gynaecology in family medicine
|
|
|
- Sheryl Sutton
- 5 years ago
- Views:
Transcription
1 gynaecology in family medicine John Short Obstetrician and Gynaecologist Christchurch

2 What s going on down there?
3 UbR4vfxBc 3 3

4
5 urinary incontinence involuntary leakage of urine stress urgency mixed
6 urine is made in the kidneys various factors influence urine production bladder is a reservoir that expands and contracts as required it has a sensory and motor nerve supply
7 Bladder Pressure vs Urethral Pressure Bladder pressure = detrusor pressure + abdominal pressure Urethral pressure = urethral sphincter + pelvic floor
8 Mental function Mobility Motivation Manual dexterity
9 categorise incontinence identify modifiable factors consider underlying medical problems and medications remember quality of life
10 demonstrate incontinence abdo-pelvic mass vaginal atrophy prolapse basic neurology weight / BMI Clinical examination
11 PADS post-void residual analyse urine diary stress test
12
13 Treat UTI Treat significant prolapse Vaginal oestrogen Lifestyle interventions Continence products
14 Lifestyle interventions Weight reduction (*) Relieving constipation Cessation of smoking/treatment of chronic cough. Bladder irritants fluid management Reduction of physical forces (exercise, work)


15
16 Pelvic floor exercises 33% of women cannot do from pamphlet alone Pelvic floor assessment vital
17 >2 leakages/day Psychotropics Symptoms >5yrs +ve stress test (first attempt) >2pads/day Significant (untreated) prolapse
18 50% significant improvement 25% mild improvement Age/BMI not predictors 4 M s Patient choice

19 Hospital episode statistics Total Colposuspension TVT Needle suspension Injectables Slings
20 20
21 Success not guaranteed Overall 80-90%, using QOL Failure RFs- OBESITY DIABETES URGENCY PREV SURGERY UNTREATED PROLAPSE SPHINCTER DEFICIENCY 36
22 complications bleeding infection injury voiding issues pain mesh erosion 22
23 Urge incontinence/oab treat prolapse treat vaginal atrophy fluid management bladder retraining pharmacotherapy synergistic effect of above 37 29
24 mixed incontinence identify most bothersome aspect and treat first 38 30
25 Summary Basic science is quite basic categorise incontinence assess QOL consider other morbidities lifestyle measures simple treatments surgery 25
26 Continence care resources Courses: NZCA: 26
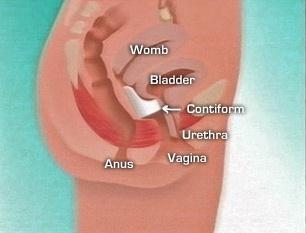
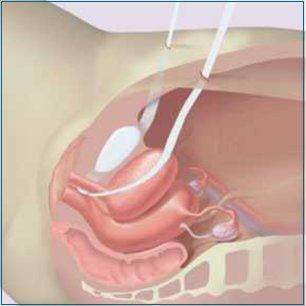
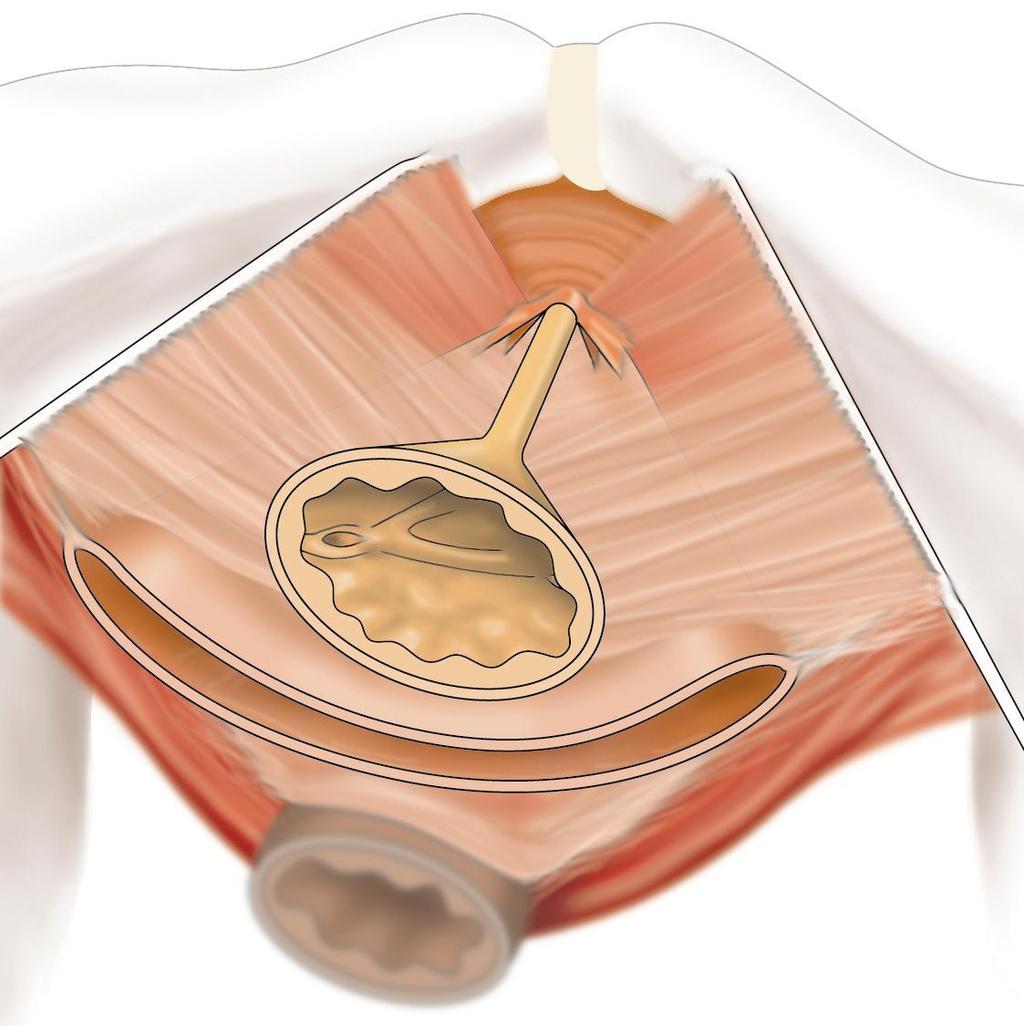
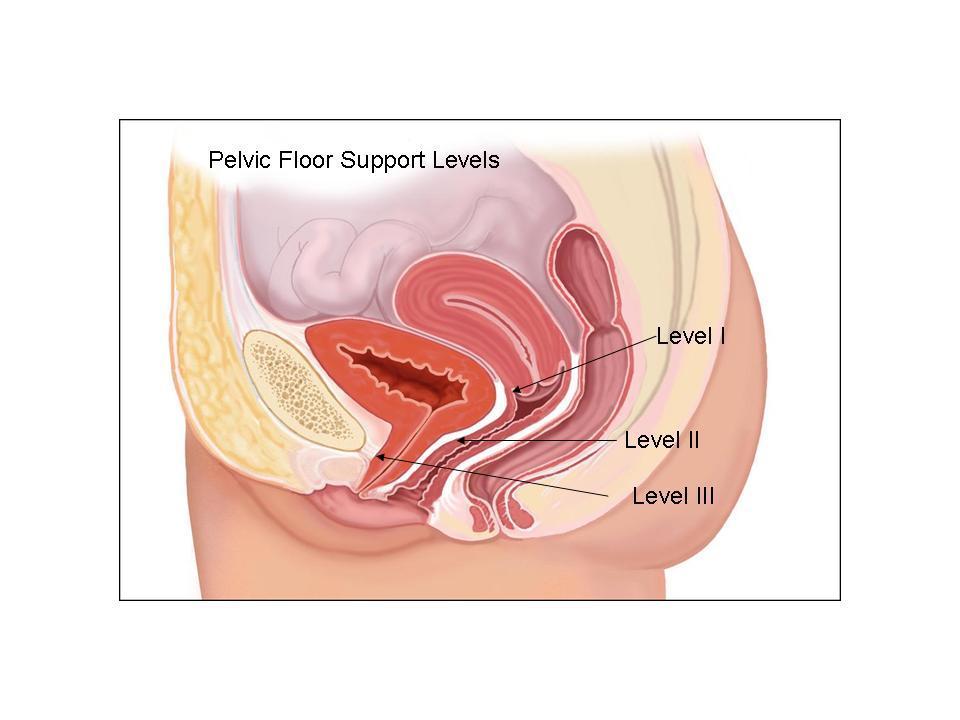
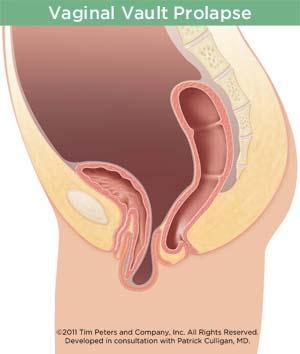
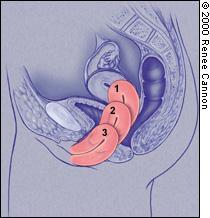
27 pelvic organ prolapse pelvic organs - uterus, bladder, rectum prolapse - displacement of viscus through an orifice orifice - vagina (and anus)
28 Internal structures that support the pelvic organs are weak, stretched or damaged such that the organs drop from their normal position and bulge into the vagina
29
30
31
32
33 aetiology genetics pelvic floor injury, eg childbirth chronic increased abdo pressure, eg obesity, constipation, coughing, pregnancy
34 symptoms often asymptomatic bulge bladder- overactivity, voiding issues bowel- obstructive defaecation sexual- physical and/or emotional
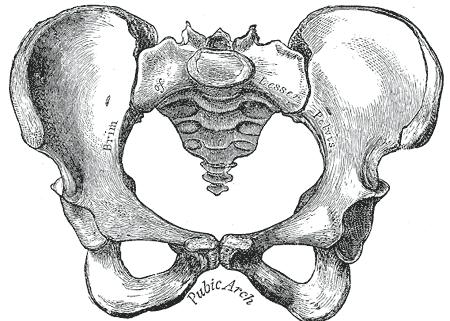
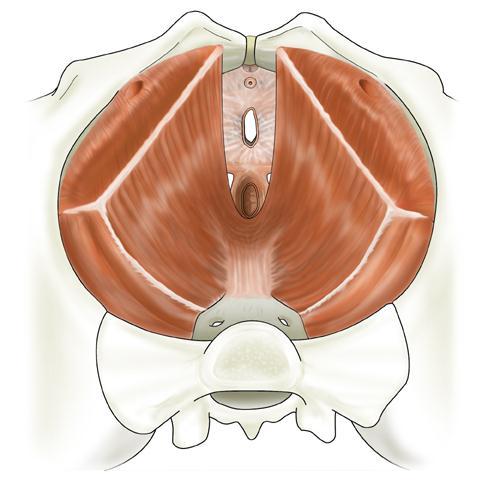
35 prolapse assessment
36 assessment aspect of vagina involved anterior, posterior, apical organ prolapsing bladder (cystocoele), rectum (rectocoele), small bowel (enterocoele), uterus (hysterocoele)
37 grading grade 0- normally sited grade 1- halfway to hymen grade 2- reaches hymen grade 3- halfway outside hymen grade 4- complete descent
38
39
40
41
42
43 Anatomy POP-Q Stage Nulliparous (n=30) CS only (n=14) CS & SVD (n=15) SVD (n=84) AVD (n=51) 0 13 (43.3%) 2 (14.3%) 1 (6.7%) 1 15 (50.0%) 9 (64.3%) 6 (40.0%) 31 (36.9%) 12 (23.5%) 2a (above the hymen) 2 (6.7%) 3 (21.4%) 6 (40.0%) 34 (40.5%) 23 (45.1%) 2b (at or below the hymen) 2 (13.3%) 19 (22.6%) 13 (25.5%) 3 3 (5.9%) 29
44 natural history deterioration is NOT inevitable atrophic tissue stiffer prolapse often longstanding and symptoms may relate to other things, eg E2 deficiency 44
45 treatment of prolapse Symptomatic Anatomical 40 45
46 treatment of prolapse Symptomatic Oestrogen Physiotherapy fibre, laxatives catheterisation weight loss unhelpful 41 46

47
48 treatment of prolapse Symptomatic Anatomical Physiotherapy Pessaries Surgery 42 48
49 problems standard physio will only treat mild prolapse. to treat moderate to severe prolapse it needs to be extremely intensive. pessaries not appealing at face value. surgery has disappointing long term results and potential complications
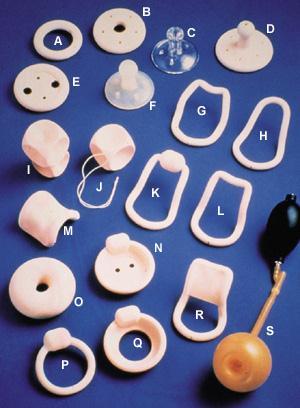
50 pessaries
51 Pessaries useful for anterior and central compartments less effective for posterior compartment At 1 year similar improvement in urinary, bowel, sexual and QOL measures when compared to surgery median duration of use 2 yrs possible to avoid surgery 44 51
52 Reasons for discontinuation Inconvenient Inadequate relief of symptoms Uncomfortable, ulceration, bleeding, discharge Elected for surgery Unable to remain in place Difficulty urinating (or bowels) Incontinence increased (different sizes or shapes may help) 52
53 Sizing up ring pessaries insert fingers deep into the posterior fornix Make note of where the hand comes into contact with the pubic bone Compare to pessary. I d e n
54 regular oestrogen annual review 54
55 operations Standard repairs Vaginal hysterectomy Sacrospinous fixation colpocleisis mesh repairs
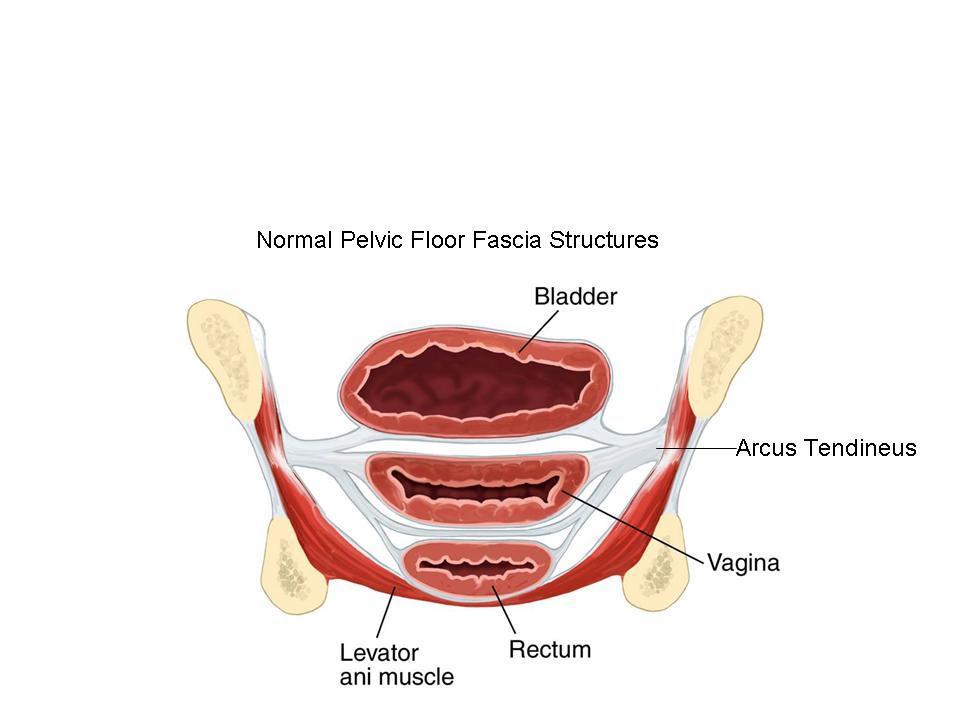
56 tradition operations done vaginally eg anterior and posterior repair repair fascia (level 2) results often disappointing? tissue beyond repair 56
57 vaginal hysterectomy uterus is innocent bystander bulk may cause symptoms hysterectomy allows access to level 1 supports apical repair can the be performed shortening / re-approximation of para-cervical and uterosacral ligaments 57
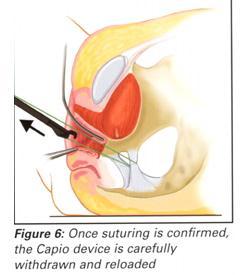
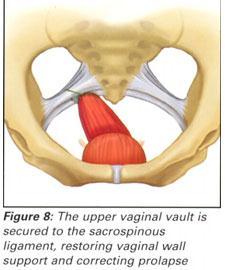
58 sacrospinous fixation

59 sacrocolpopexy sacrohysteropexy 59

60 colpocleisis closure of vaginal orifice 60
61 the only problem left unsolved by the gynaecologist of the past century is that of permanent cure of Cystocoele if only it were possible to artificially produce tissue of density and toughness of fascia and tendon, the secret of the radical cure of hernia would be discovered
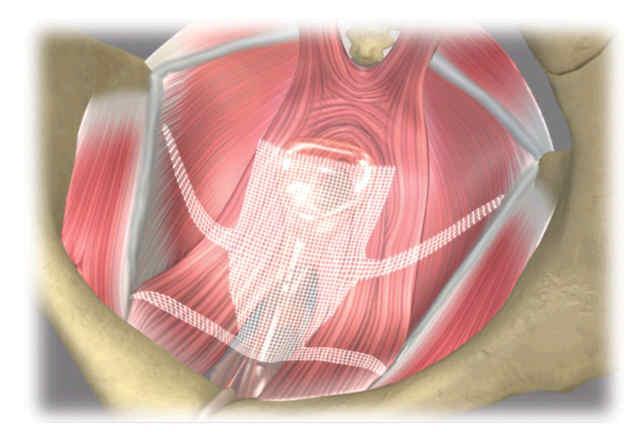
62 mesh repair Proposed for transvaginal repair of vaginal prolapse 1990s. Disappointing results of traditional surgery 2001 RCT success of anterior repair at 40% (Sand et al), 30% (Weber et al)
63 replaces (instead of repairs) level 2 (?level1) supports / fascia greater anatomical success than traditional surgery no difference in subjective outcomes 63
64
65 Complications Higher with mesh erosion pain infection bleeding dysparuenia organ injury urinary/bowel problems
66 Re-evaluation Weber et al 2001: anatomical success- 30% (based on grade 0) Based on grade 2a or less success 90% Based on symptoms success 95%
67 Mesh success 81% % No mesh success 65% %

68 mesh no mesh Enthusiasts Sceptics Early uptakers Laggards Mesh for all Mesh for some Mesh for none
69 summary POP common often asymptomatic some degree normal quality of life issues surgical or non surgical treatment subjective vs objective outcome measures 69
70 Contraceptive Update Side Effects Improving efficacy New products Eligibility criteria IUDs/implants 70
71 Contraception saves lives 50 million pregnancies terminated worldwide per year 50,000 women die as a result Up to 50,000 more deaths may be prevented Other health/societal benefits 71
72 Serious risks CVA and MI RR Ring and patch POP no increase However, overall risk v low (1-2 extra events per 10,000 women) Smoking, BP, other RFs important 72
73 Side Effects Long lists, based on postmarketing surveys, not clinical evidence Real danger of misinformation leading to discontinuation of contraception and unwanted pregnancy 73
74 COCP vs Placebo No difference: Headache Nausea and vomiting Breast pain Decreased libido Weight gain Difference: PV spotting for first 3 months (more with COCP) 74
75 POP Regular bleeding 40% Irregular bleeding 40% No bleeding 20% No evidence: weight gain, depression, CVS changes, breast cancer No evidence based treatment for bleeding patterns 75
76 depo No evidence: Headache Mood/libido issues No concerns re bone mineral density Routine testing not recommended 76
77 Mirena Alopecia in 1% 77
78 Improving pill efficacy OCs and DMPA very effective Use-continuation rate 50% IUDs and Implants most effective Use-continuation rate 80% Continuous use supported >8 continuous pills need to be missed to risk pregnancy Eliminates hormone withdrawal effects 78
79 New products Qlaira- reduced heavy menstrual bleeding Zoely- theoretical impact on haemostasis and lipids Depo-subQ- self administered DMPA, sub-cut not IM Nuva-ring- improved cycle control Yaz Flex- pill alarm reminder 79
80 Eligibility criteria 1. use in any circumstances 2. generally use the method. Benefits outweigh risks 3. use not usually recommended unless other methods not acceptable. Proven risks outweigh benefits 4. Do not use. Risk is unacceptable 80
81 COCP category 3 if BMI>35, category 2 if BMI COCP category 2 for migraine without aura, category 3 if migraine related to use (1 & 2 for POP) GTD, everything category 1, except IUD- cat 4 in cases of elevated HCG or malignancy IUDs category 1 for PID and ectopic pregnancy (no longer remove in presence of chlamydia) 81
82 Concomitant meds No additional precautions for OCs and enzymeinducing antibiotics COCP not recommended for women on lamotrigine 82
83 IUDS/implants LARCs most effective, esp on adolescents Better post TOP IUDs do not cause infections. Pre-placement swaps important Jadelle not effective with enzyme-inducers Insertion issues in thin women 83
84 IUD better postcoital contraception around ovulation and if BMI>30 84
85 resources _eng.pdf 85
Dr John Short. Obstetrician and Gynaecologist Christchurch Women s Hospital, Oxford Women's Health, Christchurch
 Dr John Short Obstetrician and Gynaecologist Christchurch Women s Hospital, Oxford Women's Health, Christchurch 8:30-9:25 WS #142: Peeling Back the Layers - The Pelvic Floor Uncovered 9:35-10:30 WS #152:
Dr John Short Obstetrician and Gynaecologist Christchurch Women s Hospital, Oxford Women's Health, Christchurch 8:30-9:25 WS #142: Peeling Back the Layers - The Pelvic Floor Uncovered 9:35-10:30 WS #152:
Ben Herbert Alex Wojtowicz
 Ben Herbert Alex Wojtowicz 54 year old female presenting with: Dragging sensation Urinary incontinence Some faecal incontinence HPC Since May 14 had noticed a mass protruding from the vagina when going
Ben Herbert Alex Wojtowicz 54 year old female presenting with: Dragging sensation Urinary incontinence Some faecal incontinence HPC Since May 14 had noticed a mass protruding from the vagina when going
Moneli Golara Consultant Obstetrician and Gynaecologist Royal Free NHS Trust Barnet Hospital
 Moneli Golara Consultant Obstetrician and Gynaecologist Royal Free NHS Trust Barnet Hospital Pelvic Organ Prolapse (POP)- herniation of pelvic organs into vaginal walls Common Huge impact on daily activities
Moneli Golara Consultant Obstetrician and Gynaecologist Royal Free NHS Trust Barnet Hospital Pelvic Organ Prolapse (POP)- herniation of pelvic organs into vaginal walls Common Huge impact on daily activities
Prolapse and Urogynae Incontinence. Lucy Tiffin and Hannah Wheldon-Holmes
 Prolapse and Urogynae Incontinence Lucy Tiffin and Hannah Wheldon-Holmes 66 year old woman with incontinence PC: 7 year Hx of urgency, frequency, nocturia (incl. incontinence at night), and stress incontinence
Prolapse and Urogynae Incontinence Lucy Tiffin and Hannah Wheldon-Holmes 66 year old woman with incontinence PC: 7 year Hx of urgency, frequency, nocturia (incl. incontinence at night), and stress incontinence
Interventional procedures guidance Published: 28 June 2017 nice.org.uk/guidance/ipg583
 Sacrocolpopexy using mesh to repair vaginal vault prolapse Interventional procedures guidance Published: 28 June 2017 nice.org.uk/guidance/ipg583 Your responsibility This guidance represents the view of
Sacrocolpopexy using mesh to repair vaginal vault prolapse Interventional procedures guidance Published: 28 June 2017 nice.org.uk/guidance/ipg583 Your responsibility This guidance represents the view of
John Laughlin 4 th year Cardiff University Medical Student
 John Laughlin 4 th year Cardiff University Medical Student Prolapse/incontinence You need to know: Pelvic floor anatomy in relation to uterovaginal support and continence The classification of uterovaginal
John Laughlin 4 th year Cardiff University Medical Student Prolapse/incontinence You need to know: Pelvic floor anatomy in relation to uterovaginal support and continence The classification of uterovaginal
Gynecology Dr. Sallama Lecture 3 Genital Prolapse
 Gynecology Dr. Sallama Lecture 3 Genital Prolapse Genital(utero-vaginal )prolapse is extremely common, with an estimated 11% of women undergoing at least one operation for this condition. Definition: A
Gynecology Dr. Sallama Lecture 3 Genital Prolapse Genital(utero-vaginal )prolapse is extremely common, with an estimated 11% of women undergoing at least one operation for this condition. Definition: A
Karanvir Virk M.D. Minimally Invasive & Pelvic Reconstructive Surgery 01/28/2015
 Karanvir Virk M.D. Minimally Invasive & Pelvic Reconstructive Surgery 01/28/2015 Disclosures I have none Objectives Identify the basic Anatomy and causes of Pelvic Organ Prolapse Examine office diagnosis
Karanvir Virk M.D. Minimally Invasive & Pelvic Reconstructive Surgery 01/28/2015 Disclosures I have none Objectives Identify the basic Anatomy and causes of Pelvic Organ Prolapse Examine office diagnosis
By:Dr:ISHRAQ MOHAMMED
 By:Dr:ISHRAQ MOHAMMED Protrusion of an organ or structure beyond its normal confines. Prolapses are classified according to their location and the organs contained within them. 1-Anterior vaginal wall
By:Dr:ISHRAQ MOHAMMED Protrusion of an organ or structure beyond its normal confines. Prolapses are classified according to their location and the organs contained within them. 1-Anterior vaginal wall
Urogynaecology. Colm McAlinden
 Urogynaecology Colm McAlinden Definitions Urinary incontinence compliant of any involuntary leakage of urine with many different causes Two main types: Stress Urge Definitions Nocturia: More than a single
Urogynaecology Colm McAlinden Definitions Urinary incontinence compliant of any involuntary leakage of urine with many different causes Two main types: Stress Urge Definitions Nocturia: More than a single
Prediction and prevention of stress urinary incontinence after prolapse surgery van der Ploeg, J.M.
 UvA-DARE (Digital Academic Repository) Prediction and prevention of stress urinary incontinence after prolapse surgery van der Ploeg, J.M. Link to publication Citation for published version (APA): van
UvA-DARE (Digital Academic Repository) Prediction and prevention of stress urinary incontinence after prolapse surgery van der Ploeg, J.M. Link to publication Citation for published version (APA): van
Prolapse and Urogynae. By Sarah Rangan & Daniel Warrell
 Prolapse and Urogynae By Sarah Rangan & Daniel Warrell Anatomy and physiology of the pelvic supports The pelvic floor supports the pelvic viscera and vaginal, urethral and rectal openings Endopelvic fascial
Prolapse and Urogynae By Sarah Rangan & Daniel Warrell Anatomy and physiology of the pelvic supports The pelvic floor supports the pelvic viscera and vaginal, urethral and rectal openings Endopelvic fascial
Content. Terminology Anatomy Aetiology Presentation Classification Management
 Prolapse Content Terminology Anatomy Aetiology Presentation Classification Management Terminology Prolapse Descent of pelvic organs into the vagina Cystocele ant. vaginal wall involving bladder Uterine
Prolapse Content Terminology Anatomy Aetiology Presentation Classification Management Terminology Prolapse Descent of pelvic organs into the vagina Cystocele ant. vaginal wall involving bladder Uterine
Management of Vaginal Prolapse
 Information for Patients Saint Mary s Hospital/Trafford General Hospital Uro-gynaecology Service Management of Vaginal Prolapse Before reading this leaflet you should read What is vaginal prolapse? If
Information for Patients Saint Mary s Hospital/Trafford General Hospital Uro-gynaecology Service Management of Vaginal Prolapse Before reading this leaflet you should read What is vaginal prolapse? If
ARTIFICIAL MESH REPAIR FOR TREATMENT OF PELVIC ORGAN PROLAPSE
 Pelvic Floor Unit / Department of Gynaecology Ward 17, Singleton Hospital, Sketty, Swansea, SA2 8QA 01792 205666 Secretary Direct Line: 01792 285688. Fax: 01792 285874 ARTIFICIAL MESH REPAIR FOR TREATMENT
Pelvic Floor Unit / Department of Gynaecology Ward 17, Singleton Hospital, Sketty, Swansea, SA2 8QA 01792 205666 Secretary Direct Line: 01792 285688. Fax: 01792 285874 ARTIFICIAL MESH REPAIR FOR TREATMENT
Advanced Care for Female Overactive Bladder & Urinary Incontinence. Department of Urology Kaiser Permanente Santa Rosa
 Advanced Care for Female Overactive Bladder & Urinary Incontinence Department of Urology Kaiser Permanente Santa Rosa Goals Participants will: Review normal urinary tract anatomy and function Understand
Advanced Care for Female Overactive Bladder & Urinary Incontinence Department of Urology Kaiser Permanente Santa Rosa Goals Participants will: Review normal urinary tract anatomy and function Understand
Urogynaecology & Prolapse. Alexander Denning and Leifa Jennings
 + Urogynaecology & Prolapse Alexander Denning and Leifa Jennings + Contents What even is prolapse / urogynaecology? Pelvic floor anatomy Prolapse Urinary incontinence Prevention The end (woot) + Urogynaecology
+ Urogynaecology & Prolapse Alexander Denning and Leifa Jennings + Contents What even is prolapse / urogynaecology? Pelvic floor anatomy Prolapse Urinary incontinence Prevention The end (woot) + Urogynaecology
LAPAROSCOPIC REPAIR OF PELVIC FLOOR
 LAPAROSCOPIC REPAIR OF PELVIC FLOOR Dr. R. K. Mishra Elements comprising the Pelvis Bones Ilium, ischium and pubis fusion Ligaments Muscles Obturator internis muscle Arcus tendineus levator ani or white
LAPAROSCOPIC REPAIR OF PELVIC FLOOR Dr. R. K. Mishra Elements comprising the Pelvis Bones Ilium, ischium and pubis fusion Ligaments Muscles Obturator internis muscle Arcus tendineus levator ani or white
Urinary Incontinence. Lora Keeling and Byron Neale
 Urinary Incontinence Lora Keeling and Byron Neale Not life threatening. Introduction But can have a huge impact on quality of life. Two main types of urinary incontinence (UI). Stress UI leakage on effort,
Urinary Incontinence Lora Keeling and Byron Neale Not life threatening. Introduction But can have a huge impact on quality of life. Two main types of urinary incontinence (UI). Stress UI leakage on effort,
Toning your pelvic floor WELCOME
 Toning your pelvic floor WELCOME Introductions Amelia Samuels, Physiotherapist, Active Rehabilitation Physiotherapy Supporting the Continence Foundation of Australia Continence Foundation of Australia
Toning your pelvic floor WELCOME Introductions Amelia Samuels, Physiotherapist, Active Rehabilitation Physiotherapy Supporting the Continence Foundation of Australia Continence Foundation of Australia
Latest Treatments for a Leaky Bladder None
 Latest Treatments for a Leaky Bladder None Financial Disclosures Jeremiah McNamara, MD, OBGYN Boulder Women s Care 303-500-1947 Boulder Women s Care Agenda: Prolapse & Urinary Incontinence The Pelvic Floor
Latest Treatments for a Leaky Bladder None Financial Disclosures Jeremiah McNamara, MD, OBGYN Boulder Women s Care 303-500-1947 Boulder Women s Care Agenda: Prolapse & Urinary Incontinence The Pelvic Floor
INCONTINENCE. Continence and Pelvic Floor Rehabilitation TYPES OF INCONTINENCE STRESS INCONTINENCE STRESS INCONTINENCE STRESS INCONTINENCE 11/08/2015
 INCONTINENCE Continence and Pelvic Floor Rehabilitation Dr Irmina Nahon PhD Pelvic Floor Physiotherapist www.nahonpfed.com.au Defined as the accidental and inappropriate passage of urine or faeces (ICI
INCONTINENCE Continence and Pelvic Floor Rehabilitation Dr Irmina Nahon PhD Pelvic Floor Physiotherapist www.nahonpfed.com.au Defined as the accidental and inappropriate passage of urine or faeces (ICI
A PATIENT GUIDE TO Understanding Stress Urinary Incontinence
 A PATIENT GUIDE TO Understanding Stress Urinary Incontinence Q: What is SUI? A: Stress urinary incontinence is defined as the involuntary leakage of urine. The problem afflicts approximately 18 million
A PATIENT GUIDE TO Understanding Stress Urinary Incontinence Q: What is SUI? A: Stress urinary incontinence is defined as the involuntary leakage of urine. The problem afflicts approximately 18 million
Prolapse & Stress Incontinence
 Advanced Pelvic Floor Course Prolapse & Stress Incontinence OVERVIEW Day One and morning of Day Two- Pelvic Organ Prolapse The Prolapse component covers the detailed anatomy of POP including the DeLancey
Advanced Pelvic Floor Course Prolapse & Stress Incontinence OVERVIEW Day One and morning of Day Two- Pelvic Organ Prolapse The Prolapse component covers the detailed anatomy of POP including the DeLancey
Stress Incontinence. Susannah Elvy Urogynaecology CNS
 Stress Incontinence Susannah Elvy Urogynaecology CNS Definitions Prevalence Assessment Investigation Treatment Surgery Men International Continence Society define as the complaint of any involuntary leakage
Stress Incontinence Susannah Elvy Urogynaecology CNS Definitions Prevalence Assessment Investigation Treatment Surgery Men International Continence Society define as the complaint of any involuntary leakage
Pelvic organ prolapse
 Page 1 of 11 Pelvic organ prolapse Introduction The aim of this leaflet is to give you information about a pelvic organ prolapse, its causes and available treatments but does not replace advice given by
Page 1 of 11 Pelvic organ prolapse Introduction The aim of this leaflet is to give you information about a pelvic organ prolapse, its causes and available treatments but does not replace advice given by
Pelvic organ prolapse. Information for patients Continence Service
 Pelvic organ prolapse Information for patients Continence Service What is a pelvic organ prolapse? A pelvic organ prolapse occurs when the uterus (womb), vagina, bladder or bowel slips out of place, resulting
Pelvic organ prolapse Information for patients Continence Service What is a pelvic organ prolapse? A pelvic organ prolapse occurs when the uterus (womb), vagina, bladder or bowel slips out of place, resulting
Management of Female Stress Incontinence
 Management of Female Stress Incontinence Dr. Arvind Goyal Associate Professor (Urology& Renal Transplant) Dayanand Medical College & Hospital, Ludhiana, Punjab, India Stress Incontinence Involuntary loss
Management of Female Stress Incontinence Dr. Arvind Goyal Associate Professor (Urology& Renal Transplant) Dayanand Medical College & Hospital, Ludhiana, Punjab, India Stress Incontinence Involuntary loss
Surgical repair of vaginal wall prolapse using mesh
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Surgical repair of vaginal wall prolapse using mesh Vaginal wall prolapse happens when the normal support
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Surgical repair of vaginal wall prolapse using mesh Vaginal wall prolapse happens when the normal support
Surgery for vaginal vault prolapse. Patient decision aid
 Surgery for vaginal vault prolapse Patient decision aid? i What is vaginal vault prolapse? Vaginal vault prolapse happens when the top of the vagina (the vault) slips from its normal position and sags
Surgery for vaginal vault prolapse Patient decision aid? i What is vaginal vault prolapse? Vaginal vault prolapse happens when the top of the vagina (the vault) slips from its normal position and sags
9/24/2015. Pelvic Floor Disorders. Agenda. What is the Pelvic Floor? Pelvic Floor Problems
 Management of Pelvic Floor Disorders Doctor, I don t want THAT mesh! Agenda What are pelvic floor disorders (PFDs)? What are the treatment options? Expectant. Conservative. Surgical. How and when are grafts
Management of Pelvic Floor Disorders Doctor, I don t want THAT mesh! Agenda What are pelvic floor disorders (PFDs)? What are the treatment options? Expectant. Conservative. Surgical. How and when are grafts
INCONTINENCE AND OTHER UROLOGICAL DILEMMAS DR. ANNA LAWRENCE UROLOGIST AUCKLAND HOSPITAL 161 UROLOGY
 INCONTINENCE AND OTHER UROLOGICAL DILEMMAS DR. ANNA LAWRENCE UROLOGIST AUCKLAND HOSPITAL 161 UROLOGY COVERING INCONTINENCE BE ON JUST NAPPIES CATHETERS TYPES AVAILABLE AND WHEN TO USE THEM JJ STENTS???
INCONTINENCE AND OTHER UROLOGICAL DILEMMAS DR. ANNA LAWRENCE UROLOGIST AUCKLAND HOSPITAL 161 UROLOGY COVERING INCONTINENCE BE ON JUST NAPPIES CATHETERS TYPES AVAILABLE AND WHEN TO USE THEM JJ STENTS???
Stop Coping. Start Living. Talk to your doctor about pelvic organ prolapse and sacrocolpopexy
 Stop Coping. Start Living Talk to your doctor about pelvic organ prolapse and sacrocolpopexy Did you know? One in three women will suffer from a pelvic health condition in her lifetime. Four of the most
Stop Coping. Start Living Talk to your doctor about pelvic organ prolapse and sacrocolpopexy Did you know? One in three women will suffer from a pelvic health condition in her lifetime. Four of the most
Interventional procedures guidance Published: 12 October 2016 nice.org.uk/guidance/ipg566
 Single-incision short sling mesh insertion for stress urinary incontinence in women Interventional procedures guidance Published: 12 October 2016 nice.org.uk/guidance/ipg566 Your responsibility This guidance
Single-incision short sling mesh insertion for stress urinary incontinence in women Interventional procedures guidance Published: 12 October 2016 nice.org.uk/guidance/ipg566 Your responsibility This guidance
This information is intended as an overview only
 This information is intended as an overview only Please refer to the INSTRUCTIONS FOR USE included with this device for indications, contraindications, warnings, precautions and other important information
This information is intended as an overview only Please refer to the INSTRUCTIONS FOR USE included with this device for indications, contraindications, warnings, precautions and other important information
Prolapse & Urogynaecology. Hester Mannion and Fabi Sica
 Prolapse & Urogynaecology Hester Mannion and Fabi Sica Take home messages Prolapse and associated incontinence is very common It has a devastating effect on the QoL of the patient and their partner Strategies
Prolapse & Urogynaecology Hester Mannion and Fabi Sica Take home messages Prolapse and associated incontinence is very common It has a devastating effect on the QoL of the patient and their partner Strategies
Surgery for stress incontinence:
 Surgery for stress incontinence: information for you aashara Published February 2005 by the RCOG Contents Key points About this information What is stress incontinence? Do I need an operation? What operation
Surgery for stress incontinence: information for you aashara Published February 2005 by the RCOG Contents Key points About this information What is stress incontinence? Do I need an operation? What operation
Understanding Pelvic Organ Prolapse. Stephanie Pickett, MD, MS Female Pelvic Medicine and Reconstructive Surgery
 Understanding Pelvic Organ Prolapse Stephanie Pickett, MD, MS Female Pelvic Medicine and Reconstructive Surgery Disclosures None I am the daughter of a physician assistant. Objectives List types of pelvic
Understanding Pelvic Organ Prolapse Stephanie Pickett, MD, MS Female Pelvic Medicine and Reconstructive Surgery Disclosures None I am the daughter of a physician assistant. Objectives List types of pelvic
q7:480499_P0 6/5/09 10:23 AM Page 1 WHAT YOU SHOULD KNOW ABOUT YOUR DIAGNOSIS OF STRESS URINARY INCONTINENCE
 493495.q7:480499_P0 6/5/09 10:23 AM Page 1 WHAT YOU SHOULD KNOW ABOUT YOUR DIAGNOSIS OF STRESS URINARY INCONTINENCE 493495.q7:480499_P0 6/5/09 10:23 AM Page 2 What is Stress Urinary Incontinence? Urinary
493495.q7:480499_P0 6/5/09 10:23 AM Page 1 WHAT YOU SHOULD KNOW ABOUT YOUR DIAGNOSIS OF STRESS URINARY INCONTINENCE 493495.q7:480499_P0 6/5/09 10:23 AM Page 2 What is Stress Urinary Incontinence? Urinary
JMSCR Volume 03 Issue 03 Page March 2015
 www.jmscr.igmpublication.org Impact Factor 3.79 ISSN (e)-2347-176x Quality of Life among Patients after Vaginal Hysterectomy and Pelvic Floor Repair Operation ABSTRACT Authors S Lovereen 1, F A Suchi 2,
www.jmscr.igmpublication.org Impact Factor 3.79 ISSN (e)-2347-176x Quality of Life among Patients after Vaginal Hysterectomy and Pelvic Floor Repair Operation ABSTRACT Authors S Lovereen 1, F A Suchi 2,
Continence Promotion in
 Everybody s Business- Continence Promotion in Aged Care Melissa O Grady Clinical Nurse Consultant Continence Warning Some graphic images are contained in this presentation Objectives What is Old Age? What
Everybody s Business- Continence Promotion in Aged Care Melissa O Grady Clinical Nurse Consultant Continence Warning Some graphic images are contained in this presentation Objectives What is Old Age? What
Urodynamics in women. Aims of Urodynamics in women. Why do Urodynamics?
 Urodynamics in women Chendrimada Madhu MD, MA, MRCOG Subspecialty Trainee in Urogynaecology Southmead Hospital 2013 Aims of Urodynamics in women n Confirmation of incontinence and its cause n Definition
Urodynamics in women Chendrimada Madhu MD, MA, MRCOG Subspecialty Trainee in Urogynaecology Southmead Hospital 2013 Aims of Urodynamics in women n Confirmation of incontinence and its cause n Definition
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE SCOPE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Urinary incontinence in women: the management of urinary incontinence in women 1.1 Short title Urinary incontinence in women
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Urinary incontinence in women: the management of urinary incontinence in women 1.1 Short title Urinary incontinence in women
Tension-free Vaginal Tape (TVT)
") Page 1 of 7 Tension-free Vaginal Tape (TVT) Introduction This leaflet will provide you with basic information about the Tension--free Vaginal Tape (TVT) procedure. What is a TVT? TVT is an operation to
Page 1 of 7 Tension-free Vaginal Tape (TVT) Introduction This leaflet will provide you with basic information about the Tension--free Vaginal Tape (TVT) procedure. What is a TVT? TVT is an operation to
Bard: Continence Therapy. Stress Urinary Incontinence. Regaining Control. Restoring Your Lifestyle.
 Bard: Continence Therapy Stress Urinary Incontinence Regaining Control. Restoring Your Lifestyle. Stress Urinary Incontinence Urinary incontinence is a common problem and one that can be resolved by working
Bard: Continence Therapy Stress Urinary Incontinence Regaining Control. Restoring Your Lifestyle. Stress Urinary Incontinence Urinary incontinence is a common problem and one that can be resolved by working
Imaging of Pelvic Floor Weakness. Dr Susan Kouloyan-Ilic Radiologist Epworth Medical Imaging The Women s, Melbourne
 Imaging of Pelvic Floor Weakness Dr Susan Kouloyan-Ilic Radiologist Epworth Medical Imaging The Women s, Melbourne Outline Overview and Epidemiology Risk Factors, Causes and Results Review of Relevant
Imaging of Pelvic Floor Weakness Dr Susan Kouloyan-Ilic Radiologist Epworth Medical Imaging The Women s, Melbourne Outline Overview and Epidemiology Risk Factors, Causes and Results Review of Relevant
NICE guideline Published: 2 April 2019 nice.org.uk/guidance/ng123
 Urinary incontinence and pelvic organ prolapse in women: management NICE guideline Published: 2 April 2019 nice.org.uk/guidance/ng123 NICE 2019. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Urinary incontinence and pelvic organ prolapse in women: management NICE guideline Published: 2 April 2019 nice.org.uk/guidance/ng123 NICE 2019. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
What are we talking about? Symptoms. Prolapse Risk Factors. Vaginal bulge 1 Splinting. ?? Pelvic pressure Back pain 1 Urinary complaints 2
 Options for Vaginal Prolapse What are we talking about? Michelle Y. Morrill, M.D. Director of Urogynecology The Permanente Medical Group Kaiser, San Francisco Assistant Professor, Volunteer Faculty Department
Options for Vaginal Prolapse What are we talking about? Michelle Y. Morrill, M.D. Director of Urogynecology The Permanente Medical Group Kaiser, San Francisco Assistant Professor, Volunteer Faculty Department
Pelvic floor repair using Manchester technique without the need for hysterectomy. Patient Information Leaflet
 Pelvic floor repair using Manchester technique without the need for hysterectomy Patient Information Leaflet About this leaflet The information provided in this leaflet should be used as a guide. There
Pelvic floor repair using Manchester technique without the need for hysterectomy Patient Information Leaflet About this leaflet The information provided in this leaflet should be used as a guide. There
Contraception for Adolescents: What s New?
 Contraception for Adolescents: What s New? US Medical Eligibility Criteria for Contraceptive Use Kathryn M. Curtis, PhD Division of Reproductive Health, CDC Expanding Our Experience and Expertise: Implementing
Contraception for Adolescents: What s New? US Medical Eligibility Criteria for Contraceptive Use Kathryn M. Curtis, PhD Division of Reproductive Health, CDC Expanding Our Experience and Expertise: Implementing
Pelvic Organ Prolapse. Natural Solutions
 Pelvic Organ Prolapse Natural Solutions Bringing your body back to its natural state There is a very common problem affecting millions of women. Many women are too embarrassed to talk to their physicians
Pelvic Organ Prolapse Natural Solutions Bringing your body back to its natural state There is a very common problem affecting millions of women. Many women are too embarrassed to talk to their physicians
Pelvic Prolapse. A Patient Guide to Pelvic Floor Reconstruction
 Pelvic Prolapse A Patient Guide to Pelvic Floor Reconstruction Pelvic Prolapse When an organ becomes displaced, or slips down in the body, it is referred to as a prolapse. Your physician has diagnosed
Pelvic Prolapse A Patient Guide to Pelvic Floor Reconstruction Pelvic Prolapse When an organ becomes displaced, or slips down in the body, it is referred to as a prolapse. Your physician has diagnosed
Female Urinary Incontinence: What It Is and What You Can Do About It
 Female Urinary Incontinence: What It Is and What You Can Do About It Urogynecology Patient Information Sheet What is Urinary Incontinence? Stress Incontinence is a leakage of urine that occurs, for example,
Female Urinary Incontinence: What It Is and What You Can Do About It Urogynecology Patient Information Sheet What is Urinary Incontinence? Stress Incontinence is a leakage of urine that occurs, for example,
Gynaecology Department Patient Information Leaflet
 Vaginal pessaries Gynaecology Department Patient Information Leaflet Introduction We have developed this information leaflet to answer some commonly-asked questions about what a vaginal pessary is, how
Vaginal pessaries Gynaecology Department Patient Information Leaflet Introduction We have developed this information leaflet to answer some commonly-asked questions about what a vaginal pessary is, how
Management of Urinary Incontinence in Older Women. Dr. Cecilia Cheon Department of Obs. & Gyn. Queen Elizabeth Hospital
 Management of Urinary Incontinence in Older Women Dr. Cecilia Cheon Department of Obs. & Gyn. Queen Elizabeth Hospital Epidemiology Causes Investigation Treatment Conclusion Elderly Women High prevalence
Management of Urinary Incontinence in Older Women Dr. Cecilia Cheon Department of Obs. & Gyn. Queen Elizabeth Hospital Epidemiology Causes Investigation Treatment Conclusion Elderly Women High prevalence
Traditional Anterior, Posterior, and Apical Compartment Repairs A Technique Based Review
 Traditional Anterior, Posterior, and Apical Compartment Repairs A Technique Based Review Sandip Vasavada, MD Center for Female Urology and Pelvic Reconstructive Surgery The Glickman Urological and Kidney
Traditional Anterior, Posterior, and Apical Compartment Repairs A Technique Based Review Sandip Vasavada, MD Center for Female Urology and Pelvic Reconstructive Surgery The Glickman Urological and Kidney
Pelvic Support Problems
 AP012, April 2010 ACOG publications are protected by copyright and all rights are reserved. ACOG publications may not be reproduced in any form or by any means without written permission from the copyright
AP012, April 2010 ACOG publications are protected by copyright and all rights are reserved. ACOG publications may not be reproduced in any form or by any means without written permission from the copyright
12/1/13. What are Pelvic Floor Disorders? What is the Pelvic Floor? Facts. Prevalence of Urinary InconOnence. What s New in Pelvic Floor Disorders?
 What are Pelvic Floor Disorders? Urinary Control Problems - InconOnence or leakage of urine Prolapse of pelvic organs - Vagina, bladder, rectum What s New in Pelvic Floor Disorders? Kimberly Kenton MD,
What are Pelvic Floor Disorders? Urinary Control Problems - InconOnence or leakage of urine Prolapse of pelvic organs - Vagina, bladder, rectum What s New in Pelvic Floor Disorders? Kimberly Kenton MD,
Various Types. Ralph Boling, DO, FACOG
 Various Types Ralph Boling, DO, FACOG The goal of this lecture is to increase assessment and treatment abilities for physicians managing urinary incontinence (UI) patients. 1. Effectively communicate with
Various Types Ralph Boling, DO, FACOG The goal of this lecture is to increase assessment and treatment abilities for physicians managing urinary incontinence (UI) patients. 1. Effectively communicate with
URINARY INCONTINENCE. Urology Division, Surgery Department Medical Faculty, University of Sumatera Utara
 URINARY INCONTINENCE Urology Division, Surgery Department Medical Faculty, University of Sumatera Utara Definition The involuntary loss of urine May denote a symptom, a sign or a condition Symptom the
URINARY INCONTINENCE Urology Division, Surgery Department Medical Faculty, University of Sumatera Utara Definition The involuntary loss of urine May denote a symptom, a sign or a condition Symptom the
Sep \8958 Appell Dmochowski.ppt LMF 1
 Surgical Outcomes (How did we get ourselves into this mess?) Roger R. Dmochowski, MD, FACS Department of Urologic Surgery Vanderbilt University School of Medicine Nashville, Tennessee Considerations Evaluation
Surgical Outcomes (How did we get ourselves into this mess?) Roger R. Dmochowski, MD, FACS Department of Urologic Surgery Vanderbilt University School of Medicine Nashville, Tennessee Considerations Evaluation
Vaginal Hysterectomy for Uterine Prolapse. Patient Information Leaflet
 Vaginal Hysterectomy for Uterine Prolapse Patient Information Leaflet About this leaflet The information provided in this leaflet should be used as a guide. There may be some variation in how each gynaecologist
Vaginal Hysterectomy for Uterine Prolapse Patient Information Leaflet About this leaflet The information provided in this leaflet should be used as a guide. There may be some variation in how each gynaecologist
Incontinence; Lets talk about it. Karanvir Virk M.D. Minimally Invasive and Pelvic Reconstructive Surgery
 Incontinence; Lets talk about it Karanvir Virk M.D. Minimally Invasive and Pelvic Reconstructive Surgery Select the most appropriate subtitle for this talk A: Bladders gone wild! B: There s no such thing
Incontinence; Lets talk about it Karanvir Virk M.D. Minimally Invasive and Pelvic Reconstructive Surgery Select the most appropriate subtitle for this talk A: Bladders gone wild! B: There s no such thing
Management of Urogenital Prolapse of Women in Primary Care. Lizzie McManus MBE RGN RMN Practice nurse Womens health practitioner
 Management of Urogenital Prolapse of Women in Primary Care Lizzie McManus MBE RGN RMN Practice nurse Womens health practitioner Primary Care Womens Health Forum www.pcwhf.org.uk Useful websites RCN genital
Management of Urogenital Prolapse of Women in Primary Care Lizzie McManus MBE RGN RMN Practice nurse Womens health practitioner Primary Care Womens Health Forum www.pcwhf.org.uk Useful websites RCN genital
NATIONAL INSTITUTE FOR CLINICAL EXCELLENCE SCOPE. Urinary incontinence: the management of urinary incontinence in women
 NATIONAL INSTITUTE FOR CLINICAL EXCELLENCE 1 Guideline title SCOPE Urinary incontinence: the management of urinary incontinence in women 1.1 Short title Urinary incontinence 2 Background a) The National
NATIONAL INSTITUTE FOR CLINICAL EXCELLENCE 1 Guideline title SCOPE Urinary incontinence: the management of urinary incontinence in women 1.1 Short title Urinary incontinence 2 Background a) The National
Women s and Men s Health Intake Form Comprehensive Physical Therapy Center
 Name: (Last, First) DOB: Date: Age: Referring Physician: Next Physician Appointment: Today s visit: What is the main reason you came to the office today? When did it start? What treatments have you had
Name: (Last, First) DOB: Date: Age: Referring Physician: Next Physician Appointment: Today s visit: What is the main reason you came to the office today? When did it start? What treatments have you had
Uterine prolapse & Fistulas. Raja Nursing Instructor RN, DCHN, Post RN. BSc.N
 Uterine prolapse & Fistulas Raja Nursing Instructor RN, DCHN, Post RN. BSc.N 31/03/2016 Objectives 1. Review the anatomy & physiology of female reproductive system 2. Discuss the causes, pathophysiology,
Uterine prolapse & Fistulas Raja Nursing Instructor RN, DCHN, Post RN. BSc.N 31/03/2016 Objectives 1. Review the anatomy & physiology of female reproductive system 2. Discuss the causes, pathophysiology,
Tension Free vaginal tape. Mrs Ami Shukla, Consultant Urogynaecologist Northampton General Hospital Northampton NN1 5BD
 Tension Free vaginal tape Mrs Ami Shukla, Consultant Urogynaecologist Northampton General Hospital Northampton NN1 5BD What is a TVT procedure? A TVT (Tension Free Vaginal Tape) procedure is an operation
Tension Free vaginal tape Mrs Ami Shukla, Consultant Urogynaecologist Northampton General Hospital Northampton NN1 5BD What is a TVT procedure? A TVT (Tension Free Vaginal Tape) procedure is an operation
Pelvic floor exercises for women. Information for patients Continence Service
 Pelvic floor exercises for women Information for patients Continence Service page 2 of 8 Why do I need to do pelvic floor exercises? Many women experience pelvic floor problems at some time during their
Pelvic floor exercises for women Information for patients Continence Service page 2 of 8 Why do I need to do pelvic floor exercises? Many women experience pelvic floor problems at some time during their
1) What conditions is vaginal mesh used to commonly treat? Vaginal mesh is used to treat two different health issues in women:
 What conditions is vaginal mesh used to commonly treat? Vaginal mesh is used to treat two different health issues in women:") Vaginal Mesh Frequently Asked Questions 1) What conditions is vaginal mesh used to commonly treat? Vaginal mesh is used to treat two different health issues in women: a) stress urinary incontinence (SUI)
Vaginal Mesh Frequently Asked Questions 1) What conditions is vaginal mesh used to commonly treat? Vaginal mesh is used to treat two different health issues in women: a) stress urinary incontinence (SUI)
Clinical Curriculum: Urogynecology
 Updated July 201 Clinical Curriculum: Urogynecology GOAL: The primary goal of the Urogynecology rotation at the University of Alabama at Birmingham (UAB) is to train physicians to have a broad knowledge
Updated July 201 Clinical Curriculum: Urogynecology GOAL: The primary goal of the Urogynecology rotation at the University of Alabama at Birmingham (UAB) is to train physicians to have a broad knowledge
The pelvic floor is a system of muscles, ligaments, and tissues that keep your pelvic organs firmly in place.
 The pelvic floor is a system of muscles, ligaments, and tissues that keep your pelvic organs firmly in place. Think of it as the hammock of muscle that holds up your uterus, vagina, bladder, small intestine,
The pelvic floor is a system of muscles, ligaments, and tissues that keep your pelvic organs firmly in place. Think of it as the hammock of muscle that holds up your uterus, vagina, bladder, small intestine,
Instruction for the patient
 WS 4 Case 3 STI and IUD Your situation Instruction for the patient You are 32 years old, divorced and have one child; you have just started a new relationship You underwent surgical resection of the left
WS 4 Case 3 STI and IUD Your situation Instruction for the patient You are 32 years old, divorced and have one child; you have just started a new relationship You underwent surgical resection of the left
Telford and Wrekin Clinical Commissioning Group
 Telford and Wrekin Clinical Commissioning Group Agenda Item 9.2 CLINICAL COMMISSIONING GROUP GOVERNANCE BOARD EXECUTIVE SUMMARY DATE: 9 th April 2013 TITLE OF PAPER: Continence pathway and Referral letter
Telford and Wrekin Clinical Commissioning Group Agenda Item 9.2 CLINICAL COMMISSIONING GROUP GOVERNANCE BOARD EXECUTIVE SUMMARY DATE: 9 th April 2013 TITLE OF PAPER: Continence pathway and Referral letter
5/29/2015. Objectives. Functions of the PFM. Various phases of PFM. Evaluation of the PFM
 The Physical Therapist s Approach to the Female Pelvic Floor Musculature Examination and Treatment. Presented By: Evelyne Burtis, DPT Objectives Core and pelvic floor muscles (PFM) Functions of the PFM
The Physical Therapist s Approach to the Female Pelvic Floor Musculature Examination and Treatment. Presented By: Evelyne Burtis, DPT Objectives Core and pelvic floor muscles (PFM) Functions of the PFM
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of infracoccygeal sacropexy using mesh to repair uterine prolapse Uterine prolapse
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of infracoccygeal sacropexy using mesh to repair uterine prolapse Uterine prolapse
Unintended Pregnancy is Common LEARNING OBJECTIVES. Distribution Of Contraception Use By Women In The Us. Unintended Pregnancy And Contraceptive Use
 3:45 4:30 pm Beyond the Pill: Long Acting Contraceptives and IUDs Presenter Disclosure Information The following relationships exist related to this presentation: Christine L. Curry, MD, PhD: No financial
3:45 4:30 pm Beyond the Pill: Long Acting Contraceptives and IUDs Presenter Disclosure Information The following relationships exist related to this presentation: Christine L. Curry, MD, PhD: No financial
Obesity. Effect on the pelvic floor Risk for surgery. Patient Information Leaflet
 Obesity Effect on the pelvic floor Risk for surgery Patient Information Leaflet About this leaflet The information provided in this leaflet should be used as a guide. You should take your time to read
Obesity Effect on the pelvic floor Risk for surgery Patient Information Leaflet About this leaflet The information provided in this leaflet should be used as a guide. You should take your time to read
Urethral Bulking to treat Stress Urinary Incontinence. Patient Information Leaflet
 Urethral Bulking to treat Stress Urinary Incontinence Patient Information Leaflet About this leaflet The information provided in this leaflet should be used as a guide. There may be some variation in how
Urethral Bulking to treat Stress Urinary Incontinence Patient Information Leaflet About this leaflet The information provided in this leaflet should be used as a guide. There may be some variation in how
PROLAPSE. By Charlotte Robinson Women s Health Speciality Attachment
 PROLAPSE. By Charlotte Robinson Women s Health Speciality Attachment Introduction Case example Pelvic organ prolapse - Epidemiology - Aetiology - Anatomy - Types of prolapse/ severity - Examination/Investigation
PROLAPSE. By Charlotte Robinson Women s Health Speciality Attachment Introduction Case example Pelvic organ prolapse - Epidemiology - Aetiology - Anatomy - Types of prolapse/ severity - Examination/Investigation
LEARNING OBJECTIVES. Beyond the Pill: Long Acting Contraception. Distribution Of Contraception Use By Women In The Us. Unintended Pregnancy is Common
 4:15 5 pm Beyond the Pill: Long Acting Contraceptives and IUDs Presenter Disclosure Information The following relationships exist related to this presentation: Christine L. Curry, MD, PhD: No financial
4:15 5 pm Beyond the Pill: Long Acting Contraceptives and IUDs Presenter Disclosure Information The following relationships exist related to this presentation: Christine L. Curry, MD, PhD: No financial
Ina S. Irabon, MD, FPOGS, FPSRM, FPSGE Obstetrics and Gynecology Reproductive Endocrinology and Infertility Laparoscopy and Hysteroscopy
 Ina S. Irabon, MD, FPOGS, FPSRM, FPSGE Obstetrics and Gynecology Reproductive Endocrinology and Infertility Laparoscopy and Hysteroscopy Comprehensive Gynecology 7 th edition, 2017 (Lobo RA, Gershenson
Ina S. Irabon, MD, FPOGS, FPSRM, FPSGE Obstetrics and Gynecology Reproductive Endocrinology and Infertility Laparoscopy and Hysteroscopy Comprehensive Gynecology 7 th edition, 2017 (Lobo RA, Gershenson
April Clinical Focus Topic URINARY FREQUENCY
 April Clinical Focus Topic URINARY FREQUENCY This month I am focusing on a topic that may seem a little boring. But I would like to look at it from a less common perspective.urinary Frequency and its relationship
April Clinical Focus Topic URINARY FREQUENCY This month I am focusing on a topic that may seem a little boring. But I would like to look at it from a less common perspective.urinary Frequency and its relationship
Loss of Bladder Control
 BLADDER HEALTH: Surgery for Urinary Incontinence Loss of Bladder Control Surgery for Urinary Incontinence Don t Let Urinary Incontinence Keep You from Enjoying Life. What is Urinary Incontinence? What
BLADDER HEALTH: Surgery for Urinary Incontinence Loss of Bladder Control Surgery for Urinary Incontinence Don t Let Urinary Incontinence Keep You from Enjoying Life. What is Urinary Incontinence? What
Patient Information. Tension Free Vaginal/ Obturator Tape (TVT) Royal Devon and Exeter NHS Foundation Trust
 Royal Devon and Exeter NHS Foundation Trust") Tension Free Vaginal/Obturator Tape (TVT) Royal Devon and Exeter NHS Foundation Trust Patient Information Tension Free Vaginal/ Obturator Tape (TVT) Reference Number: CW 08 011 003 (version date: September
Tension Free Vaginal/Obturator Tape (TVT) Royal Devon and Exeter NHS Foundation Trust Patient Information Tension Free Vaginal/ Obturator Tape (TVT) Reference Number: CW 08 011 003 (version date: September
Treating your prolapse
 Treating your prolapse This leaflet explains what a prolapse is, and how it can be treated and managed. If you have any questions or concerns, please speak to a doctor or nurse caring for you. What is
Treating your prolapse This leaflet explains what a prolapse is, and how it can be treated and managed. If you have any questions or concerns, please speak to a doctor or nurse caring for you. What is
CLINICAL PROFILE AND MANAGEMENT OF UTEROVAGINAL PROLAPSE WITH LOWER URINARY TRACT SYMPTOM (LUTS)
") CLINICAL PROFILE AND MANAGEMENT OF UTEROVAGINAL PROLAPSE WITH LOWER URINARY TRACT SYMPTOM (LUTS) *S BEGUM 1, S SHARMIN 2, P SULTANA 3, AN CHOWDHURY 4, P SULTANA 5, S NABI 6, MN UDDIN 7, MM HASAN 8 Abstract:
CLINICAL PROFILE AND MANAGEMENT OF UTEROVAGINAL PROLAPSE WITH LOWER URINARY TRACT SYMPTOM (LUTS) *S BEGUM 1, S SHARMIN 2, P SULTANA 3, AN CHOWDHURY 4, P SULTANA 5, S NABI 6, MN UDDIN 7, MM HASAN 8 Abstract:
Provenance Rehabilitation Pelvic Intake Form
 Patient Name: Age: Weight: Gender: Male Female Provenance Rehabilitation Pelvic Intake Form Date: DOB: Occupation: Relationship Status: Hobbies / Leisure Activities: Exercise Routine: Briefly describe
Patient Name: Age: Weight: Gender: Male Female Provenance Rehabilitation Pelvic Intake Form Date: DOB: Occupation: Relationship Status: Hobbies / Leisure Activities: Exercise Routine: Briefly describe
I-STOP TOMS Transobturator Male Sling
 I-STOP TOMS Transobturator Male Sling The CL Medical I-STOP TOMS sling for male stress urinary incontinence was developed in France where it is widely used and is the market leader. It is constructed with
I-STOP TOMS Transobturator Male Sling The CL Medical I-STOP TOMS sling for male stress urinary incontinence was developed in France where it is widely used and is the market leader. It is constructed with
Introduction to GYN Specialties
 Outline Introduction to GYN Specialties Gynecologic Oncology* Female Pelvic Medicine and Reconstructive Surgery* Reproductive Endocrinology and Infertility* Pediatric and Adolescent Gynecology** Family
Outline Introduction to GYN Specialties Gynecologic Oncology* Female Pelvic Medicine and Reconstructive Surgery* Reproductive Endocrinology and Infertility* Pediatric and Adolescent Gynecology** Family
Hormone Replacement Therapy (HRT) Benefits & Risks - The Facts
 Benefits & Risks - The Facts") Hormone Replacement Therapy (HRT) Benefits & Risks - The Facts HRT is a prescription only treatment that replaces some of the lost oestrogen and progesterone hormones which occur during menopause. It can
Hormone Replacement Therapy (HRT) Benefits & Risks - The Facts HRT is a prescription only treatment that replaces some of the lost oestrogen and progesterone hormones which occur during menopause. It can
Promoting Continence with Physiotherapy
 A Common problem for Men and women Promoting Continence with Physiotherapy This leaflet contains information about physiotherapy advice and treatment for anyone with bladder and bowel problems. This may
A Common problem for Men and women Promoting Continence with Physiotherapy This leaflet contains information about physiotherapy advice and treatment for anyone with bladder and bowel problems. This may
International Federation of Gynecology and Obstetrics
 International Federation of Gynecology and Obstetrics COMMITTEE FOR UROGYNAECOLOGY AND PELVIC FLOOR MEMBER: TSUNG-HSIEN (CHARLES) SU, CHAIR (TAIWAN) DAVID RICHMOND, CO-CHAIR (UK) CHITTARANJAN PURANDARE,
International Federation of Gynecology and Obstetrics COMMITTEE FOR UROGYNAECOLOGY AND PELVIC FLOOR MEMBER: TSUNG-HSIEN (CHARLES) SU, CHAIR (TAIWAN) DAVID RICHMOND, CO-CHAIR (UK) CHITTARANJAN PURANDARE,
Loss of Bladder Control
 BLADDER HEALTH: Bladder Prolapse Loss of Bladder Control Bladder Prolapse Don t Let Bladder Prolapse Keep You from Enjoying Life. What is the Bladder? The bladder is a hollow, balloon-like organ made mostly
BLADDER HEALTH: Bladder Prolapse Loss of Bladder Control Bladder Prolapse Don t Let Bladder Prolapse Keep You from Enjoying Life. What is the Bladder? The bladder is a hollow, balloon-like organ made mostly
IF YOU VE GOT TO GO, WE VE GOT SOLUTIONS.
 IF YOU VE GOT TO GO, WE VE GOT SOLUTIONS. Get the facts about urinary incontinence and get real solutions. HENRY FORD PELVIC HEALTH & CONTINENCE CENTER HENRY FORD WOMEN S HEALTH SERVICES INCONVENIENCE?
IF YOU VE GOT TO GO, WE VE GOT SOLUTIONS. Get the facts about urinary incontinence and get real solutions. HENRY FORD PELVIC HEALTH & CONTINENCE CENTER HENRY FORD WOMEN S HEALTH SERVICES INCONVENIENCE?
Las Vegas Urogynecology
 Las Vegas Urogynecology 7500 Smoke Ranch Road - #200 Las Vegas, NV 89128 Telephone: (702) 233-0727 Fax: (702) 233-4799 Physician's Surgical Procedure Disclosure and Patient s Consent TO THE PATIENT: You
Las Vegas Urogynecology 7500 Smoke Ranch Road - #200 Las Vegas, NV 89128 Telephone: (702) 233-0727 Fax: (702) 233-4799 Physician's Surgical Procedure Disclosure and Patient s Consent TO THE PATIENT: You
An operation for stress incontinence - transobturator tape (TOT, TVT-O)
") INFORMATION FOR PATIENTS An operation for stress incontinence - transobturator tape (TOT, TVT-O) We advise you to take your time to read this leaflet. If you have any questions please write them down on
INFORMATION FOR PATIENTS An operation for stress incontinence - transobturator tape (TOT, TVT-O) We advise you to take your time to read this leaflet. If you have any questions please write them down on
Pelvic Floor Disorders. Amir Darakhshan MD FRCS (Gen Surg) Consultant Colorectal and General Surgeon
 Consultant Colorectal and General Surgeon") Pelvic Floor Disorders Amir Darakhshan MD FRCS (Gen Surg) Consultant Colorectal and General Surgeon What is Pelvic Floor Disorder Surgical perspective symptoms of RED, FI or prolapse on the background
Pelvic Floor Disorders Amir Darakhshan MD FRCS (Gen Surg) Consultant Colorectal and General Surgeon What is Pelvic Floor Disorder Surgical perspective symptoms of RED, FI or prolapse on the background
Surgical Procedures for Treatment of Pelvic Organ Prolapse in Women PATIENT INFORMATION LEAFLET
 Patient Label Surgical Procedures for Treatment of Pelvic Organ Prolapse in Women PATIENT INFORMATION LEAFLET 1 About this leaflet: This leaflet gives you detailed information about the operations being
Patient Label Surgical Procedures for Treatment of Pelvic Organ Prolapse in Women PATIENT INFORMATION LEAFLET 1 About this leaflet: This leaflet gives you detailed information about the operations being
Northeast Ohio Urogynecology Patient History Intake Form. Last Name First Name Age. Date of Birth Race Referring Physician.
 Northeast Ohio Urogynecology Patient History Intake Form Last Name _First Name Age_ Date of Birth Race Referring Physician Reason for Visit: _ Allergies: Preferred Lab (circle): QUEST LABCARE PLUS LABCORP
Northeast Ohio Urogynecology Patient History Intake Form Last Name _First Name Age_ Date of Birth Race Referring Physician Reason for Visit: _ Allergies: Preferred Lab (circle): QUEST LABCARE PLUS LABCORP