Introduction to Fetal Medicine. Lloyd R. Feit M.D. Associate Professor of Pediatrics Warren Alpert Medical School Brown University
|
|
|
- Christal Todd
- 5 years ago
- Views:
Transcription
1 Associate Professor of Pediatrics Warren Alpert Medical School Brown University
2 Fetal Cardiology Important in evaluation of high risk pregnancies. Information obtainable in > 95% of patients attempted. Allows for assessment of developmental cardiovascular physiology. Best clinical management depends on strong collaboration between subspecialists: perinatology genetics obstetrics neonatology ultrasonography pediatric cardiology internal medicine cardiac surgery
3 Fetal Circulation Placenta: low resistance circuit, organ of gas exchange, nutrient supply. Lungs: high resistance, non-functional, breathing important. Brain development is primary! Shunt pathways: Foramen ovale Ductus arteriosus Ductus venosus
 lungs")
4 Fetal Circulation Shunt Pathways: Ductus venosus: bypasses fetal liver Foramen ovale: R-L shunt across atrial septum Ductus arteriosus: bypasses high resistance (nonaerated) lungs
5 Transitional circulation Separation from low resistance placenta >> increased SVR low flow constricts ductus venosus First breath expands lungs >> decreased PVR increased pulmonary blood flow increased LA pressure closes PFO increased PaO2 >> constricts PDA
6 Fetal Echocardiography First observations of normal cardiac anatomy utilizing M- mode by Winsberg in Prenatal diagnosis of congenital heart disease by Kleinman, et al (and others) in High resolution cross-sectional scanners allow real-time directed utilization of: Two-dimensional imaging Pulsed & color flow Doppler M-mode
7 Diagnostic capabilities Cardiac ultrastructure 2 - dimensional, M - mode Vascular & intracardiac flow patterns Color, pulsed & continuous wave Doppler Cardiac rate and rhythm M mode & Doppler evaluation of electromechanical events. Myocardial function
8 Indications Fetal factors: IUGR Arrhythmia Hydrops fetalis Abnormal genetic screen Extracardiac anomalies nuchal translucency Diminished fetal movement Abnormal 4 - chamber screen
9 Indications Maternal factors: CHD (risk increases from ~1% to 4-5%) Poly/oligo - hydramnios Diabetes Collagen vascular disease Teratogen exposure Pre - eclampsia Advanced parental age
10 Indications Familial factors: CHD Genetic syndromes; Marfan Noonan Ellis van Crevald Hypertrophic cardiomyopathy Tuberous sclerosis
11 Fetal echocardiography No known adverse fetal effects Optimal timing wks Diagnosis possible at wks No uniformly accepted approach 4-chamber screen Addition of great vessels/outflow tracts Association with increased nuchal translucency (>99%ile >>> 3-5x risk of CHD)
12 Technique Establish fetal lie, complete level II. Cardiac & abdominal situs. Fetal heart rate and rhythm. Four chamber view. (92% sensitivity, 99% specificity) Segmental approach for venous and arterial connections and Doppler flow patterns: Systemic, pulmonary veins AV valves LV, RV outflow tracts Aortic, ductal arch

13 Four Chamber view


14 LV outflow tract


15 RV outflow tract

16 Systemic venous confluence

17 Aortic and Ductal arch


18 Aortic arch

19 Doppler flow patterns

20 Sinus rhythm Doppler


21 AV Canal Defect
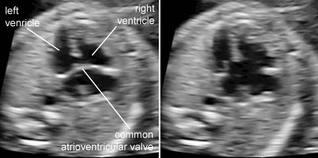
22 AV Canal

23 Complex single ventricle (Dbl inlet/dbl outlet LV)

24 Complex single ventricle

25 TV dysplasia
26 Intracardiac rhabdomyoma
27 Arrhythmias Isolated extrasystoles Sustained arrhythmia: Any irregular rhythm, or any regular rhythm outside the normal fetal range of bpm, and not associated with uterine contraction.
28 Arrhythmias Indications for Fetal Arrhythmia Evaluation Suspected arrhythmia Non-immune hydrops fetalis (esp heterotaxy syndromes, corrected transposition) Fetal cardiac tumors Maternal collagen vascular disease Maternal medications/toxins that may predispose fetus to arrhythmia
29 Arrhythmias Isolated extrasystoles (benign) Tachycardia: SVT: > 90 % reentry (AVRT) Atrial flutter / fibrillation Ventricular tachycardia (rare) Bradycardia: High degree AV block associated with collagen vascular disease or complex CHD. Hydrops indicates poor prognosis.
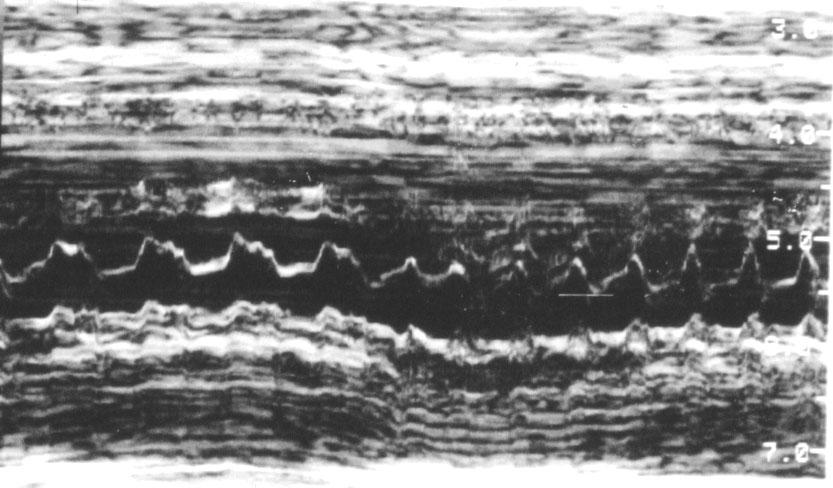
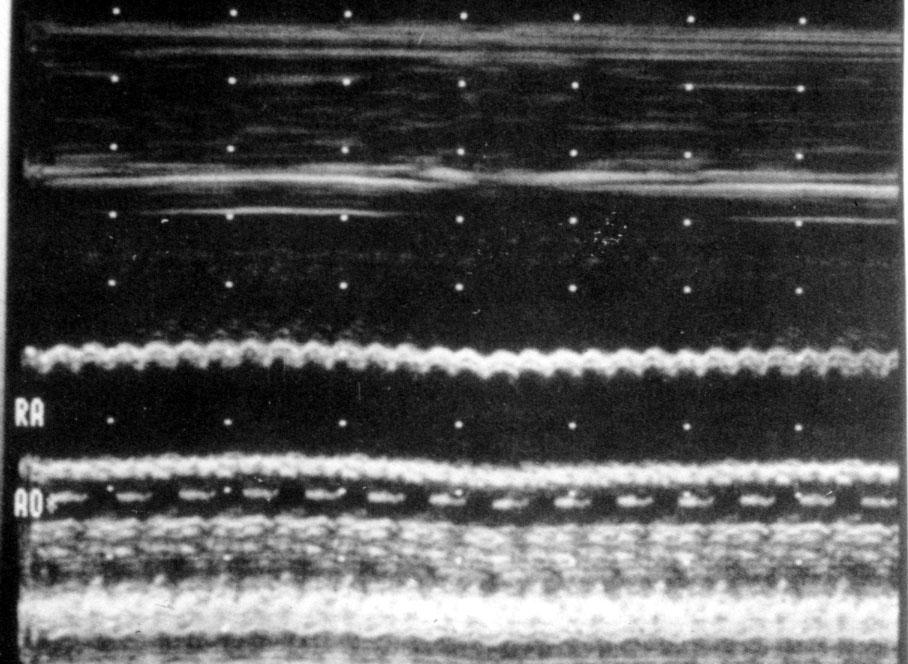
30 Arrhythmias: M-mode SVT Atrial Flutter
31 Arrhythmias Progression of fetal CHF: atrial dilation (AV valve regurgitation) liver engorgement peripheral edema &/or ascites polyhydramnios fetal demise
32 Therapeutics Consideration for intervention must incorporate: in utero and postnatal natural history of lesion. risk / benefit for both mother and fetus. Arrhythmias: sustained vs intermittent transplacental (oral, IV) vs direct (PUBS) ** knowledge of electrophysiologic mechanism & typical postnatal response.
33 Therapeutics Tachycardias: SVT digoxin, type IA (procainamide, quinidine) type IC (flecainide) Atrial fib / flutter - digoxin, type IA, type III (amiodarone) VT - type IB (lidocaine, mexilitene, amiodarone) Bradycardia / Heart Block: Steroids no clear benefit, may limit progression Plasmapheresis, pacemaker??? Early delivery?!?
34 Does antenatal diagnosis make a difference? Obstetric decisions: parental reassurance (~95% for follow-up patients) amniocentesis, genetic counseling (20-38 % aneuploid) search for other anomalies frequency of follow up? termination time, mode, place of delivery
35 Does antenatal diagnosis make a difference? Neonatal decisions: appropriate facility, staff need for prostaglandin infusion avoid circulatory collapse in duct dependant lesions very difficult to prove/quantitate survival or outcomes benefit except for: HLHS Coarctation TGA Counseling!!!
36 Does antenatal diagnosis make a difference? Parental counseling Know local surgical results Inter-stage morbidity and mortality Long term outcomes Physical Neurologic Family dynamics Potential termination Allows families to prepare for challenges of altered normality
37 Fetal intervention Fetal interventional catheterization: 1991-Maxwell, et al in utero balloon aortic valvuloplasty. 4 patients, 5 attempts; 1 survivor Marshall, et al. 20 attempts for patients with fetal aortic stenosis, 14 technically successful 3 HLHS prevented?? 12 HLHS 5 demise: 3 in utero, 1 previable, 1 termination


38 Fetal Intervention



39 Fetal Intervention
 ALL need postnatal cardiac interventions HLHS w/intact atrial septum 25 attempts (~10% fetal demise) ~95% technical success")
40 Fetal intervention Critical aortic stenosis / HLHS >120 attempts (~10% fetal demise) ~ 80% technically successful ~ 33% get to 2 ventricle repair! - high rate of EFE (endocardial fibro-elastosis) ALL need postnatal cardiac interventions HLHS w/intact atrial septum 25 attempts (~10% fetal demise) ~95% technical success ~50% avoid emergent cath at birth
41 Future Directions Results are likely to improve Better patient selection, timing Pretty clear results for predicting AS > HLHS Improved instrumentation Robotics? Experience - - learning curve Ethical issues Can a pregnant woman really give informed consent?? What about dad?? Natural history of any disease process MUST be well understood before undertaking any fetal intervention!!
42 Two ventricles are better than one! Human subtlety will never devise an invention more beautiful, more simple or more direct than does Nature, because in her inventions, nothing is lacking and nothing is superfluous. Leonardo da Vinci
Systematic approach to Fetal Echocardiography. Objectives. Introduction 11/2/2015
 Systematic approach to Fetal Echocardiography. Pediatric Echocardiography Conference, JCMCH November 7, 2015 Rajani Anand Objectives Fetal cardiology pre-test Introduction Embryology and Physiology of
Systematic approach to Fetal Echocardiography. Pediatric Echocardiography Conference, JCMCH November 7, 2015 Rajani Anand Objectives Fetal cardiology pre-test Introduction Embryology and Physiology of
Before we are Born: Fetal Diagnosis of Congenital Heart Disease
 Before we are Born: Fetal Diagnosis of Congenital Heart Disease Mohamed Sulaiman, MD Pediatric cardiologist Kidsheart: American Fetal & Children's Heart Center Dubai Healthcare City, Dubai-UAE First Pediatric
Before we are Born: Fetal Diagnosis of Congenital Heart Disease Mohamed Sulaiman, MD Pediatric cardiologist Kidsheart: American Fetal & Children's Heart Center Dubai Healthcare City, Dubai-UAE First Pediatric
Introduction. Pediatric Cardiology. General Appearance. Tools of Assessment. Auscultation. Vital Signs
 Introduction Pediatric Cardiology An introduction to the pediatric patient with heart disease: M-III Lecture Douglas R. Allen, M.D. Assistant Professor and Director of Community Pediatric Cardiology at
Introduction Pediatric Cardiology An introduction to the pediatric patient with heart disease: M-III Lecture Douglas R. Allen, M.D. Assistant Professor and Director of Community Pediatric Cardiology at
Heart and Soul Evaluation of the Fetal Heart
 Heart and Soul Evaluation of the Fetal Heart Ivana M. Vettraino, M.D., M.B.A. Clinical Associate Professor, Michigan State University College of Human Medicine Objectives Review the embryology of the formation
Heart and Soul Evaluation of the Fetal Heart Ivana M. Vettraino, M.D., M.B.A. Clinical Associate Professor, Michigan State University College of Human Medicine Objectives Review the embryology of the formation
Heart and Lungs. LUNG Coronal section demonstrates relationship of pulmonary parenchyma to heart and chest wall.
 Heart and Lungs Normal Sonographic Anatomy THORAX Axial and coronal sections demonstrate integrity of thorax, fetal breathing movements, and overall size and shape. LUNG Coronal section demonstrates relationship
Heart and Lungs Normal Sonographic Anatomy THORAX Axial and coronal sections demonstrate integrity of thorax, fetal breathing movements, and overall size and shape. LUNG Coronal section demonstrates relationship
The Fetal Cardiology Program
 The Fetal Cardiology Program at Texas Children s Fetal Center About the program Since the 1980s, Texas Children s Fetal Cardiology Program has provided comprehensive fetal cardiac care to expecting families
The Fetal Cardiology Program at Texas Children s Fetal Center About the program Since the 1980s, Texas Children s Fetal Cardiology Program has provided comprehensive fetal cardiac care to expecting families
How Does Imaging Inform Fetal Cardiovascular Treatment?
 How Does Imaging Inform Fetal Cardiovascular Treatment? Edgar Jaeggi, MD Head, Fetal Cardiac Program Labatt Family Heart Center Department of Pediatrics The Hospital for Sick Children University of Toronto
How Does Imaging Inform Fetal Cardiovascular Treatment? Edgar Jaeggi, MD Head, Fetal Cardiac Program Labatt Family Heart Center Department of Pediatrics The Hospital for Sick Children University of Toronto
Assessment of fetal heart function and rhythm
 Assessment of fetal heart function and rhythm The fetal myocardium Early Gestation Myofibrils 30% of myocytes Less sarcoplasmic reticula Late Gestation Myofibrils 60% of myocytes Increased force per unit
Assessment of fetal heart function and rhythm The fetal myocardium Early Gestation Myofibrils 30% of myocytes Less sarcoplasmic reticula Late Gestation Myofibrils 60% of myocytes Increased force per unit
Pediatric Echocardiography Examination Content Outline
 Pediatric Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 Anatomy and Physiology Normal Anatomy and Physiology 10% 2 Abnormal Pathology and Pathophysiology
Pediatric Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 Anatomy and Physiology Normal Anatomy and Physiology 10% 2 Abnormal Pathology and Pathophysiology
Screening for Critical Congenital Heart Disease
 Screening for Critical Congenital Heart Disease Caroline K. Lee, MD Pediatric Cardiology Disclosures I have no relevant financial relationships or conflicts of interest 1 Most Common Birth Defect Most
Screening for Critical Congenital Heart Disease Caroline K. Lee, MD Pediatric Cardiology Disclosures I have no relevant financial relationships or conflicts of interest 1 Most Common Birth Defect Most
The Physiology of the Fetal Cardiovascular System
 The Physiology of the Fetal Cardiovascular System Jeff Vergales, MD, MS Department of Pediatrics Division of Pediatric Cardiology jvergales@virginia.edu Disclosures I serve as the medical director for
The Physiology of the Fetal Cardiovascular System Jeff Vergales, MD, MS Department of Pediatrics Division of Pediatric Cardiology jvergales@virginia.edu Disclosures I serve as the medical director for
Diagnosis of Congenital Cardiac Defects Between 11 and 14 Weeks Gestation in High-Risk Patients
 Article Diagnosis of Congenital Cardiac Defects Between 11 and 14 Weeks Gestation in High-Risk Patients Zeev Weiner, MD, Abraham Lorber, MD, Eliezer Shalev, MD Objective. To examine the feasibility of
Article Diagnosis of Congenital Cardiac Defects Between 11 and 14 Weeks Gestation in High-Risk Patients Zeev Weiner, MD, Abraham Lorber, MD, Eliezer Shalev, MD Objective. To examine the feasibility of
Foetal Cardiology: How to predict perinatal problems. Prof. I.Witters Prof.M.Gewillig UZ Leuven
 Foetal Cardiology: How to predict perinatal problems Prof. I.Witters Prof.M.Gewillig UZ Leuven Cardiopathies Incidence : 8-12 / 1000 births ( 1% ) Most frequent - Ventricle Septum Defect 20% - Atrium Septum
Foetal Cardiology: How to predict perinatal problems Prof. I.Witters Prof.M.Gewillig UZ Leuven Cardiopathies Incidence : 8-12 / 1000 births ( 1% ) Most frequent - Ventricle Septum Defect 20% - Atrium Septum
Anatomy & Physiology
 1 Anatomy & Physiology Heart is divided into four chambers, two atrias & two ventricles. Atrioventricular valves (tricuspid & mitral) separate the atria from ventricles. they open & close to control flow
1 Anatomy & Physiology Heart is divided into four chambers, two atrias & two ventricles. Atrioventricular valves (tricuspid & mitral) separate the atria from ventricles. they open & close to control flow
Index. cardiology.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A ACHD. See Adult congenital heart disease (ACHD) Adult congenital heart disease (ACHD), 503 512 across life span prevalence of, 504 506
Index Note: Page numbers of article titles are in boldface type. A ACHD. See Adult congenital heart disease (ACHD) Adult congenital heart disease (ACHD), 503 512 across life span prevalence of, 504 506
ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT
 ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT Karen Stout, MD, FACC Divisions of Cardiology University of Washington Medical Center Seattle Children s Hospital NO DISCLOSURES
ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT Karen Stout, MD, FACC Divisions of Cardiology University of Washington Medical Center Seattle Children s Hospital NO DISCLOSURES
Congenital Heart Disease: Physiology and Common Defects
 Congenital Heart Disease: Physiology and Common Defects Jamie S. Sutherell, M.D, M.Ed. Associate Professor, Pediatrics Division of Cardiology Director, Medical Student Education in Pediatrics Director,
Congenital Heart Disease: Physiology and Common Defects Jamie S. Sutherell, M.D, M.Ed. Associate Professor, Pediatrics Division of Cardiology Director, Medical Student Education in Pediatrics Director,
Cardiac Catheterization Cases Primary Cardiac Diagnoses Facility 12 month period from to PRIMARY DIAGNOSES (one per patient)
") PRIMARY DIAGNOSES (one per patient) Septal Defects ASD (Atrial Septal Defect) PFO (Patent Foramen Ovale) ASD, Secundum ASD, Sinus venosus ASD, Coronary sinus ASD, Common atrium (single atrium) VSD (Ventricular
PRIMARY DIAGNOSES (one per patient) Septal Defects ASD (Atrial Septal Defect) PFO (Patent Foramen Ovale) ASD, Secundum ASD, Sinus venosus ASD, Coronary sinus ASD, Common atrium (single atrium) VSD (Ventricular
Supraventricular Tachycardia: From Fetus to Adult. Mohamed Hamdan, MD
 Supraventricular Tachycardia: From Fetus to Adult Mohamed Hamdan, MD Learning Objectives Define type of SVT by age Describe clinical approach Describe prenatal and postnatal management of SVT 2 SVT Across
Supraventricular Tachycardia: From Fetus to Adult Mohamed Hamdan, MD Learning Objectives Define type of SVT by age Describe clinical approach Describe prenatal and postnatal management of SVT 2 SVT Across
Congenital Heart Defects
 Normal Heart Congenital Heart Defects 1. Patent Ductus Arteriosus The ductus arteriosus connects the main pulmonary artery to the aorta. In utero, it allows the blood leaving the right ventricle to bypass
Normal Heart Congenital Heart Defects 1. Patent Ductus Arteriosus The ductus arteriosus connects the main pulmonary artery to the aorta. In utero, it allows the blood leaving the right ventricle to bypass
Cardiac Intervention in Fetus. Gyeong-hee Yoo, M.D. Department of Pediatrics Soonchunhyang University Cheonan Hospital
 10 1111 Cardiac Intervention in Fetus Gyeong-hee Yoo, M.D. Department of Pediatrics Soonchunhyang University Cheonan Hospital Fetal echocardiography Serial f/u intrauterine course of disease Cardiac anomaly
10 1111 Cardiac Intervention in Fetus Gyeong-hee Yoo, M.D. Department of Pediatrics Soonchunhyang University Cheonan Hospital Fetal echocardiography Serial f/u intrauterine course of disease Cardiac anomaly
ISOLATED ANOMALOUS DEVELOPMENT OF MYOCARDIUM DURING FETAL LIFE: EXPERIENCE OF OUR CENTRE
 Azienda Ospedaliera Universitaria Integrata Verona ISOLATED ANOMALOUS DEVELOPMENT OF MYOCARDIUM DURING FETAL LIFE: EXPERIENCE OF OUR CENTRE C.Sandrini *, L.Rossetti *, M.Rebonato *, M.A.Prioli *, F.Bettinazzi,
Azienda Ospedaliera Universitaria Integrata Verona ISOLATED ANOMALOUS DEVELOPMENT OF MYOCARDIUM DURING FETAL LIFE: EXPERIENCE OF OUR CENTRE C.Sandrini *, L.Rossetti *, M.Rebonato *, M.A.Prioli *, F.Bettinazzi,
Failing right ventricle
 Failing right ventricle U. Herberg 1, U. Gembruch 2 1 Pediatric Cardiology, 2 Prenatal Diagnostics and Fetal Therapy, University of Bonn, Germany Prenatal Physiology Right ventricle dominant ventricle
Failing right ventricle U. Herberg 1, U. Gembruch 2 1 Pediatric Cardiology, 2 Prenatal Diagnostics and Fetal Therapy, University of Bonn, Germany Prenatal Physiology Right ventricle dominant ventricle
Fetal Rhythm and Blues
 Fetal Rhythm and Blues John Cotton, MD Professor of Pediatrics Division of Pediatric Cardiology Director, Fetal Cardiology Program UNC Chapel Hill, School of Medicine Objectives To review methods used
Fetal Rhythm and Blues John Cotton, MD Professor of Pediatrics Division of Pediatric Cardiology Director, Fetal Cardiology Program UNC Chapel Hill, School of Medicine Objectives To review methods used
COMPREHENSIVE EVALUATION OF FETAL HEART R. GOWDAMARAJAN MD
 COMPREHENSIVE EVALUATION OF FETAL HEART R. GOWDAMARAJAN MD Disclosure No Relevant Financial Relationships with Commercial Interests Fetal Echo: How to do it? Timing of Study -optimally between 22-24 weeks
COMPREHENSIVE EVALUATION OF FETAL HEART R. GOWDAMARAJAN MD Disclosure No Relevant Financial Relationships with Commercial Interests Fetal Echo: How to do it? Timing of Study -optimally between 22-24 weeks
Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition
 Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition Table of Contents Volume 1 Chapter 1: Cardiovascular Anatomy and Physiology Basic Cardiac
Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition Table of Contents Volume 1 Chapter 1: Cardiovascular Anatomy and Physiology Basic Cardiac
Echocardiography in Adult Congenital Heart Disease
 Echocardiography in Adult Congenital Heart Disease Michael Vogel Kinderherz-Praxis München CHD missed in childhood Subsequent lesions after repaired CHD Follow-up of cyanotic heart disease CHD missed in
Echocardiography in Adult Congenital Heart Disease Michael Vogel Kinderherz-Praxis München CHD missed in childhood Subsequent lesions after repaired CHD Follow-up of cyanotic heart disease CHD missed in
Adult Echocardiography Examination Content Outline
 Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
PRACTICAL GUIDE TO FETAL ECHOCARDIOGRAPHY IC Huggon and LD Allan
 PRACTICAL GUIDE TO FETAL ECHOCARDIOGRAPHY IC Huggon and LD Allan Fetal Cardiology Unit, Harris Birthright Research Centre for Fetal Medicine, King's College Hospital, London, UK IMPORTANCE OF PRENATAL
PRACTICAL GUIDE TO FETAL ECHOCARDIOGRAPHY IC Huggon and LD Allan Fetal Cardiology Unit, Harris Birthright Research Centre for Fetal Medicine, King's College Hospital, London, UK IMPORTANCE OF PRENATAL
Pregnancy and Heart Disease. Shilpa Kshatriya, MD, FACC Heartland Cardiology, PA
 Pregnancy and Heart Disease Shilpa Kshatriya, MD, FACC Heartland Cardiology, PA Pregnancy and the Heart 2 % of pregnancies involve maternal CV disease CV disease does not preclude pregnancy but poses risk
Pregnancy and Heart Disease Shilpa Kshatriya, MD, FACC Heartland Cardiology, PA Pregnancy and the Heart 2 % of pregnancies involve maternal CV disease CV disease does not preclude pregnancy but poses risk
Deborah Kozik, DO Assistant Professor Division of Cardiothoracic Surgery s present: Early Repair Era
 Deborah Kozik, DO Assistant Professor Division of Cardiothoracic Surgery 1954 1960: Experimental Era 1960 s 1980 s: Palliation Era 1980 s present: Early Repair Era 2010 2030 s: Fetal Interventions Hybrid
Deborah Kozik, DO Assistant Professor Division of Cardiothoracic Surgery 1954 1960: Experimental Era 1960 s 1980 s: Palliation Era 1980 s present: Early Repair Era 2010 2030 s: Fetal Interventions Hybrid
ULTRASOUND OF THE FETAL HEART
 ULTRASOUND OF THE FETAL HEART Cameron A. Manbeian, MD Disclosure Statement Today s faculty: Cameron Manbeian, MD does not have any relevant financial relationships with commercial interests or affiliations
ULTRASOUND OF THE FETAL HEART Cameron A. Manbeian, MD Disclosure Statement Today s faculty: Cameron Manbeian, MD does not have any relevant financial relationships with commercial interests or affiliations
Adult Congenital Heart Disease: What All Echocardiographers Should Know Sharon L. Roble, MD, FACC Echo Hawaii 2016
 1 Adult Congenital Heart Disease: What All Echocardiographers Should Know Sharon L. Roble, MD, FACC Echo Hawaii 2016 DISCLOSURES I have no disclosures relevant to today s talk 2 Why should all echocardiographers
1 Adult Congenital Heart Disease: What All Echocardiographers Should Know Sharon L. Roble, MD, FACC Echo Hawaii 2016 DISCLOSURES I have no disclosures relevant to today s talk 2 Why should all echocardiographers
SWISS SOCIETY OF NEONATOLOGY. Prenatal closure of the ductus arteriosus
 SWISS SOCIETY OF NEONATOLOGY Prenatal closure of the ductus arteriosus March 2007 Leone A, Fasnacht M, Beinder E, Arlettaz R, Neonatal Intensive Care Unit (LA, AR), University Hospital Zurich, Cardiology
SWISS SOCIETY OF NEONATOLOGY Prenatal closure of the ductus arteriosus March 2007 Leone A, Fasnacht M, Beinder E, Arlettaz R, Neonatal Intensive Care Unit (LA, AR), University Hospital Zurich, Cardiology
Heart Development and Congenital Heart Disease
 Heart Development and Congenital Heart Disease Sally Dunwoodie s.dunwoodie@victorchang.edu.au Developmental and Stem Cell Biology Division Victor Chang Cardiac Research Institute for the heart of Australia...
Heart Development and Congenital Heart Disease Sally Dunwoodie s.dunwoodie@victorchang.edu.au Developmental and Stem Cell Biology Division Victor Chang Cardiac Research Institute for the heart of Australia...
"Lecture Index. 1) Heart Progenitors. 2) Cardiac Tube Formation. 3) Valvulogenesis and Chamber Formation. 4) Epicardium Development.
 Heart Progenitors. 2) Cardiac Tube Formation. 3) Valvulogenesis and Chamber Formation. 4) Epicardium Development.") "Lecture Index 1) Heart Progenitors. 2) Cardiac Tube Formation. 3) Valvulogenesis and Chamber Formation. 4) Epicardium Development. 5) Septation and Maturation. 6) Changes in Blood Flow during Development.
"Lecture Index 1) Heart Progenitors. 2) Cardiac Tube Formation. 3) Valvulogenesis and Chamber Formation. 4) Epicardium Development. 5) Septation and Maturation. 6) Changes in Blood Flow during Development.
The sinus venosus represent the venous end of the heart It receives 3 veins: 1- Common cardinal vein body wall 2- Umbilical vein from placenta 3-
 1 2 The sinus venosus represent the venous end of the heart It receives 3 veins: 1- Common cardinal vein body wall 2- Umbilical vein from placenta 3- Vitelline vein from yolk sac 3 However!!!!! The left
1 2 The sinus venosus represent the venous end of the heart It receives 3 veins: 1- Common cardinal vein body wall 2- Umbilical vein from placenta 3- Vitelline vein from yolk sac 3 However!!!!! The left
CONGENITAL HEART DISEASE (CHD)
") CONGENITAL HEART DISEASE (CHD) DEFINITION It is the result of a structural or functional abnormality of the cardiovascular system at birth GENERAL FEATURES OF CHD Structural defects due to specific disturbance
CONGENITAL HEART DISEASE (CHD) DEFINITION It is the result of a structural or functional abnormality of the cardiovascular system at birth GENERAL FEATURES OF CHD Structural defects due to specific disturbance
Doppler Echocardiography in the Diagnosis and Management of Persistent Fetal Arrhythmias
 1386 JACC Vol 7. No 6 June 19X6 I3Xh-91 Doppler Echocardiography in the Diagnosis and Management of Persistent Fetal Arrhythmias JANETTE F. STRASBURGER, MD, JAMES C. HUHTA, MD, FACC, ROBERT J. CARPENTER,
1386 JACC Vol 7. No 6 June 19X6 I3Xh-91 Doppler Echocardiography in the Diagnosis and Management of Persistent Fetal Arrhythmias JANETTE F. STRASBURGER, MD, JAMES C. HUHTA, MD, FACC, ROBERT J. CARPENTER,
Appropriate Use Criteria for Initial Transthoracic Echocardiography in Outpatient Pediatric Cardiology (scores listed by Appropriate Use rating)
") Appropriate Use Criteria for Initial Transthoracic Echocardiography in Outpatient Pediatric Cardiology (scores listed by Appropriate Use rating) Table 1: Appropriate indications (median score 7-9) Indication
Appropriate Use Criteria for Initial Transthoracic Echocardiography in Outpatient Pediatric Cardiology (scores listed by Appropriate Use rating) Table 1: Appropriate indications (median score 7-9) Indication
Intraoperative and Postoperative Arrhythmias: Diagnosis and Treatment
 Intraoperative and Postoperative Arrhythmias: Diagnosis and Treatment Karen L. Booth, MD, Lucile Packard Children s Hospital Arrhythmias are common after congenital heart surgery [1]. Postoperative electrolyte
Intraoperative and Postoperative Arrhythmias: Diagnosis and Treatment Karen L. Booth, MD, Lucile Packard Children s Hospital Arrhythmias are common after congenital heart surgery [1]. Postoperative electrolyte
Data Collected: June 17, Reported: June 30, Survey Dates 05/24/ /07/2010
 Job Task Analysis for ARDMS Pediatric Echocardiography Data Collected: June 17, 2010 Reported: Analysis Summary For: Pediatric Echocardiography Exam Survey Dates 05/24/2010-06/07/2010 Invited Respondents
Job Task Analysis for ARDMS Pediatric Echocardiography Data Collected: June 17, 2010 Reported: Analysis Summary For: Pediatric Echocardiography Exam Survey Dates 05/24/2010-06/07/2010 Invited Respondents
Fetal Echocardiography
 Marie M. Gleason, M.D. Clinical Professor of Pediatrics The Perelman School of Medicine of the University of Pennsylvania Director of Outpatient and Community Cardiology and Cardiac Outreach Associate
Marie M. Gleason, M.D. Clinical Professor of Pediatrics The Perelman School of Medicine of the University of Pennsylvania Director of Outpatient and Community Cardiology and Cardiac Outreach Associate
Summary. HVRA s Cardio Vascular Genetic Detailed L2 Obstetrical Ultrasound. CPT 76811, 76825, _ 90% CHD detection. _ 90% DS detection.
 What is the role of fetal echocardiography (2D 76825, cardiovascular color flow mapping 93325) as performed in conjunction with detailed fetal anatomy scan (CPT 76811) now that AIUM requires limited outflow
What is the role of fetal echocardiography (2D 76825, cardiovascular color flow mapping 93325) as performed in conjunction with detailed fetal anatomy scan (CPT 76811) now that AIUM requires limited outflow
Paediatric Cardiology. Acyanotic CHD. Prof F F Takawira
 Paediatric Cardiology Acyanotic CHD Prof F F Takawira Aetiology Chromosomal Down syndrome, T13, T18 Genetic syndromes (gene defects) Velo-Cardio-facial (22 del) Genetic syndromes (undefined aetiology)
Paediatric Cardiology Acyanotic CHD Prof F F Takawira Aetiology Chromosomal Down syndrome, T13, T18 Genetic syndromes (gene defects) Velo-Cardio-facial (22 del) Genetic syndromes (undefined aetiology)
Bits and Bobs secondary causes of heart problems. Dr Angela McBrien 9 th September 2017
 Bits and Bobs secondary causes of heart problems Dr Angela McBrien 9 th September 2017 Not the heart Dextroposition Heart in the right chest with the apex to the left Often caused by left sided chest mass
Bits and Bobs secondary causes of heart problems Dr Angela McBrien 9 th September 2017 Not the heart Dextroposition Heart in the right chest with the apex to the left Often caused by left sided chest mass
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acute coronary syndrome(s), anticoagulant therapy in, 706, 707 antiplatelet therapy in, 702 ß-blockers in, 703 cardiac biomarkers in,
Index Note: Page numbers of article titles are in boldface type. A Acute coronary syndrome(s), anticoagulant therapy in, 706, 707 antiplatelet therapy in, 702 ß-blockers in, 703 cardiac biomarkers in,
Regional Prenatal Congenital Heart Disease Detection and Practices Jenny Ecord, APRN Ward Family Heart Center Wichita
 Regional Prenatal Congenital Heart Disease Detection and Practices Jenny Ecord, APRN Ward Family Heart Center Wichita The Children's Mercy Hospital, 2014. 05/14 Objectives Review current local and regional
Regional Prenatal Congenital Heart Disease Detection and Practices Jenny Ecord, APRN Ward Family Heart Center Wichita The Children's Mercy Hospital, 2014. 05/14 Objectives Review current local and regional
Everything You Always Wanted to Know About Fetal Arrhythmias, in 40 Minutes!
 Everything You Always Wanted to Know About Fetal Arrhythmias, in 40 Minutes! Fetal Arrhythmias! What is clinically important?!tachycardia (>200)!Fixed bradycardia (
Everything You Always Wanted to Know About Fetal Arrhythmias, in 40 Minutes! Fetal Arrhythmias! What is clinically important?!tachycardia (>200)!Fixed bradycardia (
I have nothing to disclose.
 I have nothing to disclose. Antiarrhythmic Therapy in Pregnancy Prof. Ali Oto,MD,FESC,FACC,FHRS Department of Cardiology Hacettepe University,Faculty of Medicine Ankara Arrhythmias in pregnancy An increased
I have nothing to disclose. Antiarrhythmic Therapy in Pregnancy Prof. Ali Oto,MD,FESC,FACC,FHRS Department of Cardiology Hacettepe University,Faculty of Medicine Ankara Arrhythmias in pregnancy An increased
Pathophysiology: Left To Right Shunts
 Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
Fetal Tetralogy of Fallot
 36 Fetal Tetralogy of Fallot E.D. Bespalova, R.M. Gasanova, O.A.Pitirimova National Scientific and Practical Center of Cardiovascular Surgery, Moscow Elena D. Bespalova, MD Professor, Director Rena M,
36 Fetal Tetralogy of Fallot E.D. Bespalova, R.M. Gasanova, O.A.Pitirimova National Scientific and Practical Center of Cardiovascular Surgery, Moscow Elena D. Bespalova, MD Professor, Director Rena M,
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions
 Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS Pediatric Cardiology
 Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
PREGNANCY AND CONGENITAL HEART DISEASE
 PREGNANCY AND CONGENITAL HEART DISEASE SIDDHARTH JADHAV M.D. Assistant Professor of Radiology E.B. Singleton Department of Pediatric Radiology Texas Children's Hospital COMMERCIAL DISCLOSURE - None Objectives
PREGNANCY AND CONGENITAL HEART DISEASE SIDDHARTH JADHAV M.D. Assistant Professor of Radiology E.B. Singleton Department of Pediatric Radiology Texas Children's Hospital COMMERCIAL DISCLOSURE - None Objectives
Basic Fetal Cardiac Evaluation
 Basic Fetal Cardiac Evaluation Mert Ozan Bahtiyar, MD Director, Fetal Care Center Division of Maternal Fetal Medicine Department of Obstetrics, Gynecology and Reproductive Sciences S L I D E 1 Background
Basic Fetal Cardiac Evaluation Mert Ozan Bahtiyar, MD Director, Fetal Care Center Division of Maternal Fetal Medicine Department of Obstetrics, Gynecology and Reproductive Sciences S L I D E 1 Background
Congenital Heart Disease
 Congenital Heart Disease Mohammed Alghamdi, MD, FRCPC, FAAP, FACC Associate Professor and Consultant Pediatric Cardiology, Cardiac Science King Fahad Cardiac Centre King Saud University INTRODUCTION CHD
Congenital Heart Disease Mohammed Alghamdi, MD, FRCPC, FAAP, FACC Associate Professor and Consultant Pediatric Cardiology, Cardiac Science King Fahad Cardiac Centre King Saud University INTRODUCTION CHD
Pediatrics ECG Monitoring. Pediatric Intensive Care Unit Emergency Division
 Pediatrics ECG Monitoring Pediatric Intensive Care Unit Emergency Division 1 Conditions Leading to Pediatric Cardiology Consultation 12.7% of annual consultation Is arrhythmias problems Geggel. Pediatrics.
Pediatrics ECG Monitoring Pediatric Intensive Care Unit Emergency Division 1 Conditions Leading to Pediatric Cardiology Consultation 12.7% of annual consultation Is arrhythmias problems Geggel. Pediatrics.
3/14/2011 MANAGEMENT OF NEWBORNS CARDIAC INTENSIVE CARE CONFERENCE FOR HEALTH PROFESSIONALS IRVINE, CA. MARCH 7, 2011 WITH HEART DEFECTS
 CONFERENCE FOR HEALTH PROFESSIONALS IRVINE, CA. MARCH 7, 2011 MANAGEMENT OF NEWBORNS WITH HEART DEFECTS A NTHONY C. CHANG, MD, MBA, MPH M E D I C AL D I RE C T OR, HEART I N S T I T U T E C H I LDRE N
CONFERENCE FOR HEALTH PROFESSIONALS IRVINE, CA. MARCH 7, 2011 MANAGEMENT OF NEWBORNS WITH HEART DEFECTS A NTHONY C. CHANG, MD, MBA, MPH M E D I C AL D I RE C T OR, HEART I N S T I T U T E C H I LDRE N
Pathophysiology: Left To Right Shunts
 Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
Regional Prenatal Congenital Heart Disease Detection and Practices Lori Erickson MSN, RN, CPNP-PC Ward Family Heart Center
 Regional Prenatal Congenital Heart Disease Detection and Practices Lori Erickson MSN, RN, CPNP-PC Ward Family Heart Center The Children's Mercy Hospital, 2014. 05/14 Objectives Evaluate our regional prenatal
Regional Prenatal Congenital Heart Disease Detection and Practices Lori Erickson MSN, RN, CPNP-PC Ward Family Heart Center The Children's Mercy Hospital, 2014. 05/14 Objectives Evaluate our regional prenatal
Congenital Heart Disease
 Screening Programmes Fetal Anomaly Congenital Heart Disease Information for health professionals Publication date: April 2012 Review date: April 2013 Version 2 67 Congenital Heart Disease Information for
Screening Programmes Fetal Anomaly Congenital Heart Disease Information for health professionals Publication date: April 2012 Review date: April 2013 Version 2 67 Congenital Heart Disease Information for
Evaluation of Fetal Arrhythmias
 REVIEW ARTICLE Evaluation of Fetal Arrhythmias George M Graham III DSJUOG Evaluation of Fetal Arrhythmias Assistant Professor, Division of Maternal Fetal Medicine, Department of Obstetrics, Gynecology
REVIEW ARTICLE Evaluation of Fetal Arrhythmias George M Graham III DSJUOG Evaluation of Fetal Arrhythmias Assistant Professor, Division of Maternal Fetal Medicine, Department of Obstetrics, Gynecology
Prenatal Diagnosis of Congenital Heart Disease by Fetal Echo
 Original Article Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2018/10 Prenatal Diagnosis of Congenital Heart Disease by Fetal Echo M Selvarani Assistant Professor, Department of Cardiology,
Original Article Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2018/10 Prenatal Diagnosis of Congenital Heart Disease by Fetal Echo M Selvarani Assistant Professor, Department of Cardiology,
NCC Review Cardiac 8/22/12. Intrauterine Blood Flow. Topics
 NCC Review Cardiac Tracey Buckley MSN,RNC, NNP-BC Cape Fear Valley Health System Topics Transition to Extrauterine Life Cyanosis Congenital Heart Disease (CHD) Clinical Manifestations of CHD Therapeutic
NCC Review Cardiac Tracey Buckley MSN,RNC, NNP-BC Cape Fear Valley Health System Topics Transition to Extrauterine Life Cyanosis Congenital Heart Disease (CHD) Clinical Manifestations of CHD Therapeutic
CMR for Congenital Heart Disease
 CMR for Congenital Heart Disease * Second-line tool after TTE * Strengths of CMR : tissue characterisation, comprehensive access and coverage, relatively accurate measurements of biventricular function/
CMR for Congenital Heart Disease * Second-line tool after TTE * Strengths of CMR : tissue characterisation, comprehensive access and coverage, relatively accurate measurements of biventricular function/
The blue baby. Case 4
 Case 4 The blue baby Mrs Smith has brought her baby to A&E because she says he has started turning blue. What are your immediate differential diagnoses? 1 Respiratory causes: Congenital respiratory disorder.
Case 4 The blue baby Mrs Smith has brought her baby to A&E because she says he has started turning blue. What are your immediate differential diagnoses? 1 Respiratory causes: Congenital respiratory disorder.
Clinicians and Facilities: RESOURCES WHEN CARING FOR WOMEN WITH ADULT CONGENITAL HEART DISEASE OR OTHER FORMS OF CARDIOVASCULAR DISEASE!!
 Clinicians and Facilities: RESOURCES WHEN CARING FOR WOMEN WITH ADULT CONGENITAL HEART DISEASE OR OTHER FORMS OF CARDIOVASCULAR DISEASE!! Abha'Khandelwal,'MD,'MS' 'Stanford'University'School'of'Medicine'
Clinicians and Facilities: RESOURCES WHEN CARING FOR WOMEN WITH ADULT CONGENITAL HEART DISEASE OR OTHER FORMS OF CARDIOVASCULAR DISEASE!! Abha'Khandelwal,'MD,'MS' 'Stanford'University'School'of'Medicine'
Objectives Part 1. Objectives Part 2. Fetal Circulation Transition to Postnatal Circulation Normal Cardiac Anatomy Ductal Dependence and use of PGE1
 Cardiac Physiology Gia Marzano, AC PNP Pediatric Cardiac Surgery Rush Center for Congenital Heart Disease Rush University Medical Center Objectives Part 1 Fetal Circulation Transition to Postnatal Circulation
Cardiac Physiology Gia Marzano, AC PNP Pediatric Cardiac Surgery Rush Center for Congenital Heart Disease Rush University Medical Center Objectives Part 1 Fetal Circulation Transition to Postnatal Circulation
Valve Disease in the Pregnant Patient
 Valve Disease in the Pregnant Patient Julie B. Damp, MD December 6, 2012 VanderbiltHeart.com If single, do not allow marriage. If fertile, do not allow pregnancy. If pregnant, do not allow delivery. If
Valve Disease in the Pregnant Patient Julie B. Damp, MD December 6, 2012 VanderbiltHeart.com If single, do not allow marriage. If fertile, do not allow pregnancy. If pregnant, do not allow delivery. If
Early fetal echocardiography: congenital heart disease detection and diagnostic accuracy in the hands of an experienced fetal cardiology program
 DOI: 10.1002/pd.4372 ORIGINAL ARTICLE Early fetal echocardiography: congenital heart disease detection and diagnostic accuracy in the hands of an experienced fetal cardiology program Jodi I. Pike, Anita
DOI: 10.1002/pd.4372 ORIGINAL ARTICLE Early fetal echocardiography: congenital heart disease detection and diagnostic accuracy in the hands of an experienced fetal cardiology program Jodi I. Pike, Anita
Adult Congenital Heart Disease Certification Examination Blueprint
 Adult Congenital Heart Disease Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the
Adult Congenital Heart Disease Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the
Notes by Sandra Dankwa 2009 HF- Heart Failure DS- Down Syndrome IE- Infective Endocarditis ET- Exercise Tolerance. Small VSD Symptoms -asymptomatic
 Congenital Heart Disease: Notes. Condition Pathology PC Ix Rx Ventricular septal defect (VSD) L R shuntsdefect anywhere in the ventricle, usually perimembranous (next to the tricuspid valve) 30% 1)small
Congenital Heart Disease: Notes. Condition Pathology PC Ix Rx Ventricular septal defect (VSD) L R shuntsdefect anywhere in the ventricle, usually perimembranous (next to the tricuspid valve) 30% 1)small
Slide 1. Slide 2. Slide 3 CONGENITAL HEART DISEASE. Papworth Hospital NHS Trust INTRODUCTION. Jakub Kadlec/Catherine Sudarshan INTRODUCTION
 Slide 1 CONGENITAL HEART DISEASE Jakub Kadlec/Catherine Sudarshan NHS Trust Slide 2 INTRODUCTION Most common congenital illness in the newborn Affects about 4 9 / 1000 full-term live births in the UK 1.5
Slide 1 CONGENITAL HEART DISEASE Jakub Kadlec/Catherine Sudarshan NHS Trust Slide 2 INTRODUCTION Most common congenital illness in the newborn Affects about 4 9 / 1000 full-term live births in the UK 1.5
Prenatal diagnosis of long QT syndrome: Implications for delivery room and neonatal management
 Himmelfarb Health Sciences Library, The George Washington University Health Sciences Research Commons Pediatrics Faculty Publications Pediatrics 2-2013 Prenatal diagnosis of long QT syndrome: Implications
Himmelfarb Health Sciences Library, The George Washington University Health Sciences Research Commons Pediatrics Faculty Publications Pediatrics 2-2013 Prenatal diagnosis of long QT syndrome: Implications
Congenital Heart Disease Patient and Pregnancy
 Congenital Heart Disease Patient and Pregnancy Gurur Biliciler-Denktas, M.D. Assistant Professor Division of Pediatric Cardiology, Department of Pediatrics The University of Texas Health Science Center
Congenital Heart Disease Patient and Pregnancy Gurur Biliciler-Denktas, M.D. Assistant Professor Division of Pediatric Cardiology, Department of Pediatrics The University of Texas Health Science Center
Congenital heart disease in twin-to-twin transfusion syndrome treated with fetoscopic laser surgery
 Chapter 10 Congenital heart disease in twin-to-twin transfusion syndrome treated with fetoscopic laser surgery Enrico Lopriore MD Regina Bökenkamp MD Marry Rijlaarsdam MD Marieke Sueters MD Frank PHA Vandenbussche
Chapter 10 Congenital heart disease in twin-to-twin transfusion syndrome treated with fetoscopic laser surgery Enrico Lopriore MD Regina Bökenkamp MD Marry Rijlaarsdam MD Marieke Sueters MD Frank PHA Vandenbussche
Transposition of the Great Arteries Preoperative Diagnostic Considerations. John Simpson Evelina Children s Hospital London, UK
 Transposition of the Great Arteries Preoperative Diagnostic Considerations John Simpson Evelina Children s Hospital London, UK Areas to be covered Definitions Scope of occurrence of transposition of the
Transposition of the Great Arteries Preoperative Diagnostic Considerations John Simpson Evelina Children s Hospital London, UK Areas to be covered Definitions Scope of occurrence of transposition of the
MEDICAL MANAGEMENT WITH CAVEATS 1. In one study of 50 CHARGE patients with CHD, 75% required surgery. 2. Children with CHARGE may be resistant to chlo
 CARDIOLOGY IN CHARGE SYNDROME: FOR THE PHYSICIAN Angela E. Lin, M.D. Teratology Program/Active Malformation Surveillance, Brigham and Women's Hospital, Old PBBH-B501, 75 Francis St., Boston, MA 02115 alin@partners.org
CARDIOLOGY IN CHARGE SYNDROME: FOR THE PHYSICIAN Angela E. Lin, M.D. Teratology Program/Active Malformation Surveillance, Brigham and Women's Hospital, Old PBBH-B501, 75 Francis St., Boston, MA 02115 alin@partners.org
Adult Congenital Heart Disease
 Adult Congenital Heart Disease Anne Marie Valente, MD Boston Adult Congenital Heart Disease and Pulmonary Hypertension Program Division of Cardiology Brigham and Women s Hospital, Boston Children s Hospital
Adult Congenital Heart Disease Anne Marie Valente, MD Boston Adult Congenital Heart Disease and Pulmonary Hypertension Program Division of Cardiology Brigham and Women s Hospital, Boston Children s Hospital
Fetal Arrhythmias: Diagnosis and Management. Jonathan T Fleenor, MD, FACC, FAAP Pediatric Cardiology Children s Hospital of the King s Daughters
 Fetal Arrhythmias: Diagnosis and Management Jonathan T Fleenor, MD, FACC, FAAP Pediatric Cardiology Children s Hospital of the King s Daughters No industry or financial disclosures Thanks to Drs Abuhamad
Fetal Arrhythmias: Diagnosis and Management Jonathan T Fleenor, MD, FACC, FAAP Pediatric Cardiology Children s Hospital of the King s Daughters No industry or financial disclosures Thanks to Drs Abuhamad
Cardiac Emergencies in Infants. Michael Luceri, DO
 Cardiac Emergencies in Infants Michael Luceri, DO October 7, 2017 I have no financial obligations or conflicts of interest to disclose. Objectives Understand the scope of congenital heart disease Recognize
Cardiac Emergencies in Infants Michael Luceri, DO October 7, 2017 I have no financial obligations or conflicts of interest to disclose. Objectives Understand the scope of congenital heart disease Recognize
The fetal circulation
 Peter John Murphy MB ChB DA FRCA The fetal circulation (Fig. 1) is markedly different from the adult circulation. In the fetus, gas exchange does not occur in the lungs but in the placenta. The placenta
Peter John Murphy MB ChB DA FRCA The fetal circulation (Fig. 1) is markedly different from the adult circulation. In the fetus, gas exchange does not occur in the lungs but in the placenta. The placenta
ECHOGENIC FETAL HEART WITHOUT HEART BLOCK AND MATERNAL ANTI- Ro/ La ANTIBODIES POSITIVITY A LESS KNOWN ASSOCIATION
 ECHOGENIC FETAL HEART WITHOUT HEART BLOCK AND MATERNAL ANTI- Ro/ La ANTIBODIES POSITIVITY A LESS KNOWN ASSOCIATION DR PUNDALIK BALIGA FELLOW IN FETAL MEDICINE MEDISCAN SYSTEMS, CHENNAI CASE 1 30 year old
ECHOGENIC FETAL HEART WITHOUT HEART BLOCK AND MATERNAL ANTI- Ro/ La ANTIBODIES POSITIVITY A LESS KNOWN ASSOCIATION DR PUNDALIK BALIGA FELLOW IN FETAL MEDICINE MEDISCAN SYSTEMS, CHENNAI CASE 1 30 year old
More History. Organization. Maternal Cardiac Disease: a historical perspective. The Parturient with Cardiac Disease 9/21/2012
 The Parturient with Cardiac Disease Pamela Flood M.D. Professor of Anesthesia and Perioperative Care Obstetrics, Gynecology and Reproductive Sciences University of California, San Francisco Maternal Cardiac
The Parturient with Cardiac Disease Pamela Flood M.D. Professor of Anesthesia and Perioperative Care Obstetrics, Gynecology and Reproductive Sciences University of California, San Francisco Maternal Cardiac
Uptofate Study Summary
 CONGENITAL HEART DISEASE Uptofate Study Summary Acyanotic Atrial septal defect Ventricular septal defect Patent foramen ovale Patent ductus arteriosus Aortic coartation Pulmonary stenosis Cyanotic Tetralogy
CONGENITAL HEART DISEASE Uptofate Study Summary Acyanotic Atrial septal defect Ventricular septal defect Patent foramen ovale Patent ductus arteriosus Aortic coartation Pulmonary stenosis Cyanotic Tetralogy
EVALUATION OF PREGNANT PATIENTS WITH HEART DISEASE. Karen Stout, MD University of Washington Seattle Children s Seattle, WA
 EVALUATION OF PREGNANT PATIENTS WITH HEART DISEASE Karen Stout, MD University of Washington Seattle Children s Seattle, WA CASE PRESENTATION 24 year old woman with aortic regurgitation referred for evaluation
EVALUATION OF PREGNANT PATIENTS WITH HEART DISEASE Karen Stout, MD University of Washington Seattle Children s Seattle, WA CASE PRESENTATION 24 year old woman with aortic regurgitation referred for evaluation
Surgical Management Of Congenital Heart Disease II: Single Ventricle And Hypoplastic Left Heart Syndrome Aortic Arch Anomalies Septal Defects And...
 Surgical Management Of Congenital Heart Disease II: Single Ventricle And Hypoplastic Left Heart Syndrome Aortic Arch Anomalies Septal Defects And... Of Thoracic Arteries And Veins A Video Manual By Viktor
Surgical Management Of Congenital Heart Disease II: Single Ventricle And Hypoplastic Left Heart Syndrome Aortic Arch Anomalies Septal Defects And... Of Thoracic Arteries And Veins A Video Manual By Viktor
Cardiac MRI in ACHD What We. ACHD Patients
 Cardiac MRI in ACHD What We Have Learned to Apply to ACHD Patients Faris Al Mousily, MBChB, FAAC, FACC Consultant, Pediatric Cardiology, KFSH&RC/Jeddah Adjunct Faculty, Division of Pediatric Cardiology
Cardiac MRI in ACHD What We Have Learned to Apply to ACHD Patients Faris Al Mousily, MBChB, FAAC, FACC Consultant, Pediatric Cardiology, KFSH&RC/Jeddah Adjunct Faculty, Division of Pediatric Cardiology
DEVELOPMENT OF THE CIRCULATORY SYSTEM L E C T U R E 5
 DEVELOPMENT OF THE CIRCULATORY SYSTEM L E C T U R E 5 REVIEW OF CARDIAC ANATOMY Heart 4 chambers Base and apex Valves Pericardial sac 3 layers: epi, myo, endo cardium Major blood vessels Aorta and its
DEVELOPMENT OF THE CIRCULATORY SYSTEM L E C T U R E 5 REVIEW OF CARDIAC ANATOMY Heart 4 chambers Base and apex Valves Pericardial sac 3 layers: epi, myo, endo cardium Major blood vessels Aorta and its
Major Forms of Congenital Heart Disease: Consultant Pediatric and Fetal Cardiology King Abdulaziz Cardiac Center, National Guard Hospital Riyadh
 Major Forms of Congenital Heart Disease: Impact of Prenatal Detection and Diagnosis Dr Merna Atiyah Consultant Pediatric and Fetal Cardiology King Abdulaziz Cardiac Center, National Guard Hospital Riyadh
Major Forms of Congenital Heart Disease: Impact of Prenatal Detection and Diagnosis Dr Merna Atiyah Consultant Pediatric and Fetal Cardiology King Abdulaziz Cardiac Center, National Guard Hospital Riyadh
ADULT CONGENITAL HEART DISEASE. Stuart Lilley
 ADULT CONGENITAL HEART DISEASE Stuart Lilley More adults than children have congenital heart disease Huge variety of congenital lesions from minor to major Heart failure, re-operation and arrhythmia are
ADULT CONGENITAL HEART DISEASE Stuart Lilley More adults than children have congenital heart disease Huge variety of congenital lesions from minor to major Heart failure, re-operation and arrhythmia are
Accuracy of the Fetal Echocardiogram in Double-outlet Right Ventricle
 Blackwell Publishing IncMalden, USACHDCongenital Heart Disease 2006 The Authors; Journal compilation 2006 Blackwell Publishing, Inc.? 200723237Original ArticleFetal Echocardiogram in Double-outlet Right
Blackwell Publishing IncMalden, USACHDCongenital Heart Disease 2006 The Authors; Journal compilation 2006 Blackwell Publishing, Inc.? 200723237Original ArticleFetal Echocardiogram in Double-outlet Right
5.8 Congenital Heart Disease
 5.8 Congenital Heart Disease Congenital heart diseases (CHD) refer to structural or functional heart diseases, which are present at birth. Some of these lesions may be discovered later. prevalence of Chd
5.8 Congenital Heart Disease Congenital heart diseases (CHD) refer to structural or functional heart diseases, which are present at birth. Some of these lesions may be discovered later. prevalence of Chd
Cardiac Disease in Pregnancy
 Cardiac Disease in Pregnancy DATE: SEPTEMBER 11, 2016 PRESENTED BY: ABIGAIL KHAN, MD Outline Scope of the problem Physiology of pregnancy Cardiac risk in pregnancy Pregnancy management Contraception 1
Cardiac Disease in Pregnancy DATE: SEPTEMBER 11, 2016 PRESENTED BY: ABIGAIL KHAN, MD Outline Scope of the problem Physiology of pregnancy Cardiac risk in pregnancy Pregnancy management Contraception 1
B11. Cardiology Review. Session Summary. Session Objectives. Test Questions
 B11 Cardiology Review Lyn Vargo, PhD, NNP-BC Clinical Assistant Professor Stony Brook University NNP Program University of Missouri, Kansas City The speaker has signed a disclosure form and indicated she
B11 Cardiology Review Lyn Vargo, PhD, NNP-BC Clinical Assistant Professor Stony Brook University NNP Program University of Missouri, Kansas City The speaker has signed a disclosure form and indicated she
When to implant an ICD in systemic right ventricle?
 When to implant an ICD in systemic right ventricle? Département de rythmologie et de stimulation cardiaque Nicolas Combes n.combes@clinique-pasteur.com Pôle de cardiologie pédiatrique et congénitale Risk
When to implant an ICD in systemic right ventricle? Département de rythmologie et de stimulation cardiaque Nicolas Combes n.combes@clinique-pasteur.com Pôle de cardiologie pédiatrique et congénitale Risk
Opinion. Isolated major congenital heart disease
 Ultrasound Obstet Gynecol 2001; 17: 370 379 Opinion Blackwell Science, Ltd Isolated major congenital heart disease The principal theme of this issue of the Journal is the prenatal detection of fetal cardiac
Ultrasound Obstet Gynecol 2001; 17: 370 379 Opinion Blackwell Science, Ltd Isolated major congenital heart disease The principal theme of this issue of the Journal is the prenatal detection of fetal cardiac
PIAF study: Placental insufficiency and aortic isthmus flow Jean-Claude Fouron, MD
 Dear colleagues, I would like to thank you very sincerely for agreeing to participate in our multicentre study on the clinical significance of recording fetal aortic isthmus flow during placental circulatory
Dear colleagues, I would like to thank you very sincerely for agreeing to participate in our multicentre study on the clinical significance of recording fetal aortic isthmus flow during placental circulatory
RF & RHD Workshop 22 nd March MANAGEMENT of RHEUMATIC HEART DISEASE in PREGNANCY. Dr Dorothy Radford
 RF & RHD Workshop 22 nd March 2016 MANAGEMENT of RHEUMATIC HEART DISEASE in PREGNANCY Dr Dorothy Radford PREGNANCY PHYSIOLOGY Increased cardiac output 30%-50% Increased blood volume 30%-50% Increased heart
RF & RHD Workshop 22 nd March 2016 MANAGEMENT of RHEUMATIC HEART DISEASE in PREGNANCY Dr Dorothy Radford PREGNANCY PHYSIOLOGY Increased cardiac output 30%-50% Increased blood volume 30%-50% Increased heart