Second Generation Enteral Nutrition Feeding Protocols: Taking us the the next level of performance
|
|
|
- Hollie Griffin
- 6 years ago
- Views:
Transcription




1 Second Generation Enteral Nutrition Feeding Protocols: Taking us the the next level of performance


2 Mr CD 47 renal transplant Severe CAP Septic shock, ARDS, MODs Requires vasopressors for days Admitting resident not sure if feed, wait till AM Day 3- trickle feeds (20 cc/hr) Feeds on and off again for whole first week Nurses notes gastric residual volume of 60cc Ask resident what to do Resident says wait till rounds
3 Adequacy of EN kcal Prescribed Engergy Energy Received From Enteral Feed Days Prolonged ICU stay, discharged weak and debilitated. Dies on day 43 in hospital from massive PE


4
5 In patients with high gastric residual volumes: use of motility agents 58.7% (site average range: 0-100%) use of small bowel feeding 14.7% (range: 0-100%) Cahill N Crit Care Med 2010
6 Average time to start of EN was 46.5 hours (site average range: hours) Cahill NE CCM 2010
7 Consequences of Iatrogenic Malnutrition Adequacy of EN kcal Caloric Debt Prescribed Engergy Energy Received From Enteral Feed Days Caloric debt associated with: Longer ICU stay Days on mechanical ventilation Complications Mortality Rubinson CCM 2004; Villet Clin Nutr 2005; Dvir Clin Nutr 2006; Alberda ICM 2009

8 Point prevalence survey of nutrition practices in ICU s around the world conducted Jan. 27, 2007 Enrolled 2772 patients from 158 ICU s over 5 continents Included ventilated adult patients who remained in ICU >72 hours
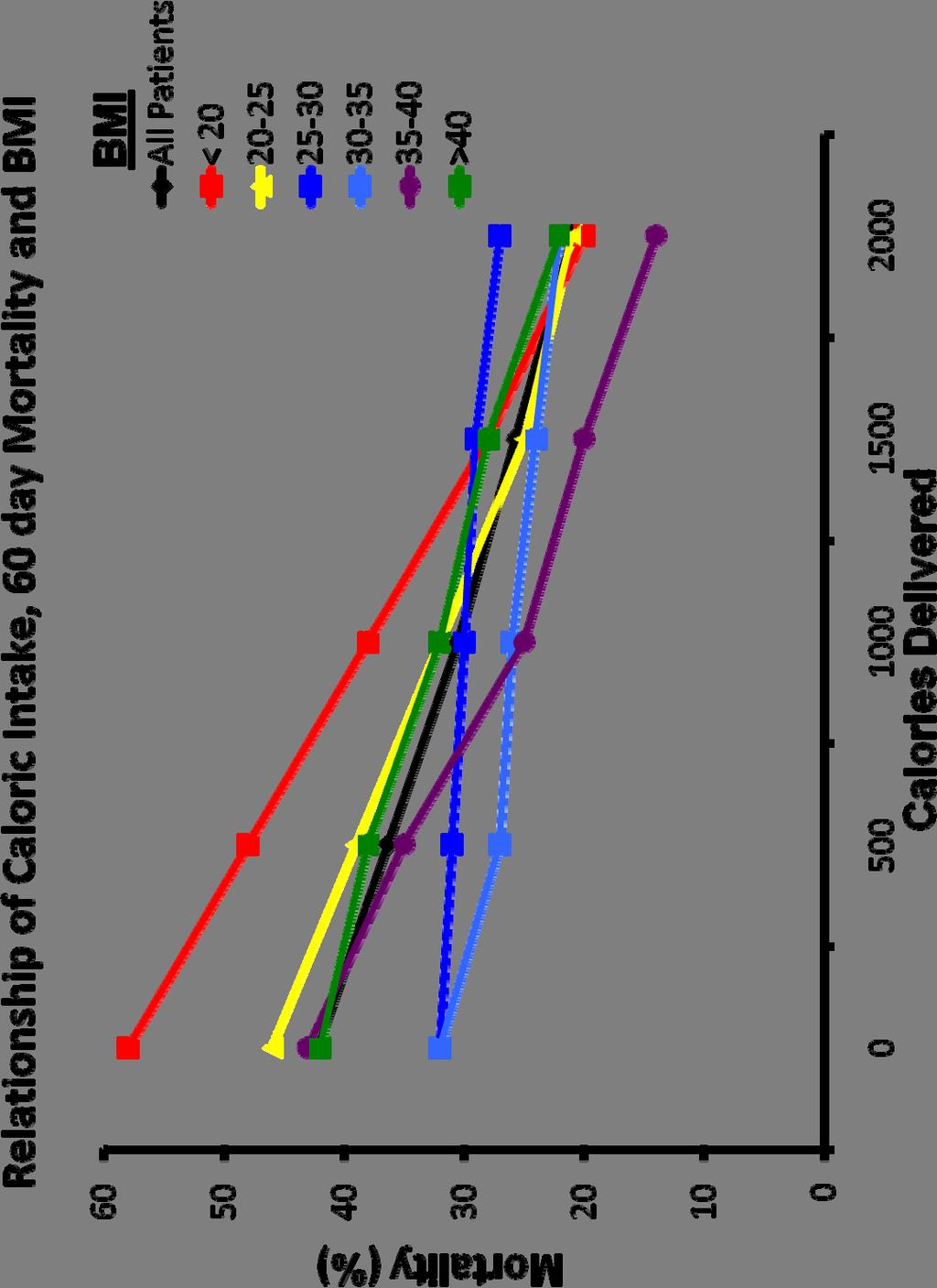
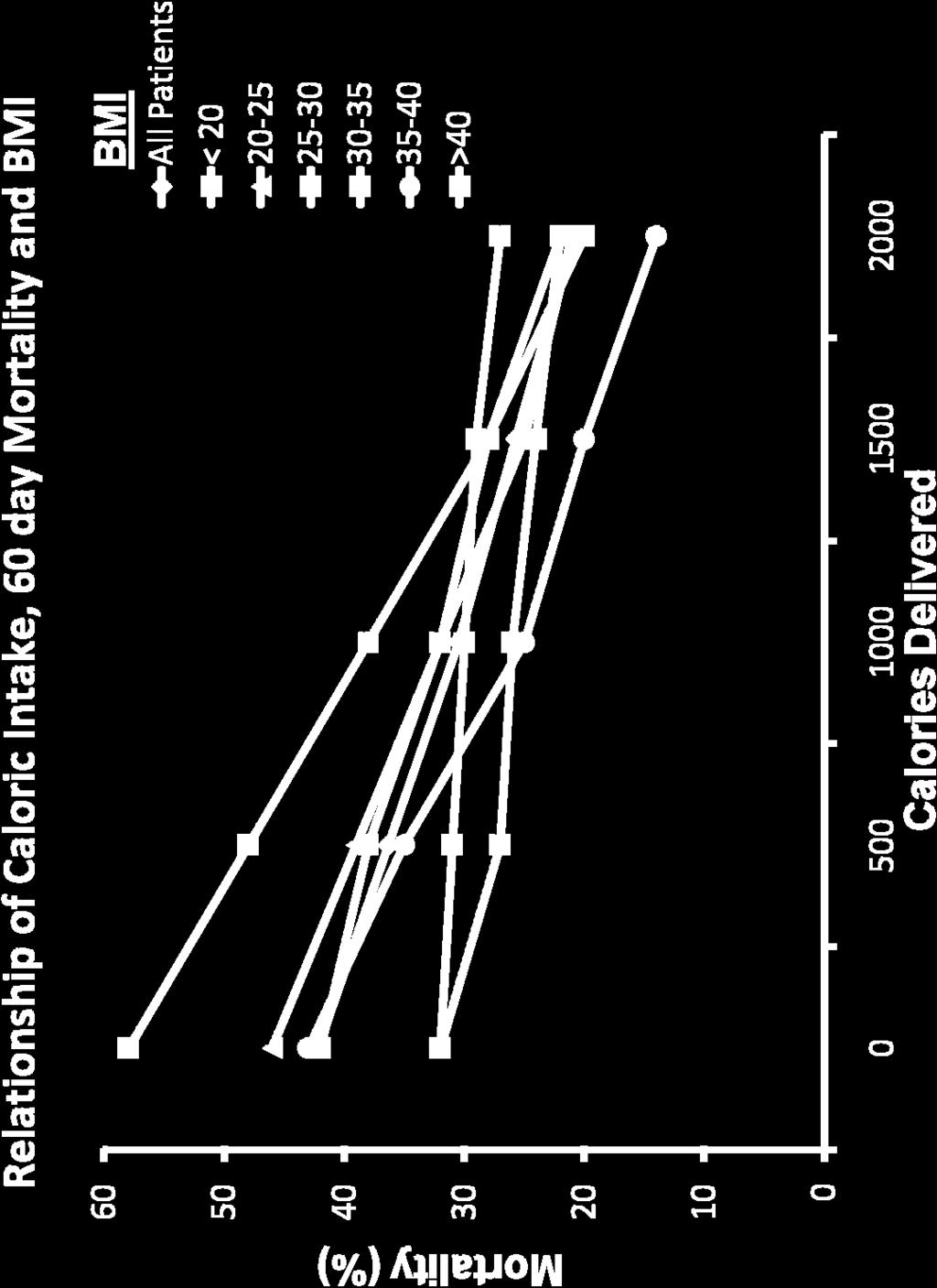
9 Hypothesis There is a relationship between amount of energy and protein received and clinical outcomes (mortality and # of days on ventilator) The relationship is influenced by nutritional risk BMI is used to define chronic nutritional risk
10 What Study Patients Actually Rec d Average Calories in all groups: 1034 kcals and 47 gm of protein Result: Average caloric deficit in Lean Pts: 7500kcal/10days Average caloric deficit in Severely Obese: 12000kcal/10days
11 Relationship Between Increased Calories and 60 day Mortality BMI Group Odds Ratio 95% Confidence Limits P-value Overall < < < < < >= Legend: Odds of 60-day Mortality per 1000 kcals received per day adjusting for nutrition days, BMI, age, admission category, admission diagnosis and APACHE II score.
12
13 Effect of Increasing Amounts of Calories from EN on Infectious Complications Multicenter observational study of 207 patients >72 hrs in ICU followed prospectively for development of infection for increase of 1000 cal/day, OR of infection at 28 days Heyland (in submission)
14 Effect of Increasing Amounts of Protein from EN on Infectious Complications Multicenter observational study of 207 patients >72 hrs in ICU followed prospectively for development of infection for increase of 30 gram/day, OR of infection at 28 days Heyland (in submission)
15 RCT Level of Evidence that More EN= Improved Outcomes RCTs of aggressive feeding protocols Results in better protein-energy intake Associated with reduced complications and improved survival Taylor et al Crit Care Med 1999; Martin CMAJ 2004 Meta-analysis of Early vs Delayed EN Reduced infections: RR 0.76 (.59,0.98),p=0.04 Reduced Mortality: RR 0.68 (0.46, 1.01) p=0.06
 is")


16 More (and Earlier) is Better! Our Field of Dream If you feed them (better!) They will leave (sooner!)
17 Updated January 2009 Summarizes 191 trials studying >15000 patients 34 topics 18 recommendations
18 Use of a feeding protocol that incorporates motility agents and small bowel feeding tubes should be considered
19

20
21 The Impact of Enteral Feeding Protocols on Enteral Nutrition Delivery: Results of a multicenter observational study International, prospective, observational, cohort studies conducted in 2007 and 2008 from 269 Intensive Care Units (ICUs) in 28 countries Included 5497 mechanically ventilated adult patients > 3 days in ICU Sites recorded the presence or absence of a feeding protocol Sites provided nutritional data on enrolled patients from ICU admission to ICU discharge for a max of 12 days. Heyland JPEN 2010 ( in press)
22 The Impact of Enteral Feeding Protocols on Enteral Nutrition Delivery: Results of a multicenter observational study Characteristics Total n=269 Feeding Protocol Yes 208 (78%) Gastric Residual Volume Tolerated in Protocol Mean (range) 217 ml (50, 500) Elements included in Protocol 15.2% using the recommended threshold volume of 250 ml Motility agents 68.5% Small bowel feeding 55.2% HOB Elevation 71.2 % Heyland JPEN 2010 ( in press)
23 The Impact of Enteral Feeding Protocols on Enteral Nutrition Delivery: Results of a multicenter observational study Calories from EN Total Calories P<0.05 Protocol No Protocol Time to start EN from ICU admission: 41.2 in protocolized sites vs 57.1 hours in those without a protocol Patients rec ing motility agents: 61.3% in protocolized sites vs 49.0% in those without P<0.05 Heyland JPEN 2010 ( in press)

24 Can we do better? The same thinking that got you into this mess won t get you out of it!
25 Enhanced Protein-Energy Provision via the Enteral Route in Critically Ill Patients: The PEP up Protocol
26 The Efficacy of Enhanced Protein-Energy Provision via the Enteral Route in Critically Ill Patients: The PEP up Protocol! Different feeding options based on hemodynamic stability and suitability for high volume intragastric feeds. In select patients, we start the EN immediately at goal rate, not at 25 ml/hr. We target a 24 hour volume of EN rather than an hourly rate and provide the nurse with the latitude to increase the hourly rate to make up the 24 hour volume. Start with a semi elemental solution, progress to polymeric Tolerate higher GRV threshold (250 ml or more) Motility agents and protein supplements are started immediately, rather than started when there is a problem. A Major Paradigm Shift in How we Feed Enterally

27 Does One Size Fit All?
28 Initial Efficacy and Tolerability of Early Enteral Nutrition with Immediate or Gradual Introduction in Intubated Patients This study randomized 100 mechanically ventilated patients (not in shock) to Immediate goal rate vs gradual ramp up (our usual standard). The immediate goal group rec d more calories with no increase in complications Desachy ICM 2008;34:1054
29 Initial Efficacy and Tolerability of Early Enteral Nutrition with Immediate or Gradual Introduction in Intubated Patients Desachy ICM 2008;34:1054
30 What About Feeding the Hypotensive Patient? Resuscitation is the priority No sense in feeding someone dying of progressive circulatory failure However, if resuscitated yet remaining on vasopressors: Safety and Efficacy of Enteral Feeding??


31 Effect of Early Enteral Feeding on Hemodynamic Variables Animal model of sepsis and lung injury Splanchnic hemodynamics decline with endotoxemia Feeding reverses this decine and improves intestinal perfusion compared to placebo fed Purcell Am J Surg 1993;165:188 Kazamias World J Surgery 1998;22:6-11 Anesthesia/Operative Model of stress Surgical insult induces inflammatory mediators and markers of oxidative stress Feeding attenuates oxidative stress and chemokine production Kotzampassi Mol Nutr Food Res 2009;53:770


32 9 patients day 1 Post-op following CPB requiring inotropes and vasopressors Feed enterally; metabolic response consistent with substrates being utilized
33 Feeding the Hypotensive Patient? Prospectively collected multi-institutional ICU database. 1,174 patients who required mechanical ventilation and were on vasopressor agents to support blood pressure for more than two days Patients divided whether or not they received enteral nutrition within 48 hours of mechanical ventilation onset. EARLY EN Group: 707 patients (60%) LATE EN Group: 467 patients (40%) The primary endpoints were overall ICU and hospital mortality. Data also analyzed after controlling for confounding by matching for propensity score Khalid et al. AJCC 2010;19:


34 Feeding the Hypotensive Patient? The beneficial effect of early feeding is more evident in the sickest patients, i.e, those on multiple vasopressor agents and those with persistent vasopressor needs (>2 days). Khalid et al. AJCC 2010;19:

35 Trophic Feeds Progressive atrophy of villous height and Crypt depth in absence of EN Leads to increased permeability and decreased IgA secretion Can be preserved by a minimum of 10-15% of goal calories. Observational study of xx critically ill patients suggests TPN+trophic feeds associated with reduced infection and mortality compared to TPN alone^ ^Marik Crit Care &Shock 2002;5:1-10 A= No EN; B = 100% EN Ohta Am J Surgery 2003;185:79-85
36 The PEP up Protocol Stable patients should be able to tolerate goal rate Begin 24 hour volume-based feeds. After initital tube placement confirmed, start Pepatmen 1.5. Totlal volume to receive in 24 hours is 17ml x weight (kg)= <write in 24 target volume>. Determine initial rate as per Volume Based Feeding Schedule. Monitor gastric residual volumes as per Adult Gastric Flow Chart and Volume Based Feeding Schedule. OR Begin Peptamen 1.5 at 10 ml/h after initial tube placement confirmed. Hold if gastric residual volume >500 ml and ask Doctor to reassess. Reassess ability to transition to 24 hour volume-based feeds next day. {Intended for patient who is hemodynamically unstable (on high dose or escalating doses of vasopressors, or inadequately resuscitated) or not suitable for high volume enteral feeding (ruptured AAA, upper intestinal anastomosis, or impending intubation)} OR NPO. Please write in reason:. (only if contraindication to EN present: bowel perforation, bowel obstruction, proximal high output fistula. Recent operation and high NG output not a contraindication to EN.) Reassess ability to transition to 24 hour volume-based feeds next day. We use a concentrated solution to maximize calories per ml If unstable or unsuitable, just use trophic feeds Note indications for trophic feeds Drs need to justify why there are keeping patients NPO We want to minimize the use of NPO but if selected, need to reassess next day Note, there are only a few absolute contraindications to EN
37 Rather than hourly goal rate, we changed to a 24 hour volume-based goal Nurse has responsibility to administer than volume over the 24 period with the following guidelines: If the total volume ordered is 1800 ml the hourly amount to feed is 75 ml/hour. If patient was fed 450 ml of feeding (6 hours) and the tube feeding is on hold for 5 hours, then subtract from goal volume the amount of feeding patient has already received. Volume Ordered per 24 hours 1800 ml Tube feeding in (current day) 450 = Volume of feeding remaining in day to feed = 1350 ml remaining to feed Patient now has 13 hours left in the day to receive 1350 ml of tube feeding. Divide remaining volume over remaining hours (1350ml/13 hrs) to determine new hourly goal rate Round up so new rate would be 105 ml/hr for 13 hours. The following day, at shift change, the rate drops back to 75 ml/hour.
38 As a consequence, our bedside feeding algorithm has changed... Adult ICU Gastric Feeding Flow Chart Place feeding tube or use existing gastric drainage tube. X-ray to confirm placement (as required) Attempt to elevate head of bed to 45 unless contraindicated. Start feed at initial rate ordered. Replace aspirate. Set rate of EN based on remaining volumes and remaining times till end of shift. See flow chart A No Measure gastric residual volumes q4 h. Is the residual volume greater than 250 ml? NOTE: Do not aspirate small bowel tubes. No Has the prescribed volume/day been delivered? Yes No Yes Replace 250 ml of aspirate. Reduce rate by 25 ml/h to no less than 10 ml/h. Step 1: Consider adding erythromycin 200 mg IV q12h (may prolong Qtc.). If 4 doses erythromycin ineffective, go to Step 2. Step 2: Consider small bowel feeding tube placement and discontinue motility agents thereafter. Yes Was the residual volume greater than 250 ml the last time it was measured? Replace aspirate. Reassess motility agents after feeds tolerated at target rate for 24 hours.
39 It s not just about calories... Inadequate protein intake Loss of lean muscle mass Immune dysfunction Weak Prolonged mechanical ventilation So in order to minimize this, we order: Protein supplement Beneprotein 14 grams mixed in 120 mls sterile water administered bid via NG

40 Aggressive feeding in patients who haven t been eating much or in skinny patients, may cause problems with electrolyte and Phos balance. Potential for refeeding syndrome That s why we check the lytes, Phos, Mg and Ca at least twice a day for the first 3 days, and then if no problem, back to usual ICU blood work. If there are problems then at rate of feeding needs to be decreased or not accelerated until the lytes etc. are corrected.

41 Other Strategies to Maximize the Benefits and Minimize the Risks of EN Head of Bed elevation to 45 (or at least 30 if the patient doesn t tolerate 45) This will reduce regurgitation, aspiration and subsequent Pneumonia List of Contraindications to HOB Elevation unstable c-spine hemodynamically unstable Pelvic fractures with instability Prone position Intra-aortic ballon pump Procedures Unable because of obesity

42 Other Strategies to Maximize the Benefits and Minimize the Risks of EN Impaired motility Medications Metabolic, electrolyte abnormalities Underlying disease Dysmotility linked to decreased tolerance of EN gastropulmonary route of infection Trials of Cisapride, Erythromycin, Metoclopramide,
43 Pro-motility Agents Conclusion: 1) Motility agents have no effect on mortality or infectious complications in critically ill patients. 2) Motility agents may be associated with an increase in gastric emptying, a reduction in feeding intolerance and a greater caloric intake in critically ill patients. Based on 1 level 1 study and 5 level 2 studies, in critically ill patients who experience feed intolerance (high gastric residuals, emesis), we recommend the use of a promotility agent. Given the safety concerns associated with erythromycin, the recommendation is made for metoclopramide. There are insufficient data to make a recommendation about the use of combined use of metoclopramide and erythromycin Canadian CPGs
44 Other Strategies to Maximize the Benefits and Minimize the Risks of EN Motility agents started at initiation of EN rather that waiting till problems with High GRV develop. Maxeran 10 mg IV q 6h (halved in renal failure) If still develops high gastric residuals, add Erythromycin 200 mg q 12h. Can be used together for up to 7 days but should be discontinued when not needed any more Reassess need for motility agents daily

45 Other Strategies to Maximize the Benefits and Minimize the Risks of EN If intragastric feeds not tolerated, problems with high GRVs refractory to motility agents, we recommend small bowel feeding tube They may need a gentle reminder to get the small bowel feeding tube in place Hey Dr. can we get that small bowel tube in place so I can get their volume of EN in asap!
46 Small Bowel vs. Gastric Feeding: A meta-analysis Effect on Nutritional Endpoints 4 studies that document increased delivery of protein and calories with small bowel feeding; 2 show no difference One study that documents time goal quicker with small bowel Fewer interruptions with high gastric residuals with small bowel 2 studies document delay in initiating feeds secondary to delay in obtaining small bowel access
47 Small Bowel vs. Gastric Feeding: A meta-analysis Effect on VAP
48 Tube Position Does Postpyloric Feeding Reduce Risk of GER and Aspiration? # of patients % positive for GER % positive for Aspiration Stomach D D D Total P=0.004 P=0.09 Heyland CCM 2001;29:

49 FRICTIONAL ENTERAL FEEDING TUBE (TIGER TUBE TM ) Flaps to allow peristalsis to pull tube passively forward Sucessful jejunal placement >95%

50 CORTRAK A new paradigm in feeding tube placement Aid to placement of feeding tubes into the stomach or small bowel The tip of the stylet is a transmitter. Signal is picked up by an external receiver unit. Signal is fed to an attached Monitor unit. Provides user with a realtime, graphic display that represents the path of the feeding tube.
51 A Change to Nursing Report Adequacy of Nutrition Support = Please report this % on rounds as part of the GI systems report 24 hour volume of EN received Volume prescribed to meet caloric requirements in 24 hours

52 When performance is measured, performance improves. When performance is measured and reported back, the rate of improvement accelerates. Thomas Monson
53 Efficacy of Enhanced Protein-Energy Provision via the Enteral Route in Critically Ill Patients: The PEP up Protocol A Single center feasibility trial

54 The Efficacy of Enhanced Protein-Energy Provision via the Enteral Route in Critically Ill Patients: The PEP up Protocol! Different feeding options based on hemodynamic stability and suitability for high volume intragastric feeds. In select patients, we start the EN immediately at goal rate, not at 25 ml/hr. We target a 24 hour volume of EN rather than an hourly rate and provide the nurse with the latitude to increase the hourly rate to make up the 24 hour volume. Start with a semi elemental solution, progress to polymeric Tolerate higher GRV threshold (250 ml or more) Motility agents and protein supplements are started immediately Nurse reports daily on nutritional adequacy. A Major Paradigm Shift in How we Feed Enterally
55 Evaluation Study Purpose: to evaluate the safety and acceptibility of this new protocol Before (n=20) and after (n=30) study Consecutive eligible mechanically ventilated patients >3days Compared nutritional outcomes At the end of each nursing shift, will ask the nurse the following 4 questions:
56 Evaluation Questions 1. Were you exposed to the educational interventions and if so, how useful did you find them? 2. Did you encounter any situation or event that in your opinion, compromised the patient s safety? 3. Overall, how acceptable was this new protocol (1-totally unacceptable; 10- totally acceptable) 4. Any suggestions for improving the protocol?
57 RESULTS
58 Nurses Ratings of Acceptability After Group Mean (range) 24 hour volume based target 7.0 (1-10) Starting at a high hourly rate 5.9 (1-10) Starting motility agents right away 7.4 (1-10) Starting protein supplements right away 7.6 (1-10) Acceptability of the overall protocol 7.1 (1-10) 1=totally unacceptable and 10=totally acceptable No adverse events noted by Nurses Heyland Crit Care 2010
59 Results Patient s initial prescription NPO trophic feeds 25 ml/ hr 24 volume based feeds Before 8 (40%) 0 12 After 6 (20%) 6 18 Day 1 use of motility agents 0 7/30 (23.3%) Day 1 use of Protein supplements Complications Vomiting Regurgitation Witnessed Aspiration VAP 0 9/30 (30.0%) 15.0% 10.0% 10.0% 25% 6.7% % Heyland Crit Care 2010
60 The Efficacy of Enhanced Protein-Energy Provision via the Enteral Route in Critically Ill Patients: The PEP up Protocol! Adequacy of Calories from EN (Before Group vs. After Group on Full Volume Feeds) Day 1 Day 2 Day 3 Day 4 Day 5 Day 6 Day 7 Total P-value < Heyland Crit Care 2010
61 The Efficacy of Enhanced Protein-Energy Provision via the Enteral Route in Critically Ill Patients: The PEP up Protocol! Adequacy of Protein from EN (Before Group vs. After Group on Full Volume Feeds) Day 1 Day 2 Day 3 Day 4 Day 5 Day 6 Day 7 Total P-value 0.03 < < Heyland Crit Care 2010
62 Conclusions Significant iatrogenic malnutrition occurs worldwide. In an attempt to maximize EN safely, feeding protocols should be part of standard of care Through optimization of different aspects of the standard feeding protocol, we can further optimize EN delivery The PEP up protocol is acceptable and safe and warrants further investigation
63 Questions?
MAIN FEATURES. OF THE PEP up PROTOCOL. All patients will receive Peptamen 1.5 initially. All patients will start on Beneprotein
 MAIN FEATURES OF THE PEP up PROTOCOL All patients will receive Peptamen 1.5 initially All patients will start on Beneprotein - 2 packets (14 g) mixed in 120ml water administered bid via NG All patients
MAIN FEATURES OF THE PEP up PROTOCOL All patients will receive Peptamen 1.5 initially All patients will start on Beneprotein - 2 packets (14 g) mixed in 120ml water administered bid via NG All patients
NO DISCLOSURES 5/9/2015
 Annette Stralovich-Romani, RD, CNSC Adult Critical Care Nutritionist UCSF Medical Center NO DISCLOSURES Incidence & consequences of malnutrition Underfeeding in the ICU Causes/ consequences Nutrition intervention
Annette Stralovich-Romani, RD, CNSC Adult Critical Care Nutritionist UCSF Medical Center NO DISCLOSURES Incidence & consequences of malnutrition Underfeeding in the ICU Causes/ consequences Nutrition intervention
Division of Acute Care Surgery Clinical Practice Policies, Guidelines, and Algorithms: Enteral Nutrition Algorithm Clinical Practice Guideline
 Division of Acute Care Surgery Clinical Practice Policies, Guidelines, and Algorithms: Enteral Nutrition Algorithm Clinical Practice Guideline Original Date: 08/2011 Purpose: To promote the early use of
Division of Acute Care Surgery Clinical Practice Policies, Guidelines, and Algorithms: Enteral Nutrition Algorithm Clinical Practice Guideline Original Date: 08/2011 Purpose: To promote the early use of
Nutrition Supplementation in the ICU
 Nutrition Supplementation in the ICU ROSEMARY KOZAR MD PHD SHOCK TRAUMA UNIVERSITY OF MARYLAND Canadian Clinical Practice Guidelines www.criticalcarenutrition.com NEJM March 27, 2014 1 Use of Enteral vs
Nutrition Supplementation in the ICU ROSEMARY KOZAR MD PHD SHOCK TRAUMA UNIVERSITY OF MARYLAND Canadian Clinical Practice Guidelines www.criticalcarenutrition.com NEJM March 27, 2014 1 Use of Enteral vs
The Meat and Potatoes of Critical Care Nutrition ROSEMARY KOZAR MD PHD SHOCK TRAUMA UNIVERSITY OF MARYLAND
 The Meat and Potatoes of Critical Care Nutrition ROSEMARY KOZAR MD PHD SHOCK TRAUMA UNIVERSITY OF MARYLAND 2013 Canadian Clinical Practice Guidelines www.criticalcarenutrition.com NEJM March 27, 2014 Use
The Meat and Potatoes of Critical Care Nutrition ROSEMARY KOZAR MD PHD SHOCK TRAUMA UNIVERSITY OF MARYLAND 2013 Canadian Clinical Practice Guidelines www.criticalcarenutrition.com NEJM March 27, 2014 Use
L.Mageswary Dietitian Hospital Selayang
 L.Mageswary Dietitian Hospital Selayang 14 15 AUG ASMIC 2015 Learning Objectives 1. To understand the importance of nutrition support in ICU 2. To know the right time to feed 3. To understand the indications
L.Mageswary Dietitian Hospital Selayang 14 15 AUG ASMIC 2015 Learning Objectives 1. To understand the importance of nutrition support in ICU 2. To know the right time to feed 3. To understand the indications
STRATEGIES TO IMPROVE ENTERAL FEEDING TOLERANCE. IS IT WORTH IT? ENGELA FRANCIS RD(SA)
") STRATEGIES TO IMPROVE ENTERAL FEEDING TOLERANCE. IS IT WORTH IT? ENGELA FRANCIS RD(SA) DEFINITION OF ENTERAL FEEDING INTOLERANCE Gastrointestinal feeding intolerance are usually defined as: High gastric
STRATEGIES TO IMPROVE ENTERAL FEEDING TOLERANCE. IS IT WORTH IT? ENGELA FRANCIS RD(SA) DEFINITION OF ENTERAL FEEDING INTOLERANCE Gastrointestinal feeding intolerance are usually defined as: High gastric
5.2 Strategies to Optimize Delivery and Minimize Risks of EN: Motility Agents May 2015
 5.2 Strategies to Optimize Delivery and Minimize Risks of EN: Motility Agents May 2015 There were no new randomized controlled trials since the 2009 and 2013 updates and hence there are no changes to the
5.2 Strategies to Optimize Delivery and Minimize Risks of EN: Motility Agents May 2015 There were no new randomized controlled trials since the 2009 and 2013 updates and hence there are no changes to the
Extremely well tolerated. Feeding shock
 Extremely well tolerated Feeding shock FEEDING DURING CIRCULATORY FAILURE Dr S Omar Chris Hani Baragwanath Hospital Hospital/University of Witwatersrand Introduction Circulatory shock lack of adequate
Extremely well tolerated Feeding shock FEEDING DURING CIRCULATORY FAILURE Dr S Omar Chris Hani Baragwanath Hospital Hospital/University of Witwatersrand Introduction Circulatory shock lack of adequate
2.0 Early vs. Delayed Nutrient Intake May 2015
 2.0 Early vs. Delayed Nutrient Intake May 2015 There were no new randomized controlled trials since the 2013 update and hence there are no changes to the following summary of evidence. 2013 Recommendation:
2.0 Early vs. Delayed Nutrient Intake May 2015 There were no new randomized controlled trials since the 2013 update and hence there are no changes to the following summary of evidence. 2013 Recommendation:
3.2 Nutritional Prescription of Enteral Nutrition: Achieving Target Dose of Enteral Nutrition March 2013
 . Nutritional Prescription of Enteral Nutrition: Achieving Target Dose of Enteral Nutrition March 01 There were no new randomized controlled trials since the 009 update and hence there are no changes to
. Nutritional Prescription of Enteral Nutrition: Achieving Target Dose of Enteral Nutrition March 01 There were no new randomized controlled trials since the 009 update and hence there are no changes to
5.5 Strategies to Optimize the Delivery of EN: Use of and Threshold for Gastric Residual Volumes May 2015
 5.5 Strategies to Optimize the Delivery of EN: Use of and Threshold for Gastric Residual Volumes May 2015 2015 Recommendation: Based on 3 level 2 studies, a gastric residual volume of either 250 or 500
5.5 Strategies to Optimize the Delivery of EN: Use of and Threshold for Gastric Residual Volumes May 2015 2015 Recommendation: Based on 3 level 2 studies, a gastric residual volume of either 250 or 500
5.3 Strategies to Optimize Delivery and Minimize Risks of EN: Small Bowel Feeding vs. Gastric May 2015
 5.3 Strategies to Optimize Delivery and Minimize Risks of EN: Small Bowel Feeding vs. Gastric May 2015 2015 Recommendation: Based on 16 level 2 studies, small bowel feeding compared to gastric feeding
5.3 Strategies to Optimize Delivery and Minimize Risks of EN: Small Bowel Feeding vs. Gastric May 2015 2015 Recommendation: Based on 16 level 2 studies, small bowel feeding compared to gastric feeding
5.3 Strategies to Optimize Delivery and Minimize Risks of EN: Small Bowel Feeding vs. Gastric February 2014
 5.3 Strategies to Optimize Delivery and Minimize Risks of EN: Small Bowel Feeding vs. Gastric February 2014 2013 Recommendation: Based on 15 level 2 studies, small bowel feeding compared to gastric feeding
5.3 Strategies to Optimize Delivery and Minimize Risks of EN: Small Bowel Feeding vs. Gastric February 2014 2013 Recommendation: Based on 15 level 2 studies, small bowel feeding compared to gastric feeding
Current concepts in Critical Care Nutrition
 Current concepts in Critical Care Nutrition Dr.N.Ramakrishnan AB (Int Med), AB (Crit Care), MMM, FACP, FCCP, FCCM Director, Critical Care Services Apollo Hospitals, Chennai Objectives Why? Enteral or Parenteral
Current concepts in Critical Care Nutrition Dr.N.Ramakrishnan AB (Int Med), AB (Crit Care), MMM, FACP, FCCP, FCCM Director, Critical Care Services Apollo Hospitals, Chennai Objectives Why? Enteral or Parenteral
Nutrition and Sepsis
 Nutrition and Sepsis Todd W. Rice, MD, MSc Associate Professor of Medicine Vanderbilt University 2017 DNS Symposium June 2, 2017 Case 55 y.o. male COPD, DM, HTN, presents with pneumonia and septic shock.
Nutrition and Sepsis Todd W. Rice, MD, MSc Associate Professor of Medicine Vanderbilt University 2017 DNS Symposium June 2, 2017 Case 55 y.o. male COPD, DM, HTN, presents with pneumonia and septic shock.
3.2 Nutritional Prescription of Enteral Nutrition: Enhanced Dose of Enteral Nutrition May 2015
 . Nutritional Prescription of Enteral Nutrition: Enhanced Dose of Enteral Nutrition May 015 015 Recommendation: Based on 1 level 1 study, level studies and cluster randomized controlled trials, when starting
. Nutritional Prescription of Enteral Nutrition: Enhanced Dose of Enteral Nutrition May 015 015 Recommendation: Based on 1 level 1 study, level studies and cluster randomized controlled trials, when starting
Feeding Protocols Enteral or Parenteral. AM Poleÿ 2012
 Practical aspects on Feeding Protocols Enteral or Parenteral AM Poleÿ 2012 Enteral Feeding Facts A reduction in mortality Prophylaxis for stress ulcers Full-strength Time to start enteral nutrition If
Practical aspects on Feeding Protocols Enteral or Parenteral AM Poleÿ 2012 Enteral Feeding Facts A reduction in mortality Prophylaxis for stress ulcers Full-strength Time to start enteral nutrition If
5.5 Strategies to Optimize the Delivery of EN: Use of and Threshold for Gastric Residual Volumes March 2013
 5.5 Strategies to Optimize the Delivery of EN: Use of and Threshold for Gastric Residual Volumes March 203 NEW SECTION in 203 Recommendation: There are insufficient data to make a recommendation for not
5.5 Strategies to Optimize the Delivery of EN: Use of and Threshold for Gastric Residual Volumes March 203 NEW SECTION in 203 Recommendation: There are insufficient data to make a recommendation for not
ESPEN Congress The Hague 2017
 ESPEN Congress The Hague 2017 Using the gut in acute care patients Permissive underfeeding in practice J.-C. Preiser (BE) PERMISSIVE UNDERFEEDING IN PRACTICE ESPEN congress Jean-Charles Preiser, M.D.,
ESPEN Congress The Hague 2017 Using the gut in acute care patients Permissive underfeeding in practice J.-C. Preiser (BE) PERMISSIVE UNDERFEEDING IN PRACTICE ESPEN congress Jean-Charles Preiser, M.D.,
Vanderbilt University Medical Center Trauma ICU Nutrition Management Guidelines
 Vanderbilt University Medical Center Trauma ICU Nutrition Management Guidelines Trauma Critical Care Nutrition Guidelines Clinical judgment may supersede guidelines as patient circumstances warrant ASSESSMENT
Vanderbilt University Medical Center Trauma ICU Nutrition Management Guidelines Trauma Critical Care Nutrition Guidelines Clinical judgment may supersede guidelines as patient circumstances warrant ASSESSMENT
SECTION 4: RECRUIT PARTICIPANTS
 SECTION 4: RECRUIT PARTICIPANTS Contents Participant Eligibility & Enrollment... 2 Screening... 2 Study ID Numbers... 2 Inclusion Criteria... 2 Exclusion Criteria... 4 Co-Enrollment... 5 Informed Consent
SECTION 4: RECRUIT PARTICIPANTS Contents Participant Eligibility & Enrollment... 2 Screening... 2 Study ID Numbers... 2 Inclusion Criteria... 2 Exclusion Criteria... 4 Co-Enrollment... 5 Informed Consent
Ernährungstherapie des Kritisch Kranken Enteral Parenteral Ganz egal?
 Ernährungstherapie des Kritisch Kranken Enteral Parenteral Ganz egal? PD Dr. med. Claudia Heidegger Service des Soins Intensifs Genf/Schweiz Dresden 11. Juni 2016 Nutrition News Nutrition controversy in
Ernährungstherapie des Kritisch Kranken Enteral Parenteral Ganz egal? PD Dr. med. Claudia Heidegger Service des Soins Intensifs Genf/Schweiz Dresden 11. Juni 2016 Nutrition News Nutrition controversy in
E S T A B L I S H I N G N U T R I T I O N I N Y O U R I C U The Need for a Protocol
 E S T A B L I S H I N G N U T R I T I O N I N Y O U R I C U The Need for a Protocol Arthur RH van Zanten, MD PhD Gelderse Vallei Hospital, Ede, The Netherlands Learning objectives Develop an evidence based
E S T A B L I S H I N G N U T R I T I O N I N Y O U R I C U The Need for a Protocol Arthur RH van Zanten, MD PhD Gelderse Vallei Hospital, Ede, The Netherlands Learning objectives Develop an evidence based
ICU NUTRITION UPDATE : ESPEN GUIDELINES Mirey Karavetian Assistant Professor Zayed University
 ICU NUTRITION UPDATE : ESPEN GUIDELINES 2018 Mirey Karavetian Assistant Professor Zayed University http://www.espen.org/files/espen- Guidelines/ESPEN_Guideline_on_clinical_nutrition_in_-ICU.pdf Medical
ICU NUTRITION UPDATE : ESPEN GUIDELINES 2018 Mirey Karavetian Assistant Professor Zayed University http://www.espen.org/files/espen- Guidelines/ESPEN_Guideline_on_clinical_nutrition_in_-ICU.pdf Medical
patients : review of advances in last five years Dr. Aditya Jindal
 Enteral nutrition in medical ICU patients : review of advances in last five years Dr. Aditya Jindal Our food should be our medicine and our medicine should be our food. Hippocrates Introduction ti Nutritional
Enteral nutrition in medical ICU patients : review of advances in last five years Dr. Aditya Jindal Our food should be our medicine and our medicine should be our food. Hippocrates Introduction ti Nutritional
5.1 Strategies to Optimize Delivery and Minimize Risks of EN: Feeding Protocols March 2013
 5.1 Strategies to Optimize Delivery and Minimize Risks of EN: Feeding Protocols March 2013 There were no new randomized controlled trials since the 2009 update and hence there are no changes to the following
5.1 Strategies to Optimize Delivery and Minimize Risks of EN: Feeding Protocols March 2013 There were no new randomized controlled trials since the 2009 update and hence there are no changes to the following
ENTERAL NUTRITION IN THE CRITICALLY ILL
 ENTERAL NUTRITION IN THE CRITICALLY ILL 1 Ebb phase Flow phase acute response (catabolic) adoptive response (anabolic) 2 3 Metabolic Response to Stress (catabolic phase) Glucose and Protein Metabolism
ENTERAL NUTRITION IN THE CRITICALLY ILL 1 Ebb phase Flow phase acute response (catabolic) adoptive response (anabolic) 2 3 Metabolic Response to Stress (catabolic phase) Glucose and Protein Metabolism
[No conflicts of interest]
![[No conflicts of interest]](/thumbs/86/94144068.jpg "[No conflicts of interest]") [No conflicts of interest] Patients and staff at: Available evidence pre-calories Three meta-analyses: Gramlich L et al. Does enteral nutrition compared to parenteral nutrition result in better outcomes
[No conflicts of interest] Patients and staff at: Available evidence pre-calories Three meta-analyses: Gramlich L et al. Does enteral nutrition compared to parenteral nutrition result in better outcomes
Int. Med J Vol. 6 No 1 June 2007 Enteral Nutrition In Intensive Care: Tiger Tube For Small Bowel Feeding In Acute Pancreatitis.
 Page 1 of 6 Int. Med J Vol. 6 No 1 June 2007 Enteral Nutrition In Intensive Care: Tiger Tube For Small Bowel Feeding In Acute Pancreatitis. Case Report Mohd Basri bin Mat Nor. Department of Anaesthesiology
Page 1 of 6 Int. Med J Vol. 6 No 1 June 2007 Enteral Nutrition In Intensive Care: Tiger Tube For Small Bowel Feeding In Acute Pancreatitis. Case Report Mohd Basri bin Mat Nor. Department of Anaesthesiology
Oklahoma Dietetic Association. Ainsley Malone, MS, RD, LD, CNSD April, 16, 2008 Permissive Underfeeding: What, Where and Why? Mt.
 The What, Why and When of Permissive Ainsley Malone, MS, RD, CNSD Nutrition Support Team Mt. Carmel West Hospital Mt. Carmel West 500 bed academic center Non-physician based NST Dietitian, pharmacist and
The What, Why and When of Permissive Ainsley Malone, MS, RD, CNSD Nutrition Support Team Mt. Carmel West Hospital Mt. Carmel West 500 bed academic center Non-physician based NST Dietitian, pharmacist and
Providing Optimal Nutritional Support on the ICU common problems and practical solutions. Pete Turner Specialist Nutritional Support Dietitian
 Providing Optimal Nutritional Support on the ICU common problems and practical solutions Pete Turner Specialist Nutritional Support Dietitian ICU Nutritional Support ACCEPT study showed improved ICU survival
Providing Optimal Nutritional Support on the ICU common problems and practical solutions Pete Turner Specialist Nutritional Support Dietitian ICU Nutritional Support ACCEPT study showed improved ICU survival
Guidelines for the Provision and Assessment of Nutrition Support Therapy in the Pediatric Critically Ill Patient: ASPEN-SCCM 2017
 Number of Patients Guidelines for the Provision and Assessment of Nutrition Support Therapy in the Pediatric Critically Ill Patient: ASPEN-SCCM 2017 Jorge A. Coss-Bu, MD Associate Professor of Pediatrics
Number of Patients Guidelines for the Provision and Assessment of Nutrition Support Therapy in the Pediatric Critically Ill Patient: ASPEN-SCCM 2017 Jorge A. Coss-Bu, MD Associate Professor of Pediatrics
Metabolic Control in Critical Care: Nutrition Therapy
 LOGO Metabolic Control in Critical Care: Nutrition Therapy ผศ.นพ.พรพจน เปรมโยธ น สาขาโภชนาการคล น ก ภาคว ชาอาย รศาสตร คณะแพทยศาสตร ศ ร ราชพยาบาล 2016 SCCM/ASPEN Guidelines Nutrition Therapy in the ICU
LOGO Metabolic Control in Critical Care: Nutrition Therapy ผศ.นพ.พรพจน เปรมโยธ น สาขาโภชนาการคล น ก ภาคว ชาอาย รศาสตร คณะแพทยศาสตร ศ ร ราชพยาบาล 2016 SCCM/ASPEN Guidelines Nutrition Therapy in the ICU
Feeding the septic patient How and when? Masterclass ICU nurses
 Feeding the septic patient How and when? Masterclass ICU nurses Case Male, 60 - No PMH - L 1.74 m and W 85 kg Pneumococcal pneumonia Stable hemodynamics - No AKI MV in prone position (PEEP 16 - FiO2 60%)
Feeding the septic patient How and when? Masterclass ICU nurses Case Male, 60 - No PMH - L 1.74 m and W 85 kg Pneumococcal pneumonia Stable hemodynamics - No AKI MV in prone position (PEEP 16 - FiO2 60%)
/03/ $03.00/0 Vol. 27, No. 5 JOURNAL OF PARENTERAL AND ENTERAL NUTRITION
 0148-6071/03/2705-0355$03.00/0 Vol. 27, No. 5 JOURNAL OF PARENTERAL AND ENTERAL NUTRITION Printed in U.S.A. Copyright 2003 by the American Society for Parenteral and Enteral Nutrition Special Interest
0148-6071/03/2705-0355$03.00/0 Vol. 27, No. 5 JOURNAL OF PARENTERAL AND ENTERAL NUTRITION Printed in U.S.A. Copyright 2003 by the American Society for Parenteral and Enteral Nutrition Special Interest
VOLUME-BASED VS. RATE-BASED FEEDING
 VOLUME-BASED VS. RATE-BASED FEEDING Amanda Holyk Critical Care Pharmacist Mount Nittany Medical Center Society of Critical Care Medicine Annual Symposium November 10, 2017 0 Disclosure I have no actual
VOLUME-BASED VS. RATE-BASED FEEDING Amanda Holyk Critical Care Pharmacist Mount Nittany Medical Center Society of Critical Care Medicine Annual Symposium November 10, 2017 0 Disclosure I have no actual
Evidence-Based. Management of Severe Sepsis. What is the BP Target?
 Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
10/3/2012. Pediatric Parenteral Nutrition A Comprehensive Review
 Critical Care Nutrition Foundation for Moving Forward Justine Turner MD PhD Department of Pediatric Gastroenterology and Nutrition University of Alberta I have the following financial relationships to
Critical Care Nutrition Foundation for Moving Forward Justine Turner MD PhD Department of Pediatric Gastroenterology and Nutrition University of Alberta I have the following financial relationships to
THE AUTHOR OF THIS WHAT S NEW IN NUTRITION? OBJECTIVES & OUTLINE EVIDENCE-BASED MEDICINE: PARENTERAL NUTRITION (PN)
") WHAT S NEW IN NUTRITION? Alisha Mutch, Pharm.D., BCPS THE AUTHOR OF THIS PRESENTATION HAS NOTHING TO DISCLOSE. OBJECTIVES & OUTLINE MALNUTRITION OBJECTIVES Indicate when parenteral nutrition (PN) is warranted
WHAT S NEW IN NUTRITION? Alisha Mutch, Pharm.D., BCPS THE AUTHOR OF THIS PRESENTATION HAS NOTHING TO DISCLOSE. OBJECTIVES & OUTLINE MALNUTRITION OBJECTIVES Indicate when parenteral nutrition (PN) is warranted
Nutrition Support in Critically Ill Cardiothoracic Patients
 Nutrition Support in Critically Ill Cardiothoracic Patients อ.นพ.พรพจน เปรมโยธ น สาชาโภชนาการคล น ก ภาคว ชาอาย รศาสตร คณะแพทยศาสตร ศ ร ราชพยาบาล Outline Malnutrition in cardiothoracic patients Nutritional
Nutrition Support in Critically Ill Cardiothoracic Patients อ.นพ.พรพจน เปรมโยธ น สาชาโภชนาการคล น ก ภาคว ชาอาย รศาสตร คณะแพทยศาสตร ศ ร ราชพยาบาล Outline Malnutrition in cardiothoracic patients Nutritional
Stressed Out: Evaluating the Need for Stress Ulcer Prophylaxis in the ICU
 Stressed Out: Evaluating the Need for Stress Ulcer Prophylaxis in the ICU Josh Arnold, PharmD PGY1 Pharmacy Resident Pharmacy Grand Rounds November 8, 2016 2016 MFMER slide-1 Objectives Identify the significance
Stressed Out: Evaluating the Need for Stress Ulcer Prophylaxis in the ICU Josh Arnold, PharmD PGY1 Pharmacy Resident Pharmacy Grand Rounds November 8, 2016 2016 MFMER slide-1 Objectives Identify the significance
WHEN To Initiate Parenteral Nutrition A Frequent Question With New Answers
 WHEN To Initiate Parenteral Nutrition A Frequent Question With New Answers Ainsley Malone, MS, RD, LD, CNSC, FAND, FASPEN Dubai International Nutrition Conference 2018 Disclosures No commercial relationship
WHEN To Initiate Parenteral Nutrition A Frequent Question With New Answers Ainsley Malone, MS, RD, LD, CNSC, FAND, FASPEN Dubai International Nutrition Conference 2018 Disclosures No commercial relationship
Enteral Nutrition in the Critically Ill Child: Challenges and Current Guidelines
 Enteral Nutrition in the Critically Ill Child: Challenges and Current Guidelines 1 Presented on January 24, 2017 Jorge A. Coss-Bu, MD Associate Professor of Pediatrics Section of Critical Care Baylor College
Enteral Nutrition in the Critically Ill Child: Challenges and Current Guidelines 1 Presented on January 24, 2017 Jorge A. Coss-Bu, MD Associate Professor of Pediatrics Section of Critical Care Baylor College
When to start SPN in critically ill patients? Refereeravond IC
 When to start SPN in critically ill patients? Refereeravond IC Introduction (1) Protein/calorie malnutrition is very frequent in critically ill patients Protein/calorie malnutrition is associated with
When to start SPN in critically ill patients? Refereeravond IC Introduction (1) Protein/calorie malnutrition is very frequent in critically ill patients Protein/calorie malnutrition is associated with
Disclosures. None. Enteral Nutrition and Vasoactive Therapy! But actually.. Stocks Advisory boards Grants Speakers Bureau. Paul Marik, MD,FCCM,FCCP
 Enteral Nutrition and Vasoactive Therapy! Paul Marik, MD,FCCM,FCCP Disclosures Stocks Advisory boards Grants Speakers Bureau None But actually.. 1 We suggest a determination of nutrition risk (NUTRIC score)
Enteral Nutrition and Vasoactive Therapy! Paul Marik, MD,FCCM,FCCP Disclosures Stocks Advisory boards Grants Speakers Bureau None But actually.. 1 We suggest a determination of nutrition risk (NUTRIC score)
Nutrition. ICU Fellowship Training Radboudumc
 Nutrition ICU Fellowship Training Radboudumc Critical Care MCQ s Nasogastric (NG) and nasojejunal (NJ) feeding tubes: A. Enteral nutrition is associated with a reduced risk of bacterial and toxin translocation.
Nutrition ICU Fellowship Training Radboudumc Critical Care MCQ s Nasogastric (NG) and nasojejunal (NJ) feeding tubes: A. Enteral nutrition is associated with a reduced risk of bacterial and toxin translocation.
SEPSIS: IT ALL BEGINS WITH INFECTION. Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft.
 SEPSIS: IT ALL BEGINS WITH INFECTION Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft. Worth 1 2 3 OBJECTIVES Review the new Sepsis 3 definitions of sepsis
SEPSIS: IT ALL BEGINS WITH INFECTION Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft. Worth 1 2 3 OBJECTIVES Review the new Sepsis 3 definitions of sepsis
Benchmarking your ICU s feeding performance: How early is early?
 Benchmarking your ICU s feeding performance: How early is early? Dr Gordon S. Doig, Associate Professor in Intensive Care, Northern Clinical School Intensive Care Research Unit, University of Sydney, Sydney,
Benchmarking your ICU s feeding performance: How early is early? Dr Gordon S. Doig, Associate Professor in Intensive Care, Northern Clinical School Intensive Care Research Unit, University of Sydney, Sydney,
A R T H U R R. H. V A N Z A N T E N, MD PHD I N T E R N I S T - I N T E N S I V I S T H O S P I T A L MEDICAL DIRECTOR G E L D E R S E V A L L E I
 FEEDING THE OBESE CRITICALLY ILL PATIENT A R T H U R R. H. V A N Z A N T E N, MD PHD I N T E R N I S T - I N T E N S I V I S T H O S P I T A L MEDICAL DIRECTOR G E L D E R S E V A L L E I HOSPITAL, EDE,
FEEDING THE OBESE CRITICALLY ILL PATIENT A R T H U R R. H. V A N Z A N T E N, MD PHD I N T E R N I S T - I N T E N S I V I S T H O S P I T A L MEDICAL DIRECTOR G E L D E R S E V A L L E I HOSPITAL, EDE,
Small Bowel Obstruction after operation in a severely malnourished man. By: Ms Bounmark Phoumesy
 Small Bowel Obstruction after operation in a severely malnourished man By: Ms Bounmark Phoumesy Normal length of GI tract Normal length(achieved by age 9) Small bowel 600cm (Men: 630 cm; Women: 592 cm)
Small Bowel Obstruction after operation in a severely malnourished man By: Ms Bounmark Phoumesy Normal length of GI tract Normal length(achieved by age 9) Small bowel 600cm (Men: 630 cm; Women: 592 cm)
Issues in Enteral Feeding: Aspiration
 Issues in Enteral Feeding: Aspiration A webinar for HealthTrust Members February 11, 2019 Co-sponsored by HealthTrust and V NOS Continuing Education Provider Presented by: Kathleen Stoessel, RN, BSN, MS
Issues in Enteral Feeding: Aspiration A webinar for HealthTrust Members February 11, 2019 Co-sponsored by HealthTrust and V NOS Continuing Education Provider Presented by: Kathleen Stoessel, RN, BSN, MS
SASPEN: Meet the Expert. Pr. Me'e M Berger Service of Intensive Care & Burns CHUV Lausanne Switzerland
 SASPEN: Meet the Expert Pr. Me'e M Berger Service of Intensive Care & Burns CHUV Lausanne Switzerland 40 Ensuring my patients are properly fed. Nutrition therapy must be planned as any other ICU therapy
SASPEN: Meet the Expert Pr. Me'e M Berger Service of Intensive Care & Burns CHUV Lausanne Switzerland 40 Ensuring my patients are properly fed. Nutrition therapy must be planned as any other ICU therapy
Nutrition therapy in the critical care setting: What is best achievable practice? An international multicenter observational study*
 Continuing Medical Education Article Nutrition therapy in the critical care setting: What is best achievable practice? An international multicenter observational study* Naomi E. Cahill, RD, MSc; Rupinder
Continuing Medical Education Article Nutrition therapy in the critical care setting: What is best achievable practice? An international multicenter observational study* Naomi E. Cahill, RD, MSc; Rupinder
Disclosures. Objectives. Procalcitonin: Pearls and Pitfalls in Daily Practice
 Procalcitonin: Pearls and Pitfalls in Daily Practice Sarah K Harrison, PharmD, BCCCP Clinical Pearl Disclosures The author of this presentation has no disclosures concerning possible financial or personal
Procalcitonin: Pearls and Pitfalls in Daily Practice Sarah K Harrison, PharmD, BCCCP Clinical Pearl Disclosures The author of this presentation has no disclosures concerning possible financial or personal
Nutrition in critical illness:
 Nutrition in critical illness: from theory to daily practice Aim of the presentation Summarize the guidelines for the provision and assessment of nutrition support therapy in the adult critically ill patient.
Nutrition in critical illness: from theory to daily practice Aim of the presentation Summarize the guidelines for the provision and assessment of nutrition support therapy in the adult critically ill patient.
Kombinierte enterale und parenterale Ernährung für welche PatientInnen?
 2014 Kombinierte enterale und parenterale Ernährung für welche PatientInnen? Dr. CP. Heidegger Intensive Care/Geneva claudia-paula.heidegger@hcuge.ch Bern Freitag, 4. April 2014 Nutrition News Worldwide
2014 Kombinierte enterale und parenterale Ernährung für welche PatientInnen? Dr. CP. Heidegger Intensive Care/Geneva claudia-paula.heidegger@hcuge.ch Bern Freitag, 4. April 2014 Nutrition News Worldwide
NUTRITION. Elizabeth Viner Smith & Catherine Jones Foundations of Critical Care Nursing September 2017
 NUTRITION Elizabeth Viner Smith & Catherine Jones Foundations of Critical Care Nursing September 2017 Step One Competency 1.19 Factors contributing to nutritional impairment in critical illness. Nutritional
NUTRITION Elizabeth Viner Smith & Catherine Jones Foundations of Critical Care Nursing September 2017 Step One Competency 1.19 Factors contributing to nutritional impairment in critical illness. Nutritional
Minimal Enteral Nutrition
 Abstract Minimal Enteral Nutrition Although parenteral nutrition has been used widely in the management of sick very low birth weight infants, a smooth transition to the enteral route is most desirable.
Abstract Minimal Enteral Nutrition Although parenteral nutrition has been used widely in the management of sick very low birth weight infants, a smooth transition to the enteral route is most desirable.
Enteral Nutrition: Whom, Why, When, What and Where to Feed?
 Meier RF, Reddy BR, Soeters PB (eds): The Importance of Nutrition as an Integral Part of Disease Management. Nestlé Nutr Inst Workshop Ser, vol 82, pp 53 59, (DOI: 10.1159/000382002) Nestec Ltd., Vevey/S.
Meier RF, Reddy BR, Soeters PB (eds): The Importance of Nutrition as an Integral Part of Disease Management. Nestlé Nutr Inst Workshop Ser, vol 82, pp 53 59, (DOI: 10.1159/000382002) Nestec Ltd., Vevey/S.
Scott A. Lynch, MD, MPH,FAAFP Assistant Professor
 Scott A. Lynch, MD, MPH,FAAFP Assistant Professor Lynch.Scott@mayo.edu 2015 MFMER 3543652-1 Nutrition in the Hospital Mayo School of Continuous Professional Development 2nd Annual Inpatient Medicine for
Scott A. Lynch, MD, MPH,FAAFP Assistant Professor Lynch.Scott@mayo.edu 2015 MFMER 3543652-1 Nutrition in the Hospital Mayo School of Continuous Professional Development 2nd Annual Inpatient Medicine for
Amanda Hernandez FND October 17, 2011 Enteral Feeding Case Study
 Amanda Hernandez FND 430-001 October 17, 2011 Enteral Feeding Case Study 1. Nutritional Assessment to determine energy and protein needs Percent Usual Body Weight [(current body weight/usual body weight)
Amanda Hernandez FND 430-001 October 17, 2011 Enteral Feeding Case Study 1. Nutritional Assessment to determine energy and protein needs Percent Usual Body Weight [(current body weight/usual body weight)
ICU Acquired Weakness: Role of Specific Nutrients
 ICU Acquired Weakness: Role of Specific Nutrients Dr Jonathan TAN Senior Consultant Dept of Anaesthesiology, Intensive Care & Pain Medicine Tan Tock Seng Hospital, Singapore Purpose? Healthcare professionals?
ICU Acquired Weakness: Role of Specific Nutrients Dr Jonathan TAN Senior Consultant Dept of Anaesthesiology, Intensive Care & Pain Medicine Tan Tock Seng Hospital, Singapore Purpose? Healthcare professionals?
Timing of Parenteral Nutrition
 Timing of Parenteral Nutrition Arun Bansal; MD, FCCM, MRCPCH Professor Pediatric Critical Care PGIMER, Chandigarh, INDIA drarunbansal@gmail.com Malnutrition in Critically Ill Incidence: from 19 32% Associated
Timing of Parenteral Nutrition Arun Bansal; MD, FCCM, MRCPCH Professor Pediatric Critical Care PGIMER, Chandigarh, INDIA drarunbansal@gmail.com Malnutrition in Critically Ill Incidence: from 19 32% Associated
What is the Role of Albumin in Sepsis? An Evidenced Based Affair. Justin Belsky MD PGY3 2/6/14
 What is the Role of Albumin in Sepsis? An Evidenced Based Affair Justin Belsky MD PGY3 2/6/14 Microcirculation https://www.youtube.com/watch?v=xao1gsyur7q Capillary Leak in Sepsis Asking the RIGHT Question
What is the Role of Albumin in Sepsis? An Evidenced Based Affair Justin Belsky MD PGY3 2/6/14 Microcirculation https://www.youtube.com/watch?v=xao1gsyur7q Capillary Leak in Sepsis Asking the RIGHT Question
What s New in Parenteral Nutrition?
 1 What s New in Parenteral Nutrition? พ นโทหญ ง ส รกานต เตชะวณ ช MD, MSc, ABPNS ห วหน าหน วยโภชนศาสตร คล น ก กองอาย รกรรม โรงพยาบาลพระมงก ฎเกล า 7 กรกฎาคม พ.ศ. 2559 What s New in Parenteral Nutrition?
1 What s New in Parenteral Nutrition? พ นโทหญ ง ส รกานต เตชะวณ ช MD, MSc, ABPNS ห วหน าหน วยโภชนศาสตร คล น ก กองอาย รกรรม โรงพยาบาลพระมงก ฎเกล า 7 กรกฎาคม พ.ศ. 2559 What s New in Parenteral Nutrition?
A number of observational studies of adult
 Carol Rees Parrish, M.S., R.D., Series Editor Full Force Enteral Nutrition: A New Hope, or the Dark Side? A Critical Look at Enhanced Enteral Feeding Protocols Joe Krenitsky Enteral nutrition (EN) is the
Carol Rees Parrish, M.S., R.D., Series Editor Full Force Enteral Nutrition: A New Hope, or the Dark Side? A Critical Look at Enhanced Enteral Feeding Protocols Joe Krenitsky Enteral nutrition (EN) is the
14-15 Aug ASMIC L.Mageswary Dietitian Hospital Selayang
 14-15 Aug ASMIC 2015 Nurses Role L.Mageswary Dietitian Hospital Selayang Doctor Dietitian Pharmacist Nurse Physiotherapist Occupational therapist Patient Patient Centered Care Patients needs & preferences
14-15 Aug ASMIC 2015 Nurses Role L.Mageswary Dietitian Hospital Selayang Doctor Dietitian Pharmacist Nurse Physiotherapist Occupational therapist Patient Patient Centered Care Patients needs & preferences
Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill
 Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill Joe Palumbo PGY-2 Critical Care Pharmacy Resident Buffalo General Medical Center Disclosures
Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill Joe Palumbo PGY-2 Critical Care Pharmacy Resident Buffalo General Medical Center Disclosures
ICU ENTERAL FEEDING GUIDELINES
 DISCLAIMER: These guidelines are intended to serve as a general statement regarding appropriate patient care practices based upon the available medical literature and clinical expertise at the time of
DISCLAIMER: These guidelines are intended to serve as a general statement regarding appropriate patient care practices based upon the available medical literature and clinical expertise at the time of
Nutrition in Acute Kidney Injury Enrico Fiaccadori
 Nutrition in Acute Kidney Injury Enrico Fiaccadori Nephrology Dept. Parma University Medical School Parma, Italy Diagnosis, epidemiology and prognostic impact of proteinenergy wasting (PEW) in AKI Pathogenetic
Nutrition in Acute Kidney Injury Enrico Fiaccadori Nephrology Dept. Parma University Medical School Parma, Italy Diagnosis, epidemiology and prognostic impact of proteinenergy wasting (PEW) in AKI Pathogenetic
OPTICS OPTimal nutrition by Informing and Capacitating family members of best nutrition practices OPTICS
 OPTICS OPTimal nutrition by Informing and Capacitating family members of best nutrition practices Educational Booklet for Families Version April 26 th 2016 Page 1 of 12 This information booklet was originally
OPTICS OPTimal nutrition by Informing and Capacitating family members of best nutrition practices Educational Booklet for Families Version April 26 th 2016 Page 1 of 12 This information booklet was originally
Investigational Product Procedures Manual
 A Randomized Trial of Supplemental Parenteral Nutrition in Under and Over Weight Critically Ill Patients: The TOP UP Trial Investigational Product Procedures Manual Intended Audience: Research Cooridnators/Pharmacists
A Randomized Trial of Supplemental Parenteral Nutrition in Under and Over Weight Critically Ill Patients: The TOP UP Trial Investigational Product Procedures Manual Intended Audience: Research Cooridnators/Pharmacists
Nutrition care plan for surgical patients. Objectives
 Slide 1 Nutrition care plan for surgical patients Surgical Nutrition Training Module Level 1 Philippine Society of General Surgeons Committee on Surgical Training In this session we will discuss the most
Slide 1 Nutrition care plan for surgical patients Surgical Nutrition Training Module Level 1 Philippine Society of General Surgeons Committee on Surgical Training In this session we will discuss the most
ASPEN Safe Practices for Enteral Nutrition Therapy
 ASPEN Safe Practices for Enteral Nutrition Therapy Ainsley Malone, MS, RDN, CNSC, FAND, FASPEN Nutrition Support Dietitian Mt. Carmel West Hospital ASPEN Clinical Practice Specialist Disclosure I have
ASPEN Safe Practices for Enteral Nutrition Therapy Ainsley Malone, MS, RDN, CNSC, FAND, FASPEN Nutrition Support Dietitian Mt. Carmel West Hospital ASPEN Clinical Practice Specialist Disclosure I have
Declaration. BBraun, Nutricia, Nestle, Adcock Ingram and other healthcare industry stakeholders
 Declaration Independent scientific and training consultant in critical care nutrition I do not claim to represent the views of any particular institution I do not claim to endorse or promote any particular
Declaration Independent scientific and training consultant in critical care nutrition I do not claim to represent the views of any particular institution I do not claim to endorse or promote any particular
Gastrointestinal Feedings Post Op: What s the deal on beginning oral feedings?
 Gastrointestinal Feedings Post Op: What s the deal on beginning oral feedings? Kate Willcutts, DCN, RD, CNSC University of Virginia Health System Charlottesville, VA kfw3w@virginia.edu Objectives 1. Discuss
Gastrointestinal Feedings Post Op: What s the deal on beginning oral feedings? Kate Willcutts, DCN, RD, CNSC University of Virginia Health System Charlottesville, VA kfw3w@virginia.edu Objectives 1. Discuss
8.0 Parenteral Nutrition vs. Standard care May 2015
 8.0 Parenteral Nutrition vs. Standard care May 015 015 Recommendation: Based on 6 level studies, in critically ill patients with an intact gastrointestinal tract, we recommend that parenteral nutrition
8.0 Parenteral Nutrition vs. Standard care May 015 015 Recommendation: Based on 6 level studies, in critically ill patients with an intact gastrointestinal tract, we recommend that parenteral nutrition
4/15/2014. Nurses Take the Lead to Improve Overall Infant Growth. Improving early nutrition. Problem Identification
 Nurses Take the Lead to Improve Overall Infant Growth Cathy Lee Leon, RN, BSN, MBA, NE-BC California Pacific Medical Center-San Francisco Improving early nutrition Standardized feeding protocol Problem
Nurses Take the Lead to Improve Overall Infant Growth Cathy Lee Leon, RN, BSN, MBA, NE-BC California Pacific Medical Center-San Francisco Improving early nutrition Standardized feeding protocol Problem
Parenteral and Enteral Nutrition
 Parenteral and Enteral Nutrition Audis Bethea, Pharm.D. Assistant Professor Therapeutics I December 5 & 9, 2003 Parenteral Nutrition Definition process of supplying nutrients via the intravenous route
Parenteral and Enteral Nutrition Audis Bethea, Pharm.D. Assistant Professor Therapeutics I December 5 & 9, 2003 Parenteral Nutrition Definition process of supplying nutrients via the intravenous route
Nutrition Support. John Cha Department of Surgery DHMC/UCHSC
 Nutrition Support John Cha Department of Surgery DHMC/UCHSC Overview Why? When? How much? What route? Fancy stuff: enhanced nutrition Advantages of Nutrition Decreased catabolism Improved wound healing
Nutrition Support John Cha Department of Surgery DHMC/UCHSC Overview Why? When? How much? What route? Fancy stuff: enhanced nutrition Advantages of Nutrition Decreased catabolism Improved wound healing
Case Discussion. Nutrition in IBD. Rémy Meier MD. Ulcerative colitis. Crohn s disease
 26.08.2017 Case Discussion Nutrition in IBD Crohn s disease Ulcerative colitis Rémy Meier MD Case Presentation 30 years old female, with diarrhea for 3 months Shool frequency 3-4 loose stools/day with
26.08.2017 Case Discussion Nutrition in IBD Crohn s disease Ulcerative colitis Rémy Meier MD Case Presentation 30 years old female, with diarrhea for 3 months Shool frequency 3-4 loose stools/day with
By; Ashraf El Houfi MD MS (pulmonology) MRCP (UK) FRCP (London) EDIC Consultant ICU Dubai Hospital
 MRCP (UK) FRCP (London) EDIC Consultant ICU Dubai Hospital") By; Ashraf El Houfi MD MS (pulmonology) MRCP (UK) FRCP (London) EDIC Consultant ICU Dubai Hospital Introduction The significance of nutrition in hospital setting (especially the ICU) cannot be overstated.
By; Ashraf El Houfi MD MS (pulmonology) MRCP (UK) FRCP (London) EDIC Consultant ICU Dubai Hospital Introduction The significance of nutrition in hospital setting (especially the ICU) cannot be overstated.
A review on enteral nutrition guidelines for traumatic brain injury
 A review on enteral nutrition guidelines for traumatic brain injury According to the Centers for Disease Control and Prevention, at least 1.7 million people suffer from traumatic brain injury (TBI) every
A review on enteral nutrition guidelines for traumatic brain injury According to the Centers for Disease Control and Prevention, at least 1.7 million people suffer from traumatic brain injury (TBI) every
Contraindications to time critical surgery; when not to proceed from the perspective of: The Physician A/Prof Peter Morley
 Contraindications to time critical surgery; when not to proceed from the perspective of: The Physician A/Prof Peter Morley British Journal of Surgery 2013; 100: 1045 1049 The risk of 30 day mortality
Contraindications to time critical surgery; when not to proceed from the perspective of: The Physician A/Prof Peter Morley British Journal of Surgery 2013; 100: 1045 1049 The risk of 30 day mortality
Presented by: Indah Dwi Pratiwi
 Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
Update in Critical Care Medicine
 Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
Pharmaconutrition in PICU. Gan Chin Seng Paediatric Intensivist UMMC
 Pharmaconutrition in PICU Gan Chin Seng Paediatric Intensivist UMMC Pharmaconutrition in Critical Care Unit Gan Chin Seng Paediatric Intensivist UMMC Definition New concept Treatment with specific nutrients
Pharmaconutrition in PICU Gan Chin Seng Paediatric Intensivist UMMC Pharmaconutrition in Critical Care Unit Gan Chin Seng Paediatric Intensivist UMMC Definition New concept Treatment with specific nutrients
Nutrition Management of the Critically Ill Pediatric Patient: Facilitating the Transition to Enteral Nutrition
 Nutrition Management of the Critically Ill Pediatric Patient: Facilitating the Transition to Enteral Nutrition Ana Abad-Jorge, EdD, MS, RDN, CNSC Program Director, Bachelor of Professional Studies in Health
Nutrition Management of the Critically Ill Pediatric Patient: Facilitating the Transition to Enteral Nutrition Ana Abad-Jorge, EdD, MS, RDN, CNSC Program Director, Bachelor of Professional Studies in Health
CLINICAL OUTCOMES OF INADEQUATE CALORIE DELIVERY AND PROTEIN DEFICIT IN SURGICAL INTENSIVE CARE PATIENTS. Nutrition in Critical Care
 Nutrition in Critical Care CLINICAL OUTCOMES OF INADEQUATE CALORIE DELIVERY AND PROTEIN DEFICIT IN SURGICAL INTENSIVE CARE PATIENTS By D. Dante Yeh, MD, Miroslav P. Peev, MD, Sadeq A. Quraishi, MD, MHA,
Nutrition in Critical Care CLINICAL OUTCOMES OF INADEQUATE CALORIE DELIVERY AND PROTEIN DEFICIT IN SURGICAL INTENSIVE CARE PATIENTS By D. Dante Yeh, MD, Miroslav P. Peev, MD, Sadeq A. Quraishi, MD, MHA,
Initial efficacy and tolerability of early enteral nutrition with immediate or gradual introduction in intubated patients
 Intensive Care Med (2008) 34:1054 1059 DOI 10.1007/s00134-007-0983-6 ORIGINAL Arnaud Desachy Marc Clavel Albert Vuagnat Sandrine Normand Valérie Gissot Bruno François Initial efficacy and tolerability
Intensive Care Med (2008) 34:1054 1059 DOI 10.1007/s00134-007-0983-6 ORIGINAL Arnaud Desachy Marc Clavel Albert Vuagnat Sandrine Normand Valérie Gissot Bruno François Initial efficacy and tolerability
Clinical Research. Keywords enteral nutrition; clinical protocols; critical illness; trauma; nutritional support; critical care
 539705NCPXXX10.1177/0884533614539705Nutrition in Clinical PracticeTaylor et al research-article2014 Clinical Research Improving Enteral Delivery Through the Adoption of the Feed Early Enteral Diet Adequately
539705NCPXXX10.1177/0884533614539705Nutrition in Clinical PracticeTaylor et al research-article2014 Clinical Research Improving Enteral Delivery Through the Adoption of the Feed Early Enteral Diet Adequately
to Implement Critical Care Nutrition Guidelines
 Make it Happen! Breaking Through Barriers to Implement Critical Care Nutrition Guidelines Sponsor Disclosure: Financial support for this presentation was provided by Nestlé HealthCare Nutrition, Inc. The
Make it Happen! Breaking Through Barriers to Implement Critical Care Nutrition Guidelines Sponsor Disclosure: Financial support for this presentation was provided by Nestlé HealthCare Nutrition, Inc. The
No conflicts of interest to disclose
 No conflicts of interest to disclose Introduction Epidemiology Surviving sepsis guidelines 2012 Updates Resuscitation protocols Map Goals Transfusion Sepsis-3 Bundle Management Questions Sepsis is a systemic,
No conflicts of interest to disclose Introduction Epidemiology Surviving sepsis guidelines 2012 Updates Resuscitation protocols Map Goals Transfusion Sepsis-3 Bundle Management Questions Sepsis is a systemic,
Protein in Critically Ill Patients. Ashraf El Houfi. MD MS(pulmonology) MRCP(UK) FRCP(London) EDIC Consultant ICU Dubai Hospital
 MRCP(UK) FRCP(London) EDIC Consultant ICU Dubai Hospital") Protein in Critically Ill Patients Ashraf El Houfi. MD MS(pulmonology) MRCP(UK) FRCP(London) EDIC Consultant ICU Dubai Hospital Proteins Proteins Protein is needed to Build, Maintain, and Repair body tissue
Protein in Critically Ill Patients Ashraf El Houfi. MD MS(pulmonology) MRCP(UK) FRCP(London) EDIC Consultant ICU Dubai Hospital Proteins Proteins Protein is needed to Build, Maintain, and Repair body tissue
Nutrition Services at a glance
 Nutrition Services at a glance Ragini Raghuveer, MS, RD, LD/N Systems Clinical Nutrition Manager Linette De Armas, RD, LD/N Clinical Dietitian Melissa Lorenzo, RD, LD/N Clinical Dietitian 1 Learning Objectives
Nutrition Services at a glance Ragini Raghuveer, MS, RD, LD/N Systems Clinical Nutrition Manager Linette De Armas, RD, LD/N Clinical Dietitian Melissa Lorenzo, RD, LD/N Clinical Dietitian 1 Learning Objectives
Why You Switched to the Tiger 2 Self-Advancing Nasal Jejunal Feeding Tube
 Why You Switched to the Tiger 2 Self-Advancing Nasal Jejunal Feeding Tube Ease of Use Self-advancing technology minimises hands-on time for clinicians. Requires no additional devices or costly capital
Why You Switched to the Tiger 2 Self-Advancing Nasal Jejunal Feeding Tube Ease of Use Self-advancing technology minimises hands-on time for clinicians. Requires no additional devices or costly capital
Tailored Volume Resuscitation in the Critically Ill is Achievable. Objectives. Clinical Case 2/16/2018
 Tailored Volume Resuscitation in the Critically Ill is Achievable Heath E Latham, MD Associate Professor Fellowship Program Director Pulmonary and Critical Care Objectives Describe the goal of resuscitation
Tailored Volume Resuscitation in the Critically Ill is Achievable Heath E Latham, MD Associate Professor Fellowship Program Director Pulmonary and Critical Care Objectives Describe the goal of resuscitation
Nutritional Support. Critical Care Nutrition: A Key to Good Outcomes
 Critical Care Nutrition: A Key to Good Outcomes Lisa M. Freeman, DVM, PhD, DACVN Nutritional Support Why is it important? Who needs it? When should it be initiated? How should it be given? How much should
Critical Care Nutrition: A Key to Good Outcomes Lisa M. Freeman, DVM, PhD, DACVN Nutritional Support Why is it important? Who needs it? When should it be initiated? How should it be given? How much should
Are Patients Hypoperfused in the ED? Rapid Perfusion Assessment in the Emergency Department
 Are Patients Hypoperfused in the ED? Rapid Perfusion Assessment in the Emergency Department R. Benjamin Saldaña DO, FACEP Associate Medical Director Methodist Emergency Care Center, Houston TX Disclosure
Are Patients Hypoperfused in the ED? Rapid Perfusion Assessment in the Emergency Department R. Benjamin Saldaña DO, FACEP Associate Medical Director Methodist Emergency Care Center, Houston TX Disclosure