HAND EXAMINATION & COMMON INJURIES OF THE HAND. Majoring in Minors Conference th January 2013 Derriford Hospital
|
|
|
- Spencer Cooper
- 6 years ago
- Views:
Transcription
1 HAND EXAMINATION & COMMON INJURIES OF THE HAND Majoring in Minors Conference th January 2013 Derriford Hospital
2 Objectives Anatomy & Terminology History Examination Look Feel Move Investigations Specific injury patterns and tests
3 Anatomy & Terminology
4 Terminology Can you name the anatomical structures?
5 Terminology
6

7 Name the bones of the hand
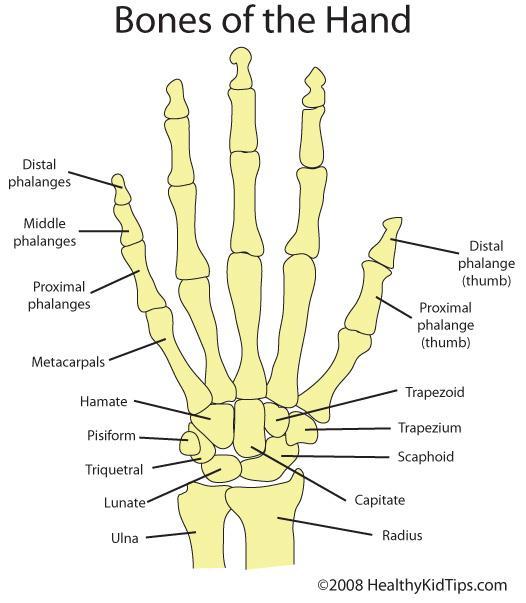
8

9 Muscles of the Hand

10 Muscles of the Hand
11 Flexor Tendons in the Fingers

12 Collateral ligaments & Volar plate
13 Extensor tendon anatomy
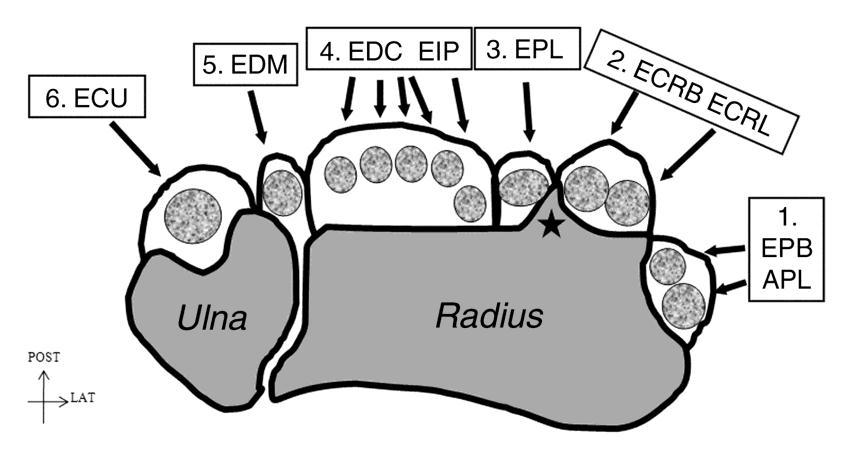

14 Extensor compartments
15 Name the nerves!

16 Nerves of the Hand

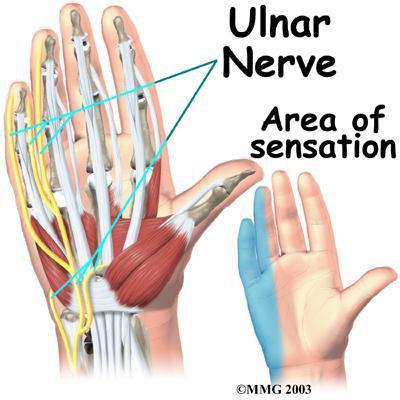
17 Sensory supply of hand by defined Ulna Nerve Ulna 1 ½ fingers Median Nerve Radial 3 ½ fingers Radial Nerve nerves Highly variable area centred on 1 st web space dorsally

18 Fingertip anatomy
19 History
20 History Age Handedness Occupation/hobbies Timing and MECHANISM of injury predicts injured structures Previous injuries/relevant conditions affecting hands/upper limb Past medical history/ Psychiatric history Allergies and medication Smoking Support at home esp if bilateral injuries!
21 Examination
22 Adequate exposure!! Colour Look Swelling/deformity/dislocations/bruising? Wounds -?size/site Active bleeding? (consider tourniquet for examination) Position hand/fingers. Digital cascade? Muscle wasting? RINGS OFF?

23
24 Feel Sites of tenderness esp. area of maximum tenderness? Crepitus/deformity Notta s nodes (+/- other incidental conditions e.g OA/RA/Dupuytrens nodules etc) Temperature/sweating? Allen s test/capillary refill Sensation - Autonomous zones/digital nerves incl. light touch/pinprick/2 point discrimination

25 Assessing sensation Light touch Pinprick 2 point discrimination In children think other methods e.g. sweat test NB. If sensory deficit both digital nerves THINK carefully re revascularisation
26 Move Gross movement - AGCF, tip to palm distance Extension (extensor lag) Flexion incl?painful/weak movement against resistance (NB. Pts with absent FDS to little finger/ linked FDS RF and LF) Abduction, adduction, circumduction, flexion, opposition and extension of thumb Wrist movements flexion/extension/ulnar and radial deviation Tenodesis/forearm flexion test Power of muscles Crepitus/locking or triggering Collaterals and joint stability Rotation/scissoring of digits
27 Range of movement Functional distance measured by tip to palm distance MCPJ = degrees hyperextension ( radial to ulnar) degrees flexion ( radial to ulnar) PIPJ= 0-15 degrees hyperextension ( ulnar to radial) degrees flexion ( ulnar to radial) DIPJ = 0-15 degrees hyperextension (no difference) degrees flexion (no difference) IPJ thumb= degrees hyperextension 80 degrees of flexion NB. Difference between flexion deformity and FIXED flexion deformity?passive movement
28

29 Testing collateral ligaments
30 Investigations XRAYS -?Others?Bony injury - need at least 2 views?soft tissues e.g FB - usually AP/Oblique/Lateral
31 Hand examination Practice
32 Specific injuries and tests


33 Nailbed injuries Probably most common hand injury esp. children Classically crush injury e.g. door Often assoc with underlying # May also be assoc with pulp injury If no nail avulsion can usually be managed conservatively +/- trephine/splint if underlying # If nail avulsed/perinychial injury will usually require nailbed repair



34 Paronychia / Felon Paronychia = infection of nailfold. Felon = pulp space infection? Need drainage PULP

35 Amputations Fingertip injuries - may be suitable for composite grafting if immediate presentation in children U R U R Ulna oblique Radial oblique
36 Proximal amputations Amputated part must be maintained adequately wrapped in clean gauze, soaked in SALINE then wrung out so only damp NOT soaking wet and NOT immersed in water/saline. then placed in sealed plastic bag plastic bag then placed on ice/in icy water Xray of both stump and amputate Need replantation ideally within 6 hours of injury



37 Volar plate injury Typically following dorsal dislocation or significant hyperextension injury Tearing of volar plate +/- avulsion fracture Tender maximally on volar aspect of jt with increased pain on hyperextension May be associated with collateral ligament injury Dorsal blocking splint 6/52


38 Closed FDP ruptures AKA Jersey finger caused by forced extension of DIPJ whilst in resisted flexion e.g. rugby jerseys/rockclimbing Typically RF FDP tendon retracts may be palpable clinically otherwise USS may help determine end of tendon Needs prompt repair

39 Flexor sheath infection Often secondary to penetrating injuries incl. small puncture wound of flexor surface e.g thorn, bites 4 Kanavels signs Finger held flexed position Fusiform swelling whole finger Excessive tenderness whole sheath Very painful passive movement Surgical emergency!!


40 Can progress into palmar spaces Also think of palmar space infections if wound more proximal Signs incl Severe pain Dorsal oedema Loss of palmar concavity Fixed finger posture Thumb abduction
41 Extensor tendon injuries Component Cause Assessment Extensor tendon Sagittal bands Laceration Attritional rupture Closed trauma, Rupture of sagittal band (usually radial) Unable to actively extend at MCPJ, Inability to maintain passively extended digit, Retain ability to extend at IPJ Subluxation of extensor, Inability to actively extend, Able to maintain passive extension, Retain extension at IPJ Central slip Lateral band Distal extensor tendon Laceration, Closed traumatic rupture, Avulsion, Attritional rupture. Unilateral laceration Bilateral lacerations rare Laceration, Attrition rupture Leads to Boutonniere deformity. Able to extend MCPJ, initially able to extend PIPJ, later ability to extend PIPJ lost, Hyperextension of DIPJ. Specific test = Elson s test No clinical deficit Inability to extend DIPJ i.e. Mallet deformity
 type injuries e.g.")


42 Mallet Finger Typically end-on (axial load) type injuries e.g. ball sports /stubbing finger Soft tissue or bony Clinical lag with inability to actively extend DIPJ Mallet splint 8-10/52


43 Traumatic rupture of central extensor slip Loss of extension at PIPJ Boutonniere deformity if not splinted/ surgically managed may become fixed ie. poor outcome if missed Elsons test PIPJ s passively flexed to 90 over table. Attempt active extension at PIPJ against resistance Central slip rupture
44 Attrition tendon ruptures Rheumatoid arthritis e.g. rupture of extensor tendons at ulna side of wrist (Vaughan-Jackson syndrome) rupture of EPL over Lister s tubercle rupture of FPL from bony spur in carpal tunnel (Mannerfelt syndrome) Iatrogenic e.g. metalwork from previous injuries

45 De Quervain s tenosynovitis Inflammation of 1 st extensor compartment i.e APL and EPB Finkelstein s test Steroid injection/physio/splint
 Also gamekeepers thumb (chronic attritional injury)")
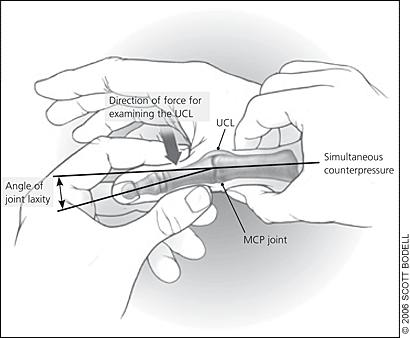
46 UCL thumb injuries Hyperabduction injury aka. skiers thumb (acute injury) Also gamekeepers thumb (chronic attritional injury) With or without bony avulsion fragment
47 In 2/3 of cases the adductor aponeurosis interposes between the bone and the torn end of the ligament STENER lesion If not treated will not heal weak pinch
48 Assess for tenderness at origin/insertion of UCL Examine for laxity with thumb in extension and in 30 degrees flexion at MCPJ.?Endpoint If too painful to allow adequate examination try LA infiltration If Stener lesion present, MAY be able to palpate mass dorsal/lateral to MCPJ Xrays to look for avulsion fragment
49 Grading of UCL thumb injury Grade 1 - no laxity, painful movement i.e. Strain Mobilise. Grade 2 - laxity WITH an endpoint, i.e. Partial tear Splint. Grade 3 - laxity with NO endpoint, i.e. Complete tear Can t exclude Stener lesion Operative fixation. N.B. If associated with undisplaced bony avulsion fracture then avoid excessive manipulation and treat in splint.
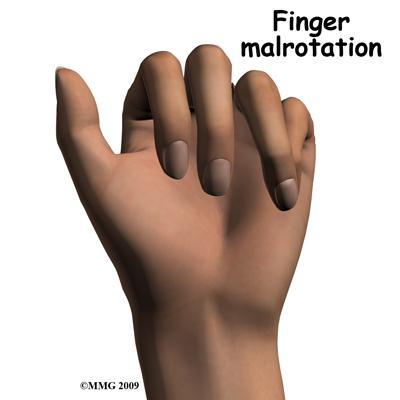
50 Hand Fractures Common!! Low energy v High energy?open or closed If open treat as per other open fractures. Need abx and formal washout If closed consider: Fracture pattern i.e. transverse/oblique/spiral?intra-articular?displacement/angulation/shortening?stability Functional impairment ie. extensor lag/rotation or scissoring

51 Paediatric Hand Fractures Salter Harris Classification SH II most common

52 Median Nerve at the Wrist Common nerve to be injured at the wrist as very superficial Can also occur as part of carpal tunnel syndrome compression as it goes through the carpal tunnel It s between FCR and PL Look for PL as it s very obvious
 Will eventually lead to thenar eminence atrophy Altered sensation in median nerve distribution Tinels")
53 Median Nerve Lesions at the Wrist Loss of function of the LOAF muscles of the hand Specifically examine oppposition/thumb abduction (APB) Will eventually lead to thenar eminence atrophy Altered sensation in median nerve distribution Tinels Phalens


54 Carpal Tunnel Syndrome Phalen s Test Tinnel s Test

55 Ulnar Nerve Lesions Supplies in Forearm Flexor Carpi Ulnaris Ulna half of FDP in Hand Superficial Branch Palmaris Brevis Sensation to 1 ½ fingers volarly Deep Branch All other small muscles of the hand except the LOAF muscles Sensation to 1 ½ fingers dorsally

56 Ulnar nerve injury-general examination Loss of function of intrinsic muscles of hand i.e. absent abduction and adduction of fingers as well as hypothenar muscles Hypothenar wasting/wasting of interossei causing guttering on dorsum (LATE) Altered sensation to little finger and ulnar border of ring finger Froment s test


57 Ulnar nerve injury in the Forearm - Wrist flexion is maintained as FCU innervated - More significant claw as ulna FDPs are intact therefore flexion at all IPJ s THE ULNAR PARADOX

58 Guyon s Canal Syndrome Can be a chronic problem similar to carpal tunnel syndrome Can be acute, as in Hook of Hamate fractures If distal, only superficial branch of nerve affected i.e. sensory only More proximal lesions may affect both sensory and motor branches hypothenar/intrinsic muscles

59 Specific Clinical Tests Froment s Sign With no functioning adductor pollicis individual can only hold paper like this by using FPL Wartenberg s Sign Inability to adduct little finger So directly test for adduction (ADM )
60 Radial nerve lesions Again depends on level of injury/lesion Superficial radial nerve branch loss of sensation on dorsum of hand - 1 st webspace Posterior interosseus branch loss of extension of fingers and wrist
61 Objectives Anatomy & Terminology History Examination Look Feel Move Investigations Specific injury patterns and tests

62 Questions??
Physical therapy of the wrist and hand
 Physical therapy of the wrist and hand Functional anatomy wrist and hand The wrist includes distal radius, scaphoid, lunate, triquetrum, pisiform, trapezium, trapezoid, capitate, and hamate. The hand includes
Physical therapy of the wrist and hand Functional anatomy wrist and hand The wrist includes distal radius, scaphoid, lunate, triquetrum, pisiform, trapezium, trapezoid, capitate, and hamate. The hand includes
Nerves of Upper limb. Dr. Brijendra Singh Professor & Head Department of Anatomy AIIMS Rishikesh
 Nerves of Upper limb Dr. Brijendra Singh Professor & Head Department of Anatomy AIIMS Rishikesh 1 Objectives Origin, course & relation of median & ulnar nerves. Motor & sensory distribution Carpal tunnel
Nerves of Upper limb Dr. Brijendra Singh Professor & Head Department of Anatomy AIIMS Rishikesh 1 Objectives Origin, course & relation of median & ulnar nerves. Motor & sensory distribution Carpal tunnel
Trapezium is by the thumb, Trapezoid is inside
 Trapezium is by the thumb, Trapezoid is inside Intercarpal Jt Radiocarpal Jt Distal Middle Proximal DIP PIP Interphalangeal Jts Metacarpalphalangeal (MCP) Jt Metacarpal Carpometacarpal (CMC) Jt Trapezium
Trapezium is by the thumb, Trapezoid is inside Intercarpal Jt Radiocarpal Jt Distal Middle Proximal DIP PIP Interphalangeal Jts Metacarpalphalangeal (MCP) Jt Metacarpal Carpometacarpal (CMC) Jt Trapezium
Hand injuries. The metacarpal bones may fracture through the base, shaft or the neck.
 Hand injuries Metacarpal injuries The metacarpal bones may fracture through the base, shaft or the neck. Shaft fractures; these are caused by direct trauma which may cause transverse # of one or more metacarpal
Hand injuries Metacarpal injuries The metacarpal bones may fracture through the base, shaft or the neck. Shaft fractures; these are caused by direct trauma which may cause transverse # of one or more metacarpal
Hand & Wrist Injuries. DR MA Manjra
 Hand & Wrist Injuries DR MA Manjra 1 Background Up to 25% of all athletic injuries General population Sport people Sport specific Position specific Multifaceted Time of season Level of athlete Parents
Hand & Wrist Injuries DR MA Manjra 1 Background Up to 25% of all athletic injuries General population Sport people Sport specific Position specific Multifaceted Time of season Level of athlete Parents
1. A 40-year-old male has dislocated his right 2 nd MCP. You have pulled as hard as you can but cannot reduce the dislocation. The problem is likely:
 CHAPTER 50 HAND 2 OCTOBER 2013 1. A 40-year-old male has dislocated his right 2 nd MCP. You have pulled as hard as you can but cannot reduce the dislocation. The problem is likely: A. He is a gamer and
CHAPTER 50 HAND 2 OCTOBER 2013 1. A 40-year-old male has dislocated his right 2 nd MCP. You have pulled as hard as you can but cannot reduce the dislocation. The problem is likely: A. He is a gamer and
Exam of the Injured Hand and Wrist. Christina M. Ward, MD Regions Hospital TRIA Woodbury
 Exam of the Injured Hand and Wrist Christina M. Ward, MD Regions Hospital TRIA Woodbury Disclosures We have no disclosures that are pertinent to this presentation Terminology Ring Long Index Small Thumb
Exam of the Injured Hand and Wrist Christina M. Ward, MD Regions Hospital TRIA Woodbury Disclosures We have no disclosures that are pertinent to this presentation Terminology Ring Long Index Small Thumb
Wrist and Hand Complaints
 Wrist and Hand Complaints Charles S. Day, M.D., M.B.A. Chief, Hand & Upper Extremity Surgery St. Elizabeth s Medical Center Tufts University School of Medicine Primary Care Internal Medicine 2018 Outline
Wrist and Hand Complaints Charles S. Day, M.D., M.B.A. Chief, Hand & Upper Extremity Surgery St. Elizabeth s Medical Center Tufts University School of Medicine Primary Care Internal Medicine 2018 Outline
MR: Finger and Thumb Injuries
 MR: Finger and Thumb Injuries Laura W. Bancroft, M.D. Professor of Radiology University of Central Florida Florida State University Outline Normal anatomy of the fingers and thumb MR imaging protocols
MR: Finger and Thumb Injuries Laura W. Bancroft, M.D. Professor of Radiology University of Central Florida Florida State University Outline Normal anatomy of the fingers and thumb MR imaging protocols
Kinesiology of The Wrist and Hand. Cuneyt Mirzanli Istanbul Gelisim University
 Kinesiology of The Wrist and Hand Cuneyt Mirzanli Istanbul Gelisim University Bones The wrist and hand contain 29 bones including the radius and ulna. There are eight carpal bones in two rows of four to
Kinesiology of The Wrist and Hand Cuneyt Mirzanli Istanbul Gelisim University Bones The wrist and hand contain 29 bones including the radius and ulna. There are eight carpal bones in two rows of four to
THE EPIDEMIOLOGY OF HAND EMERGENCIES
 THE EPIDEMIOLOGY OF HAND EMERGENCIES Dr. Adel Abdel Aziz Senior Emergency Physician Honorary Senior Clinical Lecturer, University of Southampton Training Program Director Emergency Medicine/ Health Education
THE EPIDEMIOLOGY OF HAND EMERGENCIES Dr. Adel Abdel Aziz Senior Emergency Physician Honorary Senior Clinical Lecturer, University of Southampton Training Program Director Emergency Medicine/ Health Education
Wrist & Hand Assessment and General View
 Wrist & Hand Assessment and General View Done by; Mshari S. Alghadier BSc Physical Therapy RHPT 366 m.alghadier@sau.edu.sa http://faculty.sau.edu.sa/m.alghadier/ Functional anatomy The hand can be divided
Wrist & Hand Assessment and General View Done by; Mshari S. Alghadier BSc Physical Therapy RHPT 366 m.alghadier@sau.edu.sa http://faculty.sau.edu.sa/m.alghadier/ Functional anatomy The hand can be divided
HAND SURGERY- GUIDELINES for POST-OP TREATMENT and REFERRAL to HAND THERAPY
 HAND SURGERY- GUIDELINES for POST-OP TREATMENT and REFERRAL to HAND THERAPY Please use the specific hand therapy referral form. Always give at least one telephone number for the patient so that there is
HAND SURGERY- GUIDELINES for POST-OP TREATMENT and REFERRAL to HAND THERAPY Please use the specific hand therapy referral form. Always give at least one telephone number for the patient so that there is
Hand / wrist Injections. MATS. June Condition Symptoms Conservative Treatments Location of injection CBA for surgery
 Hand / wrist Injections. MATS. June 2018. Condition Symptoms Conservative Treatments Location of injection CBA for surgery Carpal Tunnel Tingling / numbness in median nerve distribution (lateral 3 fingers)
Hand / wrist Injections. MATS. June 2018. Condition Symptoms Conservative Treatments Location of injection CBA for surgery Carpal Tunnel Tingling / numbness in median nerve distribution (lateral 3 fingers)
Kristin Kelley, DPT, OCS, FAAOMPT Orthopaedic Manual Physical Therapy Series Charlottesville Trauma/Fractures
 WRIST/HAND PATHOLOGY Kristin Kelley, DPT, OCS, FAAOMPT Orthopaedic Manual Physical Therapy Series Charlottesville 2017-2018 Trauma/Fractures Hook of Hamate Fractures Triangular Fibrocartilage Complex (TFCC)
WRIST/HAND PATHOLOGY Kristin Kelley, DPT, OCS, FAAOMPT Orthopaedic Manual Physical Therapy Series Charlottesville 2017-2018 Trauma/Fractures Hook of Hamate Fractures Triangular Fibrocartilage Complex (TFCC)
Trauma/Fractures WRIST/HAND PATHOLOGY. TFCC Injury. Hook of Hamate Fracture. Property of VOMPTI, LLC
 WRIST/HAND PATHOLOGY Kristin Kelley, DPT, OCS, FAAOMPT Orthopaedic Manual Physical Therapy Series Charlottesville 2017-2018 Trauma/Fractures Hook of Hamate Fractures Triangular Fibrocartilage Complex (TFCC)
WRIST/HAND PATHOLOGY Kristin Kelley, DPT, OCS, FAAOMPT Orthopaedic Manual Physical Therapy Series Charlottesville 2017-2018 Trauma/Fractures Hook of Hamate Fractures Triangular Fibrocartilage Complex (TFCC)
Clinical examination of the wrist, thumb and hand
 Clinical examination of the wrist, thumb and hand 20 CHAPTER CONTENTS Referred pain 319 History 319 Inspection 320 Functional examination 320 The distal radioulnar joint.............. 320 The wrist.......................
Clinical examination of the wrist, thumb and hand 20 CHAPTER CONTENTS Referred pain 319 History 319 Inspection 320 Functional examination 320 The distal radioulnar joint.............. 320 The wrist.......................
Main Menu. Wrist and Hand Joints click here. The Power is in Your Hands
 1 The Wrist and Hand Joints click here Main Menu K.5 http://www.handsonlineeducation.com/classes/k5/k5entry.htm[3/23/18, 1:40:40 PM] Bones 29 bones, including radius and ulna 8 carpal bones in 2 rows of
1 The Wrist and Hand Joints click here Main Menu K.5 http://www.handsonlineeducation.com/classes/k5/k5entry.htm[3/23/18, 1:40:40 PM] Bones 29 bones, including radius and ulna 8 carpal bones in 2 rows of
Upper Limb- Sports Medicine II
 Upper Limb- Sports Medicine II I. Palpation A. With patient sitting, supine, & prone, palpate for pain, specific tenderness, swelling, effusion, local hyperthermia B. Bony Palpation 1. Carpal Bones (8)
Upper Limb- Sports Medicine II I. Palpation A. With patient sitting, supine, & prone, palpate for pain, specific tenderness, swelling, effusion, local hyperthermia B. Bony Palpation 1. Carpal Bones (8)
LECTURE 8 HANDS: BONES AND MUSCLES
 LECTURE 8 HANDS: BONES AND MUSCLES WRIST AND HAND - Human hand can do power grip and precision grip - Thumb is 90 to the rest of the hand can do fine actions - Often able to do power actions o Take tools
LECTURE 8 HANDS: BONES AND MUSCLES WRIST AND HAND - Human hand can do power grip and precision grip - Thumb is 90 to the rest of the hand can do fine actions - Often able to do power actions o Take tools
1 Comprehensive Orthopaedic Review Hand and Wrist Tendinopathies Bernard F. Hearon, MD September 2, de Quervain Disorder Fritz de Quervain,
 1 Comprehensive Orthopaedic Review Hand and Wrist Tendinopathies Bernard F. Hearon, MD September 2, 2016 2 de Quervain Disorder Fritz de Quervain, Swiss surgeon, 1895 Stenosing tendinosis, 1st dorsal compartment
1 Comprehensive Orthopaedic Review Hand and Wrist Tendinopathies Bernard F. Hearon, MD September 2, 2016 2 de Quervain Disorder Fritz de Quervain, Swiss surgeon, 1895 Stenosing tendinosis, 1st dorsal compartment
Elbow, Wrist & Hand Evaluation.
 Elbow, Wrist & Hand Evaluation www.fisiokinesiterapia.biz Common Injuries to the Elbow, Wrist, Hand & Fingers Lateral epicondylitis tennis elbow Medial epicondylitis golfer s s elbow, little league elbow
Elbow, Wrist & Hand Evaluation www.fisiokinesiterapia.biz Common Injuries to the Elbow, Wrist, Hand & Fingers Lateral epicondylitis tennis elbow Medial epicondylitis golfer s s elbow, little league elbow
Clinical Examination of the Hand and Wrist
 Clinical Examination of the Hand and Wrist OBJECTIVES Review the clinical anatomy and physical exam of the wrist and hand Formulate a pathoanatomic diagnosis in the clinical setting Discuss common clinical
Clinical Examination of the Hand and Wrist OBJECTIVES Review the clinical anatomy and physical exam of the wrist and hand Formulate a pathoanatomic diagnosis in the clinical setting Discuss common clinical
RHEUMATOID HAND. History Pain Loss of function Neck pain. Diminished ADL assessment:
 RHEUMATOID HAND History Pain Loss of function Neck pain Diminished ADL assessment: Using toothbrush, hairbrush, knife, fork Dressing bra, Pulling up trousers / stockings Operating remote control Hobbies
RHEUMATOID HAND History Pain Loss of function Neck pain Diminished ADL assessment: Using toothbrush, hairbrush, knife, fork Dressing bra, Pulling up trousers / stockings Operating remote control Hobbies
SPECIAL ARTICLE. Missed tendon injuries INTRODUCTION
 Archives of Emergency Medicine, 1991, 8, 87-91 SPECIAL ARTICLE Missed tendon injuries H. R. GULY Consultant in A & E, Derriford Hospital, Plymouth INTRODUCTION The timing of the repair of divided tendons
Archives of Emergency Medicine, 1991, 8, 87-91 SPECIAL ARTICLE Missed tendon injuries H. R. GULY Consultant in A & E, Derriford Hospital, Plymouth INTRODUCTION The timing of the repair of divided tendons
10/10/2014. Structure and Function of the Hand. The Hand. Osteology of the Hand
 Structure and Function of the Hand 19 bones and 19 joints are necessary to produce all the motions of the hand The Hand Dorsal aspect Palmar aspect The digits are numbered 1-5 Thumb = #1 Little finger
Structure and Function of the Hand 19 bones and 19 joints are necessary to produce all the motions of the hand The Hand Dorsal aspect Palmar aspect The digits are numbered 1-5 Thumb = #1 Little finger
Hand and Wrist Editing file. Color Code Important Doctors Notes Notes/Extra explanation
 Hand and Wrist Editing file Color Code Important Doctors Notes Notes/Extra explanation Objectives Describe the anatomy of the deep fascia of the wrist & hand (flexor & extensor retinacula & palmar aponeurosis).
Hand and Wrist Editing file Color Code Important Doctors Notes Notes/Extra explanation Objectives Describe the anatomy of the deep fascia of the wrist & hand (flexor & extensor retinacula & palmar aponeurosis).
The hand is full with sweat glands, activated at times of stress. In Slide #2 there was a mistake where the doctor mentioned lateral septum twice.
 We should only know: Name, action & nerve supply Layers - Skin - Superficial fascia - Deep fascia The hand is full with sweat glands, activated at times of stress. Deep fascia In Slide #2 there was a mistake
We should only know: Name, action & nerve supply Layers - Skin - Superficial fascia - Deep fascia The hand is full with sweat glands, activated at times of stress. Deep fascia In Slide #2 there was a mistake
Common Hand Injuries Common Hand Infections. Braemar Hospital GPCME 1 November 2014
 Common Hand Injuries Common Hand Infections Braemar Hospital GPCME 1 November 2014 Waikato Hospital Tristram Clinic, 200 Collingwood Street, Hamilton P 07 838 1035 F 07 838 2032 E appts@tristramclinic.co.nz
Common Hand Injuries Common Hand Infections Braemar Hospital GPCME 1 November 2014 Waikato Hospital Tristram Clinic, 200 Collingwood Street, Hamilton P 07 838 1035 F 07 838 2032 E appts@tristramclinic.co.nz
Hand Anatomy A Patient's Guide to Hand Anatomy
 Hand Anatomy A Patient's Guide to Hand Anatomy Introduction Few structures of the human anatomy are as unique as the hand. The hand needs to be mobile in order to position the fingers and thumb. Adequate
Hand Anatomy A Patient's Guide to Hand Anatomy Introduction Few structures of the human anatomy are as unique as the hand. The hand needs to be mobile in order to position the fingers and thumb. Adequate
Common Upper Extremity Neuropathies (Not Carpal Tunnel Syndrome)
") Common Upper Extremity Neuropathies (Not Carpal Tunnel Syndrome) Nerve Compressions Common in adults, rare in children Frequently cause missed days of work and sleepless nights CDC 2001 26,794 cases of
Common Upper Extremity Neuropathies (Not Carpal Tunnel Syndrome) Nerve Compressions Common in adults, rare in children Frequently cause missed days of work and sleepless nights CDC 2001 26,794 cases of
Lecture 9: Forearm bones and muscles
 Lecture 9: Forearm bones and muscles Remember, the region between the shoulder and the elbow = brachium/arm, between elbow and wrist = antebrachium/forearm. Forearm bones : Humerus (distal ends) Radius
Lecture 9: Forearm bones and muscles Remember, the region between the shoulder and the elbow = brachium/arm, between elbow and wrist = antebrachium/forearm. Forearm bones : Humerus (distal ends) Radius
Examination of the Hand
 1 Examination of the Hand R E Page History 3 Examination 4 Movement 8 Features of Specific Conditions Affecting the Hand and Special Tests 8 Examination of the Hand 3 History General Establish important
1 Examination of the Hand R E Page History 3 Examination 4 Movement 8 Features of Specific Conditions Affecting the Hand and Special Tests 8 Examination of the Hand 3 History General Establish important
Shaun P. Garff, DO Physician of Sports Medicine
 Shaun P. Garff, DO Physician of Sports Medicine Speaker Disclosure I have no actual or potential conflicts of interest to disclose as it relates to this presentation. A little about me Born and raised
Shaun P. Garff, DO Physician of Sports Medicine Speaker Disclosure I have no actual or potential conflicts of interest to disclose as it relates to this presentation. A little about me Born and raised
Wrist & Hand Ultrasonography 대구가톨릭대학교병원재활의학과 권동락
 Wrist & Hand Ultrasonography 대구가톨릭대학교병원재활의학과 권동락 Dorsal Wrist Evaluation (1 st Compartment) EPB APL Transverse View APL, abductor pollicis longus; EPB, extensor pollicis brevis Dorsal Wrist Evaluation
Wrist & Hand Ultrasonography 대구가톨릭대학교병원재활의학과 권동락 Dorsal Wrist Evaluation (1 st Compartment) EPB APL Transverse View APL, abductor pollicis longus; EPB, extensor pollicis brevis Dorsal Wrist Evaluation
The Muscular System. Chapter 10 Part C. PowerPoint Lecture Slides prepared by Karen Dunbar Kareiva Ivy Tech Community College
 Chapter 10 Part C The Muscular System Annie Leibovitz/Contact Press Images PowerPoint Lecture Slides prepared by Karen Dunbar Kareiva Ivy Tech Community College Table 10.9: Muscles Crossing the Shoulder
Chapter 10 Part C The Muscular System Annie Leibovitz/Contact Press Images PowerPoint Lecture Slides prepared by Karen Dunbar Kareiva Ivy Tech Community College Table 10.9: Muscles Crossing the Shoulder
Fig Fig Fig. 6-3
 CHAPTER 6 UPPER EXTREMITY The surgical treatment of hand problems is a specialized area of interest in plastic surgery. The hand is a unique organ which transmits sensations from the external environment
CHAPTER 6 UPPER EXTREMITY The surgical treatment of hand problems is a specialized area of interest in plastic surgery. The hand is a unique organ which transmits sensations from the external environment
Biceps Brachii. Muscles of the Arm and Hand 4/4/2017 MR. S. KELLY
 Muscles of the Arm and Hand PSK 4U MR. S. KELLY NORTH GRENVILLE DHS Biceps Brachii Origin: scapula Insertion: radius, fascia of forearm (bicipital aponeurosis) Action: supination and elbow flexion Innervation:
Muscles of the Arm and Hand PSK 4U MR. S. KELLY NORTH GRENVILLE DHS Biceps Brachii Origin: scapula Insertion: radius, fascia of forearm (bicipital aponeurosis) Action: supination and elbow flexion Innervation:
Muscles of the hand Prof. Abdulameer Al-Nuaimi
 Muscles of the hand Prof. Abdulameer Al-Nuaimi a.alnuaimi@sheffield.ac.uk abdulameerh@yahoo.com Thenar Muscles Thenar muscles are three short muscles located at base of the thumb. All are innervated by
Muscles of the hand Prof. Abdulameer Al-Nuaimi a.alnuaimi@sheffield.ac.uk abdulameerh@yahoo.com Thenar Muscles Thenar muscles are three short muscles located at base of the thumb. All are innervated by
5/8/2017. Finger Injuries in Football. Tendon Injuries of the Hand and Wrist in Football Steve Kronlage, MD Andrews Institute Gulf Breeze, Florida
 Finger Injuries in Football Tendon Injuries of the Hand and Wrist in Football Steve Kronlage, MD Andrews Institute Gulf Breeze, Florida A jammed finger is an injury (at very least a torn ligament) A swollen
Finger Injuries in Football Tendon Injuries of the Hand and Wrist in Football Steve Kronlage, MD Andrews Institute Gulf Breeze, Florida A jammed finger is an injury (at very least a torn ligament) A swollen
CONTINUING MEDICAL EDUCATION
 CONTINUING MEDICAL EDUCATION Management of the injured hand - Principles of assessment K. Karunadasa Plastic and Reconstructive Surgical Unit, North Colombo Teaching Hospital, Ragama, Sri Lanka Keywords:
CONTINUING MEDICAL EDUCATION Management of the injured hand - Principles of assessment K. Karunadasa Plastic and Reconstructive Surgical Unit, North Colombo Teaching Hospital, Ragama, Sri Lanka Keywords:
Wrist and Hand Anatomy/Biomechanics
 Wrist and Hand Anatomy/Biomechanics Kristin Kelley, DPT, OCS, FAAOMPT Orthopaedic Manual Physical Therapy Series Charlottesville 2017-2018 Orthopaedic Manual Physical Therapy Series 2017-2018 Anatomy -
Wrist and Hand Anatomy/Biomechanics Kristin Kelley, DPT, OCS, FAAOMPT Orthopaedic Manual Physical Therapy Series Charlottesville 2017-2018 Orthopaedic Manual Physical Therapy Series 2017-2018 Anatomy -
Anatomy - Hand. Wrist and Hand Anatomy/Biomechanics. Osteology. Carpal Arch. Property of VOMPTI, LLC
 Wrist and Hand Anatomy/Biomechanics Kristin Kelley, DPT, OCS, FAAOMPT The wrist The metacarpals The Phalanges Digit 1 thumb Digit 5 digiti minimi Anatomy - Hand Orthopaedic Manual Physical Therapy Series
Wrist and Hand Anatomy/Biomechanics Kristin Kelley, DPT, OCS, FAAOMPT The wrist The metacarpals The Phalanges Digit 1 thumb Digit 5 digiti minimi Anatomy - Hand Orthopaedic Manual Physical Therapy Series
Management of Wrist and Hand Injuries
 Sunday General Session Management of Wrist and Hand Injuries Shaun Garff, DO Sports Medicine Physician Methodist Health System Dallas, Texas Educational Objectives By the end of this educational activity,
Sunday General Session Management of Wrist and Hand Injuries Shaun Garff, DO Sports Medicine Physician Methodist Health System Dallas, Texas Educational Objectives By the end of this educational activity,
Fractures and dislocations of the fingers
 Chapter 1 Fractures and dislocations of the fingers Felix S. Chew, M.D., and Catherine Maldjian, M.D. Case 1 1 Phalangeal tuft avulsion fracture 31-year-old woman injured in a ground-level fall. Lateral
Chapter 1 Fractures and dislocations of the fingers Felix S. Chew, M.D., and Catherine Maldjian, M.D. Case 1 1 Phalangeal tuft avulsion fracture 31-year-old woman injured in a ground-level fall. Lateral
Elbow/Wrist/Hand Pointers
 Elbow/Wrist/Hand Pointers Elbow Injuries -break elbow into 4 quadrants -Lateral -Medial -Posterior -Anterior 1. Lateral Epicondylosis (Tennis Elbow) a. extensor supinator tendinopathy b. repetitive gripping/wrist
Elbow/Wrist/Hand Pointers Elbow Injuries -break elbow into 4 quadrants -Lateral -Medial -Posterior -Anterior 1. Lateral Epicondylosis (Tennis Elbow) a. extensor supinator tendinopathy b. repetitive gripping/wrist
Introduction to Ultrasound Examination of the Hand and upper
 Introduction to Ultrasound Examination of the Hand and upper Emil Dionysian, M.D. Ultrasound of upper ext. Upside Convenient Opens another exam dimension Can be like a stethoscope Helps 3-D D visualization
Introduction to Ultrasound Examination of the Hand and upper Emil Dionysian, M.D. Ultrasound of upper ext. Upside Convenient Opens another exam dimension Can be like a stethoscope Helps 3-D D visualization
SPORTS INJURIES IN HAND
 Grundkurs SGSM-SSMS Sion 2015 SPORTS INJURIES IN HAND Dr S. KŠmpfen EPIDEMIOLOGY Incidence of hand, finger and wrist injuries in sports : 3% Ð 9 % RADIAL-SIDED WRIST PAIN 1)! Distal Radius Fractures 2)!
Grundkurs SGSM-SSMS Sion 2015 SPORTS INJURIES IN HAND Dr S. KŠmpfen EPIDEMIOLOGY Incidence of hand, finger and wrist injuries in sports : 3% Ð 9 % RADIAL-SIDED WRIST PAIN 1)! Distal Radius Fractures 2)!
Objectives. How your brain sees your hand. Surface anatomy Bones Joints Muscles Tendons Nerves Arteries
 Hand Therapy Review Course Washington University St. Louis, MO April 7 9, 2017 Over eighty percent of activities of daily living involve grasping or seizing objects with the hand. (Katz et al., 1970) Anatomy
Hand Therapy Review Course Washington University St. Louis, MO April 7 9, 2017 Over eighty percent of activities of daily living involve grasping or seizing objects with the hand. (Katz et al., 1970) Anatomy
The Rheumatoid Hand Deformities & Management. Dr. Anirudh Sharma Resident Department of Orthopedics
 + The Rheumatoid Hand Deformities & Management Dr. Anirudh Sharma Resident Department of Orthopedics + Why is Rheumatoid Arthritis important? + RA is a very debilitating disease median life expectancy
+ The Rheumatoid Hand Deformities & Management Dr. Anirudh Sharma Resident Department of Orthopedics + Why is Rheumatoid Arthritis important? + RA is a very debilitating disease median life expectancy
Wrist and Hand Anatomy
 Wrist and Hand Anatomy Bone Anatomy Scapoid Lunate Triquetrium Pisiform Trapeziod Trapezium Capitate Hamate Wrist Articulations Radiocarpal Joint Proximal portion Distal portion Most surface contact found
Wrist and Hand Anatomy Bone Anatomy Scapoid Lunate Triquetrium Pisiform Trapeziod Trapezium Capitate Hamate Wrist Articulations Radiocarpal Joint Proximal portion Distal portion Most surface contact found
ACUTE HAND INJURIES FOR THE PRIMARY CARE PHYSICIAN
 Vincent Shaw, MD, FAAFP Program Director Baton Rouge General Family Medicine Residency Program Baton Rouge General Sports Medicine Fellowship ACUTE HAND INJURIES FOR THE PRIMARY CARE PHYSICIAN Disclosures
Vincent Shaw, MD, FAAFP Program Director Baton Rouge General Family Medicine Residency Program Baton Rouge General Sports Medicine Fellowship ACUTE HAND INJURIES FOR THE PRIMARY CARE PHYSICIAN Disclosures
ARM Brachium Musculature
 ARM Brachium Musculature Coracobrachialis coracoid process of the scapula medial shaft of the humerus at about its middle 1. flexes the humerus 2. assists to adduct the humerus Blood: muscular branches
ARM Brachium Musculature Coracobrachialis coracoid process of the scapula medial shaft of the humerus at about its middle 1. flexes the humerus 2. assists to adduct the humerus Blood: muscular branches
Acute Wrist Injuries OUCH!
 Acute Wrist Injuries OUCH! Case the athlete FOOSH from sporting event 2 days ago C/O wrist swelling, pain, worse with movement Hmmm Wrist pain Exam of the wrist - basics Appearance Swelling, bruising,
Acute Wrist Injuries OUCH! Case the athlete FOOSH from sporting event 2 days ago C/O wrist swelling, pain, worse with movement Hmmm Wrist pain Exam of the wrist - basics Appearance Swelling, bruising,
Nerves of the upper limb Prof. Abdulameer Al-Nuaimi. E. mail:
 Nerves of the upper limb Prof. Abdulameer Al-Nuaimi E-mail: a.al-nuaimi@sheffield.ac.uk E. mail: abdulameerh@yahoo.com Brachial plexus Median nerve After originating from the brachial plexus in the axilla,
Nerves of the upper limb Prof. Abdulameer Al-Nuaimi E-mail: a.al-nuaimi@sheffield.ac.uk E. mail: abdulameerh@yahoo.com Brachial plexus Median nerve After originating from the brachial plexus in the axilla,
TENDINOSIS: TRIGGER FINGER DE QUERVAIN S TENOSYNOVITIS. Renita Sirisena Mark Puhaindran
 TENDINOSIS: TRIGGER FINGER DE QUERVAIN S TENOSYNOVITIS Renita Sirisena Mark Puhaindran Tendinosis vs Tendinitis Tendinosis: Degeneration of the tendon s collagen Related to chronic use Tendinitis Tendon
TENDINOSIS: TRIGGER FINGER DE QUERVAIN S TENOSYNOVITIS Renita Sirisena Mark Puhaindran Tendinosis vs Tendinitis Tendinosis: Degeneration of the tendon s collagen Related to chronic use Tendinitis Tendon
FINGER INJURIES. Chapter 24, pgs ,
 FINGER INJURIES Chapter 24, pgs 727 730, 741 743 1. Demonstrate mastery of anatomical references to the hand and fingers. 2. Compare and contrast Mallet Finger, Swan Neck Deformity and Boutonnière Deformity.
FINGER INJURIES Chapter 24, pgs 727 730, 741 743 1. Demonstrate mastery of anatomical references to the hand and fingers. 2. Compare and contrast Mallet Finger, Swan Neck Deformity and Boutonnière Deformity.
The Painful Elbow, Wrist, and Hand. Jennifer R Marks, MD
 The Painful Elbow, Wrist, and Hand Jennifer R Marks, MD The Painful Elbow A 44 yo M presents to clinic complaining of a sore elbow What further questions do you have for this patient? What is on your differential
The Painful Elbow, Wrist, and Hand Jennifer R Marks, MD The Painful Elbow A 44 yo M presents to clinic complaining of a sore elbow What further questions do you have for this patient? What is on your differential
The Forearm, Wrist, Hand and Fingers. Contusion Injuries to the Forearm. Forearm Fractures 12/11/2017. Oak Ridge High School Conroe, Texas
 The Forearm, Wrist, Hand and Fingers Oak Ridge High School Conroe, Texas Contusion Injuries to the Forearm The forearm is constantly exposed to bruising and contusions in contact sports. The ulna receives
The Forearm, Wrist, Hand and Fingers Oak Ridge High School Conroe, Texas Contusion Injuries to the Forearm The forearm is constantly exposed to bruising and contusions in contact sports. The ulna receives
divided by the bones ( redius and ulna ) and interosseous membrane into :
 and interosseous membrane into :") fossa Cubital Has: * floor. * roof : - Skin - superficial fasica - deep fascia ( include bicipital aponeurosis ) Structures within the roof : -cephalic and basilic veins -and between them median cubital
fossa Cubital Has: * floor. * roof : - Skin - superficial fasica - deep fascia ( include bicipital aponeurosis ) Structures within the roof : -cephalic and basilic veins -and between them median cubital
MSK Imaging Conference. 07/22/2016 Eman Alqahtani, MD, MPH R3/PGY4 UCSD Radiology
 MSK Imaging Conference 07/22/2016 Eman Alqahtani, MD, MPH R3/PGY4 UCSD Radiology A 51 years old female with chronic thumb pain, and inability to actively flex the thumb interphalyngeal joint Possible trigger
MSK Imaging Conference 07/22/2016 Eman Alqahtani, MD, MPH R3/PGY4 UCSD Radiology A 51 years old female with chronic thumb pain, and inability to actively flex the thumb interphalyngeal joint Possible trigger
Nerve Injury. 1) Upper Lesions of the Brachial Plexus called Erb- Duchene Palsy or syndrome.
 Upper Lesions of the Brachial Plexus called Erb- Duchene Palsy or syndrome.") Nerve Injury - Every nerve goes to muscle or skin so if the nerve is injured this will cause paralysis in the muscle supplied from that nerve (paralysis means loss of function) then other muscles and other
Nerve Injury - Every nerve goes to muscle or skin so if the nerve is injured this will cause paralysis in the muscle supplied from that nerve (paralysis means loss of function) then other muscles and other
Clinical Orthopaedic Rehabilitation Volume 1 and 2
 Clinical Orthopaedic Rehabilitation Volume 1 and 2 COURSE DESCRIPTION This program is a practical, clinical guide that provides guidance on the evaluation, differential diagnosis, treatment, and rehabilitation
Clinical Orthopaedic Rehabilitation Volume 1 and 2 COURSE DESCRIPTION This program is a practical, clinical guide that provides guidance on the evaluation, differential diagnosis, treatment, and rehabilitation
Carpal Tunnel Syndrome/ Cubital Tunnel Syndrome. Nerve anatomy. Pathophysiology 6/14/2014. Most common compression neuropathies of the upper extremity
 Carpal Tunnel Syndrome/ Cubital Tunnel Syndrome Justin Arnold MD Family Medicine Update 2014 Most common compression neuropathies of the upper extremity Increasing prevalence CTS 50/1000 subjects Up to
Carpal Tunnel Syndrome/ Cubital Tunnel Syndrome Justin Arnold MD Family Medicine Update 2014 Most common compression neuropathies of the upper extremity Increasing prevalence CTS 50/1000 subjects Up to
Cheyenne Kate P. Rebosura, MD Clinical Associate Orthopaedic Surgery KhooTeck PuatHospital
 Cheyenne Kate P. Rebosura, MD Clinical Associate Orthopaedic Surgery KhooTeck PuatHospital Outline I. Principles of Assessment II. Flexor Tenosynovitis III. Fight Bite IV. Animal Bite V. Compartment Syndrome
Cheyenne Kate P. Rebosura, MD Clinical Associate Orthopaedic Surgery KhooTeck PuatHospital Outline I. Principles of Assessment II. Flexor Tenosynovitis III. Fight Bite IV. Animal Bite V. Compartment Syndrome
In the name of Allah, Most gracious, Most merciful
 In the name of Allah, Most gracious, Most merciful This lecture includes the following: The Palmer Oponeurosis. The Carpel tunnel. The palmaris brevis muscle. The anatomical snuffbox. The Fibrous flexor
In the name of Allah, Most gracious, Most merciful This lecture includes the following: The Palmer Oponeurosis. The Carpel tunnel. The palmaris brevis muscle. The anatomical snuffbox. The Fibrous flexor
Hand and Upper Extremity
 Taylor_PS_C1-10.qxd 25/10/2004 04:20 PM Page 101 Chapter 8 Hand and Upper Extremity Subhro K. Sen, MD and Jesse A.Taylor, MD Hands, and in particular opposable thumbs, have played a large role in human
Taylor_PS_C1-10.qxd 25/10/2004 04:20 PM Page 101 Chapter 8 Hand and Upper Extremity Subhro K. Sen, MD and Jesse A.Taylor, MD Hands, and in particular opposable thumbs, have played a large role in human
Evaluation of the Injured Hand. Sanjay K. Sharma, M.D., F.A.C.S Regional Trauma Conference June 2, 2016
 Evaluation of the Injured Hand 2016 Regional Trauma Conference June 2, 2016 Disclosures Nothing relevant Outline General overview of Hand Trauma Anatomy/Examination Selected Cases History of Hand Surgery
Evaluation of the Injured Hand 2016 Regional Trauma Conference June 2, 2016 Disclosures Nothing relevant Outline General overview of Hand Trauma Anatomy/Examination Selected Cases History of Hand Surgery
Tendon transfers for ulnar nerve palsy
 Tendon transfers for ulnar nerve palsy Caroline LECLERCQ, de la main Paris, France Gruppo MANUS Etiology - Distal palsy - Nerve laceration at forearm & wrist - Neuromuscular diseases CMT, leprosy - Lower
Tendon transfers for ulnar nerve palsy Caroline LECLERCQ, de la main Paris, France Gruppo MANUS Etiology - Distal palsy - Nerve laceration at forearm & wrist - Neuromuscular diseases CMT, leprosy - Lower
STRUCTURAL BASIS OF MEDICAL PRACTICE EXAMINATION 5. September 30, 2011
 STRUCTURAL BASIS OF MEDICAL PRACTICE EXAMINATION 5 September 30, 2011 PART l. Answer in the space provided. (12 pts) 1. Identify the structures. (2 pts) EXAM NUMBER A. Suprascapular nerve B. Axillary nerve
STRUCTURAL BASIS OF MEDICAL PRACTICE EXAMINATION 5 September 30, 2011 PART l. Answer in the space provided. (12 pts) 1. Identify the structures. (2 pts) EXAM NUMBER A. Suprascapular nerve B. Axillary nerve
Ulnar Neuropathy in the Distal Ulnar Tunnel
 Ulnar Neuropathy in the Distal Ulnar Tunnel DAVID W. SHUPE, PT, ATC' Journal of Orthopaedic & Sports Physical Therapy A brief anatomical review of the ulnar nerve and areas of ulnar nerve entrapment is
Ulnar Neuropathy in the Distal Ulnar Tunnel DAVID W. SHUPE, PT, ATC' Journal of Orthopaedic & Sports Physical Therapy A brief anatomical review of the ulnar nerve and areas of ulnar nerve entrapment is
MCQWeek2. All arise from the common flexor origin. The posterior aspect of the medial epicondyle is the common flexor origin.
 MCQWeek2. 1. Regarding superficial muscles of anterior compartment of the forearm: All arise from the common flexor origin. The posterior aspect of the medial epicondyle is the common flexor origin. Flexor
MCQWeek2. 1. Regarding superficial muscles of anterior compartment of the forearm: All arise from the common flexor origin. The posterior aspect of the medial epicondyle is the common flexor origin. Flexor
STRUCTURAL BASIS OF MEDICAL PRACTICE EXAMINATION 5 October 6, 2006
 STRUCTURAL BASIS OF MEDICAL PRACTICE EXAMINATION 5 October 6, 2006 PART l. Answer in the space provided. (8 pts) 1. Identify the structures. (2 pts) B C A. _pisiform B. _ulnar artery A C. _flexor carpi
STRUCTURAL BASIS OF MEDICAL PRACTICE EXAMINATION 5 October 6, 2006 PART l. Answer in the space provided. (8 pts) 1. Identify the structures. (2 pts) B C A. _pisiform B. _ulnar artery A C. _flexor carpi
Fractures of the Hand in Children Which are simple? And Which have pitfalls??
 Fractures of the Hand in Children Which are simple? And Which have pitfalls?? Kaye E Wilkins DVM, MD Professor of Orthopedics and Pediatrics Departments of Orthopedics and Pediatrics University of Texas
Fractures of the Hand in Children Which are simple? And Which have pitfalls?? Kaye E Wilkins DVM, MD Professor of Orthopedics and Pediatrics Departments of Orthopedics and Pediatrics University of Texas
Common. Common Hand Problems in Elite Athletes
 Common Hand Problems in Elite Athletes Fred Corley M.D. Dept. of Orthopaedic Surgery UTHSCSA I have no disclosures concerning this talk. The University of Texas Health Science Center @ San Antonio - Orthopaedics
Common Hand Problems in Elite Athletes Fred Corley M.D. Dept. of Orthopaedic Surgery UTHSCSA I have no disclosures concerning this talk. The University of Texas Health Science Center @ San Antonio - Orthopaedics
Common Elbow Problems
 Common Elbow Problems Duncan Ferguson FRACS Knee and Shoulder Specialist Elbow Instability Common 10-25% of elbow injuries Median age 30 yrs Most simple dislocations are stable after reduction recurrence
Common Elbow Problems Duncan Ferguson FRACS Knee and Shoulder Specialist Elbow Instability Common 10-25% of elbow injuries Median age 30 yrs Most simple dislocations are stable after reduction recurrence
Hand & Wrist Casey G. Batten MD Assistant Clinical Professor UCSF Sports Medicine
 Hand & Wrist Casey G. Batten MD Assistant Clinical Professor UCSF Sports Medicine Topics: Scaphoid Fracture Scapholunate Separation TFCC Injury Thumb Ulnar Collateral Lig (UCL) Injury Extensor Injury /
Hand & Wrist Casey G. Batten MD Assistant Clinical Professor UCSF Sports Medicine Topics: Scaphoid Fracture Scapholunate Separation TFCC Injury Thumb Ulnar Collateral Lig (UCL) Injury Extensor Injury /
13 13/3/2012. Adel Muhanna
 13 13/3/2012 Adel Muhanna بسم هللا الرحمن الرحيم The Hand Extensor retinaculum: Deep fascia of anterior compartment of the wrist is thickened to form flexor retinaculum : a bridge that have 6 structures
13 13/3/2012 Adel Muhanna بسم هللا الرحمن الرحيم The Hand Extensor retinaculum: Deep fascia of anterior compartment of the wrist is thickened to form flexor retinaculum : a bridge that have 6 structures
Introduction. Paronychia. Hand Infections. Eponychium. Paronychia 1/26/2015. INFECTIONS OF THE UPPER EXTREMITY Mark Rekant M.D.
 Introduction INFECTIONS OF THE UPPER EXTREMITY Mark Rekant M.D. Thomas Jefferson University Philadelphia Hand Center South Jersey Hand Center Hand infections are frequent Taking into account the countless
Introduction INFECTIONS OF THE UPPER EXTREMITY Mark Rekant M.D. Thomas Jefferson University Philadelphia Hand Center South Jersey Hand Center Hand infections are frequent Taking into account the countless
10/15/2014. Wrist. Clarification of Terms. Clarification of Terms cont
 Wrist Clarification of Terms Palmar is synonymous with anterior aspect of the wrist and hand Ventral is also synonymous with anterior aspect of the wrist and hand Dorsal refers to the posterior aspect
Wrist Clarification of Terms Palmar is synonymous with anterior aspect of the wrist and hand Ventral is also synonymous with anterior aspect of the wrist and hand Dorsal refers to the posterior aspect
Tendon Transfers. Variability muscle 2x stronger than another Greatest force at resting length. Drag:
 Tendon Transfers Joanne Mimm, MPT, CHT Restore balance Indications Nerve injury paralyzed muscle damaged tendon/muscle CNS lesion Consider action Functional gain Strength-ability to generate tension number
Tendon Transfers Joanne Mimm, MPT, CHT Restore balance Indications Nerve injury paralyzed muscle damaged tendon/muscle CNS lesion Consider action Functional gain Strength-ability to generate tension number
The hand. it's the most important subject of the upper limb because it has a clinical importance. the palm of the hand**
 Today at 12:48 AM The hand it's the most important subject of the upper limb because it has a clinical importance. the palm of the hand** -the palmar aponeurosis located in the palm of the hand which is
Today at 12:48 AM The hand it's the most important subject of the upper limb because it has a clinical importance. the palm of the hand** -the palmar aponeurosis located in the palm of the hand which is
MANAGEMENT OF TRAUMATIC HAND INJURIES IN SPORT. Katherine Katie Faust, MD
 MANAGEMENT OF TRAUMATIC HAND INJURIES IN SPORT Katherine Katie Faust, MD None DISCLOSURES THE ATHLETE Children are hard to figure out Parents are not always better Don t Assume Maintain high index of suspicion
MANAGEMENT OF TRAUMATIC HAND INJURIES IN SPORT Katherine Katie Faust, MD None DISCLOSURES THE ATHLETE Children are hard to figure out Parents are not always better Don t Assume Maintain high index of suspicion
EXAMINATION OF THE WRIST BEYOND THE BASICS OMA SPORT MED Janice Harvey MD CCFP CFFP Dip. Sp Med.
 EXAMINATION OF THE WRIST BEYOND THE BASICS OMA SPORT MED 2019 Janice Harvey MD CCFP CFFP Dip. Sp Med. CFPC CoI Templates: Slide 1 used in Faculty presentation only. FACULTY/PRESENTER DISCLOSURE Faculty:
EXAMINATION OF THE WRIST BEYOND THE BASICS OMA SPORT MED 2019 Janice Harvey MD CCFP CFFP Dip. Sp Med. CFPC CoI Templates: Slide 1 used in Faculty presentation only. FACULTY/PRESENTER DISCLOSURE Faculty:
Hand and wrist emergencies
 Chapter1 Hand and wrist emergencies Carl A. Germann Distal radius and ulnar injuries PEARL: Fractures of the distal radius and ulna are the most common type of fractures in patients younger than 75 years.
Chapter1 Hand and wrist emergencies Carl A. Germann Distal radius and ulnar injuries PEARL: Fractures of the distal radius and ulna are the most common type of fractures in patients younger than 75 years.
Classification of Established Volkmann s Ischemic Contracture and the Program for Its Treatment
 10 Classification of Established Volkmann s Ischemic Contracture and the Program for Its Treatment In spite of the advances made in preventive treatment of muscular ischemia at the forearm and hand, there
10 Classification of Established Volkmann s Ischemic Contracture and the Program for Its Treatment In spite of the advances made in preventive treatment of muscular ischemia at the forearm and hand, there
The Elbow and the cubital fossa. Prof Oluwadiya Kehinde
 The Elbow and the cubital fossa Prof Oluwadiya Kehinde www.oluwadiya.com Elbow and Forearm Anatomy The elbow joint is formed by the humerus, radius, and the ulna Bony anatomy of the elbow Distal Humerus
The Elbow and the cubital fossa Prof Oluwadiya Kehinde www.oluwadiya.com Elbow and Forearm Anatomy The elbow joint is formed by the humerus, radius, and the ulna Bony anatomy of the elbow Distal Humerus
Viorel Nacu. The clinical anatomy of the Hand
 Viorel Nacu The clinical anatomy of the Hand The distal part of the upper limb is divided in to three regions: 1. The wrist (carpus) 2. The hand (metacarpus) 3. The digits (fingers) The landmarks of this
Viorel Nacu The clinical anatomy of the Hand The distal part of the upper limb is divided in to three regions: 1. The wrist (carpus) 2. The hand (metacarpus) 3. The digits (fingers) The landmarks of this
ACPOMIT Conference 2013 Workshop: Hand and Wrist
 ACPOMIT Conference 2013 Workshop: Hand and Wrist Sarah Turner, MCSP, Clinical Specialist in Hand Therapy Grad Dip Injection Therapy Workshop! Trigger Finger! OA 1 st CMC joint! De Quervain s Tenosynovitis!
ACPOMIT Conference 2013 Workshop: Hand and Wrist Sarah Turner, MCSP, Clinical Specialist in Hand Therapy Grad Dip Injection Therapy Workshop! Trigger Finger! OA 1 st CMC joint! De Quervain s Tenosynovitis!
Urgent Cases and Foreign Bodies
 Urgent Cases and Foreign Bodies Catherine J. Brandon, MD, MS University of Michigan Ann Arbor, MI, USA Introduction: Patients added on to the schedule from the emergency department or as urgent add-on
Urgent Cases and Foreign Bodies Catherine J. Brandon, MD, MS University of Michigan Ann Arbor, MI, USA Introduction: Patients added on to the schedule from the emergency department or as urgent add-on
Supplied in part by the musculocutaneous nerve. Forms the axis of rotation in movements of pronation and supination
 Anatomy: Upper limb (15 questions) 1. Latissimus Dorsi: Is innervated by the dorsal scapular nerve Lies above feres major muscle Medially rotates the humerus All of the above 2. Supinator muscle is: Deep
Anatomy: Upper limb (15 questions) 1. Latissimus Dorsi: Is innervated by the dorsal scapular nerve Lies above feres major muscle Medially rotates the humerus All of the above 2. Supinator muscle is: Deep
Year 2004 Paper one: Questions supplied by Megan
 QUESTION 47 A 58yo man is noted to have a right foot drop three days following a right total hip replacement. On examination there is weakness of right ankle dorsiflexion and toe extension (grade 4/5).
QUESTION 47 A 58yo man is noted to have a right foot drop three days following a right total hip replacement. On examination there is weakness of right ankle dorsiflexion and toe extension (grade 4/5).
Injuries to the Hands and Feet
 Injuries to the Hands and Feet Chapter 26 Injuries to the Hands and Feet Introduction Combat injuries to the hands and feet differ from those of the arms and legs in terms of mortality and morbidity. Death
Injuries to the Hands and Feet Chapter 26 Injuries to the Hands and Feet Introduction Combat injuries to the hands and feet differ from those of the arms and legs in terms of mortality and morbidity. Death
(i) Examination of the wrist surface anatomy of the carpal bones
 Examination of the wrist surface anatomy of the carpal bones") Current Orthopaedics (2005) 19, 171 179 www.elsevier.com/locate/cuor MINI-SYMPOSIUM: THE WRIST (i) Examination of the wrist surface anatomy of the carpal bones R. Srinivas Reddy, J. Compson Upper Limb
Current Orthopaedics (2005) 19, 171 179 www.elsevier.com/locate/cuor MINI-SYMPOSIUM: THE WRIST (i) Examination of the wrist surface anatomy of the carpal bones R. Srinivas Reddy, J. Compson Upper Limb
8 Recovering From HAND FRACTURE SURGERY
 8 Recovering From HAND FRACTURE SURGERY Hand fractures are caused by trauma and result in breaking (fracturing) the phalanges or metacarpals. Surgery involves achieving acceptable alignment and providing
8 Recovering From HAND FRACTURE SURGERY Hand fractures are caused by trauma and result in breaking (fracturing) the phalanges or metacarpals. Surgery involves achieving acceptable alignment and providing
Forearm and Wrist Regions Neumann Chapter 7
 Forearm and Wrist Regions Neumann Chapter 7 REVIEW AND HIGHLIGHTS OF OSTEOLOGY & ARTHROLOGY Radius dorsal radial tubercle radial styloid process Ulna ulnar styloid process ulnar head Carpals Proximal Row
Forearm and Wrist Regions Neumann Chapter 7 REVIEW AND HIGHLIGHTS OF OSTEOLOGY & ARTHROLOGY Radius dorsal radial tubercle radial styloid process Ulna ulnar styloid process ulnar head Carpals Proximal Row
The hand that hurts. Hand. Differential diagnosis
 Hand 511 The hand that hurts Tis article looks at the common and important causes of pain in the hand relevant to a population over 50 years of age and suggests a structure to approach the clinical assessment.
Hand 511 The hand that hurts Tis article looks at the common and important causes of pain in the hand relevant to a population over 50 years of age and suggests a structure to approach the clinical assessment.
Wrist & Hand Injury in Sports
 Wrist & Hand Injury in Sports Jennifer Allen,PT,DPT,OCS,SCS,CHT Return to Play Criteria, Clinical Pearls, & Rehab Considerations PBATS Baseball Medicine Conference 2018 Disclosures Wrist & Hand Injury
Wrist & Hand Injury in Sports Jennifer Allen,PT,DPT,OCS,SCS,CHT Return to Play Criteria, Clinical Pearls, & Rehab Considerations PBATS Baseball Medicine Conference 2018 Disclosures Wrist & Hand Injury
CASE ONE CASE ONE. RADIAL HEAD FRACTURE Mason Classification. RADIAL HEAD FRACTURE Mechanism of Injury. RADIAL HEAD FRACTURE Imaging
 CASE ONE An eighteen year old female falls during a basketball game, striking her elbow on the court. She presents to your office that day with a painful, swollen elbow that she is unable to flex or extend
CASE ONE An eighteen year old female falls during a basketball game, striking her elbow on the court. She presents to your office that day with a painful, swollen elbow that she is unable to flex or extend