Ankle Valgus in Cerebral Palsy
|
|
|
- Rose Morrison
- 5 years ago
- Views:
Transcription
1 Ankle Valgus in Cerebral Palsy Freeman Miller Contents Introduction... 2 Natural History... 2 Treatment... 3 Diagnostic Evaluations... 3 Indications for Intervention... 3 Outcome of Treatment... 5 Complications of Treatment... 5 Conclusion... 5 Cases... 5 Case 1 Silas... 5 Case 2 Lindsey... 7 Case 3 Kenneth... 9 Cross-References References Abstract Valgus deformity of the ankle joint has been well recognized as part of the external rotation planovalgus collapse of the paralyzed foot most commonly seen in spina bifida. This same association has been reported in spastic planovalgus feet of children with cerebral palsy (CP), as an unrecognized contributor of hindfoot valgus. Also, there is a well-defined syndrome of increasing ankle valgus when a section of the fibula is resected for use as bone graft. Although the ankle valgus in spastic feet is not as profound as in the paralyzed foot of spina bifida, it is nevertheless significant in some children. The ankle valgus is rarely an isolated primary deformity in spastic feet, although it may be the primary deformity in rare children who are ambulatory with primary F. Miller (*) AI DuPont Hospital for Children, Wilmington, DE, USA freeman.miller@gmail.com # Springer International Publishing AG, part of Springer Nature 2018 F. Miller et al. (eds.), Cerebral Palsy, 1
2 2 F. Miller hypotonic CP. A common factor in ankle valgus in children with CP is that it is very often missed initially. Ankle valgus is a secondary deformity associated with planovalgus and external tibial torsion. The planovalgus may be appropriately treated but then when the patient still presents with what appears to be a valgus foot during stance phase of gait. The most important aspect of ankle valgus is recognizing when it is present. Treatment options include correction associated with a tibial osteotomy and medial malleolus screw epiphysiodesis. The goal of this chapter is to define the situations where ankle valgus is a problem, how to diagnose it, and the treatment options. Keywords Cerebral palsy Ankle valgus Ankle epiphysiodesis Screw epiphysiodesis Introduction Valgus deformity of the ankle joint has been well recognized as part of the external rotation planovalgus collapse of the paralyzed foot most commonly seen in spina bifida. (Dias 1985) This same association has been reported in spastic planovalgus feet of children with cerebral palsy (CP) (McCall et al. 1985; Scott et al. 1988), as an unrecognized contributor of hindfoot valgus. Also, there is a well-defined syndrome of increasing ankle valgus when a section of the fibula is resected for use as bone graft (Hsu et al. 1972). Although the ankle valgus in spastic feet is not as profound as in the paralyzed foot of spina bifida, it is nevertheless significant in some children (Davids 2010). The ankle valgus is rarely an isolated primary deformity in spastic feet, although it may be the primary deformity in rare children who are ambulatory with primary hypotonic CP. A common factor in ankle valgus in children with CP is that it is very often missed initially. Commonly it is associated with planovalgus and the planovalgus may be appropriately treated but then when the patient still presents with what appears to be a valgus foot during stance phase of gait. The most important aspect of ankle valgus is recognized when it is present. The goal of this chapter is to define the situations where ankle valgus is a problem, how to diagnose it, and the treatment options. Natural History The natural history of ankle valgus in spastic feet is not defined. Based on our experience, the valgus gets worse during late childhood and adolescent growth, then remains stable after the completion of growth. In almost all children with CP, the ankle valgus is a secondary deformity to the primary deformity of a planovalgus foot. The pathomechanics of this deformity appear to be the initial development of a planovalgus foot, usually associated with external foot progression angle and hyperdorsiflexion which places a large moment at the ankle driving it into valgus. This force increases the load on the fibula and the lateral distal tibial growth plate. Since ankle valgus has not been reported as an isolated lesion and is almost always associated as a secondary lesion of planovalgus, and it usually includes external tibial torsion. This abnormal lateral loading also causes the fibula to be shorter as part of the valgus ankle syndrome. When hyper dorsiflexion at the ankle joint is the predominating posture, there may be a primary deformity at the anterior lateral aspect of the distal tibial epiphysis that on initial radiographs may not be apparent and the fibula may not appear short. In these situations, the patient s foot alignment typically looks quite good when the foot is in neutral dorsiflexion
3 Ankle Valgus in Cerebral Palsy 3 plantarflexion or when it is placed into plantarflexion. However, when the foot is dorsiflexed, the hindfoot will fall into valgus and the whole foot will externally rotate through the subtalor joint. This is often associated and first recognized after correction of planovalgus when there has been either a fusion of the hind foot or osteotomies all of which should stabilize and stiffen up the hind foot. In this situation in neutral or plantarflexion, hindfoot alignment and the forefoot alignment relative to the hindfoot is good. In the situation where residual deformity is recognized after the foot has been corrected, the natural history appears to be one of increasing deformity or the deformity remaining the same if the growth plates have closed. In our experience we have never seen this deformity spontaneously resolve. Correction of the deforming force by correcting the planovalgus foot and external tibial torsion is not enough to cause spontaneous correction of the valgus ankle joint in children with growth remaining. However, if both the rotational foot alignment and the hindfoot valgus and forefoot supination are corrected to neutral, the deformity will typically stabilize. To gain stability of ankle valgus deformity also requires that the ankle not be in hyper dorsiflexion during weight-bearing, this seems to create the anterior lateral defect in the distal tibia which can bring on this apparent return of hindfoot valgus. Treatment Diagnostic Evaluations The valgus of the ankle joint cannot be recognized if the appropriate radiographs are not obtained. The correct radiographs are centered on the ankle joint with a long enough image of the tibia above to measure the long axis of the tibia. The rotational position of the ankle should produce an anteroposterior mortise view showing the profile of the talus. Appropriate radiographs include an anteroposterior view of the ankle joint centered on the ankle (Fig. 1). With the common addition of torsional deformities and the goal of wanting to see a radiograph of the whole tibia, very poor images of the ankle joint are often made. Since ankle valgus has not been reported as an isolated lesion and is almost always associated as a secondary lesion of planovalgus and external tibial torsion, specific radiographs have to be ordered of the ankle joint with the mortice view being most important. Since the fibula is often shorter as part of the valgus ankle syndrome, the mortice radiograph also facilitates this assessment. The epiphysis of the normal ankle should be at the level of the ankle joint, but with CP ankle valgus, it is often at the level of the distal tibial epiphysis. Since valgus ankles in some children with spasticity also seem to have a complex rotational malalignment of the talus in the ankle mortise with more foot valgus in dorsiflexion then plantarflexion, additional imaging may be required. Usually, there is more dysplasia of the anterior lateral ankle mortise than the posterior aspect, a difference which can be hard to appreciate on standard mortice view. In this situation, it is best to obtain a CT scan of the ankle joint. This will allow imaging the asymmetry between the anterior lateral and the posterior and middle lateral aspects of the tibial epiphysis (Case 1). Indications for Intervention Because the ankle valgus is almost always a secondary deformity, there is no role for correction of only the ankle valgus unless the primary deformity is or has been corrected. This correction should be part of a reconstruction of a whole problem, which usually includes the planovalgus foot, equinus ankle, hyperdorsiflexion, and

4 4 F. Miller Fig. 1 When planning corrections of foot deformities, especially planovalgus, it is important to obtain anteroposterior radiographs of the ankle mortise to rule out significant ankle valgus as a component of the deformity. The correct radiographic view is not often obtained, as there is a need to view the whole tibia; however, to obtain an accurate view of the alignment of the ankle mortise, the beam should be perpendicular to the ankle joint. If the positioning is such that the beams are very divergent at the ankle joint, accurate assessment of valgus is not possible external tibial torsion. Indications for correction are more than 10 of ankle joint valgus relative to the long axis of the tibia. If the external tibial torsion is being corrected with an osteotomy, no more than 5 of valgus should be tolerated at the ankle joint. If more valgus is present on the postoperative radiograph, the cast should be wedged to correct the deformity (Case 2). The presence of the ankle valgus must be recognized when correcting the hindfoot because it is important to avoid overcorrection of the hindfoot valgus. If no tibial derotation is required, then correction of the ankle valgus can usually be done with a screw epiphysiodesis of the medial malleolus if there is adequate growth remaining. The ankle has to be monitored with radiographs every 4 6 months, and when the valgus has corrected, the screw should be removed (Case 3). For individuals with a closed growth plate, up to 15 of valgus can be accepted if the foot is corrected close to a neutral position below the ankle. This residual ankle valgus causes the foot to fall into external rotation and valgus with increased dorsiflexion, but tends to be less of a problem in individuals who are dependent on orthotics for ankle stability. In this situation, the ankle orthosis should be solid to prevent dorsiflexion during stance phase. Having the ankle valgus corrected is more important in individuals who are high-functioning community ambulators without orthotics or assistive devices. In the situation where the foot has been corrected but the child continues to fall into valgus with hyper dorsiflexion during stance phase and the individual is not tolerating solid ankle orthotics or they wish not to use orthotics, the correction should be considered. For the individual with an open growth plate, consideration of medial ankle epiphysiodesis is reasonable. In this situation, the ankle may be over corrected into some varus (Case 2). For individuals who are skeletally mature, the primary option is joint stabilization.
5 Ankle Valgus in Cerebral Palsy 5 Because this deformity is extremely difficult to correct with osteotomies, our primary treatment has been ankle fusion. It is typical that this deformity occurs in individuals who have ambulatory ability but are not high demand ambulators (Case 1). Outcome of Treatment There are no reports of the outcome of treating valgus deformity in spastic feet. Our experience has been that it is important not to overcorrect the deformity because a little valgus is better tolerated than a little varus. Also, there does not seem to be much loss of correction, although we have not had enough children corrected by the screw epiphysiodesis who have completed growth to be confident of this fact. A stable correction has been reported in several series with a wide variety of other diagnoses but not specifically focused on children with CP. (Beals 1991) (Davids et al. 1997; Stevens and Belle 1997; Tompkins et al. 2012). Complications of Treatment The primary complication from ankle valgus in CP is the failure to make the diagnosis. In many patients, the appearance of ankle valgus has been overlooked until the planovalgus deformity and external tibial torsion have been corrected. Recognizing the presence of ankle valgus in planning the correction of the primary deformities, external tibial torsion and planovalgus, is an important way of avoiding this late surprise. Following screw epiphysiodesis, there have been no reports of premature growth arrests after the screws were removed (Beals 1991) (Davids et al. 1997; Stevens and Belle 1997; Tompkins et al. 2012). No significant complications have been reported from medial ankle epiphysiodesis, and our only complication from correction of ankle valgus was mild overcorrection, leaving this individual with a mild varus foot position. Radiographic correction of the ankle valgus with respect to the distal tibia and the long axis of the tibia usually occurs with the epiphysiodesis; however, correction of the short fibula seldom occurs (Fig. C3.3). Because the important element in the correction is to have neutral ankle joint mortise alignment, it is better to measure the angle of the dome of the talus to the long axis of the tibia. The position of the fibula does not seem to matter. Conclusion Ankle joint valgus in children with cerebral palsy is a secondary deformity that occurs as a response to external tibial torsion and planovalgus. This deformity needs to be recognized during treatment of the primary deformities and when necessary can be easily treated with medial ankle epiphysiodesis. Cases Case 1 Silas Silas is a 17-year-old boy who is 2 years following bilateral triple arthrodesis for correction of planovalgus feet. He is GMFCS III using a posterior walker; however, over the last year the right foot has developed increased valgus, external rotation, and collapse into dorsiflexion during weight bearing (Fig. C1.1). Radiographs of the foot showed solid fusion with good foot alignment (Fig. C1.2); however, a CT Scan of the



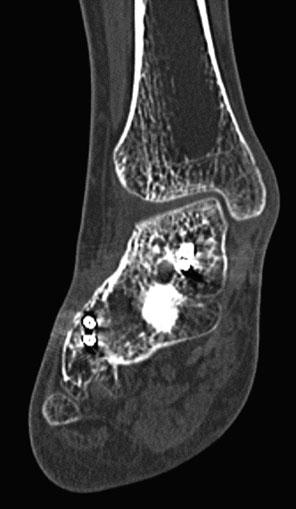
6 6 F. Miller Fig. C1.1 Fig. C1.3 Fig. C1.2 Fig. C1.4


7 Ankle Valgus in Cerebral Palsy 7 Fig. C1.5 ankle shows normal alignment at the posterior half of the ankle mortice (Fig. C1.3). The anterior aspect of the ankle shows a severe defect in both the tibia and the talus which allows the ankle to collapse into severe external rotation and valgus with dorsiflexion (Figs. C1.4 and C1.5). The only available treatment for this severe instability is an ankle fusion, which becomes a pantalar fusion due to the earlier triple arthrodesis (Fig. C1.6). Case 2 Lindsey Lindsey, a 10-year-old girl with moderate diplegia, developed a significant internal tibial torsion, Fig. C1.6 which was cosmetically objectionable to her. She and her family desired this to be corrected with a tibial osteotomy. A percutaneous osteotomy was performed with the application of a short-leg cast and a proximal tibial pin. The radiograph in the operating room showed a significant valgus deformity of the ankle (Fig. C2.1), so the cast was wedged while she was still under anesthesia to get her ankle to neutral alignment (Fig. C2.2). In general, a little valgus is better than varus because the subtalar joint can accommodate the valgus better; however, significant valgus may place an external rotation valgus moment on the foot

 defines the size of the angular correction that needs to be made. This technique will correct")
8 8 F. Miller Fig. C2.1 causing progressive valgus collapse of the foot. The goal should be to have 0 to 5 of valgus at the ankle joint. If after the cast is applied and there is more than 10 of valgus or more than 5 of varus, the cast should be wedged and the angulation corrected. The technique for doing the wedge is to make two lines down the middle of the Fig. C2.2 fragments to be aligned, and this intersection level (Fig. C2.3A) is the level at which the cast wedge is to be placed. The triangle (Fig. C2.3B) defines the size of the angular correction that needs to be made. This technique will correct
, and at this location the width of the open wedge can be measured. This method allows precutting of a block to hold open the wedge.")

9 Ankle Valgus in Cerebral Palsy 9 Fig. C2.3 Fig. C3.1 both displacement and angulation. Also, by measuring the width of the cast on the X-ray at level A (Fig. C2.3A), you can next measure the same distance from the apex on the triangle B (Fig. C2.3B), and at this location the width of the open wedge can be measured. This method allows precutting of a block to hold open the wedge. Case 3 Kenneth Kenneth, a 16-year-old boy with significant growth delay and hypotonia, was evaluated with severe planovalgus foot deformities. He had problems tolerating his AFO. On physical examination, he was hypotonic but could walk without assistance. He had severe planovalgus feet but no muscle contractures. In the operating room his feet were reduced to normal position and fixed with a subtalor fusion, but he still tended to fall into valgus with simulated weight bearing. Under fluoroscopy, he was thought to have mild instability of the ankle joint and approximately 10 to 15 of ankle valgus, but he had no torsional malalignment. He had significant amount of growth remaining so a medial malleolar epiphysiodesis screw was placed (Fig. C3.1). He was then monitored carefully, and by the 24-month follow-up, he had acquired approximately 20 of correction, (Fig. C3.2). which could be monitored as well by the presence of a faint growth arrest line (Fig. C3.3). The screw was
 The treatment of ankle valgus by surface epiphyseodesis.")
 Surgical management of ankle valgus in children: use of a transphyseal medial malleolar screw.")
10 10 F. Miller Fig. C3.3 References Fig. C3.2 then removed when he had slight overcorrection and the foot appeared in a good position. Cross-References Planovalgus Foot Deformity in Cerebral Palsy Tibial Torsion and Knee Instability in Cerebral Palsy Beals RK (1991) The treatment of ankle valgus by surface epiphyseodesis. Clin Orthop 266 SRC GoogleScholar: Davids JR (2010) The foot and ankle in cerebral palsy. Orthop Clin North Am 41: Davids JR, Valadie AL, Ferguson RL, Bray EW III, Allen BL Jr (1997) Surgical management of ankle valgus in children: use of a transphyseal medial malleolar screw. Orthop 17 SRC GoogleScholar:3 8 Dias LS (1985) Valgus deformity of the ankle joint: pathogenesis of fibular shortening. Orthop 5 SRC GoogleScholar: Hsu LC, Yau AC, O Brien JP, Hodgson AR (1972) Valgus deformity of the ankle resulting from fibular resection for a graft in subtalar fusion in children. Joint Surg Am 54 SRC GoogleScholar: McCall RE, Lillich JS, Harris JR, Johnston FA (1985) The Grice extraarticular subtalar arthrodesis: a clinical review. Orthop 5 SRC GoogleScholar: Scott SM, Janes PC, Stevens PM (1988) Grice subtalar arthrodesis followed to skeletal maturity. Orthop 8 SRC GoogleScholar: Stevens PM, Belle RM (1997) Screw epiphyseodesis for ankle valgus. Orthop 17 SRC GoogleScholar:9 12 Tompkins M, Eberson C, Ehrlich M (2012) Hemiepiphyseal stapling for ankle valgus in multiple hereditary exostoses. Am J Orthop (Belle Mead NJ) 41: E23 E26
Growth modulation with a medial malleolar screw for ankle valgus deformity
 Acta Orthopaedica 015; 86 (5): 611 615 611 Growth modulation with a medial malleolar screw for ankle valgus deformity 79 children with 15 affected ankles followed until correction or physeal closure Martin
Acta Orthopaedica 015; 86 (5): 611 615 611 Growth modulation with a medial malleolar screw for ankle valgus deformity 79 children with 15 affected ankles followed until correction or physeal closure Martin
Multiapical Deformities p. 97 Osteotomy Concepts and Frontal Plane Realignment p. 99 Angulation Correction Axis (ACA) p. 99 Bisector Lines p.
 p. 99 Bisector Lines p.") Normal Lower Limb Alignment and Joint Orientation p. 1 Mechanical and Anatomic Bone Axes p. 1 Joint Center Points p. 5 Joint Orientation Lines p. 5 Ankle p. 5 Knee p. 5 Hip p. 8 Joint Orientation Angles
Normal Lower Limb Alignment and Joint Orientation p. 1 Mechanical and Anatomic Bone Axes p. 1 Joint Center Points p. 5 Joint Orientation Lines p. 5 Ankle p. 5 Knee p. 5 Hip p. 8 Joint Orientation Angles
Management of knee flexion contractures in patients with Cerebral Palsy
 Management of knee flexion contractures in patients with Cerebral Palsy Emmanouil Morakis Orthopaedic Consultant Royal Manchester Children s Hospital 1. Introduction 2. Natural history 3. Pathophysiology
Management of knee flexion contractures in patients with Cerebral Palsy Emmanouil Morakis Orthopaedic Consultant Royal Manchester Children s Hospital 1. Introduction 2. Natural history 3. Pathophysiology
The Valgus Foot in Cerebral Palsy Equinovalgus not Plano-Valgus. Alfred D. Grant, M.D. David Feldman, M.D.
 The Valgus Foot in Cerebral Palsy Equinovalgus not Plano-Valgus Alfred D. Grant, M.D. David Feldman, M.D. Norman Otsuka, MD M.D. THE PURPOSE OF THIS PRESENTATION IS TO STATE CLEARLY THAT THE VALGUS FOOT
The Valgus Foot in Cerebral Palsy Equinovalgus not Plano-Valgus Alfred D. Grant, M.D. David Feldman, M.D. Norman Otsuka, MD M.D. THE PURPOSE OF THIS PRESENTATION IS TO STATE CLEARLY THAT THE VALGUS FOOT
FACTS 1. Most need only Gastro aponeurotic release [in positive Silverskiold test]
![FACTS 1. Most need only Gastro aponeurotic release [in positive Silverskiold test]](/thumbs/83/88335212.jpg "FACTS 1. Most need only Gastro aponeurotic release [in positive Silverskiold test]") FOOT IN CEREBRAL PALSY GAIT IN CEREBRAL PALSY I True Equinus II Jump gait III Apparent Equinus IV Crouch gait Group I True Equinus Extended hip and knee Equinus at ankle II Jump Gait [commonest] Equinus
FOOT IN CEREBRAL PALSY GAIT IN CEREBRAL PALSY I True Equinus II Jump gait III Apparent Equinus IV Crouch gait Group I True Equinus Extended hip and knee Equinus at ankle II Jump Gait [commonest] Equinus
Intoeing: When to Worry? Sukhdeep K. Dulai SPORC 2018
 Intoeing: When to Worry? Sukhdeep K. Dulai SPORC 2018 What is it? Intoeing: When to worry? Why isn t it always cause for worry? What are the benign causes of intoeing? What are the pathologic causes of
Intoeing: When to Worry? Sukhdeep K. Dulai SPORC 2018 What is it? Intoeing: When to worry? Why isn t it always cause for worry? What are the benign causes of intoeing? What are the pathologic causes of
2/24/2014. Outline. Anterior Orthotic Management for the Chronic Post Stroke Patient. Terminology. Terminology ROM. Physical Evaluation
 Outline Anterior Orthotic Management for the Chronic Post Stroke Patient Physical Evaluation Design Considerations Orthotic Design Jason M. Jennings CPO, LPO, FAAOP jajennings@hanger.com Primary patterning
Outline Anterior Orthotic Management for the Chronic Post Stroke Patient Physical Evaluation Design Considerations Orthotic Design Jason M. Jennings CPO, LPO, FAAOP jajennings@hanger.com Primary patterning
Correction of Traumatic Ankle Valgus and Procurvatum using the Taylor Spatial Frame: A Case Report
 The Foot and Ankle Online Journal Official publication of the International Foot & Ankle Foundation Correction of Traumatic Ankle Valgus and Procurvatum using the Taylor Spatial Frame: A Case Report by
The Foot and Ankle Online Journal Official publication of the International Foot & Ankle Foundation Correction of Traumatic Ankle Valgus and Procurvatum using the Taylor Spatial Frame: A Case Report by
Treatment of malunited fractures of the ankle
 Treatment of malunited fractures of the ankle A LONG-TERM FOLLOW-UP OF RECONSTRUCTIVE SURGERY I. I. Reidsma, P. A. Nolte, R. K. Marti, E. L. F. B. Raaymakers From Academic Medical Center, Amsterdam, Netherlands
Treatment of malunited fractures of the ankle A LONG-TERM FOLLOW-UP OF RECONSTRUCTIVE SURGERY I. I. Reidsma, P. A. Nolte, R. K. Marti, E. L. F. B. Raaymakers From Academic Medical Center, Amsterdam, Netherlands
Supramalleolar wedge osteotomy: a method of correcting fixed equinus and associated deformities in children
 The Foot 15 (2005) 33 39 Supramalleolar wedge osteotomy: a method of correcting fixed equinus and associated deformities in children John E. Handelsman, Jacob Weinberg Schneider Children s Hospital, Division
The Foot 15 (2005) 33 39 Supramalleolar wedge osteotomy: a method of correcting fixed equinus and associated deformities in children John E. Handelsman, Jacob Weinberg Schneider Children s Hospital, Division
Physeal Fractures and Growth Arrest
 Physeal Fractures and Growth Arrest Raymond W. Liu, M.D. Victor M. Goldberg Master Clinician-Scientist in Orthopaedics Rainbow Babies and Children s Hospital Case Western Reserve University Outline General
Physeal Fractures and Growth Arrest Raymond W. Liu, M.D. Victor M. Goldberg Master Clinician-Scientist in Orthopaedics Rainbow Babies and Children s Hospital Case Western Reserve University Outline General
Preliminary Outcome Using a New Free Motion Offloading KAFO for Postoperative Management of Hemiepiphysiodesis in Adolescent Tibia Vara
 Preliminary Outcome Using a New Free Motion Offloading KAFO for Postoperative Management of Hemiepiphysiodesis in Adolescent Tibia Vara Joseph W. Whiteside CO/LO 1399 E. Western Reserve Road, Poland, OH
Preliminary Outcome Using a New Free Motion Offloading KAFO for Postoperative Management of Hemiepiphysiodesis in Adolescent Tibia Vara Joseph W. Whiteside CO/LO 1399 E. Western Reserve Road, Poland, OH
LCP Anterior Ankle Arthrodesis Plates. Part of the Synthes Locking Compression Plate (LCP) System.
 System.") LCP Anterior Ankle Arthrodesis Plates. Part of the Synthes Locking Compression Plate (LCP) System. Technique Guide Instruments and implants approved by the AO Foundation Table of Contents Introduction
LCP Anterior Ankle Arthrodesis Plates. Part of the Synthes Locking Compression Plate (LCP) System. Technique Guide Instruments and implants approved by the AO Foundation Table of Contents Introduction
ANKLE ARTHRODESIS Discussion, technical tips, your problems?
 ANKLE ARTHRODESIS Discussion, technical tips, your problems? Integra TM Ankle Days Ankle and HindfootTraining May 09th & 10th 2014 Brussels, Belgium J. de Halleux Ankle arthrodesis - Indications Arthritis
ANKLE ARTHRODESIS Discussion, technical tips, your problems? Integra TM Ankle Days Ankle and HindfootTraining May 09th & 10th 2014 Brussels, Belgium J. de Halleux Ankle arthrodesis - Indications Arthritis
Gentle Guided Growth to Correct Knock Knees and Bowed Legs in Children
 PATIENT INFORMATION Gentle Guided Growth to Correct Knock Knees and Bowed Legs in Children The Guided Growth System eight-plate quad-plate INTRODUCTION Children need gentle guidance and correction in many
PATIENT INFORMATION Gentle Guided Growth to Correct Knock Knees and Bowed Legs in Children The Guided Growth System eight-plate quad-plate INTRODUCTION Children need gentle guidance and correction in many
Theuseofgaitanalysisin orthopaedic surgical treatment in children with cerebral palsy
 Theuseofgaitanalysisin orthopaedic surgical treatment in children with cerebral palsy Aim of treatment Correction of functional disorder Requires analysis of function Basis for decision making Basis for
Theuseofgaitanalysisin orthopaedic surgical treatment in children with cerebral palsy Aim of treatment Correction of functional disorder Requires analysis of function Basis for decision making Basis for
Hemiepiphyseal stapling for treatment of genu valgum: A case report
 Hemiepiphyseal stapling for treatment of genu valgum: A case report Nina Agrawal, BA, Danielle Cameron, BA, Lawrence Wells, MD Abstract A 12-year-old girl underwent a bilateral distal femoral and proximal
Hemiepiphyseal stapling for treatment of genu valgum: A case report Nina Agrawal, BA, Danielle Cameron, BA, Lawrence Wells, MD Abstract A 12-year-old girl underwent a bilateral distal femoral and proximal
PRONATION-ABDUCTION FRACTURES
 C H A P T E R 1 2 PRONATION-ABDUCTION FRACTURES George S. Gumann, DPM (The opinions of the author should not be considered as reflecting official policy of the US Army Medical Department.) Pronation-abduction
C H A P T E R 1 2 PRONATION-ABDUCTION FRACTURES George S. Gumann, DPM (The opinions of the author should not be considered as reflecting official policy of the US Army Medical Department.) Pronation-abduction
Use of the 20 Memory Staple in Osteotomies of Fusions of the Forefoot
 168 Forefoot Reconstruction Use of the 20 Memory Staple in Osteotomies of Fusions of the Forefoot Definition, History, Generalities This staple first provides a permanent compression both in the prongs
168 Forefoot Reconstruction Use of the 20 Memory Staple in Osteotomies of Fusions of the Forefoot Definition, History, Generalities This staple first provides a permanent compression both in the prongs
BIOMECHANICAL EXAMINATION OF THE PEDIATRIC LOWER EXTREMITY
 BIOMECHANICAL EXAMINATION OF THE PEDIATRIC LOWER EXTREMITY B.Resseque, D.P.M. ARCH HEIGHT OFF WEIGHTBEARING Evaluate arch height by placing a ruler from the heel to the first metatarsal head Compare arch
BIOMECHANICAL EXAMINATION OF THE PEDIATRIC LOWER EXTREMITY B.Resseque, D.P.M. ARCH HEIGHT OFF WEIGHTBEARING Evaluate arch height by placing a ruler from the heel to the first metatarsal head Compare arch
Financial Disclosure. The authors have not received any financial support for the preparation of this work.
 Persistent Clubfoot Deformity Following Treatment by the Ponseti Method W.B. Lehman, M.D. Alice Chu, M.D. New York Ponseti Clubfoot Center Department of Pediatric Orthopaedic Surgery Financial Disclosure
Persistent Clubfoot Deformity Following Treatment by the Ponseti Method W.B. Lehman, M.D. Alice Chu, M.D. New York Ponseti Clubfoot Center Department of Pediatric Orthopaedic Surgery Financial Disclosure
Fractures of the Ankle Region in the Skeletally Immature Patient. The Salter Classification is Worthless!!
 Fractures of the Ankle Region in the Skeletally Immature Patient. The Salter Classification is Worthless!! Kaye E Wilkins D.V.M,M.D. President's Council/Dielmann Chair in Pediatric Orthopedics Professor
Fractures of the Ankle Region in the Skeletally Immature Patient. The Salter Classification is Worthless!! Kaye E Wilkins D.V.M,M.D. President's Council/Dielmann Chair in Pediatric Orthopedics Professor
BIOMECHANICAL EXAMINATION OF THE PEDIATRIC LOWER EXTREMITY 2017
 BIOMECHANICAL EXAMINATION OF THE PEDIATRIC LOWER EXTREMITY 2017 B. RESSEQUE, D.P.M., D.A.B.P.O. Professor, N.Y. College of Podiatric Medicine ARCH HEIGHT OFF WEIGHTBEARING Evaluate arch height by placing
BIOMECHANICAL EXAMINATION OF THE PEDIATRIC LOWER EXTREMITY 2017 B. RESSEQUE, D.P.M., D.A.B.P.O. Professor, N.Y. College of Podiatric Medicine ARCH HEIGHT OFF WEIGHTBEARING Evaluate arch height by placing
FIBULAR & SYNDESMOSIS MALUNIONS
 FIBULAR & SYNDESMOSIS MALUNIONS MICHAEL P. CLARE, MD FLORIDA ORTHOPAEDIC INSTITUTE TAMPA, FL USA MORTISE INHERENTLY UNSTABLE LATERAL MALLEOLUS ACTS AS BUTTRESS / POST RESIST LATERAL TRANSLATION OF TALUS
FIBULAR & SYNDESMOSIS MALUNIONS MICHAEL P. CLARE, MD FLORIDA ORTHOPAEDIC INSTITUTE TAMPA, FL USA MORTISE INHERENTLY UNSTABLE LATERAL MALLEOLUS ACTS AS BUTTRESS / POST RESIST LATERAL TRANSLATION OF TALUS
Scar Engorged veins. Size of the foot [In clubfoot, small foot]
![Scar Engorged veins. Size of the foot [In clubfoot, small foot]](/thumbs/78/77722241.jpg "Scar Engorged veins. Size of the foot [In clubfoot, small foot]") 6. FOOT HISTORY Pain: Walking, Running Foot wear problem Swelling; tingly feeling Deformity Stiffness Disability: At work; recreation; night; walk; ADL, Sports Previous Rx Comorbidities Smoke, Sugar, Steroid
6. FOOT HISTORY Pain: Walking, Running Foot wear problem Swelling; tingly feeling Deformity Stiffness Disability: At work; recreation; night; walk; ADL, Sports Previous Rx Comorbidities Smoke, Sugar, Steroid
2017 Resident Advanced Trauma Techniques Course COMPLICATIONS / CHALLENGES MALUNIONS/DEFORMITY
 2017 Resident Advanced Trauma Techniques Course COMPLICATIONS / CHALLENGES MALUNIONS/DEFORMITY What is a Malunion? Definition: a fracture that has healed in a nonanatomic (i.e. deformed) position Must
2017 Resident Advanced Trauma Techniques Course COMPLICATIONS / CHALLENGES MALUNIONS/DEFORMITY What is a Malunion? Definition: a fracture that has healed in a nonanatomic (i.e. deformed) position Must
Duration of Follow-up (mo)
") Page 1 of 7 Fig. E-1 Fig. E-2 Fig. E-1 Medial ankle arthritis with medial translation of the talus and mortise widening. Note the shape of the medial malleolus (white arrow). Fig. E-2 Measurement of mortise
Page 1 of 7 Fig. E-1 Fig. E-2 Fig. E-1 Medial ankle arthritis with medial translation of the talus and mortise widening. Note the shape of the medial malleolus (white arrow). Fig. E-2 Measurement of mortise
radiologymasterclass.co.uk
 http://radiologymasterclass.co.uk Hip X-ray anatomy - Normal AP (anterior-posterior) Shenton's line is formed by the medial edge of the femoral neck and the inferior edge of the superior pubic ramus Loss
http://radiologymasterclass.co.uk Hip X-ray anatomy - Normal AP (anterior-posterior) Shenton's line is formed by the medial edge of the femoral neck and the inferior edge of the superior pubic ramus Loss
Surgical Correction of Lower Extremity Deformities by Triple Arthrodesis
 Surgical Correction of Lower Extremity Deformities by Triple Arthrodesis 足踝畸形矯治 振興醫療財團法人振興醫院 骨科部 熊永萬醫師 Introduction: The primary goals of a triple arthrodesis are to relieve pain from arthritic, deformed,
Surgical Correction of Lower Extremity Deformities by Triple Arthrodesis 足踝畸形矯治 振興醫療財團法人振興醫院 骨科部 熊永萬醫師 Introduction: The primary goals of a triple arthrodesis are to relieve pain from arthritic, deformed,
INVISION Total Ankle Replacement System with PROPHECY Preoperative Navigation Revision of a Failed Agility Total Ankle Replacement
 016625 REVISION R INVISION Total Ankle Replacement System with PROPHECY Preoperative Navigation Revision of a Failed Agility Total Ankle Replacement CASE STUDY Patient History The patient was a 65-year-old
016625 REVISION R INVISION Total Ankle Replacement System with PROPHECY Preoperative Navigation Revision of a Failed Agility Total Ankle Replacement CASE STUDY Patient History The patient was a 65-year-old
Distal tibial physeal arrest after meningococcal septicaemia
 CHILDREN S ORTHOPAEDICS Distal tibial physeal arrest after meningococcal septicaemia MANAGEMENT AND OUTCOME IN SEVEN ANKLES F. P. Monsell, J. R. Barnes, R. Kirubanandan, A. M. B. McBride From Bristol Royal
CHILDREN S ORTHOPAEDICS Distal tibial physeal arrest after meningococcal septicaemia MANAGEMENT AND OUTCOME IN SEVEN ANKLES F. P. Monsell, J. R. Barnes, R. Kirubanandan, A. M. B. McBride From Bristol Royal
Other Congenital and Developmental Diseases of the Foot. Department of Orthopedic Surgery St. Vincent s s Hospital, The Catholic University
 Other Congenital and Developmental Diseases of the Foot Department of Orthopedic Surgery St. Vincent s s Hospital, The Catholic University Contents Metatarsus Adductus Skewfoot Hallux Valgus Hallux Valgus
Other Congenital and Developmental Diseases of the Foot Department of Orthopedic Surgery St. Vincent s s Hospital, The Catholic University Contents Metatarsus Adductus Skewfoot Hallux Valgus Hallux Valgus
Correction of rotational deformity of the tibia in cerebral palsy by percutaneous supramalleolar osteotomy
 Correction of rotational deformity of the tibia in cerebral palsy by percutaneous supramalleolar osteotomy M. Inan, F. Ferri-de Baros, G. Chan, K. Dabney, F. Miller From The Alfred I. DuPont Hospital for
Correction of rotational deformity of the tibia in cerebral palsy by percutaneous supramalleolar osteotomy M. Inan, F. Ferri-de Baros, G. Chan, K. Dabney, F. Miller From The Alfred I. DuPont Hospital for
Dropfoot - Video Gait Analysis - Craig A. Camasta, DPM, FACFAS Atlanta, Georgia, USA
 Equinus, Pes Cavus and Dropfoot - Video Gait Analysis - Craig A. Camasta, DPM, FACFAS Atlanta, Georgia, USA Equinus = Toe Walker Soft Tissue Static fixed contracture Dynamic spastic, hypertonic Bone Procurvatum,,
Equinus, Pes Cavus and Dropfoot - Video Gait Analysis - Craig A. Camasta, DPM, FACFAS Atlanta, Georgia, USA Equinus = Toe Walker Soft Tissue Static fixed contracture Dynamic spastic, hypertonic Bone Procurvatum,,
Toe walking gives rise to parental concern. Therefore, toe-walkers are often referred at the 3 years of age.
 IDIOPATHIC TOE WALKING Toe walking is a common feature in immature gait and is considered normal up to 3 years of age. As walking ability improves, initial contact is made with the heel. Toe walking gives
IDIOPATHIC TOE WALKING Toe walking is a common feature in immature gait and is considered normal up to 3 years of age. As walking ability improves, initial contact is made with the heel. Toe walking gives
, MD. physiologic. tibia varum. in utero (in. Disease in. variation. positioning. back and legs. instead of. Blount's. Infant with bowing in both legs
 North Jersey Orthopaedic Institute Rutgers, The Statee University of New Jersey 140 Bergen Street, D1610 Newark, NJ 07101 973-972-2150 South Orange Ambulatory Center Hackensack Medical Plaza Overlook Medical
North Jersey Orthopaedic Institute Rutgers, The Statee University of New Jersey 140 Bergen Street, D1610 Newark, NJ 07101 973-972-2150 South Orange Ambulatory Center Hackensack Medical Plaza Overlook Medical
Triple Arthrodesis of Foot for Correction of Lower Extremity Deformities
 Triple Arthrodesis of Foot for Correction of Lower Extremity Deformities 振興醫療財團法人振興醫院骨科部 * 熊永萬 A triple arthrodesis consists of surgical fusion of the talocalcaneal (TC), talonavicular (TN), and calcaneocuboid
Triple Arthrodesis of Foot for Correction of Lower Extremity Deformities 振興醫療財團法人振興醫院骨科部 * 熊永萬 A triple arthrodesis consists of surgical fusion of the talocalcaneal (TC), talonavicular (TN), and calcaneocuboid
Disclosures. Syndesmosis Injury. Syndesmosis Ligaments. Objectives. Mark M. Casillas, M.D.
 Disclosures Syndesmosis Injury No relevant disclosures Mark M. Casillas, M.D. 1 Objectives Syndesmosis Ligaments Understand the syndesmosis anatomy and function Classify syndesmosis injuries Describe treatment
Disclosures Syndesmosis Injury No relevant disclosures Mark M. Casillas, M.D. 1 Objectives Syndesmosis Ligaments Understand the syndesmosis anatomy and function Classify syndesmosis injuries Describe treatment
Conversion of Pantalar fusion to total ankle replacement: A case Review. Key words: Pantalar fusion, non-union and total ankle replacement
 The Northern Ohio Foot and Ankle Journal Official Publication of the NOFA Foundation Conversion of Pantalar fusion to total ankle replacement: A case Review Author: Bryan Williams DPM 1 and Jonathan Sharpe
The Northern Ohio Foot and Ankle Journal Official Publication of the NOFA Foundation Conversion of Pantalar fusion to total ankle replacement: A case Review Author: Bryan Williams DPM 1 and Jonathan Sharpe
Cavus Foot: Subtle and Not-So-Subtle AOFAS Resident Review Course September 28, 2013
 Cavus Foot: Subtle and Not-So-Subtle Course September 28, 2013 Matthew M. Roberts, MD Associate Professor of Clinical Orthopaedic Surgery Co-Chief, Foot and Ankle Service Hospital for Special Surgery Disclosure
Cavus Foot: Subtle and Not-So-Subtle Course September 28, 2013 Matthew M. Roberts, MD Associate Professor of Clinical Orthopaedic Surgery Co-Chief, Foot and Ankle Service Hospital for Special Surgery Disclosure
V osteotomy and Ilizarov technique for residual idiopathic or neurogenic clubfeet
 Journal of Orthopaedic Surgery 2008;16(2):215-9 V osteotomy and Ilizarov technique for residual idiopathic or neurogenic clubfeet E Segev, E Ezra, M Yaniv, S Wientroub, Y Hemo Department of Pediatric Orthopaedics,
Journal of Orthopaedic Surgery 2008;16(2):215-9 V osteotomy and Ilizarov technique for residual idiopathic or neurogenic clubfeet E Segev, E Ezra, M Yaniv, S Wientroub, Y Hemo Department of Pediatric Orthopaedics,
Lower Extremity Alignment: Genu Varum / Valgum
 Lower Extremity Alignment: Genu Varum / Valgum Arthur B Meyers, MD Nemours Children s Hospital & Health System Associate Professor of Radiology, University of Central Florida Clinical Associate Professor
Lower Extremity Alignment: Genu Varum / Valgum Arthur B Meyers, MD Nemours Children s Hospital & Health System Associate Professor of Radiology, University of Central Florida Clinical Associate Professor
10/26/2017. Comprehensive & Coordinated Orthopaedic Management of Children with CP. Objectives. It s all about function. Robert Bruce, MD Sayan De, MD
 Comprehensive & Coordinated Orthopaedic Management of Children with CP Robert Bruce, MD Sayan De, MD Objectives Understand varying levels of intervention are available to optimize function of children
Comprehensive & Coordinated Orthopaedic Management of Children with CP Robert Bruce, MD Sayan De, MD Objectives Understand varying levels of intervention are available to optimize function of children
Supramalleolar derotation osteotomy of the tibia, with T plate fixation
 Supramalleolar derotation osteotomy of the tibia, with T plate fixation TECHNIQUE AND RESULTS IN PATIENTS WITH NEUROMUSCULAR DISEASE P. Selber, E. R. Filho, R. Dallalana, M. Pirpiris, G. R. Nattrass, H.
Supramalleolar derotation osteotomy of the tibia, with T plate fixation TECHNIQUE AND RESULTS IN PATIENTS WITH NEUROMUSCULAR DISEASE P. Selber, E. R. Filho, R. Dallalana, M. Pirpiris, G. R. Nattrass, H.
Orthotic Management for Children with Cerebral Palsy
 Orthotic Management for Children with Cerebral Palsy Brian Emling, MSPO, CPO, LPO Brian.emling@choa.org Karl Barner, CPO, LPO karl.barner@choa.org Learning Objectives Inform audience of the general services
Orthotic Management for Children with Cerebral Palsy Brian Emling, MSPO, CPO, LPO Brian.emling@choa.org Karl Barner, CPO, LPO karl.barner@choa.org Learning Objectives Inform audience of the general services
BIOMECHANICS OF ANKLE FRACTURES
 BIOMECHANICS OF ANKLE FRACTURES William R Reinus, MD MBA FACR Significance of Ankle Fractures Most common weight-bearing Fx 70% of all Fxs Incidence is increasing Bimodal distribution Men 15-24 Women over
BIOMECHANICS OF ANKLE FRACTURES William R Reinus, MD MBA FACR Significance of Ankle Fractures Most common weight-bearing Fx 70% of all Fxs Incidence is increasing Bimodal distribution Men 15-24 Women over
Multiple Exostoses / Multiple Osteochondroma of the Lower Limb Guide By Dror Paley M.D.,
 Multiple Exostoses / Multiple Osteochondroma of the Lower Limb Guide By Dror Paley M.D., Director of the Paley Advanced Limb Lengthening Institute at St. Mary s Hospital in West Palm Beach, Florida. Located
Multiple Exostoses / Multiple Osteochondroma of the Lower Limb Guide By Dror Paley M.D., Director of the Paley Advanced Limb Lengthening Institute at St. Mary s Hospital in West Palm Beach, Florida. Located
Second Course Motion Analysis and clinics: why set up a Motion Analysis Lab?? TRAMA Project. January th Clinical case presentation
 Second Course Motion Analysis and clinics: why set up a Motion Analysis Lab?? - Clinical cases presentation - TRAMA Project January 14-17 th 2008 Iván Carlos Uribe Prada Instituto de Ortopedia Infantil
Second Course Motion Analysis and clinics: why set up a Motion Analysis Lab?? - Clinical cases presentation - TRAMA Project January 14-17 th 2008 Iván Carlos Uribe Prada Instituto de Ortopedia Infantil
AACPDM IC#21 DFEO+PTA 1
 Roles of Distal Femoral Extension Osteotomy and Patellar Tendon Advancement in the Treatment of Severe Persistent Crouch Gait in Adolescents and Young Adults with Cerebral Palsy Instructional Course #21
Roles of Distal Femoral Extension Osteotomy and Patellar Tendon Advancement in the Treatment of Severe Persistent Crouch Gait in Adolescents and Young Adults with Cerebral Palsy Instructional Course #21
A Patient s Guide to Adult-Acquired Flatfoot Deformity
 A Patient s Guide to Adult-Acquired Flatfoot Deformity Glendale Adventist Medical Center 1509 Wilson Terrace Glendale, CA 91206 Phone: (818) 409-8000 DISCLAIMER: The information in this booklet is compiled
A Patient s Guide to Adult-Acquired Flatfoot Deformity Glendale Adventist Medical Center 1509 Wilson Terrace Glendale, CA 91206 Phone: (818) 409-8000 DISCLAIMER: The information in this booklet is compiled
RADIOGRAPHY OF THE ANKLE and LOWER LEG
 RADIOGRAPHY OF THE ANKLE and LOWER LEG Patient Position: ANKLE AP Projection Part Position: True Slight to place foot s long axis Center to Central Ray: to IR Midway Note: Ankle joint is to tips of malleoli
RADIOGRAPHY OF THE ANKLE and LOWER LEG Patient Position: ANKLE AP Projection Part Position: True Slight to place foot s long axis Center to Central Ray: to IR Midway Note: Ankle joint is to tips of malleoli
Proximal metatarsal osteotomy and distal soft tissue reconstruction as treatment for hallux valgus deformity
 REVIEW Proximal metatarsal osteotomy and distal soft tissue reconstruction as treatment for hallux valgus deformity Michael J. Coughlin and J. Speight Grimes Boise, Idaho, USA (Received for publication
REVIEW Proximal metatarsal osteotomy and distal soft tissue reconstruction as treatment for hallux valgus deformity Michael J. Coughlin and J. Speight Grimes Boise, Idaho, USA (Received for publication
Lower Extremity Orthopedic Surgery in Cerebral Palsy
 Lower Extremity Orthopedic Surgery in Cerebral Palsy Hank Chambers, MD San Diego Children s Hospital San Diego, California Indications Fixed contracture Joint dislocations Shoe wear problems Pain Perineal
Lower Extremity Orthopedic Surgery in Cerebral Palsy Hank Chambers, MD San Diego Children s Hospital San Diego, California Indications Fixed contracture Joint dislocations Shoe wear problems Pain Perineal
Results of Calcaneal Osteotomy & Flexor Digitorum Longus transfer in Stage II Acquired Flatfoot Deformity
 Results of Calcaneal Osteotomy & Flexor Digitorum Longus transfer in Stage II Acquired Flatfoot Deformity Mr Amit Chauhan Mr Prasad Karpe Ms Maire-claire Killen Mr Rajiv Limaye University Hospital of North
Results of Calcaneal Osteotomy & Flexor Digitorum Longus transfer in Stage II Acquired Flatfoot Deformity Mr Amit Chauhan Mr Prasad Karpe Ms Maire-claire Killen Mr Rajiv Limaye University Hospital of North
Physeal injuries of the ankle joint constitute 11% of all
 ORIGINAL ARTICLE Outcome of Physeal and Epiphyseal Injuries of the Distal Tibia With Intra-Articular Involvement Savvas P. Nenopoulos, MD, Vasilios A. Papavasiliou, MD, and Athanasios V. Papavasiliou,
ORIGINAL ARTICLE Outcome of Physeal and Epiphyseal Injuries of the Distal Tibia With Intra-Articular Involvement Savvas P. Nenopoulos, MD, Vasilios A. Papavasiliou, MD, and Athanasios V. Papavasiliou,
AAP Boot Camp KNEE AND ANKLE EXAM
 AAP Boot Camp KNEE AND ANKLE EXAM Disclosures I have no relevant financial relationships with the manufacturers of any commercial products and or providers of commercial services discussed in this CME
AAP Boot Camp KNEE AND ANKLE EXAM Disclosures I have no relevant financial relationships with the manufacturers of any commercial products and or providers of commercial services discussed in this CME
Deformity and Pain in Foot of Neuromuscular Disease
 Deformity and Pain in Foot of Neuromuscular Disease CHA 의과학대학재활의학과김민영 (2012.11.10 제 4 회대한발의학회 ) Neuromuscular Diseases & Foot Deformity : almost Pain : infrequent Non-ambulatory, Ambulatory Neuromuscular
Deformity and Pain in Foot of Neuromuscular Disease CHA 의과학대학재활의학과김민영 (2012.11.10 제 4 회대한발의학회 ) Neuromuscular Diseases & Foot Deformity : almost Pain : infrequent Non-ambulatory, Ambulatory Neuromuscular
Metatarsus adductus, Skew foot, Club foot 성균관대학교삼성창원병원 장현정
 Metatarsus adductus, Skew foot, Club foot 성균관대학교삼성창원병원 장현정 Metatarsus adductus Epidemiology and Etiology 0.1-12% with higher number for multiple birth Deformation and compression from intrauterine crowding
Metatarsus adductus, Skew foot, Club foot 성균관대학교삼성창원병원 장현정 Metatarsus adductus Epidemiology and Etiology 0.1-12% with higher number for multiple birth Deformation and compression from intrauterine crowding
Application of Cast Brace for Post Acute Care of Lower Extremity Fractures
 Application of Cast Brace for Post Acute Care of Lower Extremity Fractures Roy Snelson, C.P.O.*, George Irons, C.P.O.**, and Vert Mooney, M.D.*** The fracture cast brace is designed to allow early ambulation
Application of Cast Brace for Post Acute Care of Lower Extremity Fractures Roy Snelson, C.P.O.*, George Irons, C.P.O.**, and Vert Mooney, M.D.*** The fracture cast brace is designed to allow early ambulation
X-Ray Rounds: (Plain) Radiographic Evaluation of the Ankle.
 Radiographic Evaluation of the Ankle.") X-Ray Rounds: (Plain) Radiographic Evaluation of the Ankle www.fisiokinesiterapia.biz Anatomy Complex hinge joint Articulations among: Fibula Tibia Talus Tibial plafond Distal tibial articular surface
X-Ray Rounds: (Plain) Radiographic Evaluation of the Ankle www.fisiokinesiterapia.biz Anatomy Complex hinge joint Articulations among: Fibula Tibia Talus Tibial plafond Distal tibial articular surface
Introduction. The primary function of the ankle and foot is to absorb shock and impart thrust to the body during walking.
 The ankle 1 Introduction The primary function of the ankle and foot is to absorb shock and impart thrust to the body during walking. OSTEOLOGRY The term ankle refers primarily to the talocrural joint,
The ankle 1 Introduction The primary function of the ankle and foot is to absorb shock and impart thrust to the body during walking. OSTEOLOGRY The term ankle refers primarily to the talocrural joint,
Evidence-Based Examination of the Foot Presented by Alexis Wright, PT, PhD, DPT, FAAOMPT Practice Sessions/Skill Check-offs
 Evidence-Based Examination of the Foot Presented by Alexis Wright, PT, PhD, DPT, FAAOMPT Practice Sessions/Skill Check-offs Module Five: Movement Assessment of the Foot/Ankle (1 hour CEU Time) Skilled
Evidence-Based Examination of the Foot Presented by Alexis Wright, PT, PhD, DPT, FAAOMPT Practice Sessions/Skill Check-offs Module Five: Movement Assessment of the Foot/Ankle (1 hour CEU Time) Skilled
Financial Disclosure. Turf Toe
 Seth O Brien, CP, LP Financial Disclosure Mr. Seth O'Brien has no relevant financial relationships with commercial interests to disclose. Turf Toe Common in athletes playing on firm, artificial turf Forceful
Seth O Brien, CP, LP Financial Disclosure Mr. Seth O'Brien has no relevant financial relationships with commercial interests to disclose. Turf Toe Common in athletes playing on firm, artificial turf Forceful
Early experience with medial femoral tension band plating in idiopathic genu valgum
 J Child Orthop (2011) 5:11 17 DOI 10.1007/s11832-010-0310-6 ORIGINAL CLINICAL ARTICLE Early experience with medial femoral tension band plating in idiopathic genu valgum Humberto Guzman Burt Yaszay Vanessa
J Child Orthop (2011) 5:11 17 DOI 10.1007/s11832-010-0310-6 ORIGINAL CLINICAL ARTICLE Early experience with medial femoral tension band plating in idiopathic genu valgum Humberto Guzman Burt Yaszay Vanessa
Retrospective Studies & Results in Foot & Ankle Reconstruction
 C A S E S T U D I E S Sheffield Ring Fixators XCaliber Fixators Orthofix wishes to thank the surgeons listed below for their contributions to this series, with special thanks to the key contributor, Dr.
C A S E S T U D I E S Sheffield Ring Fixators XCaliber Fixators Orthofix wishes to thank the surgeons listed below for their contributions to this series, with special thanks to the key contributor, Dr.
SUBTALAR ARTHROEREISIS IN THE OLDER PATIENT
 C H A P T E R 1 7 SUBTALAR ARTHROEREISIS IN THE OLDER PATIENT William D. Fishco, DPM, MS INTRODUCTION Arthroereisis is a surgical procedure designed to limit the motion of a joint. Subtalar joint arthroereisis
C H A P T E R 1 7 SUBTALAR ARTHROEREISIS IN THE OLDER PATIENT William D. Fishco, DPM, MS INTRODUCTION Arthroereisis is a surgical procedure designed to limit the motion of a joint. Subtalar joint arthroereisis
A Patient s Guide to Rotational Deformities in Children
 A Patient s Guide to Rotational Deformities in Children 2350 Royal Boulevard Suite 200 Elgin, IL 60123 Phone: 847.931.5300 Fax: 847.931.9072 DISCLAIMER: The information in this booklet is compiled from
A Patient s Guide to Rotational Deformities in Children 2350 Royal Boulevard Suite 200 Elgin, IL 60123 Phone: 847.931.5300 Fax: 847.931.9072 DISCLAIMER: The information in this booklet is compiled from
ASSESSING GAIT IN CHILDREN WITH CP: WHAT TO DO WHEN YOU CAN T USE A GAIT LAB
 ASSESSING GAIT IN CHILDREN WITH CP: WHAT TO DO WHEN YOU CAN T USE A GAIT LAB Robert M. Kay, MD Vice Chief, Children s Orthopaedic Center Children s Hospital Los Angeles Professor of Orthopaedic Surgery
ASSESSING GAIT IN CHILDREN WITH CP: WHAT TO DO WHEN YOU CAN T USE A GAIT LAB Robert M. Kay, MD Vice Chief, Children s Orthopaedic Center Children s Hospital Los Angeles Professor of Orthopaedic Surgery
Load Response of the Hindfoot Bones in patients with the Ankle Osteoarthritis : in vivo 3D study
 Load Response of the Hindfoot Bones in patients with the Ankle Osteoarthritis : in vivo D study Hara Y, Ikoma K, Kido M, Imai K, Maki M, Takatori R, Tokunaga D, Inoue N,, Kubo T Department of Orthopaedics,
Load Response of the Hindfoot Bones in patients with the Ankle Osteoarthritis : in vivo D study Hara Y, Ikoma K, Kido M, Imai K, Maki M, Takatori R, Tokunaga D, Inoue N,, Kubo T Department of Orthopaedics,
AOFAS 2012 ANNUAL SUMMER MEETING. Subtalar Distraction Two Bone-Block Arthrodesis for Calcaneal Malunion
 AOFAS 2012 ANNUAL SUMMER MEETING Subtalar Distraction Two Bone-Block Arthrodesis for Calcaneal Malunion My disclosure is in the Final AOFAS Program Book. I have no potential conflicts with this presentation.
AOFAS 2012 ANNUAL SUMMER MEETING Subtalar Distraction Two Bone-Block Arthrodesis for Calcaneal Malunion My disclosure is in the Final AOFAS Program Book. I have no potential conflicts with this presentation.
MANUAL PRODUCT 3 RD EDITION. Pediatric Ankle Joint P: F: BeckerOrthopedic.com.
 PRODUCT MANUAL 3 RD EDITION P: 800-521-2192 248-588-7480 F: 800-923-2537 248-588-2960 BeckerOrthopedic.com Patent Pending 2018 Becker Orthopedic Appliance Co. All rights reserved. TRIPLE ACTION DIFFERENCE
PRODUCT MANUAL 3 RD EDITION P: 800-521-2192 248-588-7480 F: 800-923-2537 248-588-2960 BeckerOrthopedic.com Patent Pending 2018 Becker Orthopedic Appliance Co. All rights reserved. TRIPLE ACTION DIFFERENCE
PediLoc Extension Osteotomy Plate (PLEO)
") PediLoc Extension Osteotomy Plate (PLEO) Left PLEO Plates Sizes: 6, 8 and 10 hole plates Right PLEO Plates Sizes: 6, 8 and 10 hole plates PediLoc Extension Osteotomy Plate The technique description herein
PediLoc Extension Osteotomy Plate (PLEO) Left PLEO Plates Sizes: 6, 8 and 10 hole plates Right PLEO Plates Sizes: 6, 8 and 10 hole plates PediLoc Extension Osteotomy Plate The technique description herein
TENDON TRANSFER IN CAVUS FOOT
 TENDON TRANSFER IN CAVUS FOOT Cavovarus deformity is defined by fixed equinus of the forefoot on the hindfoot, resulting in a pathologic elevation of the longitudinal arch, with either a fixed or flexible
TENDON TRANSFER IN CAVUS FOOT Cavovarus deformity is defined by fixed equinus of the forefoot on the hindfoot, resulting in a pathologic elevation of the longitudinal arch, with either a fixed or flexible
Competence of the Deltoid Ligament in Bimalleolar Ankle Fractures After Medial Malleolar Fixation *
 Competence of the Deltoid Ligament in Bimalleolar Ankle Fractures After Medial Malleolar Fixation * BY PAUL TORNETTA, III, M.D. Investigation performed at Kings County Hospital, New York, N.Y. Abstract
Competence of the Deltoid Ligament in Bimalleolar Ankle Fractures After Medial Malleolar Fixation * BY PAUL TORNETTA, III, M.D. Investigation performed at Kings County Hospital, New York, N.Y. Abstract
SUBTLE CAVUS IN SPORTS INJURIES
 SUBTLE CAVUS IN SPORTS INJURIES MICHAEL P. CLARE, MD FLORIDA ORTHOPAEDIC INSTITUTE TAMPA, FL USA NON-NEUROMUSCULAR NORMAL VARIANT: 20-25% INCIDENCE LEDOUX, ET AL. FAI 24, 2003 FOREFOOT-DRIVEN / MORE SUBTLE
SUBTLE CAVUS IN SPORTS INJURIES MICHAEL P. CLARE, MD FLORIDA ORTHOPAEDIC INSTITUTE TAMPA, FL USA NON-NEUROMUSCULAR NORMAL VARIANT: 20-25% INCIDENCE LEDOUX, ET AL. FAI 24, 2003 FOREFOOT-DRIVEN / MORE SUBTLE
Physical Examination of the Foot & Ankle
 Inspection Standing, feet straight forward facing toward examiner Swelling Deformity Flatfoot (pes planus and hindfoot valgus) High arch (pes cavus and hindfoot varus) Peek-a-boo heel Varus Too many toes
Inspection Standing, feet straight forward facing toward examiner Swelling Deformity Flatfoot (pes planus and hindfoot valgus) High arch (pes cavus and hindfoot varus) Peek-a-boo heel Varus Too many toes
Practical Reduction Techniques: Diaphyseal Reduction. Philip Wolinsky University of California at Davis Medical Center
 OTA Specialty Day 2016 Practical Reduction Techniques: Diaphyseal Reduction Philip Wolinsky University of California at Davis Medical Center 8:55 am 9:55 am Tips and Tricks: Practical Reduction Techniques
OTA Specialty Day 2016 Practical Reduction Techniques: Diaphyseal Reduction Philip Wolinsky University of California at Davis Medical Center 8:55 am 9:55 am Tips and Tricks: Practical Reduction Techniques
Isolated congenital anterolateral bowing of the fibula : A case report with 24 years follow-up
 Acta Orthop. Belg., 2009, 75, 842-846 CASE REPORT Isolated congenital anterolateral bowing of the fibula : A case report with 24 years follow-up Karolien LELIEFELD, Hans VAN DER SLUIJS, Ibo VAN DER HAVEN
Acta Orthop. Belg., 2009, 75, 842-846 CASE REPORT Isolated congenital anterolateral bowing of the fibula : A case report with 24 years follow-up Karolien LELIEFELD, Hans VAN DER SLUIJS, Ibo VAN DER HAVEN
for children are not capable of holding the calcaneus in alignment necessary to stabilize the subtalar joint. In fact, it has come to be the opinion o
 An Effective Orthotic Design for Controlling the Unstable Subtalar Joint J. MARTIN COLSON, M.S., C.O. 1 GENE BERGLUND 2 S ome 14 years ago, Messrs. W.H. Henderson, J. W. Campbell, and others at the University
An Effective Orthotic Design for Controlling the Unstable Subtalar Joint J. MARTIN COLSON, M.S., C.O. 1 GENE BERGLUND 2 S ome 14 years ago, Messrs. W.H. Henderson, J. W. Campbell, and others at the University
HINDFOOT ARTHRODESIS FOR NEUROPATHIC DEFORMITY
 HINDFOOT ARTHRODESIS FOR NEUROPATHIC DEFORMITY Peng-Ju Huang, 1,2 Yin-Chih Fu, 3 Cheng-Chang Lu, 3 Wen-Lan Wu, 4 and Yuh-Min Cheng 2,3 1 Department of Orthopedics, Kaohsiung Municipal Hsiao-Kang Hospital,
HINDFOOT ARTHRODESIS FOR NEUROPATHIC DEFORMITY Peng-Ju Huang, 1,2 Yin-Chih Fu, 3 Cheng-Chang Lu, 3 Wen-Lan Wu, 4 and Yuh-Min Cheng 2,3 1 Department of Orthopedics, Kaohsiung Municipal Hsiao-Kang Hospital,
OTM Lecture Gait and Somatic Dysfunction of the Lower Extremity
 OTM Lecture Gait and Somatic Dysfunction of the Lower Extremity Somatic Dysfunction Tenderness Asymmetry Range of Motion Tissue Texture Changes Any one of which must be present to diagnosis somatic dysfunction.
OTM Lecture Gait and Somatic Dysfunction of the Lower Extremity Somatic Dysfunction Tenderness Asymmetry Range of Motion Tissue Texture Changes Any one of which must be present to diagnosis somatic dysfunction.
Case. 15 Y old boy presented with pain in the foot. No history of injury or any constitutional symptoms. Your diagnosis?
 Case 15 Y old boy presented with pain in the foot. No history of injury or any constitutional symptoms Your diagnosis? Diagnosis: Calcaneo-navicular tarsal coalition. C sign Talar beaking Ant eaters nose
Case 15 Y old boy presented with pain in the foot. No history of injury or any constitutional symptoms Your diagnosis? Diagnosis: Calcaneo-navicular tarsal coalition. C sign Talar beaking Ant eaters nose
Zenith. Total Ankle Replacement Surgical technique
 Total Ankle Replacement Surgical technique Contents Operative summary 4 Pre-operative planning and templating 6 Patient positioning 6 Exposure 6 Saw blades 7 Joint line definition 7 Tibial alignment jig
Total Ankle Replacement Surgical technique Contents Operative summary 4 Pre-operative planning and templating 6 Patient positioning 6 Exposure 6 Saw blades 7 Joint line definition 7 Tibial alignment jig
Fibula-related complications during bilateral tibial lengthening
 Acta Orthopaedica 2012; 83 (3): 271 275 271 Fibula-related complications during bilateral tibial lengthening 60 patients followed for mean 5 years Seung-Ju Kim, Mandar Vikas Agashe, Sang-Heon Song, and
Acta Orthopaedica 2012; 83 (3): 271 275 271 Fibula-related complications during bilateral tibial lengthening 60 patients followed for mean 5 years Seung-Ju Kim, Mandar Vikas Agashe, Sang-Heon Song, and
Fibula Lengthening Using a Modified Ilizarov Method S. Robert Rozbruch, MD; Matthew DiPaola, BA; Arkady Blyakher,MD
 Fibula Lengthening Using a Modified Ilizarov Method S. Robert Rozbruch, MD; Matthew DiPaola, BA; Arkady Blyakher,MD Limb Lengthening Service Hospital for Special Surgery Abstract A unique combination of
Fibula Lengthening Using a Modified Ilizarov Method S. Robert Rozbruch, MD; Matthew DiPaola, BA; Arkady Blyakher,MD Limb Lengthening Service Hospital for Special Surgery Abstract A unique combination of
BOW LEGS (GENU VARUM)
") BOW LEGS (GENU VARUM) By Dr John Ebnezar INTRODUCTION Have you noticed how your knees look like? If you observe carefully you will see that both your knees are not parallel but deviated slightly outwards
BOW LEGS (GENU VARUM) By Dr John Ebnezar INTRODUCTION Have you noticed how your knees look like? If you observe carefully you will see that both your knees are not parallel but deviated slightly outwards
Tibial deformity correction by Ilizarov method
 International Journal of Research in Orthopaedics http://www.ijoro.org Case Report DOI: http://dx.doi.org/10.18203/issn.2455-4510.intjresorthop20180422 Tibial deformity correction by Ilizarov method Robert
International Journal of Research in Orthopaedics http://www.ijoro.org Case Report DOI: http://dx.doi.org/10.18203/issn.2455-4510.intjresorthop20180422 Tibial deformity correction by Ilizarov method Robert
Dorsal surface-the upper area or top of the foot. Terminology
 It is important to learn the terminology as it relates to feet to properly communicate with referring physicians when necessary and to identify the relationship between the anatomical structure of the
It is important to learn the terminology as it relates to feet to properly communicate with referring physicians when necessary and to identify the relationship between the anatomical structure of the
Use of Allograft in Skeletally Immature Patients for Calcaneal Neck Lengthening Osteotomy
 Yonsei Med J 49(1):79-83, 2008 DOI 10.3349/ymj.2008.49.1.79 Use of Allograft in Skeletally Immature Patients for Calcaneal Neck Lengthening Osteotomy Yoon Hae Kwak, 1 Kun Bo Park, 2 Hui Wan Park, 1 and
Yonsei Med J 49(1):79-83, 2008 DOI 10.3349/ymj.2008.49.1.79 Use of Allograft in Skeletally Immature Patients for Calcaneal Neck Lengthening Osteotomy Yoon Hae Kwak, 1 Kun Bo Park, 2 Hui Wan Park, 1 and
Posterior Tibialis Tendon Dysfunction & Repair
 1 Posterior Tibialis Tendon Dysfunction & Repair Surgical Indications and Considerations Anatomical Considerations: The posterior tibialis muscle arises from the interosseous membrane and the adjacent
1 Posterior Tibialis Tendon Dysfunction & Repair Surgical Indications and Considerations Anatomical Considerations: The posterior tibialis muscle arises from the interosseous membrane and the adjacent
BORGinsole Measurement devices
 BORGinsole Measurement devices BORGinsole Angle-Finder Dorsal Flexion of the first Metatarsophalangeal joint - P. is sitting up on the examination table, with legs straight. - T. is sitting at the end
BORGinsole Measurement devices BORGinsole Angle-Finder Dorsal Flexion of the first Metatarsophalangeal joint - P. is sitting up on the examination table, with legs straight. - T. is sitting at the end
Calcaneus (Heel Bone) Fractures
 Fractures") Page 1 of 8 Calcaneus (Heel Bone) Fractures A fracture of the calcaneus, or heel bone, can be a painful and disabling injury. This type of fracture commonly occurs during a high-energy event such as a
Page 1 of 8 Calcaneus (Heel Bone) Fractures A fracture of the calcaneus, or heel bone, can be a painful and disabling injury. This type of fracture commonly occurs during a high-energy event such as a
Index. Clin Podiatr Med Surg 22 (2005) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Clin Podiatr Med Surg 22 (2005) 309 314 Index Note: Page numbers of article titles are in boldface type. A Abductor digiti minimi muscle, myectomy of, for tailor s bunionette, 243 Achilles tendon, lengthening
Clin Podiatr Med Surg 22 (2005) 309 314 Index Note: Page numbers of article titles are in boldface type. A Abductor digiti minimi muscle, myectomy of, for tailor s bunionette, 243 Achilles tendon, lengthening
Ankle Sprains and Their Imitators
 Ankle Sprains and Their Imitators Mark Halstead, MD Dr. Mark Halstead is the Associate Professor of the Departments of Orthopedics and Pediatrics at Washington University School of Medicine; Director of
Ankle Sprains and Their Imitators Mark Halstead, MD Dr. Mark Halstead is the Associate Professor of the Departments of Orthopedics and Pediatrics at Washington University School of Medicine; Director of
OBJECTIVES. Lower Limb Orthoses to Enhance Ambulation. Role of Orthoses in the Rehabilitation Process OBJECTIVES 3/3/2015
 OBJECTIVES Lower Limb Orthoses to Enhance Ambulation Ann Yamane, M.Ed., CO/LO University of Washington Division of Prosthetics & Orthotics Discuss the principles used in designing orthotic interventions
OBJECTIVES Lower Limb Orthoses to Enhance Ambulation Ann Yamane, M.Ed., CO/LO University of Washington Division of Prosthetics & Orthotics Discuss the principles used in designing orthotic interventions
Guided growth with tension band plate or definitive epiphysiodesis for treatment of limb length discrepancy?
 Borbas et al. Journal of Orthopaedic Surgery and Research (2019) 14:99 https://doi.org/10.1186/s13018-019-1139-4 RESEARCH ARTICLE Guided growth with tension band plate or definitive epiphysiodesis for
Borbas et al. Journal of Orthopaedic Surgery and Research (2019) 14:99 https://doi.org/10.1186/s13018-019-1139-4 RESEARCH ARTICLE Guided growth with tension band plate or definitive epiphysiodesis for
Arthrex Open Wedge Osteotomy Technique Designed in conjunction with:
 Arthrex Open Wedge Osteotomy Technique Designed in conjunction with: Dr. Giancarlo Puddu, M.D. Dr. Peter Fowler, M.D. Dr. Ned Amendola, M.D. To treat pain and instability associated with lower extremity
Arthrex Open Wedge Osteotomy Technique Designed in conjunction with: Dr. Giancarlo Puddu, M.D. Dr. Peter Fowler, M.D. Dr. Ned Amendola, M.D. To treat pain and instability associated with lower extremity
Split tendon transfers for the correction of spastic varus foot deformity: a case series study
 JOURNAL OF FOOT AND ANKLE RESEARCH RESEARCH Open Access Split tendon transfers for the correction of spastic varus foot deformity: a case series study Maria Vlachou 1*, Dimitris Dimitriadis 1,2 Abstract
JOURNAL OF FOOT AND ANKLE RESEARCH RESEARCH Open Access Split tendon transfers for the correction of spastic varus foot deformity: a case series study Maria Vlachou 1*, Dimitris Dimitriadis 1,2 Abstract
Lower Extremity Disorders in Children and Adolescents Brian G. Smith. DOI: /pir
 Lower Extremity Disorders in Children and Adolescents Brian G. Smith Pediatrics in Review 2009;30;287 DOI: 10.1542/pir.30-8-287 The online version of this article, along with updated information and services,
Lower Extremity Disorders in Children and Adolescents Brian G. Smith Pediatrics in Review 2009;30;287 DOI: 10.1542/pir.30-8-287 The online version of this article, along with updated information and services,
ROTATIONAL PILON FRACTURES
 CHAPTER 31 ROTATIONAL PILON FRACTURES George S. Gumann, DPM The opinions and commentary of the author should not be construed as refl ecting offi cial U.S. Army Medical Department policy. Pilon injuries
CHAPTER 31 ROTATIONAL PILON FRACTURES George S. Gumann, DPM The opinions and commentary of the author should not be construed as refl ecting offi cial U.S. Army Medical Department policy. Pilon injuries