Assessment of fetal heart function and rhythm
|
|
|
- Cathleen Reeves
- 5 years ago
- Views:
Transcription
1 Assessment of fetal heart function and rhythm
2 The fetal myocardium Early Gestation Myofibrils 30% of myocytes Less sarcoplasmic reticula Late Gestation Myofibrils 60% of myocytes Increased force per unit area Improved relaxation / contractile ability Active tension Passive tension
3
4 Gestational changes Systolic period stays the same Diastolic period gets longer longer early filling and atrial contraction periods Shorter isovolumic relaxation LV and RV systolic and diastolic BP increase No difference between LV and RV in paired samples Atrial pressures don t change with gestation LA mean 3.3mmHg, RA mean 3.6mmHg

5 The fetal circulation Oxygenated blood from placenta streams to left heart High pulmonary vascular resistance Low resistance placental circulation Cerebrovascular resistance is autoregulatory
6 Advantage of fetal circulation Parallel rather than series, with (at least) two options for shunting If one ventricle fails, re-distribution of blood to the other ventricle is possible in most cases This leads to the one good inlet, one good outlet rule Dysfunction usually only results in poor outcome ( fetal heart failure ) when central venous pressure is elevated
 index Cardiac output Specialized / research Tissue Doppler Strain Doppler")
7 Assessment of fetal cardiac function AHA Guidelines Routine Heart size and thickness CTR and qualitative Systolic Diastolic Specific * Qualitative Myocardiac performance (Tei) index Cardiac output Specialized / research Tissue Doppler Strain Doppler assessment

8 Cardiothoracic circumference ratio = Cardiothoracic area ratio = Cardiothoracic ratio
 =")
 end-diastolic dimension")
9 Systolic function Mainly qualitative Shortening fraction (2D or M-mode) = (end-diastolic end-systolic ventricular diameter) end-diastolic dimension Cardiac output
 Used for: High cardiac output states (anemia, teratoma, AV malformations) Low output states (e.g. Heart block, Cardiomyopathy, Ebstein s) Cardiac Output")
10 Combined cardiac output both ventricles contribute to systemic perfusion CSA x VTI x HR Accuracy: Axial plane PV and AoV diameters Axial plane PV and AoV VTI (small angle of insonation) Used for: High cardiac output states (anemia, teratoma, AV malformations) Low output states (e.g. Heart block, Cardiomyopathy, Ebstein s) Cardiac Output
11 Routine usage of Doppler Assess venous flow Ventricular inflows, Hepatic vein, Ductus venosus, UV Assess outflow gradients Assess MCA and UA PI

12 Ventricular inflow Passive (early) and active (late) filling properties of the ventricle A-wave dominant in fetal, becomes more even in later gestation Abnormal compliance leads to increased A- dominance.
13
14

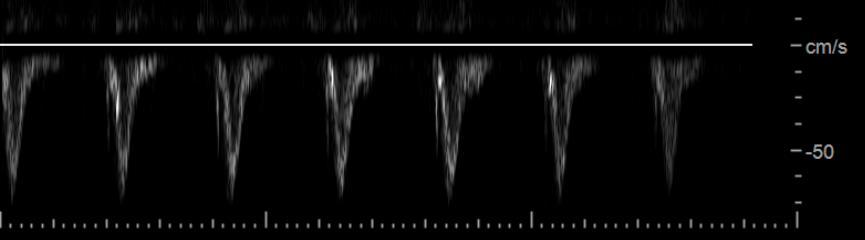
15 Hepatic vein Doppler Better alignment than IVC, and same waveform unless AV malformation Increased a-wave suggestive of high right atrial pressure low ventricular compliance atrial contraction against closed AV valve in arrhythmia Decreased s-wave suggestive of severe TR
")
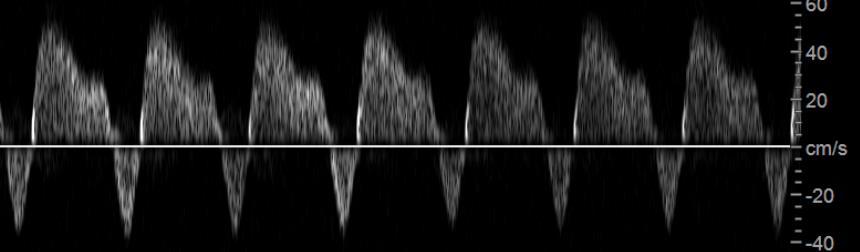
16 Ductus Venosus Follow the UV, look for aliasing Saggital view is best for Doppler Normal flow is antegrade throughout cycle A-wave reversal can be an indicator of placental dysfunction / hypoxia in IUGR babies In CHD with expected high RA pressure, A-wave reversal is expected and not associated with poor outcomes (e.g. Tricuspid atresia, Pulmonary atresia)


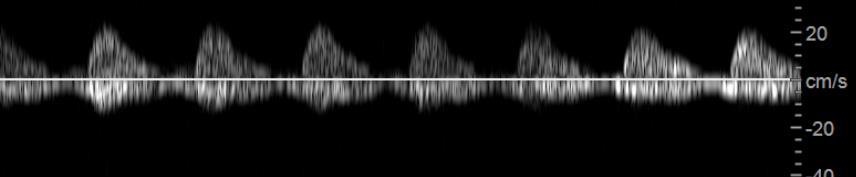
17 Should be sampled in free loop, as can vary close to fetus or placenta Umbilical vein flow should be nonpulsatile, velocity between 10 and 20cm/s UV pulsations usually indicate severely decreased ventricular compliance Umbilical artery PI decreases with gestation Elevated UA PI indicates Increased placental resistance Steal (e.g severe pulmonary regurgitation, large AVM, vein of Galen) Umbilical vein and artery

18 Flow to brain under autoregulation Low MCA PI = reduced resistance to flow brain sparing. Suggests reduced total flow AND / OR oxygen content in blood Necessitates reduced resistance to maintain nutrient delivery. High MCA PI = brain protection from elevated flow Middle Cerebral Artery

19 Cardiovascular Profile Score

.")
20 Types of dysfunction High Cardiac Output Causes Arteriovenous malformations Sacrococcygeal teratomas Fetal anemia Echo Findings Cardiomegaly Dilated RV / LV High cardiac output (greater than 625ml/m2 predicts risk of fetal death). IVC Sacrococcygeal teratoma
 Echo findings Reduced systolic function Reduced inflow time Endocardial fibroelastosis Abnormal venous Dopplers if both ventricles affected")
21 Types of dysfunction High afterload LVOT Doppler (normal <1m/s) Causes Aortic stenosis (LV) Twin-twin transfusion (RV > LV) Pulmonary stenosis; Ductal constriction (RV) Echo findings Reduced systolic function Reduced inflow time Endocardial fibroelastosis Abnormal venous Dopplers if both ventricles affected MV inflow


22 High afterload Aortic stenosis Selective IUGR, pulmonary stenosis
23 Types of dysfunction intrinsic contractile Cardiomyopathy: 2.5% of fetal heart disease 1/3 Hypertrophic 2/3 Dilated Echocardiographic Findings HCM Myocardial thickness > 2 z-scores above mean Normal RV / LV diameters Cardiomegaly DCM Decreased shortening fraction Predictors of poor outcome Uniphasic ventricular inflow Pulsatile UV flow Fetal hydrops

24
25


26 Tei index = Isovolumic time Ejection time = b a a = 0.70 (NR <0.45) a b

 = -1 FS = 0.")

27 Cardiovascular profile score: No hydrops = 0 UV pulsations = -2 CTR = 0.42 ( ) = -1 FS = / MR = -2 Total =5 Combined cardiac output = 192ml/min Tei = 0.70 Hepatic vein Ductus venosus UV
28
 = -1 FS = 0.056 / MR = -2 Total =7 Combined cardiac output = 240ml/min (50 th %) RV Tei = 0.")
29 Cardiovascular profile score No hydrops = 0 UV pulsations = 0 CTR = 0.42 ( ) = -1 FS = / MR = -2 Total =7 Combined cardiac output = 240ml/min (50 th %) RV Tei = 0.8, LV Tei 0.36

30 Another cardiomyopathy 26 weeks Family history of cardiomyopathy Non-compaction Normal inflows No venous Doppler abnormalities

31 Congenital heart disease
")
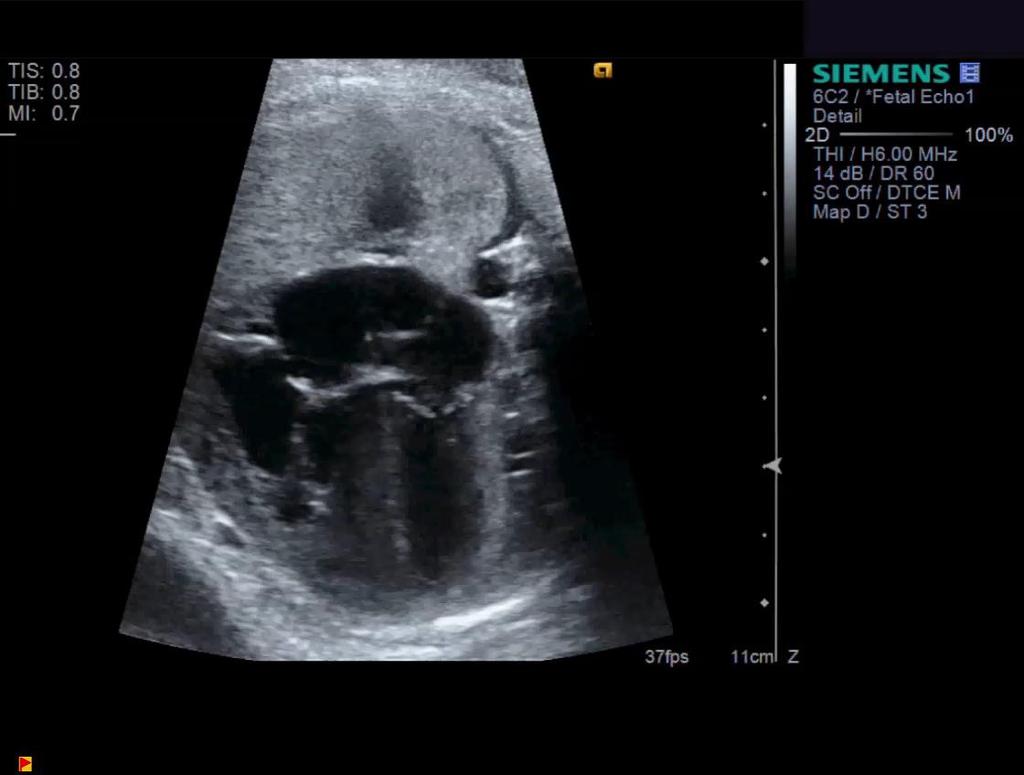
32 Types of dysfunction dyssynchrony Ebstein s Anomaly Atrialized right ventricle Volume loading of right (TR) Aneurysms

33 Newer measures of cardiac function Tissue velocity imaging (TVI) color or pulse wave High frame rates Simultaneous velocity measurement in multiple walls Angle dependent Strain imaging Need high frame rates
34 Fetal arrhythmia
35 Fetal Arrhythmias: Background Incidence Effects 2% of the pregnancies Accounts for 10-20% of referrals for fetal echo Risk factors Assessment Rhythm (irregular vs regular) Rate (fast vs slow University of Alberta Fetal and Neonatal Cardiology Program
36 Fetal Arrhythmia: Types Ectopy Premature atrial contractions (PAC) Junctional ectopic beats Premature ventricular contractions (PVC) Tachycardia Sinus tachycardia (HR bpm) Supraventricular (ectopic atrial tachycardia, AV reentry tachycardia and permanent junctional reciprocating tachycardia) Atrial Flutter (HR bpm due to AV block) Junctional ectopic tachycardia Ventricular tachycardia Bradycardia Sinus bradycardia (HR bpm) Premature atrial beats with AV block Difficult to differentiate Difficult to differentiate Congenital heart block (1 st not associated with bradycardia, 2 nd and 3 rd degree) University of Alberta Fetal and Neonatal Cardiology Program
37 Fetal Tachycardias: Risk factors Usually no identified risk factors Maternal conditions Maternal Beta-stimulation Thyroid-stimulating antibodies Fetal conditions Severe RA enlargement Ebstein s anomaly, tricuspid dysplasia, RA aneurysm Cardiac tumors University of Alberta Fetal and Neonatal Cardiology Program
38 Fetal Bradycardias: Risk Factors Maternal conditions: Auto-immune antibodies (Lupus, Sjogren s) 1 st, 2 nd, CHB. Exposure to medication (i.e. beta-blocker) Fetal conditions: Long QT syndrome Left atrial isomerism Fetal L-TGA sinus bradycardia / torsades sinus bradycardia / complete block complete heart block University of Alberta Fetal and Neonatal Cardiology Program
39 Fetal Arrhythmias: Making a Diagnosis Fetal echocardiogram-inferences based on mechanical atrial and ventricular events Blood-flow PW Doppler LV inflow-outflow PW Doppler SVC-Ao flow PW Doppler pulmonary branch artery-vein Muscular movement M-mode (cursor through the atrium and ventricle) Tissue Doppler Imaging Fetal ECG Fetal magnetocardiogram University of Alberta Fetal and Neonatal Cardiology Program





40 Fetal Arrhythmias: Making a Diagnosis M-mode: Left atrium - right ventricle PW Doppler: SVC - Ao flow V V V V V V A A A A A A PW Doppler: LV inflow/outflow PW Doppler: pulmonary vein/artery inflow PA flow outflow University of Alberta Fetal and Neonatal Cardiology Program Pulm vein flow





41 Fetal Arrhythmias: Making a Diagnosis Mechanical PR interval PW Doppler: SVC AO PW Doppler: LV inflow/outflow SVC Ao A A V A V V University of Alberta Fetal and Neonatal Cardiology Program
42 Fetal Arrhythmias: Types Ectopy Premature atrial contractions (PAC) Junctional ectopic beats Premature ventricular contractions (PVC) Tachycardia Sinus tachycardia (HR bpm) Supraventricular (EAT, AVRT and PJRT) Atrial Flutter (HR bpm) Junctional ectopic tachycardia Difficult to differentiate Ventricular tachycardia Bradycardia Sinus bradycardia (HR bpm) Premature atrial beats with AV block Congenital heart block (1 st, 2 nd and complete) Difficult to differentiate University of Alberta Fetal and Neonatal Cardiology Program
43 Fetal Arrhythmias: Ectopy Premature atrial contractions (PAC) Incidence: 5% of all pregnancies >30 weeks Benign in 98%; ~ 2% will trigger/be associated with intermittent SVT or atrial flutter Associated with CHD in 1-10% cases University of Alberta Fetal and Neonatal Cardiology Program


44 Conducted PACs Fetal Ectopy: PACs V V V V V V V V A PAC A PAC A PAC A PAC V Blocked PACs V A PAC A PAC University of Alberta Fetal and Neonatal Cardiology Program
45 Fetal Ectopy: PVCs Premature ventricular contractions (PVC) PVCs are 10x less common than PACs PVCs can be associated with VT Difficult to differentiate from junctional ectopic beats without an ECG Associated with cardiomyopathies myocarditis intracardiac tumors University of Alberta Fetal and Neonatal Cardiology Program

46 Fetal Ectopy: PVCs 2X V V V V V V X A A A A A A X University of Alberta Fetal and Neonatal Cardiology Program
47 Fetal Arrhythmias: Types Tachycardia Sinus tachycardia (HR bpm) Supraventricular (SVT) Ectopic atrial tachycardia (EAT) Atrioventricular re-entry tachycardia (AVRT) Permanent junctional re-entry tachycardia (PJRT) Atrial Flutter (HR bpm) Junctional ectopic tachycardia Ventricular tachycardia Bradycardia Sinus bradycardia (HR bpm) Premature atrial beats with AV block Congenital heart block (1 st, 2 nd and complete) Difficult to differentiate Difficult to differentiate University of Alberta Fetal and Neonatal Cardiology Program
48 Fetal Tachycardias: SVT SVT Most common fetal tachycardia (66-90%) Usually 1:1 A-V conduction Includes: AVRT, EAT and PJRT Nonimmune hydrops in 40-50% (older series) and 20-25% (recent series) which increases risk of fetal and neonatal demise even with treatment (with successful treatement <10%) Hydrops is associated with slower response to therapy and need for more than 1 medication Hydropic mechanism: ventricular compliance of the fetus filling time atrial and ventricular filling pressures pressure through the venous system University of Alberta Fetal and Neonatal Cardiology Program transudative forces cell and tissue edema

49 250 ms V V V V V A A A A A

 University of Alberta Fetal and Neonatal")
50 Fetal Tachycardias: SVT LV inflow/outflow Short AV-long VA relationship = EAT SVC-AO flow Long AV-short VA relationship= AVRT short AV interval (75ms) Long AV interval (133ms) University of Alberta Fetal and Neonatal Cardiology Program
 > 27 weeks Hydrops ~13% University of Alberta Fetal and Neonatal Cardiology")
51 Fetal Tachycardias: Atrial Flutter Atrial flutter 20-25% of fetal tachycardias Rate~ bpm AV conduction (2:1; 3:1) > 27 weeks Hydrops ~13% University of Alberta Fetal and Neonatal Cardiology Program
52 Fetal Tachycardias: V Tachycardia/JET Rare HR ranges between bpm Intermittent runs Complete A-V dissociation Exception: retrograde conduction through the AV node = 1:1 conduction Associated with long QT syndrome suspect if intermittently bradycardic University of Alberta Fetal and Neonatal Cardiology Program


53 Fetal Tachycardias: V Tachycardia/JET o AV dissociation o Ventricular rate~ 210 bpm o 1:1 conduction o Rate bpm A A A A A A V V V V V V V University of Alberta Fetal and Neonatal Cardiology Program
54 Fetal Arrhythmias:Types Ectopy Premature atrial contractions (PAC) Junctional ectopic beats Premature ventricular contractions (PVC) Tachycardia Sinus tachycardia (HR bpm) Supraventricular (EAT, AVRT and PJRT) Atrial Flutter (HR bpm) Junctional ectopic tachycardia Ventricular tachycardia Bradycardia Sinus bradycardia (HR bpm) Premature atrial beats with AV block Congenital heart block (1 st, 2 nd and complete) Difficult to differentiate Difficult to differentiate University of Alberta Fetal and Neonatal Cardiology Program


55 Fetal Bradycardias Sinus bradycardia 1:1 AV conduction If transient, is benign Persistently low HR: Blocked PACs - common! Fetal distress usually gradual Long QT syndrome Structural CHD Left atrial isomerism L-TGA A V V A V V A A University of Alberta Fetal and Neonatal Cardiology Program

56 Fetal Bradycardias: AV Block 1 0 AVB olong A-V interval 2 0 AVB; Mobitz I oa-v interval progressively increases, then drops conduction University of Alberta Fetal and Neonatal Cardiology Program


57 Fetal Bradycardias: AV Block 2 0 AVB; Mobitz I oa-a interval regular oa-v dissociation Complete AVB oa-v dissociation oventricular rate:60-70 bpm o47% structural CHD o47% maternal antibodies University of Alberta Fetal and Neonatal Cardiology Program
58 Questions?
Failing right ventricle
 Failing right ventricle U. Herberg 1, U. Gembruch 2 1 Pediatric Cardiology, 2 Prenatal Diagnostics and Fetal Therapy, University of Bonn, Germany Prenatal Physiology Right ventricle dominant ventricle
Failing right ventricle U. Herberg 1, U. Gembruch 2 1 Pediatric Cardiology, 2 Prenatal Diagnostics and Fetal Therapy, University of Bonn, Germany Prenatal Physiology Right ventricle dominant ventricle
Heart and Soul Evaluation of the Fetal Heart
 Heart and Soul Evaluation of the Fetal Heart Ivana M. Vettraino, M.D., M.B.A. Clinical Associate Professor, Michigan State University College of Human Medicine Objectives Review the embryology of the formation
Heart and Soul Evaluation of the Fetal Heart Ivana M. Vettraino, M.D., M.B.A. Clinical Associate Professor, Michigan State University College of Human Medicine Objectives Review the embryology of the formation
Introduction to Fetal Medicine. Lloyd R. Feit M.D. Associate Professor of Pediatrics Warren Alpert Medical School Brown University
 Associate Professor of Pediatrics Warren Alpert Medical School Brown University Fetal Cardiology Important in evaluation of high risk pregnancies. Information obtainable in > 95% of patients attempted.
Associate Professor of Pediatrics Warren Alpert Medical School Brown University Fetal Cardiology Important in evaluation of high risk pregnancies. Information obtainable in > 95% of patients attempted.
COMPREHENSIVE EVALUATION OF FETAL HEART R. GOWDAMARAJAN MD
 COMPREHENSIVE EVALUATION OF FETAL HEART R. GOWDAMARAJAN MD Disclosure No Relevant Financial Relationships with Commercial Interests Fetal Echo: How to do it? Timing of Study -optimally between 22-24 weeks
COMPREHENSIVE EVALUATION OF FETAL HEART R. GOWDAMARAJAN MD Disclosure No Relevant Financial Relationships with Commercial Interests Fetal Echo: How to do it? Timing of Study -optimally between 22-24 weeks
Appendix II: ECHOCARDIOGRAPHY ANALYSIS
 Appendix II: ECHOCARDIOGRAPHY ANALYSIS Two-Dimensional (2D) imaging was performed using the Vivid 7 Advantage cardiovascular ultrasound system (GE Medical Systems, Milwaukee) with a frame rate of 400 frames
Appendix II: ECHOCARDIOGRAPHY ANALYSIS Two-Dimensional (2D) imaging was performed using the Vivid 7 Advantage cardiovascular ultrasound system (GE Medical Systems, Milwaukee) with a frame rate of 400 frames
Fetal Rhythm and Blues
 Fetal Rhythm and Blues John Cotton, MD Professor of Pediatrics Division of Pediatric Cardiology Director, Fetal Cardiology Program UNC Chapel Hill, School of Medicine Objectives To review methods used
Fetal Rhythm and Blues John Cotton, MD Professor of Pediatrics Division of Pediatric Cardiology Director, Fetal Cardiology Program UNC Chapel Hill, School of Medicine Objectives To review methods used
Fetal Arrhythmias: Diagnosis and Management. Jonathan T Fleenor, MD, FACC, FAAP Pediatric Cardiology Children s Hospital of the King s Daughters
 Fetal Arrhythmias: Diagnosis and Management Jonathan T Fleenor, MD, FACC, FAAP Pediatric Cardiology Children s Hospital of the King s Daughters No industry or financial disclosures Thanks to Drs Abuhamad
Fetal Arrhythmias: Diagnosis and Management Jonathan T Fleenor, MD, FACC, FAAP Pediatric Cardiology Children s Hospital of the King s Daughters No industry or financial disclosures Thanks to Drs Abuhamad
FETAL ECHO IN TWIN PREGNACY: MONOCHORIONIC TWINS DELHI CHILD HEART CENTER & INDRAPRASTHA APOLLO HOSPITAL NEW DELHI
 FETAL ECHO IN TWIN PREGNACY: MONOCHORIONIC TWINS DELHI CHILD HEART CENTER & INDRAPRASTHA APOLLO HOSPITAL NEW DELHI Scope of this talk Twin to Twin Transfusion TRAP Sequence Congenital Heart Defects in
FETAL ECHO IN TWIN PREGNACY: MONOCHORIONIC TWINS DELHI CHILD HEART CENTER & INDRAPRASTHA APOLLO HOSPITAL NEW DELHI Scope of this talk Twin to Twin Transfusion TRAP Sequence Congenital Heart Defects in
Bits and Bobs secondary causes of heart problems. Dr Angela McBrien 9 th September 2017
 Bits and Bobs secondary causes of heart problems Dr Angela McBrien 9 th September 2017 Not the heart Dextroposition Heart in the right chest with the apex to the left Often caused by left sided chest mass
Bits and Bobs secondary causes of heart problems Dr Angela McBrien 9 th September 2017 Not the heart Dextroposition Heart in the right chest with the apex to the left Often caused by left sided chest mass
How Does Imaging Inform Fetal Cardiovascular Treatment?
 How Does Imaging Inform Fetal Cardiovascular Treatment? Edgar Jaeggi, MD Head, Fetal Cardiac Program Labatt Family Heart Center Department of Pediatrics The Hospital for Sick Children University of Toronto
How Does Imaging Inform Fetal Cardiovascular Treatment? Edgar Jaeggi, MD Head, Fetal Cardiac Program Labatt Family Heart Center Department of Pediatrics The Hospital for Sick Children University of Toronto
Evaluation of Fetal Arrhythmias
 REVIEW ARTICLE Evaluation of Fetal Arrhythmias George M Graham III DSJUOG Evaluation of Fetal Arrhythmias Assistant Professor, Division of Maternal Fetal Medicine, Department of Obstetrics, Gynecology
REVIEW ARTICLE Evaluation of Fetal Arrhythmias George M Graham III DSJUOG Evaluation of Fetal Arrhythmias Assistant Professor, Division of Maternal Fetal Medicine, Department of Obstetrics, Gynecology
Supraventricular Tachycardia: From Fetus to Adult. Mohamed Hamdan, MD
 Supraventricular Tachycardia: From Fetus to Adult Mohamed Hamdan, MD Learning Objectives Define type of SVT by age Describe clinical approach Describe prenatal and postnatal management of SVT 2 SVT Across
Supraventricular Tachycardia: From Fetus to Adult Mohamed Hamdan, MD Learning Objectives Define type of SVT by age Describe clinical approach Describe prenatal and postnatal management of SVT 2 SVT Across
PIAF study: Placental insufficiency and aortic isthmus flow Jean-Claude Fouron, MD
 Dear colleagues, I would like to thank you very sincerely for agreeing to participate in our multicentre study on the clinical significance of recording fetal aortic isthmus flow during placental circulatory
Dear colleagues, I would like to thank you very sincerely for agreeing to participate in our multicentre study on the clinical significance of recording fetal aortic isthmus flow during placental circulatory
First Trimester Fetal Echocardiography: Insight Into the Fetal Circulation
 First Trimester Fetal Echocardiography: Insight Into the Fetal Circulation Lisa K. Hornberger, MD Fetal & Neonatal Cardiology Program Department of Pediatrics, Division of Cardiology Department of Obstetrics
First Trimester Fetal Echocardiography: Insight Into the Fetal Circulation Lisa K. Hornberger, MD Fetal & Neonatal Cardiology Program Department of Pediatrics, Division of Cardiology Department of Obstetrics
Right Ventricle Steven J. Lester MD, FACC, FRCP(C), FASE Mayo Clinic, Arizona
, FASE Mayo Clinic, Arizona") Right Ventricle Steven J. Lester MD, FACC, FRCP(C), FASE Mayo Clinic, Arizona 1. In which scenario will applying the simplified Bernoulli equation to the peak tricuspid regurgitation velocity and adding
Right Ventricle Steven J. Lester MD, FACC, FRCP(C), FASE Mayo Clinic, Arizona 1. In which scenario will applying the simplified Bernoulli equation to the peak tricuspid regurgitation velocity and adding
4/19/2018. St. Cloud Hospital Perinatology Kristin Olson, RDMS, RVT
 St. Cloud Hospital Perinatology Kristin Olson, RDMS, RVT Review Fetal Circulation Provide Indications for Umbilical Artery, Middle Cerebral Artery, and Ductus Venosus Doppler studies. Demonstrate normal
St. Cloud Hospital Perinatology Kristin Olson, RDMS, RVT Review Fetal Circulation Provide Indications for Umbilical Artery, Middle Cerebral Artery, and Ductus Venosus Doppler studies. Demonstrate normal
HEMODYNAMIC ASSESSMENT
 HEMODYNAMIC ASSESSMENT INTRODUCTION Conventionally hemodynamics were obtained by cardiac catheterization. It is possible to determine the same by echocardiography. Methods M-mode & 2D echo alone can provide
HEMODYNAMIC ASSESSMENT INTRODUCTION Conventionally hemodynamics were obtained by cardiac catheterization. It is possible to determine the same by echocardiography. Methods M-mode & 2D echo alone can provide
Adult Echocardiography Examination Content Outline
 Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
Introduction. Pediatric Cardiology. General Appearance. Tools of Assessment. Auscultation. Vital Signs
 Introduction Pediatric Cardiology An introduction to the pediatric patient with heart disease: M-III Lecture Douglas R. Allen, M.D. Assistant Professor and Director of Community Pediatric Cardiology at
Introduction Pediatric Cardiology An introduction to the pediatric patient with heart disease: M-III Lecture Douglas R. Allen, M.D. Assistant Professor and Director of Community Pediatric Cardiology at
Heart and Lungs. LUNG Coronal section demonstrates relationship of pulmonary parenchyma to heart and chest wall.
 Heart and Lungs Normal Sonographic Anatomy THORAX Axial and coronal sections demonstrate integrity of thorax, fetal breathing movements, and overall size and shape. LUNG Coronal section demonstrates relationship
Heart and Lungs Normal Sonographic Anatomy THORAX Axial and coronal sections demonstrate integrity of thorax, fetal breathing movements, and overall size and shape. LUNG Coronal section demonstrates relationship
The Fetus: Five Top Do Not Miss Diagnoses. Doppler Ultrasound
 The Fetus: Five Top Do Not Miss Diagnoses Doppler Ultrasound Giancarlo Mari, MD, MBA Professor and Chair Department of Obstetrics and Gynecology University of Tennessee Health Science Center Memphis, TN
The Fetus: Five Top Do Not Miss Diagnoses Doppler Ultrasound Giancarlo Mari, MD, MBA Professor and Chair Department of Obstetrics and Gynecology University of Tennessee Health Science Center Memphis, TN
Adel Hasanin Ahmed 1
 Adel Hasanin Ahmed 1 PERICARDIAL DISEASE The pericardial effusion ends anteriorly to the descending aorta and is best visualised in the PLAX. PSAX is actually very useful sometimes for looking at posterior
Adel Hasanin Ahmed 1 PERICARDIAL DISEASE The pericardial effusion ends anteriorly to the descending aorta and is best visualised in the PLAX. PSAX is actually very useful sometimes for looking at posterior
Cardiac Arrhythmias. Cathy Percival, RN, FALU, FLMI VP, Medical Director AIG Life and Retirement Company
 Cardiac Arrhythmias Cathy Percival, RN, FALU, FLMI VP, Medical Director AIG Life and Retirement Company The Cardiovascular System Three primary functions Transport of oxygen, nutrients, and hormones to
Cardiac Arrhythmias Cathy Percival, RN, FALU, FLMI VP, Medical Director AIG Life and Retirement Company The Cardiovascular System Three primary functions Transport of oxygen, nutrients, and hormones to
The Doppler Examination. Katie Twomley, MD Wake Forest Baptist Health - Lexington
 The Doppler Examination Katie Twomley, MD Wake Forest Baptist Health - Lexington OUTLINE Principles/Physics Use in valvular assessment Aortic stenosis (continuity equation) Aortic regurgitation (pressure
The Doppler Examination Katie Twomley, MD Wake Forest Baptist Health - Lexington OUTLINE Principles/Physics Use in valvular assessment Aortic stenosis (continuity equation) Aortic regurgitation (pressure
Hemodynamic Assessment. Assessment of Systolic Function Doppler Hemodynamics
 Hemodynamic Assessment Matt M. Umland, RDCS, FASE Aurora Medical Group Milwaukee, WI Assessment of Systolic Function Doppler Hemodynamics Stroke Volume Cardiac Output Cardiac Index Tei Index/Index of myocardial
Hemodynamic Assessment Matt M. Umland, RDCS, FASE Aurora Medical Group Milwaukee, WI Assessment of Systolic Function Doppler Hemodynamics Stroke Volume Cardiac Output Cardiac Index Tei Index/Index of myocardial
Everything You Always Wanted to Know About Fetal Arrhythmias, in 40 Minutes!
 Everything You Always Wanted to Know About Fetal Arrhythmias, in 40 Minutes! Fetal Arrhythmias! What is clinically important?!tachycardia (>200)!Fixed bradycardia (
Everything You Always Wanted to Know About Fetal Arrhythmias, in 40 Minutes! Fetal Arrhythmias! What is clinically important?!tachycardia (>200)!Fixed bradycardia (
LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital
 LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital LV inflow across MV LV LV outflow across AV LV LV geometric changes Pressure overload
LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital LV inflow across MV LV LV outflow across AV LV LV geometric changes Pressure overload
The Fetal Cardiology Program
 The Fetal Cardiology Program at Texas Children s Fetal Center About the program Since the 1980s, Texas Children s Fetal Cardiology Program has provided comprehensive fetal cardiac care to expecting families
The Fetal Cardiology Program at Texas Children s Fetal Center About the program Since the 1980s, Texas Children s Fetal Cardiology Program has provided comprehensive fetal cardiac care to expecting families
Rate: The atrial and ventricular rates are equal; heart rate is greater than 100 bpm (usually between bpm).
.") Sinus Bradycardia Regularity: The R-R intervals are constant; the rhythm is regular. Rate: The atrial and ventricular rates are equal; heart rate is less than 60 bpm. P wave: There is a uniform P wave
Sinus Bradycardia Regularity: The R-R intervals are constant; the rhythm is regular. Rate: The atrial and ventricular rates are equal; heart rate is less than 60 bpm. P wave: There is a uniform P wave
CRC 431 ECG Basics. Bill Pruitt, MBA, RRT, CPFT, AE-C
 CRC 431 ECG Basics Bill Pruitt, MBA, RRT, CPFT, AE-C Resources White s 5 th ed. Ch 6 Electrocardiography Einthoven s Triangle Chest leads and limb leads Egan s 10 th ed. Ch 17 Interpreting the Electrocardiogram
CRC 431 ECG Basics Bill Pruitt, MBA, RRT, CPFT, AE-C Resources White s 5 th ed. Ch 6 Electrocardiography Einthoven s Triangle Chest leads and limb leads Egan s 10 th ed. Ch 17 Interpreting the Electrocardiogram
ULTRASOUND OF THE FETAL HEART
 ULTRASOUND OF THE FETAL HEART Cameron A. Manbeian, MD Disclosure Statement Today s faculty: Cameron Manbeian, MD does not have any relevant financial relationships with commercial interests or affiliations
ULTRASOUND OF THE FETAL HEART Cameron A. Manbeian, MD Disclosure Statement Today s faculty: Cameron Manbeian, MD does not have any relevant financial relationships with commercial interests or affiliations
What effects will proximal or distal disease have on a waveform?
 Spectral Doppler Interpretation Director of Ultrasound Education & Quality Assurance Baylor College of Medicine Division of Maternal-Fetal Medicine Maternal Fetal Center Imaging Manager Texas Children
Spectral Doppler Interpretation Director of Ultrasound Education & Quality Assurance Baylor College of Medicine Division of Maternal-Fetal Medicine Maternal Fetal Center Imaging Manager Texas Children
Dr.Binoy Skaria 13/07/15
 Dr.Binoy Skaria binoyskaria@hotmail.com binoy.skaria@heartofengland.nhs.uk 13/07/15 Acknowledgement Medtronic, Google images & Elsevier for slides Natalie Ryan, Events Manager, HEFT- for organising the
Dr.Binoy Skaria binoyskaria@hotmail.com binoy.skaria@heartofengland.nhs.uk 13/07/15 Acknowledgement Medtronic, Google images & Elsevier for slides Natalie Ryan, Events Manager, HEFT- for organising the
EKG Competency for Agency
 EKG Competency for Agency Name: Date: Agency: 1. The upper chambers of the heart are known as the: a. Atria b. Ventricles c. Mitral Valve d. Aortic Valve 2. The lower chambers of the heart are known as
EKG Competency for Agency Name: Date: Agency: 1. The upper chambers of the heart are known as the: a. Atria b. Ventricles c. Mitral Valve d. Aortic Valve 2. The lower chambers of the heart are known as
Prenatal diagnosis of long QT syndrome: Implications for delivery room and neonatal management
 Himmelfarb Health Sciences Library, The George Washington University Health Sciences Research Commons Pediatrics Faculty Publications Pediatrics 2-2013 Prenatal diagnosis of long QT syndrome: Implications
Himmelfarb Health Sciences Library, The George Washington University Health Sciences Research Commons Pediatrics Faculty Publications Pediatrics 2-2013 Prenatal diagnosis of long QT syndrome: Implications
Basic Approach to the Echocardiographic Evaluation of Ventricular Diastolic Function
 Basic Approach to the Echocardiographic Evaluation of Ventricular Diastolic Function J A F E R A L I, M D U N I V E R S I T Y H O S P I T A L S C A S E M E D I C A L C E N T E R S T A F F C A R D I O T
Basic Approach to the Echocardiographic Evaluation of Ventricular Diastolic Function J A F E R A L I, M D U N I V E R S I T Y H O S P I T A L S C A S E M E D I C A L C E N T E R S T A F F C A R D I O T
Dr. Schroeder has no financial relationships to disclose
 Valerie A Schroeder MD MS Assistant Professor University of Kansas Medical Center READING THE WAVES- THE HEART S ELECTRICAL MESSAGE FINANCIAL DISCLOSURE Dr. Schroeder has no financial relationships to
Valerie A Schroeder MD MS Assistant Professor University of Kansas Medical Center READING THE WAVES- THE HEART S ELECTRICAL MESSAGE FINANCIAL DISCLOSURE Dr. Schroeder has no financial relationships to
Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition
 Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition Table of Contents Volume 1 Chapter 1: Cardiovascular Anatomy and Physiology Basic Cardiac
Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition Table of Contents Volume 1 Chapter 1: Cardiovascular Anatomy and Physiology Basic Cardiac
ISOLATED ANOMALOUS DEVELOPMENT OF MYOCARDIUM DURING FETAL LIFE: EXPERIENCE OF OUR CENTRE
 Azienda Ospedaliera Universitaria Integrata Verona ISOLATED ANOMALOUS DEVELOPMENT OF MYOCARDIUM DURING FETAL LIFE: EXPERIENCE OF OUR CENTRE C.Sandrini *, L.Rossetti *, M.Rebonato *, M.A.Prioli *, F.Bettinazzi,
Azienda Ospedaliera Universitaria Integrata Verona ISOLATED ANOMALOUS DEVELOPMENT OF MYOCARDIUM DURING FETAL LIFE: EXPERIENCE OF OUR CENTRE C.Sandrini *, L.Rossetti *, M.Rebonato *, M.A.Prioli *, F.Bettinazzi,
COPYRIGHTED MATERIAL. The fetal circulation CHAPTER 1. Postnatal circulation
 1 CHAPTER 1 The fetal circulation The circulation in the fetus differs from that in the adult. Knowledge of the course and distribution of the fetal circulation is important to our understanding of the
1 CHAPTER 1 The fetal circulation The circulation in the fetus differs from that in the adult. Knowledge of the course and distribution of the fetal circulation is important to our understanding of the
Cardiovascular Physiology. Heart Physiology. Introduction. The heart. Electrophysiology of the heart
 Cardiovascular Physiology Heart Physiology Introduction The cardiovascular system consists of the heart and two vascular systems, the systemic and pulmonary circulations. The heart pumps blood through
Cardiovascular Physiology Heart Physiology Introduction The cardiovascular system consists of the heart and two vascular systems, the systemic and pulmonary circulations. The heart pumps blood through
PATIENT WITH ARRHYTHMIA IN DENTIST S OFFICE. Małgorzata Kurpesa, MD., PhD. Chair&Department of Cardiology
 PATIENT WITH ARRHYTHMIA IN DENTIST S OFFICE Małgorzata Kurpesa, MD., PhD. Chair&Department of Cardiology Medical University of Łódź The heart is made up of four chambers Left Atrium Right Atrium Left Ventricle
PATIENT WITH ARRHYTHMIA IN DENTIST S OFFICE Małgorzata Kurpesa, MD., PhD. Chair&Department of Cardiology Medical University of Łódź The heart is made up of four chambers Left Atrium Right Atrium Left Ventricle
(D) (E) (F) 6. The extrasystolic beat would produce (A) increased pulse pressure because contractility. is increased. increased
 (E) (F) 6. The extrasystolic beat would produce (A) increased pulse pressure because contractility. is increased. increased") Review Test 1. A 53-year-old woman is found, by arteriography, to have 5% narrowing of her left renal artery. What is the expected change in blood flow through the stenotic artery? Decrease to 1 2 Decrease
Review Test 1. A 53-year-old woman is found, by arteriography, to have 5% narrowing of her left renal artery. What is the expected change in blood flow through the stenotic artery? Decrease to 1 2 Decrease
Before we are Born: Fetal Diagnosis of Congenital Heart Disease
 Before we are Born: Fetal Diagnosis of Congenital Heart Disease Mohamed Sulaiman, MD Pediatric cardiologist Kidsheart: American Fetal & Children's Heart Center Dubai Healthcare City, Dubai-UAE First Pediatric
Before we are Born: Fetal Diagnosis of Congenital Heart Disease Mohamed Sulaiman, MD Pediatric cardiologist Kidsheart: American Fetal & Children's Heart Center Dubai Healthcare City, Dubai-UAE First Pediatric
Quantitation of right ventricular dimensions and function
 SCCS Basics of cardiac assessment Quantitation of right ventricular dimensions and function Tomasz Kukulski, MD PhD Dept of Cardiology, Congenital Heart Disease and Electrotherapy Silesian Medical University
SCCS Basics of cardiac assessment Quantitation of right ventricular dimensions and function Tomasz Kukulski, MD PhD Dept of Cardiology, Congenital Heart Disease and Electrotherapy Silesian Medical University
FLB s What Are Those Funny-Looking Beats?
 FLB s What Are Those Funny-Looking Beats? Reading Assignment (pages 27-45 in Outline ) The 5-Step Method ECG #: Mearurements: Rhythm (s): Conduction: Waveform: Interpretation: A= V= PR= QRS= QT= Axis=
FLB s What Are Those Funny-Looking Beats? Reading Assignment (pages 27-45 in Outline ) The 5-Step Method ECG #: Mearurements: Rhythm (s): Conduction: Waveform: Interpretation: A= V= PR= QRS= QT= Axis=
SWISS SOCIETY OF NEONATOLOGY. Prenatal closure of the ductus arteriosus
 SWISS SOCIETY OF NEONATOLOGY Prenatal closure of the ductus arteriosus March 2007 Leone A, Fasnacht M, Beinder E, Arlettaz R, Neonatal Intensive Care Unit (LA, AR), University Hospital Zurich, Cardiology
SWISS SOCIETY OF NEONATOLOGY Prenatal closure of the ductus arteriosus March 2007 Leone A, Fasnacht M, Beinder E, Arlettaz R, Neonatal Intensive Care Unit (LA, AR), University Hospital Zurich, Cardiology
Basic Fetal Cardiac Evaluation
 Basic Fetal Cardiac Evaluation Mert Ozan Bahtiyar, MD Director, Fetal Care Center Division of Maternal Fetal Medicine Department of Obstetrics, Gynecology and Reproductive Sciences S L I D E 1 Background
Basic Fetal Cardiac Evaluation Mert Ozan Bahtiyar, MD Director, Fetal Care Center Division of Maternal Fetal Medicine Department of Obstetrics, Gynecology and Reproductive Sciences S L I D E 1 Background
UNDERSTANDING YOUR ECG: A REVIEW
 UNDERSTANDING YOUR ECG: A REVIEW Health professionals use the electrocardiograph (ECG) rhythm strip to systematically analyse the cardiac rhythm. Before the systematic process of ECG analysis is described
UNDERSTANDING YOUR ECG: A REVIEW Health professionals use the electrocardiograph (ECG) rhythm strip to systematically analyse the cardiac rhythm. Before the systematic process of ECG analysis is described
Uncommon Doppler Echocardiographic Findings of Severe Pulmonic Insufficiency
 Uncommon Doppler Echocardiographic Findings of Severe Pulmonic Insufficiency Rahul R. Jhaveri, MD, Muhamed Saric, MD, PhD, FASE, and Itzhak Kronzon, MD, FASE, New York, New York Background: Two-dimensional
Uncommon Doppler Echocardiographic Findings of Severe Pulmonic Insufficiency Rahul R. Jhaveri, MD, Muhamed Saric, MD, PhD, FASE, and Itzhak Kronzon, MD, FASE, New York, New York Background: Two-dimensional
Index of subjects. effect on ventricular tachycardia 30 treatment with 101, 116 boosterpump 80 Brockenbrough phenomenon 55, 125
 145 Index of subjects A accessory pathways 3 amiodarone 4, 5, 6, 23, 30, 97, 102 angina pectoris 4, 24, 1l0, 137, 139, 140 angulation, of cavity 73, 74 aorta aortic flow velocity 2 aortic insufficiency
145 Index of subjects A accessory pathways 3 amiodarone 4, 5, 6, 23, 30, 97, 102 angina pectoris 4, 24, 1l0, 137, 139, 140 angulation, of cavity 73, 74 aorta aortic flow velocity 2 aortic insufficiency
Arrhythmic Complications of MI. Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine
 Arrhythmic Complications of MI Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine Objectives Brief overview -Pathophysiology of Arrhythmia ECG review of typical
Arrhythmic Complications of MI Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine Objectives Brief overview -Pathophysiology of Arrhythmia ECG review of typical
LV FUNCTION ASSESSMENT: WHAT IS BEYOND EJECTION FRACTION
 LV FUNCTION ASSESSMENT: WHAT IS BEYOND EJECTION FRACTION Jamilah S AlRahimi Assistant Professor, KSU-HS Consultant Noninvasive Cardiology KFCC, MNGHA-WR Introduction LV function assessment in Heart Failure:
LV FUNCTION ASSESSMENT: WHAT IS BEYOND EJECTION FRACTION Jamilah S AlRahimi Assistant Professor, KSU-HS Consultant Noninvasive Cardiology KFCC, MNGHA-WR Introduction LV function assessment in Heart Failure:
Standardising echocardiography and images. Version 2, 13/04/15
 Standardising echocardiography and images 1. Review of ECHO eligibility criteria - trial entry - rescue treatment 2. Assessments - personnel - timing 3. Technical aspects of ECHO examination 1. Trial entry
Standardising echocardiography and images 1. Review of ECHO eligibility criteria - trial entry - rescue treatment 2. Assessments - personnel - timing 3. Technical aspects of ECHO examination 1. Trial entry
What effects will proximal or distal disease have on an waveform?
 Spectral Doppler Interpretation Director Director of of Ultrasound Ultrasound Education Education & & Quality Quality Assurance Assurance Baylor Baylor College College of of Medicine Medicine Division
Spectral Doppler Interpretation Director Director of of Ultrasound Ultrasound Education Education & & Quality Quality Assurance Assurance Baylor Baylor College College of of Medicine Medicine Division
ADULT CONGENITAL HEART DISEASE. Stuart Lilley
 ADULT CONGENITAL HEART DISEASE Stuart Lilley More adults than children have congenital heart disease Huge variety of congenital lesions from minor to major Heart failure, re-operation and arrhythmia are
ADULT CONGENITAL HEART DISEASE Stuart Lilley More adults than children have congenital heart disease Huge variety of congenital lesions from minor to major Heart failure, re-operation and arrhythmia are
Diagnostic approach to heart disease
 Diagnostic approach to heart disease Initial work up History Physical exam Chest radiographs ECG Special studies Echocardiography Cardiac catheterization Echocardiography principles Technique of producing
Diagnostic approach to heart disease Initial work up History Physical exam Chest radiographs ECG Special studies Echocardiography Cardiac catheterization Echocardiography principles Technique of producing
Step by step approach to EKG rhythm interpretation:
 Sinus Rhythms Normal sinus arrhythmia Small, slow variation of the R-R interval i.e. variation of the normal sinus heart rate with respiration, etc. Sinus Tachycardia Defined as sinus rhythm with a rate
Sinus Rhythms Normal sinus arrhythmia Small, slow variation of the R-R interval i.e. variation of the normal sinus heart rate with respiration, etc. Sinus Tachycardia Defined as sinus rhythm with a rate
Most common fetal cardiac anomalies
 Most common fetal cardiac anomalies Common congenital heart defects CHD % of cardiac defects Chromosomal Infants Fetuses anomaly (%) 22q11 deletion (%) VSD 30 5~10 20~40 10 PS 9 5 (PA w/ VSD) HLHS 7~9
Most common fetal cardiac anomalies Common congenital heart defects CHD % of cardiac defects Chromosomal Infants Fetuses anomaly (%) 22q11 deletion (%) VSD 30 5~10 20~40 10 PS 9 5 (PA w/ VSD) HLHS 7~9
BME 5742 Bio-Systems Modeling and Control. Lecture 41 Heart & Blood Circulation Heart Function Basics
 BME 5742 Bio-Systems Modeling and Control Lecture 41 Heart & Blood Circulation Heart Function Basics Dr. Zvi Roth (FAU) 1 Pumps A pump is a device that accepts fluid at a low pressure P 1 and outputs the
BME 5742 Bio-Systems Modeling and Control Lecture 41 Heart & Blood Circulation Heart Function Basics Dr. Zvi Roth (FAU) 1 Pumps A pump is a device that accepts fluid at a low pressure P 1 and outputs the
HR: 50 bpm (Sinus) PR: 280 ms QRS: 120 ms QT: 490 ms Axis: -70. Sinus bradycardia with one ventricular escape (*)
 PR: 280 ms QRS: 120 ms QT: 490 ms Axis: -70. Sinus bradycardia with one ventricular escape (*)") 1? HR: 50 bpm (Sinus) PR: 280 ms QRS: 120 ms QT: 490 ms Axis: -70 1 Sinus P waves? 2 sinus cycles The pause (2 sinus cycles) suggests that the sinus fired (?) but did not conduct to the atria (i.e., missing
1? HR: 50 bpm (Sinus) PR: 280 ms QRS: 120 ms QT: 490 ms Axis: -70 1 Sinus P waves? 2 sinus cycles The pause (2 sinus cycles) suggests that the sinus fired (?) but did not conduct to the atria (i.e., missing
Atrial Septal Defects
 Supplementary ACHD Echo Acquisition Protocol for Atrial Septal Defects The following protocol for echo in adult patients with atrial septal defects (ASDs) is a guide for performing a comprehensive assessment
Supplementary ACHD Echo Acquisition Protocol for Atrial Septal Defects The following protocol for echo in adult patients with atrial septal defects (ASDs) is a guide for performing a comprehensive assessment
Tehran Arrhythmia Center
 Tehran Arrhythmia Center The Worst Scenario A 4 year old kid High heart rates first noted by parents at 20 months of age. Family physician detected rates as high as 220 bpm at that age. He was visited,
Tehran Arrhythmia Center The Worst Scenario A 4 year old kid High heart rates first noted by parents at 20 months of age. Family physician detected rates as high as 220 bpm at that age. He was visited,
CARDIOVASCULAR SYSTEM
 CARDIOVASCULAR SYSTEM 1. Resting membrane potential of the ventricular myocardium is: A. -55 to-65mv B. --65 to-75mv C. -75 to-85mv D. -85 to-95 mv E. -95 to-105mv 2. Regarding myocardial contraction:
CARDIOVASCULAR SYSTEM 1. Resting membrane potential of the ventricular myocardium is: A. -55 to-65mv B. --65 to-75mv C. -75 to-85mv D. -85 to-95 mv E. -95 to-105mv 2. Regarding myocardial contraction:
ISUOG Basic Training. Obtaining & Interpreting Heart Views Correctly Alfred Abuhamad, USA. Basic training. Editable text here
 ISUOG Basic Training Obtaining & Interpreting Heart Views Correctly Alfred Abuhamad, USA Learning Objectives 6, 7 & 8 At the end of the lecture you will be able to: describe how to assess cardiac situs
ISUOG Basic Training Obtaining & Interpreting Heart Views Correctly Alfred Abuhamad, USA Learning Objectives 6, 7 & 8 At the end of the lecture you will be able to: describe how to assess cardiac situs
Basic Dysrhythmia Interpretation
 Basic Dysrhythmia Interpretation Objectives 2 To understand the Basic ECG To understand the meaning of Dysrhythmia To describe the normal heart conduction system. To describe the normal impulse pathways.
Basic Dysrhythmia Interpretation Objectives 2 To understand the Basic ECG To understand the meaning of Dysrhythmia To describe the normal heart conduction system. To describe the normal impulse pathways.
ECHOGENIC FETAL HEART WITHOUT HEART BLOCK AND MATERNAL ANTI- Ro/ La ANTIBODIES POSITIVITY A LESS KNOWN ASSOCIATION
 ECHOGENIC FETAL HEART WITHOUT HEART BLOCK AND MATERNAL ANTI- Ro/ La ANTIBODIES POSITIVITY A LESS KNOWN ASSOCIATION DR PUNDALIK BALIGA FELLOW IN FETAL MEDICINE MEDISCAN SYSTEMS, CHENNAI CASE 1 30 year old
ECHOGENIC FETAL HEART WITHOUT HEART BLOCK AND MATERNAL ANTI- Ro/ La ANTIBODIES POSITIVITY A LESS KNOWN ASSOCIATION DR PUNDALIK BALIGA FELLOW IN FETAL MEDICINE MEDISCAN SYSTEMS, CHENNAI CASE 1 30 year old
REtrive. REpeat. RElearn Design by. Test-Enhanced Learning based ECG practice E-book
 Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning based ECG practice E-book REtrive REpeat RElearn Design by S I T T I N U N T H A N G J U I P E E R I Y A W A
Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning based ECG practice E-book REtrive REpeat RElearn Design by S I T T I N U N T H A N G J U I P E E R I Y A W A
CMR for Congenital Heart Disease
 CMR for Congenital Heart Disease * Second-line tool after TTE * Strengths of CMR : tissue characterisation, comprehensive access and coverage, relatively accurate measurements of biventricular function/
CMR for Congenital Heart Disease * Second-line tool after TTE * Strengths of CMR : tissue characterisation, comprehensive access and coverage, relatively accurate measurements of biventricular function/
Pediatric Echocardiography Examination Content Outline
 Pediatric Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 Anatomy and Physiology Normal Anatomy and Physiology 10% 2 Abnormal Pathology and Pathophysiology
Pediatric Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 Anatomy and Physiology Normal Anatomy and Physiology 10% 2 Abnormal Pathology and Pathophysiology
THE CARDIOVASCULAR SYSTEM
 THE CARDIOVASCULAR SYSTEM AND RESPONSES TO EXERCISE Mr. S. Kelly PSK 4U North Grenville DHS THE HEART: A REVIEW Cardiac muscle = myocardium Heart divided into two sides, 4 chambers (L & R) RS: pulmonary
THE CARDIOVASCULAR SYSTEM AND RESPONSES TO EXERCISE Mr. S. Kelly PSK 4U North Grenville DHS THE HEART: A REVIEW Cardiac muscle = myocardium Heart divided into two sides, 4 chambers (L & R) RS: pulmonary
Fetal Echocardiography
 Marie M. Gleason, M.D. Clinical Professor of Pediatrics The Perelman School of Medicine of the University of Pennsylvania Director of Outpatient and Community Cardiology and Cardiac Outreach Associate
Marie M. Gleason, M.D. Clinical Professor of Pediatrics The Perelman School of Medicine of the University of Pennsylvania Director of Outpatient and Community Cardiology and Cardiac Outreach Associate
Doppler Basic & Hemodynamic Calculations
 Doppler Basic & Hemodynamic Calculations August 19, 2017 Smonporn Boonyaratavej MD Division of Cardiology, Department of Medicine Chulalongkorn University Cardiac Center, King Chulalongkorn Memorial Hospital
Doppler Basic & Hemodynamic Calculations August 19, 2017 Smonporn Boonyaratavej MD Division of Cardiology, Department of Medicine Chulalongkorn University Cardiac Center, King Chulalongkorn Memorial Hospital
10. Thick deposits of lipids on the walls of blood vessels, called, can lead to serious circulatory issues. A. aneurysm B. atherosclerosis C.
 Heart Student: 1. carry blood away from the heart. A. Arteries B. Veins C. Capillaries 2. What is the leading cause of heart attack and stroke in North America? A. alcohol B. smoking C. arteriosclerosis
Heart Student: 1. carry blood away from the heart. A. Arteries B. Veins C. Capillaries 2. What is the leading cause of heart attack and stroke in North America? A. alcohol B. smoking C. arteriosclerosis
P = 4V 2. IVC Dimensions 10/20/2014. Comprehensive Hemodynamic Evaluation by Doppler Echocardiography. The Simplified Bernoulli Equation
 Comprehensive Hemodynamic Evaluation by Doppler Echocardiography Itzhak Kronzon, MD North Shore LIJ/ Lenox Hill Hospital New York, NY Disclosure: Philips Healthcare St. Jude Medical The Simplified Bernoulli
Comprehensive Hemodynamic Evaluation by Doppler Echocardiography Itzhak Kronzon, MD North Shore LIJ/ Lenox Hill Hospital New York, NY Disclosure: Philips Healthcare St. Jude Medical The Simplified Bernoulli
ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT
 ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT Karen Stout, MD, FACC Divisions of Cardiology University of Washington Medical Center Seattle Children s Hospital NO DISCLOSURES
ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT Karen Stout, MD, FACC Divisions of Cardiology University of Washington Medical Center Seattle Children s Hospital NO DISCLOSURES
Study methodology for screening candidates to athletes risk
 1. Periodical Evaluations: each 2 years. Study methodology for screening candidates to athletes risk 2. Personal history: Personal history of murmur in childhood; dizziness, syncope, palpitations, intolerance
1. Periodical Evaluations: each 2 years. Study methodology for screening candidates to athletes risk 2. Personal history: Personal history of murmur in childhood; dizziness, syncope, palpitations, intolerance
Paediatric Cardiology. Acyanotic CHD. Prof F F Takawira
 Paediatric Cardiology Acyanotic CHD Prof F F Takawira Aetiology Chromosomal Down syndrome, T13, T18 Genetic syndromes (gene defects) Velo-Cardio-facial (22 del) Genetic syndromes (undefined aetiology)
Paediatric Cardiology Acyanotic CHD Prof F F Takawira Aetiology Chromosomal Down syndrome, T13, T18 Genetic syndromes (gene defects) Velo-Cardio-facial (22 del) Genetic syndromes (undefined aetiology)
Chad Morsch B.S., ACSM CEP
 What Is Cardiac Stress Testing? Chad Morsch B.S., ACSM CEP A Cardiac Stress Test is a test used to measure the heart's ability to respond to external stress in a controlled clinical environment. Cardiac
What Is Cardiac Stress Testing? Chad Morsch B.S., ACSM CEP A Cardiac Stress Test is a test used to measure the heart's ability to respond to external stress in a controlled clinical environment. Cardiac
Echo Doppler Assessment of Right and Left Ventricular Hemodynamics.
 Echo Doppler Assessment of Right and Left Ventricular Hemodynamics. Itzhak Kronzon, MD, FASE, FACC, FESC, FAHA, FACP, FCCP Northwell, Lenox Hill Hospital, New York Professor of Cardiology Hofstra University
Echo Doppler Assessment of Right and Left Ventricular Hemodynamics. Itzhak Kronzon, MD, FASE, FACC, FESC, FAHA, FACP, FCCP Northwell, Lenox Hill Hospital, New York Professor of Cardiology Hofstra University
Electrocardiography Biomedical Engineering Kaj-Åge Henneberg
 Electrocardiography 31650 Biomedical Engineering Kaj-Åge Henneberg Electrocardiography Plan Function of cardiovascular system Electrical activation of the heart Recording the ECG Arrhythmia Heart Rate
Electrocardiography 31650 Biomedical Engineering Kaj-Åge Henneberg Electrocardiography Plan Function of cardiovascular system Electrical activation of the heart Recording the ECG Arrhythmia Heart Rate
Maternal and Fetal Physiology
 Background Maternal and Fetal Physiology Anderson Lo, DO Fellow, Maternal-Fetal Medicine Wayne State University School of Medicine SEMCME Fetal Assessment Course July 20, 2018 Oxygen pathway Mother Placenta
Background Maternal and Fetal Physiology Anderson Lo, DO Fellow, Maternal-Fetal Medicine Wayne State University School of Medicine SEMCME Fetal Assessment Course July 20, 2018 Oxygen pathway Mother Placenta
The Fontan circulation. Folkert Meijboom
 The Fontan circulation Folkert Meijboom What to expect? Why a Fontan-circulation Indications How does it work Types of Fontan circulation Historical overview Role of echocardiography What to expect? Why
The Fontan circulation Folkert Meijboom What to expect? Why a Fontan-circulation Indications How does it work Types of Fontan circulation Historical overview Role of echocardiography What to expect? Why
Arrhythmia Management Joshua M. Cooper, MD, FHRS, FACC
 Arrhythmia Management Joshua M. Cooper, MD, FHRS, FACC Professor of Medicine Director of Cardiac Electrophysiology Temple University Health System Plumbing Electrical System Bradyarrhythmias Sinus Node
Arrhythmia Management Joshua M. Cooper, MD, FHRS, FACC Professor of Medicine Director of Cardiac Electrophysiology Temple University Health System Plumbing Electrical System Bradyarrhythmias Sinus Node
Chapter 16: Arrhythmias and Conduction Disturbances
 Complete the following. Chapter 16: Arrhythmias and Conduction Disturbances 1. Cardiac arrhythmias result from abnormal impulse, abnormal impulse, or both mechanisms together. 2. is the ability of certain
Complete the following. Chapter 16: Arrhythmias and Conduction Disturbances 1. Cardiac arrhythmias result from abnormal impulse, abnormal impulse, or both mechanisms together. 2. is the ability of certain
Congenital Heart Disease: Physiology and Common Defects
 Congenital Heart Disease: Physiology and Common Defects Jamie S. Sutherell, M.D, M.Ed. Associate Professor, Pediatrics Division of Cardiology Director, Medical Student Education in Pediatrics Director,
Congenital Heart Disease: Physiology and Common Defects Jamie S. Sutherell, M.D, M.Ed. Associate Professor, Pediatrics Division of Cardiology Director, Medical Student Education in Pediatrics Director,
Dysrhythmias. Dysrythmias & Anti-Dysrhythmics. EKG Parameters. Dysrhythmias. Components of an ECG Wave. Dysrhythmias
 Dysrhythmias Dysrythmias & Anti-Dysrhythmics Rhythm bad in the heart: Whitewater rafting Electrical impulses coordinate heart Reduction in Cardiac Output PEA Asystole Components of an ECG Wave EKG Parameters
Dysrhythmias Dysrythmias & Anti-Dysrhythmics Rhythm bad in the heart: Whitewater rafting Electrical impulses coordinate heart Reduction in Cardiac Output PEA Asystole Components of an ECG Wave EKG Parameters
ECG Interpretation. Best to have a system to methodically evaluate ECG (from Dubin) * Rate * Rhythm * Axis * Intervals * Hypertrophy * Infarction
 * Rate * Rhythm * Axis * Intervals * Hypertrophy * Infarction") ECG to save Babies ECG Interpretation Best to have a system to methodically evaluate ECG (from Dubin) * Rate * Rhythm * Axis * Intervals * Hypertrophy * Infarction Electrical Activity in the heart 5 events
ECG to save Babies ECG Interpretation Best to have a system to methodically evaluate ECG (from Dubin) * Rate * Rhythm * Axis * Intervals * Hypertrophy * Infarction Electrical Activity in the heart 5 events
Effect of physiological heart rate changes on left ventricular dimensions and mitral blood flow velocities in the normal fetus
 ELSEVIER Early Human Development 40 (1995) 109-114 Effect of physiological heart rate changes on left ventricular dimensions and mitral blood flow velocities in the normal fetus P.B. Tsyvian a, K.V. Malkin
ELSEVIER Early Human Development 40 (1995) 109-114 Effect of physiological heart rate changes on left ventricular dimensions and mitral blood flow velocities in the normal fetus P.B. Tsyvian a, K.V. Malkin
Foetal Cardiology: How to predict perinatal problems. Prof. I.Witters Prof.M.Gewillig UZ Leuven
 Foetal Cardiology: How to predict perinatal problems Prof. I.Witters Prof.M.Gewillig UZ Leuven Cardiopathies Incidence : 8-12 / 1000 births ( 1% ) Most frequent - Ventricle Septum Defect 20% - Atrium Septum
Foetal Cardiology: How to predict perinatal problems Prof. I.Witters Prof.M.Gewillig UZ Leuven Cardiopathies Incidence : 8-12 / 1000 births ( 1% ) Most frequent - Ventricle Septum Defect 20% - Atrium Septum
Evaluation of the Right Ventricle and Risk Stratification for Sudden Cardiac Death
 Evaluation of the Right Ventricle and Risk Stratification for Sudden Cardiac Death Presenters: Sabrina Phillips, MD FACC FASE Director, Adult Congenital Heart Disease Services The University of Oklahoma
Evaluation of the Right Ventricle and Risk Stratification for Sudden Cardiac Death Presenters: Sabrina Phillips, MD FACC FASE Director, Adult Congenital Heart Disease Services The University of Oklahoma
The Physiology of the Fetal Cardiovascular System
 The Physiology of the Fetal Cardiovascular System Jeff Vergales, MD, MS Department of Pediatrics Division of Pediatric Cardiology jvergales@virginia.edu Disclosures I serve as the medical director for
The Physiology of the Fetal Cardiovascular System Jeff Vergales, MD, MS Department of Pediatrics Division of Pediatric Cardiology jvergales@virginia.edu Disclosures I serve as the medical director for
September 28-30, 2018
 September 28-30, 2018 Course Director Optimizing Detection of Congenital Heart Disease: Important Anatomic Cardiac Regions The Top 5 Critical Anatomic Regions in Fetal Cardiac Imaging Alfred Abuhamad,
September 28-30, 2018 Course Director Optimizing Detection of Congenital Heart Disease: Important Anatomic Cardiac Regions The Top 5 Critical Anatomic Regions in Fetal Cardiac Imaging Alfred Abuhamad,
Heart Failure. Cardiac Anatomy. Functions of the Heart. Cardiac Cycle/Hemodynamics. Determinants of Cardiac Output. Cardiac Output
 Cardiac Anatomy Heart Failure Professor Qing ZHANG Department of Cardiology, West China Hospital www.blaufuss.org Cardiac Cycle/Hemodynamics Functions of the Heart Essential functions of the heart to cover
Cardiac Anatomy Heart Failure Professor Qing ZHANG Department of Cardiology, West China Hospital www.blaufuss.org Cardiac Cycle/Hemodynamics Functions of the Heart Essential functions of the heart to cover
Cardiac Arrhythmias in the Human Fetus
 Pediatr Cardiol 25:234 251, 2004 DOI: 10.1007/s00246-003-0589-x Cardiac Arrhythmias in the Human Fetus C.S. Kleinman, 1 R.A. Nehgme 2 1 Professor of Clinical Pediatrics in Obstetrics & Gynecology, Columbia
Pediatr Cardiol 25:234 251, 2004 DOI: 10.1007/s00246-003-0589-x Cardiac Arrhythmias in the Human Fetus C.S. Kleinman, 1 R.A. Nehgme 2 1 Professor of Clinical Pediatrics in Obstetrics & Gynecology, Columbia
DOPPLER HEMODYNAMICS (1) QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES
 QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES") THORAXCENTRE DOPPLER HEMODYNAMICS (1) QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES J. Roelandt DOPPLER HEMODYNAMICS Intracardiac pressures and pressure gradients Volumetric measurement
THORAXCENTRE DOPPLER HEMODYNAMICS (1) QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES J. Roelandt DOPPLER HEMODYNAMICS Intracardiac pressures and pressure gradients Volumetric measurement
First-Trimester Fetal Cardiac Function
 CME Article First-Trimester Fetal Cardiac Function Noirin E. Russell, MRCPI, Fionnuala M. McAuliffe, MD, FRCPI, MRCOG Objective. The purpose of this study was to establish normal values for fetal heart
CME Article First-Trimester Fetal Cardiac Function Noirin E. Russell, MRCPI, Fionnuala M. McAuliffe, MD, FRCPI, MRCOG Objective. The purpose of this study was to establish normal values for fetal heart
Coronary Anomalies & Hemodynamic Identification
 Coronary Anomalies & Hemodynamic Identification David Stultz, MD Cardiology Fellow, PGY 6 May 2, 2006 Anomaly #1 Anomaly #2 Anomaly #3 Figure 18-27 Anomalous origin of the left circumflex artery.
Coronary Anomalies & Hemodynamic Identification David Stultz, MD Cardiology Fellow, PGY 6 May 2, 2006 Anomaly #1 Anomaly #2 Anomaly #3 Figure 18-27 Anomalous origin of the left circumflex artery.
Adult Congenital Heart Disease: What All Echocardiographers Should Know Sharon L. Roble, MD, FACC Echo Hawaii 2016
 1 Adult Congenital Heart Disease: What All Echocardiographers Should Know Sharon L. Roble, MD, FACC Echo Hawaii 2016 DISCLOSURES I have no disclosures relevant to today s talk 2 Why should all echocardiographers
1 Adult Congenital Heart Disease: What All Echocardiographers Should Know Sharon L. Roble, MD, FACC Echo Hawaii 2016 DISCLOSURES I have no disclosures relevant to today s talk 2 Why should all echocardiographers
Echocardiographic Cardiovascular Risk Stratification: Beyond Ejection Fraction
 Echocardiographic Cardiovascular Risk Stratification: Beyond Ejection Fraction October 4, 2014 James S. Lee, M.D., F.A.C.C. Associates in Cardiology, P.A. Silver Spring, M.D. Disclosures Financial none
Echocardiographic Cardiovascular Risk Stratification: Beyond Ejection Fraction October 4, 2014 James S. Lee, M.D., F.A.C.C. Associates in Cardiology, P.A. Silver Spring, M.D. Disclosures Financial none