Pediatric foot. Razan Krishan
|
|
|
- Ashley Dixon
- 5 years ago
- Views:
Transcription
1
2 Pediatric foot Razan Krishan
3
4 The ankle includes three joints: 1- the ankle joint proper (tibiotalar) plantarflexion and dorsiflexion 2- the subtalar joint inversion and eversion 3- the Inferior tibiofibular joint.
5 Glossary of foot postures Plantigrade is the normal neutral position of the foot i.e. when the patient stands the sole is at right angles to the leg. Talipes equinus refers to the shape of a horse s foot i.e. the hindfoot is fixed in plantarflexion (pointing downwards). Plantaris looks similar, but the ankle is neutral and only the forefoot is plantarflexed. Equinovarus describes a foot that points both downwards and inwards. Calcaneus is fixed dorsiflexion at the ankle. A dorsiflexion deformity in the midfoot produces a rocker-bottom foot.


6
7 Congenital Talipes equinovarus (CTEV) club foot
 ankle joint: plantarflexed/equines (ii) subtalar joint inverted/varus (iii) forefoot adducted In a normal baby the foot can be dorsiflexed and everted until the toes")
8 Talipes (means foot), Equino (means flexed), Varus (means twisted internally). Also, it comes with adduction of the forefoot. In this deformity the foot is curved downwards and inwards. Three main deformities: (i) ankle joint: plantarflexed/equines (ii) subtalar joint inverted/varus (iii) forefoot adducted In a normal baby the foot can be dorsiflexed and everted until the toes almost touch the front of the leg. In club-foot this manoeuvre meets with varying degrees of resistance and in severe cases the deformity is fixed.
9 Incidence : Common birth defect 1:1000 Male: Female 2:1 50% bilateral. A family history increases the risk by times.
10 Classification of CTEV: Postural (physiologic): the deformity can be easily corrected by the examiner, not considered a real club foot. Fixed (pathologic): could be idiopathic (most common), syndromatic (comes with other congenital deformities,ex;myelomeningocele and arthrogryposis.)
11 Diagnosis Diagnosis is clinically, no need for X-ray. Newborn babies have only calcified calcaneus, talus, cuboid (we see them on x-ray), we don't see the navicular bone Can be detected on US, but nothing can be done.
12 Treatment depends on the age mainly or recurrence: 1- Less than 3 months we treat it conservatively by Ponseti method which includes: Serial casting (supination of the foot), fix point: talar neck. Tendo-achilles lengthening, needed in 70% of patients. Bracing (Dennis- brown) Tibialis tendon transfer. 2- More than 3 months or recurrent: surgery. By complete soft tissue release usually performed at 6-12 months. The goal is to correct all the components of the clubfoot deformity at the time of surgery.
13 Congenital vertical talus (rockerbottom foot)
14 Irreducible dorsal dislocation of the navicular on the talus producing a rigid flatfoot deformity: irreducible dorsolateral navicular dislocation vertically oriented talus calcaneal eversion with attenuated spring ligament soft tissue contractures: displacement of peroneal longus and posterior tibialis tendon so they function as dorsiflexors rather than plantar flexors contracture of the Achilles tendon Worse prognosis than club foot.

15
16 incidence High incidence with various congenital anomalies and neuromuscular diseases; such as: Myelomeningocele DDH Arthrogryposis Trisomy 13 Marfan syndrome
17 Clinical presentation : Rigid rocker-bottom deformity: fixed hindfoot equinovalgus due to contracture of the Achilles and peroneal tendons rigid midfoot dorsiflexion secondary to the dislocated navicular forefoot abducted and dorsiflexed Treatment by serial casting if failed surgery.
18 Pes planus flat foot
19 The term flat-foot applies when the apex of the longitudinal arch has collapsed and the medial border of the foot is in contact (or nearly in contact) with the ground; the heel becomes valgus and the foot pronates at the midfoot. The appearance of flat-foot can be normal and without symptoms but some conditions are characterized by flat-feet that are stiff and painful.
20 Classified into either: 1. Rigid (Stiff,which cannot be corrected passively should), caused by Congenital vertical talus Coalition of tarsals (calcaionavicular,(often a bar of bone connecting the calcaneus to the talus or the navicular) Juvenile chronic arthritis. 2. Flexible (Mobile,most common), asymptomatic but is associated with peroneal spasm. often appears in toddlers as a normal stage in development, and it usually disappears after a few years when medial arch development is complete. Ask the patient to stand on his tip toes and look from behind, heel valgus corrects on tip toe and the medial arch appears on extending the great toe at MTP joint.
21 Clinical assessment The deformity becomes noticeable when the youngster stands. The first test is to ask him or her to go up on their toes: if the heels invert and the medial arches form up, it is probably a flexible (or mobile) deformity. This can be checked by performing the jack test (also called the great toe extension test): with the child seated, feet planted firmly on the floor, the examiner firmly dorsiflexes the great toe; the medial arch should re-appear
22 treatment Physiologic flexible flat foot: reassurance deformity will probably correct itself in time. (Medial arch support only if there was genuine medial foot pain, but this doesn t get rid of the flat foot deformity.) Rigid type needs surgery.
23 Pes cavus Foot is highly arched and the toes are drawn up into a clawed position, forcing the metatarsal heads down into the sole. Think of abnormal neurology until proven otherwise Treat according to symptoms no pain, no surgery can be seen in neurological disorders (Neurological examination is important), where the intrinsic muscles are weak or paralysed, suggests that all forms of pes cavus are due to some type of muscle imbalance.

24
25 Common deformities of the toes are: lateral deviation of the big toe (hallux valgus), proximal interphalangeal flexion of one of the lesser toes (hammertoe) flexion of both interphalangeal joints of several toes (claw-toes )
26 FRACTURES IN CHILDREN Marah Marahleh
27 FRACTURES IN CHILDREN Fractures in growing bones are subject to influences which do not apply to adult bones : 1. The presence of growth plate increases longitudinal growth 2. The presence of perichondral plate increases the bone thickness 3. In very young children, the bone ends are largely cartilaginous and therefore do not show up in x-ray images. Fractures at these sites are difficult to diagnose; it helps to x-ray both limbs and compare the appearances on the two sides. 4. Children s bones are less brittle, and more liable to plastic deformation, than those of adults. Hence the frequency of incomplete fractures torus fractures (buckling of the cortex) and greenstick fractures, injuries which are very rare in adults. 5. The periosteum is thicker than in adult bones; this may explain why fracture displacement is more controlled. Cellular activity is also more marked, which is why children s fractures heal so much more rapidly than those of adults. The younger the child, the quicker is the rate of union. Femoral shaft fractures in infants will heal within 3 weeks, and in young children in 4 6 weeks, compared to 14 weeks or longer in adults.
28 6. Non-union is very unusual. 7. Bone growth involves modelling and remodelling, processes which determine the structure and overall form of the bone. This makes for a considerable capacity to reshape fracture deformities (other than rotational deformities) over time. 8. Injuries of the physis have no equivalent in adults. Damage to the growth plate can have serious consequences however rapidly and securely the fracture might heal. Common sites of bone fracture according to age group seen on X-ray - Infants: diaphysis (midshaft) 1st site of ossification - Toddlers: metaphysis - Adolescent: epiphysis
29 Fractures of the growth plate The epiphyseal plate (growth plate) is a hyaline cartilage plate in the metaphysis at each end of a long bone. It is the part of a long bone where new bone growth takes place. The plate is found in children and adolescents; in adults, who have stopped growing, the plate is replaced by an epiphyseal line. This replacement is known as epiphyseal closure. 14 years old +/- 2 years is the age of growth plate closing Transitional fractures occur in this period.
![Layers of growth plate: 1. Germinal : the most important, the source of all layers and it s the first layer near the epiphysis. [Remember: Growth is from epiphysis toward metaphysis] 2.](/docs-images/96/127042139/images/30-0.jpg "Proliferative 3. Hypertrophic : the weakest; because of increased size of cells so less number of cells in same area + increase fluids and less connections between cells. 4.")
30 Layers of growth plate: 1. Germinal : the most important, the source of all layers and it s the first layer near the epiphysis. [Remember: Growth is from epiphysis toward metaphysis] 2. Proliferative 3. Hypertrophic : the weakest; because of increased size of cells so less number of cells in same area + increase fluids and less connections between cells. 4. Zone of provisional calcification

31
32 Fractures of the growth plate More than 10 per cent of childhood fractures involve injury to the physis (or growth plate). The fracture usually runs transversely through the hypertrophic (calcified) layer of the growth plate, often veering off towards the shaft to include a triangular piece of the metaphysis. This has little effect on longitudinal growth, which takes place in the germinal and proliferating layers of the physis. However, if the fracture traverses the cellular reproductive layers of the plate, it may result in premature ossification of the injured part and cessation of growth or deformity of the bone end.

33 Classification The most widely used classification of physeal injuries is that of Salter and Harris, which distinguishes five basic types of injury. Type 1 A transverse fracture through the hypertrophic or calcified zone of the plate. Even if the fracture is quite alarmingly displaced, the growing zone of the physis is usually not injured and growth disturbance is uncommon. Type 2 This is similar to type 1, but towards the edge the fracture deviates away from the physis and splits off a triangular piece of metaphyseal bone. Growth is usually not affected.
34 Type 3 A fracture running partly along the physis and then veering off through the epiphysis into the joint. Inevitably it damages the reproductive zone of the physis and may result in growth disturbance. Type 4 As with type 3, the fracture splits the epiphysis, but it continues through the physis into the metaphysis. These fractures are particularly liable to displacement and a consequent misfit between the separated parts of the physis, resulting in asymmetrical growth. Type 5 A longitudinal compression injury of the physis. There is no visible fracture, but the growth plate is crushed and this may result in growth arrest, diagnosed after long time like for example one year with retrospective history of falling down because nothing seen on x-ray acutely, after one year you see shortening of limb disproportionately. You can not prevent it!



35


36
37 The higher the grade of classification the higher the severity, the worse the prognosis, with the younger the age (5>4>3>2>1)
38 Clinical Features Physeal fractures usually result from falls or traction injuries; they occur mostly in road accidents and during sport or playground activities and are more common in boys than in girls. Deformity is usually minimal, but any injury in a child followed by pain and tenderness near the joint should arouse suspicion, and x-ray examination is essential.
39 X-ray The physis itself is radiolucent and the epiphysis may be incompletely ossified; this makes it hard to tell whether the bone end is damaged or deformed. The younger the child, the smaller the visible part of the epiphysis and thus the more difficult it is to make the diagnosis; comparison with the normal side is a great help. Tell-tale features are widening of the physeal gap, incongruity of the joint or tilting of the epiphyseal axis. if there is the faintest suspicion of a physeal fracture, a second x-ray examination after 4 or 5 days is essential. Type 5 injuries are usually diagnosed only in retrospect.
40
41 Treatment 1. Undisplaced fractures : These may be treated by splinting the part in a cast or a closefitting plaster slab for 2 4 weeks (depending on the site of injury and the age of the child). However, with type 3 and 4 fractures, a check x- ray after 4 days and again at about 10 days is mandatory in order not to miss late displacement.
42 2. Displaced fractures : must be reduced as soon as possible. With types 1 and 2, this can usually be done closed; the part is then splinted securely for 3 6 weeks. Type 3 and 4 fractures demand perfect anatomical reduction. An attempt can be made to achieve this by gentle manipulation under general anaesthesia; if this is successful, the limb is held in a cast for 4 8 weeks (the longer periods for type 4 injuries). Here again, check x-rays at about 4 and 10 days are essential to ensure that the position has been retained. If a type 3 or 4 fracture cannot be reduced accurately by closed manipulation, immediate open reduction and internal fixation is called for. The limb is then splinted for 4 6 weeks, but it takes that long again before the child is ready to resume unrestricted activities
43 1. Premature fusion Complications Type 1 and 2 injuries, if properly reduced, usually have an excellent prognosis and bone growth is not adversely affected. Exceptions to this rule are injuries involving the distal femoral and proximal tibial physes; both are undulating in shape, so a transverse fracture may pass through several zones in the physis and result in a focal point of fusion. Type 3, 4 and 5 injuries are more likely to cause premature fusion of part of the growth plate, resulting in cessation of growth or asymmetrical growth and deformity of the bone end.
44 2. Deformity Established deformity, whether from asymmetrical growth or from malunion of a displaced fracture (e.g. a valgus elbow due to proximal displacement or nonunion of a lateral humeral condylar fracture), should be treated by corrective osteotomy. If further growth is abnormal, the osteotomy may have to be repeated
45 FRACTURES OF THE DISTAL HUMERUS IN CHILDREN The elbow is second only to the distal forearm for frequency of fractures in children. Most of these injuries are supracondylar fractures, the remainder being divided between condylar, epicondylar and proximal radial and ulnar fractures. Boys are injured more often than girls and more than half the patients are under 10 years old. The usual accident is a fall directly on the point of the elbow or onto the outstretched hand with the elbow forced into valgus or varus. Pain and swelling are often marked and examination is difficult. X-ray interpretation also has its problems: the bone ends are largely cartilaginous and therefore radiographically incompletely visualized

46 Normal Anatomy

47 Normal Anatomy
48 Supracondylar Fractures These are among the commonest fractures in children. The distal fragment may be displaced and/or tilted either posteriorly or anteriorly, medially or laterally; sometimes it is also rotate. Posterior displacement and tilt is the commonest (95 per cent of all cases), suggesting a hyperextension injury, usually due to a fall on the outstretched hand. The jagged end of the proximal fragment pokes into the soft tissues anteriorly, sometimes injuring the brachial artery or median nerve. Anterior displacement is rare, but may result from over-reduction of the usual posterior displacements.


49

50
51 * Extension type Posterior displacement of the distal fragment
52 * Flexion Type Anterior displacement of the distal fragment.

53
54 Special features Following a fall, the child is in pain and the elbow is swollen; with a posteriorly displaced fracture, the S-deformity of the elbow is usually obvious It is essential to feel the pulse and check the capillary return.
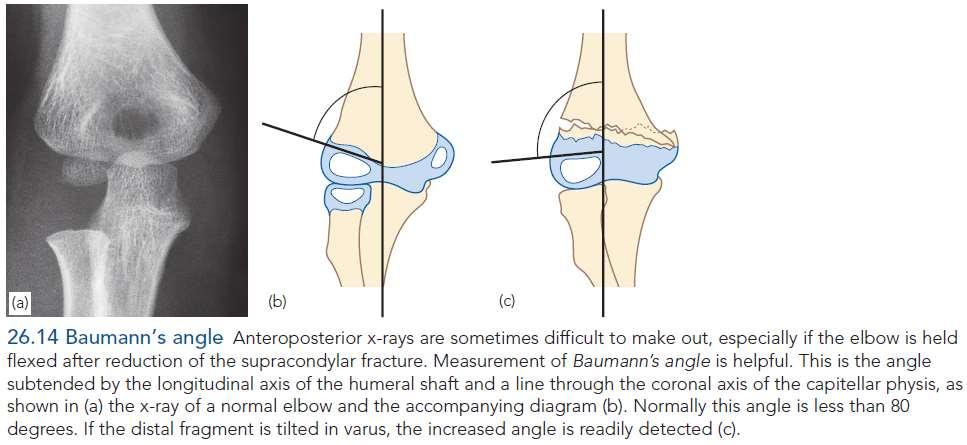
55 X ray Undisplaced fractures are easily missed; there may be no more than subtle features of a soft-tissue haematoma. The anteroposterior x-ray is often difficult to interpret because it is taken with the elbow flexed. The degree of sideways tilt (angulation) may therefore not be appreciated. This is where Baumann s angle is most helpful; wherever possible it should be accurately measured and compared with that of the uninjured side more than 5 degree variation indicate coronal plate deformity and is not accepted Baumann s angle : This is the angle subtended by the longitudinal axis of the humeral shaft and a line through the coronal axis of the capitellar physis,. Normally this angle is less than 80 degrees. If the distal fragment is tilted in varus, the increased angle is readily detected.
56
57 Treatment If there is even a suspicion of a fracture, the elbow is gently splinted in 30 degrees of flexion to prevent movement and possible neurovascular injury during the x-ray examination. 1. Undisplaced fractures The elbow is immobilized at 90 degrees and neutral rotation in a light-weight splint or cast and the arm is supported by a sling. It is essential to obtain an x-ray 5 7 days later to check that there has been no displacement. The splint is retained for 3 weeks and supervised movement is then allowed.
58 Treatment 2. Posteriorly angulated fracture If the posterior cortices are in continuity, the fracture can be reduced under general anaesthesia by the following step-wise manoeuvre: (1) traction for 2 3 minutes in the length of the arm with countertraction above the elbow; (2) correction of any sideways tilt or shift and rotation (in comparison with the other arm); (3) gradual flexion of the elbow to 120 degrees, and pronation of the forearm, while maintaining traction and exerting finger pressure behind the distal fragment to correct posterior tilt.
59 X-rays are taken to confirm reduction, checking carefully to see that there is no varus or valgus angulation and no rotational deformity. If the acutely flexed position cannot be maintained without disturbing the circulation, or if the reduction is unstable, the fracture should be fixed with percutaneous crossed Kirschner wires (take care not to skewer the ulnar nerve!). Following reduction, the arm is held in a collar and cuff; the circulation should be checked repeatedly during the first 24 hours. An x- ray is obtained after 3 5 days to confirm that the fracture has not slipped. If it has, do not delay a further attempt at reduction is still possible. If reduction is satisfactory, the splint is retained for 3 weeks, after which movements are begun.
60 Treatment 3. Posteriorly displaced fractures These are usually associated with severe swelling, are difficult to reduce and are often unstable; moreover, there is a considerable risk of neurovascular injury or circulatory compromise due to swelling. The fracture should be reduced under general anaesthesia as soon as possible, by the method described above, and then held with percutaneous crossed Kirschner wires; this obviates the necessity to hold the elbow acutely flexed. Care should be taken not to injure the ulnar and radial nerves. Postoperative management is the same as for simple angulated fractures.
61 Treatment 4. Anteriorly displaced fractures The fracture is reduced by pulling on the forearm with the elbow semi-flexed, applying thumb pressure over the front of the distal fragment and then extending the elbow fully. A posterior slab is bandaged on and retained for 3 weeks. Thereafter, the child is allowed to regain flexion gradually.
62 Complications 1. Vascular injury : The great danger of supracondylar fracture is injury to the brachial artery 2. Nerve injury : The median nerve may be injured. Fortunately, loss of function is usually temporary and recovery can be expected in 6 8 weeks 3. Malunion : Malunion is common Cubitus varus is disfiguring and cubitus valgus may cause late ulnar palsy. If deformity is marked, it will need correction by supracondylar osteotomy.
63 Complications 4. Elbow stiffness : Full movement may take months to return and must not be hurried. Forced movement will only make matters worse and may contribute to the development of heterotopic ossification.
64 Thank you
Pediatric Fractures. Objectives. Epiphyseal Complex. Anatomy and Physiology. Ligaments. Bony matrix
 1 Pediatric Fractures Nicholas White, MD Assistant Professor of Pediatrics Eastern Virginia Medical School Attending, Pediatric Emergency Department Children s Hospital of The King s Daughters Objectives
1 Pediatric Fractures Nicholas White, MD Assistant Professor of Pediatrics Eastern Virginia Medical School Attending, Pediatric Emergency Department Children s Hospital of The King s Daughters Objectives
PEM GUIDE CHILDHOOD FRACTURES
 PEM GUIDE CHILDHOOD FRACTURES INTRODUCTION Skeletal injuries account for 10-15% of all injuries in children; 20% of those are fractures, 3 out of 4 fractures affect the physis or growth plate. Always consider
PEM GUIDE CHILDHOOD FRACTURES INTRODUCTION Skeletal injuries account for 10-15% of all injuries in children; 20% of those are fractures, 3 out of 4 fractures affect the physis or growth plate. Always consider
Fractures and dislocations around elbow in adult
 Lec: 3 Fractures and dislocations around elbow in adult These include fractures of distal humerus, fracture of the capitulum, fracture of the radial head, fracture of the olecranon & dislocation of the
Lec: 3 Fractures and dislocations around elbow in adult These include fractures of distal humerus, fracture of the capitulum, fracture of the radial head, fracture of the olecranon & dislocation of the
Physical Examination of the Foot & Ankle
 Inspection Standing, feet straight forward facing toward examiner Swelling Deformity Flatfoot (pes planus and hindfoot valgus) High arch (pes cavus and hindfoot varus) Peek-a-boo heel Varus Too many toes
Inspection Standing, feet straight forward facing toward examiner Swelling Deformity Flatfoot (pes planus and hindfoot valgus) High arch (pes cavus and hindfoot varus) Peek-a-boo heel Varus Too many toes
Scar Engorged veins. Size of the foot [In clubfoot, small foot]
![Scar Engorged veins. Size of the foot [In clubfoot, small foot]](/thumbs/78/77722241.jpg "Scar Engorged veins. Size of the foot [In clubfoot, small foot]") 6. FOOT HISTORY Pain: Walking, Running Foot wear problem Swelling; tingly feeling Deformity Stiffness Disability: At work; recreation; night; walk; ADL, Sports Previous Rx Comorbidities Smoke, Sugar, Steroid
6. FOOT HISTORY Pain: Walking, Running Foot wear problem Swelling; tingly feeling Deformity Stiffness Disability: At work; recreation; night; walk; ADL, Sports Previous Rx Comorbidities Smoke, Sugar, Steroid
Upper Extremity Injury Management. Jonathan Pirie MD, Med, FRCPC, FAAP
 Upper Extremity Injury Management Jonathan Pirie MD, Med, FRCPC, FAAP Learning Objectives At the end of this session, you will be able to manage common fractures of the: 1. Humerus 2. Elbow 3. Forearm
Upper Extremity Injury Management Jonathan Pirie MD, Med, FRCPC, FAAP Learning Objectives At the end of this session, you will be able to manage common fractures of the: 1. Humerus 2. Elbow 3. Forearm
Copyright 2004, Yoshiyuki Shiratori. All right reserved.
 Ankle and Leg Evaluation 1. History Chief Complaint: A. What happened? B. Is it a sharp or dull pain? C. How long have you had the pain? D. Can you pinpoint the pain? E. Do you have any numbness or tingling?
Ankle and Leg Evaluation 1. History Chief Complaint: A. What happened? B. Is it a sharp or dull pain? C. How long have you had the pain? D. Can you pinpoint the pain? E. Do you have any numbness or tingling?
Evidence-Based Examination of the Foot Presented by Alexis Wright, PT, PhD, DPT, FAAOMPT Practice Sessions/Skill Check-offs
 Evidence-Based Examination of the Foot Presented by Alexis Wright, PT, PhD, DPT, FAAOMPT Practice Sessions/Skill Check-offs Module Five: Movement Assessment of the Foot/Ankle (1 hour CEU Time) Skilled
Evidence-Based Examination of the Foot Presented by Alexis Wright, PT, PhD, DPT, FAAOMPT Practice Sessions/Skill Check-offs Module Five: Movement Assessment of the Foot/Ankle (1 hour CEU Time) Skilled
International Journal of Biological & Medical Research
 Int J Biol Med Res. 2013; 4(1): 2986-2990 Int J Biol Med Res Volume 3, Issue 1, Jan 2012 www.biomedscidirect.com BioMedSciDirect Publications Contents lists available at BioMedSciDirect Publications International
Int J Biol Med Res. 2013; 4(1): 2986-2990 Int J Biol Med Res Volume 3, Issue 1, Jan 2012 www.biomedscidirect.com BioMedSciDirect Publications Contents lists available at BioMedSciDirect Publications International
FACTS 1. Most need only Gastro aponeurotic release [in positive Silverskiold test]
![FACTS 1. Most need only Gastro aponeurotic release [in positive Silverskiold test]](/thumbs/83/88335212.jpg "FACTS 1. Most need only Gastro aponeurotic release [in positive Silverskiold test]") FOOT IN CEREBRAL PALSY GAIT IN CEREBRAL PALSY I True Equinus II Jump gait III Apparent Equinus IV Crouch gait Group I True Equinus Extended hip and knee Equinus at ankle II Jump Gait [commonest] Equinus
FOOT IN CEREBRAL PALSY GAIT IN CEREBRAL PALSY I True Equinus II Jump gait III Apparent Equinus IV Crouch gait Group I True Equinus Extended hip and knee Equinus at ankle II Jump Gait [commonest] Equinus
Childhood Fractures. Incomplete fractures more common. Ligaments stronger than bone. Tendons stronger than bone. Fractures may be pathologic
 Childhood Fractures Incomplete fractures more common Plastic bowing Torus / Buckle Greenstick Ligaments stronger than bone Fracture patterns different Physeal injury, not dislocation Tendons stronger than
Childhood Fractures Incomplete fractures more common Plastic bowing Torus / Buckle Greenstick Ligaments stronger than bone Fracture patterns different Physeal injury, not dislocation Tendons stronger than
Foot and Ankle Natalie Stork, MD
 Foot and Ankle Natalie Stork, MD Assistant Professor University of Missouri-Kansas City School of Medicine, Department of Orthopaedic Surgery and Department of Pediatrics Children s Mercy Kansas City,
Foot and Ankle Natalie Stork, MD Assistant Professor University of Missouri-Kansas City School of Medicine, Department of Orthopaedic Surgery and Department of Pediatrics Children s Mercy Kansas City,
Dorsal surface-the upper area or top of the foot. Terminology
 It is important to learn the terminology as it relates to feet to properly communicate with referring physicians when necessary and to identify the relationship between the anatomical structure of the
It is important to learn the terminology as it relates to feet to properly communicate with referring physicians when necessary and to identify the relationship between the anatomical structure of the
Therapeutic Foot Care Certificate Program Part I: Online Home Study Program
 Therapeutic Foot Care Certificate Program Part I: Online Home Study Program 1 Anatomy And Terminology Of The Lower Extremity Joan E. Edelstein, MA, PT, FISPO Associate Professor of Clinical Physical Therapy
Therapeutic Foot Care Certificate Program Part I: Online Home Study Program 1 Anatomy And Terminology Of The Lower Extremity Joan E. Edelstein, MA, PT, FISPO Associate Professor of Clinical Physical Therapy
Other Upper Extremity Trauma. Inje University Sanggye Paik Hospital Yong-Woon Shin
 Other Upper Extremity Trauma Inje University Sanggye Paik Hospital Yong-Woon Shin Forearm Fractures Forearm fractures - the most common orthopaedic injuries in children - 30-50% of all pediatric fractures
Other Upper Extremity Trauma Inje University Sanggye Paik Hospital Yong-Woon Shin Forearm Fractures Forearm fractures - the most common orthopaedic injuries in children - 30-50% of all pediatric fractures
Surgical Care at the District Hospital. EMERGENCY & ESSENTIAL SURGICAL CARE
 Surgical Care at the District Hospital 1 18 Orthopedic Trauma Key Points 2 18.1 Upper Extremity Injuries Clavicle Fractures Diagnose fractures from the history and by physical examination Treat with a
Surgical Care at the District Hospital 1 18 Orthopedic Trauma Key Points 2 18.1 Upper Extremity Injuries Clavicle Fractures Diagnose fractures from the history and by physical examination Treat with a
Radiographic Assessment of Pediatric Foot Alignment: Self-Assessment Module
 1.5 CME AJR Integrative Imaging LIFELONG LEARNING FOR RADIOLOGY Radiographic Assessment of Pediatric Foot Alignment: Self-Assessment Module Mahesh M. Thapa 1,2, Sumit Pruthi 1,2, Felix S. Chew 2 ABSTRACT
1.5 CME AJR Integrative Imaging LIFELONG LEARNING FOR RADIOLOGY Radiographic Assessment of Pediatric Foot Alignment: Self-Assessment Module Mahesh M. Thapa 1,2, Sumit Pruthi 1,2, Felix S. Chew 2 ABSTRACT
Metatarsus adductus, Skew foot, Club foot 성균관대학교삼성창원병원 장현정
 Metatarsus adductus, Skew foot, Club foot 성균관대학교삼성창원병원 장현정 Metatarsus adductus Epidemiology and Etiology 0.1-12% with higher number for multiple birth Deformation and compression from intrauterine crowding
Metatarsus adductus, Skew foot, Club foot 성균관대학교삼성창원병원 장현정 Metatarsus adductus Epidemiology and Etiology 0.1-12% with higher number for multiple birth Deformation and compression from intrauterine crowding
Other Congenital and Developmental Diseases of the Foot. Department of Orthopedic Surgery St. Vincent s s Hospital, The Catholic University
 Other Congenital and Developmental Diseases of the Foot Department of Orthopedic Surgery St. Vincent s s Hospital, The Catholic University Contents Metatarsus Adductus Skewfoot Hallux Valgus Hallux Valgus
Other Congenital and Developmental Diseases of the Foot Department of Orthopedic Surgery St. Vincent s s Hospital, The Catholic University Contents Metatarsus Adductus Skewfoot Hallux Valgus Hallux Valgus
Fractures of the shoulder girdle, elbow and fractures of the humerus. H. Sithebe 2012
 Fractures of the shoulder girdle, elbow and fractures of the humerus H. Sithebe 2012 Fractures of the Clavicle (mid-shaft). Fractures of the clavicle Fractures of the clavicle Treatment- conservative.
Fractures of the shoulder girdle, elbow and fractures of the humerus H. Sithebe 2012 Fractures of the Clavicle (mid-shaft). Fractures of the clavicle Fractures of the clavicle Treatment- conservative.
Cavus Foot: Subtle and Not-So-Subtle AOFAS Resident Review Course September 28, 2013
 Cavus Foot: Subtle and Not-So-Subtle Course September 28, 2013 Matthew M. Roberts, MD Associate Professor of Clinical Orthopaedic Surgery Co-Chief, Foot and Ankle Service Hospital for Special Surgery Disclosure
Cavus Foot: Subtle and Not-So-Subtle Course September 28, 2013 Matthew M. Roberts, MD Associate Professor of Clinical Orthopaedic Surgery Co-Chief, Foot and Ankle Service Hospital for Special Surgery Disclosure
Upper Extremity Fractures
 Upper Extremity Fractures Ranie Whatley, RN,FNP-C David W. Gray, MD Skeletal Trauma 10 to 15 % of all Childhood Injuries Physeal (Growth Plate) Injuries are ~ 15% of all Skeletal Injuries Orthopaedic Assessment
Upper Extremity Fractures Ranie Whatley, RN,FNP-C David W. Gray, MD Skeletal Trauma 10 to 15 % of all Childhood Injuries Physeal (Growth Plate) Injuries are ~ 15% of all Skeletal Injuries Orthopaedic Assessment
Clarification of Terms
 Clarification of Terms The plantar aspect of the foot refers to the role or its bottom The dorsal aspect refers to the top or its superior portion The ankle and foot perform three main functions: 1. shock
Clarification of Terms The plantar aspect of the foot refers to the role or its bottom The dorsal aspect refers to the top or its superior portion The ankle and foot perform three main functions: 1. shock
Chapter XIX.1. Fractures May 2002
 Case Based Pediatrics For Medical Students and Residents Department of Pediatrics, University of Hawaii John A. Burns School of Medicine Chapter XIX.1. Fractures May 2002 Annemarie Uliasz The skeletal
Case Based Pediatrics For Medical Students and Residents Department of Pediatrics, University of Hawaii John A. Burns School of Medicine Chapter XIX.1. Fractures May 2002 Annemarie Uliasz The skeletal
BIOMECHANICAL EXAMINATION OF THE PEDIATRIC LOWER EXTREMITY
 BIOMECHANICAL EXAMINATION OF THE PEDIATRIC LOWER EXTREMITY B.Resseque, D.P.M. ARCH HEIGHT OFF WEIGHTBEARING Evaluate arch height by placing a ruler from the heel to the first metatarsal head Compare arch
BIOMECHANICAL EXAMINATION OF THE PEDIATRIC LOWER EXTREMITY B.Resseque, D.P.M. ARCH HEIGHT OFF WEIGHTBEARING Evaluate arch height by placing a ruler from the heel to the first metatarsal head Compare arch
Fractures of the Hand in Children Which are simple? And Which have pitfalls??
 Fractures of the Hand in Children Which are simple? And Which have pitfalls?? Kaye E Wilkins DVM, MD Professor of Orthopedics and Pediatrics Departments of Orthopedics and Pediatrics University of Texas
Fractures of the Hand in Children Which are simple? And Which have pitfalls?? Kaye E Wilkins DVM, MD Professor of Orthopedics and Pediatrics Departments of Orthopedics and Pediatrics University of Texas
Pediatric Injuries/Fractures. Rena Heathcote
 Pediatric Injuries/Fractures Rena Heathcote INTRODUCTION Incidence Anatomy of the Growing Bone Injury Patterns What can we X-ray PEDIATRIC FRACTURES INCIDENCE What makes children susceptible to fractures?
Pediatric Injuries/Fractures Rena Heathcote INTRODUCTION Incidence Anatomy of the Growing Bone Injury Patterns What can we X-ray PEDIATRIC FRACTURES INCIDENCE What makes children susceptible to fractures?
Foot Injuries. Dr R B Kalia
 Foot Injuries Dr R B Kalia Overview Dramatic impact on the overall health, activity, and emotional status More attention and aggressive management Difficult appendage to study and diagnose. Aim- a stable
Foot Injuries Dr R B Kalia Overview Dramatic impact on the overall health, activity, and emotional status More attention and aggressive management Difficult appendage to study and diagnose. Aim- a stable
Managing Tibialis Posterior Tendon Injuries
 Managing Tibialis Posterior Tendon Injuries by Thomas C. Michaud, DC Published April 1, 2015 by Dynamic Chiropractic Magazine Tibialis posterior is the deepest, strongest, and most central muscle of the
Managing Tibialis Posterior Tendon Injuries by Thomas C. Michaud, DC Published April 1, 2015 by Dynamic Chiropractic Magazine Tibialis posterior is the deepest, strongest, and most central muscle of the
Evaluation of Gait Mechanics Using Computerized Plantar Surface Pressure Analysis and it s Relation to Common Musculoskeletal Problems
 Evaluation of Gait Mechanics Using Computerized Plantar Surface Pressure Analysis and it s Relation to Common Musculoskeletal Problems Laws of Physics effecting gait Ground Reaction Forces Friction Stored
Evaluation of Gait Mechanics Using Computerized Plantar Surface Pressure Analysis and it s Relation to Common Musculoskeletal Problems Laws of Physics effecting gait Ground Reaction Forces Friction Stored
A Patient s Guide to Adult-Acquired Flatfoot Deformity
 A Patient s Guide to Adult-Acquired Flatfoot Deformity Glendale Adventist Medical Center 1509 Wilson Terrace Glendale, CA 91206 Phone: (818) 409-8000 DISCLAIMER: The information in this booklet is compiled
A Patient s Guide to Adult-Acquired Flatfoot Deformity Glendale Adventist Medical Center 1509 Wilson Terrace Glendale, CA 91206 Phone: (818) 409-8000 DISCLAIMER: The information in this booklet is compiled
Paediatric fractures in the Emergency Department. October 2012
 Paediatric fractures in the Emergency Department October 2012 Victorian Paediatric Orthopaedic Network What this presentation covers Paediatric bone anatomy Buckle injury of distal radius Supracondylar
Paediatric fractures in the Emergency Department October 2012 Victorian Paediatric Orthopaedic Network What this presentation covers Paediatric bone anatomy Buckle injury of distal radius Supracondylar
Elbow. Chapter 2 LISTEN. Mechanism of Injury (If Applicable) Pain
 Pain") Chapter 2 Elbow LISTEN Mechanism of Injury (If Applicable) Patient usually remembers their position at the time of injury Certain mechanisms of injury result in characteristic patterns Fall on outstretched
Chapter 2 Elbow LISTEN Mechanism of Injury (If Applicable) Patient usually remembers their position at the time of injury Certain mechanisms of injury result in characteristic patterns Fall on outstretched
Foot. Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology
 Foot Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology Dorsum of the Foot Sole of the Foot Plantar aponeurosis It is a triangular thickening of deep fascia in the sole of the foot Attachments:
Foot Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology Dorsum of the Foot Sole of the Foot Plantar aponeurosis It is a triangular thickening of deep fascia in the sole of the foot Attachments:
Results of Calcaneal Osteotomy & Flexor Digitorum Longus transfer in Stage II Acquired Flatfoot Deformity
 Results of Calcaneal Osteotomy & Flexor Digitorum Longus transfer in Stage II Acquired Flatfoot Deformity Mr Amit Chauhan Mr Prasad Karpe Ms Maire-claire Killen Mr Rajiv Limaye University Hospital of North
Results of Calcaneal Osteotomy & Flexor Digitorum Longus transfer in Stage II Acquired Flatfoot Deformity Mr Amit Chauhan Mr Prasad Karpe Ms Maire-claire Killen Mr Rajiv Limaye University Hospital of North
The Valgus Foot in Cerebral Palsy Equinovalgus not Plano-Valgus. Alfred D. Grant, M.D. David Feldman, M.D.
 The Valgus Foot in Cerebral Palsy Equinovalgus not Plano-Valgus Alfred D. Grant, M.D. David Feldman, M.D. Norman Otsuka, MD M.D. THE PURPOSE OF THIS PRESENTATION IS TO STATE CLEARLY THAT THE VALGUS FOOT
The Valgus Foot in Cerebral Palsy Equinovalgus not Plano-Valgus Alfred D. Grant, M.D. David Feldman, M.D. Norman Otsuka, MD M.D. THE PURPOSE OF THIS PRESENTATION IS TO STATE CLEARLY THAT THE VALGUS FOOT
Main Menu. Ankle and Foot Joints click here. The Power is in Your Hands
 1 The Ankle and Foot Joints click here Main Menu Copyright HandsOn Therapy Schools 2009 K.8 http://www.handsonlineeducation.com/classes/k8/k8entry.htm[3/27/18, 1:40:03 PM] Ankle and Foot Joint 26 bones
1 The Ankle and Foot Joints click here Main Menu Copyright HandsOn Therapy Schools 2009 K.8 http://www.handsonlineeducation.com/classes/k8/k8entry.htm[3/27/18, 1:40:03 PM] Ankle and Foot Joint 26 bones
Conservative management of idiopathic clubfoot: Kite versus Ponseti method
 Journal of Orthopaedic Surgery 2009;17(1):67-71 Conservative management of idiopathic clubfoot: Kite versus Ponseti method AV Sanghvi, 1 VK Mittal 2 1 Department of Orthopaedics, Government Medical College
Journal of Orthopaedic Surgery 2009;17(1):67-71 Conservative management of idiopathic clubfoot: Kite versus Ponseti method AV Sanghvi, 1 VK Mittal 2 1 Department of Orthopaedics, Government Medical College
First & second layers of muscles of the sole
 The FOOT First & second layers of muscles of the sole introduction The muscles acting on the foot can be divided into two distinct groups; extrinsic and intrinsic muscles. The extrinsic muscles arise from
The FOOT First & second layers of muscles of the sole introduction The muscles acting on the foot can be divided into two distinct groups; extrinsic and intrinsic muscles. The extrinsic muscles arise from
BIOMECHANICAL EXAMINATION OF THE PEDIATRIC LOWER EXTREMITY 2017
 BIOMECHANICAL EXAMINATION OF THE PEDIATRIC LOWER EXTREMITY 2017 B. RESSEQUE, D.P.M., D.A.B.P.O. Professor, N.Y. College of Podiatric Medicine ARCH HEIGHT OFF WEIGHTBEARING Evaluate arch height by placing
BIOMECHANICAL EXAMINATION OF THE PEDIATRIC LOWER EXTREMITY 2017 B. RESSEQUE, D.P.M., D.A.B.P.O. Professor, N.Y. College of Podiatric Medicine ARCH HEIGHT OFF WEIGHTBEARING Evaluate arch height by placing
HUMERAL SHAFT FRACTURES. Fractures of the shaft of the humerus are common, especially in the elderly.
 HUMERAL SHAFT FRACTURES Introduction Fractures of the shaft of the humerus are common, especially in the elderly. The majority can be treated conservatively but patient coping issues may be significant.
HUMERAL SHAFT FRACTURES Introduction Fractures of the shaft of the humerus are common, especially in the elderly. The majority can be treated conservatively but patient coping issues may be significant.
MEDIAL EPICONDYLE FRACTURES
 MEDIAL EPICONDYLE FRACTURES Demographic 20% of elbow fractures 60% of which are associated with elbow dislocation. 75% in boys between 6-12 years 20% of elbow dislocation with ME fracture, the ME is incarcerated
MEDIAL EPICONDYLE FRACTURES Demographic 20% of elbow fractures 60% of which are associated with elbow dislocation. 75% in boys between 6-12 years 20% of elbow dislocation with ME fracture, the ME is incarcerated
Radiographic Assessment of Pediatric Foot Alignment: Review
 JR Integrative Imaging LIFELONG LERNING FOR RDIOLOGY Radiographic ssessment of Pediatric Foot lignment: Review Mahesh M. Thapa 1,2, Sumit Pruthi 1,2, Felix S. Chew 2 Objective The purpose of this article
JR Integrative Imaging LIFELONG LERNING FOR RDIOLOGY Radiographic ssessment of Pediatric Foot lignment: Review Mahesh M. Thapa 1,2, Sumit Pruthi 1,2, Felix S. Chew 2 Objective The purpose of this article
Review relevant anatomy of the foot and ankle. Learn the approach to examining the foot and ankle
 Objectives Review relevant anatomy of the foot and ankle Learn the approach to examining the foot and ankle Learn the basics of diagnosis and treatment of ankle sprains Overview of other common causes
Objectives Review relevant anatomy of the foot and ankle Learn the approach to examining the foot and ankle Learn the basics of diagnosis and treatment of ankle sprains Overview of other common causes
Fractures of the Ankle Region in the Skeletally Immature Patient. The Salter Classification is Worthless!!
 Fractures of the Ankle Region in the Skeletally Immature Patient. The Salter Classification is Worthless!! Kaye E Wilkins D.V.M,M.D. President's Council/Dielmann Chair in Pediatric Orthopedics Professor
Fractures of the Ankle Region in the Skeletally Immature Patient. The Salter Classification is Worthless!! Kaye E Wilkins D.V.M,M.D. President's Council/Dielmann Chair in Pediatric Orthopedics Professor
Surgery-Ortho. Fractures of the tibia and fibula. Management. Treatment of low energy fractures. Fifth stage. Lec-6 د.
 Fifth stage Lec-6 د. مثنى Surgery-Ortho 28/4/2016 Indirect force: (low energy) Fractures of the tibia and fibula Twisting: spiral fractures of both bones Angulatory: oblique fractures with butterfly segment.
Fifth stage Lec-6 د. مثنى Surgery-Ortho 28/4/2016 Indirect force: (low energy) Fractures of the tibia and fibula Twisting: spiral fractures of both bones Angulatory: oblique fractures with butterfly segment.
Case 1 7 yo male Right elbow injury 3 months ago Medial elbow pain and tenderness over medial epicondyle Long arm cast given but off himself 1 month a
 Case presentations Case 1 7 yo male Right elbow injury 3 months ago Medial elbow pain and tenderness over medial epicondyle Long arm cast given but off himself 1 month after Progressive limited elbow flexion
Case presentations Case 1 7 yo male Right elbow injury 3 months ago Medial elbow pain and tenderness over medial epicondyle Long arm cast given but off himself 1 month after Progressive limited elbow flexion
OBJECTIVES: Define basic assessments skills needed to identify orthopedic injuries. Differentiate when an orthopedic injury is a medical emergency
 1 2 How to Triage Orthopaedic Care David W. Gray, M.D. OBJECTIVES: Define basic assessments skills needed to identify orthopedic injuries Differentiate when an orthopedic injury is a medical emergency
1 2 How to Triage Orthopaedic Care David W. Gray, M.D. OBJECTIVES: Define basic assessments skills needed to identify orthopedic injuries Differentiate when an orthopedic injury is a medical emergency
J of Evolution of Med and Dent Sci/ eissn , pissn / Vol. 4/ Issue 50/ June 22, 2015 Page 8632
 MANAGEMENT OF DISPLACED SUPRACONDYLAR FRACTURES OF THE HUMERUS IN CHILDREN BY CLOSED REDUCTION AND PERCUTANEOUS PINNING P. L. Srinivas 1, K. Jagadish 2, B. Mahesh 3 HOW TO CITE THIS ARTICLE: P. L. Srinivas,
MANAGEMENT OF DISPLACED SUPRACONDYLAR FRACTURES OF THE HUMERUS IN CHILDREN BY CLOSED REDUCTION AND PERCUTANEOUS PINNING P. L. Srinivas 1, K. Jagadish 2, B. Mahesh 3 HOW TO CITE THIS ARTICLE: P. L. Srinivas,
1 Humeral fractures 1.13 l Distal humeral fractures Treatment with a splint
 1 Executive Editor: Chris Colton Authors: Mariusz Bonczar, Daniel Rikli, David Ring 1 Humeral fractures 1.13 l Distal humeral fractures Treatment with a splint Indication All 13-A type fractures, excluding
1 Executive Editor: Chris Colton Authors: Mariusz Bonczar, Daniel Rikli, David Ring 1 Humeral fractures 1.13 l Distal humeral fractures Treatment with a splint Indication All 13-A type fractures, excluding
Results of Using Reversed Ponseti Technique in Treatment of Congenital Vertical Talus
 Med. J. Cairo Univ., Vol. 85, No. 4, June: 1447-1453, 217 www.medicaljournalofcairouniversity.net Results of Using Reversed Ponseti Technique in Treatment of Congenital Vertical Talus MOHAMED F. EL-KHOSOUSY,
Med. J. Cairo Univ., Vol. 85, No. 4, June: 1447-1453, 217 www.medicaljournalofcairouniversity.net Results of Using Reversed Ponseti Technique in Treatment of Congenital Vertical Talus MOHAMED F. EL-KHOSOUSY,
Financial Disclosure. The authors have not received any financial support for the preparation of this work.
 Persistent Clubfoot Deformity Following Treatment by the Ponseti Method W.B. Lehman, M.D. Alice Chu, M.D. New York Ponseti Clubfoot Center Department of Pediatric Orthopaedic Surgery Financial Disclosure
Persistent Clubfoot Deformity Following Treatment by the Ponseti Method W.B. Lehman, M.D. Alice Chu, M.D. New York Ponseti Clubfoot Center Department of Pediatric Orthopaedic Surgery Financial Disclosure
ANKLE PLANTAR FLEXION
 ANKLE PLANTAR FLEXION Evaluation and Measurements By Isabelle Devreux 1 Ankle Plantar Flexion: Gastrocnemius and Soleus ROM: 0 to 40-45 A. Soleus: Origin: Posterior of head of fibula and proximal1/3 of
ANKLE PLANTAR FLEXION Evaluation and Measurements By Isabelle Devreux 1 Ankle Plantar Flexion: Gastrocnemius and Soleus ROM: 0 to 40-45 A. Soleus: Origin: Posterior of head of fibula and proximal1/3 of
11/5/14. I will try to make this painless. Great, a Fracture, Now What? Objectives. Basics for Fracture Workup. Basics for Fracture Workup
 Great, a Fracture, Now What? I will try to make this painless Mary Greve MS, PA-C Department of Orthopedic Surgery Trauma Team University of Iowa Hospitals and Clinics Mary-Greve@uiowa.edu Pager 2121 Objectives
Great, a Fracture, Now What? I will try to make this painless Mary Greve MS, PA-C Department of Orthopedic Surgery Trauma Team University of Iowa Hospitals and Clinics Mary-Greve@uiowa.edu Pager 2121 Objectives
Anatomy of Foot and Ankle
 Anatomy of Foot and Ankle Surface anatomy of the ankle & foot Surface anatomy of the ankle & foot Medial orientation point medial malleous sustentaculum tali tuberosity of navicular TA muscle TP muscle
Anatomy of Foot and Ankle Surface anatomy of the ankle & foot Surface anatomy of the ankle & foot Medial orientation point medial malleous sustentaculum tali tuberosity of navicular TA muscle TP muscle
Dr Nabil khouri MD. MSc. Ph.D
 Dr Nabil khouri MD. MSc. Ph.D Foot Anatomy The foot consists of 26 bones: 14 phalangeal, 5 metatarsal, and 7 tarsal. Toes are used to balance the body. Metatarsal Bones gives elasticity to the foot in
Dr Nabil khouri MD. MSc. Ph.D Foot Anatomy The foot consists of 26 bones: 14 phalangeal, 5 metatarsal, and 7 tarsal. Toes are used to balance the body. Metatarsal Bones gives elasticity to the foot in
Leg. Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology
 Leg Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology Skin of the Leg Cutaneous Nerves Medially: The saphenous nerve, a branch of the femoral nerve supplies the skin on the medial surface
Leg Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology Skin of the Leg Cutaneous Nerves Medially: The saphenous nerve, a branch of the femoral nerve supplies the skin on the medial surface
The University Of Jordan Faculty Of Medicine FOOT. Dr.Ahmed Salman Assistant Prof. of Anatomy. The University Of Jordan
 The University Of Jordan Faculty Of Medicine FOOT Dr.Ahmed Salman Assistant Prof. of Anatomy. The University Of Jordan Tarsal Tunnel Syndrome Due to compression of Tibial nerve as it travels through the
The University Of Jordan Faculty Of Medicine FOOT Dr.Ahmed Salman Assistant Prof. of Anatomy. The University Of Jordan Tarsal Tunnel Syndrome Due to compression of Tibial nerve as it travels through the
CHRONIC FOOT PROBLEMS FOOT and ANKLE BASICS
 CHRONIC FOOT PROBLEMS FOOT and ANKLE BASICS ABC s of Comprehensive Musculoskeletal Care December 1 st, 2007 Stephen Pinney MD Chief, UCSF Foot and Ankle Service Chronic problems typically occur gradually
CHRONIC FOOT PROBLEMS FOOT and ANKLE BASICS ABC s of Comprehensive Musculoskeletal Care December 1 st, 2007 Stephen Pinney MD Chief, UCSF Foot and Ankle Service Chronic problems typically occur gradually
A Patient s Guide to Flatfoot Deformity (Pes Planus) in Children
 in Children") A Patient s Guide to Flatfoot Deformity (Pes Planus) in Children 2350 Royal Boulevard Suite 200 Elgin, IL 60123 Phone: 847.931.5300 Fax: 847.931.9072 DISCLAIMER: The information in this booklet is compiled
A Patient s Guide to Flatfoot Deformity (Pes Planus) in Children 2350 Royal Boulevard Suite 200 Elgin, IL 60123 Phone: 847.931.5300 Fax: 847.931.9072 DISCLAIMER: The information in this booklet is compiled
BASIC PRINCIPLES OF HAND TRAUMA: ARE CHILDREN DIFFERENT? SUSAN THOMPSON, MD, FRCSC
 BASIC PRINCIPLES OF HAND TRAUMA: ARE CHILDREN DIFFERENT? SUSAN THOMPSON, MD, FRCSC EPIDEMIOLOGY HAND FRACTURES MAKE UP 2.3% OF ER VISITS INCIDENCE VARIES WITH AGE LOW IN TODDLERS INCREASES WITH AGE (20
BASIC PRINCIPLES OF HAND TRAUMA: ARE CHILDREN DIFFERENT? SUSAN THOMPSON, MD, FRCSC EPIDEMIOLOGY HAND FRACTURES MAKE UP 2.3% OF ER VISITS INCIDENCE VARIES WITH AGE LOW IN TODDLERS INCREASES WITH AGE (20
Introduction to Fractures. Traumatology RHS 231 Dr. Einas Al-Eisa Lecture 3
 Introduction to Fractures Traumatology RHS 231 Dr. Einas Al-Eisa Lecture 3 Definitions A fracture is an interruption in the continuity of bone Fracture = Break Fracture: mechanical damage produced in a
Introduction to Fractures Traumatology RHS 231 Dr. Einas Al-Eisa Lecture 3 Definitions A fracture is an interruption in the continuity of bone Fracture = Break Fracture: mechanical damage produced in a
Orthopaedics. Current concepts Common errors in the treatment of congenital clubfoot. International. I. V. Ponseti
 International Orthopaedics (SICOT) (1997) 21: 137 141 Orthopaedics International Springer-Verlag 1997 Current concepts Common errors in the treatment of congenital clubfoot I. V. Ponseti Department of
International Orthopaedics (SICOT) (1997) 21: 137 141 Orthopaedics International Springer-Verlag 1997 Current concepts Common errors in the treatment of congenital clubfoot I. V. Ponseti Department of
Ponseti Treatment Method for Idiopathic Clubfoot Continuing Education Module
 Ponseti Treatment Method for Idiopathic Clubfoot Continuing Education Module Michelle J. Hall, CPO, BSE 1 Ignacio V. Ponseti, MD 2 1. Certified Prosthetist Orthotist at American Prosthetics & Orthotics,
Ponseti Treatment Method for Idiopathic Clubfoot Continuing Education Module Michelle J. Hall, CPO, BSE 1 Ignacio V. Ponseti, MD 2 1. Certified Prosthetist Orthotist at American Prosthetics & Orthotics,
A Patient s Guide to Clubfoot
 A Patient s Guide to Clubfoot 651 Old Country Road Plainview, NY 11803 Phone: 5166818822 Fax: 5166813332 p.lettieri@aol.com DISCLAIMER: The information in this booklet is compiled from a variety of sources.
A Patient s Guide to Clubfoot 651 Old Country Road Plainview, NY 11803 Phone: 5166818822 Fax: 5166813332 p.lettieri@aol.com DISCLAIMER: The information in this booklet is compiled from a variety of sources.
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Abductor hallucis tendon procedures, for hallux varus, 536 537 Acetabular disorders, intoeing in, 551 553 Akron dome osteotomy, for cavus deformities,
Note: Page numbers of article titles are in boldface type. A Abductor hallucis tendon procedures, for hallux varus, 536 537 Acetabular disorders, intoeing in, 551 553 Akron dome osteotomy, for cavus deformities,
1/19/2018. Winter injuries to the shoulder and elbow. Highgate Private Hospital (Whittington Health NHS Trust)
") Winter injuries to the shoulder and elbow Omar Haddo Consultant Orthopaedic Surgeon, Shoulder, Elbow, Hand & Wrist Specialist MBBS, BmedSci, FRCS(Orth) Highgate Private Hospital (Whittington Health NHS
Winter injuries to the shoulder and elbow Omar Haddo Consultant Orthopaedic Surgeon, Shoulder, Elbow, Hand & Wrist Specialist MBBS, BmedSci, FRCS(Orth) Highgate Private Hospital (Whittington Health NHS
Foot and Ankle. in the Primary Care Setting. September 29, 2018 WOJCIECH L CZOCH, MD COHEN CHILDREN S MEDICAL CENTER LONG ISLAND, NY
 Foot and Ankle in the Primary Care Setting September 29, 2018 WOJCIECH L CZOCH, MD COHEN CHILDREN S MEDICAL CENTER LONG ISLAND, NY Disclosures I have no relevant financial relationships with the manufacturers
Foot and Ankle in the Primary Care Setting September 29, 2018 WOJCIECH L CZOCH, MD COHEN CHILDREN S MEDICAL CENTER LONG ISLAND, NY Disclosures I have no relevant financial relationships with the manufacturers
Pathology & Primary Treatment of Clubfoot
 Pathology & Primary Treatment of Clubfoot Hyun-Dae Shin, MD, PhD. Department of Orthopedic Surgery, School of Medicine, Chungnam National University, Daejeon, Korea Introduction The affected foot Restricted
Pathology & Primary Treatment of Clubfoot Hyun-Dae Shin, MD, PhD. Department of Orthopedic Surgery, School of Medicine, Chungnam National University, Daejeon, Korea Introduction The affected foot Restricted
Index. Clin Podiatr Med Surg 22 (2005) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Clin Podiatr Med Surg 22 (2005) 309 314 Index Note: Page numbers of article titles are in boldface type. A Abductor digiti minimi muscle, myectomy of, for tailor s bunionette, 243 Achilles tendon, lengthening
Clin Podiatr Med Surg 22 (2005) 309 314 Index Note: Page numbers of article titles are in boldface type. A Abductor digiti minimi muscle, myectomy of, for tailor s bunionette, 243 Achilles tendon, lengthening
What Happens to the Paediatric Flat Foot? Peter J Briggs Freeman Hospital Newcastle upon Tyne
 What Happens to the Paediatric Flat Foot? Peter J Briggs Freeman Hospital Newcastle upon Tyne We don t know!! Population Studies 2300 children aged 4-13 years Shoe wearers Flat foot 8.6% Non-shoe wearers
What Happens to the Paediatric Flat Foot? Peter J Briggs Freeman Hospital Newcastle upon Tyne We don t know!! Population Studies 2300 children aged 4-13 years Shoe wearers Flat foot 8.6% Non-shoe wearers
Understanding Leg Anatomy and Function THE UPPER LEG
 Understanding Leg Anatomy and Function THE UPPER LEG The long thigh bone is the femur. It connects to the pelvis to form the hip joint and then extends down to meet the tibia (shin bone) at the knee joint.
Understanding Leg Anatomy and Function THE UPPER LEG The long thigh bone is the femur. It connects to the pelvis to form the hip joint and then extends down to meet the tibia (shin bone) at the knee joint.
Upper limb injuries in children. Key points, # & dislocations 7/23/2009 (MIMIC)
") Upper limb injuries in children (MIMIC) Key points, # & dislocations Before the age of 16 around 50% of boys & 25% of girls will sustain a # Dislocations are very uncommon Children s bones are less brittle
Upper limb injuries in children (MIMIC) Key points, # & dislocations Before the age of 16 around 50% of boys & 25% of girls will sustain a # Dislocations are very uncommon Children s bones are less brittle
Abd Ali Muhsin FICMS.
 Comparative study between close reductions versus close reduction with K-Wire fixation in completely dorsally displaced distal radial metaphyseal fracture, in children and adolescent. Abd Ali Muhsin FICMS.
Comparative study between close reductions versus close reduction with K-Wire fixation in completely dorsally displaced distal radial metaphyseal fracture, in children and adolescent. Abd Ali Muhsin FICMS.
The Language of Anatomy. (Anatomical Terminology)
") The Language of Anatomy (Anatomical Terminology) Terms of Position The anatomical position is a fixed position of the body (cadaver) taken as if the body is standing (erect) looking forward with the upper
The Language of Anatomy (Anatomical Terminology) Terms of Position The anatomical position is a fixed position of the body (cadaver) taken as if the body is standing (erect) looking forward with the upper
بسم هللا الرحمن الرحيم
 بسم هللا الرحمن الرحيم Laboratory RHS 221 Manual Muscle Testing Theory 1 hour practical 2 hours Dr. Ali Aldali, MS, PT Department of Physical Therapy King Saud University Talocrural and Subtalar Joint
بسم هللا الرحمن الرحيم Laboratory RHS 221 Manual Muscle Testing Theory 1 hour practical 2 hours Dr. Ali Aldali, MS, PT Department of Physical Therapy King Saud University Talocrural and Subtalar Joint
Elbow Problems.
 Elbow Problems www.fisiokinesiterapia.biz Anatomy Hinged joint formed by humerus and ulna produces flexion and extension Rotation producing pronation and supination from radial head and humerus Assessment
Elbow Problems www.fisiokinesiterapia.biz Anatomy Hinged joint formed by humerus and ulna produces flexion and extension Rotation producing pronation and supination from radial head and humerus Assessment
SUBTALAR ARTHROEREISIS IN THE OLDER PATIENT
 C H A P T E R 1 7 SUBTALAR ARTHROEREISIS IN THE OLDER PATIENT William D. Fishco, DPM, MS INTRODUCTION Arthroereisis is a surgical procedure designed to limit the motion of a joint. Subtalar joint arthroereisis
C H A P T E R 1 7 SUBTALAR ARTHROEREISIS IN THE OLDER PATIENT William D. Fishco, DPM, MS INTRODUCTION Arthroereisis is a surgical procedure designed to limit the motion of a joint. Subtalar joint arthroereisis
QUEST.6. This patient fell from a tree a. What is the diagnosis? (2) b. What would be your management for this injury in casualty?
 b. What would be your management for this injury in casualty?") QUEST.6 This patient fell from a tree a. What is the diagnosis? (2) b. What would be your management for this injury in casualty? (3) P381 A. Right sided fractures of medial and lateral malleoli with a
QUEST.6 This patient fell from a tree a. What is the diagnosis? (2) b. What would be your management for this injury in casualty? (3) P381 A. Right sided fractures of medial and lateral malleoli with a
The plantar aponeurosis
 Anatomy of the foot The plantar aponeurosis Is a triangular thickening of the deep fascia Its apex is attached to the medial and lateral tubercles of the calcaneum. The base of the aponeurosis divides
Anatomy of the foot The plantar aponeurosis Is a triangular thickening of the deep fascia Its apex is attached to the medial and lateral tubercles of the calcaneum. The base of the aponeurosis divides
Paediatric Foot Disorders. Foot Disorders
 Paediatric B Milne FRACS (Orth) Paediatric Orthopaedic Fellow Anatomy Bones of the foot Valgus Deviation of the distal body part away from the midline Varus Deviation of the distal body part towards the
Paediatric B Milne FRACS (Orth) Paediatric Orthopaedic Fellow Anatomy Bones of the foot Valgus Deviation of the distal body part away from the midline Varus Deviation of the distal body part towards the
The Leg. Prof. Oluwadiya KS
 The Leg Prof. Oluwadiya KS www.oluwadiya.sitesled.com Compartments of the leg 4 Four Compartments: 1. Anterior compartment Deep fibular nerve Dorsiflexes the foot and toes 2. Lateral Compartment Superficial
The Leg Prof. Oluwadiya KS www.oluwadiya.sitesled.com Compartments of the leg 4 Four Compartments: 1. Anterior compartment Deep fibular nerve Dorsiflexes the foot and toes 2. Lateral Compartment Superficial
Financial Disclosure. Turf Toe
 Seth O Brien, CP, LP Financial Disclosure Mr. Seth O'Brien has no relevant financial relationships with commercial interests to disclose. Turf Toe Common in athletes playing on firm, artificial turf Forceful
Seth O Brien, CP, LP Financial Disclosure Mr. Seth O'Brien has no relevant financial relationships with commercial interests to disclose. Turf Toe Common in athletes playing on firm, artificial turf Forceful
Hand and wrist emergencies
 Chapter1 Hand and wrist emergencies Carl A. Germann Distal radius and ulnar injuries PEARL: Fractures of the distal radius and ulna are the most common type of fractures in patients younger than 75 years.
Chapter1 Hand and wrist emergencies Carl A. Germann Distal radius and ulnar injuries PEARL: Fractures of the distal radius and ulna are the most common type of fractures in patients younger than 75 years.
Multiapical Deformities p. 97 Osteotomy Concepts and Frontal Plane Realignment p. 99 Angulation Correction Axis (ACA) p. 99 Bisector Lines p.
 p. 99 Bisector Lines p.") Normal Lower Limb Alignment and Joint Orientation p. 1 Mechanical and Anatomic Bone Axes p. 1 Joint Center Points p. 5 Joint Orientation Lines p. 5 Ankle p. 5 Knee p. 5 Hip p. 8 Joint Orientation Angles
Normal Lower Limb Alignment and Joint Orientation p. 1 Mechanical and Anatomic Bone Axes p. 1 Joint Center Points p. 5 Joint Orientation Lines p. 5 Ankle p. 5 Knee p. 5 Hip p. 8 Joint Orientation Angles
Assessment of percutaneous V osteotomy of the calcaneus with Ilizarov application for correction of complex foot deformities
 Acta Orthop. Belg., 2004, 70, 586-590 ORIGINAL STUDY Assessment of percutaneous V osteotomy of the calcaneus with Ilizarov application for correction of complex foot deformities Hani EL-MOWAFI From Mansoura
Acta Orthop. Belg., 2004, 70, 586-590 ORIGINAL STUDY Assessment of percutaneous V osteotomy of the calcaneus with Ilizarov application for correction of complex foot deformities Hani EL-MOWAFI From Mansoura
TENDON TRANSFER IN CAVUS FOOT
 TENDON TRANSFER IN CAVUS FOOT Cavovarus deformity is defined by fixed equinus of the forefoot on the hindfoot, resulting in a pathologic elevation of the longitudinal arch, with either a fixed or flexible
TENDON TRANSFER IN CAVUS FOOT Cavovarus deformity is defined by fixed equinus of the forefoot on the hindfoot, resulting in a pathologic elevation of the longitudinal arch, with either a fixed or flexible
PEDIATRIC ELBOW FRACTURES.
 PEDIATRIC ELBOW FRACTURES www.fisiokinesiterapia.biz INCIDENCE SECOND MOST COMMON PEDIATRIC INJURY OSSIFICATION 1. CAPITELLUM (6 mo. - 2 yrs.) 2. MED. EPICONDYLE (5-9 yrs.) 3. TROCHLEA (7-13 yrs.) 4. LAT.
PEDIATRIC ELBOW FRACTURES www.fisiokinesiterapia.biz INCIDENCE SECOND MOST COMMON PEDIATRIC INJURY OSSIFICATION 1. CAPITELLUM (6 mo. - 2 yrs.) 2. MED. EPICONDYLE (5-9 yrs.) 3. TROCHLEA (7-13 yrs.) 4. LAT.
radiologymasterclass.co.uk
 http://radiologymasterclass.co.uk Hip X-ray anatomy - Normal AP (anterior-posterior) Shenton's line is formed by the medial edge of the femoral neck and the inferior edge of the superior pubic ramus Loss
http://radiologymasterclass.co.uk Hip X-ray anatomy - Normal AP (anterior-posterior) Shenton's line is formed by the medial edge of the femoral neck and the inferior edge of the superior pubic ramus Loss
Hip joint Type: Articulating bones:
 Ana (242 ) Hip joint Type: Synovial, ball & socket Articulating bones: Formed between head of femur and lunate surface of acetabulum of hip bone. Capsule: it is a strong fibrous sleeve connecting the articulating
Ana (242 ) Hip joint Type: Synovial, ball & socket Articulating bones: Formed between head of femur and lunate surface of acetabulum of hip bone. Capsule: it is a strong fibrous sleeve connecting the articulating
Terms of Movements by Prof. Dr. Muhammad Imran Qureshi
 Terms of Movements by Prof. Dr. Muhammad Imran Qureshi Three systems of the body work in coordination to perform various movements of the body. These are: A System of Bones (Osteology), A System of Muscles
Terms of Movements by Prof. Dr. Muhammad Imran Qureshi Three systems of the body work in coordination to perform various movements of the body. These are: A System of Bones (Osteology), A System of Muscles
Section Three: The Leg, Ankle, and Foot Lecture: Review of Clinical Anatomy, Patterns of Dysfunction and Injury, and
 Section Three: The Leg, Ankle, and Foot Lecture: Review of Clinical Anatomy, Patterns of Dysfunction and Injury, and Treatment Implications for the Leg, Ankle, and Foot Levels I and II Demonstration and
Section Three: The Leg, Ankle, and Foot Lecture: Review of Clinical Anatomy, Patterns of Dysfunction and Injury, and Treatment Implications for the Leg, Ankle, and Foot Levels I and II Demonstration and
Calcaneus (Heel Bone) Fractures
 Fractures") Page 1 of 8 Calcaneus (Heel Bone) Fractures A fracture of the calcaneus, or heel bone, can be a painful and disabling injury. This type of fracture commonly occurs during a high-energy event such as a
Page 1 of 8 Calcaneus (Heel Bone) Fractures A fracture of the calcaneus, or heel bone, can be a painful and disabling injury. This type of fracture commonly occurs during a high-energy event such as a
FOOSH It sounded like a fun thing at the time!
 FOOSH It sounded like a fun thing at the time! Evaluating acute hand and wrist injuries Larry Collins, MPAS, PA-C, ATC, DFAAPA Assistant Professor, Physician Assistant Program Assistant Professor, Department
FOOSH It sounded like a fun thing at the time! Evaluating acute hand and wrist injuries Larry Collins, MPAS, PA-C, ATC, DFAAPA Assistant Professor, Physician Assistant Program Assistant Professor, Department
Case 57 What is the diagnosis? Insidious onset forefoot pain in a 50 year old female for last 3 months.
 Case 57 What is the diagnosis? Insidious onset forefoot pain in a 50 year old female for last 3 months. Diagnosis: II MTP instability Demographics of MT instability Lesser MTP joint instability occurs
Case 57 What is the diagnosis? Insidious onset forefoot pain in a 50 year old female for last 3 months. Diagnosis: II MTP instability Demographics of MT instability Lesser MTP joint instability occurs
The Lower Limb VII: The Ankle & Foot. Anatomy RHS 241 Lecture 7 Dr. Einas Al-Eisa
 The Lower Limb VII: The Ankle & Foot Anatomy RHS 241 Lecture 7 Dr. Einas Al-Eisa Ankle joint Synovial, hinge joint Allow movement of the foot in the sagittal plane only (1 degree of freedom): dorsiflexion:
The Lower Limb VII: The Ankle & Foot Anatomy RHS 241 Lecture 7 Dr. Einas Al-Eisa Ankle joint Synovial, hinge joint Allow movement of the foot in the sagittal plane only (1 degree of freedom): dorsiflexion:
Introduction. The primary function of the ankle and foot is to absorb shock and impart thrust to the body during walking.
 The ankle 1 Introduction The primary function of the ankle and foot is to absorb shock and impart thrust to the body during walking. OSTEOLOGRY The term ankle refers primarily to the talocrural joint,
The ankle 1 Introduction The primary function of the ankle and foot is to absorb shock and impart thrust to the body during walking. OSTEOLOGRY The term ankle refers primarily to the talocrural joint,
ORTHOSCAN MOBILE DI POSITIONING GUIDE
 ORTHOSCAN MOBILE DI POSITIONING GUIDE Table of Contents SHOULDER A/P of Shoulder... 4 Tangential (Y-View) of Shoulder... 5 Lateral of Proximal Humerus... 6 ELBOW A/P of Elbow... 7 Extended Elbow... 8 Lateral
ORTHOSCAN MOBILE DI POSITIONING GUIDE Table of Contents SHOULDER A/P of Shoulder... 4 Tangential (Y-View) of Shoulder... 5 Lateral of Proximal Humerus... 6 ELBOW A/P of Elbow... 7 Extended Elbow... 8 Lateral
2017 SAFSA CONGRESS PROGRAMME
 2017 SAFSA CONGRESS PROGRAMME THURSDAY, MAY 25 07h45 07h55: WELCOME & INTRODUCTIONS Forefoot I: Hallux Valgus and Lesser Toes (08h00-10h00 Lectures) 08h00 08h30: Surgical Management of Hallux Valgus Rippstein,
2017 SAFSA CONGRESS PROGRAMME THURSDAY, MAY 25 07h45 07h55: WELCOME & INTRODUCTIONS Forefoot I: Hallux Valgus and Lesser Toes (08h00-10h00 Lectures) 08h00 08h30: Surgical Management of Hallux Valgus Rippstein,