Mechanical Ventilation & Cardiopulmonary Interactions: Clinical Application in Non- Conventional Circulations. Eric M. Graham, MD
|
|
|
- Beverley Ferguson
- 5 years ago
- Views:
Transcription

1 Mechanical Ventilation & Cardiopulmonary Interactions: Clinical Application in Non- Conventional Circulations Eric M. Graham, MD



2 Background Heart & lungs work to meet oxygen demands Imbalance between supply and demand may result in hypoxia and death Critical to maintain cardiopulmonary function
3 Background Heart & lungs work to meet oxygen demands Imbalance between supply and demand may result in hypoxia and death Critical to maintain cardiopulmonary function Interventions aimed at improving one system can negatively affect the other
4 Basic Principles Ventilation induce changes in intrathoracic pressure & lung volume Independently affect cardiac output Preload (atrial filling) Afterload (impedence to ventricular emptying) Myocardial contractility Heart rate
5 Spontaneous Inspiration Negative pleural pressure transmitted to RA Increase in intraabdominal pressure Larger driving pressure gradient from extrathoracic veins to the RA Increasing RA filling
6 Spontaneous Inspiration Negative pleural pressure transmitted to RA Increase in intraabdominal pressure Larger driving pressure gradient from extrathoracic veins to the RA Increasing RA filling
7 Spontaneous Inspiration Negative pleural pressure transmitted to RA Increase in intraabdominal pressure Larger driving pressure gradient from extrathoracic veins to the RA Increasing RA filling
8 Spontaneous Inspiration Negative pleural pressure transmitted to RA Increase in intraabdominal pressure Larger driving pressure gradient from extrathoracic veins to the RA Increasing RA filling
9 Intermittent Positive Pressure IPPV produces inspiratory increase in intrathoracic and RA pressure Ventilation (IPPV) If PEEP is added, intrathoracic > atmospheric pressures Hinder RA filling
10 Superior Cavopulmonary Connection Glenn 1957 SVC to RPA BDG SVC to confluent PA s Hemi-Fontan
11 SCPC Circulation Cerebral & pulmonary circulations are in series Aortic blood brain SVC lungs Without a pulmonary ventricle Dependant on low resistance pulmonary vascular bed
12 SCPC Circulation Cerebral & pulmonary circulations are in series Aortic blood brain SVC lungs Without a pulmonary ventricle Dependant on low resistance pulmonary vascular bed
13 SCPC Circulation Cerebral & pulmonary circulations are in series Aortic blood brain SVC lungs Without a pulmonary ventricle Dependant on low resistance pulmonary vascular bed
14 SCPC Circulation Cerebral & pulmonary circulations are in series Aortic blood brain SVC lungs Without a pulmonary ventricle Dependant on low resistance pulmonary vascular bed

15 SCPC Circulation Cerebral & pulmonary circulations are in series Aortic blood brain SVC lungs Without a pulmonary ventricle Dependant on low resistance pulmonary vascular bed
16 Pulmonary Blood Flow Following SCPC Anatomic Patent anastamosis Pulmonary artery size Aortopulmonary collaterals Venovenous collaterals Cerebral & pulmonary autoregulation Ventilation, PC02 Pulmonary vasodilators
17 Pulmonary Blood Flow Following SCPC Anatomic Patent anastamosis Pulmonary artery size Aortopulmonary collaterals Venovenous collaterals Cerebral & pulmonary autoregulation Ventilation, PC02 Pulmonary vasodilators
18 The Effect Of Hyperventilation Hyperventilation PCO 2 Respiratory alkalosis ph Cerebral resistance Cerebral flow Pulmonary flow PVR Pulmonary flow?
19 Hyperventilation Following SCPC 12 patients Within 6 hours of SCPC Sedated & paralyzed Baseline hyperventilation baseline Cerebral flow measured with transcranial Doppler Bradley SM. Circulation 1998
20 Hyperventilation After BSCC Baseline Hypervent Baseline ph PCO
21 Arterial PO torr * Baseline Hypervent Baseline
22 Systemic O 2 Saturation % * Baseline Hypervent Baseline
23 Cerebral Blood Flow Velocity cm/sec * Baseline Hypervent Baseline Transcranial doppler of middle cerebral artery
24 Hyperventilation After BSCC Baseline Hypervent Baseline Syst PA O Airway pressure Peak Mean 4 8 4
25 Pulmonary Artery Pressure Transpulmonary Gradient mm Hg * * Baseline Hypervent Baseline PAP TPG
26 Hyperventilation After SCPC Impairs systemic oxygenation Despite decreasing PAP, TPG PCO 2 decreases cerebral, SVC, pulmonary blood flow Bradley SM. Circulation 1998
27 Hypoventilation Following SCPC 15 patients Within 8 hours of SCPC Sedated & paralyzed Baseline hypoventilation Sodium bicarbonate administered prior Cerebral flow measured with transcranial Doppler Bradley SM. J Thorac Cardiovasc Surg 2003
28 Hypoventilation After SCPC Na Bicarbonate + Baseline Hypoventilation PCO ph
29 Arterial PO 2 torr Baseline * 61 Hypoventilation
30 Systemic O 2 Saturation * % Baseline Hypoventilation
31 Cerebral Blood Flow Velocity cm/sec Baseline * Hypoventilation Transcranial doppler of middle cerebral artery
32 Hypoventilation After BSCC Baseline Hypovent Syst PA O Airway pressure Peak Mean 6 4
33 Pulmonary Artery Pressure Transpulmonary Gradient mm Hg Baseline * * Hypoventilation PAP TPG
34 Hypoventilation After SCPC Improves systemic oxygenation Despite increasing PAP & TPG PCO 2 increases cerebral, SVC, pulmonary blood flow Bradley SM. J Thorac Cardiovasc Surg 2003
35 Altering Ventilation After SCPC Remaining Questions Flows not directly measured Role of airway pressure Cerebral flow steal from lower body vs. increase in overall cardiac output
36 PCO 2 After SCPC 9 patients early after SCPC Sedated & paralyzed PCO 2 by adding inspired CO 2 Blood flow, cardiac output by Fick O 2 consumption by mass spectrometry Hoskote A. J Am Coll Cardiol 2004
37 PCO 2 After SCPC Baseline Inspired CO 2 PCO ph PO O 2 Sat 72 80
38 Blood Flows 5 l/min/m Q IVC Baseline Q P
39 5 Blood Flows 4.9 C.O. l/min/m Q IVC Baseline Inspired CO2 Q P
40 PCO 2 After SCPC 12 patients, 20 months after SCPC PCO 2 by adding inspired CO 2 Blood flows by MRI velocity mapping Fogel MA. Circulation 2004
41 PCO 2 After BSCC Baseline Inspired CO 2 PCO ph PO
42 Blood Flows l/min/m C.O. Q IVC Q P 0 Baseline Inspired CO2
43 Hypercarbia After SCPC Improves systemic oxygenation Cerebral, SVC, pulmonary flow Cardiac output; No steal from IVC Inspired CO 2 No Δ in airway pressures Early and late after SCPC Hoskote A. J Am Coll Cardiol 2004; Fogel MA. Circulation 2004
44 Pulmonary Vasodilators Oxygen Nitric oxide
45 Oxygen After SCPC 12 patients, 20 months after BSCC Flows by MRI velocity mapping 100% oxygen No Δ cerebral, pulmonary flow Fogel MA. Circulation 2004
46 Nitric Oxide After SCPC Selective pulmonary vasodilator 26 patients Systemic O 2 Sat < 75% 1 st day after SCPC Baseline nitric oxide baseline Adatia I. J Thorac Cardiovasc Surg 2005
47 Nitric Oxide After SCPC Baseline NO Baseline PAP 17 15* 16 TPG PO O 2 Sat
48 Pulmonary Vasodilators After SCPC Oxygen & Nitric Oxide PVR low, nonreactive Pulmonary vasoconstriction limits neither: Pulmonary blood flow Systemic oxygenation Fogel MA. Circulation 2004; Adatia I. J Thorac Cardiovasc Surg 2005
49 Nitric Oxide After SCPC Retrospective study over 30 months ino initiated within 3 hrs of operation SCPC pressures ~ 20 mmhg, instability 16 patients received ino vs 28 did not Pre-op cath: higher mpap and PVR Agarwal H. Ann Thorac Surg 2006
50 Nitric Oxide After SCPC Retrospective study over 30 months ino initiated within 3 hrs of operation SCPC pressures ~ 20 mmhg, instability 16 patients received ino vs 28 did not Pre-op cath: higher mpap and PVR 11 (69%) responded All 5 non-responders were found to have an anatomic lesion Agarwal H. Ann Thorac Surg 2006
51 11 Responders: Nitric Oxide After SCPC Baseline 1 hour ino 3 hour ino PAP 23 19* 17* Inotrope score 15 12* 11* PO 2 /FiO * 74* PO Agarwal H. Ann Thorac Surg 2006

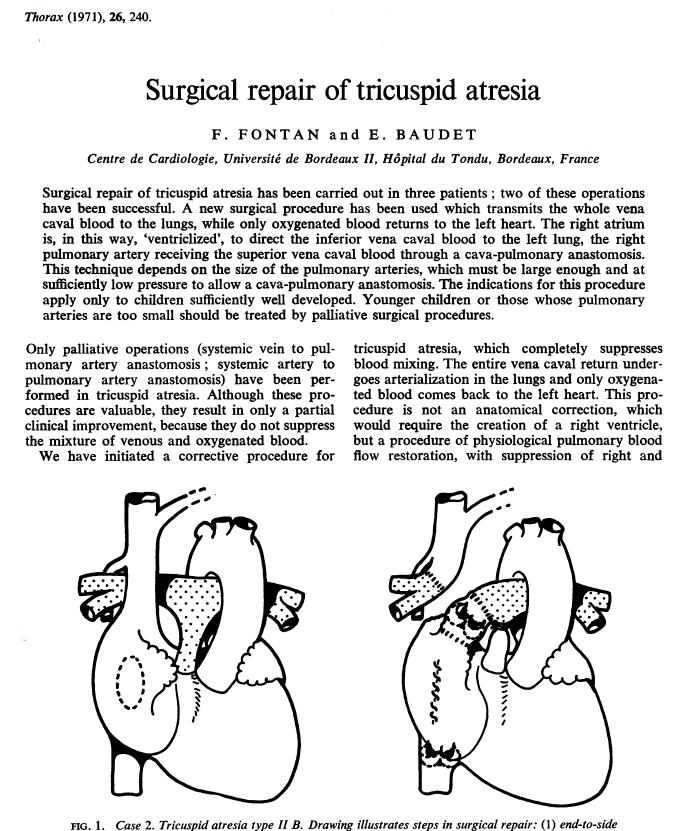
52 Total Cavopulmonary Connection Fontan 1971 Pulmonary blood flow is cardiac output Passive diastolic phenomenon Strongly influenced by changes in intrathoracic pressures
53 Spontaneous Respiration Redington AN. Br Heart J 1991

54 Spontaneous Respiration Redington AN. Br Heart J 1991
55 Brief Valsalva Redington AN. Br Heart J 1991

56 Brief Valsalva Redington AN. Br Heart J 1991
57 Prolonged Valsalva Redington AN. Br Heart J 1991

58 Prolonged Valsalva Redington AN. Br Heart J 1991

59 Prolonged Valsalva Redington AN. Br Heart J 1991
60 Detrimental Effects of Positive Pressure Ventilation Antegrade pulmonary flow and hence cardiac output can be significantly reduced with increased intrathoracic pressure Intermittent positive pressure ventilation Short inspiratory time Low inspiratory pressures Minimal PEEP Early extubation
61
62

63
64 Hemodynamic Benefits of Spontaneous Respiration 50 consecutive patients BDG (n=23) Fontan (n=27) Cardiac output determined utilizing extra vascular probes on ascending aorta (n=12) All patients extubated in the OR or within 1 hour after arrival to the ICU Lofland GK. Eur J Cardiothorac Surg 2001
65 Mean PAP mmhg Pre Post 6 hrs Post 12 hrs Post
66 Cardiac Index Pre Post 12 hrs Post
67 Benefits of Extubation in the OR Retrospective review 112 Fontan pts During the study period all patients were considered for extubation in the OR Clinical judgment Pts were grouped into those extubated in the OR and those extubated in the ICU 34% (n=38) extubated in the OR Morales DLS. Ann Thorac Surg 2008
68 Improved Hemodynamics Extubated in OR Mean PA pressure Mean systemic arterial pressure
69 Results Extubated OR Extubated ICU Inotropic support (days) ICU stay (days) Hospital stay (days) ICU cost ($) 32,000 49,000 Hospital cost ($) 44,000 64,000 Survival (%) 100% 99% All p < 0.05
70 Extubation in the OR Limited by nonrandom assignment Affirms the hemodynamic benefits of early extubation Safe Effective Reduced costs
 Mahle WT.")
71 Data from the STS Database Association of early extubation with LOS Centers stratified into tertiles by frequency of early extubation (<6 hrs) Mahle WT. Ann Thorac Surg 2016
72 Benefits of Early Extubation 92 centers Early extubation in 70% 1,153/1,653 Mahle WT. Ann Thorac Surg 2016
73 Benefits of Early Extubation 92 centers Early extubation in 70% 1,153/1, Mahle WT. Ann Thorac Surg 2016
74 Benefits of Early Extubation 92 centers Early extubation in 70% 1,153/1,653 9 Mahle WT. Ann Thorac Surg 2016
75 Benefits of Early Extubation 92 centers Early extubation in 70% 1,153/1,653 Median LOS was 9 days (IQR 7-14 days) Mahle WT. Ann Thorac Surg 2016
 No association with early extubation & LOS Mahle WT.")
76 Benefits of Early Extubation 92 centers Early extubation in 70% 1,153/1,653 Median LOS was 9 days (IQR 7-14 days) No association with early extubation & LOS Mahle WT. Ann Thorac Surg 2016
77 Unfortunately early extubation is not always feasible, and paradoxically, it is in those children in whom this is most desirable that continued ventilator support is needed
78 Negative Pressure Ventilation Hemodynamic effects of NPV on Fontan N=9, immediate post-op period N=9, late phase (5mo-15yrs) after elective cath Paralyzed, sedated, IPPV Blood flow, cardiac output by Fick O 2 consumption by mass spectrometry IPPV NPV Subgroup 1: reinstitution of IPPV Subgroup 2: extended period of NPV Shekerdemian LS. Circulation 1997
79 Pulmonary Blood Flow
80 Pulmonary Blood Flow %
81 Results IPPV NPV Stroke volume (ml/m 2 ) Oxygen consumption (ml/min/m 2 ) Mixed venous saturation (%) Mean PA pressure (mmhg) PVR (U/m 2 ) All p < 0.05
82 Reinstitution of IPPV
83 Extended NPV
84 Predictors of Improvement with NPV Strong positive correlation Acute patients Preop Ventricular EDP Postop mean PA pressure Marked in pulmonary blood flow and cardiac output


85 Deshpande SR. Heart, lung, and Circ 2011


86


87 Deshpande SR. World J Cardiol 2014
88 Alternative Modes of Ventilation High-Frequency Jet Ventilation 13 pts following Fontan; IPPV HFJV Mean airway pressure: PVR: Cardiac index: ( all p 0.001) High-Frequency Oscillation 5 pts following Fontan No effect on cardiac output or PVR Meliones JN. Circulation 1991; Kornecki A. Pediatr Crit Care Med 2002
89 Alternative Modes of Ventilation High-Frequency Jet Ventilation 13 pts following Fontan; IPPV HFJV Mean airway pressure: PVR: Cardiac index: ( all p 0.001) High-Frequency Oscillation 5 pts following Fontan No effect on cardiac output or PVR Meliones JN. Circulation 1991; Kornecki A. Pediatr Crit Care Med 2002
90 Summary Avoid hyperventilation Encourage mild hypercarbia Pulmonary vasodilators not determinants Early extubation Alternative modes of ventilation Negative pressure High-frequency jet
Management of a Patient after the Bidirectional Glenn
 Management of a Patient after the Bidirectional Glenn Melissa B. Jones MSN, APRN, CPNP-AC CICU Nurse Practitioner Children s National Health System Washington, DC No Disclosures Objectives qbriefly describe
Management of a Patient after the Bidirectional Glenn Melissa B. Jones MSN, APRN, CPNP-AC CICU Nurse Practitioner Children s National Health System Washington, DC No Disclosures Objectives qbriefly describe
Cardiorespiratory Interactions:
 Cardiorespiratory Interactions: The Heart - Lung Connection Jon N. Meliones, MD, MS, FCCM Professor of Pediatrics Duke University Medical Director PCVICU Optimizing CRI Cardiorespiratory Economics O2:
Cardiorespiratory Interactions: The Heart - Lung Connection Jon N. Meliones, MD, MS, FCCM Professor of Pediatrics Duke University Medical Director PCVICU Optimizing CRI Cardiorespiratory Economics O2:
Objective 2/9/2012. Blood Gas Analysis In The Univentricular Patient: The Need For A Different Perspective. VENOARTERIAL CO2 GRADIENT
 Blood Gas Analysis In The Univentricular Patient: The Need For A Different Perspective. Gary Grist RN CCP Chief Perfusionist The Children s Mercy Hospitals and Clinics Kansas City, Mo. Objective The participant
Blood Gas Analysis In The Univentricular Patient: The Need For A Different Perspective. Gary Grist RN CCP Chief Perfusionist The Children s Mercy Hospitals and Clinics Kansas City, Mo. Objective The participant
Effects of mechanical ventilation on organ function. Masterclass ICU nurses
 Effects of mechanical ventilation on organ function Masterclass ICU nurses Case Male, 60 - No PMH - L 1.74 m and W 85 kg Pneumococcal pneumonia Stable hemodynamics - No AKI MV in prone position (PEEP 16
Effects of mechanical ventilation on organ function Masterclass ICU nurses Case Male, 60 - No PMH - L 1.74 m and W 85 kg Pneumococcal pneumonia Stable hemodynamics - No AKI MV in prone position (PEEP 16
ino in neonates with cardiac disorders
 ino in neonates with cardiac disorders Duncan Macrae Paediatric Critical Care Terminology PAP Pulmonary artery pressure PVR Pulmonary vascular resistance PHT Pulmonary hypertension - PAP > 25, PVR >3,
ino in neonates with cardiac disorders Duncan Macrae Paediatric Critical Care Terminology PAP Pulmonary artery pressure PVR Pulmonary vascular resistance PHT Pulmonary hypertension - PAP > 25, PVR >3,
CMR EVALUATION OF AORTO- PULMONARY COLLATERALS PRIOR TO FONTAN AND THEIR IMPACT ON EARLY OUTCOME
 XLIII CONGRESSO NAZIONALE SOCIETÀ ITALIANA DI CARDIOLOGIA PEDIATRICA Padova 16-19 Ottobre 2013 L.Ait-Ali, L. Arcieri, V. Pak, R. Moschetti, P. Festa. Istiituto di fisiologia clinica CNR Massa U.O. Cardiologia
XLIII CONGRESSO NAZIONALE SOCIETÀ ITALIANA DI CARDIOLOGIA PEDIATRICA Padova 16-19 Ottobre 2013 L.Ait-Ali, L. Arcieri, V. Pak, R. Moschetti, P. Festa. Istiituto di fisiologia clinica CNR Massa U.O. Cardiologia
Pulmonary Vasodilator Treatments in the ICU Setting
 Pulmonary Vasodilator Treatments in the ICU Setting Lara Shekerdemian Circulation 1979 Ann Thorac Surg 27 Anesth Analg 211 1 Factors in the ICU Management of Pulmonary Hypertension After Cardiopulmonary
Pulmonary Vasodilator Treatments in the ICU Setting Lara Shekerdemian Circulation 1979 Ann Thorac Surg 27 Anesth Analg 211 1 Factors in the ICU Management of Pulmonary Hypertension After Cardiopulmonary
Glenn Shunts Revisited
 Glenn Shunts Revisited What is a Super Glenn Patricia O Brien, MSN, CPNP-AC Nurse Practitioner, Pediatric Cardiology No Disclosures Single Ventricle Anatomy Glenn Shunt Cavopulmonary Anastomosis Anastomosis
Glenn Shunts Revisited What is a Super Glenn Patricia O Brien, MSN, CPNP-AC Nurse Practitioner, Pediatric Cardiology No Disclosures Single Ventricle Anatomy Glenn Shunt Cavopulmonary Anastomosis Anastomosis
Right Heart Catheterization. Franz R. Eberli MD Chief of Cardiology Stadtspital Triemli, Zurich
 Right Heart Catheterization Franz R. Eberli MD Chief of Cardiology Stadtspital Triemli, Zurich Right Heart Catheterization Pressure measurements Oxygen saturation measurements Cardiac output, Vascular
Right Heart Catheterization Franz R. Eberli MD Chief of Cardiology Stadtspital Triemli, Zurich Right Heart Catheterization Pressure measurements Oxygen saturation measurements Cardiac output, Vascular
a. Describe the physiological consequences of intermittent positive pressure ventilation and positive end-expiratory pressure.
 B. 10 Applied Respiratory Physiology a. Describe the physiological consequences of intermittent positive pressure ventilation and positive end-expiratory pressure. Intermittent positive pressure ventilation
B. 10 Applied Respiratory Physiology a. Describe the physiological consequences of intermittent positive pressure ventilation and positive end-expiratory pressure. Intermittent positive pressure ventilation
4/21/2018. The Role of Cardiac Catheterization in Pediatric PVD. The Role(s) of Cath in PVD. Pre Cath Management. Catheterization Mechanics in PVD
 of Cath in PVD. Pre Cath Management. Catheterization Mechanics in PVD") UCSF Pediatric Heart Center Benioff Children s Hospitals Oakland & San Francisco April 19, 2018 The Role of Cardiac Catheterization in Pediatric PVD Phillip Moore MD, MBA The Role(s) of Cath in PVD Diagnosis
UCSF Pediatric Heart Center Benioff Children s Hospitals Oakland & San Francisco April 19, 2018 The Role of Cardiac Catheterization in Pediatric PVD Phillip Moore MD, MBA The Role(s) of Cath in PVD Diagnosis
9/19/2011. Damien Beilman, RRT Adult Clinical Specialist Wesley Medical Center. Epidural Hematoma: Lens Shaped.
 Damien Beilman, RRT Adult Clinical Specialist Wesley Medical Center Epidural Hematoma: Lens Shaped. 1 Epidural Hematoma Subdural Hematoma: Crescent-shaped Subdural Hematoma 2 Cerebral Contusion Cause of
Damien Beilman, RRT Adult Clinical Specialist Wesley Medical Center Epidural Hematoma: Lens Shaped. 1 Epidural Hematoma Subdural Hematoma: Crescent-shaped Subdural Hematoma 2 Cerebral Contusion Cause of
Case scenario V AV ECMO. Dr Pranay Oza
 Case scenario V AV ECMO Dr Pranay Oza Case Summary 53 y/m, k/c/o MVP with myxomatous mitral valve with severe Mitral regurgitation underwent Mitral valve replacement with mini thoracotomy Pump time nearly
Case scenario V AV ECMO Dr Pranay Oza Case Summary 53 y/m, k/c/o MVP with myxomatous mitral valve with severe Mitral regurgitation underwent Mitral valve replacement with mini thoracotomy Pump time nearly
The Vigileo monitor by Edwards Lifesciences supports both the FloTrac Sensor for continuous cardiac output and the Edwards PreSep oximetry catheter
 1 2 The Vigileo monitor by Edwards Lifesciences supports both the FloTrac Sensor for continuous cardiac output and the Edwards PreSep oximetry catheter for continuous central venous oximetry (ScvO2) 3
1 2 The Vigileo monitor by Edwards Lifesciences supports both the FloTrac Sensor for continuous cardiac output and the Edwards PreSep oximetry catheter for continuous central venous oximetry (ScvO2) 3
FUNDAMENTALS OF HEMODYNAMICS, VASOACTIVE DRUGS AND IABP IN THE FAILING HEART
 FUNDAMENTALS OF HEMODYNAMICS, VASOACTIVE DRUGS AND IABP IN THE FAILING HEART CINDY BITHER, MSN, ANP, ANP, AACC, CHFN CHIEF NP, ADV HF PROGRAM MEDSTAR WASHINGTON HOSPITAL CENTER CONFLICTS OF INTEREST NONE
FUNDAMENTALS OF HEMODYNAMICS, VASOACTIVE DRUGS AND IABP IN THE FAILING HEART CINDY BITHER, MSN, ANP, ANP, AACC, CHFN CHIEF NP, ADV HF PROGRAM MEDSTAR WASHINGTON HOSPITAL CENTER CONFLICTS OF INTEREST NONE
Topics to be Covered. Cardiac Measurements. Distribution of Blood Volume. Distribution of Pulmonary Ventilation & Blood Flow
 Topics to be Covered MODULE F HEMODYNAMIC MONITORING Cardiac Output Determinants of Stroke Volume Hemodynamic Measurements Pulmonary Artery Catheterization Control of Blood Pressure Heart Failure Cardiac
Topics to be Covered MODULE F HEMODYNAMIC MONITORING Cardiac Output Determinants of Stroke Volume Hemodynamic Measurements Pulmonary Artery Catheterization Control of Blood Pressure Heart Failure Cardiac
Glenn and Fontan Caths:
 Glenn and Fontan Caths: Pre-operative evaluation and Trouble-shooting Cavo-Pulmonary Shunts Daniel H. Gruenstein, M.D. Director, Pediatric Interventional Cardiology University of Minnesota Children s Hospital,
Glenn and Fontan Caths: Pre-operative evaluation and Trouble-shooting Cavo-Pulmonary Shunts Daniel H. Gruenstein, M.D. Director, Pediatric Interventional Cardiology University of Minnesota Children s Hospital,
PHYSIOLOGY MeQ'S (Morgan) All the following statements related to blood volume are correct except for: 5 A. Blood volume is about 5 litres. B.
 All the following statements related to blood volume are correct except for: 5 A. Blood volume is about 5 litres. B.") PHYSIOLOGY MeQ'S (Morgan) Chapter 5 All the following statements related to capillary Starling's forces are correct except for: 1 A. Hydrostatic pressure at arterial end is greater than at venous end.
PHYSIOLOGY MeQ'S (Morgan) Chapter 5 All the following statements related to capillary Starling's forces are correct except for: 1 A. Hydrostatic pressure at arterial end is greater than at venous end.
The Challenging Pediatric Cardiac Patient. Edmund Jooste
 The Challenging Pediatric Cardiac Patient Edmund Jooste A 5 -year old female with hypoplastic left heart syndrome s/p the Fontan procedure presents for laparoscopic appendectomy for acute appendicitis.
The Challenging Pediatric Cardiac Patient Edmund Jooste A 5 -year old female with hypoplastic left heart syndrome s/p the Fontan procedure presents for laparoscopic appendectomy for acute appendicitis.
2010 년순환기관련학회춘계통합학술대회. Kim, Soo-Jin. Sejong General Hospital, Sejong Cardiovascular center
 2010 년순환기관련학회춘계통합학술대회 세종병원 Sejong General Hospital Debate in Congenital Heart Disease : Pulmonary Vasodilator in Fontan Kim, Soo-Jin Sejong General Hospital, Sejong Cardiovascular center 12 yrs, s/p Fontan
2010 년순환기관련학회춘계통합학술대회 세종병원 Sejong General Hospital Debate in Congenital Heart Disease : Pulmonary Vasodilator in Fontan Kim, Soo-Jin Sejong General Hospital, Sejong Cardiovascular center 12 yrs, s/p Fontan
Chapter 38: Pulmonary Circulation, Pulmonary Edema, Pleural Fluid UNIT VII. Slides by Robert L. Hester, PhD
 UNIT VII Chapter 38: Pulmonary Circulation, Pulmonary Edema, Pleural Fluid Slides by Robert L. Hester, PhD Objectives Describe the pulmonary circulation Describe the pulmonary blood pressures List the
UNIT VII Chapter 38: Pulmonary Circulation, Pulmonary Edema, Pleural Fluid Slides by Robert L. Hester, PhD Objectives Describe the pulmonary circulation Describe the pulmonary blood pressures List the
The Single Ventricle. Karim Rafaat, M.D.
 The Single Ventricle Karim Rafaat, M.D. The title single ventricle includes those lesions designated as both HLHS HRHS HLHS is far more common, and the strategy for palliation of both lesions similar,
The Single Ventricle Karim Rafaat, M.D. The title single ventricle includes those lesions designated as both HLHS HRHS HLHS is far more common, and the strategy for palliation of both lesions similar,
Mechanical Ventilation Following Cardiac Surgery in Children
 44 Current Respiratory Medicine Reviews, 2012, 8, 44-52 Mechanical Ventilation Following Cardiac Surgery in Children Alexandre Tellechea Rotta *,1 and Werther Brunow de Carvalho 2 1 Indiana University
44 Current Respiratory Medicine Reviews, 2012, 8, 44-52 Mechanical Ventilation Following Cardiac Surgery in Children Alexandre Tellechea Rotta *,1 and Werther Brunow de Carvalho 2 1 Indiana University
Nothing to Disclose. Severe Pulmonary Hypertension
 Severe Ronald Pearl, MD, PhD Professor and Chair Department of Anesthesiology Stanford University Rpearl@stanford.edu Nothing to Disclose 65 year old female Elective knee surgery NYHA Class 3 Aortic stenosis
Severe Ronald Pearl, MD, PhD Professor and Chair Department of Anesthesiology Stanford University Rpearl@stanford.edu Nothing to Disclose 65 year old female Elective knee surgery NYHA Class 3 Aortic stenosis
Review Article. Interactive Physiology in Critical Illness : Pulmonary and Cardiovascular Systems. Introduction
 310 Indian Deepak J Physiol Shrivastava Pharmacol 2016; 60(4) : 310 314 Indian J Physiol Pharmacol 2016; 60(4) Review Article Interactive Physiology in Critical Illness : Pulmonary and Cardiovascular Systems
310 Indian Deepak J Physiol Shrivastava Pharmacol 2016; 60(4) : 310 314 Indian J Physiol Pharmacol 2016; 60(4) Review Article Interactive Physiology in Critical Illness : Pulmonary and Cardiovascular Systems
Prof. Dr. Iman Riad Mohamed Abdel Aal
 The Use of New Ultrasound Indices to Evaluate Volume Status and Fluid Responsiveness in Septic Shock Patients Thesis Submitted for partial fulfillment of MD degree in Anesthesiology, Surgical Intensive
The Use of New Ultrasound Indices to Evaluate Volume Status and Fluid Responsiveness in Septic Shock Patients Thesis Submitted for partial fulfillment of MD degree in Anesthesiology, Surgical Intensive
Heart Transplantation for Patients with a Fontan Procedure
 Heart Transplantation for Patients with a Fontan Procedure Kirk R. Kanter MD Professor of Surgery Pediatric Cardiac Surgery Emory University School of Medicine Children s Healthcare of Atlanta Atlanta,
Heart Transplantation for Patients with a Fontan Procedure Kirk R. Kanter MD Professor of Surgery Pediatric Cardiac Surgery Emory University School of Medicine Children s Healthcare of Atlanta Atlanta,
Ventricular-Pulmonary Vascular Coupling after the Total Cavopulmonary Anastomosis (Fontan)
") Ventricular-Pulmonary Vascular Coupling after the Total Cavopulmonary Anastomosis (Fontan) 6th International Neonatal & Childhood Pulmonary Vascular Disease Conference Fontan Physiology Single ventricular
Ventricular-Pulmonary Vascular Coupling after the Total Cavopulmonary Anastomosis (Fontan) 6th International Neonatal & Childhood Pulmonary Vascular Disease Conference Fontan Physiology Single ventricular
Airway pressure release ventilation. Airway pressure release ventilation improves pulmonary blood flow in infants after cardiac surgery*
 Airway pressure release ventilation improves pulmonary blood flow in infants after cardiac surgery* Mark A. Walsh, MD; Michele Merat, MD; Gustavo La Rotta, MD; Pretha Joshi, MD; Vinay Joshi, MD; Tuyen
Airway pressure release ventilation improves pulmonary blood flow in infants after cardiac surgery* Mark A. Walsh, MD; Michele Merat, MD; Gustavo La Rotta, MD; Pretha Joshi, MD; Vinay Joshi, MD; Tuyen
A practical method of measuring oxygen consumption in children with complex mixing circulations by the use of thermodilution cardiac output studies
 A practical method of measuring oxygen consumption in children with complex mixing circulations by the use of thermodilution cardiac output studies Daryl I. Schantz, MD, and Robert P. Chen, MD Objective:
A practical method of measuring oxygen consumption in children with complex mixing circulations by the use of thermodilution cardiac output studies Daryl I. Schantz, MD, and Robert P. Chen, MD Objective:
Diastolic Heart Failure
 Chronic Heart Failure Prevalence overall = 2-3 % Diastolic Heart Failure Patrick Wouters University Hospital Ghent Belgium (Heart Failure + Asymptomatic Ventricular Dysfunction) Prevalence > 70 y = 10-20
Chronic Heart Failure Prevalence overall = 2-3 % Diastolic Heart Failure Patrick Wouters University Hospital Ghent Belgium (Heart Failure + Asymptomatic Ventricular Dysfunction) Prevalence > 70 y = 10-20
Is there an Optimal Mode of Ventilation Following Paediatric Cardiac Surgery? Dr Steve Ponde Busamed Modderfontein Hospital
 Is there an Optimal Mode of Ventilation Following Paediatric Cardiac Surgery? Dr Steve Ponde Busamed Modderfontein Hospital There have been many advances in the perioperative care of adults and children
Is there an Optimal Mode of Ventilation Following Paediatric Cardiac Surgery? Dr Steve Ponde Busamed Modderfontein Hospital There have been many advances in the perioperative care of adults and children
Cath Lab Essentials: Basic Hemodynamics for the Cath Lab and ICU
 Cath Lab Essentials: Basic Hemodynamics for the Cath Lab and ICU Ailin Barseghian El-Farra, MD, FACC Assistant Professor, Interventional Cardiology University of California, Irvine Department of Cardiology
Cath Lab Essentials: Basic Hemodynamics for the Cath Lab and ICU Ailin Barseghian El-Farra, MD, FACC Assistant Professor, Interventional Cardiology University of California, Irvine Department of Cardiology
Heart Transplantation in Patients with Superior Vena Cava to Pulmonary Artery Anastomosis: A Single-Institution Experience
 Korean J Thorac Cardiovasc Surg 2018;51:167-171 ISSN: 2233-601X (Print) ISSN: 2093-6516 (Online) CLINICAL RESEARCH https://doi.org/10.5090/kjtcs.2018.51.3.167 Heart Transplantation in Patients with Superior
Korean J Thorac Cardiovasc Surg 2018;51:167-171 ISSN: 2233-601X (Print) ISSN: 2093-6516 (Online) CLINICAL RESEARCH https://doi.org/10.5090/kjtcs.2018.51.3.167 Heart Transplantation in Patients with Superior
Brief View of Calculation and Measurement of Cardiac Hemodynamics
 Cronicon OPEN ACCESS EC CARDIOLOGY Review Article Brief View of Calculation and Measurement of Cardiac Hemodynamics Samah Alasrawi* Pediatric Cardiologist, Al Jalila Children Heart Center, Dubai, UAE *
Cronicon OPEN ACCESS EC CARDIOLOGY Review Article Brief View of Calculation and Measurement of Cardiac Hemodynamics Samah Alasrawi* Pediatric Cardiologist, Al Jalila Children Heart Center, Dubai, UAE *
Introduction. Invasive Hemodynamic Monitoring. Determinants of Cardiovascular Function. Cardiovascular System. Hemodynamic Monitoring
 Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
-12. -Ensherah Mokheemer - ABDULLAH ZREQAT. -Faisal Mohammad. 1 P a g e
 -12 -Ensherah Mokheemer - ABDULLAH ZREQAT -Faisal Mohammad 1 P a g e In the previous lecture we talked about: - cardiac index: we use the cardiac index to compare the cardiac output between different individuals,
-12 -Ensherah Mokheemer - ABDULLAH ZREQAT -Faisal Mohammad 1 P a g e In the previous lecture we talked about: - cardiac index: we use the cardiac index to compare the cardiac output between different individuals,
Disclosures. Objectives 6/16/2016. A Look at the Other Side: Focus on the Right Ventricle and Pulmonary Hypertension
 A Look at the Other Side: Focus on the Right Ventricle and Pulmonary Hypertension Susan P. D Anna MSN, APN-BC, CHFN June 24, 2016 Disclosures Objectives Differentiate structure and function of RV and LV
A Look at the Other Side: Focus on the Right Ventricle and Pulmonary Hypertension Susan P. D Anna MSN, APN-BC, CHFN June 24, 2016 Disclosures Objectives Differentiate structure and function of RV and LV
Critical Care Monitoring. Assessing the Adequacy of Tissue Oxygenation. Tissue Oxygenation - Step 1. Tissue Oxygenation
 Critical Care Monitoring 1 Assessing the Adequacy of Tissue oxygenation is the end-product of many complex steps 2 - Step 1 Oxygen must be made available to alveoli 3 1 - Step 2 Oxygen must cross the alveolarcapillary
Critical Care Monitoring 1 Assessing the Adequacy of Tissue oxygenation is the end-product of many complex steps 2 - Step 1 Oxygen must be made available to alveoli 3 1 - Step 2 Oxygen must cross the alveolarcapillary
Shock, Monitoring Invasive Vs. Non Invasive
 Shock, Monitoring Invasive Vs. Non Invasive Paula Ferrada MD Assistant Professor Trauma, Critical Care and Emergency Surgery Virginia Commonwealth University Shock Fluid Pressors Ionotrope Intervention
Shock, Monitoring Invasive Vs. Non Invasive Paula Ferrada MD Assistant Professor Trauma, Critical Care and Emergency Surgery Virginia Commonwealth University Shock Fluid Pressors Ionotrope Intervention
Constrictive/Restrictive Cardiomyopathies: Diagnosis and Management Update; Radiation Induced Heart Disease. Alexander (Sandy) Dick, MD
 Dick, MD") Constrictive/Restrictive Cardiomyopathies: Diagnosis and Management Update; Radiation Induced Heart Disease Alexander (Sandy) Dick, MD Outline Pericardial Constriction Diagnosis: Imaging, Hemodynamics
Constrictive/Restrictive Cardiomyopathies: Diagnosis and Management Update; Radiation Induced Heart Disease Alexander (Sandy) Dick, MD Outline Pericardial Constriction Diagnosis: Imaging, Hemodynamics
Outline. Congenital Heart Disease. Special Considerations for Special Populations: Congenital Heart Disease
 Special Considerations for Special Populations: Congenital Heart Disease Valerie Bosco, FNP, EdD Alison Knauth Meadows, MD, PhD University of California San Francisco Adult Congenital Heart Program Outline
Special Considerations for Special Populations: Congenital Heart Disease Valerie Bosco, FNP, EdD Alison Knauth Meadows, MD, PhD University of California San Francisco Adult Congenital Heart Program Outline
Deok Young Choi, Gil Hospital, Gachon University NEONATES WITH EBSTEIN S ANOMALY: PROBLEMS AND SOLUTION
 Deok Young Choi, Gil Hospital, Gachon University NEONATES WITH EBSTEIN S ANOMALY: PROBLEMS AND SOLUTION Carpentier classification Chauvaud S, Carpentier A. Multimedia Manual of Cardiothoracic Surgery 2007
Deok Young Choi, Gil Hospital, Gachon University NEONATES WITH EBSTEIN S ANOMALY: PROBLEMS AND SOLUTION Carpentier classification Chauvaud S, Carpentier A. Multimedia Manual of Cardiothoracic Surgery 2007
Right Ventricular Failure: Prediction, Prevention and Treatment
 Right Ventricular Failure: Prediction, Prevention and Treatment 3 rd European Training Symposium for Heart Failure Cardiologists and Cardiac Surgeons University Hospital Bern June 24-25, 2016 Disclosures:
Right Ventricular Failure: Prediction, Prevention and Treatment 3 rd European Training Symposium for Heart Failure Cardiologists and Cardiac Surgeons University Hospital Bern June 24-25, 2016 Disclosures:
Evaluation of Left Ventricular Diastolic Dysfunction by Doppler and 2D Speckle-tracking Imaging in Patients with Primary Pulmonary Hypertension
 ESC Congress 2011.No 85975 Evaluation of Left Ventricular Diastolic Dysfunction by Doppler and 2D Speckle-tracking Imaging in Patients with Primary Pulmonary Hypertension Second Department of Internal
ESC Congress 2011.No 85975 Evaluation of Left Ventricular Diastolic Dysfunction by Doppler and 2D Speckle-tracking Imaging in Patients with Primary Pulmonary Hypertension Second Department of Internal
CATHETERIZATION PROTOCOL Prepared by Matthew Crystal ( )
") CATHETERIZATION PROTOCOL Prepared by Matthew Crystal (2006-06-21) Cath Procedure Diagnosis: Hospitalization Requirement Blood on hold Cath Lab Fontan Yes (CCU after completion) Yes (as per OR protocols)
CATHETERIZATION PROTOCOL Prepared by Matthew Crystal (2006-06-21) Cath Procedure Diagnosis: Hospitalization Requirement Blood on hold Cath Lab Fontan Yes (CCU after completion) Yes (as per OR protocols)
Pulmonary Hypertension Perioperative Management
 Pulmonary Hypertension Perioperative Management Bruce J Leone, MD Professor of Anesthesiology Chief, Neuroanesthesiology Vice Chair for Academic Affairs Mayo Clinic Jacksonville, Florida Introduction Definition
Pulmonary Hypertension Perioperative Management Bruce J Leone, MD Professor of Anesthesiology Chief, Neuroanesthesiology Vice Chair for Academic Affairs Mayo Clinic Jacksonville, Florida Introduction Definition
Pulmonary Hypertension Due to Left Heart Disease
 ACC Middle East Conference 2018 Pulmonary Hypertension Due to Left Heart Disease Ammar Chaudhary, MBChB, FRCPC Advanced Heart Failure & Transplantation King Faisal Specialist Hospital and Research Center
ACC Middle East Conference 2018 Pulmonary Hypertension Due to Left Heart Disease Ammar Chaudhary, MBChB, FRCPC Advanced Heart Failure & Transplantation King Faisal Specialist Hospital and Research Center
M5 BOARD REVIEW. Q s. Q s. Q s. Q s. Q s. Equations. Be Brilliant Today. Respiratory ( ) Alveolar Gas Equation. Dead Space (Bohr Equation)
 Alveolar Gas Equation. Dead Space (Bohr Equation)") Be Brilliant Today Respiratory Alveolar Gas Equation Dead Space (Bohr Equation) PA O2 FI O2 ( P ATM P H2 O ) Pa CO2 / RQ V D V T P a P ECO CO2 2 P a CO 2 PA O2 Alveolar partial pressure of oxygen P a CO
Be Brilliant Today Respiratory Alveolar Gas Equation Dead Space (Bohr Equation) PA O2 FI O2 ( P ATM P H2 O ) Pa CO2 / RQ V D V T P a P ECO CO2 2 P a CO 2 PA O2 Alveolar partial pressure of oxygen P a CO
Management of refractory ARDS. Saurabh maji
 Management of refractory ARDS Saurabh maji Refractory hypoxemia as PaO2/FIO2 is less than 100 mm Hg, inability to keep plateau pressure below 30 cm H2O despite a VT of 4 ml/kg development of barotrauma
Management of refractory ARDS Saurabh maji Refractory hypoxemia as PaO2/FIO2 is less than 100 mm Hg, inability to keep plateau pressure below 30 cm H2O despite a VT of 4 ml/kg development of barotrauma
Radboud University Nijmegen Medical Centre Why measure cardiac output in critically ill children?
 Radboud University Nijmegen Medical Centre Why measure cardiac output in critically ill children? J. Lemson Anesthesiologist/(pediatric)intensivist Case; Girl 2 years, 12 kg, severe meningococcal septic
Radboud University Nijmegen Medical Centre Why measure cardiac output in critically ill children? J. Lemson Anesthesiologist/(pediatric)intensivist Case; Girl 2 years, 12 kg, severe meningococcal septic
Revision of 10/27/2017 Form #280 Page 1 of 12 PVDOMICS STUDY Clinical Center Right Heart Catheterization (RHC) Results Form #280
 Results Form #280") Revision of 10/27/2017 Form #280 Page 1 of 12 PVDOMICS STUDY Clinical Center Right Heart Catheterization (RHC) Results Form #280 Instructions: Review PVDOMICS MOP Chapter 100 prior to completing right
Revision of 10/27/2017 Form #280 Page 1 of 12 PVDOMICS STUDY Clinical Center Right Heart Catheterization (RHC) Results Form #280 Instructions: Review PVDOMICS MOP Chapter 100 prior to completing right
Chapter 9, Part 2. Cardiocirculatory Adjustments to Exercise
 Chapter 9, Part 2 Cardiocirculatory Adjustments to Exercise Electrical Activity of the Heart Contraction of the heart depends on electrical stimulation of the myocardium Impulse is initiated in the right
Chapter 9, Part 2 Cardiocirculatory Adjustments to Exercise Electrical Activity of the Heart Contraction of the heart depends on electrical stimulation of the myocardium Impulse is initiated in the right
Mechanical circulatory support in cardiogenic shock The Cardiologist s view ACCA Masterclass 2017
 Mechanical circulatory support in cardiogenic shock The Cardiologist s view ACCA Masterclass 2017 Pascal Vranckx MD, PhD. Medical director Cardiac Critical Care Services Hartcentrum Hasselt Belgium Disclosure
Mechanical circulatory support in cardiogenic shock The Cardiologist s view ACCA Masterclass 2017 Pascal Vranckx MD, PhD. Medical director Cardiac Critical Care Services Hartcentrum Hasselt Belgium Disclosure
Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor
 Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
Cardiac Emergencies in Infants. Michael Luceri, DO
 Cardiac Emergencies in Infants Michael Luceri, DO October 7, 2017 I have no financial obligations or conflicts of interest to disclose. Objectives Understand the scope of congenital heart disease Recognize
Cardiac Emergencies in Infants Michael Luceri, DO October 7, 2017 I have no financial obligations or conflicts of interest to disclose. Objectives Understand the scope of congenital heart disease Recognize
Left atrial function. Aliakbar Arvandi MD
 In the clinic Left atrial function Abstract The left atrium (LA) is a left posterior cardiac chamber which is located adjacent to the esophagus. It is separated from the right atrium by the inter-atrial
In the clinic Left atrial function Abstract The left atrium (LA) is a left posterior cardiac chamber which is located adjacent to the esophagus. It is separated from the right atrium by the inter-atrial
Non-Invasive Bed-Side Assessment of Pulmonary Vascular Resistance in Critically Ill Pediatric Patients with Acute Respiratory Distress Syndrome
 Aim of the Work This study aimed to evaluate the degree of pulmonary hypertension as well as alterations in the pulmonary vascular resistance in critically ill children with ARDS using bed- side echocardiography.
Aim of the Work This study aimed to evaluate the degree of pulmonary hypertension as well as alterations in the pulmonary vascular resistance in critically ill children with ARDS using bed- side echocardiography.
7/4/2015. diffuse lung injury resulting in noncardiogenic pulmonary edema due to increase in capillary permeability
 Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Identify the 5 criteria for the diagnosis of ARDS. Discuss the common etiologies
Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Identify the 5 criteria for the diagnosis of ARDS. Discuss the common etiologies
ARDS: an update 6 th March A. Hakeem Al Hashim, MD, FRCP SQUH
 ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
Total cavopulmonary connection (TCPC) is a palliative
 is a palliative") Effects of Exercise and Respiration on Blood Flow in Total Cavopulmonary Connection A Real-Time Magnetic Resonance Flow Study V.E. Hjortdal, MD, DMSc; K. Emmertsen, MD, DMSc; E. Stenbøg, MD, PhD; T. Fründ,
Effects of Exercise and Respiration on Blood Flow in Total Cavopulmonary Connection A Real-Time Magnetic Resonance Flow Study V.E. Hjortdal, MD, DMSc; K. Emmertsen, MD, DMSc; E. Stenbøg, MD, PhD; T. Fründ,
Principles of Biomedical Systems & Devices. Lecture 8: Cardiovascular Dynamics Dr. Maria Tahamont
 Principles of Biomedical Systems & Devices Lecture 8: Cardiovascular Dynamics Dr. Maria Tahamont Review of Cardiac Anatomy Four chambers Two atria-receive blood from the vena cave and pulmonary veins Two
Principles of Biomedical Systems & Devices Lecture 8: Cardiovascular Dynamics Dr. Maria Tahamont Review of Cardiac Anatomy Four chambers Two atria-receive blood from the vena cave and pulmonary veins Two
 Derivation and Validation of a Novel Right-Sided Heart Failure Model After Implantation of Continuous Flow Left Ventricular Assist Devices: the EUROMACS-RHF Risk Score Osama I.I. Soliman, MD, PhD, FACC,
Derivation and Validation of a Novel Right-Sided Heart Failure Model After Implantation of Continuous Flow Left Ventricular Assist Devices: the EUROMACS-RHF Risk Score Osama I.I. Soliman, MD, PhD, FACC,
Evolutionary origins of the right ventricle. S Magder Department of Critical Care, McGill University Health Centre
 Evolutionary origins of the right ventricle S Magder Department of Critical Care, McGill University Health Centre Fully separated four chamber heart only evolved in birds and mammals What are the evolutionary
Evolutionary origins of the right ventricle S Magder Department of Critical Care, McGill University Health Centre Fully separated four chamber heart only evolved in birds and mammals What are the evolutionary
Assessing the Impact on the Right Ventricle
 Advances in Tricuspid Regurgitation Congress of the European Society of Cardiology (ESC) Munich, August 25-29, 2012 Assessing the Impact on the Right Ventricle Stephan Rosenkranz, MD Clinic III for Internal
Advances in Tricuspid Regurgitation Congress of the European Society of Cardiology (ESC) Munich, August 25-29, 2012 Assessing the Impact on the Right Ventricle Stephan Rosenkranz, MD Clinic III for Internal
First-stage palliation for hypoplastic left heart syndrome
 Comparison of Norwood Shunt Types: Do the Outcomes Differ 6 Years Later? Eric M. Graham, MD, Sinai C. Zyblewski, MD, Jacob W. Phillips, MD, Girish S. Shirali, MBBS, Scott M. Bradley, MD, Geoffery A. Forbus,
Comparison of Norwood Shunt Types: Do the Outcomes Differ 6 Years Later? Eric M. Graham, MD, Sinai C. Zyblewski, MD, Jacob W. Phillips, MD, Girish S. Shirali, MBBS, Scott M. Bradley, MD, Geoffery A. Forbus,
Disclosures. Objectives. RV vs LV. Structure and Function 9/25/2016. A Look at the Other Side: Focus on the Right Ventricle and Pulmonary Hypertension
 Disclosures A Look at the Other Side: Focus on the Right Ventricle and Pulmonary Hypertension No financial relationships Susan P. D Anna MSN, APN BC, CHFN September 29, 2016 Objectives RV vs LV Differentiate
Disclosures A Look at the Other Side: Focus on the Right Ventricle and Pulmonary Hypertension No financial relationships Susan P. D Anna MSN, APN BC, CHFN September 29, 2016 Objectives RV vs LV Differentiate
NIV use in ED. Dr. Khalfan AL Amrani Emergency Resuscitation Symposium 2 nd May 2016 SQUH
 NIV use in ED Dr. Khalfan AL Amrani Emergency Resuscitation Symposium 2 nd May 2016 SQUH Outline History & Introduction Overview of NIV application Review of proven uses of NIV History of Ventilation 1940
NIV use in ED Dr. Khalfan AL Amrani Emergency Resuscitation Symposium 2 nd May 2016 SQUH Outline History & Introduction Overview of NIV application Review of proven uses of NIV History of Ventilation 1940
Καθετηριασμός δεξιάς κοιλίας. Σ. Χατζημιλτιάδης Καθηγητής Καρδιολογίας ΑΠΘ
 Καθετηριασμός δεξιάς κοιλίας Σ. Χατζημιλτιάδης Καθηγητής Καρδιολογίας ΑΠΘ The increasing interest in pulmonary arterial hypertension (PAH), the increasing interest in implantation of LVADs, and the evolution
Καθετηριασμός δεξιάς κοιλίας Σ. Χατζημιλτιάδης Καθηγητής Καρδιολογίας ΑΠΘ The increasing interest in pulmonary arterial hypertension (PAH), the increasing interest in implantation of LVADs, and the evolution
Right Ventricular Failure and Pulmonary Hypertension 2011
 Right Ventricular Failure and Pulmonary Hypertension 2011 George G. Sokos, DO FACC Assistant Professor of Medicine, Temple University Director, Advanced Heart Failure and Cardiac Transplant Fellowship
Right Ventricular Failure and Pulmonary Hypertension 2011 George G. Sokos, DO FACC Assistant Professor of Medicine, Temple University Director, Advanced Heart Failure and Cardiac Transplant Fellowship
On-Pump vs. Off-Pump CABG: The Controversy Continues. Miguel Sousa Uva Immediate Past President European Association for Cardiothoracic Surgery
 On-Pump vs. Off-Pump CABG: The Controversy Continues Miguel Sousa Uva Immediate Past President European Association for Cardiothoracic Surgery On-pump vs. Off-Pump CABG: The Controversy Continues Conflict
On-Pump vs. Off-Pump CABG: The Controversy Continues Miguel Sousa Uva Immediate Past President European Association for Cardiothoracic Surgery On-pump vs. Off-Pump CABG: The Controversy Continues Conflict
Appendix II: ECHOCARDIOGRAPHY ANALYSIS
 Appendix II: ECHOCARDIOGRAPHY ANALYSIS Two-Dimensional (2D) imaging was performed using the Vivid 7 Advantage cardiovascular ultrasound system (GE Medical Systems, Milwaukee) with a frame rate of 400 frames
Appendix II: ECHOCARDIOGRAPHY ANALYSIS Two-Dimensional (2D) imaging was performed using the Vivid 7 Advantage cardiovascular ultrasound system (GE Medical Systems, Milwaukee) with a frame rate of 400 frames
Admission of patient CVICU and hemodynamic monitoring
 Admission of patient CVICU and hemodynamic monitoring Prepared by: Rami AL-Khatib King Fahad Medical City Pi Prince Salman Heart tcentre CVICU-RN Admission patient to CVICU Introduction All the patients
Admission of patient CVICU and hemodynamic monitoring Prepared by: Rami AL-Khatib King Fahad Medical City Pi Prince Salman Heart tcentre CVICU-RN Admission patient to CVICU Introduction All the patients
가천의대길병원소아심장과최덕영 PA C IVS THE EVALUATION AND PRINCIPLES OF TREATMENT STRATEGY
 가천의대길병원소아심장과최덕영 PA C IVS THE EVALUATION AND PRINCIPLES OF TREATMENT STRATEGY PA c IVS (not only pulmonary valve disease) Edwards JE. Pathologic Alteration of the right heart. In: Konstam MA, Isner M, eds.
가천의대길병원소아심장과최덕영 PA C IVS THE EVALUATION AND PRINCIPLES OF TREATMENT STRATEGY PA c IVS (not only pulmonary valve disease) Edwards JE. Pathologic Alteration of the right heart. In: Konstam MA, Isner M, eds.
Impedance Cardiography (ICG) Application of ICG in Intensive Care and Emergency
 Application of ICG in Intensive Care and Emergency") Impedance Cardiography (ICG) Application of ICG in Intensive Care and Emergency Aim of haemodynamic monitoring in ICU and ED Detection and therapy of insufficient organ perfusion Answers to common cardiovascular
Impedance Cardiography (ICG) Application of ICG in Intensive Care and Emergency Aim of haemodynamic monitoring in ICU and ED Detection and therapy of insufficient organ perfusion Answers to common cardiovascular
Παθοφυσιολογια αποτυχίας αποδέσμευσης. Καρδιαγγειακό
 Παθοφυσιολογια αποτυχίας αποδέσμευσης Καρδιαγγειακό Θεόδωρος Βασιλακόπουλος Καθηγητής Πνευμονολογίας-Εντατικής Θεραπείας Εθνικό & Καποδιστριακό Πανεπιστήμιο Αθηνών Νοσοκομείο «ο Ευαγγελισμός» Adjunct Professor,
Παθοφυσιολογια αποτυχίας αποδέσμευσης Καρδιαγγειακό Θεόδωρος Βασιλακόπουλος Καθηγητής Πνευμονολογίας-Εντατικής Θεραπείας Εθνικό & Καποδιστριακό Πανεπιστήμιο Αθηνών Νοσοκομείο «ο Ευαγγελισμός» Adjunct Professor,
Squeeze, Squeeze, Squeeze: The Importance of Right Ventricular Function and PH
 Squeeze, Squeeze, Squeeze: The Importance of Right Ventricular Function and PH Javier Jimenez MD PhD FACC Director, Advanced Heart Failure and Pulmonary Hypertension Miami Cardiac & Vascular Institute
Squeeze, Squeeze, Squeeze: The Importance of Right Ventricular Function and PH Javier Jimenez MD PhD FACC Director, Advanced Heart Failure and Pulmonary Hypertension Miami Cardiac & Vascular Institute
Mechanical Ventilation. Assessing the Adequacy of Tissue Oxygenation. Tissue Oxygenation - Step 1. Tissue Oxygenation
 1 Mechanical Ventilation Assessing the Adequacy of 2 Tissue oxygenation is the end-product of many complex steps - Step 1 3 Oxygen must be made available to alveoli 1 - Step 2 4 Oxygen must cross the alveolarcapillary
1 Mechanical Ventilation Assessing the Adequacy of 2 Tissue oxygenation is the end-product of many complex steps - Step 1 3 Oxygen must be made available to alveoli 1 - Step 2 4 Oxygen must cross the alveolarcapillary
Ann Vasc Dis Vol. 6, No. 3; 2013; pp Online August 12, Annals of Vascular Diseases doi: /avd.oa Original Article
 Ann Vasc Dis Vol. 6, No. 3; 2013; pp 578 582 Online August 12, 2013 2013 Annals of Vascular Diseases doi:10.3400/avd.oa.13-00056 Original Article Respiratory and Hemodynamic Changes in Patients with Chronic
Ann Vasc Dis Vol. 6, No. 3; 2013; pp 578 582 Online August 12, 2013 2013 Annals of Vascular Diseases doi:10.3400/avd.oa.13-00056 Original Article Respiratory and Hemodynamic Changes in Patients with Chronic
The Who, How and When of Advanced Heart Failure Therapies. Disclosures. What is Advanced Heart Failure?
 The Who, How and When of Advanced Heart Failure Therapies 9 th Annual Dartmouth Conference on Advances in Heart Failure Therapies Dartmouth-Hitchcock Medical Center Lebanon, NH May 20, 2013 Joseph G. Rogers,
The Who, How and When of Advanced Heart Failure Therapies 9 th Annual Dartmouth Conference on Advances in Heart Failure Therapies Dartmouth-Hitchcock Medical Center Lebanon, NH May 20, 2013 Joseph G. Rogers,
Impedance Cardiography (ICG) Application of ICG for Hypertension Management
 Application of ICG for Hypertension Management") Application of ICG for Hypertension Management 1mA @ 100 khz Impedance Cardiography (ICG) Non-invasive Beat-to-beat Hemodynamic Monitoring Diastole Systole Aortic valve is closed No blood flow in the aorta
Application of ICG for Hypertension Management 1mA @ 100 khz Impedance Cardiography (ICG) Non-invasive Beat-to-beat Hemodynamic Monitoring Diastole Systole Aortic valve is closed No blood flow in the aorta
Exam KEY. NROSCI/BIOSC 1070 and MSNBIO 2070 Exam # 2 October 23, 2015 Total POINTS: % of grade in class
 NROSCI/BIOSC 1070 and MSNBIO 2070 Exam # 2 October 23, 2015 Total POINTS: 100 20% of grade in class 1) Arterial and venous blood samples are taken, and other physiological measures are obtained, from a
NROSCI/BIOSC 1070 and MSNBIO 2070 Exam # 2 October 23, 2015 Total POINTS: 100 20% of grade in class 1) Arterial and venous blood samples are taken, and other physiological measures are obtained, from a
Disclosures. ICU Management of Advanced Lung Disease 5/9/2015. No Disclosures. All pictures from commercial sources
 Disclosures ICU Management of Advanced Lung Disease No Disclosures All pictures from commercial sources Lundy J. Campbell, MD UCSF Department of Anesthesia and Perioperative Care Division of Critical Care
Disclosures ICU Management of Advanced Lung Disease No Disclosures All pictures from commercial sources Lundy J. Campbell, MD UCSF Department of Anesthesia and Perioperative Care Division of Critical Care
Respiratory Physiology Part II. Bio 219 Napa Valley College Dr. Adam Ross
 Respiratory Physiology Part II Bio 219 Napa Valley College Dr. Adam Ross Gas exchange Gas exchange in the lungs (to capillaries) occurs by diffusion across respiratory membrane due to differences in partial
Respiratory Physiology Part II Bio 219 Napa Valley College Dr. Adam Ross Gas exchange Gas exchange in the lungs (to capillaries) occurs by diffusion across respiratory membrane due to differences in partial
Weeks 1-3:Cardiovascular
 Weeks 1-3:Cardiovascular Cardiac Output The total volume of blood ejected from the ventricles in one minute is known as the cardiac output. Heart Rate (HR) X Stroke Volume (SV) = Cardiac Output Normal
Weeks 1-3:Cardiovascular Cardiac Output The total volume of blood ejected from the ventricles in one minute is known as the cardiac output. Heart Rate (HR) X Stroke Volume (SV) = Cardiac Output Normal
Surgical Thrombectomy for PE: Is it Making a Comeback
 Surgical Thrombectomy for PE: Is it Making a Comeback Prashanth Vallabhajosyula, MD MS The University of Pennsylvania Health System Philadelphia, PA Case - 84 year old female presents with submassive right
Surgical Thrombectomy for PE: Is it Making a Comeback Prashanth Vallabhajosyula, MD MS The University of Pennsylvania Health System Philadelphia, PA Case - 84 year old female presents with submassive right
Cardiovascular Physiology. Heart Physiology. Introduction. The heart. Electrophysiology of the heart
 Cardiovascular Physiology Heart Physiology Introduction The cardiovascular system consists of the heart and two vascular systems, the systemic and pulmonary circulations. The heart pumps blood through
Cardiovascular Physiology Heart Physiology Introduction The cardiovascular system consists of the heart and two vascular systems, the systemic and pulmonary circulations. The heart pumps blood through
Disclaimer. Improving MET-based patient care using treatment algorithms. Michael R. Pinsky, MD, Dr hc. Different Environments Demand Different Rules
 Michael R. Pinsky, MD - June 29, 26 Improving MET-based patient care using Michael R. Pinsky, MD, Dr hc Department of Critical Care Medicine University of Pittsburgh Disclaimer Michael R. Pinsky, MD is
Michael R. Pinsky, MD - June 29, 26 Improving MET-based patient care using Michael R. Pinsky, MD, Dr hc Department of Critical Care Medicine University of Pittsburgh Disclaimer Michael R. Pinsky, MD is
Outline. Echocardiographic Assessment of Pericardial Effusion/Tamponade: The Essentials
 Echocardiographic Assessment of Pericardial Effusion/Tamponade: The Essentials John R Schairer DO FACC Henry Ford Heart and Vascular Institute No Disclosures Outline Normal Anatomy and Physiology Pathophysiology
Echocardiographic Assessment of Pericardial Effusion/Tamponade: The Essentials John R Schairer DO FACC Henry Ford Heart and Vascular Institute No Disclosures Outline Normal Anatomy and Physiology Pathophysiology
RV dysfunction and failure PATHOPHYSIOLOGY. Adam Torbicki MD, Dept Chest Medicine Institute of Tuberculosis and Lung Diseases Warszawa, Poland
 RV dysfunction and failure PATHOPHYSIOLOGY Adam Torbicki MD, Dept Chest Medicine Institute of Tuberculosis and Lung Diseases Warszawa, Poland Normal Right Ventricle (RV) Thinner wall Weaker myocytes Differences
RV dysfunction and failure PATHOPHYSIOLOGY Adam Torbicki MD, Dept Chest Medicine Institute of Tuberculosis and Lung Diseases Warszawa, Poland Normal Right Ventricle (RV) Thinner wall Weaker myocytes Differences
Complications of VAD therapy - RV failure
 Complications of VAD therapy - RV failure Nana Afari-Armah, MD Advanced heart failure and transplant cardiology Temple University Hospital 3/24/18 Goals Understand the role of the right ventricle in LVAD
Complications of VAD therapy - RV failure Nana Afari-Armah, MD Advanced heart failure and transplant cardiology Temple University Hospital 3/24/18 Goals Understand the role of the right ventricle in LVAD
What is the Definition of Small Systemic Ventricle. Hong Ryang Kil, MD Department of Pediatrics, College of Medicine, Chungnam National University
 What is the Definition of Small Systemic Ventricle Hong Ryang Kil, MD Department of Pediatrics, College of Medicine, Chungnam National University Contents Introduction Aortic valve stenosis Aortic coarctation
What is the Definition of Small Systemic Ventricle Hong Ryang Kil, MD Department of Pediatrics, College of Medicine, Chungnam National University Contents Introduction Aortic valve stenosis Aortic coarctation
Ventricular Interactions in the Normal and Failing Heart
 Ventricular Interactions in the Normal and Failing Heart Congenital Cardiac Anesthesia Society 2015 Pressure-volume relations Matched Left ventricle to low hydraulic impedance Maximal stroke work limited
Ventricular Interactions in the Normal and Failing Heart Congenital Cardiac Anesthesia Society 2015 Pressure-volume relations Matched Left ventricle to low hydraulic impedance Maximal stroke work limited
Part 3a. Physiology: the cardiovascular system
 Part 3a Physiology: the cardiovascular system 105 Part 3a Intravascular pressure waveforms and the ECG waveform With the exception of systemic arterial pressure, intravascular pressure waveforms can be
Part 3a Physiology: the cardiovascular system 105 Part 3a Intravascular pressure waveforms and the ECG waveform With the exception of systemic arterial pressure, intravascular pressure waveforms can be
Surgical Management of Failing Fontan Operation
 Surgical Management of Failing Fontan Operation Jeong-Jun Park Dept. of Thoracic & cardiovascular Surgery Asan Medical Center, Ulsan University Fontan operation 1995-2001, 123 procedures in 71 pts EJCTS
Surgical Management of Failing Fontan Operation Jeong-Jun Park Dept. of Thoracic & cardiovascular Surgery Asan Medical Center, Ulsan University Fontan operation 1995-2001, 123 procedures in 71 pts EJCTS
ARDS Assisted ventilation and prone position. ICU Fellowship Training Radboudumc
 ARDS Assisted ventilation and prone position ICU Fellowship Training Radboudumc Fig. 1 Physiological mechanisms controlling respiratory drive and clinical consequences of inappropriate respiratory drive
ARDS Assisted ventilation and prone position ICU Fellowship Training Radboudumc Fig. 1 Physiological mechanisms controlling respiratory drive and clinical consequences of inappropriate respiratory drive
A new diagnostic algorithm for assessment of patients with single ventricle before a Fontan operation
 A new diagnostic algorithm for assessment of patients with single ventricle before a Fontan operation Ashwin Prakash, MD, Muhammad A. Khan, MD, Rose Hardy, BA, Alejandro J. Torres, MD, Jonathan M. Chen,
A new diagnostic algorithm for assessment of patients with single ventricle before a Fontan operation Ashwin Prakash, MD, Muhammad A. Khan, MD, Rose Hardy, BA, Alejandro J. Torres, MD, Jonathan M. Chen,
CARDIOVASCULAR SURGERY
 Volume 107, Number 4 April 1994 The Journal of THORACIC AND CARDIOVASCULAR SURGERY Cardiac and Pulmonary Transplantation Risk factors for graft failure associated with pulmonary hypertension after pediatric
Volume 107, Number 4 April 1994 The Journal of THORACIC AND CARDIOVASCULAR SURGERY Cardiac and Pulmonary Transplantation Risk factors for graft failure associated with pulmonary hypertension after pediatric
Sepsis Wave II Webinar Series. Sepsis Reassessment
 Sepsis Wave II Webinar Series Sepsis Reassessment Presenters Nova Panebianco, MD Todd Slesinger, MD Fluid Reassessment in Sepsis Todd L. Slesinger, MD, FACEP, FCCM, FCCP, FAAEM Residency Program Director
Sepsis Wave II Webinar Series Sepsis Reassessment Presenters Nova Panebianco, MD Todd Slesinger, MD Fluid Reassessment in Sepsis Todd L. Slesinger, MD, FACEP, FCCM, FCCP, FAAEM Residency Program Director
Born Blue. Anesthesia and CHD. Kristine Faust, CRNA, MS, MBA, DNAP
 Born Blue Anesthesia and CHD Kristine Faust, CRNA, MS, MBA, DNAP Disclosures Disclosures None to Report Objectives Review all congenital defects in which the patient is blue Describe physiology of the
Born Blue Anesthesia and CHD Kristine Faust, CRNA, MS, MBA, DNAP Disclosures Disclosures None to Report Objectives Review all congenital defects in which the patient is blue Describe physiology of the