Ductal-dependent cardiac anomalies. Donna Cheung Pediatric Emergency Rotation January 31, 2014
|
|
|
- Ann Richards
- 5 years ago
- Views:
Transcription

1 Ductal-dependent cardiac anomalies Donna Cheung Pediatric Emergency Rotation January 31, 2014
2 Case 1 A 6 day old Caucasian male presents to the ER with poor feeding and SOB. He was born FT via VD with an uncomplicated antenatal period. APGARs were 9 and 9 for 1 and 5 min, BW was 3.2kg. He was sent home on day 2 of life for routine WCC in 1 week. He was well appearing but his skin was slightly dark / had a black-purple hue since birth. On discharge he initially took 2oz of Enfamil formula Q3H but gradually since then he has progressed to taking 1 oz of formula Q3H which takes him an hour to feed associated with SOB and occasionally sweating. He was also noted to be sweating excessively sometimes when he sleeps and has been sleeping a lot; when he is not trying to take the hour to feed, he is sleeping. When awoken he is very irritable.

3 Case 1 His vitals on presentation are: T37.2C RR80 P170 BPs - RUL 68/40 LUL 65/39 RLL 67/41 LLL 68/39. Weight 2.7kg. 02 at of RUL is 90% but of LLL is 58%. Examination does not reveal a murmur but he has a gallop rhythm, his liver is 2cm below the costal margin and all his pulses are equally reduced. Of the following the MOST likely diagnosis is: A. Coarctation of the Aorta B. Transposition of the Great Arteries C. Hypoplastic Left Heart Syndrome D. Hypertrophic Cardiomyopathy secondary to Gestational Diabetes
4 Ductal-dependent cardiac anomalies Neonates with congenital heart lesions may not be symptomatic during the birth hospitalization because the ductus arteriosus has not yet closed but they often present by two weeks of age. The lesions not diagnosed prior to discharge were primarily ductal dependent: coarctation of the aorta, interrupted aortic arch, aortic stenosis, hypoplastic left heart syndrome, and transposition of the great arteries. Closure of a patent ductus arteriosus can precipitate rapid clinical deterioration with potentially life-threatening consequences (ie, severe metabolic acidosis, seizures, cardiogenic shock, cardiac arrest, or end-organ injury).
5 Ductal-dependent cardiac anomalies Parents most commonly notice difficulty with feeding: intake of a limited volume of milk, feedings that are taking too long or are frequently interrupted by sleeping or resting, choking, gagging, +/- vomiting. Infants may have respiratory distress worse with feedings, or a persistent cough or wheeze. Other manifestations include: Color changes, such as central cyanosis or persistent pallor Excessive, unexplained irritability Excessive sweating that is increased with feeding and may occur during sleep Poor weight gain Decreased activity or excessive sleeping Delay in motor milestones
6 Hypoplastic Left Heart Syndrome 2 in 1,000 live births 3% of congenital heart disease hypoplasia of the mitral/aortic valves to valvar atresia virtually always coarctation of the aorta, and the left ventricle is markedly hypoplastic and dysfunctional infants may initially appear well, the only clinical finding may be cyanosis, which may be overlooked soft murmur or absence of a murmur because the blood flow typically is not turbulent

7 because the ductus arteriosus must supply circulation to the area distal to the area of aortic arch hypoplasia, the oxygen saturation is reduced in the lower body due to the obligate ductal right-to-left shunt of desaturated right heart blood.
8 Why not the other options? Coarctation of the aorta : absence of a blood pressure discrepancy in the neonate described*** Hypertrophic cardiomyopathy: high-pitched murmur, no oxygen saturation disparity between arm and leg. Transposition of the great vessels: it involves the left heart supplying well-saturated blood flow to the pulmonary artery, ductus arteriosus, and lower body, while the desaturated blood from the right heart travels to the aorta and upper body, thus resulting in lower saturation in the upper extremities compared to the lower extremities

9 Case 2 A 9 day old male presents to the ER with tachypnea. Antenatal and delivery periods were uncomplicated. He went home with his mother with no concerns on day 2 of life. Tachypnea worsened rapidly over 2 days. In the ER: T37.6C P180 RR85 RUL BP 85/48 LLL BP 65/37. He has a 2/6 systolic murmur in the ULSE. Lower limb pulses are not palpable. Which of the following is NOT appropriate in managing this patient. A. Take off an ABG B. Insert a urinary catheter C. Bolus with N/S 10mL/kg D. Administer Alprostadil 0.05mcg/kg/min

10 Option C again? ABGs monitor for acidosis Insertion of urinary catheter allows for monitoring of urine output and renal perfusion Alprostadil - prostaglandin E 1 : maintains patency of the ductus arteriosus. The dose is mcg/kg/min. The neonate in the vignette is not in shock and thus a bolus is not necessary. Management of CHF involves diuretics and inotropic drugs.

11 Thank you!

12 References Question 92 of 2012 PREP Questions and the accompanying explanation 3.
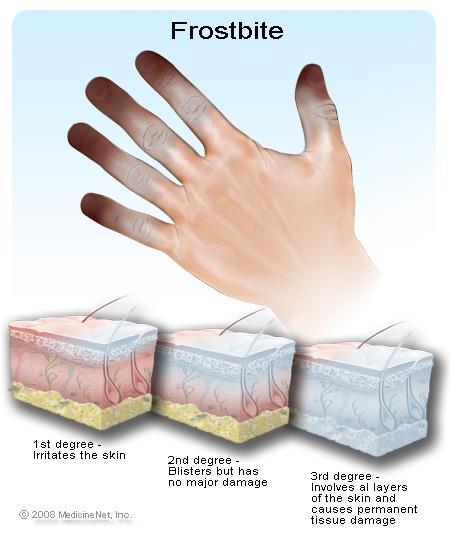
13 Frostbite Jessica Cardona PGY1 Jackson Memorial Hospital Pediatrics Department
14 Question 1 An 8 year old male is brought in by EMS from an icy mountain. He was with his family skiing but was separated from them and alone in the cold for approximately 4 hours. On arrival to the ED, vitals were T 36C, HR 70, RR 20, BP 90/50. On PE, patient is alert and oriented but shivering. You notice large blisters on both of his feet that contain clear fluid surrounded by edema and erythema. The patient has no past medical history. This type of finding would be considered:
15 Question 1 A. First degree frostbite B. Second degree frostbite C. Third degree frostbite D. Fourth degree frostbite
16 Question 1 A. First degree frostbite B. Second degree frostbite C. Third degree frostbite D. Fourth degree frostbite
17 Question 1-Answers The answer is B. First-degree frostbite tend to be very superficial and is characterized by a central area of pallor and anesthesia of the skin surrounded by edema. Second-degree frostbite is recognized by large blisters containing clear fluid surrounded by edema and erythema, developing within 24 hours and extending to or nearly to the tips of digits. The blisters can develop an eschar but it eventually sloughs off to reveal healthy granulation tissue with no tissue loss.
18 Question 1- Answers Third-degree frostbite is different from seconddegree in that the injury is deeper and the blisters are smaller, hemorrhagic and more proximal. The skin forms a black eschar in one to several weeks. Fourth-degree frostbite, which extends to muscle and bone, involves complete tissue necrosis. Mummification can be seen in 4 to 10 days.
19
20 Question 2 A 13 year old female is brought it by EMS after being found unconscious by an ice fishing lake in Michigan. It is unclear how long she has been exposed to the cold, but it is estimated that she has been by the fishing lake for about 4 hours. After being given pre-hospital care, the patient's vitals were rectal temperature of 35 degrees celsius, HR 60, RR 15, BP 100/60, O2 sat of 97% on RA. Once airway, breathing and circulation are assessed, preliminary studies are ordered. PE exam reveals a lethargic female with cold, significant for pale extremities with small blisters that appear hemorrhagic on feet and hands. Of the following, which would be the ideal treatments used for frostbite?
21 Question 2 - Answers A. Rewarming with water heated no higher than 36ºC as to prevent a painful warming process B. intravenous heparin given along with tetanus prophylaxis C. intra-arterial tpa given along with tetanus prophylaxis D. debridment of blisters and consult surgery
22 Question 2 - Answers A. Rewarming with water heated no higher than 36ºC as to prevent a painful warming process B. intravenous heparin given along with tetanus prophylaxis C. intra-arterial tpa given along with tetanus prophylaxis D. debridment of blisters and consult surgery
23 Question 2--Answers The answer is C. Several studies have been done in demonstrating the benefit from tpa, which helps prevent vascular thrombosis of the frostbite affected tissue. The recommended dose is a bolus of two to four mg followed by an infusion started 0.5 to 1 mg/hour given via the femoral or brachial artery * (child dose mg/kg per hour). Repeat angiograms were done every 8 to 12 hours and treatment was continued until perfusion was restored or a time limit of 48 hours was reached. There is no evidence that intravenous heparin alone improves outcomes in frostbite. Tetanus is a reported complication of frostbite, which is why prophylaxis is recommended.
24 Questions 2 Answers Rewarming is most effectively accomplished by immersing the affected area in water heated to 37º to 39ºC, ideally in a whirlpool. Higher temperatures do not warm the injured area any faster and cause the warming process to be much more painful. Dry heat is difficult to regulate and is therefore not used. There is some discord on the management of frostbiteinduced blisters. Some believe blister fluid should be drained to eliminate high concentrations of inflammatory mediators.
25 Questions 2 Answers The other, more conservative approach is to drain, debride, and bandage large non-hemorrhagic bullae that interfere with movement, for instance over joints. Hemorrhagic bullae of comparable size and location are drained by aspiration, but are not debrided. They usually reflect more significant damage to the microvasculature. Other minor bullae should be left intact.
26 References An Open-Label Study to Evaluate the Safety and Efficacy of Tissue Plasminogen Activator in Treatment of Severe Frostbite Journal of Trauma Injury and Critical Care Dec 2005 Volume 59 Issue 6 Uptodate: Frostbite Uptodate: Treatment of hypothermia in children Low-dose tissue plasminogen activator thrombolysis in children. J Pediatr Hematol Oncol May;25(5):
Frostbite. Jessica Cardona PGY1 Jackson Memorial Hospital Pediatrics Department
 Frostbite Jessica Cardona PGY1 Jackson Memorial Hospital Pediatrics Department Question 1 An 8 year old male is brought in by EMS from an icy mountain. He was with his family skiing but was separated from
Frostbite Jessica Cardona PGY1 Jackson Memorial Hospital Pediatrics Department Question 1 An 8 year old male is brought in by EMS from an icy mountain. He was with his family skiing but was separated from
How to Recognize a Suspected Cardiac Defect in the Neonate
 Neonatal Nursing Education Brief: How to Recognize a Suspected Cardiac Defect in the Neonate https://www.seattlechildrens.org/healthcareprofessionals/education/continuing-medical-nursing-education/neonatalnursing-education-briefs/
Neonatal Nursing Education Brief: How to Recognize a Suspected Cardiac Defect in the Neonate https://www.seattlechildrens.org/healthcareprofessionals/education/continuing-medical-nursing-education/neonatalnursing-education-briefs/
Screening for Critical Congenital Heart Disease
 Screening for Critical Congenital Heart Disease Caroline K. Lee, MD Pediatric Cardiology Disclosures I have no relevant financial relationships or conflicts of interest 1 Most Common Birth Defect Most
Screening for Critical Congenital Heart Disease Caroline K. Lee, MD Pediatric Cardiology Disclosures I have no relevant financial relationships or conflicts of interest 1 Most Common Birth Defect Most
When is Risky to Apply Oxygen for Congenital Heart Disease 부천세종병원 소아청소년과최은영
 When is Risky to Apply Oxygen for Congenital Heart Disease 부천세종병원 소아청소년과최은영 The Korean Society of Cardiology COI Disclosure Eun-Young Choi The author have no financial conflicts of interest to disclose
When is Risky to Apply Oxygen for Congenital Heart Disease 부천세종병원 소아청소년과최은영 The Korean Society of Cardiology COI Disclosure Eun-Young Choi The author have no financial conflicts of interest to disclose
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions
 Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS Pediatric Cardiology
 Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
The Blue Baby. Network Stabilisation of the Term Infant Study Day 15 th March 2017 Joanna Behrsin
 The Blue Baby Network Stabilisation of the Term Infant Study Day 15 th March 2017 Joanna Behrsin Session Structure Definitions and assessment of cyanosis Causes of blue baby Structured approach to assessing
The Blue Baby Network Stabilisation of the Term Infant Study Day 15 th March 2017 Joanna Behrsin Session Structure Definitions and assessment of cyanosis Causes of blue baby Structured approach to assessing
Duct Dependant Congenital Heart Disease
 Children s Acute Transport Service Clinical Guidelines Duct Dependant Congenital Heart Disease This guideline has been agreed by both NTS & CATS Document Control Information Author CATS/NTS Author Position
Children s Acute Transport Service Clinical Guidelines Duct Dependant Congenital Heart Disease This guideline has been agreed by both NTS & CATS Document Control Information Author CATS/NTS Author Position
Cardiac Emergencies in Infants. Michael Luceri, DO
 Cardiac Emergencies in Infants Michael Luceri, DO October 7, 2017 I have no financial obligations or conflicts of interest to disclose. Objectives Understand the scope of congenital heart disease Recognize
Cardiac Emergencies in Infants Michael Luceri, DO October 7, 2017 I have no financial obligations or conflicts of interest to disclose. Objectives Understand the scope of congenital heart disease Recognize
Duct Dependant Congenital Heart Disease
 Children s Acute Transport Service Clinical Guidelines Duct Dependant Congenital Heart Disease Document Control Information Author CATS/NTS Author Position CC Transport Services Document Owner E. Polke
Children s Acute Transport Service Clinical Guidelines Duct Dependant Congenital Heart Disease Document Control Information Author CATS/NTS Author Position CC Transport Services Document Owner E. Polke
Heart Disorders. Cardiovascular Disorders (Part B-1) Module 5 -Chapter 8. Overview Heart Disorders Vascular Disorders
 Module 5 -Chapter 8. Overview Heart Disorders Vascular Disorders") Cardiovascular Disorders (Part B-1) Module 5 -Chapter 8 Overview Heart Disorders Vascular Disorders Susie Turner, MD 1/7/13 Heart Disorders Coronary Artery Disease Cardiac Arrhythmias Congestive Heart
Cardiovascular Disorders (Part B-1) Module 5 -Chapter 8 Overview Heart Disorders Vascular Disorders Susie Turner, MD 1/7/13 Heart Disorders Coronary Artery Disease Cardiac Arrhythmias Congestive Heart
Patent ductus arteriosus PDA
 Patent ductus arteriosus PDA Is connecting between the aortic end just distal to the origin of the LT sub clavian artery& the pulmonary artery at its bifurcation. Female/male ratio is 2:1 and it is more
Patent ductus arteriosus PDA Is connecting between the aortic end just distal to the origin of the LT sub clavian artery& the pulmonary artery at its bifurcation. Female/male ratio is 2:1 and it is more
Infection. Risk factor for infection ACoRN alerting sign with * Clinical deterioration. Problem List. Respiratory. Cardiovascular
 The ACoRN Process Baby at risk Unwell Risk factors Post-resuscitation requiring stabilization Resuscitation Ineffective breathing Heart rate < 100 bpm Central cyanosis Support Infection Risk factor for
The ACoRN Process Baby at risk Unwell Risk factors Post-resuscitation requiring stabilization Resuscitation Ineffective breathing Heart rate < 100 bpm Central cyanosis Support Infection Risk factor for
CongHeartDis.doc. Андрій Миколайович Лобода
 CongHeartDis.doc Андрій Миколайович Лобода 2015 Зміст 3 Зміст Зміст 4 A child with tetralogy of Fallot is most likely to exhibit: -Increased pulmonary blood flow -Increased pressure in the right ventricle
CongHeartDis.doc Андрій Миколайович Лобода 2015 Зміст 3 Зміст Зміст 4 A child with tetralogy of Fallot is most likely to exhibit: -Increased pulmonary blood flow -Increased pressure in the right ventricle
Critical Heart Disease in the Newborn. What you need to know
 Critical Heart Disease in the Newborn What you need to know DISCLOSURES Nothing to report OBJECTIVES DESCRIBE NEONATAL CARDIOVASCULAR PHYSIOLOGY RECOGNIZE NEONATAL CARDIAC EMERGENCIES FORMULATE TREATMENT
Critical Heart Disease in the Newborn What you need to know DISCLOSURES Nothing to report OBJECTIVES DESCRIBE NEONATAL CARDIOVASCULAR PHYSIOLOGY RECOGNIZE NEONATAL CARDIAC EMERGENCIES FORMULATE TREATMENT
Student Guide Module 4: Pediatric Trauma
 Student Guide Module 4: Pediatric Trauma Problem based learning exercise objectives Understand how to manage traumatic injuries in mass casualty events. Discuss the features and the approach to pediatric
Student Guide Module 4: Pediatric Trauma Problem based learning exercise objectives Understand how to manage traumatic injuries in mass casualty events. Discuss the features and the approach to pediatric
Anatomy & Physiology
 1 Anatomy & Physiology Heart is divided into four chambers, two atrias & two ventricles. Atrioventricular valves (tricuspid & mitral) separate the atria from ventricles. they open & close to control flow
1 Anatomy & Physiology Heart is divided into four chambers, two atrias & two ventricles. Atrioventricular valves (tricuspid & mitral) separate the atria from ventricles. they open & close to control flow
Stabilization and Transportation guidelines for Neonates and infants with Heart disease:
 Stabilization and Transportation guidelines for Neonates and infants with Heart disease: Background: Referral Pediatric Cardiac Units, frequently receive neonates and infants referred and transported from
Stabilization and Transportation guidelines for Neonates and infants with Heart disease: Background: Referral Pediatric Cardiac Units, frequently receive neonates and infants referred and transported from
Paediatrics Revision Session Cardiology. Emma Walker 7 th May 2016
 Paediatrics Revision Session Cardiology Emma Walker 7 th May 2016 Cardiovascular Examination! General:! Make it fun!! Change how you act depending on their age! Introduction! Introduce yourself & check
Paediatrics Revision Session Cardiology Emma Walker 7 th May 2016 Cardiovascular Examination! General:! Make it fun!! Change how you act depending on their age! Introduction! Introduce yourself & check
CONGENITAL HEART DISEASE (CHD)
") CONGENITAL HEART DISEASE (CHD) DEFINITION It is the result of a structural or functional abnormality of the cardiovascular system at birth GENERAL FEATURES OF CHD Structural defects due to specific disturbance
CONGENITAL HEART DISEASE (CHD) DEFINITION It is the result of a structural or functional abnormality of the cardiovascular system at birth GENERAL FEATURES OF CHD Structural defects due to specific disturbance
PAEDIATRIC EMQs. Andrew A Mallick Paediatrics.info.
 PAEDIATRIC EMQs Andrew A Mallick Paediatrics.info www.paediatrics.info Paediatric EMQs Paediatrics.info First published in the United Kingdom in 2012. While the advice and information in this book is believed
PAEDIATRIC EMQs Andrew A Mallick Paediatrics.info www.paediatrics.info Paediatric EMQs Paediatrics.info First published in the United Kingdom in 2012. While the advice and information in this book is believed
Pediatric Advanced Life Support
 Pediatric Advanced Life Support Pediatric Chain of Survival Berg M D et al. Circulation 2010;122:S862-S875 Prevention Early cardiopulmonary resuscitation (CPR) Prompt access to the emergency response system
Pediatric Advanced Life Support Pediatric Chain of Survival Berg M D et al. Circulation 2010;122:S862-S875 Prevention Early cardiopulmonary resuscitation (CPR) Prompt access to the emergency response system
Nursing Care of Children and their Families: Alterations in Cardiac Function
 Nursing Care of Children and their Families: Alterations in Cardiac Function Congenital Heart Disease Incidence 4-10 per live births Extra cardiac defects: TE fistula, renal agenesis and diaphragmatic
Nursing Care of Children and their Families: Alterations in Cardiac Function Congenital Heart Disease Incidence 4-10 per live births Extra cardiac defects: TE fistula, renal agenesis and diaphragmatic
Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University
 Dr Mubarak Abdelrahman Assistant Professor Jazan University") Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University SHOCK Definition: Shock is a syndrome = inability to provide sufficient oxygenated blood to tissues. Oxygen
Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University SHOCK Definition: Shock is a syndrome = inability to provide sufficient oxygenated blood to tissues. Oxygen
Daniel A. Beals MD, FACS, FAAP Pediatric Surgery and Urology Community Medical Center Associate Professor of Surgery and Pediatrics University of
 Daniel A. Beals MD, FACS, FAAP Pediatric Surgery and Urology Community Medical Center Associate Professor of Surgery and Pediatrics University of Washington Seattle Children s Hospital Objectives Define
Daniel A. Beals MD, FACS, FAAP Pediatric Surgery and Urology Community Medical Center Associate Professor of Surgery and Pediatrics University of Washington Seattle Children s Hospital Objectives Define
Cold-Related Illness. Matthew Gammons, MD Killington Medical Clinic Vermont Orthopaedic Clinic
 Cold-Related Illness Matthew Gammons, MD Killington Medical Clinic Vermont Orthopaedic Clinic Hypothermia Frost nip Frostbite Chillbains Trench foot Cold-Related Illness Who gets it? How common? Outdoor
Cold-Related Illness Matthew Gammons, MD Killington Medical Clinic Vermont Orthopaedic Clinic Hypothermia Frost nip Frostbite Chillbains Trench foot Cold-Related Illness Who gets it? How common? Outdoor
Introduction. Pediatric Cardiology. General Appearance. Tools of Assessment. Auscultation. Vital Signs
 Introduction Pediatric Cardiology An introduction to the pediatric patient with heart disease: M-III Lecture Douglas R. Allen, M.D. Assistant Professor and Director of Community Pediatric Cardiology at
Introduction Pediatric Cardiology An introduction to the pediatric patient with heart disease: M-III Lecture Douglas R. Allen, M.D. Assistant Professor and Director of Community Pediatric Cardiology at
Vital Signs. Vital Signs. Vital Signs
 Vital Signs Vital Signs Why do vital signs? Determine relative status of vital organs Establish baseline Monitor response to Rx, meds Observe trends Determine need for further evaluation, Rx, intervention
Vital Signs Vital Signs Why do vital signs? Determine relative status of vital organs Establish baseline Monitor response to Rx, meds Observe trends Determine need for further evaluation, Rx, intervention
SHOCK AETIOLOGY OF SHOCK (1) Inadequate circulating blood volume ) Loss of Autonomic control of the vasculature (3) Impaired cardiac function
 Inadequate circulating blood volume ) Loss of Autonomic control of the vasculature (3) Impaired cardiac function") SHOCK Shock is a condition in which the metabolic needs of the body are not met because of an inadequate cardiac output. If tissue perfusion can be restored in an expeditious fashion, cellular injury may
SHOCK Shock is a condition in which the metabolic needs of the body are not met because of an inadequate cardiac output. If tissue perfusion can be restored in an expeditious fashion, cellular injury may
Notes by Sandra Dankwa 2009 HF- Heart Failure DS- Down Syndrome IE- Infective Endocarditis ET- Exercise Tolerance. Small VSD Symptoms -asymptomatic
 Congenital Heart Disease: Notes. Condition Pathology PC Ix Rx Ventricular septal defect (VSD) L R shuntsdefect anywhere in the ventricle, usually perimembranous (next to the tricuspid valve) 30% 1)small
Congenital Heart Disease: Notes. Condition Pathology PC Ix Rx Ventricular septal defect (VSD) L R shuntsdefect anywhere in the ventricle, usually perimembranous (next to the tricuspid valve) 30% 1)small
3/14/2011 MANAGEMENT OF NEWBORNS CARDIAC INTENSIVE CARE CONFERENCE FOR HEALTH PROFESSIONALS IRVINE, CA. MARCH 7, 2011 WITH HEART DEFECTS
 CONFERENCE FOR HEALTH PROFESSIONALS IRVINE, CA. MARCH 7, 2011 MANAGEMENT OF NEWBORNS WITH HEART DEFECTS A NTHONY C. CHANG, MD, MBA, MPH M E D I C AL D I RE C T OR, HEART I N S T I T U T E C H I LDRE N
CONFERENCE FOR HEALTH PROFESSIONALS IRVINE, CA. MARCH 7, 2011 MANAGEMENT OF NEWBORNS WITH HEART DEFECTS A NTHONY C. CHANG, MD, MBA, MPH M E D I C AL D I RE C T OR, HEART I N S T I T U T E C H I LDRE N
CETEP PRE-TEST For questions 1 through 3, consider the following scenario:
 CETEP PRE-TEST For questions 1 through 3, consider the following scenario: A two and half month infant comes to the health centre looking very lethargic. Her mother reports that the infant has felt very
CETEP PRE-TEST For questions 1 through 3, consider the following scenario: A two and half month infant comes to the health centre looking very lethargic. Her mother reports that the infant has felt very
PALS Pulseless Arrest Algorithm.
 PALS Pulseless Arrest Algorithm. Kleinman M E et al. Circulation 2010;122:S876-S908 PALS Bradycardia Algorithm. Kleinman M E et al. Circulation 2010;122:S876-S908 PALS Tachycardia Algorithm. Kleinman M
PALS Pulseless Arrest Algorithm. Kleinman M E et al. Circulation 2010;122:S876-S908 PALS Bradycardia Algorithm. Kleinman M E et al. Circulation 2010;122:S876-S908 PALS Tachycardia Algorithm. Kleinman M
TRAINING NEONATOLOGY SILVANA PARIS
 TRAINING ON NEONATOLOGY SILVANA PARIS RESUSCITATION IN DELIVERY ROOM INTRODUCTION THE GLOBAL RESUSCITATION BURDEN IN NEWBORN 136 MILL NEWBORN BABIES EACH YEAR (WHO WORLD REPORT) 5-8 MILL NEWBORN INFANTS
TRAINING ON NEONATOLOGY SILVANA PARIS RESUSCITATION IN DELIVERY ROOM INTRODUCTION THE GLOBAL RESUSCITATION BURDEN IN NEWBORN 136 MILL NEWBORN BABIES EACH YEAR (WHO WORLD REPORT) 5-8 MILL NEWBORN INFANTS
Patient guide: pfm Nit-Occlud PDA coil occlusion system. Catheter occlusion of. Patent Ductus Arteriosus. with the
 Patient guide: Catheter occlusion of Patent Ductus Arteriosus with the pfm Nit-Occlud PDA coil occlusion system pfm Produkte für die Medizin - AG Wankelstr. 60 D - 50996 Cologne Phone: +49 (0) 2236 96
Patient guide: Catheter occlusion of Patent Ductus Arteriosus with the pfm Nit-Occlud PDA coil occlusion system pfm Produkte für die Medizin - AG Wankelstr. 60 D - 50996 Cologne Phone: +49 (0) 2236 96
Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: PALS Revised: 11/2013
 NUMBERS Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: PALS Revised: 11/2013 Weight in kg = 8 + (age in yrs X 2) Neonate (less than 1 month)
NUMBERS Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: PALS Revised: 11/2013 Weight in kg = 8 + (age in yrs X 2) Neonate (less than 1 month)
DORV: The Great Chameleon. Heart Conference October 15, 2016 Tina Kwan, MD
 DORV: The Great Chameleon Heart Conference October 15, 2016 Tina Kwan, MD Kenneth Maehara, Ph.D. May 7, 1942 - August 26, 2013 A.R. A classic case of broken heart 38 week AGA F born at an OSH to
DORV: The Great Chameleon Heart Conference October 15, 2016 Tina Kwan, MD Kenneth Maehara, Ph.D. May 7, 1942 - August 26, 2013 A.R. A classic case of broken heart 38 week AGA F born at an OSH to
The blue baby. Case 4
 Case 4 The blue baby Mrs Smith has brought her baby to A&E because she says he has started turning blue. What are your immediate differential diagnoses? 1 Respiratory causes: Congenital respiratory disorder.
Case 4 The blue baby Mrs Smith has brought her baby to A&E because she says he has started turning blue. What are your immediate differential diagnoses? 1 Respiratory causes: Congenital respiratory disorder.
Neonatal Resuscitation. Dustin Coyle, M.D. Anesthesiology
 Neonatal Resuscitation Dustin Coyle, M.D. Anesthesiology Recognize complications Maternal-fetal factors Maternal DM PIH Chronic HTN Previous stillbirth Rh sensitization Infection Substance abuse/certain
Neonatal Resuscitation Dustin Coyle, M.D. Anesthesiology Recognize complications Maternal-fetal factors Maternal DM PIH Chronic HTN Previous stillbirth Rh sensitization Infection Substance abuse/certain
Pulse Oximetry Screening in Newborns to Enhance the Detection Of Critical Congenital Heart Disease. Frequently Asked Questions
 Pulse Oximetry Screening in Newborns to Enhance the Detection Of Critical Congenital Heart Disease Frequently Asked Questions Current Recommendation: The current recommendation from the Canadian Cardiovascular
Pulse Oximetry Screening in Newborns to Enhance the Detection Of Critical Congenital Heart Disease Frequently Asked Questions Current Recommendation: The current recommendation from the Canadian Cardiovascular
Neonatal Life Support Provider (NLSP) Certification Preparatory Materials
 Certification Preparatory Materials") Neonatal Life Support Provider (NLSP) Certification Preparatory Materials NEONATAL LIFE SUPPORT PROVIDER (NRP) CERTIFICATION TABLE OF CONTENTS NEONATAL FLOW ALGORITHM.2 INTRODUCTION 3 ANTICIPATION OF RESUSCITATION
Neonatal Life Support Provider (NLSP) Certification Preparatory Materials NEONATAL LIFE SUPPORT PROVIDER (NRP) CERTIFICATION TABLE OF CONTENTS NEONATAL FLOW ALGORITHM.2 INTRODUCTION 3 ANTICIPATION OF RESUSCITATION
Oh SCH It s a neonatal emergency
 trekk.ca 1 1 Oh SCH It s a neonatal emergency Emma Burns, MD, FRCPC IWK Health Centre 2 1 Objectives Critically ill neonate approach and tips Stay on time! Thanks to: Shannon MacPhee, Mike Young, Jon Cherry,
trekk.ca 1 1 Oh SCH It s a neonatal emergency Emma Burns, MD, FRCPC IWK Health Centre 2 1 Objectives Critically ill neonate approach and tips Stay on time! Thanks to: Shannon MacPhee, Mike Young, Jon Cherry,
Pediatric Board Review Congenital Heart Disease. Steven H. Todman, M.D. Pediatric Cardiologist Louisiana State University
 Pediatric Board Review Congenital Heart Disease Steven H. Todman, M.D. Pediatric Cardiologist Louisiana State University Our Mission To discuss various types of congenital heart disease that are commonly
Pediatric Board Review Congenital Heart Disease Steven H. Todman, M.D. Pediatric Cardiologist Louisiana State University Our Mission To discuss various types of congenital heart disease that are commonly
Slide 1. Slide 2. Slide 3 CONGENITAL HEART DISEASE. Papworth Hospital NHS Trust INTRODUCTION. Jakub Kadlec/Catherine Sudarshan INTRODUCTION
 Slide 1 CONGENITAL HEART DISEASE Jakub Kadlec/Catherine Sudarshan NHS Trust Slide 2 INTRODUCTION Most common congenital illness in the newborn Affects about 4 9 / 1000 full-term live births in the UK 1.5
Slide 1 CONGENITAL HEART DISEASE Jakub Kadlec/Catherine Sudarshan NHS Trust Slide 2 INTRODUCTION Most common congenital illness in the newborn Affects about 4 9 / 1000 full-term live births in the UK 1.5
Congenital Heart Defects
 Normal Heart Congenital Heart Defects 1. Patent Ductus Arteriosus The ductus arteriosus connects the main pulmonary artery to the aorta. In utero, it allows the blood leaving the right ventricle to bypass
Normal Heart Congenital Heart Defects 1. Patent Ductus Arteriosus The ductus arteriosus connects the main pulmonary artery to the aorta. In utero, it allows the blood leaving the right ventricle to bypass
An Overview of Bronchopulmonary Dysplasia and Chronic Lung Disease in Infancy
 An Overview of Bronchopulmonary Dysplasia and Chronic Lung Disease in Infancy Housekeeping: I have no financial disclosures Learning objectives: Develop an understanding of bronchopulmonary dysplasia (BPD)
An Overview of Bronchopulmonary Dysplasia and Chronic Lung Disease in Infancy Housekeeping: I have no financial disclosures Learning objectives: Develop an understanding of bronchopulmonary dysplasia (BPD)
CCHD Screening with Pulse Oximetry: A Success Story!
 CCHD Screening with Pulse Oximetry: A Success Story! Nicole Spillane, MD Associate Director of Neonatology, HackensackUMC Hackensack Meridian Health Objective Recognize the contribution of pulse oximetry
CCHD Screening with Pulse Oximetry: A Success Story! Nicole Spillane, MD Associate Director of Neonatology, HackensackUMC Hackensack Meridian Health Objective Recognize the contribution of pulse oximetry
AORTIC COARCTATION. Synonyms: - Coarctation of the aorta
 AORTIC COARCTATION Synonyms: - Coarctation of the aorta Definition: Aortic coarctation is a congenital narrowing of the aorta, usually located after the left subclavian artery, near the ductus or the ligamentum
AORTIC COARCTATION Synonyms: - Coarctation of the aorta Definition: Aortic coarctation is a congenital narrowing of the aorta, usually located after the left subclavian artery, near the ductus or the ligamentum
Pediatric Shock. Hypovolemia. Sepsis. Most common cause of pediatric shock Small blood volumes (80cc/kg)
") Critical Concepts: Shock Inadequate peripheral perfusion where oxygen delivery does not meet metabolic demand Adult vs Pediatric Shock - Same causes/different frequencies Pediatric Shock Hypovolemia Most
Critical Concepts: Shock Inadequate peripheral perfusion where oxygen delivery does not meet metabolic demand Adult vs Pediatric Shock - Same causes/different frequencies Pediatric Shock Hypovolemia Most
Care of the Deteriorating Patient in Recovery NADIA TICEHURST : CLINICAL NURSE EDUCATOR PERI ANAESTHETICS BENDIGO HEALTH
 Care of the Deteriorating Patient in Recovery NADIA TICEHURST : CLINICAL NURSE EDUCATOR PERI ANAESTHETICS BENDIGO HEALTH Intended learning outcomes Describe the components of a comprehensive clinician
Care of the Deteriorating Patient in Recovery NADIA TICEHURST : CLINICAL NURSE EDUCATOR PERI ANAESTHETICS BENDIGO HEALTH Intended learning outcomes Describe the components of a comprehensive clinician
Congenital Heart Disease
 Congenital Heart Disease Mohammed Alghamdi, MD, FRCPC, FAAP, FACC Associate Professor and Consultant Pediatric Cardiology, Cardiac Science King Fahad Cardiac Centre King Saud University INTRODUCTION CHD
Congenital Heart Disease Mohammed Alghamdi, MD, FRCPC, FAAP, FACC Associate Professor and Consultant Pediatric Cardiology, Cardiac Science King Fahad Cardiac Centre King Saud University INTRODUCTION CHD
Algorithm Focus. Emergency Cardiovascular Care: EMT-Intermediate Treatment Algorithms. Perspective regarding the EMT- Intermediate algorithms
 Emergency Cardiovascular Care: EMT-Intermediate Treatment Algorithms Algorithms for the Conscious Patient Prehospital Medication Profiles Algorithm Focus Bradycardia Acute Pulmonary Edema and Shock Hypothermia
Emergency Cardiovascular Care: EMT-Intermediate Treatment Algorithms Algorithms for the Conscious Patient Prehospital Medication Profiles Algorithm Focus Bradycardia Acute Pulmonary Edema and Shock Hypothermia
-Cardiogenic: shock state resulting from impairment or failure of myocardium
 Shock chapter Shock -Condition in which tissue perfusion is inadequate to deliver oxygen, nutrients to support vital organs, cellular function -Affects all body systems -Classic signs of early shock: Tachycardia,tachypnea,restlessness,anxiety,
Shock chapter Shock -Condition in which tissue perfusion is inadequate to deliver oxygen, nutrients to support vital organs, cellular function -Affects all body systems -Classic signs of early shock: Tachycardia,tachypnea,restlessness,anxiety,
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv
 Rv") ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
NEONATAL HYPOXIC-ISCHAEMIC ENCEPHALOPATHY (HIE) & COOLING THERAPY
 & COOLING THERAPY") Background NEONATAL HYPOXIC-ISCHAEMIC ENCEPHALOPATHY (HIE) & COOLING THERAPY A perinatal hypoxic-ischaemic insult may present with varying degrees of neonatal encephalopathy, neurological disorder and
Background NEONATAL HYPOXIC-ISCHAEMIC ENCEPHALOPATHY (HIE) & COOLING THERAPY A perinatal hypoxic-ischaemic insult may present with varying degrees of neonatal encephalopathy, neurological disorder and
9/8/2009 < 1 1,2 3,4 5,6 7,8 9,10 11,12 13,14 15,16 17,18 > 18. Tetralogy of Fallot. Complex Congenital Heart Disease.
 Current Indications for Pediatric CTA S Bruce Greenberg Professor of Radiology Arkansas Children s Hospital University of Arkansas for Medical Sciences greenbergsbruce@uams.edu 45 40 35 30 25 20 15 10
Current Indications for Pediatric CTA S Bruce Greenberg Professor of Radiology Arkansas Children s Hospital University of Arkansas for Medical Sciences greenbergsbruce@uams.edu 45 40 35 30 25 20 15 10
Shock Quiz! By Clare Di Bona
 Shock Quiz! By Clare Di Bona Test Question What is Mr Burns full legal name? Answer Charles Montgomery Plantagenet Schicklgruber Burns. (Season 22, episode 11) Question 1. What is the definition of shock?
Shock Quiz! By Clare Di Bona Test Question What is Mr Burns full legal name? Answer Charles Montgomery Plantagenet Schicklgruber Burns. (Season 22, episode 11) Question 1. What is the definition of shock?
1. What additional information needs to be collected to properly treat this client?
 CASE 1 A 45-year-old male presents to the emergency department with a complaint of chest pain for the past two hours. 1. What additional information needs to be collected to properly treat this client?
CASE 1 A 45-year-old male presents to the emergency department with a complaint of chest pain for the past two hours. 1. What additional information needs to be collected to properly treat this client?
Pathophysiology: Left To Right Shunts
 Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
Cardiology Competency Based Goals and Objectives
 Cardiology Competency Based Goals and Objectives COMPETENCY 1. Patient Care. Provide family centered patient care that is developmentally and age appropriate, compassionate, and effective for the treatment
Cardiology Competency Based Goals and Objectives COMPETENCY 1. Patient Care. Provide family centered patient care that is developmentally and age appropriate, compassionate, and effective for the treatment
Quick review of Assessment. Pediatric Medical Assessment Review And Case Studies. Past Medical History. S.A.M.P.L.E. History is a great start.
 EMS Live at Night January 12 th, 2010 Pediatric Medical Assessment Review And Case Studies Brian Rogge RN Northwest Medstar Pediatric/Perinatal Team Quick review of Assessment S.A.M.P.L.E. History is a
EMS Live at Night January 12 th, 2010 Pediatric Medical Assessment Review And Case Studies Brian Rogge RN Northwest Medstar Pediatric/Perinatal Team Quick review of Assessment S.A.M.P.L.E. History is a
Congenital Heart Disease: Physiology and Common Defects
 Congenital Heart Disease: Physiology and Common Defects Jamie S. Sutherell, M.D, M.Ed. Associate Professor, Pediatrics Division of Cardiology Director, Medical Student Education in Pediatrics Director,
Congenital Heart Disease: Physiology and Common Defects Jamie S. Sutherell, M.D, M.Ed. Associate Professor, Pediatrics Division of Cardiology Director, Medical Student Education in Pediatrics Director,
Acute arterial embolism
 Acute arterial embolism Definition Thrombus come from heart or blood vessel or other embolus such as tumor,air gas or fat flow with blood stream and occlude distal limb or visceral arteries which causes
Acute arterial embolism Definition Thrombus come from heart or blood vessel or other embolus such as tumor,air gas or fat flow with blood stream and occlude distal limb or visceral arteries which causes
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acute coronary syndrome(s), anticoagulant therapy in, 706, 707 antiplatelet therapy in, 702 ß-blockers in, 703 cardiac biomarkers in,
Index Note: Page numbers of article titles are in boldface type. A Acute coronary syndrome(s), anticoagulant therapy in, 706, 707 antiplatelet therapy in, 702 ß-blockers in, 703 cardiac biomarkers in,
Total Anomalous Pulmonary Venous Connections: Anatomy and Diagnostic Imaging
 Total Anomalous Pulmonary Venous Connections: Anatomy and Diagnostic Imaging Timothy Slesnick, MD March 12, 2015 Congenital Cardiac Anesthesia Society Annual Meeting Disclosures I will discuss the use
Total Anomalous Pulmonary Venous Connections: Anatomy and Diagnostic Imaging Timothy Slesnick, MD March 12, 2015 Congenital Cardiac Anesthesia Society Annual Meeting Disclosures I will discuss the use
Objectives Part 1. Objectives Part 2. Fetal Circulation Transition to Postnatal Circulation Normal Cardiac Anatomy Ductal Dependence and use of PGE1
 Cardiac Physiology Gia Marzano, AC PNP Pediatric Cardiac Surgery Rush Center for Congenital Heart Disease Rush University Medical Center Objectives Part 1 Fetal Circulation Transition to Postnatal Circulation
Cardiac Physiology Gia Marzano, AC PNP Pediatric Cardiac Surgery Rush Center for Congenital Heart Disease Rush University Medical Center Objectives Part 1 Fetal Circulation Transition to Postnatal Circulation
SPECIFIC HEART DEFECTS
 A. Acyanotic Defects 1. Ventricular Septal Defect (VSD): SPECIFIC HEART DEFECTS Which side of the heart is stronger? Left This is when there is an opening between the left and right ventricle (in the septum)
A. Acyanotic Defects 1. Ventricular Septal Defect (VSD): SPECIFIC HEART DEFECTS Which side of the heart is stronger? Left This is when there is an opening between the left and right ventricle (in the septum)
Emergency Triage Assessment and Management (ETAT) POST-TEST: Module 1
 POST-TEST: Module 1") Emergency Triage Assessment and Management (ETAT) POST-TEST: Module 1 For questions 1 through 3, consider the following scenario: A three year old comes with burns to her face and chest after a kerosene
Emergency Triage Assessment and Management (ETAT) POST-TEST: Module 1 For questions 1 through 3, consider the following scenario: A three year old comes with burns to her face and chest after a kerosene
Absent Pulmonary Valve Syndrome
 Absent Pulmonary Valve Syndrome Fact sheet on Absent Pulmonary Valve Syndrome In this condition, which has some similarities to Fallot's Tetralogy, there is a VSD with narrowing at the pulmonary valve.
Absent Pulmonary Valve Syndrome Fact sheet on Absent Pulmonary Valve Syndrome In this condition, which has some similarities to Fallot's Tetralogy, there is a VSD with narrowing at the pulmonary valve.
Pediatrics. Blue Baby Syndrome (Cyanotic Newborn) and Hyperoxia Test. Definition. See online here
 and Hyperoxia Test. Definition. See online here") Pediatrics Blue Baby Syndrome (Cyanotic Newborn) and Hyperoxia Test See online here Blue babies lack sufficient hemoglobin, resulting in the bluish discoloration of tissues, a term referred to as cyanosis.
Pediatrics Blue Baby Syndrome (Cyanotic Newborn) and Hyperoxia Test See online here Blue babies lack sufficient hemoglobin, resulting in the bluish discoloration of tissues, a term referred to as cyanosis.
Congenital Heart Disease. CCCHD In WI. Critical Congenital Heart Disease. Why Screen? 4/20/2018. Early Detection = Better Outcomes
 Congenital Heart Disease A Positive Screen? What Does it Mean? A Review of Pulse Oximetry Screening for Critical Congenital Heart Disease Elizabeth Goetz MD MPH 8-10/1000 livebirths 3% of all infant mortality
Congenital Heart Disease A Positive Screen? What Does it Mean? A Review of Pulse Oximetry Screening for Critical Congenital Heart Disease Elizabeth Goetz MD MPH 8-10/1000 livebirths 3% of all infant mortality
WOLFF PARKINSON WHITE SYNDROME. Katarzyna Bigaj PGY-1
 WOLFF PARKINSON WHITE SYNDROME Katarzyna Bigaj PGY-1 Preexcitation is defined as a premature activation of the ventricular myocardium by an impulse that travels by an anomalous path and avoids physiologic
WOLFF PARKINSON WHITE SYNDROME Katarzyna Bigaj PGY-1 Preexcitation is defined as a premature activation of the ventricular myocardium by an impulse that travels by an anomalous path and avoids physiologic
Nursing Process Focus: Patients Receiving Dextran 40 (Gentran 40)
") Assess for presence/history of hypovolemia, shock, venous thrombosis. Assess vital signs: Hypovolemic shock secondary to surgery, burns, hemorrhage, other serious condition PT and PTT abnormalities Venous
Assess for presence/history of hypovolemia, shock, venous thrombosis. Assess vital signs: Hypovolemic shock secondary to surgery, burns, hemorrhage, other serious condition PT and PTT abnormalities Venous
Review of Neonatal Respiratory Problems
 Review of Neonatal Respiratory Problems Respiratory Distress Occurs in about 7% of infants Clinical presentation includes: Apnea Cyanosis Grunting Inspiratory stridor Nasal flaring Poor feeding Tachypnea
Review of Neonatal Respiratory Problems Respiratory Distress Occurs in about 7% of infants Clinical presentation includes: Apnea Cyanosis Grunting Inspiratory stridor Nasal flaring Poor feeding Tachypnea
Hypoglycaemia of the neonate. Dr. L.G. Lloyd Dept. Paediatrics
 Hypoglycaemia of the neonate Dr. L.G. Lloyd Dept. Paediatrics Why is glucose important? It provides 60-70% of energy needs Utilization obligatory by red blood cells, brain and kidney as major source of
Hypoglycaemia of the neonate Dr. L.G. Lloyd Dept. Paediatrics Why is glucose important? It provides 60-70% of energy needs Utilization obligatory by red blood cells, brain and kidney as major source of
McHenry Western Lake County EMS System CE for Paramedics, EMT-B and PHRN s Sepsis Patients. November/December 2017
 McHenry Western Lake County EMS System CE for Paramedics, EMT-B and PHRN s Sepsis Patients November/December 2017 This month we are going to take a look at the patient with Sepsis. Webster s defines septic
McHenry Western Lake County EMS System CE for Paramedics, EMT-B and PHRN s Sepsis Patients November/December 2017 This month we are going to take a look at the patient with Sepsis. Webster s defines septic
PALS Case Scenario Testing Checklist Respiratory Case Scenario 1 Upper Airway Obstruction
 Respiratory Case Scenario 1 Upper Airway Obstruction Directs administration of 100% oxygen or supplementary oxygen as needed to support oxygenation Identifies signs and symptoms of upper airway obstruction
Respiratory Case Scenario 1 Upper Airway Obstruction Directs administration of 100% oxygen or supplementary oxygen as needed to support oxygenation Identifies signs and symptoms of upper airway obstruction
Physiological Measurements Training for Care/Nursing & LD Small Group Home Staff
 Physiological Measurements Training for Care/Nursing & LD Small Group Home Staff CONTENTS 1. The National Early Warning Score 2. Respiratory Rate 3. Oxygen Saturations 4. Temperature 5. Blood Pressure
Physiological Measurements Training for Care/Nursing & LD Small Group Home Staff CONTENTS 1. The National Early Warning Score 2. Respiratory Rate 3. Oxygen Saturations 4. Temperature 5. Blood Pressure
Written 01/09/17 Rewritten 3/29/17 for Interior Regional EMS Symposium
 Written 01/09/17 Rewritten 3/29/17 for Interior Regional EMS Symposium MARIA E. MANDICH MD Fairbanks Memorial Hospital Emergency Department Attending Physician Interior Region EMS Council Medical Director
Written 01/09/17 Rewritten 3/29/17 for Interior Regional EMS Symposium MARIA E. MANDICH MD Fairbanks Memorial Hospital Emergency Department Attending Physician Interior Region EMS Council Medical Director
Acid Base Imbalance. 1. Prior to obtaining the ABG s an Allen s test should be performed. Explain the rationale for this.
 Acid Base Imbalance Case 1. An 18-year-old male arrives via EMS to the emergency department. He is experiencing Tachypnea, dizziness, numbness and paraesthesia. He is anxious, respirations are 28 per minute
Acid Base Imbalance Case 1. An 18-year-old male arrives via EMS to the emergency department. He is experiencing Tachypnea, dizziness, numbness and paraesthesia. He is anxious, respirations are 28 per minute
Appropriate Use Criteria for Initial Transthoracic Echocardiography in Outpatient Pediatric Cardiology (scores listed by Appropriate Use rating)
") Appropriate Use Criteria for Initial Transthoracic Echocardiography in Outpatient Pediatric Cardiology (scores listed by Appropriate Use rating) Table 1: Appropriate indications (median score 7-9) Indication
Appropriate Use Criteria for Initial Transthoracic Echocardiography in Outpatient Pediatric Cardiology (scores listed by Appropriate Use rating) Table 1: Appropriate indications (median score 7-9) Indication
1 Pediatric Advanced Life Support Science Update What s New for 2010? 3 CPR. 4 4 Steps of BLS Survey 5 CPR 6 CPR.
 1 Pediatric Advanced Life Support Science Update 2010 2 What s New for 2010? 3 CPR Take no longer than seconds for pulse check Rate at least on per minute (instead of around 100 per minute ) Depth change:
1 Pediatric Advanced Life Support Science Update 2010 2 What s New for 2010? 3 CPR Take no longer than seconds for pulse check Rate at least on per minute (instead of around 100 per minute ) Depth change:
Debate in Management of native COA; Balloon Versus Surgery
 Debate in Management of native COA; Balloon Versus Surgery Dr. Amira Esmat, El Tantawy, MD Professor of Pediatrics Consultant Pediatric Cardiac Interventionist Faculty of Medicine Cairo University 23/2/2017
Debate in Management of native COA; Balloon Versus Surgery Dr. Amira Esmat, El Tantawy, MD Professor of Pediatrics Consultant Pediatric Cardiac Interventionist Faculty of Medicine Cairo University 23/2/2017
Coarctation of the aorta
 T H E P E D I A T R I C C A R D I A C S U R G E R Y I N Q U E S T R E P O R T Coarctation of the aorta In the normal heart, blood flows to the body through the aorta, which connects to the left ventricle
T H E P E D I A T R I C C A R D I A C S U R G E R Y I N Q U E S T R E P O R T Coarctation of the aorta In the normal heart, blood flows to the body through the aorta, which connects to the left ventricle
Neonatal/Pediatric Cardiopulmonary Care. Persistent Pulmonary Hypertension of the Neonate (PPHN) PPHN. Other. Other Diseases
 PPHN. Other. Other Diseases") Neonatal/Pediatric Cardiopulmonary Care Other Diseases Persistent Pulmonary Hypertension of the Neonate (PPHN) PPHN 3 Also known as Persistent Fetal Circulation (PFC) Seen most frequently in term, post-term
Neonatal/Pediatric Cardiopulmonary Care Other Diseases Persistent Pulmonary Hypertension of the Neonate (PPHN) PPHN 3 Also known as Persistent Fetal Circulation (PFC) Seen most frequently in term, post-term
Patient Management Code Blue in the CT Suite
 Patient Management Code Blue in the CT Suite David Stultz, MD November 28, 2001 Case Presentation A 53-year-old woman experienced acute respiratory distress during an IV contrast enhanced CT scan of the
Patient Management Code Blue in the CT Suite David Stultz, MD November 28, 2001 Case Presentation A 53-year-old woman experienced acute respiratory distress during an IV contrast enhanced CT scan of the
Bleeding and Shock *** CME Version *** Aaron J. Katz, AEMT-P, CIC
 Bleeding and Shock *** CME Version *** Aaron J. Katz, AEMT-P, CIC www.es26medic.net Circulatory System Composed of heart, blood vessels and blood A closed system Pumps oxygenated blood and nutrients to
Bleeding and Shock *** CME Version *** Aaron J. Katz, AEMT-P, CIC www.es26medic.net Circulatory System Composed of heart, blood vessels and blood A closed system Pumps oxygenated blood and nutrients to
SWISS SOCIETY OF NEONATOLOGY. Prenatal closure of the ductus arteriosus
 SWISS SOCIETY OF NEONATOLOGY Prenatal closure of the ductus arteriosus March 2007 Leone A, Fasnacht M, Beinder E, Arlettaz R, Neonatal Intensive Care Unit (LA, AR), University Hospital Zurich, Cardiology
SWISS SOCIETY OF NEONATOLOGY Prenatal closure of the ductus arteriosus March 2007 Leone A, Fasnacht M, Beinder E, Arlettaz R, Neonatal Intensive Care Unit (LA, AR), University Hospital Zurich, Cardiology
Approach to a baby with cyanosis
 Approach to a baby with cyanosis Objectives Cyanosis : types Differentials: cardiac vs. non cardiac Approach Case scenarios Cyanosis Greek word kuaneos meaning dark blue Bluish discolouration of skin,
Approach to a baby with cyanosis Objectives Cyanosis : types Differentials: cardiac vs. non cardiac Approach Case scenarios Cyanosis Greek word kuaneos meaning dark blue Bluish discolouration of skin,
Toxins and Environmental: HEAT- and COLD-RELATED EMERGENCIES. Accidental Hypothermia/Cold Exposure
 Toxins and Environmental: HEAT- and COLD-RELATED EMERGENCIES Accidental Hypothermia/Cold Exposure Goal: To aid EMS Providers in: the recognition and treatment of systemic effects of accidental hypothermia
Toxins and Environmental: HEAT- and COLD-RELATED EMERGENCIES Accidental Hypothermia/Cold Exposure Goal: To aid EMS Providers in: the recognition and treatment of systemic effects of accidental hypothermia
Pathophysiology: Left To Right Shunts
 Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
Supplemental Information
 ARTICLE Supplemental Information SUPPLEMENTAL TABLE 6 Mosaic and Partial Trisomies Thirty-eight VLBW infants were identified with T13, of whom 2 had mosaic T13. T18 was reported for 128 infants, of whom
ARTICLE Supplemental Information SUPPLEMENTAL TABLE 6 Mosaic and Partial Trisomies Thirty-eight VLBW infants were identified with T13, of whom 2 had mosaic T13. T18 was reported for 128 infants, of whom
Objectives. Objectives 10/12/2011. Case Study: Initial Assessment of the Critically Ill Child. By Rebecca Saul, MSN, CRNP
 Case Study: Initial Assessment of the Critically Ill Child By Rebecca Saul, MSN, CRNP Objectives Define the anatomic variations between children and adults Recognize and implement exam techniques useful
Case Study: Initial Assessment of the Critically Ill Child By Rebecca Saul, MSN, CRNP Objectives Define the anatomic variations between children and adults Recognize and implement exam techniques useful
1st Annual Clinical Simulation Conference
 1st Annual Clinical Simulation Conference Newborns with Acute Respiratory Distress: Diagnosis and Management Ma Teresa C. Ambat, MD Assistant Professor Division of Neonatology, Department of Pediatrics
1st Annual Clinical Simulation Conference Newborns with Acute Respiratory Distress: Diagnosis and Management Ma Teresa C. Ambat, MD Assistant Professor Division of Neonatology, Department of Pediatrics
EVALUATION OF PREGNANT PATIENTS WITH HEART DISEASE. Karen Stout, MD University of Washington Seattle Children s Seattle, WA
 EVALUATION OF PREGNANT PATIENTS WITH HEART DISEASE Karen Stout, MD University of Washington Seattle Children s Seattle, WA CASE PRESENTATION 24 year old woman with aortic regurgitation referred for evaluation
EVALUATION OF PREGNANT PATIENTS WITH HEART DISEASE Karen Stout, MD University of Washington Seattle Children s Seattle, WA CASE PRESENTATION 24 year old woman with aortic regurgitation referred for evaluation
ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT
 ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT Karen Stout, MD, FACC Divisions of Cardiology University of Washington Medical Center Seattle Children s Hospital NO DISCLOSURES
ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT Karen Stout, MD, FACC Divisions of Cardiology University of Washington Medical Center Seattle Children s Hospital NO DISCLOSURES
The Crashing Pediatric Patient: Stopping the Fall
 The Crashing Pediatric Patient: Stopping the Fall I can t breathe... 4 year old BIBA from school with sudden severe resp distress Hx of asthma, food allergies Judith Klein, MD FACEP Assistant Professor
The Crashing Pediatric Patient: Stopping the Fall I can t breathe... 4 year old BIBA from school with sudden severe resp distress Hx of asthma, food allergies Judith Klein, MD FACEP Assistant Professor
SURGICAL TREATMENT AND OUTCOME OF CONGENITAL HEART DISEASE
 SURGICAL TREATMENT AND OUTCOME OF CONGENITAL HEART DISEASE Mr. W. Brawn Birmingham Children s Hospital. Aims of surgery The aim of surgery in congenital heart disease is to correct or palliate the heart
SURGICAL TREATMENT AND OUTCOME OF CONGENITAL HEART DISEASE Mr. W. Brawn Birmingham Children s Hospital. Aims of surgery The aim of surgery in congenital heart disease is to correct or palliate the heart
CONGENITAL TRACHEAL STENOSIS PRESENTING IN THE NEONATAL PERIOD
 CONGENITAL TRACHEAL STENOSIS PRESENTING IN THE NEONATAL PERIOD J Reiter, C Springer, E Erez Israel Society of Pediatric Pulmonolgy Jerusalem, September 2 nd, 2015 Topics Case Presentation Surgical Intervention
CONGENITAL TRACHEAL STENOSIS PRESENTING IN THE NEONATAL PERIOD J Reiter, C Springer, E Erez Israel Society of Pediatric Pulmonolgy Jerusalem, September 2 nd, 2015 Topics Case Presentation Surgical Intervention