3/30/18. Common Radiology Studies in Pediatric Surgery. Disclosure Information. Objectives
|
|
|
- Jodie Gardner
- 5 years ago
- Views:
Transcription

1 Common Radiology Studies in Pediatric Surgery A Scenario Based Approach to Interpretation for the Pediatric Nurse and Provider presented by Elizabeth A. Paton, DNP, RN-BC, PNP-A, PPCNP-BC, CPEN, FAEN Disclosure Information I have no disclosures Objectives By the end of this presentation, the learner will be able to: 1. Discuss a basic approach to interpreting common radiology studies, including chest and abdominal X-rays, upper GIs, and CT scans. 2. Discuss key radiographic findings exhibited by patients with congenital abnormalities. 3. Recognize key abnormal radiological findings with acquired surgical diagnoses. 1
2 Specific Radiology Examinations Chest X-ray (CXR) Abdominal X-ray (KUB) Computerized topography (CT) o Chest o Abdomen Ultrasound Upper gastrointestinal series (UGI) Contrast enema Esophagram Chest X-ray Quality: Rotation Inclusion Penetration Expansion Interpretation: Airway Bone Cardiac Diaphragm Extrathoracic tissues Fields Gastric bubble Hilum and mediastinum Instrumentation Abdominal X-ray Interpretation: Air Bowel Calcifications Diaphragm Everything else 2

")



3 Normal Abdominal X-ray Air? Bowel Calcifications? Diaphragm Everything else Flat Upright Computerized Topography (CT) Abdomen Axial- Axial- Abdominal Coronal Sagittal Lung Window Ultrasound May be used for diagnosis or evaluation of: Masses Appendicitis Intussusception Cholelithiasis/cholecystitis Hypertrophic pyloric stenosis Malrotation Ovarian pathologies 3

 Other congenital abnormalities Esophagram 4")
4 SMA/SMV to Evaluate for Malrotation SMA= Superior Mesenteric Artery SMV= Superior Mesenteric Vein Esophagram May be used for: Evaluation for esophageal stricture Integrity of anastomosis after TE fistula repair Retained food bolus Esophageal damage after caustic ingestion (e.g. battery) Other congenital abnormalities Esophagram 4

 Normal")
5 Upper Gastrointestinal Series (UGI) Used to evaluate for: Duodenal atresia Malrotation Strictures or atresias of small bowel Hypertrophic pyloric stenosis (not modality of choice) Normal UGI Normal UGI 5


6 Contrast Enema Used to evaluate for: Hirschprung disease Strictures or atresias of colon Other reasons for delayed passage of meconium Treatment for intussusception May use: Air Water soluble contrast Barium Normal Contrast Enema PLACEMEN RADIOLOGICAL FINDINGS OF SPECIFIC SURGICAL DIAGNOSES MEDICAL DEVICES 6

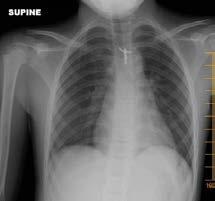
7 Case Scenario 1 15 year old male presents with acute onset of left sided chest pain History PMHx Vital Signs o Temperature 37.0 ºC o Heart Rate 84 bpm o Respiratory Rate 36 bpm o Pulse Ox 95% room air Case Progression What are your differential diagnoses? Costochondritis Trauma Pneumonia Pneumothorax Cardiac process What test(s) do you want to order? Chest X-ray Quality: Rotation Inclusion Penetration Expansion Interpretation: Airway Bone Cardiac Diaphragm Extrathoracic tissues Fields Gastric bubble Hilum and mediastinum Instrumentation 7



8 3/30/18 Pneumothorax Pneumothorax Case Progression What are your interventions? o Chest tube? o Oxygen? o Incentive spirometry? 8

9 Pneumothorax Case Progression What are your interventions? o Chest tube? o Oxygen? o Incentive spirometry? Pneumothorax 9


10 Chest Tube Placement (Chest X-ray: Tubes- chest drains-position, 2017) Case Scenario 2 18 month old female presents with an acute onset of difficulty swallowing History PMHx Vital Signs o Temperature 37.0 ºC o o o Heart Rate 116 bpm Respiratory Rate 32 bpm Pulse Ox 99% room air Esophageal Foreign Body 10


11 Why obtain 2 view X-ray? Esophageal Foreign Body Esophageal Foreign Body 11

12 Bronchial Foreign Body Case Scenario 3 9 year old female presents with 1 day history of abdominal pain History PMHx Vital Signs o Temperature 38.0 ºC o Heart Rate 92 bpm o Respiratory Rate 26 bpm o Pulse Ox 99% room air Case Progression What are your differential diagnoses? Gastroenteritis Constipation Urinary Tract Infection Ovarian pathology Appendicitis What test(s) do you want to order? 12



13 Appendicitis Diagnostic Criteria: Enlarged >6mm diameter Wall thickening >2mm Wall enhancement Fat stranding Appendicolith Fluid filled Appendicitis Appendicitis 13


14 Appendicitis Case Scenario 4 5 week old male presents with vomiting History PMHx Vital Signs o Temperature 37.0 ºC o Heart Rate 144 bpm o Respiratory Rate 36 bpm o Pulse Ox 99% room air Case Progression What are your differential diagnoses? Gastroesophageal reflux Formula intolerance Malrotation Pyloric stenosis What test(s) do you want to order? 14



15 3/30/18 Pyloric Stenosis Diagnostic Criteria: Muscle Thickness >3mm Channel Length >14mm Failure of channel to open and stomach contents to empty Pyloric Stenosis Pyloric Stenosis 15
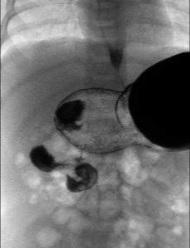
16 Case Progression What are your interventions? o o o o Fluid resuscitation NPO Monitoring of electrolytes until corrected CO2 <30, Chloride >100 Surgery- pyloromyotomy Case Scenario 5 15 month old male presents with crampy, intermittent abdominal pain History PMHx Vital Signs o Temperature 37.0 ºC o Heart Rate 118 bpm o Respiratory Rate 36 bpm o Pulse Ox 99% room air Case Progression What are your differential diagnoses? Gastroesophageal reflux Gastroenteritis Constipation Intussusception What test(s) do you want to order? 16



17 Intussusception Intussusception Intussusception 17
18 Case Scenario 6 5 day old, 29 week preemie, presents with feeding intolerance and blood in stool History PMHx Vital Signs o Temperature 37.2 ºC o o o Heart Rate 156 bpm Respiratory Rate 36 bpm Pulse Ox 97% room air Case Progression What are your differential diagnoses? Milk protein intolerance Anal fissure Sepsis Non-accidental trauma Necrotizing Enterocolitis (NEC) What test(s) do you want to order? Necrotizing Enterocolitis Modified Bell Staging Criteria: IA: Signs of sepsis, abdominal distention, guaiac positive stools, KUB with normal gas pattern or mildly dilated loops of bowel IB: Same except bright blood from rectum IIA: Same except pneumatosis intestinalis noted on KUB IIB: Thrombocytopenia, abdominal tenderness, portal venous gas IIIA: Severely ill, acidotic, neutropenia, DIC, peritonitis, portal venous gas + ascites IIIB: Same as IIIA but KUB demonstrates pneumoperitoneum 18



19 Necrotizing Enterocolitis Pneumatosis Necrotizing Enterocolitis PLACEMENT OF MEDICAL DEVICES MEDICAL DEVICES 19



20 3/30/18 Central Venous Line Placement Superior Vena Cava Right Atrium (Chest X-ray: Tubes- CVL lines position, 2017) Tip of CVL should be in the superior vena cava or at the cavo-atrial junction Central Venous Line Placement Central Venous Line Placement 20



21 Central Venous Line Placement Lines!!!! ETT Leadwire Leadwire NGT UAC Temperature Probe Nasogastric Tube Placement Note position of side holes 21




22 Post-Pyloric Tube Weighted feeding tube Nasojejunal Tube Gastrostomy Tube Placement Contrast within stomach Contrast outside stomach 22

")
23 CONGENITAL ABNORMALITIES MEDICAL DEVICES Duodenal Atresia What is your diagnosis? Coiled Orogastric Tube (OGT) Absence of distal bowel gas 23


24 Long Gap Esophageal Atresia Long Gap Esophageal Atresia 24

25 Esophageal Atresia with Distal Fistula (C) What is your diagnosis? Coiled OGT Presence of distal bowel gas Work Up for Midline Defects Esophageal Atresia +/- Tracheoesophageal Fistula Imperforate Anus +/- Fistula Omphalocele Work Up for Midline Defects Physical Exam Echocardiogram Renal Ultrasound Spinal Ultrasound +/- Delayed MRI Skeletal Survey 25




26 Imperforate Anus with Bucket Handle Cross-table Lateral Skeletal Survey 26


27 Skeletal Survey High Pressure Distal Colostogram Malrotation 27





28 Malrotation with Midgut Volvulus Hirschsprung Disease Hirschsprung Disease 28

29 TRAUMA RADIOGRAPHS MEDICAL DEVICES AAST Liver Trauma Classification Grade I: Subcapsular hematoma <10% surface area, capsular tear <1cm Grade II: Subcapsular hematoma 10-50% surface area, capsular tear 1-3 cm Grade III: Subcapsular hematoma >50%, capsular tear >3cm Grade IV: Parenchymal disruption 25-76% hepatic lobe or 1-3 segments Grade V: Parenchymal disruption >75% hepatic lobe or >3 segments Grade VI: Hepatic avulsion (Khan, 2017) Grade III Liver Laceration 29




30 Grade IV Liver Laceration Grade V Liver Laceration MISCELLANEOUS ABNORMALITIES MEDICAL DEVICES 30





31 Pectus Excavatum Haller Index: 243/72 = 3.37 Bezoar Esophageal Stricture 31



32 LET S REVIEW SOME IMAGES. Free Air Free Air 32


33 Pneumothorax Central Venous Line Placement Right Sided Congenital Diaphragmatic Hernia 33



34 Portal Venous Gas and Pneumatosis Appendicitis Radiation Exposure Radiation exposure may lead to: Increased cancer risk throughout lifetime Pediatric considerations Children are more radiation sensitive Potential for radiation exposure over lifetime 34
35 Radiation Exposure Radiation exposure expressed as effective dose Millisievert (msv) Considered whole body dose of radiation in relation to environmental exposure Typical environmental exposure is 3 msv/year Qualitative risk levels Negligible- less than 2 days background exposure Minimal- more than 2 days, less than 1 month background exposure Very low- more than 1 month, less than 8 months Low- 8 months to 6 years Moderate- more than 6 years Radiation Exposure Type of Exam Months of Annual Background Radiation 2 view CXR 10 days CT scan of abdomen and pelvis 3 years Upper GI 2 years CT chest 2 years CT head 8 months Radiation Exposure Helpful websites regarding guidelines for pediatrics: American College of Radiology Image Gently The Society for Pediatric Radiology 35


. In Radiology Masterclass online. Retrieved from http://www.")

36 One last story.. Special thanks to Tom Boulden, MD for his help and review References Chest X-ray: Tubes- chest drains-position. (n.d.). In Radiology Masterclass online. Retrieved from _xray_chest_drain Chest X-ray:Tubes-CVL catheters-position. (n.d.). In Radiology Masterclass online. Retrieved from _xray_central_line_anatomy Khan, A.N. (2017). Liver trauma imaging. Medscape. Retrieved from Murphy, A. & Hartley, L. (n.d.). Lines and tubes (chest radiograph). In Radiopaedia. Retrieved from 36
Back to Basics: What Imaging Test should I order? Jeanne G. Hill, M.D. Pediatric Radiology Medical University of South Carolina
 Back to Basics: What Imaging Test should I order? Jeanne G. Hill, M.D. Pediatric Radiology Medical University of South Carolina Disclosure Neither I nor any member of my immediate family has a relevant
Back to Basics: What Imaging Test should I order? Jeanne G. Hill, M.D. Pediatric Radiology Medical University of South Carolina Disclosure Neither I nor any member of my immediate family has a relevant
Interpret clinical and laboratory tests to identify conditions that require surgical intervention, including:
 Pediatric Surgery Note: The goals and objectives described in detail below are not meant to be completed in a single one month block rotation but are meant to be cumulative, culminating in a thorough and
Pediatric Surgery Note: The goals and objectives described in detail below are not meant to be completed in a single one month block rotation but are meant to be cumulative, culminating in a thorough and
Hirschprung s. Meconium plug R/S >1 R/S <1
 NEONATAL ABDOMINAL EMERGENCIES LOW OBSTRUCTION HIGH OBSTRUCTION INTESTINAL OBSTRUCTION High obstruction - proximal to mid-ileumileum Few dilated, air filled bowel loops Complete obstruction diagnosed by
NEONATAL ABDOMINAL EMERGENCIES LOW OBSTRUCTION HIGH OBSTRUCTION INTESTINAL OBSTRUCTION High obstruction - proximal to mid-ileumileum Few dilated, air filled bowel loops Complete obstruction diagnosed by
Abdominal Pain in Pediatric Patients Image Gently
 Abdominal Pain in Pediatric Patients Image Gently Susan D. John, M.D. Baptist Health Emergency Radiology 2017 Disclosure I have no financial relationships with a commercial entity producing healthcarerelated
Abdominal Pain in Pediatric Patients Image Gently Susan D. John, M.D. Baptist Health Emergency Radiology 2017 Disclosure I have no financial relationships with a commercial entity producing healthcarerelated
LOOKING FOR AIR IN ALL THE WRONG PLACES Richard M. Gore, MD North Shore University Health System University of Chicago Evanston, IL
 SIGNIFICANCE OF EXTRALUMINAL ABDOMINAL GAS: LOOKING FOR AIR IN ALL THE WRONG PLACES Richard M. Gore, MD North Shore University Health System University of Chicago Evanston, IL SCBT/MR 2012 October 26,
SIGNIFICANCE OF EXTRALUMINAL ABDOMINAL GAS: LOOKING FOR AIR IN ALL THE WRONG PLACES Richard M. Gore, MD North Shore University Health System University of Chicago Evanston, IL SCBT/MR 2012 October 26,
Pediatric Surgery MUHC MCH Siste. Objectives of Training
 Preamble A rotation in Pediatric Surgery must give residents the opportunity to become familiar with the unique needs of infants and children as surgical patients. Some of the surgical diseases encountered
Preamble A rotation in Pediatric Surgery must give residents the opportunity to become familiar with the unique needs of infants and children as surgical patients. Some of the surgical diseases encountered
Pediatric abdominal emergencies In the first year of life
 Common Pediatric abdominal emergencies In the first year of life Kristian Stien Thomassen Section of Pediatric Radiology Dept. of Radiology and Nuclear Medicine Oslo University Hospital Understand the
Common Pediatric abdominal emergencies In the first year of life Kristian Stien Thomassen Section of Pediatric Radiology Dept. of Radiology and Nuclear Medicine Oslo University Hospital Understand the
Neonatal intestinal obstruction: how to make etiological diagnosis?
 Neonatal intestinal obstruction: how to make etiological diagnosis? Poster No.: C-1414 Congress: ECR 2013 Type: Educational Exhibit Authors: W. Mnari, M. Zguidi, A. Zrig, M. Maatouk, B. Hmida, R. Salem,
Neonatal intestinal obstruction: how to make etiological diagnosis? Poster No.: C-1414 Congress: ECR 2013 Type: Educational Exhibit Authors: W. Mnari, M. Zguidi, A. Zrig, M. Maatouk, B. Hmida, R. Salem,
Neonatal intestinal obstruction: how to make etiological diagnosis?
 Neonatal intestinal obstruction: how to make etiological diagnosis? Poster No.: C-1414 Congress: ECR 2013 Type: Educational Exhibit Authors: W. MNARI, M. Zguidi, A. Zrig, M. MAATOUK, B. Hmida, R. Salem,
Neonatal intestinal obstruction: how to make etiological diagnosis? Poster No.: C-1414 Congress: ECR 2013 Type: Educational Exhibit Authors: W. MNARI, M. Zguidi, A. Zrig, M. MAATOUK, B. Hmida, R. Salem,
Acquired pediatric esophageal diseases Imaging approaches and findings. M. Mearadji International Foundation for Pediatric Imaging Aid
 Acquired pediatric esophageal diseases Imaging approaches and findings M. Mearadji International Foundation for Pediatric Imaging Aid Acquired pediatric esophageal diseases The clinical signs of acquired
Acquired pediatric esophageal diseases Imaging approaches and findings M. Mearadji International Foundation for Pediatric Imaging Aid Acquired pediatric esophageal diseases The clinical signs of acquired
Vomiting in children: The good coordination between radiologists and pediatricians is the key to success
 Vomiting in children: The good coordination between radiologists and pediatricians is the key to success C. Santos Montón 1, M. T. Garzon Guiteria 2, A. Hortal Benito-Sendín 1, K. El Karzazi 1, P. Sanchez
Vomiting in children: The good coordination between radiologists and pediatricians is the key to success C. Santos Montón 1, M. T. Garzon Guiteria 2, A. Hortal Benito-Sendín 1, K. El Karzazi 1, P. Sanchez
Topics for discussion. Pediatric General Surgery. Physiology. Surgical Newborns. Neonatal Intestinal Obstruction
 Topics for discussion Pediatric General Surgery Professor General & Thoracic Surgery What makes Pediatric Surgery unique? Neonatal intestinal obstruction Abdominal wall defects Inguinal hernias Appendicitis
Topics for discussion Pediatric General Surgery Professor General & Thoracic Surgery What makes Pediatric Surgery unique? Neonatal intestinal obstruction Abdominal wall defects Inguinal hernias Appendicitis
Gastroschisis Sequelae and Management
 Gastroschisis Sequelae and Management Mary Finn Gillian Lieberman, MD Primary Care Radiology Beth Israel Deaconess Medical Center Harvard Medical School April 2014 Outline I. Definition and Epidemiology
Gastroschisis Sequelae and Management Mary Finn Gillian Lieberman, MD Primary Care Radiology Beth Israel Deaconess Medical Center Harvard Medical School April 2014 Outline I. Definition and Epidemiology
Pediatric Bowel Obstruction
 Pediatric Bowel Obstruction Matt Zerden, Harvard Medical School III Patient 1 16 year old presents with severe, episodic abdominal pain, nausea and vomiting. Questionable abdominal mass in RLQ Previous
Pediatric Bowel Obstruction Matt Zerden, Harvard Medical School III Patient 1 16 year old presents with severe, episodic abdominal pain, nausea and vomiting. Questionable abdominal mass in RLQ Previous
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal injuries clinical presentation of, 23 24 Abdominal trauma evaluation for pediatric surgeon, 59 74 background of, 60 colon and
Index Note: Page numbers of article titles are in boldface type. A Abdominal injuries clinical presentation of, 23 24 Abdominal trauma evaluation for pediatric surgeon, 59 74 background of, 60 colon and
Suspected Foreign Body Ingestion
 Teresa Liang Suspected Foreign Body Ingestion 1. General Presentation Background: Of more than 100,000 cases of foreign body ingestion reported each year in the United States, 80% occur in children, with
Teresa Liang Suspected Foreign Body Ingestion 1. General Presentation Background: Of more than 100,000 cases of foreign body ingestion reported each year in the United States, 80% occur in children, with
Radiology of the abdomen Lecture -1-
 Radiology of the abdomen Lecture -1- Objectives To know radiology modalities used in abdomen imaging mainly GI tract. To know advantages and disadvantages of each modality. To know indications and contraindications
Radiology of the abdomen Lecture -1- Objectives To know radiology modalities used in abdomen imaging mainly GI tract. To know advantages and disadvantages of each modality. To know indications and contraindications
PEDIATRIC EMERGENCY DEPARTMENT CLINICAL GUIDELINE: GI SURGICAL EMERGENCIES: VOMITING
 GI SURGICAL EMERGENCIES: VOMITING PYLORIC STENOSIS Population: Infants: onset between 2-5 weeks of age 1 in 250 births Male: female ratio 4:1 Familial incidence History: No vomiting in the first few weeks
GI SURGICAL EMERGENCIES: VOMITING PYLORIC STENOSIS Population: Infants: onset between 2-5 weeks of age 1 in 250 births Male: female ratio 4:1 Familial incidence History: No vomiting in the first few weeks
Gastro Intestinal pg 1 of 6
 Gastro Intestinal pg 1 of 6 Diabetic Ketoacidosis -Treatment differences True Na: adjust upward 1.6 mleq/l for every 100 mg/dl increase in blood glucose Potential serious CNS effects; 2-5% mortality rate
Gastro Intestinal pg 1 of 6 Diabetic Ketoacidosis -Treatment differences True Na: adjust upward 1.6 mleq/l for every 100 mg/dl increase in blood glucose Potential serious CNS effects; 2-5% mortality rate
Plain abdomen The standard films are supine & erect AP views (alternative to erect, lateral decubitus film is used in ill patients).
.") Plain abdomen The standard films are supine & erect AP views (alternative to erect, lateral decubitus film is used in ill patients). The stomach can be readily identified by its location, gastric rugae
Plain abdomen The standard films are supine & erect AP views (alternative to erect, lateral decubitus film is used in ill patients). The stomach can be readily identified by its location, gastric rugae
Learning Radiology: Recognizing the Basics. Text with Student Consult Online Access Code
 Learning Radiology: Recognizing the Basics. Text with Student Consult Online Access Code Herring, W ISBN-13: 9780323074445 Table of Contents 1. Recognizing Anything The "colorful" world of radiology A
Learning Radiology: Recognizing the Basics. Text with Student Consult Online Access Code Herring, W ISBN-13: 9780323074445 Table of Contents 1. Recognizing Anything The "colorful" world of radiology A
Flouroscopy CT. Principal Modality (2): Case Report # [] Date accepted: 14 May 2015
![Flouroscopy CT. Principal Modality (2): Case Report # [] Date accepted: 14 May 2015](/thumbs/85/92263701.jpg "Flouroscopy CT. Principal Modality (2): Case Report # [] Date accepted: 14 May 2015") Radiological Category: Emergency Principal Modality (1): Principal Modality (2): Flouroscopy CT Case Report # [] Submitted by: Haider Virani, M.D. Faculty reviewer: Naga Chinapuvvula, MD Date accepted:
Radiological Category: Emergency Principal Modality (1): Principal Modality (2): Flouroscopy CT Case Report # [] Submitted by: Haider Virani, M.D. Faculty reviewer: Naga Chinapuvvula, MD Date accepted:
Introduction and Definitions
 Bowel obstruction Introduction and Definitions Accounts for 5% of all acute surgical admissions Patients are often extremely ill requiring prompt assessment, resuscitation and intensive monitoring Obstruction
Bowel obstruction Introduction and Definitions Accounts for 5% of all acute surgical admissions Patients are often extremely ill requiring prompt assessment, resuscitation and intensive monitoring Obstruction
The University of Arizona Pediatric Residency Program. Primary Goals for Rotation. Surgery, Pediatric
 The University of Arizona Pediatric Residency Program Primary Goals for Rotation Surgery, Pediatric 1. GOAL: Anesthesia. Participate in the care and management of pediatric patients requiring general and
The University of Arizona Pediatric Residency Program Primary Goals for Rotation Surgery, Pediatric 1. GOAL: Anesthesia. Participate in the care and management of pediatric patients requiring general and
Lab Monitor Images Dissection of the Abdominal Vasculature + Lower Digestive System
 Lab Monitor Images Dissection of the Abdominal Vasculature + Lower Digestive System Stomach & Duodenum Frontal (AP) View Nasogastric tube 2 1 3 4 Stomach Pylorus Duodenum 1 Duodenum 2 Duodenum 3 Duodenum
Lab Monitor Images Dissection of the Abdominal Vasculature + Lower Digestive System Stomach & Duodenum Frontal (AP) View Nasogastric tube 2 1 3 4 Stomach Pylorus Duodenum 1 Duodenum 2 Duodenum 3 Duodenum
Lines and tubes. 1 Nasogastric tubes Endotracheal tubes Central lines Permanent pacemakers Chest drains...
 Lines and tubes 1 Nasogastric tubes... 15 2 Endotracheal tubes.... 19 3 Central lines... 21 4 Permanent pacemakers.... 25 5 Chest drains... 30 This page intentionally left blank 1 Nasogastric tubes Background
Lines and tubes 1 Nasogastric tubes... 15 2 Endotracheal tubes.... 19 3 Central lines... 21 4 Permanent pacemakers.... 25 5 Chest drains... 30 This page intentionally left blank 1 Nasogastric tubes Background
Emergent Pediatric Ultrasound. Katharine Dennis, RDMS/RVT Tiffany Schultz, RDMS UNC Health Care Dept of General Ultrasound
 Emergent Pediatric Ultrasound Katharine Dennis, RDMS/RVT Tiffany Schultz, RDMS UNC Health Care Dept of General Ultrasound Introduction Learning Objectives Review common pediatric emergent ultrasound exams
Emergent Pediatric Ultrasound Katharine Dennis, RDMS/RVT Tiffany Schultz, RDMS UNC Health Care Dept of General Ultrasound Introduction Learning Objectives Review common pediatric emergent ultrasound exams
Total Parenteral Nutrition and Enteral Nutrition in the Home. Original Policy Date 12:2013
 MP 1.02.01 Total Parenteral Nutrition and Enteral Nutrition in the Home Medical Policy Section Durable Medical Equipment Issue Original Policy Date Last Review Status/Date Return to Medical Policy Index
MP 1.02.01 Total Parenteral Nutrition and Enteral Nutrition in the Home Medical Policy Section Durable Medical Equipment Issue Original Policy Date Last Review Status/Date Return to Medical Policy Index
Pediatric Surgical Emergencies Veronica Victorian, PA-C
 Pediatric Surgical Emergencies Veronica Victorian, PA-C Texas Children s Hospital Division of Pediatric General Surgery Assistant Professor, Baylor College of Medicine Objectives 1. Define Pediatric Surgical
Pediatric Surgical Emergencies Veronica Victorian, PA-C Texas Children s Hospital Division of Pediatric General Surgery Assistant Professor, Baylor College of Medicine Objectives 1. Define Pediatric Surgical
Objectives. Pediatric Mortality. Another belly pain. Gastroenteritis. Spewing & Pooing Child 4/18/16
 Gastro-tastrophies A Review of Pediatric GI Emergencies Objectives Discuss common presentations of Pediatric Abdominal Pain complaints Discuss work up and physical exam findings Discuss care, management
Gastro-tastrophies A Review of Pediatric GI Emergencies Objectives Discuss common presentations of Pediatric Abdominal Pain complaints Discuss work up and physical exam findings Discuss care, management
Chapter 14: Training in Radiology. DDSEP Chapter 1: Question 12
 DDSEP Chapter 1: Question 12 A 52-year-old white male presents for evaluation of sudden onset of abdominal pain and shoulder pain. His past medical history is notable for a history of coronary artery disease,
DDSEP Chapter 1: Question 12 A 52-year-old white male presents for evaluation of sudden onset of abdominal pain and shoulder pain. His past medical history is notable for a history of coronary artery disease,
Nasogastric tube. Stomach. Pylorus. Duodenum 1. Duodenum 2. Duodenum 3. Duodenum 4
 Esophagus Barium Swallow Stomach and Duodenum 4 year old Upper GI Nasogastric tube Stomach and Duodenum 4 year old Upper GI Nasogastric tube Stomach Pylorus Duodenum 1 Duodenum 2 Duodenum 3 Duodenum 4
Esophagus Barium Swallow Stomach and Duodenum 4 year old Upper GI Nasogastric tube Stomach and Duodenum 4 year old Upper GI Nasogastric tube Stomach Pylorus Duodenum 1 Duodenum 2 Duodenum 3 Duodenum 4
Endoscopic Treatment of Luminal Perforations and Leaks
 Endoscopic Treatment of Luminal Perforations and Leaks Ali A. Siddiqui, MD Professor of Medicine Director of Interventional Endoscopy Jefferson Medical College Philadelphia, PA When Do You Suspect a Luminal
Endoscopic Treatment of Luminal Perforations and Leaks Ali A. Siddiqui, MD Professor of Medicine Director of Interventional Endoscopy Jefferson Medical College Philadelphia, PA When Do You Suspect a Luminal
Chest X rays and Case Studies. No disclosures. Outline 5/31/2018. Carlo Manalo, M.D. Department of Radiology Loma Linda University Children s Hospital
 Chest X rays and Case Studies Carlo Manalo, M.D. Department of Radiology Loma Linda University Children s Hospital No disclosures. Outline Importance of history Densities delineated on radiography An approach
Chest X rays and Case Studies Carlo Manalo, M.D. Department of Radiology Loma Linda University Children s Hospital No disclosures. Outline Importance of history Densities delineated on radiography An approach
Role of imaging in the evaluation of the acute abdomen
 Prof. András Palkó MD, PhD Role of imaging in the evaluation of the acute abdomen Faculty of General Medicine University of Szeged Hungary 1 Definition Sudden onset of severe symptoms requiring emergency
Prof. András Palkó MD, PhD Role of imaging in the evaluation of the acute abdomen Faculty of General Medicine University of Szeged Hungary 1 Definition Sudden onset of severe symptoms requiring emergency
CT abdomen and pelvis
 CT abdomen and pelvis General indications: Assessment of vague abdominal symptoms (pain, colics,distenstion,...) Varifecation of a lesion discovered by other diagnostic modalities as US, barium,ivp, Staging
CT abdomen and pelvis General indications: Assessment of vague abdominal symptoms (pain, colics,distenstion,...) Varifecation of a lesion discovered by other diagnostic modalities as US, barium,ivp, Staging
Tracheoesophageal Fistula and Esophageal Atresia
 Patient and Family Education Tracheoesophageal Fistula and Esophageal Atresia What is tracheoesophageal fistula? The word fistula means abnormal connection. Tracheoesophageal fistula (TEF) is a condition
Patient and Family Education Tracheoesophageal Fistula and Esophageal Atresia What is tracheoesophageal fistula? The word fistula means abnormal connection. Tracheoesophageal fistula (TEF) is a condition
General Data. 王 X 村 78 y/o 男性
 General Data 王 X 村 78 y/o 男性 Chief Complaint Vomiting twice this early morning Fever up to 38.9ºC was noted Present Illness (1) Old CVA with left side weakness for more than 10 years and with bed ridden
General Data 王 X 村 78 y/o 男性 Chief Complaint Vomiting twice this early morning Fever up to 38.9ºC was noted Present Illness (1) Old CVA with left side weakness for more than 10 years and with bed ridden
Neonatal Perforated Gut: Etiology and Risk Factors
 Cronicon OPEN ACCESS EC PAEDIATRICS Research Article Mostafa Kotb 1 * and Marwa Beyaly 2 1 Pediatric Surgery Department, Alexandria Faculty of Medicine, Egypt. 2 Human Genetics Department, Medical Research
Cronicon OPEN ACCESS EC PAEDIATRICS Research Article Mostafa Kotb 1 * and Marwa Beyaly 2 1 Pediatric Surgery Department, Alexandria Faculty of Medicine, Egypt. 2 Human Genetics Department, Medical Research
Tubes and lines in neonatal chest radiograph
 Tubes and lines in neonatal chest radiograph Poster No.: C-1008 Congress: ECR 2014 Type: Educational Exhibit Authors: R. TUMMA, N. AHMED, V. Prasad ; Hyderabad/IN, 1 2 1 1 2 HYDERABAD, ANDHRA PRADESH/IN
Tubes and lines in neonatal chest radiograph Poster No.: C-1008 Congress: ECR 2014 Type: Educational Exhibit Authors: R. TUMMA, N. AHMED, V. Prasad ; Hyderabad/IN, 1 2 1 1 2 HYDERABAD, ANDHRA PRADESH/IN
Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased
 1 2 3 4 5 6 7 Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased Ingestion of Caustic Substances Poor Bowel Habits
1 2 3 4 5 6 7 Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased Ingestion of Caustic Substances Poor Bowel Habits
Medical application of transabdominal ultrasound in gastrointestinal diseases
 Medical application of transabdominal ultrasound in gastrointestinal diseases Hsiu-Po Wang Department of Emergency Medicine National Taiwan University Hospital Real-time ultrasound has become a standard
Medical application of transabdominal ultrasound in gastrointestinal diseases Hsiu-Po Wang Department of Emergency Medicine National Taiwan University Hospital Real-time ultrasound has become a standard
Critically Ill Children in Pediatric Surgery. No disclosures to report.
 Critically Ill Children in Pediatric Surgery Hillary J. Collyer RN, MSN, CPNP, CCRN Pediatric Surgery Nurse Practitioner Hasbro Children s Hospital Disclosure Information Speaker: Hillary Collyer No disclosures
Critically Ill Children in Pediatric Surgery Hillary J. Collyer RN, MSN, CPNP, CCRN Pediatric Surgery Nurse Practitioner Hasbro Children s Hospital Disclosure Information Speaker: Hillary Collyer No disclosures
UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN
 UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN Radiology Enterprises radiologyenterprises@gmail.com www.radiologyenterprises.com STOMACH AND SMALL BOWEL STOMACH AND SMALL BOWEL Swallowed air is a
UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN Radiology Enterprises radiologyenterprises@gmail.com www.radiologyenterprises.com STOMACH AND SMALL BOWEL STOMACH AND SMALL BOWEL Swallowed air is a
Gastrointestinal Emergencies CEN REVIEW 2017 MARY RALEY, BSN, RN, CEN, TCRN, TNSCC
 Gastrointestinal Emergencies CEN REVIEW 2017 MARY RALEY, BSN, RN, CEN, TCRN, TNSCC Gastrointestinal Emergencies is 7% of the CEN A. Acute abdomen B. Bleeding C. Cholecystitis D. Cirrhosis E. Diverticulitis
Gastrointestinal Emergencies CEN REVIEW 2017 MARY RALEY, BSN, RN, CEN, TCRN, TNSCC Gastrointestinal Emergencies is 7% of the CEN A. Acute abdomen B. Bleeding C. Cholecystitis D. Cirrhosis E. Diverticulitis
Basic Abdominal and Pelvic Imaging Concepts. David L. Smith, MD Assistant Professor of Radiology
 Basic Abdominal and Pelvic Imaging Concepts David L. Smith, MD Assistant Professor of Radiology Basic Imaging Concepts Contrast Resolution vs Spacial Resolution Spacial Resolution......refers to the ability
Basic Abdominal and Pelvic Imaging Concepts David L. Smith, MD Assistant Professor of Radiology Basic Imaging Concepts Contrast Resolution vs Spacial Resolution Spacial Resolution......refers to the ability
X-ray Corner. Imaging of the Small Bowel. Pantongrag-Brown L. Case 1. A 63-year-old man presented with abdominal pain, nausea and vomiting.
 THAI J 42 Imaging of the Small Bowel GASTROENTEROL 2015 X-ray Corner Imaging of the Small Bowel Pantongrag-Brown L Small bowel is the longest tubular organ in the body, about 18-22 feet. It is anchored
THAI J 42 Imaging of the Small Bowel GASTROENTEROL 2015 X-ray Corner Imaging of the Small Bowel Pantongrag-Brown L Small bowel is the longest tubular organ in the body, about 18-22 feet. It is anchored
NEC. cathy e. shin childrens hospital los angeles department of surgery university of southern california keck school of medicine
 NEC cathy e. shin childrens hospital los angeles department of surgery university of southern california keck school of medicine Necrotizing enterocolitis (NEC) the most common and most lethal disease
NEC cathy e. shin childrens hospital los angeles department of surgery university of southern california keck school of medicine Necrotizing enterocolitis (NEC) the most common and most lethal disease
Pediatric Learning Solutions A clinical education program exclusively for pediatric professionals
 Pediatric Learning Solutions A clinical education program exclusively for pediatric professionals The following Pediatric Learning Solutions courses align to focus areas of the Neonatal CCRN Exam Content
Pediatric Learning Solutions A clinical education program exclusively for pediatric professionals The following Pediatric Learning Solutions courses align to focus areas of the Neonatal CCRN Exam Content
No Disclosures. Approach to Abdominal Radiographs
 Approach to Abdominal Radiographs Tapas K. Tejura, M.D. Assistant Professor of Clinical Radiology Keck Medical Center of USC tapas.tejura@med.usc.edu No Disclosures 34-year-old male with acute abdominal
Approach to Abdominal Radiographs Tapas K. Tejura, M.D. Assistant Professor of Clinical Radiology Keck Medical Center of USC tapas.tejura@med.usc.edu No Disclosures 34-year-old male with acute abdominal
Interesting Pediatric ultrasound cases. Presented by: Falguni Patel (RDMS, RVT)
") Interesting Pediatric ultrasound cases Presented by: Falguni Patel (RDMS, RVT) Role of ultrasound to rule out Appendicitis Overview: Ultrasound is relatively inexpensive, safe and quick solution to rule
Interesting Pediatric ultrasound cases Presented by: Falguni Patel (RDMS, RVT) Role of ultrasound to rule out Appendicitis Overview: Ultrasound is relatively inexpensive, safe and quick solution to rule
HREE Questions. Setting 3: Inpatient Facilities. Block
 Block HREE Questions Setting 3: Inpatient Facilities You have general admitting privileges to the hospital. You may see patients in the critical care unit, the pediatrics unit, the maternity unit, or recovery
Block HREE Questions Setting 3: Inpatient Facilities You have general admitting privileges to the hospital. You may see patients in the critical care unit, the pediatrics unit, the maternity unit, or recovery
Paediatric surgical emergencies. Mani Thyagarajan BWCH
 Paediatric surgical emergencies Mani Thyagarajan BWCH General points Always discuss Call consultant for help ASAP CT scan is a bad modality in paediatrics Ultrasound? Intussusception? Renal colic? UTI
Paediatric surgical emergencies Mani Thyagarajan BWCH General points Always discuss Call consultant for help ASAP CT scan is a bad modality in paediatrics Ultrasound? Intussusception? Renal colic? UTI
Necrotizing Enterocolitis: the role of ultrasound in the assessment of bowel viability
 Necrotizing Enterocolitis: the role of ultrasound in the assessment of bowel viability Ricardo Faingold, MD. Department of Medical Imaging The Montreal Children s Hospital McGill University SPR Vancouver
Necrotizing Enterocolitis: the role of ultrasound in the assessment of bowel viability Ricardo Faingold, MD. Department of Medical Imaging The Montreal Children s Hospital McGill University SPR Vancouver
CASE CONFERENCE GASTRIC VOLVULUS PIKOM, MD NONGLUK, MD; RADIOLOGIST
 CASE CONFERENCE GASTRIC VOLVULUS PIKOM, MD NONGLUK, MD; RADIOLOGIST IDENTIFICATION DATA ผ ป วยเด กชายไทย อาย 13 ว น เช อชาต ไทย ส ญชาต ไทย ภ ม ล าเนา จ งหว ด อ ท ยธาน เข าร บการร กษาท รพ.มหาว ทยาล ยนเรศวรว
CASE CONFERENCE GASTRIC VOLVULUS PIKOM, MD NONGLUK, MD; RADIOLOGIST IDENTIFICATION DATA ผ ป วยเด กชายไทย อาย 13 ว น เช อชาต ไทย ส ญชาต ไทย ภ ม ล าเนา จ งหว ด อ ท ยธาน เข าร บการร กษาท รพ.มหาว ทยาล ยนเรศวรว
ACUTE ABDOMEN IN OLDER CHILDREN. Carlos J. Sivit M.D.
 ACUTE ABDOMEN IN OLDER CHILDREN Carlos J. Sivit M.D. ACUTE ABDOMEN Clinical condition characterized by severe abdominal pain developing over several hours ACUTE ABDOMINAL PAIN Common childhood complaint
ACUTE ABDOMEN IN OLDER CHILDREN Carlos J. Sivit M.D. ACUTE ABDOMEN Clinical condition characterized by severe abdominal pain developing over several hours ACUTE ABDOMINAL PAIN Common childhood complaint
Pitfalls of the Pediatric Chest and Abdomen SPR 2017
 Pitfalls of the Pediatric Chest and Abdomen SPR 2017 Richard I. Markowitz, MD, FACR Children s Hospital of Philadelphia Perelman School of Medicine University of Pennsylvania No Disclosures Cognitive Perceptual
Pitfalls of the Pediatric Chest and Abdomen SPR 2017 Richard I. Markowitz, MD, FACR Children s Hospital of Philadelphia Perelman School of Medicine University of Pennsylvania No Disclosures Cognitive Perceptual
Physical Exam. Vitals stable on room air Abdomen soft, non-distented Normal external genitalia Patent anus No limb anomalies
 Case Presentation 1 day-old full-term baby girl noted to have drooling of saliva and increased secretions at birth Fetal US @32wks had shown polyhydramnios Birth weight 3515g Apgar 7@1min and 8@5min Unable
Case Presentation 1 day-old full-term baby girl noted to have drooling of saliva and increased secretions at birth Fetal US @32wks had shown polyhydramnios Birth weight 3515g Apgar 7@1min and 8@5min Unable
Spleen indications of splenectomy complications OPSI
 Intestinal obstruction Differences between adynamic ileus and mechanical obstruction Aetiology Pathophysiology (Cluster contractions- bowel proximal to the obstruction dilate- wall of obstructed gut is
Intestinal obstruction Differences between adynamic ileus and mechanical obstruction Aetiology Pathophysiology (Cluster contractions- bowel proximal to the obstruction dilate- wall of obstructed gut is
RADIOLOGY REQUEST MANUAL. (615)
") RADIOLOGY REQUEST MANUAL www.vanderbiltchildrens.com RADIOLOGY REQUEST MANUAL EXAM PROTOCOL QUESTIONS? Please call: DIAGNOSTIC RADIOLOGY (X-RAY) Pager (615) 835-1714 CT (615) 936-4920 MRI (615) 936-4933
RADIOLOGY REQUEST MANUAL www.vanderbiltchildrens.com RADIOLOGY REQUEST MANUAL EXAM PROTOCOL QUESTIONS? Please call: DIAGNOSTIC RADIOLOGY (X-RAY) Pager (615) 835-1714 CT (615) 936-4920 MRI (615) 936-4933
Gastrointestinal tract
 Chapter 7 Gastrointestinal tract NORMAL SONOGRAPHIC ANATOMY Sonographically, the fetal stomach is visible from 9 weeks of gestation as a sonolucent cystic structure in the upper left quadrant of the abdomen.
Chapter 7 Gastrointestinal tract NORMAL SONOGRAPHIC ANATOMY Sonographically, the fetal stomach is visible from 9 weeks of gestation as a sonolucent cystic structure in the upper left quadrant of the abdomen.
A novel plain abdominal radiograph sign to diagnose malrotation with volvulus
 A novel plain abdominal radiograph sign to diagnose malrotation with volvulus Nataraja RM 1, Mahomed AA 1* 1. Department of Paediatric Surgery, Royal Alexandra Hospital for Sick Children, Brighton,UK *
A novel plain abdominal radiograph sign to diagnose malrotation with volvulus Nataraja RM 1, Mahomed AA 1* 1. Department of Paediatric Surgery, Royal Alexandra Hospital for Sick Children, Brighton,UK *
Approach to Pediatric Abdominal X-Rays
 Approach to Pediatric Abdominal X-Rays Ben Pi, Dr. J. Jaremko PedsCases University of Alberta Hello and welcome to a PedsCases podcast on a basic approach to interpreting pediatric abdominal x-rays. My
Approach to Pediatric Abdominal X-Rays Ben Pi, Dr. J. Jaremko PedsCases University of Alberta Hello and welcome to a PedsCases podcast on a basic approach to interpreting pediatric abdominal x-rays. My
ASSESSING THE PLAIN ABDOMINAL RADIOGRAPH M A A M E F O S U A A M P O F O
 ASSESSING THE PLAIN ABDOMINAL RADIOGRAPH M A A M E F O S U A A M P O F O Introduction The abdomen (less formally called the belly, stomach, is that part of the body between the thorax (chest) and pelvis,
ASSESSING THE PLAIN ABDOMINAL RADIOGRAPH M A A M E F O S U A A M P O F O Introduction The abdomen (less formally called the belly, stomach, is that part of the body between the thorax (chest) and pelvis,
Abdomen and Pelvis CT (1) By the end of the lecture students should be able to:
 By the end of the lecture students should be able to:") RAD 451 Abdomen and Pelvis CT (1) By the end of the lecture students should be able to: State the common indications for Abdomen and pelvis CT exams Identify possible contra indications for Abdomen and
RAD 451 Abdomen and Pelvis CT (1) By the end of the lecture students should be able to: State the common indications for Abdomen and pelvis CT exams Identify possible contra indications for Abdomen and
Good morning! July 24, 2014
 Good morning! July 24, 2014 Prep #1 A 2-year-old boy presents to your office with a 2-day history of swelling of the right eye. He has been otherwise well. There are scattered insect bites on his body,
Good morning! July 24, 2014 Prep #1 A 2-year-old boy presents to your office with a 2-day history of swelling of the right eye. He has been otherwise well. There are scattered insect bites on his body,
Pediatric Radiology Curriculum
 Pediatric Radiology Curriculum Introduction: Greetings! Welcome to your pediatric radiology rotation. Whether this is your first trip with us or you are back for additional rotations, your time here should
Pediatric Radiology Curriculum Introduction: Greetings! Welcome to your pediatric radiology rotation. Whether this is your first trip with us or you are back for additional rotations, your time here should
Gastrointestinal Disorders. Disorders of the Esophagus 3/7/2013. Congenital Abnormalities. Achalasia. Not an easy repair. Types
 Gastrointestinal Disorders Congenital Abnormalities Disorders of the Esophagus Types Stenosis Atresia Fistula Newborn aspirates while feeding. Pneumonia Not an easy repair Achalasia Lack of relaxation
Gastrointestinal Disorders Congenital Abnormalities Disorders of the Esophagus Types Stenosis Atresia Fistula Newborn aspirates while feeding. Pneumonia Not an easy repair Achalasia Lack of relaxation
The Case Begins. The case continued. Necrotizing Enterocolitis
 Bugs, Drugs and Things that go Bump in the Night From ghoulies to ghosties and long leggety beasties & things that go bump in the night, good lord deliver us Old Cornish Prayer Caring for premature infant
Bugs, Drugs and Things that go Bump in the Night From ghoulies to ghosties and long leggety beasties & things that go bump in the night, good lord deliver us Old Cornish Prayer Caring for premature infant
Pediatric ER Half-day Rounds October 12, 2011 Dr. Karen Bailey
 Pediatric ER Half-day Rounds October 12, 2011 Dr. Karen Bailey Objectives to identify various enteral and vascular access lines what do they look like? indications & contraindications proper placement
Pediatric ER Half-day Rounds October 12, 2011 Dr. Karen Bailey Objectives to identify various enteral and vascular access lines what do they look like? indications & contraindications proper placement
Radiology. Undergraduate Radiology Sample Questions
 Radiology Undergraduate Radiology Sample Questions April 2012 The following examples are offered of questions that might be used to assess undergraduate radiology. There are 3 different styles: An OSCE
Radiology Undergraduate Radiology Sample Questions April 2012 The following examples are offered of questions that might be used to assess undergraduate radiology. There are 3 different styles: An OSCE
Imaging of Thoracic Trauma: Tips and Traps. Arun C. Nachiappan, MD Associate Professor of Clinical Radiology University of Pennsylvania
 Imaging of Thoracic Trauma: Tips and Traps Arun C. Nachiappan, MD Associate Professor of Clinical Radiology University of Pennsylvania None Disclosures Objectives Describe blunt and penetrating traumatic
Imaging of Thoracic Trauma: Tips and Traps Arun C. Nachiappan, MD Associate Professor of Clinical Radiology University of Pennsylvania None Disclosures Objectives Describe blunt and penetrating traumatic
PAEDIATRIC GASTROINTESTINAL RADIOLOGY
 Objective Guide to Radiology of the Paediatric Intestinal Tract Responsibility / Registrar Frequency As required Associated Documents : RADFLPAEPR003 Contrast mixes RADFLPAEPR001 Paediatric Barium swallow
Objective Guide to Radiology of the Paediatric Intestinal Tract Responsibility / Registrar Frequency As required Associated Documents : RADFLPAEPR003 Contrast mixes RADFLPAEPR001 Paediatric Barium swallow
Interventional Radiology for Solid Organ Trauma. Case Study 8/17/2017. Diagnosis? Case Study (cont d)
") Interventional Radiology for Solid Organ Trauma Jamie Gallivan RN, BSN Interventional Radiology Case Study 6 y/o boy fell out of 2 nd story window onto concrete Hemodynamically stable at scene Arrival
Interventional Radiology for Solid Organ Trauma Jamie Gallivan RN, BSN Interventional Radiology Case Study 6 y/o boy fell out of 2 nd story window onto concrete Hemodynamically stable at scene Arrival
Pediatric Radiology Update
 Pediatric Radiology Update Douglas Rivard, DO Vice Chairman, Radiology Dept Children s Mercy Hospital Asst Professor of Radiology University of Missouri-Kansas City Objectives Review radiation biology
Pediatric Radiology Update Douglas Rivard, DO Vice Chairman, Radiology Dept Children s Mercy Hospital Asst Professor of Radiology University of Missouri-Kansas City Objectives Review radiation biology
Request Card Task ANSWERS
 Request Card Task ANSWERS Medical Student Workbook Author: Dr Sam Leach, SpR Case 1 What differential diagnoses are most likely? Which investigation is most appropriate? Case 1 The most likely diagnosis
Request Card Task ANSWERS Medical Student Workbook Author: Dr Sam Leach, SpR Case 1 What differential diagnoses are most likely? Which investigation is most appropriate? Case 1 The most likely diagnosis
Neonatal Intensive Care Unit Skills Checklist
 _ XXX-XX- Print Name Last 4 of SS # Date Completed Directions Please circle a value for each question to provide us and the interested facilities with an assessment of your clinical experience. These values
_ XXX-XX- Print Name Last 4 of SS # Date Completed Directions Please circle a value for each question to provide us and the interested facilities with an assessment of your clinical experience. These values
SUMPh N. Testemitanu Radiology and Medical imaging department PEDIATRIC IMAGING. M. Crivceanschii, assistant professor
 SUMPh N. Testemitanu Radiology and Medical imaging department PEDIATRIC IMAGING M. Crivceanschii, assistant professor GOALS AND OBJECTIVES to be aware of the role of modern diagnostic imaging modalities
SUMPh N. Testemitanu Radiology and Medical imaging department PEDIATRIC IMAGING M. Crivceanschii, assistant professor GOALS AND OBJECTIVES to be aware of the role of modern diagnostic imaging modalities
Anti-Reflux Surgery in Cerebral Palsy Patients
 Anti-Reflux Surgery in Cerebral Palsy Patients Cecostomy for Bowel Management Surgery for Prenatally Identified Congenital Lung Lesions Dr. Mike Giacomantonio IWK Health Centre, Halifax, NS G. E. Reflux
Anti-Reflux Surgery in Cerebral Palsy Patients Cecostomy for Bowel Management Surgery for Prenatally Identified Congenital Lung Lesions Dr. Mike Giacomantonio IWK Health Centre, Halifax, NS G. E. Reflux
Intestinal Obstruction Clinical Presentation & Causes
 Intestinal Obstruction Clinical Presentation & Causes V Chidambaram-Nathan Consultant Transplant and General Surgeon Sheffield Kidney Institute Northern General Hospital Intestinal Obstruction One of the
Intestinal Obstruction Clinical Presentation & Causes V Chidambaram-Nathan Consultant Transplant and General Surgeon Sheffield Kidney Institute Northern General Hospital Intestinal Obstruction One of the
Question 1 History. Likely Diagnosis Differential. Further Investigation or Management. Requires Paediatric Surgical referral for laparotomy
 Question 1 Male newborn spilling green tinged vomit day 1 of life Imaging Abdominal X-Rays performed on 03/05/2012 Upper and lower gastrointestinal contrast studies performed on 03/05/2012 Abdominal X-Rays
Question 1 Male newborn spilling green tinged vomit day 1 of life Imaging Abdominal X-Rays performed on 03/05/2012 Upper and lower gastrointestinal contrast studies performed on 03/05/2012 Abdominal X-Rays
Document Title: Non-Traumatic Abdominal Pain/Abdominal Emergencies. Author(s): Joseph House (University of Michigan), MD 2012
: Joseph House (University of Michigan), MD 2012") Project: Ghana Emergency Medicine Collaborative Document Title: Non-Traumatic Abdominal Pain/Abdominal Emergencies Author(s): Joseph House (University of Michigan), MD 2012 License: Unless otherwise noted,
Project: Ghana Emergency Medicine Collaborative Document Title: Non-Traumatic Abdominal Pain/Abdominal Emergencies Author(s): Joseph House (University of Michigan), MD 2012 License: Unless otherwise noted,
The Physician as Medical Illustrator
 The Physician as Medical Illustrator Francois Luks Arlet Kurkchubasche Division of Pediatric Surgery Wednesday, December 9, 2015 Week 5 A good picture is worth a 1,000 bad ones How to illustrate an operation
The Physician as Medical Illustrator Francois Luks Arlet Kurkchubasche Division of Pediatric Surgery Wednesday, December 9, 2015 Week 5 A good picture is worth a 1,000 bad ones How to illustrate an operation
Pediatric Gastroenterology Referral Guidelines
 Suggested Pre-Referral Workup This is a general suggestion of possible testing to confirm a suspected diagnosis. Although referrals will be accepted without the suggested work up being complete, to ensure
Suggested Pre-Referral Workup This is a general suggestion of possible testing to confirm a suspected diagnosis. Although referrals will be accepted without the suggested work up being complete, to ensure
Shedding Light on Neonatal X-rays. Objectives. Indications for X-Rays 5/14/2018
 Shedding Light on Neonatal X-rays Barbara C. Mordue, MSN, NNP-BC Neonatal Nurse Practitioner LLUH Children s Hospital, NICU Objectives Utilize a systematic approach to neonatal x-ray interpretation Identify
Shedding Light on Neonatal X-rays Barbara C. Mordue, MSN, NNP-BC Neonatal Nurse Practitioner LLUH Children s Hospital, NICU Objectives Utilize a systematic approach to neonatal x-ray interpretation Identify
Imaging Children with Acute Abdominal Pain -- Role/Protocols of US, CT, MR
 Imaging Children with Acute Abdominal Pain -- Role/Protocols of US, CT, MR Kimberly E. Applegate, MD, MS Emory University Financial disclosures: AIM (American Imaging Management) radiation protection advisory
Imaging Children with Acute Abdominal Pain -- Role/Protocols of US, CT, MR Kimberly E. Applegate, MD, MS Emory University Financial disclosures: AIM (American Imaging Management) radiation protection advisory
11/21/2017 JUST THE FACTS!
 JUST THE FACTS! Katharine C Long, MD Establish differential diagnosis for the critically ill infant Create management approach for the critically ill infant Identify laboratory tests and interventions
JUST THE FACTS! Katharine C Long, MD Establish differential diagnosis for the critically ill infant Create management approach for the critically ill infant Identify laboratory tests and interventions
Disclosure of Commercial Interest
 Evidence Based Imaging: Getting the Right Study for Your Patient Johanne E. Dillon, MD, FAAP Pediatric Radiology UK HealthCare Assistant Professor of Radiology and Pediatrics University of Kentucky College
Evidence Based Imaging: Getting the Right Study for Your Patient Johanne E. Dillon, MD, FAAP Pediatric Radiology UK HealthCare Assistant Professor of Radiology and Pediatrics University of Kentucky College
Small bowel atresia. Great Ormond Street Hospital for Children NHS Foundation Trust: Information for Families
 Great Ormond Street Hospital for Children NHS Foundation Trust: Information for Families Small bowel atresia This information sheet from Great Ormond Street Hospital explains the causes, symptoms and treatment
Great Ormond Street Hospital for Children NHS Foundation Trust: Information for Families Small bowel atresia This information sheet from Great Ormond Street Hospital explains the causes, symptoms and treatment
PEDIATRICS. Module Topic/Content Student Learning Outcomes Resources Clinical Assessment Activities Course/Clinical Outcomes
 PEDIATRICS N332 Outline 1 Welcome back: Instructor Role and Student Role Discuss course requirements. Explain personal learning style and study patterns. Explain critical thinking and clinical judgment
PEDIATRICS N332 Outline 1 Welcome back: Instructor Role and Student Role Discuss course requirements. Explain personal learning style and study patterns. Explain critical thinking and clinical judgment
Bowel Obstructions in Older Children
 Residents Section Pattern of the Month Hryhorczuk et al. owel Obstructions in Older Children Residents Section Pattern of the Month Residents inradiology nastasia Hryhorczuk 1 Edward Y. Lee 1,2 Ronald
Residents Section Pattern of the Month Hryhorczuk et al. owel Obstructions in Older Children Residents Section Pattern of the Month Residents inradiology nastasia Hryhorczuk 1 Edward Y. Lee 1,2 Ronald
Safe Answers For The American Board of Surgery Certifying Exam & Recertifying Exam
 Safe Answers For The American Board of Surgery Certifying Exam & Recertifying Exam By Sarmad Aji, MD., FACS. A comprehensive review of the most commonly asked questions on the American Board of Surgery
Safe Answers For The American Board of Surgery Certifying Exam & Recertifying Exam By Sarmad Aji, MD., FACS. A comprehensive review of the most commonly asked questions on the American Board of Surgery
Pathology of Intestinal Obstruction. Dr. M. Madhavan, MBBS., MD., MIAC, Professor of Pathology Saveetha Medical College
 Pathology of Intestinal Obstruction Dr. M. Madhavan, MBBS., MD., MIAC, Professor of Pathology Saveetha Medical College Pathology of Intestinal Obstruction Objectives list the causes of intestinal obstruction
Pathology of Intestinal Obstruction Dr. M. Madhavan, MBBS., MD., MIAC, Professor of Pathology Saveetha Medical College Pathology of Intestinal Obstruction Objectives list the causes of intestinal obstruction
Management of Common Paediatric Surgical G.I. Problems
 Management of Common Paediatric Surgical G.I. Problems Dr. Loh Ser Kheng Dale Lincoln Senior Consultant Department of Paediatric Surgery National University Hospital National University Health System Tongue
Management of Common Paediatric Surgical G.I. Problems Dr. Loh Ser Kheng Dale Lincoln Senior Consultant Department of Paediatric Surgery National University Hospital National University Health System Tongue
Sick or not sick? Objectives. Bilious vomiting. Deadly Misdiagnoses: Kids with GI Complaints. Ronald Dieckmann, MD. Problems in assessment
 Deadly Misdiagnoses: Kids with GI Complaints Objectives Understand key assessment techniques for recognition of serious illness in children. Ronald Dieckmann, MD Professor of Clinical Pediatrics and Emergency
Deadly Misdiagnoses: Kids with GI Complaints Objectives Understand key assessment techniques for recognition of serious illness in children. Ronald Dieckmann, MD Professor of Clinical Pediatrics and Emergency
Diagnostic Imaging
 www.fisiokinesiterapia.biz Diagnostic Imaging Diagnostic Imaging is no longer limited to radiography. Major technological advancements have lead to the use of new and improved imaging technologies. The
www.fisiokinesiterapia.biz Diagnostic Imaging Diagnostic Imaging is no longer limited to radiography. Major technological advancements have lead to the use of new and improved imaging technologies. The
GI POTPOURRI. What is the best diagnostic test? Presentation #1: Vomiting. I have no disclosures
 I have no disclosures GI POTPOURRI Andi Marmor, MD Associate Professor, Pediatrics UCSF, San Francisco General Hospital Presentation #1: Vomiting Caraway, a 3 week old boy, is brought to your walk-in clinic
I have no disclosures GI POTPOURRI Andi Marmor, MD Associate Professor, Pediatrics UCSF, San Francisco General Hospital Presentation #1: Vomiting Caraway, a 3 week old boy, is brought to your walk-in clinic
SWISS SOCIETY OF NEONATOLOGY. Prenatal diagnosis and postnatal management of meconium pseudocysts
 SWISS SOCIETY OF NEONATOLOGY Prenatal diagnosis and postnatal management of meconium pseudocysts September 2007 2 Burch E, Caduff JH, Hodel M, Berger TM, Neonatal and Pediatric Intensive Care Unit (BE,
SWISS SOCIETY OF NEONATOLOGY Prenatal diagnosis and postnatal management of meconium pseudocysts September 2007 2 Burch E, Caduff JH, Hodel M, Berger TM, Neonatal and Pediatric Intensive Care Unit (BE,
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal pain, abdominal considerations in, 183 184 antiemetics in, 182 auscultation in, 170 C-reactive protein in, 174 175 character
Index Note: Page numbers of article titles are in boldface type. A Abdominal pain, abdominal considerations in, 183 184 antiemetics in, 182 auscultation in, 170 C-reactive protein in, 174 175 character
Pediatric Surgery Residency Program Division of General and Thoracic Surgery Hospital for Sick Children Year 1. Goals and Objectives
 Pediatric Surgery Residency Program Division of General and Thoracic Surgery Hospital for Sick Children Year 1 Goals and Objectives Revised June 13 2010 GOALS To develop the skills necessary to assume
Pediatric Surgery Residency Program Division of General and Thoracic Surgery Hospital for Sick Children Year 1 Goals and Objectives Revised June 13 2010 GOALS To develop the skills necessary to assume