Consolidated Report on MHSA Community Engagement Activities. Contra Costa County Behavioral Health Services
|
|
|
- Diana Skinner
- 6 years ago
- Views:
Transcription

1 Consolidated Report on MHSA Community Engagement Activities Contra Costa County Behavioral Health Services
2
3 Consolidated Report on MHSA Community Engagement Activities Page 3 Table of Contents Introduction... 7 Background on the MHSA... 8 Community Engagement Description of Community Engagement Activities Planning Approach and Process Community Engagement Activities Stakeholder Participation Focus Groups Community Meetings Community Engagement Results Overview County-Wide Results Community Engagement Results by Population Children System of Care Transitional Age Youth (TAY) System of Care Adult System of Care Older Adult System of Care People Experiencing Homelessness Latino Community Asian & Pacific Islander (API) and Native American Communities Lesbian, Gay, Bisexual, Transgender, and Queer (LGBTQ) Community Family Members and Loved Ones of Consumers Appendices Appendix A: Focus Group Facilitator s Protocol Appendix B: Informational Flyer for Focus Group Events... 61
4 Consolidated Report on MHSA Community Engagement Activities Page 4 Appendix C: Logistical Flyer for Focus Group Events Appendix D: Contra Costa Mental Health Assessment of Needs Handout Appendix E: Contra Costa Mental Health Service Providers Handout Appendix F: MHSA Values and Components Handout Appendix G: Focus Group Participation Summary Handout Appendix H: Participant Demographic Form Appendix I: Community Forum Presentation... 76
5 Consolidated Report on MHSA Community Engagement Activities Page 5 List of Tables and Figures Figure 1: MHSA Values... 8 Figure 2: Community Program Planning Process... 8 Figure 3: Community Engagement Activities Table 1: Community Planning Activities and Dates Table 2: Total Count of Participants by Community Planning Activity Figure 4: Community Engagement Participants by Communities and Geographies Table 3: Total Count of Participating Consumers and Family Members by Population Table 4: Total Count of Participating Service Providers by System of Care Table 5: Total Count and Percentage of Participants by Stakeholder Affiliation Figure 5: Percent of Focus Group Participants by Age (n=220) Figure 6: Percent of Focus Group Participants by Gender (n=222) Figure 7: Count of Focus Group Participants by Race/Ethnicity (n=220) Table 6: Count of Focus Group Participants by County Region (n=223) Table 7: Count of Community Forum Participants by County Region (n=111) Figure 8: Percent of Community Meeting Participants by Stakeholder Affiliation Figure 9: Percent of Community Meeting Participants by Age (n= 32) Figure 10: Percent of Community Meeting Participants by Gender (n= 32) Figure 11: Percent of Community Meeting Participants by Race/Ethnicity (n=32) Figure 12: Percent of Community Meeting Participants by Place of Residence... 20
6 Consolidated Report on MHSA Community Engagement Activities Page 6 Page intentionally left blank.
7 Consolidated Report on MHSA Community Engagement Activities Page 7 Introduction Contra Costa County began the Community Program Planning (CPP) process for its Mental Health Services Act (MHSA) Three-Year Program and Expenditure Plan in September Contra Costa Behavioral Health Services (CCBHS) contracted with Resource Development Associates (RDA), a consulting firm with mental health planning expertise, to facilitate the community engagement phase and inform CCBHS s development of the Three-Year MHSA plan. The community engagement portion was conducted from January April 2014 and encompassed a portion of the CPP process in which RDA facilitated 23 stakeholder focus groups and four community forums with consumers, family members of consumers, providers of MHSA services, and County mental health staff. RDA conducted community engagement activities in collaboration with Peers Envisioning & Engaging in Recovery Services (PEERS), a consumer-led organization that promotes social inclusion through outreach, consumer empowerment training, and media that challenges stigma and discrimination against people with mental health issues. The purpose of this report is to describe Contra Costa County s community engagement efforts and summarize the community s prioritized mental health needs and strategies to improve the mental health system. This report is comprised of the following sections: Overview of the community engagement activities that took place in Contra Costa County from January 2014 through April Community engagement included the participation of mental health consumers, family members, mental health providers, County staff, and stakeholders from community based organizations across various sectors, including law enforcement and education. The community engagement activities sought broad participation by stakeholders in order to reflect the needs and ideas of its diverse communities. These groups include consumers at every age group (Children/Parents, Transitional Age Youth (TAY), Adults, and Older Adults); people experiencing homelessness; and the Latino, African American, Asian Pacific Islander (API), and LGBT communities. Review of prioritized mental health needs that outlines both the strengths and opportunities to improve the mental health service system in Contra Costa County. Based on stakeholders feedback obtained during the community engagement events, this portion of the report identifies the priority mental health needs by target demographic. Review of prioritized ideas and/or strategies to address the priority mental health needs and enhance the current mental health system. Strategies and ideas were developed by participants across all of the community engagement events.

.")
8 Consolidated Report on MHSA Community Engagement Activities Page 8 Background on the MHSA Proposition 63 (Mental Health Services Act) was approved by California voters in 2004 to expand and transform the public mental health system. The MHSA is funded by imposing a one percent tax on individual annual incomes exceeding one million dollars. The MHSA represents a statewide movement to provide a better coordinated and more comprehensive system of care for those with serious mental illness, and to define an approach to the planning, delivery, and evaluation of mental health services that are in alignment with the MHSA Values (see Figure 1). The CPP process is an integral component Figure 1: MHSA Values of MHSA, which requires a meaningful stakeholder process to provide subject matter expertise to the development of plans focused on utilizing the MHSA funds at the local level. In 2013, Contra Costa initiated this activity by completing an initial needs assessment for the Three-Year Program and Expenditure Plan RDA and PEERS were contracted to carry out the next phase community engagement of the CPP process (see Figure 2: Overview of the CPP Process). Figure 2: Community Program Planning Process
9 Consolidated Report on MHSA Community Engagement Activities Page 9 Community engagement activities sought to obtain stakeholder input on addressing service delivery gaps that have emerged as well as enhancing those mental health services offered by current MHSA programs. This report reflects the deep commitment of Contra Costa County BHS leadership, staff, providers, consumers, family members, and other stakeholders to the meaningful participation of the community as a whole in designing MHSA programs that are wellness and recovery focused, client and family driven, culturally competent, integrated, and collaborative. We are hopeful that this synthesized report of community voices will inform the development of the Three Year MHSA Program and Expenditure Plan.
 initiated a planning process for the Mental Health Service Act (MHSA) Three-Year Program and Expenditure Plan for fiscal years 2014-2017.")
, a consulting firm with mental health planning expertise.")
10 Consolidated Report on MHSA Community Engagement Activities Page 10 Community Engagement Description of Community Engagement Activities Planning Approach and Process In December 2013, Contra Costa Behavioral Health Services (CCBHS) initiated a planning process for the Mental Health Service Act (MHSA) Three-Year Program and Expenditure Plan for fiscal years The planning team was led by Warren Hayes, CCBHS MHSA Program Manager; Gerold Loenicker, CCBHS Mental Health Program Supervisor; Erin McCarty, CCBHS Acting MHSA Project Manager; and Resource Development Associates (RDA), a consulting firm with mental health planning expertise. The planning team used a participatory framework to encourage buy-in and involvement from stakeholders including consumers and family members, mental health service providers, and other interested community members. Community engagement was divided into four phases: 1) Project Launch, 2) Conducting and Documenting Events, 3) Report Back to Community, and 4) Consolidated Report. Figure 3 lists the activities included in each phase. Figure 3: Community Engagement Activities Throughout the community engagement phase of the CPP process, the team held regular phone meetings. At these meetings, updates were provided on community engagement activities, community outreach and ways to improve outreach based on stakeholders feedback. For instance, after meeting with the planning team and based on feedback from the Consolidated Planning and Advisory Workgroup
11 Consolidated Report on MHSA Community Engagement Activities Page 11 (CPAW), it was decided to include a County-wide LGBT consumer focus group, add a Latino community focus group in Central County, and expand the Latino focus group in East County to include the African American community and focus on children and family issues. An additional general stakeholder focus group was organized to ensure the participation of community members, specifically parents of adult consumers, who were unable to attend previous focus groups events. Community Engagement Activities RDA carried out a set of community focus groups and community forums to ensure that the prioritized mental health needs and ideas/strategies for improvement reflected stakeholders experiences and suggestions. Community engagement activities and their corresponding dates are presented in the table below, followed by a detailed description of each activity. Table 1: Community Planning Activities and Dates Activity Date Planning Process Refinement Kickoff Meeting with CCBHS and CPAW December 5, 2013 Community Engagement Consumer and Family Member Focus Groups January 28 February 25, 2014 Provider Focus Groups February 25-27, 2014 Reporting of Program Strengths and Needs Community Forums March 19-26, 2014 Presentation to CPAW & MHC April 3, 2014 To initiate the planning process, the RDA held a project launch meeting with CCBHS and the Consolidated Planning and Advisory Workgroup (CPAW). At this meeting, RDA presented an overview of the community engagement activities in relation to Contra Costa s CPP process, timeline of events, and the types of stakeholders the County would engage in community focus groups. Based on input from CPAW, RDA expedited its timeline for conducting community engagement activities to end in April 2014 and ensure our efforts coincided with the development of the County s Three-Year Program and Expenditure Plan. RDA and PEERS staff conducted 23 focus groups to gather input from mental health providers and community members about their experiences with the County s mental health system as well as their recommendations for improvement. Participants were asked to reflect on what works well in the current system, what is missing or where there are gaps, and what strategies or programs could address identified gaps or improve MHSA services. The complete facilitator s protocol has been included in Appendix A.
12 Consolidated Report on MHSA Community Engagement Activities Page 12 The focus group format allowed the planning team to reach a greater number of participants, and gave participants the chance to discuss topics among themselves, thereby producing additional information that might not have emerged in individual interviews. Outreach and recruitment efforts for the focus groups were conducted by CCBHS staff involved in the MHSA planning team and service providers with connections to the various priority populations. Focus groups were advertised through the distribution of two flyers. The first flyer explained the purpose and format of the meetings (see Appendix B). The second flyer provided logistical information, such as the date, time, and location of each event (see Appendix C). Focus groups were held at various community-based and mental health agencies throughout the County. Each meeting lasted approximately 90 minutes and snacks/light refreshments were provided. Eighteen of the focus groups were targeted for consumers, family members, and representatives from unserved, underserved, and inappropriately served groups. This included focus groups specifically for each age group identified in the MHSA (Children, TAY, Adults, and Older Adults) as well as people experiencing homelessness and the Latino, African American, Asian Pacific Islander (API), and LGBT communities. Consumer and family member focus groups were held throughout the county in the west, east, and central regions, which represent the highest concentration of people who access and are eligible for the public mental health system. Consumers and family members were offered $15 gift cards in appreciation for their participation in the community focus groups. An additional five focus groups were held with MHSA providers. There was one focus group for each age range (Children, TAY, Adults, and Older Adults), and an additional focus group for Older Adults. Provider focus groups were convened in the central part of the County, however providers from all County regions were in attendance. After completion of the consumer and provider focus groups, RDA and PEERS synthesized the results in order to integrate program strengths, key mental health needs for each population, barriers to entry and access to mental health services, and recommendations for addressing the challenges and barriers. The results and analysis of 23 focus groups with consumers, family members, and service providers were presented to stakeholders in a second series of community engagement activities. RDA and PEERS cofacilitated four community forums, one for each region of the County and one joint presentation to CPAW and the Mental Health Commission (MHC) at a regularly scheduled CPAW meeting. The community meetings were two hours long and each had an average of 40 participants. The purpose of the community meetings was to review the findings from across the community, validate findings, and solicit further feedback on the proposed needs and strategies that were developed from the focus groups. Flyers for the community meetings were distributed by to MHSA stakeholders, including MHSA providers, community-based providers, and all individuals who signed up for updates during the focus groups activities as well as through the MHSA coordinator s list serve. Additionally, advertisements were placed in the local Contra Costa newspaper.
13 Consolidated Report on MHSA Community Engagement Activities Page 13 During the community forums, stakeholders had an opportunity to comment on the results of the focus groups. Stakeholders also provided feedback on how well the community engagement activities reflected their input. Participants were given four handouts to guide the discussion: 1) Overview of the CCBHS Assessment of Mental Health Needs, 2) Overview of Current MHSA Providers, and 3) Overview of the MHSA Values and Components (see Appendices D F). Demographic Data of the Community Engagement Participants (see Appendix G) included information regarding the total number of participating consumers and family members by population, participating service providers by systems of care, the stakeholder affiliation of participants, as well as proportion of participants by gender, age, race/ethnicity, and place of residence. Stakeholder Participation Special efforts were made to ensure that consumers were represented in all phases of community engagement. RDA and PEERS conducted 23 focus groups, of which 18 of the meetings were held with consumers and family members; five focus groups were with service providers. The community planning process concluded with three community meetings and a presentation at the April CPAW and Mental Health Commission (MHC) meeting. A total of 427 stakeholders participated in all community planning activities. The following table presents the number of participants at each activity. Focus Groups Table 2: Total Count of Participants by Community Planning Activity Community Planning Activity Total Count of Participants Consumer and Family Member Focus Groups 232 Service Providers Focus Groups 55 Community Meetings & CPAW/MHC Meeting 140 Total 427 Emphasis was placed on guaranteeing consumers and family members were represented in all community engagement activities with consideration for the demographic and geographic diversity of Contra Costa County. CCBHS sought input from consumers and family members throughout the life span as well as specific target groups. These target groups included people experiencing homelessness and the LGBTQ community in addition to several communities of color African American, Asian and Pacific Islander, and Latino communities. See Figure 4 below that summarizes the different communities and geographies of community engagement participants.

14 Consolidated Report on MHSA Community Engagement Activities Page 14 Figure 4: Community Engagement Participants by Communities and Geographies In an effort to reach Contra Costa County s large Latino community, a Spanish-language interpreter was provided at the Latino consumer focus groups in West and East Counties, and the Central County focus group was conducted in Spanish by a bilingual facilitator. Additionally, handouts, demographic forms, and comment cards were translated into Spanish. Because only three community members participated at the API consumer focus group, an interpreter was not requested. One focus group also targeted African American families, in addition to Latino families; however, no African American stakeholders attended this group. The TAY, Adult, and Older Adult focus groups included African American consumers. Table 3: Total Count of Participating Consumers and Family Members by Population summarizes the focus groups conducted with consumers and family members by population. Table 4: Total Count of Participating Service Providers by System of Care presents the number of participants at each provider focus group, organized by system of care. Table 3: Total Count of Participating Consumers and Family Members by Population Focus Group Type Count of Participants % of Total Transitional Age Youth (TAY) 66 28% Adult 22 9% LGBTQ 28 12% Older Adult 24 10% People Experiencing Homeless 19 8% General Consumers and Family Members 14 6% Latino Community 54 23% Children & Parents 2 1% Asian & Pacific Islander Community (API) 3 1% Total %
15 Consolidated Report on MHSA Community Engagement Activities Page 15 Table 4: Total Count of Participating Service Providers by System of Care Count of % of Focus Group Type Participants Total TAY Provider 23 42% Children Provider 10 18% Adult Provider 7 13% Older Adult Provider 15 27% Total % Of those who participated in the focus groups, 167 participants indicated their organizational affiliation. Table 5: Total Count and Percentage of Participants by Stakeholder Affiliation illustrates the number and percentage of each type of stakeholder group represented in the community focus group events. The majority of participants affiliation was with a community-based organization (39%) or county government agency (15%). In addition to an affiliation with a community-based organization, many participants specified the sector in which they worked. As a result, these participants checked law enforcement, education, alcohol and drug services, medical or healthcare, or Veterans organization. Table 5: Total Count and Percentage of Participants by Stakeholder Affiliation Stakeholder Affiliation Count of Participants % of Total Community-based organization 65 39% County government agency 25 15% Education agency 17 10% Provider of mental health services 14 8% Medical or health care organization 6 4% Social service agency 6 4% Law Enforcement agency 1 1% Provider of alcohol and drug services 1 1% Other 32 19% Total % Participants who did not affiliate with an institution, identified with a particular population (e.g. consumer, caregiver for foster youth, disability) or occupation (e.g. in-home care, public benefits advocate, life coaching). Each focus group requested participants to complete an anonymous demographic form (see Appendix H). These forms asked participants to report their age, gender, race/ethnicity, and whether they identified as a consumer, family member, or service provider (participants could choose more than one status). Responses from the demographic forms are described below. Because demographic forms were optional for participants, some participants may not have submitted forms or may have declined to respond to certain questions.

 Under 16 4% 60 and older 22% 16-24 22% 25-59 52% Participant Gender Sixty")
 Transgender / Genderfluid 3% Male 37% Female 60% Participant Race/Ethnicity Figure 7: Count of Focus Group Participants by")
16 Participant Age Range Contra Costa Behavioral Health Services Consolidated Report on MHSA Community Engagement Activities Page 16 Participants were given the choice of selecting from four different age ranges corresponding to the MHSA categories of Children, TAY, Adults, and Older Adults. A little more than half of participants were years of age. The proportion of Transitional-Age Youth and Older Adults was the same (22%). Four percent of participants were under 16 years of age (see Figure 5: Percent of Focus Group Participants by Age (n=220) Under 16 4% 60 and older 22% % % Participant Gender Sixty percent of focus group participants identified as female, a little over a third (37%) identified as male, and 3% identified as transgender (see Figure 6). Figure 6: Percent of Focus Group Participants by Gender (n=222) Transgender / Genderfluid 3% Male 37% Female 60% Participant Race/Ethnicity Figure 7: Count of Focus Group Participants by Race/Ethnicity (n=220) indicates that the majority of focus group participants were Caucasian. Approximately sixty participants identified as Hispanic/Latinos, resulting in the second highest racial/ethnic group to be represented in the stakeholder focus groups. The majority of bi-racial participants identified as Caucasian and African American, Caucasian and Latino, and Caucasian and Native American. The two participants who checked other, identified as Middle Eastern.

17 Consolidated Report on MHSA Community Engagement Activities Page 17 Figure 7: Count of Focus Group Participants by Race/Ethnicity (n=220) Other American Indian/Native Alaskan Multi-Race Asian or Pacific Islander African American/Black Hispanic/Latino White/Caucasian Number of Participants Participant Place of Residence Because Contra Costa is a vast county, with each region characterized by diverse needs and challenges, focus groups with target populations were conducted in each region. Table 6: Count of Focus Group Participants by County Region (n=223) illustrates the total number of participants and percentage based on county region. The majority of focus group participants were from Central County (40%). Approximately a quarter of participants resided in West and East County, respectively. Within Central County, the majority of participants reported they reside in Concord and Richmond. Other popular cities of residence include: Antioch, Martinez, Pittsburg, and Walnut Creek. Table 6: Count of Focus Group Participants by County Region (n=223) County Region Count of % of Participants Total West 54 24% Central 90 40% East 57 26% Other 22 10% Total % Community Meetings The second phase of the community engagement process involved presenting the findings from the 23 focus groups and soliciting further feedback on identified mental health needs and recommendations. Three community meetings were held, one in each region. A fourth meeting was organized to present to CPAW and the Mental Health Commission (MHC). At each forum, RDA presented both the consolidated and population specific results of the focus group events (see Appendix I for the Community Forum Presentation). Table 7 lists the total count of participants at each community meeting and the CPAW/MHC meeting. Similar to the focus groups, the Central County community forum drew the largest number of participants (29%).

18 Consolidated Report on MHSA Community Engagement Activities Page 18 Table 7: Count of Community Forum Participants by County Region (n=111) County Region Count of Participants % of Total Central 41 29% East 38 27% West 29 21% CPAW 32 23% Total % Community meeting participants were asked to identify their stakeholder affiliation. Of the 32 participants who responded to the demographics survey, the majority of participants (44%) were providers of mental health services (see Figure 8: Percent of Community Meeting Participants by Stakeholder Affiliation). In addition to citing they were a mental health provider, some participants also checked they were providers at a community-based organization, education agency, or law enforcement. Those participants who marked Other specified they identified as a consumer or peer specialist. Several participants identified with the advocacy group, National Alliance on Mental Illness (NAMI). Figure 8: Percent of Community Meeting Participants by Stakeholder Affiliation Other Provider of alcohol and other drug services Medical or healthcare organization Law enforcement County government agency 7% 4% 4% 4% 7% Education agency Community-based organization 15% 15% Provider of mental health services 44% 0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100% Similar to the focus groups, facilitators requested the participants to fill out an anonymous demographic form (see Appendix H). Participants were asked questions regarding age, gender, race/ethnicity. In addition, they were asked their city of residence in the County and if they identified as a consumer, family member, or service provider (participants could choose more than one status).

, Adults, and Older")
19 Consolidated Report on MHSA Community Engagement Activities Page 19 This section reviews the results from the demographic surveys. Because demographic forms were optional for participants, some participants may not have submitted forms or may have declined to respond to certain questions. As a result, the following tables and figures do not necessarily reflect the total number of participants. Participant Age Range Participants were given the choice of selecting from four different age ranges corresponding to the MHSA categories of Children, Transition-Age Youth (TAY), Adults, and Older Adults. Of the 32 participants, a large proportion of participants were years of age. The remaining seven participants were 60 and older years of age (see Figure 9: Percent of Community Meeting Participants by Age (n= 32)). Figure 9: Percent of Community Meeting Participants by Age (n= 32) 60 and older 22% % Participant Gender Of the 32 participants who filled out the demographics form, a large majority of respondents were female (78%). The remaining seven respondents were male (22%) (see Figure 10: Percent of Community Meeting Participants by Gender (n= 32)). Figure 10: Percent of Community Meeting Participants by Gender (n= 32) Male 22% Female 78% Participant Race/Ethnicity Figure 11: Percent of Community Meeting Participants by Race/Ethnicity (n=32) indicates that majority of community meeting participants who filled out the demographics form were White/Caucasian (70%).





20 Consolidated Report on MHSA Community Engagement Activities Page 20 Thirteen percent of respondents were multi-racial. The remaining respondents identified as African American, Hispanic/Latino, Asian/Pacific Islander, and American Indian/Native American. Figure 11: Percent of Community Meeting Participants by Race/Ethnicity (n=32) 100% 90% 80% 70% 67.7% 60% 50% 40% 30% 20% 10% 0% 6.5% African American/Black 3.2% 3.2% American Indian/Native Alaskan Asian or Pacific Islander 12.9% 6.5% Hispanic/Latino Multi-Race White/Caucasian Participant Place of Residence Figure 12: Percent of Community Meeting Participants by Place of Residence illustrates community meeting participants place of residence by region. Of the 32 participants who responded to the demographics survey, the majority of participants reside in West County (38%) and Central County (31%). A smaller proportion resided in South and East Counties. The 12% of respondents who marked Other did not specify their place of residence. Figure 12: Percent of Community Meeting Participants by Place of Residence West 38% Central 31% South 3% Other 12% East 16%
21 Consolidated Report on MHSA Community Engagement Activities Page 21 Community Engagement Results Overview County-Wide Results At the conclusion of focus group events, the facilitation team synthesized the results across age groups and populations to develop findings that apply to the County s mental health system as a whole. These findings were presented at the community forums held at the end of March 2014 and at the April 3, 2014 Consolidated Planning and Advisory Workgroup (CPAW) meeting. Based on feedback from forum participants, we refined these findings in between each meeting. Below are the consolidated findings that represent overall results of community engagement activities. Active and engaged stakeholder groups. Contra Costa County has a diverse network of active and engaged stakeholders in the mental health system. Consumers, family members and loved ones, and providers demonstrated their commitment to improving the mental health system in the community. At many of the focus group events, there was overwhelming participation by different stakeholder groups. Stakeholders came prepared to brainstorm ideas to close the gaps in mental health services, and the discussion was passionate. Programs that support and adapt to the needs of consumers. In all of our focus groups, stakeholders discussed programs that serve as models for success in mental health services. Consumers felt that many programs are responsive to their needs and honor their experiences in the mental health system. Providers reported back about the innovative programs they have developed to provide comprehensive, recovery-oriented care for consumers. Family members discussed their selfless efforts and shared deeply about their experiences in supporting their loved ones through recovery. I keep hearing the words too high functioning, I had to go to speech therapy. I couldn t speak. I m tired of hearing this; it doesn t mean nothing is wrong. Deep inside bombs are going off. I ve kind of jumped over here, here, and here. I want to voice it. -Central County Homeless Adult Consumer Inconsistent experience of wellness and recovery. While some programs and sites are recovery oriented, there is an inconsistent experience of wellness and recovery. Focus group participants from underserved cultural groups identified programs lacking a whole-person approach to wellness as a barrier to participating in mental health services. In addition, different stakeholders had very different accounts of how recovery oriented
22 Consolidated Report on MHSA Community Engagement Activities Page 22 programs were, indicating that there is an inconsistent experience of wellness and recovery across the mental health system. This was especially true for some consumers who believed that recovery is disincentivized because services become less available as recovery is achieved, placing them at risk of relapse. I don t want to be handcuffed so to speak in that I m mandated to live this way or that way. You can lead me so far. I don t want to become dependent on someone else in doing something for me. What happens if the funding stops and I m thrown out? I don t want them holding my hand. You ve helped me so far, what would keep me going further? Central County Adult Consumer Lack of consumer and family driven services. Participants noted that services seem more available to consumers who are better able to advocate for themselves and less available for those who are less likely or able to assertively seek services. Family members are relied upon as a critical resource for consumers, especially in in cases of crisis, but are not included in service or treatment planning. Services that are collaborative and integrated across the mental health system. Consumers, family members, and providers all agree that the mental health system contains a lot of valuable components, but the experience of the system is disjointed. This increases the risk of people falling through the cracks. For some participants, there was a pervasive lack of knowledge about service availability and frustration with the process to obtain needed services for themselves or a loved one. Participants said the County needs to improve its partnerships with non-mental health providers such as the schools, criminal and juvenile justice, and social service agencies. Culturally competent services for unserved and underserved groups. In every focus group event, participants acknowledged that stigma of mental health and unserved/underserved groups is a barrier to receiving services. We heard participants emphasize the stigma of the Lesbian, Gay, Bisexual, Transgender, and Queer (LGBTQ) community as pervasive throughout the mental health system and in the community. The LGBTQ community noted that a lack of trained professionals on LGTBQ health issues is a significant barrier to We do LGBTQI cultural competence training we could do more of it. We ve only done about 15 trainings last year, but I want it to be 45 trainings. LGTBQ Provider accessing services. Bullying and physical harassment was a specific concern of young people, especially within the Transgender community, as a result of stigma. Although cultural-specific services are available in certain settings, focus group participants suggested that they are not available across the mental health system. Other cultural barriers to mental health services exist; for example, reliance on telephone translation and the access line not trusted by some cultural backgrounds. Lack of access to basic resources gets in the way of recovery. Despite the County s best efforts to ensure access to housing, benefits, transportation and other basic resources, there remains a significant need for additional resources. Focus group participants offered these specific examples where additional resources are needed:
23 Consolidated Report on MHSA Community Engagement Activities Page 23 The shelter environment is difficult for those who are engaging in dual recovery. There is a lack of single occupancy units compared to shared housing. Lack of transportation is a barrier to receiving services. Clothing, food, childcare, and income were all cited as significant needs. Continuity and comprehensiveness of crisis specific services. For all age groups, focus group participants described a lack of crisis supports before, during, and following a crisis event. Consumers, family members and loved ones, and providers noted that there are minimal crisis services outside of business hours that would help prevent or respond to a crisis. It was also acknowledged that the County lacks comprehensive discharge planning and followup support for consumers after a crisis event. High utilizers of involuntary services, such as the hospital and jail, experience difficulty in engaging in services pre and post crisis. In addition, crisis-specific resources for minors and young people were reported as significant needs in the community. Accountability to the MHSA and consumers served by mental health services. Upon reflection and discussion of the priority needs and strategies to close the gaps at the Community Forum events, participants suggested that there is a lack of information and transparency to support data-driven decision making. Stakeholders specifically requested to know the number and demographics of persons Where s the context? Where s the data? Where s the information? I want to see the data on what is evidenced based. I want to see what we re doing that s working. -Family members The ability for us to connect people to services right after that is almost impossible so they can get the medications and the services they need. I think MH access is a really slow process. We need something that can respond to the urgency in terms of the nature of this population they wait too long for psych assessments and for medication assistance. -TAY Provider served by MHSA programs, funding amounts for each program and how those funds were spent, and the outcomes of consumers in MHSA funded programs. Program outcomes and evaluation that was inclusive of peers/consumers was another specific request of stakeholders. Develop a continuum of services that provides support at all levels of recovery. Stakeholders reported specific suggestions on how the County can develop a continuum of services that provides support at all levels of recovery. Examples include developing career pathways for people with lived experience in and out of the mental health system, and to maximize the use of wellness, community, and multi-service centers to expand meaningful daily activities that promote engagement in services, recovery, and wellness.
24 Consolidated Report on MHSA Community Engagement Activities Page 24 I ve done this work. I m not just telling you something and blowing in the wind - those are some things I did to do advocate work. I ve done some case management. I wake up every day to do something to improve my life. -Central County Homeless Adult Consumer Consider ways to promote the meaningful inclusion of peers and family members in the mental health system. Focus group participants believed the County can do more to promote the meaningful inclusion of peers and family members in the mental health system. Stakeholder suggested that CCBHS develop a Consumer Self-Advocacy Training program and build upon Speaker s Bureau type activities (such as the Office of Consumer Empowerment s WREACH: Wellness Recovery Education for Acceptance, Choice, and Hope) to help consumers develop the skills to more assertively navigate the mental health system. Focus group participants also noted that the number and roles of peer and family providers can be expanded, especially in outreach and engagement, systems navigation, and crisis response and follow-up. Specifically, peer and family member positions could be considered to address gaps related to recovery, collaboration, integration, and cultural relevance. Additional services to collaborate with and support families and loved ones who serve as primary resources for consumers in recovery were also requested. Strengthen the collaboration between the County, providers, and other stakeholders. In order to address the disjointedness felt by consumers, family members and loved ones, and providers in the mental health system, focus group participants suggested a number of ways to increase collaboration and awareness of the County s mental health services. Providers suggested that the County develop formal mechanisms for collaboration using Memorandums of Understanding (MOUs) or contracts as leverage. Participants suggested that the County develop a comprehensive resource/referral guide for all stakeholders that includes a service description, referral process, and eligibility criteria to increase people s knowledge of the services available. Participants also suggested CCBHS increase We need to increase the number of bilingual and bicultural workers, especially: Spanish, Farsi, Arabic, and Southeast Asian Languages We especially need trainings that address cultural competency with LGBTQI issues. Children s Provider Training on bullying [is needed]. The school just slaps kids on the wrist and moves on. That s not taking care of the situation. One killed pulled a knife on my daughter on the bus and they didn t do anything. Central County Parent mental health awareness for non-mental health professions (i.e. school faculty and staff, probation officers, etc.) such as Mental Health First Aid and Youth Mental Health First Aid, Applied Suicide Intervention Skills Training (ASIST), Safe Talk, Crisis Intervention Team (CIT) training, and more. Stakeholders also believed that integration between primary care and substance use services could be enhanced for all age groups, and specifically for older adults. In addition, a stronger partnership with law enforcement and the County s Community Corrections Partnership (CCP) was encouraged by participants to strengthen
25 Consolidated Report on MHSA Community Engagement Activities Page 25 collaboration around AB109 (also known as Criminal Justice and Public Safety Realignment ). Promote a culturally competent and diverse mental health workforce. Focus group participants, particularly those from underrepresented cultural groups, said that institutionalized stigma needs to be addressed proactively by CCBHS via culturally relevant interventions. Stakeholders suggested that the County consider non-traditional ways to allow access to core mental health services and increase the number of clinical services available in cultural-specific programs. Other suggestions to address institutionalized stigma were to increase public awareness through targeted media campaigns and outreach in the community. Increase access to basic resources such as housing, transportation, and entitlement benefits. Focus group participants made the follow suggestions to improve access to basic resources: Housing: Increase the availability of housing options from transitional through permanent supportive housing. CCBHS should also consider a sober shelter space for those in dual recovery. The County should also prioritize the development of affordable single occupancy housing. Transportation should be written into our [treatment] plan, like how to get to mental health appointments. Maybe shelter staff should consult with mental health staff to get things more incorporated. Central County Homeless Adult Consumer Transportation: Consumers requested that the county increase access to transportation resources, though no preference is given to a particular solution. Consumers reported that the type of transportation (bus, shuttle, van service, etc.) is less important than its availability. Partnership with Social Services: Providers and consumers said CCBHS could strengthen its collaboration with social services agencies to streamline access to entitlement benefits. Enhance the continuity and comprehensiveness of crisis services for all age groups and for high utilizers of criminal justice and hospital systems. Consumers, family members and loved ones, and providers prioritized the need to develop programs that address the revolving door of Psychiatric Emergency Services (PES) and the jails. Specific suggestions they included are: Intensive outreach to engage people that are less able to advocate for themselves or are difficult to engage. Mobile crisis services to reduce inappropriate use of jails/pes and increase recovery supports. Discharge and post crisis follow-up services to facilitate engagement with the mental health system. One of the things that I noticed throughout is the discussion is that there isn t enough support for recovery after the crisis It sounds like we really need to talk about the programming and what we can do after that crisis. It seems to be a huge gap for all ages. CPAW member
26 Consolidated Report on MHSA Community Engagement Activities Page 26 Specific requests were made by providers and parents of minors and young people to consider the exploration of in-county children s crisis and residential services. Family members and loved ones of consumers strongly suggested and supported the implementation of AB1421 Assisted Outpatient Treatment (also known as Laura s Law ) to address the needs of consumers who are difficult or hard to engage, don t readily participate in treatment, and have repetitive contact with the jails and psychiatric emergency services. Improve staff and provider professional development and prioritize hiring and recruitment of bicultural/bilingual staff. Across all of the community engagement events, we heard that consumers, family members and loved ones, and providers supported the further improvement and training of mental health staff in the following areas: Wellness and recovery-focused services Engagement and welcoming environment (e.g. customer service orientation) Cultural competence and relevance Collaboration and integration Trauma informed care HIPAA regulations What about staff development for contracted agencies like on cultural competency, etc.? Many CBOs don t have the money to get it, but if they County can do that and open it up to our providers that would be helpful. CPAW member Consumers also requested that the County prioritize the hiring and recruitment of bicultural/bilingual mental health staff that is reflective of the populations served.
27 Consolidated Report on MHSA Community Engagement Activities Page 27 Community Engagement Results by Population Children System of Care Parents, providers, and children s mental health staff contributed to a series of in-depth discussions about the children s system of care in Contra Costa. Overwhelmingly, providers, staff, and parents all agree that once enrolled in a program or with a provider, children receive a comprehensive array of services that contribute towards their resiliency and wellness. However, common challenges that parents with children receiving mental health services face include long wait-times in-between appointments, a lack of culturally and linguistically competent providers, and inadequate supports pre and post crisis. Focus group participants offered several strategies to address these gaps in mental health services for children such as hiring additional child psychologists (especially those who are bilingual and bicultural), developing more mobile or home-based services to increase entry into mental health services, and training to non-mental health professionals on how to intervene in the event of a crisis and where to go for help. CCBHS continues to develop new and innovative programs, especially those that implement evidence based and promising practices. Children s providers and staff acknowledged that even with limited resources, CCBHS is dedicated to enhancing the children s system of care with new and innovative programs and services. In particular, children s providers are focusing on the integration of evidence based best practices, such as Trauma Informed Care. Once children are enrolled in services, parents are very satisfied with the care and attention their children receive in mental health services. Parents were supportive of the notion that once enrolled in mental health services, their children received great care. Parents reported that providers and mental health staff were very informative, helpful in connecting them with The principal kept blaming my daughter for a meltdown she had and kept asking her to do something [different] that she wasn t capable of. -Central County Parent other services, and supportive to parents and other family members. The staff are easy on the kids. My kids enjoy coming here [CCMH]. They like it and that s what makes it comfortable. They re not in fear, they re safe and relaxed. -Central County Parent Continuity and care coordination. Focus group participants reported there is a lack of care coordination, especially between medication management and
28 Consolidated Report on MHSA Community Engagement Activities Page 28 psychosocial supports. Parents discussed the importance of having the psychologist and psychiatrist work together as a team. Parents noted the lack of mental health supports and awareness in the schools as a particular concern. Parent/family supports. For parents and families seeking services or coordinating between different providers, focus group participants discussed the lack of navigation support from the County. Parents found community-based providers helpful in their capacity to navigate certain services, but there is a lack of navigation support between County mental health services and between County and CBO services. Awareness and accessibility to mental health services. Parents and providers of mental health services discussed the lack of awareness of the types of mental health services and the lack of accessibility to services. In particular, parents discussed how difficult it was to know where to go to get their children help when mental health problems arose; parents reported that getting initial entry into the mental health system is difficult. Providers spoke to the geographic and transportation barriers to their clients receiving ongoing mental health services. Some providers felt that services are too consolidated in only certain parts of the County, and paired with a lack of transportation options, were difficult for parents or family members to physically get to. The whole experience wasn t very pleasant when I was 5150 ed. The staff weren t horrible, but they weren t personable. They didn t get to know my name They didn t go out of their way to help me at all. It was a scary environment. They put you in a little room and that s scary. -Central County Youth We ended up going to mental health services out in Oakland because I felt there was nothing here that could help her. -Central County Parent Crisis services continuum. Parents and providers both agreed that more can be done to enhance the continuum of crisis services for children. Pre and post crisis services are especially difficult to navigate and access due to a lack of information and awareness about what pre and post crisis services are available. Specific requests were made by parents and families to increase awareness with school staff on how to both intervene in the event of a crisis and how to refer a family to the County during a crisis. Mental health workforce needs. Contra Costa County is a diverse County with a variety of cultural and linguistic needs represented by those seeking mental health services. As such, providers and parents from several different cultural and linguistic backgrounds indicated that there is a lack of bicultural and bilingual mental health workers. Other mental health workforce needs includes a lack of child psychiatrists and a bilingual/bicultural (Spanish) child psychologist. Enhance the continuity and care coordination of mental health services through increased collaboration and decentralizing service delivery. Focus group participants suggested several ideas or strategies to help enhance the continuity and care coordination of mental health services. Providers
29 Consolidated Report on MHSA Community Engagement Activities Page 29 noted that the lack of basic resources of consumers gets in the way of providing mental health treatment. Focus group participants suggest enhancing the partnership between mental health and the Department of Social Services to increase access to basic supports, e.g. food, clothing, housing, childcare, etc. Providers also discussed the need for more opportunities to collaborate on mental health services and suggested that the County can use Memorandums of Understanding (MOUs) or contracts as leverage to facilitate collaboration. Finally, to increase access to children s mental health services, especially for working parents, both parents and providers suggested adding mobile services to treat children in the home and expanding the hours of services beyond normal business hours. Increase the amount of support to parents and family members. Parents and providers both acknowledged the importance of having more supports for families with children accessing mental health services. In particular, focus group participants suggested that the County recruit more family partners/systems navigators to help parents seeking mental health services for their children. Parents and providers also noted the importance of integrating consumers and family members into the mental health system and supported the idea to involve consumers/family members in service planning, delivery, and quality improvement (QI). Increase awareness and accessibility to mental health services. Focus group participants spoke to the difficulty in the initial entry into mental health services. To address this gap, participants suggested enhancing the information about mental health services on Contra Costa County More comprehensive resource guides available at all County and provider locations on mental health services would also increase information access at all mental health entry points. Enhance the continuity of pre and post crisis services. Increasing the support of consumers pre and post crisis was a common theme throughout the community engagement phase. For children accessing crisis services, parents suggest that more can be done to increase awareness and training about crisis services and crisis intervention. Crisis intervention training for non-mental health professionals, especially in the schools, is needed and Mental Health First Aid and/or Mental Health Youth First Aid are evidence-based models to achieve better crisis training. Families and parents also indicated that they need more training on how The second time I took my daughter to the county hospital They just put me in a waiting room that was glassenclosed and locked I knew nothing about what was going on I wish someone would just come and talk to you. I wish I could have stayed with my daughter. I mean, I wish an exception existed that, when appropriate, I could stay with her. -Central County Parent to help their children in the event of a mental health crisis. Providers and parents both believed more pre and post crisis services for families are needed, especially support following a crisis event that could be provided by a family partner. Providers and older children who participated in the focus groups suggested that a separate crisis hospital or unit is needed. Increase hiring and training of the mental health workforce. In order to meet the mental health needs of consumers in Contra Costa County, focus group participants suggested that the County focus on
30 Consolidated Report on MHSA Community Engagement Activities Page 30 hiring additional mental health workers. Participants made specific requests to increase the number of child psychiatrists and bilingual/bicultural (Spanish) child psychologists. More bilingual/bicultural workers are needed in general throughout the County. Providers also suggested that mental health workers from different cultural backgrounds cross-train each other to increase their competency working with consumers that have different backgrounds from their own. Transitional Age Youth (TAY) System of Care Strong network of community-based providers that are highly supportive of youth consumers. The community engagement phase saw a large proportion of highly engaged youth and TAY providers participating in the events. Youth felt that mental health service providers were highly supportive of their own wellness goals and attentive to their mental health needs. TAY providers were also highly engaged and demonstrated how their programs sought to adapt to the needs of their consumers. TAY peer staff help consumers feel more welcome and engaged in services. Youth participants in the focus group events discussed the importance of having peer staff in TAY mental health programs. Youth felt peer staff help them speak openly about their recovery and that they perceived peer staff as role models. They keep me busy. When I used to come here, I used to run the streets and do delinquent actions. This keeps me busy. -West County Youth Activity-based programs promote wellness and recovery. Activitybased programs that promote wellness and recovery helped youth feel more welcome and less-stigmatized for seeking out mental health services. For those youth that are engaging in TAY mental health services, they appreciated the diversity and accessibility of activity-based programming that taught them developmentally appropriate skills. Mental Health Awareness in the schools. Across all focus groups with youth and providers, participants strongly agreed that there is a lack of mental health awareness and sensitivity in the County s schools. Youth and staff retold stories of bullying, harassment, and violence in the schools due to the stigma attached to mental health and other issues that affect young people. TAY suggested that school faculty, staff, and other students did not understand mental health; school staff and faculty particularly lacked the skills to respond to mental health crises competently. Awareness and accessibility to mental health services. Many youth and parents of youth discussed the difficulty in accessing information about mental health services for TAY. Similarly, students and parents discussed the lack of knowledge school staff and faculty have about County mental health resources. Youth participants suggested the stigma associated with receiving treatment for mental health prevents them from seeking mental health services in traditional treatment settings.
31 Consolidated Report on MHSA Community Engagement Activities Page 31 Youth development approach across mental health services. Youth focus group participants felt that mental health services lacked a whole-person approach to mental health. Youth face a broad range of challenges as they transition to adulthood including school, employment, and life-skills. Youth note that the types of programs that integrate these various components into an approach, i.e. Youth Development, are needed. In addition, there are a lack of opportunities for youth to develop these skills and become peer staff. Young folks need a space where they are wanted and needed. [They need] someone who can relate to what you are going through and not telling you you can control it or you re not trying hard enough. You need someone to understand what you can and can t control with support. -East County Youth As a foster mom, what would be really good for the county is to provide more mental health care in a short period of time for the kids that come to us. When I get an emergency placement, they don t get mental health services for months, whereas I need them to be talked to and assessed within a week. -East County Parent Prevention and early intervention services. Focus group participants discussed the need to continue and or enhance activity-based programs that promote wellness and recovery. In addition, providers and youth strongly felt that there were a lack of therapists and psychosocial supports for youth with mental illness to prevent relapse. Suicide prevention and intervention. Suicide prevention and intervention skills are essential to the friends and loved ones of people with mental illness; suicide prevention is especially important to the TAY age group. Focus group participants noted that there is a lack of regular training and supports in developing the skills related to suicide prevention and early intervention. Partner with the school districts to deliver trainings and resources on mental health to increase awareness and accessibility to services. Focus group participants suggested that the County could form stronger partnerships with the school districts to provide and enhance trainings that address mental health awareness. Youth and TAY providers suggested Mental Health First Aid and Youth Mental Health First Aid as training curriculums to give school staff and faculty the skills they need to recognize and address mental health issues. Develop stronger outreach to TAY in the communities and enhance access to mental health services in non-traditional settings. In addition to increasing awareness of mental health in schools, focus group participants said that increasing outreach to TAY is critical to promoting accessibility of mental health services to youth. In addition TAY providers and youth participants made several suggestions to increase access to mental health services. Participants suggested increasing the access points to mental health services in non-mental health settings (schools, community centers, wellness centers, community events, etc.) where youth are already present. In addition, youth participants suggested the County
32 Consolidated Report on MHSA Community Engagement Activities Page 32 could work towards developing a smart-phone application for mental health services that would include a comprehensive resource directory, live chat with a mental health representative or clinician, and a calendar of community wellness events. Enhance opportunities for youth to develop life-skills and to serve as peer mentors/staff. Youth participants suggested that mental health programs for TAY continue to develop career pathways for youth to serve as peer staff or mentors and to increase the accessibility of programs that promote wellness and recovery. Programs that youth say are working are activity-based, focus on life-skills, employment skills, and on adapting to the transition to adulthood. In general, focus group participants emphasized the need for TAY mental health programs to take a whole-person approach to promoting wellness and recovery. I like 1:1 [therapy] because she s [the therapist] is focused on how I feel and how I can work on it from a different perspective. They [the County] should add counseling with the parents. The counseling with parents can help them see from someone else s perspective what they need. I would love that. -East County Youth Increase the number of programs that focus on wellness and recovery in order to prevent relapse. In addition to increasing activity-based programming discussed above, youth and providers say that increasing the number and types of therapy and counseling available to youth will help prevent relapse. Participants suggest that the County should support therapy and counseling approaches that also promote a family-inclusive approach, noting the importance of increasing the resiliency of family members supporting youth. Increase targeted trainings on suicide prevention and intervention skills in the community and schools. In order to address the lack of trainings that address suicide prevention and intervention skills, TAY providers and youth felt strongly that more trainings across the County should be offered that address suicide. Participants suggested models such as Applied Suicide Intervention Skills Training (ASIST) and SAFETalk as evidence-based curriculums the County can use to train the community on suicide prevention and intervention. Youth Mental Health First Aid was similarly supported by participants as necessary trainings to conduct with mental health system stakeholders. Adult System of Care Adult consumers across Contra Costa County and their mental health providers shared similar experiences in accessing and navigating the County s public mental health system. Consumers and providers agreed that once consumers and family members are able to receive services through community-based organizations, the experiences have generally been positive and productive, however, accessing and interfacing with County-provided services has been more difficult.
33 Consolidated Report on MHSA Community Engagement Activities Page 33 When available, system navigation is helpful and appreciated. When there is a provider or peer to help consumers navigate the mental health system, consumers and family members are better able to access and engage in the services they need. Community programs provide social support. Consumers praised the structure of community programs and the social support found in participating in community-based organizations. And you get frustrated when you re calling to get help and you re at your weakest already, feeling at your wit s end and couldn t get connected to the proper person. [The Navigator] was there to help you through and get to the community help. She was there to give you that extra push to help us stay standing. West County Adult Consumer And I left the group at one point, but [the provider] was on the phone, calling me, leaving me messages, made me come back and helped me. That s how powerful that group is. We need more groups and communities like that because it helps and it speaks volumes. West County Adult Consumer CBO case managers are caring and helpful. Consumers praised the case managers and case workers provided by several community-based organizations. The appreciated the dedicated oneon-one counseling and care coordination. Employment readiness/opportunities for consumers. Consumers expressed the difficulty of obtaining employment that would allow them adequate means. While some have been able to find part-time and/or entry-level work, the wages are high enough to disqualify them from receiving supplemental security income, but not enough to meet their daily living needs. Processing time to access entitlement benefits. Stakeholders felt that there were disconnects between CCBHS, CBO services, and social services. This disconnect often resulted in a gap of services during which consumers are waiting for benefits to be granted (e.g., food stamps, SSI, housing eligibility, Medi-Cal enrollment, etc.) while having reached the expiry or maximum level of service in another area. I understand because you got people coming in, but if you still have SSI pending and your time is up at the shelter what, you let your time run out and go back to the street? Why put me back on the streets when I ll use on the street? Central County Adult Consumer
34 Consolidated Report on MHSA Community Engagement Activities Page 34 I feel like there has to be a traumatic experience for people to receive to counseling. Why does it have to go that far? When people that are witnessing crimes, they need counseling too. East County Provider Recovery focus across all adult mental health programs. Both consumers and providers felt that in order for consumers to access County services, they needed to have chronic and/or serious mental illness in order to be connected to any County service. Further, the consumers expressed that once they were able to receive the adequate dosage of medication to reduce symptoms, they were switched to medication management services only and/or were terminated from program without referrals for follow-up services. Warm and welcoming environment. Both consumers and providers reported that while some clinics and programs are able to provide warm and welcoming environments, some locations, especially County clinics, have uninviting atmospheres and discourteous staff. Additionally, coordination amongst the personal service coordinators can be an issue. Consumers reported needing to re-tell their story multiple times and that it can be difficult to get all team members to come to a consensus on the plan for treatment. Mental health workforce. Consumers, family members, and providers agreed that providers are overburdened with the current distribution of work. This has resulted in consumers receiving impersonal care, both consumers and providers being unaware of services available, and providers being unable to ensure client handoffs. They just want to get you in, get your money and get you out in 15 minutes or 4-5 people who have the same time apt and they ll give you a 5 minute window before they reschedule you. You can be a minute late and they won t take you. West County Adult Consumer The hospitals are really far away. I m using Kaiser Hospitals when I m supposed to go to Martinez. It s crazy that I d have to go to Kaiser. West County Homeless Adult Consumer Crisis services in West County. Currently, the only County facility that will treat adults in crisis from West County is the County hospital in Martinez. Clients discussed the burden to travel to Martinez when they are in crisis and believe there should be a place to go that is located in West County during a crisis event. Develop programs to increase consumer employment readiness and opportunities for employment. Stakeholders suggested partnering with local businesses to create more employment opportunities for consumers. Additionally, CCBHS should work with CBOs to enhance employment readiness programming for consumers, providing them with professional development and basic technical skills. I would like to see a partnership between CCBHS with local workplaces like Home Depot, Wal-Mart, Lowe s that allows people who are stable and can work, to allow them to work. - West County Family Member

35 Consolidated Report on MHSA Community Engagement Activities Page 35 Establish stronger partnership with Social Services to decrease time process entitlements. To address these issues, CCBHS could strengthen linkages with social services to ensure timely benefits processing and assistance. The goal of such a strategy is to decrease wait times for issuing entitlements and ensure consumers basic needs are met as they work toward recovery. There are so many factors in life affecting your mental condition. If you just want to define Mental Illness, it s very different from Mental Health. Every time you [the County] encourage the client to come in, you run down a list of symptoms and never running a list of strengths. If you talk about strengths, you can promote wellness and promote Mental Health. Adult Provider members in program planning, implementation, and evaluation. Increase the recovery focus across all adult mental health programs. Focus group participants expressed the need for services to be more holistic and focused on consumers wellness and recovery, as opposed to the current approach of triage, medication, and symptom reduction. Providers and consumers believed that CCBHS could adapt a strengths-based and community-driven approach to recovery planning and wellness promotion. Such a process would involve consumers and family Create a warm and welcoming environment through workforce improvements. Consumers, family members, and providers agreed that overall customer service could be improved. In addition to providing regular customer service training and professional development to program staff, CCBHS should also increase the number of peer mentors/providers to help consumers and family members navigate the large CCBHS system. Increase the number of peer mentors/peer providers. To help alleviate provider burden, CCBHS could increase the number of peer mentor/provider positions and enhance consumer selfadvocacy training so that consumers can access the appropriate mental health services more easily, complete insurance forms, and schedule appointments. Have a person working here to provide 1 on 1 to help you with [system navigation]. West County Homeless Adult Consumer Develop crisis-specific services in West County. A possible solution addressing this need would be for CCBHS to explore a partnership with Kaiser Permanente to provide crisis intervention and treatment in West County. Consumers reported that the Richmond Medical Center would be easier to access in times of crisis. Older Adult System of Care Older adult consumers across Contra Costa County and their mental health providers shared similar experiences interfacing with the County s public mental health system. Consumers and providers agreed that services for older adults have been effective and generally easy to coordinate. However, the
36 Consolidated Report on MHSA Community Engagement Activities Page 36 stakeholders reported a lack of integration between mental health, physical health, and alcohol and other drug services. Socialization programs are engaging and effective in promoting wellness and resiliency. Consumers reported that social activities, such as art classes, field trips to neighboring areas, and eating together, brought peers together and promoted socialization. I really like this program, I have something to do. I get to make friends from other sites, I get to meet people. I enjoy the Spanish class a lot. I have learned quite a bit. West County Older Adult Consumer Timely, expedient service. Sometimes, we can see people in the moment if it s an emergent situation, or in a week, two days, three days from now. That may change as our census grows higher, but we work well with board and cares and residential places. Older Adult Provider Services are available and are individualized. Providers reported that due to the smaller consumer population, they have been able to provide adequate and timely services for older adults. Further, they noted the importance of providing specialized services for older adults as they have different needs from general adult consumers. Linkages between physical and mental health. Older adult providers expressed frustration arranging care for their consumers between CCBHS and their primary care physicians. Providers stated that there was a lack of integration between the service departments. Social supports. While consumers appreciated the socialization programs available for older adults, they felt that additional and varied programming was needed. I do not have anyone right now. I have out lived them all. I have to seek out some support. West County Older Adult Consumer There needs to be a look at also how compliant patients are and how those people are affected by the medication they ve been taking for a long time. Lithium killed my kidneys. And then when I had surgery, my doctor cut off one of my psych meds and it [nearly] killed me I was 5150 ed on all three grounds and I almost got fired from my job. Central County Older Adult Consumer Continuity and care coordination. Older adult providers shared that in addition to feeling like mental health, physical health, and AOD work in silos, they also experienced difficulty arranging care across services for shared consumers. This is a marked difficulty for providers caring for consumers with dementia and other cognitive problems.
37 Consolidated Report on MHSA Community Engagement Activities Page 37 Inclusive treatment approaches. Older adult consumers shared that they do not feel included in developing their case management or direction of services. They expressed that the experience often resulted in them halfheartedly following the providers directions which they did not always agree with. Competent services for older adults with co-occurring disorders. Providers expressed a need for specialized and targeted services for older adults with co-occurring disorders, especially for older adults engaged in both mental health and AOD services. The current residential There are no drug and alcohol services. We can do our best to be competent with people who have dual diagnosis. Our 70- year-old alcoholic doesn t want to go to a place with a 20-yearold meth addict so they just drink themselves to death. Older Adult Provider Roles and responsibilities. Providers shared that is not functional or appropriate for case managers to also act as money managers for older adult consumers. This creates an unequal power dynamic that could harm the providerconsumer relationship. You want the person to cooperate and you also have to participate back so it s reciprocal. So when you have people to come out, you want people to partner with you, so you work as a team. Central County Older Adult Consumer and sober living environments are not age appropriate as they combine young adults and older adults with a one-size-fits-all strategy. It causes a barrier for the case manager and makes the patient hate them because they can t afford $20 or they can t be honest because you re managing their money and you have some much power over them. It s a huge amount of control over their lives. Older Adult Provider Develop stronger linkages between physical and mental health. To initiate collaboration between mental health and physical health service providers, CCBHS, can develop cross-trainings for mental health and physical health staff to better assess and support Quarterly meetings between the mental health and the physical health side and facilitate better communication between the two sides. It feels like everyone is in their own little silo. Older Adult Provider consumers with dementia and mental health problems. Additionally, CCBHS could increase wraparound services and expand home-based supports, especially for consumers living independently in the community. Further, CCBHS could explore ways that mental health and physical health providers could work together to increase support for integrated medication management.
38 Consolidated Report on MHSA Community Engagement Activities Page 38 Continue to offer programs that increase social supports. To address consumers need for additional and varied social supports, and to ensure that there are enough services as the population grows, CCBHS could increase the array of activities that support socialization and physical activity among older adults. Additionally, CCBHS could increase access to therapy and counseling, especially for consumers facing issues of aging and grief. Enhance collaboration with physical health and community providers to increase continuity and care coordination. In a health system as large as Contra Costa County s, it may be difficult for individual providers and CBOs to initiate and sustain collaborative relationships across practices. The County should develop mechanisms that enhance and support enhanced collaboration among service providers. Have them work alongside us and go out and see the reality, rather than a training where they can veg out. Older Adult Provider Develop more inclusive treatment approaches through staff training. To develop and practice more inclusive treatment approaches, CCBHS could increase training support for providers on how to create a partnership with older adult consumers. Additionally, older adult consumers requested education and support on how to partner with providers and work together to identify individual needs and supports. Develop Older Adult specific services for consumers with co-occurring disorders. CCBHS could develop a targeted program for older adult consumers with co-occurring disorders to ensure that the level and appropriateness of services is adequate. This is another strategy to enhance linkages between mental health, physical health, and AOD services. Buy a plot like Rossmoor and have that continuum of services for people. Neighborhood activities, lectures, enrichment, travel, exercise, pools, good nutrition, organic local products, like the CCC Cafes... Older Adult Provider There needs to be education. When we have meetings with AOD services, they tell us that older adults don t use drugs and alcohol. They said, That s odd, I thought people would die if they used drugs when they re 60. Older Adult Provider Define roles and responsibilities for certain staff. CCBHS could consider separating case management and money management responsibilities or explore ways to provide additional checks and balances.
39 Consolidated Report on MHSA Community Engagement Activities Page 39 People Experiencing Homelessness Homeless programs are predominately staffed by peers/people with lived experience. People experiencing homelessness in our focus groups showed appreciation for how well homeless programs integrate peer providers and people with lived experience as staff. Resident counsel to provide opportunities for consumers to shape programs/services. Focus group participants from the Brookside and Concord shelters identified the Resident Counsel as an asset to homeless programs. Through the Resident Counsel, They ve streamlined the appointments, so you can press a number to get to the appointment desk instead of the run around. Being able to leave a message for the psychiatrist and get a call back, you can get ahold of a nurse for medications and set that up if you can t get to the psychiatrist. -Central County Homeless Adult Consumer consumers can provide their input on shelter activities, programs, and services that are offered on site. Healthcare for the Homeless facilitates access to county services. Shelter residents who participated in the focus group events said that the Healthcare for the Homeless Program helps facilitate access to county mental health and health services. Participants liked having nurses, therapists/counselors, and other support medical staff on site to triage their needs and link them with other county programs. Welcoming environment throughout the mental health system. People experiencing homelessness identified the lack of a welcoming environment at the shelters and mental health service provider locations as a significant gap in the mental health system. Participants discussed how staff at various locations do not openly greet consumers or proactively interact with consumers and appear to lack a sincere interest in or support for their recovery. Recovery orientation of mental health services. Focus group attendees emphasized that mental health treatment often consists of crisis and medication management, but lacks sufficient It s harder for us. The one that gets high and [acts] over the top and [then] they re like, I got my housing! You want to know how? Be stupid, be ratchet, be off the hook do all the wrong things and they will help you. That is what gets you out of this place. The people who won t follow the rules [they] need to get out of here and get them the help. Why is that working? That doesn t make sense. -Central County Homeless Adult Consumers
40 Consolidated Report on MHSA Community Engagement Activities Page 40 support for consumers to achieve their recovery goals. In addition to a recovery focus, participants described that mental health services lack a wellness and whole-person approach to care. Continuity and care coordination of mental health services. Similarly to other groups that participated in community engagement activities, people experiencing homelessness described a disjointed experience in navigating different mental health services throughout the system. People experiencing homelessness also described a lack of services that prevents homelessness for those who are at-risk, difficulty accessing benefits in a timely and efficient manner, and a lack of continuity in their case management across housing settings and mental health providers. One of the things as a recovering alcoholic, we re a wet shelter. You can t use in the facility, but they can drink outside and come in blitzed. As a recovering alcoholic it s really hard. Drug and alcohol counselors need to be available all the time. -West County Homeless Adult Consumer Services for co-occurring disorders. The homeless shelters in Contra Costa cater to a wide-range of people experiencing homelessness with complex co-occurring mental health and medical problems. Specifically, people experiencing homeless identified that there is a lack of services that address co-occurring mental health and substance use. Therapists and counselors to support those with co-occurring disorders are infrequently available and their slots fill quickly on days they rotate through the shelters. Co-occurring services was identified as a need for both Adult and TAY populations experiencing homelessness. Access to housing. Overall, people experiencing homelessness identified housing as a need. Participants identified the lack of single occupancy units, sober shelter environment separate from the wet shelter, and TAY shelter beds, as an unmet need in Contra Costa County. Enhance the welcoming environment of the mental health system through staff training. Focus group participants suggested several different types of staff training to encourage a more welcoming environment at mental health service locations. Training suggestions included customer service training, professional development training, and confidentiality training for all mental health staff. I was waiting on my daughter to arrive and I m just standing by them, and they said, Nosy bitch you need to move away. I wasn t doing anything but waiting for my kid. I wanted to write her up. You have to see and know what the problem is before you can correct it. -Central County Homeless Adult Consumer
41 Consolidated Report on MHSA Community Engagement Activities Page 41 They need staff with lived experience that is stable and can be employed How do I tell my case manager that I wanna go out and use and they never used drugs before so they don t even know what I m experiencing right here? -West County Homeless Adult Consumer Enhance the continuity and care coordination of services by forming stronger partnerships with other departments. Similarly to other focus groups, people experiencing homelessness also felt that the mental health system is disjointed. In order to create a more continuous system of care, participants said to increase access to services for those Increase the recovery oriented nature of mental health services through intentional program and staff support. People experiencing homelessness described mental health services as needing to be more whole-person centered, and wellness and recovery focused. In order to accomplish this, incorporate more wellness and recovery supports such as counseling and WRAP in addition to medication management. [There should be] housing specialists to help find you housing, mental health workers, vans to pick people up, washers, meals, showers -West County Homeless Adult Consumer who are at-risk of homelessness, case management, and benefits assistance as early as possible. Increasing the integration and collaboration of multidisciplinary teams and enhancing collaboration with Social Services are essential components to achieving continuity and care coordination. Develop targeted programs for homeless adults and transitional age youth (TAY) that address cooccurring disorders. To address the lack of services that address co-occurring disorders, focus group participants indicated that more therapists and counselors that treat co-occurring disorders should be hired and staffed at homeless shelters and other sites. Additionally, more supportive housing options need to be created for Adult and TAY homeless consumers with co-occurring disorders. You can t take a one size and fit it on everybody and think that everyone will succeed. And then give them a set amount of time before you push them out the door. How do you help someone when you don t address the issue that got them here in the first place? -West County Homeless Adult Consumer Increase access to safe, supportive, and stable housing along the housing continuum (emergency, transitional, and permanent). Focus group participants said that the County should invest more in increasing the number of available beds and single-occupancy units of available housing. Increasing available beds at TAY homeless shelters throughout the County was a particular concern with TAY providers. People in recovery from co-occurring disorders felt that the County needed to develop a sober shelter environment separate from the wet shelter. In addition, focus group participants either experiencing homelessness or who have experienced homelessness in the past feel that the County needs to develop a protocol to determine length of stay in transitional housing on a case-by-case basis that takes into account an individual s progress
42 Consolidated Report on MHSA Community Engagement Activities Page 42 towards their recovery goals. Latino Community Community programs provide social support. Consumers praised the structure of community programs and the social support found through participating in communitybased organizations. Focus group participants felt that providers partnered with them and their families to understand the challenges that they faced every day. Bilingual/bicultural staff capacity. Participants reported a lack of bilingual services that presented many challenges, including restricted access to services, reduced awareness of service options, and inability to participate in wellness and recovery activities due to language barriers. Participants also reported that the lack of staff cultural competency played a large role in how much they engaged in services. They give us information on all the services available in the community and also information about all programs available. And being with other families with the same problems going through the same things and they [providers] want to learn more [about] what distracts us from the problems we have. West County Latino Consumer My doctor told me that the reason told me the reason he was sending me to Familias Unidas was because you don t have Medi-Cal and there are no services in Spanish in the County Clinic. West County Latino Consumer Mental health service awareness. Participants reported knowing of few services that could help them, especially if they did not quality for Medi-Cal. Providers also reported a lack of awareness of outside resources for appropriate referrals. Mental health stigma. Participants felt that there was great stigma and lack of understanding about mental health and available services in the Latino community. Their discussion revealed a lack of understanding about mental health and the varied services provided for mental health. Continuity and care coordination. In addition to needing more bilingual providers and staff to help consumer and family members navigate the system and One of the problems is culturally that Latinos, though most are depressed, but we don t want to accept that because we don t want to be seen by a psychiatrist. Its machismo and we don t want to admit that seeing a psychiatrist would mean that we are locas. West County Latino Consumers
43 Consolidated Report on MHSA Community Engagement Activities Page 43 receive adequate care, consumers reported a need for better follow-up and care coordination. Focus group participants discussed barriers to getting appointments for different mental health services, a lack of follow up care, and supports for family members who care for their loved ones in recovery. There s no psych services or appointments or therapy. Everyone should have access to these services and supports. You can call and they can give you an apt with a psychologist, but it takes a long time, minimum 25 days to a month. East County Latino Family Member Access to mental health services. Participants reported that it was very difficult to find and receive services. Further, family members reported a need for more accessible and more adequate services for family members to provide necessary assistance to their loved ones who have mental health issues. Increase bilingual staff capacity through hiring and recruitment. One of the clear needs expressed by stakeholders was that of having a bilingual child psychologist on staff in addition to increasing the staff s bilingual and bicultural competency. To further support this development, CCBHS may also increase training and support for bilingual/bicultural staff in evidence-based mental health practices. Additionally, CCBHS might consider enhancing access and the use of in-person interpreters and translators. Increase mental health service awareness. CCBHS might increase service awareness among stakeholders by increasing community resource information list in 211 and developing comprehensive guides to mental health resources in the County in public and high-traffic locations, such as the internet and community centers. Address mental health stigma through community outreach and education. Stakeholders cited a large need for outreach and education in the Latino community. CCBHS could conduct greater outreach to these Educate all parents what it means for a student to have special needs not just the parents of that children. Help families identify the differences between misbehavior and special needs. West County Latino Consumers Have flyers and pamphlets that are bilingual in Spanish language so that families know where and how to find services. Because we go to trainings and there is someone interpreting there, but the flyers are given in English. East County Latino Family Member communities and provide education about mental health to those who are linguistically isolated and those who are undocumented. Such information and notification of services could be diffused throughout the Latino community through CBOs targeting the Latino population. Enhance continuity and care coordination through stronger partnerships. To provide smoother transition of services, CCBHS could work on enhancing linkages between mental health, social services, and physical health agencies. Further, CCBHS may consider enhancing linkages between these
44 Consolidated Report on MHSA Community Engagement Activities Page 44 agencies and school districts as Latino families perceive schools as trust sources of information receive a lot of information from schools. Increase access to mental health services. Participants reported that it was very difficult to find and receive services. Further, family members reported a need for more accessible and adequate services for family members to provide necessary assistance to their loved ones who have mental health issues. Place counselors/therapists in the field, at places where residents go on a regular basis this both increases visibility and access to service and potentially serves to reduce stigma in the community. West County Latino Consumer Asian & Pacific Islander (API) and Native American Communities This West Contra Costa County focus group had participants from both the Asian & Pacific Islander (API) and Native American communities present. Focus group participants noted that resources and awareness for domestic violence, mental health stigma, and the bilingual/bicultural capacity of staff as gaps in mental health services for the API and Native American populations. Consumers and providers present at this group suggested the County develop community-wide initiatives to increase awareness and develop resources that address domestic violence, develop a comprehensive campaign that addresses mental health stigma in all communities, and increase the hiring of bilingual/bicultural workers that are representative of the consumers they serve. I can contact my worker, I work with him one day a week, gets me around, helps me get out to meet people or another company, like a family, he listens to me, he takes care of a lot of people, my manager was promoted but they had me with another provider. - API Consumer Personal Service Coordinators (PSCs) are essential to accessing a continuum of mental health services and supports. Focus group participants felt strongly that PSCs were essential to accessing mental health services and a wide variety of other supportive services such as housing, primary care, and wellness activities. Community based organizations (CBOs) that reflect the communities they serve provide a safe space for marginalized and underserved consumers. We heard from focus group participants about the important role CBOs have in immigrant communities, Native Americans, and other underserved groups. Without these organizations, focus group participants said, many consumers would forgo reaching out for help in a crisis event and potentially risk their lives by staying in an unsafe situation.
45 Consolidated Report on MHSA Community Engagement Activities Page 45 Resources and awareness about Domestic Violence (DV). The API and Native American communities were concerned that there is a lack of DV resources in Contra Costa County. Focus group participants even recounted calling the County s DV warm-line and receiving no answer and no follow up from a phone operator. Participants stated that their communities lack DV awareness. I have friends suffering from domestic violence, but no services out of Contra Costa. What to do? No one answered the call, too late. She died. - API Consumer Domestic violence hotline Why give out numbers if no one is going to answer the phones? - API Provider Youth have a real challenge to seek services [for] refugee parents; [they are] not sure how to protect themselves or the teenagers This drives many to gangs for protection. - API Provider Support for newly immigrated parents and youth. API focus group participants were especially concerned about the lack of mental health and social supports for newly immigrated parents and youth in Contra Costa County. Participants stated that youth to join gangs for protection in the absence of other institutions that create community and social cohesion. Mental health stigma. Both the API and Native American focus group participants believed their communities face significant stigma around mental health. They reported that stigma was getting in the way of people talking about mental health and accessing mental health services. EPSDT program, under federal guidelines, pulls student out of classroom [and] this is stigmatizing and it does not help the kid get well. - API Provider Bilingual/bicultural capacity of mental health staff. API focus group participants in particular described a lack of mental health workers that spoke various Asian languages representative of the communities in West Contra Costa County. Both the API and Native American focus group participants described a lack of mental health workers that are reflective of their own cultures. Maybe we can do the outreach that allows us to give information more discretely, we know it has happened, but it is not ok to talk about it\domestic violence- Vietnamese, Taiwanese, Lao, need to be able to talk about. - API Provider Develop community-wide interventions that increase DV awareness and resources. Focus group participants from both API and Native American communities discussed the importance of developing DV awareness through initiatives that address the whole community. Addressing the whole community and identifying leaders within the community that
46 Consolidated Report on MHSA Community Engagement Activities Page 46 can discuss DV related issues is a much safer way of increasing awareness rather than singling out individuals for intervention. In addition to developing community-wide DV awareness initiatives, the County should increase its oversight of the DV warm-line to ensure that the phones are being answered and cases are followed-up on in a timely manner. DV resource materials should be distributed with discretion; focus group participants discussed the danger especially women face if they are found with DV branded materials. Increase support for newly immigrated parents and youths through alternative mental health services. API and Native American focus group participants suggested that more County support is needed to increase access to alternative mental health services. In particular, newly immigrated parents and youth and the Native American community do not trust traditional mental health services and must be engaged in other ways through clubs, social gatherings, or community events to reduce the stigma associated with mental health. API focus group participants suggested that programs need to offer newly immigrated youth a sense of safety and protection as an alternative to joining local gangs. Increasing access to mental health services in non-traditional settings like community centers is imperative to these efforts. There need to be advertisements and posts on Bus shelters, BART, AC transit, public places, bus shelters, with different faces of people where you cannot pick out the person who has a mental health issues. Use people of different ethnic backgrounds, ages, etc. -API Consumer Create a community-wide campaign that addresses mental health stigma. Both API and Native American focus group participants discussed the need to decrease stigma and increase awareness about mental health. One focus group participant suggested that the County develop an advertisement campaign with posters on bus stops, grocery stores, community centers, provider sites, and elsewhere that depict people in recovery from all ages and cultural backgrounds. This ensures people know mental health can affect anyone in the community and decreases feelings of isolation from those afraid to seek help for their mental health. Service providers have to open their doors for young people to help de-stigmatize mental health. -Native American Provider Increase the number of bilingual and bicultural mental health workers. Although County mental health services offer the language line and video conference calling for consumers who need it, focus group participants said it is difficult for people from the API and Native American communities to trust someone through a machine. Face-to-face interaction with a provider is essential and the County should prioritize the hiring of bilingual and bicultural workers to meet the needs of culturally diverse consumers.
47 Consolidated Report on MHSA Community Engagement Activities Page 47 Lesbian, Gay, Bisexual, Transgender, and Queer (LGBTQ) Community Stakeholders requested a focus group event that target Lesbian, Gay, Bisexual, Transgender, and Queer (LGBTQ) consumers from across Contra Costa County. Consumers reported that there is a lack of transcapable services, institutionalized LGBTQ stigma, and a need for additional family supports. LGBTQ participants suggested that through additional staff training, increasing LGBTQ competent providers, and developing more family-inclusive approaches to mental health services can help close the mental health gaps. Providers create a safe space for LGBTQ consumers. Focus group participants felt that LGBTQ providers create a safe space for them to be themselves, explore their gender, and meet other queer people. Trans-capable services. Providers and consumers of mental health and LGBTQ services identified a need for more services that are capable of serving people who are transgender. Specifically, participants note how people who are transgender face deeper stigma due to providers lack of understanding about the fluidity of gender identity and the distinction between sexuality and gender, in general. How can MHSA address the pathology of the system and its fears of the LGBTQ community? We need to switch the attitude from viewing the gender identity as the problem to systematic solutions. -LGBTQ Provider for rejection when coming out and compromises the potential safety of the consumer. Mental health and LGBTQ stigma within non LGBTQspecific services. Although there are providers that target the LGBTQ population, outside of those specific programs, LGBTQ stigma is still pervasive across the County. There is a lack of education and awareness among mental health and I enjoy coming because you get to express a different side of you - gender identity, gender expression, sexuality. I can express to a side of me that you couldn t express to the outside world. -LGBTQ Consumer Cultural competency for the LGBTQ experience. Focus group participants identified that the lack of cultural competency/humility/compassion within the mental health system prevents providers and mental health staff from understanding the LGBTQ experience. Family inclusiveness and supports. Providers and consumers discussed how there are not enough resources for parents to engage with services and supports alongside their LGBTQ children. This lack of support increases the risk As soon as the crisis becomes specific to a person who is LGBTQ, [the consumer] is sent to Rainbow even though Rainbow services do not fit the full needs that were assessed for the individual. -LGBTQ Provider
48 Consolidated Report on MHSA Community Engagement Activities Page 48 non-mental health staff about LGBTQ issues and mental health resources for people who are LGTBQ. Mental health workforce training for non-mental health staff. Providers said that they do provide training to mental health staff on LGBTQ competence, but there is a lack of resources to expand those trainings into parts of the county where it is needed the most. Increase the number of providers who can provide trans-capable services. Participants suggested that the County conduct focused outreach to identify and retain service providers that are capable of serving the transgender community to be part of the mental health system. There needs to be better language used on applications and paperwork for mental health services that is more inclusive. Staff need to know how to use language that is respectful. -LGBTQ Consumer LGBTQ inclusive. Increase the LGBTQ cultural competency of mental health staff through training. Participants from the LGBTQ community and LGBTQ providers noted that mental health staff and providers should receive more training on LGBTQ cultural competency. LGBTQ cultural competency training should include increasing the awareness of providers about the experience of people who are LGBTQ in the community. In addition, focus group participants strongly emphasized the need to make all mental health forms Increase supports for family of people who are LGBTQ. Providers spoke to the potential harms especially youth face when coming out to their family and suggest that the County develop programs that are more family inclusive. Family-inclusive LGBTQ programs could address rejection reduction and provide a safe place for LGBTQ youth. Focus group participants also said that CCBHS should provide more counseling services available for consumers and their families and loved ones. Address LGBTQ stigma through cross training and developing LGBTQ competent core mental health services. Providers and consumers noted that more training to reduce LGBTQ stigma is needed for providers of core mental health services, crisis services, and outpatient services. Education needs to be provided to staff on proper protocols for appropriately triaging mental health care for LGBTQ consumers in crisis. Cross-training providers and core mental health staff to increase the capacity and knowledge around mental health services and LGBTQ competency is another form of training the county could facilitate. [The County needs] advocacy training for people who have lived experience. They need to develop a program that trains peers to be advocates within the mental health workforce. -LGBTQ Consumer Increase training for non-mental health staff. In addition to reducing stigma and increasing competency within core mental health services, focus group participants suggested that there needs to be more training within the community across Contra Costa County to help increase awareness about LGBTQ issues. Focus group participants said to increase peer-led outreach and education to schools,
49 Consolidated Report on MHSA Community Engagement Activities Page 49 incorporate a LGBTQ component to Mental Health First Aid and Youth Mental Health First Aid, and to enhance the connection between CCBHS and Gay-Straight Alliance organizations. Within the schools, the County should help facilitate a stronger partnership with school faculty and staff to reduce bullying and to consider a youth-led speakers bureau. Family Members and Loved Ones of Consumers We conducted an additional focus group for family members and loved ones of mental health consumers that included significant participation from the National Alliance on Mental Illness (NAMI) Contra Costa County. Family members and loved ones of consumers felt that the mental health system lacked the continuity and comprehensiveness of crisis services as well as a warm and welcoming environment to both consumers and family members. In order to address those gaps, focus group participants suggested that the County increase crisis services, especially post crisis services such as intensive follow-up care and the implementation of AB1421 (also known as Laura s Law), and find opportunities to increase the meaningful involvement of consumers and family members throughout the mental health system. National Alliance on Mental Illness (NAMI) serves as a strong network of support for parents and families of mental health services consumers. Participants in the Family Member and Loved Ones focus group expressed the importance of NAMI in providing a space where family members and loved ones can provide mutual aid and exchange resources and knowledge about the mental health system. NAMI also provides trainings that help family members and loved ones learn how to effectively advocate for themselves and their loved ones in mental health treatment. NAMI also supports family members and loved ones to conduct trainings across the County and the Bay Area on a variety of topics. Comprehensiveness and continuity of crisis services. Family members and loved ones of consumers in mental health services described the continuum of crisis services to be a weakness in the mental health system. Post crisis services were of a particular concern of this group. Focus group participants described follow-up from the hospital as a critical point where consumers fall through the cracks and lack the resources to achieve a fuller recovery from a crisis episode. Family members also noted that consumers accept treatment in the hospital but are likely to lose their commitment to participate in treatment or take prescribed medication upon release. Just last year, around this time, I went through a crisis with my son. I was almost successful in getting him into Contra Costa Regional Center. We waited seven days for transport. The second he said, I do not think I m going to kill myself, he was released. There was no phone call. -Family member
50 Consolidated Report on MHSA Community Engagement Activities Page 50 The psychiatrist changed his [appointment] date and I asked why did you not notify me? Well, we only have this one number and it didn t work. And the demeanor was not welcoming, very dismissive. -Family member Family members and loved ones as part of the treatment team. Focus group participants said that more can be done to help mental health providers consider family members and loved ones as part of the treatment team for consumers. Particularly, family members and loved ones felt that psychiatrists and psychologists did not regard them as a source of valuable information or as a critical part of the consumer s support system. Warm and welcoming environment throughout the mental health system. Similarly to other focus group findings, family members and loved ones of consumers found that the mental health system lacked a warm and welcoming environment for both them and consumers of mental health services. Increase the comprehensiveness and the continuity of crisis services for adult consumers. Family members and loved ones of consumers suggested several strategies to strengthen the comprehensiveness and continuity of crisis services. We have summarized suggestions for improvement in the bullets below: Increase Crisis Intervention Team (CIT) training with local law enforcement: NAMI representatives said the County should increase their capacity to support CIT training with Contra Costa County law enforcement. Develop a peer supported crisis intervention team that responds to mental health calls alongside law enforcement: Focus group participants requested that the County develop a peer supported crisis intervention team that would act as the first responder to mental health crisis calls in partnership with law enforcement. Enhance post-crisis follow-up care for consumers: Family members and loved ones of consumers expressed that the period following a crisis event is the We need triage and team.. [with] a Psychiatric Nurse along with EMS people that would go to answer the If we have these other units that can go in, this would not create the trauma that police officers would create. San Francisco has this triage/ crisis intervention team. -Family member most critical to ensuring their safety and health. Focus group participants suggested that the County develop the capacity and personnel to provide intensive follow-up care for consumers in the period immediately following a crisis. Post-crisis follow-up care includes linking consumers to treatment, checking in with the consumers about their recovery after a crisis incident, and to coordinate the transition back into the community from a hospital setting.
51 Consolidated Report on MHSA Community Engagement Activities Page 51 Laura s Law- It is paramount that we get help for those who are not getting help at this time. Our families struggle with this. AOT, Laura s Law, needs to get implemented. Here we are and we have the board of supervisors saying we don t have the money. It s not up to us to get the money. The needs are there. -Family members Implement AB1421 (also known as Laura s Law ): Family members, loved ones, and representatives of NAMI support the implementation of AB1421 in Contra Costa County as part of enhancing the comprehensiveness and continuity of crisis services, specifically for those who are less likely to engage in voluntary services. Focus group participants expressed that AB1421 implementation would create a safety net for consumers that need more intensive core mental health services, such as Assisted Outpatient Treatment (AOT), to prevent unnecessary hospitalization, incarceration, and potential death. Redefine family of consumers to include loved ones or others close to the consumer; incorporate family members and loved ones as part of the treatment team. Focus group participants said the County should redefine the meaning of family to be more inclusive of those people close to a consumer and in their immediate circle of social supports. In addition to redefining family, focus group participants suggested that the County should consider family members and loved ones as part of the consumer defined treatment team. Increase the meaningful involvement consumers and family members in the mental health system. Family members and loved ones of consumers requested that the County develop more opportunities for themselves and consumers to participate meaningfully in the mental health system. Focus group participants suggested that the County increase opportunities for consumer and family member employment, vocational training, and peer/family member led services throughout the mental health system. Define family families are those people who care about loved ones. There are many non-traditional families. These are the people who do a lot of work for the county, taking care of our citizens. It would behoove the county to make use of family members, save them money and aggravation and help everybody. -Family member
52 Consolidated Report on MHSA Community Engagement Activities Page 52 Page intentionally left blank.
53 Consolidated Report on MHSA Community Engagement Activities Page 53 Appendices
54 Consolidated Report on MHSA Community Engagement Activities Page 54 Appendix A: Focus Group Facilitator s Protocol Focus Group Background (5 ) Facilitator s Guide (talking points) Contra Costa Mental Health (CCMH) is in the process of developing its three-year program and expenditure plan for mental health services in accordance with Prop 63, the Mental Health Services Act (MHSA). An essential part of this effort is the inclusion of community members in the planning process. As such, CCMH has contracted Resource Development Associates (RDA) to help gather information from community members such as yourselves. We will be conducting a series of focus groups in which we will: 1. Review findings from 2013 CCMH Preliminary Assessment of Need (30 ) 2. Affirm findings and discuss any other strengths and needs (10 ) 3. Prioritize areas of need (5 ) 4. Brainstorm ideas for meeting these needs (35 ) 5. Closing remarks/next steps (5 ) Information gathered from these focus groups in addition to the assessment of needs will provide us with a comprehensive look of the strengths and needs of the community. This will help Contra Costa Health Services develop its Mental Health Services Act (MHSA) Plan for Guidelines Designed to be a safe place to talk about issues you might not otherwise feel comfortable talking about Participants names will not be linked to any comments unless we specifically ask if we can use your comment as a quote. Silence your cell phones turn off the ringer and any alarms There are no wrong or right opinions, please share your thoughts honestly Limit side conversations so everyone can hear what is being said Stand up; stand down Listen before responding Are there any other guidelines that you would like to add? Introductions Before we begin reviewing the assessment of needs findings, let s get to know each other a little bit. As you are comfortable, please share: Your name
55 Consolidated Report on MHSA Community Engagement Activities Page 55 If you are a community member, county staff or representing a community based organization. What you hope will come of today s focus group Project Background (2 ) About CCMH (refer to infographic handout) Contra Costa County has over 1 million residents o Estimated 60,000 residents have serious mental (adults) or serious emotional disturbance (children) CCMH serves about 20,000 individuals annually o Individuals served are typically poor and struggle with housing, employment, transportation, and medical and behavioral health care CCMH is integrated with Alcohol and Other Drug and Homeless Programs under Behavioral Health CCMH works with primary care, education, social services, juvenile and criminal justice, and community-based organizations CCMH services include: o Crisis intervention o Outreach and engagement o Therapy o Medication and case management o Day programs o Housing and employment supports About MHSA 63 passed November 2, 2004 o 1% tax on income over $1 million o To EXPAND and TRANSFORM mental health services in California Core Values o Wellness, Recovery, and Resiliency o Cultural Competence o Client/Family-Driven Mental Health System o Integrated Service Experience o Community Collaboration (why we re here today) Contra Costa s three-year plan should encompass these values Current CCMH programs fall under the following MHSA components: o Community Supports and Services o Prevention and Early Intervention o Workforce, Education, and Training o Capitals, Facilities, and Technology Needs o Innovative Projects
56 Consolidated Report on MHSA Community Engagement Activities Page CCMH Assessment of Needs (28 ) Procedures (refer to infographic handout) MHSA requires analysis of community mental health needs as part of the three-year program and expenditure plan Assessment of needs began in September 2013 with a stratified sampling of people who are currently providing mental health services, and those who are currently receiving services: o Across 25 sites, all 3 county regions o Across 4 age groups, 2 languages o Input from over 200 service providers, consumers, and family members Results from the surveys and focus groups focused on four main areas of mental health service: access to services, workforce capacity, service capacity, and integration of services. System-Wide Findings This area of needs involves practices and procedures that are used throughout the CCMH system, including consumers and family members ability to access mental health services that are currently provided. The CCMH system has enabled some programs to successfully provide the following services: Proactive engagement of clients and community members Warm & welcoming environment Transportation provided or coordinated Culturally & linguistically competent services Services are located where people live Some systematic difficulties of consumers being able to access these services include: Lack of outreach to at-risk youth, new immigrants, and LGBTQ populations Eligibility rules Need for more bilingual/bicultural workers Further, not all programs are providing all of these services, or they are not providing them at an adequate level. As a result, there are: Inefficient or lack of public transportation Facilities are in need of improvements Need to enhance the continuity of care between different systems of care (e.g. TAY to adult) or departments More opportunities for meaningful daily activities that promote wellness and recovery
57 Check-In Questions: Contra Costa Behavioral Health Services Consolidated Report on MHSA Community Engagement Activities Page 57 Does this reflect your experience? Is there anything missing that should be added to this finding? Do you disagree with any of these findings? CCMH Workforce Findings This area of need involves the gaps in providers ability to delivery adequate services. In some programs CCMH uses a multi-disciplinary team approach which provides consumers and family members with: Team-based care approach Coordination of care Utilizing family/peer partners or navigators However, further growth is needed in the CCMH workforce. CCMH found the following specific workforce needs: More employment and career counseling for consumers/family members More opportunities for meaningful daily activities that promote wellness and recovery Shortage of case managers and psychiatrists Lack of admin/support staff Better trauma-informed mental health service system to support staff and address vicarious trauma Check-In Questions: Does this reflect your experience? Is there anything missing that should be added to this finding? Do you disagree with any of these findings? Findings about Current MHSA Programs This section reviews the current MHSA programs in Contra Costa County and looks at the accomplishments programs have made in the provision of services, reviews areas that programs could improve, and identifies services gaps not covered by the existing programs.
58 Consolidated Report on MHSA Community Engagement Activities Page 58 Overall- programs are working to address the needs of the community. Services that were noted to have a successful impact are: Provision of integrated health and behavioral health services Coordination of care between mental health, law enforcement, education, social services, and other community or faith-based providers Care that results in a successful outcome for the consumer However, areas in which programs could improve include: Provide better medication management services for clients Determine and match the appropriate level of care based on mental health needs Connect consumers to more affordable housing Develop better continuity in services for before, during, and after a mental health crisis Conduct more thorough evaluation and performance measurement of program outcomes Better integration of peer-led services with clinic services CCMH identified the following needs that still exist and have not been met by the current services: Services for adults at all stages of recovery, not just for those who have a serious mental illness First break program for young adults Inpatient beds for children Club house in West and East County Drug treatment for youth Flex-funds to address basic living emergencies Check-In Questions: Does this reflect your experience? Is there anything missing that should be added to this finding? Do you disagree with any of these findings? Focus Group Questions (10 ) 1. Are there any other areas of strengths that we have not reviewed? 2. Are there any other areas of need or barriers to receiving services that we have not reviewed? Prioritization Activity (5 ) Thank you for reviewing the findings and providing your input about them. Now that we ve discussed each of these areas of need, let s talk about which areas have the most need. We ve re-categorized the discussed needs into small buckets of needs. At this point, we ve already reviewed and made edits to
59 Consolidated Report on MHSA Community Engagement Activities Page 59 these findings. We are now moving into talking about how CCMH can overcome these barriers and meet these needs. In front of you, there are three colored flags. As I read through each area of need, ask yourself, Is this area of need a high-priority concern for the CCMH consumers, their family members, and the service providers? If you think that the area of need is a top priority, raise the red flag. If you think that the area of need is important, but perhaps not the number one priority, raise the blue flag. If you think that the area of need is unimportant, or something that can be addressed at a later date, raise the white flag. Please remember that the focus group is designed to be a safe place to share your opinion, however, if you so wish, you may abstain from voting. Once the flags are counted and tallied across the buckets of needs, we ll narrow the topics of discussion to the top 3-5 buckets and think of ways we can overcome the needs. Brainstorming Solutions (35 ) Here are the top five buckets of needs you ve identified [list them]. Do you agree that there are areas of generally high priority? Are you ready to move forward in discussing how we may overcome these barriers? Great, let s briefly talk about each of these in order and think through what needs to take place for these issues to be resolved. If time allows, we ll move on the remaining areas of need. 1. Refer to the current programs handout, are there ways we can modify any of these existing programs to meet this need? a. If so, what does that change look like? b. What are the necessary resources to accomplish the change? 2. If not, is there an existing program that we can add to or enhance to meet this need? a. If so, what would that addition look like?/how would it function? b. What are the necessary resources to implement the new component? 3. If none of the existing programs can possibly accommodate the need, does CCMH need to create a new program to meet the demand? a. If so, who would the program serve? b. How would the program operate? c. How could CCMH ensure the success of the program? d. What resources could CCMH leverage to implement a program like this?
60 Consolidated Report on MHSA Community Engagement Activities Page 60 In the event of additional time, briefly review the other areas of need and ask the group to sketch some ideas for addressing or removing those barriers. Thank you for your time and participation today. Your contributions are essential to this project as you are essentially building this plan for yourselves. is here from the Office of Consumer Empowerment (OCE) to help you complete a survey on mental health services and integration in the county. Please stay to complete the survey. If you have further questions or ideas, please don t hesitate to contact Roberta Chambers at rchambers@resourcedevelopment.net or at x 102.
61 Consolidated Report on MHSA Community Engagement Activities Page 61 Appendix B: Informational Flyer for Focus Group Events Contra Costa County Behavioral Health Services invites you to the: MHSA Three-Year Program and Expenditure Plan Community Planning Process Provider Focus Group Objectives: Contra Costa County is developing its MHSA Three-Year Program & Expenditure Plan for We are inviting you to participate in a focus group about mental health services in Contra Costa County. We want to hear about your priorities for mental health services and your ideas about how to improve mental health services in the county. Your input will be incorporated with other stakeholder feedback to produce the new MHSA Three-Year Program & Expenditure Plan for Please join us! We will be serving light snacks and refreshments! Ensure that your voice is heard in the Community Planning Process for Contra Costa County s MHSA programs!

62 Consolidated Report on MHSA Community Engagement Activities Page 62 Appendix C: Logistical Flyer for Focus Group Events Contra Costa County Behavioral Health Services invites you to the: MHSA Three-Year Program and Expenditure Plan Community Planning Process Date: Time: Location: Provider Focus Group Meeting Objectives: Introduce RDA and MHSA Review Preliminary Needs Assessment findings Collect stakeholder feedback on ideas to bridge current gaps in the County s mental health system Prioritize stakeholders ideas to continue the transformation of the County s mental health system Please join us! We will be serving light snacks and refreshments! Ensure that your voice is heard in the Community Planning Process for Contra Costa County s MHSA programs!
63 Consolidated Report on MHSA Community Engagement Activities Page 63 Appendix D: Contra Costa Mental Health Assessment of Needs Handout 2013 Contra Costa County Mental Health (CCMH) Assessment of Needs This area of needs involves practices and procedures that are used throughout the CCMH system, including the strengths and challenges consumers and family members ability to access mental health services that are currently provided. The CCMH system has enabled some programs to successfully provide the following services: Proactive engagement of clients and community members Warm & welcoming environment Transportation provided or coordinated Culturally & linguistically competent services Services are located where people live Some systematic difficulties of consumers being able to access these services include: Lack of outreach to at-risk youth, new immigrants, and LGBTQ populations Eligibility rules Need for more bilingual/bicultural workers Further, not all programs are providing all of these services, or they are not providing them at an adequate level. As a result, there are: Inefficient or lack of public transportation Facilities are in need of improvements Need to enhance the continuity of care between different systems of care (e.g. TAY to adult) or departments More opportunities for meaningful daily activities that promote wellness and recovery
64 Consolidated Report on MHSA Community Engagement Activities Page 64 This area of need involves the strengths and challenges in providers ability to delivery adequate services. In some programs CCMH uses a multi-disciplinary team approach which provides consumers and family members with: Team-based care approach Coordination of care Utilizing family/peer partners or navigators However, further growth is needed in the CCMH workforce. CCMH found the following specific workforce needs: More employment and career counseling for consumers/family members More opportunities for meaningful daily activities that promote wellness and recovery Shortage of case managers and psychiatrists Lack of administrative/support staff Better trauma-informed mental health service system to support staff and address vicarious trauma
65 Consolidated Report on MHSA Community Engagement Activities Page 65 This section reviews the current MHSA programs in Contra Costa County and looks at the accomplishments programs have made in the provision of services, reviews areas where programs could improve, and identifies services gaps not covered by the existing programs. Overall, programs are working to address the needs of the community. Services that were noted to have a successful impact are: Provision of integrated health and behavioral health services Coordination of care between mental health, law enforcement, education, social services, and other community or faith-based providers Care that results in a successful outcome for the consumer However, areas in which programs could improve include: Provide better medication management services for clients Determine and match the appropriate level of care based on mental health needs Connect consumers to more affordable housing Develop better continuity in services for before, during, and after a mental health crisis Conduct more thorough evaluation and performance measurement of program outcomes Better integration of peer-led services with clinic services CCMH identified the following needs that still exist and have not been met by the current services: Services for adults at all stages of recovery, not just for those who have a serious mental illness First break program for young adults Inpatient beds for children Club house in West and East County Drug treatment for youth Flex-funds to address basic living emergencies
66 Consolidated Report on MHSA Community Engagement Activities Page 66 Appendix E: Contra Costa Mental Health Service Providers Handout Mental Health Services Act (MHSA) Providers by Component Provider Counseling Options Parent Education (COPE) Juvenile Assessment and Consulting Services # Unduplicated Programs Clients Served FY Countywide services for families 575 Supporting Families in the Juveniles Justice System First Hope Early Identification/Intervention in 106* Psychosis Office of Consumer Empowerment Stigma Reduction Not reported *Total # unduplicated clients served from January 1, 2013 through December 31, Provider Programs # Unduplicated Clients Served FY Contra Costa Crisis Center Suicide Prevention 30,582 La Clínica de La Raza 1. Vias de Salud (Pathways to Health), also serves east county 2. Familias Fuertes (Strong Families) 1. 4, ,062 Jewish Family and Children s Community Bridges 475 Services Putnam Clubhouse (aka Contra Supporting Families Experiencing Mental 278 Costa Clubhouse) Illness Contra Costa Interfaith Housing Strengthening Vulnerable Families 238 Child Abuse Prevention Council The Nurturing Parent Program 126 Martinez Unified School District New Leaf Youth Development 51 Provider Programs # Unduplicated Clients Served FY People Who Care Youth services 205 Center for Human Development African American Health Conductors 248
67 Consolidated Report on MHSA Community Engagement Activities Page 67 Provider Programs # Unduplicated Clients Served FY STAND! For Families Free of Violence 1,334 YMCA Building Blocks for Kids 1,015 RYSE Trauma Response & Resilience System 260 Health & Wellness James Morehouse Project at El Cerrito 355 YMCA of the East Bay High School (fiscally sponsored by Youth Development) The Latina Center Primo Nuestros Ninos (Our Children First) 305 Native American Health Center Native American Wellness Center 171 Lifelong Medical Care SNAP! Senior Network and Activity Program 147 Provider Programs # Unduplicated Clients Served FY Rainbow Community Center LGBT Community Mobilization & Social 829 Support Project Older Adult Senior Peer Counseling 237 Asian Community Mental Health Services, Inc. Asian Family Resource Center 67
68 Consolidated Report on MHSA Community Engagement Activities Page 68 Provider Programs # Unduplicated Clients Served FY Rainbow Community Center Counseling/Case Management Services New for Target: 125 Older Adult Mental Health Programs Seneca Family of Agencies 1. Intensive Care Management Teams (ICMT) 2. Improving Mood Providing Access to Collaborative Treatment (IMPACT) Short Term Assessment of Resources and Treatment (START) SHELTER, Inc. MHSA Housing Target: 109 Recovery Innovations Wellness and Recovery Centers New for Target: 200 Community Options for Families and Multisystemic Therapy New for Youth (COFY) County-Wide Assessment Team County-Wide Assessment Team New for Lincoln Child Care Center Multi-Disciplinary Family Therapy New for Telecare Corporation Crisis Residential Facility: Hope House New for Provider Central County Adult Mental Health Clinic (includes PEI and INN services) Central County Children s Mental Health Clinic Anka Behavioral Health, Inc. Programs Suicide Prevention Pilot Women Embracing Life and Learning (WELL) Libby Madelyn Collins Trauma Recovery Project Direct Providers for Treatment and Case Management Peer Support Improving Service Delivery Parent Partners Vehicles Evidence Based Practice Clinical Specialist 1. Bridges to Home (BTH), also served west county 2. Behavioral Health Court # Unduplicated Clients Served FY , ** Crestwood Behavioral Health, Inc. Not specified Not reported **Bridges to Home (BTH) served a total of 185 individuals across multiple providers 810
69 Consolidated Report on MHSA Community Engagement Activities Page 69 Provider East County Adult Mental Health Clinic East County Children s Mental Health Clinic Portia Bell Hume Behavioral Health and Training Center Youth Homes, Inc. Programs Direct Providers for Treatment and Case Management Peer Support Improving Service Delivery Parent Partners Vehicles Evidence Based Practice Clinical Specialist # Unduplicated Clients Served FY ,960 Adult Full Service Partnership New for Target: 60 Transition Age Youth Full Service New for Partnership Target: Provider West County Adult Mental Health Clinic West County Children s Mental Health Clinic Programs Bridges to Home Contra Costa Transition Age Youth Direct Providers for Treatment and Case Management Peer Support Improving Service Delivery Parent Partners Vehicles Evidence Based Practice Clinical Specialist # Unduplicated Clients Served FY ,720 1,482 Desarrollo Familiar, Inc. Familias Unidas 37 Community Mental Health for Asians Bridges to Home (BTH) 185** Also served central county Rubicon Programs Bridges to Home (BTH) 185** Also served central county Fred Finch Also served central county Contra Costa Transition Age Youth Program 90 **Bridges to Home (BTH) served a total of 185 individuals across multiple providers
70 Consolidated Report on MHSA Community Engagement Activities Page 70 Provider Community Violence Solutions Served countywide Rainbow Community Center Served central county Programs/Services # Unduplicated Clients Served Reluctant to Rescue 62 Creating a Safe Haven to Support Transgender and LGBTQQI2-S Youth Involved in Sexual Exploitation 12 in person Web visit # not available Other mental health service providers in Contra Costa County included: Provider Programs/Services # Unduplicated Clients Served Mental Health Consumer Concerns Adult services 200 Served countywide Contract ended 12/13/13 Lao Family Community Development Served west county Family services 126
71 Consolidated Report on MHSA Community Engagement Activities Page 71 Appendix F: MHSA Values and Components Handout Mental Health Services Act (MHSA) Values Wellness, Recovery, and Resilience This value promotes services and systems that support consumers and family members in their efforts to overcome mental health illness and to live productive and fulfilling lives. The MHSA works towards strengthening and transforming mental health services and systems to reduce disparities in access, utilization, and outcomes by age, race/ethnicity, gender, sexual orientation, language, disability, economic status, and other affiliations. Cultural Competence This value promotes mental health services that reflect the values, customs, and beliefs of the population served by ensuring consumers and family members are involved in the development of treatment plans that consider their strengths, goals, cultural background, and social beliefs. Client and Family Driven Services This value promotes participation of consumers and family members at all phases of the design, planning, implementation, and evaluation of mental health services. Integrated Services This value promotes coordination among different service systems to provide a seamless experience for consumers and family members in accessing services and supports in mental health, substance use, and primary care. Community Collaborations This value promotes partnerships and collaborations among service delivery systems and communitybased organizations to support an infrastructure for seamless and competent service delivery.
72 Consolidated Report on MHSA Community Engagement Activities Page 72 Mental Health Services Act (MHSA) Components Community Services and Supports (CSS) The majority of Prop 63 money provides treatment for individuals with serious mental illness, using a whatever it takes approach. The CSS component establishes Full Service Partnerships to provide wraparound services to clients/consumers. The CSS component also addresses housing by leveraging the funds in local partnerships to build and renovate housing units for people with serious mental illness, many of whom are homeless. Prevention and Early Intervention (PEI) The goal of Prevention & Early Intervention programs is to prevent mental illness from becoming severe and disabling and to improve timely access to services for people who are underserved by the mental health system. Innovation (INN) Five percent of all MHSA funds support Innovation projects to test novel, creative and/or ingenious mental health practices/approaches that show promise in improving services to mental health service delivery with time-limited pilot programs. Workforce Education and Training (WET) The goal of the Workforce Education and Training (WET) component is to develop a diverse workforce. WET funds may be used to increase the number of qualified individuals to provide mental health services consistent with the MHSA values, and to improve the cultural and language competency of the mental health workforce. Capital Facilities and Technological Needs (CFTN) The Capital Facilities and Technological Needs (CFTN) component works towards the creation of a facility or facilities that is used for the delivery of MHSA services to mental health clients and their families or for administrative offices. Funds may also be used to support an increase in peer-support and consumerrun facilities, development of community-based settings, and the development of a technological infrastructure for the mental health system to facilitate the highest quality and cost-effective services and supports for clients and their families.
 54 29% Latino & African American 26")
73 Consolidated Report on MHSA Community Engagement Activities Page 73 Appendix G: Focus Group Participation Summary Handout MHSA Community Engagement Events: Demographics of Community Engagement Participants Total Count of Participating Consumers and Family Members by Population Focus Group Type Count of Participants % of Total Transitional Age Youth (TAY) 54 29% Latino & African American 26 14% Adult 23 12% LGBTQ 18 10% Older Adult 18 10% People Experiencing Homeless 17 9% General Consumers and Family Members 14 7% Latino Community 12 6% Children & Parents 4 2% Asian & Pacific Islander Community (API) Consumer 3 2% Total % Total Count of Participating Service Providers by System of Care Count of % of Focus Group Type Participants Total TAY Provider 11 31% Adult Provider 6 17% Children Provider 9 26% Older Adult Provider 9 26% Total % Number of Partcipants Count of Focus Group Participants by selfidentified stakeholder group (n=235) Consumer Service Provider 55 Family Member 16 Consumer and Family Member Stakeholder Affiliation of Focus Group Participants Stakeholder Affiliation Count of Participants % of Total Community-based organization 65 39% County government agency 25 15% Education agency 17 10% Provider of mental health services 14 8% Medical or health care organization 6 4% Social service agency 6 4% Law Enforcement agency 1 1% Provider of alcohol and drug services 1 1% Other 32 19% Total %
 Under 16 4% 25-29 1% Percent of Focus Group")
")


74 Consolidated Report on MHSA Community Engagement Activities Page 74 Percent of Focus Group Participants by Age (n=220) Under 16 4% % Percent of Focus Group Participants by Gender (n=222) Transgender / Genderfluid 3% % 60 and older 22% % Male 37% Female 60% Count of Focus Group Participants by Race/Ethnicity (n=220) Other 2 American Indian/Native Alaskan 4 Multi-Race 14 Asian or Pacific Islander 22 African American/Black 39 Hispanic/Latino 59 White/Caucasian Number of Participants Count of Focus Group Participants by County Region (n=223) County Region Count of % of Participants Total West 54 24% Central 90 40% East 57 26% Other 22 10% Total %
75 Consolidated Report on MHSA Community Engagement Activities Page 75 Appendix H: Participant Demographic Form Contra Costa MHSA Community Engagement Participant Information 1. Do you identify yourself as a consumer or a family member of a consumer of mental health services? No Consumer Family Member 2. Do you identify as a service provider? No Yes 3. What is your stakeholder affiliation? County government agency Community-based organization Law Enforcement Education agency Social service agency Veterans or Veterans Organizations Provider of mental health services Provider of alcohol and other drug services Medical or health care organization Other: 4. Please indicate your age range: Under and older 5. Please indicate your gender: Female Male Transmale/transman Transfemale/transwoman Intersex Genderqueer Prefer not to answer Other: 6. What is your race/ethnicity? (check all that apply) White/Caucasian African American/Black Hispanic /Latino Asian or Pacific Islander American Indian/Native Alaskan Multi-Race Other: 7. In which part of Contra Costa do you live? Antioch Brentwood Clayton Concord Danville El Cerrito Hercules Lafayette Martinez Moraga Oakley Orinda Pinole Pittsburg Pleasant Hill Richmond San Pablo San Ramon Walnut Creek Other:

76 Consolidated Report on MHSA Community Engagement Activities Page 76 Appendix I: Community Forum Presentation
77 Consolidated Report on MHSA Community Engagement Activities Page 77
78 Consolidated Report on MHSA Community Engagement Activities Page 78


79 Consolidated Report on MHSA Community Engagement Activities Page 79
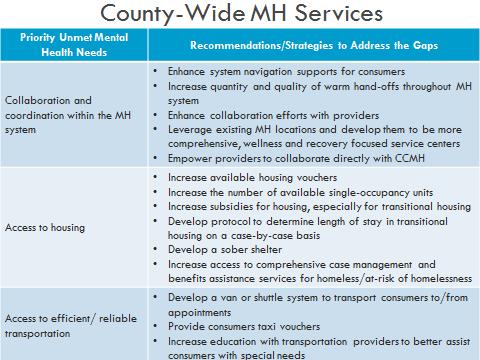
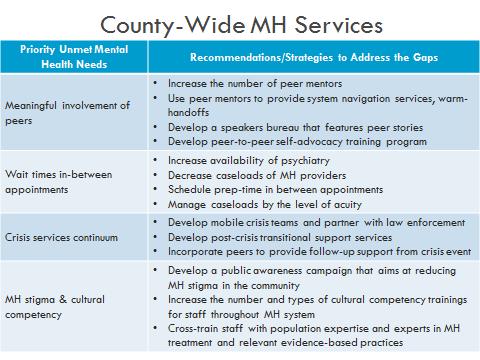
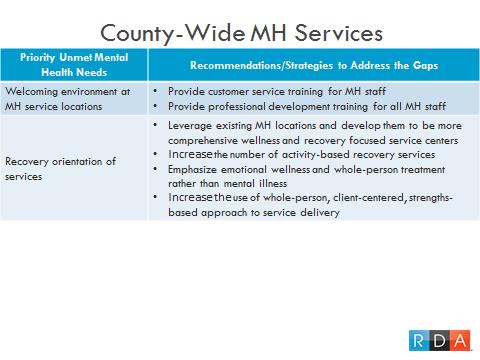
80 Consolidated Report on MHSA Community Engagement Activities Page 80
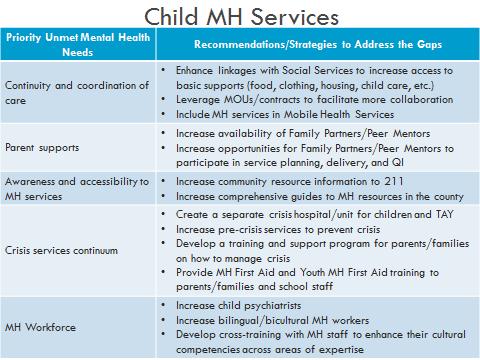
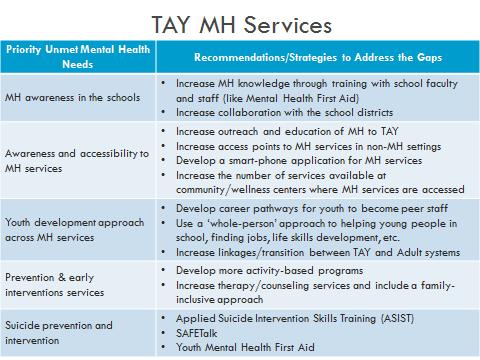
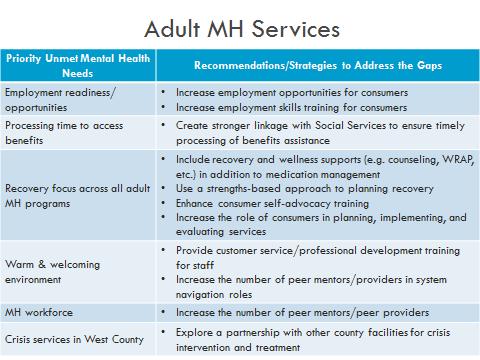
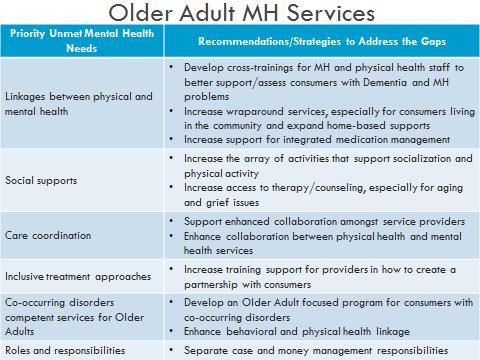

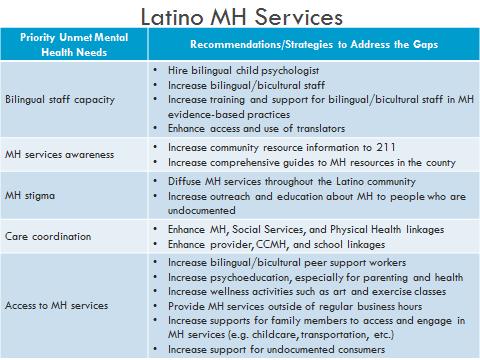
81 Consolidated Report on MHSA Community Engagement Activities Page 81
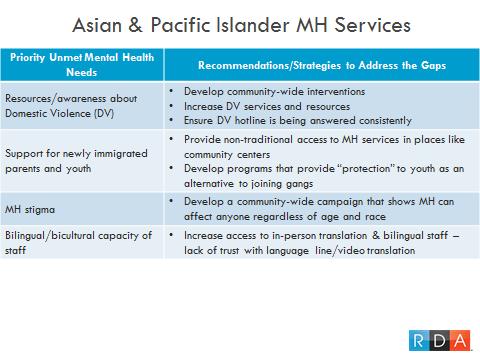
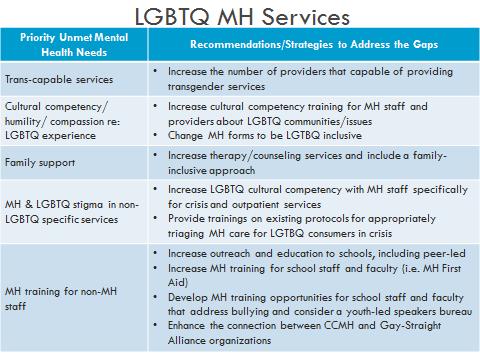
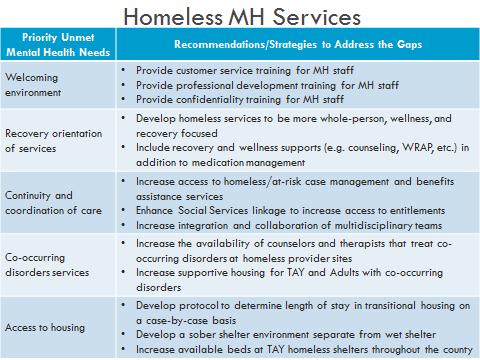
82 Consolidated Report on MHSA Community Engagement Activities Page 82
Contra Costa County Mental Health Services Act Community Forum
 Contra Costa County Mental Health Services Act Community Forum Community Program Planning Process for the Fiscal Year 2017-20 MHSA Three Year Program and Expenditure Plan November 3, 2016 Central Contra
Contra Costa County Mental Health Services Act Community Forum Community Program Planning Process for the Fiscal Year 2017-20 MHSA Three Year Program and Expenditure Plan November 3, 2016 Central Contra
Enclosure B Description of Community Program Planning (CPP) and Local Review Processes PEI Statewide Program Funding Request
 and Local Review Processes PEI Statewide Program Funding Request") Enclosure B Description of Community Program Planning (CPP) and Local Review Processes PEI Statewide Program Funding Request County s Name s: Alameda County and City of Berkeley Instructions: Utilizing
Enclosure B Description of Community Program Planning (CPP) and Local Review Processes PEI Statewide Program Funding Request County s Name s: Alameda County and City of Berkeley Instructions: Utilizing
Summary Report MHSOAC Community Forum - Stanislaus County The Seasons Multicultural Event Center, Modesto December 8, 2011
 Summary Report MHSOAC Community Forum - Stanislaus County The Seasons Multicultural Event Center, Modesto December 8, 2011 The Mental Health Services Oversight and Accountability Commission (MHSOAC) hosted
Summary Report MHSOAC Community Forum - Stanislaus County The Seasons Multicultural Event Center, Modesto December 8, 2011 The Mental Health Services Oversight and Accountability Commission (MHSOAC) hosted
County of Santa Barbara Fiscal Years , ,
 MENTAL HEALTH SERVICES ACT THREE-YEAR PROGRAM & EXPENDITURE PLAN COMMUNITY SERVICES & SUPPORTS County of Santa Barbara Fiscal Years 2005-06, 2006-07, 2007-08 SUMMARY OF PROPOSED PROGRAMS IN THE DRAFT FOR
MENTAL HEALTH SERVICES ACT THREE-YEAR PROGRAM & EXPENDITURE PLAN COMMUNITY SERVICES & SUPPORTS County of Santa Barbara Fiscal Years 2005-06, 2006-07, 2007-08 SUMMARY OF PROPOSED PROGRAMS IN THE DRAFT FOR
MENTAL HEALTH SERVICES ACT. Program and Expenditures Plan Update Fiscal Year
 MENTAL HEALTH SERVICES ACT Program and Expenditures Plan Update Fiscal Year 2018-2019 In November of 2004, California voters passed Proposition 63, creating the Mental Health Services Act. WHAT IS MHSA?
MENTAL HEALTH SERVICES ACT Program and Expenditures Plan Update Fiscal Year 2018-2019 In November of 2004, California voters passed Proposition 63, creating the Mental Health Services Act. WHAT IS MHSA?
INSTRUCTIONS FOR COMPLETING QUARTERLY REPORTS
 INSTRUCTIONS FOR COMPLETING QUARTERLY REPORTS PART A: MHSA PROGRAM BACKGROUND 1. Agency/Organization: Enter the name of your contracted agency/program. MHSA Initiative: Check the MHSA initiative that funds
INSTRUCTIONS FOR COMPLETING QUARTERLY REPORTS PART A: MHSA PROGRAM BACKGROUND 1. Agency/Organization: Enter the name of your contracted agency/program. MHSA Initiative: Check the MHSA initiative that funds
Strategic Plan
 2017-18 Strategic Plan 1 Strategic Planning Process The Summit County Opiate Task Force has made great strides in addressing the opiate crisis in the last few years. More than 100 Summit County citizens
2017-18 Strategic Plan 1 Strategic Planning Process The Summit County Opiate Task Force has made great strides in addressing the opiate crisis in the last few years. More than 100 Summit County citizens
Listening Tour: What is Many Minds? 4/12/17. Early Findings and Emerging Strategies to Improve Youth Mental Health
 Listening Tour: Early Findings and Emerging Strategies to Improve Youth Mental Health King County Re-engagement Provider Network April 14, 2017 Meeting 1 What is Many Minds? We are a non-profit collaborative
Listening Tour: Early Findings and Emerging Strategies to Improve Youth Mental Health King County Re-engagement Provider Network April 14, 2017 Meeting 1 What is Many Minds? We are a non-profit collaborative
Monterey County MHSA Prevention and Early Intervention
 Monterey County MHSA Prevention and Early Intervention FY 2016-17 & Data Summary Prepared for Monterey County Behavioral Health Bureau By Made possible through funding from Monterey County Behavioral Health
Monterey County MHSA Prevention and Early Intervention FY 2016-17 & Data Summary Prepared for Monterey County Behavioral Health Bureau By Made possible through funding from Monterey County Behavioral Health
County of San Diego, Health and Human Services Agency IN HOME OUTREACH TEAM PROGRAM REPORT (IHOT)
") County of San Diego, Health and Human Services Agency IN HOME OUTREACH TEAM PROGRAM REPORT (IHOT) Annual Report January 1, 2012 to December 31, 2012 County of San Diego, Health and Human Services Agency
County of San Diego, Health and Human Services Agency IN HOME OUTREACH TEAM PROGRAM REPORT (IHOT) Annual Report January 1, 2012 to December 31, 2012 County of San Diego, Health and Human Services Agency
517 Individuals 23 Families
 LATINO COMMUNITY CONNECTION Program Overview is a multi-layered program to provide behavioral health outreach, engagement, and prevention services in the Latino community. Canal Alliance, a trusted multi-service
LATINO COMMUNITY CONNECTION Program Overview is a multi-layered program to provide behavioral health outreach, engagement, and prevention services in the Latino community. Canal Alliance, a trusted multi-service
Making the Connection: County Mental Health, Community Providers, and Other Campuses
 Making the Connection: County Mental Health, Community Providers, and Other Campuses Sally Jue, MSW, Facilitator Michele Renfrow, Clinical Psychologist, Resource Navigation and Crisis Specialist Sylvia
Making the Connection: County Mental Health, Community Providers, and Other Campuses Sally Jue, MSW, Facilitator Michele Renfrow, Clinical Psychologist, Resource Navigation and Crisis Specialist Sylvia
GLENN COUNTY HEALTH SERVICES AGENCY Mental Health Department. Plan Update Fiscal Year
 GLENN COUNTY HEALTH SERVICES AGENCY Mental Health Department Mental Health Services Act Community Services and Supports (CSS) and Prevention and Early Intervention (PEI) Plan Update Fiscal Year 2009-2010
GLENN COUNTY HEALTH SERVICES AGENCY Mental Health Department Mental Health Services Act Community Services and Supports (CSS) and Prevention and Early Intervention (PEI) Plan Update Fiscal Year 2009-2010
Training needs assessment summary: One-on-one interviews
 Training needs assessment summary: One-on-one interviews Background July 2014 To collect information about ATOD training needs across Minnesota, Wilder Research, ADAD, and the SPF SIG Advisory Council
Training needs assessment summary: One-on-one interviews Background July 2014 To collect information about ATOD training needs across Minnesota, Wilder Research, ADAD, and the SPF SIG Advisory Council
Let s talk about the Mental Health Services Act (Proposition 63) in San Joaquin County. Transforming Mental Health Services
 in San Joaquin County. Transforming Mental Health Services") Let s talk about the Mental Health Services Act (Proposition 63) in San Joaquin County Transforming Mental Health Services Goals of Presentation Learn about a historical change beginning to happen in California
Let s talk about the Mental Health Services Act (Proposition 63) in San Joaquin County Transforming Mental Health Services Goals of Presentation Learn about a historical change beginning to happen in California
City of Berkeley Mental Health Services Act (MHSA) Innovations (INN) Technology Suite Project Plan
 Innovations (INN) Technology Suite Project Plan") City of Berkeley Mental Health Services Act (MHSA) Innovations (INN) Technology Suite Project Plan Mental Health Division Health, Housing & Community Services (HHCS) Department MENTAL HEALTH SERVICES ACT
City of Berkeley Mental Health Services Act (MHSA) Innovations (INN) Technology Suite Project Plan Mental Health Division Health, Housing & Community Services (HHCS) Department MENTAL HEALTH SERVICES ACT
Santa Clara County Consumer Survey
 Santa Clara County Consumer Survey In the questions below, Provider means: doctor, psychiatrist, psychologist, therapist, counselor, case manager, practitioner, or any professional that provides mental
Santa Clara County Consumer Survey In the questions below, Provider means: doctor, psychiatrist, psychologist, therapist, counselor, case manager, practitioner, or any professional that provides mental
City of Lawrence 2010 Alcohol Tax Funds Request for Proposals Calendar Year 2010 ( January December) Cover Page
 Cover Page") City of Lawrence 2010 Alcohol Tax Funds Request for Proposals Calendar Year 2010 ( January December) Cover Page Agency Name: Program Name: Contact Person: DCCCA, Inc First Step at Lake View Lisa Carter,
City of Lawrence 2010 Alcohol Tax Funds Request for Proposals Calendar Year 2010 ( January December) Cover Page Agency Name: Program Name: Contact Person: DCCCA, Inc First Step at Lake View Lisa Carter,
Exploration of Child Sexual Abuse Prevention Efforts in Washington State
 Exploration of Child Sexual Abuse Prevention Efforts in Washington State Over the last two years, WCSAP has prioritized the issue of child sexual abuse (CSA) prevention in Washington State. Our initial
Exploration of Child Sexual Abuse Prevention Efforts in Washington State Over the last two years, WCSAP has prioritized the issue of child sexual abuse (CSA) prevention in Washington State. Our initial
Together We Can Progress Update
 Together We Can Progress Update January 2016 Together We Can, government s fiveyear mental health and addictions strategy, has made significant progress since it was released in May 2012. We are improving
Together We Can Progress Update January 2016 Together We Can, government s fiveyear mental health and addictions strategy, has made significant progress since it was released in May 2012. We are improving
United Advocates for Children and Families. Stigma and Discrimination Reduction: Strategies for a Supportive Environment: Capacity Building
 United Advocates for Children and Families Stigma and Discrimination Reduction: Strategies for a Supportive Environment: Capacity Building Background United Advocates for Children and Families (UACF) received
United Advocates for Children and Families Stigma and Discrimination Reduction: Strategies for a Supportive Environment: Capacity Building Background United Advocates for Children and Families (UACF) received
Stanislaus County. Mental Health Services Act. Community Services and Supports Request for Funding FY
 Stanislaus County Mental Health Services Act Community Services and Supports Request for Funding FY 2007 2008 Additional One-Time Funding Augmentation To Expand Local Mental Health Services December 2007
Stanislaus County Mental Health Services Act Community Services and Supports Request for Funding FY 2007 2008 Additional One-Time Funding Augmentation To Expand Local Mental Health Services December 2007
Mental Health Services Act Three Year Program and Expenditure Plan Fiscal Years through
 Mental Health Services Act Three Year Program and Expenditure Plan Fiscal Years 2017-2018 through 2019-2020 "All lives are beautiful, regardless of appearance. Photovoice Empowerment Project coordinated
Mental Health Services Act Three Year Program and Expenditure Plan Fiscal Years 2017-2018 through 2019-2020 "All lives are beautiful, regardless of appearance. Photovoice Empowerment Project coordinated
Kaiser Telecare Program for Intensive Community Support Intensive Case Management Exclusively for Members within a Managed Care System
 Kaiser Telecare Program for Intensive Community Support Intensive Case Management Exclusively for Members within a Managed Care System 12-Month Customer Report, January to December, 2007 We exist to help
Kaiser Telecare Program for Intensive Community Support Intensive Case Management Exclusively for Members within a Managed Care System 12-Month Customer Report, January to December, 2007 We exist to help
Ending HIV/AIDS in Southwest Minnesota
 Ending HIV/AIDS in Southwest Minnesota SUMMARY OF REGIONAL STAKEHOLDER INPUT July 2018 Prepared by Wilder Research ENDING HIV/AIDS IN SOUTHWEST MINNESOT A Ending HIV/AIDS in Southwest Minnesota Minnesota
Ending HIV/AIDS in Southwest Minnesota SUMMARY OF REGIONAL STAKEHOLDER INPUT July 2018 Prepared by Wilder Research ENDING HIV/AIDS IN SOUTHWEST MINNESOT A Ending HIV/AIDS in Southwest Minnesota Minnesota
Ending HIV/AIDS Among Transgender People in Minnesota
 Ending HIV/AIDS Among Transgender People in Minnesota SUMMARY OF COMMUNITY STAKEHOLDER INPUT July 2018 Prepared by Wilder Research Ending HIV/AIDS Among Transgender People in Minnesota Minnesota Department
Ending HIV/AIDS Among Transgender People in Minnesota SUMMARY OF COMMUNITY STAKEHOLDER INPUT July 2018 Prepared by Wilder Research Ending HIV/AIDS Among Transgender People in Minnesota Minnesota Department
Traditional Health Workers: Oregon s model
 Traditional Health Workers: Oregon s model Community Health Workers, Peer Support Specialists, Family Support Specialist, Youth Support Specialist Peer Wellness Specialists, Personal Health Navigators,
Traditional Health Workers: Oregon s model Community Health Workers, Peer Support Specialists, Family Support Specialist, Youth Support Specialist Peer Wellness Specialists, Personal Health Navigators,
Provider: MHP Work Plan:
 PROGRAM INFORMATION: Program Title: Program Description: Kings View Behavioral Health Mental Health Services Peer/Family Support Wellness Center (Blue Sky) A prevention and early intervention peer centered
PROGRAM INFORMATION: Program Title: Program Description: Kings View Behavioral Health Mental Health Services Peer/Family Support Wellness Center (Blue Sky) A prevention and early intervention peer centered
Core Competencies for Peer Workers in Behavioral Health Services
 Core Competencies for Peer Workers in Behavioral Health Services Category I: Engages peers in collaborative and caring relationships This category of competencies emphasized peer workers' ability to initiate
Core Competencies for Peer Workers in Behavioral Health Services Category I: Engages peers in collaborative and caring relationships This category of competencies emphasized peer workers' ability to initiate
JOINT TESTIMONY. Homeless Services United Catherine Trapani Executive Director, HSU
 New York City Council Committees on General Welfare and Health Oversight - Part 1: Medical Health Services in the DHS Shelter System Int. No. 929 - in relation to requiring information on health services
New York City Council Committees on General Welfare and Health Oversight - Part 1: Medical Health Services in the DHS Shelter System Int. No. 929 - in relation to requiring information on health services
From Shelter to Safe Housing: Reframing our Movement s Response to Survivors Housing Needs
 From Shelter to Safe Housing: Reframing our Movement s Response to Survivors Housing Needs Objectives Discuss what it means to respond to survivors housing needs within the context of our movement today
From Shelter to Safe Housing: Reframing our Movement s Response to Survivors Housing Needs Objectives Discuss what it means to respond to survivors housing needs within the context of our movement today
San Francisco s Assisted Outpatient Treatment Program
 San Francisco s Assisted Outpatient Treatment Program 2016 Annual Report April 29, 2016 Assisted Outpatient Treatment (AOT) is a program of the San Francisco Department of Public Health Behavioral Health
San Francisco s Assisted Outpatient Treatment Program 2016 Annual Report April 29, 2016 Assisted Outpatient Treatment (AOT) is a program of the San Francisco Department of Public Health Behavioral Health
Healing, Justice, & Trust
 Healing, Justice, & Trust A National Report on Outcomes for Children's Advocacy Centers 2015 National Children s Alliance Healing, Justice, & Trust - A National Report on Outcomes for Children s Advocacy
Healing, Justice, & Trust A National Report on Outcomes for Children's Advocacy Centers 2015 National Children s Alliance Healing, Justice, & Trust - A National Report on Outcomes for Children s Advocacy
RICHLAND COUNTY MENTAL HEALTH AND RECOVERY SERVICES
 RICHLAND COUNTY MENTAL HEALTH AND RECOVERY SERVICES 5-YEAR STRATEGIC PLAN SUMMARY 2017 TO 2022 Mission Statement The mission of the Richland County Mental Health and Recovery Services Board is to facilitate
RICHLAND COUNTY MENTAL HEALTH AND RECOVERY SERVICES 5-YEAR STRATEGIC PLAN SUMMARY 2017 TO 2022 Mission Statement The mission of the Richland County Mental Health and Recovery Services Board is to facilitate
Community Intervention Pre-crisis Team (CIPT) Report Executive Summary
 Report Executive Summary") Community Intervention Pre-crisis Team (CIPT) Report Executive Summary Data from: January-December 1 TABLE OF CONTENTS Overview... Community Outreach Activity... Community Access Telephone Line Activity...
Community Intervention Pre-crisis Team (CIPT) Report Executive Summary Data from: January-December 1 TABLE OF CONTENTS Overview... Community Outreach Activity... Community Access Telephone Line Activity...
NAME: If interpreters are used, what is their training in child trauma? This depends upon the agency.
 0000: General Name Spelled Culture-Specific Out Engagement For which specific cultural group(s) (i.e., SES, religion, race, ethnicity, gender, immigrants/refugees, disabled, homeless, LGBTQ, rural/urban
0000: General Name Spelled Culture-Specific Out Engagement For which specific cultural group(s) (i.e., SES, religion, race, ethnicity, gender, immigrants/refugees, disabled, homeless, LGBTQ, rural/urban
Facilitated Discussion Notes Autism and Mental Health May 12, 2014
 Facilitated Discussion Notes Autism and Mental Health May 12, 2014 Below are notes distilling the comments made by participants during a Facilitated Discussion of this topic. Generally, the comments are
Facilitated Discussion Notes Autism and Mental Health May 12, 2014 Below are notes distilling the comments made by participants during a Facilitated Discussion of this topic. Generally, the comments are
Core Competencies for Peer Workers in Behavioral Health Services
 BRINGING RECOVERY SUPPORTS TO SCALE Technical Assistance Center Strategy (BRSS TACS) Core Competencies for Peer Workers in Behavioral Health Services OVERVIEW In 2015, SAMHSA led an effort to identify
BRINGING RECOVERY SUPPORTS TO SCALE Technical Assistance Center Strategy (BRSS TACS) Core Competencies for Peer Workers in Behavioral Health Services OVERVIEW In 2015, SAMHSA led an effort to identify
COUNTY SNAPSHOT GLENN COUNTY CONTACTS OVERVIEW. Method of Data Collection Utilized: In-Person Interview January 31, 2012
 COUNTY SNAPSHOT GLENN COUNTY CONTACTS Interview Participants: Roxanne Baillergeon 530.865.6459 rbaillergeon@glenncountyhealth.net Amy Lindsey, MFT Behavioral Health Deputy Director 530.934.6582 alindsey@glenncountyhealth.net
COUNTY SNAPSHOT GLENN COUNTY CONTACTS Interview Participants: Roxanne Baillergeon 530.865.6459 rbaillergeon@glenncountyhealth.net Amy Lindsey, MFT Behavioral Health Deputy Director 530.934.6582 alindsey@glenncountyhealth.net
Nebraska Statewide Suicide Prevention Plan
 Nebraska Statewide Suicide Prevention Plan 2016-2020 This plan provides a framework to help Nebraskans work together to prevent suicide. It sets out shared strategies for suicide prevention and sets the
Nebraska Statewide Suicide Prevention Plan 2016-2020 This plan provides a framework to help Nebraskans work together to prevent suicide. It sets out shared strategies for suicide prevention and sets the
ADDRESSING HEALTH CARE AND OTHER RESOURCE BARRIERS AMONG SOMALI FAMILIES OF CHILDREN WITH AUTISM DAKOTA COUNTY PUBLIC HEALTH
 ADDRESSING HEALTH CARE AND OTHER RESOURCE BARRIERS AMONG SOMALI FAMILIES OF CHILDREN WITH AUTISM DAKOTA COUNTY PUBLIC HEALTH January 2019 Addressing Health Care and Other Resource Barriers Among Somali
ADDRESSING HEALTH CARE AND OTHER RESOURCE BARRIERS AMONG SOMALI FAMILIES OF CHILDREN WITH AUTISM DAKOTA COUNTY PUBLIC HEALTH January 2019 Addressing Health Care and Other Resource Barriers Among Somali
6/26/2015. Recovery Oriented Systems of Care: Where Does Prevention Fit In? Long Term Recovery
 Recovery Oriented Systems of Care: Where Does Prevention Fit In? Langeston Hughes, Comprehensive Community Services Coordinator Andrea Jacobson, Substance Abuse Treatment Coordinator June 12, 2015 Division
Recovery Oriented Systems of Care: Where Does Prevention Fit In? Langeston Hughes, Comprehensive Community Services Coordinator Andrea Jacobson, Substance Abuse Treatment Coordinator June 12, 2015 Division
Thank you for agreeing to complete the Canadian Mental Health Association (CMHA) of Central Alberta 2017 Speak Up for Mental Health
 of Central Alberta 2017 Speak Up for Mental Health") The 2017 CMHA Speak Up for Mental Health Survey 1. Introduction Thank you for agreeing to complete the Canadian Mental Health Association (CMHA) of Central Alberta 2017 Speak Up for Mental Health survey.
The 2017 CMHA Speak Up for Mental Health Survey 1. Introduction Thank you for agreeing to complete the Canadian Mental Health Association (CMHA) of Central Alberta 2017 Speak Up for Mental Health survey.
DASH s Survivor Resilience Fund: Utilizing flexible funds to help survivors avoid homelessness
 DASH s Survivor Resilience Fund: Utilizing flexible funds to help survivors avoid homelessness Presentation Outline I. About DASH II. Survivor Resilience Fund (SRF) Overview III. SRF Pilot Project Study
DASH s Survivor Resilience Fund: Utilizing flexible funds to help survivors avoid homelessness Presentation Outline I. About DASH II. Survivor Resilience Fund (SRF) Overview III. SRF Pilot Project Study
Douglas County s Mental Health Diversion Program
 Douglas County s Mental Health Diversion Program Cynthia A. Boganowski The incarceration of people with serious mental illness is of growing interest and concern nationally. Because jails and prisons are
Douglas County s Mental Health Diversion Program Cynthia A. Boganowski The incarceration of people with serious mental illness is of growing interest and concern nationally. Because jails and prisons are
Community Needs Assessment. June 26, 2013
 Community Needs Assessment June 26, 2013 Agenda Purpose Methodology for Collecting Data Geographic Area Demographic Information Community Health Data Prevalence of Alcohol & Drug Use Utilization data Findings
Community Needs Assessment June 26, 2013 Agenda Purpose Methodology for Collecting Data Geographic Area Demographic Information Community Health Data Prevalence of Alcohol & Drug Use Utilization data Findings
At COLAGE, the only national youth-driven movement of people with lesbian, gay,
 Final Report Emily McGranachan COLAGE At COLAGE, the only national youth-driven movement of people with lesbian, gay, bisexual, transgender and/or queer parents, I had a fair amount of responsibility and
Final Report Emily McGranachan COLAGE At COLAGE, the only national youth-driven movement of people with lesbian, gay, bisexual, transgender and/or queer parents, I had a fair amount of responsibility and
Massachusetts Alzheimer s Disease & Other Dementias Online Training Program 2017
 Massachusetts Alzheimer s Disease & Other Dementias Online Training Program 2017 Final Evaluation Report from Boston University April 2018 1 I. INTRODUCTION Boston University s Center for Aging and Disability
Massachusetts Alzheimer s Disease & Other Dementias Online Training Program 2017 Final Evaluation Report from Boston University April 2018 1 I. INTRODUCTION Boston University s Center for Aging and Disability
WELLNESS CENTERS: A Coordinated Model to Support Students Physical & Emotional Health and Well-being in TUHSD High Schools
 WELLNESS CENTERS: A Coordinated Model to Support Students Physical & Emotional Health and Well-being in TUHSD High Schools Jessica Colvin, MSW, MPH, PPSC Wellness Director Tamalpais Union High School District
WELLNESS CENTERS: A Coordinated Model to Support Students Physical & Emotional Health and Well-being in TUHSD High Schools Jessica Colvin, MSW, MPH, PPSC Wellness Director Tamalpais Union High School District
NCACH RAPID CYCLE APPLICATION: OPIOID PROJECT North Central Accountable Community of Health - Medicaid Transformation Project
 NCACH RAPID CYCLE APPLICATION: OPIOID PROJECT North Central Accountable Community of Health - Introduction The North Central Accountable Community of Health (NCACH) is accepting applications from partners
NCACH RAPID CYCLE APPLICATION: OPIOID PROJECT North Central Accountable Community of Health - Introduction The North Central Accountable Community of Health (NCACH) is accepting applications from partners
TYPES OF FAMILY PEER SUPPORT SERVICES. Outreach and Information FAMILY PEER SUPPORT SERVICES DEFINITION
 FAMILY PEER SUPPORT SERVICES DEFINITION Family Peer Support Services (FPSS) are an array of formal and informal services and supports provided to families raising a child up to age 26 who is experiencing
FAMILY PEER SUPPORT SERVICES DEFINITION Family Peer Support Services (FPSS) are an array of formal and informal services and supports provided to families raising a child up to age 26 who is experiencing
Peer Supports for Transition-Aged Youth
 Peer Supports for Transition-Aged Youth Matt Gallagher: Living in Recovery from Depression and Anxiety: Received Peer Support Services Former Youth Advocate (Transitional Age Youth Peer Mentor) For Mental
Peer Supports for Transition-Aged Youth Matt Gallagher: Living in Recovery from Depression and Anxiety: Received Peer Support Services Former Youth Advocate (Transitional Age Youth Peer Mentor) For Mental
Kirsten Barlow, Executive Director County Behavioral Health Directors Association of California (CBHDA)
") Kirsten Barlow, Executive Director County Behavioral Health Directors Association of California (CBHDA) May 2017 Who do counties serve? * All ages * Primarily Medi-Cal beneficiaries * People with a serious
Kirsten Barlow, Executive Director County Behavioral Health Directors Association of California (CBHDA) May 2017 Who do counties serve? * All ages * Primarily Medi-Cal beneficiaries * People with a serious
KEYS TO A FUTURE WITHOUT YOUTH HOMELESSNESS Writing a Comprehensive Community Plan to End Youth Homelessness in Cincinnati & Hamilton County
 KEYS TO A FUTURE WITHOUT YOUTH HOMELESSNESS Writing a Comprehensive Community Plan to End Youth Homelessness in Cincinnati & Hamilton County Jen Best, She/Her/Hers Strategies to End Homelessness YHDP Shared
KEYS TO A FUTURE WITHOUT YOUTH HOMELESSNESS Writing a Comprehensive Community Plan to End Youth Homelessness in Cincinnati & Hamilton County Jen Best, She/Her/Hers Strategies to End Homelessness YHDP Shared
DISCUSSION GUIDE FOOD FOR THOUGHT: A YOUTH PERSPECTIVE ON RECOVERY ORIENTED PRACTICE
 DISCUSSION GUIDE FOOD FOR THOUGHT: A YOUTH PERSPECTIVE ON RECOVERY ORIENTED PRACTICE How confident are you about how to deliver great recovery-oriented services to a young person? How is recovery-oriented
DISCUSSION GUIDE FOOD FOR THOUGHT: A YOUTH PERSPECTIVE ON RECOVERY ORIENTED PRACTICE How confident are you about how to deliver great recovery-oriented services to a young person? How is recovery-oriented
MHSA Idea Bank for February 26, 2016
 Children/Youth (Ages 0-5/6-17) Prevention & Early Intervention Idea #1 - MoPride: Sub-Population: LGBTQ Results: Support and education in ; Social Inclusion, Strategy: Outreach & Engagement; support, peer
Children/Youth (Ages 0-5/6-17) Prevention & Early Intervention Idea #1 - MoPride: Sub-Population: LGBTQ Results: Support and education in ; Social Inclusion, Strategy: Outreach & Engagement; support, peer
Health Share of Oregon
 Health Share of Oregon Community Health Improvement Plan: Update & Next Steps CAC Meeting December 5, 2014 HEALTH SHARE OF OREGON DECEMBER 10, 2014 COMMUNITY HEALTH ASSESSMENT P. 1 Community Advisory Council
Health Share of Oregon Community Health Improvement Plan: Update & Next Steps CAC Meeting December 5, 2014 HEALTH SHARE OF OREGON DECEMBER 10, 2014 COMMUNITY HEALTH ASSESSMENT P. 1 Community Advisory Council
TRAUMA RECOVERY CENTER SERVICE FLOW
 TRAUMA RECOVERY CENTER SERVICE FLOW Photograph by Ezme Kozuszek What wisdom can you find that is greater than kindness? Jean Jacques Rousseau The UC San Francisco Trauma Recovery Center Model: Removing
TRAUMA RECOVERY CENTER SERVICE FLOW Photograph by Ezme Kozuszek What wisdom can you find that is greater than kindness? Jean Jacques Rousseau The UC San Francisco Trauma Recovery Center Model: Removing
Perspectives from Minnesota NASDDDS Annual Conference November 14, 2014
 Cultural Competence: Making it Happen Perspectives from Minnesota NASDDDS Annual Conference November 14, 2014 100% 90% 80% Minnesota's Changing Population Diversity 86% 84% 81% 80% 78% 77% 75% 70% 60%
Cultural Competence: Making it Happen Perspectives from Minnesota NASDDDS Annual Conference November 14, 2014 100% 90% 80% Minnesota's Changing Population Diversity 86% 84% 81% 80% 78% 77% 75% 70% 60%
New Jersey Alliance of Family Support Organizations Annual Membership Report
 New Jersey Alliance of Family Support Organizations Annual Membership Report 2011-2012 Helping youth with emotional, behavioral, and mental health needs and their families 1 Why the New Jersey Alliance
New Jersey Alliance of Family Support Organizations Annual Membership Report 2011-2012 Helping youth with emotional, behavioral, and mental health needs and their families 1 Why the New Jersey Alliance
Marin County MHSA Three-Year Community Planning Process FY2017-FY2020
 Marin County MHSA Three-Year Community Planning Process FY2017-FY2020 Mental Health Services Act Historical Overview Local systems stretched beyond capacity Consumers and family members without adequate
Marin County MHSA Three-Year Community Planning Process FY2017-FY2020 Mental Health Services Act Historical Overview Local systems stretched beyond capacity Consumers and family members without adequate
AFFORDABLE CARE ACT IMPLICATIONS AND OPPORTUNITIES FOR IMPROVING ENROLLMENT FOR HOMELESS POPULATIONS
 AFFORDABLE CARE ACT IMPLICATIONS AND OPPORTUNITIES FOR IMPROVING ENROLLMENT FOR HOMELESS POPULATIONS Kevin Malone Substance Abuse and Mental Health Services Administration National Alliance to End Homelessness
AFFORDABLE CARE ACT IMPLICATIONS AND OPPORTUNITIES FOR IMPROVING ENROLLMENT FOR HOMELESS POPULATIONS Kevin Malone Substance Abuse and Mental Health Services Administration National Alliance to End Homelessness
SUPPORTING COLLABORATIVE CARE THROUGH MENTAL HEALTH GROUPS IN PRIMARY CARE Hamilton Family Health Team
 SUPPORTING COLLABORATIVE CARE THROUGH MENTAL HEALTH GROUPS IN PRIMARY CARE Hamilton Family Health Team Jackie Bootsma, MSW, RSW Marian Schorr, MSW, RSW About Family Health Teams Family Health Teams are
SUPPORTING COLLABORATIVE CARE THROUGH MENTAL HEALTH GROUPS IN PRIMARY CARE Hamilton Family Health Team Jackie Bootsma, MSW, RSW Marian Schorr, MSW, RSW About Family Health Teams Family Health Teams are
ADVANCING WOMEN AND GIRLS, ONE CITY AT A TIME
 ADVANCING WOMEN AND GIRLS, ONE CITY AT A TIME It s Time Network s Mayors Guide: Accelerating Gender Equality is the first comprehensive guide for accelerating gender equality at the local level. The guide
ADVANCING WOMEN AND GIRLS, ONE CITY AT A TIME It s Time Network s Mayors Guide: Accelerating Gender Equality is the first comprehensive guide for accelerating gender equality at the local level. The guide
Executive Director Position Announcement August, 2018
 Executive Director Position Announcement August, 2018 Overview This is an excellent opportunity for a seasoned nonprofit leader with a proven ability to positively engage people to lead an organization
Executive Director Position Announcement August, 2018 Overview This is an excellent opportunity for a seasoned nonprofit leader with a proven ability to positively engage people to lead an organization
NORTH YORKSHIRE POLICE AND CRIME COMMISSIONER (PCC) AND NORTH YORKSHIRE YOUTH COMMISSION BIG CONVERSATION
 AND NORTH YORKSHIRE YOUTH COMMISSION BIG CONVERSATION") APPENDIX 3 Throughout the year a great deal of local engagement work has been undertaken by key partners to ensure that the voice of children, young people and their families are represented in all stages
APPENDIX 3 Throughout the year a great deal of local engagement work has been undertaken by key partners to ensure that the voice of children, young people and their families are represented in all stages
CULTURE-SPECIFIC INFORMATION
 NAME: Sanctuary 0000: General Name Model Spelled Culture-Specific Information Out Information Engagement For which specific cultural group(s) (i.e., SES, religion, race, ethnicity, gender, immigrants/refugees,
NAME: Sanctuary 0000: General Name Model Spelled Culture-Specific Information Out Information Engagement For which specific cultural group(s) (i.e., SES, religion, race, ethnicity, gender, immigrants/refugees,
Humboldt County Department of Health and Human Services Mental Health Branch. Mental Health Services Act Prevention and Early Intervention Plan
 Humboldt County Department of Health and Human Services Mental Health Branch Mental Health Services Act Prevention and Early Intervention Plan December 2008 Table of Contents Prevention and Early Intervention
Humboldt County Department of Health and Human Services Mental Health Branch Mental Health Services Act Prevention and Early Intervention Plan December 2008 Table of Contents Prevention and Early Intervention
MHSA. Representative Stakeholder Steering Committee. Behavioral Health & Recovery Services Mental Health Services Act Planning Meeting
 MHSA Representative Stakeholder Steering Committee Behavioral Health & Recovery Services Mental Health Services Act Planning Meeting February 26, 2016 1 MHSA Representative Stakeholder Steering Committee
MHSA Representative Stakeholder Steering Committee Behavioral Health & Recovery Services Mental Health Services Act Planning Meeting February 26, 2016 1 MHSA Representative Stakeholder Steering Committee
HIV Prevention Service Provider Survey 2014
 Respondent Demographics This survey will help the Florida HIV Prevention Planning Group (PPG) establish the resources and unmet needs of the communities we serve. Please take a few minutes to complete
Respondent Demographics This survey will help the Florida HIV Prevention Planning Group (PPG) establish the resources and unmet needs of the communities we serve. Please take a few minutes to complete
A Qualitative Study of Families of Children with Autism in the Somali Community: Comparing the Experiences of Immigrant Groups
 Commissioner s Office PO Box 64975 St. Paul, MN 55164-0975 651-201-5000 http://www.health.state.mn.us A Qualitative Study of Families of Children with Autism in the Somali Community: Comparing the Experiences
Commissioner s Office PO Box 64975 St. Paul, MN 55164-0975 651-201-5000 http://www.health.state.mn.us A Qualitative Study of Families of Children with Autism in the Somali Community: Comparing the Experiences
Fremantle. Community Engagement and Co-Design Workshop Report
 Fremantle Integrated Systems of Care to support people with mental health, alcohol and other drug issues (ISC) Community Engagement and Co-Design Workshop Report 2017 Executive Summary: Fremantle Area
Fremantle Integrated Systems of Care to support people with mental health, alcohol and other drug issues (ISC) Community Engagement and Co-Design Workshop Report 2017 Executive Summary: Fremantle Area
Personal Assessment for Advocates Working with Victims of Sexual Violence
 Personal Assessment for Advocates Working with Victims of Sexual Violence The work of responding to sexual assault and helping survivors rebuild their lives is done by advocates in an array of organizational
Personal Assessment for Advocates Working with Victims of Sexual Violence The work of responding to sexual assault and helping survivors rebuild their lives is done by advocates in an array of organizational
2 WHO 1 Who do you need to involve? a specific condition, service or treatment
 PATIENT AND PUBLIC ENGAGEMENT PLANNING TEMPLATE Instructions: Patient engagement is about meaningful engagement of patients/public in the research process (not just as subjects of research). This template
PATIENT AND PUBLIC ENGAGEMENT PLANNING TEMPLATE Instructions: Patient engagement is about meaningful engagement of patients/public in the research process (not just as subjects of research). This template
Consumer Perception Survey (Formerly Known as POQI)
") Department of Behavioral Health Consumer Perception Survey (Formerly Known as POQI) CPS Comparison May 2017 On a semi-annual basis the County of Fresno, Department of Behavioral Health (DBH) conducts its
Department of Behavioral Health Consumer Perception Survey (Formerly Known as POQI) CPS Comparison May 2017 On a semi-annual basis the County of Fresno, Department of Behavioral Health (DBH) conducts its
Optum Behavioral Health Services
 Optum Behavioral Health Services A whole-person approach to improve outcomes for Medicaid agencies and their members Serving the needs of the whole person At Optum, we re keenly aware of the challenges
Optum Behavioral Health Services A whole-person approach to improve outcomes for Medicaid agencies and their members Serving the needs of the whole person At Optum, we re keenly aware of the challenges
Improving Emotional Wellbeing for Young People. Mike Derry and Anna D Agostino - Healthwatch Richmond
 Improving Emotional Wellbeing for Young People Mike Derry and Anna D Agostino - Healthwatch Richmond Aim To collect young people's experiences of: Emotional wellbeing and related services Recommend improvements
Improving Emotional Wellbeing for Young People Mike Derry and Anna D Agostino - Healthwatch Richmond Aim To collect young people's experiences of: Emotional wellbeing and related services Recommend improvements
Report: Proposition 63: Money for Mental Health: Are We Getting It Right in Santa Cruz?
 Responses to the 2013-2014 Grand Jury Report Every year, when the annual Santa Cruz County Grand Jury Report is published, designated agencies are requested to respond to the findings and recommendations
Responses to the 2013-2014 Grand Jury Report Every year, when the annual Santa Cruz County Grand Jury Report is published, designated agencies are requested to respond to the findings and recommendations
Reducing the Impact of Cancer. Listening to American Indians in Minnesota
 Reducing the Impact of Cancer Listening to American Indians in Minnesota Table of Contents Background... 2 Summary of Results... 3 Part 1: Summary of responses from American Indian listening sessions...
Reducing the Impact of Cancer Listening to American Indians in Minnesota Table of Contents Background... 2 Summary of Results... 3 Part 1: Summary of responses from American Indian listening sessions...
MHSA PEI March Mental Health Services Act Prevention and Early Intervention. Jill D. Sharkey, Ph.D. Erin Dowdy, Ph.D. Michael J. Furlong, Ph.D.
 MHSA PEI March 2009 Mental Health Services Act Prevention and Early Intervention Jill D. Sharkey, Ph.D. Erin Dowdy, Ph.D. Michael J. Furlong, Ph.D. Gevirtz Graduate School of Education Department of Counseling,
MHSA PEI March 2009 Mental Health Services Act Prevention and Early Intervention Jill D. Sharkey, Ph.D. Erin Dowdy, Ph.D. Michael J. Furlong, Ph.D. Gevirtz Graduate School of Education Department of Counseling,
UNDERSTANDING GIVING: ACROSS GENERATIONS
 UNDERSTANDING GIVING: ACROSS GENERATIONS A REPORT OF THE COLORADO GENEROSITY PROJECT In Understanding Giving: Beliefs & Behaviors of Colorado s Donors, we explored what, how, and why Coloradans give. The
UNDERSTANDING GIVING: ACROSS GENERATIONS A REPORT OF THE COLORADO GENEROSITY PROJECT In Understanding Giving: Beliefs & Behaviors of Colorado s Donors, we explored what, how, and why Coloradans give. The
Focus of Today s Presentation. Partners in Healing Model. Partners in Healing: Background. Data Collection Tools. Research Design
 Exploring the Impact of Delivering Mental Health Services in NYC After-School Programs Gerald Landsberg, DSW, MPA Stephanie-Smith Waterman, MSW, MS Ana Maria Pinter, M.A. Focus of Today s Presentation
Exploring the Impact of Delivering Mental Health Services in NYC After-School Programs Gerald Landsberg, DSW, MPA Stephanie-Smith Waterman, MSW, MS Ana Maria Pinter, M.A. Focus of Today s Presentation
Dr. David M. Johnson, Chief Executive Officer. Cindy Spanton, Navos, and Sunny Lovin, Harborview Medical Center
 2016 Community Health Leadership Award Nomination Nominator Name: Organization Being Nominated: Name of Program: Program Contact: Dr. David M. Johnson, Chief Executive Officer Navos and Harborview Medical
2016 Community Health Leadership Award Nomination Nominator Name: Organization Being Nominated: Name of Program: Program Contact: Dr. David M. Johnson, Chief Executive Officer Navos and Harborview Medical
Ministry of Children and Youth Services. Follow-up to VFM Section 3.01, 2013 Annual Report RECOMMENDATION STATUS OVERVIEW
 Chapter 4 Section 4.01 Ministry of Children and Youth Services Autism Services and Supports for Children Follow-up to VFM Section 3.01, 2013 Annual Report RECOMMENDATION STATUS OVERVIEW # of Status of
Chapter 4 Section 4.01 Ministry of Children and Youth Services Autism Services and Supports for Children Follow-up to VFM Section 3.01, 2013 Annual Report RECOMMENDATION STATUS OVERVIEW # of Status of
Joint Mental Health Commissioning Strategy for Adults
 Joint Mental Health Commissioning Strategy for Adults 2014-2019 Summary Developed in partnership with: NHS Ipswich and East Suffolk CCG, NHS West Suffolk CCG, Suffolk Constabulary and Suffolk County Council
Joint Mental Health Commissioning Strategy for Adults 2014-2019 Summary Developed in partnership with: NHS Ipswich and East Suffolk CCG, NHS West Suffolk CCG, Suffolk Constabulary and Suffolk County Council
Mental Wellness of Students at Harvard Chan
 HARVARD CHAN MENTAL HEALTH STUDENT ALLIANCE Mental Wellness of Students at Harvard Chan SPRING 2017 SURVEY Executive Summary Overview of Results & Recommendations HARVARD CHAN MENTAL HEALTH STUDENT ALLIANCE
HARVARD CHAN MENTAL HEALTH STUDENT ALLIANCE Mental Wellness of Students at Harvard Chan SPRING 2017 SURVEY Executive Summary Overview of Results & Recommendations HARVARD CHAN MENTAL HEALTH STUDENT ALLIANCE
LEADERSHIP PROFILE. Executive Director Gateway Center Atlanta, GA THE OPPORTUNITY
 LEADERSHIP PROFILE Executive Director Gateway Center Atlanta, GA The core mission of the Gateway Center is to provide a supportive and compassionate setting where individuals can receive the tools, programs,
LEADERSHIP PROFILE Executive Director Gateway Center Atlanta, GA The core mission of the Gateway Center is to provide a supportive and compassionate setting where individuals can receive the tools, programs,
Language Assistance Plan
 Language Assistance Plan I. Identification of LEP persons II. Language Assistance Measures III. Court Staff and Volunteer Recruitment IV. Training Staff V. Providing Notice to LEP Persons VI. Monitoring
Language Assistance Plan I. Identification of LEP persons II. Language Assistance Measures III. Court Staff and Volunteer Recruitment IV. Training Staff V. Providing Notice to LEP Persons VI. Monitoring
STAKEHOLDER SURVEY RESULTS SUMMARY
 PROJECT SAFETY NET (PSN) MISSION/VISION PROJECT STAKEHOLDER SURVEY RESULTS SUMMARY with February 2019 Amari Romero-Thomas Mosaic Consulting and Coaching SURVEY PURPOSE To collect input on key elements
PROJECT SAFETY NET (PSN) MISSION/VISION PROJECT STAKEHOLDER SURVEY RESULTS SUMMARY with February 2019 Amari Romero-Thomas Mosaic Consulting and Coaching SURVEY PURPOSE To collect input on key elements
Peer Supports New Roles in Integrated Care Promoting Health and Wellness for Families and Communities
 Peer Supports New Roles in Integrated Care Promoting Health and Wellness for Families and Communities Cathy Callahan-Clem, CPC Jody Schreven, CPC Theresa Winther, LMFT, CMHS, MAC 1 Introduction In this
Peer Supports New Roles in Integrated Care Promoting Health and Wellness for Families and Communities Cathy Callahan-Clem, CPC Jody Schreven, CPC Theresa Winther, LMFT, CMHS, MAC 1 Introduction In this
Toronto Mental Health and Addictions Supportive Housing Network TERMS OF REFERENCE
 1 Toronto Mental Health and Addictions Supportive Housing Network BACKGROUND: TERMS OF REFERENCE The Toronto Mental Health and Addictions Supportive Housing Network (TMHASHN), is a network of organizations
1 Toronto Mental Health and Addictions Supportive Housing Network BACKGROUND: TERMS OF REFERENCE The Toronto Mental Health and Addictions Supportive Housing Network (TMHASHN), is a network of organizations
EXHIBIT A COUNTY CERTIFICATION MHSA FY 2009/10 PLAN AMENDMENT
 EXHIBIT A COUNTY CERTIFICATION MHSA FY 2009/10 PLAN AMENDMENT County Name: Sacramento County Mental Health Director Name: Mary Ann Bennett Telephone Number: 916-875-9904 E-mail: BennettMa@SacCounty.net
EXHIBIT A COUNTY CERTIFICATION MHSA FY 2009/10 PLAN AMENDMENT County Name: Sacramento County Mental Health Director Name: Mary Ann Bennett Telephone Number: 916-875-9904 E-mail: BennettMa@SacCounty.net
Mood Disorders Society of Canada Mental Health Care System Study Summary Report
 Mood Disorders Society of Canada Mental Health Care System Study Summary Report July 2015 Prepared for the Mood Disorders Society of Canada by: Objectives and Methodology 2 The primary objective of the
Mood Disorders Society of Canada Mental Health Care System Study Summary Report July 2015 Prepared for the Mood Disorders Society of Canada by: Objectives and Methodology 2 The primary objective of the
Welcome to Progress in Community Health Partnerships latest episode our Beyond the Manuscript podcast. In each
 Beyond the Manuscript 91 Podcast Interview Transcript Erin Kobetz, Joan Bloom, Irma Robbins, Kim Engelman Welcome to Progress in Community Health Partnerships latest episode our Beyond the Manuscript podcast.
Beyond the Manuscript 91 Podcast Interview Transcript Erin Kobetz, Joan Bloom, Irma Robbins, Kim Engelman Welcome to Progress in Community Health Partnerships latest episode our Beyond the Manuscript podcast.
What is CCS. More Than Therapy and Medicine 10/20/2016. Recovery-Oriented Systems of Care (ROSC) and Comprehensive Community Services
 and Comprehensive Community Services") Recovery-Oriented Systems of Care (ROSC) and Comprehensive Community Services Langeston Hughes, CCS Coordinator Danielle Graham-Heine, CCS Coordinator October 27, 2016 What is CCS Publicly-operated behavioral
Recovery-Oriented Systems of Care (ROSC) and Comprehensive Community Services Langeston Hughes, CCS Coordinator Danielle Graham-Heine, CCS Coordinator October 27, 2016 What is CCS Publicly-operated behavioral
Moving Towards a Continuum of Services. Plumas County Alcohol & Drug Strategic Planning Process DRAFT PLAN
 Moving Towards a Continuum of Services Plumas County Alcohol & Drug Strategic Planning Process DRAFT PLAN Summary Substance use, abuse and addiction range in intensity from experimentation to severe and
Moving Towards a Continuum of Services Plumas County Alcohol & Drug Strategic Planning Process DRAFT PLAN Summary Substance use, abuse and addiction range in intensity from experimentation to severe and
City of Berkeley Mental Health Mental Health Services Act (MHSA)
") City of Berkeley Mental Health Mental Health Services Act (MHSA) FY2017-2018, 2018-2019, 2019-2020 Three Year Plan TABLE OF CONTENTS Background and Overview..1 Message From The Mental Health Manager 4
City of Berkeley Mental Health Mental Health Services Act (MHSA) FY2017-2018, 2018-2019, 2019-2020 Three Year Plan TABLE OF CONTENTS Background and Overview..1 Message From The Mental Health Manager 4
Multi-Dimensional Family Therapy. Full Service Partnership Outcomes Report
 MHSA Multi-Dimensional Family Therapy Full Service Partnership Outcomes Report TABLE OF CONTENTS Enrollment 5 Discontinuance 5 Demographics 6-7 Length of Stay 8 Outcomes 9-11 Youth Outcome Questionnaire
MHSA Multi-Dimensional Family Therapy Full Service Partnership Outcomes Report TABLE OF CONTENTS Enrollment 5 Discontinuance 5 Demographics 6-7 Length of Stay 8 Outcomes 9-11 Youth Outcome Questionnaire
Note: Staff who work in case management programs should attend the AIDS Institute training, "Addressing Prevention in HIV Case Management.
 Addressing Prevention with HIV Positive Clients This one-day training will prepare participants to help people living with HIV to avoid sexual and substance use behaviors that can result in transmitting
Addressing Prevention with HIV Positive Clients This one-day training will prepare participants to help people living with HIV to avoid sexual and substance use behaviors that can result in transmitting
ViiV Healthcare Positive Action for Youth 2019 Amp Grant Program Lead Request for Proposals
 ViiV Healthcare Positive Action for Youth 2019 Amp Grant Program Lead Request for Proposals Table of Contents About ViiV Healthcare 2 Our Response 3 The Amp Grant 4 Objectives and Intended Outcomes 6 Budget
ViiV Healthcare Positive Action for Youth 2019 Amp Grant Program Lead Request for Proposals Table of Contents About ViiV Healthcare 2 Our Response 3 The Amp Grant 4 Objectives and Intended Outcomes 6 Budget