Use of DXA / Bone Density in the Care of Your Patients. Brenda Lee Holbert, M.D. Associate Professor Senior Staff Radiologist
|
|
|
- Kristina Ferguson
- 6 years ago
- Views:
Transcription
1 Use of DXA / Bone Density in the Care of Your Patients Brenda Lee Holbert, M.D. Associate Professor Senior Staff Radiologist
2
3 Important Websites Resources for Clinicians and Patients health/content.html
4 Dual-Energy X-ray Absorptiometry Preferred current abbreviation DXA Some people will always use DEXA

5 The New York Times Health Guide
6 DXA Technology Detector (detects 2 tissue types - bone and soft tissue) Very low radiation to patient. Patient Very little scatter radiation to technologist Photons Collimator (pinhole for pencil beam, slit for fan beam) X-ray Source (produces 2 photon energies with different attenuation profiles)
7 What do our bones do?? Give us structure and strength Protect against injury Help us be mobile Store release minerals (calcium/phosphate)
8

9 On a city bus, an angry bus passenger grows irritated with Peter s music and threatens to break every bone in his body. Peter quickly wishes that he was boneless and collapses into a fleshy heap


10 Normal Bone: Osteoporotic
11 IOF reports: ONE in THREE women over age 50 and ONE in FIVE men over age 50 will experience osteoporotic fractures. OUCH!
12 Why Should We Care About Osteoporosis? Osteoporosis is serious - Osteoporotic fractures cause increased morbidity and mortality Good treatments are available- Fracture risk can be reduced by about 50% Osteoporosis is easy to diagnose - Bone density testing can detect osteoporosis BEFORE the first fracture occurs
13 You have probably told your patients this advice: EAT RIGHT: Get your daily recommended amounts of Calcium and Vitamin D. EXERCISE: Engage in regular weight-bearing and muscle strengthening exercise. MAINTAIN A HEALTHY LIFESTYLE: Avoid smoking and excessive alcohol consumption.
14 Two other items of advice from the National Osteoporosis Foundation TALK TO YOUR HEALTHCARE PROVIDER: Talk to your healthcare provider about bone health. GET TESTED: Have a bone density test and take medication when appropriate.
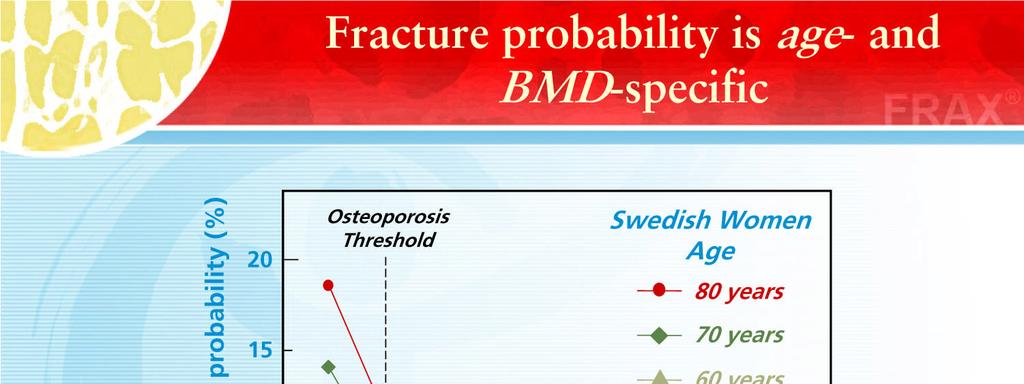
15 Why Measure BMD (bone mineral density)? BMD is a strong independent predictor of fracture risk. Clear relation of BMD and fracture risk on older women---for each standard deviation drop in BMD (in spine 10 to 12% loss), fracture risk increases 1.5 to 2.5 times
16 Why Measure BMD? Conventional radiographs good for fracture detection, insensitive for bone density loss detection Estimated that it takes about a 30% loss of bone density to show, and technique can make someone with normal BMD look like low BMD

17 Do you have criteria for who should have a DXA?? DXA---measures the BMD (Somebody must have liked alphabet soup as a kid to come up with all these initials )
18 U.S. Preventive Services Task Force recommends screening for osteoporosis in women aged 65 years or older and in younger women whose fracture risk is equal to or greater than that of a 65-year-old white woman who has no additional risk factors.
19 U.S. Preventive Services Task Force concludes that the current evidence is insufficient to assess the balance of benefits and harms of screening for osteoporosis in men.
20
21
22 Who should have BMD tested? Those with clinical red flags ISCD has recommendations (generally correspond to the red flags )
23 Red Flags History of fractures related to mild or moderate trauma (e.g., a fall from standing height or less) Family history of bone disease Low body weight Weight loss of more than 1 percent per year in the elderly Late onset of sexual development Unusual cessation of menstrual periods
24 Red Flags Anorexia nervosa (often related to marked weight reduction) Athletic amenorrhea syndrome (related to intense physical activity) Patients being treated with drugs that affect bone metabolism (e.g., glucocorticoids) Patients with diseases linked to secondary osteoporosis
25 Red Flags High levels of serum calcium or alkaline phosphatase in otherwise healthy patients Hyperparathyroidism, hyperthyroidism, or treatment with high doses of thyroid hormone Height loss or progressive spinal curvature

26 National Osteoporosis Foundation
27 Bone Health and Osteoporosis: A Report of the Surgeon General Chapter 8: Assessing the Risk of Bone Disease and Fracture


28 ISCD Official Positions 2007 Copyright ISCD, October 2007 Supersedes all prior Official Positions publications.
29 FRAX is a computer-based algorithm which uses easily obtained clinical risk factors to estimate an individual s 10-year fracture probability. It may be utilized by clinicians to assist in the identification of patients at high risk for fractures.
30 2010 Official Positions of the ISCD/IOF on the Interpretation and Use of FRAX in Clinical Practice
31 Garbage In----Garbage Out Change in a single answer on the FRAX questionnaire may shift the 10 year fracture risk from medical treatment advised to routine follow-up VERY important for primary health care provider to understand FRAX At Scott & White, we do not put FRAX results on the actual DXA report
32
33 DXA Gold-standard for BMD measurement Measures central or axial skeletal sites: spine and hip May measure other sites: total body and forearm Extensive epidemiologic data Correlation with bone strength in-vitro Validated in many clinical trials Widely available (over 10,000 DXA machines in USA still increasing until 3/2012 attrition due to 50% cut in amount Medicare pays)
34 Which Skeletal Sites Should Be Measured? Every Patient Spine L1-L4 Hip Some Patients Forearm (33% Radius) Total Proximal Femur Femoral Neck Trochanter If hip or spine cannot be measured Hyperparathyroidism Very obese Use lowest T-score of these sites
35 What DXA Really Measures: Bone Mineral Content (BMC) In Grams and Area In cm2 Areal BMD is calculated in g/cm2 T-score compares the patient s BMD with the young-normal mean BMD and expresses the difference as a standard deviation (SD) score
36 T-score Patient s BMD Young-Adult Mean BMD 1 SD of Young-Adult Mean BMD Example: T-score = 0.7 g/cm2-1.0 g/cm2 0.1 g/cm2 = - 3.0
37 Reference Database for T-Scores Use a uniform Caucasian (non-race adjusted) female normative database for women of all ethnic groups.* Use a uniform Caucasian (non-race adjusted) male normative database for men of all ethnic groups.*---some places use only one standard for females & males The NHANES III database should be used for Tscore derivation at the hip regions. *Note: Application of recommendation may vary according to local requirements.
38 Central DXA for Diagnosis The WHO international reference standard for osteoporosis diagnosis is a T-score of 2.5 or less at the femoral neck. o The reference standard from which the T-score is calculated is the female, white, age years, NHANES III database
39 Central DXA for Diagnosis Osteoporosis may be diagnosed in postmenopausal women and in men age 50 and older if the T-score of the lumbar spine, total hip, or femoral neck is -2.5 or less:* o In certain circumstances the 33% radius (also called 1/3 radius) may be utilized *Note: Other hip regions of interest, including Ward's area and the greater trochanter, should not be used for diagnosis. Application of recommendation may vary according to local requirements.
40 Central DXA for Diagnosis Skeletal sites to measure o Measure BMD at both the PA spine and hip in all patients o Forearm BMD should be measured under the following circumstances: Hip and/or spine cannot be measured or interpreted. Hyperparathyroidism Very obese patients (over the weight limit for DXA table)
41 Central DXA for Diagnosis Spine Region of Interest (ROI) o Use PA L1-L4 for spine BMD measurement o Use all evaluable vertebrae and only exclude vertebrae that are affected by local structural change or artifact. Use three vertebrae if four cannot be used and two if three cannot be used o BMD based diagnostic classification should not be made using a single vertebra. o If only one evaluable vertebra remains after excluding other vertebrae, diagnosis should be based on a different valid skeletal site
42 Central DXA for Diagnosis o o o Anatomically abnormal vertebrae may be excluded from analysis if: They are clearly abnormal and non-assessable within the resolution of the system; or There is more than a 1.0 T-score difference between the vertebra in question and adjacent vertebrae When vertebrae are excluded, the BMD of the remaining vertebrae is used to derive the T-score The lateral spine should not be used for diagnosis, but may have a role in monitoring
43 Fracture Risk Doubles With Every SD Decrease in BMD Relative Risk for Fracture Bone Density (T-score)
44 Z-score Patient s BMD Age-Matched Mean BMD 1 SD of Age-Matched Mean BMD in g/cm2 Low Z-score (less than -2.0) may suggest increased likelihood of secondary osteoporosis, however... This is not validated in clinical trials High index of suspicion for secondary causes of osteoporosis is suggested in all patients
45 Z-Score Reference Database Z-scores should be population specific where adequate reference data exist. For the purpose of Z-score calculation, the patient's self-reported ethnicity should be used.
46 Diagnostic Classification Classification T-score Normal -1 or greater Osteopenia Between -1 and -2.5 Osteoporosis -2.5 or less Severe Osteoporosis -2.5 or less and fragility fracture WHO Study Group
47 ISCD Official Positions 2007 : Use of the Term Osteopenia The term osteopenia is retained, but low bone mass or low bone density is preferred. People with low bone mass or density are not necessarily at high fracture risk.
48 Diagnosis Caveats T-score -2.5 or less does not always mean osteoporosis Clinical diagnosis of osteoporosis may be made with T-score greater than -2.5 Example: osteomalacia Example: atraumatic vertebral fracture with T-score equals -1.9 Low T-score does not identify the cause Medical evaluation should be considered Example: celiac disease with malabsorption
49 BMD Reporting in Postmenopausal Women and in Men Age 50 and Older The WHO densitometric classification is applicable. T-scores are preferred.
50 BMD Reporting in Females Prior to Menopause and in Males Younger Than Age 50 Z-scores, not T-scores, are preferred. This is particularly important in children. A Z-score of -2.0 or lower is defined as below the expected range for age, and a Z-score above 2.0 is within the expected range for age. Osteoporosis cannot be diagnosed in men under age 50 on the basis of BMD alone The WHO diagnostic criteria many be applied to women in the menopausal transition

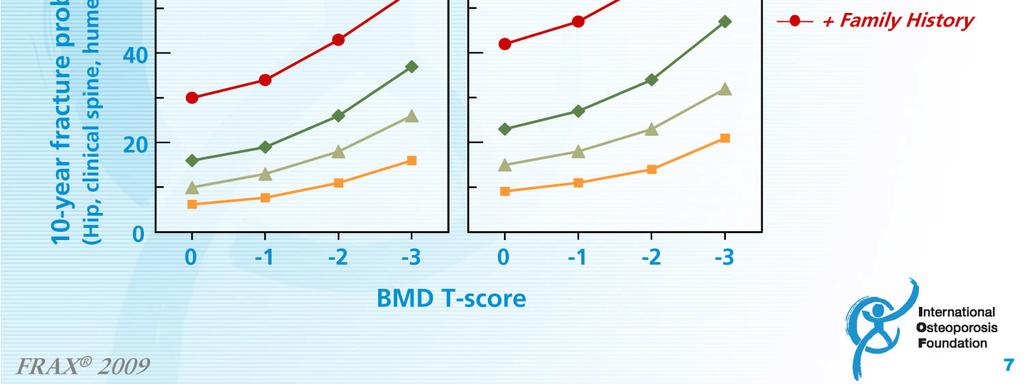
51 DXA L-Spine Image

52 Image Dual Femur

53 DXA IMAGE Forearm
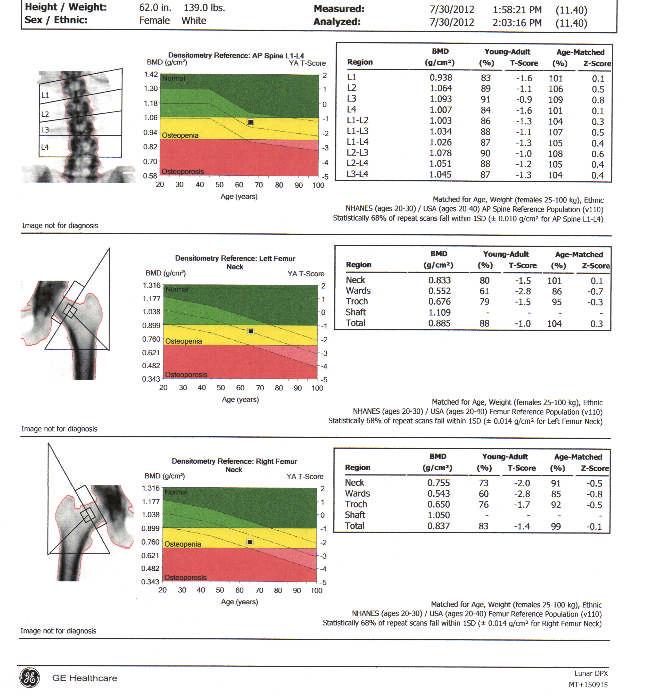
54 Sample BMD results Postmenopausal Patient L1-L g/cm2 Right Femoral Neck g/cm2 T-score 0.1 Left Femoral Neck g/cm2 T- score -0.2 Do you treat?? T-score -0.4
55 Sample BMD results Postmenopausal Patient L1-L g/cm2 Right Femoral Neck g/cm2 T-score 0.1 Left Femoral Neck g/cm2 T- score -0.2 T-score -0.4 When do you request a follow-up DXA?
56 Bone-Density Testing Interval and Transition to Osteoporosis in Older Women Margaret L. Gourlay, M.D., M.P.H., Jason P. Fine, Sc.D., John S. Preisser, Ph.D., Ryan C. May, Ph.D., Chenxi Li, Ph.D., LiYung Lui, M.S., David F. Ransohoff, M.D., Jane A. Cauley, Dr.P.H., and Kristine E. Ensrud, M.D., M.P.H. for the Study of Osteoporotic Fractures Research Group N Engl J Med 2012; 366: January 19, 2012
57 Bone-Density Testing Interval and Transition to Osteoporosis in Older Women Background :Although bone mineral density (BMD) testing to screen for osteoporosis (BMD T -score, 2.50 or lower) is recommended for women 65 years of age or older, there are few data to guide decisions about the interval between BMD tests.
58 Bone-Density Testing Interval and Transition to Osteoporosis in Older Women Methods We studied 4957 women, 67 years of age or older, with normal BMD (T- score at the femoral neck and total hip, 1.00 or higher) or osteopenia (T- score, 1.01 to 2.49) and with no history of hip or clinical vertebral fracture or of treatment for osteoporosis, followed prospectively for up to 15 years.
59 Bone-Density Testing Interval and Transition to Osteoporosis in Older Women Methods The BMD testing interval was defined as the estimated time for 10% of women to make the transition to osteoporosis before having a hip or clinical vertebral fracture, with adjustment for estrogen use and clinical risk factors
60 Bone-Density Testing Interval and Transition to Osteoporosis in Older Women Methods Transitions from normal BMD and from three subgroups of osteopenia (mild, moderate, and advanced) were analyzed with the use of parametric cumulative incidence models.
61 Bone-Density Testing Interval and Transition to Osteoporosis in Older Women Methods Incident hip and clinical vertebral fractures and initiation of treatment with bisphosphonates, calcitonin, or raloxifene were treated as competing risks.
62 Bone-Density Testing Interval and Transition to Osteoporosis in Older Women Results The estimated BMD testing interval was 16.8 years (95% confidence interval [CI], 11.5 to 24.6) for women with normal BMD, 17.3 years (95% CI, 13.9 to 21.5) for women with mild osteopenia, 4.7 years (95% CI, 4.2 to 5.2) for women with moderate osteopenia, and 1.1 years (95% CI, 1.0 to 1.3) for women with advanced osteopenia.
63 Bone-Density Testing Interval and Transition to Osteoporosis in Older Women Conclusions Our data indicate that osteoporosis would develop in less than 10% of older, postmenopausal women during rescreening intervals of approximately 15 years for women with normal bone density or mild osteopenia, 5 years for women with moderate osteopenia, and 1 year for women with advanced osteopenia. (Funded by the National Institutes of Health.)
64 In other words Normal or mild osteopenia on initial DXA could follow-up in approx 15 years Moderate osteopenia on initial DXA could follow-up in 5 years Advanced osteopenia could follow-up in 1 year
65 Least Significant Change TECHNICAL INFORMATION: Temple studies are performed on Lunar Prodigy DF with encore version 9.1software Mobile studies are performed on Lunar Prodigy DPXMT with encore version software Least significant change data: L1-L g/cm2 Left Femoral Neck 0.038g/cm2
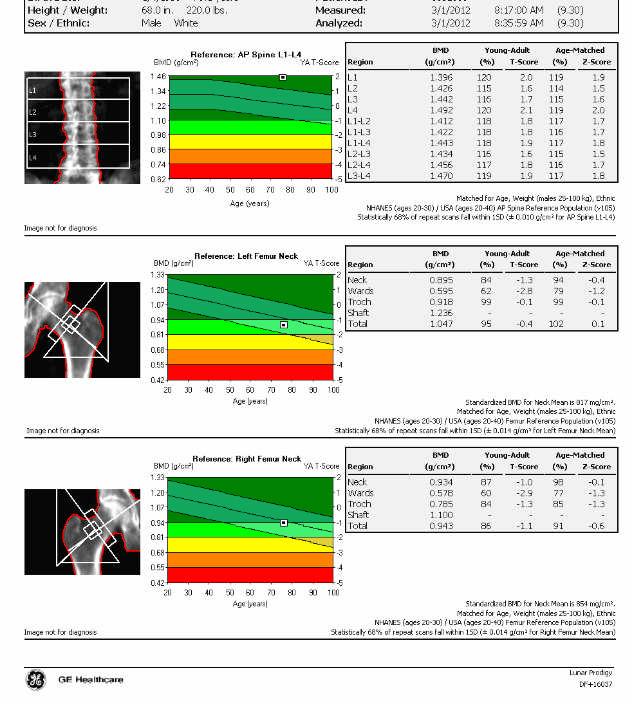
66 Sample BMD results Postmenopausal Patient L1-L g/cm2 Right Femoral Neck g/cm2 T- score 0.0 T-score -1.4 Left Femoral Neck g/cm2 T-score -1.5
67 Sample BMD Results Postmenopausal Patient L1-L g/cm2 T- score 0.0 Right Femoral Neck g/cm2 T-score -1.4 Left Femoral Neck g/cm2 T-score -1.5 Pt age 90 or age 50? Takes steroids? Heavy smoker? Now do you treat??
68
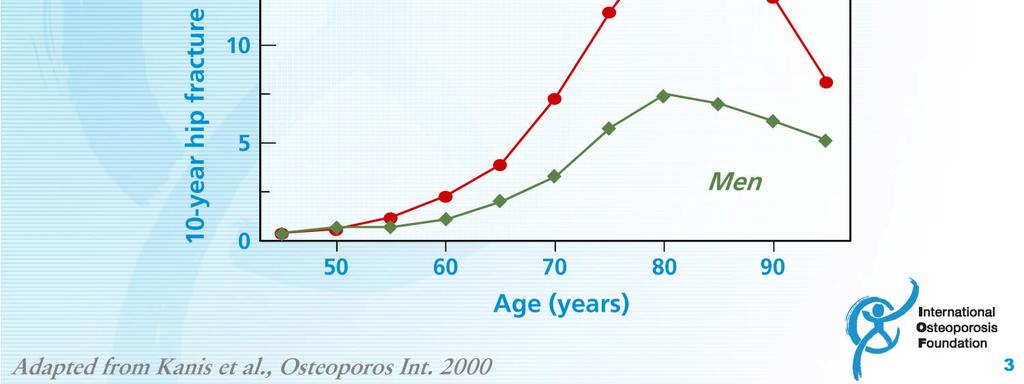
69 Age 75
70
71
72 Age 65
73
74 Male, age 76
75
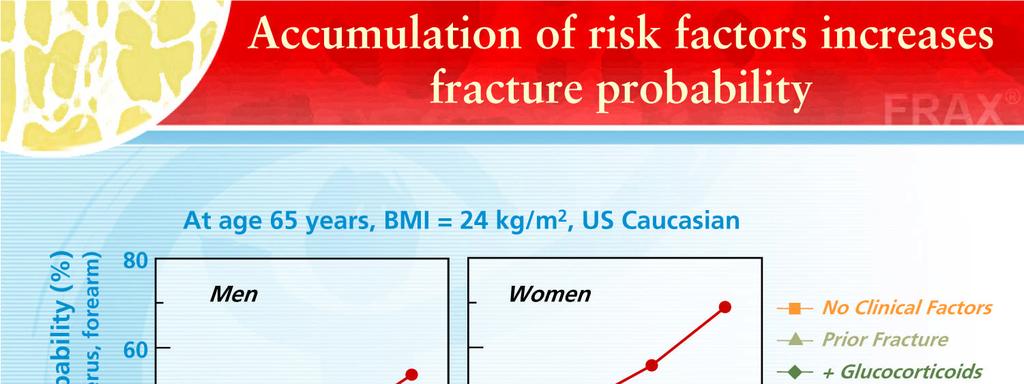
76 FRAX is a useful tool. FRAX does not replace your clinical judgment
77 FRAX WHO fracture risk assessment tool 10 year probability of fracture Uses BMD but also looks at multiple other risk factors Age (40 to 90 years), gender, country ONLY ON UNTREATED PEOPLE
78 2010 Official Positions of the ISCD/IOF on the Interpretation and Use of FRAX in Clinical Practice
79 13 clinical statements regarding FRAX: Impaired functional status in patients with rheumatoid arthritis may be a risk factor for clinical fractures. FRAX may underestimate fracture probability in such patients.
80 13 clinical statements regarding FRAX: There is no consistent evidence that non-glucocorticoid medications for rheumatoid arthritis alter fracture risk.
81 13 clinical statements regarding FRAX: While there is evidence that duration and dose of tobacco smoking may impact on fracture risk, quantification of this risk is not possible.
82 13 clinical statements regarding FRAX: Falls are a risk factor for fractures but are not accommodated as an entry variable in the current FRAX model. Fracture probability may be underestimated in individuals with a history of frequent falls, but quantification of this risk is not currently possible.
83 13 clinical statements regarding FRAX: There is a relationship between number of prior fractures and subsequent fracture risk. FRAX underestimates fracture probability in persons with a history of multiple fractures.
84 13 clinical statements regarding FRAX: There is a relationship between severity of prior vertebral fractures and subsequent fracture risk. FRAX may underestimate fracture probability in individuals with prevalent severe vertebral fractures.
85 13 clinical statements regarding FRAX: While there is evidence that hip, vertebral, and humeral fractures appear to confer greater risk of subsequent fracture than fractures at other sites, quantification of this incremental risk in FRAX is not possible.
86 13 clinical statements regarding FRAX: A parental history of non-hip fragility fracture may be a risk factor for fracture. FRAX may underestimate fracture probability in individuals with a parental history of non-hip fragility fracture.
87 13 clinical statements regarding FRAX: Evidence that bone turnover markers predict fracture risk independent of Bone Mineral Density (BMD) is inconclusive. Therefore, bone turnover markers are not included as risk factors in FRAX.
88 13 clinical statements regarding FRAX: There is a dose relationship between glucocorticoid use of greater than 3 months and fracture risk. The average dose exposure captured within FRAX is likely to be a prednisone dose of mg/day or its equivalent. Fracture probability is under-estimated when prednisone dose is greater than 7.5 mg/day and is over-estimated when prednisone dose is less than 2.5 mg/day.
89 13 clinical statements regarding FRAX: Frequent intermittent use of higher doses of glucocorticoids increases fracture risk. Because of variability in the dose and dosing schedule, quantification of this risk is not possible.
90 13 clinical statements regarding FRAX: High dose inhaled glucocorticoids may be a risk factor for fracture. FRAX may underestimate fracture probability in users of high dose inhaled glucocorticoids.
91 13 clinical statements regarding FRAX: Appropriate glucocorticoid replacement in individuals with adrenal insufficiency has not been shown to increase fracture risk. In such patients, use of glucocorticoids should not be included in FRAX calculations.
92 FRAX BMD STATEMENTS Measurements other than BMD or T-score at the femoral neck by Dual-energy X-ray Absorptiometry (DXA) are not recommended for use in FRAX. FRAX may underestimate or overestimate major osteoporotic fracture risk when lumbar spine T-score is much lower or higher (>1 Standard Deviation discrepancy) than femoral neck T-score.
93 FRAX BMD STATEMENTS A procedure based upon the difference (off set) between the Lumbar Spine and Femoral Neck Tscores can enhance fracture prediction in the current version of FRAX.
94 FRAX BMD STATEMENTS The ISCD 2007 PDC Statements on fracture risk prediction and application of heel Quantitative Ultrasounds (QUS) are supported by a higher level of evidence in men and women than was available in 2007.
95 FRAX BMD STATEMENTS Currently validated heel QUS devices, using criteria defined in the 2007 ISCD PDC, predict fracture risk similarly.
96 FRAX BMD STATEMENTS FRAX with BMD predicts fracture risk better than clinical risk factors or BMD alone. Use of FRAX without BMD is appropriate when BMD is not readily available or to identify individuals who may benefit from a BMD measurement.
97 FRAX BMD STATEMENTS It is not appropriate to use FRAX to monitor treatment response.
98 FRAX BMD STATEMENTS Evidence that rate of bone loss may be an independent risk factor for fracture is conflicting. Therefore, rate of bone loss is not included as a FRAX risk factor.

99 Thank you --- and may all your DXA decisions be wise.
Official Positions on FRAX
 196 96 DEPLIANT 3,5x8,5.indd 1 2010 Official Positions on FRAX 21.03.11 11:45 Interpretation and Use of FRAX in Clinical Practice from the International Society for Clinical Densitometry and International
196 96 DEPLIANT 3,5x8,5.indd 1 2010 Official Positions on FRAX 21.03.11 11:45 Interpretation and Use of FRAX in Clinical Practice from the International Society for Clinical Densitometry and International
DXA When to order? How to interpret? Dr Nikhil Tandon Department of Endocrinology and Metabolism All India Institute of Medical Sciences New Delhi
 DXA When to order? How to interpret? Dr Nikhil Tandon Department of Endocrinology and Metabolism All India Institute of Medical Sciences New Delhi Clinical Utility of Bone Densitometry Diagnosis (DXA)
DXA When to order? How to interpret? Dr Nikhil Tandon Department of Endocrinology and Metabolism All India Institute of Medical Sciences New Delhi Clinical Utility of Bone Densitometry Diagnosis (DXA)
Osteoporosis/Fracture Prevention
 Osteoporosis/Fracture Prevention NATIONAL GUIDELINE SUMMARY This guideline was developed using an evidence-based methodology by the KP National Osteoporosis/Fracture Prevention Guideline Development Team
Osteoporosis/Fracture Prevention NATIONAL GUIDELINE SUMMARY This guideline was developed using an evidence-based methodology by the KP National Osteoporosis/Fracture Prevention Guideline Development Team
Interpreting DEXA Scan and. the New Fracture Risk. Assessment. Algorithm
 Interpreting DEXA Scan and the New Fracture Risk Assessment Algorithm Prof. Samir Elbadawy *Osteoporosis affect 30%-40% of women in western countries and almost 15% of men after the age of 50 years. Osteoporosis
Interpreting DEXA Scan and the New Fracture Risk Assessment Algorithm Prof. Samir Elbadawy *Osteoporosis affect 30%-40% of women in western countries and almost 15% of men after the age of 50 years. Osteoporosis
2013 ISCD Official Positions Adult
 2013 ISCD Official Positions Adult These are the Official Positions of the ISCD as updated in 2013. The Official Positions that are new or revised since 2007 are in bold type. Indications for Bone Mineral
2013 ISCD Official Positions Adult These are the Official Positions of the ISCD as updated in 2013. The Official Positions that are new or revised since 2007 are in bold type. Indications for Bone Mineral
Bone Mass Measurement BONE MASS MEASUREMENT HS-042. Policy Number: HS-042. Original Effective Date: 8/25/2008
 Easy Choice Health Plan, Inc. Harmony Health Plan of Illinois, Inc. Missouri Care, Inc. Ohana Health Plan, a plan offered by WellCare Health Insurance of Arizona, Inc. WellCare Health Insurance of Illinois,
Easy Choice Health Plan, Inc. Harmony Health Plan of Illinois, Inc. Missouri Care, Inc. Ohana Health Plan, a plan offered by WellCare Health Insurance of Arizona, Inc. WellCare Health Insurance of Illinois,
Bone Mineral Densitometry with Dual Energy X-Ray Absorptiometry
 Bone Mineral Densitometry with Dual Energy X-Ray Absorptiometry R Gilles, Laurentius Ziekenhuis Roermond 1. Introduction Osteoporosis is characterised by low bone mass, disruption of the micro-architecture
Bone Mineral Densitometry with Dual Energy X-Ray Absorptiometry R Gilles, Laurentius Ziekenhuis Roermond 1. Introduction Osteoporosis is characterised by low bone mass, disruption of the micro-architecture
Challenging the Current Osteoporosis Guidelines. Carolyn J. Crandall, MD, MS Professor of Medicine David Geffen School of Medicine at UCLA
 Challenging the Current Osteoporosis Guidelines Carolyn J. Crandall, MD, MS Professor of Medicine David Geffen School of Medicine at UCLA Whom to screen Which test How to diagnose Whom to treat Benefits
Challenging the Current Osteoporosis Guidelines Carolyn J. Crandall, MD, MS Professor of Medicine David Geffen School of Medicine at UCLA Whom to screen Which test How to diagnose Whom to treat Benefits
Using the FRAX Tool. Osteoporosis Definition
 How long will your bones remain standing? Using the FRAX Tool Gary Salzman M.D. Director Banner Good Samaritan/ Hayden VAMC Internal Medicine Geriatric Fellowship Program Phoenix, Arizona Using the FRAX
How long will your bones remain standing? Using the FRAX Tool Gary Salzman M.D. Director Banner Good Samaritan/ Hayden VAMC Internal Medicine Geriatric Fellowship Program Phoenix, Arizona Using the FRAX
Bone density scanning and osteoporosis
 Bone density scanning and osteoporosis What is osteoporosis? Osteoporosis occurs when the struts which make up the mesh-like structure within bones become thin causing them to become fragile and break
Bone density scanning and osteoporosis What is osteoporosis? Osteoporosis occurs when the struts which make up the mesh-like structure within bones become thin causing them to become fragile and break
Building Bone Density-Research Issues
 Building Bone Density-Research Issues Helping to Regain Bone Density QUESTION 1 What are the symptoms of Osteoporosis? Who is at risk? Symptoms Bone Fractures Osteoporosis 1,500,000 fractures a year Kyphosis
Building Bone Density-Research Issues Helping to Regain Bone Density QUESTION 1 What are the symptoms of Osteoporosis? Who is at risk? Symptoms Bone Fractures Osteoporosis 1,500,000 fractures a year Kyphosis
Bone Densitometry. What is a Bone Density Scan (DXA)? What are some common uses of the procedure?
? What are some common uses of the procedure?") Scan for mobile link. Bone Densitometry What is a Bone Density Scan (DXA)? Bone density scanning, also called dual-energy x-ray absorptiometry (DXA) or bone densitometry, is an enhanced form of x-ray technology
Scan for mobile link. Bone Densitometry What is a Bone Density Scan (DXA)? Bone density scanning, also called dual-energy x-ray absorptiometry (DXA) or bone densitometry, is an enhanced form of x-ray technology
Osteoporosis. Overview
 v2 Osteoporosis Overview Osteoporosis is defined as compromised bone strength that increases risk of fracture (NIH Consensus Conference, 2000). Bone strength is characterized by bone mineral density (BMD)
v2 Osteoporosis Overview Osteoporosis is defined as compromised bone strength that increases risk of fracture (NIH Consensus Conference, 2000). Bone strength is characterized by bone mineral density (BMD)
Clinician s Guide to Prevention and Treatment of Osteoporosis
 Clinician s Guide to Prevention and Treatment of Osteoporosis Published: 15 August 2014 committee of the National Osteoporosis Foundation (NOF) Tipawan khiemsontia,md outline Basic pathophysiology screening
Clinician s Guide to Prevention and Treatment of Osteoporosis Published: 15 August 2014 committee of the National Osteoporosis Foundation (NOF) Tipawan khiemsontia,md outline Basic pathophysiology screening
Clinical Appropriateness Guidelines: Advanced Imaging
 Clinical Appropriateness Guidelines: Advanced Imaging Appropriate Use Criteria: Quantitative CT (QCT) Bone Mineral Densitometry Effective Date: September 5, 2017 Proprietary Date of Origin: 05/21/2007
Clinical Appropriateness Guidelines: Advanced Imaging Appropriate Use Criteria: Quantitative CT (QCT) Bone Mineral Densitometry Effective Date: September 5, 2017 Proprietary Date of Origin: 05/21/2007
2013 ISCD Combined Official Positions
 2013 ISCD Combined Oicial Positions Oicial Positions of the International Society for Clinical Densitometry The International Society for Clinical Densitometry (ISCD) is a not-for-profit multidisciplinary
2013 ISCD Combined Oicial Positions Oicial Positions of the International Society for Clinical Densitometry The International Society for Clinical Densitometry (ISCD) is a not-for-profit multidisciplinary
Module 5 - Speaking of Bones Osteoporosis For Health Professionals: Fracture Risk Assessment. William D. Leslie, MD MSc FRCPC
 Module 5 - Speaking of Bones Osteoporosis For Health Professionals: Fracture Risk Assessment William D. Leslie, MD MSc FRCPC Case #1 Age 53: 3 years post-menopause Has always enjoyed excellent health with
Module 5 - Speaking of Bones Osteoporosis For Health Professionals: Fracture Risk Assessment William D. Leslie, MD MSc FRCPC Case #1 Age 53: 3 years post-menopause Has always enjoyed excellent health with
Understanding the Development of Osteoporosis and Preventing Fractures: WHO Do We Treat Now?
 Understanding the Development of Osteoporosis and Preventing Fractures: WHO Do We Treat Now? Steven M. Petak, MD, JD, FACE, FCLM Texas Institute for Reproductive Medicine And Endocrinology, Houston, Texas
Understanding the Development of Osteoporosis and Preventing Fractures: WHO Do We Treat Now? Steven M. Petak, MD, JD, FACE, FCLM Texas Institute for Reproductive Medicine And Endocrinology, Houston, Texas
Osteoporosis: An Overview. Carolyn J. Crandall, MD, MS
 Osteoporosis: An Overview Carolyn J. Crandall, MD, MS Osteoporosis: An Overview Carolyn J. Crandall, MD, MS Professor of Medicine David Geffen School of Medicine at UCLA Objectives Review osteoporosis
Osteoporosis: An Overview Carolyn J. Crandall, MD, MS Osteoporosis: An Overview Carolyn J. Crandall, MD, MS Professor of Medicine David Geffen School of Medicine at UCLA Objectives Review osteoporosis
Osteoporosis. Treatment of a Silently Developing Disease
 Osteoporosis Treatment of a Silently Developing Disease Marc K. Drezner, MD Senior Associate Dean Emeritus Professor of Medicine Emeritus University of Wisconsin-Madison Auditorium The Forest at Duke October
Osteoporosis Treatment of a Silently Developing Disease Marc K. Drezner, MD Senior Associate Dean Emeritus Professor of Medicine Emeritus University of Wisconsin-Madison Auditorium The Forest at Duke October
Nutritional Aspects of Osteoporosis Care and Treatment Cynthia Smith, FNP-BC, RN, MSN, CCD Pars Osteoporosis Clinic, Belpre, Ohio
 Osteoporosis 1 Nutritional Aspects of Osteoporosis Care and Treatment Cynthia Smith, FNP-BC, RN, MSN, CCD Pars Osteoporosis Clinic, Belpre, Ohio 1) Objectives: a) To understand bone growth and development
Osteoporosis 1 Nutritional Aspects of Osteoporosis Care and Treatment Cynthia Smith, FNP-BC, RN, MSN, CCD Pars Osteoporosis Clinic, Belpre, Ohio 1) Objectives: a) To understand bone growth and development
EXAMINATION CONTENT SPECIFICATIONS ARRT BOARD APPROVED: JANUARY 2017 IMPLEMENTATION DATE: JULY 1, 2017
 EXAMINATION CONTENT SPECIFICATIONS Bone Densitometry The purpose of the bone densitometry examination is to assess the knowledge and cognitive skills underlying the intelligent performance of the tasks
EXAMINATION CONTENT SPECIFICATIONS Bone Densitometry The purpose of the bone densitometry examination is to assess the knowledge and cognitive skills underlying the intelligent performance of the tasks
LOVE YOUR BONES Protect your future
 www.worldosteoporosisday.org LOVE YOUR BONES Protect your future Know your risk for osteoporosis www.iofbonehealth.org Osteoporosis is a problem worldwide, and in many countries, up to one in three women
www.worldosteoporosisday.org LOVE YOUR BONES Protect your future Know your risk for osteoporosis www.iofbonehealth.org Osteoporosis is a problem worldwide, and in many countries, up to one in three women
STRUCTURED EDUCATION REQUIREMENTS IMPLEMENTATION DATE: JULY 1, 2017
 STRUCTURED EDUCATION REQUIREMENTS Bone Densitometry The purpose of structured education is to provide the opportunity for individuals to develop mastery of discipline-specific knowledge that, when coupled
STRUCTURED EDUCATION REQUIREMENTS Bone Densitometry The purpose of structured education is to provide the opportunity for individuals to develop mastery of discipline-specific knowledge that, when coupled
Bone Mineral Density Studies in Adult Populations
 Bone Mineral Density Studies in Adult Populations Last Review Date: July 14, 2017 Number: MG.MM.RA10aC6 Medical Guideline Disclaimer Property of EmblemHealth. All rights reserved. The treating physician
Bone Mineral Density Studies in Adult Populations Last Review Date: July 14, 2017 Number: MG.MM.RA10aC6 Medical Guideline Disclaimer Property of EmblemHealth. All rights reserved. The treating physician
Management of postmenopausal osteoporosis
 Management of postmenopausal osteoporosis Yeap SS, Hew FL, Chan SP, on behalf of the Malaysian Osteoporosis Society Committee Working Group for the Clinical Guidance on the Management of Osteoporosis,
Management of postmenopausal osteoporosis Yeap SS, Hew FL, Chan SP, on behalf of the Malaysian Osteoporosis Society Committee Working Group for the Clinical Guidance on the Management of Osteoporosis,
Guideline for the investigation and management of osteoporosis. for hospitals and General Practice
 Guideline for the investigation and management of osteoporosis for hospitals and General Practice Background Low bone density is an important risk factor for fracture. The aim of assessing bone density
Guideline for the investigation and management of osteoporosis for hospitals and General Practice Background Low bone density is an important risk factor for fracture. The aim of assessing bone density
Bone Densitometry Pathway
 Bone Densitometry Pathway The goal of the Bone Densitometry pathway is to manage our diagnosed osteopenic and osteoporotic patients, educate and monitor the patient population at risk for bone density
Bone Densitometry Pathway The goal of the Bone Densitometry pathway is to manage our diagnosed osteopenic and osteoporotic patients, educate and monitor the patient population at risk for bone density
Learning Objectives. Controversies in Osteoporosis Prevention and Management. Etiology. Presenter Disclosure Information. Epidemiology.
 12:45 1:30pm Controversies in Osteoporosis Prevention and Management SPEAKER Carolyn Crandall, MD, MS Presenter Disclosure Information The following relationships exist related to this presentation: Carolyn
12:45 1:30pm Controversies in Osteoporosis Prevention and Management SPEAKER Carolyn Crandall, MD, MS Presenter Disclosure Information The following relationships exist related to this presentation: Carolyn
CASE 1 WHY IS IT IMPORTANT TO TREAT? FACTS CONCERNS
 4:30-5:15pm Ask the Expert: Osteoporosis SPEAKERS Silvina Levis, MD OSTEOPOROSIS - FACTS 1:3 older women and 1:5 older men will have a fragility fracture after age 50 After 3 years of treatment, depending
4:30-5:15pm Ask the Expert: Osteoporosis SPEAKERS Silvina Levis, MD OSTEOPOROSIS - FACTS 1:3 older women and 1:5 older men will have a fragility fracture after age 50 After 3 years of treatment, depending
New Developments in Osteoporosis: Screening, Prevention and Treatment
 Osteoporosis: Overview New Developments in Osteoporosis: Screening, Prevention and Treatment Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF Definitions Risk factors
Osteoporosis: Overview New Developments in Osteoporosis: Screening, Prevention and Treatment Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF Definitions Risk factors
Management of Osteoporosis : What Do the Guidelines Say? Robert D. Blank, MD, PhD Endocrinology, U of Wisconsin GRECC Service, Middleton VAMC
 Management of Osteoporosis : What Do the Guidelines Say? Robert D. Blank, MD, PhD Endocrinology, U of Wisconsin GRECC Service, Middleton VAMC Learning Goals Review guidelines for osteoporosis Consider
Management of Osteoporosis : What Do the Guidelines Say? Robert D. Blank, MD, PhD Endocrinology, U of Wisconsin GRECC Service, Middleton VAMC Learning Goals Review guidelines for osteoporosis Consider
Osteoporosis Update: Keys to Improving Diagnosis and Preventing Fractures
 Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/spotlight-on/osteoporosis-update-keys-improving-diagnosis-preventingfractures/9812/
Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/spotlight-on/osteoporosis-update-keys-improving-diagnosis-preventingfractures/9812/
Objectives: What is Osteoporosis 10/8/2015. Bone Health/ Osteoporosis: BASICS OF SCREENING, INTERPRETING, AND TREATING
 Bone Health/ Osteoporosis: BASICS OF SCREENING, INTERPRETING, AND TREATING TIFFANY PAUL, APN, CNP, CCD Objectives: Review the diagnosis of Osteoporosis Describe the basics of a bone density exam Identify
Bone Health/ Osteoporosis: BASICS OF SCREENING, INTERPRETING, AND TREATING TIFFANY PAUL, APN, CNP, CCD Objectives: Review the diagnosis of Osteoporosis Describe the basics of a bone density exam Identify
Prevalence of Osteoporosis p. 262 Consequences of Osteoporosis p. 263 Risk Factors for Osteoporosis p. 264 Attainment of Peak Bone Density p.
 Dedication Preface Acknowledgments Continuing Education An Introduction to Conventions in Densitometry p. 1 Densitometry as a Quantitative Measurement Technique p. 2 Accuracy and Precision p. 2 The Skeleton
Dedication Preface Acknowledgments Continuing Education An Introduction to Conventions in Densitometry p. 1 Densitometry as a Quantitative Measurement Technique p. 2 Accuracy and Precision p. 2 The Skeleton
AMERICAN COLLEGE OF RHEUMATOLOGY POSITION STATEMENT. Committee on Rheumatologic Care
 AMERICAN COLLEGE OF RHEUMATOLOGY POSITION STATEMENT SUBJECT: PRESENTED BY: FOR DISTRIBUTION TO: Bone Mineral Density Measurement and the Role of Rheumatologists in the Management of Osteoporosis Committee
AMERICAN COLLEGE OF RHEUMATOLOGY POSITION STATEMENT SUBJECT: PRESENTED BY: FOR DISTRIBUTION TO: Bone Mineral Density Measurement and the Role of Rheumatologists in the Management of Osteoporosis Committee
The Bone Densitometry Examination
 The Bone Densitometry Examination The purpose of The American Registry of Radiologic Technologist (ARRT ) Bone Densitometry Examination is to assess the knowledge and cognitive skills underlying the intelligent
The Bone Densitometry Examination The purpose of The American Registry of Radiologic Technologist (ARRT ) Bone Densitometry Examination is to assess the knowledge and cognitive skills underlying the intelligent
Bone Densitometry. Total 30 Maximum CE 14. DXA Scanning (10) 7
 7") STRUCTURED SELF ASSESSMENT CONTENT SPECIFICATIONS SSA LAUNCH DATE: JANUARY 1, 2018 Bone Densitometry The purpose of continuing qualifications requirements (CQR) is to assist registered technologists in
STRUCTURED SELF ASSESSMENT CONTENT SPECIFICATIONS SSA LAUNCH DATE: JANUARY 1, 2018 Bone Densitometry The purpose of continuing qualifications requirements (CQR) is to assist registered technologists in
My joints ache. What is the difference between osteoporosis and osteoarthritis?
 Osteoporosis What is osteoporosis? Osteoporosis means bones are less dense, more fragile, and at greater risk for breaking, even with small injuries. This problem often affects bones in the hip, spine,
Osteoporosis What is osteoporosis? Osteoporosis means bones are less dense, more fragile, and at greater risk for breaking, even with small injuries. This problem often affects bones in the hip, spine,
Osteoporosis: Who, What, When, Why, and How
 Osteoporosis: Who, What, When, Why, and How Doris J. Uh, PharmD, AE-C Pharm 445 September 20, 2005 Objectives define osteoporosis (what) determine high risk groups (who, when) review modifiable, non-modifiable
Osteoporosis: Who, What, When, Why, and How Doris J. Uh, PharmD, AE-C Pharm 445 September 20, 2005 Objectives define osteoporosis (what) determine high risk groups (who, when) review modifiable, non-modifiable
Helpful information about bone health & osteoporosis Patient Resource
 Helpful information about bone health & osteoporosis Patient Resource Every year In the United States, 2.5 million fractures occur due to osteoporosis. Out of these, 330,000 are hip fractures, and half
Helpful information about bone health & osteoporosis Patient Resource Every year In the United States, 2.5 million fractures occur due to osteoporosis. Out of these, 330,000 are hip fractures, and half
An audit of osteoporotic patients in an Australian general practice
 professional Darren Parker An audit of osteoporotic patients in an Australian general practice Background Osteoporosis is a major contributor to morbidity and mortality in Australia, and is predicted to
professional Darren Parker An audit of osteoporotic patients in an Australian general practice Background Osteoporosis is a major contributor to morbidity and mortality in Australia, and is predicted to
Osteoporosis/Fracture Prevention Clinician Guide SEPTEMBER 2017
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Osteoporosis/Fracture Prevention Clinician Guide SEPTEMBER 2017 Introduction This Clinician Guide was developed to assist Primary Care physicians
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Osteoporosis/Fracture Prevention Clinician Guide SEPTEMBER 2017 Introduction This Clinician Guide was developed to assist Primary Care physicians
International Journal of Health Sciences and Research ISSN:
 International Journal of Health Sciences and Research www.ijhsr.org ISSN: 2249-9571 Original Research Article Osteoporosis- Do We Need to Think Beyond Bone Mineral Density? Dr Preeti Soni 1, Dr Shipra
International Journal of Health Sciences and Research www.ijhsr.org ISSN: 2249-9571 Original Research Article Osteoporosis- Do We Need to Think Beyond Bone Mineral Density? Dr Preeti Soni 1, Dr Shipra
1
 www.osteoporosis.ca 1 2 Overview of the Presentation Osteoporosis: An Overview Bone Basics Diagnosis of Osteoporosis Drug Therapies Risk Reduction Living with Osteoporosis 3 What is Osteoporosis? Osteoporosis:
www.osteoporosis.ca 1 2 Overview of the Presentation Osteoporosis: An Overview Bone Basics Diagnosis of Osteoporosis Drug Therapies Risk Reduction Living with Osteoporosis 3 What is Osteoporosis? Osteoporosis:
OSTEOPOROSIS: PREVENTION AND MANAGEMENT
 OSTEOPOROSIS: OVERVIEW OSTEOPOROSIS: PREVENTION AND MANAGEMENT Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF Definitions Key Risk factors Screening and Monitoring
OSTEOPOROSIS: OVERVIEW OSTEOPOROSIS: PREVENTION AND MANAGEMENT Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF Definitions Key Risk factors Screening and Monitoring
NIH Public Access Author Manuscript Endocr Pract. Author manuscript; available in PMC 2014 May 11.
 NIH Public Access Author Manuscript Published in final edited form as: Endocr Pract. 2013 ; 19(5): 780 784. doi:10.4158/ep12416.or. FRAX Prediction Without BMD for Assessment of Osteoporotic Fracture Risk
NIH Public Access Author Manuscript Published in final edited form as: Endocr Pract. 2013 ; 19(5): 780 784. doi:10.4158/ep12416.or. FRAX Prediction Without BMD for Assessment of Osteoporotic Fracture Risk
Bone Density Measurement in Women
 Bone Density Measurement in Women Revised 2005 Scope This guideline defines the medical necessity of bone mineral density (BMD) measurement using dualenergy x-ray absorptiometry (DXA or DEXA), and applies
Bone Density Measurement in Women Revised 2005 Scope This guideline defines the medical necessity of bone mineral density (BMD) measurement using dualenergy x-ray absorptiometry (DXA or DEXA), and applies
nogg Guideline for the diagnosis and management of osteoporosis in postmenopausal women and men from the age of 50 years in the UK
 nogg NATIONAL OSTEOPOROSIS GUIDELINE GROUP Guideline for the diagnosis and management of osteoporosis in postmenopausal women and men from the age of 50 years in the UK Produced by J Compston, A Cooper,
nogg NATIONAL OSTEOPOROSIS GUIDELINE GROUP Guideline for the diagnosis and management of osteoporosis in postmenopausal women and men from the age of 50 years in the UK Produced by J Compston, A Cooper,
Study of secondary causes of male osteoporosis
 Study of secondary causes of male osteoporosis Suárez, S.M., Giunta J., Meneses G., Costanzo P.R., Knoblovits P. Department of Endocrinology, Metabolism and Nuclear Medicine of Hospital Italiano of Buenos
Study of secondary causes of male osteoporosis Suárez, S.M., Giunta J., Meneses G., Costanzo P.R., Knoblovits P. Department of Endocrinology, Metabolism and Nuclear Medicine of Hospital Italiano of Buenos
Measuring Bone Mineral Density
 Measuring Bone Mineral Density Osteoporosis Screening by Pharmacists 9/20/06 Don Downing Institute for Innovative Pharmacy Practice Today s Topics What is osteoporosis? What causes osteoporosis? Screening
Measuring Bone Mineral Density Osteoporosis Screening by Pharmacists 9/20/06 Don Downing Institute for Innovative Pharmacy Practice Today s Topics What is osteoporosis? What causes osteoporosis? Screening
Bone Mineral Density Studies
 Bone Mineral Density Studies Policy Number: 6.01.01 Last Review: 3/2019 Origination: 10/1988 Next Review: 3/2020 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for bone
Bone Mineral Density Studies Policy Number: 6.01.01 Last Review: 3/2019 Origination: 10/1988 Next Review: 3/2020 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for bone
New 2010 Osteoporosis Guidelines: What you and your health provider need to know QUESTIONS&ANSWERS
 New 2010 Osteoporosis Guidelines: What you and your health provider need to know QUESTIONS&ANSWERS Wednesday, December 1, 2010 1:00 p.m. to 2:00 p.m. ET 1. I m 55 years old. I ve been taking Fosavance
New 2010 Osteoporosis Guidelines: What you and your health provider need to know QUESTIONS&ANSWERS Wednesday, December 1, 2010 1:00 p.m. to 2:00 p.m. ET 1. I m 55 years old. I ve been taking Fosavance
Adina Alazraki, MD, FAAP Assistant Professor, Radiology and Pediatrics Emory University School of Medicine Children s Healthcare of Atlanta
 Adina Alazraki, MD, FAAP Assistant Professor, Radiology and Pediatrics Emory University School of Medicine Technical: Patient positioning Performance of the scan Analysis of the data Theoretical: Identification
Adina Alazraki, MD, FAAP Assistant Professor, Radiology and Pediatrics Emory University School of Medicine Technical: Patient positioning Performance of the scan Analysis of the data Theoretical: Identification
sad EFFECTIVE DATE: POLICY LAST UPDATED:
 Medical Coverage Policy Bone Mineral Density Studies sad EFFECTIVE DATE: 06 07 2011 POLICY LAST UPDATED: 11 06 2018 OVERVIEW Bone density studies can be used to identify individuals with osteoporosis and
Medical Coverage Policy Bone Mineral Density Studies sad EFFECTIVE DATE: 06 07 2011 POLICY LAST UPDATED: 11 06 2018 OVERVIEW Bone density studies can be used to identify individuals with osteoporosis and
Original Article. Ramesh Keerthi Gadam, MD 1 ; Karen Schlauch, PhD 2 ; Kenneth E. Izuora, MD, MBA 1 ABSTRACT
 Original Article Ramesh Keerthi Gadam, MD 1 ; Karen Schlauch, PhD 2 ; Kenneth E. Izuora, MD, MBA 1 ABSTRACT Objective: To compare Fracture Risk Assessment Tool (FRAX) calculations with and without bone
Original Article Ramesh Keerthi Gadam, MD 1 ; Karen Schlauch, PhD 2 ; Kenneth E. Izuora, MD, MBA 1 ABSTRACT Objective: To compare Fracture Risk Assessment Tool (FRAX) calculations with and without bone
Section 4. Scans and tests. How do I know if I have osteoporosis? Investigations for spinal fractures. Investigations after you break a bone
 Section 4 Scans and tests How do I know if I have osteoporosis? Investigations for spinal fractures Investigations after you break a bone Investigations if you have risk factors Investigations for children
Section 4 Scans and tests How do I know if I have osteoporosis? Investigations for spinal fractures Investigations after you break a bone Investigations if you have risk factors Investigations for children
John J. Wolf, DO Family Medicine
 John J. Wolf, DO Family Medicine Objectives: 1. Review incidence & Risk of Osteoporosis 2.Review indications for testing 3.Review current pharmacologic & Non pharmacologic Tx options 4.Understand & Utilize
John J. Wolf, DO Family Medicine Objectives: 1. Review incidence & Risk of Osteoporosis 2.Review indications for testing 3.Review current pharmacologic & Non pharmacologic Tx options 4.Understand & Utilize
2002 clinical practice guidelines for the diagnosis and management of osteoporosis in Canada
 2002 clinical practice guidelines for the diagnosis and management of osteoporosis in Canada Jacques P. Brown, Robert G. Josse, for the Scientific Advisory Council of the Osteoporosis Society of Canada
2002 clinical practice guidelines for the diagnosis and management of osteoporosis in Canada Jacques P. Brown, Robert G. Josse, for the Scientific Advisory Council of the Osteoporosis Society of Canada
OSTEOPOROSIS IN MEN. Nelson B. Watts, MD OSTEOPOROSIS AND BONE HEALTH SERVICES CINCINNATI, OHIO
 OSTEOPOROSIS IN MEN Nelson B. Watts, MD OSTEOPOROSIS AND BONE HEALTH SERVICES CINCINNATI, OHIO DISCLOSURES Speakers Bureau: Amgen, Radius Consultant: Abbvie, Amgen, Janssen, Radius, Sanofi Watts NB et
OSTEOPOROSIS IN MEN Nelson B. Watts, MD OSTEOPOROSIS AND BONE HEALTH SERVICES CINCINNATI, OHIO DISCLOSURES Speakers Bureau: Amgen, Radius Consultant: Abbvie, Amgen, Janssen, Radius, Sanofi Watts NB et
Osteoporosis challenges
 Osteoporosis challenges Osteoporosis challenges Who should have a fracture risk assessment? Who to treat? Drugs, holidays and unusual adverse effects Fracture liaison service? The size of the problem 1
Osteoporosis challenges Osteoporosis challenges Who should have a fracture risk assessment? Who to treat? Drugs, holidays and unusual adverse effects Fracture liaison service? The size of the problem 1
Osteoporosis - New Guidelines. Michelle Glass B.Sc. (Pharm) June 15, 2011
 June 15, 2011") Osteoporosis - New Guidelines Michelle Glass B.Sc. (Pharm) June 15, 2011 Outline What is Osteoporosis? Who is at risk? What treatments are available? Role of the Pharmacy technician Definition of Osteoporosis
Osteoporosis - New Guidelines Michelle Glass B.Sc. (Pharm) June 15, 2011 Outline What is Osteoporosis? Who is at risk? What treatments are available? Role of the Pharmacy technician Definition of Osteoporosis
Overview. Bone Biology Osteoporosis Osteomalacia Paget s Disease Cases. People Centred Positive Compassion Excellence
 Overview Osteoporosis and Metabolic Bone Disease Dr Chandini Rao Consultant Rheumatologist Bone Biology Osteoporosis Osteomalacia Paget s Disease Cases Bone Biology Osteoporosis Increased bone remodelling
Overview Osteoporosis and Metabolic Bone Disease Dr Chandini Rao Consultant Rheumatologist Bone Biology Osteoporosis Osteomalacia Paget s Disease Cases Bone Biology Osteoporosis Increased bone remodelling
Osteoporosis and Lupus. Andrew Ruthberg, MD University Rheumatologists
 Osteoporosis and Lupus Andrew Ruthberg, MD University Rheumatologists 1 Forget the medical terminology (osteoporosis, osteopenia, low bone mass, DEXA, DXA, T score etc) The bottom line is that you don
Osteoporosis and Lupus Andrew Ruthberg, MD University Rheumatologists 1 Forget the medical terminology (osteoporosis, osteopenia, low bone mass, DEXA, DXA, T score etc) The bottom line is that you don
To understand bone growth and development across the lifespan. To develop a better understanding of osteoporosis.
 Nutrition Aspects of Osteoporosis Care and Treatment t Cynthia Smith, FNP-BC, RN, MSN, CCD Pars Osteoporosis Clinic, Belpre, OH. Objectives To understand bone growth and development across the lifespan.
Nutrition Aspects of Osteoporosis Care and Treatment t Cynthia Smith, FNP-BC, RN, MSN, CCD Pars Osteoporosis Clinic, Belpre, OH. Objectives To understand bone growth and development across the lifespan.
Learning Objectives. ! Students will become familiar with the 3 treatment solutions for osteoporosis. ! Students should be able to define osteoporosis
 Learning Objectives! Students should be able to define osteoporosis! Students should be able to identify some risk factors of osteoporosis! Students should be able to identify some of the people in the
Learning Objectives! Students should be able to define osteoporosis! Students should be able to identify some risk factors of osteoporosis! Students should be able to identify some of the people in the
Screening Guidelines: Women
 The Situation 1 in 2 postmenopausal women and 1 in 5 older men will have an osteoporosis-related fracture in their lifetimes Osteoporosis Definition NIH Consensus Conference A skeletal disorder characterized
The Situation 1 in 2 postmenopausal women and 1 in 5 older men will have an osteoporosis-related fracture in their lifetimes Osteoporosis Definition NIH Consensus Conference A skeletal disorder characterized
NEW DEVELOPMENTS IN OSTEOPOROSIS: SCREENING, PREVENTION AND TREATMENT
 NEW DEVELOPMENTS IN OSTEOPOROSIS: SCREENING, PREVENTION AND TREATMENT Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF OSTEOPOROSIS: OVERVIEW Definitions Risk factors
NEW DEVELOPMENTS IN OSTEOPOROSIS: SCREENING, PREVENTION AND TREATMENT Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF OSTEOPOROSIS: OVERVIEW Definitions Risk factors
Fragile Bones and how to recognise them. Rod Hughes Consultant physician and rheumatologist St Peter s hospital Chertsey
 Fragile Bones and how to recognise them Rod Hughes Consultant physician and rheumatologist St Peter s hospital Chertsey Osteoporosis Osteoporosis is a skeletal disorder characterised by compromised bone
Fragile Bones and how to recognise them Rod Hughes Consultant physician and rheumatologist St Peter s hospital Chertsey Osteoporosis Osteoporosis is a skeletal disorder characterised by compromised bone
Coordinator of Post Professional Programs Texas Woman's University 1
 OSTEOPOROSIS Update 2007-2008 April 26, 2008 How much of our BMD is under our control (vs. genetics)? 1 2 Genetic effects on bone loss: longitudinal twin study (Makovey, 2007) Peak BMD is under genetic
OSTEOPOROSIS Update 2007-2008 April 26, 2008 How much of our BMD is under our control (vs. genetics)? 1 2 Genetic effects on bone loss: longitudinal twin study (Makovey, 2007) Peak BMD is under genetic
Current and Emerging Strategies for Osteoporosis
 Current and Emerging Strategies for Osteoporosis I have nothing to disclose. Anne Schafer, MD Assistant Professor of Medicine Division of Endocrinology & Metabolism December 12, 2014 Outline Osteoporosis
Current and Emerging Strategies for Osteoporosis I have nothing to disclose. Anne Schafer, MD Assistant Professor of Medicine Division of Endocrinology & Metabolism December 12, 2014 Outline Osteoporosis
AACE/ACE Osteoporosis Treatment Decision Tool
 AACE/ACE Osteoporosis Treatment Decision Tool What is Osteoporosis? OSTEOPOROSIS is defined as reduced bone strength leading to an increased risk of fracture. Osteoporosis, or porous bones, occurs when
AACE/ACE Osteoporosis Treatment Decision Tool What is Osteoporosis? OSTEOPOROSIS is defined as reduced bone strength leading to an increased risk of fracture. Osteoporosis, or porous bones, occurs when
chapter Bone Density (Densitometry) RADIOPHARMACY INDICATIONS Radionuclide Localization Quality Control Adult Dose Range Method of Administration
 RADIOPHARMACY INDICATIONS Radionuclide Localization Quality Control Adult Dose Range Method of Administration") 10766-04_CH04_redo.qxd 12/3/07 3:47 PM Page 17 chapter 4 Bone Density (Densitometry) RADIOPHARMACY Radionuclide Single radionuclide: 125 I t 1/2 : 60.1 days Energies: 23 31 kev Type: EC, x, γ, accelerator
10766-04_CH04_redo.qxd 12/3/07 3:47 PM Page 17 chapter 4 Bone Density (Densitometry) RADIOPHARMACY Radionuclide Single radionuclide: 125 I t 1/2 : 60.1 days Energies: 23 31 kev Type: EC, x, γ, accelerator
Skeletal Manifestations
 Skeletal Manifestations of Metabolic Bone Disease Mishaela R. Rubin, MD February 21, 2008 The Three Ages of Women Gustav Klimt 1905 1 Lecture Outline Osteoporosis epidemiology diagnosis secondary causes
Skeletal Manifestations of Metabolic Bone Disease Mishaela R. Rubin, MD February 21, 2008 The Three Ages of Women Gustav Klimt 1905 1 Lecture Outline Osteoporosis epidemiology diagnosis secondary causes
Forteo (teriparatide) Prior Authorization Program Summary
 Prior Authorization Program Summary") Forteo (teriparatide) Prior Authorization Program Summary FDA APPROVED INDICATIONS DOSAGE 1 FDA Indication 1 : Forteo (teriparatide) is indicated for: the treatment of postmenopausal women with osteoporosis
Forteo (teriparatide) Prior Authorization Program Summary FDA APPROVED INDICATIONS DOSAGE 1 FDA Indication 1 : Forteo (teriparatide) is indicated for: the treatment of postmenopausal women with osteoporosis
Learning Objectives. Controversies in Osteoporosis Prevention and Management. Definition. Presenter Disclosure Information.
 4 4:45 pm Controversies in Osteoporosis Prevention and Management SPEAKER Carolyn Crandall, MD, MS Presenter Disclosure Information The following relationships exist related to this presentation: Carolyn
4 4:45 pm Controversies in Osteoporosis Prevention and Management SPEAKER Carolyn Crandall, MD, MS Presenter Disclosure Information The following relationships exist related to this presentation: Carolyn
Bone mineral density testing: Is a T score enough to determine the screening interval?
 Interpreting Key Trials CME CREDIT EDUCATIONAL OBJECTIVE: Readers will measure bone mineral density at reasonable intervals in their older postmenopausal patients Krupa B. Doshi, MD, CCD Department of
Interpreting Key Trials CME CREDIT EDUCATIONAL OBJECTIVE: Readers will measure bone mineral density at reasonable intervals in their older postmenopausal patients Krupa B. Doshi, MD, CCD Department of
Clinical Study Comparison of QCT and DXA: Osteoporosis Detection Rates in Postmenopausal Women
 International Endocrinology Volume 3, Article ID 895474, 5 pages http://dx.doi.org/.55/3/895474 Clinical Study Comparison of QCT and DXA: Osteoporosis Detection Rates in Postmenopausal Women Na Li, Xin-min
International Endocrinology Volume 3, Article ID 895474, 5 pages http://dx.doi.org/.55/3/895474 Clinical Study Comparison of QCT and DXA: Osteoporosis Detection Rates in Postmenopausal Women Na Li, Xin-min
Objectives. Discuss bone health and the consequences of osteoporosis on patients medical and disability status.
 Objectives Discuss bone health and the consequences of osteoporosis on patients medical and disability status. Discuss the pathophysiology of osteoporosis and major risk factors. Assess the major diagnostic
Objectives Discuss bone health and the consequences of osteoporosis on patients medical and disability status. Discuss the pathophysiology of osteoporosis and major risk factors. Assess the major diagnostic
New Osteoporosis Guidelines: What you and your health provider need to know QUESTION & ANSWER
 The first of the newsletters on these Qs and As should include a refresher on the Virtual Forums what they are, how they work, etc. The fact is that less than 5% of COPN members tune in for any given Forum.
The first of the newsletters on these Qs and As should include a refresher on the Virtual Forums what they are, how they work, etc. The fact is that less than 5% of COPN members tune in for any given Forum.
HIV and your Bones Osteopenia and Osteoporosis
 Osteopenia and Osteoporosis Background information For reasons not yet fully understood, higher rates of bone disease are starting to be seen in people living with HIV. These bone diseases include osteopenia
Osteopenia and Osteoporosis Background information For reasons not yet fully understood, higher rates of bone disease are starting to be seen in people living with HIV. These bone diseases include osteopenia
OSTEOPOROSIS IN INDONESIA
 OSTEOPOROSIS IN INDONESIA Hana Ratnawati Faculty of Medicine Maranatha Christian University Bandung - Indonesia 5th SBA Conference 2013 1 5th SBA Conference 2013 2 INTRODUCTION Indonesia is an archipelago
OSTEOPOROSIS IN INDONESIA Hana Ratnawati Faculty of Medicine Maranatha Christian University Bandung - Indonesia 5th SBA Conference 2013 1 5th SBA Conference 2013 2 INTRODUCTION Indonesia is an archipelago
Osteoporosis: A Tale of 3 Task Forces!
 Osteoporosis: A Tale of 3 Task Forces! Robert A. Adler, MD McGuire Veterans Affairs Medical Center Virginia Commonwealth University Richmond, Virginia, USA Disclosures The opinions are those of the speaker
Osteoporosis: A Tale of 3 Task Forces! Robert A. Adler, MD McGuire Veterans Affairs Medical Center Virginia Commonwealth University Richmond, Virginia, USA Disclosures The opinions are those of the speaker
Contractor Number 03201
 Local Coverage Article for Bone Mass Measurements Coverage - 2012 CPT Updates (A51577) Contractor Information Contractor Name Noridian Administrative Services, LLC opens in new window Contractor Number
Local Coverage Article for Bone Mass Measurements Coverage - 2012 CPT Updates (A51577) Contractor Information Contractor Name Noridian Administrative Services, LLC opens in new window Contractor Number
BMD: A Continuum of Risk WHO Bone Density Criteria
 Pathogenesis of Osteoporosis Osteoporosis Diagnosis: BMD, FRAX and Assessment of Secondary Osteoporosis AGING MENOPAUSE OTHER RISK FACTORS RESORPTION > FORMATION Bone Loss LOW PEAK BONE MASS Steven T Harris
Pathogenesis of Osteoporosis Osteoporosis Diagnosis: BMD, FRAX and Assessment of Secondary Osteoporosis AGING MENOPAUSE OTHER RISK FACTORS RESORPTION > FORMATION Bone Loss LOW PEAK BONE MASS Steven T Harris
They are updated regularly as new NICE guidance is published. To view the latest version of this NICE Pathway see:
 : assessing the risk of fragility fracture bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to be used online. They are updated regularly as new
: assessing the risk of fragility fracture bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to be used online. They are updated regularly as new
Osteoporosis Screening and Treatment in Type 2 Diabetes
 Osteoporosis Screening and Treatment in Type 2 Diabetes Ann Schwartz, PhD! Dept. of Epidemiology and Biostatistics! University of California San Francisco! October 2011! Presenter Disclosure Information
Osteoporosis Screening and Treatment in Type 2 Diabetes Ann Schwartz, PhD! Dept. of Epidemiology and Biostatistics! University of California San Francisco! October 2011! Presenter Disclosure Information
1 of 10 5/14/15 2:48 PM
 Close window Guideline Synthesis: Screening and Risk Assessment for Osteoporosis Guidelines Being Compared: 1. The North American Menopause Society (). Management of osteoporosis in postmenopausal women:
Close window Guideline Synthesis: Screening and Risk Assessment for Osteoporosis Guidelines Being Compared: 1. The North American Menopause Society (). Management of osteoporosis in postmenopausal women:
Because the low bone mass and deterioration
 OSTEOPOROSIS A look at recent expert guidelines and key studies in bone health, the findings of which affect your patients young and old Steven R. Goldstein, MD Dr. Goldstein is Professor of Obstetrics
OSTEOPOROSIS A look at recent expert guidelines and key studies in bone health, the findings of which affect your patients young and old Steven R. Goldstein, MD Dr. Goldstein is Professor of Obstetrics
Awareness, Diagnosis, and Management of Osteoporosis in Adults with Developmental Disabilities
 Awareness, Diagnosis, and Management of Osteoporosis in Adults with Developmental Disabilities Sunil J. Wimalawansa, MD, PhD, MBA, FACP, FRCP University Professor Professor of Medicine, Physiology & Pharmacology
Awareness, Diagnosis, and Management of Osteoporosis in Adults with Developmental Disabilities Sunil J. Wimalawansa, MD, PhD, MBA, FACP, FRCP University Professor Professor of Medicine, Physiology & Pharmacology
Annotations Part III Vertebral Fracture Initiative. International Osteoporosis Foundation March 2011
 Annotations Part III Vertebral Fracture Initiative International Osteoporosis Foundation March 2011 Slide 1-3 Topics to be covered: What is vertebral fracture assessment? How does VFA compare to standard
Annotations Part III Vertebral Fracture Initiative International Osteoporosis Foundation March 2011 Slide 1-3 Topics to be covered: What is vertebral fracture assessment? How does VFA compare to standard
Pharmacy Management Drug Policy
 SUBJECT: - Forteo (teriparatide), Prolia (denosumab), Tymlos (abaloparatide) POLICY NUMBER: Pharmacy-35 EFFECTIVE DATE: 9/07 LAST REVIEW DATE: 9/29/2017 If the member s subscriber contract excludes coverage
SUBJECT: - Forteo (teriparatide), Prolia (denosumab), Tymlos (abaloparatide) POLICY NUMBER: Pharmacy-35 EFFECTIVE DATE: 9/07 LAST REVIEW DATE: 9/29/2017 If the member s subscriber contract excludes coverage
Disclosures. Diagnostic Challenges in Osteoporosis: Whom To Treat 9/25/2014
 Disclosures Diagnostic Challenges in Osteoporosis: Whom To Treat Ethel S. Siris, MD Columbia University Medical Center New York, NY Consultant on scientific issues for: AgNovos Amgen Eli Lilly Merck Novartis
Disclosures Diagnostic Challenges in Osteoporosis: Whom To Treat Ethel S. Siris, MD Columbia University Medical Center New York, NY Consultant on scientific issues for: AgNovos Amgen Eli Lilly Merck Novartis
All about Osteoporosis symptoms, diagnosis, treatment
 Health & Fitness Published : 07 Sep 2017, 14:41 All about Osteoporosis symptoms, diagnosis, treatment By : BD Post Desk Osteoporosis is a bone disease. Its name comes from the Latin for porous bones. The
Health & Fitness Published : 07 Sep 2017, 14:41 All about Osteoporosis symptoms, diagnosis, treatment By : BD Post Desk Osteoporosis is a bone disease. Its name comes from the Latin for porous bones. The
IEHP UM Subcommittee Approved Authorization Guidelines DEXA Scan
 Policy: IEHP UM Subcommittee Approved Authorization Guidelines IEHP considers bone mineral density testing using DEXA medically necessary for members who meet any of the following criteria: Women aged
Policy: IEHP UM Subcommittee Approved Authorization Guidelines IEHP considers bone mineral density testing using DEXA medically necessary for members who meet any of the following criteria: Women aged
Major Recommendations Recommendations apply to postmenopausal women and men age 50 and older.
 Clinical Practice Guideline Effective August 2007 (Revised 10/09) This guideline is based upon the guideline developed by an expert committee of the National Osteoporosis Foundation (NOF) in collaboration
Clinical Practice Guideline Effective August 2007 (Revised 10/09) This guideline is based upon the guideline developed by an expert committee of the National Osteoporosis Foundation (NOF) in collaboration
Corporate Medical Policy
 Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: bone_mineral_density_studies 12/1996 9/2017 9/2018 9/2017 Description of Procedure or Service Bone density
Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: bone_mineral_density_studies 12/1996 9/2017 9/2018 9/2017 Description of Procedure or Service Bone density
Bone Densitometry Equipment Operator
 Bone Densitometry Equipment Operator The purpose of the Bone Densitometry Equipment Operator Examination, which is made available to state licensing agencies, is to assess the knowledge and cognitive skills
Bone Densitometry Equipment Operator The purpose of the Bone Densitometry Equipment Operator Examination, which is made available to state licensing agencies, is to assess the knowledge and cognitive skills
Prodigy. from GE Healthcare. Most trusted, reliable and best-selling DXA system with one of the largest installed base in the world. gehealthcare.
 Prodigy from GE Healthcare Most trusted, reliable and best-selling DXA system with one of the largest installed base in the world gehealthcare.com Prodigy High performance, efficient and reliable DXA system
Prodigy from GE Healthcare Most trusted, reliable and best-selling DXA system with one of the largest installed base in the world gehealthcare.com Prodigy High performance, efficient and reliable DXA system
ReviewArticle. Frequently Asked Questions About Bone Mineral Density Test
 ReviewArticle Frequently Asked Questions About Bone Mineral Density Test Jiraporn Sriprapaporn, M.D.*,** *Division of Nuclear Medicine, Department of Radiology, Faculty of Medicine Siriraj Hospital, Mahidol
ReviewArticle Frequently Asked Questions About Bone Mineral Density Test Jiraporn Sriprapaporn, M.D.*,** *Division of Nuclear Medicine, Department of Radiology, Faculty of Medicine Siriraj Hospital, Mahidol