Grand Rounds: A 42-Year-Old Man with Chest, Abdominal Discomfort. By Ari Thomas, Danielle Levine and Laurel Edington
|
|
|
- Sheena Daniels
- 5 years ago
- Views:
Transcription
1 Grand Rounds: A 42-Year-Old Man with Chest, Abdominal Discomfort By Ari Thomas, Danielle Levine and Laurel Edington
2 Case Presentation 42-year old male Chief complaint chest and abdominal discomfort for two days
3 History of Present Illness Pain increasing in intensity Nausea and early satiety No outside meals No recent abdominal trauma, rectal bleeding or black stools

4 History of Present Illness Cont. Substernal chest pressure consistent with usual angina Not responsive to single sublingual nitroglyercin tablet Only responsive to a group of administered medicines
5 Patient Medical History Has hypertension, hyperlipidemia, coronary artery disease, and angina Myocardial infarction at 32 years old Coronary artery angioplasty with stent placement and subsequent bypass grafting
6 Patient Medical History Cont. Family history of colon cancer Recent colonoscopy was unremarkable Chronic diarrhea for ten years Past six months experienced: daily headaches, nocturia, feeling warm at night but no fevers or night sweats, occasional early satiety and 35 lb. weight loss Takes cholesterol-lowering medication
7 Current Medications Ramipril Aspririn n-3 Fatty Acids Folic Acid Isosorbide Dinitrate Atorvastatin Multivitamins Fenofibrate Nicotinic Acid Amlopidine Extended-release Metoprolol Succinate
8 Social and Family History Married with 2 children Occupation: nurse Remote history of blood exposure to HIV and hepatitis B and C (work-related) No tobacco or recreational drug use Additional family history of prostate cancer and coronary artery disease (both father)
9 Differential Diagnosis Acute chest syndrome Acute abdominal syndrome Inflammatory disorder Cancer
10 Physical Exam Chest clear ruled out acute chest syndrome Normal cardiac examination Abdomen soft, nondistended, no hepatosplenomegaly or masses Normal bowel sounds, normal rectal exam Upper right quadrant tender o Upper abdominal disorder
11 Acute Coronary Syndrome Electrocardiogram Normal sinus rhythm No ST-segment or T-wave abnormalities Chest radiography No acute cardiopulmonary process
12 Inflammatory Disorders Lipase, aminotransferase, and amylase levels elevated o Pancreatitis o Liver disease, injury, cancer o Autoimmune, inflammatory disorder


13 CT Scan
14 Exploratory Laparotomy Reactive follicular and interfollicular hyperplasia Lipogranulomas Lipids from GI tract o Inflammatory abdominal disorder No evidence lymphoproliferative disorders o No cancer
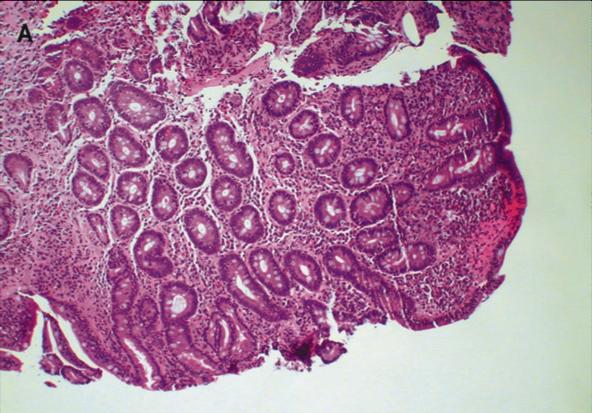

15 Small-Bowel Biopsy
16 Celiac Disease Confirmation IgA tissue transglutaminase antibodies IgA endomysial antibodies
17 Physicians Overlooked Celiac Disease Surgery was non-diagnostic and invasive Simple blood test succeeded, more specific Important for physicians to consider celiac disease when patients present with symptoms suggestive of celiac disease
18 Treatment Gluten-free diet Intramuscular iron supplementation Multivitamin

19 Mechanisms of Disease Autoimmune disorder provoked by intaking gluten Affects small bowel o Abnormal immune response to o o o gliadin in gluten protein Type 1 helper T cells cause inflammation in epithelium and lamina propria of small intestine Alters structure of intestinal villi Malabsorption

20 Symptoms Intestinal Symptoms o Abdominal pain o Diarrhea o Elevation of aminotransferase levels o Increased risk of pancreatitis Extragastrointestinal Symptoms o Rashes o Arthralgias o Neurologic and psychiatric effects o Fatigue o Infertility Other associations with type 1 diabetes, thyroiditis, and hepatitis
21 Prevalence 1-2% of general population in North America, South America, Europe, North Africa, the Middle East, and India Increasing diagnosis due to improved testing methods and increased prevalence Celiac disease still under-diagnosed in the US
22 Gluten-Free Fad Diet Placebo component to unnecessarily removing gluten from diet Non-celiac gluten intolerance has not presented itself to be a real medical issue GFD can cause gastrointestinal problems in people without celiac disease Research on the subject is preliminary
23 Works Cited 1. Ole-Petter Riksfjord Hamnvik, M.D., Fidencio Saldana, M.D., Bruce D. Levy, M.D., and Joseph Loscalzo, M.D., Ph.D. N Engl J Med 2014; 371: Medline Plus: Medical Dictionary. Besthesda, MD: U.S. National Library of Medicine, (Accessed January 13, 2015 at 3. Leffler, D. Celiac Disease Diagnosis and Management: A 46-Year-Old Woman With Anemia. Jama 2011; 306: Rubio-Tapia, A., Hill, I. D., Kelly, C. P., Calderwood, A. H., & Murray, J. A. American College of Gastroenterology Clinical Guideline: Diagnosis and Management of Celiac Disease. The American Journal of Gastroenterology 2013, 108:
Patient Interview Form
 Patient Interview Form Patient Information First Name: Last Name: Date of Birth: Age: Email Personal: Race Select one or more Referring Physician White Black or African Asian American Indian Native Hawaiian
Patient Interview Form Patient Information First Name: Last Name: Date of Birth: Age: Email Personal: Race Select one or more Referring Physician White Black or African Asian American Indian Native Hawaiian
PLEASE LET US KNOW YOUR REASON FOR TODAY S VISIT : CURRENT MEDICATIONS (WITH DOSAGE) PLEASE INCLUDE VITAMINS AND HERBAL MEDICATIONS:
 PLEASE INCLUDE VITAMINS AND HERBAL MEDICATIONS:") 1 NAME: DATE OF BIRTH PLEASE LET US KNOW YOUR REASON FOR TODAY S VISIT : CURRENT MEDICATIONS (WITH DOSAGE) PLEASE INCLUDE VITAMINS AND HERBAL MEDICATIONS: PAST MEDICAL HISTORY (YOUR MEDICAL HISTORY) :
1 NAME: DATE OF BIRTH PLEASE LET US KNOW YOUR REASON FOR TODAY S VISIT : CURRENT MEDICATIONS (WITH DOSAGE) PLEASE INCLUDE VITAMINS AND HERBAL MEDICATIONS: PAST MEDICAL HISTORY (YOUR MEDICAL HISTORY) :
GASTROENTEROLOGY PATIENT QUESTIONNAIRE - PLEASE PRINT
 GASTROENTEROLOGY PATIENT QUESTIONNAIRE - PLEASE PRINT Full name: Date: Telephone Number: Age: Address: Email address: CHIEF COMPLAINTS(List the problems about which you came to see the doctor) 1) 2) 3)
GASTROENTEROLOGY PATIENT QUESTIONNAIRE - PLEASE PRINT Full name: Date: Telephone Number: Age: Address: Email address: CHIEF COMPLAINTS(List the problems about which you came to see the doctor) 1) 2) 3)
VASCULAR SURGERY PATIENT HEALTH HISTORY
 VASCULAR SURGERY PATIENT HEALTH HISTORY Chief Complaint - Please describe the problem that brings you into the office today: Allergies 1. Do you have any allergies? if so, please list To Medications? To
VASCULAR SURGERY PATIENT HEALTH HISTORY Chief Complaint - Please describe the problem that brings you into the office today: Allergies 1. Do you have any allergies? if so, please list To Medications? To
Pediatric Gastroenterology Referral Guidelines
 Suggested Pre-Referral Workup This is a general suggestion of possible testing to confirm a suspected diagnosis. Although referrals will be accepted without the suggested work up being complete, to ensure
Suggested Pre-Referral Workup This is a general suggestion of possible testing to confirm a suspected diagnosis. Although referrals will be accepted without the suggested work up being complete, to ensure
Patient Interview Form
 Page 1 of 5 Patient Interview Form Patient Information First Name: MRN: Last Name: Date Of Birth: Contact Preference Email Telephone call- Work Telephone call - Home Email Please check one as your preferred
Page 1 of 5 Patient Interview Form Patient Information First Name: MRN: Last Name: Date Of Birth: Contact Preference Email Telephone call- Work Telephone call - Home Email Please check one as your preferred
PLAS/RECON SURGERY PATIENT HEALTH HISTORY
 PLAS/RECON SURGERY PATIENT HEALTH HISTORY Chief Complaint - Please describe the problem that brings you into the office today: Allergies 1. Do you have any allergies? if so, please list To Medications?
PLAS/RECON SURGERY PATIENT HEALTH HISTORY Chief Complaint - Please describe the problem that brings you into the office today: Allergies 1. Do you have any allergies? if so, please list To Medications?
PAGE 1 NEURO-OPHTHALMIC QUESTIONNAIRE NAME: AGE: DATE OF EXAM: CHART #: (Office Use Only)
") PAGE 1 NEURO-OPHTHALMIC QUESTIONNAIRE NAME: AGE: DATE OF EXAM: CHART #: (Office Use Only) 1. What is the main problem that you are having? (If additional space is required, please use the back of this
PAGE 1 NEURO-OPHTHALMIC QUESTIONNAIRE NAME: AGE: DATE OF EXAM: CHART #: (Office Use Only) 1. What is the main problem that you are having? (If additional space is required, please use the back of this
GASTROENTEROLOGY ESSENTIALS
 GASTROENTEROLOGY ESSENTIALS Practical Gastroenterology 8/25/2018 Jahnavi Koppala, MBBS Abdullah Abdussalam, MD A 48-year-old male was evaluated for noncardiac chest pain. Treatment with PPI twice daily
GASTROENTEROLOGY ESSENTIALS Practical Gastroenterology 8/25/2018 Jahnavi Koppala, MBBS Abdullah Abdussalam, MD A 48-year-old male was evaluated for noncardiac chest pain. Treatment with PPI twice daily
Patient Name Date of Birth MALE / FEMALE Date. Left handed or Right handed. Marital Status: Single Married Divorced Widowed Children?
 PH NEW PATIENT HISTORY Patient Name Date of Birth MALE / FEMALE Date Occupation: Left handed or Right handed Marital Status: Single Married Divorced Widowed Children? Y or N # Previous Treating Physician:
PH NEW PATIENT HISTORY Patient Name Date of Birth MALE / FEMALE Date Occupation: Left handed or Right handed Marital Status: Single Married Divorced Widowed Children? Y or N # Previous Treating Physician:
Digestion: Small and Large Intestines Pathology
 Digestion: Small and Large Intestines Pathology Dr. Ritamarie Loscalzo Medical Disclaimer: The information in this presentation is not intended to replace a one onone relationship with a qualified health
Digestion: Small and Large Intestines Pathology Dr. Ritamarie Loscalzo Medical Disclaimer: The information in this presentation is not intended to replace a one onone relationship with a qualified health
Patient Name Date of Birth Age. Other phone ( ) . Other
 . Other") GASTROINTESTINAL & MINIMALLY INVASIVE SURGERY HEALTH HISTORY QUESTIONNAIRE Date Patient Name _ Date of Birth Age Daytime phone ( ) Other phone ( ) Email How did you hear about us? My doctor Yellow pages
GASTROINTESTINAL & MINIMALLY INVASIVE SURGERY HEALTH HISTORY QUESTIONNAIRE Date Patient Name _ Date of Birth Age Daytime phone ( ) Other phone ( ) Email How did you hear about us? My doctor Yellow pages
Patient Interview Form
 Page 1 of 5 Orange Coast Memorial Office: 18111 Brookhurst Ave. Suite 5200, Fountain Valley, CA 92708 * Tel: (714) 962-7705 * Fax: (714) 861-4552 www.unitedgi.com Patient Interview Form Patient Information
Page 1 of 5 Orange Coast Memorial Office: 18111 Brookhurst Ave. Suite 5200, Fountain Valley, CA 92708 * Tel: (714) 962-7705 * Fax: (714) 861-4552 www.unitedgi.com Patient Interview Form Patient Information
J. Van Lier Ribbink, M.D., F.A.C.S. Center for Endocrine and Pancreas Surgery at Honor Health
 J. Van Lier Ribbink, M.D., F.A.C.S. Center for Endocrine and Pancreas Surgery at Honor Health Patient Clinical Information Questionnaire 1.0 Date of Questionnaire Completion; / / 2.0 Patient Data 2.1 Name:
J. Van Lier Ribbink, M.D., F.A.C.S. Center for Endocrine and Pancreas Surgery at Honor Health Patient Clinical Information Questionnaire 1.0 Date of Questionnaire Completion; / / 2.0 Patient Data 2.1 Name:
Johns Hopkins Hospital Division of Gastroenterology Patient Questionnaire
 Johns Hopkins Hospital Division of Gastroenterology Patient Questionnaire Please complete this questionnaire before your scheduled appointment and bring this form with you the day of your visit. Patient
Johns Hopkins Hospital Division of Gastroenterology Patient Questionnaire Please complete this questionnaire before your scheduled appointment and bring this form with you the day of your visit. Patient
WASHINGTON UNIVERSITY SCHOOL OF MEDICINE. Cranial Health History Form
 WASHINGTON UNIVERSITY SCHOOL OF MEDICINE Cranial Health History Form Welcome to the Neurosurgery Department at Washington University. To help us treat you, please fill this form out completely. Your Name:
WASHINGTON UNIVERSITY SCHOOL OF MEDICINE Cranial Health History Form Welcome to the Neurosurgery Department at Washington University. To help us treat you, please fill this form out completely. Your Name:
New Patient Medical History Form
 New Patient Medical History Form Date: Name: Date of Birth: Address: City: ZIP: Home Phone #: Cell Phone #: Emergency Contact: Relationship: Emergency Contact Phone #: Primary Care Physician: Referring
New Patient Medical History Form Date: Name: Date of Birth: Address: City: ZIP: Home Phone #: Cell Phone #: Emergency Contact: Relationship: Emergency Contact Phone #: Primary Care Physician: Referring
Patient History Form
 Acct #: Patient History Form Please answer ALL questions by filling out the appropriate box(es). Name: Gender: M F Primary Care Provider: DOB: Today s Date: Referring Provider (if different from PCP):
Acct #: Patient History Form Please answer ALL questions by filling out the appropriate box(es). Name: Gender: M F Primary Care Provider: DOB: Today s Date: Referring Provider (if different from PCP):
Biomarkers of GI tract diseases. By Dr. Gouse Mohiddin Shaik
 By Dr. Gouse Mohiddin Shaik Introduction The gastrointestinal (GI) tract is a complex system performing multiple biological functions which are anatomically distributed Site for food processing and absorption
By Dr. Gouse Mohiddin Shaik Introduction The gastrointestinal (GI) tract is a complex system performing multiple biological functions which are anatomically distributed Site for food processing and absorption
DIVISION OF CARDIOLOGY
 Name: Date of Birth: / / Home Phone #: Cell Phone #: Work Phone #: Fax #: Address: City: State: Zip: Primary Care Physician: Office Address: Work #: Fax #: Referring Physician (if different): Office Address:
Name: Date of Birth: / / Home Phone #: Cell Phone #: Work Phone #: Fax #: Address: City: State: Zip: Primary Care Physician: Office Address: Work #: Fax #: Referring Physician (if different): Office Address:
SURGERY SPECIALTY PATIENT HEALTH HISTORY
 SURGERY SPECIALTY PATIENT HEALTH HISTORY Chief Complaint - Please describe the problem that brings you into the office today: Allergies 1. Do you have any allergies? if so, please list To Medications?
SURGERY SPECIALTY PATIENT HEALTH HISTORY Chief Complaint - Please describe the problem that brings you into the office today: Allergies 1. Do you have any allergies? if so, please list To Medications?
Medical PCCN. AACN Progressive Critical Care Nursing.
 Medical PCCN AACN Progressive Critical Care Nursing http://killexams.com/pass4sure/exam-detail/pccn Question: 83 What would be identified on the arterial blood gas results as a reflection of acute respiratory
Medical PCCN AACN Progressive Critical Care Nursing http://killexams.com/pass4sure/exam-detail/pccn Question: 83 What would be identified on the arterial blood gas results as a reflection of acute respiratory
PATIENT HISTORY FORM
 PATIENT HISTORY FORM Date: Page 1 of 5 Last Name: First Name: Middle Initial: Referred By: Age: Primary Care Doctor: Please provide name(s) of other physician(s) that you have visited within the last year:
PATIENT HISTORY FORM Date: Page 1 of 5 Last Name: First Name: Middle Initial: Referred By: Age: Primary Care Doctor: Please provide name(s) of other physician(s) that you have visited within the last year:
PATIENT INFORMATION Last Name: First Name: Middle: Date of Birth: EMERGENCY CONTACT INFORMATION PRIMARY INSURANCE INFORMATION
 PATIENT INFORMATION Last Name: First Name: Middle: Date of Birth: Gender: SSN: Race: Marital Status: Address Line: City: State: Zip Code: Home Phone: Work Phone: Email Address: Cell Phone: Primary Care
PATIENT INFORMATION Last Name: First Name: Middle: Date of Birth: Gender: SSN: Race: Marital Status: Address Line: City: State: Zip Code: Home Phone: Work Phone: Email Address: Cell Phone: Primary Care
Please list any treatments you have previously had for current illness. (Physical Therapy, Surgery, Radiation, etc.)
") Date: Patient Name: D.O.B Last First M.I History of Present Illness: What is the reason for your visit? Date symptom started? Please list any treatments you have previously had for current illness. (Physical
Date: Patient Name: D.O.B Last First M.I History of Present Illness: What is the reason for your visit? Date symptom started? Please list any treatments you have previously had for current illness. (Physical
NEW PATIENT VISIT QUESTIONNAIRE
 HeartHealth A Program of the Dalio Institute of Cardiovascular Imaging NEW PATIENT VISIT QUESTIONNAIRE Name: Date of Birth: / / Address: City: State: Zip: Home Phone #: Work Phone #: Cell #: Email: Preferred
HeartHealth A Program of the Dalio Institute of Cardiovascular Imaging NEW PATIENT VISIT QUESTIONNAIRE Name: Date of Birth: / / Address: City: State: Zip: Home Phone #: Work Phone #: Cell #: Email: Preferred
JOHN MICHAEL ROACH, MD
 GASTROENTEROLOGY JOHN MICHAEL ROACH, MD 520 N. 4 TH AVE. PASCO, WA 99301 Phone: (509) 546-8383 Name: Date of Birth: First Middle (full) Last m/d/yr Primary care provider: Referring physician: Local Pharmacy:
GASTROENTEROLOGY JOHN MICHAEL ROACH, MD 520 N. 4 TH AVE. PASCO, WA 99301 Phone: (509) 546-8383 Name: Date of Birth: First Middle (full) Last m/d/yr Primary care provider: Referring physician: Local Pharmacy:
City State Zip. Cell Phone. Other Phone. Gender Male Female Status Single Married Divorced Widowed. Height Weight EXERCISE Yes No Times per Week
 Patient Name (First Middle Last) Date of Birth Social Security # Address City State Zip Home Phone Work Phone Cell Phone Other Phone Email Place of Birth Occupation Retired Yes No Gender Male Female Status
Patient Name (First Middle Last) Date of Birth Social Security # Address City State Zip Home Phone Work Phone Cell Phone Other Phone Email Place of Birth Occupation Retired Yes No Gender Male Female Status
Abstracting Hematopoietic Neoplasms
 CASE 1: LYMPHOMA PHYSICAL EXAMINATION 43yo male with a history of lower gastrointestinal bleeding and melena undergoing colonoscopy and biopsy to rule out neoplasm versus inflammation. Patient had no other
CASE 1: LYMPHOMA PHYSICAL EXAMINATION 43yo male with a history of lower gastrointestinal bleeding and melena undergoing colonoscopy and biopsy to rule out neoplasm versus inflammation. Patient had no other
Patient Information Last Name: First Name: Middle Initial: Address: City: State: Zip Code:
 Patient Information Last Name: First Name: Middle Initial: Address: City: State: Zip Code: Date of Birth (MM/DD/YY): Social Security #: Sex: Male Female Home Phone #: Mobile Phone #: Email Address: Marital
Patient Information Last Name: First Name: Middle Initial: Address: City: State: Zip Code: Date of Birth (MM/DD/YY): Social Security #: Sex: Male Female Home Phone #: Mobile Phone #: Email Address: Marital
Contrast Materials Patient Safety: What are contrast materials and how do they work?
 Contrast Materials Patient Safety: What are contrast materials and how do they work? Which imaging exams use contrast materials? How safe are contrast materials? How should I prepare for my imaging procedure
Contrast Materials Patient Safety: What are contrast materials and how do they work? Which imaging exams use contrast materials? How safe are contrast materials? How should I prepare for my imaging procedure
ADVANCED GASTROENTEROLOGY & ENDOSCOPY, P.C. ALI S. KARAKURUM, MD, FACP, FACG
 ADVANCED GASTROENTEROLOGY & ENDOSCOPY, P.C. ALI S. KARAKURUM, MD, FACP, FACG DATE SOC. SEC. NUMBER FULL NAME DATE OF BIRTH ADDRESS: STREET TOWN STATE ZIP PHONE: HOME WORK CELL EMPLOYER OCCUPATION ADDRESS
ADVANCED GASTROENTEROLOGY & ENDOSCOPY, P.C. ALI S. KARAKURUM, MD, FACP, FACG DATE SOC. SEC. NUMBER FULL NAME DATE OF BIRTH ADDRESS: STREET TOWN STATE ZIP PHONE: HOME WORK CELL EMPLOYER OCCUPATION ADDRESS
PLEASE COMPLETE ALL SECTIONS OF THIS FORM
 PLEASE COMPLETE ALL SECTIONS OF THIS FORM Patient Name: Date of Birth: Referring Doctor? (Name, telephone number and address) Chief Complaint: Why have you come here? How did it start? What are the symptoms?
PLEASE COMPLETE ALL SECTIONS OF THIS FORM Patient Name: Date of Birth: Referring Doctor? (Name, telephone number and address) Chief Complaint: Why have you come here? How did it start? What are the symptoms?
AUTHORIZATION TO RELEASE AND/OR OBTAIN PATIENT INFORMATION
 Medical Record # Patient Name(s) Date of Birth Social Security # Contact Phone # AUTHORIZATION TO RELEASE AND/OR OBTAIN PATIENT INFORMATION OBTAIN FROM: (Releasing facility) RELEASE TO: (Receiving entity)
Medical Record # Patient Name(s) Date of Birth Social Security # Contact Phone # AUTHORIZATION TO RELEASE AND/OR OBTAIN PATIENT INFORMATION OBTAIN FROM: (Releasing facility) RELEASE TO: (Receiving entity)
Level 2. Non Responsive Celiac Disease KEY POINTS:
 Level 2 Non Responsive Celiac Disease KEY POINTS: Celiac Disease (CD) is an autoimmune condition triggered by ingestion of gluten leading to intestinal damage and a variety of clinical manifestations.
Level 2 Non Responsive Celiac Disease KEY POINTS: Celiac Disease (CD) is an autoimmune condition triggered by ingestion of gluten leading to intestinal damage and a variety of clinical manifestations.
TEXAS VASCULAR ASSOCIATES, P.A. PATIENT CLINICAL INTAKE FORM
 TEXAS VASCULAR ASSOCIATES, P.A. PATIENT CLINICAL INTAKE FORM PATIENT NAME: DATE OF BIRTH: TVA Physician being seen: Date of Visit: PAST MEDICAL HISTORY HEART PROBLEMS NEUROLOGICAL Congestive Heart Failure
TEXAS VASCULAR ASSOCIATES, P.A. PATIENT CLINICAL INTAKE FORM PATIENT NAME: DATE OF BIRTH: TVA Physician being seen: Date of Visit: PAST MEDICAL HISTORY HEART PROBLEMS NEUROLOGICAL Congestive Heart Failure
725 Jesse Jewell Pkwy, Suite 390 Gainesville, GA (770) (770) (facsimile)
 (770) (facsimile)") Charles Nash, III, M.D., F.A.C.P. Richard J. LoCicero, M.D. Anup K. Lahiry, M.D. Timothy M. Carey, M.D. Andrew Johnson, M.D. 725 Jesse Jewell Pkwy, Suite 390 Gainesville, GA 30501 (770) 297-5700 (770)
Charles Nash, III, M.D., F.A.C.P. Richard J. LoCicero, M.D. Anup K. Lahiry, M.D. Timothy M. Carey, M.D. Andrew Johnson, M.D. 725 Jesse Jewell Pkwy, Suite 390 Gainesville, GA 30501 (770) 297-5700 (770)
New Patient Intake Form
 501 Islington Street, Suite 2B Portsmouth, NH 03801 P: 603-610-8882 F: 603-463-0943 New Patient Intake Form Personal Information Today s Date Name Age DOB: Phone: H ( ) W ( ) Cell ( ) Preferred Home Work
501 Islington Street, Suite 2B Portsmouth, NH 03801 P: 603-610-8882 F: 603-463-0943 New Patient Intake Form Personal Information Today s Date Name Age DOB: Phone: H ( ) W ( ) Cell ( ) Preferred Home Work
Tips for Managing Celiac Disease. Robert Berger MD FRCPC Gastroenterology New Brunswick Internal Medicine Update April 22, 2016
 Tips for Managing Celiac Disease Robert Berger MD FRCPC Gastroenterology New Brunswick Internal Medicine Update April 22, 2016 Disclosures None relevant to this presentation Objectives Briefly review the
Tips for Managing Celiac Disease Robert Berger MD FRCPC Gastroenterology New Brunswick Internal Medicine Update April 22, 2016 Disclosures None relevant to this presentation Objectives Briefly review the
OhioHealth Orthopedic & Sports Medicine Physicians
 Page 1 of 6 OhioHealth Orthopedic & Sports Medicine Physicians 335 Glessner Avenue, Mansfield, Ohio 44903 PATIENT INTAKE ASSESSMENT OFFICE USE ONLY Fax to: OR Control 419-520-2831 For Joint Replacement
Page 1 of 6 OhioHealth Orthopedic & Sports Medicine Physicians 335 Glessner Avenue, Mansfield, Ohio 44903 PATIENT INTAKE ASSESSMENT OFFICE USE ONLY Fax to: OR Control 419-520-2831 For Joint Replacement
GUPTA SPORTS & SPINE CENTER
 GUPTA SPORTS & SPINE CENTER NEW PATIENT INFORMATION FORM -ORTHO Please print all information. Thank you for your cooperation. Patient Name: Date of Birth: _ Social Security # Address: City: _ State: Zip
GUPTA SPORTS & SPINE CENTER NEW PATIENT INFORMATION FORM -ORTHO Please print all information. Thank you for your cooperation. Patient Name: Date of Birth: _ Social Security # Address: City: _ State: Zip
Patient Interview Form
 Page 1 of 5 Physicians: D.F. Jackson, III, MD William D. McLaughlin, MD Robert P. Albares, MD Jeffrey J. Crittenden, MD Physicians: Samuel J. Tarwater, MD Travis J. Rutland, MD Ashwani Kapoor, MD Pathologist:
Page 1 of 5 Physicians: D.F. Jackson, III, MD William D. McLaughlin, MD Robert P. Albares, MD Jeffrey J. Crittenden, MD Physicians: Samuel J. Tarwater, MD Travis J. Rutland, MD Ashwani Kapoor, MD Pathologist:
New Patient Medical Questionnaire DATE:
 New Patient Medical Questionnaire DATE: Patient Name: DOB: AGE: Other Physicians: Who can we thank for referring you to our practice? Pharmacy Name & Location:` Phone # CHIEF COMPLAINT What problems are
New Patient Medical Questionnaire DATE: Patient Name: DOB: AGE: Other Physicians: Who can we thank for referring you to our practice? Pharmacy Name & Location:` Phone # CHIEF COMPLAINT What problems are
PATIENT INFORMATION. Are we currently seeing one of your family members at our practice, or have we previously? YES patient s name:
 PATIENT INFORMATION Date Name Address First Middle Last City State Zip Home # Cell # Check this box to authorize text messaging for confirming and reminders Email Check this box to authorize our office
PATIENT INFORMATION Date Name Address First Middle Last City State Zip Home # Cell # Check this box to authorize text messaging for confirming and reminders Email Check this box to authorize our office
New Patient History. Name: DOB: Sex: Date: If yes, give the name of the physician who did your evaluation or ordered your tests:
 New Patient History Name: DOB: Sex: Date: Chief Complaint: 1. Give a brief description of the problem you are seeking treatment for today: 2. Have you been evaluated for this problem or had any tests for
New Patient History Name: DOB: Sex: Date: Chief Complaint: 1. Give a brief description of the problem you are seeking treatment for today: 2. Have you been evaluated for this problem or had any tests for
Primary causes: Complement dysregulation (50% of non-shiga toxin-producing E. coli ) Secondary causes:
 Secondary causes:") General department INTRODUCTION The hemolytic uremic syndrome (HUS): microangiopathic hemolytic anemia, thrombocytopenia, and acute kidney injury One of the main causes of acute kidney injury in children
General department INTRODUCTION The hemolytic uremic syndrome (HUS): microangiopathic hemolytic anemia, thrombocytopenia, and acute kidney injury One of the main causes of acute kidney injury in children
Renal Remission and Hypertension Consultants PLLC
 Past Medical History. Please provide us with the list of your medical problems. Please indicate year of onset or when you became aware of it and year of resolution (if resolved) 1 2 3 4 5 6 7 8 9 10 11
Past Medical History. Please provide us with the list of your medical problems. Please indicate year of onset or when you became aware of it and year of resolution (if resolved) 1 2 3 4 5 6 7 8 9 10 11
Past Medical History. Chief Complaint: Patient Name: Appointment Date: Page 1
 Appointment Date: Page 1 Chief Complaint: (Please write reason, symptoms, condition or diagnosis that prompts your appointment) Past Medical History PERSONAL SKIN HISTORY YES NO Yes - Details Melanoma
Appointment Date: Page 1 Chief Complaint: (Please write reason, symptoms, condition or diagnosis that prompts your appointment) Past Medical History PERSONAL SKIN HISTORY YES NO Yes - Details Melanoma
Patient Interview Form
 Page 1 of 5 Gastroenterologists: D.F. Jackson, III, MD William D. McLaughlin, MD Robert P. Albares, MD Jeffrey J. Crittenden, MD Samuel J. Tarwater, MD Travis J. Rutland, MD Gastroenterologists: Marc L.
Page 1 of 5 Gastroenterologists: D.F. Jackson, III, MD William D. McLaughlin, MD Robert P. Albares, MD Jeffrey J. Crittenden, MD Samuel J. Tarwater, MD Travis J. Rutland, MD Gastroenterologists: Marc L.
MALE MEDICAL HISTORY FORM (please circle answers/complete blanks) rev 2/2014
 rev 2/2014") MALE MEDICAL HISTORY FORM (please circle answers/complete blanks) rev 2/2014 Name: Date of Birth: Today s Date: Where did you get healthcare before? May we request records? Y N (requires signed release)
MALE MEDICAL HISTORY FORM (please circle answers/complete blanks) rev 2/2014 Name: Date of Birth: Today s Date: Where did you get healthcare before? May we request records? Y N (requires signed release)
Name: Date: Street Address: Referring Physician: How long have you had your current problem?
 3851 Piper Street, Suite U464 Anchorage, AK 99508 p 907.339.4800 f 907.339.4801 New Patient Health Questionnaire Name: Date: Street Address: City: State Zip Sex: Age: Birth Date: Insurance: SS# Home Phone:
3851 Piper Street, Suite U464 Anchorage, AK 99508 p 907.339.4800 f 907.339.4801 New Patient Health Questionnaire Name: Date: Street Address: City: State Zip Sex: Age: Birth Date: Insurance: SS# Home Phone:
Bend Surgical Associates. Michael J. Mastrangelo, MD, FACS. Medication Name Dosage Frequency Medication Name Dosage Frequency
 Bend Surgical Associates Michael J. Mastrangelo, MD, FACS PATIENT NAME: DATE F BIRTH: MEDICATINS Please list all of your current prescription, non-prescription medications, vitamins, minerals, and supplements.
Bend Surgical Associates Michael J. Mastrangelo, MD, FACS PATIENT NAME: DATE F BIRTH: MEDICATINS Please list all of your current prescription, non-prescription medications, vitamins, minerals, and supplements.
DATE OF BIRTH: MELANOMA INTAKE
 MELANOMA INTAKE GENERAL INFORMATION How was your first diagnosed? (Check the diagnosis that describes your condition.) Melanoma Merkel Cell Carcinoma Squamous Cell Carcinoma Basal Cell Carcinoma Other
MELANOMA INTAKE GENERAL INFORMATION How was your first diagnosed? (Check the diagnosis that describes your condition.) Melanoma Merkel Cell Carcinoma Squamous Cell Carcinoma Basal Cell Carcinoma Other
Please list any medications you currently taking along with dosage and directions (including birth control, vitamins and OTC medications):
:") Name: DOB: Date of Appointment: Please list all doctors you currently see (Primary Care Physician and Specialists i.e. Cardiologist): Please list any medications you currently taking along with dosage
Name: DOB: Date of Appointment: Please list all doctors you currently see (Primary Care Physician and Specialists i.e. Cardiologist): Please list any medications you currently taking along with dosage
New Patient Questionnaire
 New Patient Questionnaire Name: Primary Care Physician: Date of Birth: / / Home Phone: ( ) Cell Phone: ( ) Why are you seeing a cardiologist? (please answer in detail) Have you ever seen a cardiologist
New Patient Questionnaire Name: Primary Care Physician: Date of Birth: / / Home Phone: ( ) Cell Phone: ( ) Why are you seeing a cardiologist? (please answer in detail) Have you ever seen a cardiologist
Occult GI Bleed. July 2015
 Occult GI Bleed July 2015 Occult GI Bleed Occult vs Obscure Occult positive FOB and/or IDA, but no evidence of visible blood loss to pt or physician Obscure GI bleed that persist/ recurs without obvious
Occult GI Bleed July 2015 Occult GI Bleed Occult vs Obscure Occult positive FOB and/or IDA, but no evidence of visible blood loss to pt or physician Obscure GI bleed that persist/ recurs without obvious
BROADWAY SPORTS & INTERNAL MEDICINE, P.S TH AVE NE SUITE 202 BELLEVUE, WA P: F:
 BROADWAY SPORTS & INTERNAL MEDICINE, P.S. 1600 116 TH AVE NE SUITE 202 BELLEVUE, WA 98004 P: 206 215-2288 F:206 215-2289 MEDICAL HISTORY QUESTIONNAIRE Date Name Date of Birth HT WT Current Medical Complaints
BROADWAY SPORTS & INTERNAL MEDICINE, P.S. 1600 116 TH AVE NE SUITE 202 BELLEVUE, WA 98004 P: 206 215-2288 F:206 215-2289 MEDICAL HISTORY QUESTIONNAIRE Date Name Date of Birth HT WT Current Medical Complaints
Bowel cancer risk in the under 50s. Greg Rubin Professor of General Practice and Primary Care
 Bowel cancer risk in the under 50s Greg Rubin Professor of General Practice and Primary Care Prevalence of GI problems in the consulting population Thompson et al, Gut 2000 Number of patients % of patients
Bowel cancer risk in the under 50s Greg Rubin Professor of General Practice and Primary Care Prevalence of GI problems in the consulting population Thompson et al, Gut 2000 Number of patients % of patients
Laboratory Methods for Diagnosing Celiac Disease. Vijay Kumar, PhD, FACB IMMCO Diagnostics, Inc. Buffalo, NY
 Laboratory Methods for Diagnosing Celiac Disease Vijay Kumar, PhD, FACB IMMCO Diagnostics, Inc. Buffalo, NY Prevalence of Celiac Disease Group With Symptoms Adults Children Associated Symptoms Chronic
Laboratory Methods for Diagnosing Celiac Disease Vijay Kumar, PhD, FACB IMMCO Diagnostics, Inc. Buffalo, NY Prevalence of Celiac Disease Group With Symptoms Adults Children Associated Symptoms Chronic
Celiac Disease. M. Nedim Ince, MD University of Iowa Hospital
 Celiac Disease M. Nedim Ince, MD University of Iowa Hospital Contents Cases Definition Etiopathogenesis Pathology Diagnosis Management of the disease Management of complications Case I Five year old boy
Celiac Disease M. Nedim Ince, MD University of Iowa Hospital Contents Cases Definition Etiopathogenesis Pathology Diagnosis Management of the disease Management of complications Case I Five year old boy
Name: Today s Date: Address: State, Zip Code
 New Patient Health History Questionnaire Name: Today s Date: Address: City State, Zip Code Email Address: Date of Birth: Home Telephone #: Cell Number: Work Number: Emergency Contact name & number: Referred
New Patient Health History Questionnaire Name: Today s Date: Address: City State, Zip Code Email Address: Date of Birth: Home Telephone #: Cell Number: Work Number: Emergency Contact name & number: Referred
LECOM Health Ophthalmology
 Patient Name: Date of Birth: New Patient Questionnaire Your answers will be used by your healthcare provider get an accurate history of your medical conditions and ocular concerns. If you are uncomfortable
Patient Name: Date of Birth: New Patient Questionnaire Your answers will be used by your healthcare provider get an accurate history of your medical conditions and ocular concerns. If you are uncomfortable
Adams Memorial Hospital Decatur, Indiana EXPLANATION OF LABORATORY TESTS
 Adams Memorial Hospital Decatur, Indiana EXPLANATION OF LABORATORY TESTS Your health is important to us! The test descriptions listed below are for educational purposes only. Laboratory test interpretation
Adams Memorial Hospital Decatur, Indiana EXPLANATION OF LABORATORY TESTS Your health is important to us! The test descriptions listed below are for educational purposes only. Laboratory test interpretation
Initial Consultation
 Today s Date: Initial Consultation Thank you for choosing Apollo Health and Wellness. Please take your time to fill out this form. It will help us to concentrate on areas of your health that need attention
Today s Date: Initial Consultation Thank you for choosing Apollo Health and Wellness. Please take your time to fill out this form. It will help us to concentrate on areas of your health that need attention
Patient Interview Form
 Page 1 of 5 Patient Interview Form Patient Information First Name: Date Of Birth: Last Name: Age: Email Please check one as your preferred email for communications Personal: Work: Race Select one or more
Page 1 of 5 Patient Interview Form Patient Information First Name: Date Of Birth: Last Name: Age: Email Please check one as your preferred email for communications Personal: Work: Race Select one or more
PATIENT INFORMATION (Please print all information) Date:
 Date:") 320 Lillington Ave Suite 101 Charlotte, NC 28204-3189 Phone: 704.362.4403 Fax: 704.362.4405 Please fill out the following form completely so that we may obtain the necessary information for our files and
320 Lillington Ave Suite 101 Charlotte, NC 28204-3189 Phone: 704.362.4403 Fax: 704.362.4405 Please fill out the following form completely so that we may obtain the necessary information for our files and
Patient Interview Form
 Patient Interview Form Patient Information First Name: MRN: Age: Last Name: Date Of Birth: tes: Contact Preference Email Telephone call/leave message Patient declines to specify Email Please check one
Patient Interview Form Patient Information First Name: MRN: Age: Last Name: Date Of Birth: tes: Contact Preference Email Telephone call/leave message Patient declines to specify Email Please check one
PATIENT HEALTH QUESTIONNAIRE Radiation Oncology
 REVIEWED DATE / INITIALS Safety: Yes No Are you at risk for falls? Do you have a Pacemaker? Females; Is there a possibility you may be pregnant? Allergies: Yes No If YES, please list medication allergies:
REVIEWED DATE / INITIALS Safety: Yes No Are you at risk for falls? Do you have a Pacemaker? Females; Is there a possibility you may be pregnant? Allergies: Yes No If YES, please list medication allergies:
Refractory celiac disease (RCD) KASSEM BARADA LEBANESE SOCIETY OF GASTROENTEROLOGY NOVEMBER, 2014
 KASSEM BARADA LEBANESE SOCIETY OF GASTROENTEROLOGY NOVEMBER, 2014") Refractory celiac disease (RCD) KASSEM BARADA LEBANESE SOCIETY OF GASTROENTEROLOGY NOVEMBER, 2014 Case scenario (1) A 49 year woman presents with intermittent watery diarrhea and bloating of two years
Refractory celiac disease (RCD) KASSEM BARADA LEBANESE SOCIETY OF GASTROENTEROLOGY NOVEMBER, 2014 Case scenario (1) A 49 year woman presents with intermittent watery diarrhea and bloating of two years
Patient Registration Form
 Patient Registration Form Name: Today s Date: FIRST MIDDLE LAST Home Address: City: State: Zip: Telephone: ( ) Birthdate: Age: Occupation: SSN: Employer: Years There: Employer s Address: City: State: Zip:
Patient Registration Form Name: Today s Date: FIRST MIDDLE LAST Home Address: City: State: Zip: Telephone: ( ) Birthdate: Age: Occupation: SSN: Employer: Years There: Employer s Address: City: State: Zip:
Lower Gastrointestinal Tract KNH 406
 Lower Gastrointestinal Tract KNH 406 Lower GI Tract A&P Small Intestine Anatomy Duodenum, jejunum, ileum Maximum surface area for digestion and absorption Specialized enterocytes from stem cells of crypts
Lower Gastrointestinal Tract KNH 406 Lower GI Tract A&P Small Intestine Anatomy Duodenum, jejunum, ileum Maximum surface area for digestion and absorption Specialized enterocytes from stem cells of crypts
Adult Health History
 Patient Name Date of Birth Adult Health History This form will assist us in obtaining a complete medical history and health record on you. By completing this ahead of time it will also simply your visit
Patient Name Date of Birth Adult Health History This form will assist us in obtaining a complete medical history and health record on you. By completing this ahead of time it will also simply your visit
MCKAY UROLOGY LINCOLNTON OFFICE PATIENT HISTORY FORM
 Patient name: MRN #: Current Medications (prescription and over the counter medications including vitamins, herbs, aspirin, antacids, injectables, hormones and birth control medication) If you brought
Patient name: MRN #: Current Medications (prescription and over the counter medications including vitamins, herbs, aspirin, antacids, injectables, hormones and birth control medication) If you brought
Health Questionnaire
 Patient Name Date of Birth Thank you for choosing Southern Cancer Center for your care. To help us best prepare for your appointment, please complete this form and bring it to your appointment. If you
Patient Name Date of Birth Thank you for choosing Southern Cancer Center for your care. To help us best prepare for your appointment, please complete this form and bring it to your appointment. If you
DOB: / / Please list the names and telephone numbers of the other physicians involved in your care: Name Specialty Phone Address Receive Report (Y/N)
") Medical History: Patient: DOB: / / Please list the names and telephone numbers of the other physicians involved in your care: Name Specialty Phone Address Receive Report (Y/N) List the names of prescription
Medical History: Patient: DOB: / / Please list the names and telephone numbers of the other physicians involved in your care: Name Specialty Phone Address Receive Report (Y/N) List the names of prescription
Interventional Pain Medicine. P. Tennent Slack, M.D. Dr. Greg Jackson, M.D. Ben Fleming, PA-C
 Interventional Pain Medicine P. Tennent Slack, M.D. Dr. Greg Jackson, M.D. Ben Fleming, PA-C Gainesville Braselton Medical Park 1, Suite 300 Medical Plaza B, Suite 402 1315 Jesse Jewell Parkway 1404 River
Interventional Pain Medicine P. Tennent Slack, M.D. Dr. Greg Jackson, M.D. Ben Fleming, PA-C Gainesville Braselton Medical Park 1, Suite 300 Medical Plaza B, Suite 402 1315 Jesse Jewell Parkway 1404 River
MONTEFIORE MEDICAL CENTER TRANSPLANT PROGRAM LIVING DONOR EVALUATION FORM History Questionnaire
 MONTEFIORE MEDICAL CENTER TRANSPLANT PROGRAM LIVING DONOR EVALUATION FORM History Questionnaire Donor s Name: Today s Date: Social Security #: Date of Birth Age Sex Address: Telephone #: (home) (work)
MONTEFIORE MEDICAL CENTER TRANSPLANT PROGRAM LIVING DONOR EVALUATION FORM History Questionnaire Donor s Name: Today s Date: Social Security #: Date of Birth Age Sex Address: Telephone #: (home) (work)
CELIAC DISEASE. A Family Physician Perspective. Dr. Kanwal Brar BSc MD CCFP June 6, 2015
 CELIAC DISEASE A Family Physician Perspective Dr. Kanwal Brar BSc MD CCFP June 6, 2015 Conflict of interest: No conflicts of interest or medical disclosures pertaining to this talk Objectives: Through
CELIAC DISEASE A Family Physician Perspective Dr. Kanwal Brar BSc MD CCFP June 6, 2015 Conflict of interest: No conflicts of interest or medical disclosures pertaining to this talk Objectives: Through
Providence Medical Group
 Providence Medical Group To our valued patients: In order to provide you with our full attention when you come for an appointment, we would like to ask you to be aware of the following guidelines. Insurance
Providence Medical Group To our valued patients: In order to provide you with our full attention when you come for an appointment, we would like to ask you to be aware of the following guidelines. Insurance
HD CLINIC MEDICAL HISTORY FORM
 HD CLINIC MEDICAL HISTORY FORM Welcome to the HDSA Center of Excellence HD Clinic. Please take a few moments to answer the questions below as best as you can. If you need assistance, a caregiver/companion
HD CLINIC MEDICAL HISTORY FORM Welcome to the HDSA Center of Excellence HD Clinic. Please take a few moments to answer the questions below as best as you can. If you need assistance, a caregiver/companion
Questionnaire for Lipedema Patients
 Questionnaire for Lipedema Patients Name Date of diagnosis Date Name of physician making diagnosis Do you also have lymphedema? What areas of the body are affected? Outside of thighs Inner thighs Knees
Questionnaire for Lipedema Patients Name Date of diagnosis Date Name of physician making diagnosis Do you also have lymphedema? What areas of the body are affected? Outside of thighs Inner thighs Knees
Tuesday 10 th April 2018 Dr Rukhsana Hussain. Disclaimers apply:
 Tuesday 10 th April 2018 Dr Rukhsana Hussain What is Non-Coeliac Gluten Sensitivity (NCGS)? Symptoms Pathophysiology Diagnosis Treatment Summary NCGS is a condition in which consumption of gluten leads
Tuesday 10 th April 2018 Dr Rukhsana Hussain What is Non-Coeliac Gluten Sensitivity (NCGS)? Symptoms Pathophysiology Diagnosis Treatment Summary NCGS is a condition in which consumption of gluten leads
Columbus Oncology and Hematology Associates 810 Jasonway Ave. Columbus, OH 43214, Ph: , Fax:
 Columbus Oncology and Hematology Associates 810 Jasonway Ave. Columbus, OH 43214, www.coainc.cc Ph: 614.442.3130, Fax: 614.442.3145 Name (Last, First, Middle) Birth Date Age Social Security # Appointment
Columbus Oncology and Hematology Associates 810 Jasonway Ave. Columbus, OH 43214, www.coainc.cc Ph: 614.442.3130, Fax: 614.442.3145 Name (Last, First, Middle) Birth Date Age Social Security # Appointment
A Trip Through the GI Tract: Common GI Diseases and Complaints. Jennifer Curtis, MD
 A Trip Through the GI Tract: Common GI Diseases and Complaints Jennifer Curtis, MD Colon Cancer How does it develop? Most cancers arise from polyps Over time these can turn into cancer Combination of genetic
A Trip Through the GI Tract: Common GI Diseases and Complaints Jennifer Curtis, MD Colon Cancer How does it develop? Most cancers arise from polyps Over time these can turn into cancer Combination of genetic
Center for Advanced Wound Care New Patient Questionnaire Page 1 of 6
 Center for Advanced Wound Care New Patient Questionnaire Page 1 of 6 These questions are general screening questions designed to identify areas where additional attention may be required. Please bring
Center for Advanced Wound Care New Patient Questionnaire Page 1 of 6 These questions are general screening questions designed to identify areas where additional attention may be required. Please bring
PATIENT HEALTH QUESTIONNAIRE Radiation Oncology
 REVIEWED DATE / INITIALS Safety: Are you at risk for falls? Do you have a Pacemaker? Females; Is there a possibility you may be pregnant? Allergies: If YES, please list medication allergies: Do you have
REVIEWED DATE / INITIALS Safety: Are you at risk for falls? Do you have a Pacemaker? Females; Is there a possibility you may be pregnant? Allergies: If YES, please list medication allergies: Do you have
Chapter 14: Training in Radiology. DDSEP Chapter 1: Question 12
 DDSEP Chapter 1: Question 12 A 52-year-old white male presents for evaluation of sudden onset of abdominal pain and shoulder pain. His past medical history is notable for a history of coronary artery disease,
DDSEP Chapter 1: Question 12 A 52-year-old white male presents for evaluation of sudden onset of abdominal pain and shoulder pain. His past medical history is notable for a history of coronary artery disease,
Broward Oncology Associates, P.A. PATIENT INFORMATION
 NAME: BIRTHDATE: AGE: LOCAL ADDRESS (Street city state zip): HOME TELEPHONE# CELL # SOCIAL SECURITY #: - - SEX MARITAL STATUS WHAT IS YOUR HT? WHAT IS YOUR WT? EMPLOYER WORK# SPOUSE'S NAME SPOUSE'S EMPLOYER
NAME: BIRTHDATE: AGE: LOCAL ADDRESS (Street city state zip): HOME TELEPHONE# CELL # SOCIAL SECURITY #: - - SEX MARITAL STATUS WHAT IS YOUR HT? WHAT IS YOUR WT? EMPLOYER WORK# SPOUSE'S NAME SPOUSE'S EMPLOYER
Your treatment with XELJANZ
 Your treatment with XELJANZ (tofacitinib citrate) THIS BROCHURE HAS BEEN PRODUCED FOR PATIENTS WHO HAVE BEEN PRESCRIBED XELJANZ. BEFORE USING XELJANZ, PLEASE REVIEW THE PACKAGE LEAFLET FOR THIS MEDICINAL
Your treatment with XELJANZ (tofacitinib citrate) THIS BROCHURE HAS BEEN PRODUCED FOR PATIENTS WHO HAVE BEEN PRESCRIBED XELJANZ. BEFORE USING XELJANZ, PLEASE REVIEW THE PACKAGE LEAFLET FOR THIS MEDICINAL
Patient Interview Form
 Patient Interview Form Patient Information First Name: Date Of Birth: Last Name: Email Please check one as your preferred email for communications Personal: Work: Race Select one or more White Unknown
Patient Interview Form Patient Information First Name: Date Of Birth: Last Name: Email Please check one as your preferred email for communications Personal: Work: Race Select one or more White Unknown
Dear Mercy Cancer Center Radiation Oncology Patient
 Dear Mercy Cancer Center Radiation Oncology Patient Welcome to our Department. In order to complete our records, and enable our physicians to ensure that your questions are fully addressed, we appreciate
Dear Mercy Cancer Center Radiation Oncology Patient Welcome to our Department. In order to complete our records, and enable our physicians to ensure that your questions are fully addressed, we appreciate
Patient Name: Date of Birth: Preferred Pharmacy: (name/location/phone #)
") Patient Name: Date of Birth: Referring Doctor: Primary Care Dr: Preferred Pharmacy: (name/location/phone #) CURRENT MEDICATIONS: Please list all Medication Dose Frequency 1 2 3 4 5 6 7 8 9 10 11 12 13
Patient Name: Date of Birth: Referring Doctor: Primary Care Dr: Preferred Pharmacy: (name/location/phone #) CURRENT MEDICATIONS: Please list all Medication Dose Frequency 1 2 3 4 5 6 7 8 9 10 11 12 13
New Patient Information
 Geoffrey G Glidden MD PA New Patient Information Name Address City/State/Zip Cell Phone Home Phone DL# SSN# Age of Birth Sex: Male / Female Your employer Occupation Work Phone E-Mail Referring Physician
Geoffrey G Glidden MD PA New Patient Information Name Address City/State/Zip Cell Phone Home Phone DL# SSN# Age of Birth Sex: Male / Female Your employer Occupation Work Phone E-Mail Referring Physician
Lecture 8 Cardiovascular Health Lecture 8 1. Introduction 2. Cardiovascular Health 3. Stroke 4. Contributing Factors
 Lecture 8 Cardiovascular Health 1 Lecture 8 1. Introduction 2. Cardiovascular Health 3. Stroke 4. Contributing Factors 1 Human Health: What s Killing Us? Health in America Health is the U.S Average life
Lecture 8 Cardiovascular Health 1 Lecture 8 1. Introduction 2. Cardiovascular Health 3. Stroke 4. Contributing Factors 1 Human Health: What s Killing Us? Health in America Health is the U.S Average life
Health History Questionaire
 Patient DOB: Patient Name: Date: Health History Questionaire Who referred your consultation? If no one referred you, how did you hear about us? Who is your primary care physician? Have you ever seen a
Patient DOB: Patient Name: Date: Health History Questionaire Who referred your consultation? If no one referred you, how did you hear about us? Who is your primary care physician? Have you ever seen a
Referring Physician/Therapist. Primary Care Physician. Reason for Visit
 Name Age Date Referring Physician/Therapist Primary Care Physician Reason for Visit If you are having pain, use the diagram and symbols to indicate where it is. Ache: AAA Burning:XXX Numbness:OOO Pins/Needles:
Name Age Date Referring Physician/Therapist Primary Care Physician Reason for Visit If you are having pain, use the diagram and symbols to indicate where it is. Ache: AAA Burning:XXX Numbness:OOO Pins/Needles:
New Patient Questionnaire. Name DOB Date
 Medical History (This refers to medical problems that have already been diagnosed or treated. Please explain how this is treated, such as diet, medication, surgery, etc.) Condition Abnormal Pap smear Alcohol
Medical History (This refers to medical problems that have already been diagnosed or treated. Please explain how this is treated, such as diet, medication, surgery, etc.) Condition Abnormal Pap smear Alcohol
58 year old male complaining of 3-week history of increasing epigastric pain
 Peptic Ulcer Disease 58 year old male complaining of 3-week history of increasing epigastric pain Has had dyspepsia in the past for which he took Tums, but this is much worse and only partially relieved
Peptic Ulcer Disease 58 year old male complaining of 3-week history of increasing epigastric pain Has had dyspepsia in the past for which he took Tums, but this is much worse and only partially relieved