ORTHOPAEDIC CHOICE. Pathways
|
|
|
- Austin Walker
- 6 years ago
- Views:
Transcription
1 ORTHOPAEDIC CHOICE Pathways
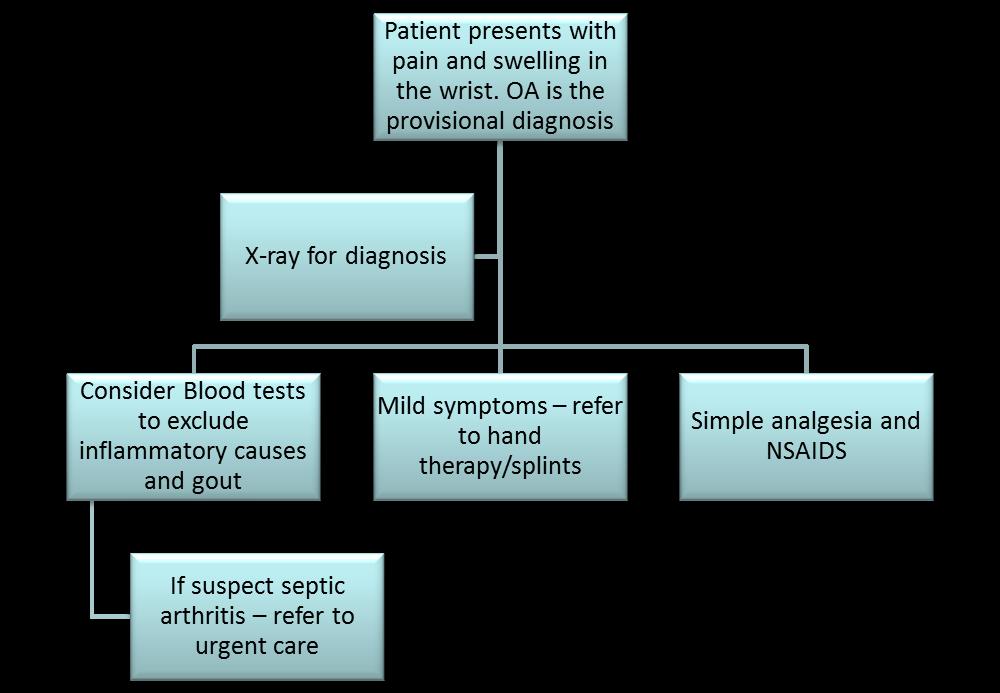
2 OA Wrist
3 Ganglion/Cysts
4 Dupuytrens contracture
5 Carpal Tunnel Syndrome Carpal Tunnel pathway For advice on management of CTS please follow link to Map of Medicine
6 Trigger Finger Trigger finger pathway For advice on management of trigger finger please follow link to Map of Medicine
7 Shoulder Shoulder pathway For advice on management of shoulder pain please follow link to Map of Medicine There are also further local guidelines
8 Is it Neck or Shoulder? Ask the patient to first move the neck and the move the shoulder. Which reproduces the pain? Red Flags = Urgent to Secondary Care Any mass or swelling -? Tumour Red skin, fever or systemically unwell -? Infection? Unreduced dislocation? Fracture Urgent Referral to Orthopaedic Choice History of trauma with loss of active abduction in younger patient -? Acute Cuff Tear Primary Care Refer If assistance is required with diagnosis Orthopaedic Choice Confirm Diagnosis Neck Follow Spinal Guidelines Shoulder History of Instability? Does the shoulder ever come out of joint? Is the patient worried that shoulder may dislocate? N o Y Instability Physio if Atraumatic Instability Traumatic dislocation Ongoing Symptoms Atraumatic with failed physio Instability X-ray Refer for extensive physio with specialist guidance Atraumatic if above fails for MRA Traumatic if 2 or more dislocations - consider surgical referal Is the pain localised to the AC joint and associated with tenderness? Is there high arc pain? Is there positive cross arm test? N o Y ACJ Disease Rest/NSAIDS/ analgesics ACJ Injection Physio Xray if no improvement ACJ Disease Refer if transient or no response to injection or physio ACJ Disease X-ray ACJ injection Guided injection if failed Persistent symptoms refer for ACJ resection Surgical referral for Gr 4,5,6 instability
9 Is there reduces passive external rotation? N o Y Glenohumeral joint Frozen shoulder or Arthritis X-ray to differentiate Analgesics Patient information Steroid injection Physio Glenohumeral joint Frozen shoulder with normal x-ray refer only if atypical and/or severe functional limitation Arthritis refer if poor response to analgesics and injection Glenohumeral joint Frozen Shoulder Confirm Diagnosis Intra-articular injection Patient information and analgesics Physio in stage 2 and 3 Refer for MUA/capsular release severe pain and functionally not coping Is there a painful arc on abduction? Is the pain on abduction worse with the thumb down, worse against resistance? History of trauma with loss of abduction in younger patient See Urgent N o Y Subacromial Pain Rest/Analgesics Subacromial injection Physiotherapy Subacromial Pain Transient or no response to injection and physiotherapy Glenohumeral joint Arthritis Confirm Diagnosis Advice and analgesics Intra-articulas injection Refer for joint replacement for pain relief Subacromial Pain X-ray Differentiate calsific tendinitis/ cuff pathology/ impingement USS if suspected cuff tear or prior to ASAD Repeat subacromial injection Refer for Barbotage for calsific tendinits Refer for Decompression of cuff repair. Other causes of Neck or Arm Pain Unexplained wasting, significant sensory or motor deficits, neurovascular compromise Y Neurological lesion Depending on severity refer to Orthopaedic Choice or Secondary Care A&E if suspected stroke Neurological lesion MRI - cervical spine or brachial plexus as appropriate Nerve conduction studies Onwards referral as appropriate
10 HIP/KNEE Hip/Knee pathway For advice on management of Hip and Knee pain please follow link to Map of Medicine There are also further local guidelines
11 Map of medicine knee pain pathway Referred to Orthopaedic Choice Knee slow to resolve after injury despite conservative management, or lack of confidence in return to sport Suspected anterior cruciate ligament tear history of significant twisting or hyperextension knee injury associated with rapid effusion ongoing painless instability associated with twisting activities positive Lachman s test +/- anterior drawer May have associated mensical tear, other ligamentous injuries including posteroloateral corner Follow ACL pathway Suspected posterior cruciate ligament tear history of blow to anterior proximal tibia, or hyperflexion or hyperextension injury may experience rapid knee effusion positive posterior sag and drawer of tibia positive dial at 90 may have concurrent injuries including posterolateral corner (with positive dial test at 30 and/or positive Hughston s test) or meniscal tear may experience instability sensation on descending slopes and stairs, and pushing heavy loads Suspected medial collateral ligament tear history of forceful valgus injury may develop effusion can be associated with mensical tear or other ligamentous injury depending on severity localised tenderness Follow MCL pathway Suspected lateral collateral ligament tear history of forceful varus injury usually develops localised swelling can be associated with meniscal or other ligamentous injury depending on severity localised tenderness Follow LCL pathway Follow PCL pathway
12 ACL injury pathway Suspected anterior cruciate ligament tear history of significant twisting or hyperextension knee injury associated with rapid effusion ongoing painless instability associated with twisting activities positive Lachman s test +/- anterior drawer May have associated mensical tear, other ligamentous injuries including posteroloateral corner MRI confirms isolated ACL rupture Recurrently unstable knee Patient young and wants to continue cutting activities Discuss with patient potential for ACL reconstructive surgery, including goals of surgery, expected postoperative timescales and rehabilitation requirements If patient keen to go ahead with surgery, refer for surgical opinion May 2013 Refer for MRI scan to confirm ACL tear and investigate other concurrent knee pathology MRI confirms isolated ACL rupture Recurrently unstable knee Discuss with patient potential for ACL reconstructive surgery, including goals of surgery, expected postoperative timescales and rehabilitation requirements If patient not keen to go ahead with surgery, refer for ACL brace and physiotherapy MRI confirms ACL rupture with meniscal tear Symptomatic meniscal tear Intermittently unstable knee Patient may require ACL reconstruction if young and wishes to participate in cutting sports and willing to comply with post-operative rehabilitation Patient may only require arthroscopic debridement of meniscal tear if knee remains stable on day-today activities, and does not participate in cutting activities Refer for surgical opinion MRI confirms ACL rupture with meniscal tear Asymptomatic meniscal tear Intermittently unstable knee Patient may require ACL reconstruction if young and wishes to participate in cutting sports and willing to comply with postoperative rehabilitation Refer for surgical opinion MRI confirms ACL rupture with PLC rupture Patient more likely to have functionally unstable knee Refer for surgical opinion
13 PCL injury pathway Suspected posterior cruciate ligament tear history of blow to anterior proximal tibia, or hyperflexion or hyperextension injury may experience rapid knee effusion positive posterior sag and drawer of tibia positive dial at 90 may have concurrent injuries including posterolateral corner (with positive dial test at 30 and/or positive Hughston s test) or meniscal tear may experience instability sensation on descending slopes and stairs, and pushing heavy loads Refer for MRI scan to confirm PCL tear and investigate other concurrent knee pathology Clinical findings and MRI confirm isolated PCL rupture Refer to physiotherapy for PCL injury rehabilitation program Patients do not usually require isolated PCL reconstruction Clinical findings and MRI confirm PCL rupture with symptomatic meniscal tear Refer for surgical opinion regarding meniscal tear May require physiotherapy referral for PCL injury rehabilitation program in meantime if able to tolerate Clinical findings and MRI confirm PCL rupture with PLC or other ligament involvement and instability Refer for surgical opinion May also require referral for combined instability brace in meantime if knee unstable If failed conservative management, refer for PCL brace or surgical opinion depending on level of disability and patient wishes
14 MCL injury pathway Suspected medial collateral ligament tear history of forceful valgus injury may develop effusion can be associated with medial mensical tear or ACL injury depending on severity localised tenderness If clinical findings suggest isolated Grade 1-2 MCL injury Refer to physiotherapy for MCL injury rehabilitation program (ROM and strengthening work) May need referral for x- ray to exclude bony injury If clinical findings suggest Grade 1-2 MCL injury + meniscal tear Refer MRI scan to investigate presence of meniscal tear If clinical findings and MRI scan confirms symptomatic meniscal tear, refer for surgical opinion May also require referral to physiotherapy if limited ROM and muscle strength If clinical findings suggest Grade 3 MCL injury, concurrent meniscal and other ligamentous involvement is likely Refer for x- ray and MRI scan to investigate any concurrent injuries Refer for surgical opinion If acute injury, brace locked at 30 for 3-6 weeks If non-acute, referral for brace if knee is unstable Referral for physiotherapy if limited ROM and reduced muscle strength
15 LCL injury pathway Suspected lateral collateral ligament tear history of forceful varus injury usually develops localised swelling can be associated with meniscal or other ligamentous injury depending on severity localised tenderness If clinical findings suggest isolated Grade 1-2 LCL injury Refer to physiotherapy for MCL injury rehabilitation program (ROM and strengthening work) If clinical findings suggest Grade 1-2 LCL injury + meniscal tear Refer MRI scan to investigate presence of meniscal tear If clinical findings suggest Grade 3 MCL injury, concurrent meniscal and other ligamentous involvement is likely May need referral for x- ray to exclude bony injury If clinical findings and MRI scan confirms symptomatic meniscal tear, refer for surgical opinion May also require referral to physiotherapy if limited ROM and muscle strength Refer for x- ray and MRI scan to investigate any concurrent injuries Refer for surgical opinion Referral for brace if knee is unstable Referral for physiotherapy if limited ROM and reduced muscle strength
16 Map of medicine suspected meniscal tear primary care management Degenerate-type meniscal tears Meniscal tears following acute injury Over 50yrs, x-ray (WB AP and lateral) In presence of mild to moderate OA changes, refer for surgical opinion if patient experiencing true locking and symptomatic In absence of true locking, see OA knee pathway In absence of OA changes refer for MRI scan Refer for MRI scan to confirm presence of meniscal tear and evaluate chondral changes Physiotherapy may be indicated if loss of muscle power and decreased ROM. If locked knee, or strong clinical suspicion of meniscal tear and symptomatic, refer directly on for surgical opinion Patient will require either x- ray or MRI prior to surgery If MRI scan confirms meniscal tear, and remains symptomatic, refer for surgical opinion Suspected symptomatic meniscal tear from history and examination, refer for MRI scan to confirm meniscal tear
17 Map of medicine patellofemoral OA primary care management Referred to Orthopaedic Choice X-rays within last 6/12 Weightbearing AP, lateral Early stage OA Physiotherapy to increase ROM, increase quadriceps power and help with pain management Advice re non-weight bearing activities Advice re pain control medication incl. NSAID s and analgesia Advice re weight-loss if appropriate Provision of OA knee information to patient Mid stage OA As for early stage if not already attempted Steroid injection if appropriate see appendix 1 Advanced OA As above if not already attempted Refer for surgical opinion if significant pain levels, affecting ADL and/or disturbed sleep. This is only following discussion with patient regarding pros and cons of surgery, surgical goals, expected recovery timescales. Patient should have completed shared decision making tool prior to referral X-rays skyline views if not already done Appendix 1 Steroid injection indications include acute flare-up of symptoms Cautions include Diabetes Contra-indications include Known hypersensitivity to local anaesthetic Local/systemic infection Tendon bodies and other classic avascular areas Unstable joints Tuberculosis Pregnancy and breast feeding Children under 18 Peripheral vascular disease Poor diabetic control HbA1/C > 8.5/9.0 Peptic ulcers active or history of peptic ulcer Prosthetic joint Recent trauma how recent? When? Spinal conditions Anticoagulant therapy Psychogenic disorders
18 Map of medicine tibiofemoral OA primary care management Referred to Orthopaedic Choice X-rays within last 6/12 Weightbearing AP, lateral Early stage OA Physiotherapy to increase ROM, increase quadriceps power and help with pain management Advice re non-weight bearing activities Advice re pain control medication incl. NSAID s and analgesia Advice re weight-loss if appropriate Possible offloading OA knee brace if appropriate Provision of OA knee information to patient Mid stage OA As for early stage if not already attempted Steroid injection if appropriate see appendix 1 Advanced OA As above if not already attempted Refer for surgical opinion if significant pain levels, affecting ADL and/or disturbed sleep. This is only following discussion with patient regarding pros and cons of surgery, surgical goals, expected recovery timescales. Patient should have completed shared decision making tool prior to referral X-rays skyline views if not already done Appendix 1 Steroid injection indications include acute flare-up of symptoms Cautions include Diabetes Contra-indications include Known hypersensitivity to local anaesthetic Local/systemic infection Tendon bodies and other classic avascular areas Unstable joints Tuberculosis Pregnancy and breast feeding Children under 18 Peripheral vascular disease Poor diabetic control HbA1/C > 8.5/9.0 Peptic ulcers active or history of peptic ulcer Prosthetic joint Recent trauma how recent? When? Spinal conditions Anticoagulant therapy Psychogenic disorders
19 Ankle Ankle injury pathway For advice on management of Ankle pain please follow link to Map of Medicine
20 Bursitis pathway Referred to Orthopaedic Choice DB July 2013 ITERMETATARSAL BURSITIS Advice re footwear - lower heel height, activity appropriate, good fit, appropriate fore sole Toe spring/ rocker sole footwear/ Thomas bar modification Assessment of foot and lower limb mechanics with provision of orthoses or offloading devices Advice re pain control medication incl. NSAIDs and analgesia If inflammatory arthropathy suspected, bloods and referral to rheumatology If not improving Ultrasound scan Ultrasound guided steroid injection if appropriate see appendix 1 If not improving RETRO-CALCANEAL BURSITIS Assessment of foot and lower limb mechanics, then provision of appropriate functional foot orthoses As above if not already undertaken Discussion with patient regarding risks/benefits of surgery and recovery timescales Refer for surgical opinion Appendix 1 Steroid injection indications include acute flare-up of symptoms Cautions include Diabetes Contra-indications include Known hypersensitivity to local anaesthetic Local/systemic infection Tendon bodies and other classic avascular areas Unstable joints Tuberculosis Pregnancy and breast feeding Children under 18 Peripheral vascular disease Poor diabetic control HbA1/C > 8.5/9.0 Peptic ulcers active or history of peptic ulcer Prosthetic joint Recent trauma how recent? When? Spinal conditions Anticoagulant therapy Psychogenic disorders
21 MTPJ capsulitis/ synovitis pathway Referred to Orthopaedic Choice DB July 2013 Advice re footwear - lower heel height, activity appropriate, good fit, appropriate fore sole Toe spring/ rocker sole footwear/ Thomas bar modification Assessment of foot and lower limb mechanics with provision of orthoses or offloading devices Advice re pain control medication incl. NSAIDs and analgesia Advice re appropriate stretches Advice re weight-loss if appropriate If not improving X-ray and/or ultrasound As above if not already undertaken Ultrasound guided steroid injection if appropriate see appendix 1 If not improving MRI scan As above if not already undertaken Discussion with patient regarding risks/benefits of surgery and recovery timescales Refer for surgical opinion if significant pain levels, affecting ADL and/or disturbed sleep Appendix 1 Steroid injection indications include acute flare-up of symptoms Cautions include Diabetes Contra-indications include Known hypersensitivity to local anaesthetic Local/systemic infection Tendon bodies and other classic avascular areas Unstable joints Tuberculosis Pregnancy and breast feeding Children under 18 Peripheral vascular disease Poor diabetic control HbA1/C > 8.5/9.0 Peptic ulcers active or history of peptic ulcer Prosthetic joint Recent trauma how recent? When? Spinal conditions Anticoagulant therapy Psychogenic disorders
22 Freiberg s/ avascular necrosis pathway Referred to Orthopaedic Choice Advice re footwear - lower heel height, activity appropriate, good fit, appropriate fore sole Toe spring/ rocker sole footwear/ Thomas bar modification Assessment of foot and lower limb mechanics with provision of orthoses or offloading devices Advice re pain control medication incl. NSAIDs and analgesia Advice re activity and pacing Advice re weight-loss if appropriate If not improving X-ray to exclude differential diagnoses and for classification (A to E, depending on severity) Short term immobilisation If not improving Discussion with patient regarding risks/benefits of surgery and recovery timescales Refer for surgical opinion re debridement/ removal of loose bodies / osteotomy if significant pain levels, affecting ADL and/or disturbed sleep DB July 2013
23 Sinus tarsi pathway Referred to Orthopaedic Choice Assessment of foot and lower limb mechanics and provision of appropriate functional foot orthoses Advice re footwear and activities (particularly running) Strengthening exercises / stretches Mobilisation DB July 2013 If not improving Ultrasound scan Ultrasound guided steroid injection if appropriate see appendix 1 If not improving MRI scan As above if not already undertaken Discussion with patient regarding risks/benefits of surgery and recovery timescales Refer for surgical opinion Appendix 1 Steroid injection indications include acute flare-up of symptoms Cautions include Diabetes Contra-indications include Known hypersensitivity to local anaesthetic Local/systemic infection Tendon bodies and other classic avascular areas Unstable joints Tuberculosis Pregnancy and breast feeding Children under 18 Peripheral vascular disease Poor diabetic control HbA1/C > 8.5/9.0 Peptic ulcers active or history of peptic ulcer Prosthetic joint Recent trauma how recent? When? Spinal conditions Anticoagulant therapy Psychogenic disorders
24 Tarsal tunnel pathway Referred to Orthopaedic Choice DB July 2013 Assessment of foot and lower limb mechanics and provision of appropriate functional foot orthoses Rest /ice Advice re footwear and activities Advice re pain control medication incl. NSAIDs and analgesia Strengthening exercises / stretches If not improving MRI / Nerve conduction studies Period of immobilisation Ultrasound guided steroid injection if appropriate see appendix 1 If not improving MRI scan As above if not already undertaken Discussion with patient regarding risks/benefits of surgery and recovery timescales Refer for surgical opinion re decompression Appendix 1 Steroid injection indications include acute flare-up of symptoms Cautions include Diabetes Contra-indications include Known hypersensitivity to local anaesthetic Local/systemic infection Tendon bodies and other classic avascular areas Unstable joints Tuberculosis Pregnancy and breast feeding Children under 18 Peripheral vascular disease Poor diabetic control HbA1/C > 8.5/9.0 Peptic ulcers active or history of peptic ulcer Prosthetic joint Recent trauma how recent? When? Spinal conditions Anticoagulant therapy Psychogenic disorders
25 Charcot arthropathy pathway ACTIVE, WARM AND/OR SWOLLEN CHARCOT FOOT Limb threatening emergency; urgent referral to orthopaedics and diabetic foot team for immediate immobilisation, with possible admission and IV medication. Active phase resolved INACTIVE, COOL BURNT OUT CHARCOT FOOT If not already done, refer to diabetic foot team Referral to orthopaedic choice Foot protection measures including offloading orthoses and accommodative footwear, bespoke if required. Protection measures for contralateral foot. DB May 2013
26 Hallux Rigidus pathway Referred to Orthopaedic Choice STRUCTURAL HALLUX RIGIDUS If conservative option needed or chosen by patient: Orthoses with forefoot extension Footwear with toe spring feature Advice re activity FUNCTIONAL HALLUX RIGIDUS Assessment of foot and lower limb mechanics, then provision of appropriate functional foot orthoses DB July 2013 If not improving X-ray Intra-articular ultrasound guided steroid injection if appropriate see appendix 1 If not improving As above if not already undertaken Discussion with patient regarding risks/benefits of surgery and recovery timescales Refer for surgical opinion re cheilectomy/ arthrodesis if significant pain levels, affecting ADL and/or disturbed sleep Appendix 1 Steroid injection indications include acute flare-up of symptoms Cautions include Diabetes Contra-indications include Known hypersensitivity to local anaesthetic Local/systemic infection Tendon bodies and other classic avascular areas Unstable joints Tuberculosis Pregnancy and breast feeding Children under 18 Peripheral vascular disease Poor diabetic control HbA1/C > 8.5/9.0 Peptic ulcers active or history of peptic ulcer Prosthetic joint Recent trauma how recent? When? Spinal conditions Anticoagulant therapy Psychogenic disorders
27 Digital deformity/contracture pathway Referred to Orthopaedic Choice FLEXIBLE DEFORMITY Orthodigital splinting Orthoses to influence forefoot and digital alignment Advice re pain control medication incl. NSAIDs and analgesia RIGID DEFORMITY Pressure deflective /palliative devices Extra depth/ modified footwear Advice re pain control medication incl. NSAIDs and analgesia DB July 2013 If not improving X-ray As above if not already undertaken Intra-articular ultrasound guided steroid injection if appropriate see appendix 1 If not improving As above if not already undertaken Discussion with patient regarding risks/benefits of surgery and recovery timescales Refer for surgical opinion re tendon lengthening or release/ cheilectomy/ excisional arthroplasty/ arthrodesis if significant pain levels, affecting ADL and/or disturbed sleep Appendix 1 Steroid injection indications include acute flare-up of symptoms Cautions include Diabetes Contra-indications include Known hypersensitivity to local anaesthetic Local/systemic infection Tendon bodies and other classic avascular areas Unstable joints Tuberculosis Pregnancy and breast feeding Children under 18 Peripheral vascular disease Poor diabetic control HbA1/C > 8.5/9.0 Peptic ulcers active or history of peptic ulcer Prosthetic joint Recent trauma how recent? When? Spinal conditions Anticoagulant therapy Psychogenic disorders

28 Low Back pain & Sciatica Low Back pain and radicular pathway


29 Neck Pain Neck pain pathway This includes;

30 Spinal Stenosis
31 Osteoporosis Spinal fracture This is not appropriate for Orthopaedic Choice Please see Map of Medicine pathway. Osteoporosis pathway
Dupuytrens contracture
 OA Wrist Ganglion/Cysts Dupuytrens contracture Carpal Tunnel Syndrome Carpal Tunnel pathway For advice on management of CTS please follow link to Map of Medicine Trigger Finger Trigger finger pathway For
OA Wrist Ganglion/Cysts Dupuytrens contracture Carpal Tunnel Syndrome Carpal Tunnel pathway For advice on management of CTS please follow link to Map of Medicine Trigger Finger Trigger finger pathway For
On Field Assessment and Management of Acute Knee Injuries: A Physiotherapist s Perspective
 On Field Assessment and Management of Acute Knee Injuries: A Physiotherapist s Perspective Jessica Condliffe Physiotherapist / Clinic Manager TBI Health Wellington Presentation Outline Knee anatomy review
On Field Assessment and Management of Acute Knee Injuries: A Physiotherapist s Perspective Jessica Condliffe Physiotherapist / Clinic Manager TBI Health Wellington Presentation Outline Knee anatomy review
An older systematic review looked at the evidence behind the best approach to evaluate acute knee pain in primary care (Ann Int Med.2003;139:575).
.") There is so much we don't know in medicine that could make a difference, and often we focus on the big things, and the little things get forgotten. To highlight some smaller but important issues, we've
There is so much we don't know in medicine that could make a difference, and often we focus on the big things, and the little things get forgotten. To highlight some smaller but important issues, we've
ACL Athletic Career. ACL Rupture - Warning Features Intensive pain Immediate swelling Locking Feel a Pop Dead leg Cannot continue to play
 FIMS Ambassador Tour to Eastern Europe, 2004 Belgrade, Serbia Montenegro Acute Knee Injuries - Controversies and Challenges Professor KM Chan OBE, JP President of FIMS Belgrade ACL Athletic Career ACL
FIMS Ambassador Tour to Eastern Europe, 2004 Belgrade, Serbia Montenegro Acute Knee Injuries - Controversies and Challenges Professor KM Chan OBE, JP President of FIMS Belgrade ACL Athletic Career ACL
SOFT TISSUE KNEE INJURIES
 SOFT TISSUE KNEE INJURIES Soft tissue injuries of the knee commonly occur in all sports or in any activity that requires sudden changes in activity or movement. The knee is a complex joint and any injury
SOFT TISSUE KNEE INJURIES Soft tissue injuries of the knee commonly occur in all sports or in any activity that requires sudden changes in activity or movement. The knee is a complex joint and any injury
Diagnosis and Management of Knee Conditions. Jenny Love / Lynn Robertson AFLAR Oct 2009
 Diagnosis and Management of Knee Conditions Jenny Love / Lynn Robertson AFLAR Oct 2009 AIMS Review 4 common Knee Conditions: Anterior knee pain Meniscal Injuries Ligament injuries ACL Osteoarthritis Discuss
Diagnosis and Management of Knee Conditions Jenny Love / Lynn Robertson AFLAR Oct 2009 AIMS Review 4 common Knee Conditions: Anterior knee pain Meniscal Injuries Ligament injuries ACL Osteoarthritis Discuss
Evaluation of the Knee and Shoulder
 Evaluation of the Knee and Shoulder Karen J. Boselli, MD Northeast Regional Nurse Practitioner Conference May 2018 Knee Overview History Examination Top 5 diagnoses When to image When to refer Pain most
Evaluation of the Knee and Shoulder Karen J. Boselli, MD Northeast Regional Nurse Practitioner Conference May 2018 Knee Overview History Examination Top 5 diagnoses When to image When to refer Pain most
6/5/2018. The Management of Shoulder Conditions in Primary Care. Mr Rupen Dattani (FRCS (Tr & Orth) Consultant Shoulder & Elbow Surgeon
 Consultant Shoulder & Elbow Surgeon") The Management of Shoulder Conditions in Primary Care Mr Rupen Dattani (FRCS (Tr & Orth) Consultant Shoulder & Elbow Surgeon Highgate Private Hospital (Chelsea & Westminster Hospital NHS Foundation Trust)
The Management of Shoulder Conditions in Primary Care Mr Rupen Dattani (FRCS (Tr & Orth) Consultant Shoulder & Elbow Surgeon Highgate Private Hospital (Chelsea & Westminster Hospital NHS Foundation Trust)
Salisbury Foundation Trust Radiology Department Referral Guidelines for Primary Care: Musculoskeletal Imaging
 Salisbury Foundation Trust Radiology Department Referral Guidelines for Primary Care: Musculoskeletal Imaging These guidelines have been issued in conjunction with the Royal College of Radiology referral
Salisbury Foundation Trust Radiology Department Referral Guidelines for Primary Care: Musculoskeletal Imaging These guidelines have been issued in conjunction with the Royal College of Radiology referral
W. Dilworth Cannon, M.D. Professor of Clinical Orthopaedic Surgery University of California San Francisco
 Knee Pain And Injuries In Adults W. Dilworth Cannon, M.D. Professor of Clinical Orthopaedic Surgery University of California San Francisco Pain Control Overview Narcotics rarely necessary after 1 st 1-2
Knee Pain And Injuries In Adults W. Dilworth Cannon, M.D. Professor of Clinical Orthopaedic Surgery University of California San Francisco Pain Control Overview Narcotics rarely necessary after 1 st 1-2
SOFT TISSUE INJURIES OF THE KNEE: Primary Care and Orthopaedic Management
 SOFT TISSUE INJURIES OF THE KNEE: Primary Care and Orthopaedic Management Gauguin Gamboa Australia has always been a nation where emphasis on health and fitness has resulted in an active population engaged
SOFT TISSUE INJURIES OF THE KNEE: Primary Care and Orthopaedic Management Gauguin Gamboa Australia has always been a nation where emphasis on health and fitness has resulted in an active population engaged
Kineto. Orthopaedics & Rehabilitation Products
 Member of Vincent Medical Holdings Limited Kineto Orthopaedics & Rehabilitation Products Our orthopaedic and rehabilitation products comprise of a variety of adjustable rehabilitation braces for support,
Member of Vincent Medical Holdings Limited Kineto Orthopaedics & Rehabilitation Products Our orthopaedic and rehabilitation products comprise of a variety of adjustable rehabilitation braces for support,
Rotator Cuff Pathology. Shoulder Instability. Adhesive Capsulitis. AC Joint Dysfunction
 Shoulder Pain Red Flags Unexplained deformity or swelling Significant weakness not due to pain Suspected malignancy Fever/chills/malaise Significant/unexplained sensory/motor deficit Pulmonary or vascular
Shoulder Pain Red Flags Unexplained deformity or swelling Significant weakness not due to pain Suspected malignancy Fever/chills/malaise Significant/unexplained sensory/motor deficit Pulmonary or vascular
Common Elbow Problems
 Common Elbow Problems Duncan Ferguson FRACS Knee and Shoulder Specialist Elbow Instability Common 10-25% of elbow injuries Median age 30 yrs Most simple dislocations are stable after reduction recurrence
Common Elbow Problems Duncan Ferguson FRACS Knee and Shoulder Specialist Elbow Instability Common 10-25% of elbow injuries Median age 30 yrs Most simple dislocations are stable after reduction recurrence
SERVICES. Contact us. Rapid Assessment, Intervention and Treatment
 Contact us For more information about Orthopaedic Services, please visit our website at www.londonbridgehospital.com or contact: GP Liaison Department Tel: +44 (0)20 7234 2009 Fax: +44 (0)20 7234 2019
Contact us For more information about Orthopaedic Services, please visit our website at www.londonbridgehospital.com or contact: GP Liaison Department Tel: +44 (0)20 7234 2009 Fax: +44 (0)20 7234 2019
Physical Examination of the Knee
 History: Pain Traumatic vs. atraumatic Acute vs Chronic Mechanism of injury Swelling, catching, instability Previous evaluation and treatment General Setup Examine standing, sitting and supine Evaluate
History: Pain Traumatic vs. atraumatic Acute vs Chronic Mechanism of injury Swelling, catching, instability Previous evaluation and treatment General Setup Examine standing, sitting and supine Evaluate
The examination of the painful knee. Maja K Artandi, MD, FACP Clinical Associate Professor of Medicine Stanford University
 The examination of the painful knee Maja K Artandi, MD, FACP Clinical Associate Professor of Medicine Stanford University Objectives of the talk By the end of this talk you will know The important anatomy
The examination of the painful knee Maja K Artandi, MD, FACP Clinical Associate Professor of Medicine Stanford University Objectives of the talk By the end of this talk you will know The important anatomy
VSRF+ Orthopaedics Referral Form. Triage Categories/ Appointment Wait Time Emergency/After Hours:
 Northern Health Orthopaedic Pre referral Management Guidelines Orthopaedic Consultants: Mr A. Bonomo Mr R. Hau Mr A. Chia Mr D. Robin Ms J. Gentle Mr A. Chehata Mr R. Unni Osteoarthritis Hip & Knee Service
Northern Health Orthopaedic Pre referral Management Guidelines Orthopaedic Consultants: Mr A. Bonomo Mr R. Hau Mr A. Chia Mr D. Robin Ms J. Gentle Mr A. Chehata Mr R. Unni Osteoarthritis Hip & Knee Service
- within 16 weeks. Semi-urgent - within 8 weeks
 National Access Criteria for First Specialist Assessment Category Definitions: These are recommended guidelines for HHS specialists prioritizing referrals from primary care Immediate - within 1 week Urgent
National Access Criteria for First Specialist Assessment Category Definitions: These are recommended guidelines for HHS specialists prioritizing referrals from primary care Immediate - within 1 week Urgent
Clinical Musculoskeletal Assessment and Treatment Service (CMATS) pathway
 pathway") Pathway Clinical Musculoskeletal Assessment and Treatment Service (CMATS) pathway Patient aged 16 years and over presents to GP with symptoms of knee, shoulder or spinal pain Present Screen for: Emergency
Pathway Clinical Musculoskeletal Assessment and Treatment Service (CMATS) pathway Patient aged 16 years and over presents to GP with symptoms of knee, shoulder or spinal pain Present Screen for: Emergency
Physical Examination of the Knee
 History: Pain Traumatic vs. atraumatic? Acute vs Chronic Previous procedures done on the knee? Swelling, catching, instability General Setup Examine standing, sitting and supine Evaluate gait Examine hip
History: Pain Traumatic vs. atraumatic? Acute vs Chronic Previous procedures done on the knee? Swelling, catching, instability General Setup Examine standing, sitting and supine Evaluate gait Examine hip
Anterior Cruciate Ligament (ACL)
") Anterior Cruciate Ligament (ACL) The anterior cruciate ligament (ACL) is one of the 4 major ligament stabilizers of the knee. ACL tears are among the most common major knee injuries in active people of
Anterior Cruciate Ligament (ACL) The anterior cruciate ligament (ACL) is one of the 4 major ligament stabilizers of the knee. ACL tears are among the most common major knee injuries in active people of
Knee Injuries. PSK 4U Mr. S. Kelly North Grenville DHS. Medial Collateral Ligament Sprain
 Knee Injuries PSK 4U Mr. S. Kelly North Grenville DHS Medial Collateral Ligament Sprain Result from either a direct blow from the lateral side in a medial direction or a severe outward twist Greater injury
Knee Injuries PSK 4U Mr. S. Kelly North Grenville DHS Medial Collateral Ligament Sprain Result from either a direct blow from the lateral side in a medial direction or a severe outward twist Greater injury
Foot and ankle update
 Foot and ankle update Mr Ian Garnham Consultant Foot and Ankle Surgeon Whipps Cross University Hospital Hallux Rigidus Symptoms first ray and 1st MTP pain and swelling worse with push off or forced dorsiflexion
Foot and ankle update Mr Ian Garnham Consultant Foot and Ankle Surgeon Whipps Cross University Hospital Hallux Rigidus Symptoms first ray and 1st MTP pain and swelling worse with push off or forced dorsiflexion
ACL AND PCL INJURIES OF THE KNEE JOINT
 ACL AND PCL INJURIES OF THE KNEE JOINT Dr.KN Subramanian M.Ch Orth., FRCS (Tr & Orth), CCT Orth(UK) Consultant Orthopaedic Surgeon, Special interest: Orthopaedic Sports Injury, Shoulder and Knee Surgery,
ACL AND PCL INJURIES OF THE KNEE JOINT Dr.KN Subramanian M.Ch Orth., FRCS (Tr & Orth), CCT Orth(UK) Consultant Orthopaedic Surgeon, Special interest: Orthopaedic Sports Injury, Shoulder and Knee Surgery,
SMF PCP Treatment & Referral Guideline Orthopedics Developed February 1, 2003 Revised: October, 2011
 SUTTER MEDICAL FOUNDATION (SMF) 2800 L Street, 7 th Floor Sacramento, CA 95816 SMF PCP Treatment & Referral Guideline Orthopedics Developed February 1, 2003 Revised: October, 2011 I. Shoulder Pain...Page
SUTTER MEDICAL FOUNDATION (SMF) 2800 L Street, 7 th Floor Sacramento, CA 95816 SMF PCP Treatment & Referral Guideline Orthopedics Developed February 1, 2003 Revised: October, 2011 I. Shoulder Pain...Page
Musculoskeletal Referral Guidelines
 Musculoskeletal Referral Guidelines Introduction These guidelines have been developed to provide an integrated musculoskeletal service. They are based on reasonable clinical practice and will initially
Musculoskeletal Referral Guidelines Introduction These guidelines have been developed to provide an integrated musculoskeletal service. They are based on reasonable clinical practice and will initially
Evaluation and Management of Knee Pain. Michael Cassat, MD University of Arkansas for Medical Sciences
 Evaluation and Management of Knee Pain Michael Cassat, MD University of Arkansas for Medical Sciences Disclosure I have no actual or potential conflict of interest in relation to this program/presentation.
Evaluation and Management of Knee Pain Michael Cassat, MD University of Arkansas for Medical Sciences Disclosure I have no actual or potential conflict of interest in relation to this program/presentation.
Diagnostic and Management Approach to the Painful Shoulder
 Diagnostic and Management Approach to the Painful Shoulder Introduction What conditions causing shoulder pain commonly present in General Practice? Subacromial impingement Rotator cuff tears AC joint pathology
Diagnostic and Management Approach to the Painful Shoulder Introduction What conditions causing shoulder pain commonly present in General Practice? Subacromial impingement Rotator cuff tears AC joint pathology
Nursing Management: Musculoskeletal Trauma and Orthopedic Surgery. By: Aun Lauriz E. Macuja SAC_SN4
 Nursing Management: Musculoskeletal Trauma and Orthopedic Surgery By: Aun Lauriz E. Macuja SAC_SN4 The most common cause of musculoskeletal injuries is a traumatic event resulting in fracture, dislocation,
Nursing Management: Musculoskeletal Trauma and Orthopedic Surgery By: Aun Lauriz E. Macuja SAC_SN4 The most common cause of musculoskeletal injuries is a traumatic event resulting in fracture, dislocation,
Overview Ligament Injuries. Anatomy. Epidemiology Very commonly injured joint. ACL Injury 20/06/2016. Meniscus Tears. Patellofemoral Problems
 Overview Ligament Injuries Meniscus Tears Pankaj Sharma MBBS, FRCS (Tr & Orth) Consultant Orthopaedic Surgeon Manchester Royal Infirmary Patellofemoral Problems Knee Examination Anatomy Epidemiology Very
Overview Ligament Injuries Meniscus Tears Pankaj Sharma MBBS, FRCS (Tr & Orth) Consultant Orthopaedic Surgeon Manchester Royal Infirmary Patellofemoral Problems Knee Examination Anatomy Epidemiology Very
Primary care referral criteria for musculoskeletal MRI scans
 Appendix 1 Primary care referral criteria for musculoskeletal MRI scans Accepted Criteria for Direct Access MRI Body Part Symptoms Imaging indicated Lumbar Spine Low Back Pain with adverse symptoms or
Appendix 1 Primary care referral criteria for musculoskeletal MRI scans Accepted Criteria for Direct Access MRI Body Part Symptoms Imaging indicated Lumbar Spine Low Back Pain with adverse symptoms or
ASSESSMENT AND MANAGEMENT OF THE KNEE AND LOWER LIMB.
 ASSESSMENT AND MANAGEMENT OF THE KNEE AND LOWER LIMB www.fisiokinesiterapia.biz Overview History Examination X-rays Fractures and Dislocations. Soft Tissue Injuries Other Knee/Lower limb Problems Anatomy
ASSESSMENT AND MANAGEMENT OF THE KNEE AND LOWER LIMB www.fisiokinesiterapia.biz Overview History Examination X-rays Fractures and Dislocations. Soft Tissue Injuries Other Knee/Lower limb Problems Anatomy
REFERRAL GUIDELINES: ORTHOPAEDIC SURGERY
 All patients referred to specialist clinics are assigned to a priority category based on their clinical need and related psychosocial factors. The examples given are indicative only and the clinician reviewing
All patients referred to specialist clinics are assigned to a priority category based on their clinical need and related psychosocial factors. The examples given are indicative only and the clinician reviewing
Priorities Forum Statement GUIDANCE
 Priorities Forum Statement Number 21 Subject Knee Arthroscopy including arthroscopic knee washouts Date of decision November 2016 Date refreshed March 2017 Date of review November 2018 Osteoarthritis of
Priorities Forum Statement Number 21 Subject Knee Arthroscopy including arthroscopic knee washouts Date of decision November 2016 Date refreshed March 2017 Date of review November 2018 Osteoarthritis of
Trauma & Orthopaedic Undergraduate Syllabus
 Trauma & Orthopaedic Undergraduate Syllabus Introduction The purpose of this document is to provide a recommended syllabus for medical students in Trauma & Orthopaedics (T&0). It should help students on
Trauma & Orthopaedic Undergraduate Syllabus Introduction The purpose of this document is to provide a recommended syllabus for medical students in Trauma & Orthopaedics (T&0). It should help students on
Welcome to White Rock Orthopaedic Surgery Centre
 White Rock Orthopaedic Surgery Excellence in Orthopaedic Surgery since 2008 Over 700 surgical cases (spring of 2013) Fully Accredited Class-1 Facility Expedient initial assessment Secure, online registration
White Rock Orthopaedic Surgery Excellence in Orthopaedic Surgery since 2008 Over 700 surgical cases (spring of 2013) Fully Accredited Class-1 Facility Expedient initial assessment Secure, online registration
Musculoskeletal Examination Benchmarks
 Musculoskeletal Examination Benchmarks _ The approach to examining the musculoskeletal system is the same no matter what joint or limb is being examined. The affected and contralateral region should both
Musculoskeletal Examination Benchmarks _ The approach to examining the musculoskeletal system is the same no matter what joint or limb is being examined. The affected and contralateral region should both
Exclude referred pain from the neck, diaphragm, heart, lungs, & polymyalgia rheumatica YES. NSAIDs/analgesics as required
 Shoulder Pain Clinical Presentation info for GPs who refer into PAH more info History and Examination Exclude referred pain from the neck, diaphragm, heart, lungs, & polymyalgia rheumatica more info for
Shoulder Pain Clinical Presentation info for GPs who refer into PAH more info History and Examination Exclude referred pain from the neck, diaphragm, heart, lungs, & polymyalgia rheumatica more info for
KNEE EXAMINATION. Tips & Tricks from an Emergency Physician Perspective. EM Physicians Less Exposed to MSK Medicine
 KNEE EXAMINATION Tips & Tricks from an Emergency Physician Perspective Dr P O CONNOR Emergency Medicine Physician EUSEM 10/09/2018 EM Physicians Less Exposed to MSK Medicine Musculoskeletal Medicine becoming
KNEE EXAMINATION Tips & Tricks from an Emergency Physician Perspective Dr P O CONNOR Emergency Medicine Physician EUSEM 10/09/2018 EM Physicians Less Exposed to MSK Medicine Musculoskeletal Medicine becoming
 www.fisiokinesiterapia.biz Shoulder Problems Fractures Instability Impingement Miscellaneous Anatomy Bones Joints / Ligaments Muscles Neurovascular Anatomy Anatomy Supraspinatus Anterior Posterior Anatomy
www.fisiokinesiterapia.biz Shoulder Problems Fractures Instability Impingement Miscellaneous Anatomy Bones Joints / Ligaments Muscles Neurovascular Anatomy Anatomy Supraspinatus Anterior Posterior Anatomy
Your Orthotics service is changing
 Your Orthotics service is changing Important for referrers on changes effective from January 2015 Why is the service changing? As demand for the orthotics service increases and budgets remain relatively
Your Orthotics service is changing Important for referrers on changes effective from January 2015 Why is the service changing? As demand for the orthotics service increases and budgets remain relatively
Your Orthotics service is changing
 Your Orthotics service is changing Important information for service users on changes effective from July 2015 Why is the service changing? As demand for the Orthotics service increases, Livewell Southwest
Your Orthotics service is changing Important information for service users on changes effective from July 2015 Why is the service changing? As demand for the Orthotics service increases, Livewell Southwest
Treatment of Acute Traumatic Knee Dislocations
 Treatment of Acute Traumatic Knee Dislocations Angelo J. Colosimo, MD Head Orthopaedic Surgeon University of Cincinnati Athletics Director of Sports Medicine University of Cincinnati Medical Center Associate
Treatment of Acute Traumatic Knee Dislocations Angelo J. Colosimo, MD Head Orthopaedic Surgeon University of Cincinnati Athletics Director of Sports Medicine University of Cincinnati Medical Center Associate
Treatment of Acute Traumatic Knee Dislocations
 Treatment of Acute Traumatic Knee Dislocations Angelo J. Colosimo, MD Head Orthopaedic Surgeon University of Cincinnati Athletics Director of Sports Medicine University of Cincinnati Medical Center Associate
Treatment of Acute Traumatic Knee Dislocations Angelo J. Colosimo, MD Head Orthopaedic Surgeon University of Cincinnati Athletics Director of Sports Medicine University of Cincinnati Medical Center Associate
Page 1 of 6. Appendix 1
 Page 1 Appendix 1 Rotation Objectives and Schedule 1. Introductory Month 4 weeks 2. Total Joints 4 weeks a. Diagnosis and management of hip and knee arthritis b. Indications for surgery c. Implant selection;
Page 1 Appendix 1 Rotation Objectives and Schedule 1. Introductory Month 4 weeks 2. Total Joints 4 weeks a. Diagnosis and management of hip and knee arthritis b. Indications for surgery c. Implant selection;
CHRONIC FOOT PROBLEMS FOOT and ANKLE BASICS
 CHRONIC FOOT PROBLEMS FOOT and ANKLE BASICS ABC s of Comprehensive Musculoskeletal Care December 1 st, 2007 Stephen Pinney MD Chief, UCSF Foot and Ankle Service Chronic problems typically occur gradually
CHRONIC FOOT PROBLEMS FOOT and ANKLE BASICS ABC s of Comprehensive Musculoskeletal Care December 1 st, 2007 Stephen Pinney MD Chief, UCSF Foot and Ankle Service Chronic problems typically occur gradually
Management of Chronic Elbow Pain
 Mr. Nashat Siddiqui Consultant Upper Limb Orthopaedic Surgeon Management of Chronic Elbow Pain Patients presenting with elbow pain can pose a diagnostic challenge, especially if there is no obvious recent
Mr. Nashat Siddiqui Consultant Upper Limb Orthopaedic Surgeon Management of Chronic Elbow Pain Patients presenting with elbow pain can pose a diagnostic challenge, especially if there is no obvious recent
Orthopaedic (Ankles & Feet) Referral Guidelines
 Referral Guidelines") Orthopaedic (Ankles & Feet) Referral Guidelines Austin Health Orthopaedic Clinic holds weekly multidisciplinary meetings to discuss and plan the treatment of patients with Orthopaedic and Fracture conditions.
Orthopaedic (Ankles & Feet) Referral Guidelines Austin Health Orthopaedic Clinic holds weekly multidisciplinary meetings to discuss and plan the treatment of patients with Orthopaedic and Fracture conditions.
5 COMMON CONDITIONS IN THE FOOT & ANKLE
 5 COMMON CONDITIONS IN THE FOOT & ANKLE MICHAEL P. CLARE, MD FLORIDA ORTHOPAEDIC INSTITUTE TAMPA, FL USA IN A NUTSHELL ~ ALL ANATOMY & BIOMECHANICS >90% OF CONDITIONS IN FOOT & ANKLE DIAGNISED FROM GOOD
5 COMMON CONDITIONS IN THE FOOT & ANKLE MICHAEL P. CLARE, MD FLORIDA ORTHOPAEDIC INSTITUTE TAMPA, FL USA IN A NUTSHELL ~ ALL ANATOMY & BIOMECHANICS >90% OF CONDITIONS IN FOOT & ANKLE DIAGNISED FROM GOOD
I have nothing to disclose
 Management of Common Knee Disorders: What You Knee d to Know UCSF Essentials of Women s Health July 8, 2015 Carlin Senter, M.D. I have nothing to disclose Learning objectives: in 1 hour you will be able
Management of Common Knee Disorders: What You Knee d to Know UCSF Essentials of Women s Health July 8, 2015 Carlin Senter, M.D. I have nothing to disclose Learning objectives: in 1 hour you will be able
Recognizing common injuries to the lower extremity
 Recognizing common injuries to the lower extremity Bones Femur Patella Tibia Tibial Tuberosity Medial Malleolus Fibula Lateral Malleolus Bones Tarsals Talus Calcaneus Metatarsals Phalanges Joints - Knee
Recognizing common injuries to the lower extremity Bones Femur Patella Tibia Tibial Tuberosity Medial Malleolus Fibula Lateral Malleolus Bones Tarsals Talus Calcaneus Metatarsals Phalanges Joints - Knee
Sports Medicine Unit 16 Elbow
 Sports Medicine Unit 16 Elbow I. Bones a. b. c. II. What movements does the elbow perform? a. Flexion b. c. Pronation d. III. Muscles in motion a. FLEXION (supinated) i Brachialis (pronated) ii (neutral)
Sports Medicine Unit 16 Elbow I. Bones a. b. c. II. What movements does the elbow perform? a. Flexion b. c. Pronation d. III. Muscles in motion a. FLEXION (supinated) i Brachialis (pronated) ii (neutral)
Humber NHS Foundation Trust. Joint Effort
 Joint Joint is a new community based musculoskeletal service that treats patients with complex problems of the spine, upper and lower limb. Joint s experienced Consultant Orthopaedic Surgeons and Extended
Joint Joint is a new community based musculoskeletal service that treats patients with complex problems of the spine, upper and lower limb. Joint s experienced Consultant Orthopaedic Surgeons and Extended
Goals &Objectives. 1. Review the anatomy of the knee 2. Practice your hands-on skills 3. By the end of the workshop:
 Clinical Knee Exam Goals &Objectives 1. Review the anatomy of the knee 2. Practice your hands-on skills 3. By the end of the workshop: Be able to categorize knee injuries Understand the significance of
Clinical Knee Exam Goals &Objectives 1. Review the anatomy of the knee 2. Practice your hands-on skills 3. By the end of the workshop: Be able to categorize knee injuries Understand the significance of
Knee Dislocation: Spectrum of Injury, Evolution of Treatment & Modern Outcomes
 Knee Dislocation: Spectrum of Injury, Evolution of Treatment & Modern Outcomes William M Weiss, MD MSc FRCSC Orthopedic Surgery & Rehabilitation Sports Medicine, Arthroscopy & Extremity Reconstruction
Knee Dislocation: Spectrum of Injury, Evolution of Treatment & Modern Outcomes William M Weiss, MD MSc FRCSC Orthopedic Surgery & Rehabilitation Sports Medicine, Arthroscopy & Extremity Reconstruction
COMMON KNEE AND SHOULDER INJURIES IN THE YOUNG ATHLETE. Outline 5/11/2017
 COMMON KNEE AND SHOULDER INJURIES IN THE YOUNG ATHLETE IRVING RAPHAEL MD Syracuse Orthopedic Specialists Former S.U. Head Team Physician May 19, 2017 Meniscal Injuries anatomy Exam Treatment ACL Injuries
COMMON KNEE AND SHOULDER INJURIES IN THE YOUNG ATHLETE IRVING RAPHAEL MD Syracuse Orthopedic Specialists Former S.U. Head Team Physician May 19, 2017 Meniscal Injuries anatomy Exam Treatment ACL Injuries
Lateral knee injuries
 Created as a free resource by Clinical Edge Based on Physio Edge podcast episode 051 with Matt Konopinski Get your free trial of online Physio education at Orthopaedic timeframes Traditionally Orthopaedic
Created as a free resource by Clinical Edge Based on Physio Edge podcast episode 051 with Matt Konopinski Get your free trial of online Physio education at Orthopaedic timeframes Traditionally Orthopaedic
Mr. Duy Thai Orthopaedic Surgeon, Melbourne VIC
 Mr. Duy Thai Orthopaedic Surgeon, Melbourne VIC International Convention of the Vietnamese Physicians, Dentists and Pharmacists of the Free World Melbourne 8 10 August 2014 Conflict of Interest None Subacromial
Mr. Duy Thai Orthopaedic Surgeon, Melbourne VIC International Convention of the Vietnamese Physicians, Dentists and Pharmacists of the Free World Melbourne 8 10 August 2014 Conflict of Interest None Subacromial
Common Foot and Ankle Pathology DOTS 17th April Nick Savva Orthopaedic Foot and Ankle Surgeon. Monday, 29 April 13
 Common Foot and Ankle Pathology DOTS 17th April 2013 Nick Savva Orthopaedic Foot and Ankle Surgeon Monday, 29 April 13 Topics Forefoot pain Hindfoot/Ankle pain Hallux rigidus Bunions Toe deformity Mortons
Common Foot and Ankle Pathology DOTS 17th April 2013 Nick Savva Orthopaedic Foot and Ankle Surgeon Monday, 29 April 13 Topics Forefoot pain Hindfoot/Ankle pain Hallux rigidus Bunions Toe deformity Mortons
RN(EC) ENC(C) GNC(C) MN ACNP *** MECHANISM OF INJURY.. MOST IMPORTANT *** - Useful in determining mechanism of injury / overuse
 ENC(C) GNC(C) MN ACNP *** MECHANISM OF INJURY.. MOST IMPORTANT *** - Useful in determining mechanism of injury / overuse") HISTORY *** MECHANISM OF INJURY.. MOST IMPORTANT *** Age of patient Sport / Occupation - Certain conditions are more prevalent in particular age groups (Osgood Schlaters in youth / Degenerative Joint Disease
HISTORY *** MECHANISM OF INJURY.. MOST IMPORTANT *** Age of patient Sport / Occupation - Certain conditions are more prevalent in particular age groups (Osgood Schlaters in youth / Degenerative Joint Disease
NORTH BAY SYMPOSIUM SATURDAY JANUARY 20 TH 2018
 NORTH BAY SYMPOSIUM SATURDAY JANUARY 20 TH 2018 ROBERT HAIMSON, M.D. ORTHOPEDIC SURGEON SMGR FELLOW IN AAOS DIPLOMATE IN ABOS COMMON MUSCULOSKELETAL CONDITIONS COMMON MUSCULOSKELETAL CONDITIONS: WHAT
NORTH BAY SYMPOSIUM SATURDAY JANUARY 20 TH 2018 ROBERT HAIMSON, M.D. ORTHOPEDIC SURGEON SMGR FELLOW IN AAOS DIPLOMATE IN ABOS COMMON MUSCULOSKELETAL CONDITIONS COMMON MUSCULOSKELETAL CONDITIONS: WHAT
BCCH Emergency Department LOWER LIMB INJURIES Resource pack
 1 BCCH Emergency Department LOWER LIMB INJURIES Resource pack Developed by: Rena Heathcote RN. 2 Knee Injuries The knee joint consists of a variety of structures including: 3 bones (excluding the patella)
1 BCCH Emergency Department LOWER LIMB INJURIES Resource pack Developed by: Rena Heathcote RN. 2 Knee Injuries The knee joint consists of a variety of structures including: 3 bones (excluding the patella)
Impingement syndrome. Clinical features. Management. Rotator cuff tear diagnosed. Go to rotator cuff tear
 Impingement syndrome Clinical features Management Poor response Good response Refer to orthopaedic surgery R Review as appropriate Investigations Rotator cuff tear diagnosed Go to rotator cuff tear Consider
Impingement syndrome Clinical features Management Poor response Good response Refer to orthopaedic surgery R Review as appropriate Investigations Rotator cuff tear diagnosed Go to rotator cuff tear Consider
WEEKLY CLINICAL SCHEDULES. Martin Boyer (hand surgery) Monday Tuesday Wednesday Thursday Friday AM PM AM PM AM PM AM PM AM PM Academic
 Monday Tuesday Wednesday Thursday Friday AM PM AM PM AM PM AM PM AM PM Academic") WEEKLY CLINICAL SCHEDULES Martin Boyer (hand surgery) Academic AM OC OC day CAM CAM PM with Dr. Lindley Wall Carpal tunnel syndrome PIP dislocation CMC arthritis Cubital Tunnel Syndrome Distal Radius Fracture
WEEKLY CLINICAL SCHEDULES Martin Boyer (hand surgery) Academic AM OC OC day CAM CAM PM with Dr. Lindley Wall Carpal tunnel syndrome PIP dislocation CMC arthritis Cubital Tunnel Syndrome Distal Radius Fracture
DISEASES AND DISORDERS
 DISEASES AND DISORDERS 9. 53 10. Rheumatoid arthritis 59 11. Spondyloarthropathies 69 12. Connective tissue diseases 77 13. Osteoporosis and metabolic bone disease 95 14. Crystal arthropathies 103 15.
DISEASES AND DISORDERS 9. 53 10. Rheumatoid arthritis 59 11. Spondyloarthropathies 69 12. Connective tissue diseases 77 13. Osteoporosis and metabolic bone disease 95 14. Crystal arthropathies 103 15.
10/25/2018. Treatment Approaches for Back and Knee Patients. OBJECTIVES By the end of this seminar, participants will be able to:
 Treatment Approaches for Back and Knee Patients Dr. Martin Yuson PT, JD, DPT Dr. Justin Hamilton PT, DPT, OCS OBJECTIVES By the end of this seminar, participants will be able to: Review decision making
Treatment Approaches for Back and Knee Patients Dr. Martin Yuson PT, JD, DPT Dr. Justin Hamilton PT, DPT, OCS OBJECTIVES By the end of this seminar, participants will be able to: Review decision making
Mastering the Musculoskeletal Exam UCSF Essentials of Women s Health July 7, 2016 Carlin Senter, M.D. Henry Crevensten, M.D.
 Mastering the Musculoskeletal Exam UCSF Essentials of Women s Health July 7, 2016 Carlin Senter, M.D. Henry Crevensten, M.D. I have nothing to disclose Outline Knee exam Shoulder exam Knee Anatomy The
Mastering the Musculoskeletal Exam UCSF Essentials of Women s Health July 7, 2016 Carlin Senter, M.D. Henry Crevensten, M.D. I have nothing to disclose Outline Knee exam Shoulder exam Knee Anatomy The
Sports Medicine in your office: What not to miss!
 Sports Medicine in your office: What not to miss! 2018 Primary Care Approach to Treating the Injured Athlete May 4, 2018 John H. Wilckens, MD Associate Professor, Dept of Orthopaedic Surgery Disclosures
Sports Medicine in your office: What not to miss! 2018 Primary Care Approach to Treating the Injured Athlete May 4, 2018 John H. Wilckens, MD Associate Professor, Dept of Orthopaedic Surgery Disclosures
Foot and Ankle Pearls
 Foot and Ankle Pearls Steve Milner Consultant Trauma, Orthopaedic and Foot & Ankle Surgeon Royal Derby Hospital Foot and Ankle PERILS Steve Milner Consultant Trauma, Orthopaedic and Foot & Ankle Surgeon
Foot and Ankle Pearls Steve Milner Consultant Trauma, Orthopaedic and Foot & Ankle Surgeon Royal Derby Hospital Foot and Ankle PERILS Steve Milner Consultant Trauma, Orthopaedic and Foot & Ankle Surgeon
Ankle Arthroscopy.
 Ankle Arthroscopy Key words: Ankle pain, ankle arthroscopy, ankle sprain, ankle stiffness, day case surgery, articular cartilage, chondral injury, chondral defect, anti-inflammatory medication Our understanding
Ankle Arthroscopy Key words: Ankle pain, ankle arthroscopy, ankle sprain, ankle stiffness, day case surgery, articular cartilage, chondral injury, chondral defect, anti-inflammatory medication Our understanding
Lower Extremity Sports Injuries
 Lower Extremity Sports Injuries AAP Musculoskeletal Boot Camp Sigrid F. Wolf, MD Pediatric Sports Medicine Fellow Northwestern University Lurie Children s Hospital Disclosure I have no relevant financial
Lower Extremity Sports Injuries AAP Musculoskeletal Boot Camp Sigrid F. Wolf, MD Pediatric Sports Medicine Fellow Northwestern University Lurie Children s Hospital Disclosure I have no relevant financial
Financial Disclosure. Medial Collateral Ligament
 Matthew Murray, M.D. UTHSCSA Sports Medicine Financial Disclosure Dr. Matthew Murray has no relevant financial relationships with commercial interests to disclose. Medial Collateral Ligament Most commonly
Matthew Murray, M.D. UTHSCSA Sports Medicine Financial Disclosure Dr. Matthew Murray has no relevant financial relationships with commercial interests to disclose. Medial Collateral Ligament Most commonly
ANTERIOR CRUCIATE LIGAMENT INJURY
 ANTERIOR CRUCIATE LIGAMENT INJURY WHAT IS THE ANTERIOR CRUCIATE LIGAMENT? The anterior cruciate ligament (ACL) is one of four major ligaments that stabilizes the knee joint. A ligament is a tough band
ANTERIOR CRUCIATE LIGAMENT INJURY WHAT IS THE ANTERIOR CRUCIATE LIGAMENT? The anterior cruciate ligament (ACL) is one of four major ligaments that stabilizes the knee joint. A ligament is a tough band
An Update of Upper Limb Conditions
 An Update of Upper Limb Conditions Dr. Gavin Nimon Head of Upper Limb and Hand - QEH Senior Lecturer- University of Adelaide MBBS FRACS (Orth) FRCS (Ed) Orthopaedic Surgeon Shoulder, Hand & Knee Injuries
An Update of Upper Limb Conditions Dr. Gavin Nimon Head of Upper Limb and Hand - QEH Senior Lecturer- University of Adelaide MBBS FRACS (Orth) FRCS (Ed) Orthopaedic Surgeon Shoulder, Hand & Knee Injuries
PRIMARY CARE EXAMINATION OF KEY JOINTS. Thomas M. Howard, MD, FACSM FFPC Sports Medicine
 PRIMARY CARE EXAMINATION OF KEY JOINTS Thomas M. Howard, MD, FACSM FFPC Sports Medicine General exam principles: Expose entire joint and opposite limb for comparison Have a Differential Diagnosis Exam
PRIMARY CARE EXAMINATION OF KEY JOINTS Thomas M. Howard, MD, FACSM FFPC Sports Medicine General exam principles: Expose entire joint and opposite limb for comparison Have a Differential Diagnosis Exam
Surgery-Ortho. Fractures of the tibia and fibula. Management. Treatment of low energy fractures. Fifth stage. Lec-6 د.
 Fifth stage Lec-6 د. مثنى Surgery-Ortho 28/4/2016 Indirect force: (low energy) Fractures of the tibia and fibula Twisting: spiral fractures of both bones Angulatory: oblique fractures with butterfly segment.
Fifth stage Lec-6 د. مثنى Surgery-Ortho 28/4/2016 Indirect force: (low energy) Fractures of the tibia and fibula Twisting: spiral fractures of both bones Angulatory: oblique fractures with butterfly segment.
KNEE DISLOCATION. The most common injury will be an anterior dislocation, and this usually results from a hyperextension mechanism.
 KNEE DISLOCATION Introduction Dislocation of the knee is a severe injury associated with major soft tissue injury and a high incidence of damage to the popliteal artery. There is displacement of the tibia
KNEE DISLOCATION Introduction Dislocation of the knee is a severe injury associated with major soft tissue injury and a high incidence of damage to the popliteal artery. There is displacement of the tibia
Case. 5 year old with 2 weeks leg pain and now refusing to walk + Fevers, lower leg swelling, warmth Denies and history of trauma or wounds
 Case 5 year old with 2 weeks leg pain and now refusing to walk + Fevers, lower leg swelling, warmth Denies and history of trauma or wounds Exam I: Swelling over entire tibia extending to foot P: Tenderness
Case 5 year old with 2 weeks leg pain and now refusing to walk + Fevers, lower leg swelling, warmth Denies and history of trauma or wounds Exam I: Swelling over entire tibia extending to foot P: Tenderness
Message of the Month for GPs June 2013
 Message of the Month for GPs June 2013 Dr Winn : Consultant Musculoskeletal Radiologist, Manchester Royal Infirmary Imaging of the musculoskeletal system Musculoskeletal pain is a common problem in the
Message of the Month for GPs June 2013 Dr Winn : Consultant Musculoskeletal Radiologist, Manchester Royal Infirmary Imaging of the musculoskeletal system Musculoskeletal pain is a common problem in the
Referral Criteria: Carpal Tunnel Syndrome Feb
 Referral Criteria: Carpal Tunnel Syndrome Feb 2019 1 5.2. Carpal Tunnel Syndrome Background Carpal tunnel syndrome present with non-traumatic tingling of the fingers due to compression of the median nerve
Referral Criteria: Carpal Tunnel Syndrome Feb 2019 1 5.2. Carpal Tunnel Syndrome Background Carpal tunnel syndrome present with non-traumatic tingling of the fingers due to compression of the median nerve
Ankle Arthritis and Ankle Replacement
 Ankle Arthritis and Ankle Replacement Ryan DeBlis, MD Disclosures I have no disclosures. 1 Diagnosis Ankle arthritis Majority (70%) of patients are post-traumatic (ie, after ankle fracture) Primary arthritis
Ankle Arthritis and Ankle Replacement Ryan DeBlis, MD Disclosures I have no disclosures. 1 Diagnosis Ankle arthritis Majority (70%) of patients are post-traumatic (ie, after ankle fracture) Primary arthritis
Disclosures. Outline. The Posterior Cruciate Ligament 5/3/2016
 The Posterior Cruciate Ligament Christopher J. Utz, MD Assistant Professor of Orthopaedic Surgery University of Cincinnati Disclosures I have no disclosures relevant to this topic. Outline 1. PCL Basic
The Posterior Cruciate Ligament Christopher J. Utz, MD Assistant Professor of Orthopaedic Surgery University of Cincinnati Disclosures I have no disclosures relevant to this topic. Outline 1. PCL Basic
Ankle Replacement Surgery
 Ankle Replacement Surgery Ankle replacement surgery is performed to replace the damaged articular surfaces of the three bones of the ankle joint with artificial implants. This procedure is now being preferred
Ankle Replacement Surgery Ankle replacement surgery is performed to replace the damaged articular surfaces of the three bones of the ankle joint with artificial implants. This procedure is now being preferred
CASE ONE CASE ONE. RADIAL HEAD FRACTURE Mason Classification. RADIAL HEAD FRACTURE Mechanism of Injury. RADIAL HEAD FRACTURE Imaging
 CASE ONE An eighteen year old female falls during a basketball game, striking her elbow on the court. She presents to your office that day with a painful, swollen elbow that she is unable to flex or extend
CASE ONE An eighteen year old female falls during a basketball game, striking her elbow on the court. She presents to your office that day with a painful, swollen elbow that she is unable to flex or extend
Oh My Aching Knee. Oh My Aching Knee WHO AM I? 10/15/2012. Jan Pieter Hommen, MD Orthopedic Surgeon Sports Medicine Arthroscopy Joint Replacements
 Oh My Aching Knee Jan Pieter Hommen, MD Orthopedic Surgeon Sports Medicine Arthroscopy Joint Replacements Oh My Aching Knee Jan Pieter Hommen, MD Orthopedic Surgeon Sports Medicine Arthroscopy Joint Replacements
Oh My Aching Knee Jan Pieter Hommen, MD Orthopedic Surgeon Sports Medicine Arthroscopy Joint Replacements Oh My Aching Knee Jan Pieter Hommen, MD Orthopedic Surgeon Sports Medicine Arthroscopy Joint Replacements
Disclosures Head to Toe: Common Sports Injuries in Kids
 Disclosures Head to Toe: Common Sports Injuries in Kids None R. Jay Lee MD Director Pediatric Orthopaedic Fellowship Assistant Professor Pediatric Orthopaedics Johns Hopkins / Bloomberg Children s Objectives
Disclosures Head to Toe: Common Sports Injuries in Kids None R. Jay Lee MD Director Pediatric Orthopaedic Fellowship Assistant Professor Pediatric Orthopaedics Johns Hopkins / Bloomberg Children s Objectives
Rehabilitation Guidelines for Anterior Cruciate Ligament (ACL) Reconstruction
 Reconstruction") Rehabilitation Guidelines for Anterior Cruciate Ligament (ACL) Reconstruction The knee is the body's largest joint, and the place where the femur, tibia, and patella meet to form a hinge-like joint. These
Rehabilitation Guidelines for Anterior Cruciate Ligament (ACL) Reconstruction The knee is the body's largest joint, and the place where the femur, tibia, and patella meet to form a hinge-like joint. These
Foot & Ankle. Mr Peter Black, FRCSEd. Specialist Orthopaedic Surgeon Anglesea Clinic Orthopaedics
 Foot & Ankle Mr Peter Black, FRCSEd Specialist Orthopaedic Surgeon Anglesea Clinic Orthopaedics Foot & Ankle Problems - Myths and Leg-ends All foot and ankle surgery is cripplingly painful There s no point
Foot & Ankle Mr Peter Black, FRCSEd Specialist Orthopaedic Surgeon Anglesea Clinic Orthopaedics Foot & Ankle Problems - Myths and Leg-ends All foot and ankle surgery is cripplingly painful There s no point
Lower Extremity Dislocations: Management and Triage on the Field
 Lower Extremity Dislocations: Management and Triage on the Field Scott J Tarantino, MD Towson Orthopaedic Associates, Towson, MD None Disclsures Purpose To provide you with knowledge which may guide you
Lower Extremity Dislocations: Management and Triage on the Field Scott J Tarantino, MD Towson Orthopaedic Associates, Towson, MD None Disclsures Purpose To provide you with knowledge which may guide you
Clinical Guideline for: Diagnosis and Management of Charcot Foot
 Clinical Guideline for: Diagnosis and Management of Charcot Foot SUMMARY This guideline outlines the clinical features of Charcot foot (Charcot Neuroarthropathy). It also explains the process of diagnosis
Clinical Guideline for: Diagnosis and Management of Charcot Foot SUMMARY This guideline outlines the clinical features of Charcot foot (Charcot Neuroarthropathy). It also explains the process of diagnosis
Foot & Ankle Disorders
 Foot & Ankle Disorders Hillingdon PGMC 6-7-2013 Htwe Zaw FRCS (Tr&Orth) Consultant Foot & Ankle and Trauma Surgeon Hillingdon Hospitals NHS Foundation Trust Overview Anatomy: hindfoot-midfoot coupling
Foot & Ankle Disorders Hillingdon PGMC 6-7-2013 Htwe Zaw FRCS (Tr&Orth) Consultant Foot & Ankle and Trauma Surgeon Hillingdon Hospitals NHS Foundation Trust Overview Anatomy: hindfoot-midfoot coupling
Exam of the Knee and Ankle I HAVE NO FINANCIAL DISCLOSURES RELEVANT TO THIS PRESENTATION
 Exam of the Knee and Ankle I HAVE NO FINANCIAL DISCLOSURES RELEVANT TO THIS PRESENTATION Disclosures I have no relevant financial relationships with the manufacturers of any commercial products and or
Exam of the Knee and Ankle I HAVE NO FINANCIAL DISCLOSURES RELEVANT TO THIS PRESENTATION Disclosures I have no relevant financial relationships with the manufacturers of any commercial products and or
BATES VISUAL GUIDE TO PHYSICAL EXAMINATION. OSCE 4: Knee Pain
 BATES VISUAL GUIDE TO PHYSICAL EXAMINATION OSCE 4: Knee Pain This video format is designed to help you prepare for objective structured clinical examinations, or OSCEs. You are going to observe and participate
BATES VISUAL GUIDE TO PHYSICAL EXAMINATION OSCE 4: Knee Pain This video format is designed to help you prepare for objective structured clinical examinations, or OSCEs. You are going to observe and participate
WEEKLY CLINICAL SCHEDULES. Martin Boyer (hand surgery) Monday Tuesday Wednesday Thursday Friday AM PM AM PM AM PM AM PM AM PM VA OR Wohl
 Monday Tuesday Wednesday Thursday Friday AM PM AM PM AM PM AM PM AM PM VA OR Wohl") WEEKLY CLINICAL SCHEDULES Martin Boyer (hand surgery) VA OR Wohl Dr. Goldfarb CAM OC OC OR CAM CAM OR Carpal tunnel syndrome PIP dislocation CMC arthritis Cubital Tunnel Syndrome Distal Radius Fracture
WEEKLY CLINICAL SCHEDULES Martin Boyer (hand surgery) VA OR Wohl Dr. Goldfarb CAM OC OC OR CAM CAM OR Carpal tunnel syndrome PIP dislocation CMC arthritis Cubital Tunnel Syndrome Distal Radius Fracture
Knee Case Studies. You might KNEED to know some of this stuff
 Knee Case Studies You might KNEED to know some of this stuff Mark Mildren, MD Specializing in Adult Reconstruction Slocum Center for Orthopedics & Sports Medicine 25 th Annual Orthopedic & Sports Medicine
Knee Case Studies You might KNEED to know some of this stuff Mark Mildren, MD Specializing in Adult Reconstruction Slocum Center for Orthopedics & Sports Medicine 25 th Annual Orthopedic & Sports Medicine
American College of Physicians 2013 Ohio Chapter Scientific Meeting Columbus, OH October 11, 2013
 American College of Physicians 2013 Ohio Chapter Scientific Meeting Columbus, OH October 11, 2013 Paul J. Gubanich, MD, MPH Assistant Professor of Internal Medicine/Sports Medicine Team Physician, Ohio
American College of Physicians 2013 Ohio Chapter Scientific Meeting Columbus, OH October 11, 2013 Paul J. Gubanich, MD, MPH Assistant Professor of Internal Medicine/Sports Medicine Team Physician, Ohio
Your Orthopaedic Experience: Bones, Muscles and Joints. Getting you back into motion. Hospitals + Health Checks + Physio + Gyms
 Your Orthopaedic Experience: Bones, Muscles and Joints. Getting you back into motion. Hospitals + Health Checks + Physio + Gyms Taking on your aches and pains. Getting you mobile your way. You want to
Your Orthopaedic Experience: Bones, Muscles and Joints. Getting you back into motion. Hospitals + Health Checks + Physio + Gyms Taking on your aches and pains. Getting you mobile your way. You want to
4) Gamekeeper s Thumb Dr. Jwamer
 Gamekeeper s Thumb Dr. Jwamer") 4) Gamekeeper s Thumb Dr. Jwamer Gamekeeper s Thumb Injury to the ulnar collateral ligament (UCL) of thumb MPJ UCL is an important stabilizer of the thumb Acute & chronic Acute injury known as skier s
4) Gamekeeper s Thumb Dr. Jwamer Gamekeeper s Thumb Injury to the ulnar collateral ligament (UCL) of thumb MPJ UCL is an important stabilizer of the thumb Acute & chronic Acute injury known as skier s