UBC Department of Urologic Sciences Lecture Series. Voiding Dysfunction & BPH
|
|
|
- Penelope O’Connor’
- 5 years ago
- Views:
Transcription



1 UBC Department of Urologic Sciences Lecture Series Voiding Dysfunction & BPH
2 Objectives Today 1. Anatomy of the lower urinary tract A) Innervation of the bladder B) Normal voiding 2. Classify Neurogenic Bladder 3. Classify Urinary Incontinence A) Rx for different types of incontinence 4. BPH & LUTS


3 Disclaimer: This is a lot of information to cover and we are unlikely to cover it all today These slides are to be utilized for your reference to guide your self study
4 Disclaimer: These concepts were all addressed in Year 1 FERGU block: Normal and Dysfunctional Voiding
5 MCC Objectives For LMCC Part 1 Objectives applicable to this lecture: Urinary Tract Obstruction

6 1 Male Anatomy

7 1 Female Anatomy
8 Anatomy Bladder Innervation Detrusor (parasympathetic S2,3,4) Trigone (sympathetic L1,2) Urethra Male Internal/Involuntary Sphincter (Sympathetic L1,2) Prostatic External/Voluntary Sphincter (Pudental S2,3,4) Membranous Bulbar Penile (spongy, pendulous etc)
9 Conceptual Neuro-anatomy Parasympathetic Sympathetic PEE STORE
 = Pee From pelvic splanchnic nerves cause detrusor to contract Somatic (voluntary) control Pudendal nerve(s2,3,4) External")
10 Anatomy Nerves Sympathetics(T11-L2) = Store From aortic and superior hypogastric plexis hypogastric nerves pelvic plexus cause detrusor relaxation and bladder neck contraction Parasympathetics(S2,3,4) = Pee From pelvic splanchnic nerves cause detrusor to contract Somatic (voluntary) control Pudendal nerve(s2,3,4) External Spincter
11 Anatomy Nerve Summary Parasympathetic S2,3,4 + Bladder contraction, relax sphincters Arise from sacral Cord Sympathetic L1,2 + Tight trigone, + internal sphincter tone, relax detrusor Arise from lumbar Somatic S2,3,4 + External sphincter tone
12 Conceptual Neuro-anatomy Parasympathetic Sympathetic PEE STORE
13 Objectives Today 1. Anatomy of the lower urinary tract A) Innervation of the bladder B) Normal voiding 2. Classify Neurogenic Bladder 3. Classify Urinary Incontinence A) Rx for different types of incontinence 4. BPH & LUTS
14 Voiding Filling Emptying Voiding
15 Voiding Normal Filling Requires: Accommodation of urine volume at low pressure (compliance) Closed bladder outlet No involuntary detrusor contractions Normal sensation of bladder filling
16 How does filling work? As bladder fills sympathetic reflex initiated to keep you dry! Stimulation of alpha adrenergic receptors at bladder neck increase resistance of bladder neck Activation of beta3 receptors in detrusor inhibiting contraction Direct inhibition of detrusor motor neurons in sacral spinal cord Gradual increase in urethral pressure as bladder fills due to pudendal nerve activation of external sphincter Formation of urethral mucousal seal
17 How does emptying work? Emptying Requires: Coordinated detrusor contraction of adequate magnitude Lowering of resistance at the level of the urinary sphincters (bladder outlet) Absence of obstruction (either anatomical or functional)
18 How does emptying work? Emptying Specifically: Increased intravesical pressure produces the sensation of distension I want to void!! Coordination of detrusor contraction and external sphincter relaxation Brain (pontine micturition center) inhibits the steady state spinal reflex of staying continent: Stimulates Parasympathetics contraction of detrusor Inhibits sympathetics = internal sphincter relaxation Inhibits pudendal = External Sphincter relaxation
19 V
20 Objectives Today 1. Anatomy of the lower urinary tract A) Innervation of the bladder B) Normal voiding 2. Classify Neurogenic Bladder 3. Classify Urinary Incontinence A) Rx for different types of incontinence 4. BPH & LUTS
21 Neurogenic Bladder Definition: dysfunction of the urinary bladder due to neurologic dysfunction or insult
22 Classifying Neurogenic Bladder Upper Motor Neuron Lower Motor Neuron spastic flaccid
23 Neurogenic UMN Upper Motor Neuron Cerebral Injury (stroke,tumour,brain injury) Normal function to inhibit reflexive bladder emptying Allows socially acceptable timing of voiding Dysfunction leads to loss of voluntary control of micturition Detrusor Overactivity
24 Neurogenic UMN Upper Motor Neuron Diseases Basal Ganglia disease (Parkinson s disease) Detrusor overactivity Contractions are short, relaxation of ext. sphincter is slowed urgency, urge incontinence, slow flow
25 Neurogenic UMN Upper Motor Neuron Diseases Suprasacral spinal cord damage Above T6 reflex micturition with detrusor-sphincter dyssynergia Below T6 reflex micturition with detrusor-sphincter synergia
26 Neurogenic UMN Upper Motor Neuron Diseases Cerebral Injury (stroke,tumour,brain injury) detrusor overactivity Basal Ganglia disease (Parkinson s disease) Detrusor overactivity Contractions are short, relaxation of ext. sphincter is slowed urgency, urge incontinence, slow flow Suprasacral spinal cord damage Above T6 reflex micturition with detrusor-sphincter dyssynergia Below T6 reflex micturition with detrusor-sphincter synergia
27 Neurogenic LMN Lower Motor Neuron Sacral Spinal cord damage Pelvic fracture, cauda equina Acontractile bladder, poor bladder sensation Peripheral Nerve Damage. Diabetes, pelvic surgery, XRT
28 Objectives Today 1. Anatomy of the lower urinary tract A) Innervation of the bladder B) Normal voiding 2. Classify Neurogenic Bladder 3. Classify Urinary Incontinence A) Rx for different types of incontinence 4. BPH & LUTS
29 Voiding Dysfunction
30 Voiding Dysfunction Etiology Failure to Store (AKA Incontinence) Detrusor overactivity Outlet incompetence Failure to Empty (AKA Retaining) Detrusor underactivity Outlet obstruction
31 Voiding Dysfunction Failure to Store Urge Incontinence -involuntary loss of urine with a strong desire to void. Stress Incontinence -loss of urine with increased intraabdominal pressure (cough, laugh, jump, rise to standing etc). Overflow Incontinence -loss of urine with bladder overdistension. Functional Incontinence -loss of urine associated with cognitive or physical impairment. Mixed Incontinence -combinations of above
32 Urge Incontinence Etiology Stone, UTI, Tumor, Overactive Bladder Investigations Hx, PE +/- urodynamics
33 Urge Incontinence Treatment Treat underlying cause Timed voiding Bladder training Biofeedback Pharmacologic Anticholinergic Oxybutinin TCA s Imipramine Surgical Bladder pacemaker Bladder denervation (rare) Bladder Augmentation Mitrofanoff Urinary Diversion
34 Stress Urinary Incontinence Etiology Urinary retention + incr abdo pressure Detrusor overactivity + incr abdo pressure Intrinsic sphincter deficiency Urethral hypermobility Often related to weak pelvic floor muscles Risk Factors Obesity, female, pregnancy, Vaginal deliveries, hysterectomy, prostatectomy, family Hx, caucasian, smoking, strenuous activity.
35 Stress Incontinence Treatment Kegel exercises Biofeedback Pharmacologic Alpha agonist (TCA, SSRI s, pseudoephedrine) incr sphincter tone and bladder outflow resistance Estrogen cream/pill Periurethral collagen injections Pessaries Surgery Bladder neck suspension (Burch, MMK) Urethral Slings (TVT, TOT) Artificial sphincter

36 Stress Incontinence Retropubic Bladder Neck Suspension (BURCH)
37 Urethral Slings Stress Incontinence

38 Artificial Sphincter Stress Incontinence
39 Overflow Incontinence Etiology Obstruction Treatment Treat underlying cause, eg BPH Acontractile Bladder Treatment Timed Voiding Double voiding Clean intermittent Catheterization Keep bladder volumes < 400ml and pt dry between catheterizations Indwelling Catheter Suprapubic Catheter
40 Transient Urinary Incontinence DIAPERS D I A P E R S Delirium cognitive dysfunction can impair voiding Infection bladder irritation Atrophic Vaginitis post menopausal may cause, nocturia, freq, urgency Pharmaceuticals/ Polypharmacy Excessive Urine production diuretics, untreated DM Restricted mobility Stool Impaction/Constipation impairs bladder function and pelvic floor muscle function
41 Transient Urinary Incontinence Pharmaceuticals Diuretics Anticholinergics impair bladder contraction Sedatives- bzd s delirium Narcotics impair bladder contraction, constipate, delirium Alpha agonist increase sphincter tone retention (nasal decongestants, imipramine) Alpha blocker lead to stress incontinence CCB s impair bladder contraction
42 Voiding Dysfunction Case So, you have this friend that has mentioned they occasionally have a case of wet undies

43 Dx?
44 Dx?
45 Voiding Evaluation History Urgency, frequency, dysuria Association with valsalva maneuver (sneeze,cough,lifting etc.) Medications (diuretics,benzos,narcotics) Fluid intake Back or head injury Parathesias, fecal incontinence Diabetes Other neurological disease (MS, Parkinson etc.)
46 Voiding Physical mental status, mobility abdominal and pelvic exam neurological exam anal tone, peri-anal sensation Bulbocavernosus reflex (S2,3,4) Investigations Urinalysis, serum creatinine Voiding Diary Post Void Residual (PVR; by U/S or catheterization) Urine cytology- pts with irritative voiding symptoms
47 Voiding Special Urology Tests Urodynamics Uroflowmetry Multichannel urodynamics Video-urodynamics Endoscopy (Cystoscopy) Upper tract imaging (renal ultrasound)
48 Voiding Indications for Referral: History or physical suggestive of neurologic disease Hematuria, recurrent UTIs, bladder stones, renal insufficiency (post-renal) with incontinence Elevated PVR, overflow incontinence Incontinence in pts with prior lower GU surgery Persistence of incontinence once reversible causes are corrected
49 Objectives Today 1. Anatomy of the lower urinary tract A) Innervation of the bladder B) Normal voiding 2. Classify Neurogenic Bladder 3. Classify Urinary Incontinence A) Rx for different types of incontinence 4. BPH & LUTS
50 Lower Urinary Tract Symptoms (LUTS).. A constellation of obstructive and irritative voiding disturbances of the lower urinary tract
51 LUTS LUTS Storage symptoms/ irritative Frequency, urgency, nocturia Voiding symptoms/ obstructive Hesitancy, slow stream, stuttering stream, straining to void, sense of incomplete emptying, doub;e voiding, post void dribble Dysuria and incontinence are not usually seen in uncomplicated BPH. Microhematuria is common
52 DDx of LUTS in Old Men Prostate: BPH, prostate cancer, prostatitis Bladder: cystitis, bladder tumour, bladder stone Urethra: urethral stricture, meatal stenosis, phimosis Neurologic: Parkinson s disease, stroke, Alzheimer s disease, spinal cord disease Other: Diabetes, sleep apnea, medication, diet, distal ureteral stone, pelvic mass
53 Evaluation of LUTS Hx PE IPSS/AUA symptom score General & GU exam, DRE, Focused Neurourologic Exam UA/ UCx
54 Evaluation of LUTS +/- Serum Creatinine +/- PSA +/- Post void residual (PVR) Measures amount of urine after voiding Large volume may suggest blockage Measured by bladder scanner (U/S) or Catheter +/- Abdo Ultrasound If hematuria, renal impairment, UTI s, atypical symptoms +/- Cystoscopy +/- Urodynamics If urinary retention, incontinence, atypical symptoms, neurological disease.
55 LUTS History Some specific questions to ask Hematuria Dysuria Incontinence Abdo/flank pain Previous transurethral surgery CNS, neurologic diseases (parkinson s, stroke) Meds (oral decongestants, antidepressants) DM Previous STD s or perineal trauma
56 LUTS Risk Factors Increasing age Weight gain and abdominal adiposity in adulthood may contribute to LUTS Excessive alcohol drinking (>75 g/day) was associated with LUTS and BP Smoking Nicotine increases sympathetic nervous system activity exacerbating LUTS
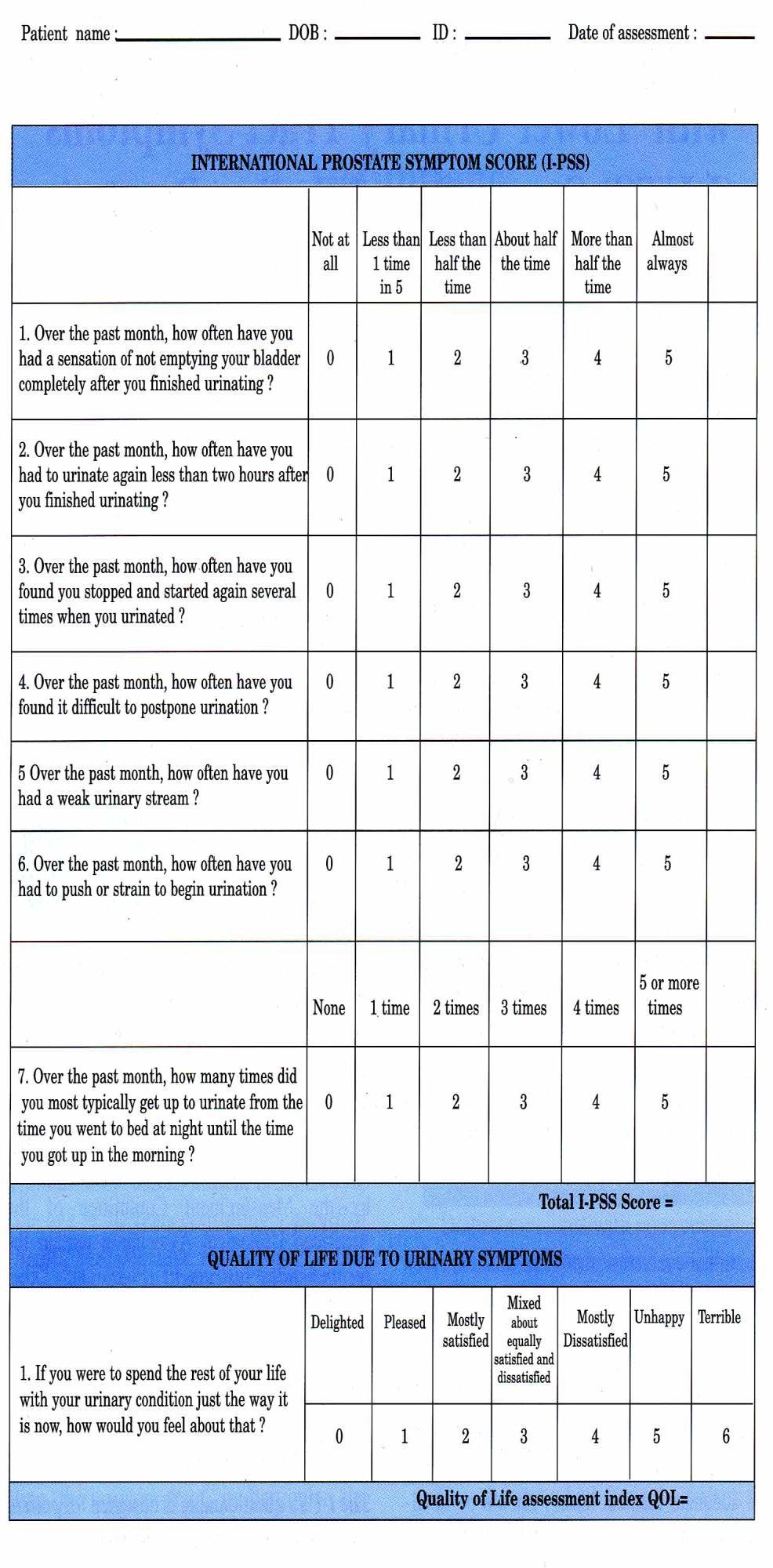
57 IPSS IPSS

58 LUTS DRE Healthy Symmetric soft Size walnut/20g at 20 years of age Unhealthy Hard Assymetrical Nodule enlarged

59 LUTS Size of gland NOT = LUTS severity

60 Benign Prostatic Hyperplasia BPH is prevalent and relevant Don t forget it.
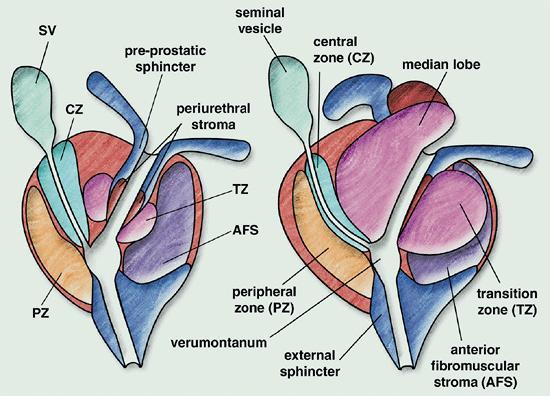
61 BPH Anatomy Prostate has 2 main types of tissue Stroma Smooth muscle Collagen Epithelium BPH occurs in transitional zone Prostate Cancer typically occurs in peripheral zones
62 LUTS
63 BPH Prevalence Increasing prevalence with age, 80% of 80yo s Pathophysiology Growth of stromal component of prostate Increased alpha 1A receptors leading to increased smooth muscle tone Size and degree of BOO (bladder outlet obstruction) do not fully correlate with degree of symptoms
 Renal failure Recurrent UTIs Bladder stones")
64 Complications of BPH Urinary retention (acute or chronic) Renal failure Recurrent UTIs Bladder stones Hematuria
65 Current practice The therapeutic cascade (step-up): lifestyle measures, phytotherapy alpha blockade 5 ARIs combination med therapy anticholinergics (occasionally) intermediate therapies (MIS) intervention under GA (TUR, etc)

66 Lifestyle Modification decrease fluids caffeine alcohol time diuretics decongestants exercise weight loss sleep apnea diet
67 BPH Pharmacotherapy Alpha Blockers Tamsulosin (Flomax): α1-subtype A selective; 0.4 mg daily; similar effectiveness but significantly fewer side effects compared to other α- blockers; retrograde ejaculation prevalent Silodosin (Rapaflo): α1-subtype A selective; 8 mg daily.se: retrograde ejaculation. Rapid onset action Terazosin (Hytrin): α1 selective; 2 mg 10 mg daily; approximately 70% of men experience satisfactory improvement in symptoms; common side effects include dizziness, fatigue and rhinorrhea Doxazosin (Cardura): α1 selective; 4 mg 8 mg daily; side effects similar to terazosin; effectiveness similar to terazosin Alfuzosin (Xatral): α1-subtype A selective; 10 mg daily; similar to flomax but less retrograde ejaculation
68 BPH Pharmacotherapy Alpha Blockers Side Effects Dizziness Asthenia (fatigue) Nasal congestion Retrograde ejaculation Orthostatic hypotension (uncommon) Syncope (rare)
69 BPH Pharmacotherapy 5 alpha reductase inbhibitors Finasteride Dutasteride Lets look at physiology...
70 Regulation of Cell Growth in the Prostate in BPH Serum testosterone (T) Serum DHT T Growth factors Increased Cell growth 5AR (1 and 2) DHT DHT-androgen receptor complex Unbalanced Prostate cell Cell death


71 Two 5a-reductase (5-AR) Isoenzymes Convert Testosterone to DHT Type II 5AR Testosterone DHT Type I 5AR Prostate enlargement Bartsch G et al. Eur Urol. 2000;37:

72 Different Type I and Type II 5-AR Isoenzyme Inhibition by Dutasteride and Finasteride Type II 5AR Dutasteride Finasteride Prostate volume reduced Testosterone DHT Type I 5AR Dutasteride Bartsch G et al. Eur Urol. 2000;37:
73 BPH Pharmacotherapy 5 alpha reductase inhibitors: Reduce rate of Acute Urinary Retention Decrease rate of surgery over 6 years Work best in larger prostates Decrease size by 25% Decrease PSA by 50% Slower onset of action than alpha blockers
74 Incidence of Acute Urinary Retention at Year 4 by Baseline Prostate Volume Tertile = Reduction in risk over 4 years (Life Table Analysis) Revised Nov 2008

75 Incidence of BPH-Related Surgery at Year 4 by Baseline PSA Tertile = Reduction in risk over 4 years (Life Table Analysis)
76 BPH Pharmacology 5 Alpha reductase inhibitors Side Effects Erectile Dysfunction <5% Decreased libido <4% Decreased Volume Ejaculate < 3% Gynecomastia <1%
77 BPH Pharmacotherapy Combination of Alpha Blockers and 5 Alpha reductase inhibitors Long and short of it is: IF prostate small and PSA low Use alpha blocker IF prostate large and PSA high Use Combo
78 BPH and Surgery Surgical Options Minimally invasive therapy Injections eg. Botox, alcohol Photodynamic therapy (PTD) Microwave heat treatment High Intensity Frequency Ultrasound (HIFU) Needle ablation / radio-wave treatment Electrovaporization of prostate Green light Laser therapy Transurethral resection (TURP) Open prostatectomy
79 BPH and Surgery Indications for surgery Symptoms refractory to medical therapy Recurrent UTI Urinary Retention Recurrent Hematuria Renal Impairment Bladder Calculi
80 TURP Gold Standard TURP Transurethral Resection of prostate Electrocautery resection of of prostatic tissue Endoscopic Pt stay is usually 1 night
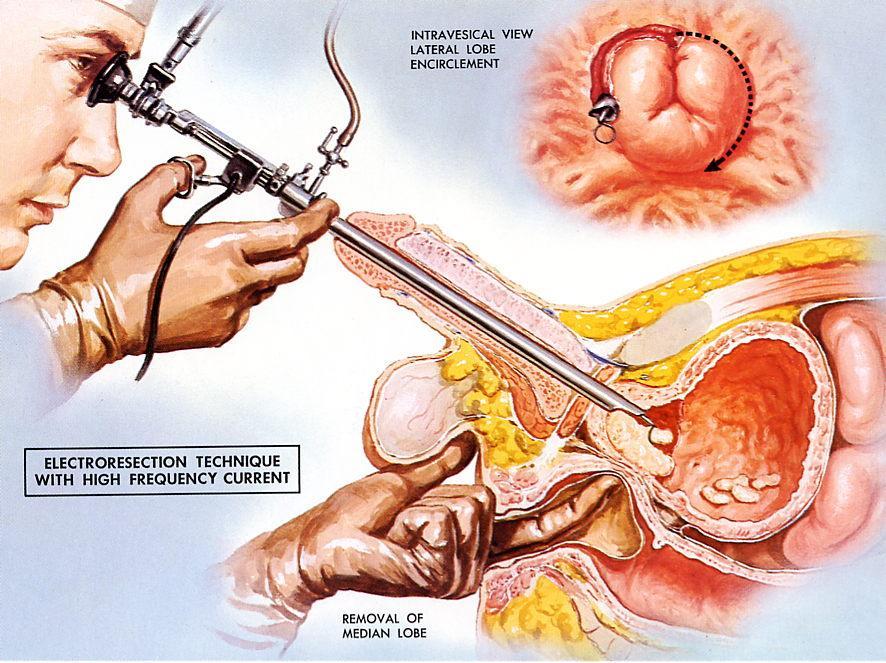
81 TURP


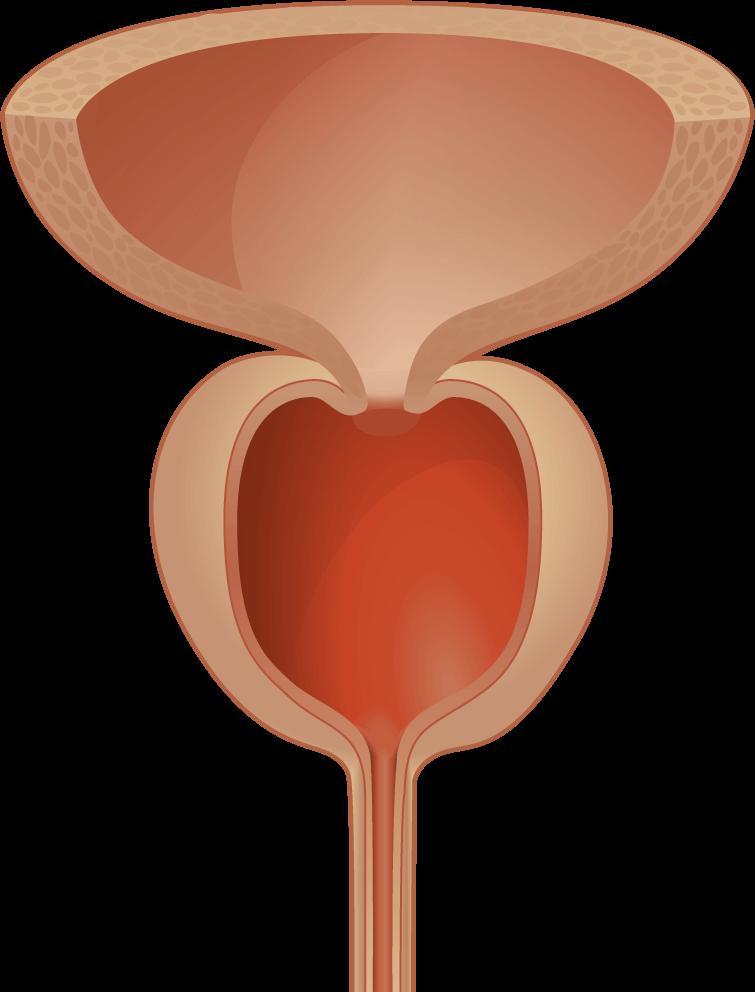
82 Before and After TURP BEFORE AFTER
83 TURP Complications Bleeding Perforation TUR Syndrome With prolonged procedure Absorption of hypotonic solution leads to: Hyponatremia, hypervolemia, hypertension, mental confusion, seizures, nausea, vomiting, visual disturbances Occurs in < 2% of cases


84 Other Surgical Options Green light laser

85 Other Surgical Options Open Prostatectomy For LARGE prostates
86 Objectives Today 1. Anatomy of the lower urinary tract A) Innervation of the bladder B) Normal voiding 2. Classify Neurogenic Bladder 3. Classify Urinary Incontinence A) Rx for different types of incontinence 4. BPH & LUTS
Lower Urinary Tract Symptoms K Kuruvilla Zachariah Associate Specialist
 Lower Urinary Tract Symptoms K Kuruvilla Zachariah Associate Specialist Lower Urinary Tract Symptoms Storage Symptoms Frequency, urgency, incontinence, Nocturia Voiding Symptoms Hesitancy, poor flow, intermittency,
Lower Urinary Tract Symptoms K Kuruvilla Zachariah Associate Specialist Lower Urinary Tract Symptoms Storage Symptoms Frequency, urgency, incontinence, Nocturia Voiding Symptoms Hesitancy, poor flow, intermittency,
MANAGING BENIGN PROSTATIC HYPERTROPHY IN PRIMARY CARE DR GEORGE G MATHEW CONSULTANT FAMILY PHYSICIAN FELLOW IN SEXUAL & REPRODUCTIVE HEALTH
 MANAGING BENIGN PROSTATIC HYPERTROPHY IN PRIMARY CARE DR GEORGE G MATHEW CONSULTANT FAMILY PHYSICIAN FELLOW IN SEXUAL & REPRODUCTIVE HEALTH INTRODUCTION (1) Part of male sexual reproductive organ Size
MANAGING BENIGN PROSTATIC HYPERTROPHY IN PRIMARY CARE DR GEORGE G MATHEW CONSULTANT FAMILY PHYSICIAN FELLOW IN SEXUAL & REPRODUCTIVE HEALTH INTRODUCTION (1) Part of male sexual reproductive organ Size
Benign Prostatic Hyperplasia (BPH):
:") Benign Prostatic Hyperplasia (BPH): Evidence Based Guidelines for Primary Care Providers Jeanne Martin, DNP, ANP-BC Objectives 1. Understand the pathophysiology and prevalence of BPH 2. Select the appropriate
Benign Prostatic Hyperplasia (BPH): Evidence Based Guidelines for Primary Care Providers Jeanne Martin, DNP, ANP-BC Objectives 1. Understand the pathophysiology and prevalence of BPH 2. Select the appropriate
Management of LUTS after TURP and MIT
 Management of LUTS after TURP and MIT Hong Sup Kim Konkuk University TURP & MIT TURP : Gold standard MIT TUIP TUNA TUMT HIFU LASER Nd:YAG, ILC, HoLRP, KTP LUTS after TURP and MIT Improved : about 70% Persistent
Management of LUTS after TURP and MIT Hong Sup Kim Konkuk University TURP & MIT TURP : Gold standard MIT TUIP TUNA TUMT HIFU LASER Nd:YAG, ILC, HoLRP, KTP LUTS after TURP and MIT Improved : about 70% Persistent
Benign Prostatic Hyperplasia. Jay Lee, MD, FRCSC Clinical Associate Professor University of Calgary
 Benign Prostatic Hyperplasia Jay Lee, MD, FRCSC Clinical Associate Professor University of Calgary Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied,
Benign Prostatic Hyperplasia Jay Lee, MD, FRCSC Clinical Associate Professor University of Calgary Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied,
Voiding Dysfunction Block lecture, 5 th year student. Choosak Pripatnanont, Department of Surgery, PSU.
 Voiding Dysfunction 2009 Block lecture, 5 th year student. Choosak Pripatnanont, Department of Surgery, PSU. Objectives Understand and explain physiologic function and dysfunction of lower urinary tract.
Voiding Dysfunction 2009 Block lecture, 5 th year student. Choosak Pripatnanont, Department of Surgery, PSU. Objectives Understand and explain physiologic function and dysfunction of lower urinary tract.
Lower Urinary Tract Symptoms (LUTS) and Nurse-Led Clinics. Sean Diver Urology Advanced Nurse Practitioner candidate Letterkenny University Hospital
 and Nurse-Led Clinics. Sean Diver Urology Advanced Nurse Practitioner candidate Letterkenny University Hospital") Lower Urinary Tract Symptoms (LUTS) and Nurse-Led Clinics Sean Diver Urology Advanced Nurse Practitioner candidate Letterkenny University Hospital 01/02/2018 Lower Urinary Tract Symptoms LUTS - one of
Lower Urinary Tract Symptoms (LUTS) and Nurse-Led Clinics Sean Diver Urology Advanced Nurse Practitioner candidate Letterkenny University Hospital 01/02/2018 Lower Urinary Tract Symptoms LUTS - one of
The Neurogenic Bladder
 The Neurogenic Bladder Outline Brandon Haynes, MD Resident Physician Department of Urology Jelena Svircev, MD Assistant Professor Department of Rehabilitation Medicine Anatomy and Bladder Physiology Bladder
The Neurogenic Bladder Outline Brandon Haynes, MD Resident Physician Department of Urology Jelena Svircev, MD Assistant Professor Department of Rehabilitation Medicine Anatomy and Bladder Physiology Bladder
Victoria Sharp, MD, MBA, FAAFP. Clinical Professor of Urology and Family Medicine
 Victoria Sharp, MD, MBA, FAAFP Clinical Professor of Urology and Family Medicine Victoria Sharp, MD, MBA, FAAFP Market Chief Medial Officer AmeriHealth Caritas Family of Companies Office phone: (515) 330-3740
Victoria Sharp, MD, MBA, FAAFP Clinical Professor of Urology and Family Medicine Victoria Sharp, MD, MBA, FAAFP Market Chief Medial Officer AmeriHealth Caritas Family of Companies Office phone: (515) 330-3740
Prostate Disease. Chad Baxter, MD
 Prostate Disease Chad Baxter, MD Managing BPH and LUTS Chad Baxter, MD Department of Urology cbaxter@mednet.ucla.edu 33 nd Annual UCLA Intensive Course in Geriatric Medicine & Board Review Prevalence of
Prostate Disease Chad Baxter, MD Managing BPH and LUTS Chad Baxter, MD Department of Urology cbaxter@mednet.ucla.edu 33 nd Annual UCLA Intensive Course in Geriatric Medicine & Board Review Prevalence of
Neurogenic bladder. Neurogenic bladder is a type of dysfunction of the bladder due to neurological disorder.
 Definition: Neurogenic bladder Neurogenic bladder is a type of dysfunction of the bladder due to neurological disorder. Types: Nervous system diseases: Congenital: like myelodysplasia like meningocele.
Definition: Neurogenic bladder Neurogenic bladder is a type of dysfunction of the bladder due to neurological disorder. Types: Nervous system diseases: Congenital: like myelodysplasia like meningocele.
Disclosures. Geriatric Incontinence and Voiding Dysfunction. Agenda. Agenda. UI: a Geriatric Syndrome. Geriatric Syndromes 9/7/2018.
 Disclosures Geriatric Incontinence and Voiding Dysfunction None Shachi Tyagi MD, MS Assistant Professor Division of Geriatric Medicine University of Pittsburgh Medical Center UI: a Geriatric Syndrome Geriatric
Disclosures Geriatric Incontinence and Voiding Dysfunction None Shachi Tyagi MD, MS Assistant Professor Division of Geriatric Medicine University of Pittsburgh Medical Center UI: a Geriatric Syndrome Geriatric
URGE MOTOR INCONTINENCE
 URGE MOTOR INCONTINENCE URGE INCONTINENCE COMMONEST TYPE IN ELDERLY WOMEN Causes: 1 - Defects in CNS regulation Stroke Parkinson s disease Dementia (Alzheimer s and other types) Normopressure hydrocephalus
URGE MOTOR INCONTINENCE URGE INCONTINENCE COMMONEST TYPE IN ELDERLY WOMEN Causes: 1 - Defects in CNS regulation Stroke Parkinson s disease Dementia (Alzheimer s and other types) Normopressure hydrocephalus
Incontinence. When I was given this topic in urology to discuss with you today I
 Incontinence When I was given this topic in urology to discuss with you today I was slightly disappointed. I personally see mostly men for problems such as stones, benign prostatic hyperplasia, prostate
Incontinence When I was given this topic in urology to discuss with you today I was slightly disappointed. I personally see mostly men for problems such as stones, benign prostatic hyperplasia, prostate
NEUROGENIC BLADDER. Dr Harriet Grubb Dr Alison Seymour Dr Alexander Joseph
 NEUROGENIC BLADDER Dr Harriet Grubb Dr Alison Seymour Dr Alexander Joseph OUTLINE Definition Anatomy and physiology of bladder function Types of neurogenic bladder Assessment and management Complications
NEUROGENIC BLADDER Dr Harriet Grubb Dr Alison Seymour Dr Alexander Joseph OUTLINE Definition Anatomy and physiology of bladder function Types of neurogenic bladder Assessment and management Complications
MODULE 3: BENIGN PROSTATIC HYPERTROPHY
 MODULE 3: BENIGN PROSTATIC HYPERTROPHY KEYWORDS: Prostatic hypertrophy, prostatic hyperplasia, PSA, voiding dysfunction, lower urinary tract symptoms (LUTS) At the end of this clerkship, the medical student
MODULE 3: BENIGN PROSTATIC HYPERTROPHY KEYWORDS: Prostatic hypertrophy, prostatic hyperplasia, PSA, voiding dysfunction, lower urinary tract symptoms (LUTS) At the end of this clerkship, the medical student
Incontinence: Risks, Causes and Care
 Welcome To Incontinence: Risks, Causes and Care Presented by Kamal Masaki, MD Professor and Chair Department of Geriatric Medicine John A. Burns School of Medicine, UH Manoa September 5, 2018 10:00 11:00
Welcome To Incontinence: Risks, Causes and Care Presented by Kamal Masaki, MD Professor and Chair Department of Geriatric Medicine John A. Burns School of Medicine, UH Manoa September 5, 2018 10:00 11:00
Neuropathic Bladder. Magda Kujawa Consultant Urologist Stockport NHS Foundation Trust 12/03/2014
 Neuropathic Bladder Magda Kujawa Consultant Urologist Stockport NHS Foundation Trust 12/03/2014 Plan Physiology- bladder and sphincter behaviour in neurological disease Clinical consequences of Symptoms
Neuropathic Bladder Magda Kujawa Consultant Urologist Stockport NHS Foundation Trust 12/03/2014 Plan Physiology- bladder and sphincter behaviour in neurological disease Clinical consequences of Symptoms
Overactive Bladder: Diagnosis and Approaches to Treatment
 Overactive Bladder: Diagnosis and Approaches to Treatment A Hidden Condition* Many Many patients self-manage by voiding frequently, reducing fluid intake, and wearing pads Nearly Nearly two-thirds thirds
Overactive Bladder: Diagnosis and Approaches to Treatment A Hidden Condition* Many Many patients self-manage by voiding frequently, reducing fluid intake, and wearing pads Nearly Nearly two-thirds thirds
Index. urologic.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Ablative therapies, transurethral needle ablation, Adverse events, sexual side effects of BPH Aging, and incidence of BPH associated with
Index Note: Page numbers of article titles are in boldface type. A Ablative therapies, transurethral needle ablation, Adverse events, sexual side effects of BPH Aging, and incidence of BPH associated with
Objectives. Prevalence of Urinary Incontinence URINARY INCONTINENCE: EVALUATION AND CURRENT TREATMENT OPTIONS
 URINARY INCONTINENCE: EVALUATION AND CURRENT TREATMENT OPTIONS Lisa S Pair, MSN, CRNP Division of Urogynecology and Pelvic Reconstructive Surgery Department of Obstetrics and Gynecology University of Alabama
URINARY INCONTINENCE: EVALUATION AND CURRENT TREATMENT OPTIONS Lisa S Pair, MSN, CRNP Division of Urogynecology and Pelvic Reconstructive Surgery Department of Obstetrics and Gynecology University of Alabama
Urodynamics in Neurological Lower Urinary Tract Dysfunction. Mr Chris Harding Consultant Urologist Freeman Hospital Newcastle-upon-Tyne
 Urodynamics in Neurological Lower Urinary Tract Dysfunction Mr Chris Harding Consultant Urologist Freeman Hospital Newcastle-upon-Tyne Learning Objectives Review functional neurology relevant to lower
Urodynamics in Neurological Lower Urinary Tract Dysfunction Mr Chris Harding Consultant Urologist Freeman Hospital Newcastle-upon-Tyne Learning Objectives Review functional neurology relevant to lower
Male Lower Urinary Tract Symptoms: Management in primary care and beyond. Daniel Cohen PhD FRCS(Urol) Consultant Urological Surgeon
 Consultant Urological Surgeon") Male Lower Urinary Tract Symptoms: Management in primary care and beyond Daniel Cohen PhD FRCS(Urol) Consultant Urological Surgeon 1 LUTS Very common: 1/3 men over age of 50 have moderate to severe LUTS
Male Lower Urinary Tract Symptoms: Management in primary care and beyond Daniel Cohen PhD FRCS(Urol) Consultant Urological Surgeon 1 LUTS Very common: 1/3 men over age of 50 have moderate to severe LUTS
Benign Prostatic Hyperplasia (BPH)
") Benign Prostatic Hyperplasia (BPH) Definition Prostate gland enlargement is a common condition as men get older. Also called benign prostatic hyperplasia (BPH), prostate gland enlargement can cause bothersome
Benign Prostatic Hyperplasia (BPH) Definition Prostate gland enlargement is a common condition as men get older. Also called benign prostatic hyperplasia (BPH), prostate gland enlargement can cause bothersome
Overactive Bladder Syndrome
 Overactive Bladder Syndrome behavioural modifications to pharmacological and surgical treatments Dr Jos Jayarajan Urologist Austin Health, Eastern Health Warringal Private, Northpark Private, Epworth Overactive
Overactive Bladder Syndrome behavioural modifications to pharmacological and surgical treatments Dr Jos Jayarajan Urologist Austin Health, Eastern Health Warringal Private, Northpark Private, Epworth Overactive
Pelvic Floor Therapy for the Neurologic Client Carina Siracusa, PT, DPT, WCS
 Pelvic Floor Therapy for the Neurologic Client Carina Siracusa, PT, DPT, WCS OhioHealth, Columbus Ohio Disclosures I have nothing to disclose Objectives Describe the role of a pelvic floor therapist in
Pelvic Floor Therapy for the Neurologic Client Carina Siracusa, PT, DPT, WCS OhioHealth, Columbus Ohio Disclosures I have nothing to disclose Objectives Describe the role of a pelvic floor therapist in
Various Types. Ralph Boling, DO, FACOG
 Various Types Ralph Boling, DO, FACOG The goal of this lecture is to increase assessment and treatment abilities for physicians managing urinary incontinence (UI) patients. 1. Effectively communicate with
Various Types Ralph Boling, DO, FACOG The goal of this lecture is to increase assessment and treatment abilities for physicians managing urinary incontinence (UI) patients. 1. Effectively communicate with
Dr. Aso Urinary Symptoms
 Haematuria The presence of blood in the urine (haematuria) is always abnormal and may be the only indication of pathology in the urinary tract. False positive stick tests and the discolored urine caused
Haematuria The presence of blood in the urine (haematuria) is always abnormal and may be the only indication of pathology in the urinary tract. False positive stick tests and the discolored urine caused
TREATMENT METHODS FOR DISORDERS OF SMALL ANIMAL BLADDER FUNCTION
 Vet Times The website for the veterinary profession https://www.vettimes.co.uk TREATMENT METHODS FOR DISORDERS OF SMALL ANIMAL BLADDER FUNCTION Author : SIMONA T RADAELLI Categories : Vets Date : July
Vet Times The website for the veterinary profession https://www.vettimes.co.uk TREATMENT METHODS FOR DISORDERS OF SMALL ANIMAL BLADDER FUNCTION Author : SIMONA T RADAELLI Categories : Vets Date : July
Causes of Transient Incontinence. Geriatrics: Urinary Incontinence, Dementia, and Delirium. Classification of Established Incontinence
 Causes of Transient Geriatrics: Urinary, Dementia, and Delirium Carla Zeilmann, PharmD, BCPS St. Louis College of Pharmacy Therapeutics 3 Fall 2003 D delirium I infection A atrophic urethritis and vaginitis
Causes of Transient Geriatrics: Urinary, Dementia, and Delirium Carla Zeilmann, PharmD, BCPS St. Louis College of Pharmacy Therapeutics 3 Fall 2003 D delirium I infection A atrophic urethritis and vaginitis
Management of Voiding Problems in Older Men. Dr. John Fenn Consultant, QEH 10 th October, 2005
 Management of Voiding Problems in Older Men Dr. John Fenn Consultant, QEH 10 th October, 2005 Voiding Problems Poor stream Hesitancy Straining Incomplete emptying Intermittent micturition Terminal dribbling
Management of Voiding Problems in Older Men Dr. John Fenn Consultant, QEH 10 th October, 2005 Voiding Problems Poor stream Hesitancy Straining Incomplete emptying Intermittent micturition Terminal dribbling
Disease Management. Incontinence Care. Chan Sau Kuen Continence Nurse Consultant United Christian Hospital 14/11/09
 Disease Management in Incontinence Care Chan Sau Kuen Continence Nurse Consultant United Christian Hospital 14/11/09 What is incontinence? Definition of Incontinence - Is the compliant of any involuntary
Disease Management in Incontinence Care Chan Sau Kuen Continence Nurse Consultant United Christian Hospital 14/11/09 What is incontinence? Definition of Incontinence - Is the compliant of any involuntary
Canadian Undergraduate Urology Curriculum (CanUUC): Prostate Diseases
: Prostate Diseases") Canadian Undergraduate Urology Curriculum (CanUUC): Prostate Diseases LUTS/Benign Prostate Hyperplasia Objectives 1. List the lower urinary tract symptoms (LUTS) found in men with BPH. 2. List the differential
Canadian Undergraduate Urology Curriculum (CanUUC): Prostate Diseases LUTS/Benign Prostate Hyperplasia Objectives 1. List the lower urinary tract symptoms (LUTS) found in men with BPH. 2. List the differential
URINARY INCONTINENCE. Urology Division, Surgery Department Medical Faculty, University of Sumatera Utara
 URINARY INCONTINENCE Urology Division, Surgery Department Medical Faculty, University of Sumatera Utara Definition The involuntary loss of urine May denote a symptom, a sign or a condition Symptom the
URINARY INCONTINENCE Urology Division, Surgery Department Medical Faculty, University of Sumatera Utara Definition The involuntary loss of urine May denote a symptom, a sign or a condition Symptom the
Male LUTS. Dr. Brian Ho. Division of Urology Department of Surgery Queen Mary Hospital
 Male LUTS Dr. Brian Ho Division of Urology Department of Surgery Queen Mary Hospital Mr. Siu M/78 Known to have HT & DM since 2008 on follow up with General ut-patient Clinic (GPC) Noticed to have worsening
Male LUTS Dr. Brian Ho Division of Urology Department of Surgery Queen Mary Hospital Mr. Siu M/78 Known to have HT & DM since 2008 on follow up with General ut-patient Clinic (GPC) Noticed to have worsening
What should we consider before surgery? BPH with bladder dysfunction. Inje University Sanggye Paik Hospital Sung Luck Hee
 What should we consider before surgery? BPH with bladder dysfunction Inje University Sanggye Paik Hospital Sung Luck Hee Diagnostic tests in three categories Recommendation: there is evidence to support
What should we consider before surgery? BPH with bladder dysfunction Inje University Sanggye Paik Hospital Sung Luck Hee Diagnostic tests in three categories Recommendation: there is evidence to support
All about the Prostate
 MEN S HEALTH Dr Nick Pendleton January 16 th 2018 All about the Prostate 1 What does it do? Functions of the Prostate 1. Secretes Prostatic Fluid slightly alkaline fluid, 30% of volume of seminal fluid,
MEN S HEALTH Dr Nick Pendleton January 16 th 2018 All about the Prostate 1 What does it do? Functions of the Prostate 1. Secretes Prostatic Fluid slightly alkaline fluid, 30% of volume of seminal fluid,
Urogynecology in EDS. Joan L. Blomquist, MD Greater Baltimore Medical Center August 2018
 Urogynecology in EDS Joan L. Blomquist, MD Greater Baltimore Medical Center August 2018 One in three like me Voiding Issues Frequency/Urgency Urinary Incontinence neurogenic bladder Neurologic supply
Urogynecology in EDS Joan L. Blomquist, MD Greater Baltimore Medical Center August 2018 One in three like me Voiding Issues Frequency/Urgency Urinary Incontinence neurogenic bladder Neurologic supply
Urogynaecology. Colm McAlinden
 Urogynaecology Colm McAlinden Definitions Urinary incontinence compliant of any involuntary leakage of urine with many different causes Two main types: Stress Urge Definitions Nocturia: More than a single
Urogynaecology Colm McAlinden Definitions Urinary incontinence compliant of any involuntary leakage of urine with many different causes Two main types: Stress Urge Definitions Nocturia: More than a single
Incontinence; Lets talk about it. Karanvir Virk M.D. Minimally Invasive and Pelvic Reconstructive Surgery
 Incontinence; Lets talk about it Karanvir Virk M.D. Minimally Invasive and Pelvic Reconstructive Surgery Select the most appropriate subtitle for this talk A: Bladders gone wild! B: There s no such thing
Incontinence; Lets talk about it Karanvir Virk M.D. Minimally Invasive and Pelvic Reconstructive Surgery Select the most appropriate subtitle for this talk A: Bladders gone wild! B: There s no such thing
What is Benign Prostatic Hyperplasia (BPH)?
?") What is Benign Prostatic Hyperplasia (BPH)? Benign prostatic hyperplasia (BPH) is an enlarged prostate. The prostate goes through two main growth periods as a man ages. The first occurs early in puberty,
What is Benign Prostatic Hyperplasia (BPH)? Benign prostatic hyperplasia (BPH) is an enlarged prostate. The prostate goes through two main growth periods as a man ages. The first occurs early in puberty,
The Enlarged Prostate Symptoms, Diagnosis and Treatment
 The Enlarged Prostate Symptoms, Diagnosis and Treatment MAC00031-01 Rev G Financial support for this seminar has been provided by NeoTract, Inc., the manufacturer of the UroLift System. 1 Today s Agenda
The Enlarged Prostate Symptoms, Diagnosis and Treatment MAC00031-01 Rev G Financial support for this seminar has been provided by NeoTract, Inc., the manufacturer of the UroLift System. 1 Today s Agenda
Benign Prostatic Hyperplasia. Management of Benign Prostatic Hyperplasia. Goals of Therapy
 Benign Prostatic Hyperplasia Management of Benign Prostatic Hyperplasia Goals of Therapy Improve or abolish lower urinary tract symptoms (LUTS) Prevent or delay clinical progression of benign prostatic
Benign Prostatic Hyperplasia Management of Benign Prostatic Hyperplasia Goals of Therapy Improve or abolish lower urinary tract symptoms (LUTS) Prevent or delay clinical progression of benign prostatic
Overview. Urology Dine and Learn: Erectile Dysfunction & Benign Prostatic Hyperplasia. Iain McAuley September 15, 2014
 Urology Dine and Learn: Erectile Dysfunction & Benign Prostatic Hyperplasia Iain McAuley September 15, 2014 Overview Review of the most recent guidelines for ED and BPH ED Guidelines CUA 2006 AUA 2011
Urology Dine and Learn: Erectile Dysfunction & Benign Prostatic Hyperplasia Iain McAuley September 15, 2014 Overview Review of the most recent guidelines for ED and BPH ED Guidelines CUA 2006 AUA 2011
Elimination Patterns: Bladder
 Elimination Patterns: Bladder CRRN Review Material Christa Carter, RN, BSN, CRRN Objectives Identify different types of neurogenic bladder Identify different types of incontinence Identify at least three
Elimination Patterns: Bladder CRRN Review Material Christa Carter, RN, BSN, CRRN Objectives Identify different types of neurogenic bladder Identify different types of incontinence Identify at least three
Guidelines on Urinary Incontinence
 Guidelines on Urinary Incontinence J. Thüroff (chairman), P. Abrams, K.E. Andersson, W. Artibani, E. Chartier-Kastler, C. Hampel, Ph. van Kerrebroeck European Association of Urology 2006 TABLE OF CONTENTS
Guidelines on Urinary Incontinence J. Thüroff (chairman), P. Abrams, K.E. Andersson, W. Artibani, E. Chartier-Kastler, C. Hampel, Ph. van Kerrebroeck European Association of Urology 2006 TABLE OF CONTENTS
Diagnosis and Mangement of Nocturia in Adults
 Diagnosis and Mangement of Nocturia in Adults Christopher Chapple Professor of Urology Sheffield Teaching Hospitals University of Sheffield Sheffield Hallam University UK 23 rd October 2015 Terminology
Diagnosis and Mangement of Nocturia in Adults Christopher Chapple Professor of Urology Sheffield Teaching Hospitals University of Sheffield Sheffield Hallam University UK 23 rd October 2015 Terminology
Physiology & Neurophysiology of lower U.T.
 Physiology & Neurophysiology of lower U.T. Classification of voiding dysfunction Evaluation of a child with voiding dysfunction Management Storage Ø Adequate volume of urine Ø At LOW pressure Ø With NO
Physiology & Neurophysiology of lower U.T. Classification of voiding dysfunction Evaluation of a child with voiding dysfunction Management Storage Ø Adequate volume of urine Ø At LOW pressure Ø With NO
Management of LUTS. Simon Woodhams February 2012
 Management of LUTS Simon Woodhams February 2012 The management of lower urinary tract symptoms (LUTS) in men Implementing NICE guidance May 2010 NICE clinical guideline 97 Background Lower urinary tract
Management of LUTS Simon Woodhams February 2012 The management of lower urinary tract symptoms (LUTS) in men Implementing NICE guidance May 2010 NICE clinical guideline 97 Background Lower urinary tract
Ben Herbert Alex Wojtowicz
 Ben Herbert Alex Wojtowicz 54 year old female presenting with: Dragging sensation Urinary incontinence Some faecal incontinence HPC Since May 14 had noticed a mass protruding from the vagina when going
Ben Herbert Alex Wojtowicz 54 year old female presenting with: Dragging sensation Urinary incontinence Some faecal incontinence HPC Since May 14 had noticed a mass protruding from the vagina when going
Diagnostic approach to LUTS in men. Prof Dato Dr. Zulkifli Md Zainuddin Consultant Urologist / Head Of Urology Unit UKM Medical Center
 Diagnostic approach to LUTS in men Prof Dato Dr. Zulkifli Md Zainuddin Consultant Urologist / Head Of Urology Unit UKM Medical Center Classification of LUTS Storage symptoms Voiding symptoms Post micturition
Diagnostic approach to LUTS in men Prof Dato Dr. Zulkifli Md Zainuddin Consultant Urologist / Head Of Urology Unit UKM Medical Center Classification of LUTS Storage symptoms Voiding symptoms Post micturition
Management of Female Stress Incontinence
 Management of Female Stress Incontinence Dr. Arvind Goyal Associate Professor (Urology& Renal Transplant) Dayanand Medical College & Hospital, Ludhiana, Punjab, India Stress Incontinence Involuntary loss
Management of Female Stress Incontinence Dr. Arvind Goyal Associate Professor (Urology& Renal Transplant) Dayanand Medical College & Hospital, Ludhiana, Punjab, India Stress Incontinence Involuntary loss
Spinal Cord Injury. R Hamid Consultant Neuro-Urologist London Spinal Injuries Unit, Stanmore & National Hospital for Neurology & Neurosurgery, UCLH
 Spinal Cord Injury R Hamid Consultant Neuro-Urologist London Spinal Injuries Unit, Stanmore & National Hospital for Neurology & Neurosurgery, UCLH SCI 800 1000 new cases per year in UK Car accidents 35%
Spinal Cord Injury R Hamid Consultant Neuro-Urologist London Spinal Injuries Unit, Stanmore & National Hospital for Neurology & Neurosurgery, UCLH SCI 800 1000 new cases per year in UK Car accidents 35%
R. Matthew Smith M.D. Mercy Urology
 R. Matthew Smith M.D. Mercy Urology None Disclosures Goals Update growth of Mercy Urology Clinic Quick Review of Hematuria and PSA Present common urologic complaints seen by the primary care physician
R. Matthew Smith M.D. Mercy Urology None Disclosures Goals Update growth of Mercy Urology Clinic Quick Review of Hematuria and PSA Present common urologic complaints seen by the primary care physician
Geriatric Urinary Incontinence
 Geriatric Urinary Incontinence Neil M. Resnick, MD Thomas Detre Professor of Medicine Chief, Division of Geriatric Medicine University of Pittsburgh/UPMC UI: The Problem Prevalence in elderly 33% Morbidity
Geriatric Urinary Incontinence Neil M. Resnick, MD Thomas Detre Professor of Medicine Chief, Division of Geriatric Medicine University of Pittsburgh/UPMC UI: The Problem Prevalence in elderly 33% Morbidity
LUTS A plea for a holistic approach. HUBERT GALLAGHER, MCh; FRCSI, FRCSI(Urol) Head of Urology Beacon Hospital
 Head of Urology Beacon Hospital") LUTS A plea for a holistic approach. HUBERT GALLAGHER, MCh; FRCSI, FRCSI(Urol) Head of Urology Beacon Hospital LUTS- Classification Men LUTS can be divided into: Storage Voiding Frequency Nocturia Urgency
LUTS A plea for a holistic approach. HUBERT GALLAGHER, MCh; FRCSI, FRCSI(Urol) Head of Urology Beacon Hospital LUTS- Classification Men LUTS can be divided into: Storage Voiding Frequency Nocturia Urgency
Table 1. International Consultation on Incontinence recommendations for frail older adults
 Table 1. International Consultation on Incontinence recommendations for frail older adults Clinicians need to assess and manage co-existing co morbid conditions which are known to have an impact on continence
Table 1. International Consultation on Incontinence recommendations for frail older adults Clinicians need to assess and manage co-existing co morbid conditions which are known to have an impact on continence
Urinary Incontinence for the Primary Care Provider
 Urinary Incontinence for the Primary Care Provider Diana J Scott FNP-BC https://youtu.be/gmzaue1ojn4 1 Assessment of Urinary Incontinence Urge Stress Mixed Other overflow, postural, continuous, insensible,
Urinary Incontinence for the Primary Care Provider Diana J Scott FNP-BC https://youtu.be/gmzaue1ojn4 1 Assessment of Urinary Incontinence Urge Stress Mixed Other overflow, postural, continuous, insensible,
Evaluation and Treatment of Incontinence
 Evaluation and Treatment of Incontinence Classification of Incontinence Failure to empty: Overflow incontinence Failure to store Stress Incontinence Urge Incontinence Physiology of voiding CNS Brain sends
Evaluation and Treatment of Incontinence Classification of Incontinence Failure to empty: Overflow incontinence Failure to store Stress Incontinence Urge Incontinence Physiology of voiding CNS Brain sends
GUIDELINES ON NEUROGENIC LOWER URINARY TRACT DYSFUNCTION
 GUIDELINES ON NEUROGENIC LOWER URINARY TRACT DYSFUNCTION M. Stöhrer (chairman), D. Castro-Diaz, E. Chartier-Kastler, G. Kramer, A. Mattiasson, J-J. Wyndaele Introduction NLUTD (neurogenic lower urinary
GUIDELINES ON NEUROGENIC LOWER URINARY TRACT DYSFUNCTION M. Stöhrer (chairman), D. Castro-Diaz, E. Chartier-Kastler, G. Kramer, A. Mattiasson, J-J. Wyndaele Introduction NLUTD (neurogenic lower urinary
Appendix E: Continence Care and Bowel Management Program Training Presentation. Audience: For Registered Staff Release Date: December 22, 2010
 Appendix E: Continence Care and Bowel Management Program Training Presentation Audience: For Registered Staff Release Date: December 22, 2010 Objectives Address individual needs and preferences with respect
Appendix E: Continence Care and Bowel Management Program Training Presentation Audience: For Registered Staff Release Date: December 22, 2010 Objectives Address individual needs and preferences with respect
10/9/2015. Dana A. Brown, Pharm.D., BCPS Assistant Dean for Academics, Associate Professor of Pharmacy Practice Palm Beach Atlantic University
 Dana A. Brown, Pharm.D., BCPS Assistant Dean for Academics, Associate Professor of Pharmacy Practice Palm Beach Atlantic University 1. Explain the pathophysiology of benign prostatic hyperplasia (BPH),
Dana A. Brown, Pharm.D., BCPS Assistant Dean for Academics, Associate Professor of Pharmacy Practice Palm Beach Atlantic University 1. Explain the pathophysiology of benign prostatic hyperplasia (BPH),
Summary. Neuro-urodynamics. The bladder cycle. and voiding. 14/12/2015. Neural control of the LUT Initial assessment Urodynamics
 Neuro-urodynamics Summary Neural control of the LUT Initial assessment Urodynamics Marcus Drake, Bristol Urological Institute SAFETY FIRST; renal failure, dysreflexia, latex allergy SYMPTOMS SECOND; storage,
Neuro-urodynamics Summary Neural control of the LUT Initial assessment Urodynamics Marcus Drake, Bristol Urological Institute SAFETY FIRST; renal failure, dysreflexia, latex allergy SYMPTOMS SECOND; storage,
NON-Neurogenic Chronic Urinary Retention AUA White Paper
 NON-Neurogenic Chronic Urinary Retention AUA White Paper Great Lakes SUNA Inside Urology March 16, 2018 Michelle J. Lajiness FNP-BC Nurse Practitioner DMC Urology Incidence Really unknown Lack consensus
NON-Neurogenic Chronic Urinary Retention AUA White Paper Great Lakes SUNA Inside Urology March 16, 2018 Michelle J. Lajiness FNP-BC Nurse Practitioner DMC Urology Incidence Really unknown Lack consensus
Tools for Evaluation. Urodynamics Case Studies. Case 1. Evaluation. Case 1. Bladder Diary SUI 19/01/2018
 Urodynamics Case Studies Christopher K. Payne, MD Vista Urology & Pelvic Pain Partners Emeritus Professor of Urology, Stanford University Tools for Evaluation Ears, Eyes, and Brain Bladder diary Stress
Urodynamics Case Studies Christopher K. Payne, MD Vista Urology & Pelvic Pain Partners Emeritus Professor of Urology, Stanford University Tools for Evaluation Ears, Eyes, and Brain Bladder diary Stress
Module 3 Causes Of Urinary Incontinence
 Causes Of Urinary Incontinence V4: Last Reviewed September 2017 Learning Outcomes Appreciate the numerous requirements and skills necessary for the person to achieve and maintain urinary continence Discuss
Causes Of Urinary Incontinence V4: Last Reviewed September 2017 Learning Outcomes Appreciate the numerous requirements and skills necessary for the person to achieve and maintain urinary continence Discuss
Regulation of the Urinary Bladder Chapter 26
 Regulation of the Urinary Bladder Chapter 26 Anatomy 1. The urinary bladder is smooth muscle lined internally by transitional epithelium and externally by the parietal peritoneum. Contraction of the smooth
Regulation of the Urinary Bladder Chapter 26 Anatomy 1. The urinary bladder is smooth muscle lined internally by transitional epithelium and externally by the parietal peritoneum. Contraction of the smooth
Guidelines on Neurogenic Lower Urinary Tract Dysfunction
 Guidelines on Neurogenic Lower Urinary Tract Dysfunction (Text update March 2009) M. Stöhrer (chairman), B. Blok, D. Castro-Diaz, E. Chartier- Kastler, P. Denys, G. Kramer, J. Pannek, G. del Popolo, P.
Guidelines on Neurogenic Lower Urinary Tract Dysfunction (Text update March 2009) M. Stöhrer (chairman), B. Blok, D. Castro-Diaz, E. Chartier- Kastler, P. Denys, G. Kramer, J. Pannek, G. del Popolo, P.
Recommandations de prise en charge des vessies neurogènes EAU 2006
 Annexe 4-1 Recommandations de prise en charge des vessies neurogènes EAU 2006 (Version courte) 685 686 GUIDELINES ON NEUROGENIC LOWER URINARY TRACT DYSFUNCTION M. Stöhrer (chairman), D. Castro-Diaz, E.
Annexe 4-1 Recommandations de prise en charge des vessies neurogènes EAU 2006 (Version courte) 685 686 GUIDELINES ON NEUROGENIC LOWER URINARY TRACT DYSFUNCTION M. Stöhrer (chairman), D. Castro-Diaz, E.
PROSTATIC ARTERY EMBOLISATION (PAE) FOR BENIGN PROSTATIC HYPERPLASIA. A Minimally Invasive Innovative Treatment
 FOR BENIGN PROSTATIC HYPERPLASIA. A Minimally Invasive Innovative Treatment") PROSTATIC ARTERY EMBOLISATION (PAE) FOR BENIGN PROSTATIC HYPERPLASIA A Minimally Invasive Innovative Treatment What is the prostate? The prostate is an accessory organ of the male reproductive system.
PROSTATIC ARTERY EMBOLISATION (PAE) FOR BENIGN PROSTATIC HYPERPLASIA A Minimally Invasive Innovative Treatment What is the prostate? The prostate is an accessory organ of the male reproductive system.
Dysfunctional voiding
 Dysfunctional voiding The importance of assessment, diagnosis and treatment of dysfunctional voiding and its role in recurrent UTI Dr Dean Wallace Consultant Paediatric Nephrologist RMCH Objectives Development
Dysfunctional voiding The importance of assessment, diagnosis and treatment of dysfunctional voiding and its role in recurrent UTI Dr Dean Wallace Consultant Paediatric Nephrologist RMCH Objectives Development
Mr. GIT KAH ANN. Pakar Klinikal Urologi Hospital Kuala Lumpur.
 Mr. GIT KAH ANN Pakar Klinikal Urologi Hospital Kuala Lumpur drgitka@yahoo.com 25 Jan 2007 HIGHLIGHTS Introduction ICS Definition Making a Diagnosis Voiding Chart Investigation Urodynamics Ancillary Investigations
Mr. GIT KAH ANN Pakar Klinikal Urologi Hospital Kuala Lumpur drgitka@yahoo.com 25 Jan 2007 HIGHLIGHTS Introduction ICS Definition Making a Diagnosis Voiding Chart Investigation Urodynamics Ancillary Investigations
Case studies: LUTS. Case 1 history. Case 1 - questions. Case 1 - outcome. Case 2 - history. Case 1 learning point 14/07/2015 DR JON REES
 Case 1 history Case studies: LUTS DR JON REES A 49 year old male comes to see you he has had gradual deterioration of his flow over the last few years- he saw a colleague of yours 6 weeks ago who recorded
Case 1 history Case studies: LUTS DR JON REES A 49 year old male comes to see you he has had gradual deterioration of his flow over the last few years- he saw a colleague of yours 6 weeks ago who recorded
Dr Jonathan Evans Paediatric Nephrologist
 How do I manage a patient with intractable daytime wetting: Dr Jonathan Evans Paediatric Nephrologist Of 107 children aged 11-12 with day-wetting 91 (85%) were dry at 15-16 yr Swithinbank et al BJU 1998
How do I manage a patient with intractable daytime wetting: Dr Jonathan Evans Paediatric Nephrologist Of 107 children aged 11-12 with day-wetting 91 (85%) were dry at 15-16 yr Swithinbank et al BJU 1998
URINARY INCONTINENCE
 Center for Continence Care and Pelvic Medicine What is urinary incontinence? URINARY INCONTINENCE Urinary incontinence is the uncontrollable loss of urine. The amount of urine leaked can vary from only
Center for Continence Care and Pelvic Medicine What is urinary incontinence? URINARY INCONTINENCE Urinary incontinence is the uncontrollable loss of urine. The amount of urine leaked can vary from only
THE ACONTRACTILE BLADDER - FACT OR FICTION?
 THE ACONTRACTILE BLADDER - FACT OR FICTION? Jacob Golomb Department of Urology Chaim Sheba Medical Center Tel Hashomer NEUROGENIC UNDERACTIVE DETRUSOR Central (complete/incomplete): Spinal cord injury-
THE ACONTRACTILE BLADDER - FACT OR FICTION? Jacob Golomb Department of Urology Chaim Sheba Medical Center Tel Hashomer NEUROGENIC UNDERACTIVE DETRUSOR Central (complete/incomplete): Spinal cord injury-
Patient Expectations Following Greenlight XPS
 Patient Expectations Following Greenlight XPS 1. Hematuria it is common for men to have light pink to cherry red urine following the procedure. This small amount of blood in the urine usually resolves
Patient Expectations Following Greenlight XPS 1. Hematuria it is common for men to have light pink to cherry red urine following the procedure. This small amount of blood in the urine usually resolves
김준철 가톨릭대학교의과대학비뇨기과학교실
 비뇨기계자율신경병증의치료 김준철 가톨릭대학교의과대학비뇨기과학교실 Introduction Urologic complications have increasingly become a concern in those affected by DM Genitourinary problems are included among these complications, related
비뇨기계자율신경병증의치료 김준철 가톨릭대학교의과대학비뇨기과학교실 Introduction Urologic complications have increasingly become a concern in those affected by DM Genitourinary problems are included among these complications, related
Policy for Prostatism/Lower Urinary Tract Symptoms in men
 NHS Halton Clinical Commissioning Group NHS Liverpool Clinical Commissioning Group NHS St Helens Clinical Commissioning Group NHS South Sefton Clinical Commissioning Group NHS Southport and Formby Clinical
NHS Halton Clinical Commissioning Group NHS Liverpool Clinical Commissioning Group NHS St Helens Clinical Commissioning Group NHS South Sefton Clinical Commissioning Group NHS Southport and Formby Clinical
Overactive bladder can result from one or more of the following causes:
 Overactive bladder can affect people of any age; however, it is more common in older people. Effective treatments are available and seeing your doctor for symptoms of overactive bladder often results in
Overactive bladder can affect people of any age; however, it is more common in older people. Effective treatments are available and seeing your doctor for symptoms of overactive bladder often results in
Management of Urinary Incontinence in Older Women. Dr. Cecilia Cheon Department of Obs. & Gyn. Queen Elizabeth Hospital
 Management of Urinary Incontinence in Older Women Dr. Cecilia Cheon Department of Obs. & Gyn. Queen Elizabeth Hospital Epidemiology Causes Investigation Treatment Conclusion Elderly Women High prevalence
Management of Urinary Incontinence in Older Women Dr. Cecilia Cheon Department of Obs. & Gyn. Queen Elizabeth Hospital Epidemiology Causes Investigation Treatment Conclusion Elderly Women High prevalence
Urine a Mess: Micturition Disorders Joe Bartges, DVM, PhD, DACVIM, DACVN Cornell University Veterinary Specialists Stamford, CT
 Urine a Mess: Micturition Disorders Joe Bartges, DVM, PhD, DACVIM, DACVN Cornell University Veterinary Specialists Stamford, CT 1. Micturition refers to the process of storing and periodically voiding
Urine a Mess: Micturition Disorders Joe Bartges, DVM, PhD, DACVIM, DACVN Cornell University Veterinary Specialists Stamford, CT 1. Micturition refers to the process of storing and periodically voiding
BPH / LUTS. Prevalence. Prevalence of BPH. It is abnormal NOT to have benign growth of the prostate with increasing age. Prevalence.
 BPH / LUTS Dr Jonny Coxon MA MD MRCS MRCGP DRCOG FECSM Beaconsfield Medical Practice, Brighton & Brighton & Sussex Universities NHS Trust As man draws near the common goal Can anything be sadder Than he
BPH / LUTS Dr Jonny Coxon MA MD MRCS MRCGP DRCOG FECSM Beaconsfield Medical Practice, Brighton & Brighton & Sussex Universities NHS Trust As man draws near the common goal Can anything be sadder Than he
Index. urologic.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Ablation, of prostate, holmium laser, 485 495 African prune tree (Pygeum africanum), 454 455 Alfuzosin, 445 446 Alpha-adrenergic agonists,
Index Note: Page numbers of article titles are in boldface type. A Ablation, of prostate, holmium laser, 485 495 African prune tree (Pygeum africanum), 454 455 Alfuzosin, 445 446 Alpha-adrenergic agonists,
Practical urodynamics What PA s need to know. Gary E. Lemack, MD Professor of Urology and Neurology
 Practical urodynamics What PA s need to know Gary E. Lemack, MD Professor of Urology and Neurology Urodynamics essential elements Urethral catheter Fill rate Catheter size Intravesical pressure measurements
Practical urodynamics What PA s need to know Gary E. Lemack, MD Professor of Urology and Neurology Urodynamics essential elements Urethral catheter Fill rate Catheter size Intravesical pressure measurements
Urinary Incontinence. Lee A. Jennings, MD, MSHS. Assistant Professor Reynolds Department of Geriatrics University of Oklahoma Health Sciences Center
 Urinary Incontinence Lee A. Jennings, MD, MSHS Assistant Professor Reynolds Department of Geriatrics University of Oklahoma Health Sciences Center Slides adapted from Alison Moore, MD, MPH University of
Urinary Incontinence Lee A. Jennings, MD, MSHS Assistant Professor Reynolds Department of Geriatrics University of Oklahoma Health Sciences Center Slides adapted from Alison Moore, MD, MPH University of
Urinary Continence & Management Post Stroke
 Urinary Continence & Management Post Stroke Incontinence and Stroke occurs in greater than 50% of acute stroke patients despite the personal, economic and psychosocial impact treatment evidence specific
Urinary Continence & Management Post Stroke Incontinence and Stroke occurs in greater than 50% of acute stroke patients despite the personal, economic and psychosocial impact treatment evidence specific
Bladder dysfunction in ALD and AMN
 Bladder dysfunction in ALD and AMN Sara Simeoni, MD Department of Uro-Neurology National Hospital for Neurology and Neurosurgery Queen Square, London 10:15 Dr Sara Simeoni- Bladder issues for AMN patients
Bladder dysfunction in ALD and AMN Sara Simeoni, MD Department of Uro-Neurology National Hospital for Neurology and Neurosurgery Queen Square, London 10:15 Dr Sara Simeoni- Bladder issues for AMN patients
As man draws near the common goal Can anything be sadder Than he who, master of his soul Is servant to his bladder LUTS 2. Prevalence of BPH LUTS 5
 BPH / LUTS Dr Jonny Coxon MA MD MRCS MRCGP DRCOG Beaconsfield Medical Practice, Brighton As man draws near the common goal Can anything be sadder Than he who, master of his soul Is servant to his bladder
BPH / LUTS Dr Jonny Coxon MA MD MRCS MRCGP DRCOG Beaconsfield Medical Practice, Brighton As man draws near the common goal Can anything be sadder Than he who, master of his soul Is servant to his bladder
Urinary Adverse Events after Radiation Therapy for Prostate Cancer
 Urinary Adverse Events after Radiation Therapy for Prostate Cancer Sexual Medicine Society of North America Scottsdale, Arizona 2016 Jaspreet S. Sandhu, MD Department of Surgery/Urology Memorial Sloan
Urinary Adverse Events after Radiation Therapy for Prostate Cancer Sexual Medicine Society of North America Scottsdale, Arizona 2016 Jaspreet S. Sandhu, MD Department of Surgery/Urology Memorial Sloan
Diane K. Newman DNP, ANP-BC, PCB-PMD, FAAN
 Diane K. Newman DNP, ANP-BC, PCB-PMD, FAAN Diane K. Newman, DNP is a Biofeedback Certified Continence Specialist. With over 35-years experience, she is an expert in the assessment and management of pelvic-floor
Diane K. Newman DNP, ANP-BC, PCB-PMD, FAAN Diane K. Newman, DNP is a Biofeedback Certified Continence Specialist. With over 35-years experience, she is an expert in the assessment and management of pelvic-floor
Some people experience occasional, minor leaks of urine. Others wet their clothes frequently.
 Urinary Incontinence Urinary incontinence the loss of bladder control is a common and often embarrassing problem. The severity ranges from occasionally leaking urine when you cough or sneeze to having
Urinary Incontinence Urinary incontinence the loss of bladder control is a common and often embarrassing problem. The severity ranges from occasionally leaking urine when you cough or sneeze to having
Glossary of terms Urinary Incontinence
 Patient Information English Glossary of terms Urinary Incontinence Anaesthesia (general, spinal, or local) Before a procedure you will get medication to make sure that you don t feel pain. Under general
Patient Information English Glossary of terms Urinary Incontinence Anaesthesia (general, spinal, or local) Before a procedure you will get medication to make sure that you don t feel pain. Under general
50% of men. 90% of men PATIENT FACTSHEET: BPH CONDITION AND TREATMENTS. Want more information? What are the symptoms?
 PATIENT FACTSHEET: BPH CONDITION AND TREATMENTS What is Benign Prostatic Hyperplasia (enlarged prostate)? Benign prostatic hyperplasia (BPH) is a noncancerous enlargement of the prostate, the gland that
PATIENT FACTSHEET: BPH CONDITION AND TREATMENTS What is Benign Prostatic Hyperplasia (enlarged prostate)? Benign prostatic hyperplasia (BPH) is a noncancerous enlargement of the prostate, the gland that
CASES FOR TRAINING OF THE INTERNATIONAL SPINAL CORD INJURY LOWER URINARY TRACT FUNCTION BASIC DATA SET CASE 1
 1 CASES FOR TRAINING OF THE INTERNATIONAL SPINAL CORD INJURY LOWER URINARY TRACT FUNCTION BASIC DATA SET CASE 1 35 years old man, who previously has been completely healthy, was shot twice in the neck
1 CASES FOR TRAINING OF THE INTERNATIONAL SPINAL CORD INJURY LOWER URINARY TRACT FUNCTION BASIC DATA SET CASE 1 35 years old man, who previously has been completely healthy, was shot twice in the neck
URINARY TRACT NERVOUS SYSTEM DISORDERS: DRUG THERAPY REVIEW
 Vet Times The website for the veterinary profession https://www.vettimes.co.uk URINARY TRACT NERVOUS SYSTEM DISORDERS: DRUG THERAPY REVIEW Author : Ian Battersby Categories : Vets Date : August 3, 2009
Vet Times The website for the veterinary profession https://www.vettimes.co.uk URINARY TRACT NERVOUS SYSTEM DISORDERS: DRUG THERAPY REVIEW Author : Ian Battersby Categories : Vets Date : August 3, 2009
Urogynecology ICD-9 to ICD-10 Crosswalks
 1100 Wayne Ave, Suite 825 Silver Spring, MD 20910 301.273.0570 Fax 301.273.0778 info@augs.org www.augs.org Urogynecology ICD-9 to ICD-10 Crosswalks ICD 9 ICD 9 Description ICD 10 Code ICD 10 Description
1100 Wayne Ave, Suite 825 Silver Spring, MD 20910 301.273.0570 Fax 301.273.0778 info@augs.org www.augs.org Urogynecology ICD-9 to ICD-10 Crosswalks ICD 9 ICD 9 Description ICD 10 Code ICD 10 Description