Chapter 1 Introduction
|
|
|
- Alannah Lane
- 5 years ago
- Views:
Transcription
1 Chapter 1 Introduction Increasing life expectancy and higher patient expectations have led to a large increase in the number of patients presenting to doctors with musculoskeletal complaints. The World Health Organisation state that musculoskeletal and rheumatic diseases are major causes of morbidity throughout the world, having a substantial influence on health and quality of life, and inflicting an enormous burden of cost on health systems. Examples of this worldwide burden include: 1. 40% of people over the age of 70 years suffer from osteoarthritis of the knee % of patients with osteoarthritis have some degree of limitation of movement, and 25% cannot perform their major daily activities of life. 3. Rheumatoid arthritis, within a decade of its onset, leads to work disability defined as a total cessation of employment for between 51% and 59% of patients. 4. Low back pain has reached epidemic proportions, being reported by about 80% of people at some time in their lives. To enable us to correctly treat this increasing volume of patients, knowledge of common orthopaedic and rheumatologic complaints is vital for all student doctors. In this book, we have attempted to cover the major musculoskeletal diseases, describing clinical presentation, investigation and treatments. It is aimed at not only providing adequate knowledge for the final undergraduate exams but also for junior doctors at work. Extensive yet simple illustrations should aid the student in gaining an understanding of these problems. Enhanced versions of this blinkbook include videos of examination techniques and sample, interactive exam questions. Chapter 2 Trauma basics Fracture description and classification A fracture is defined as a break in the continuity of a bone with an associated soft tissue injury. Fractures are caused by the application of a force, which exceeds the strength of the bone. A direct force or blow applied to a bone will often result in a transverse fracture at the site of application. A twisting or torsional force applied often results in a spiral or oblique fracture at some
2 distance from the site of application. A force of high energy often results in multiple fracture fragments and is referred to as a comminuted (or multifragmentary) fracture. Bones may become weaker if they are infiltrated by tumours (primary or secondary) or in metabolic disorders, such as osteoporosis, that lead to decreased bone mineral density. If a fracture occurs through this region of diseased bone, it often requires much lower force, and is referred to as a pathological fracture. Some fractures occur due to repeated excessive stress application to a bone. This for example occurs in the second metatarsal shaft when an active patient has changed their training regimen and is referred to as a stress fracture. A sudden forceful contraction of a muscle may pull off the tendon's bony attachment rather than rupturing the tendon. This is referred to as an avulsion fracture. Avulsion fractures may also be a result of traction upon a ligament or joint capsule attachment. A fracture without disruption of the overlying skin is a closed fracture. When the skin and soft tissues overlying a fracture are broken, this is referred to as an open fracture. The skin may be broken from within by the sharp bone fragments (within to out) or by direct trauma to the skin (without to in). Fractures are further described by: X-ray appearance: Transverse - fracture line runs roughly perpendicular to long axis of the bone (if aligned, may be stable) Oblique - fracture line runs at an angle from the long axis of the bone (potentially unstable) Spiral - fracture line is spiral in shape (potentially unstable) Comminuted/multifragmentary - more than 2 fragments; greater force applied will result in more fracture fragments (unstable) Impacted - bone fragments are driven into each other (potentially stable)
3 Position in the bone: Thirds - bone is divided into proximal, middle and distal third (common descriptive terms) Anatomical - bone is divided into epiphyseal, metaphyseal and diaphyseal sections (less common) Displacement: NB: the position of the distal fragment is always described in relation to the proximal fragment. Translation - bone fragments have shifted relative to each other ie. lateral, medial, anterior or posterior Tilt - describes angular deviation of the distal fracture fragment ie. dorsal, volar (palmar in the hand and plantar in the foot), valgus or varus Rotation - bone fragments that are rotated with respect to each other. Can be difficult to recognise with plain radiographs Fracture healing Bone healing is a proliferative physiological response. Acceptable healing requires reduction of the fracture, adequate stabilisation in this position and time for healing. A common saying is "Reduce, Fix, Wait, Rehabilitate". Fracture healing occurs in phases, the length of which varies with severity of injury. Periosteum (the connective tissue membrane covering bone) is vital for healing, supplying precursor cells and nutrient supply. Stripping of the periosteum in a severe comminuted fracture or during surgery may lead to the fracture not healing (non-union).

4 The process of healing occurs in 4 stages: 1. Haemorrhage and haematoma formation - bleeding into the fracture site leads to haematoma formation. Infiltration of phagocytes removes dead or damaged cells. Fibroblasts survive in the damaged area to form vascular granulation tissue. 2. Soft callus formation - periosteal cells at the fracture gap and fibroblasts in the granulation tissue develop into chondroblasts and produce hyaline cartilage. Further from the fracture site, periosteal cells develop into osteoblasts and form woven bone. The cartilage and woven bone grow until they bridge the fracture gap. This is referred to as fracture callus. This restores some stability but minimal strength to the bone. 3. Hard callus formation - the callus is substituted by lamellar bone. During this period, initially the woven bone, and then the hyaline cartilage, are replaced by osteoblasts to form new lamellar bone in the form of trabecular bone. This process restores most of the bone's original strength. 4. Remodelling - trabecular bone is digested by osteoclasts followed by osteoblasts laying down compact bone. This occurs in response to the forces applied across the bone (Wolff's Law). This process may take up to 5 years and allows the bone to be restored to a configuration closely resembling its original shape and strength. Inadequate blood supply, stability or soft tissue (and periosteal) coverage and the presence of infection, dead tissue, tumour or systemic conditions such as diabetes can lead to fracture delayed union and eventually to non-union. Principles of fracture management Fracture management is aimed at protecting the healing process whilst maintaining adequate alignment and allowing for rehabilitation. If the fracture is undisplaced or the patient is unfit for anaesthetic, the position may be accepted and a cast applied.
5 Management: Reduction - may be achieved by local anaesthetic block, sedation and analgesia or general anaesthetic. Traction, or closed, and open reduction procedures may be used. Stabilisation - application of plaster cast, percutaneous wires, plate and screws, external fixator or intra-medullary nails may be required. This decision is made according to fracture pattern, complexity, involvement of a joint and relative stability. Immobilisation - a period of immobilisation in a cast may be required even after fixation with implants. Rehabilitation - range of motion along with muscle strengthening exercises must begin as early as is practical but must not compromise fracture healing. Specific examples are covered in the next chapter. Major trauma Major trauma is a term used to describe multiple injuries involving different tissues and organ systems that are, or may be, life threatening. Trauma patients require specialist care from a multidisciplinary group of professionals in a major trauma centre. These hospitals must provide 24-hours a day a fully staffed emergency department, a consultant-led resuscitative trauma team, dedicated trauma theatres and operating lists, the presence of all major surgical specialties on a single site (orthopaedic trauma, general and vascular surgery, neurosurgery, plastic surgery, cardiothoracic surgery, head and neck surgery and urology), interventional radiology and anaesthesia with appropriate intensive care facilities. Advanced Trauma Life Support (ATLS) An algorithm for management of major trauma patients, developed in the 1970s in the USA. Now adopted worldwide, the system allows a trauma team to manage a multiply injured patient in a standardised manner, allowing early identification and treatment of injuries, prioritised to the most life-threatening injuries first. The mnemonic ABCDE acts as an aide-memoir for the primary survey during which the simultaneous processes of identification of injuries and resuscitation occur. This is followed by the secondary survey to discover other, less severe injuries. Primary survey A - Airway with C-spine control - treatment of any threat to the airway with manoeuvres such as chin lift and jaw thrust, use of adjuncts (oro- and nasopharyngeal airways) or securing it with a cuffed endotracheal tube or tracheostomy. Throughout the resuscitation process, the cervical (C-) spine
6 must be immobilised in a hard collar and sand bags or with inline immobilisation and log rolling when transferring. This must be continued until the spine is cleared clinically and radiologically. B - Breathing - thorough examination including palpation, percussion, auscultation and on to chest X-ray to identify and treat life-threatening conditions such as airways obstruction (treated with removal of obstruction, bronchoscopy or tracheostomy), tension pneumothorax and massive haemothorax (both treated with a chest drain), flail chest with pulmonary contusion (treated with analgesia, physiotherapy and selective ventilation) and cardiac tamponade (treated with cardiocentesis or thoracotomy). C - Circulation and haemorrhage control - haemorrhage is a major cause of preventable death in trauma. Two large-bore intravenous lines are established and crystalloid solution given followed, if necessary, by blood products. External bleeding is controlled by direct pressure. Occult bleeding may be into the chest, abdomen, pelvis or long bone fractures. Severe abdominal or thoracic haemorrhage may require emergency laparotomy or thoracotomy to control bleeding. Pelvic fracture causing bleeding may initially be controlled with a pelvic binder but may require laparotomy with pelvic packing or interventional radiology and embolisation. D - Disability - assessment of neurological function using the Glasgow Coma Score (GCS) and examination of pupil light reflexes. Alteration of conscious level indicates a need to re-evaluate oxygenation, ventilation and perfusion status. Alcohol, drugs and hypoglycaemia may influence consciousness level. If these causes are ruled out, traumatic brain injury must be considered and searched for. E - Exposure/Environment - the patient must be fully exposed and examined thoroughly for major injuries. Then warming blankets must be applied. Secondary survey This entails a complete history and head to toe examination performed at a time when the patient has been stabilised. Every part of the body must be examined and appropriate X-rays obtained to rule out other injuries. Any deterioration in the patient s vital signs means the primary survey should restart at the Airway stage to identify a cause. Complications of fractures Acute Compartment syndrome - increased pressure within a myofascial compartment of fixed volume, caused by bleeding and oedema, exacerbated by diminished venous outflow. The raised intra-compartmental pressure can
7 lead to arterial occlusion within a few hours, leading to muscle and nerve necrosis. Signs are pain out of proportion of the injury and there is pain upon passive stretch of muscle within the compartment. Initially split any constricting bandages or cast. If there is no resolution, an emergency fasciotomy is required. Arterial injury - often due to joint dislocation, high energy injury or penetrating trauma. This is identified by absent distal pulses manually or on Doppler examination and requires stabilisation of skeletal injury (often with external fixator), followed by revascularisation by vascular surgeons. Fasciotomies may be performed to prevent compartment syndrome secondary to revascularisation after prolonged ischaemia. Nerve injury - often due to grossly displaced fractures, dislocations or penetrating trauma. Many will recover and can be observed. Those involved in open fractures, associated with vascular injury or injured during surgery require exploration. Intermediate Infection - deep bone and soft tissue infection is due to contamination of an open fracture or during surgical fixation. It may be difficult to resolve, may require multiple debridements (excision of dead tissue), long-term antibiotics and reconstruction using external frames. When causing severe disability or sepsis, the limb part may require amputation. Non-union - failure of fracture to unite due to problems with the bone (local tumour, infection, unstable fracture, severe comminuted fracture), surrounding soft tissues (infection, periosteal stripping, poor vascular supply, skin/muscle loss), and underlying patient issues (diabetes, smoking, malnourishment). Non-union may require multiple procedures to overcome the cause, including revision fixation with bone grafting, vascularised skin/muscle flaps and excision of infected bone and bone growth stimulation with an external frame. Mal-union fractures may unite in an abnormal position, leading to pain, reduced function and diminished motion in local joints. Malunited fractures may require surgery to cut and realign the bones. Late Osteoarthritis (see chapter 4) - injury to a joint may lead to early development of arthritic pain and reduced function of the joint (secondary/post-traumatic arthritis). Established osteoarthritis may eventually require joint replacement surgery (arthroplasty). Chapter 3

8 Common fractures Hip fractures Typically a fragility fracture (associated with osteoporosis) is seen in postmenopausal women over the age of 70 years. Risk factors include medical morbidity, falls history and previous fractures. The incidence is between 70,000 to 75,000 fractures each year and the annual cost in the UK is about 2 billion. About 10% of patients with a hip fracture die within 1 month and about one-third within 12 months. Most of the deaths are due to associated conditions and not to the fracture itself, reflecting the high prevalence of comorbidity. In young adults, this is a high-energy injury and should be treated as an orthopaedic emergency. There are two major common types of hip fracture and one rarer configuration, all of which require different treatments. These are defined by the position of the fracture on the neck of the femur: Intracapsular hip fractures The fracture line is proximal to the insertion of the hip capsule on the femoral neck. A displaced fracture disrupts the retinacular arteries that run up the neck, cutting the blood supply to the weight-bearing femoral head. If the head is subsequently fixed back in place, there is a high risk of it dying and collapsing due to avascular necrosis (AVN). Therefore, if displaced, the head is cut out (excised) and replaced with a half (hemi) or total hip replacement


9 (arthroplasty). If entirely undisplaced, the head may be retained and fixed with screws (relying on the assumption that the lack of fracture displacement means the arteries are undamaged). The Garden classification of intracapsular fractures is commonly used to describe displacement: Garden I - partial fracture, undisplaced - fix fracture with screws Garden II - complete fracture, undisplaced - fix fracture with screws Garden III - complete fracture, partial displacement - replace head with hemiarthroplasty or hip joint with total hip arthroplasty Garden IV - complete fracture, totally displaced - replace head with hemiarthroplasty or hip joint with total hip replacement Although widely accepted, the Garden classification has been shown to have large intra- and inter-observer error and is rarely used. It is easier to just describe these fractures as undisplaced or displaced.
arthroplasty include infection, dislocation, venous thromboembolism and wear through the acetabulum in hemiarthroplasty (requiring total hip arthroplasty).")
 and the number of fracture fragments e.g. intertrochanteric 3-part fracture.")
10 Complications of screw fixation include infection, non-union, loss of position and femoral head AVN (if painful, requires total hip replacement). Complications of hip (hemi)arthroplasty include infection, dislocation, venous thromboembolism and wear through the acetabulum in hemiarthroplasty (requiring total hip arthroplasty). Extracapsular hip fractures The fracture line is distal to the insertion of the capsule and therefore there is no risk of AVN. These fractures are described by the position in the proximal femur (intertrochanteric or sub-trochanteric) and the number of fracture fragments e.g. intertrochanteric 3-part fracture. Intertrochanteric fractures are usually treated by fixation with a special plate and screw called a dynamic hip screw (DHS). The screw grips into the
 will be more")

11 femoral head and can slide down through plate barrel (yellow arrow on diagram), allowing the fracture to compress and heal. Complex fracture configurations involving more pieces (4-part or if involving the lesser trochanter) will be more unstable and are often treated with a proximal femoral intramedullary nail. An intramedullary nail provides a mechanically stronger construct, although current literature does not show a difference in the outcome between this device and a DHS.

 guidelines target surgery within 24-36 hours of admission, combined management by orthopaedic")
12 Subtrochanteric fractures are inherently unstable due to the position of the fracture and require fixation with a femoral intramedullary nail. Treatment principles The priority of treatment of all hip fractures revolves around early surgery, which allows immediate mobility, reducing the risk of chest infection, venous thromboembolism and pressure sores. Current National Institute of Clinical Excellence (NICE) guidelines target surgery within hours of admission, combined management by orthopaedic surgeons and geriatricians and commencement of bone protection medication (such as bisphosphonates). Wrist fractures

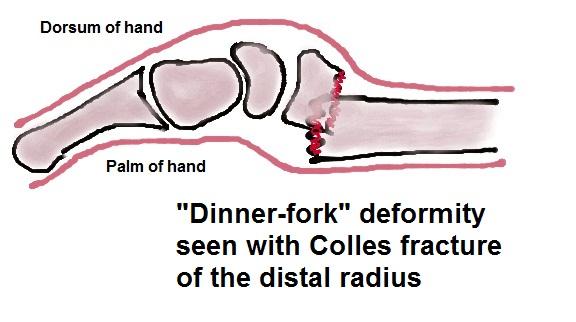
13 These are commonly seen, especially in the distal radius, in elderly osteoporotic bone or paediatric wrist joints with open growth plates (physes). Distal radius fractures in mature adults are typically high-energy injuries. The incidence is between 40,000 to 60,000 distal radius fractures in adults per year in the UK. Elderly fractures The most common fracture in the elderly population is a Colles fracture caused by a fall onto a flexed wrist in osteoporotic bone. The incidence increases with age. Other risk factors include female sex and postmenopause. A Colles fracture has five distinct deformities described in terms of the distal fragment: 1. Dorsal displacement 2. Dorsal tilt 3. Radial displacement 4. Radial tilt 5. Impaction (shortening)
14

15 Treatment principles Initially analgesia is given and assessment made for nerve compromise (typically median nerve) and other injuries. Preceding causes of the fall including cardiac and neurological disease must be considered. Diagnosis is with AP and lateral X-rays. Reduction is attempted by manipulation in the emergency department under haematoma block, Biers block or conscious sedation. Reduction is via in-line traction followed by a manoeuvre to initially increase the deformity (wrist extension) followed by reduction (flexion and ulnar deviation). A back slab is applied in this position and the wrist immobilised for 5-6 weeks with weekly check X-rays for the first 3 weeks to ensure reduction is maintained. If adequate reduction is not achieved or is lost, re-manipulation may be considered. If the patient is fit and functional, this may include reduction under general anaesthesia plus fixation with percutaneous K-wires or plate and screws. These elderly patients are at risk of further falls and other osteoporotic fractures, including spine wedge fractures and hip fractures. Thus, they must also be considered by their geriatrician for review in a falls prevention clinic and introduction of bone protection medication. Ankle fractures
 and the medial and lateral collateral ligaments of the ankle.")
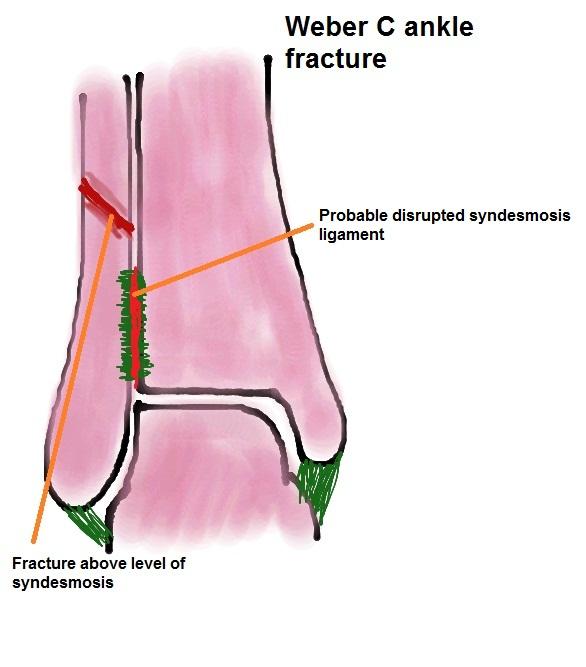
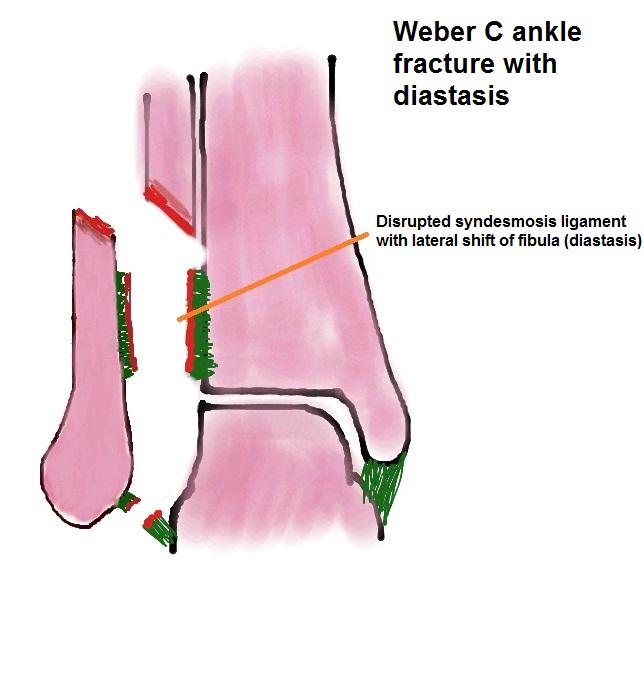
16 Increasing in incidence since the 1960s, most involve a single malleolus with about 30% being bi- or tri-malleolar. The ankle is a complex hinge joint with stability dependent upon the ligaments between the distal tibia and fibula (the syndesmosis) and the medial and lateral collateral ligaments of the ankle. Disruption of the syndesmosis following an ankle fracture allows the tibia and fibula to drift apart (diastasis). If the medial collateral ligament is also disrupted, the talus position under the tibia may displace laterally (talar shift). These must be detected and treated early to avoid the early onset of ankle arthritis. Injury pattern is related to the foot and ankle position at the time of injury. The level of the fracture on the lateral malleolus is indicative of the risk of injury to the syndesmosis (the more proximal, the greater the risk). Commonly described by the Weber classification: Weber A: fracture below the level of the distal tibial joint surface. No risk of diastasis. Weber B: fracture at the level of the syndesmosis. 50% have associated disruption of the syndesmosis. Weber C: fracture above the level of the syndesmosis. Syndesmosis almost always disrupted.
17
18
19 Treatment principles Weber C fractures require open reduction and internal fixation (ORIF) with plate and screws and a large screw holding the fibula reduced on the tibia (known as a diastasis or syndesmosis screw). This screw will often be removed once the ligament has healed after 8-9 weeks. Typically Weber B fractures require fixation of the lateral malleolus with plate and screws but if there is associated diastasis, they will also require a diastasis screw. Weber A fractures and undisplaced Weber B fractures may be managed nonoperatively in a non-weight bearing below-knee cast for 6 weeks.

20 Tibial and femoral shaft fractures Femoral shaft fractures occur in a bimodal distribution, most frequently in young men after high-energy trauma and elderly women after a low-energy fall. Neurovascular injury is uncommon after these injuries but major blood loss may occur with greater than 1.2L being the average loss and about 40% of patients requiring transfusion. Careful evaluation for other injuries must be carried out. Tibial fractures are the most common long bone fractures. Men are most commonly affected, with incidence being about 41 per 100,000 per year. Injury may be via direct high-energy blows, penetrating trauma and bending or torsional forces. The tibia has a subcutaneous border and so has a high incidence of open fractures. These require early antibiotics (and tetanus cover), skeletal stabilisation, aggressive wound debridement and early skin coverage or closure. Compartment syndrome is a risk in long bone fractures, particularly those of the tibia, and must be closely monitored for. Pain out of proportion to the injury is the most reliable sign. Any suspicion of compartment syndrome requires emergency fasciotomy - delay leads to extensive muscle necrosis with the risk of acute renal injury and toxic shock and eventual chronic contractures and limited limb function.
21 Treatment principles The aims of treatment are to stabilise the fracture allowing the patient to mobilise (and possibly ambulate) whilst allowing the fracture to heal. The most common treatment is intra-medullary nail fixation. This should be performed within 24 hours and early stabilisation of long bone fractures appears particularly important in the multiply injured patient. External fixators may be used as a temporary or permanent stabilisation technique, particularly in fractures with open wounds or complex articular injuries. External fixators are rarely used as definitive treatment for femoral fractures. Plates are rarely used for tibial and femoral shaft fractures and are often reserved for intra-articular involvement or for treatment of non-unions.
Surgery-Ortho. Fractures of the tibia and fibula. Management. Treatment of low energy fractures. Fifth stage. Lec-6 د.
 Fifth stage Lec-6 د. مثنى Surgery-Ortho 28/4/2016 Indirect force: (low energy) Fractures of the tibia and fibula Twisting: spiral fractures of both bones Angulatory: oblique fractures with butterfly segment.
Fifth stage Lec-6 د. مثنى Surgery-Ortho 28/4/2016 Indirect force: (low energy) Fractures of the tibia and fibula Twisting: spiral fractures of both bones Angulatory: oblique fractures with butterfly segment.
Surgical Care at the District Hospital. EMERGENCY & ESSENTIAL SURGICAL CARE
 Surgical Care at the District Hospital 1 18 Orthopedic Trauma Key Points 2 18.1 Upper Extremity Injuries Clavicle Fractures Diagnose fractures from the history and by physical examination Treat with a
Surgical Care at the District Hospital 1 18 Orthopedic Trauma Key Points 2 18.1 Upper Extremity Injuries Clavicle Fractures Diagnose fractures from the history and by physical examination Treat with a
Fractures and dislocations around elbow in adult
 Lec: 3 Fractures and dislocations around elbow in adult These include fractures of distal humerus, fracture of the capitulum, fracture of the radial head, fracture of the olecranon & dislocation of the
Lec: 3 Fractures and dislocations around elbow in adult These include fractures of distal humerus, fracture of the capitulum, fracture of the radial head, fracture of the olecranon & dislocation of the
Vasu Pai FRACS, MCh, MS, Nat Board Ortho Surgeon Gisborne
 Vasu Pai FRACS, MCh, MS, Nat Board Ortho Surgeon Gisborne FRACTURE MANAGEMENT I Simple closed fracture : Complete or Incomplete Stable or unstable II Open fracture III Multiple fracture IV Polytrauma Fractures
Vasu Pai FRACS, MCh, MS, Nat Board Ortho Surgeon Gisborne FRACTURE MANAGEMENT I Simple closed fracture : Complete or Incomplete Stable or unstable II Open fracture III Multiple fracture IV Polytrauma Fractures
Fractures Healing & Management. Traumatology RHS 231 Dr. Einas Al-Eisa Lecture 4
 Fractures Healing & Management Traumatology RHS 231 Dr. Einas Al-Eisa Lecture 4 Fractures Despite their strength, bones are susceptible to fractures. In young people, most fractures result from trauma
Fractures Healing & Management Traumatology RHS 231 Dr. Einas Al-Eisa Lecture 4 Fractures Despite their strength, bones are susceptible to fractures. In young people, most fractures result from trauma
Calcaneus (Heel Bone) Fractures
 Fractures") Page 1 of 8 Calcaneus (Heel Bone) Fractures A fracture of the calcaneus, or heel bone, can be a painful and disabling injury. This type of fracture commonly occurs during a high-energy event such as a
Page 1 of 8 Calcaneus (Heel Bone) Fractures A fracture of the calcaneus, or heel bone, can be a painful and disabling injury. This type of fracture commonly occurs during a high-energy event such as a
7/23/2018 DESCRIBING THE FRACTURE. Pattern Open vs closed Location BASIC PRINCIPLES OF FRACTURE MANAGEMENT. Anjan R. Shah MD July 21, 2018.
 BASIC PRINCIPLES OF FRACTURE MANAGEMENT Anjan R. Shah MD July 21, 2018 DESCRIBING THE FRACTURE Pattern Open vs closed Location POLL OPEN HOW WOULD YOU DESCRIBE THIS FRACTURE PATTERN? 1 Spiral 2 Transverse
BASIC PRINCIPLES OF FRACTURE MANAGEMENT Anjan R. Shah MD July 21, 2018 DESCRIBING THE FRACTURE Pattern Open vs closed Location POLL OPEN HOW WOULD YOU DESCRIBE THIS FRACTURE PATTERN? 1 Spiral 2 Transverse
Chapter 30 - Musculoskeletal_Trauma
 Introduction to Emergency Medical Care 1 OBJECTIVES 30.1 Define key terms introduced in this chapter. Slides 11 12, 19 20, 22 23, 37 30.2 Describe the anatomy of elements of the musculoskeletal system.
Introduction to Emergency Medical Care 1 OBJECTIVES 30.1 Define key terms introduced in this chapter. Slides 11 12, 19 20, 22 23, 37 30.2 Describe the anatomy of elements of the musculoskeletal system.
.org. Tibia (Shinbone) Shaft Fractures. Anatomy. Types of Tibial Shaft Fractures
 Shaft Fractures. Anatomy. Types of Tibial Shaft Fractures") Tibia (Shinbone) Shaft Fractures Page ( 1 ) The tibia, or shinbone, is the most common fractured long bone in your body. The long bones include the femur, humerus, tibia, and fibula. A tibial shaft fracture
Tibia (Shinbone) Shaft Fractures Page ( 1 ) The tibia, or shinbone, is the most common fractured long bone in your body. The long bones include the femur, humerus, tibia, and fibula. A tibial shaft fracture
Tibial Shaft Fractures
 Tibial Shaft Fractures Mr Krishna Vemulapalli Consultant Orthopaedics Surgeon Queens & King George Hospitals Queens Hospital 14/03/2018 Google Maps Map data 2018 Google 10 km Orthopaedics Department Covers
Tibial Shaft Fractures Mr Krishna Vemulapalli Consultant Orthopaedics Surgeon Queens & King George Hospitals Queens Hospital 14/03/2018 Google Maps Map data 2018 Google 10 km Orthopaedics Department Covers
The pilon tibiale fracture
 The pilon tibiale fracture Thomas Beck Spitalzentrum Oberwallis OTC Trauma course september 2017 xxx I have no financial relationships with commercial entities that produce healthcare related products.
The pilon tibiale fracture Thomas Beck Spitalzentrum Oberwallis OTC Trauma course september 2017 xxx I have no financial relationships with commercial entities that produce healthcare related products.
Pediatric Tibia Fractures Key Points. Christopher Iobst, MD
 Pediatric Tibia Fractures Key Points Christopher Iobst, MD Goals Bone to heal Return to full weight bearing Acceptable alignment rule of 10s 10 degrees of varus 8 degrees of valgus 12 degrees of procurvatum
Pediatric Tibia Fractures Key Points Christopher Iobst, MD Goals Bone to heal Return to full weight bearing Acceptable alignment rule of 10s 10 degrees of varus 8 degrees of valgus 12 degrees of procurvatum
1/3/2008. Karen Burke Priscilla LeMone Elaine Mohn-Brown. Medical-Surgical Nursing Care, 2e Karen Burke, Priscilla LeMone, and Elaine Mohn-Brown
 Medical-Surgical Nursing Care Second Edition Karen Burke Priscilla LeMone Elaine Mohn-Brown Chapter 42 Caring for Clients with Musculoskeletal Trauma Musculoskeletal Trauma Tissue is subjected to more
Medical-Surgical Nursing Care Second Edition Karen Burke Priscilla LeMone Elaine Mohn-Brown Chapter 42 Caring for Clients with Musculoskeletal Trauma Musculoskeletal Trauma Tissue is subjected to more
Multiapical Deformities p. 97 Osteotomy Concepts and Frontal Plane Realignment p. 99 Angulation Correction Axis (ACA) p. 99 Bisector Lines p.
 p. 99 Bisector Lines p.") Normal Lower Limb Alignment and Joint Orientation p. 1 Mechanical and Anatomic Bone Axes p. 1 Joint Center Points p. 5 Joint Orientation Lines p. 5 Ankle p. 5 Knee p. 5 Hip p. 8 Joint Orientation Angles
Normal Lower Limb Alignment and Joint Orientation p. 1 Mechanical and Anatomic Bone Axes p. 1 Joint Center Points p. 5 Joint Orientation Lines p. 5 Ankle p. 5 Knee p. 5 Hip p. 8 Joint Orientation Angles
EVOS MINI with IM Nailing
 Case Series Dr. John A. Scolaro EVOS MINI with IM Nailing A series of studies Introduction Intramedullary nailing has become the standard for many long bone fractures. Fracture reduction prior to nail
Case Series Dr. John A. Scolaro EVOS MINI with IM Nailing A series of studies Introduction Intramedullary nailing has become the standard for many long bone fractures. Fracture reduction prior to nail
PEM GUIDE CHILDHOOD FRACTURES
 PEM GUIDE CHILDHOOD FRACTURES INTRODUCTION Skeletal injuries account for 10-15% of all injuries in children; 20% of those are fractures, 3 out of 4 fractures affect the physis or growth plate. Always consider
PEM GUIDE CHILDHOOD FRACTURES INTRODUCTION Skeletal injuries account for 10-15% of all injuries in children; 20% of those are fractures, 3 out of 4 fractures affect the physis or growth plate. Always consider
1 Chapter 29 Orthopaedic Injuries Principles of Splinting 2 Types of Muscles. Striated Skeletal. Smooth
 1 Chapter 29 Orthopaedic Injuries Principles of Splinting 2 Types of Muscles Striated Skeletal Smooth 3 Anatomy and Physiology of the Musculoskeletal System 4 Skeletal System 5 Skeletal System Functions
1 Chapter 29 Orthopaedic Injuries Principles of Splinting 2 Types of Muscles Striated Skeletal Smooth 3 Anatomy and Physiology of the Musculoskeletal System 4 Skeletal System 5 Skeletal System Functions
Rehabilitation after Total Elbow Arthroplasty
 Rehabilitation after Total Elbow Arthroplasty Total Elbow Atrthroplasty Total elbow arthroplasty (TEA) Replacement of the ulnohumeral articulation with a prosthetic device. Goal of TEA is to provide pain
Rehabilitation after Total Elbow Arthroplasty Total Elbow Atrthroplasty Total elbow arthroplasty (TEA) Replacement of the ulnohumeral articulation with a prosthetic device. Goal of TEA is to provide pain
Chapter 29 Orthopaedic Injuries Principles of Splinting Types of Muscles
 1 2 3 4 5 6 7 Chapter 29 Orthopaedic Injuries Principles of Splinting Types of Muscles Striated Skeletal Smooth Anatomy and Physiology of the Musculoskeletal System Skeletal System Skeletal System Functions
1 2 3 4 5 6 7 Chapter 29 Orthopaedic Injuries Principles of Splinting Types of Muscles Striated Skeletal Smooth Anatomy and Physiology of the Musculoskeletal System Skeletal System Skeletal System Functions
Injuries to the Hands and Feet
 Injuries to the Hands and Feet Chapter 26 Injuries to the Hands and Feet Introduction Combat injuries to the hands and feet differ from those of the arms and legs in terms of mortality and morbidity. Death
Injuries to the Hands and Feet Chapter 26 Injuries to the Hands and Feet Introduction Combat injuries to the hands and feet differ from those of the arms and legs in terms of mortality and morbidity. Death
Pelvis injuries Fractures of the femur (proximal,shaft) Dr Tamás Bodzay
 Dr Tamás Bodzay") Pelvis injuries Fractures of the femur (proximal,shaft) Dr Tamás Bodzay Pelvis anatomy Pelvis function - axial load bearing - protection: abdominal, pelvic structures Pelvic injury mechanism Falling from
Pelvis injuries Fractures of the femur (proximal,shaft) Dr Tamás Bodzay Pelvis anatomy Pelvis function - axial load bearing - protection: abdominal, pelvic structures Pelvic injury mechanism Falling from
Fracture Classification
 Fracture Classification Lisa K. Cannada MD Updated: 05/2016 18 th & 19 th century History of Fracture History based on clinical appearance of limb alone Classification Colles Fracture Dinner Fork Deformity
Fracture Classification Lisa K. Cannada MD Updated: 05/2016 18 th & 19 th century History of Fracture History based on clinical appearance of limb alone Classification Colles Fracture Dinner Fork Deformity
Basic Principles of Fractures & Easily Missed Fractures. Mr Irfan Merchant Trauma & Orthopaedic Registrar Bedford Hospital, East of England
 Basic Principles of Fractures & Easily Missed Fractures Mr Irfan Merchant Trauma & Orthopaedic Registrar Bedford Hospital, East of England Objectives Types Fracture Patterns Fracture Healing Assessing
Basic Principles of Fractures & Easily Missed Fractures Mr Irfan Merchant Trauma & Orthopaedic Registrar Bedford Hospital, East of England Objectives Types Fracture Patterns Fracture Healing Assessing
The Orthopaedic Enigma: A Simplified Classification
 ISPUB.COM The Internet Journal of Orthopedic Surgery Volume 3 Number 2 The Orthopaedic Enigma: A Simplified Classification D Iyer Citation D Iyer. The Orthopaedic Enigma: A Simplified Classification. The
ISPUB.COM The Internet Journal of Orthopedic Surgery Volume 3 Number 2 The Orthopaedic Enigma: A Simplified Classification D Iyer Citation D Iyer. The Orthopaedic Enigma: A Simplified Classification. The
BCCH Emergency Department LOWER LIMB INJURIES Resource pack
 1 BCCH Emergency Department LOWER LIMB INJURIES Resource pack Developed by: Rena Heathcote RN. 2 Knee Injuries The knee joint consists of a variety of structures including: 3 bones (excluding the patella)
1 BCCH Emergency Department LOWER LIMB INJURIES Resource pack Developed by: Rena Heathcote RN. 2 Knee Injuries The knee joint consists of a variety of structures including: 3 bones (excluding the patella)
Nursing Management: Musculoskeletal Trauma and Orthopedic Surgery. By: Aun Lauriz E. Macuja SAC_SN4
 Nursing Management: Musculoskeletal Trauma and Orthopedic Surgery By: Aun Lauriz E. Macuja SAC_SN4 The most common cause of musculoskeletal injuries is a traumatic event resulting in fracture, dislocation,
Nursing Management: Musculoskeletal Trauma and Orthopedic Surgery By: Aun Lauriz E. Macuja SAC_SN4 The most common cause of musculoskeletal injuries is a traumatic event resulting in fracture, dislocation,
Traumatic injuries of knee and hip
 Traumatic injuries of knee and hip Martin W. Korn, MD The United States secretary of transportation recently announced that highway deaths had risen from the previously announced 56,000 for 1969 to a new
Traumatic injuries of knee and hip Martin W. Korn, MD The United States secretary of transportation recently announced that highway deaths had risen from the previously announced 56,000 for 1969 to a new
4/28/2010. Fractures. Normal Bone and Normal Ossification Bone Terms. Epiphysis Epiphyseal Plate (physis) Metaphysis
 Metaphysis") Fractures Normal Bone and Normal Ossification Bone Terms Epiphysis Epiphyseal Plate (physis) Metaphysis Diaphysis 1 Fracture Classifications A. Longitudinal B. Transverse C. Oblique D. Spiral E. Incomplete
Fractures Normal Bone and Normal Ossification Bone Terms Epiphysis Epiphyseal Plate (physis) Metaphysis Diaphysis 1 Fracture Classifications A. Longitudinal B. Transverse C. Oblique D. Spiral E. Incomplete
OBJECTIVES: Define basic assessments skills needed to identify orthopedic injuries. Differentiate when an orthopedic injury is a medical emergency
 1 2 How to Triage Orthopaedic Care David W. Gray, M.D. OBJECTIVES: Define basic assessments skills needed to identify orthopedic injuries Differentiate when an orthopedic injury is a medical emergency
1 2 How to Triage Orthopaedic Care David W. Gray, M.D. OBJECTIVES: Define basic assessments skills needed to identify orthopedic injuries Differentiate when an orthopedic injury is a medical emergency
European Resuscitation Council
 European Resuscitation Council Incidence of Trauma in Childhood Leading cause of death and disability in children older than one year all over the world Structured approach Primary survey and resuscitation
European Resuscitation Council Incidence of Trauma in Childhood Leading cause of death and disability in children older than one year all over the world Structured approach Primary survey and resuscitation
Hip Fractures. Anatomy. Causes. Symptoms
 Hip Fractures A hip fracture is a break in the upper quarter of the femur (thigh) bone. The extent of the break depends on the forces that are involved. The type of surgery used to treat a hip fracture
Hip Fractures A hip fracture is a break in the upper quarter of the femur (thigh) bone. The extent of the break depends on the forces that are involved. The type of surgery used to treat a hip fracture
Pediatric Fractures. Objectives. Epiphyseal Complex. Anatomy and Physiology. Ligaments. Bony matrix
 1 Pediatric Fractures Nicholas White, MD Assistant Professor of Pediatrics Eastern Virginia Medical School Attending, Pediatric Emergency Department Children s Hospital of The King s Daughters Objectives
1 Pediatric Fractures Nicholas White, MD Assistant Professor of Pediatrics Eastern Virginia Medical School Attending, Pediatric Emergency Department Children s Hospital of The King s Daughters Objectives
ผศ.นพ.ธรา ธรรมโรจน ภาควชาออรโธปดกส คณะแพทยศาสตร, มหาวทยาล!ยขอนแก#น
 1972 ผศ.นพ.ธรา ธรรมโรจน ภาควชาออรโธปดกส คณะแพทยศาสตร, มหาวทยาล!ยขอนแก#น Common Fracture in lower Extremity Common Fracture in Adult(Traumatic Associated Fracture) Fracture of Tibia and Fibular Fracture
1972 ผศ.นพ.ธรา ธรรมโรจน ภาควชาออรโธปดกส คณะแพทยศาสตร, มหาวทยาล!ยขอนแก#น Common Fracture in lower Extremity Common Fracture in Adult(Traumatic Associated Fracture) Fracture of Tibia and Fibular Fracture
.org. Ankle Fractures (Broken Ankle) Anatomy
 Anatomy") Ankle Fractures (Broken Ankle) Page ( 1 ) A broken ankle is also known as an ankle fracture. This means that one or more of the bones that make up the ankle joint are broken. A fractured ankle can range
Ankle Fractures (Broken Ankle) Page ( 1 ) A broken ankle is also known as an ankle fracture. This means that one or more of the bones that make up the ankle joint are broken. A fractured ankle can range
Osteosynthesis involving a joint Thomas P Rüedi
 Osteosynthesis involving a joint Thomas P Rüedi How to use this handout? The left column contains the information given during the lecture. The column at the right gives you space to make personal notes.
Osteosynthesis involving a joint Thomas P Rüedi How to use this handout? The left column contains the information given during the lecture. The column at the right gives you space to make personal notes.
Common Limb Fractures. Mr Sheraz Malik MB BS MRCS Instructor Mr Paul Ofori-Atta Mb ChB FRCS President Motc Life UK April 2009
 Common Limb Fractures Mr Sheraz Malik MB BS MRCS Instructor Mr Paul Ofori-Atta Mb ChB FRCS President Motc Life UK April 2009 Objectives To be able to describe all characteristics of a fracture Describe
Common Limb Fractures Mr Sheraz Malik MB BS MRCS Instructor Mr Paul Ofori-Atta Mb ChB FRCS President Motc Life UK April 2009 Objectives To be able to describe all characteristics of a fracture Describe
Hand injuries. The metacarpal bones may fracture through the base, shaft or the neck.
 Hand injuries Metacarpal injuries The metacarpal bones may fracture through the base, shaft or the neck. Shaft fractures; these are caused by direct trauma which may cause transverse # of one or more metacarpal
Hand injuries Metacarpal injuries The metacarpal bones may fracture through the base, shaft or the neck. Shaft fractures; these are caused by direct trauma which may cause transverse # of one or more metacarpal
PRONATION-ABDUCTION FRACTURES
 C H A P T E R 1 2 PRONATION-ABDUCTION FRACTURES George S. Gumann, DPM (The opinions of the author should not be considered as reflecting official policy of the US Army Medical Department.) Pronation-abduction
C H A P T E R 1 2 PRONATION-ABDUCTION FRACTURES George S. Gumann, DPM (The opinions of the author should not be considered as reflecting official policy of the US Army Medical Department.) Pronation-abduction
Index. Note: Page numbers of article titles are in boldface type. Hand Clin 21 (2005)
") Hand Clin 21 (2005) 501 505 Index Note: Page numbers of article titles are in boldface type. A Antibiotics, following distal radius fracture treatment, 295, 296 Arthritis, following malunion of distal
Hand Clin 21 (2005) 501 505 Index Note: Page numbers of article titles are in boldface type. A Antibiotics, following distal radius fracture treatment, 295, 296 Arthritis, following malunion of distal
DISLOCATION AND FRACTURES OF THE HIP. Dr Károly Fekete
 DISLOCATION AND FRACTURES OF THE HIP Dr Károly Fekete 1 OUTLINE Epidemiology Incidence Anatomy Patient s examination, clinical symptons Diagnosis Classification Management Special complications 2 EPIDEMIOLOGY,
DISLOCATION AND FRACTURES OF THE HIP Dr Károly Fekete 1 OUTLINE Epidemiology Incidence Anatomy Patient s examination, clinical symptons Diagnosis Classification Management Special complications 2 EPIDEMIOLOGY,
Management of Fractures. Traumatology RHS 231 Dr. Einas Al-Eisa Lecture 5
 Management of Fractures Traumatology RHS 231 Dr. Einas Al-Eisa Lecture 5 Common methods of fracture immobilization Plaster of Paris (POP): A high quality gypsum The standard method of external splinting
Management of Fractures Traumatology RHS 231 Dr. Einas Al-Eisa Lecture 5 Common methods of fracture immobilization Plaster of Paris (POP): A high quality gypsum The standard method of external splinting
CLINICAL AND OPERATIVE APPROACH FOR TOTAL KNEE REPLACEMENT DR.VINMAIE ORTHOPAEDICS PG 2 ND YEAR
 CLINICAL AND OPERATIVE APPROACH FOR TOTAL KNEE REPLACEMENT DR.VINMAIE ORTHOPAEDICS PG 2 ND YEAR Evolution of TKR In 1860, Verneuil proposed interposition arthroplasty, involving the insertion of soft tissue
CLINICAL AND OPERATIVE APPROACH FOR TOTAL KNEE REPLACEMENT DR.VINMAIE ORTHOPAEDICS PG 2 ND YEAR Evolution of TKR In 1860, Verneuil proposed interposition arthroplasty, involving the insertion of soft tissue
Femoral Shaft Fracture
 Femoral Shaft Fracture The femoral shaft is well padded with muscles(an advantage in protecting the bone from all but the most powerful forces)but the disadvantage is that fractures are often severely
Femoral Shaft Fracture The femoral shaft is well padded with muscles(an advantage in protecting the bone from all but the most powerful forces)but the disadvantage is that fractures are often severely
Pathophysiology of fracture healing
 Pathophysiology of fracture healing Bone anatomy and biomechanics Fracture patterns Bone healing and blood supply Influence of implants 1 What is the structure of bone? 2 Bone structure Four levels: Chemical
Pathophysiology of fracture healing Bone anatomy and biomechanics Fracture patterns Bone healing and blood supply Influence of implants 1 What is the structure of bone? 2 Bone structure Four levels: Chemical
Fractures of the Hand in Children Which are simple? And Which have pitfalls??
 Fractures of the Hand in Children Which are simple? And Which have pitfalls?? Kaye E Wilkins DVM, MD Professor of Orthopedics and Pediatrics Departments of Orthopedics and Pediatrics University of Texas
Fractures of the Hand in Children Which are simple? And Which have pitfalls?? Kaye E Wilkins DVM, MD Professor of Orthopedics and Pediatrics Departments of Orthopedics and Pediatrics University of Texas
Fractures of the shoulder girdle, elbow and fractures of the humerus. H. Sithebe 2012
 Fractures of the shoulder girdle, elbow and fractures of the humerus H. Sithebe 2012 Fractures of the Clavicle (mid-shaft). Fractures of the clavicle Fractures of the clavicle Treatment- conservative.
Fractures of the shoulder girdle, elbow and fractures of the humerus H. Sithebe 2012 Fractures of the Clavicle (mid-shaft). Fractures of the clavicle Fractures of the clavicle Treatment- conservative.
Treatment of malunited fractures of the ankle
 Treatment of malunited fractures of the ankle A LONG-TERM FOLLOW-UP OF RECONSTRUCTIVE SURGERY I. I. Reidsma, P. A. Nolte, R. K. Marti, E. L. F. B. Raaymakers From Academic Medical Center, Amsterdam, Netherlands
Treatment of malunited fractures of the ankle A LONG-TERM FOLLOW-UP OF RECONSTRUCTIVE SURGERY I. I. Reidsma, P. A. Nolte, R. K. Marti, E. L. F. B. Raaymakers From Academic Medical Center, Amsterdam, Netherlands
Principle Management of Wound and Fracture in Emergency Department
 Principle Management of Wound and Fracture in Emergency Department Presented in Clinical Update Seminar January 15 th 2011 dr. Tedjo Rukmoyo, SpOT (K) Spine Initial Management ATLS Procedure A : airway
Principle Management of Wound and Fracture in Emergency Department Presented in Clinical Update Seminar January 15 th 2011 dr. Tedjo Rukmoyo, SpOT (K) Spine Initial Management ATLS Procedure A : airway
Introduction to Fractures. Traumatology RHS 231 Dr. Einas Al-Eisa Lecture 3
 Introduction to Fractures Traumatology RHS 231 Dr. Einas Al-Eisa Lecture 3 Definitions A fracture is an interruption in the continuity of bone Fracture = Break Fracture: mechanical damage produced in a
Introduction to Fractures Traumatology RHS 231 Dr. Einas Al-Eisa Lecture 3 Definitions A fracture is an interruption in the continuity of bone Fracture = Break Fracture: mechanical damage produced in a
1/19/2018. Winter injuries to the shoulder and elbow. Highgate Private Hospital (Whittington Health NHS Trust)
") Winter injuries to the shoulder and elbow Omar Haddo Consultant Orthopaedic Surgeon, Shoulder, Elbow, Hand & Wrist Specialist MBBS, BmedSci, FRCS(Orth) Highgate Private Hospital (Whittington Health NHS
Winter injuries to the shoulder and elbow Omar Haddo Consultant Orthopaedic Surgeon, Shoulder, Elbow, Hand & Wrist Specialist MBBS, BmedSci, FRCS(Orth) Highgate Private Hospital (Whittington Health NHS
CURRENT TREATMENT OPTIONS
 CURRENT TREATMENT OPTIONS Fix single column or both: Always fix both. A study by Svend-Hansen corroborated the poor results associated with isolated medial malleolar fixation in bimalleolar ankle fractures.
CURRENT TREATMENT OPTIONS Fix single column or both: Always fix both. A study by Svend-Hansen corroborated the poor results associated with isolated medial malleolar fixation in bimalleolar ankle fractures.
Cluster - 26 ORTHOPEDICS. X Ray of Affected Limb, MIR of Shoulder
 Sr.No Package no 1708 26.1 Orthopeidc 1709 26.2 Orthopeidc Sub speciality Procedure name Pre-Operative Investigation AC joint reconstruction/ Stabilization/ Acromionplasty (Nonoperative management is recommended
Sr.No Package no 1708 26.1 Orthopeidc 1709 26.2 Orthopeidc Sub speciality Procedure name Pre-Operative Investigation AC joint reconstruction/ Stabilization/ Acromionplasty (Nonoperative management is recommended
CHAPTER 28 Musculoskeletal Injuries
 CHAPTER 28 Musculoskeletal Injuries Musculoskeletal System Anatomy & Physiology Bones provide framework. Joints allow for bending. Muscles allow for movement. Cartilage provides flexibility. Tendons connect
CHAPTER 28 Musculoskeletal Injuries Musculoskeletal System Anatomy & Physiology Bones provide framework. Joints allow for bending. Muscles allow for movement. Cartilage provides flexibility. Tendons connect
Musculoskeletal System
 CHAPTER 28 Musculoskeletal Injuries Musculoskeletal System Anatomy & Physiology Bones provide framework. Joints allow for bending. Muscles allow for movement. Cartilage provides flexibility. Tendons connect
CHAPTER 28 Musculoskeletal Injuries Musculoskeletal System Anatomy & Physiology Bones provide framework. Joints allow for bending. Muscles allow for movement. Cartilage provides flexibility. Tendons connect
Comparitive Study between Proximal Femoral Nailing and Dynamic Hip Screw in Intertrochanteric Fracture of Femur *
 Open Journal of Orthopedics, 2013, 3, 291-295 Published Online November 2013 (http://www.scirp.org/journal/ojo) http://dx.doi.org/10.4236/ojo.2013.37053 291 Comparitive Study between Proximal Femoral Nailing
Open Journal of Orthopedics, 2013, 3, 291-295 Published Online November 2013 (http://www.scirp.org/journal/ojo) http://dx.doi.org/10.4236/ojo.2013.37053 291 Comparitive Study between Proximal Femoral Nailing
Hand and wrist emergencies
 Chapter1 Hand and wrist emergencies Carl A. Germann Distal radius and ulnar injuries PEARL: Fractures of the distal radius and ulna are the most common type of fractures in patients younger than 75 years.
Chapter1 Hand and wrist emergencies Carl A. Germann Distal radius and ulnar injuries PEARL: Fractures of the distal radius and ulna are the most common type of fractures in patients younger than 75 years.
St Mary Orthopaedic Conference. Steven A. Caruso, MD Trenton Orthopaedic Group Trauma and Complex Fracture Surgeon October 25, 2014
 St Mary Orthopaedic Conference Steven A. Caruso, MD Trenton Orthopaedic Group Trauma and Complex Fracture Surgeon October 25, 2014 Nothing to disclose Goals To discuss common orthopaedic pathologies and
St Mary Orthopaedic Conference Steven A. Caruso, MD Trenton Orthopaedic Group Trauma and Complex Fracture Surgeon October 25, 2014 Nothing to disclose Goals To discuss common orthopaedic pathologies and
Presented at 2015 TQIP conference. Developed by a panel of experts. Evidence based with expert opinion as needed
 Presented at 2015 TQIP conference Developed by a panel of experts Evidence based with expert opinion as needed Orthopaedic Trauma Best Practice Guidelines (BPG) Goals Offer guidance on what is practical
Presented at 2015 TQIP conference Developed by a panel of experts Evidence based with expert opinion as needed Orthopaedic Trauma Best Practice Guidelines (BPG) Goals Offer guidance on what is practical
Carpal rows injuries!
 Carpal rows injuries! Michael Papaloïzos! Center for Hand Surgery and Therapy Geneva, Switzerland no conflict of interest to declare Fractures of carpal bones! The fractured scaphoid! Fracture-dislocations
Carpal rows injuries! Michael Papaloïzos! Center for Hand Surgery and Therapy Geneva, Switzerland no conflict of interest to declare Fractures of carpal bones! The fractured scaphoid! Fracture-dislocations
Lower Extremity Fracture Management. Fractures of the Hip. Lower Extremity Fractures. Vascular Anatomy. Lower Extremity Fractures in Children
 Lower Extremity Fracture Management Brian Brighton, MD, MPH Levine Children s s Hospital Carolinas Medical Center Charlotte, NC Oscar Miller Day October 16, 2009 Lower Extremity Fractures in Children Anatomic
Lower Extremity Fracture Management Brian Brighton, MD, MPH Levine Children s s Hospital Carolinas Medical Center Charlotte, NC Oscar Miller Day October 16, 2009 Lower Extremity Fractures in Children Anatomic
Chapter 4: Forearm 4.3 Forearm shaft fractures, transverse (12-D/4)
") AO Manual of ESIN in children s fractures Chapter 4: Forearm 4.3 Forearm shaft fractures, transverse (12-D/4) Title AO Manual of ESIN in children Subtitle Elastic stable intramedullary nailing (ESIN) Author
AO Manual of ESIN in children s fractures Chapter 4: Forearm 4.3 Forearm shaft fractures, transverse (12-D/4) Title AO Manual of ESIN in children Subtitle Elastic stable intramedullary nailing (ESIN) Author
Surgical Care at the District Hospital. EMERGENCY & ESSENTIAL SURGICAL CARE
 Surgical Care at the District Hospital 1 17 Orthopedic Techniques Key Points 2 17.1 Traction Use an appropriate method of traction to treat fractures of the extremities and cervical spine Apply extremity
Surgical Care at the District Hospital 1 17 Orthopedic Techniques Key Points 2 17.1 Traction Use an appropriate method of traction to treat fractures of the extremities and cervical spine Apply extremity
Foot Injuries. Dr R B Kalia
 Foot Injuries Dr R B Kalia Overview Dramatic impact on the overall health, activity, and emotional status More attention and aggressive management Difficult appendage to study and diagnose. Aim- a stable
Foot Injuries Dr R B Kalia Overview Dramatic impact on the overall health, activity, and emotional status More attention and aggressive management Difficult appendage to study and diagnose. Aim- a stable
QUEST.6. This patient fell from a tree a. What is the diagnosis? (2) b. What would be your management for this injury in casualty?
 b. What would be your management for this injury in casualty?") QUEST.6 This patient fell from a tree a. What is the diagnosis? (2) b. What would be your management for this injury in casualty? (3) P381 A. Right sided fractures of medial and lateral malleoli with a
QUEST.6 This patient fell from a tree a. What is the diagnosis? (2) b. What would be your management for this injury in casualty? (3) P381 A. Right sided fractures of medial and lateral malleoli with a
A comparative study of 30 cases of trochanteric fracture femur treated with dynamic hip screw and proximal femoral nailing
 Original Article A comparative study of 30 cases of trochanteric fracture femur treated with dynamic hip screw and proximal femoral nailing Jaswinder Pal Singh Walia *, Himanshu Tailor**, H S Mann ***,
Original Article A comparative study of 30 cases of trochanteric fracture femur treated with dynamic hip screw and proximal femoral nailing Jaswinder Pal Singh Walia *, Himanshu Tailor**, H S Mann ***,
Provision of Rotational Stability: Prevention of Collapse: Closed Fracture Reduction: Minimally Invasive Surgery with no Exposure of the Fracture:
 INTRODUCTION Percutaneous Compression Plating was developed by considering each of the stages in the surgical procedure for pertrochanteric fractures and the ways in which these might be improved. Primary
INTRODUCTION Percutaneous Compression Plating was developed by considering each of the stages in the surgical procedure for pertrochanteric fractures and the ways in which these might be improved. Primary
Fractures of the tibia shaft treated with locked intramedullary nail Retrospective clinical and radiographic assesment
 ARS Medica Tomitana - 2013; 4(75): 197-201 DOI: 10.2478/arsm-2013-0035 Șerban Al., Botnaru V., Turcu R., Obadă B., Anderlik St. Fractures of the tibia shaft treated with locked intramedullary nail Retrospective
ARS Medica Tomitana - 2013; 4(75): 197-201 DOI: 10.2478/arsm-2013-0035 Șerban Al., Botnaru V., Turcu R., Obadă B., Anderlik St. Fractures of the tibia shaft treated with locked intramedullary nail Retrospective
Periarticular knee osteotomy
 Periarticular knee osteotomy Turnberg Building Orthopaedics 0161 206 4803 All Rights Reserved 2018. Document for issue as handout. Knee joint The knee consists of two joints which allow flexion (bending)
Periarticular knee osteotomy Turnberg Building Orthopaedics 0161 206 4803 All Rights Reserved 2018. Document for issue as handout. Knee joint The knee consists of two joints which allow flexion (bending)
Trauma & Orthopaedic Undergraduate Syllabus
 Trauma & Orthopaedic Undergraduate Syllabus Introduction The purpose of this document is to provide a recommended syllabus for medical students in Trauma & Orthopaedics (T&0). It should help students on
Trauma & Orthopaedic Undergraduate Syllabus Introduction The purpose of this document is to provide a recommended syllabus for medical students in Trauma & Orthopaedics (T&0). It should help students on
Unicompartmental Knee Resurfacing
 Disclaimer This movie is an educational resource only and should not be used to manage knee pain. All decisions about the management of knee pain must be made in conjunction with your Physician or a licensed
Disclaimer This movie is an educational resource only and should not be used to manage knee pain. All decisions about the management of knee pain must be made in conjunction with your Physician or a licensed
Study of Ender s Nailing in Paediatric Tibial Shaft Fractures
 Study of Ender s Nailing in Paediatric Tibial Shaft Fractures Dr. Himanshu G. Ladani 1* 1 Ex. Assistant Professor of Orthopaedics, M.P.Shah Medical College, Jamnagar, Gujarat. ABSTRACT Background: Closed
Study of Ender s Nailing in Paediatric Tibial Shaft Fractures Dr. Himanshu G. Ladani 1* 1 Ex. Assistant Professor of Orthopaedics, M.P.Shah Medical College, Jamnagar, Gujarat. ABSTRACT Background: Closed
Fractures of the Ankle Region in the Skeletally Immature Patient. The Salter Classification is Worthless!!
 Fractures of the Ankle Region in the Skeletally Immature Patient. The Salter Classification is Worthless!! Kaye E Wilkins D.V.M,M.D. President's Council/Dielmann Chair in Pediatric Orthopedics Professor
Fractures of the Ankle Region in the Skeletally Immature Patient. The Salter Classification is Worthless!! Kaye E Wilkins D.V.M,M.D. President's Council/Dielmann Chair in Pediatric Orthopedics Professor
General Concepts. Growth Around the Knee. Topics. Evaluation
 General Concepts Knee Injuries in Skeletally Immature Athletes Zachary Stinson, M.D. Increased rate and ability of healing Higher strength of ligaments compared to growth plates Continued growth Children
General Concepts Knee Injuries in Skeletally Immature Athletes Zachary Stinson, M.D. Increased rate and ability of healing Higher strength of ligaments compared to growth plates Continued growth Children
Physeal Fractures and Growth Arrest
 Physeal Fractures and Growth Arrest Raymond W. Liu, M.D. Victor M. Goldberg Master Clinician-Scientist in Orthopaedics Rainbow Babies and Children s Hospital Case Western Reserve University Outline General
Physeal Fractures and Growth Arrest Raymond W. Liu, M.D. Victor M. Goldberg Master Clinician-Scientist in Orthopaedics Rainbow Babies and Children s Hospital Case Western Reserve University Outline General
Aesculap Targon FN. Head Preserving Solution for Medial Femoral Neck Fractures. Aesculap Orthopaedics
 Aesculap Targon FN Head Preserving Solution for Medial Femoral Neck Fractures Aesculap Orthopaedics Targon FN Operating Technique Indications for Targon FN AO 3 B. AO 3 B.2 AO 3 B.3 Undisplaced intracapsular
Aesculap Targon FN Head Preserving Solution for Medial Femoral Neck Fractures Aesculap Orthopaedics Targon FN Operating Technique Indications for Targon FN AO 3 B. AO 3 B.2 AO 3 B.3 Undisplaced intracapsular
The Kienböck disease and scaphoid fractures. Mariusz Bonczar
 The Kienböck disease and scaphoid fractures Mariusz Bonczar The Kienböck disease and scaphoid fractures Mariusz Bonczar Kienböck disease personal experience My special interest for almost 25 years Thesis
The Kienböck disease and scaphoid fractures Mariusz Bonczar The Kienböck disease and scaphoid fractures Mariusz Bonczar Kienböck disease personal experience My special interest for almost 25 years Thesis
Goals. Initial management skeletal trauma. Physical Exam ABC OF PRIMARY CARE MEDICINE FRACTURE MANAGEMENT 12/4/2010
 ABC OF PRIMARY CARE MEDICINE FRACTURE MANAGEMENT Brian Feeley, MD UCSF Sports Medicine and Shoulder Surgery Goals Discuss common fractures and initial management, treatment guidelines Let your patients
ABC OF PRIMARY CARE MEDICINE FRACTURE MANAGEMENT Brian Feeley, MD UCSF Sports Medicine and Shoulder Surgery Goals Discuss common fractures and initial management, treatment guidelines Let your patients
Y: Orthopedic Specialty
 Y: Orthopedic Specialty Alberta Licensed Practical Nurses Competency Profile 253 Major Competency Area: Y Priority: One Competency: Y-1 HPA Authorization and Standards Date: September 1, 2005 Y-1-1 Demonstrate
Y: Orthopedic Specialty Alberta Licensed Practical Nurses Competency Profile 253 Major Competency Area: Y Priority: One Competency: Y-1 HPA Authorization and Standards Date: September 1, 2005 Y-1-1 Demonstrate
EPIPHYSEAL PLATE IN FEMUR
 Reviewing: Epiphyseal Plates (younger skeletons) eventually will disappear. Bones grow lengthwise up and down from each plate, and in a circular collar like fashion around the diaphysis. These plates will
Reviewing: Epiphyseal Plates (younger skeletons) eventually will disappear. Bones grow lengthwise up and down from each plate, and in a circular collar like fashion around the diaphysis. These plates will
NICE guideline Published: 17 February 2016 nice.org.uk/guidance/ng38
 Fractures (non-complex): assessment and management NICE guideline Published: 17 February 2016 nice.org.uk/guidance/ng38 NICE 2017. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Fractures (non-complex): assessment and management NICE guideline Published: 17 February 2016 nice.org.uk/guidance/ng38 NICE 2017. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
11/5/14. I will try to make this painless. Great, a Fracture, Now What? Objectives. Basics for Fracture Workup. Basics for Fracture Workup
 Great, a Fracture, Now What? I will try to make this painless Mary Greve MS, PA-C Department of Orthopedic Surgery Trauma Team University of Iowa Hospitals and Clinics Mary-Greve@uiowa.edu Pager 2121 Objectives
Great, a Fracture, Now What? I will try to make this painless Mary Greve MS, PA-C Department of Orthopedic Surgery Trauma Team University of Iowa Hospitals and Clinics Mary-Greve@uiowa.edu Pager 2121 Objectives
Types of Plates 1. New Dynamic Compression Plate: Diaphyseal fracture: Radius, Ulna, Humerus, Rarely tibia
 Types of Plates 1. New Dynamic Compression Plate: DCP Diaphyseal fracture: Radius, Ulna, Humerus, Rarely tibia 1. Undercut adjacent to the holes low contact: less stress shield 2. Undercut at the undersurface
Types of Plates 1. New Dynamic Compression Plate: DCP Diaphyseal fracture: Radius, Ulna, Humerus, Rarely tibia 1. Undercut adjacent to the holes low contact: less stress shield 2. Undercut at the undersurface
Type I : At the level of lesser trochanter Type II : Less than 2.5 cm below lesser trochanter. Type III : cm below lesser trochanter
 Type II : Major fracture line along the intertrochanteric line with communition in coronal plain. Type III : Fracture at the level of lesser trochanter with variable communition and extension in subtrochanteric
Type II : Major fracture line along the intertrochanteric line with communition in coronal plain. Type III : Fracture at the level of lesser trochanter with variable communition and extension in subtrochanteric
FIBULAR & SYNDESMOSIS MALUNIONS
 FIBULAR & SYNDESMOSIS MALUNIONS MICHAEL P. CLARE, MD FLORIDA ORTHOPAEDIC INSTITUTE TAMPA, FL USA MORTISE INHERENTLY UNSTABLE LATERAL MALLEOLUS ACTS AS BUTTRESS / POST RESIST LATERAL TRANSLATION OF TALUS
FIBULAR & SYNDESMOSIS MALUNIONS MICHAEL P. CLARE, MD FLORIDA ORTHOPAEDIC INSTITUTE TAMPA, FL USA MORTISE INHERENTLY UNSTABLE LATERAL MALLEOLUS ACTS AS BUTTRESS / POST RESIST LATERAL TRANSLATION OF TALUS
CORE STANDARDS STANDARDS USED IN TARN REPORTS
 CORE STANDARDS Time to CT Scan BEST PRACTICE TARIFF SECTION 4.10 MAJOR TRAUMA 7 If the patient is admitted directly to the MTC or transferred as an emergency, the patient must be received by a trauma team
CORE STANDARDS Time to CT Scan BEST PRACTICE TARIFF SECTION 4.10 MAJOR TRAUMA 7 If the patient is admitted directly to the MTC or transferred as an emergency, the patient must be received by a trauma team
5/31/2018. Ipsilateral Femoral Neck And Shaft Fractures. Ipsilateral Neck-Shaft Fractures Introduction. Ipsilateral Neck-Shaft Fractures Introduction
 Ipsilateral Femoral Neck And Shaft Fractures Exchange Nailing For Non- Union Donald Wiss MD Cedars-Sinai Medical Center Los Angeles, California Introduction Uncommon Injury Invariably High Energy Trauma
Ipsilateral Femoral Neck And Shaft Fractures Exchange Nailing For Non- Union Donald Wiss MD Cedars-Sinai Medical Center Los Angeles, California Introduction Uncommon Injury Invariably High Energy Trauma
NE Nebraska Trauma Conference Tristan Hartzell, MD November 8, 2017
 NE Nebraska Trauma Conference 2017 Tristan Hartzell, MD November 8, 2017 Traumatic arm injuries in the elderly Fractures Hand Wrist Elbow Shoulder Soft tissue injuries Definitions Elderly? old or aging
NE Nebraska Trauma Conference 2017 Tristan Hartzell, MD November 8, 2017 Traumatic arm injuries in the elderly Fractures Hand Wrist Elbow Shoulder Soft tissue injuries Definitions Elderly? old or aging
Injuries to the Hands and Feet
 Injuries to the Hands and Feet Chapter 24 Injuries to the Hands and Feet Introduction Combat injuries to the hands and feet differ from those of the arms and legs in terms of mortality and morbidity. The
Injuries to the Hands and Feet Chapter 24 Injuries to the Hands and Feet Introduction Combat injuries to the hands and feet differ from those of the arms and legs in terms of mortality and morbidity. The
Fracture fixation. Types. Mechanical considerations. Biomechanics of fracture fixation. External fixation. Internal fixation
 Fracture fixation Biomechanics of fracture fixation Types External fixation Mechanical considerations Internal fixation Mechanical considerations in treatment of 1. In the external fixation: fracture When
Fracture fixation Biomechanics of fracture fixation Types External fixation Mechanical considerations Internal fixation Mechanical considerations in treatment of 1. In the external fixation: fracture When
Orthopedic Trauma. I have nothing to disclose. Objectives 3/7/2018. What is Orthopedic Trauma? What is Orthopedic Trauma? Trauma
 Orthopedic Trauma I have nothing to disclose. David Miller Memorial Trauma Symposium 2017 James Black, MD Mercy Orthopedic Trauma - Springfield 10/27/2017 Objectives What is Orthopedic Trauma? What is
Orthopedic Trauma I have nothing to disclose. David Miller Memorial Trauma Symposium 2017 James Black, MD Mercy Orthopedic Trauma - Springfield 10/27/2017 Objectives What is Orthopedic Trauma? What is
MIDFOOT INJURIES-ARE WE UNDERTREATING IT? Mr Rajiv Limaye Mr Prasad Karpe University Hospital of North Tees 3 rd Foot and Ankle Symposium
 MIDFOOT INJURIES-ARE WE UNDERTREATING IT? Mr Rajiv Limaye Mr Prasad Karpe University Hospital of North Tees 3 rd Foot and Ankle Symposium Introduction Increasing sports injuries RTA and traumatic injuries
MIDFOOT INJURIES-ARE WE UNDERTREATING IT? Mr Rajiv Limaye Mr Prasad Karpe University Hospital of North Tees 3 rd Foot and Ankle Symposium Introduction Increasing sports injuries RTA and traumatic injuries
Recurrent Fifth Metatarsal Fractures. Carol Frey MD Fellowship Co - Director West Coast Sports Medicine Foundation UCLA Manhattan Beach, California
 Recurrent Fifth Metatarsal Fractures Carol Frey MD Fellowship Co - Director West Coast Sports Medicine Foundation UCLA Manhattan Beach, California General 5th MT fracture fairly common Mechanism: Hindfoot
Recurrent Fifth Metatarsal Fractures Carol Frey MD Fellowship Co - Director West Coast Sports Medicine Foundation UCLA Manhattan Beach, California General 5th MT fracture fairly common Mechanism: Hindfoot
Post test for O&P 2 Hrs CE. The Exam
 Post test for O&P 2 Hrs CE The Exam This examination is taken in "open book" format. That means you are free to answer the questions after research or discussion with your fellow workers. We feel this
Post test for O&P 2 Hrs CE The Exam This examination is taken in "open book" format. That means you are free to answer the questions after research or discussion with your fellow workers. We feel this
PediLoc Extension Osteotomy Plate (PLEO)
") PediLoc Extension Osteotomy Plate (PLEO) Left PLEO Plates Sizes: 6, 8 and 10 hole plates Right PLEO Plates Sizes: 6, 8 and 10 hole plates PediLoc Extension Osteotomy Plate The technique description herein
PediLoc Extension Osteotomy Plate (PLEO) Left PLEO Plates Sizes: 6, 8 and 10 hole plates Right PLEO Plates Sizes: 6, 8 and 10 hole plates PediLoc Extension Osteotomy Plate The technique description herein
Principles of Musculoskeletal Injuries
 Principles of Musculoskeletal Injuries Wiroon Laupattarakasem, M.D. Professor in Orthopaedics Faculty of Medicine Khon Kaen University Contents: Fractures and Dislocations Mechanisms of injuries Description
Principles of Musculoskeletal Injuries Wiroon Laupattarakasem, M.D. Professor in Orthopaedics Faculty of Medicine Khon Kaen University Contents: Fractures and Dislocations Mechanisms of injuries Description
Contents SECTION 1: GENERAL TRAUMA AND RECONSTRUCTIVE HIP SURGERY
 SECTION 1: GENERAL TRAUMA AND RECONSTRUCTIVE HIP SURGERY 1. Acetabular and Pelvic Fractures...3 2. Acetabular Orientation (Total Hips)...6 3. Acetabular Osteotomy...7 4. Achilles Tendon Ruptures...9 5.
SECTION 1: GENERAL TRAUMA AND RECONSTRUCTIVE HIP SURGERY 1. Acetabular and Pelvic Fractures...3 2. Acetabular Orientation (Total Hips)...6 3. Acetabular Osteotomy...7 4. Achilles Tendon Ruptures...9 5.
Bone Injuries and Treatment. Fractures and Dislocations
 Bone Injuries and Treatment Fractures and Dislocations Bellwork Research the small bones in the foot and wrist. Draw them in your notes. State Standards 16) Understand principles of and successfully perform
Bone Injuries and Treatment Fractures and Dislocations Bellwork Research the small bones in the foot and wrist. Draw them in your notes. State Standards 16) Understand principles of and successfully perform
Radial head fractures; ORIF radial head; radial head arthroplasty; coronoid process fracture; ligament repair Elbow Anatomy Spectrum of injuries
 Radial head fractures; ORIF radial head; radial head arthroplasty; coronoid process fracture; ligament repair This information aims to help you understand your condition and gain maximum benefit from your
Radial head fractures; ORIF radial head; radial head arthroplasty; coronoid process fracture; ligament repair This information aims to help you understand your condition and gain maximum benefit from your
UNDERSTANDING FRACTURE CARE CAUSES, DIAGNOSIS, AND TREATMENT
 UNDERSTANDING FRACTURE CARE CAUSES, DIAGNOSIS, AND TREATMENT PremierOrtho.com UNDERSTANDING FRACTURE CARE CAUSES, DIAGNOSIS, AND TREATMENT Table of Contents Introduction...3 Causes...4 Who s at Risk?...5
UNDERSTANDING FRACTURE CARE CAUSES, DIAGNOSIS, AND TREATMENT PremierOrtho.com UNDERSTANDING FRACTURE CARE CAUSES, DIAGNOSIS, AND TREATMENT Table of Contents Introduction...3 Causes...4 Who s at Risk?...5
Index. B Backslap technique depth assessment, 82, 83 diaphysis distal trocar, 82 83
 Index A Acromial impingement, 75, 76 Aequalis intramedullary locking avascular necrosis, 95 central humeral head, 78, 80 clinical and functional outcomes, 95, 96 design, 77, 79 perioperative complications,
Index A Acromial impingement, 75, 76 Aequalis intramedullary locking avascular necrosis, 95 central humeral head, 78, 80 clinical and functional outcomes, 95, 96 design, 77, 79 perioperative complications,