Bushra Arafa Zayed & Hanan Jamal. - Dana AF
|
|
|
- Erik Townsend
- 5 years ago
- Views:
Transcription




1 Bushra Arafa Zayed & Hanan Jamal - Dana AF - Mohammad Al Muhtaseb
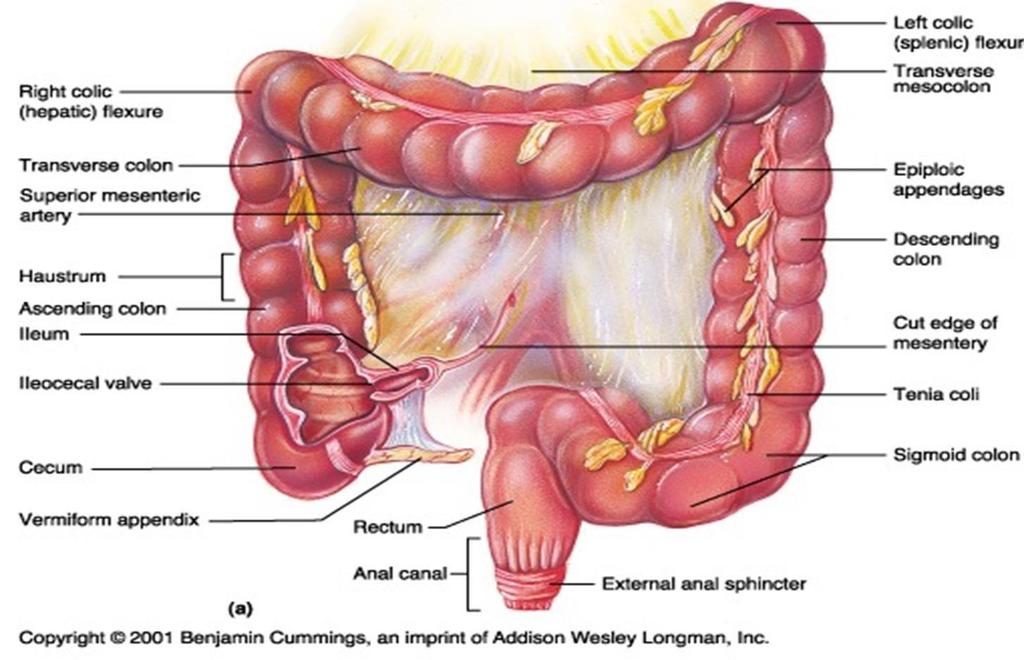
2 Notes: This sheet was written in the same order as the slides, and everything in the slides is mentioned in this sheet. Pictures that contain arteries veins and lymphatic vessels are in the last 3 page, s. Anatomy of the Large Intestine Extends from ileocecal valve to anus The left colic flexure is slightly higher than the right colic flexure Larger diameter than the small intestine Length = m = 5feet Unlike the length of the small intestine, which is constant (6 meters), the length of the large intestine varies among individuals. This variation is mainly found in the transverse and sigmoid colon. *Regions: (memorize them) Cecum = inch Appendix= 3-5 inch Colon Ascending= 5 inch Transverse= 15 inch Descending= 10 inch Sigmoid colon = inch Rectum= 5 inch Anal canal= 4 cm General Features of the Large Intestine Teania coli (three separate longitudinal ribbons of smooth muscle) are not present in the appendix and rectum. This is a landmarkfor the base of the appendix as the teania coli disappears at the level of the base of the appendix. When teania coli contracts, it causes the later walls to make sacculations. Teania coli protrudes from the outer longitudinal muscle. P a g e 2 Sacculations, or Haustra (helps in absorption of water and formation of
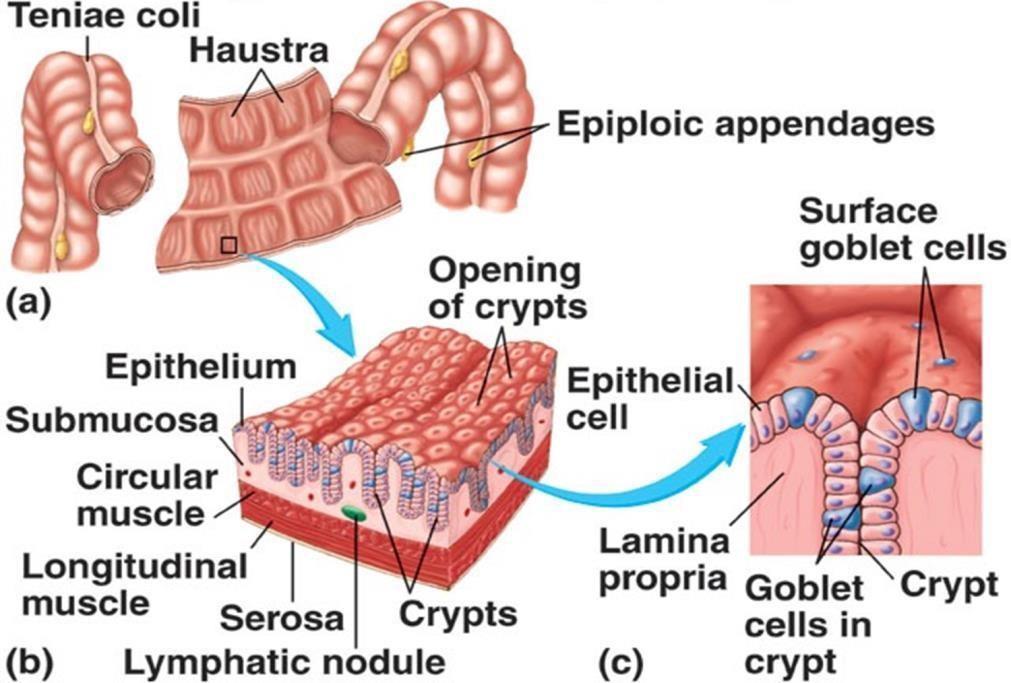
3 feces) formed by teania coli. It appears in the X-ray. Appendices epiploicae (or epiploic appendages) are adipose structures protruding from the serosal surface of the colon). Appendices epiploicae are not present in the appendix, caecum and rectum, but are found in all other areas of the large intestine (especially the transverse colon because it is intraperitoneal). The functions of the large intestine: absorption of water, secretion of mucous and formation of feces. Histologically, the linning epithelium is formed by simple columnar cells (mucous and (absorptive cellswith numerous goblet cells for lubrication. The glands are simple tubular glands. 3 P a g e
4 4 Page
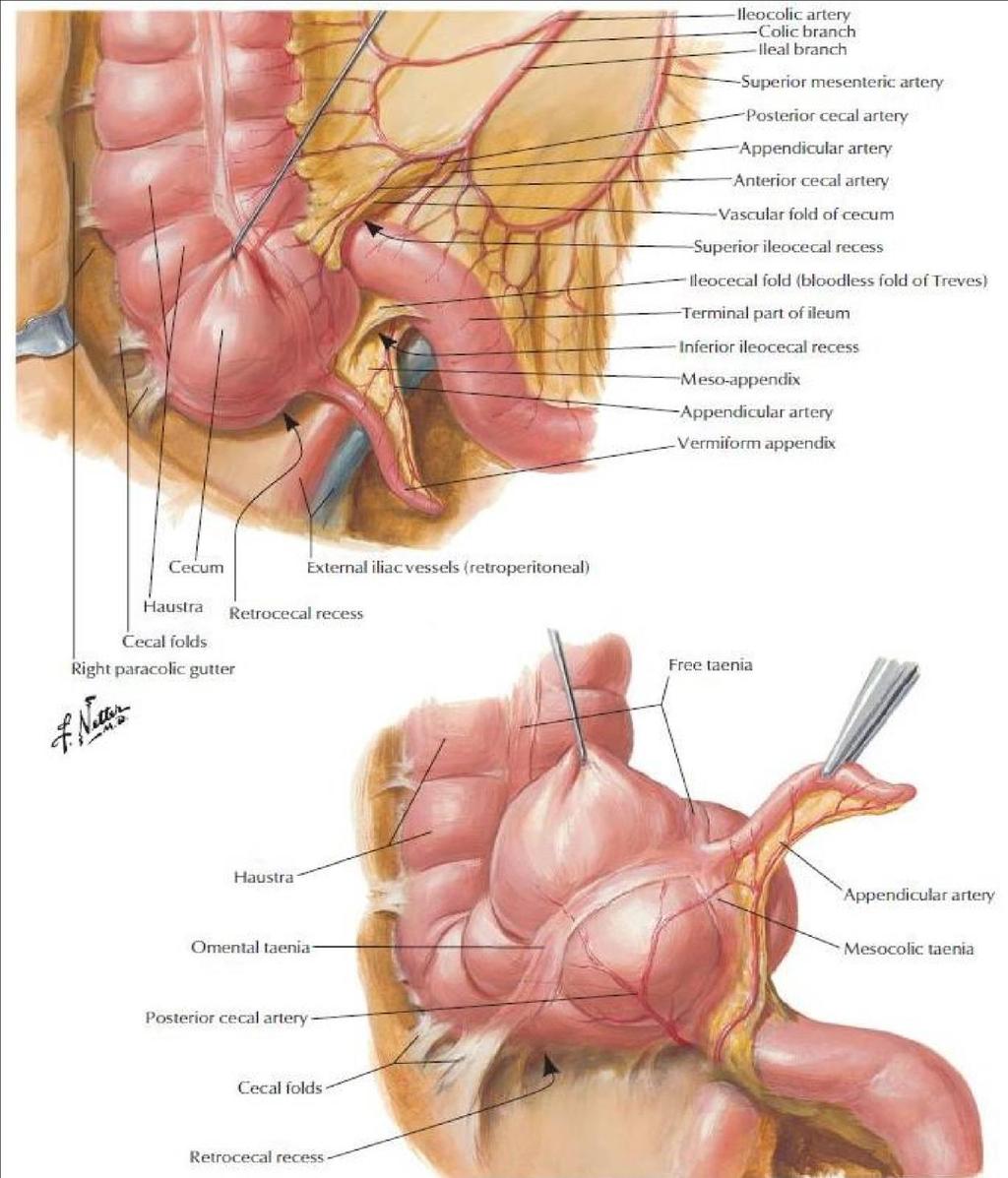
5 Caecum It is a blind ended pouch and it has three openings ( opens at the ilium, appendix and ascending colon). Site: situated in the right iliac fossa (right inguinal region), above and parallel to the lateral ½ of the inguinal ligament Size: about 3 inch in diameter It is completely covered by peritoneum; the peritoneum holds it and makes it fixed to it s position. There is a space between the appendix and the right Iliac fossa called the retrocecal space. Although it does not have a mesentery (very rare property), it possesses a considerable amount of mobility. The caecum is attached to: a) Ascending colon b) Posteromedially, the appendix, 1 inch below ileocecal valve c) Medially: Ileum : The presence of peritoneal folds in the vicinity of the caecum creates a) The superior ileocecal recesses (pouch) b) The inferior ileocecal recesses c) The retrocecal recesses The appendix may be withi it and sometimes. the small intestine may enter in it. This case is also known as internal hernia and strangulated hernia (when blood supply is cut). It will increase the pressure on the blood vessels causing gangrene which requires urgent treatment. Around the cecum or the duodenum between retroperitoneal and intraperitoneal organs? Why is there peritoneal folds Because the ilium is intraperitoneal and the cecum is fixed in the posterior wall of iliac fossa making folds of peritoneum. And around the cecum we ll have pouches. or recesses The longitudinal muscle is restricted to three flat bands, the teniae coli, which converge on the base of the appendix and provide for it a complete. longitudinal muscle coat 5 P a g e
6 P a g e 6
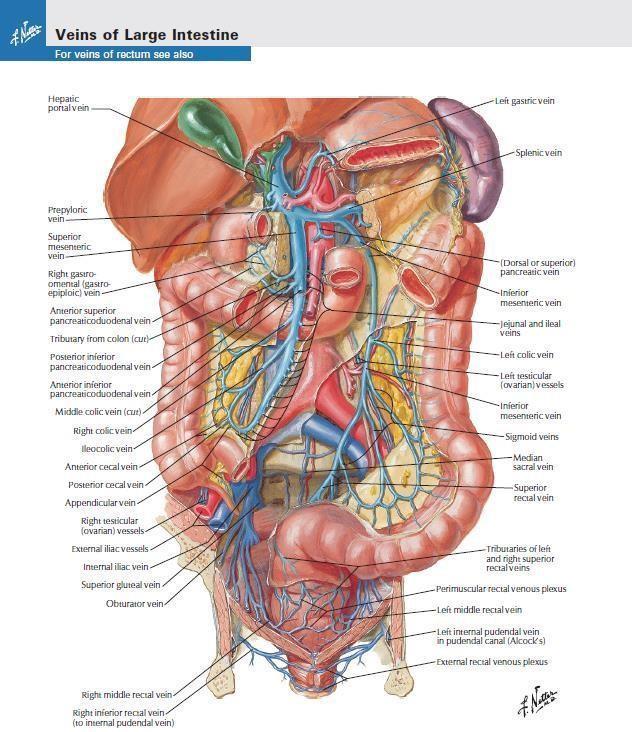
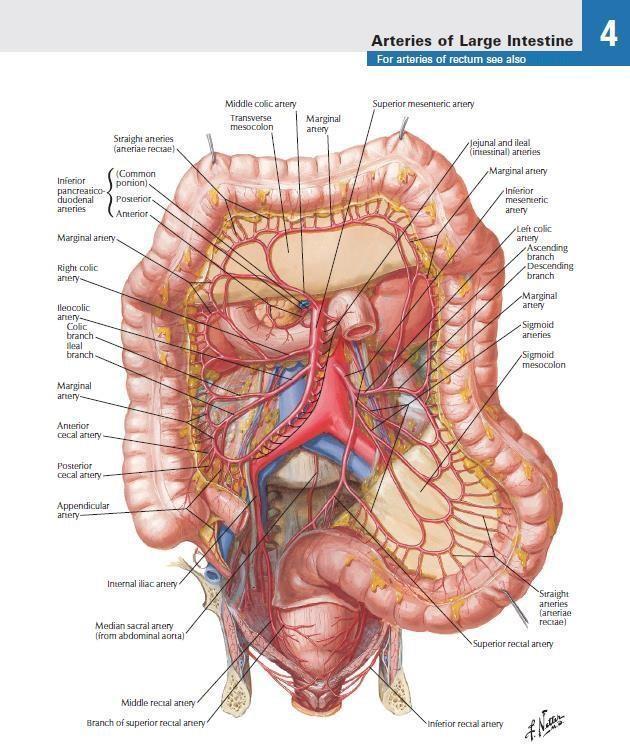
7 Relations of Caecum Anteriorly: 1. Coils of small intestine 2. The greater omentum 3. The anterior abdominal wall in the right iliac region. Posteriorly: 1. The psoas and the iliacus muscles which are inserted into the lesser trochanter of the femur 2. The femoral nerve between the two muscles 3. The lateral cutaneous nerve of the thigh to anterior superior iliac spine 4. Posteromedially: the appendix if it is in the retrocecal space (which is common) : Medially Small intestine (ileum). Blood Supply of Caecum Arteries Anterior and posterior cecal arteries are branches of the ileocecal artery Note: the superior mesenteric artery supplies the midgut by giving ileal, jejunal, right colic, middle colic and the ileocolic arteries. which is a branch of the superior mesenteric artery. Veins: 1. Correspond to the arteries and drain finally into the superior mesenteric vein which joins the splenic vein behind the neck of pancreas to form the portal vein. 2. Note: we should know the relation between each artery and vein, which one is medial and who is the lateral, like: the superior mesenteric artery is on the left side of the vein. The inferior mesenteric artery is on the right side of the vein. 7 P a g e
 and also drain into the superior mesenteric nodes.")
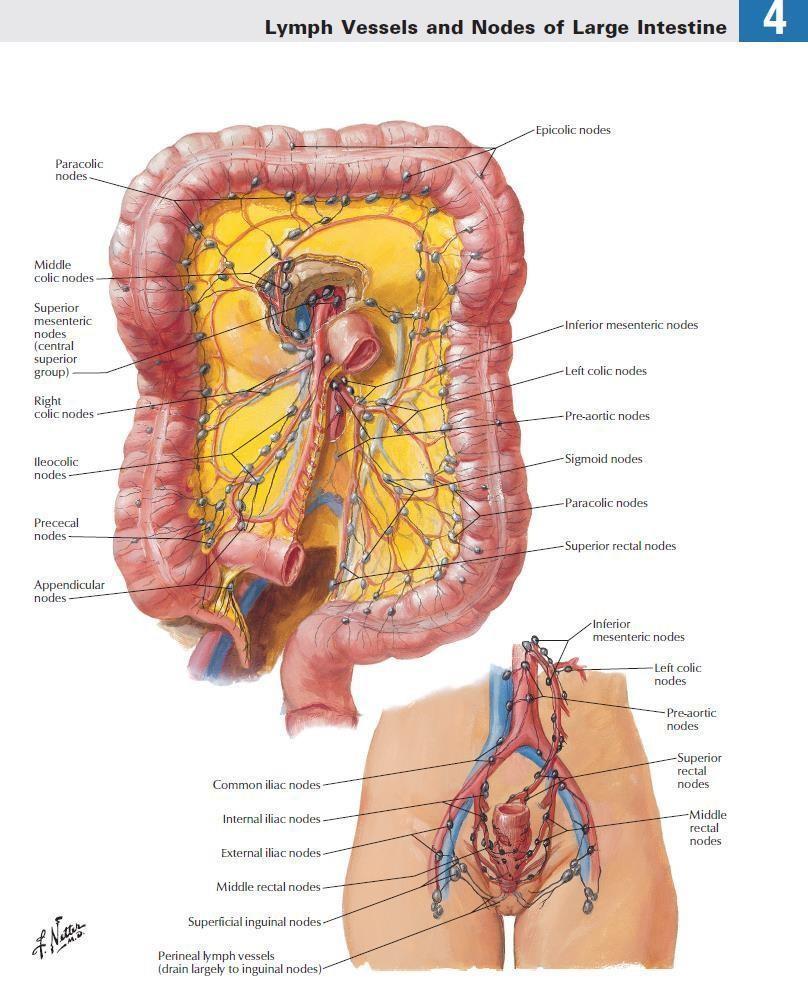
8 Lymphatic Drainage of Caecum The lymphatic vessels pass through several mesenteric nodes and eventually reach the superior mesenteric nodes around the origin of the superior mesenteric artery. Some of the nodes may be located on/near the veins (hence have the same names of the veins) and also drain into the superior mesenteric nodes. Nerve Supply of Caecum P a g e 8 Branches from the sympathetic (superior sympathetic ganglia) and parasympathetic (vagus) nerves form the superior mesenteric plexus. The vagus nerve gives parasympathetic innervation until the junction between the medial 2 thirds of the transverse colon and the lateral third( which is the end of the midgut).
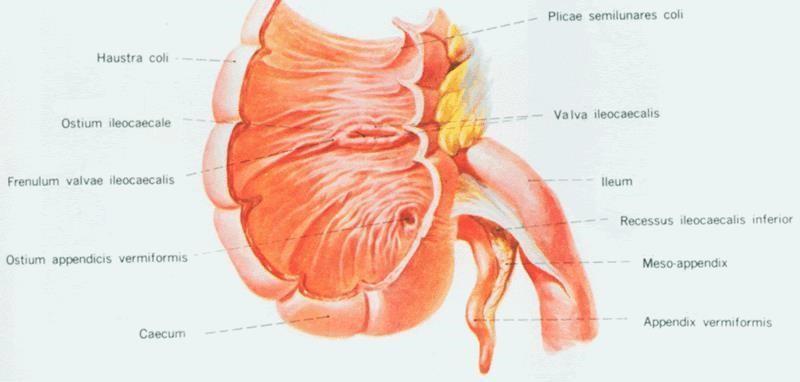
9 Ileocecal Valve Physiological valve A rudimentary structure Consists of two horizontal folds of mucous membrane to prevent regurgitation Project around the orifice of the ileum Anatomically, there is no thickening of the smooth muscle so it is not considered an anatomical sphincter. There is only two horizontal folding of mucosa at the opening of the ileocecal valve. This folding leads to closure of this junction by causing pressure on the caecum when it is extended, so the material will not go back to the ileum, instead it will go towards the. ascending colon These two folds of the mucosa are called: the superior ileocecal fold and the. inferior ileocecal fold Meanwhile, the Ileocecal sphincter formed by the circular smooth muscle layer of the lower part of the ileum plays an important role in the control of the flow of contents from the ileum into the colon. 9 P a g e

10 P a g e 10
11 Appendix It is very important clinically because of the frequent cases of the appendicitis The treatment is surgery. This surgery is also known as "appendectomy" (discussed later). It is very important to do this surgery as soon as possible for the case of appendicitis because the expanded and swollen appendix (filled with fluids and blood) could rupture, leading to peritonitis. Location and Description: 1.. It is a narrow and muscular tube 2. Contains a large amount of lymphoid tissue (as nodules) It is also referred to as a lymphatic organ 3. It has no role in digestion although it is in the GI tract. 4. It normally varies in length from 3 to 5 inches. However, due to the variation it may be very small (2cm) or very long up to 22 cm. The base is attached to the posteromedial surface of the caecum about 1 inch below the ileocecal junctio )cm 2.5( n. 5.. The remainder of the appendix is free : Peritoneum 1. It has a complete peritoneal covering, which is attached to the mesentery of the small intestine by a short mesentery of its own, the. mesoappendix 2. The mesoappendix contains the appendicular vessels, nerves and. lymphatic vessels and nodes Position: The appendix lies in the right iliac fossa, and in relation to the anterior abdominal wall, it may be found in different positions, including: a) Retrocecal: in retrocecal recess behind caecum in 74% of the population b) Pelvic: in the pelvis related to right ovary and uterine tube (descends downwards to the pelvis) in 21% of the population Therefore the clinical picture between the retrocecal and pelvic is different. c) Subcecal: below caecum in 3.5% of the population d) Pre -ileal: in front of ileum in 1% of the population e) Post-ileal: behind the ileum % P a g e

12 P a g e 12
13 Surface Anatomy of Appendix McBurney's point McBurney's line: the line between the anterior superior iliac spine and the umbilicus. The base of the appendix is situated: one third of the way up along the line joining the right anterior superior iliac spine to the umbilicus, in other words, in the point between the upper 2 thirds and the lower third of the line.( McBurney s point) In the past, appendectomy was done by making an incision along the line between anterior superior iliac spine to the umbilicus. This incision, called McBurney's incision, passes through McBurney's point and is parallel to the inguinal ligament. Back then they used to separate the muscles and when reaching the peritoneum, they make an incision that leads directly to the base. of the appendix To reach the appendix during an appendectomy, follow the taeniae coli which. converge toward the base of the appendix Nowadays, appendectomy is done by a laparoscope that makes an opening. around the umbilicus to reach the appendix Blood Supply of Appendix Arteries: 1. The appendicular artery is a branch of the posterior cecal artery.(ileocecal artery) which descends behind the ileum 2. Note: the superior mesenteric artery gives off a branch that is called the ileocecal artery which gives off a branch called posterior cecal artery. 3. Appendicular artery runs in free margin of the. mesoappendix Veins: The appendicular vein drains into the posterior cecal vein to superior. mesenteric vein.1 13 P a g e
 nerves.")
14 Lymphatic Drainage of Appendix The lymph vessels drain into one or two nodes lying in the mesoappendix. which eventually drain into the superior mesenteric nodes Nerve Supply of Appendix The appendix is supplied by the sympathetic from the superior mesenteric plexus and parasympathetic (vagus) nerves. Afferent nerve fibers concerned with the conduction of visceral pain from the appendix accompany the sympathetic nerves and enter the spinal cord at the level of the 10th thoracic segment. T10 also supplies the skin around the umbilicus. Thus, the patient will feel pain around the umbilicus at the beginning of the inflammation of appendix (appendicitis). Then, it will be concentrated in the region of the right iliac fossa. The peritoneum over the appendix is innervated by the 10 th intercostal nerve skin of umbilicu = s. P a g e 14 Clinical Notes
15 Acute appendicitis is uncom mon in the two extremes of life. Thrombosis of appendicular artery completely cuts off the blood supply which results in gangrene since there is just one artery for appendix. This results in perforation and fluids from the appendix will drain into the right. paracolic gutter (which is a space on the right side of the ascending colon) While in acute cholecystitis, there will be no gangrene because more than one artery supplies the gallbladder because it is embedded in the liver and takes blood supply from it directly. When the appendix is inflamed, it will be expand increasing its length, congestion and obstruction of the lumen will occur and it will be filled with fluids and blood. So it is very important to treat it immediately to avoid its. rupture that causes a very dangerous condition known as peritonitis The treatment is removal of the appendix surgically (Appendectomy) which : include 4 steps 1.. Make 2 ligations in each vein and artery 2.. Cut between the 2 ligations to prevent bleeding 3. Stitch around the base of the appendix in and out in a circular manner. so when the ends of the stitches are pulled, the base will be closed 4.. Cut the appendix from the base Ascending Colon Most of the relations of the ascending colon are the same as the descending colon except for few structures, due to the difference in the length between the two (the descending colon is longer, it descends until the level of iliac.( fossa. Ascending colon is on the right side while the descending is on the left side Location and Description 1. The ascending colon is about 5 inch. (13 cm) long 2.. Lies in the right lower quadrant 3. It extends upward from the caecum (above right iliac fossa) to the inferior surface of the right lobe of the liver, where it turns to the left, forming the right colic flexure (hepatic flexure). On the other side, there is the left colic flexure (splenic flexure) which is found on a higher level than the right flexure and is attached to the diaphragm by a ligament called the phrenicocolic ligament, and above the ligament is. the spleen 15 P a g e
16 4. It becomes continuous with the transverse colon. Taeniae. coli, sacculations & appendices epiploicae are present The peritoneum 1.. It covers the front and the sides of the ascending colon 2. It is fixed to the posterior abdominal wall. This fixation results in the. formation of the paracolic gutter (groove) 3. Again, any infection or fluids may pass through the gutter to reach the area below the diaphragm (subphrenic) and pelvis. It cant reach the diaphragm on the left side only the pelvis because its closed by. ligament 4.. Therefore, the ascending and descending colons are retroperitoneal : Importance of the paracolic gutter In a severe case of appendicitis, The infection has spread and abscess is formed. The patient will most likely sleep of the right side (side of infection). And is always laying down therefore the abscess will accumulate on the lateral side and will spread to the diaphragm, to Morrison s pouch (between liver and kidney) or sub-phrenic on the right side (open with the gutter). And treatment is drainage of the abscess. From this history a good doctor will know that there is abscess. and will know where to search for it Relations of Ascending Colon Anteriorly: 1. Coils of small intestine: the ascending colon is on the right side so its relation is with the ileum. While the descending colon is on the left. side, so it is related to the jejunum 2. The greater omentum: descends from the greater curvature of the stomach as 2 layers of peritoneum then ascends back as 2 layers. The greater omentum is considered the policeman of the abdomen due to the fact that it localizes the infection by surrounding the infected area. This means if the appendix is surrounded by the greater omentum,. there might be an infection in it 16 P a g e
17 3. The anterior abdominal wall Note: the ascending colon can be felt on the lumbar region anteriorly (after the anterior abdominal wall) specially if there is distention or a mass Posteriorly: 1. The iliacus 2. The iliac crest 3. The quadratus lumborum 4. The origin of the transversus abdominis muscle 5. The lower pole of the right kidney 6. The iliohypogastric nerve 7. The ilioinguinal nerve Blood Supply of Ascending Colon Arteries: 1. The ileocolic & right colic branches of the superior mesenteric artery (from midgut) supply this area. The right colic artery is the main artery. that supplies the ascending colon 2. the middle colic artery supplies the upper part of the ascending colon and m ainly the transverse colon 3. Note: the ileocolic artery supplies the ileum, caecum and the beginning. of the ascending colon Veins: The veins correspond to the arteries and drain into the superior. mesenteric vein.1 Lymphatic Drainage of Ascending Colon Lymph nodes lying along the course of the colic blood vessels drain into the. superior mesenteric nodes 17 P a g e
18 Nerve Supply of Ascending Colon Sympathetic nerves from the superior mesenteric plexus and parasympathetic (vagus) nerves Transverse Colon Location and Description.1 It is intraperitoneal, completely covered by peritoneum (the greater omentum from the stomach descends downward then upward and.( covers upper and lower surfaces of the transverse colon. The transverse colon is about 15 in. (38 cm) long 2 3. Extends across the abdomen 4.. It is located in the umbilical region 5. It begins at the right colic flexure below the right lobe of the liver 6. Hangs downwards 7. Suspended by the transverse mesocolon from the pancreas 8. It ascends then ends at left colic flexure below the spleen (note.( that the spleen is anterior to the pancreas 9. The left colic flexure is higher than the right colic flexure and is suspended from the diaphragm by the phrenicocolic ligament.(very important; prevent spreading of infections upward) 10. Taeniae coli, sacculations & appendices epiploicae are present The Transverse Mesocolon = mesentery of the transverse colon (mobile (structure 1. It suspends the transverse colon from the anterior border of the. pancreas 2. The mesentery is attached to the superior border of the transverse. colon 18 P a g e
19 3. The posterior layers of the greater omentum are attached to the. inferior border 4. The position of the transverse colon is extremely variable and may. sometimes reach down as far as the pelvis Note: the mesocolon extends to (and ends at) the anterior border of the pancreas The transverse colon : is divided into. 1 Proximal 2 thirds: midgut supplied by the superior ( ) mesenteric artery. 2 Lateral third: hindgut supplied by inferior ( ) mesenteric artery 19 P a g e

20 P a g e 19
21 . Relations of Transverse Colon Anteriorly:.1 The anterior abdominal wall (umbilical and hypogastric regions) if the mesentery is long it will descend downward to the hypogastric region The greater omentum. 2 Posteriorly: 1. The second part of the duodenum 2. The head of the pancreas 3. The coils of the jejunum and ileum: this depends on the mesentery of the transverse colon: if short, then it s anterior; if long, then it s. posterior Blood Supply of Transverse Colon Arteries: 1. The proximal two thirds are supplied by the middle colic artery, which. is a branch of the superior mesenteric artery 2. The distal third is supplied by the left colic artery, which is a branch of. the inferior mesenteric artery. 3 Note: Arcades and vasa recta are mainly for jejunum and ilium. And in the large intestine we have Marginal artery: continuous artery that anastomoses between. the end arteries of the large intestine Veins: The veins correspond to the arteries and drain into the superior &.inferior mesenteric veins to the portal vein.1 Lymphatic Drainage of Transverse Colon The proximal two thirds drain into the colic nodes and then into the superior. mesenteric nodes 21 P a g e
22 The distal third drains into the colic nodes which drain into the inferior. mesenteric nodes Nerve Supply of Transverse Colon The proximal two thirds are innervated by sympathetic and vagal nerves. through the superior mesenteric plexus The distal (lateral) third is innervated by parasympathetic ( spinal nerve S2, 3, 4 sacral) and sympathetic (pelvic splanchnic nerves) through the inferior. mesenteric plexus )called hypogastric plexus( Descending Colon Location and Description: 1.. The descending colon is about 10 in. (25 cm) long 2. It extends downward from the left colic flexure, to the pelvic brim.(left iliac fossa), where it becomes continuous with the sigmoid colon 3. Taeniae coli, sacculations & appendices epiploicae are present The peritoneum It covers the front and the sides and binds it to the posterior.abdominal wall so it is retroperitoneal.1 Relations of Descending Colon : Anteriorly 1. Coils of small intestine 2. The greater omentum 3. The anterior abdominal wall : Posteriorly 1. The lateral border of the left kidney 2. The origin of the transversus abdominis muscle 22 P a g e
23 3. The quadratus lumborum 4. The iliac crest 5. The iliacus 6. * The left psoas 7. The iliohypogastric and ilioinguinal nerves 8. * The lateral cutaneous nerve of the thigh 9. * The femoral nerve The structures marked with an asterisk (*) are related to the descending colon but not the ascending colon. The descending colon is longer and it.descends to the pelvis Blood Supply of Descending Colon Arteries: The left colic and the sigmoid branches of the inferior mesenteric.1 artery (From hindgut) Veins: The veins correspond to the arteries. The veins drain into the inferior.1 mesenteric vein which in turn drains in the splenic vein. The splenic vein and the superior mesenteric vein join together to form the. hepatic portal vein Lymphatic Drainage of Descending Colon Lymphatic drains into the colic lymphatic nodes & the inferior mesenteric. nodes around the origin of the inferior mesenteric artery Nerve Supply of Descending Colon The sympathetic innervation is through the inferior mesenteric plexus and parasympathetic through the pelvic splanchnic nerves (S2, 3, 4 sacral.(spinal nerve 23 P a g e
24 23 Page
25
26
Anatomy of the Large Intestine
 Large intestine Anatomy of the Large Intestine 2 Large Intestine Extends from ileocecal valve to anus Length = 1.5-2.5m = 5 feet Regions Cecum = 2.5-3 inch Appendix= 3-5 inch Colon Ascending= 5 inch Transverse=
Large intestine Anatomy of the Large Intestine 2 Large Intestine Extends from ileocecal valve to anus Length = 1.5-2.5m = 5 feet Regions Cecum = 2.5-3 inch Appendix= 3-5 inch Colon Ascending= 5 inch Transverse=
ANATOMY OF THE SMALL & LARGE INTESTINES. Semester 1, 2011 A. Mwakikunga
 ANATOMY OF THE SMALL & LARGE INTESTINES Semester 1, 2011 A. Mwakikunga LEARNING OBJECTIVES 1. List the parts and anatomical regions of the small and large intestines 2. State anatomical relations of the
ANATOMY OF THE SMALL & LARGE INTESTINES Semester 1, 2011 A. Mwakikunga LEARNING OBJECTIVES 1. List the parts and anatomical regions of the small and large intestines 2. State anatomical relations of the
Al-Mohtaseb. Saba Alfayoumi. Mo Alfarra
 8 Al-Mohtaseb Saba Alfayoumi Mo Alfarra For the comparison purposes refer to the last page where you can find a table that summarizes them. Enjoy Jejunum and Ileum -They're intraperitoneal and freely mobile
8 Al-Mohtaseb Saba Alfayoumi Mo Alfarra For the comparison purposes refer to the last page where you can find a table that summarizes them. Enjoy Jejunum and Ileum -They're intraperitoneal and freely mobile
THE ORAL CAVITY
 THE ORAL CAVITY WALL OF ABDOMEN (ANTERIOR) The paraumbilical vein drains into the portal vein and then through the liver. This is an important clinical connection. THE ABDOMINAL VISCERA The small
THE ORAL CAVITY WALL OF ABDOMEN (ANTERIOR) The paraumbilical vein drains into the portal vein and then through the liver. This is an important clinical connection. THE ABDOMINAL VISCERA The small
Duodenum retroperitoneal
 Duodenum retroperitoneal C shaped Initial region out of stomach into small intestine RETROperitoneal viscus Superior 1 st part duodenal cap ; moves upwards and backwards to lie on the R crura medial to
Duodenum retroperitoneal C shaped Initial region out of stomach into small intestine RETROperitoneal viscus Superior 1 st part duodenal cap ; moves upwards and backwards to lie on the R crura medial to
Preview from Notesale.co.uk Page 1 of 34
 Abdominal viscera and digestive tract Digestive tract Abdominal viscera comprise majority of the alimentary system o Terminal oesophagus, stomach, pancreas, spleen, liver, gallbladder, kidneys, suprarenal
Abdominal viscera and digestive tract Digestive tract Abdominal viscera comprise majority of the alimentary system o Terminal oesophagus, stomach, pancreas, spleen, liver, gallbladder, kidneys, suprarenal
Small Plicae Circularis. Short Closely packed together. Sparse, completely absent at distal part Lymphoid Nodule
 Intestines Differences Between Jejunum and Ileum Types Jejunum Ileum Color Deeper red Paler pink Calibre Bigger Smaller Thickness of wall Thick and Heavy Thin and Lighter Vascularity Highly vascularised
Intestines Differences Between Jejunum and Ileum Types Jejunum Ileum Color Deeper red Paler pink Calibre Bigger Smaller Thickness of wall Thick and Heavy Thin and Lighter Vascularity Highly vascularised
Mousa Salah. Dr. Mohammad Al. Mohtasib. 1 P a g e
 8 Mousa Salah Dr. Mohammad Al. Mohtasib 1 P a g e In the previous lecture we talked about the peritoneum, and we said that the peritonium is a serous sac, and it consists of two layers, visceral and parietal.
8 Mousa Salah Dr. Mohammad Al. Mohtasib 1 P a g e In the previous lecture we talked about the peritoneum, and we said that the peritonium is a serous sac, and it consists of two layers, visceral and parietal.
Exploring Anatomy: the Human Abdomen
 Exploring Anatomy: the Human Abdomen PERITONEUM AND PERITONEAL CAVITY PERITONEUM The peritoneum is a thin serous membrane that lines the abdominal cavity and covers, in variable amounts, the viscera within
Exploring Anatomy: the Human Abdomen PERITONEUM AND PERITONEAL CAVITY PERITONEUM The peritoneum is a thin serous membrane that lines the abdominal cavity and covers, in variable amounts, the viscera within
The posterior abdominal wall. Prof. Oluwadiya KS
 The posterior abdominal wall Prof. Oluwadiya KS www.oluwadiya.sitesled.com Posterior Abdominal Wall Lumbar vertebrae and discs. Muscles opsoas, quadratus lumborum, iliacus, transverse, abdominal wall
The posterior abdominal wall Prof. Oluwadiya KS www.oluwadiya.sitesled.com Posterior Abdominal Wall Lumbar vertebrae and discs. Muscles opsoas, quadratus lumborum, iliacus, transverse, abdominal wall
BLOCK IV: OFFICIAL BODY PARTS LIST FOR ANTERIOR ABDOMINAL WALL AND ABDOMINAL CONTENTS
 BLOCK IV: OFFICIAL BODY PARTS LIST FOR ANTERIOR ABDOMINAL WALL AND ABDOMINAL CONTENTS External oblique muscle Muscular portion Aponeurotic portion Superficial inguinal ring Lateral (inferior) crus Medial
BLOCK IV: OFFICIAL BODY PARTS LIST FOR ANTERIOR ABDOMINAL WALL AND ABDOMINAL CONTENTS External oblique muscle Muscular portion Aponeurotic portion Superficial inguinal ring Lateral (inferior) crus Medial
Peritoneum: Def. : It is a thin serous membrane that lines the walls of the abdominal and pelvic cavities and clothes the viscera.
 Peritoneum: Def. : It is a thin serous membrane that lines the walls of the abdominal and pelvic cavities and clothes the viscera. Layers of the peritoneum: 1. Outer Layer ( Parietal Peritoneum) : lines
Peritoneum: Def. : It is a thin serous membrane that lines the walls of the abdominal and pelvic cavities and clothes the viscera. Layers of the peritoneum: 1. Outer Layer ( Parietal Peritoneum) : lines
Biology Human Anatomy Abdominal and Pelvic Cavities
 Biology 351 - Human Anatomy Abdominal and Pelvic Cavities Please place your name and I.D. number on the back of the last page of this exam. You must answer all questions on this exam. Because statistics
Biology 351 - Human Anatomy Abdominal and Pelvic Cavities Please place your name and I.D. number on the back of the last page of this exam. You must answer all questions on this exam. Because statistics
Anatomy of the SMALL INTESTINE. Dr. Noman Ullah Wazir PMC
 Anatomy of the SMALL INTESTINE Dr. Noman Ullah Wazir PMC SMALL INTESTINE The small intestine, consists of the duodenum, jejunum, and illium. It extends from the pylorus to the ileocecal junction were the
Anatomy of the SMALL INTESTINE Dr. Noman Ullah Wazir PMC SMALL INTESTINE The small intestine, consists of the duodenum, jejunum, and illium. It extends from the pylorus to the ileocecal junction were the
Dr. Zahiri. In the name of God
 Dr. Zahiri In the name of God small intestine = small bowel is the part of the gastrointestinal tract Boundaries: Pylorus Ileosecal junction Function: digestion and absorption of food It receives bile
Dr. Zahiri In the name of God small intestine = small bowel is the part of the gastrointestinal tract Boundaries: Pylorus Ileosecal junction Function: digestion and absorption of food It receives bile
Pancreas & Biliary System. Dr. Vohra & Dr. Jamila
 Pancreas & Biliary System Dr. Vohra & Dr. Jamila 1 Objectives At the end of the lecture, the student should be able to describe the: Location, surface anatomy, parts, relations & peritoneal reflection
Pancreas & Biliary System Dr. Vohra & Dr. Jamila 1 Objectives At the end of the lecture, the student should be able to describe the: Location, surface anatomy, parts, relations & peritoneal reflection
Netter's Anatomy Flash Cards Section 4 List 4 th Edition
 Netter's Anatomy Flash Cards Section 4 List 4 th Edition https://www.memrise.com/course/1577335/ Section 4 Abdomen (31 cards) Plate 4-1 Bony Framework of Abdomen 1.1 Costal cartilages 1.2 Iliac crest 1.3
Netter's Anatomy Flash Cards Section 4 List 4 th Edition https://www.memrise.com/course/1577335/ Section 4 Abdomen (31 cards) Plate 4-1 Bony Framework of Abdomen 1.1 Costal cartilages 1.2 Iliac crest 1.3
Block 3: DISSECTION 2 CELIAC TRUNK, JEJUNUM/ILEUM, LARGE INTESTINE, DUODENUM, PANCREAS, PORTAL VEIN; MOBILIZATION OF THE LIVER
 1 Block 3: DISSECTION 2 CELIAC TRUNK, JEJUNUM/ILEUM, LARGE INTESTINE, DUODENUM, PANCREAS, PORTAL VEIN; MOBILIZATION OF THE LIVER Attempt to complete as much as you can of the dissection explained in the
1 Block 3: DISSECTION 2 CELIAC TRUNK, JEJUNUM/ILEUM, LARGE INTESTINE, DUODENUM, PANCREAS, PORTAL VEIN; MOBILIZATION OF THE LIVER Attempt to complete as much as you can of the dissection explained in the
The jejunum and the Ileum. Prof. Oluwadiya KS
 The jejunum and the Ileum Prof. Oluwadiya KS www.oluwadiya.siteled.com Introduction Introduction The small intestine (SI) comprises of the duodenum, jejunum and the ileum The jejunum is the second part
The jejunum and the Ileum Prof. Oluwadiya KS www.oluwadiya.siteled.com Introduction Introduction The small intestine (SI) comprises of the duodenum, jejunum and the ileum The jejunum is the second part
-Ensherah Mokheemer. -Shatha Al-Jaberi محمد المحتسب- 1 P a g e
 9-9 -Ensherah Mokheemer -Shatha Al-Jaberi محمد المحتسب- 1 P a g e Small intestine has three regions: ( االثني عشر( The duodenum The jejunum The ileum Small intestine Duodenum: -c-shaped -The concavity
9-9 -Ensherah Mokheemer -Shatha Al-Jaberi محمد المحتسب- 1 P a g e Small intestine has three regions: ( االثني عشر( The duodenum The jejunum The ileum Small intestine Duodenum: -c-shaped -The concavity
The peritoneum. Prof. Oluwadiya KS, MBBS, FMCS(Orthop) Website:
 Website:") The peritoneum Prof. Oluwadiya KS, MBBS, FMCS(Orthop) Website: http://oluwadiya.com The peritoneum Serous membrane that lines the abdominopelvic cavity and invests the viscera The largest serous membrane
The peritoneum Prof. Oluwadiya KS, MBBS, FMCS(Orthop) Website: http://oluwadiya.com The peritoneum Serous membrane that lines the abdominopelvic cavity and invests the viscera The largest serous membrane
The abdominal Esophagus, Stomach and the Duodenum. Prof. Oluwadiya KS
 The abdominal Esophagus, Stomach and the Duodenum Prof. Oluwadiya KS www.oluwadiya.com Viscera of the abdomen Abdominal esophagus: Terminal part of the esophagus The stomach Intestines: Small and Large
The abdominal Esophagus, Stomach and the Duodenum Prof. Oluwadiya KS www.oluwadiya.com Viscera of the abdomen Abdominal esophagus: Terminal part of the esophagus The stomach Intestines: Small and Large
GI module Lecture: 9 د. عصام طارق. Objectives:
 GI module Lecture: 9 د. عصام طارق Objectives: To list structures forming posterior abdominal wall. To follow aorta & its main branches. To describe IVC & its main tributaries. To list nerves of posterior
GI module Lecture: 9 د. عصام طارق Objectives: To list structures forming posterior abdominal wall. To follow aorta & its main branches. To describe IVC & its main tributaries. To list nerves of posterior
Anatomy: Know Your Abdomen
 Anatomy: Know Your Abdomen Glossary Abdomen - part of the body below the thorax (chest cavity); separated by the diaphragm. Anterior - towards the front of the body. For example, the umbilicus is anterior
Anatomy: Know Your Abdomen Glossary Abdomen - part of the body below the thorax (chest cavity); separated by the diaphragm. Anterior - towards the front of the body. For example, the umbilicus is anterior
ABDOMEN - GI. Duodenum
 TALA SALEH ABDOMEN - GI Duodenum - Notice the shape of the duodenum, it looks like capital G shape tube which extends from the pyloroduodenal junction to the duodenojejunal junction. - It is 10 inches
TALA SALEH ABDOMEN - GI Duodenum - Notice the shape of the duodenum, it looks like capital G shape tube which extends from the pyloroduodenal junction to the duodenojejunal junction. - It is 10 inches
-12. -Renad Habahbeh. -Dr Mohammad mohtasib
 -12 -Renad Habahbeh - -Dr Mohammad mohtasib The Gallbladder -The gallbladder has a body, a fundus (a rounded end), a neck, Hartmann s pouch before the neck and a cystic duct that meets the common hepatic
-12 -Renad Habahbeh - -Dr Mohammad mohtasib The Gallbladder -The gallbladder has a body, a fundus (a rounded end), a neck, Hartmann s pouch before the neck and a cystic duct that meets the common hepatic
د. عصام طارق. Objectives:
 GI anatomy Lecture: 5 د. عصام طارق Objectives: To describe anatomy of stomach, duodenum & pancreas. To list their main relations. To define their blood & nerve supply. To list their lymph drainage. To
GI anatomy Lecture: 5 د. عصام طارق Objectives: To describe anatomy of stomach, duodenum & pancreas. To list their main relations. To define their blood & nerve supply. To list their lymph drainage. To
In the name ofgod. Abdomen 3. Dr. Zahiri
 In the name ofgod Abdomen 3 Dr. Zahiri Peritoneum Peritoneum It is the serous membrane(a type of loose connective tissue and is covered by mesothelium) that lines the abdominal cavity. Extensions of the
In the name ofgod Abdomen 3 Dr. Zahiri Peritoneum Peritoneum It is the serous membrane(a type of loose connective tissue and is covered by mesothelium) that lines the abdominal cavity. Extensions of the
STRUCTURAL BASIS OF MEDICAL PRACTICE EXAMINATION 3. October 16, 2015
 STRUCTURAL BASIS OF MEDICAL PRACTICE EXAMINATION 3 October 16, 2015 PART l. Answer in the space provided. (12 pts) 1. Identify the structures. (2 pts) A. B. A B C. D. C D 2. Identify the structures. (2
STRUCTURAL BASIS OF MEDICAL PRACTICE EXAMINATION 3 October 16, 2015 PART l. Answer in the space provided. (12 pts) 1. Identify the structures. (2 pts) A. B. A B C. D. C D 2. Identify the structures. (2
The Digestive System and Body Metabolism
 14 PART B The Digestive System and Body Metabolism PowerPoint Lecture Slide Presentation by Jerry L. Cook, Sam Houston University ESSENTIALS OF HUMAN ANATOMY & PHYSIOLOGY EIGHTH EDITION ELAINE N. MARIEB
14 PART B The Digestive System and Body Metabolism PowerPoint Lecture Slide Presentation by Jerry L. Cook, Sam Houston University ESSENTIALS OF HUMAN ANATOMY & PHYSIOLOGY EIGHTH EDITION ELAINE N. MARIEB
Lab 9 Abdomen MUSCLES
 Lab 9 Abdomen MUSCLES External abdominal oblique continuous with the external intercostal muscle; its fibers point in a caudal direction as it moves anteriorly until it inserts on the linea alba via its
Lab 9 Abdomen MUSCLES External abdominal oblique continuous with the external intercostal muscle; its fibers point in a caudal direction as it moves anteriorly until it inserts on the linea alba via its
Surface Anatomy. Location Shape Weight Role of Five Surfaces Borders Fissures Lobes Peritoneal Lig
 The Liver Functions Bile production and secretion Detoxification Storage of glycogen Protein synthesis Production of heparin and bile pigments Erythropoiesis (in fetus) Surface Anatomy Location Shape Weight
The Liver Functions Bile production and secretion Detoxification Storage of glycogen Protein synthesis Production of heparin and bile pigments Erythropoiesis (in fetus) Surface Anatomy Location Shape Weight
Lab Monitor Images Dissection of the Abdominal Vasculature + Lower Digestive System
 Lab Monitor Images Dissection of the Abdominal Vasculature + Lower Digestive System Stomach & Duodenum Frontal (AP) View Nasogastric tube 2 1 3 4 Stomach Pylorus Duodenum 1 Duodenum 2 Duodenum 3 Duodenum
Lab Monitor Images Dissection of the Abdominal Vasculature + Lower Digestive System Stomach & Duodenum Frontal (AP) View Nasogastric tube 2 1 3 4 Stomach Pylorus Duodenum 1 Duodenum 2 Duodenum 3 Duodenum
Posterior Abdominal wall-
 Structures of posterior abdominal wall: o Bony boundaries: 5 lumber vertebra and their intervertebral disc, iliac fossa and iliac crest. o Muscles: psoas major, quadrates lumborum, transversus abdominis,
Structures of posterior abdominal wall: o Bony boundaries: 5 lumber vertebra and their intervertebral disc, iliac fossa and iliac crest. o Muscles: psoas major, quadrates lumborum, transversus abdominis,
[ANATOMY #12] April 28, 2013
![[ANATOMY #12] April 28, 2013](/thumbs/86/93473883.jpg "[ANATOMY #12] April 28, 2013") Sympathetic chain : Sympathetic chain is each of the pair of ganglionated longitudinal cords of the sympathetic nervous system; extend from level of atlas (base of skull) till coccyx. It is paravertebral
Sympathetic chain : Sympathetic chain is each of the pair of ganglionated longitudinal cords of the sympathetic nervous system; extend from level of atlas (base of skull) till coccyx. It is paravertebral
Peritoneal cavity. Infracolic compartment. Assoc. prof. dr. S. Delchev, MD, PhD
 Peritoneal cavity. Infracolic compartment Assoc. prof. dr. S. Delchev, MD, PhD Infracolic compartment The infracolic compartment lies inferior to the transverse mesocolon and posterior to the greater omentum
Peritoneal cavity. Infracolic compartment Assoc. prof. dr. S. Delchev, MD, PhD Infracolic compartment The infracolic compartment lies inferior to the transverse mesocolon and posterior to the greater omentum
BY DR NOMAN ULLAH WAZIR
 BY DR NOMAN ULLAH WAZIR The stomach (from ancient Greek word stomachos, stoma means mouth) is a muscular, hollow and the most dilated part of the GIT. It starts from the point where esophagus ends. It
BY DR NOMAN ULLAH WAZIR The stomach (from ancient Greek word stomachos, stoma means mouth) is a muscular, hollow and the most dilated part of the GIT. It starts from the point where esophagus ends. It
Accessory Glands of Digestive System
 Accessory Glands of Digestive System The liver The liver is soft and pliable and occupies the upper part of the abdominal cavity just beneath the diaphragm. The greater part of the liver is situated under
Accessory Glands of Digestive System The liver The liver is soft and pliable and occupies the upper part of the abdominal cavity just beneath the diaphragm. The greater part of the liver is situated under
Jhia Anjela D. Rivera 1 1. BS Biology, Department of Biology, College of Science, Polytechnic University of the Philippines
 DIGESTIVE SYSTEM Jhia Anjela D. Rivera 1 1 BS Biology, Department of Biology, College of Science, Polytechnic University of the Philippines DIGESTIVE SYSTEM Consists of the digestive tract (gastrointestinal
DIGESTIVE SYSTEM Jhia Anjela D. Rivera 1 1 BS Biology, Department of Biology, College of Science, Polytechnic University of the Philippines DIGESTIVE SYSTEM Consists of the digestive tract (gastrointestinal
Done by: Dina Sawadha & Mohammad Abukabeer
 Done by: Dina Sawadha & Mohammad Abukabeer The stomach *the stomach is a dilated part of the gastro intestinal tract, it's "J" shape. *the lower surface of the stomach ( the greater curvature ) reaches
Done by: Dina Sawadha & Mohammad Abukabeer The stomach *the stomach is a dilated part of the gastro intestinal tract, it's "J" shape. *the lower surface of the stomach ( the greater curvature ) reaches
Pancreas and Biliary System
 Pancreas and Biliary System Please view our Editing File before studying this lecture to check for any changes. Color Code Important Doctors Notes Notes/Extra explanation Objectives At the end of the lecture,
Pancreas and Biliary System Please view our Editing File before studying this lecture to check for any changes. Color Code Important Doctors Notes Notes/Extra explanation Objectives At the end of the lecture,
Omran Saeed. Mohammad Al-muhtaseb. 1 P a g e
 13 Omran Saeed Mohammad Al-muhtaseb 1 P a g e Posterior abdominal wall - The diaphragm separates between thoracic cavity and abdominal cavity. Structures of posterior abdominal wall: (below diaphragm)
13 Omran Saeed Mohammad Al-muhtaseb 1 P a g e Posterior abdominal wall - The diaphragm separates between thoracic cavity and abdominal cavity. Structures of posterior abdominal wall: (below diaphragm)
GASTROINTESTINAL SYSTEM
 GASTROINTESTINAL SYSTEM Topographic Anatomy of the Abdomen Surface Landmarks Xiphoid process T9/T10 Inferior costal margin L2/L3 Iliac Crest L4 level ASIS L5/S1 level Pubic symphysis level of greater trochanter
GASTROINTESTINAL SYSTEM Topographic Anatomy of the Abdomen Surface Landmarks Xiphoid process T9/T10 Inferior costal margin L2/L3 Iliac Crest L4 level ASIS L5/S1 level Pubic symphysis level of greater trochanter
The Spleen. Dr Fahad Ullah
 The Spleen BY Dr Fahad Ullah Spleen The spleen is an largest lymphoid organ shaped like a shoe that lies relative to the 9th and 11th ribs and is located in the left hypochondrium. Thus, the spleen is
The Spleen BY Dr Fahad Ullah Spleen The spleen is an largest lymphoid organ shaped like a shoe that lies relative to the 9th and 11th ribs and is located in the left hypochondrium. Thus, the spleen is
STRUCTURAL BASIS OF MEDICAL PRACTICE EXAMINATION 3. October 17, 2014
 STRUCTURAL BASIS OF MEDICAL PRACTICE EXAMINATION 3 October 17, 2014 PART l. Answer in the space provided. (12 pts) 1. Identify the structures. (2 pts) A. B. A B C. D. C D 2. Identify the structures. (2
STRUCTURAL BASIS OF MEDICAL PRACTICE EXAMINATION 3 October 17, 2014 PART l. Answer in the space provided. (12 pts) 1. Identify the structures. (2 pts) A. B. A B C. D. C D 2. Identify the structures. (2
SUBJECTS 2nd year, 1st semester I. 1. Primitive gut - limits, derivatives 2. Foregut -limits, evolution, derivatives 3. Midgut -limits, evolution,
 SUBJECTS 2nd year, 1st semester I. 1. Primitive gut - limits, derivatives 2. Foregut -limits, evolution, derivatives 3. Midgut -limits, evolution, derivatives 4. Hindgut- limits, evolution, derivatives
SUBJECTS 2nd year, 1st semester I. 1. Primitive gut - limits, derivatives 2. Foregut -limits, evolution, derivatives 3. Midgut -limits, evolution, derivatives 4. Hindgut- limits, evolution, derivatives
It passes through the diaphragm at the level of the 10th thoracic vertebra to join the stomach
 The esophagus is a tubular structure (muscular, collapsible tube ) about 10 in. (25 cm) long that is continuous above with the laryngeal part of the pharynx opposite the sixth cervical vertebra The esophagus
The esophagus is a tubular structure (muscular, collapsible tube ) about 10 in. (25 cm) long that is continuous above with the laryngeal part of the pharynx opposite the sixth cervical vertebra The esophagus
Anatomy of the renal system. Professor Nawfal K. Al-Hadithi
 Anatomy of the renal system Professor Nawfal K. Al-Hadithi Objectives To describe the posterior abdominal wall To identify the main anatomical landmarks of the kidneys & ureters To describe the suprarenal
Anatomy of the renal system Professor Nawfal K. Al-Hadithi Objectives To describe the posterior abdominal wall To identify the main anatomical landmarks of the kidneys & ureters To describe the suprarenal
LECTURE 11 & 12: ABDOMINAL VISCERA ABDOMINAL CONTENTS DIVISION. The location of abdominal viscera is divided into 4 quadrants:
 LECTURE 11 & 12: ABDOMINAL VISCERA ABDOMINAL CONTENTS DIVISION The location of abdominal viscera is divided into 4 quadrants: - horizontal line across the umbilicus divides the upper quadrants from the
LECTURE 11 & 12: ABDOMINAL VISCERA ABDOMINAL CONTENTS DIVISION The location of abdominal viscera is divided into 4 quadrants: - horizontal line across the umbilicus divides the upper quadrants from the
musculoskeletal system anatomy nerves of the lower limb 1 done by: dina sawadha & mohammad abukabeer
 musculoskeletal system anatomy nerves of the lower limb 1 done by: dina sawadha & mohammad abukabeer What is the importance of plexuses? plexuses provides us the advantage of a phenomenon called convergence
musculoskeletal system anatomy nerves of the lower limb 1 done by: dina sawadha & mohammad abukabeer What is the importance of plexuses? plexuses provides us the advantage of a phenomenon called convergence
Embryology of the Midgut and Hind gut
 Embryology of the Midgut and Hind gut Prof. Abdulameer Al-Nuaimi E-mail: a.al-nuaimi@sheffield.ac.uk E-mail: abdulameerh@yahoo.com Abdominal organs www.google.co.uk/search? Development of Duodenum The
Embryology of the Midgut and Hind gut Prof. Abdulameer Al-Nuaimi E-mail: a.al-nuaimi@sheffield.ac.uk E-mail: abdulameerh@yahoo.com Abdominal organs www.google.co.uk/search? Development of Duodenum The
Abdomen: Introduction. Prof. Oluwadiya KS
 Abdomen: Introduction Prof. Oluwadiya KS www.oluwadiya.com Abdominopelvic Cavity Abdominal Cavity Pelvic Cavity Extends from the inferior margin of the thorax to the superior margin of the pelvis and the
Abdomen: Introduction Prof. Oluwadiya KS www.oluwadiya.com Abdominopelvic Cavity Abdominal Cavity Pelvic Cavity Extends from the inferior margin of the thorax to the superior margin of the pelvis and the
Development of pancreas and Small Intestine. ANATOMY DEPARTMENT DR.SANAA AL-AlSHAARAWY DR.ESSAM Eldin Salama
 Development of pancreas and Small Intestine ANATOMY DEPARTMENT DR.SANAA AL-AlSHAARAWY DR.ESSAM Eldin Salama OBJECTIVES At the end of the lecture, the students should be able to : Describe the development
Development of pancreas and Small Intestine ANATOMY DEPARTMENT DR.SANAA AL-AlSHAARAWY DR.ESSAM Eldin Salama OBJECTIVES At the end of the lecture, the students should be able to : Describe the development
Dana Alrafaiah. - Amani Nofal. - Ahmad Alsalman. 1 P a g e
 - 2 - Dana Alrafaiah - Amani Nofal - Ahmad Alsalman 1 P a g e This lecture will discuss five topics as follows: 1- Arrangement of pelvic viscera. 2- Muscles of Pelvis. 3- Blood Supply of pelvis. 4- Nerve
- 2 - Dana Alrafaiah - Amani Nofal - Ahmad Alsalman 1 P a g e This lecture will discuss five topics as follows: 1- Arrangement of pelvic viscera. 2- Muscles of Pelvis. 3- Blood Supply of pelvis. 4- Nerve
To describe the liver. To list main structures in porta hepatis.
 GI anatomy Lecture: 6 د. عصام طارق Objectives: To describe the liver. To list main structures in porta hepatis. To define portal system & portosystemic anastomosis. To list parts of biliary system. To
GI anatomy Lecture: 6 د. عصام طارق Objectives: To describe the liver. To list main structures in porta hepatis. To define portal system & portosystemic anastomosis. To list parts of biliary system. To
Midgut. Over its entire length the midgut is supplied by the superior mesenteric artery
 Gi Embryology 3 Midgut the midgut is suspended from the dorsal abdominal wall by a short mesentery and communicates with the yolk sac by way of the vitelline duct or yolk stalk Over its entire length the
Gi Embryology 3 Midgut the midgut is suspended from the dorsal abdominal wall by a short mesentery and communicates with the yolk sac by way of the vitelline duct or yolk stalk Over its entire length the
ANATOMY OF THE DIGESTIVE SYSTEM PART II
 ANATOMY OF THE DIGESTIVE SYSTEM PART II 9.12.2014 Kaan Yücel M.D., Ph.D. http://fhs121.org Dr.Kaan Yücel http://fhs121.org Digestive system Part II 1. LIVER The liver is the largest gland in the body and,
ANATOMY OF THE DIGESTIVE SYSTEM PART II 9.12.2014 Kaan Yücel M.D., Ph.D. http://fhs121.org Dr.Kaan Yücel http://fhs121.org Digestive system Part II 1. LIVER The liver is the largest gland in the body and,
Abdomen. Retroperitoneal space
 Abdomen. Retroperitoneal space Abdominal cavity The space bounded by: Anterolateral abdominal wall Posterior abdominal wall Diaphragm Pelvic walls and pelvic floor. Subdivided into: True abdominal cavity
Abdomen. Retroperitoneal space Abdominal cavity The space bounded by: Anterolateral abdominal wall Posterior abdominal wall Diaphragm Pelvic walls and pelvic floor. Subdivided into: True abdominal cavity
This lab activity is aligned with Visible Body s Human Anatomy Atlas app. Learn more at visiblebody.com/professors
 1 This lab activity is aligned with Visible Body s Human Anatomy Atlas app. Learn more at visiblebody.com/professors 2 A. Digestive System Overview To Start: Go to the Views menu and scroll down to the
1 This lab activity is aligned with Visible Body s Human Anatomy Atlas app. Learn more at visiblebody.com/professors 2 A. Digestive System Overview To Start: Go to the Views menu and scroll down to the
Nasogastric tube. Stomach. Pylorus. Duodenum 1. Duodenum 2. Duodenum 3. Duodenum 4
 Esophagus Barium Swallow Stomach and Duodenum 4 year old Upper GI Nasogastric tube Stomach and Duodenum 4 year old Upper GI Nasogastric tube Stomach Pylorus Duodenum 1 Duodenum 2 Duodenum 3 Duodenum 4
Esophagus Barium Swallow Stomach and Duodenum 4 year old Upper GI Nasogastric tube Stomach and Duodenum 4 year old Upper GI Nasogastric tube Stomach Pylorus Duodenum 1 Duodenum 2 Duodenum 3 Duodenum 4
Anatomy of the spleen. Oluwadiya KS
 Anatomy of the spleen Oluwadiya KS www.oluwadiya.com Introduction The spleen is an ovoid, usually purplish, pulpy mass about the size and shape of one's fist. It is the largest lymphoid tissue in the body
Anatomy of the spleen Oluwadiya KS www.oluwadiya.com Introduction The spleen is an ovoid, usually purplish, pulpy mass about the size and shape of one's fist. It is the largest lymphoid tissue in the body
-the stones will obstruct the common bile duct and it might also be precancerous. -so the best treatment is chlolycyctoctomy.
 At the beginning this sheet includes the rest of last lecture s slides liver +gallbladder and the new lecture posterior abdominal wall and its vessels. We will start talking about Cholelithiasis -it means
At the beginning this sheet includes the rest of last lecture s slides liver +gallbladder and the new lecture posterior abdominal wall and its vessels. We will start talking about Cholelithiasis -it means
ANATOMY OF PELVICAYCEAL SYSTEM -DR. RAHUL BEVARA
 1 ANATOMY OF PELVICAYCEAL SYSTEM -DR. RAHUL BEVARA 2 KIDNEY:ANATOMY OVERVIEW Kidneys are retroperitoneal, in posterior abdominal region, extending from T12 L3 Bean-shaped Right kidney is lower than left
1 ANATOMY OF PELVICAYCEAL SYSTEM -DR. RAHUL BEVARA 2 KIDNEY:ANATOMY OVERVIEW Kidneys are retroperitoneal, in posterior abdominal region, extending from T12 L3 Bean-shaped Right kidney is lower than left
- Digestion occurs during periods of low activity - Produces more energy than it uses. - Mucosa
 Introduction Digestive System Chapter 29 Provides processes to break down molecules into a state easily used by cells - A disassembly line: Starts at the mouth and ends at the anus Digestive functions
Introduction Digestive System Chapter 29 Provides processes to break down molecules into a state easily used by cells - A disassembly line: Starts at the mouth and ends at the anus Digestive functions
Gastrointestinal Tract. Anatomy of GI Tract. Anatomy of GI Tract. (Effective February 2007) (1%-5%)
 (1%-5%)") Gastrointestinal Tract (Effective February 2007) (1%-5%) Anatomy of GI Tract Esophagus bulls-eye or target EG junction seen on sagittal scan posterior to left lobe of liver and anterior to aorta Anatomy
Gastrointestinal Tract (Effective February 2007) (1%-5%) Anatomy of GI Tract Esophagus bulls-eye or target EG junction seen on sagittal scan posterior to left lobe of liver and anterior to aorta Anatomy
Femoral Triangle and Adductor Canal. Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology
 Femoral Triangle and Adductor Canal Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology Femoral Triangle and Adductor Canal Femoral triangle Is a triangular depressed area located in the upper
Femoral Triangle and Adductor Canal Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology Femoral Triangle and Adductor Canal Femoral triangle Is a triangular depressed area located in the upper
HBA 531 THE BODY. Trunk Examination September 30, What is the effect of the parasympathetic nervous system on: (2.5)
") HBA 531 THE BODY Trunk Examination September 30, 2013 Name: 1. What is the effect of the parasympathetic nervous system on: (2.5) a) Heart rate b) Male reproductive function c) Pylorus d) Internal anal
HBA 531 THE BODY Trunk Examination September 30, 2013 Name: 1. What is the effect of the parasympathetic nervous system on: (2.5) a) Heart rate b) Male reproductive function c) Pylorus d) Internal anal
1 Right & left Hepatic ducts Gastric Impression of spleen
 Pancreatic Model 1 Right & left Hepatic ducts 14 Gastric Impression of spleen 2 Common hepatic duct 15 Renal Impression of spleen 3 Cystic Duct 16 Colic Impression of spleen 4 Common Bile Duct 17 Splenic
Pancreatic Model 1 Right & left Hepatic ducts 14 Gastric Impression of spleen 2 Common hepatic duct 15 Renal Impression of spleen 3 Cystic Duct 16 Colic Impression of spleen 4 Common Bile Duct 17 Splenic
Lecture 02 Anatomy of the LIVER
 Lecture 02 Anatomy of the LIVER BY Dr Farooq Khan Aurakzai Dated: 02.01.2018 Introduction to Liver Largest gland in the body. 2 nd largest organ of the body. Weight approximately 1500 gm, and is roughly
Lecture 02 Anatomy of the LIVER BY Dr Farooq Khan Aurakzai Dated: 02.01.2018 Introduction to Liver Largest gland in the body. 2 nd largest organ of the body. Weight approximately 1500 gm, and is roughly
The stomach is formed of three parts: -
 The stomach is formed of three parts: - (a) CARDIAC STOMACH: - It receives the oesophagus through Cardiac aperture guarded by a cardiac sphincter which prevents regurgitation of food. (b) FUNDIC PART:
The stomach is formed of three parts: - (a) CARDIAC STOMACH: - It receives the oesophagus through Cardiac aperture guarded by a cardiac sphincter which prevents regurgitation of food. (b) FUNDIC PART:
Nerves on the Posterior Abdominal Wall
 Nerves on the Posterior Abdominal Wall Lumbar Plexus The lumbar plexus, which is one of the main nervous pathways supplying the lower limb, is formed in the psoasmuscle from the anterior ramiof the upper
Nerves on the Posterior Abdominal Wall Lumbar Plexus The lumbar plexus, which is one of the main nervous pathways supplying the lower limb, is formed in the psoasmuscle from the anterior ramiof the upper
The Human Body: An Overview of Anatomy. Anatomy. Physiology. Anatomy - Study of internal and external body structures
 C H A P T E R 1 The Human Body: An Orientation An Overview of Anatomy Anatomy The study of the structure of the human body Physiology The study of body function Anatomy - Study of internal and external
C H A P T E R 1 The Human Body: An Orientation An Overview of Anatomy Anatomy The study of the structure of the human body Physiology The study of body function Anatomy - Study of internal and external
- Tamara Wahbeh. - Fareed Khdair. 0 P a g e
 -1 - Tamara Wahbeh - - Fareed Khdair 0 P a g e GI Embryology Note: I included everything in the records and slides; anything in the slide not included in this sheet was not mentioned by the doctor during
-1 - Tamara Wahbeh - - Fareed Khdair 0 P a g e GI Embryology Note: I included everything in the records and slides; anything in the slide not included in this sheet was not mentioned by the doctor during
Biology Human Anatomy Abdominal and Pelvic Cavities
 Biology 351 - Human Anatomy Abdominal and Pelvic Cavities You must answer all questions on this exam. Because statistics demonstrate that, on average, between 2-5 questions on every 100-point exam are
Biology 351 - Human Anatomy Abdominal and Pelvic Cavities You must answer all questions on this exam. Because statistics demonstrate that, on average, between 2-5 questions on every 100-point exam are
Lab 8: Digestive System
 BIOL 221 A&P II Lab 8: Digestive System Become familiar with the gross anatomy of the digestive system (Exercise 38) using the models, Fig. 38.1 (Activity 1), and the rat. Recognize and know the functions
BIOL 221 A&P II Lab 8: Digestive System Become familiar with the gross anatomy of the digestive system (Exercise 38) using the models, Fig. 38.1 (Activity 1), and the rat. Recognize and know the functions
- Digestion occurs during periods of low activity - Produces more energy than it uses. 3 Copyright 2016 by Elsevier Inc. All rights reserved.
 Introduction Digestive System Chapter 29 Provides processes to break down molecules into a state easily used by cells - A disassembly line: Starts at the mouth and ends at the anus Digestive functions
Introduction Digestive System Chapter 29 Provides processes to break down molecules into a state easily used by cells - A disassembly line: Starts at the mouth and ends at the anus Digestive functions
ABDOMINAL WALL & RECTUS SHEATH
 ABDOMINAL WALL & RECTUS SHEATH Learning Objectives Describe the anatomy, innervation and functions of the muscles of the anterior, lateral and posterior abdominal walls. Discuss their functional relations
ABDOMINAL WALL & RECTUS SHEATH Learning Objectives Describe the anatomy, innervation and functions of the muscles of the anterior, lateral and posterior abdominal walls. Discuss their functional relations
Anatomical Considerations for Lab Practical II
 Anatomical Considerations for Lab Practical II For each of the following please be prepared to provide: Identification System Organ(s) or ducts to Function(s) location which it is attached Use your lecture
Anatomical Considerations for Lab Practical II For each of the following please be prepared to provide: Identification System Organ(s) or ducts to Function(s) location which it is attached Use your lecture
2. List the 8 pelvic spaces: list one procedure or dissection which involves entering that space.
 Name: Anatomy Quiz: Pre / Post 1. In making a pfannensteil incision you would traverse through the following layers: a) Skin, Camper s fascia, Scarpa s fascia, external oblique aponeurosis, internal oblique
Name: Anatomy Quiz: Pre / Post 1. In making a pfannensteil incision you would traverse through the following layers: a) Skin, Camper s fascia, Scarpa s fascia, external oblique aponeurosis, internal oblique
Development of the Digestive System. W.S. O The University of Hong Kong
 Development of the Digestive System W.S. O The University of Hong Kong Plan for the GI system Then GI system in the abdomen first develops as a tube suspended by dorsal and ventral mesenteries. Blood
Development of the Digestive System W.S. O The University of Hong Kong Plan for the GI system Then GI system in the abdomen first develops as a tube suspended by dorsal and ventral mesenteries. Blood
Ureters, Urinary Bladder & Urethra
 Ureters, Urinary Bladder & Urethra Please check our Editing File هذا العمل ال يغني عن المصدر األساسي للمذاكرة Lecture 2 } و م ن ي ت و ك ع ل ا لل ه ف ه و ح س ب ه { Objectives o Describe the course of ureter
Ureters, Urinary Bladder & Urethra Please check our Editing File هذا العمل ال يغني عن المصدر األساسي للمذاكرة Lecture 2 } و م ن ي ت و ك ع ل ا لل ه ف ه و ح س ب ه { Objectives o Describe the course of ureter
The Digestive System
 The Digestive System Identify the Structure and Function. Mesentery of the Large Intestine The mesentery functions to connect the visceral organs to the abdominal wall. Identify the Structure. Nasal Cavity
The Digestive System Identify the Structure and Function. Mesentery of the Large Intestine The mesentery functions to connect the visceral organs to the abdominal wall. Identify the Structure. Nasal Cavity
Benha University. Faculty of Medicine. Anatomy Department Course code (MED 0701) Model answer of Anatomy examination. (Abdomen,Pelvis and Thorax)
 Model answer of Anatomy examination. (Abdomen,Pelvis and Thorax)") 1 Benha University Faculty of Medicine Anatomy Department Course code (MED 0701) Model answer of Anatomy examination (Abdomen,Pelvis and Thorax) 1 st year 2 nd term Date :18 /5 /2013 2 I-Short account
1 Benha University Faculty of Medicine Anatomy Department Course code (MED 0701) Model answer of Anatomy examination (Abdomen,Pelvis and Thorax) 1 st year 2 nd term Date :18 /5 /2013 2 I-Short account
The embryonic endoderm initially is widely connected with the yolk sac. As a consequence of cephalocaudal and lateral folding, a portion of the
 DIGESTIVE SYSTEM The embryonic endoderm initially is widely connected with the yolk sac. As a consequence of cephalocaudal and lateral folding, a portion of the endoderm-lined yolk sac cavity is incorporated
DIGESTIVE SYSTEM The embryonic endoderm initially is widely connected with the yolk sac. As a consequence of cephalocaudal and lateral folding, a portion of the endoderm-lined yolk sac cavity is incorporated
Lab 5 Digestion and Hormones of Digestion. 7/16/2015 MDufilho 1
 Lab 5 Digestion and Hormones of Digestion 1 Figure 23.1 Alimentary canal and related accessory digestive organs. Mouth (oral cavity) Tongue* Parotid gland Sublingual gland Submandibular gland Salivary
Lab 5 Digestion and Hormones of Digestion 1 Figure 23.1 Alimentary canal and related accessory digestive organs. Mouth (oral cavity) Tongue* Parotid gland Sublingual gland Submandibular gland Salivary
-15. -Alaa Albandi. -Dr. Mohammad Almohtasib. 0 P a g e
 -15 -Alaa Albandi - -Dr. Mohammad Almohtasib 0 P a g e In this last lecture, we will talk about the sigmoid colon, rectum, and anal canal. Sigmoid colon It has a mesentery called pelvic mesocolon or sigmoidal
-15 -Alaa Albandi - -Dr. Mohammad Almohtasib 0 P a g e In this last lecture, we will talk about the sigmoid colon, rectum, and anal canal. Sigmoid colon It has a mesentery called pelvic mesocolon or sigmoidal
ABDOMEN. 2. The highest branch of the abdominal aorta is: (a) R suprarenal a (b) Coeliac trunk (c) L renal a (d) L gonadal a (e) SMA
 R suprarenal a (b) Coeliac trunk (c) L renal a (d) L gonadal a (e) SMA") ABDOMEN 1. The duodenum: (a) is a retroperitoneal structure (b) is 25cm long (c) lies between the levels of L2-L4 (d) in its fourth part lies to the R of the aorta (e) all of the above 2. The highest branch
ABDOMEN 1. The duodenum: (a) is a retroperitoneal structure (b) is 25cm long (c) lies between the levels of L2-L4 (d) in its fourth part lies to the R of the aorta (e) all of the above 2. The highest branch
ANATYOMY OF The thigh
 ANATYOMY OF The thigh 1- Lateral cutaneous nerve of the thigh Ι) Skin of the thigh Anterior view 2- Femoral branch of the genitofemoral nerve 5- Intermediate cutaneous nerve of the thigh 1, 2 and 3 are
ANATYOMY OF The thigh 1- Lateral cutaneous nerve of the thigh Ι) Skin of the thigh Anterior view 2- Femoral branch of the genitofemoral nerve 5- Intermediate cutaneous nerve of the thigh 1, 2 and 3 are
Overview of the Digestive
 Overview of the Digestive System Bởi: OpenStaxCollege The function of the digestive system is to break down the foods you eat, release their nutrients, and absorb those nutrients into the body. Although
Overview of the Digestive System Bởi: OpenStaxCollege The function of the digestive system is to break down the foods you eat, release their nutrients, and absorb those nutrients into the body. Although
The Thoracic wall including the diaphragm. Prof Oluwadiya KS
 The Thoracic wall including the diaphragm Prof Oluwadiya KS www.oluwadiya.com Components of the thoracic wall Skin Superficial fascia Chest wall muscles (see upper limb slides) Skeletal framework Intercostal
The Thoracic wall including the diaphragm Prof Oluwadiya KS www.oluwadiya.com Components of the thoracic wall Skin Superficial fascia Chest wall muscles (see upper limb slides) Skeletal framework Intercostal
Perineum. done by : zaid al-ghnaneem
 Perineum done by : zaid al-ghnaneem Hello everyone, this sheet will talk about 2 nd Lecture which is Perineum but there are some slides and info from 1 st Lecture. Everything included Slides + Pics Let
Perineum done by : zaid al-ghnaneem Hello everyone, this sheet will talk about 2 nd Lecture which is Perineum but there are some slides and info from 1 st Lecture. Everything included Slides + Pics Let
THE ABDOMEN SUPRARENAL GLANDS KIDNEY URETERS URINARY BLADDER
 THE ABDOMEN SUPRARENAL GLANDS KIDNEY URETERS URINARY BLADDER THE SUPRARENAL GLANDS The suprarenal (adrenal) glands lie immediately superior and slightly anterior to the upper pole of either kidney. Golden
THE ABDOMEN SUPRARENAL GLANDS KIDNEY URETERS URINARY BLADDER THE SUPRARENAL GLANDS The suprarenal (adrenal) glands lie immediately superior and slightly anterior to the upper pole of either kidney. Golden
The Digestive System Laboratory
 The Digestive System Laboratory 1 The Digestive Tract The alimentary canal is a continuous tube stretching from the mouth to the anus. Liver Gallbladder Small intestine Anus Parotid, sublingual, and submaxillary
The Digestive System Laboratory 1 The Digestive Tract The alimentary canal is a continuous tube stretching from the mouth to the anus. Liver Gallbladder Small intestine Anus Parotid, sublingual, and submaxillary
Gross Anatomy of the Urinary System
 Gross Anatomy of the Urinary System Lecture Objectives Overview of the urinary system. Describe the external and internal anatomical structure of the kidney. Describe the anatomical structure of the ureter
Gross Anatomy of the Urinary System Lecture Objectives Overview of the urinary system. Describe the external and internal anatomical structure of the kidney. Describe the anatomical structure of the ureter
SMALL INTESTINE LARGE INTESTINE RECTUM ABDOMINAL AORTA INFERIOR VENA CAVA THE ABDOMEN
 SMALL INTESTINE LARGE INTESTINE RECTUM ABDOMINAL AORTA INFERIOR VENA CAVA THE ABDOMEN THE SMALL INTESTINE THE SMALL INTESTINE: Is the longest part of the gastrointesanal tract - length of 5 metres (3 7
SMALL INTESTINE LARGE INTESTINE RECTUM ABDOMINAL AORTA INFERIOR VENA CAVA THE ABDOMEN THE SMALL INTESTINE THE SMALL INTESTINE: Is the longest part of the gastrointesanal tract - length of 5 metres (3 7
Basic Body Structure
 Basic Body Structure The Cell All life consists of microscopic living structures called cells. They perform various functions throughout the body. All cells are similar in structure, but not identical.
Basic Body Structure The Cell All life consists of microscopic living structures called cells. They perform various functions throughout the body. All cells are similar in structure, but not identical.
Gastrointestinal System!
 Gastrointestinal System! Assoc. Prof. Prasit Suwannalert, Ph.D. (Email: prasit.suw@mahidol.ac.th)! Objectives: After learning, student should be able to describe and discuss in topics of! 1. Anatomical
Gastrointestinal System! Assoc. Prof. Prasit Suwannalert, Ph.D. (Email: prasit.suw@mahidol.ac.th)! Objectives: After learning, student should be able to describe and discuss in topics of! 1. Anatomical
Midterm 2 is Tuesday 5/28/13
 Business Reminder: No class Monday (Memorial Day) Midterm 2 is Tuesday 5/28/13 Optional review session tomorrow @ 5pm Homework due in Lab 1. PreLab 8 (1pt) 2. Replace a Missing Assignment (4 pts) Homework
Business Reminder: No class Monday (Memorial Day) Midterm 2 is Tuesday 5/28/13 Optional review session tomorrow @ 5pm Homework due in Lab 1. PreLab 8 (1pt) 2. Replace a Missing Assignment (4 pts) Homework
#1 - Chapter 1 - Anatomy. General Anatomical Terms The Anatomical Position
 #1 - Chapter 1 - Anatomy General Anatomical Terms The Anatomical Position The anatomical position is a stance in which a person stands erect with the feet flat on the floor and close together, arms at
#1 - Chapter 1 - Anatomy General Anatomical Terms The Anatomical Position The anatomical position is a stance in which a person stands erect with the feet flat on the floor and close together, arms at
consists of: Muscular, hollow tube (= digestive tract ) + Various accessory organs
 + Various accessory organs") DIGESTIVE SYSTEM consists of: Muscular, hollow tube (= digestive tract ) + Various accessory organs FUNCTION Individual parts function in: ingestion mechanical digestion chemical and enzymatic digestion
DIGESTIVE SYSTEM consists of: Muscular, hollow tube (= digestive tract ) + Various accessory organs FUNCTION Individual parts function in: ingestion mechanical digestion chemical and enzymatic digestion