Profix. Total Knee System. As described by
|
|
|
- Kathlyn Collins
- 6 years ago
- Views:
Transcription
1 Profix Total Knee System P R I M A R Y P R O C E D U R E As described by Leo A. Whiteside, M.D. Associate Research Professor Washington University School of Medicine Director, Biomechanical Research Laboratory Barnes Jewish West County Hospital St. Louis, Missouri Nota Bene: The technique description herein is made available to the healthcare professional to illustrate the author s suggested treatment for the uncomplicated procedure. In the final analysis, the preferred treatment is that which addresses the needs of the specific patient. This system is intended for cemented use only. 1
2 REOPERATIVE PLANNING PProper surgical procedures are the responsibility of the medical professional, especially the operating surgeon. The following guidelines are furnished for informational purposes only as techniques used by Leo A. Whiteside, M.D. Each surgeon must evaluate the appropriateness of these procedures based on his or her medical training, experience, and patient evaluation. The size of the prosthesis is estimated by comparing the lateral radiograph of the femur with the implant templates (Figure 1). The template size which most closely matches the profile of the femur on the anterior and posterior aspects is chosen. To maintain proper quadriceps tension in flexion and extension, the patellar flange should not be radically shifted either anteriorly or posteriorly. Tibial templates are also available to approximate the size and thickness of components that will be needed for surgery. The geometric dimensions for the Profix Femoral and Tibial Implants are provided. All Profix Femoral and Tibial Implant sizes are interchangeable when using the Conforming Insert. Conforming Plus Inserts can be used with any femoral component up to two sizes larger than the selected insert. Femoral Implant Specifications Size Range M-L A-P Dimensions Dimensions Size 1 60 mm 48 mm Size 2 65 mm 52 mm Size 3 67 mm 56 mm Size 4 69 mm 59 mm Size 5 73 mm 63 mm Size 6 78 mm 68 mm Size 7 83 mm 73 mm Tibial Implant Specifications Size Range M-L A-P Dimensions Dimensions Size 1 61 mm 42 mm Size 2 65 mm 45 mm Size 3 70 mm 48 mm Size 4 75 mm 51 mm Size 5 80 mm 55 mm Size 6 85 mm 58 mm Size 7 91 mm 61 mm 2

3 Figure 1 3
4 SURGICAL APPROACH A long, anterior midline skin incision and medial parapatellar fascial incision will allow the patella to be reflected laterally (Figure 2). To achieve good lateral position of the patella, it is usually necessary to completely detach the oblique portion of the vastus medialis from the distal one-third of the quadriceps tendon. The vastus intermedius, lateralis, and rectus femoris are left in continuity with the patella so that early quadriceps rehabilitation will be possible. Synovium and fat proximal to the patellar groove should be excised to allow proper function of the anterior stylus later in surgery. For maximum exposure of the joint, flex the knee to its maximum point without jeopardizing the stability of the patellar tendon. Ligament assessment and balancing should be done after osteophytes have been removed and trials are in place. 4

5 Figure 2 5
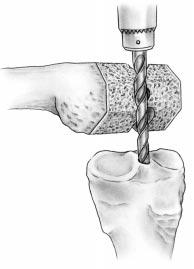
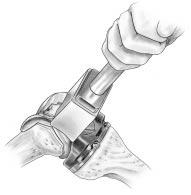
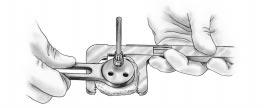
6 S T A G E 1 FOnce the knee is flexed and positioned for surgery, the femoral shaft is drilled to accept the 8 mm Reamer Rod. The Femoral Sizer is then placed over the Reamer Rod to determine necessary size of femoral prosthesis. Note: As a matter of convenience, the author will use the 3/8" drill to open the proximal tibia if IM Tibial Alignment is being used. STEPS: EMORAL PREPARATION AND SIZING A. Using the Femoral 3/8" Drill, make a hole anterior to the posterior cruciate ligament attachment (Figure 3). This drill is easily attached to power equipment using the Power Quick Connect. This starter hole is larger than the 8 mm Reamer Rod. B. Attach the T-Handle Quick Connect to the 8 mm Reamer Rod and slowly insert into femoral canal. C. Place the Femoral Sizer over the 8 mm Reamer Rod and advance it to rest on the distal condyles. Leave the sliding module in the center loose (Figure 4). D. Attach the External Rotation Guide (Neutral or 3 ) to the holes in the face of the sizer. Move the External Rotation Guide anteriorly until the paddles contact the posterior femoral condyles. Tighten the sliding module (Figure 5). E. Use the Anterior Referencing Guide to determine the appropriate femoral component size. On the lateral side, place the Anterior Referencing Guide through one of the slots numbered one through seven (Figure 6). The tip of the guide will show the point where the saw blade will exit the bone for a particular size. This allows a visual check to ensure that the anterior femoral cut will not notch the femur. F. Choose appropriate femoral size and prepare for femoral bone resection. If between sizes, move down one size for anterior referencing or up one size for posterior referencing Femoral 3/8" Drill Power Quick Connect T-Handle Quick Connect mm Reamer Rod (Standard) Femoral Sizer External Rotation Guide 3 Left Anterior Referencing Guide Quick Release Handle 6



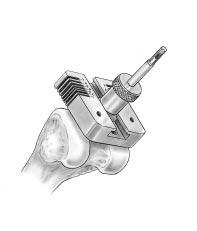
7 Figure 3 Figure 4 Figure 5 Figure 6 7
8 S T A G E 2 FEMORAL RESECTION (ANTERIOR REFERENCING) NOTE: If posterior referencing is desired, refer to Appendix A. If additional femoral bone resection is desired, refer to Appendix B. Femoral resection will require the appropriate size Femoral Cutting Block, Valgus Module (5 or 7 ), Anterior Stylus, and Distal Cutting Block. The correct valgus angle is determined from the preoperative radiographs. The Cutting Block is stabilized by sliding the block over the 8 mm Reamer Rod and spiking it to the bone. If desired, the 8 mm Reamer Rod may be removed. STEPS: A. Loosely attach the appropriate Valgus Module into the center of the Femoral Cutting Block by tightening the thumb screw on the module (Figure 7). If resecting the right knee, Right Up will face anteriorly. Left Up will face anteriorly if resecting the left knee (Figure 8). Attach the Anterior Stylus to the Femoral Cutting Block. B. Place the Femoral Cutting Block over the 8 mm Reamer Rod. Advance the Cutting Block until it is firmly seated against the distal femur. It may be necessary to tap the top of the Valgus Module with a mallet to assure that the Femoral Cutting Block is resting on the distal femur. Allow the Anterior Stylus to rest on the highest point of the lateral cortex. Tighten the Valgus Module completely. Orient the Cutting Block so the central opening is parallel with the deepest part of the patellofemoral groove and the intercondylar notch. This will position the cutting block at approximately 3 external rotation. C. Spike the Cutting Block to the femoral bone with the hollow tip Bone Spikes. Spike the side first (medial or lateral) that is in contact with the distal femur. As the Spikes are driven in, tighten the Valgus Module to ensure firm seating. Use Spikes in all four holes. Remove the Anterior Stylus. The 8 mm Reamer Rod may be removed without compromising the block stability. D. In the following order, cut (1) Anterior, (2) Anterior Chamfer, (3) Posterior, and (4) Posterior Chamfer (Figure 9). NOTE: If a long stem is desired in a primary case, align marks on Valgus Module with marks on Cutting Block and tighten Module. Establish appropriate rotation of Cutting Block as described in Step B and then pin block º Valgus Module Femoral Cutting Block, Size Anterior Stylus Long Bone Spike Short Bone Spike 8

9 Figure 8 Figure 7 2 Figure Anterior 2. Anterior Chamfer 3. Posterior 4. Posterior Chamfer 9
10 FEMORAL RESECTION (ANTERIOR REFERENCING) E. Attach the Distal Cutting Block to the anterior aspect of the Femoral Cutting Block and tighten the thumb screws (Figure 10). Cut the distal femur. Remove Bone Spikes from the block using the Bone Spike Extractor. F. Remove bone fragments or osteophytes with the Osteogator Distal Cutting Block, Size Bone Spike Extractor Osteogator S T A G E 3 IBIAL PREPARATION (IM ALIGNMENT) TEM Alignment Technique described in Appendix A As noted, the author opens the tibia at the same time the femur is drilled. The knee is positioned so the tibial surface will sublux anteriorly from under the femoral condyles. STEPS: A. Using the Femoral 3/8" Drill, open the proximal tibial medullary canal just posterior to the tibial attachment of the anterior cruciate ligament (Figure 11). Slowly place the 8 mm Reamer Rod into the tibial shaft using the T-Handle Quick Connect. Note: To assure proper positioning of the drill hole, a Tibial Prep Plate may be used as a template to determine the appropriate location of a stem extension. Mark the center hole of the prep plate with methylene blue. This will approximate the stem extension location, which is slightly medial on the final tibial implant Femoral 3/8" Drill mm Reamer Rod T-Handle Quick Connect Tibial Prep Plate, Size 4 Left 10

11 Figure 10 Figure 11 11
12 S T A G E 4 ROXIMAL TIBIAL RESECTION (IM ALIGNMENT) PInstruments include the Tibial Alignment Assembly and Tibial Cutting Block (Neutral or 4 slope). These instruments are assembled prior to placement on the bone. STEPS: A. Set the desired resection level by adjusting the Tibial Stylus on the Tibial Alignment Assembly. Usually, 8 mm 10 mm of bone is resected referencing from the unaffected side of the tibial plateau. The assembly is now placed over the 8 mm Reamer Rod (Figure 12). B. Lower the assembly until the stylus touches the most central point of the highest or good side of the tibial plateau. Tighten the screw against the 8 mm Reamer Rod. Move the Tibial Cutting Block until it contacts the anterior tibial cortex. The sliding screw is then tightened. C. The Tibial Cutting Block is now in the proper location to remove the desired amount of bone established in Step A. Spike the Cutting Block to the bone and remove the Reamer Rod and Tibial Alignment Assembly if desired. Note: If using the 4 slope Tibial Cutting Block, centralize the hash marks on the tibial block over the medial third of the tibial tubercle before spiking to bone. D. Resect the proximal tibia through the slotted block using a Profix Sawblade (Figure 13) Tibial Alignment Assembly Tibial Cutting Block 0º Hex Screwdriver 12

13 Figure 12 Figure 13 13
14 S T A G E 5 IBIAL SECONDARY FINISHING TNote: Secondary finishing can be done only when using the IM Alignment Technique. The Tibial Secondary Prep Guide (Neutral or 4 Slope) produces a smooth, more precise, finishing resection of the proximal tibia. The guide is placed over the 8 mm Reamer Rod and lightly tapped into the proximal tibia. Adding a 4 posterior slope with the Tibial Secondary Prep Guide is an excellent alternative (versus downsizing the femoral component) to gain increased flexion if the knee is tight following an initial neutral resection. STEPS: A. Place the Tibial Secondary Prep Guide over the Reamer Rod and tap it until the proximal edge of the fins on the guide are slightly below the proximal surface and are no longer visible (Figure 14). Tighten hex head screw against Reamer Rod. Note: If using the 4 Tibial Secondary Prep Guide, centralize the hash marks of the guide over the medial third of the tibial tubercle. B. Using a Profix Sawblade, resect a thin layer of bone from the proximal surface (Figure 15). As the Sawblade is moved posterior, be careful to prevent the sawblade from resecting below the proximal edge of the guide fins. Once the Sawblade rests on top of the fins, the fins guide the sawblade for the remainder of the cut. Remove the Guide and Reamer Rod as an assembly by tapping with a Mallet on the underside of the Cutting Guide Tibial Secondary Prep Guide Large Mallet 14

15 Figure 14 Figure 15 15
16 S T A G E 6 IBIAL & FEMORAL PREPARATION TThe Tibial Prep Plate and desired Articular Insert Trial are placed on the proximal tibia to determine coverage and necessary thickness of insert to restore the joint line. The femoral trial is placed on the distal femur. STEPS: A. Place the Tibial Prep Plate on the proximal tibia. Place the 12 mm Stem Plug into the central hole of the Prep Plate and tap into position (Figure 16). This will serve as a rotational axis. The Stem Plug can be removed from Prep Plate with the Quick Release Handle. Note: If trialing with a tibial long stem trial is desired, ream up to an odd size reamer. The Trial Taper Stem is attached to the Tibial Prep Plate for stem trial attachment. Thread the Stem Coupler (Neutral or 4 ) into desired long stem trial and impact onto the Trial Taper Stem (see Revision technique). B. Place the Conforming or Conforming Plus Articular Insert Trial onto the Prep Plate using the Articular Insert Trial Rotation Handle (Figure 17). C. Place the appropriate size Femoral Trial onto the distal femur and determine correct medial/lateral coverage (Figure 18). Spike the Femoral Trial into place through distal condyles using short Bone Spikes. D. Using a Profix Sawblade, resect the patellofemoral groove, cutting along the medial and lateral sides of the femoral trial (Figure 19). Maintain blade contact against the femoral trial to assure proper resection. Insert the proper size Patellofemoral Groove Trial Tibial Prep Plate Size 4 Left mm Stem Plug Quick Release Handle Trial Taper Stem Stem Coupler Articular Insert Trial Rotation Handle Femoral Trial Size 4 Left Patellofemoral Groove Trial Size 4 16



17 Figure 16 Figure 17 Figure 18 Figure 19 17
18 S T A G E 7 KAlignment of the knee is assessed with the femoral and tibial trials in place. The Tibial Prep Plate is rotated to assure that the line on the insert matches with the line on the Patellofemoral Groove Trial with the knee in full extension. STEPS: NEE ALIGNMENT ASSESSMENT A. In full extension, assess the alignment of trials and evaluate range of motion. B. Insert the Articular Insert Trial Rotation Handle into the anterior slot on the Articular Insert Trial. Rotate the handle until the lines on the Femoral and Tibial Trials are perfectly aligned (Figure 20). C. With the knee in full extension, align the marks on the Insert Trial and Femoral Trial to assure proper rotational alignment. Using a cautery pencil, mark the tibia below the alignment markers on the Tibial Prep Plate. When using a Nonporous Tibial Implant, remove the Articular Insert Trial and prepare for the distal fins on the implant using the appropriate Nonporous Tibial Fin Punch, All- Poly Tibial Fin Punch, or Tibial Keel Stem Punch (Figure 21). To prevent the Prep Plate from shifting while using the punch, it is recommended to pin the Prep Plate in place through the anterior spike holes. If using the I-beam stem, use the appropriate size Nonporous Tibial Fin Punch, then remove the prep plate. Place the I-beam stem punch on the proximal tibia by inserting the fins of the punch into the prepared fin slots, then punch. Note: The Tibial Keel Stem Punch is designed to be used with Profix Tibial Implants sizes 3 7. When using a Size 1 or 2 Profix Tibial Implant, it is recommended to use the 14 mm Metaphyseal Stem Femoral Trial Size 4 Left Articular Insert Trial Size 4 Left 10 mm Nonporous Tibial Fin Punch Size All-Poly Tibial Fin Punch Tibial Keel Stem Punch 18


19 Figure 20 Figure 21 19
20 S T A G E 8 20 ATELLAR PREPARATION (INSET AND ONSET) PThe inset patellar reaming includes the Patellar Clamp, Ring Gauge, Reamer, Reamer Collet, and Reamer Stop. Inset patellas are 23 mm, 26 mm, and 29 mm in diameter. Thicknesses are 11 mm, 12 mm, and 14 mm, respectively. The onset patellas are available in 29 mm, 32 mm, 35 mm, and 39 mm diameters. The onset technique includes the Patellar Peg Drill, Drill Guide, and Patellar Clamp. STEPS: INSET TECHNIQUE A. Place the Patellar Ring Gauge against the patellar surface to determine appropriate diameter (Figure 22). Slide the correct diameter Patellar Reamer Collet over the Patellar Clamp. Position the Reamer Collet over the vertical ridge of the patella and tighten the thumb screw (Figure 23). Lightly tap the proximal (top) edge of the collet with the mallet to engage the teeth of the collet into the patella. Tighten the thumb screw another half turn. B. Place the appropriate diameter Patellar Reamer into the collet. Slide the appropriate diameter of the Ring Gauge onto the shaft of the Patellar Reamer above the Reamer Collet and lower the Reamer Stop on top of the Ring Gauge (Figures 24 and 25). Note: The word UP should be visible on the reamer stop. C. Remove the Ring Gauge and ream the patella until the Reamer Stop contacts the Reamer Collet. D. Place appropriate diameter Patellar Trial into prepared bone cavity (Figure 26). Begin range of motion to evaluate patellar tracking. Remove the Patellar Femoral Trial using the Femoral Extractor. STEPS: ONSET TECHNIQUE A. Clamp the patella on the outermost regions of the bone. Using a Profix Sawblade, resect the patellar bone. B. Using the Patellar Drill Guide and the Peg Drill, drill three holes in the remaining patellar bone (Figure 27). C. Place the Onset Patellar Trial onto resurfaced patella and begin range of motion to evaluate patellar tracking. Remove the Femoral Trial using the Femoral Extractor. Note: Soft tissue and ligament balancing should be checked at this point to assure appropriate alignment and stability of the joint Patellar Ring Gauge Patellar Reamer Collet 26 mm Patellar Clamp Patellar Reamer 26 mm Reamer Stop Patellar Trial 26 mm Femoral Extractor Patellofemoral Groove Trial Size 4




21 Figure 22 Figure 23 Figure 24 Figure 25 Figure 26 Figure 27 21
22 S T A G E 9 IBIAL IMPLANTATION* TOnce removed from the packaging material, the Profix Tibial Implant is placed on the table. If a stem extension is desired, the stem should be removed from its packaging, the keyed marks on the stem aligned with the marks on the taper of the tibial implant, and impacted onto the tibial implant. Firmly impact the stem several times to assure a rigid lock of the morse taper. Note: The author recommends the use of the Metaphyseal Stem on the Porous or Nonporous Tibial Implants. Alternate Primary Tibial Stems are available. STEPS: A. Using the Tibial Rotation Alignment Guide, position the implant so the cautery markings are aligned with the markings on the tibial implant (Figure 28). Slowly force the tibial implant with the Metaphyseal Stem (or other primary stem extension) into the proximal tibia. Remove the alignment guide once the tibial stem has established alignment. Note: If the Metaphyseal Stem is desired, the 12 mm Stem Plug is the only preparation necessary to accept the Metaphyseal Stem. It is important to assure the markings align to avoid malpositioning of the tibial implant. B. Using the Tibial Impactor, seat the tibial implant on the proximal tibia. If using screws, orient the Tibial Screw Drill Guide over each hole and drill using the Tibial Screw Drill (Figure 29). The three peripheral holes in the drill guide are angled at 10 to reach the cortex if desired (each hole is angled toward the center of the drill guide). C. Using the Depth Gauge, determine the depth of each screw hole to accept the appropriate size screw. Insert and tighten screws of the tibial implant, alternating to avoid liftoff. D. After determining the thickness of the articular insert, slide the insert posteriorly into the tibial implant and engage the peripheral locking mechanism (Figure 30). A light tap is all that should be required to seat insert securely. *CEMENTING TECHNIQUE Using the standard mixing protocol for bone cement, mix and prepare bone cement for placement on the tibial component. Place bone cement on the undersurface of the tibial component and impact the tibial component into place. Remove excess cement Tibial Rotation Alignment Guide Metaphyseal Stem Tibial Impactor Tibial Screw Drill Guide Tibial Screw Drill Depth Gauge 22


23 Figure 29 Figure 28 Figure 30 23
24 S T A G E 1 0 EMORAL IMPLANTATION FUsing the standard mixing protocol for bone cement, apply bone cement to the undersurface of the femoral component. The femoral component is impacted into place. Remove excess cement. STEPS: A. Prior to applying cement to the femoral component, use the Femoral Peg Drill to prepare for Femoral Pegs (Figure 31). Drill to the depth of the circular groove on the peg drill. Apply cement to the femoral component and place on the distal femur. Locate the peg holes, and impact into place using the Femoral Impactor (Figure 32). It is recommended to place the knee at 90 of flexion and use the articular insert to help guide the femoral component onto the femur Femoral Peg Drill Femoral Impactor S T A G E 1 1 ATELLAR IMPLANTATION PThe Profix Patellar Implant is available in both inset and onset designs. Cement is used in both cases to affix the Patellar Implant to the bone. STEPS: A. Apply bone cement to the undersurface of the Patellar Implant. B. Place the Patellar Implant in the resected bone (Figure 33). The Patellar Cement Clamp Fitting inserted into the 23 mm Patellar Reamer Collet, will be used when cementing the 23 mm, 26 mm, and 29 mm Inset Patellar Implants. Trim excess osteophytes. CLOSURE: Closure is performed in the usual manner Patellar Cement Clamp Fitting Patellar Reamer Collet 23 mm 24



25 Figure 31 Figure 32 Figure 33 25
26 26
27 R E V I S I O N T E C H N I Q U E Revision Technique 27
28 S T A G E 1 REVISION FEMORAL/TIBIAL PREPARATION Once femoral and tibial primary implants are removed, reamer placement and resection for the femur and tibia are performed. This will prepare for revision femoral and tibial trialing. STEPS: A. Open tibial canal with the appropriate Femoral Drill. Ream tibial canal with the appropriate Long Stem Reamer (typically start with 10 mm reamer). Progressively ream the canal by increasing the reamer diameter 1 mm at a time until the desired stability is obtained (Figure 1). Stopping on an odd size reamer is ideal. Reamer depth is determined by using the marks on the shaft of the reamer (100 mm, 150 mm, 200 mm). Note: If the reamer diameter is 13 mm or less, the Long Stem Drill must be used to prepare for a 10 mm or 12 mm long stem implant. B. Place the Tibial Alignment Assembly on the Long Stem Reamer. Set the stylus for a minimal amount of bone resection to shave prominent bone. Once the stylus is resting on the most proximal portion of the tibial plateau, tighten nut to Reamer (Figure 2). Resect the proximal tibia using Tibial Cutting Block (Neutral or 4º). If a 4 cut is desired, the Tibial Alignment Assembly should be rotated to the medial third of the tibial tubercle and pinned into place. Note: Optional technique is to use Tibial Secondary Prep Instrument as described on page 14. C. Ream femoral canal using the same technique as tibia (Figure 3). D. Place the Revision Distal Cutting Block over the Reamer. Establish approximate external rotation of cutting block by rotating the Block until the two bone spike ears are in line with the epicondylar axis. Tap the Block to ensure it rests firmly on the bone and tighten the Valgus Module. Pin the Block to bone. Set the resection level of the distal slot by loosening the thumb screws and adjusting to appropriate resection level. Tighten screws. Proceed with distal resection to achieve a flat distal femoral surface (Figure 4) Femoral 3/8" Drill mm Long Stem Reamer Long Stem Drill Tibial Alignment Assembly Tibial Cutting Block 0º Revision Distal Cutting Block º Valgus Module 28


29 Figure 1 Figure 2 Figure 4 Figure 3 29
30 S T A G E 2 EVISION FEMORAL/TIBIAL TRIALING RFemoral and tibial preparation are complete. Both femoral and tibial trials can be prepared on the back table. The femoral trial (possibly including long stem trial and wedges) will be impacted into the femoral bone, and the tibial trial (possibly including long stem trial and wedges) will be impacted into tibial bone. STEPS: A. Attach Long Stem Trial to Stem Trial Coupler (Neutral* or 7º); then impact onto the Revision Femoral Trial. Always use one size smaller diameter Long Stem Trial than the reamed canal. Make certain that the trial is in the correct external rotation by rotating the trial until the epicondylar axis line is parallel to the imaginary line between the epicondyles of the femur. The Long Stem Trial will guide the Femoral Trial into proper A-P and M-L position. Drive Femoral Trial onto femur using Femoral Impactor (Figure 5). B. The sharp cutting edges of the posterior condyles and anterior aspect of the Femoral Trial will shave any prominent bone (Figure 6). Once seated, proceed with resection of distal bone for appropriate wedge placement. If the trial does not fully seat on the distal femur, resect through the Anterior Chamfer slots. If wedges are desired, resect bone through the respective parallel slots in Femoral Trial (Figure 7). If L-shaped wedges will be used, remove Femoral Trial and attach Femoral Wedge Trial to determine appropriate trial fit (Figure 8). The sharp cutting edges of the posterior condyles of the wedge trials will shave remaining bone if L-Wedges are desired. For Distal-Only Wedges, resect distal femoral bone through the respective parallel slots in the Femoral Trial. Trials do not exist for Distal-Only Wedges. C. Attach Trial Taper Stem to Tibial Prep Plate. Remove the top piece of the Trial Taper Stem by loosening the screw inset in the top. Place the distal side of the Prep Plate on top of the taper piece so that the taper piece is keyed into the central opening of the Prep Plate. From the proximal side, place the top piece of the Trial Taper Stem through the Prep Plate opening and tighten screw in top piece. Attach Long Stem Trial to Stem Trial Coupler (Neutral* or 4 ); then impact onto Trial Taper Stem (Figure 9). Always use one size smaller diameter Long Stem Trial than will be used for the implant. *Using a neutral coupler on a femoral component with taper will achieve a 5 angle Long Stem Trial 150 mm x 10 mm Stem Trial Coupler 7º Revision Femoral Trial Size 4 Left Femoral Impactor Distal-Only Wedge Femoral Wedge Trial LL/RM Small Size Trial Taper Stem Tibial Prep Plate, Size 4 Left 30





31 Figure 6 Figure 5 Figure 7 Figure 8 Figure 9 31
32 S T A G E 2 REVISION FEMORAL/TIBIAL TRIALING D. Place Conforming or Conforming Plus Trial Insert into Tibial Prep Plate using Articular Insert Trial Rotation Handle (Figure 10). E. In full extension, assess the alignment of trials and evaluate range of motion. F. With the knee in full extension, align the marks on the Insert Trial and Femoral Trial to assure proper rotational alignment. Using a cautery pencil, mark the tibia below the alignment markers on the Tibial Prep Plate. When using a Nonporous Tibial Implant, remove the Articular Insert Trial and prepare for the distal fins on the implant using the appropriate Nonporous Tibial Fin Punch. To prevent the Prep Plate from shifting while using the punch, it is recommended to pin the Prep Plate in place through the anterior spike holes. If Step Wedges are desired, remove Trial Insert and spike Tibial Prep Plate using the anterior spike hole on the good tibial plateau. Note: Tibial wedges are for nonporous implants only. G. Place Tibial Wedge Resection Guide onto Tibial Prep Plate. The peg on the Guide will fit into the hole in the top of trial taper and the fins on the Guide will fit into the slots in the Prep Plate. Slide the cutting block portion of the guide until it contacts the anterior tibial cortex. Tighten the hex screw on wedge platform. Pin the cutting block into place. Place a pin or small drill bit into pin hole adjacent to slot used for resection to restrict resection to desired side of tibial plateau. If desired, the Tibial Trial and Wedge Platform can be removed by loosening hex screw on wedge platform. Then resect for desired thickness (Figure 11). Remove Wedge Resection Guide. Using the Quick Release Handle, insert appropriate size Tibial Wedge Spacer to evaluate wedge size and stability (Figure 12) Conforming Plus Trial Insert Size 4 Left 10 mm Articular Insert Trial Rotation Handle Nonporous Tibial Fin Punch Size Tibial Wedge Resection Guide Quick Release Handle Tibial Wedge Spacer Size


33 Figure 10 Figure 11 Figure 12 33
34 S T A G E 3 REVISION FEMORAL/TIBIAL IMPLANTING After trials have been removed, proceed with manufacturer suggested cementing technique to attach femoral and tibial wedges to implants. STEPS: A.. Impact Long Stem (Neutral or 7º) onto femoral implant. Impact Long Stem (Neutral or 4º) onto tibial implant. The keyed mark on the stem should be aligned with the keyed mark on the taper of the implant. Firmly impact the stem several times to assure a rigid lock on the morse taper. Long Stems should be 1 mm larger than reamed femoral and tibial canals if the canals were reamed to an odd size. If the canals were reamed to an even size, use the same size diameter Long Stem. Cement appropriate thickness wedges to femoral and tibial implants using the Wedge Cement Clamp. NOTE: A tibial wedge used on the medial side will underhang the tibial implant periphery slightly in the posterior medial area. A tibial wedge used on the lateral side will match the tibial implant periphery. NOTE: Current cementing techniques should be used for all prepared surfaces. B. Insert Tibial Implant and Long Stem into tibial canal. Use the Tibial Rotation Alignment Guide with the Long Alignment Plate to align the cautery marks on the bone with the marks on the implant (Figure 13). Slowly impact the Tibial Implant with the stem into the proximal tibia. Remove the alignment guide once the tibial stem has established alignment. Impact Tibial Implant into place using Tibial Impactor. Place appropriate thickness Conforming or Conforming Plus Insert into the Tibial Implant. Note: For a porous Tibial Implant, use the Tibial Screw Drill Guide and drill for screws. Insert depth gauge and hook cortical bone to determine screw length. Drill screws into Tibial Implant alternating until screws are seated firmly in bone (Figure 14). Place appropriate thickness Conforming or Conforming Plus Insert into Tibial Implant. C. Place femoral component and Long Stem into femoral canal. Impact Femoral Implant into bone using the Femoral Impactor (Figure 15). Before impacting, make sure that the Femoral Implant is in the same rotational position as the trial Long Stem Wedge Cement Clamp Tibial Rotational Alignment Guide Long Alignment Plate Tibial Impactor Femoral Impactor 34


35 Figure 13 Figure 14 Figure 15 35
36 36
37 Posterior -Stabilized Technique: Primary & Revision P O S T E R I O R S T A B I L I Z E D T E C H N I Q U E : P R I M A R Y & R E V I S I O N 37
38 S T A G E 1 RIMARY POSTERIOR STABILIZED PThis portion of the technique will prepare the femur for the femoral housing of the PS implant. Instruments required for this procedure include the PS Positioner, PS Box Reamer Guide, PS Box Reamer, PS Box Chisel Guide, PS Box Chisel, and the PS Femoral Trial. STEPS: A. Make all femoral and tibial cuts in the manner described in the Primary Technique. B. Place the appropriate size Femoral Trial onto the distal femur and determine correct medial/lateral coverage. Spike Femoral Trial into place through distal condyles using short Bone Spikes. Using a Profix Sawblade, resect the patellofemoral groove, cutting along the medial and lateral sides of the Femoral Trial. Maintain blade contact against the Femoral Trial to assure proper resection. Then remove the Femoral Trial. C. Attach the PS Positioner (Figure 1) referencing off the femoral spike holes (which were already created by the Femoral Trial) or use the Anterior Chamfer and distal cut intersection. Predrill and pin the PS Positioner with bone spikes. Note: If desired, the Quick Release Handles may be attached to the PS Positioner. D. With the thumb screws on the PS Positioner loose, place the PS Box Reamer Guide (Figure 2) into the Positioner, then tighten the thumb screw to firmly hold the Reamer Guide in place. Proceed to ream through both holes with the PS Box Reamer (Figure 3). This will prepare the majority of the femoral housing area. E. Loosen the positioner thumb screw and remove the Reamer Guide. Place the PS Box Chisel Guide into the Positioner and tighten the thumb screw firmly to hold the Chisel Guide in place. Attach the Fin Punch Handle to the PS Box Chisel and impact the PS Box Chisel (Figure 4) through the Box Chisel Guide. This will complete the bone resection for the PS Femoral Housing PS Positioner PS Box Reamer Guide PS Box Reamer PS Box Chisel Guide Fin Punch Handle PS Box Chisel 38


39 Figure 1 Figure 2 Figure 3 Figure 4 39
40 P RIMARY POSTERIOR STABILIZED F. Remove the positioner and assemble the PS Femoral Trial. Place the Primary Femoral Trial Module (without taper) into the appropriate size trial and tighten one of the module lugs with an implant screwdriver. After one turn, tighten the other lug one turn, and alternate until the module is seated in the trial (Figure 5). Place the PS Femoral Trial onto the distal femur (Figure 6). Do not directly impact the trial on the anteromedial or anterolateral flanges. Impacting these areas could deform the anterior cutting slots. G. After evaluating the range of motion with Femoral and Tibial Trials, implant the PS Femoral Implant in the distal femur. Implant the Tibial and the PS Articular Insert. Assess range of motion for the final implants (Figure 7) PS Femoral Trial Primary Femoral Trial Module without Taper 40


41 Figure 5 Figure 6 Figure 7 41
42 S T A G E 1 EVISION POSTERIOR STABILIZED RSteps A and B are standard throughout the Revision PS technique. Based on quality of bone and surgeon preference, choose from one of the following techniques: Use the Revision PS Femoral Trial as the cutting device (with or without wedges). Use the PS instrumentation without wedge augmentation options. Use the PS instrumentation with wedge augmentation options. STEPS: A. Open the femoral and tibial canals with the appropriate Femoral Drill. Ream the femoral and tibial canals with the appropriate Long Stem Reamer (typically starting with the 10 mm reamer). Progressively ream canals by increasing the reamer diameter 1 mm at a time until the desired stability is obtained (Figure 1). Stopping on an odd size reamer is ideal. Reamer depth is determined by using the marks on the shaft of the reamer (100 mm, 150 mm, 200 mm). Note: If the reamer diameter is 13 mm or less, the Long Stem Drill must be used to prepare for a 10 mm or 12 mm Long Stem Implant. B. Place the Revision Distal Cutting Block over the reamer in the femur. Establish approximate external rotation of the Cutting Block by rotating the Cutting Block until the two bone spike ears are in line with the epicondylar axis. Tap the block to ensure it rests firmly on the bone and tighten the Valgus Module. Pin the Block to bone (Figure 2). Set the resection level of the distal slot by loosening the thumb screws and adjusting to the appropriate resection level. Tighten the screws. Proceed with distal resection to achieve a flat distal surface. Assess bone stock to determine which of the following techniques will be indicated for the Revision PS procedure Long Stem Drill Femoral 3/8" Drill mm Long Stem Reamer Revision Distal Cutting Block º Valgus Module 42

43 Figure 1 Figure 2 43
44 R EVISION POSTERIOR STABILIZED If using the Revision PS Femoral Trial as the cutting device for the procedure: C. Assemble the PS Femoral Trial. Place the Revision Femoral Trial Module with taper (left or right indicated) into the appropriate size trial and tighten both of the module lugs with an implant screw driver. Attach the Long Stem Trial and Coupler to the Femoral Trial Taper (Figure 1). Always use one size smaller diameter Long Stem Trial than the reamed canal if the canal was reamed to an odd size. Impact on the end of the Long Stem to secure morse taper lock. Place the PS Femoral Trial onto the distal femur (Figure 2). Do not directly impact the trial on the anteromedial or anterolateral flanges. Impacting these areas could deform the anterior cutting slots. D. Align the epicondylar axis of the PS Femoral Trial with the epicondyles of the femur. Impact the femoral trial in the usual manner. As the femoral trial is being impacted, the posterior condyles, PS Housing, and anterior surface of the femur are being resected. The Femoral Trial Module has cutting walls which will prepare for the PS Housing. Remove any bone fragments from the PS Housing using an osteotome (Figure 3). Leave trials in place to assess range of motion with the PS Articular Insert. E. After evaluating the range of motion with femoral and tibial trials, implant the PS Femoral Implant with long stem on the distal femur. Long stems should be 1 mm larger than reamed femoral canal if the canal was reamed to an odd size. Implant the tibial and the PS Articular Insert. Assess range of motion for the final implants Femoral Trial Module with Taper Long Stem Trial 150 mm x 10 mm Stem Trial Coupler 7º PS Articular Insert 44


45 Figure 2 Figure 1 Figure 3 45
46 R EVISION POSTERIOR STABILIZED If using the PS instrumentation without wedge augmentation: C. Impact the appropriate size Long Stem Trial and coupler onto the PS Taper Attachment. Place the Taper Attachment onto the PS Positioner (Figure 1) and tighten down the set screw. Make certain that the PS Taper Attachment is correctly oriented for the left or right knee. Establish the correct external rotation by rotating the Positioner relative to the epicondylar axis. Predrill and pin the Positioner into place with bone spikes. D. Remove the PS Taper Attachment with the Long Stem Trial through the top of the Positioner (Figure 2). Make sure that the Positioner is rigidly attached to the femur. E. With the thumb screws on the PS Positioner loose, place the PS Box Reamer Guide (Figure 3) into the Positioner, then tighten the thumb screw to firmly hold the reamer guide in place. Proceed to ream through both holes with the PS Box Reamer (Figure 4). This will prepare the majority of the femoral housing area Long Stem Trial 150 mm x 10 mm PS Taper Attachment PS Positioner PS Box Reamer Guide PS Box Reamer 46

47 Figure 1 Figure 2 Figure 3 Figure 4 47
48 REVISION POSTERIOR STABILIZED F. Loosen the Positioner thumb screw and remove the Reamer Guide. Place the PS Box Chisel Guide into the Positioner and tighten the thumb screw firmly to hold the Chisel Guide in place. Attach the Fin Punch Handle to the PS Box Chisel and impact the PS Box Chisel (Figure 5) through the Box Chisel Guide. This will complete the bone resection for the PS femoral housing. G. Remove the Positioner and assemble the PS Femoral Trial. Place the Revision Femoral Trial Module with taper (left or right indicated) into the appropriate size trial and tighten one of the module lugs with an implant screwdriver. Attach the Long Stem Trial and Coupler to the Femoral Trial taper (Figure 6). Always use one size smaller diameter Long Stem Trial than the reamed canal if the canal was reamed to an odd size. Impact on the end of the Long Stem to secure the morse taper lock. Place the PS Femoral Trial onto the distal femur (Figure 7). Do not directly impact on the anteromedial or anteriolateral flanges. Impacting these areas could deform the anterior cutting slots. H. After evaluating the range of motion with femoral and tibial trials, implant the PS Femoral Implant with Long Stem on the distal femur. Long Stems should be 1 mm larger than reamed femoral canal if the canal was reamed to an odd size. Implant the Tibial and the PS Articular Insert. Assess range of motion for the final implants PS Box Chisel Guide PS Femoral Trial Fin Punch Handle PS Box Chisel 48
49 Figure 5 Figure 7 Figure 6 49
50 R EVISION POSTERIOR STABILIZED 50 If using the PS instrumentation with wedge augmentation options: C. Attach the Long Stem Trial to the Stem Trial Coupler. Always use one size smaller diameter Long Stem Trial than the reamed canal if the canal was reamed to an odd size, then impact onto the Revision Femoral Trial (Figure 1). Drive the Revision Femoral Trial onto the femur using the Femoral Impactor. Before driving trial into place, make certain it is in the correct external rotation by rotating the trial until the epicondylar axis line is parallel to the imaginary line between the epicondyles of the femur. The sharp cutting edges of the posterior condyles and anterior aspect of the femoral trial will shave any prominent bone. Once seated, proceed with resection of distal bone for appropriate wedge placement through the wedge resection slots provided. Remove Femoral Trial and attach the appropriate thickness Wedge Spacers to the undersurface of the PS Positioner (Figure 2). D. Remove the Long Stem Trial and Coupler from the Revision Femoral Trial and impact onto the PS Taper Attachment. Place the PS Taper Attachment onto the PS Positioner (Figure 3) and tighten down the set screw. Make certain that the PS Taper Attachment is correctly oriented for the left or right knee. Establish the correct external rotation by rotating the positioner relative the the epicondylar axis. Predrill and pin the Positioner into place with bone spikes. E. Remove the PS Taper Attachment with Long Stem Trial through the top of the Positioner (Figure 4). Make sure that the Positioner is rigidly attached to the femur Long Stem Trial 150 mm x 10 mm Stem Trial Coupler 7º Revision Femoral Trial Size 4 Left Femoral Impactor Wedge Spacers PS Positioner PS Taper Attachment PS Femoral Trial



51 Figure 2 Figure 1 Figure 3 Figure 4 51
52 REVISION POSTERIOR STABILIZED F. With the thumb screws on the PS Positioner loose, place the PS Box Reamer Guide (Figure 5) into the positioner, then tighten the thumb screw to firmly hold the Reamer Guide in place. Proceed to ream through both holes with the PS Box Reamer (Figure 6). This will prepare the majority of the femoral housing area. G. Loosen the Positioner thumb screw and remove the Reamer Guide. Place the PS Box Chisel Guide into the Positioner and tighten the thumb screw firmly to hold the Chisel Guide in place. Attach the Fin Punch Handle to the PS Box Chisel and impact the PS Box Chisel (Figure 7) through the PS Box Chisel Guide. Remove any bone fragments from the PS Housing using an osteotome. This will complete the bone resection for the PS Femoral Housing. H. Remove the Positioner and assemble the PS Femoral Trial. Place the Revision Femoral Trial Module with taper (left or right indicated) into the appropriate size Trial and tighten either a lug or wedge trial with an implant screwdriver (Figure 8). Attach the Long Stem Trial and Coupler to the Femoral Trial Taper. Impact on the end of the Long Stem to secure the morse taper lock. Place the PS Femoral Trial onto the distal femur (Figure 9). Do not directly impact the trial on the anteromedial or anterolateral flanges. Impacting these areas could deform the anterior cutting slots. I. After evaluating the range of motion with Femoral and Tibial Trials, implant the PS Femoral Implant with Long Stem on the distal femur. Long Stems should be 1 mm larger than reamed femoral canal if the canal was reamed to an odd size. Implant the Tibial and PS Articular Insert. Assess range of motion for the final implants PS Box Reamer Guide PS Box Reamer PS Box Chisel Guide Fin Punch Handle PS Femoral Trial PS Articular Insert 52


53 Figure 5 Figure 6 Figure 7 Figure 9 Figure 8 53
54 54
55 Appendix A Optional Posterior Referencing Technique & Tibial EM Alignment 55 A P P E N D I X A O P T I O N A L P O S T E R I O R R E F E R E N C I N G T E C H N I Q U E & T I B I A L E M A L I G N M E N T
56 S T A G E 2 A FEMORAL RESECTION (POSTERIOR REFERENCING) Three external rotation guides (Neutral, 3 Left, 3 Right) are available to attach to the femoral cutting blocks if posterior referencing of the femur is desired. The Anterior Stylus is not used for posterior referencing. STEPS: A. Loosely attach the appropriate Valgus Module into the center of the Femoral Cutting Block by tightening the thumb screw on the Module. If resecting the right knee, Right Up will face anteriorly. Left Up will face anteriorly if resecting the left knee. Place the Femoral Cutting Block over the 8 mm Reamer Rod. Advance the Cutting Block until it is firmly seated against the distal femur. It may be necessary to tap the top of the Valgus Module with a mallet to assure the Cutting Block is resting on the distal femur. B. Determine whether neutral or 3 of external rotation is desired; attach the appropriate External Rotation Guide to the posterior side of the Femoral Cutting Block using the Quick Release Handle (Figure 33). C. Orient the Femoral Cutting Block until the posterior paddles firmly seat on the posterior condyles. Tighten the Valgus Module and spike the Femoral Cutting Block into place.* Remove the External Rotation Guide using the Quick Release Handle. Proceed with femoral resection as described in Stage 2 of the Primary Technique. *Note: This was described in Step C on page º Valgus Module Femoral Cutting Block, Size mm Reamer Rod External Rotation Guide (Neutral) Quick Release Handle 56

57 External Rotation Guide Figure 1 57
58 S T A G E 3 A ROXIMAL TIBIAL RESECTION (EM ALIGNMENT) PRequired instruments include the Ankle Clamp and Alignment Sleeve, the Tibial Cutting Block (Neutral or 4 slope), Tibial Alignment Assembly, EM Alignment Spike, and the Proximal Rod. The choice of a neutral or 4 cutting block will depend on the desired amount of posterior slope of the proximal tibia. STEPS: A. The EM Alignment Spike is impacted into the tibial spine just posterior to the anterior cruciate ligament insertion point. Place entire assembly over the EM Alignment Spike and around ankle to secure in place (Figure 2). B. Set the desired resection level by adjusting the Tibial Stylus on the Tibial Alignment Assembly. Usually, 8 mm-10 mm of bone is resected referencing from the unaffected side of the tibial plateau. The Assembly is now placed over the EM Alignment Spike (Figure 3). C. Lower the assembly until the Stylus touches the most central point of the highest or good side of the tibial plateau. Tighten the screw against the 8 mm Reamer Rod. Move the Tibial Cutting Block until it contacts the anterior tibial cortex. The sliding screw is then tightened. D. The Tibial Cutting Block is now in the proper location to remove the desired amount of bone established in Step B. Spike the Cutting Block to the bone and remove the EM spike and Tibial Stylus. Note: If using the 4 slope Tibial Cutting Block, centralize the hash marks on the tibial block over the medial third of the tibial tubercle before spiking to bone. E. Resect the proximal tibia through the slotted block using a Profix Sawblade EM Alignment Spike Tibial Alignment Assembly Tibial Cutting Block 0º Ankle Clamp & Alignment Sleeve 58

59 Figure 2 Figure 3 59
60 60
61 Appendix B Additional Bone Resection Procedure A P P E N D I X B A D D I T I O N A L B O N E R E S E C T I O N P R O C E D U R E 61
62 T E C H N I Q U E NITIAL 2.5 MM DISTAL RESECTION 1 IIn the event of a flexion contracture or the necessity to remove 2.5 mm of distal femoral bone as the initial cut (in addition to a full distal cut to be made later), this technique is recommended. The required instruments include the Femoral Cutting Block, Valgus Module, Provisional Distal Cutting Block, Distal Cutting Block, and 8 mm Reamer Rod. STEPS: A. Using the T-Handle Quick Connect, insert the 8 mm Reamer Rod and place the Femoral Sizer over the rod. Size the femur using the standard Profix technique. Remove the Sizer and slide the Femoral Cutting Block over the 8 mm Reamer Rod. Leave the Valgus Module loose. B. Attach the Provisional Distal Cutting Block to the anterior side of the Femoral Cutting Block. Establish approximate external rotation, tighten Valgus Module, and spike the Femoral Cutting Block to the bone. C. Make 2.5 mm distal resection through the slot on the Provisional Distal Cutting Block (Figure 1). D. Remove the Provisional Distal Cutting Block and spikes. Place the Femoral Cutting Block against the cut distal surface. Using anterior or posterior referencing, establish external rotation and tighten the Valgus Module. Spike the Femoral Cutting Block into place and proceed with femoral resection (Anterior, Anterior Chamfer, Posterior, Posterior Chamfer, and Distal cuts) using the appropriate size Distal Cutting Block (Figures 2 and 3) T-Handle Quick Connect mm Reamer Rod (Standard) Femoral Sizer Femoral Cutting Block, Size º Valgus Module Provisional Distal Cutting Block Distal Cutting Block, Size 4 62


63 Figure 1 1. Anterior 2. Anterior Chamfer 3. Posterior 4. Posterior Chamfer Figure 2 Figure 3 63
64 T E C H N I Q U E 2 DDITIONAL DISTAL BONE RESECTION AIn the event of a flexion contracture after all femoral cuts have been made, this technique is recommended. This technique will remove either a full distal thickness or an additional 3.3 mm to 6.6 mm of distal bone depending on the size of the femoral block desired. The required instruments include the Femoral Cutting Block, Distal Cutting Block, Valgus Module, Cutting Block Alignment Plate, and Half Distal Spacer Gauge. A chart is provided for the amount of additional resection for each size femoral block. STEPS: A. Insert the 8 mm Reamer Rod into the femoral canal and place the Femoral Cutting Block on the resected femoral bone. Leave the Valgus Module loose. B. Insert the Cutting Block Alignment Plate into the anterior slots of the Femoral Cutting Block (Figure 4). C. Confirm that the Femoral Cutting Block rests on the cut distal surface. Slide the block posteriorly until the Cutting Block Alignment Plate rests against the cut anterior cortex. Tighten the Valgus Module. If full distal resection is desired, spike the Femoral Cutting Block to the bone and proceed with all cuts listed in Step E. D. If approximately half of the normal distal thickness is desired, insert the Half Distal Spacer Gauge into the open slots of the Cutting Block Alignment Plate. The Half Distal Spacer Gauge should now rest between the Cutting Block and the distal femur. This will raise the femoral block 4 mm off the distal surface (Figure 5). E. Spike the Femoral Cutting Block into place. Remove the Half Distal Spacer Gauge and the Cutting Block Alignment Plate. Proceed with all femoral cuts in the suggested order (Figure 6). Make the distal cuts using the same size Distal Cutting Block as Femoral Cutting Block (Figure 7). Size Amount of Additional Resection mm mm mm mm mm mm mm mm Reamer Rod Femoral Cutting Block, Size º Valgus Module Cutting Block Alignment Plate Half Distal Spacer Gauge Distal Cutting Block, Size 4 64
65 Figure 4 Figure 5 1. Anterior 2. Anterior Chamfer 3. Posterior 4. Posterior Chamfer Figure 6 Figure 7 65
66 T E C H N I Q U E 3 OVING DOWN ONE FEMORAL SIZE MIf it is desired to move down one femoral size (i.e., Size 5 to Size 4) after all femoral cuts are made, the required instruments include the smaller Femoral Cutting Block, Distal Cutting Block, Valgus Module, and the Cutting Block Alignment Plate. STEPS: A. Insert the 8 mm Reamer Rod into the femoral canal and slide the next smaller size Femoral Cutting Block over it. Leave the Valgus Module loose. B. Insert the Cutting Block Alignment Plate into the anterior slots of the Femoral Cutting Block and slide the block posteriorly until the Alignment Plate is flush with the anterior cortex. Tighten the Valgus Module (Figure 8). C. Remove the Cutting Block Alignment Plate and insert into the Anterior Chamfer slot. Raise the block until the Cutting Block Alignment Plate rests on the Anterior Chamfer (Figure 9). Spike the femoral block to the bone (Figure 10) and remove the Cutting Block Alignment Plate. D. Perform all cuts including distal (Figures 11 and 12), as described in Step E. on page mm Reamer Rod Femoral Cutting Block, Size º Valgus Module Cutting Block Alignment Plate Distal Cutting Block, Size 4 66


67 Figure 8 Figure 9 Figure Anterior 2. Anterior Chamfer 3. Posterior 4. Posterior Chamfer 2 Figure Figure 11 67
68 IMPORTANT MEDICAL INFORMATION Warnings and Precautions SMITH & NEPHEW KNEE SYSTEMS For Cemented Use Only 68 MATERIALS Femoral components are cobalt chromium alloy (ASTM F75 and ISO 5832/4) or oxidized zirconium alloy. Conversion modules are cobalt chromium alloy (ASTM F75 and ISO 5832/4). Patellar components, all-polyethylene tibial components, tibial articular inserts, and Flex-Lok pegs are ultra-high molecular weight polyethylene (ASTM 648). Components that are made of only polyethylene may include x-ray marking wire made of stainless steel (ASTM F138 and ISO 5842/1) or cobalt chromium (ASTM F90). Tibia trays, patellar bases, tibial and femoral wedges, tibial and femoral stems, screws, and pegs are titanium 6A1-4V alloy (ISO 5832/3) or cobalt chromium alloy (ASTM F75 or ISO 5832/4). Porous coated cobalt chromium and titanium components feature a porous coating of cobalt chromium beads (ASTM F75 and ISO 5832/4) and unalloyed titanium beads (ASTM F67 and ISO 5832/2), respectively. The component material is provided on the outside carton label. Each total knee system is designed as a system and does not allow the substitution of components from other systems. All implantable devices are for single use. Some of the alloys needed to produce orthopedic implants contain some metallic components that may be carcinogenic in tissue cultures or intact organism under very unique circumstances. Questions have been raised in the scientific literature as to whether or not these alloys may be carcinogenic in implant recipients. Studies conducted to evaluate this issue have not identified convincing evidence of such phenomenon, in spite of the millions of implants un use. INDICATIONS, CONTRAINDICATIONS, AND ADVERSE EFFECTS The general principles of good patient selection and sound surgical judgment apply to the total knee procedure. Preoperative planning and meticulous surgical technique are essential to achieve optimum results. Considerations of anatomic loading, soft tissue condition, and component placement are critical to minimize a variety of postoperative complications. Indications for Total Knee Replacement 1. Rheumatoid arthritis. 2. Posttraumatic arthritis, osteoarthritis, or degenerative arthritis in older patients whose age, weight, and activity level are compatible with an adequate long-term result. 3. Failed osteotomies, unicompartmental replacement, or total knee replacement. 4. Posterior- stabilized knee systems and systems with a deep articular surface are designed for use in patients in primary and revision surgery, where the anterior and posterior cruciate ligaments are incompetent and the collateral ligaments remain intact. 5. Constrained knee systems are designed for use in patients in primary and revision surgery, where the posterior cruciate ligament and one or both of the collateral ligaments (i.e. medial collateral and/or lateral collateral ligament) are absent or incompetent. 6. The Tricon -M and Tricon-P Total Knee System can be implanted with or without cement; the Flex-Lok pegs are driven into cancellous bone to secure the components in place. Contraindications for Total Knee Replacement 1. Cases where there is poor bone stock which would make the procedure unjustifiable. 2. Active, local infection or previous intra-articular infections. 3. Mental or neurologic conditions that tend to preempt the patient s ability or willingness to restrict activities. 4. Neuropathic joint (Charcot). 5. Conditions that tend to place increased loads on implants such as age, weight, and activity level, which are incompatible with a satisfactory long-term result. 6. Collateral ligament insufficiency (except in cases where a constrained knee system is indicated and used). 7. Cementless applications for the Tricon-M and Tricon-P Total Knee Systems is contraindicated with non-correctable ligamentous laxity of the affected knee. 8. Skeletal immaturity. 9. Use of a supracondylar nail through intercondylar notch of Profix primary femoral components. 10. Use of slotted tibial stems without adequate bony support. Contraindications for Unicompartmental Knee Replacement: The contraindications for Unicompartmental Knee Replacement include all of the contraindications listed for Total Knee Replacement and also inflammatory arthritis, such as rheumatoid arthritis, gout, lupus, etc. Possible Adverse Effects: 1. Wear of the polyethylene articulating surfaces of knee replacement components has been reported following total knee replacement. Higher rates of wear may be initiated by particles of cement, metal, or other debris which can cause abrasion of the articulating surfaces. Higher rates of wear may shorten the useful life of the prosthesis, and lead to early revision surgery to replace the worn prosthetic component. 2. With all joint replacements, asymptomatic, localized, progressive bone resorption (osteolysis) may occur around the prosthetic components as a consequence of foreign-body reaction to particulate wear debris. Particles are generated by interaction between components, as well as between the components and bone, primarily through wear mechanisms of adhesion, abrasion, and fatigue. Secondarily, particles may also be generated by third-body wear. Osteolysis can lead to future complications necessitating the removal and replacement of prosthetic components. See Important Physician Information section for more information. 3. Loosening, bending, cracking, or fracture of implant components. Fracture of the implant can occur as a result of trauma, strenuous activity, improper alignment, or duration of service. 4. Dislocation, subluxation, excessive rotation, flexion contracture, decreased range of motion, lengthening or shortening of the leg, looseness of components, unusual stress concentrations, and extraneous bone can result from trauma, improper implant selection, improper implant positioning, improper fixation, and/or migration of the components. Muscle and fibrous tissue laxity can also contribute to these conditions. 5. Tibia, femur, or patellar fractures. 6. Acute postsurgical wound infection, late deep wound sepsis and/or low-grade synovitis. 7. Peripheral neuropathies have been reported following total joint surgery. Subclinical nerve damage has been reported, and may be a result of surgical trauma. Temporary or permanent nerve damage can result in pain or numbness of the affected limb 8. Wound hematoma, thromboembolic diseases including venous thrombosis, pulmonary embolus, or myocardial infarction. 9. Myositis ossificans. Periarticular calcification or ossification, with or without impediment to joint mobility. Periarticular calcification can cause decreased range of motion. 10. Skin sloughs or delayed wound healing. 11. Although rare, metal sensitivity or allergic reactions in patients following joint replacement have been reported. Implantation of foreign material in tissues can result in histological reactions involving macrophages and fibroblasts. 12. Damage to blood vessels. 13. Varus-valgus deformity. WARNINGS AND PRECAUTIONS The patient should be warned of surgical risks, and made aware of possible adverse effects. The patient should be warned that the device does not replace normal healthy bone, and that the implant can break or become damaged as a result of strenuous activity or trauma, and has a finite expected service life and may need to be replaced in the future. Preoperative: 1. Use care in handling and storing of implant components. Cutting, bending, or scratching the surfaces of components can significantly reduce the strength, fatigue resistance, and/or wear characteristics of the implant system. These in turn may induce internal stresses that are not obvious to the eye and may lead to fracture of the component. Do not allow the porous surfaces to come in contact with cloth or other fiber releasing materials.
69 2. Surgical information is available upon request. The surgeon should be familiar with the technique. 3. An adequate inventory of implant sizes should be available at the time of surgery. 4. Intraoperative fracture or braking of instruments can occur. Instruments which have experienced extensive use or excessive force are susceptible to fracture. Instruments should be examined for wear and damage prior to surgery. Intraoperative: 1. The correct selection of the implant is extremely important. The appropriate type and size should be selected for patients with consideration of anatomical and biomechanical factors such as patient age and activity levels, weight, bone and muscle conditions, etc. Generally, the largest cross-section component which will allow adequate bone support to be maintained is preferred. Failure to use the optimum size component may result in loosening, bending cracking, or fracture of the component and/or bone. 2. Modular components must be assembled securely to prevent dissassociation. Avoid repeated assembly and disassembly of the modular components which could compromise a critical locking action of the components. Surgical debris must be cleaned from components before assembly. Debris inhibits the proper fit and locking of modular components which may lead to early failure of the procedure. 3. Care is to be taken to assure complete support of all parts of the device embedded in bone cement to prevent stress concentration which may lead to failure of the procedure. During curing of cement, care should be taken to prevent movement of the implant components. 4. Fixation screws, when used, should be fully seated to assure stable fixation, and to avoid interference with the proper seating of components. Use only screws recommended by the manufacturer for the specific prosthesis to avoid improper fit, and to avoid improper mixing of metals. 5. Prior to closure, the surgical site should be thoroughly cleaned of bone chips, extraneous cement, ectopic bone, etc. Foreign particles at the metal-plastic interface may cause excessive wear and/or friction. 6. Posterior stabilized knee systems, constrained knee systems, and systems with a deep articular surface should not be utilized without significant adjunctive fixation (stems, screws, etc.). 7. It is essential that the patient s bone stock be of sufficient quality to support the plastic and metallic fixation pegs in the Tricon-M and Tricon-P Total Knee Systems. 8. An implant should never be reused. While it may appear undamaged, imperfection may exist which would reduce the service life of the implant. 9. Use the Richards Torque Wrench to secure the distal femoral wedges and the conversion modules to the GENESIS femoral component. The femoral lugs should be torqued to 70 in-lbs. Postoperative: 1. Postoperative patient care, and directions and warnings to patients by physicians, are extremely important. Protected weight bearing with external support is recommended for a period of time to allow healing. 2. Use extreme care in patient handling. 3. Postoperative therapy should be structured to prevent excessive loading of the operative knee and to encourage bone healing. 4. Periodic, long-term follow-up is recommended to monitor the position and state of the prosthetic components, as well as the condition of the adjoining bone. Important Physician Information Bone resorption is a natural consequence of total joint arthroplasty due to changes in bone remodeling patterns. Bone remodeling is mediated by the changes in stress distribution caused by implantation. Extensive resorption around the prosthesis leads to implant loosening and failure. Progressive bone resorption due to reasons other than stress shielding or infection has been termed osteolysis. It is generally agreed that osteolysis is the result of localized foreign-body reaction to particulate debris generated by cement, metal, ultra-high molecular weight polyethylene (UHMWPE), and ceramic. Regarding the etiology, it has been hypothesized that particulate debris generated by the components of a prosthesis migrate into the synovial cavity and the boneimplant interface, where they recruit macrophages and stimulate phagocytic action. The degree of recruitment is determined by the size, distribution, and amount of particulate debris (rate of debris generation). The phagocytic action results in the release of cytokines and intercellular mediators (IL-1, 2 PE2) which encourages osteoclastic bone resorption. Clinical and basic research is continuing in order to provide scientific basis for the causes of this phenomenon and potential ways to reduce its occurrence. Osteolysis can be asymptomatic and therefore routine periodic radiographic examination is vital to prevent any serious future complication. Presence of local lesions which are progressive may necessitate replacement of the prosthetic component(s). Packaging and Labeling: Knee implants are sterilized products and should only be accepted if received by the hospital or surgeon with the factory packaging and labeling intact. If the sterile barrier has been broken, refer to the Resterilization section below. STERILIZATION All metal components have been sterilized by a minimum of 25 kilograys of gamma irradiation. Plastic components have been sterilized by ethylene oxide gas. All components are supplied in protective trays. Inspect packages for punctures or other damage prior to surgery. RESTERILIZATION Metal Components: Metal components may be resterilized, if necessary, by steam autoclaving in appropriate protective wrapping after the removal of all the original packaging and labeling. Protect prosthesis, particularly mating surfaces, from contact with metal or other hard objects. The following process parameters are recommended for these devices: Prevacuum cycle, 4 minutes at 132 C to 135 C, followed by 20 minutes of drying time. If porous-coated implants are inadvertently contaminated, return the unsoiled prosthesis to Richards for resterilization. DO NOT RESTERIL- IZE porous-coated implants. The porous-coating requires special cleaning procedures. Plastic Components: Plastic components may be resterilized by ethylene oxide gas using the following procedures: Max. Exposure Sterilant Temp. Humidity Pressure Concentration Time 10% EtO 130 F 40-60% 28 PSIA mg/l 120 minutes 90% HCFC 10% EtO 100 F 40-60% 28 PSIA mg/l 6 hours 90% HCFC 100% EtO 131 F 30-60% 10 PSIA 736 mg/l 80 minutes INFORMATION For further information, please contact Customer Service at for calls within the continental USA an (901) for all international calls Rev. A 01/97 69
70 70 Notes
71 71
72 Smith & Nephew, Inc Brooks Road Memphis, TN U.S.A. (901) For information: For orders and order inquiries: Profix, Tricon, and FlexLok are registered trademarks of Smith & Nephew, Inc Smith & Nephew, Inc. 01/

73 Surgical Technique Profix Total Knee System
Distal Cut First Femoral Preparation
 Surgical Technique Distal Cut First Femoral Preparation Primary Total Knee Arthroplasty LEGION Total Knee System Femoral preparation Contents Introduction...3 DCF femoral highlights...4 Preoperative planning...6
Surgical Technique Distal Cut First Femoral Preparation Primary Total Knee Arthroplasty LEGION Total Knee System Femoral preparation Contents Introduction...3 DCF femoral highlights...4 Preoperative planning...6
Surgical Technique. VISIONAIRE Disposable Instruments for the LEGION Total Knee System
 Surgical Technique VISIONAIRE Disposable Instruments for the LEGION Total Knee System VISIONAIRE and LEGION Disposable instrument technique* Note: All disposable instruments are interchangeable with the
Surgical Technique VISIONAIRE Disposable Instruments for the LEGION Total Knee System VISIONAIRE and LEGION Disposable instrument technique* Note: All disposable instruments are interchangeable with the
ANATOMIC SURGICAL TECHNIQUE. 5 in 1. Conventional instrumentation 07/11/2013
 ANATOMIC SURGICAL TECHNIQUE 5 in 1 Conventional instrumentation PRO.GB.933/1.0 Octobre 2013 2 Tibial step 3 Intramedullary technique - Based on the preoperative plan, drill the medullary canal with the
ANATOMIC SURGICAL TECHNIQUE 5 in 1 Conventional instrumentation PRO.GB.933/1.0 Octobre 2013 2 Tibial step 3 Intramedullary technique - Based on the preoperative plan, drill the medullary canal with the
Intramedullary Tibial Preparation
 Surgical Technique Intramedullary Tibial Preparation Primary Total Knee Arthroplasty LEGION Total Knee System Intramedullary tibial preparation Contents Introduction...2 IM tibial highlights...3 Preoperative
Surgical Technique Intramedullary Tibial Preparation Primary Total Knee Arthroplasty LEGION Total Knee System Intramedullary tibial preparation Contents Introduction...2 IM tibial highlights...3 Preoperative
TOTAL KNEE ARTHROPLASTY SYSTEM
 SURGICAL TECHNIQUE TOTAL KNEE ARTHROPLASTY SYSTEM 90-SRK-700000 B.0 0 Contents 1. Implant Sizing 2. Surgical Technique a. Incision and Exposure b. Distal Femoral Resection c. Tibial Resection d. Femoral
SURGICAL TECHNIQUE TOTAL KNEE ARTHROPLASTY SYSTEM 90-SRK-700000 B.0 0 Contents 1. Implant Sizing 2. Surgical Technique a. Incision and Exposure b. Distal Femoral Resection c. Tibial Resection d. Femoral
Surgical Technique. VISIONAIRE FastPak Instruments for the LEGION Total Knee System
 Surgical Technique VISIONAIRE FastPak Instruments for the LEGION Total Knee System VISIONAIRE FastPak for LEGION Instrument Technique* Nota Bene The technique description herein is made available to the
Surgical Technique VISIONAIRE FastPak Instruments for the LEGION Total Knee System VISIONAIRE FastPak for LEGION Instrument Technique* Nota Bene The technique description herein is made available to the
Extramedullary Tibial Preparation
 Surgical Technique Extramedullary Tibial Preparation Primary Total Knee Arthroplasty LEGION Total Knee System Extramedullary tibial preparation Contents Introduction...2 EM tibial highlights...3 Preoperative
Surgical Technique Extramedullary Tibial Preparation Primary Total Knee Arthroplasty LEGION Total Knee System Extramedullary tibial preparation Contents Introduction...2 EM tibial highlights...3 Preoperative
Triathlon Knee System
 Triathlon Knee System Express Instruments Surgical Protocol Posterior Stabilized & Cruciate Retaining TriathlonKneeSystem Express Instruments Surgical Protocol Acknowledgments..........................................................2
Triathlon Knee System Express Instruments Surgical Protocol Posterior Stabilized & Cruciate Retaining TriathlonKneeSystem Express Instruments Surgical Protocol Acknowledgments..........................................................2
Anterior Cut First Surgical Technique
 Anterior Cut First Surgical Technique GENESIS II Anterior Cut First Surgical Technique Table of Contents Introduction....................................... 2 Preop Planning....................................
Anterior Cut First Surgical Technique GENESIS II Anterior Cut First Surgical Technique Table of Contents Introduction....................................... 2 Preop Planning....................................
Zimmer NexGen MIS Tibial Component. Cemented Surgical Technique IMAGE TO COME
 Zimmer NexGen MIS Tibial Component Cemented Surgical Technique IMAGE TO COME Zimmer NexGen MIS Tibial Component Cemented Surgical Technique 1 Zimmer NexGen MIS Tibial Component Cemented Surgical Technique
Zimmer NexGen MIS Tibial Component Cemented Surgical Technique IMAGE TO COME Zimmer NexGen MIS Tibial Component Cemented Surgical Technique 1 Zimmer NexGen MIS Tibial Component Cemented Surgical Technique
TRK REVISION KNEE Surgical Technique
 1 TRK REVISION KNEE Surgical Technique 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. INTERCONDYLAR RESECTION...... page FEMORAL STEM...... page NON CEMENTED FEMORAL STEM...... page TRIAL FEMORAL COMPONENTS...... page
1 TRK REVISION KNEE Surgical Technique 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. INTERCONDYLAR RESECTION...... page FEMORAL STEM...... page NON CEMENTED FEMORAL STEM...... page TRIAL FEMORAL COMPONENTS...... page
Revolution. Unicompartmental Knee System
 Revolution Unicompartmental Knee System While Total Knee Arthroplasty (TKA) is one of the most predictable procedures in orthopedic surgery, many patients undergoing TKA are in fact excellent candidates
Revolution Unicompartmental Knee System While Total Knee Arthroplasty (TKA) is one of the most predictable procedures in orthopedic surgery, many patients undergoing TKA are in fact excellent candidates
FLK167 02/08. Biomet UK Ltd Waterton Industrial Estate Bridgend, South Wales CF31 3XA, United Kingdom. Tel Fax:
 FLK167 02/08 Biomet UK Ltd Waterton Industrial Estate Bridgend, South Wales CF31 3XA, United Kingdom Tel. 01656 655221 Fax: 01656 645454 Premier Instrumentation CR or PS Surgical Technique Vanguard Premier
FLK167 02/08 Biomet UK Ltd Waterton Industrial Estate Bridgend, South Wales CF31 3XA, United Kingdom Tel. 01656 655221 Fax: 01656 645454 Premier Instrumentation CR or PS Surgical Technique Vanguard Premier
Knee. Surgical Protocol
 U2 TM PS CR Knee Surgical Protocol Table of Contents Pre-Operative Planning... Surgical Incision... 1 2 A. Femoral Preparation A.1. Pilot Hole... A.2. Femoral Valgus Angle Confirmation... A.3. Distal
U2 TM PS CR Knee Surgical Protocol Table of Contents Pre-Operative Planning... Surgical Incision... 1 2 A. Femoral Preparation A.1. Pilot Hole... A.2. Femoral Valgus Angle Confirmation... A.3. Distal
MIS Cemented Tibial Component
 MIS Cemented Tibial Component NexGen Complete Knee Solution Surgical Technique Table of Contents Surgical Exposure... 2 Finish the Tibia... 2 Position Based on Anatomic Landmarks... 3 Lateral Posterior
MIS Cemented Tibial Component NexGen Complete Knee Solution Surgical Technique Table of Contents Surgical Exposure... 2 Finish the Tibia... 2 Position Based on Anatomic Landmarks... 3 Lateral Posterior
U2 PSA. Revision Knee. Surgical Protocol
 U2 PSA TM Revision Knee Surgical Protocol Table of Contents 1 Component Removal... 1 2 Tibial Preparation... 1 2.1 Tibial Canal Preparation... 1 2.2 Proximal Tibial Resection... 2 2.3 Non Offset Tibial
U2 PSA TM Revision Knee Surgical Protocol Table of Contents 1 Component Removal... 1 2 Tibial Preparation... 1 2.1 Tibial Canal Preparation... 1 2.2 Proximal Tibial Resection... 2 2.3 Non Offset Tibial
NATURAL MOTION TECHNOLOGY SURGICAL TECHNIQUE. EMPOWR 3D Knee. EMPOWR PS Knee
 NATURAL MOTION TECHNOLOGY EMPOWR 3D Knee EMPOWR PS Knee SURGICAL TECHNIQUE Contents System Features.... 3 Indications and Contraindications.... 4 Surgical Snap Shot.... Preoperative Planning.... Surgical
NATURAL MOTION TECHNOLOGY EMPOWR 3D Knee EMPOWR PS Knee SURGICAL TECHNIQUE Contents System Features.... 3 Indications and Contraindications.... 4 Surgical Snap Shot.... Preoperative Planning.... Surgical
The information contained in this document is intended for healthcare professionals only.
 The information contained in this document is intended for healthcare professionals only. Triathlon Knee System Posterior Stabilized & Cruciate Retaining Table of Contents Acknowledgments.......................................................1
The information contained in this document is intended for healthcare professionals only. Triathlon Knee System Posterior Stabilized & Cruciate Retaining Table of Contents Acknowledgments.......................................................1
TRIAL COMPONENTS SURGICAL TECHNIQUE REAMING THE TIBIAL AND FEMORAL INTRAMEDULLARY CANAL
 Ref. no. 99.27.2TRIALS TRIAL COMPONENTS SURGICAL TECHNIQUE CLINICAL INDICATION This technique is indicated in the case of revisions with significant bone loss when minimal or any resection of bone is required.
Ref. no. 99.27.2TRIALS TRIAL COMPONENTS SURGICAL TECHNIQUE CLINICAL INDICATION This technique is indicated in the case of revisions with significant bone loss when minimal or any resection of bone is required.
Surgical Technique. Anterior Cut First Surgical Technique
 Surgical Technique Anterior Cut First Surgical Technique Introduction The GENESIS II Total Knee System has been designed to offer the orthopaedic surgeon solutions to address intraoperative situations.
Surgical Technique Anterior Cut First Surgical Technique Introduction The GENESIS II Total Knee System has been designed to offer the orthopaedic surgeon solutions to address intraoperative situations.
U2 KNEE SYSTEM. High Flexion Engineered
 U2 KNEE SYSTEM High Flexion Engineered TABLE OF CONTENTS Pre-Operative Planning...1 Surgical Incision...2 A. Femoral Preparation A.1. Pilot Hole...3 A.2. Femoral Valgus Angle Confirmation...4 A.3. Distal
U2 KNEE SYSTEM High Flexion Engineered TABLE OF CONTENTS Pre-Operative Planning...1 Surgical Incision...2 A. Femoral Preparation A.1. Pilot Hole...3 A.2. Femoral Valgus Angle Confirmation...4 A.3. Distal
1. Pre-Operative Planning Skin Incision and Arthrotomy
 Stage of Operation 1. Pre-Operative Planning --------------------------1 2. Skin Incision and Arthrotomy ------------------1 3. Femoral valgus angle confirmation ------------2 4. Distal Femur Cutting -----------------------------3
Stage of Operation 1. Pre-Operative Planning --------------------------1 2. Skin Incision and Arthrotomy ------------------1 3. Femoral valgus angle confirmation ------------2 4. Distal Femur Cutting -----------------------------3
Minimally Invasive TKA PROFIX Distal Cut First
 Surgical Technique INNOVATIONS IN MINIMALLY INVASIVE JOINT SURGERY Minimally Invasive TKA PROFIX Distal Cut First Instruments Femoral Sizing Guide 7151-3311 Femoral Anterior Referencing Stylus 7151-3313
Surgical Technique INNOVATIONS IN MINIMALLY INVASIVE JOINT SURGERY Minimally Invasive TKA PROFIX Distal Cut First Instruments Femoral Sizing Guide 7151-3311 Femoral Anterior Referencing Stylus 7151-3313
Triathlon TS Knee System. Surgical Protocol
 Triathlon TS Knee System Surgical Protocol Triathlon TS Knee System Surgical Protocol Table of Contents Acknowledgments..........................................................2 Exposure...................................................................4
Triathlon TS Knee System Surgical Protocol Triathlon TS Knee System Surgical Protocol Table of Contents Acknowledgments..........................................................2 Exposure...................................................................4
Knee. Surgical Protocol
 U2 TM PS CR Knee Surgical Protocol Table of Contents Pre-Operative Planning... Surgical Incision... 1 2 A. Femoral Preparation A.1. Pilot Hole... A.2. Femoral Valgus Angle Confirmation... A.3. Distal
U2 TM PS CR Knee Surgical Protocol Table of Contents Pre-Operative Planning... Surgical Incision... 1 2 A. Femoral Preparation A.1. Pilot Hole... A.2. Femoral Valgus Angle Confirmation... A.3. Distal
MRH Knee System Modular Peg Baseplate Surgical Protocol
 MRH Knee System Modular Peg Baseplate Surgical Protocol Using Monogram IM Revision Instruments 4 N 4 N Modular Rotating Hinge Knee System Using Monogram IM Revision Instruments Mr C R Howie FRCS Consultant
MRH Knee System Modular Peg Baseplate Surgical Protocol Using Monogram IM Revision Instruments 4 N 4 N Modular Rotating Hinge Knee System Using Monogram IM Revision Instruments Mr C R Howie FRCS Consultant
PRIMARY POROUS PATELLA WITH TRABECULAR METAL. Surgical Technique
 PRIMARY POROUS PATELLA WITH TRABECULAR METAL Surgical Technique 1 SURGICAL TECHNIQUE FOR NEXGEN PRIMARY POROUS PATELLA * WITH TRABECULAR METAL CONTENTS PREPARE THE PATELLA............... 2 Patella Reamer
PRIMARY POROUS PATELLA WITH TRABECULAR METAL Surgical Technique 1 SURGICAL TECHNIQUE FOR NEXGEN PRIMARY POROUS PATELLA * WITH TRABECULAR METAL CONTENTS PREPARE THE PATELLA............... 2 Patella Reamer
Resurfacing Distal Femur. Orthopaedic Salvage System
 Resurfacing Distal Femur Orthopaedic Salvage System Primary Arthroplasty OSS 3cm Resurfacing Distal Femur Distal Femoral Resection Drill and ream the distal femur in the following sequence: (Figure 1)
Resurfacing Distal Femur Orthopaedic Salvage System Primary Arthroplasty OSS 3cm Resurfacing Distal Femur Distal Femoral Resection Drill and ream the distal femur in the following sequence: (Figure 1)
ANTERIOR REFERENCE NEXGEN COMPLETE KNEE SOLUTION. Multi-Reference 4-in-1 Femoral Instrumentation Anterior Reference Surgical Technique
 ANTERIOR REFERENCE NEXGEN COMPLETE KNEE SOLUTION Multi-Reference 4-in-1 Femoral Instrumentation Anterior Reference Surgical Technique For NexGen Cruciate Retaining & Legacy Posterior Stabilized Knees INTRODUCTION
ANTERIOR REFERENCE NEXGEN COMPLETE KNEE SOLUTION Multi-Reference 4-in-1 Femoral Instrumentation Anterior Reference Surgical Technique For NexGen Cruciate Retaining & Legacy Posterior Stabilized Knees INTRODUCTION
The ACL-PCL Substituting Knee. BioFoam Tibial Bases. Surgical Technique For Cementless Tibial Fixation
 The CL-PCL Substituting Knee BioFoam Surgical Technique For Cementless Tibial Fixation Surgical techniques and instrument recommendations were provided by: Michael nderson, MD Milwaukee, WI G. Lynn Rasmussen,
The CL-PCL Substituting Knee BioFoam Surgical Technique For Cementless Tibial Fixation Surgical techniques and instrument recommendations were provided by: Michael nderson, MD Milwaukee, WI G. Lynn Rasmussen,
Total Knee Original System Primary Surgical Technique
 Surgical Procedure Total Knee Original System Primary Surgical Technique Where as a total hip replacement is primarily a bony operation, a total knee replacement is primarily a soft tissue operation. Excellent
Surgical Procedure Total Knee Original System Primary Surgical Technique Where as a total hip replacement is primarily a bony operation, a total knee replacement is primarily a soft tissue operation. Excellent
Zimmer NexGen Trabecular Metal Tibial Tray
 Zimmer NexGen Trabecular Metal Tibial Tray Surgical Technique Zimmer NexGen Trabecular Metal Tibial Tray Surgical Technique Give Bone A Solid Hold Zimmer NexGen Trabecular Metal Tibial Tray Surgical Technique
Zimmer NexGen Trabecular Metal Tibial Tray Surgical Technique Zimmer NexGen Trabecular Metal Tibial Tray Surgical Technique Give Bone A Solid Hold Zimmer NexGen Trabecular Metal Tibial Tray Surgical Technique
NexGen Cruciate Retaining (CR) and Revision Instrumentation. Surgical Technique
 and Revision Instrumentation. Surgical Technique") NexGen Cruciate Retaining (CR) and Revision Instrumentation Surgical Technique Table of Contents Introduction... 4 Revision Arthroplasty... 4 Multi-Reference 4-in-1 Instrumentation System MICRO-MILL Instrumentation
NexGen Cruciate Retaining (CR) and Revision Instrumentation Surgical Technique Table of Contents Introduction... 4 Revision Arthroplasty... 4 Multi-Reference 4-in-1 Instrumentation System MICRO-MILL Instrumentation
ELEOS Limb Salvage System
 ELEOS Limb Salvage System Surgical Technique Hinge Knee Replacement The ELEOS Limb Salvage System offers options for patients with significant bone loss due to cancer, trauma, or previous surgical procedures.
ELEOS Limb Salvage System Surgical Technique Hinge Knee Replacement The ELEOS Limb Salvage System offers options for patients with significant bone loss due to cancer, trauma, or previous surgical procedures.
OPERATIVE TECHNIQUE SKS Total Knee Replacement
 OPERATIVE TECHNIQUE SKS Total Knee Replacement Femoral preparation A40577 1 2 5 1: Alignment rod A30049 + A30124 2: Centromedullary rod A40224 4: T-handle A40232 6: Femoral measuring device A40411 + A40414
OPERATIVE TECHNIQUE SKS Total Knee Replacement Femoral preparation A40577 1 2 5 1: Alignment rod A30049 + A30124 2: Centromedullary rod A40224 4: T-handle A40232 6: Femoral measuring device A40411 + A40414
Zimmer NexGen RH Knee Primary/Revision. Surgical Technique
 Zimmer NexGen Primary/Revision Surgical Technique Zimmer NexGen Primary/Revision Surgical Technique INTRO Introduction The NexGen Rotating Hinge Knee () is designed for revision, difficult primary, and
Zimmer NexGen Primary/Revision Surgical Technique Zimmer NexGen Primary/Revision Surgical Technique INTRO Introduction The NexGen Rotating Hinge Knee () is designed for revision, difficult primary, and
A novel cementless option. Zimmer NexGen Trabecular Metal Primary Patella Surgical Technique
 A novel cementless option Zimmer NexGen Trabecular Metal Primary Patella Surgical Technique Zimmer Trabecular Metal Primary Patella 1 Zimmer NexGen Trabecular Metal Primary Patella Surgical Technique
A novel cementless option Zimmer NexGen Trabecular Metal Primary Patella Surgical Technique Zimmer Trabecular Metal Primary Patella 1 Zimmer NexGen Trabecular Metal Primary Patella Surgical Technique
POSTERIOR REFERENCE NEXGEN COMPLETE KNEE SOLUTION. Multi-Reference 4-in-1 Femoral Instrumentation Posterior Reference Surgical Technique
 POSTERIOR REFERENCE NEXGEN COMPLETE KNEE SOLUTION Multi-Reference 4-in-1 Femoral Instrumentation Posterior Reference Surgical Technique For NexGen Cruciate Retaining & Legacy Posterior Stabilized Knees
POSTERIOR REFERENCE NEXGEN COMPLETE KNEE SOLUTION Multi-Reference 4-in-1 Femoral Instrumentation Posterior Reference Surgical Technique For NexGen Cruciate Retaining & Legacy Posterior Stabilized Knees
ClassiQ. Scorpio. Anterior Referencing Surgical Protocol. Anterior Referencing. For use with Scorpio ClassiQ Instrument System
 Scorpio ClassiQ Anterior Referencing Surgical Protocol For use with Scorpio ClassiQ Instrument System For use with Scorpio ClassiQ Single Radius Total Knee System AR Anterior Referencing This document
Scorpio ClassiQ Anterior Referencing Surgical Protocol For use with Scorpio ClassiQ Instrument System For use with Scorpio ClassiQ Single Radius Total Knee System AR Anterior Referencing This document
Jan Victor, MD Orthopaedic Department AZ Sint-Lucas Brugge, Belgium
 Surgical Technique Contributing surgeons: Johan Bellemans, MD, PhD Head of Orthopaedic Department University Hospital Pellenberg Pellenberg, Belgium Jonathan Garino, MD University of Pennsylvania Philadelphia,
Surgical Technique Contributing surgeons: Johan Bellemans, MD, PhD Head of Orthopaedic Department University Hospital Pellenberg Pellenberg, Belgium Jonathan Garino, MD University of Pennsylvania Philadelphia,
Trabecular Metal Primary Patella
 Trabecular Metal Primary Patella NexGen Complete Knee Solution Surgical Technique Table of Contents Introduction... 2 Prepare the Patella... 2 Patella Reamer Technique... 3 Insetting Technique... 5 Universal
Trabecular Metal Primary Patella NexGen Complete Knee Solution Surgical Technique Table of Contents Introduction... 2 Prepare the Patella... 2 Patella Reamer Technique... 3 Insetting Technique... 5 Universal
AGC Total Knee System. Concise Surgical Technique Featuring EquiFlex Instrumentation
 AGC Total Knee System Concise Surgical Technique Featuring EquiFlex Instrumentation AGC TOTAL KNEE SYSTEM Concise Surgical Technique Instrumentation Disclaimer This brochure provides a description of the
AGC Total Knee System Concise Surgical Technique Featuring EquiFlex Instrumentation AGC TOTAL KNEE SYSTEM Concise Surgical Technique Instrumentation Disclaimer This brochure provides a description of the
S U R G I C A L T E C H N I Q U E David A. McQueen, MD Return to Menu
 S U R G I C A L T E C H N I Q U E David A. McQueen, MD TOTAL KNEE INSTRUMENTS Wichita Fusion Nail Introduction...1 Preoperative Planning...2 Surgical Technique...3-8 Wichita Fusion Nail Surgical Technique
S U R G I C A L T E C H N I Q U E David A. McQueen, MD TOTAL KNEE INSTRUMENTS Wichita Fusion Nail Introduction...1 Preoperative Planning...2 Surgical Technique...3-8 Wichita Fusion Nail Surgical Technique
Zimmer FuZion Instruments. Surgical Technique (Beta Version)
") Zimmer FuZion Surgical Technique (Beta Version) INTRO Surgical Technique Introduction Surgical goals during total knee arthroplasty (TKA) include establishment of normal leg alignment, secure implant fixation,
Zimmer FuZion Surgical Technique (Beta Version) INTRO Surgical Technique Introduction Surgical goals during total knee arthroplasty (TKA) include establishment of normal leg alignment, secure implant fixation,
Zimmer Trabecular Metal Ankle Interpositional Spacer and Trabecular Metal Ankle Fusion Spacer
 Zimmer Trabecular Metal Ankle Interpositional Spacer and Trabecular Metal Ankle Fusion Spacer Surgical Technique 2 Zimmer Trabecular Metal Ankle Interpositional Spacer and Trabecular Metal Ankle Fusion
Zimmer Trabecular Metal Ankle Interpositional Spacer and Trabecular Metal Ankle Fusion Spacer Surgical Technique 2 Zimmer Trabecular Metal Ankle Interpositional Spacer and Trabecular Metal Ankle Fusion
NEXGEN COMPLETE KNEE SOLUTION S A. Tibial Stem Extension & Augmentation Surgical. ATechnique
 NEXGEN COMPLETE KNEE SOLUTION ATechnique Tibial Stem Extension & Augmentation Surgical INTRODUCTION The NexGen Complete Knee Solution Intramedullary Tibial Instruments have been designed to provide an
NEXGEN COMPLETE KNEE SOLUTION ATechnique Tibial Stem Extension & Augmentation Surgical INTRODUCTION The NexGen Complete Knee Solution Intramedullary Tibial Instruments have been designed to provide an
Contact your Zimmer representative or visit us at
 Please refer to the package inserts for complete product information, including contraindications, warnings, precautions, and adverse effects. Contact your Zimmer representative or visit us at www.zimmer.com
Please refer to the package inserts for complete product information, including contraindications, warnings, precautions, and adverse effects. Contact your Zimmer representative or visit us at www.zimmer.com
Surgical Technique. Hinge Disassembly and Rebuild Technique
 Surgical Technique Hinge Disassembly and Rebuild Technique Revision Knee Arthroplasty Surgical Technique LEGION HK Hinge Knee System Introduction The LEGION HK Hinge Knee System has been designed as an
Surgical Technique Hinge Disassembly and Rebuild Technique Revision Knee Arthroplasty Surgical Technique LEGION HK Hinge Knee System Introduction The LEGION HK Hinge Knee System has been designed as an
Scorpio TS Single Axis Revision Knee System. Scorpio Total Stabilizer Revision Knee System Surgical Protocol
 Scorpio TS Single Axis Revision Knee System Scorpio Total Stabilizer Revision Knee System Surgical Protocol Table of Contents Scorpio Total Stabilizer Revision Knee System Surgical Protocol Component
Scorpio TS Single Axis Revision Knee System Scorpio Total Stabilizer Revision Knee System Surgical Protocol Table of Contents Scorpio Total Stabilizer Revision Knee System Surgical Protocol Component
PIN GUIDE SYSTEM SURGICAL TECHNIQUE. with the SIGMA High Performance Instruments System. This publication is not intended for distribution in the USA.
 PIN GUIDE SYSTEM with the SIGMA High Performance Instruments System This publication is not intended for distribution in the USA. SURGICAL TECHNIQUE Pin Guide Surgical Technique The following steps are
PIN GUIDE SYSTEM with the SIGMA High Performance Instruments System This publication is not intended for distribution in the USA. SURGICAL TECHNIQUE Pin Guide Surgical Technique The following steps are
CONTRIBUTING SURGEON. Barry Waldman, MD Director, Center for Joint Preservation and Replacement Sinai Hospital of Baltimore Baltimore, MD
 CONTRIBUTING SURGEON Barry Waldman, MD Director, Center for Joint Preservation and Replacement Sinai Hospital of Baltimore Baltimore, MD System Overview The EPIK Uni is designed to ease the use of the
CONTRIBUTING SURGEON Barry Waldman, MD Director, Center for Joint Preservation and Replacement Sinai Hospital of Baltimore Baltimore, MD System Overview The EPIK Uni is designed to ease the use of the
Resurfacing Patellar Preparation
 Surgical Technique Resurfacing Patellar Preparation Primary Total Knee Arthroplasty LEGION Total Knee System Resurfacing Patellar preparation Contents Introduction...2 Instrument assembly...3 Resurfacing
Surgical Technique Resurfacing Patellar Preparation Primary Total Knee Arthroplasty LEGION Total Knee System Resurfacing Patellar preparation Contents Introduction...2 Instrument assembly...3 Resurfacing
Proven Gen-Flex Revision Knee System. Surgical Protocol
 Proven Gen-Flex Revision Knee System Surgical Protocol Proven Gen-Flex Revision Knee System Surgeon Design Team The Proven Gen-Flex Revision Knee System Instrumentation and Surgical Protocol were developed
Proven Gen-Flex Revision Knee System Surgical Protocol Proven Gen-Flex Revision Knee System Surgeon Design Team The Proven Gen-Flex Revision Knee System Instrumentation and Surgical Protocol were developed
Trabecular Metal Femoral Component. Surgical Technique
 Trabecular Metal Femoral Component Surgical Technique INTRO Trabecular Metal Femoral Component Surgical Technique Introduction The Persona Trabecular Metal Femoral Component is designed to unite stable
Trabecular Metal Femoral Component Surgical Technique INTRO Trabecular Metal Femoral Component Surgical Technique Introduction The Persona Trabecular Metal Femoral Component is designed to unite stable
Microplasty Elite Total Knee Instrumentation
 Microplasty Elite Total Knee Instrumentation Vanguard Complete Knee System Surgical Technique Table of Contents Indications and Contraindications... 3 Introduction... 4 Patient Selection Preoperative
Microplasty Elite Total Knee Instrumentation Vanguard Complete Knee System Surgical Technique Table of Contents Indications and Contraindications... 3 Introduction... 4 Patient Selection Preoperative
Zimmer MOST Options System
 Zimmer MOST Options System Surgical Technique Modular Options for Severe Bone Loss and Trauma Zimmer MOST Options System Surgical Technique 1 MOST Options System Surgical Technique Developed in conjunction
Zimmer MOST Options System Surgical Technique Modular Options for Severe Bone Loss and Trauma Zimmer MOST Options System Surgical Technique 1 MOST Options System Surgical Technique Developed in conjunction
NexGen Complete Knee Solution. Cruciate Retaining (CR) and Revision Instrumentation Surgical Technique for Cruciate Retaining Augmentable (CRA) Knees
 and Revision Instrumentation Surgical Technique for Cruciate Retaining Augmentable (CRA) Knees") NexGen Complete Knee Solution Cruciate Retaining (CR) and Revision Instrumentation Surgical Technique for Cruciate Retaining Augmentable (CRA) Knees INTRODUCTION This surgical technique document combines
NexGen Complete Knee Solution Cruciate Retaining (CR) and Revision Instrumentation Surgical Technique for Cruciate Retaining Augmentable (CRA) Knees INTRODUCTION This surgical technique document combines
NexGen LPS Fixed Bearing Knee. Surgical Technique
 NexGen LPS Fixed Bearing Knee Surgical Technique Table of Contents Introduction...2 Preoperative Planning...2 Surgical Technique...3 Step One: Align the Tibia...3 MICRO-MILL Hand Piece Assembly and Usage
NexGen LPS Fixed Bearing Knee Surgical Technique Table of Contents Introduction...2 Preoperative Planning...2 Surgical Technique...3 Step One: Align the Tibia...3 MICRO-MILL Hand Piece Assembly and Usage
TRUMATCH PERSONALIZED SOLUTIONS with the SIGMA High Performance Instruments
 TRUMATCH PERSONALIZED SOLUTIONS with the SIGMA High Performance Instruments Resection Guide System SURGICAL TECHNIQUE RESECTION GUIDE SURGICAL TECHNIQUE The following steps are an addendum to the SIGMA
TRUMATCH PERSONALIZED SOLUTIONS with the SIGMA High Performance Instruments Resection Guide System SURGICAL TECHNIQUE RESECTION GUIDE SURGICAL TECHNIQUE The following steps are an addendum to the SIGMA
Zimmer NexGen Tibial Stem Extension & Augmentation. Surgical Technique IMAGE TO COME. Stem Extensions and Augments
 Zimmer NexGen Tibial Stem Extension & Augmentation Surgical Technique IMAGE TO COME Stem Extensions and Augments Zimmer NexGen Tibial Stem Extension & Augmentation Surgical Technique 1 Zimmer NexGen Tibial
Zimmer NexGen Tibial Stem Extension & Augmentation Surgical Technique IMAGE TO COME Stem Extensions and Augments Zimmer NexGen Tibial Stem Extension & Augmentation Surgical Technique 1 Zimmer NexGen Tibial
Zimmer NexGen MIS Tibial Component. Cemented Surgical Technique. IMAGE TO COME Designed for minimally invasive procedures
 Zimmer NexGen MIS Tibial Component Cemented Surgical Technique IMAGE TO COME Designed for minimally invasive procedures Zimmer NexGen MIS Tibial Component Cemented Surgical Technique 1 Zimmer NexGen MIS
Zimmer NexGen MIS Tibial Component Cemented Surgical Technique IMAGE TO COME Designed for minimally invasive procedures Zimmer NexGen MIS Tibial Component Cemented Surgical Technique 1 Zimmer NexGen MIS
Contributing surgeons
 Surgical Technique Contributing surgeons Mike Ries, MD Fred Tria, MD Murali Jasty, MD David Drucker, MD Gerald Jerry, MD Neil Thomas, MD Johan Bellemans, MD Jan Victor, MD Gerry Engh, MD Mark Schinsky,
Surgical Technique Contributing surgeons Mike Ries, MD Fred Tria, MD Murali Jasty, MD David Drucker, MD Gerald Jerry, MD Neil Thomas, MD Johan Bellemans, MD Jan Victor, MD Gerry Engh, MD Mark Schinsky,
Constrained Posterior Stabilized (CPS) Surgical Technique
 Surgical Technique") Constrained Posterior Stabilized (CPS) Surgical Technique Constrained Posterior Stabilized (CPS) Surgical Technique INTRO Introduction The Constrained Posterior Stabilized (CPS) articular surfaces can
Constrained Posterior Stabilized (CPS) Surgical Technique Constrained Posterior Stabilized (CPS) Surgical Technique INTRO Introduction The Constrained Posterior Stabilized (CPS) articular surfaces can
Wichita Fusion Nail Surgical Technique. David A. McQueen, MD
 Wichita Fusion Nail Surgical Technique David A. McQueen, MD The patented design with a dual advantage Generates compression intraoperatively Innovative compression screw (a) locks femoral and tibial components
Wichita Fusion Nail Surgical Technique David A. McQueen, MD The patented design with a dual advantage Generates compression intraoperatively Innovative compression screw (a) locks femoral and tibial components
for Standard version (STD) for Postero-stabilized version (PS) for Ultra-Congruent version (UC)
 for Postero-stabilized version (PS) for Ultra-Congruent version (UC)") A L L I N O N E s u r g i c a l t e c h n i q u e I N T R O D u c t i O N This document describes the Surgical Technique for all the three version of Evolis Total Knee System (Standard, Postero-stabilized
A L L I N O N E s u r g i c a l t e c h n i q u e I N T R O D u c t i O N This document describes the Surgical Technique for all the three version of Evolis Total Knee System (Standard, Postero-stabilized
SCORE Revision. Revision Total Knee Arthroplasty Cemented. Surgical Technique With Conventional Instrumentation Primary cases
 SCORE Revision Revision Total Knee Arthroplasty Cemented Surgical Technique With Conventional Instrumentation Primary cases SCORE REVISION FOR PRIMARY CASES The SCORE Revision is a revision total knee
SCORE Revision Revision Total Knee Arthroplasty Cemented Surgical Technique With Conventional Instrumentation Primary cases SCORE REVISION FOR PRIMARY CASES The SCORE Revision is a revision total knee
Orthopedic Bone Nail System - Distal Femoral Nail Surgical Technique Manual
 Orthopedic Bone Nail System - Distal Femoral Nail Surgical Technique Manual Note: The surgical procedures should be performed under the guidance of qualified skilled orthopedic surgeons, and this surgical
Orthopedic Bone Nail System - Distal Femoral Nail Surgical Technique Manual Note: The surgical procedures should be performed under the guidance of qualified skilled orthopedic surgeons, and this surgical
Zimmer Unicompartmental High Flex Knee. Spacer Block Surgical Technique
 Zimmer Unicompartmental High Flex Knee Spacer Block Surgical Technique INTRO Zimmer Unicompartmental High Flex Knee Spacer Block Surgical Technique Introduction Unicompartmental knee arthroplasty (UKA)
Zimmer Unicompartmental High Flex Knee Spacer Block Surgical Technique INTRO Zimmer Unicompartmental High Flex Knee Spacer Block Surgical Technique Introduction Unicompartmental knee arthroplasty (UKA)
Zimmer MIS Intramedullary Instrumentation
 Zimmer MIS Intramedullary Instrumentation Surgical Technique For NexGen Cruciate Retaining & NexGen Legacy Posterior Stabilized Knees Zimmer MIS Intramedullary Instrumentation Surgical Technique Surgical
Zimmer MIS Intramedullary Instrumentation Surgical Technique For NexGen Cruciate Retaining & NexGen Legacy Posterior Stabilized Knees Zimmer MIS Intramedullary Instrumentation Surgical Technique Surgical
Operative Technique. Constrained Condylar. The Right Track It s not just a road we re on, it s a trail we re blazing.
 Operative Technique Constrained Condylar The Right Track It s not just a road we re on, it s a trail we re blazing. TABLE OF CONTENTS Introduction...1 Design rationale...1 operative technique Overview...2
Operative Technique Constrained Condylar The Right Track It s not just a road we re on, it s a trail we re blazing. TABLE OF CONTENTS Introduction...1 Design rationale...1 operative technique Overview...2
Contributing surgeons
 Surgical Technique Contributing surgeons Mike Ries, MD Fred Tria, MD Murali Jasty, MD David Drucker, MD Gerald Jerry, MD Neil Thomas, MD Johan Bellemans, MD Jan Victor, MD Gerry Engh, MD Mark Schinsky,
Surgical Technique Contributing surgeons Mike Ries, MD Fred Tria, MD Murali Jasty, MD David Drucker, MD Gerald Jerry, MD Neil Thomas, MD Johan Bellemans, MD Jan Victor, MD Gerry Engh, MD Mark Schinsky,
The Modular Knee System GenuX MK Revision Knee
 The Modular Knee System GenuX MK Revision Knee Surgical Technique GenuX MK Revision Knee Surgical Technique Table of content Preoperative Planning...5 System Overview...6 Compatibility Matrix...7 Surgical
The Modular Knee System GenuX MK Revision Knee Surgical Technique GenuX MK Revision Knee Surgical Technique Table of content Preoperative Planning...5 System Overview...6 Compatibility Matrix...7 Surgical
Triathlon with Single-Use Instrumentation Optimize Your TKA Experience. Posterior Referencing Surgical Protocol
 Triathlon with Single-Use Instrumentation Optimize Your TKA Experience Posterior Referencing Surgical Protocol Introduction............................................................2 Assembly Instructions...................................................6
Triathlon with Single-Use Instrumentation Optimize Your TKA Experience Posterior Referencing Surgical Protocol Introduction............................................................2 Assembly Instructions...................................................6
G K SPHERE. Surgical Technique STABILITY FOR LIFE. Hip Knee Spine Navigation
 G K SPHERE M E D I A L L Y S T A B I L I Z E D K N E E STABILITY FOR LIFE Surgical Technique Hip Knee Spine Navigation GMK SPHERE Surgical Technique Hip Knee Spine Navigation INTRODUCTION This brochure
G K SPHERE M E D I A L L Y S T A B I L I Z E D K N E E STABILITY FOR LIFE Surgical Technique Hip Knee Spine Navigation GMK SPHERE Surgical Technique Hip Knee Spine Navigation INTRODUCTION This brochure
Zimmer NexGen Rotating Hinge Knee Primary/ Revision
 Zimmer NexGen Rotating Hinge Knee Primary/ Revision Surgical Technique Designed for use in revision and difficult primary surgeries 1 INTRODUCTION The NexGen Rotating Hinge Knee Components are designed
Zimmer NexGen Rotating Hinge Knee Primary/ Revision Surgical Technique Designed for use in revision and difficult primary surgeries 1 INTRODUCTION The NexGen Rotating Hinge Knee Components are designed
Premier Total Knee Instrumentation
 Premier Total Knee Instrumentation Vanguard Complete Knee System Surgical Technique Table of Contents Indications and Contraindications... 3 Introduction... 4 Patient Selection Preoperative Planning Approaches...
Premier Total Knee Instrumentation Vanguard Complete Knee System Surgical Technique Table of Contents Indications and Contraindications... 3 Introduction... 4 Patient Selection Preoperative Planning Approaches...
The information contained in this document is intended for healthcare professionals only.
 The information contained in this document is intended for healthcare professionals only. Orthopaedics GMRS Distal Femoral Surgical Protocol Global Modular Replacement System Acknowledgements Stryker would
The information contained in this document is intended for healthcare professionals only. Orthopaedics GMRS Distal Femoral Surgical Protocol Global Modular Replacement System Acknowledgements Stryker would
ELEOS Limb Salvage System
 ELEOS Limb Salvage System Surgical Technique Total Femoral Replacement The ELEOS Limb Salvage System offers options for patients with significant bone loss due to cancer, trauma, or previous surgical procedures.
ELEOS Limb Salvage System Surgical Technique Total Femoral Replacement The ELEOS Limb Salvage System offers options for patients with significant bone loss due to cancer, trauma, or previous surgical procedures.
LCS COMPLETE SURGICAL TECHNIQUE. MILESTONE Instruments with MBT Tray Preparation
 LCS COMPLETE MILESTONE Instruments with MBT Tray Preparation SURGICAL TECHNIQUE CONTENTS Preface 2 Surgical Concepts 3 Instruments 4 Surgical Technique Summary 6 Surgical Technique 8 Preparation 8 Incision
LCS COMPLETE MILESTONE Instruments with MBT Tray Preparation SURGICAL TECHNIQUE CONTENTS Preface 2 Surgical Concepts 3 Instruments 4 Surgical Technique Summary 6 Surgical Technique 8 Preparation 8 Incision
Aesculap Orthopaedics Columbus MIOS
 Aesculap Orthopaedics Columbus MIOS Minimally Invasive Orthopaedic Solutions Manual TKA Surgical Technique MIOS 4-in-1 Cutting Block MIOS Distal Femoral Cutting Block MIOS Tibial Left and Right Cutting
Aesculap Orthopaedics Columbus MIOS Minimally Invasive Orthopaedic Solutions Manual TKA Surgical Technique MIOS 4-in-1 Cutting Block MIOS Distal Femoral Cutting Block MIOS Tibial Left and Right Cutting
TRUMATCH PERSONALIZED SOLUTIONS with the SIGMA High Performance Instruments
 TRUMATCH PERSONALIZED SOLUTIONS with the SIGMA High Performance Instruments Pin Guide System SURGICAL TECHNIQUE PIN GUIDE SURGICAL TECHNIQUE The following steps are an addendum to the SIGMA High Performance
TRUMATCH PERSONALIZED SOLUTIONS with the SIGMA High Performance Instruments Pin Guide System SURGICAL TECHNIQUE PIN GUIDE SURGICAL TECHNIQUE The following steps are an addendum to the SIGMA High Performance
NexGen Intramedullary Instrumentation. Surgical Technique
 NexGen Intramedullary Instrumentation Surgical Technique Table of Contents Introduction... 2 Preoperative Planning... 2 Surgical Technique... 3 Step One: Size the Femur/Establish External Rotation...
NexGen Intramedullary Instrumentation Surgical Technique Table of Contents Introduction... 2 Preoperative Planning... 2 Surgical Technique... 3 Step One: Size the Femur/Establish External Rotation...
Uniglide. Unicompartmental Knee Replacement Mk III surgical technique
 Uniglide Unicompartmental Knee Replacement Mk III surgical technique Uniglide Contents Operative summary 4 Pre-operative assessment 6 Preparation 7 Incision 7 Approach 7 Medial procedure 8 Tibial preparation
Uniglide Unicompartmental Knee Replacement Mk III surgical technique Uniglide Contents Operative summary 4 Pre-operative assessment 6 Preparation 7 Incision 7 Approach 7 Medial procedure 8 Tibial preparation
KneeTec Deep Dish SURGICAL TECHNIQUE
 KneeTec Deep Dish KneeTec Deep Dish SURGICAL TECHNIQUE SURGICAL TECHNIQUE This surgical technique describes the use of the instrumentation dedicated to the KneeTec DEEP DISH implant: cemented version.
KneeTec Deep Dish KneeTec Deep Dish SURGICAL TECHNIQUE SURGICAL TECHNIQUE This surgical technique describes the use of the instrumentation dedicated to the KneeTec DEEP DISH implant: cemented version.
STABILITY FOR LIFE. Surgical Technique
 STABILITY FOR LIFE Surgical Technique Joint Spine Sports Med GMK Sphere Surgical Technique 2 INDEX 1. INTRODUCTION 4 1.1 Indications 4 1.2 Contraindications 4 1.3 Preoperative planning 5 1.4 Surgical approach
STABILITY FOR LIFE Surgical Technique Joint Spine Sports Med GMK Sphere Surgical Technique 2 INDEX 1. INTRODUCTION 4 1.1 Indications 4 1.2 Contraindications 4 1.3 Preoperative planning 5 1.4 Surgical approach
NEXGEN COMPLETE KNEE SOLUTION. Revision Instrumentation Surgical Technique For Legacy Knee Constrained Condylar Knee
 NEXGEN COMPLETE KNEE SOLUTION Revision Instrumentation Surgical Technique For Legacy Knee Constrained Condylar Knee INTRODUCTION Revision total knee arthroplasty can be a very challenging task for any
NEXGEN COMPLETE KNEE SOLUTION Revision Instrumentation Surgical Technique For Legacy Knee Constrained Condylar Knee INTRODUCTION Revision total knee arthroplasty can be a very challenging task for any
Single Axis Revision Knee System
 Orthopaedics Scorpio TS Single Axis Revision Knee System Scorpio TS Trial Cutting Guide Surgical Protocol Orthopaedics Scorpio TS Single Axis Revision Knee System Scorpio TS Trial Cutting Guide Surgical
Orthopaedics Scorpio TS Single Axis Revision Knee System Scorpio TS Trial Cutting Guide Surgical Protocol Orthopaedics Scorpio TS Single Axis Revision Knee System Scorpio TS Trial Cutting Guide Surgical
Triathlon Knee System. Universal Baseplate Surgical Protocol
 Triathlon Knee System Universal Baseplate Surgical Protocol Table of Contents Acknowledgments..........................................................2 Introduction...............................................................2
Triathlon Knee System Universal Baseplate Surgical Protocol Table of Contents Acknowledgments..........................................................2 Introduction...............................................................2
THE P.F.C. SIGMA FEMORAL ADAPTER. Surgical Technique
 THE P.F.C. SIGMA FEMORAL ADAPTER Surgical Technique Contents P.F.C. Sigma Femoral Adapter and Revision Knee Surgery Introduction 2 Preoperative Planning 2 Overview 3 Surgical Technique Preparation of the
THE P.F.C. SIGMA FEMORAL ADAPTER Surgical Technique Contents P.F.C. Sigma Femoral Adapter and Revision Knee Surgery Introduction 2 Preoperative Planning 2 Overview 3 Surgical Technique Preparation of the
Triathlon Knee System. Anterior Referencing Surgical Protocol
 Triathlon Knee System Anterior Referencing Surgical Protocol Triathlon Knee System Anterior Referencing Surgical Protocol Table of Contents Acknowledgments..........................................................2
Triathlon Knee System Anterior Referencing Surgical Protocol Triathlon Knee System Anterior Referencing Surgical Protocol Table of Contents Acknowledgments..........................................................2
Triathlon Tritanium. Surgical Protocol. with Triathlon Cementless Beaded PA Femoral Component
 Triathlon Tritanium Surgical Protocol with Triathlon Cementless Beaded PA Femoral Component Triathlon Tritanium Surgical Protocol with Triathlon Cementless Beaded PA Femoral Component Description...............................
Triathlon Tritanium Surgical Protocol with Triathlon Cementless Beaded PA Femoral Component Triathlon Tritanium Surgical Protocol with Triathlon Cementless Beaded PA Femoral Component Description...............................
Constrained Posterior Stabilized (CPS)
") Constrained Posterior Stabilized (CPS) Persona The Personalized Knee Surgical Technique Table of Contents Introduction... 2 Constraint Options Initial Knee Assessment... 3 Femoral Box Cut CPS Tibial Bearing
Constrained Posterior Stabilized (CPS) Persona The Personalized Knee Surgical Technique Table of Contents Introduction... 2 Constraint Options Initial Knee Assessment... 3 Femoral Box Cut CPS Tibial Bearing
EXACTECH KNEE. Operative Technique ADDENDUM. Metaphyseal Cones. Surgeon focused. Patient driven. TM
 EXACTECH KNEE Operative Technique ADDENDUM Metaphyseal Cones Surgeon focused. Patient driven. TM TABLE OF CONTENTS INTRODUCTION...1 DESCRIPTION...1 DETAILED OPERATIVE TECHNIQUE Initial Preparation and
EXACTECH KNEE Operative Technique ADDENDUM Metaphyseal Cones Surgeon focused. Patient driven. TM TABLE OF CONTENTS INTRODUCTION...1 DESCRIPTION...1 DETAILED OPERATIVE TECHNIQUE Initial Preparation and
Persona The Personalized Knee. Surgical Technique
 Persona The Personalized Knee Surgical Technique Table of Contents Introduction... 2 Constraint Options Preoperative Planning Surgical Approach Patient Preparation Magnet Usage Symbols Screw/Pin Information
Persona The Personalized Knee Surgical Technique Table of Contents Introduction... 2 Constraint Options Preoperative Planning Surgical Approach Patient Preparation Magnet Usage Symbols Screw/Pin Information
BIOTECH FUTURE KNEE Minimal Invasive (and classic) Surgical Technique
 Surgical Technique") BIOTECH FUTURE KNEE Minimal Invasive (and classic) Surgical Technique Page No. Product description 2. Pre-operational planning 3. 1st step Femoral resection 4. P/S Femoral component 7. 2nd step Proximal
BIOTECH FUTURE KNEE Minimal Invasive (and classic) Surgical Technique Page No. Product description 2. Pre-operational planning 3. 1st step Femoral resection 4. P/S Femoral component 7. 2nd step Proximal
Triathlon Knee System Universal Baseplate Surgical Protocol
 Triathlon Knee System Universal Baseplate Surgical Protocol Triathlon Knee System Universal Baseplate Surgical Protocol Table of Contents Acknowledgments... 2 Introduction... 2 Assembly Instructions...
Triathlon Knee System Universal Baseplate Surgical Protocol Triathlon Knee System Universal Baseplate Surgical Protocol Table of Contents Acknowledgments... 2 Introduction... 2 Assembly Instructions...
Balanced Surgical Technique
 2 Balanced Surgical Technique Contemporary total knee arthroplasty demands high performance instrumentation that provides enhanced efficiency, precision, and flexibility. Through a program of continuous
2 Balanced Surgical Technique Contemporary total knee arthroplasty demands high performance instrumentation that provides enhanced efficiency, precision, and flexibility. Through a program of continuous
14 mm x +30 mm Stem Extension
 14 mm x +30 mm Stem Extension Persona The Personalized Knee Surgical Technique Table of Contents Introduction...2 Preoperative Planning Surgical Approach Patient Preparation Magnet Usage Symbols Screw/Pin
14 mm x +30 mm Stem Extension Persona The Personalized Knee Surgical Technique Table of Contents Introduction...2 Preoperative Planning Surgical Approach Patient Preparation Magnet Usage Symbols Screw/Pin
Surgical Technique with Offsetting Instruments
 MONOGRAM IM REVISION INSTRUMENT Surgical Technique with Offsetting Instruments Introduction...2 Component Removal, Canal Preparation...3 Femoral Canal Preparation (continued)...4 Distal Femoral Resection...5-7
MONOGRAM IM REVISION INSTRUMENT Surgical Technique with Offsetting Instruments Introduction...2 Component Removal, Canal Preparation...3 Femoral Canal Preparation (continued)...4 Distal Femoral Resection...5-7
INTUITION INSTRUMENTS SURGICAL TECHNIQUE
 INTUITION INSTRUMENTS SURGICAL TECHNIQUE Introduction This surgical technique provides guidelines for the implantation of the ATTUNE Knee System Family of Knee Implants with the INTUITION Instrumentation.
INTUITION INSTRUMENTS SURGICAL TECHNIQUE Introduction This surgical technique provides guidelines for the implantation of the ATTUNE Knee System Family of Knee Implants with the INTUITION Instrumentation.