric tubes... 15 2 Endotracheal tubes.... 19 3 Central lines... 21 4 Permanent pacemakers.... 25 5 Chest drains... 30 This page intentionally left blank 1 Nasogastric tubes Background
Lines and tubes 1 Nasogastric tubes... 15 2 Endotracheal tubes.... 19 3 Central lines... 21 4 Permanent pacemakers.... 25 5 Chest drains... 30 This page intentionally left blank 1 Nasogastric tubes Background
Michigan Pediatric Cardiac Protocols. Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS
 Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Post-Cardiac Arrest Syndrome. MICU Lecture Series
 Post-Cardiac Arrest Syndrome MICU Lecture Series Case 58 y/o female collapses at home, family attempts CPR, EMS arrives and notes VF, defibrillation x 3 with return of spontaneous circulation, brought
Post-Cardiac Arrest Syndrome MICU Lecture Series Case 58 y/o female collapses at home, family attempts CPR, EMS arrives and notes VF, defibrillation x 3 with return of spontaneous circulation, brought
Surgical Care at the District Hospital. EMERGENCY & ESSENTIAL SURGICAL CARE
 Surgical Care at the District Hospital 1 13 Resuscitation and Preparation for Anesthesia & Surgery Key Points 2 13.1 Management of Emergencies and Cardiopulmonary Resuscitation The emergency measures that
Surgical Care at the District Hospital 1 13 Resuscitation and Preparation for Anesthesia & Surgery Key Points 2 13.1 Management of Emergencies and Cardiopulmonary Resuscitation The emergency measures that
Traumatic A-V A V Fistula
 Traumatic A-V A V Fistula PRESENT HISTORY PAST HISTORY 30 year-old, male ( XX); Denied other systemic disease before. PRESENT HISTORY A deep stabbing wound (3*1 cm) noted on 07/01/2002 over Right anterior
Traumatic A-V A V Fistula PRESENT HISTORY PAST HISTORY 30 year-old, male ( XX); Denied other systemic disease before. PRESENT HISTORY A deep stabbing wound (3*1 cm) noted on 07/01/2002 over Right anterior
Innovative Endovascular Approach to Pulmonary Embolism by Ultrasound Enhanced Thrombolysis. Prof. Ralf R.Kolvenbach MD,PhD,FEBVS
 Innovative Endovascular Approach to Pulmonary Embolism by Ultrasound Enhanced Thrombolysis Prof. Ralf R.Kolvenbach MD,PhD,FEBVS Catheter-based thrombolysis Local administration of lytic agent Higher local
Innovative Endovascular Approach to Pulmonary Embolism by Ultrasound Enhanced Thrombolysis Prof. Ralf R.Kolvenbach MD,PhD,FEBVS Catheter-based thrombolysis Local administration of lytic agent Higher local
I-Ming Chen, MD. Endovascular Stenting for Palliative Treatment of Superior Vena Cava Syndrome in End-Stage Lung Cancer
 Endovascular Stenting for Palliative Treatment of Superior Vena Cava Syndrome in End-Stage Lung Cancer I-Ming Chen, MD Division of CardioVascular Surgery Taipei Veterans General Hospital, Taiwan (Live
Endovascular Stenting for Palliative Treatment of Superior Vena Cava Syndrome in End-Stage Lung Cancer I-Ming Chen, MD Division of CardioVascular Surgery Taipei Veterans General Hospital, Taiwan (Live
Presentation, symptoms and signs of heart failure
 3 Presentation, symptoms and signs of heart failure What will I learn? In this section you will learn: Who is at risk of heart failure The symptoms of heart failure The signs of heart failure The importance
3 Presentation, symptoms and signs of heart failure What will I learn? In this section you will learn: Who is at risk of heart failure The symptoms of heart failure The signs of heart failure The importance
SHOCK and the Trauma Victim. JP Pretorius Department of Surgery & SICU Steve Biko Academic Hospital.
 SHOCK and the Trauma Victim JP Pretorius Department of Surgery & SICU Steve Biko Academic Hospital. Classification of Shock Cardiogenic - Myopathic Arrythmic Mechanical Hypovolaemic - Haemorrhagic Non-haemorrhagic
SHOCK and the Trauma Victim JP Pretorius Department of Surgery & SICU Steve Biko Academic Hospital. Classification of Shock Cardiogenic - Myopathic Arrythmic Mechanical Hypovolaemic - Haemorrhagic Non-haemorrhagic
1. In a rear-impact motor vehicle crash, which area of the spine is most susceptible to injury? A. Cervical B. Thoracic C. Lumbar D.
 1. In a rear-impact motor vehicle crash, which area of the spine is most susceptible to injury? A. Cervical B. Thoracic C. Lumbar D. Sacral-coccygeal 2. A 36-year-old male sustains blunt force thoracic
1. In a rear-impact motor vehicle crash, which area of the spine is most susceptible to injury? A. Cervical B. Thoracic C. Lumbar D. Sacral-coccygeal 2. A 36-year-old male sustains blunt force thoracic
What is the mechanism of the audible carotid bruit? How does one calculate the velocity of blood flow?
 CASE 8 A 65-year-old man with a history of hypertension and coronary artery disease presents to the emergency center with complaints of left-sided facial numbness and weakness. His blood pressure is normal,
CASE 8 A 65-year-old man with a history of hypertension and coronary artery disease presents to the emergency center with complaints of left-sided facial numbness and weakness. His blood pressure is normal,
Worsening Hypoxemia in the Face of Increasing PEEP: A Case of Large Pulmonary Embolism in the Setting of Intracardiac Shunt
 ISSN 1941-5923 DOI: 10.12659/AJCR.898521 Received: 2016.03.15 Accepted: 2016.04.18 Published: 2016.07.05 Worsening Hypoxemia in the Face of Increasing PEEP: A Case of Large Pulmonary Embolism in the Setting
ISSN 1941-5923 DOI: 10.12659/AJCR.898521 Received: 2016.03.15 Accepted: 2016.04.18 Published: 2016.07.05 Worsening Hypoxemia in the Face of Increasing PEEP: A Case of Large Pulmonary Embolism in the Setting
PROTOCOL 1 Endotracheal Intubation (Adult and Pediatric) REQUEST EMT-P RESPONSE DO NOT DELAY TRANSPORT
 REQUEST EMT-P RESPONSE DO NOT DELAY TRANSPORT") PROTOCOL 1 Endotracheal Intubation (Adult and Pediatric) 1. Basic Life Support airway management procedures are initiated. 2. Endotracheal Intubation is indicated under any of the following conditions:
PROTOCOL 1 Endotracheal Intubation (Adult and Pediatric) 1. Basic Life Support airway management procedures are initiated. 2. Endotracheal Intubation is indicated under any of the following conditions: