OVERVIEW OF PRESENTATION
|
|
|
- Kory Pope
- 5 years ago
- Views:
Transcription

1 Thanh D. Hoang, DO, FACP, FACE Division of Endocrinology Department of Internal Medicine WRNMMC 13 Aug 2018 OVERVIEW OF PRESENTATION Take Home Points Definition of Hypogonadism Clinical Manifestations History and Physical Examination Laboratory Studies Imaging Differential Diagnosis Hypergonadotropic Hypogonadism Hypogonadotropic Hypogonadism Andropause Chronic Illness and Androgen Replacement Therapeutic options, contraindications, side effects and guidance for surveillance. Take Home Points (again!) 1

2 Take Home Points Measure T only if reliable symptoms are suggestive. Diagnose if symptoms are consistent and T levels are unmistakably low. Determine the cause. Consider secondary causes including use of performance enhancers and age related decline. Image only if indicated. Identify patients who are likely to benefit. Know contraindications and side effects. Educate about the lack of long term safety and efficacy data supporting diagnosis and treatment. Hypogonadism; The perspective in


3 Hypogonadism; The perspective in


4 Lots of Expert$ out There Definition of Hypogonadism Definition: a clinical syndrome that results from failure of the testis to produce physiological concentrations of testosterone (T) and/or a normal number of spermatozoa due to pathology at one or more concentrations of the hypothalamic pituitary testicular axis. 4
5 Prevalence of Low Levels of Total and Bioavailable Testosterone as an Index of Male Hypogonadism According to Decade of Life Rhoden, E. L. et al. N Engl J Med 2004;350: Manifestations of Hypogonadism by Age of Onset Age of onset: In utero Varying degree of masculinity or pseudohermaphroditism Defects in testicular descent or cryptorchidism Microphallus Prepubertal: Small testes, phallus, and prostate Scant pubic and axillary hair Eunochoid body habitus Reduced male musculature Gynecomastia Persistently high pitched voice 5

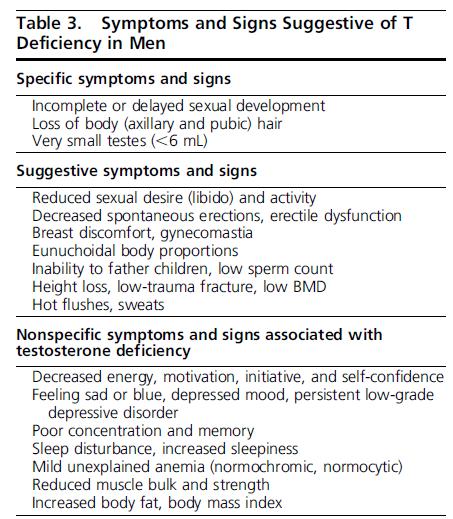
6 A 17-day-old black neonate with hermaphroditism Karam, J. A. et al. N Engl J Med 2004;350:393 Manifestations of Hypogonadism Post pubertal adult male: Diminished libido, ED, or orgasmal difficulties Increased fatigue, depressed mood. Diminished muscle mass or strength and decreased physical performance Low testicular volume Anemia Loss of body hair or decreased frequency of shaving Menopausal hot flashes or sweats Gynecomastia WHEN SHOULD A BIOCHEMICAL SCREEN BE DONE? WHAT LABS SHOULD BE ORDER? 6

7 Endocrine Society Position Statement on Literature Supporting Screening Tests for Men With High Likelihood of Hypogonadism Endo Soc: Strength of recommendation: WEAK Quality of evidence: LOW Benefit:Risk Data: NOT AVAILABLE When to Obtain Labs? NEJM 2010;363: men age years surveyed in Europe. Levels of total testosterone checked by mass spectroscopy and calculated. Univariate and multivariate analyses performed. Three symptoms consistently associated with lower testosterone levels in both analyses: Poor morning erection Low sexual desire Erectile dysfunction Physical performance 7
8 8
9 Evaluation of the Hypogonad Male Patient/Labs 1. Serum Total Testosterone: Conditions: Off of all performance enhancing supplements x 3mo 2 fasting early morning samples drawn on 2 separate occasions (30% of men normalize on second test if first test is low). Lower limit of normal range is not known; use institutional assay. If near the lower limit or mildly low, consider ordering free T from equilibrium dialysis or calculating the free fraction: (need alb, SHBG, total T) when near the lower limit of the normal range: Evaluation of the Hypogonad Male Patient/Labs 2. Sex Hormone Binding Globulin (SHBG; 60% of T is bound) SHBG low causing false decrease in total T: Obesity Hypothyroidism Acromegaly Diabetes mellitus Glucocorticoids and androgenic steroids! Nephrotic syndrome SHBG gene polymorphisms SHBG elevated causing false elevations in total T: Hyperthyroidism Liver disease (cirrhosis/ hepatitis) Severe androgen deficiency Use of Estrogens and Anticonvulsants Elderly men/ aging HIV 4. Thyroid Function Tests (Hypo/Hyperthyroid). 5. FSH, LH, Estradiol. 9
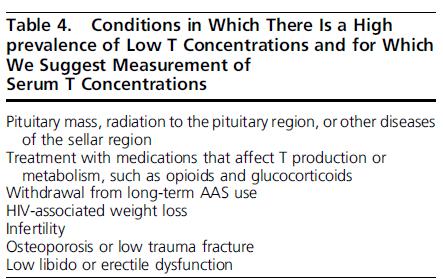
10 Evaluation of the Hypogonad Male Patient/Other Studies MRI Sella Turcica when indicated: Hypogonadotropic hypogonadism (central cause). Total testosterone < 150 ng/ml (w/low FSH and LH or inappropriately normal) Panhypopituitarism Persistent hyperprolactinemia (esp if >200) Symptoms or signs of mass effect DEXA: baseline (no studies support!) Genetic studies and karyotyping Testicular ultrasound Classification of the Biochemically Confirmed Hypogonad Patient 1. Hypergonadotropic Hypogonadism? 2. Hypogonadotropic Hypogonadism? 10
11 Classification of the Biochemically Confirmed Hypogonad Patient Hypergonadotropic Hypogonadism [ FSH LH Total Testosterone] Hypergonadotropic Hypogonadism/Common Causes [ FSH LH Total Testosterone] Klinefelter s syndrome: Incidence: 1:400 male births; pubertal manifestation 47 XXY or mosaicism Reduction (~50%) in testosterone production. Small (<2.5cm) firm testes Arm span > height; crown:pubis/pubis:floor <0.92. Taurodontism early tooth decay Partial virilization Gynecomastia 20 X risk of breast cancer Learning disabilities and dyssocial behaviors 11
![Hypergonadotropic Hypogonadism/Common Causes [ FSH LH Total Testosterone] Klinefelter s syndrome: Hypergonadotropic Hypogonadism/Common Subtypes Others: Hemochromatosis: Iron overload Primary or](/docs-images/89/99248886/images/12-0.jpg "secondary testicular failure External testicular insults: Testicular trauma or torsion AIDS or mumps orchitis Radiation or chemotherapy Autoimmune syndromes Vanishing testes syndrome: Testicular")
12 Hypergonadotropic Hypogonadism/Common Causes [ FSH LH Total Testosterone] Klinefelter s syndrome: Hypergonadotropic Hypogonadism/Common Subtypes Others: Hemochromatosis: Iron overload Primary or secondary testicular failure External testicular insults: Testicular trauma or torsion AIDS or mumps orchitis Radiation or chemotherapy Autoimmune syndromes Vanishing testes syndrome: Testicular insult during fetal life 12
13 Hypergonadotropic Hypogonadism/Other Subtypes 5 alpha reductase deficiency: Autosomal recessive Female phenotype until puberty; then virilization Elevated T:DHT ratio Myotonic dystrophy Testicular failure after age 40 Cryptorchidism Androgen receptor defects: Partial resistance Reifenstein s syndrome Male phenotype with pseudohermaphroditism Total resistance testicular feminization Female phenotype with blind vaginal pouch 47 XYY syndrome: 0.1 % of males ( supermales ). Classification of the Biochemically Confirmed Hypogonad Patient Hypogonadotropic Hypogonadism [ FSH LH Testosterone] 13
14 Etiology: Hypogonadotropic Hypogonadism/Subtypes [ FSH LH Testosterone] Use of performance enhancing supplements Use of anabolic steroids. AIDS Malnutrition Critical illness ETOH dependence Glucocorticoids Chronic narcotics use. Hyperprolactinemia Hypothyroidism Large sellar masses Hemochromatosis Kallman s Syndrome: olfactory tract maldevelopment. anosmia, short stature, hypogonadism. Andropause and the Elderly Male No consensus on definition among Endocrine Society Expert Panel Consider levels below <200 ng/dl with symptoms 14

15 Andropause and the Elderly Male: (choose your role models wisely) Andropause and the Elderly Male: Endocrine Society position statement: We recommend against a general policy of offering T to all older men with low T levels. We suggest offering T.. after explicit discussion of the uncertainty about risks and benefits. American Association of Clinical Endocrinologists: Treat if the benefit:risk ratio warrants it. We lack knowledge regarding benefit and we lack knowledge regarding risks. 15
16 Andropause and the Elderly Male If choose to treat, aim for low end of normal range for normal healthy young men ( ng/dl). Sreekumaran, K; N Eng J Med; 355; elderly men with bioavailable testosterone in the 15 th percentile of younger men. Double blind study. Supplemented with testosterone, DHEA, or placebo and followed for 2 years. Bioavailable testosterone significantly increased in treatment groups compared to the placebo group. Statistically significant (yet small) increases in fat free mass and BMD in femoral neck in testosterone treated group. No change in body composition, physical performance, insulin sensitivity, or quality of life. Liu, P et al; Clinical Review 171. JCEM 89(10): Chronic illness and low T Consider treatment if warranted: HIV/AIDS with low T & weight loss To induce/maintain body wt & lean mass gain Glucocorticoid therapy Chronic narcotic use (wounded warriors?) If you choose to treat, attempt a wean off of androgen therapy after period requiring narcotics ends 16
17 Goals for Treatment with Testosterone 1. Restore sexual function, libido, well being. 2. Produce and maintain virilization and fertility. 3. Increase hematopoiesis to normal levels. 4. Optimize bone density and prevent osteoporosis. 5. Minimize short term side effects 6. Minimize long term side effects. 1. Unknown! Contraindications for Androgen Therapy Prostate cancer. Unless S/P radical prostatectomy, disease free x 2 years, and undetectable PSA. Breast cancer Elevated Hematocrit Severe lower urinary tract symptoms Palpable prostate nodule or induration Baseline PSA>4 or >3 AND higher risk population Uncontrolled congestive heart failure. MI, acute coronary event, unstable angina, or coronary revascularization procedure in prior 6 months. Thrombophilia Untreated severe obstructive sleep apnea Men planning fertility in near term 17
18 General Side Effects of Androgen Therapy General side effects associated with use of T: Erythrocytosis Acne and oily skin Detection of subclinical prostate cancer Growth of metastatic prostate cancer Reduced sperm production and fertility Uncommon side effects: Gynecomastia Male pattern baldness (familial) Growth of breast cancer Induction or worsening of obstructive sleep apnea Androgen Therapy Options and Specific Side Effects Oral alkylated androgens (anabolics): Alkylation retards degradation by the liver Hepatotoxicity, dyslipidemia, testicular atrophy Hepatomas, peliosis of the liver Not aromatized to estrogen osteoporosis Intramuscular preparations Testosterone enanthate and cypionate mg IM q 2 weeks or mg q week. Peak 2 5 days post tx; baseline at days. The roller coaster effect (well documented). Pain at injection site Excessive erythrocytosis Cough (oil embolization? Rare.). 18

19 IM, Patch, and Gel Androgen Therapy Options and Serum Testosterone Androgen Therapy Options and Specific Side Effects Transdermal preparations: Transdermal patch (skin irritation; 5% allergic) Scrotal patch mg patches applied qhs to non pressured skin. Transdermal gel: Potential risk for testosterone transfer to person in close contact. Ok to wash site 4 6h after application. Skin irritation grams of gel applied to a covered area of skin Transbuccal preparation: 30mg bioadehesive buccal testosterone tablet applied to buccal mucosa q 12 hours. Alterations in taste. Irritation of gums and oral mucosa. Testosterone pellet preparation: Subcutaneous implant Q3 6 mo. Infection or expulsion of pellets. 19
20 20

21 Other Less Common Options for Androgen Therapy Endocrinology/Urology Infertility: Clomiphene. Gonadotropin pumps. HCG GnRH pump. Counseling Assisted reproductive technology 21
22 Monitoring Testosterone-Replacement Therapy Check baseline T, hematocrit, and PSA (if PSA indicated). If age 40yo or older obtain baseline PSA. If baseline PSA >0.6ng/mL then digital rectal exam + PSA Repeat PSA at 3 and 6 months and then defer to societal recommendations for monitoring PSA. If PSA rises > 1.4 ng/ml in 12 months OR If PSA velocity > 0.4 ng/ml in 6 months OR Detection of prostate abnormality OR severe lower urinary tract sx. Discontinue testosterone and refer! Interval: Q3 6 months after initiation then annually. Aim for T levels ng/dl after initiation. Injectables: check T 2 3 days after the injection. Take Home Points Measure T only if reliable symptoms are suggestive. Diagnose if symptoms are consistent and T levels are unmistakably low. Determine the cause. Consider secondary causes including use of performance enhancers and age related decline. Image only if indicated. Identify patients who are likely to benefit. Know contraindications and side effects. Educate about the lack of long term safety and efficacy data supporting diagnosis and treatment. 22
23 QUESTIONS? 23
Testosterone Therapy in Men with Hypogonadism
 Testosterone Therapy in Men with Hypogonadism (Endocrine Society 2018 Guideline) Ngwe Yin, MD Assistant Clinical Professor of Medicine, UCSF Fresno Medical Education Program Disclosures None Objective
Testosterone Therapy in Men with Hypogonadism (Endocrine Society 2018 Guideline) Ngwe Yin, MD Assistant Clinical Professor of Medicine, UCSF Fresno Medical Education Program Disclosures None Objective
Hypogonadism 4/27/2018. Male Hypogonadism -- Definition. Epidemiology. Objectives HYPOGONADISM. Men with Hypogonadism. 95% untreated.
 Male Hypogonadism -- Definition - Low T, Low Testosterone Hypogonadism -...a clinical syndrome that results from failure of the testes to produce physiological concentrations of testosterone due to pathology
Male Hypogonadism -- Definition - Low T, Low Testosterone Hypogonadism -...a clinical syndrome that results from failure of the testes to produce physiological concentrations of testosterone due to pathology
6/14/2010. GnRH=Gonadotropin-Releasing Hormone.
 Male Androgen Replacement Mitchell Sorsby, MD June 19, 2010. QUESTION # 1 Which of the following is not a symptom associated with low T levels? a) decreased libido b) erectile dysfunction c) depression
Male Androgen Replacement Mitchell Sorsby, MD June 19, 2010. QUESTION # 1 Which of the following is not a symptom associated with low T levels? a) decreased libido b) erectile dysfunction c) depression
Testosterone Treatment: Myths Vs Reality. Fadi Al-Khayer, M.D, F.A.C.E
 Testosterone Treatment: Myths Vs Reality Fadi Al-Khayer, M.D, F.A.C.E The Biological Functions of Testosterone in Men Testosterone is essential to the musculoskeletal and metabolic systems throughout a
Testosterone Treatment: Myths Vs Reality Fadi Al-Khayer, M.D, F.A.C.E The Biological Functions of Testosterone in Men Testosterone is essential to the musculoskeletal and metabolic systems throughout a
Evaluation and Treatment of Primary Androgen Deficiency Syndrome in Male Patients
 Evaluation and Treatment of Primary Androgen Deficiency Syndrome in Male Patients Jeff Unger, MD Director Chino Medical Group Diabetes and Headache Intervention Center Chino, California January 16, 2008
Evaluation and Treatment of Primary Androgen Deficiency Syndrome in Male Patients Jeff Unger, MD Director Chino Medical Group Diabetes and Headache Intervention Center Chino, California January 16, 2008
GUIDELINES ON. Introduction. G.R. Dohle, S. Arver, C. Bettocchi, S. Kliesch, M. Punab, W. de Ronde
 GUIDELINES ON Male Hypogonadism G.R. Dohle, S. Arver,. Bettocchi, S. Kliesch, M. Punab, W. de Ronde Introduction Male hypogonadism is a clinical syndrome caused by androgen deficiency. It may adversely
GUIDELINES ON Male Hypogonadism G.R. Dohle, S. Arver,. Bettocchi, S. Kliesch, M. Punab, W. de Ronde Introduction Male hypogonadism is a clinical syndrome caused by androgen deficiency. It may adversely
ANDROGEN DEFICIENCY/MALE HYPOGONADISM
 ANDROGEN DEFICIENCY/MALE HYPOGONADISM 1. Medical Condition Hypogonadism in men is a clinical syndrome that results from failure of the testes to produce physiological levels of testosterone (androgen deficiency)
ANDROGEN DEFICIENCY/MALE HYPOGONADISM 1. Medical Condition Hypogonadism in men is a clinical syndrome that results from failure of the testes to produce physiological levels of testosterone (androgen deficiency)
ANDROGEN DEFICIENCY/MALE HYPOGONADISM
 Medical Information to Support the Decisions of TUE Committees 1. Medical Condition Hypogonadism in men is a clinical syndrome that results from failure of the testes to produce physiological levels of
Medical Information to Support the Decisions of TUE Committees 1. Medical Condition Hypogonadism in men is a clinical syndrome that results from failure of the testes to produce physiological levels of
EAU GUIDELINES ON MALE HYPOGONADISM
 EAU GUIDELINES ON MALE HYPOGONADISM (Text update March 2015) G.R. Dohle (Chair), S. Arver, C. Bettocchi, T.H. Jones, S. Kliesch, M. Punab Introduction Male hypogonadism is a clinical syndrome caused by
EAU GUIDELINES ON MALE HYPOGONADISM (Text update March 2015) G.R. Dohle (Chair), S. Arver, C. Bettocchi, T.H. Jones, S. Kliesch, M. Punab Introduction Male hypogonadism is a clinical syndrome caused by
Recognizing and Managing Testosterone Deficiency
 Recognizing and Managing Testosterone Deficiency J. Bruce Redmon, M.D. Professor Division of Endocrinology Departments of Medicine and Urologic Surgery Disclosure Information I have no financial relationships
Recognizing and Managing Testosterone Deficiency J. Bruce Redmon, M.D. Professor Division of Endocrinology Departments of Medicine and Urologic Surgery Disclosure Information I have no financial relationships
Androgen deficiency. Dr Rakesh Iyer Staff Specialist in Endocrinology Calvary hospital
 Androgen deficiency Dr Rakesh Iyer Staff Specialist in Endocrinology Calvary hospital Outline Pathological androgen deficiency - Background, causes, interpretation - Indications for treatment Androgen
Androgen deficiency Dr Rakesh Iyer Staff Specialist in Endocrinology Calvary hospital Outline Pathological androgen deficiency - Background, causes, interpretation - Indications for treatment Androgen
GUIDELINES ON MALE HYPOGONADISM
 GUIDELINES ON MALE HYPOGONADISM (Text update March 2015) G.R. Dohle (Chair), S. Arver, C. Bettocchi, T.H. Jones, S. Kliesch, M. Punab Introduction Male hypogonadism is a clinical syndrome caused by androgen
GUIDELINES ON MALE HYPOGONADISM (Text update March 2015) G.R. Dohle (Chair), S. Arver, C. Bettocchi, T.H. Jones, S. Kliesch, M. Punab Introduction Male hypogonadism is a clinical syndrome caused by androgen
TESTOSTERONE DEFINITION
 DEFINITION A hormone that is a hydroxyl steroid ketone (C19H28O2) produced especially by the testes or made synthetically and that is responsible for inducing and maintaining male secondary sex characteristics.
DEFINITION A hormone that is a hydroxyl steroid ketone (C19H28O2) produced especially by the testes or made synthetically and that is responsible for inducing and maintaining male secondary sex characteristics.
Laboratory Investigation of Male Gonadal Function. Dr N Oosthuizen Dept of Chemical Pathology UP 2010
 Laboratory Investigation of Male Gonadal Function Dr N Oosthuizen Dept of Chemical Pathology UP 2010 1 Figure 1. Hypothalamic-pituitary pituitary-testicular testicular axis 2 Testosterone (T) measurement
Laboratory Investigation of Male Gonadal Function Dr N Oosthuizen Dept of Chemical Pathology UP 2010 1 Figure 1. Hypothalamic-pituitary pituitary-testicular testicular axis 2 Testosterone (T) measurement
EAU GUIDELINES ON MALE HYPOGONADISM
 EAU GUIDELINES ON MALE HYPOGONADISM (Limited text update March 2017) G.R. Dohle (Chair), S. Arver, C. Bettocchi, T.H. Jones, S. Kliesch Introduction Male hypogonadism is a clinical syndrome caused by androgen
EAU GUIDELINES ON MALE HYPOGONADISM (Limited text update March 2017) G.R. Dohle (Chair), S. Arver, C. Bettocchi, T.H. Jones, S. Kliesch Introduction Male hypogonadism is a clinical syndrome caused by androgen
What Is the Low T Syndrome? Is Testosterone Supplementation Safe?
 What Is the Low T Syndrome? Is Testosterone Supplementation Safe? UCSF Osher Mini Medical School March 7, 2018 Dolores Shoback, MD Staff Physician SF-VAMC Professor of Medicine, UCSF No disclosures or
What Is the Low T Syndrome? Is Testosterone Supplementation Safe? UCSF Osher Mini Medical School March 7, 2018 Dolores Shoback, MD Staff Physician SF-VAMC Professor of Medicine, UCSF No disclosures or
Index. urologic.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Acquired hypogonadism, prevalence of, 165 167 primary, 165 secondary, 167 Adipose tissue, as an organ, 240 241 Adrenal hyperplasia, congenital,
Note: Page numbers of article titles are in boldface type. A Acquired hypogonadism, prevalence of, 165 167 primary, 165 secondary, 167 Adipose tissue, as an organ, 240 241 Adrenal hyperplasia, congenital,
Testosterone Injection and Implant
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.33 Subject: Testosterone Injection Implant Page: 1 of 10 Last Review Date: December 8, 2017 Testosterone
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.33 Subject: Testosterone Injection Implant Page: 1 of 10 Last Review Date: December 8, 2017 Testosterone
Testosterone Injection / Implant
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: Testosterone Injection / Implant Page: 1 of 9 Last Review Date: December 5, 2014 Testosterone
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: Testosterone Injection / Implant Page: 1 of 9 Last Review Date: December 5, 2014 Testosterone
Late onset Hypogonadism. Dr KhooSay Chuan Department of Urology Penang General Hospital
 Late onset Hypogonadism Dr KhooSay Chuan Department of Urology Penang General Hospital Late onset hypogonadism(loh) Definition LOH age associated testoteronedeficiency syndrome (TDS) Male menopause, andropause,
Late onset Hypogonadism Dr KhooSay Chuan Department of Urology Penang General Hospital Late onset hypogonadism(loh) Definition LOH age associated testoteronedeficiency syndrome (TDS) Male menopause, andropause,
GA KS KY LA MD NJ NV NY TN TX WA Applicable X X N/A N/A X N/A X X X X X X N/A N/A NA *FHK- Florida Healthy Kids. Androgens
 Androgens Override(s) Prior Authorization Quantity Limit Approval Duration Varies upon diagnosis Medication Strengths Quantity Limit Comments Generic Androgel 1% (2.5 g) packet 2 packets per day (testosterone
Androgens Override(s) Prior Authorization Quantity Limit Approval Duration Varies upon diagnosis Medication Strengths Quantity Limit Comments Generic Androgel 1% (2.5 g) packet 2 packets per day (testosterone
Testosterone Injection and Implant
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.33 Subject: Testosterone Injection Implant Page: 1 of 10 Last Review Date: November 30, 2018 Testosterone
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.33 Subject: Testosterone Injection Implant Page: 1 of 10 Last Review Date: November 30, 2018 Testosterone
BIOCHEMICAL TESTS FOR THE INVESTIGATION OF COMMON ENDOCRINE PROBLEMS IN THE MALE
 Authoriser: Moya O Doherty Page 1 of 7 BIOCHEMICAL TESTS FOR THE INVESTIGATION OF COMMON ENDOCRINE PROBLEMS IN THE MALE The purpose of this protocol is to describe common tests used for the investigation
Authoriser: Moya O Doherty Page 1 of 7 BIOCHEMICAL TESTS FOR THE INVESTIGATION OF COMMON ENDOCRINE PROBLEMS IN THE MALE The purpose of this protocol is to describe common tests used for the investigation
Testosterone Injection and Implant
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.33 Subject: Testosterone Injection Implant Page: 1 of 10 Last Review Date: March 17, 2017 Testosterone
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.33 Subject: Testosterone Injection Implant Page: 1 of 10 Last Review Date: March 17, 2017 Testosterone
Male Hypogonadism. Types and causes of hypogonadism. What is male hypogonadism? Symptoms. Testosterone production. Patient Information.
 Patient Information English 31 Male Hypogonadism The underlined terms are listed in the glossary. What is male hypogonadism? Male hypogonadism means the testicles do not produce enough of the male sex
Patient Information English 31 Male Hypogonadism The underlined terms are listed in the glossary. What is male hypogonadism? Male hypogonadism means the testicles do not produce enough of the male sex
Testosterone Oral Buccal Nasal. Android, Androxy, Methitest, Natesto, Striant, Testred. Description
 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.32 Subject: Testosterone Oral Buccal Nasal Page: 1 of 10 Last Review Date: March 17, 2017 Testosterone Oral Buccal Nasal Description
1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.32 Subject: Testosterone Oral Buccal Nasal Page: 1 of 10 Last Review Date: March 17, 2017 Testosterone Oral Buccal Nasal Description
Androderm patch, AndroGel packets and pump, Axiron solution, First- Testosterone, First-Testosterone MC, Fortesta gel, Testim gel, Vogelxo
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.31 Subject: Testosterone Topical Page: 1 of 9 Last Review Date: September 23, 2016 Testosterone topical
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.31 Subject: Testosterone Topical Page: 1 of 9 Last Review Date: September 23, 2016 Testosterone topical
ISSM QUICK REFERENCE GUIDE ON TESTOSTERONE DEFICIENCY FOR MEN
 International Society for Sexual Medicine - www.issm.info ISSM QUICK REFERENCE GUIDE ON TESTOSTERONE DEFICIENCY FOR MEN Version: September 2015 What is testosterone deficiency? Testosterone deficiency
International Society for Sexual Medicine - www.issm.info ISSM QUICK REFERENCE GUIDE ON TESTOSTERONE DEFICIENCY FOR MEN Version: September 2015 What is testosterone deficiency? Testosterone deficiency
Testosterone Therapy in Men with Androgen Deficiency Syndromes: An Endocrine Society Clinical Practice Guideline
 SPECIAL FEATURE Clinical Practice Guideline Testosterone Therapy in Men with Androgen Deficiency Syndromes: An Endocrine Society Clinical Practice Guideline Shalender Bhasin, Glenn R. Cunningham, Frances
SPECIAL FEATURE Clinical Practice Guideline Testosterone Therapy in Men with Androgen Deficiency Syndromes: An Endocrine Society Clinical Practice Guideline Shalender Bhasin, Glenn R. Cunningham, Frances
Clinical evaluation of infertility
 Clinical evaluation of infertility DR. FARIBA KHANIPOUYANI OBSTETRICIAN & GYNECOLOGIST PRENATOLOGIST Definition: inability to achieve conception despite one year of frequent unprotected intercourse. Male
Clinical evaluation of infertility DR. FARIBA KHANIPOUYANI OBSTETRICIAN & GYNECOLOGIST PRENATOLOGIST Definition: inability to achieve conception despite one year of frequent unprotected intercourse. Male
ANDROGEN DEFICIENCY Update on Evaluation and Management
 ANDROGEN DEFICIENCY Update on Evaluation and Management Kristen Gill Hairston, MD, MPH Associate Professor of Internal Medicine Section of Endocrinology and Metabolism Wake Forest University School of
ANDROGEN DEFICIENCY Update on Evaluation and Management Kristen Gill Hairston, MD, MPH Associate Professor of Internal Medicine Section of Endocrinology and Metabolism Wake Forest University School of
Testosterone Oral Buccal Nasal. Android, Androxy, Methitest, Natesto, Striant, Testred. Description
 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.32 Subject: Testosterone Oral Buccal Nasal Page: 1 of 10 Last Review Date: November 30, 2018 Testosterone Oral Buccal Nasal
1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.32 Subject: Testosterone Oral Buccal Nasal Page: 1 of 10 Last Review Date: November 30, 2018 Testosterone Oral Buccal Nasal
Corporate Medical Policy Testosterone Pellet Implantation for Androgen Deficiency
 Corporate Medical Policy Testosterone Pellet Implantation for Androgen Deficiency File Name: Origination: Last CAP Review: Next CAP Review: Last Review: testosterone_pellet_implantation_for_androgen_deficiency
Corporate Medical Policy Testosterone Pellet Implantation for Androgen Deficiency File Name: Origination: Last CAP Review: Next CAP Review: Last Review: testosterone_pellet_implantation_for_androgen_deficiency
Pharmacy Coverage Guidelines are subject to change as new information becomes available.
 TESTOSTERONE REPLACEMENT THERAPY: ANDRODERM transdermal patch ANDROGEL pump transdermal gel and transdermal gel AXIRON transdermal solution FORTESTA transdermal gel NATESTO nasal gel STRIANT buccal mucoadhesive
TESTOSTERONE REPLACEMENT THERAPY: ANDRODERM transdermal patch ANDROGEL pump transdermal gel and transdermal gel AXIRON transdermal solution FORTESTA transdermal gel NATESTO nasal gel STRIANT buccal mucoadhesive
Low Testosterone Consultation Information
 T Low Testosterone Consultation Information www.urologyaustin.com Andropause or Male Menopause This syndrome has been nicknamed ADAM, which stands for androgen deficiency of the aging male. It differs
T Low Testosterone Consultation Information www.urologyaustin.com Andropause or Male Menopause This syndrome has been nicknamed ADAM, which stands for androgen deficiency of the aging male. It differs
Testosterone Oral Buccal Nasal. Android, Androxy, Methitest, Natesto, Striant, Testred. Description
 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.32 Subject: Testosterone Oral Buccal Nasal Page: 1 of 10 Last Review Date: June 24, 2016 Testosterone Oral Buccal Nasal Description
1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.32 Subject: Testosterone Oral Buccal Nasal Page: 1 of 10 Last Review Date: June 24, 2016 Testosterone Oral Buccal Nasal Description
Why is my body not changing? Conflicts of interest. Overview 11/9/2015. None
 Why is my body not changing? Murthy Korada Pediatrician, Pediatric Endocrinologist Ridge Meadows Hospital Surrey Memorial Hospital None Conflicts of interest Overview Overview of normal pubertal timing
Why is my body not changing? Murthy Korada Pediatrician, Pediatric Endocrinologist Ridge Meadows Hospital Surrey Memorial Hospital None Conflicts of interest Overview Overview of normal pubertal timing
Testosterone Therapy in Men With Hypogonadism: An Endocrine Society* Clinical Practice Guideline
 CLINICAL PRACTICE GUIDELINE Testosterone Therapy in Men With Hypogonadism: An Endocrine Society* Clinical Practice Guideline Shalender Bhasin, 1 Juan P. Brito, 2 Glenn R. Cunningham, 3 Frances J. Hayes,
CLINICAL PRACTICE GUIDELINE Testosterone Therapy in Men With Hypogonadism: An Endocrine Society* Clinical Practice Guideline Shalender Bhasin, 1 Juan P. Brito, 2 Glenn R. Cunningham, 3 Frances J. Hayes,
Pharmacy Coverage Guidelines are subject to change as new information becomes available.
 TESTOSTERONE REPLACEMENT THERAPY: ANDRODERM transdermal patch ANDROGEL pump transdermal gel and transdermal gel ANDROID (methyltestosterone) oral capsule ANDROXY (fluoxymesterone) oral tablet AXIRON transdermal
TESTOSTERONE REPLACEMENT THERAPY: ANDRODERM transdermal patch ANDROGEL pump transdermal gel and transdermal gel ANDROID (methyltestosterone) oral capsule ANDROXY (fluoxymesterone) oral tablet AXIRON transdermal
in Primary Care (Part 2) Jonathan R. Anolik, MD, FACP, FACE Lewis Katz School of Medicine at Temple University
 Jonathan R. Anolik, MD, FACP, FACE Lewis Katz School of Medicine at Temple University") Common Endocrine Problems Seen in Primary Care (Part 2) Lecture #34 Jonathan R. Anolik, MD, FACP, FACE Lewis Katz School of Medicine at Temple University None Conflict of Interest Topics to be Covered
Common Endocrine Problems Seen in Primary Care (Part 2) Lecture #34 Jonathan R. Anolik, MD, FACP, FACE Lewis Katz School of Medicine at Temple University None Conflict of Interest Topics to be Covered
Androgens. Medication Strengths Quantity Limit Comments Androderm (testosterone patch) 1% pump 2 pump bottles per Non-Preferred
 1% pump 2 pump bottles per Non-Preferred") Market DC Androgens Override(s) Prior Authorization Quantity Limit Approval Duration Varies upon diagnosis Medication Strengths Quantity Limit Comments Androderm (testosterone patch) AndroGel (testosterone
Market DC Androgens Override(s) Prior Authorization Quantity Limit Approval Duration Varies upon diagnosis Medication Strengths Quantity Limit Comments Androderm (testosterone patch) AndroGel (testosterone
Prior Authorization Criteria Update: Androgens, Topical and Parenteral
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
How to treat: TRT modalities and formulations
 How to treat: TRT modalities and formulations Paul PIETTE, PharmD Senior Research Fellow Clinique Antoine Depage - Belgium ppiette@besins-healthcare.com Bruges 2014, May 15 th Testosterone-replacement
How to treat: TRT modalities and formulations Paul PIETTE, PharmD Senior Research Fellow Clinique Antoine Depage - Belgium ppiette@besins-healthcare.com Bruges 2014, May 15 th Testosterone-replacement
PUBERTY. Preetha Krishnamoorthy. Division of Pediatric Endocrinology
 PUBERTY Preetha Krishnamoorthy Division of Pediatric Endocrinology Case 1 8-year-old girl referred for breast development noted by mom What do you want to know? Normal or abnormal? What if this was an
PUBERTY Preetha Krishnamoorthy Division of Pediatric Endocrinology Case 1 8-year-old girl referred for breast development noted by mom What do you want to know? Normal or abnormal? What if this was an
TUE Physician Guidelines Medical Information to Support the Decisions of TUE Committees MALE HYPOGONADISM MALE HYPOGONADISM
 1. Medical Condition Hypogonadism in men is a clinical syndrome that results from failure of the testes to produce physiological levels of testosterone (testosterone deficiency) and in some instances normal
1. Medical Condition Hypogonadism in men is a clinical syndrome that results from failure of the testes to produce physiological levels of testosterone (testosterone deficiency) and in some instances normal
Clinical Policy: Testosterone Pellet (Testopel) Reference Number: CP.CPA.## [Pre-P&T approval] Effective Date:
![Clinical Policy: Testosterone Pellet (Testopel) Reference Number: CP.CPA.## [Pre-P&T approval] Effective Date:](/thumbs/75/72057018.jpg "Clinical Policy: Testosterone Pellet (Testopel) Reference Number: CP.CPA.## [Pre-P&T approval] Effective Date:") Clinical Policy: (Testopel) Reference Number: CP.CPA.## [Pre-P&T approval] Effective Date: 07.25.17 Last Review Date: 11.17 Line of Business: Commercial Coding Implications Revision Log See Important Reminder
Clinical Policy: (Testopel) Reference Number: CP.CPA.## [Pre-P&T approval] Effective Date: 07.25.17 Last Review Date: 11.17 Line of Business: Commercial Coding Implications Revision Log See Important Reminder
Testosterone Therapy in Adult Men with Androgen Deficiency Syndromes:
 The Endocrine Society s CLINICAL GUIDELINES Testosterone Therapy in Adult Men with Androgen Deficiency Syndromes: An Endocrine Society Clinical Practice Guideline Authors: Shalender Bhasin, Glenn R. Cunningham,
The Endocrine Society s CLINICAL GUIDELINES Testosterone Therapy in Adult Men with Androgen Deficiency Syndromes: An Endocrine Society Clinical Practice Guideline Authors: Shalender Bhasin, Glenn R. Cunningham,
Male History, Clinical Examination and Testing
 Male History, Clinical Examination and Testing Dirk Vanderschueren, MD, PhD Case Jan is 29 years old and consults for 1 year primary subfertility partner 28 years old and normal gynaecological investigation
Male History, Clinical Examination and Testing Dirk Vanderschueren, MD, PhD Case Jan is 29 years old and consults for 1 year primary subfertility partner 28 years old and normal gynaecological investigation
Reproductive Health and Pituitary Disease
 Reproductive Health and Pituitary Disease Janet F. McLaren, MD Assistant Professor Division of Reproductive Endocrinology and Infertility Department of Obstetrics and Gynecology jmclaren@uabmc.edu Objectives
Reproductive Health and Pituitary Disease Janet F. McLaren, MD Assistant Professor Division of Reproductive Endocrinology and Infertility Department of Obstetrics and Gynecology jmclaren@uabmc.edu Objectives
John Sutton, DO, FACOI, FACE, CCD. Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989
 John Sutton, DO, FACOI, FACE, CCD Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989 Gonadal Physiology and Disease 3 No Disclosures Gonadal Axis Hypothalamic-pituitary-gonadal Feedback mechanisms
John Sutton, DO, FACOI, FACE, CCD Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989 Gonadal Physiology and Disease 3 No Disclosures Gonadal Axis Hypothalamic-pituitary-gonadal Feedback mechanisms
5/7/2013. Patrick Nolan, DO, FACE
 Patrick Nolan, DO, FACE Patient: T.W. 83 year old male 9/18/2012 AM sudden onset of Vertigo ER visit Had MRI, some labs Home on Zofran and medicines Complete resolution of sx after 2 days MRI chronic sinus
Patrick Nolan, DO, FACE Patient: T.W. 83 year old male 9/18/2012 AM sudden onset of Vertigo ER visit Had MRI, some labs Home on Zofran and medicines Complete resolution of sx after 2 days MRI chronic sinus
A dro r gen e R e R p e lac a e c m e e m n e t t T her e a r p a y Androgen Replacement Therapy in the Aging O j b ecti t ve v s Male
 Androgen Replacement Therapy in the Aging Male Thomas J. Walsh, MD, MS Department of Urology University of California, San Francisco Objectives 1. List 3 effects of androgens on normal male physiology.
Androgen Replacement Therapy in the Aging Male Thomas J. Walsh, MD, MS Department of Urology University of California, San Francisco Objectives 1. List 3 effects of androgens on normal male physiology.
Testosterone (cypionate, enanthate, and propionate) powder, Fluoxymesterone powder, Methyltestosterone powder
 powder, Fluoxymesterone powder, Methyltestosterone powder") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.37 Subject: Testosterone Powder Page: 1 of 12 Last Review Date: November 30, 2018 Testosterone powder
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.37 Subject: Testosterone Powder Page: 1 of 12 Last Review Date: November 30, 2018 Testosterone powder
Implantable Hormone Pellets
 Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Hormone Balance - Female Report SAMPLE. result graph based on Luteal Phase. result graph based on Luteal Phase
 Patient Name: Patient DOB: Gender: Physician: Test Hormone Balance - Female Report SAMPLE Grote, Mary Jane Batch Number: B6437 2/16/1954 Accession Number: N52281 F Date Received: 2/3/2015 Any Lab Test
Patient Name: Patient DOB: Gender: Physician: Test Hormone Balance - Female Report SAMPLE Grote, Mary Jane Batch Number: B6437 2/16/1954 Accession Number: N52281 F Date Received: 2/3/2015 Any Lab Test
Late onset hypogonadism
 Late onset hypogonadism Farrukh Javid Male Menopause Clinical AND biochemical syndrome Testosterone levels decline by 0.4-3% per year after the age of 30, as opposed to the more rapid decline that occurs
Late onset hypogonadism Farrukh Javid Male Menopause Clinical AND biochemical syndrome Testosterone levels decline by 0.4-3% per year after the age of 30, as opposed to the more rapid decline that occurs
Consent for Testosterone Therapy-Men Revised 4/10/18
 Consent for Testosterone Therapy in Men You have been diagnosed with or have an increased risk of having a hormone deficiency and your provider has recommended treatment with bio-identical hormone replacement
Consent for Testosterone Therapy in Men You have been diagnosed with or have an increased risk of having a hormone deficiency and your provider has recommended treatment with bio-identical hormone replacement
Testosterone (cypionate, enanthate, and propionate) powder, Fluoxymesterone powder, Methyltestosterone powder
 powder, Fluoxymesterone powder, Methyltestosterone powder") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.08.37 Subject: Testosterone Powder Page: 1 of 11 Last Review Date: September 18, 2015 Testosterone powder
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.08.37 Subject: Testosterone Powder Page: 1 of 11 Last Review Date: September 18, 2015 Testosterone powder
HYPOGONADISM DEFINITION: PRODUCTION OF SEX HORMONES AND GERM CELLS IS INADEQUATE (ENDOCRINE SOCIETY)
") HYPOGONADISM DEFINITION: PRODUCTION OF SEX HORMONES AND GERM CELLS IS INADEQUATE (ENDOCRINE SOCIETY) DEFECT OF THE REPRODUCTIVE SYSTEM THAT RESULTS IN LACK OF FUNCTION OF THE GONADS (Wikipedia) REDUCTION
HYPOGONADISM DEFINITION: PRODUCTION OF SEX HORMONES AND GERM CELLS IS INADEQUATE (ENDOCRINE SOCIETY) DEFECT OF THE REPRODUCTIVE SYSTEM THAT RESULTS IN LACK OF FUNCTION OF THE GONADS (Wikipedia) REDUCTION
Prof. Dr. Michael Zitzmann Internal Medicine Endocrinology, Diabetology, Andrology University of Muenster, Germany
 Induction of fertility in hypogonadal men Prof. Dr. Michael Zitzmann Internal Medicine Endocrinology, Diabetology, Andrology University of Muenster, Germany Induction of fertility in hypogonadal men Prof.
Induction of fertility in hypogonadal men Prof. Dr. Michael Zitzmann Internal Medicine Endocrinology, Diabetology, Andrology University of Muenster, Germany Induction of fertility in hypogonadal men Prof.
OBJECTIVES. Rebecca McEachern, MD. Puberty: Too early, Too Late or Just Right? Special Acknowledgements. Maryann Johnson M.Ed.
 1 Puberty: Too early, Too Late or Just Right? Maryann Johnson M.Ed., BSN, RN Special Acknowledgements Rebecca McEachern, MD OBJECTIVES Illustrate basic endocrine system and hormonal pathways Define the
1 Puberty: Too early, Too Late or Just Right? Maryann Johnson M.Ed., BSN, RN Special Acknowledgements Rebecca McEachern, MD OBJECTIVES Illustrate basic endocrine system and hormonal pathways Define the
Implantable Hormone Pellets
 Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
TUE Application for Testosterone Physician Worksheet
 TUE Application for Testosterone Physician Worksheet Attention Physicians - USADA will not process Therapeutic Use Exemptions (TUE) for the use of testosterone unless all of the requirements for documentation
TUE Application for Testosterone Physician Worksheet Attention Physicians - USADA will not process Therapeutic Use Exemptions (TUE) for the use of testosterone unless all of the requirements for documentation
66 M with erectile dysfunction and abnormal labs RAJESH JAIN ENDORAMA 10/29/2015
 66 M with erectile dysfunction and abnormal labs RAJESH JAIN ENDORAMA 10/29/2015 HPI 66 M presenting as a referral for erectile dysfunction and abnormal labs Has been seeing a facility specializing in
66 M with erectile dysfunction and abnormal labs RAJESH JAIN ENDORAMA 10/29/2015 HPI 66 M presenting as a referral for erectile dysfunction and abnormal labs Has been seeing a facility specializing in
Prof Dato Dr TAN Hui Meng University of Malaya, Kuala Lumpur University of Pennsylvania, USA
 Prof Dato Dr TAN Hui Meng University of Malaya, Kuala Lumpur University of Pennsylvania, USA Prevailing context Increase number of men who are potential candidates for Testosterone Replacement Therapy
Prof Dato Dr TAN Hui Meng University of Malaya, Kuala Lumpur University of Pennsylvania, USA Prevailing context Increase number of men who are potential candidates for Testosterone Replacement Therapy
Disclosures. Learning Objectives. Effects of Hormone Therapy on the Metabolic Syndrome and Cardiovascular Disease. None
 Effects of Hormone Therapy on the Metabolic Syndrome and Cardiovascular Disease Micol S. Rothman, MD Associate Professor of Medicine Endocrinology, Diabetes and Metabolism Clinical Director Metabolic Bone
Effects of Hormone Therapy on the Metabolic Syndrome and Cardiovascular Disease Micol S. Rothman, MD Associate Professor of Medicine Endocrinology, Diabetes and Metabolism Clinical Director Metabolic Bone
Puberty and Pubertal Disorders Part 3: Delayed Puberty
 PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Puberty and Pubertal Disorders Part 3: Delayed Puberty These podcasts are designed to give medical students an overview
PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Puberty and Pubertal Disorders Part 3: Delayed Puberty These podcasts are designed to give medical students an overview
Point-Counterpoint: Late Onset Hypogonadism (LOH)
") Point-Counterpoint: Late Onset Hypogonadism (LOH) We are Under-diagnosing and Treating Men with LOH LOH is a Non-existent Disease ~ Robert E. Donohue, MD Late Onset Hypogonadism LOH: underdx. & undertx
Point-Counterpoint: Late Onset Hypogonadism (LOH) We are Under-diagnosing and Treating Men with LOH LOH is a Non-existent Disease ~ Robert E. Donohue, MD Late Onset Hypogonadism LOH: underdx. & undertx
Board Review with The Chiefs. October 17, 2016 October 23, 2016
 Board Review with The Chiefs October 17, 2016 October 23, 2016 Overview Registration Exam Details Test Day Details Study Resources Study Strategies Women s Health Men s Health What to Expect: Exam Registration
Board Review with The Chiefs October 17, 2016 October 23, 2016 Overview Registration Exam Details Test Day Details Study Resources Study Strategies Women s Health Men s Health What to Expect: Exam Registration
More than meets the eye
 More than meets the eye Ana Paula Abreu, MD, PhD American Association of Clinical Endocrinologists New England Chapter Annual Meeting September 8, 2018 Disclosures No conflict of interest or significant
More than meets the eye Ana Paula Abreu, MD, PhD American Association of Clinical Endocrinologists New England Chapter Annual Meeting September 8, 2018 Disclosures No conflict of interest or significant
Hypogonadism and Testosterone Replacement Therapy: Pharmacist
 Hypogonadism and Testosterone Replacement Therapy: Practical Insights for the Pharmacist Roger G. Hefflinger, PharmD Associate Professor of Pharmacy Practice and Administrative Services Idaho State University,
Hypogonadism and Testosterone Replacement Therapy: Practical Insights for the Pharmacist Roger G. Hefflinger, PharmD Associate Professor of Pharmacy Practice and Administrative Services Idaho State University,
DEFINITION HX & PH/EX
 DEFINITION HX & PH/EX Because of the success of the assisted reproductive techniques (ART), the evaluation of the man is often ignored. The physician should not forget the fact that many causes of male
DEFINITION HX & PH/EX Because of the success of the assisted reproductive techniques (ART), the evaluation of the man is often ignored. The physician should not forget the fact that many causes of male
Basics of Male Libido: Dysfunction & Treatment. Ripu Hundal MD FACE First State Endocrinology Newark, DE
 Basics of Male Libido: Dysfunction & Treatment Ripu Hundal MD FACE First State Endocrinology Newark, DE Sexual Hormones Steroid hormones Commonly referred to as male sex hormones and female sex hormones,
Basics of Male Libido: Dysfunction & Treatment Ripu Hundal MD FACE First State Endocrinology Newark, DE Sexual Hormones Steroid hormones Commonly referred to as male sex hormones and female sex hormones,
Over the past decade, androgen replacement
 J. Andrew Hoover, MD; Jeffrey T. Kirchner, DO, FAAFP Department of Family and Community Medicine, Lancaster General Hospital, Pa jhoover4@lghealth.org The authors reported no potential conflict of interest
J. Andrew Hoover, MD; Jeffrey T. Kirchner, DO, FAAFP Department of Family and Community Medicine, Lancaster General Hospital, Pa jhoover4@lghealth.org The authors reported no potential conflict of interest
IOWA MEDICAID DRUG UTILIZATION REVIEW COMMISSION 100 Army Post Road 5)
") IOWA MEDICAID DRUG UTILIZATION REVIEW COMMISSION 100 Army Post Road 5) 974-3131 -866-626-0216 Brett Faine, Pharm.D. Larry Ambroson, R.Ph. Brian Couse, M.D. Date: February 10, 2015 Mark Graber, M.D., FACEP,
IOWA MEDICAID DRUG UTILIZATION REVIEW COMMISSION 100 Army Post Road 5) 974-3131 -866-626-0216 Brett Faine, Pharm.D. Larry Ambroson, R.Ph. Brian Couse, M.D. Date: February 10, 2015 Mark Graber, M.D., FACEP,
Didactic Series. Hypogonadism and HIV. Daniel Lee, MD UCSD Medical Center, Owen Clinic July 28, 2016
 Didactic Series Hypogonadism and HIV Daniel Lee, MD UCSD Medical Center, Owen Clinic July 28, 2016 This project is supported by the Health Resources and Services Administration (HRSA) of the U.S. Department
Didactic Series Hypogonadism and HIV Daniel Lee, MD UCSD Medical Center, Owen Clinic July 28, 2016 This project is supported by the Health Resources and Services Administration (HRSA) of the U.S. Department
43 year old man with low libido. Katie Stanley, MD August 16, 2012
 43 year old man with low libido Katie Stanley, MD August 16, 2012 HPI 43 yo M with history of heroin addiction on methadone maintenance Reported low libido to PCP PCP checked testosterone and found to
43 year old man with low libido Katie Stanley, MD August 16, 2012 HPI 43 yo M with history of heroin addiction on methadone maintenance Reported low libido to PCP PCP checked testosterone and found to
Sexual dysfunction of chronic kidney disease. Razieh salehian.md psychiatrist
 Sexual dysfunction of chronic kidney disease Razieh salehian.md psychiatrist Disturbances in sexual function are a common feature of chronic renal failure. Sexual dysfunction is inversely associated with
Sexual dysfunction of chronic kidney disease Razieh salehian.md psychiatrist Disturbances in sexual function are a common feature of chronic renal failure. Sexual dysfunction is inversely associated with
3 year old boy with puberty. Katie Stanley, MD August 1, 2013
 3 year old boy with puberty Katie Stanley, MD August 1, 2013 Initial presentation 3 and 11/12 year old boy with signs of puberty Presented to outside endocrinologist in 2002 with: Pubic hair since 2.5
3 year old boy with puberty Katie Stanley, MD August 1, 2013 Initial presentation 3 and 11/12 year old boy with signs of puberty Presented to outside endocrinologist in 2002 with: Pubic hair since 2.5
Diagnosis and Clinical Evaluation of Hypogonadism in Adult Patients with Obesity and Diabetes
 Diagnosis and Clinical Evaluation of Hypogonadism in Adult Patients with Obesity and Diabetes Adrian Dobs, M.D., M.H.S. Professor of Medicine and Oncology The Johns Hopkins University School of Medicine
Diagnosis and Clinical Evaluation of Hypogonadism in Adult Patients with Obesity and Diabetes Adrian Dobs, M.D., M.H.S. Professor of Medicine and Oncology The Johns Hopkins University School of Medicine
HIGHLIGHTS. From Testosterone Update Disease State Theater. American Urological Association and Endocrine Society Annual Meetings
 HIGHLIGHTS From Testosterone Update Disease State Theater Presentations held at the 2008 American Urological Association and Endocrine Society Annual Meetings Jointly sponsored by the Annenberg Center
HIGHLIGHTS From Testosterone Update Disease State Theater Presentations held at the 2008 American Urological Association and Endocrine Society Annual Meetings Jointly sponsored by the Annenberg Center
Endocrine Update Mary T. Korytkowski MD Division of Endocrinology University of Pittsburgh
 Endocrine Update 2016 Mary T. Korytkowski MD Division of Endocrinology University of Pittsburgh Disclosure of Financial Relationships Mary Korytkowski MD Honoraria British Medical Journal Diabetes Research
Endocrine Update 2016 Mary T. Korytkowski MD Division of Endocrinology University of Pittsburgh Disclosure of Financial Relationships Mary Korytkowski MD Honoraria British Medical Journal Diabetes Research
Growth hormone therapy in a girl with Turner syndrome showing a large increase over the initially predicted ht of 4 5
 Disorders of Growth and Puberty: How to Recognize the Normal Variants vs Patients Who Need to be Evaluated Paul Kaplowitz, M.D Pediatric Endocrinology. VCU School of Medicine Interpretation of Growth Charts
Disorders of Growth and Puberty: How to Recognize the Normal Variants vs Patients Who Need to be Evaluated Paul Kaplowitz, M.D Pediatric Endocrinology. VCU School of Medicine Interpretation of Growth Charts
Hypogonadism in Men. CME Away India & Sri Lanka March 23 - April 7, 2018
 Hypogonadism in Men CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi Copyright 2017
Hypogonadism in Men CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi Copyright 2017
Hormone Replacement Therapy
 Hormone Replacement Therapy What Role Should It Play With Our Patients? Noel R. Williams MD, FACOG TESTOSTERONE FOR MEN: SALVATION OR SNAKE OIL? Definition Male hypogonadism means the testicles don't produce
Hormone Replacement Therapy What Role Should It Play With Our Patients? Noel R. Williams MD, FACOG TESTOSTERONE FOR MEN: SALVATION OR SNAKE OIL? Definition Male hypogonadism means the testicles don't produce
Male New Patient Package
 Male New Patient Package The contents of this package are your first step to restore your vitality. Please take time to read this carefully and answer all the questions as completely as possible. Thank
Male New Patient Package The contents of this package are your first step to restore your vitality. Please take time to read this carefully and answer all the questions as completely as possible. Thank
Assessment and management of male androgen disorders: an update
 Irene Chan Mark Ng Tang Fui Jeffrey D Zajac Mathis Grossmann Assessment and management of male androgen disorders: an update Background Male hypogonadism, caused by intrinsic pathology of the hypothalamic
Irene Chan Mark Ng Tang Fui Jeffrey D Zajac Mathis Grossmann Assessment and management of male androgen disorders: an update Background Male hypogonadism, caused by intrinsic pathology of the hypothalamic
Testosterone Therapy in Men An update
 Testosterone Therapy in Men An update SANDEEP DHINDSA Associate Professor of Medicine Director, Division of Endocrinology and Metabolism, Saint Louis University, St. Louis, MO Presenter Disclosure None
Testosterone Therapy in Men An update SANDEEP DHINDSA Associate Professor of Medicine Director, Division of Endocrinology and Metabolism, Saint Louis University, St. Louis, MO Presenter Disclosure None
Male Patient Questionnaire & History
 Male Patient Questionnaire & History Name: Today s Date: (Last) (First) (Middle) Date of Birth: Age: Weight: Occupation: Home Address: City: State: Zip: E-Mail Address: May we contact you via E-Mail? (
Male Patient Questionnaire & History Name: Today s Date: (Last) (First) (Middle) Date of Birth: Age: Weight: Occupation: Home Address: City: State: Zip: E-Mail Address: May we contact you via E-Mail? (
Hormone Replacement Therapy For Men Consultation Information
 Hormone Replacement Therapy For Men Consultation Information www.urologyaustin.com Biological Aging and Hormones As we age, a natural degeneration and aging of organs causes the levels of our hormones
Hormone Replacement Therapy For Men Consultation Information www.urologyaustin.com Biological Aging and Hormones As we age, a natural degeneration and aging of organs causes the levels of our hormones
Advisory Committee Industry Briefing Document. Testosterone Replacement Therapy
 Advisory Committee Industry Briefing Document Testosterone Replacement Therapy Bone, Reproductive and Urologic Drugs Advisory Committee and the Drug Safety and Risk Management Advisory Committee Meeting
Advisory Committee Industry Briefing Document Testosterone Replacement Therapy Bone, Reproductive and Urologic Drugs Advisory Committee and the Drug Safety and Risk Management Advisory Committee Meeting
Overview of Reproductive Endocrinology
 Overview of Reproductive Endocrinology I have no conflicts of interest to report. Maria Yialamas, MD Female Hypothalamic--Gonadal Axis 15 4 Hormone Secretion in the Normal Menstrual Cycle LH FSH E2, Progesterone,
Overview of Reproductive Endocrinology I have no conflicts of interest to report. Maria Yialamas, MD Female Hypothalamic--Gonadal Axis 15 4 Hormone Secretion in the Normal Menstrual Cycle LH FSH E2, Progesterone,
The Male Andropause. What are the symptoms? What are the risks of hormone deficiencies?
 The Male Andropause By: Dr. Sangeeta Pati MD, FACOG Although, the male andropause has not been widely recognized, increased medical research has turned attention to the gradual hormone decline in males
The Male Andropause By: Dr. Sangeeta Pati MD, FACOG Although, the male andropause has not been widely recognized, increased medical research has turned attention to the gradual hormone decline in males
Patient education for transgender masculinizing hormone therapy
 Date name DOB Patient education for transgender masculinizing hormone therapy o Some transsexual, transgender, and gender non-conforming people choose to take hormone therapy to treat gender dysphoria
Date name DOB Patient education for transgender masculinizing hormone therapy o Some transsexual, transgender, and gender non-conforming people choose to take hormone therapy to treat gender dysphoria
PTA/OTA 106 Unit 2 Lecture 4 Introduction to the Endocrine System
 PTA/OTA 106 Unit 2 Lecture 4 Introduction to the Endocrine System 1 Anterior Pituitary or Adenohypophysis Corticotrophs Adrenocorticotropic hormone (ACTH) Hypothalamic Control Corticotropic releasing hormone
PTA/OTA 106 Unit 2 Lecture 4 Introduction to the Endocrine System 1 Anterior Pituitary or Adenohypophysis Corticotrophs Adrenocorticotropic hormone (ACTH) Hypothalamic Control Corticotropic releasing hormone
Early or late childhood? Age driven. LH driven Start testosterone when LH begins to rise Indicates that the pituitary is trying and failing
 Philip S. Zeitler MD. PhD Division of Endocrinology Children s Hospital Colorado Aurora, Colorado Primary testicular failure Central hormones responsible for onset of puberty are normal The testis itself
Philip S. Zeitler MD. PhD Division of Endocrinology Children s Hospital Colorado Aurora, Colorado Primary testicular failure Central hormones responsible for onset of puberty are normal The testis itself
06-Mar-17. Premature menopause. Menopause. Premature menopause. Menstrual cycle oestradiol. Premature menopause. Prevalence ~1% Higher incidence:
 Menopause Dr Sonia Davison MBBS FRACP PhD Endocrinologist and Clinical Fellow, Jean Hailes for Women s Health Women s Health Research Program, Monash University = the last natural menstrual period depletion
Menopause Dr Sonia Davison MBBS FRACP PhD Endocrinologist and Clinical Fellow, Jean Hailes for Women s Health Women s Health Research Program, Monash University = the last natural menstrual period depletion
One Day Hormone Check
 One Day Hormone Check Patient: EMILY TEST DOB: January 18, 1948 Sex: F MRN: 0000000004 Order Number: J5070009 Completed: March 07, 2014 Received: March 07, 2014 Collected: March 07, 2014 Alec Smart, ND
One Day Hormone Check Patient: EMILY TEST DOB: January 18, 1948 Sex: F MRN: 0000000004 Order Number: J5070009 Completed: March 07, 2014 Received: March 07, 2014 Collected: March 07, 2014 Alec Smart, ND
MALE HYPOGONADISM: CHOOSING THE APPROPRIATE THERAPY. Michael S. Irwig, M.D. Director, Center for Andrology Division of Endocrinology & Metabolism
 MALE HYPOGONADISM: CHOOSING THE APPROPRIATE THERAPY Michael S. Irwig, M.D. Director, Center for Andrology Division of Endocrinology & Metabolism Disclosures Aromatase inhibitors & clomiphene citrate are
MALE HYPOGONADISM: CHOOSING THE APPROPRIATE THERAPY Michael S. Irwig, M.D. Director, Center for Andrology Division of Endocrinology & Metabolism Disclosures Aromatase inhibitors & clomiphene citrate are