McMaster Neonatal Skills Workshop Procedure Pearls
|
|
|
- Iris Neal
- 5 years ago
- Views:
Transcription

1 McMaster Neonatal Skills Workshop Procedure Pearls November 2, 2016 Image from:





2 Procedures ekja.org

3 NRP Epinephrine: 0.1ml/kg IV 1: ml/kg ETT 1:10000

4 NRP Useful reminders
 Lager occiput Narrowest portion of airway is cricoid http://www.ceu-emt.")
5 The neonatal airway Smaller More anterior Epiglottis is floppier Larger tongue (proportionally) Lager occiput Narrowest portion of airway is cricoid

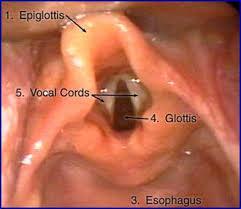
6 Anatomy and positioning
7 Indications for intubation In delivery room Apnea Cardio-respiratory instability Meconium, depressed infant Surfactant administration (prematurity) Congenital malformations (CDH, neck mass) In NICU Apnea(s) Unable to protect airway Respiratory failure (hypercarbic / hypoxic) Other therapeutic indication
 2.5 < 1000 < 28 3.0 1001 2000 28 34 3.5 2001 3000 34 38 3.5 4.0 > 3000 > 38 Gestational age (weeks) Neonatal resuscitation. AAP, CPS.")
8 Endotracheal tube measurements ETT length (cm) rule for kg infants or Tip-to-lip: 6 + weight (kg) Tube size (internal diameter in mm) Weight (grams) 2.5 < 1000 < > 3000 > 38 Gestational age (weeks) Neonatal resuscitation. AAP, CPS.
9


10 Indications: drainage of large or symptomatic a) Pneumothorax b) Pleural effusion
11 Umbilical vessel catheterization McMaster Pediatrics 2016

12 Anatomy- umbilical arterial catheter

13 Anatomy umbilical venous catheter

14 Equipment Cleaning solution Drape Scalpel Umbilical tape Needle driver Vessel dilators

15 Catheter set up UVC UAC 3 way stop cock Pressure tubing

16 Clean the cord

17 Use umbilical tape to tie the base

18 Cut cord

19 Place sterile drapes

20 Identify the vessels

21 Gently dilate vessels and insert catheter

")
] + 9")


22 Umbilical line position Umbilical artery catheter (high) cm: [3 x weight (kg)] + 9 Umbilical venous catheter cm: ½ x UAC measure radiographics.rsna.org
23 Umbilical line insertion complications Hemorrhage Perforation (peritoneal cavity, urachus, pericardium) Hepatic laceration Thrombi/emboli Retained broken off fragment Calcification portal vein/ umbilical vein Catheter associated infection
24 Peripheral IV insertion McMaster Pediatrics 2016

25 Anatomy of the vein

26 Veins hand & upper extremity

27 Veins of the lower extremities

28 veins of the lower extremity & foot

29 Veins on the scalp

30 Commonly used..

31 Direction of insertion
32 Video of catheter insertion %20prod%20vid.swf
33 McMaster Peds NICU procedure skills day 2016 Neonatal Intubation Indications: 1. Ventilation/oxygenation failure with mask airway management 2. Prolonged resuscitation 3. Meconium aspiration 4. Administration of surfactant 5. Apneas (premature infants) 6. Congenital or structural airway anomalies 7. Respiratory support in neonatal sepsis/necrotizing enterocolitis 8. Pre- or post-operative respiratory support Potential complications: Acute Prolonged 1. Trauma (pharyngeal, esophageal, tracheal) 2. Cardiorespiratory instability during intubation attempts 3. Intubation of right main-stem bronchus 1. Nosocomial respiratory infection/ventilator associated pneumonia 2. Erosion of nares/septum 3. Palatal groove formation/acquired cleft palate 4. Subglottic stenosis Equipment: 1. Laryngoscope with appropriate sized blades a. 00 for extreme preterms b. 0 for preterms c. 1 for terms 2. Appropriate size endotracheal tube (ETT) Weight (g) ETT internal diameter < > Stylet 4. Suction catheter (+/- meconium aspirator) 5. Magill s forceps 6. Carbon-dioxide detector 7. Stethoscope 8. Bag (flow-inflating/self-inflating) with compressed gas source and blender 9. Equipment to secure ETT (tape/scissors) 10. Monitoring equipment (cardiorespiratory and saturation) 11. Pre-medications (Atropine, Fentanyl, muscle-relaxant) 12. Naso- or orogastric tube FAQs: 1. Why straight blade (instead of curved)?
34 McMaster Peds NICU procedure skills day 2016 a. Straight blade can lift epiglottis (which can be relatively large and floppy in neonate) 2. Insertion depth? a. Black line of ETT at level of vocal cords b. If oral intubation: 6 cm + weight (in kg) c. If nasal intubation: 7 cm + weight (in kg) 3. When to give pre-medications? a. All newborn infants should receive analgesic premedication for endotracheal intubation except in emergency situations CPS statement on Premedications b. Patients with potential difficult airway should not receive pre-medications Pearls/Tips: 1. Ensure appropriate bagging technique (may mitigate need for intubation) a. Mask adjustment b. Reposition airway c. Suction d. Open mouth e. Pressure (need to increase) f. Alternate airway 2. Ensure bed height appropriate/comfortable for you 3. Roll/towel under infant s shoulder may help 4. Give fentanyl slowly (1-2 min) due to risk of chest wall rigidity 5. Ensure head stabilized during intubation (may assign someone to hold head) 6. Consider going deep with laryngoscope blade then withdraw slowly until vocal cords in view 7. Can use 5 th finger of laryngoscope hand to give cricoid (or may assign to someone else) 8. Assign someone to pass suction/magill s/meconium aspirator 9. Once vocal cords in view, don t take eyes off until ETT through 10. If cannot see vocal cords, consider the following a. Is neck hyper-extended? b. In laryngoscope blade too deep? Too shallow? c. Laryngoscope blade inappropriate size? d. Airway too anterior need cricoid e. Secretions/Meconium blocking view suction 11. If End-tidal CO2 monitor does not change consider, consider whether cardiovascular compromise as cause rather than improper ETT placement Laryngeal mask airway: For use when mask ventilation not effective and ETT not feasible or difficult Examples: Congenital anomalies of mouth/lip/palate Anomalies of pharynx/neck making intubation difficult Small mandible/large tongue Limitations: Cannot be used to suction meconium Need for high pressures can cause leak and cause gastric inflation Cannot give intra-tracheal medications reliably Cannot use is VLBW babies (i.e. > 1,500 grams only)
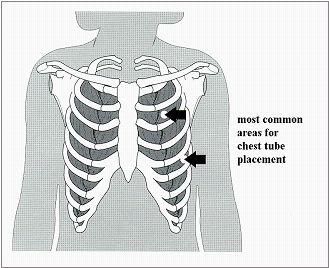
35 McMaster Peds NICU procedure skills day 2016 Needle thoracostomy procedure check list: Indications: Pneumothorax Pleural fluid (different landmark) A. Needle aspiration: Equipment: 1. 23/25 G butterfly needle, 22G/24 G IV catheter 2. 10/20 ml syringe 3. 3 way stopcock Procedure: 1. Attach the butterfly needle/catheter to the syringe fitted with a 3 way stop cock. 2. Confirm side with reviewing X ray/ clinical exam 3. Prepare the overlying skin with antibacterial solution 4. Identify the 2nd intercostal space in the mid clavicular line 5. Insert the needle firmly into the intercostal space, just above the top of the 3 rd rib (below the clavicle, minimizes chances of laceration to the intercostal vessels) 6. Have an assistant apply continuous suction as the needle is inserted 7. Rapid flow of air will occur once the needle enters the pleural space. 8. Once in the space stop advancing needle (reduce risk of puncturing the lung) Continuous air leak can be aspirated while a chest tube is inserted Technique can be used in emergency situations Potential complications: Mal-placement Hemorrhage, cardiac tamponade Lung perforation Phrenic nerve injury
36 McMaster Peds NICU procedure skills day 2016 Insertion of umbilical vein and umbilical artery catheters Procedure checklist: A. Umbilical artery catheter: Indications: 1. For invasive blood pressure monitoring 2. For frequent monitoring of arterial blood gases, other labs 3. For exchange transfusion (withdrawal) Contraindications: 1. Abdominal wall defects ex. Omphalocele 2. Peritonitis Complications: 1. Vascular accident, clot 2. Infection 3. Hemorrhage Equipment: 1. Umbilical catheter: 3.5 Fr 2. Cleaning solution 3. Umbilical tape 4. Drapes 5. Scalpel 6. Iris forceps 7. Straight clamps 8. Needle driver 9. Suture way stop cock cc syringes Procedure: 1. Determine catheter insertion length 2. Ensure line and stop cock are flushed with saline, no air is in the system as negative intrathoracic pressure can cause air embolism 3. Clean umbilical stump 4. Place cord tie 5. Cut umbilical cord 6. Place sterile drape 7. Stabilize cord with a forceps/hemostat 8. Identify 2 arteries 9. Open tip of iris forceps inserted into the vessel and gently dilated 10. Insert catheter into the vessel till calculated length
37 McMaster Peds NICU procedure skills day Check for blood flow. 12. X rays to confirm position (above the diaphragm) 13. Suture and secure with tapes/bridge 14. Documentation: size of catheter, length it is inserted to and any complications *** document any adjustments *** 15. Order heparin infusion (NICU protocol) Problems: 1. Catheter may not pass into the abdominal aorta 2. The catheter may pass into the aorta but loop caudad back into the contralateral iliac artery 3. Persistent cyanosis, blanching, poor distal extremity perfusion B. Umbilical venous catheter: Indications 1. Emergency vascular access in a resuscitation (insert 4-5cm until blood return) 2. Exchange transfusions (infuse) 3. Central venous access 4. Preferable route for inotrope administration 5. As a stable route for infusion of parenteral fluids (concentrated solutions) Complications: 1. Malposition 2. Infection 3. Perforation Equipment: Same as UA: 3 way stop cock not required; attach appropriate tubing connector Procedure Steps 1-7 same as above Catheter size: 3.5 Fr for <1500g, 5 Fr for >1500g 8. Identify Umbilical vein 9. Thread catheter to determined length 10. Confirm blood flow back in the catheter 11. In emergency situations insert catheter till blood flow is obtained, at 4-5 cm 12. Secure line (suture, bridge as above) 13. X ray to conform position (above the diaphragm, not in the heart) 14. Document as above 15. Only isotonic solution to be infused till tip position is confirmed on X ray Formulae: Umbilical artery catheter (high) cm: [3 x weight (kg)] + 9 Umbilical venous catheter cm: ½ x UAC measure + 1
Equipment: NRP algorithm, MRSOPA table, medication chart, SpO 2 table Warm
 NRP Skills Stations Performance Skills Station OR Integrated Skills Station STATION: Assisting with and insertion of endotracheal tube (ETT) Equipment: NRP algorithm, MRSOPA table, medication chart, SpO
NRP Skills Stations Performance Skills Station OR Integrated Skills Station STATION: Assisting with and insertion of endotracheal tube (ETT) Equipment: NRP algorithm, MRSOPA table, medication chart, SpO
ENDOTRACHEAL INTUBATION POLICY
 POLICY Indications: Ineffective ventilation with mask and t-piece, or mask and bag technique Inability to maintain a patent airway Need or anticipation of need for prolonged ventilation Need for endotracheal
POLICY Indications: Ineffective ventilation with mask and t-piece, or mask and bag technique Inability to maintain a patent airway Need or anticipation of need for prolonged ventilation Need for endotracheal
PEMSS PROTOCOLS INVASIVE PROCEDURES
 PEMSS PROTOCOLS INVASIVE PROCEDURES Panhandle Emergency Medical Services System SURGICAL AND NEEDLE CRICOTHYROTOMY Inability to intubate is the primary indication for creating an artificial airway. Care
PEMSS PROTOCOLS INVASIVE PROCEDURES Panhandle Emergency Medical Services System SURGICAL AND NEEDLE CRICOTHYROTOMY Inability to intubate is the primary indication for creating an artificial airway. Care
1 Chapter 40 Advanced Airway Management 2 Advanced Airway Management The advanced airway management techniques discussed in this chapter are to
 1 Chapter 40 Advanced Airway Management 2 Advanced Airway Management The advanced airway management techniques discussed in this chapter are to introduce the EMT-B student to these procedures only. In
1 Chapter 40 Advanced Airway Management 2 Advanced Airway Management The advanced airway management techniques discussed in this chapter are to introduce the EMT-B student to these procedures only. In
Chapter 40 Advanced Airway Management
 1 2 3 4 5 Chapter 40 Advanced Airway Management Advanced Airway Management The advanced airway management techniques discussed in this chapter are to introduce the EMT-B student to these procedures only.
1 2 3 4 5 Chapter 40 Advanced Airway Management Advanced Airway Management The advanced airway management techniques discussed in this chapter are to introduce the EMT-B student to these procedures only.
Anatomy and Physiology. The airways can be divided in to parts namely: The upper airway. The lower airway.
 Airway management Anatomy and Physiology The airways can be divided in to parts namely: The upper airway. The lower airway. Non-instrumental airway management Head Tilt and Chin Lift Jaw Thrust Advanced
Airway management Anatomy and Physiology The airways can be divided in to parts namely: The upper airway. The lower airway. Non-instrumental airway management Head Tilt and Chin Lift Jaw Thrust Advanced
Advanced Airway Management. University of Colorado Medical School Rural Track
 Advanced Airway Management University of Colorado Medical School Rural Track Advanced Airway Management Basic Airway Management Airway Suctioning Oxygen Delivery Methods Laryngeal Mask Airway ET Intubation
Advanced Airway Management University of Colorado Medical School Rural Track Advanced Airway Management Basic Airway Management Airway Suctioning Oxygen Delivery Methods Laryngeal Mask Airway ET Intubation
Adult Intubation Skill Sheet
 Adult Intubation 2. Opens the airway manually and inserts an oral airway *** 3. Ventilates the patient with BVM attached to oxygen at 15 lpm *** 4. Directs assistant to oxygenate the patient 5. Selects
Adult Intubation 2. Opens the airway manually and inserts an oral airway *** 3. Ventilates the patient with BVM attached to oxygen at 15 lpm *** 4. Directs assistant to oxygenate the patient 5. Selects
Advanced Airway Management
 CHAPTER 37 Advanced Airway Management Airway Anatomy and Physiology Review Respiratory System: The Airway Respiratory System (Supine) Physiology: Factors of Adequate Breathing Functioning brainstem Open
CHAPTER 37 Advanced Airway Management Airway Anatomy and Physiology Review Respiratory System: The Airway Respiratory System (Supine) Physiology: Factors of Adequate Breathing Functioning brainstem Open
This interdisciplinary clinical support document provides guidelines for the safe establishment of an artificial airway.
 PURPOSE This interdisciplinary clinical support document provides guidelines for the safe establishment of an artificial airway. POLICY STATEMENTS Endotracheal intubation will be performed by the Most
PURPOSE This interdisciplinary clinical support document provides guidelines for the safe establishment of an artificial airway. POLICY STATEMENTS Endotracheal intubation will be performed by the Most
CHEST DRAIN PROTOCOL
 CHEST DRAIN PROTOCOL Rationale The pleural membranes have an important role in effective lung expansion. The visceral pleura is a thin, smooth, serous membrane covering the surface of the lungs and is
CHEST DRAIN PROTOCOL Rationale The pleural membranes have an important role in effective lung expansion. The visceral pleura is a thin, smooth, serous membrane covering the surface of the lungs and is
Addendum to the NRP Provider Textbook 6 th Edition Recommendations for specific modifications in the Canadian context
 Addendum to the NRP Provider Textbook 6 th Edition Recommendations for specific modifications in the Canadian context A subcommittee of the Canadian Neonatal Resuscitation Program (NRP) Steering Committee
Addendum to the NRP Provider Textbook 6 th Edition Recommendations for specific modifications in the Canadian context A subcommittee of the Canadian Neonatal Resuscitation Program (NRP) Steering Committee
PRODUCTS FOR THE DIFFICULT AIRWAY. Courtesy of Cook Critical Care
 PRODUCTS FOR THE DIFFICULT AIRWAY Courtesy of Cook Critical Care EMERGENCY CRICOTHYROTOMY Thyroid Cartilage Access Site Cricoid Cartilage Identify the cricothyroid membrane between the cricoid and thyroid
PRODUCTS FOR THE DIFFICULT AIRWAY Courtesy of Cook Critical Care EMERGENCY CRICOTHYROTOMY Thyroid Cartilage Access Site Cricoid Cartilage Identify the cricothyroid membrane between the cricoid and thyroid
Pediatric Patients. BCFPD Paramedic Education Program. EMS Education Paramedic Level
 Pediatric Patients BCFPD Program Basic Considerations Much of the initial patient assessment can be done during visual examination of the scene. Involve the caregiver or parent as much as possible. Allow
Pediatric Patients BCFPD Program Basic Considerations Much of the initial patient assessment can be done during visual examination of the scene. Involve the caregiver or parent as much as possible. Allow
Airway/Breathing. Chapter 5
 Airway/Breathing Chapter 5 Airway/Breathing Introduction Skillful, rapid assessment and management of airway and ventilation are critical to preventing morbidity and mortality. Airway compromise can occur
Airway/Breathing Chapter 5 Airway/Breathing Introduction Skillful, rapid assessment and management of airway and ventilation are critical to preventing morbidity and mortality. Airway compromise can occur
Airway Management. Teeradej Kuptanon, MD
 Airway Management Teeradej Kuptanon, MD Outline Anatomy Detect difficult airway Rapid sequence intubation Difficult ventilation Difficult intubation Surgical airway access ICU setting Intubation Difficult
Airway Management Teeradej Kuptanon, MD Outline Anatomy Detect difficult airway Rapid sequence intubation Difficult ventilation Difficult intubation Surgical airway access ICU setting Intubation Difficult
H. Mitchell Shulman MDCM FRCPC CSPQ Assistant Professor, Dept. of Surgery, McGill Medical School Attending Physician, Royal Victoria Hospital,
 H. Mitchell Shulman MDCM FRCPC CSPQ Assistant Professor, Dept. of Surgery, McGill Medical School Attending Physician, Royal Victoria Hospital, Montreal General Hospital, McGill University Health Center
H. Mitchell Shulman MDCM FRCPC CSPQ Assistant Professor, Dept. of Surgery, McGill Medical School Attending Physician, Royal Victoria Hospital, Montreal General Hospital, McGill University Health Center
5 Million neonatal deaths each year worldwide. 20% caused by neonatal asphyxia. Improvement of the outcome of 1 million newborns every year
 1 5 Million neonatal deaths each year worldwide 20% caused by neonatal asphyxia Improvement of the outcome of 1 million newborns every year International Liaison Committee on Resuscitation (ILCOR) American
1 5 Million neonatal deaths each year worldwide 20% caused by neonatal asphyxia Improvement of the outcome of 1 million newborns every year International Liaison Committee on Resuscitation (ILCOR) American
Chest Tube Thoracostomy
 Chest Tube Thoracostomy INTRODUCTION A chest tube thoracostomy is commonly done in the ED to evacuate an abnormal accumulation of fluid (blood, empyema) or air from the pleural space under an elective,
Chest Tube Thoracostomy INTRODUCTION A chest tube thoracostomy is commonly done in the ED to evacuate an abnormal accumulation of fluid (blood, empyema) or air from the pleural space under an elective,
Overview. The Team Concept. Chapter 7. Assisting the ALS Provider 9/11/2012. The Team Concept ALS Procedures and Equipment
 Chapter 7 Assisting the ALS Provider Slide 1 Overview The Team Concept ALS Procedures and Equipment Electrocardiogram (ECG) Monitoring Slide 2 The Team Concept Prehospital care involves many individuals
Chapter 7 Assisting the ALS Provider Slide 1 Overview The Team Concept ALS Procedures and Equipment Electrocardiogram (ECG) Monitoring Slide 2 The Team Concept Prehospital care involves many individuals
Dr. prakruthi Dept. of anaesthesiology, Rrmch, bangalore
 CENTRAL VENOUS CATHETERIZATION Dr. prakruthi Dept. of anaesthesiology, Rrmch, bangalore OBJECTIVES Introduction Indications and Contraindications Complications Technique Basic principles Specifics by Site
CENTRAL VENOUS CATHETERIZATION Dr. prakruthi Dept. of anaesthesiology, Rrmch, bangalore OBJECTIVES Introduction Indications and Contraindications Complications Technique Basic principles Specifics by Site
PROFESSOR DR. NUMAN NAFIE HAMEED الاستاذ الدكتور نعمان نافع الحمداني
 Lecture 6 PROFESSOR DR. NUMAN NAFIE HAMEED الاستاذ الدكتور نعمان نافع الحمداني Neonatal Resuscitation Program (NRP) 2010 MCQ? In neonatal resuscitation program, the preterm neonates need special preparations
Lecture 6 PROFESSOR DR. NUMAN NAFIE HAMEED الاستاذ الدكتور نعمان نافع الحمداني Neonatal Resuscitation Program (NRP) 2010 MCQ? In neonatal resuscitation program, the preterm neonates need special preparations
Procedure: Chest Tube Placement (Tube Thoracostomy)
") Procedure: Chest Tube Placement (Tube Thoracostomy) Basic Information: The insertion and placement of a chest tube into the pleural cavity for the purpose of removing air, blood, purulent drainage, or
Procedure: Chest Tube Placement (Tube Thoracostomy) Basic Information: The insertion and placement of a chest tube into the pleural cavity for the purpose of removing air, blood, purulent drainage, or
Orotracheal Intubation
 T h e n e w e ng l a nd j o u r na l o f m e dic i n e videos in clinical medicine Orotracheal Intubation Christopher Kabrhel, M.D., Todd W. Thomsen, M.D., Gary S. Setnik, M.D., and Ron M. Walls, M.D.
T h e n e w e ng l a nd j o u r na l o f m e dic i n e videos in clinical medicine Orotracheal Intubation Christopher Kabrhel, M.D., Todd W. Thomsen, M.D., Gary S. Setnik, M.D., and Ron M. Walls, M.D.
Paediatric Resuscitation. EMS Rounds Gurinder Sangha MD Paediatric Emergency Fellow June 18, 2009
 Paediatric Resuscitation EMS Rounds Gurinder Sangha MD Paediatric Emergency Fellow June 18, 2009 Essentials of Resuscitation Airway Breathing Circulation AIRWAY Differences in Paediatric Airway Shorter
Paediatric Resuscitation EMS Rounds Gurinder Sangha MD Paediatric Emergency Fellow June 18, 2009 Essentials of Resuscitation Airway Breathing Circulation AIRWAY Differences in Paediatric Airway Shorter
The Pediatric Patient. Morgen Bernius, MD NCEMS Conference February 24, 2007
 The Pediatric Patient Morgen Bernius, MD NCEMS Conference February 24, 2007 Rule #1: Everyone Loves the Pediatric Patient Pediatrics in EMS Approximately 10% of all EMS treatment is for children younger
The Pediatric Patient Morgen Bernius, MD NCEMS Conference February 24, 2007 Rule #1: Everyone Loves the Pediatric Patient Pediatrics in EMS Approximately 10% of all EMS treatment is for children younger
All bedside percutaneously placed tracheostomies
 Page 1 of 5 Scope: All bedside percutaneously placed tracheostomies Population: All ICU personnel Outcomes: To standardize and outline the steps necessary to safely perform a percutaneous tracheostomy
Page 1 of 5 Scope: All bedside percutaneously placed tracheostomies Population: All ICU personnel Outcomes: To standardize and outline the steps necessary to safely perform a percutaneous tracheostomy
Airway Workshop Lecture. University of Ottawa
 Airway Workshop Lecture Department of Anesthesiology University of Ottawa Overview Ventilation Airway assessment Difficult airways Airway management equipment aids Intubation/Improving Intubation Success
Airway Workshop Lecture Department of Anesthesiology University of Ottawa Overview Ventilation Airway assessment Difficult airways Airway management equipment aids Intubation/Improving Intubation Success
Shedding Light on Neonatal X-rays. Objectives. Indications for X-Rays 5/14/2018
 Shedding Light on Neonatal X-rays Barbara C. Mordue, MSN, NNP-BC Neonatal Nurse Practitioner LLUH Children s Hospital, NICU Objectives Utilize a systematic approach to neonatal x-ray interpretation Identify
Shedding Light on Neonatal X-rays Barbara C. Mordue, MSN, NNP-BC Neonatal Nurse Practitioner LLUH Children s Hospital, NICU Objectives Utilize a systematic approach to neonatal x-ray interpretation Identify
General Medical Procedure. Emergency Airway Techniques (General Airway Protocol)
") General Medical Procedure Appropriate airway management is often the most important intervention a prehospital care provider makes, as ensuring adequate oxygenation and ventilation is crucial to the survival
General Medical Procedure Appropriate airway management is often the most important intervention a prehospital care provider makes, as ensuring adequate oxygenation and ventilation is crucial to the survival
Other methods for maintaining the airway (not definitive airway as still unprotected):
:") Page 56 Where anaesthetic skills and drugs are available, endotracheal intubation is the preferred method of securing a definitive airway. This technique comprises: rapid sequence induction of anaesthesia
Page 56 Where anaesthetic skills and drugs are available, endotracheal intubation is the preferred method of securing a definitive airway. This technique comprises: rapid sequence induction of anaesthesia
NRP Raising the Bar for Providers and Instructors
 NRP 2011 Raising the Bar for Providers and Instructors What is the same? 1. Minimum course requirement is Lessons 1 through 4 and Lesson 9. The NRP Provider Card requires renewal every 2 years. Your facility
NRP 2011 Raising the Bar for Providers and Instructors What is the same? 1. Minimum course requirement is Lessons 1 through 4 and Lesson 9. The NRP Provider Card requires renewal every 2 years. Your facility
Procedure No: Procedure Approved for Use By: WCCSS Divisional Quality Meeting. Date: May 2017
 Standard Operating Procedure (SOP): Standard operating procedure for Neonatal Difficult Airway Kit and Intubation Pathway Procedure No: 1 Document replaced: Version 1 Version: 2.0 Procedure Written By:
Standard Operating Procedure (SOP): Standard operating procedure for Neonatal Difficult Airway Kit and Intubation Pathway Procedure No: 1 Document replaced: Version 1 Version: 2.0 Procedure Written By:
Airway/Breathing. Chapter 5
 Airway/Breathing Chapter 5 Airway/Breathing Introduction Rapid assessment and management of airway and ventilation are critical to preventing morbidity and mortality. Airway compromise can occur rapidly
Airway/Breathing Chapter 5 Airway/Breathing Introduction Rapid assessment and management of airway and ventilation are critical to preventing morbidity and mortality. Airway compromise can occur rapidly
Overview. Chapter 37. Advanced Airway Techniques. Sellick Maneuver 9/11/2012
 Chapter 37 Advanced Airway Techniques Slide 1 Sellick Maneuver Purpose Anatomic Location Technique Special Considerations Overview Advanced Airway Management of Adults Esophageal Tracheal Combitubes Tracheal
Chapter 37 Advanced Airway Techniques Slide 1 Sellick Maneuver Purpose Anatomic Location Technique Special Considerations Overview Advanced Airway Management of Adults Esophageal Tracheal Combitubes Tracheal
Neonatal Life Support Provider (NLSP) Certification Preparatory Materials
 Certification Preparatory Materials") Neonatal Life Support Provider (NLSP) Certification Preparatory Materials NEONATAL LIFE SUPPORT PROVIDER (NRP) CERTIFICATION TABLE OF CONTENTS NEONATAL FLOW ALGORITHM.2 INTRODUCTION 3 ANTICIPATION OF RESUSCITATION
Neonatal Life Support Provider (NLSP) Certification Preparatory Materials NEONATAL LIFE SUPPORT PROVIDER (NRP) CERTIFICATION TABLE OF CONTENTS NEONATAL FLOW ALGORITHM.2 INTRODUCTION 3 ANTICIPATION OF RESUSCITATION
Handling Common Problems & Pitfalls During. Oxygen desaturation in patients receiving mechanical ventilation ACUTE SEVERE RESPIRATORY FAILURE
 Handling Common Problems & Pitfalls During ACUTE SEVERE RESPIRATORY FAILURE Pravit Jetanachai, MD QSNICH Oxygen desaturation in patients receiving mechanical ventilation Causes of oxygen desaturation 1.
Handling Common Problems & Pitfalls During ACUTE SEVERE RESPIRATORY FAILURE Pravit Jetanachai, MD QSNICH Oxygen desaturation in patients receiving mechanical ventilation Causes of oxygen desaturation 1.
Endoscopy. Pulmonary Endoscopy
 Pulmonary 1 Direct visualization of TB tree Developed in 1890 s to remove foreign bodies - rigid metal tube Advances added light system, Sx Flexible fiberoptic scopes introduced in early 1960 s 2 Used
Pulmonary 1 Direct visualization of TB tree Developed in 1890 s to remove foreign bodies - rigid metal tube Advances added light system, Sx Flexible fiberoptic scopes introduced in early 1960 s 2 Used
TRAINING NEONATOLOGY SILVANA PARIS
 TRAINING ON NEONATOLOGY SILVANA PARIS RESUSCITATION IN DELIVERY ROOM INTRODUCTION THE GLOBAL RESUSCITATION BURDEN IN NEWBORN 136 MILL NEWBORN BABIES EACH YEAR (WHO WORLD REPORT) 5-8 MILL NEWBORN INFANTS
TRAINING ON NEONATOLOGY SILVANA PARIS RESUSCITATION IN DELIVERY ROOM INTRODUCTION THE GLOBAL RESUSCITATION BURDEN IN NEWBORN 136 MILL NEWBORN BABIES EACH YEAR (WHO WORLD REPORT) 5-8 MILL NEWBORN INFANTS
NTS Clinical Guideline
 NTS Clinical Guideline Title: Authored by: Reviewed by: Indications for Umbilical Arterial Catheter Frequent arterial sampling Direct BP measurement Frequent acid-base and oxygen monitoring Exchange transfusion
NTS Clinical Guideline Title: Authored by: Reviewed by: Indications for Umbilical Arterial Catheter Frequent arterial sampling Direct BP measurement Frequent acid-base and oxygen monitoring Exchange transfusion
The following equipment and supplies shall be maintained at a minimum. Agencies should consider typical or expected usage for optimal inventory
 The following equipment and supplies shall be maintained at a minimum. Agencies should consider typical or expected usage for optimal inventory A. ALL BLS AND ALS RESPONSE AND/OR TRANSPORT UNITS Transport
The following equipment and supplies shall be maintained at a minimum. Agencies should consider typical or expected usage for optimal inventory A. ALL BLS AND ALS RESPONSE AND/OR TRANSPORT UNITS Transport
MODULE VII. Delivery and Immediate Neonatal Care
 MODULE VII Delivery and Immediate Neonatal Care NEONATAL ASPHYXIA About one million deaths per year In Latin America 12% of newborns suffer some degree of asphyxia Main cause of perinatal and neonatal
MODULE VII Delivery and Immediate Neonatal Care NEONATAL ASPHYXIA About one million deaths per year In Latin America 12% of newborns suffer some degree of asphyxia Main cause of perinatal and neonatal
Table 1: The major changes in AHA / AAP neonatal resuscitation guidelines2010 compared to previous recommendations in 2005
 Table 1: The major changes in AHA / AAP neonatal guidelines2010 compared to previous recommendations in 2005 Resuscitation step Recommendations (2005) Recommendations (2010) Comments/LOE 1) Assessment
Table 1: The major changes in AHA / AAP neonatal guidelines2010 compared to previous recommendations in 2005 Resuscitation step Recommendations (2005) Recommendations (2010) Comments/LOE 1) Assessment
Central Venous Catheter Insertion: Assisting
 Approved by: Central Venous Catheter Insertion: Assisting Gail Cameron Senior Director, Operations, Maternal, Neonatal & Child Health Programs Dr. Santiago Ensenat Medical Director, Neonatology Neonatal
Approved by: Central Venous Catheter Insertion: Assisting Gail Cameron Senior Director, Operations, Maternal, Neonatal & Child Health Programs Dr. Santiago Ensenat Medical Director, Neonatology Neonatal
AIRWAY MANAGEMENT SUZANNE BROWN, CRNA
 AIRWAY MANAGEMENT SUZANNE BROWN, CRNA OBJECTIVE OF LECTURE Non Anesthesia Sedation Providers Review for CRNA s Informal Questions encouraged 2 AIRWAY MANAGEMENT AWARENESS BASICS OF ANATOMY EQUIPMENT 3
AIRWAY MANAGEMENT SUZANNE BROWN, CRNA OBJECTIVE OF LECTURE Non Anesthesia Sedation Providers Review for CRNA s Informal Questions encouraged 2 AIRWAY MANAGEMENT AWARENESS BASICS OF ANATOMY EQUIPMENT 3
The Blue Baby. Network Stabilisation of the Term Infant Study Day 15 th March 2017 Joanna Behrsin
 The Blue Baby Network Stabilisation of the Term Infant Study Day 15 th March 2017 Joanna Behrsin Session Structure Definitions and assessment of cyanosis Causes of blue baby Structured approach to assessing
The Blue Baby Network Stabilisation of the Term Infant Study Day 15 th March 2017 Joanna Behrsin Session Structure Definitions and assessment of cyanosis Causes of blue baby Structured approach to assessing
Airway Anatomy. Soft palate. Hard palate. Nasopharynx. Tongue. Oropharynx. Hypopharynx. Thyroid cartilage
 Airway Anatomy Hard palate Soft palate Tongue Nasopharynx Oropharynx Hypopharynx Thyroid cartilage Airway Anatomy Hyoid bone Thyroid cartilage Cricoid cartilage Trachea Cricothyroid membrane Airway Anatomy
Airway Anatomy Hard palate Soft palate Tongue Nasopharynx Oropharynx Hypopharynx Thyroid cartilage Airway Anatomy Hyoid bone Thyroid cartilage Cricoid cartilage Trachea Cricothyroid membrane Airway Anatomy
MODULE VII. Delivery and Immediate Neonatal Care
 MODULE VII Delivery and Immediate Neonatal Care NEONATAL ASPHYXIA About one million deaths per year In Latin America 12% of newborns suffer some degree of asphyxia A major cause of perinatal and neonatal
MODULE VII Delivery and Immediate Neonatal Care NEONATAL ASPHYXIA About one million deaths per year In Latin America 12% of newborns suffer some degree of asphyxia A major cause of perinatal and neonatal
CARDIAC EMERGENCIES Other Cardiac Dysrhythmias C9
 CARDIAC EMERGENCIES Other Cardiac Dysrhythmias C9 ATRIAL FLUTTER Variable rate depending on block. Atrial rate between 250-350, saw-tooth pattern. (see Appendix B for energy settings for bi-phasic low
CARDIAC EMERGENCIES Other Cardiac Dysrhythmias C9 ATRIAL FLUTTER Variable rate depending on block. Atrial rate between 250-350, saw-tooth pattern. (see Appendix B for energy settings for bi-phasic low
Practical Application of CPAP
 CHAPTER 3 Practical Application of CPAP Dr. Srinivas Murki Neonatologist Fernadez Hospital, Hyderabad. A.P. Practical Application of CPAP Continuous positive airway pressure (CPAP) applied to premature
CHAPTER 3 Practical Application of CPAP Dr. Srinivas Murki Neonatologist Fernadez Hospital, Hyderabad. A.P. Practical Application of CPAP Continuous positive airway pressure (CPAP) applied to premature
Mary Lou Garey MSN EMT-P MedFlight of Ohio
 Mary Lou Garey MSN EMT-P MedFlight of Ohio Function Prolonged and frequent access to venous circulation Allows for patient to carry on normal life; decrease number of needle sticks Medications, parenteral
Mary Lou Garey MSN EMT-P MedFlight of Ohio Function Prolonged and frequent access to venous circulation Allows for patient to carry on normal life; decrease number of needle sticks Medications, parenteral
Respiratory Management in Pediatrics
 Respiratory Management in Pediatrics Children s Hospital Omaha Critical Care Transport Sue Holmer RN, C-NPT Objectives Examine the differences between the pediatric and adults airways. Recognize respiratory
Respiratory Management in Pediatrics Children s Hospital Omaha Critical Care Transport Sue Holmer RN, C-NPT Objectives Examine the differences between the pediatric and adults airways. Recognize respiratory
Advocate Christ Medical Center CVC Placement Certification Course
 Advocate Christ Medical Center CVC Placement Certification Course July 12th, 2012 Hannah Watts, MD Medical Simulation Director Modified August 10, 2017 Taajwar Khan, MD Chief Resident of Internal Medicine
Advocate Christ Medical Center CVC Placement Certification Course July 12th, 2012 Hannah Watts, MD Medical Simulation Director Modified August 10, 2017 Taajwar Khan, MD Chief Resident of Internal Medicine
October Paediatric Respiratory Workbook APCP RESPIRATORY COMMITTEE
 October 2017 Paediatric Respiratory Workbook APCP RESPIRATORY COMMITTEE This workbook is designed to introduce to you the difference between paediatric and adult anatomy and physiology. It will also give
October 2017 Paediatric Respiratory Workbook APCP RESPIRATORY COMMITTEE This workbook is designed to introduce to you the difference between paediatric and adult anatomy and physiology. It will also give
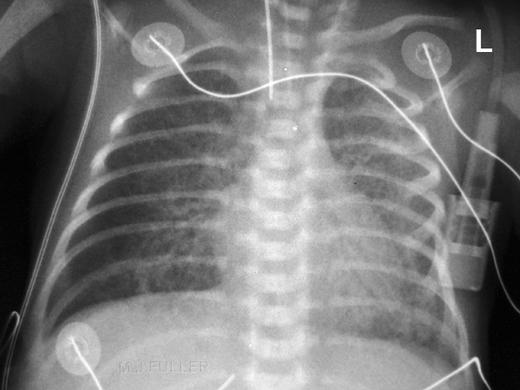
Tubes and lines in neonatal chest radiograph
 Tubes and lines in neonatal chest radiograph Poster No.: C-1008 Congress: ECR 2014 Type: Educational Exhibit Authors: R. TUMMA, N. AHMED, V. Prasad ; Hyderabad/IN, 1 2 1 1 2 HYDERABAD, ANDHRA PRADESH/IN
Tubes and lines in neonatal chest radiograph Poster No.: C-1008 Congress: ECR 2014 Type: Educational Exhibit Authors: R. TUMMA, N. AHMED, V. Prasad ; Hyderabad/IN, 1 2 1 1 2 HYDERABAD, ANDHRA PRADESH/IN
 NEONATAL LIFE SUPPORT PROVIDER (NLSP) CERTIFICATION EXAMINATION 1. To determine if an infant requires resuscitation, you must rapidly assess gestation period, presence of meconium in amniotic fluid, breaths
NEONATAL LIFE SUPPORT PROVIDER (NLSP) CERTIFICATION EXAMINATION 1. To determine if an infant requires resuscitation, you must rapidly assess gestation period, presence of meconium in amniotic fluid, breaths
Simulation 3: Post-term Baby in Labor and Delivery
 Simulation 3: Post-term Baby in Labor and Delivery Opening Scenario (Links to Section 1) You are an evening-shift respiratory therapist in a large hospital with a level III neonatal unit. You are paged
Simulation 3: Post-term Baby in Labor and Delivery Opening Scenario (Links to Section 1) You are an evening-shift respiratory therapist in a large hospital with a level III neonatal unit. You are paged
CHEST PHYSIOTHERAPY IN NICU PURPOSE POLICY STATEMENTS SITE APPLICABILITY PRACTICE LEVEL/COMPETENCIES. The role of chest physiotherapy in the NICU
 PURPOSE The role of chest physiotherapy in the NICU POLICY STATEMENTS In principle chest physiotherapy should be limited to those infants considered most likely to benefit with significant respiratory
PURPOSE The role of chest physiotherapy in the NICU POLICY STATEMENTS In principle chest physiotherapy should be limited to those infants considered most likely to benefit with significant respiratory
Surgical Care at the District Hospital. EMERGENCY & ESSENTIAL SURGICAL CARE
 Surgical Care at the District Hospital 1 14 Practical Anesthesia Key Points 2 14.1 General Anesthesia Have a clear plan before starting anesthesia Never use an unfamiliar anesthetic technique in an emergency
Surgical Care at the District Hospital 1 14 Practical Anesthesia Key Points 2 14.1 General Anesthesia Have a clear plan before starting anesthesia Never use an unfamiliar anesthetic technique in an emergency
Educational Session: Evaluation and Management of the Difficult Airway
 Educational Session: Evaluation and Management of the Difficult Airway Diane M. Birnbaumer, MD, FACEP 3/24/2010 7:30 AM - 8:30 AM The Difficult Airway What s Up YOUR Sleeve? Diane M. Birnbaumer, M.D.,
Educational Session: Evaluation and Management of the Difficult Airway Diane M. Birnbaumer, MD, FACEP 3/24/2010 7:30 AM - 8:30 AM The Difficult Airway What s Up YOUR Sleeve? Diane M. Birnbaumer, M.D.,
Home Health Foundation, Inc. To create more permanent IV access for patients undergoing long term IV therapy.
 PROCEDURE ORIGINAL DATE: 06/99 Revised Date: 09/02 Home Health Foundation, Inc. SUBJECT: PURPOSE: MIDLINE CATHETER INSERTION To create more permanent IV access for patients undergoing long term IV therapy.
PROCEDURE ORIGINAL DATE: 06/99 Revised Date: 09/02 Home Health Foundation, Inc. SUBJECT: PURPOSE: MIDLINE CATHETER INSERTION To create more permanent IV access for patients undergoing long term IV therapy.
Per-Q-Cath* PICC Catheters with Excalibur Introducer* System
 Bard Access Systems Per-Q-Cath* PICC and Catheters with Excalibur Introducer* System Instructions For Use Table of Contents Table of Contents Page Contents 1 Product Description, Indications & Contraindications
Bard Access Systems Per-Q-Cath* PICC and Catheters with Excalibur Introducer* System Instructions For Use Table of Contents Table of Contents Page Contents 1 Product Description, Indications & Contraindications
Pedi-Cap CO 2 detector
 Pedi-Cap CO 2 detector Presentation redeveloped for this program by Rosemarie Boland from an original presentation by Johnston, Adams & Stewart, (2006) Background Clinical methods of endotracheal tube
Pedi-Cap CO 2 detector Presentation redeveloped for this program by Rosemarie Boland from an original presentation by Johnston, Adams & Stewart, (2006) Background Clinical methods of endotracheal tube
Arabian Gulf University Kingdom of Bahrain Year 5 Pediatrics 3 rd Week Discussion with Dr. Muna Al-Jufairi (Part 2)
") Arabian Gulf University Kingdom of Bahrain Year 5 Pediatrics 3 rd Week Discussion with Dr. Muna Al-Jufairi (Part 2) - Case 1: a 32 weeks preterm developed RDS 4 hours after delivery. Chest X-ray shows:
Arabian Gulf University Kingdom of Bahrain Year 5 Pediatrics 3 rd Week Discussion with Dr. Muna Al-Jufairi (Part 2) - Case 1: a 32 weeks preterm developed RDS 4 hours after delivery. Chest X-ray shows:
Waitin In The Wings. Esophageal/Tracheal Double Lumen Airway (Combitube ) Indications and Use for the Pre-Hospital Provider
 Indications and Use for the Pre-Hospital Provider") Waitin In The Wings Esophageal/Tracheal Double Lumen Airway (Combitube ) Indications and Use for the Pre-Hospital Provider 1 CombiTube Kit General Description The CombiTube is A double-lumen tube with
Waitin In The Wings Esophageal/Tracheal Double Lumen Airway (Combitube ) Indications and Use for the Pre-Hospital Provider 1 CombiTube Kit General Description The CombiTube is A double-lumen tube with
They re not little adults, but they are little humans. Pearls for your next pediatric trauma patient. Children are little humans
 They re not little adults, but they are little humans Pearls for your next pediatric trauma patient Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago Alisa McQueen
They re not little adults, but they are little humans Pearls for your next pediatric trauma patient Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago Alisa McQueen
Background & Indications Probe Selection
 Teresa S. Wu, MD, FACEP Director, EM Ultrasound Program & Fellowship Co-Director, Simulation Based Training Program & Fellowship Associate Program Director, EM Residency Program Maricopa Medical Center
Teresa S. Wu, MD, FACEP Director, EM Ultrasound Program & Fellowship Co-Director, Simulation Based Training Program & Fellowship Associate Program Director, EM Residency Program Maricopa Medical Center
Resuscitation efforts for Mom & Baby
 Resuscitation efforts for Mom & Baby Beth Ann Clayton, CRNA, MS AmSol Obstetric Anesthesia CRNA Educator Obstetric Anesthesia Clinical Coordinator Mercy Health-Fairfield Hospital Assistant Professor, University
Resuscitation efforts for Mom & Baby Beth Ann Clayton, CRNA, MS AmSol Obstetric Anesthesia CRNA Educator Obstetric Anesthesia Clinical Coordinator Mercy Health-Fairfield Hospital Assistant Professor, University
The Pediatric Airway. Andrew Wackett, MD
 The Pediatric Airway Andrew Wackett, MD Objectives 1) Demonstrate understanding of the indications for intubation 2) Perform rapid sequence intubation 3) Learn the pharmacology behind emergency airway
The Pediatric Airway Andrew Wackett, MD Objectives 1) Demonstrate understanding of the indications for intubation 2) Perform rapid sequence intubation 3) Learn the pharmacology behind emergency airway
Difficult Airway. Victor M. Gomez, M.D. Pulmonary Critical Care Medicine Medical City Dallas Hospital
 Difficult Airway Victor M. Gomez, M.D. Pulmonary Critical Care Medicine Medical City Dallas Hospital Difficult Airway Definition Predicting a difficult airway Preparing for a difficult airway Extubation
Difficult Airway Victor M. Gomez, M.D. Pulmonary Critical Care Medicine Medical City Dallas Hospital Difficult Airway Definition Predicting a difficult airway Preparing for a difficult airway Extubation
LESSON ASSIGNMENT. Emergency Surgical Procedures. After completing this lesson, you should be able to:
 LESSON ASSIGNMENT LESSON 3 Emergency Surgical Procedures. LESSON ASSIGNMENT Paragraphs 3-1 through 3-6. LESSON OBJECTIVES After completing this lesson, you should be able to: 3-1. Identify the steps in
LESSON ASSIGNMENT LESSON 3 Emergency Surgical Procedures. LESSON ASSIGNMENT Paragraphs 3-1 through 3-6. LESSON OBJECTIVES After completing this lesson, you should be able to: 3-1. Identify the steps in
Neonatal Resuscitation
 Neonatal Resuscitation High Risk Deliveries A person trained in neonatal resuscitation is usually called to be present for the following deliveries: 1. Antepartum factors Maternal diabetes Pregnancy induced
Neonatal Resuscitation High Risk Deliveries A person trained in neonatal resuscitation is usually called to be present for the following deliveries: 1. Antepartum factors Maternal diabetes Pregnancy induced
Policies & Procedures. RNSP - RN Procedure. I.D. Number: 1097
 Policies & Procedures Title: ESOPHAGEAL TAMPONADE TUBE (MINNESOTA Tube) ASSISTING WITH INSERTION, CARE OF A PATIENT, ASSISTING WITH REMOVAL RNSP - RN Procedure I.D. Number: 1097 Authorization [x] Nursing
Policies & Procedures Title: ESOPHAGEAL TAMPONADE TUBE (MINNESOTA Tube) ASSISTING WITH INSERTION, CARE OF A PATIENT, ASSISTING WITH REMOVAL RNSP - RN Procedure I.D. Number: 1097 Authorization [x] Nursing
Angkana Lurngnateetape,, MD. Department of Anesthesiology Siriraj Hospital
 AIRWAY MANAGEMENT Angkana Lurngnateetape,, MD. Department of Anesthesiology Siriraj Hospital Perhaps the most important responsibility of the anesthesiologist is management of the patient s airway Miller
AIRWAY MANAGEMENT Angkana Lurngnateetape,, MD. Department of Anesthesiology Siriraj Hospital Perhaps the most important responsibility of the anesthesiologist is management of the patient s airway Miller
Erik Adler AMC Penetrating Neck Injury: Anatomy and Management Plus Common Procedures Performed in the Emergency Dept.
 Erik Adler AMC 2009 Penetrating Neck Injury: Anatomy and Management Plus Common Procedures Performed in the Emergency Dept. Brief History Penetrating neck injury (PNI) comprises 5 to 10 percent of traumatic
Erik Adler AMC 2009 Penetrating Neck Injury: Anatomy and Management Plus Common Procedures Performed in the Emergency Dept. Brief History Penetrating neck injury (PNI) comprises 5 to 10 percent of traumatic
TruCorp AirSim Child
 TruCorp AirSim Baby Part No: TCJR10001 AirSim Baby is the latest addition to the TruCorp family of advanced airway and resuscitation mannequins. This simulator incorporates realistic anatomy and clinical
TruCorp AirSim Baby Part No: TCJR10001 AirSim Baby is the latest addition to the TruCorp family of advanced airway and resuscitation mannequins. This simulator incorporates realistic anatomy and clinical
ADVANCED AIRWAY MANAGEMENT
 The Advanced Airway Management protocol should be used on all patients requiring advanced airway management procedures. This protocol is divided into three sections the Crash Airway Algorithm, the Rapid
The Advanced Airway Management protocol should be used on all patients requiring advanced airway management procedures. This protocol is divided into three sections the Crash Airway Algorithm, the Rapid
Neonatal Intensive Care Unit Skills Checklist
 _ XXX-XX- Print Name Last 4 of SS # Date Completed Directions Please circle a value for each question to provide us and the interested facilities with an assessment of your clinical experience. These values
_ XXX-XX- Print Name Last 4 of SS # Date Completed Directions Please circle a value for each question to provide us and the interested facilities with an assessment of your clinical experience. These values
Dr.Bharghavi.M 2 nd year post graduate Dept of Anaesthesia
 DIFFICULT AIRWAY CANNOT VENTILATE, CANNOT INTUBATE. Dr.Bharghavi.M 2 nd year post graduate Dept of Anaesthesia Difficult airway According to AMERICAN SOCIETY OF ANAESTHESIOLOGISTS Difficult Airway is defined
DIFFICULT AIRWAY CANNOT VENTILATE, CANNOT INTUBATE. Dr.Bharghavi.M 2 nd year post graduate Dept of Anaesthesia Difficult airway According to AMERICAN SOCIETY OF ANAESTHESIOLOGISTS Difficult Airway is defined
Infection. Risk factor for infection ACoRN alerting sign with * Clinical deterioration. Problem List. Respiratory. Cardiovascular
 The ACoRN Process Baby at risk Unwell Risk factors Post-resuscitation requiring stabilization Resuscitation Ineffective breathing Heart rate < 100 bpm Central cyanosis Support Infection Risk factor for
The ACoRN Process Baby at risk Unwell Risk factors Post-resuscitation requiring stabilization Resuscitation Ineffective breathing Heart rate < 100 bpm Central cyanosis Support Infection Risk factor for
Jefferson Tower Task Trainer List
 Jefferson Tower Task Trainer List Table of Contents Blue Phantom Ultrasound Central Line Training Model 2 Blue Phantom Femoral Vascular Access Training Model 3 Blue Phantom Thoracentesis Ultrasound Training
Jefferson Tower Task Trainer List Table of Contents Blue Phantom Ultrasound Central Line Training Model 2 Blue Phantom Femoral Vascular Access Training Model 3 Blue Phantom Thoracentesis Ultrasound Training
CCTC Minnesota Procedure: Minnesota Tube, Assisting with Insertion and Care of Patient
 CCTC Minnesota Procedure: Minnesota Tube, Assisting with Insertion and Care of Patient Purpose: To control bleeding from esophageal or gastric varices that have not responded to medical therapy (ie. Sclerotherapy,
CCTC Minnesota Procedure: Minnesota Tube, Assisting with Insertion and Care of Patient Purpose: To control bleeding from esophageal or gastric varices that have not responded to medical therapy (ie. Sclerotherapy,
Airway/Breathing. Chapter 5
 Airway/Breathing Chapter 5 Airway/Breathing Introduction Skillful, rapid, assessment and management of airway and ventilation are critical to preventing morbidity and mortality. Airway compromise can occur
Airway/Breathing Chapter 5 Airway/Breathing Introduction Skillful, rapid, assessment and management of airway and ventilation are critical to preventing morbidity and mortality. Airway compromise can occur
1 Chapter 13 Respiratory Emergencies 2 Respiratory Distress Patients often complain about. Shortness of breath Symptom of many different Cause can be
 1 Chapter 13 Respiratory Emergencies 2 Respiratory Distress Patients often complain about. Shortness of breath Symptom of many different Cause can be difficult to determine. Even for physician in hospital
1 Chapter 13 Respiratory Emergencies 2 Respiratory Distress Patients often complain about. Shortness of breath Symptom of many different Cause can be difficult to determine. Even for physician in hospital
Intraosseous Vascular Access. Dr Merl & Dr Veera
 Intraosseous Vascular Access Dr Merl & Dr Veera INDICATIONS The EZ-IO can be used for adult and pediatric patients, Is indicated any time vascular access is difficult to obtain Can be in emergent, urgent,
Intraosseous Vascular Access Dr Merl & Dr Veera INDICATIONS The EZ-IO can be used for adult and pediatric patients, Is indicated any time vascular access is difficult to obtain Can be in emergent, urgent,
Trauma operating room
 Section 1 Chapter 1 Operating Room General Conduct Trauma operating room Kenji Inaba and Lisa L. Schlitzkus Operating room A large operating room (OR) situated near the emergency department, elevators,
Section 1 Chapter 1 Operating Room General Conduct Trauma operating room Kenji Inaba and Lisa L. Schlitzkus Operating room A large operating room (OR) situated near the emergency department, elevators,
Introducing the Fastrach-LMA. Prepared by Jim Medeiros, NREMT-P Regional Field Coordinator Lord Fairfax EMS Council
 Introducing the Fastrach-LMA Prepared by Jim Medeiros, NREMT-P Regional Field Coordinator Lord Fairfax EMS Council Objectives Review Anatomy of the Upper Airway Review LFEMSC LMA Protocol Discuss Indications
Introducing the Fastrach-LMA Prepared by Jim Medeiros, NREMT-P Regional Field Coordinator Lord Fairfax EMS Council Objectives Review Anatomy of the Upper Airway Review LFEMSC LMA Protocol Discuss Indications
Michigan General Procedures EMERGENCY AIRWAY. Date: November 15, 2012 Page 1 of 16
 Date: November 15, 2012 Page 1 of 16 Emergency Airway Effective airway management and ventilation are important lifesaving interventions that all EMS providers must be able to perform. The approach to
Date: November 15, 2012 Page 1 of 16 Emergency Airway Effective airway management and ventilation are important lifesaving interventions that all EMS providers must be able to perform. The approach to
Lecture 2: Clinical anatomy of thoracic cage and cavity II
 Lecture 2: Clinical anatomy of thoracic cage and cavity II Dr. Rehan Asad At the end of this session, the student should be able to: Identify and discuss clinical anatomy of mediastinum such as its deflection,
Lecture 2: Clinical anatomy of thoracic cage and cavity II Dr. Rehan Asad At the end of this session, the student should be able to: Identify and discuss clinical anatomy of mediastinum such as its deflection,
Central Venous Line Insertion
 Central Venous Line Insertion Understand the indications and risks of CVC insertion Understand and troubleshoot the seldinger technique Understand available sites and select the appropriate site for clinical
Central Venous Line Insertion Understand the indications and risks of CVC insertion Understand and troubleshoot the seldinger technique Understand available sites and select the appropriate site for clinical
Duct Dependant Congenital Heart Disease
 Children s Acute Transport Service Clinical Guidelines Duct Dependant Congenital Heart Disease This guideline has been agreed by both NTS & CATS Document Control Information Author CATS/NTS Author Position
Children s Acute Transport Service Clinical Guidelines Duct Dependant Congenital Heart Disease This guideline has been agreed by both NTS & CATS Document Control Information Author CATS/NTS Author Position
Pediatric Shock. Hypovolemia. Sepsis. Most common cause of pediatric shock Small blood volumes (80cc/kg)
") Critical Concepts: Shock Inadequate peripheral perfusion where oxygen delivery does not meet metabolic demand Adult vs Pediatric Shock - Same causes/different frequencies Pediatric Shock Hypovolemia Most
Critical Concepts: Shock Inadequate peripheral perfusion where oxygen delivery does not meet metabolic demand Adult vs Pediatric Shock - Same causes/different frequencies Pediatric Shock Hypovolemia Most
Emergency Room Resuscitation of the Unstable Trauma Patient
 Emergency Room Resuscitation of the Unstable Trauma Patient Goals of trauma resuscitation Maintain: Systemic oxygenation Systemic perfusion Neurologic function Approach to unstable trauma patient Primary
Emergency Room Resuscitation of the Unstable Trauma Patient Goals of trauma resuscitation Maintain: Systemic oxygenation Systemic perfusion Neurologic function Approach to unstable trauma patient Primary
County of Santa Clara Emergency Medical Services System
 County of Santa Clara Emergency Medical Services System Policy # 700-M08: Intraosseous Infusion INTRAOSSEOUS INFUSION Effective Date February 7, 2014 Replaces June 2012 Review November 2016 I. Purpose
County of Santa Clara Emergency Medical Services System Policy # 700-M08: Intraosseous Infusion INTRAOSSEOUS INFUSION Effective Date February 7, 2014 Replaces June 2012 Review November 2016 I. Purpose
APPROACH TO THE EMERGENCY AIRWAY. Scott B. Davidson MD, FACS Trauma Surgery Service Bronson Methodist Hospital
 APPROACH TO THE EMERGENCY AIRWAY Scott B. Davidson MD, FACS Trauma Surgery Service Bronson Methodist Hospital Objectives History Initial recognition Get your act together Surgical options Complications
APPROACH TO THE EMERGENCY AIRWAY Scott B. Davidson MD, FACS Trauma Surgery Service Bronson Methodist Hospital Objectives History Initial recognition Get your act together Surgical options Complications
Stabilization of the Newborn for Transport. Relevant Disclosure. Learning Objectives
 Stabilization of the Newborn for Transport Arlen Foulks, DO FAAP FACOP Medical Director, CCMH Level II NICU Medical Director, NeoFlight Assistant Professor of Pediatrics Neonatal Perinatal Medicine Section,
Stabilization of the Newborn for Transport Arlen Foulks, DO FAAP FACOP Medical Director, CCMH Level II NICU Medical Director, NeoFlight Assistant Professor of Pediatrics Neonatal Perinatal Medicine Section,
GENERAL ANAESTHESIA AND FAILED INTUBATION
 GENERAL ANAESTHESIA AND FAILED INTUBATION INTRODUCTION The majority of caesarean sections in the UK are performed under regional anaesthesia. However, there are situations where general anaesthesia (GA)
GENERAL ANAESTHESIA AND FAILED INTUBATION INTRODUCTION The majority of caesarean sections in the UK are performed under regional anaesthesia. However, there are situations where general anaesthesia (GA)
2. Need for serial arterial blood gas determinations. 2. Anticipation of the initiation of thrombolytic therapy
 I. Subject: Arterial Cannulation II. Policy: Arterial cannulation will be performed upon a physician's order by Cardiopulmonary and Respiratory Therapy personnel certified in the arterial catheterization
I. Subject: Arterial Cannulation II. Policy: Arterial cannulation will be performed upon a physician's order by Cardiopulmonary and Respiratory Therapy personnel certified in the arterial catheterization
Neonatal/Pediatric Cardiopulmonary Care
 Neonatal/Pediatric Cardiopulmonary Care Resuscitation 2 When To Resuscitate Need usually related Combination of Can occur in 3 Causes of Fetal Asphyxia 1 4 Apnea Hypoxia Stimulates chemoreceptors & baroreceptors
Neonatal/Pediatric Cardiopulmonary Care Resuscitation 2 When To Resuscitate Need usually related Combination of Can occur in 3 Causes of Fetal Asphyxia 1 4 Apnea Hypoxia Stimulates chemoreceptors & baroreceptors
Exchange Transfusion
 Approved by: Exchange Transfusion Gail Cameron Director, Maternal, Neonatal & Child Health Programs Neonatal Nursery Policy & Procedures Manual : Next Review March 2016 Dr. Ensenat Medical Director, Neonatology
Approved by: Exchange Transfusion Gail Cameron Director, Maternal, Neonatal & Child Health Programs Neonatal Nursery Policy & Procedures Manual : Next Review March 2016 Dr. Ensenat Medical Director, Neonatology