Podo-Pediatrics in Private Practice. Elisabeth Hibbert B.Sc. D.Ch. November 11, 2016
|
|
|
- Sharon Conley
- 6 years ago
- Views:
Transcription

1 Podo-Pediatrics in Private Practice Elisabeth Hibbert B.Sc. D.Ch. November 11, 2016
2 My background Private Practice since 1998 Began promoting children s foot care in 2007 In % of new patients are under the age of 16 Associates that specialize in Pediatrics I have three children myself
3 What makes for a successful Pediatric Practice? Child friendly office Children friendly staff Chiropodists experienced with children and know how to talk to parents


4 Child friendly office Waiting room with Children s chairs Children activities in waiting room Foot related books Patient rewards


5 Patient Rewards
6 Working with Parents and Children A Parent with the correct information is a happy Parent Children are reacting to their surroundings. Communicate with both Ages, Stages of Development and Personality?

7 Erik Erikson s Psychosocial Development
8 Personality Types Fearful- nervous, anxiety, clingy Flexible- comfortable, cooperative, compliant Feisty- curious, energetic, loud (Lally et al, 1990)
9 So Far.. Differences Age Development- Socio-emotional Personality Now we are ready look at the child physiologically and then treat..
10 Recommended Reading
11 Common Children concerns Walk funny Toes are crooked Flat feet Feet turn in Crooked or bent legs Trip and fall lots I can t find shoes

12
13 What do parents want? Parents want to know. Is this normal? Why is this happening? What can be done to help? What will happen if we do nothing? Education and knowledge lead to relief
14 What is normal? Is it. What is most common? The average? Being with out pain? Visual appearance? Ability to wear normal shoes?
15 Merriam Webster dictionary definition: Normal- usual or ordinary : not strange Deformity- a condition in which part of the body does not have the normal or expected shape It is our job to determine what is expected

16 Extra Toe Nail

17 Pediatric History Ask the right questions when doing the History: Pregnancy/ Labour/ Birth Milestones? Sleep and Sitting position Coordination walk / run Trip/ Tire easily Onset, Progression, Prior Tt, Family History
18 Normal Milestones- development Foot to mouth Sit/ roll over Crawl Stand Walk Heel-Toe Gait 3 months 6 months 8 months 10 months 12 months 36 months
19 Look what I found!
20 Examine the child Look at child Standing Sitting Non Weight Bearing- Supine / Prone Walking

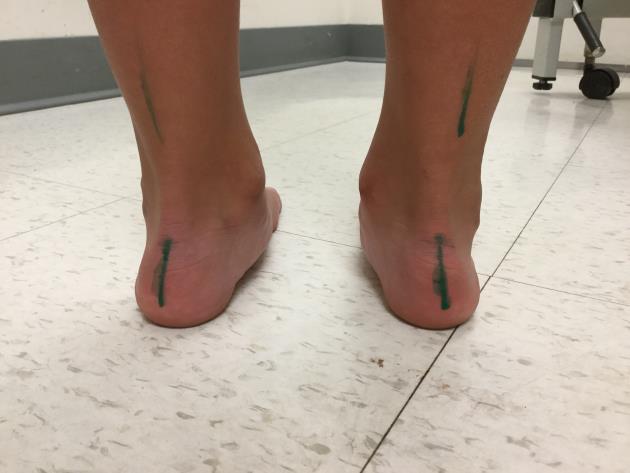
21 Standing- Weight Bearing Assessment Posture Base Angle of leg/ knee RCSP NCSP Arch profile Jacks Test- Flexible vs Rigid- Windlass? Supination Resistance Test- Skive?

22 Sitting Ask the child to sit and see how they naturally sit on the ground. W position and Sitting on feet - internal rotates the Femur and Tibia
23 Non Weight bearing Supine Hip External/ Internal rotation Genu Varum/ Valgum (Patella) Malleolar Torsion Ankle Dorsiflexion Prone Femoral Anteversion Internal/ External Tibia Torsion Metatarsus Adductus



24 Hip/Femur Femoral Anteversion - Position with Frontal plane - Birth to adult deg. Femoral Antetorsion - Twist in femur bone shaft - Birth to adult deg.

25 Examine Hip Prone ROM Ext- Internal rotation Position with Greater trochanter Lateral Supine Check ROM hips flexed and extended The Foot examination & Diagnosis Second Edition, I J Alexander Illustrated by J Kanasz 1997
26 Examine Knee- 3 planes Sagittal- Flexion and Extension Frontal- Varum and Valgum Transverse- Internal and External

27 Examine knee- Frontal Frontal plane Patellar position Measure Intra malleolar distance/ Inter condylar distance


28 Examine Knee-Tibia Transverse plane Knee ROM Check for medial genicular biased Foot to Thigh angle Measures Internal Tibial Torsion Normal 0-30 deg. Ext. rotated Malleolar Position Indirectly represents Tibial Torsion The Foot examination & Diagnosis Second Edition, I J Alexander Illustrated by J Kanasz
 Feet come in all shapes and")
29 Foot Assessment Ankle Equinus (AQ) Range of motion (ROM) RF- FF relationship Metatarsus Adductus (MTA) Feet come in all shapes and sizes

30 Examine Foot- Metatarsus Adductus Common at Birth Resolve by 12 weeks old Bisection of Heel Normal between the 2 nd /3 rd digits The Foot examination & Diagnosis Second Edition, I J Alexander Illustrated by J Kanasz 1997

31 Non Wt. Bear Summary so far Hip: Ext>>Int. normal age 0-6 years Genu Varum: normal age 0-2 years Genu Valgum: normal age 3-7 years Int. Tibial Torsion: normal 0-18 months MTA: normal 0-12 weeks The Foot examination & Diagnosis Second Edition, I J Alexander Illustrated by J Kanasz 1997
32
33 Gait related milestones Walk Run Jump Hop Skip 12 months 18 months 2 years 4 years 6 years
34 Gait -Walking Assess: Balance, Stability, Speed, Control, Symmetry Look at: Head/ Shoulder Position Arm Swing Pelvis Position Knee Rotation Patella Position Tibial Rotation Foot: Calcaneus Position, RF/ FF Arches Base of Gait Stride Length Ankle ROM Foot Progression Angle
35 Gait through the Ages. Yr Balance Stable Speed control Base Stride Arm Knee Tibia Ankle Calc. MLA Other 1 Un Balance Un Stable slow Low Control Wide short Bent Elbows Varum Ltd Flex ITT No DF Evert 5-10 Wt. B FF Abd. 2 More Balance stable low Some Control Less Wide Longer Swing Some Flex ST Ltd DF Evert low Prop Start 3 Balance Stable Inc. More Control More Narrow Increase 7 Balance Stable Inc. Control Narrow Short Inc. Cad 8-12 Balance Stable Inc. Increase Control Recip. swing Recip. Swing Narrow Increase Recip. Swing Valgum Hyp-Ext ST Ltd DF Evert - ST ST ST Start DF ST ST DF Inc. MLA Dec Fat Heel Toe ST Yes RF-FF Align ST Yes Inc. Single Leg
36 Gait Analysis
37 In the Private Practice Now Let s see what comes into our Office
38 Recommended Reading
39 Common Children Concerns Curly toes Metatarsus Adductus Flat Feet Genu Varum/ Valgum In toe Gait Out toe/ Toe walker Pains

40 Curly Toes My child has crooked toes Claw/ Curly Toes: most common Etiology : Development, Shoe, Heredity Treatment: Mobilize, Stretch, Tape, Silicone, Shoes childrens-podiatry/curly-toes/ Michener chiropody notes 1997
41 Flat Feet Is it Normal? Yes! What age?...up to Age 3 (pre Heel-Toe gait) Types of Pes Planus: Flexible Flat Feet Rigid Flat feet Rocker Bottom How Flat is it? Flexible or Rigid? Arch height fat pad? Heel eversion? Talus Position- rotate? Navicular Position- bulge? Forefoot Position- adducted?
42 Treatment- When? If Heel-Toe Gait- Arch lowers, Leg alignment changes and flexible type Earlier if Pain, Weakness, Unilateral, not Flexible Treat: Stable Shoes OTC Insoles Custom Orthotics What if don t treat?


43 OTC Insoles Kiddy Orthotics- Paris Orthotics Globotec Insoles- Langer Orthotics





44 Custom Orthotics


45 Flexible Pes Planus


46 Flexible Pes Planus Ligament Laxity, Hypotonia
47 Knee- Genu Deformities Bow Legs Knock Knees Crooked or Bent legs Frontal Plane Angular Deformities

48 Genu Varum- Bow legs Commonly Associated with In toe gait

49 Genu Valgum- Knocked Knees Commonly Associated with Out toe Gait

50 In-Toe gait- a symptom Trips and Falls a lot 3 main causes: Metatarsus Adductus Internal Tibial Torsion Femoral Anteversion
51 Is In Toe gait normal? In toe gait occurs in 1:10 children between the age of 2-5, of those 50% will correct by age 6-8 Cause - mostly Developmentally, Familiar or Neurological Need to treat if: Delayed development Changes Function- trip /limp Pain Affects Mobility Asymmetric Angela M Evans The pocket Podiatry Guide to Pediatrics



52 In toe- Metatarsus Adductus (MTA) A transverse plane deformity Metatarsal Adduct at the Tarsal-Metatarsal joints C shaped foot Etiology: In utero Position, Genetics, Muscular tightness Occurrence 1:1000 births, 4 Types of MTA Assoc. with Internal Tibial torsion, In toe gait Angela M Evans The pocket Podiatry Guide to Pediatrics

53 Treatment MTA Ideal to treat between 3-8 months Passive stretches and massage Manipulations, Serial casting, Splints Straight last Shoes, Orthotics Surgery- Osteotomy




54 Splints Splints instead of serial cast, if mild and flexible Denis Browne, Telescoping, Bebax, Wheaton Brace Alimed.com


55 Straight last Shoes



56 Serial Casting Materials





57 Serial Casting



58



59 Case study MTA

60 MTA

61 In Toe- Internal Tibial Torsion (ITT) Tibial bone is medially rotated Thigh Foot angle < 0 Normal 0-18 months Gait: In toe Trip Etiology- in utero position, Familiar, Developmental delay The Foot examination & Diagnosis Second Edition, I J Alexander Illustrated by J Kanasz 1997

")
62 How to treat for ITT Usually treated after 15 months Mobilizations Bracing Dennis Browne Telescoping brace (single) Orthoses Gait Plates

63 Gait Plates! Effective or not? Research varies. Do not generally improve the Progression angle of gait, Decrease tripping and parents see a benefits Journal of the American Podiatric Medical Association > February 2000 > The effectiveness of gait plates in controlling in-toeing symptoms
64
65 In Toe Gait Normal: Mild Anteversion Abnormal: Genu Varum Internal Tibial Torsion Metatarsus Adductus



66 Internal Tibial Torsion Flexible Pediatric Pes Planus

 www.clinicalgaitanalysis.")

67 In Toe- Femoral Anteversion Femur twisted inward Medial Patella Position Gait: In toe Knee squint Anteversion- Int. rotation > Ext. rotation (> 70 degrees) The Foot examination & Diagnosis Second Edition, I J Alexander Illustrated by J Kanasz 1997

68 Treatment Sit cross legged encourage rotation resolution W sitting position promotes internal rotation of the Femur and Tibia



69 In toe Gait Corrected Internal Tibial torsion Metatarsus Adductus Left with mild Fem. Anteversion Rearfoot Varus Forefoot Varus
70 In toe Gait- Assessment Summary MTA ITT Fem AV Heel bisection to Digits (Lateral to 3 rd digit = MTA) Thigh- foot angle (<0 = ITT) Craig s Test (Int. >> Ext. = Anteversion)
71 Treatment Summary-In Toe gait Metatarsus Adductus: Mobilizations Serial casting Braces: Wheaton, Bebax, Straight last shoes Orthoses Internal Tibial Torsion: Mobilizations, Serial Casting Denis Browne splint Orthoses Gait plates Anteversion- Do not treat, Surgery later Change sit and sleep pattern

72 Out Toe Gait Less common Etiology: Calcaneal Valgus External Tibial Torsion Ext Hip Rotation External Tibial Torsion




73 Shoes
74 Injury to Bones in child Deform with: Strain/ Force Quick growth Diaphysis- Torsional Skeletal deformities Metaphysis- Frontal Skeletal deformities Force or Mechanical disorder Epiphysis- Apophysitis occurs here
75 Apophysis- Pain Apophysis- a secondary ossification centre where tendon inserts Apophysitis- inflammation of the apophysis, Etiology- Overuse injury in young growing athletes Iselin Dz., Sever s Dz., Osgoode Schlatter s Dz
76 Sever s Dz- Calcaneal Apophysitis Heel pain on Medial-Lateral Palpation Common age 8-15 years old, No injury or disorder S/S- Pain, inflammation Etiology- Overuse, Growth, Footwear, Sports, poor training Treatment- Reduce activity 50%, Ice, Stretch, Tape, Heel lifts, BMA



77 Calcaneal Apophysitis



78
79 Growing pains ok? Pain that is intermittent, in the muscles Bilateral, Usually in afternoon and evening Diagnose-? Etiology- Rapid bone growth, Fatigue, Overuse, Family history 70% Treatment- Medications, Massage, Stretch, Vitamins
80 Podo-Pediatrics in Private Practice Know what to Expect Treat what is not Normal and you will have happy Children (and Parents) Thank You
BIOMECHANICAL EXAMINATION OF THE PEDIATRIC LOWER EXTREMITY
 BIOMECHANICAL EXAMINATION OF THE PEDIATRIC LOWER EXTREMITY B.Resseque, D.P.M. ARCH HEIGHT OFF WEIGHTBEARING Evaluate arch height by placing a ruler from the heel to the first metatarsal head Compare arch
BIOMECHANICAL EXAMINATION OF THE PEDIATRIC LOWER EXTREMITY B.Resseque, D.P.M. ARCH HEIGHT OFF WEIGHTBEARING Evaluate arch height by placing a ruler from the heel to the first metatarsal head Compare arch
BIOMECHANICAL EXAMINATION OF THE PEDIATRIC LOWER EXTREMITY 2017
 BIOMECHANICAL EXAMINATION OF THE PEDIATRIC LOWER EXTREMITY 2017 B. RESSEQUE, D.P.M., D.A.B.P.O. Professor, N.Y. College of Podiatric Medicine ARCH HEIGHT OFF WEIGHTBEARING Evaluate arch height by placing
BIOMECHANICAL EXAMINATION OF THE PEDIATRIC LOWER EXTREMITY 2017 B. RESSEQUE, D.P.M., D.A.B.P.O. Professor, N.Y. College of Podiatric Medicine ARCH HEIGHT OFF WEIGHTBEARING Evaluate arch height by placing
PAEDIATRIC ORTHOPAEDICS BRENT WEATHERHEAD, MD, FRCSC PAEDIATRIC ORTHOPAEDIC SURGEON MEDICAL DIRECTOR, REBALANCE
 PAEDIATRIC ORTHOPAEDICS BRENT WEATHERHEAD, MD, FRCSC PAEDIATRIC ORTHOPAEDIC SURGEON MEDICAL DIRECTOR, REBALANCE DISCLOSURES I HAVE NO INDUSTRY CONFLICTS TO DECLARE I AM AN ORTHOPAEDIC SURGEON TRAINED IN
PAEDIATRIC ORTHOPAEDICS BRENT WEATHERHEAD, MD, FRCSC PAEDIATRIC ORTHOPAEDIC SURGEON MEDICAL DIRECTOR, REBALANCE DISCLOSURES I HAVE NO INDUSTRY CONFLICTS TO DECLARE I AM AN ORTHOPAEDIC SURGEON TRAINED IN
In-toeing, Out-toeing, Growing Pains, Bowlegs, Knock-Knees and Flat Feet
 Jeffrey B. Neustadt, M.D. Scott W. Beck, M.D. Gregory V. Hahn, M.D. Drew E. Warnick, M.D. Paul L. Benfanti, M.D. Lee G. Phillips, M.D. Daniel C. Bland, M.D. Common Benign Orthopaedic Conditions In-toeing,
Jeffrey B. Neustadt, M.D. Scott W. Beck, M.D. Gregory V. Hahn, M.D. Drew E. Warnick, M.D. Paul L. Benfanti, M.D. Lee G. Phillips, M.D. Daniel C. Bland, M.D. Common Benign Orthopaedic Conditions In-toeing,
Evaluation of Gait Mechanics Using Computerized Plantar Surface Pressure Analysis and it s Relation to Common Musculoskeletal Problems
 Evaluation of Gait Mechanics Using Computerized Plantar Surface Pressure Analysis and it s Relation to Common Musculoskeletal Problems Laws of Physics effecting gait Ground Reaction Forces Friction Stored
Evaluation of Gait Mechanics Using Computerized Plantar Surface Pressure Analysis and it s Relation to Common Musculoskeletal Problems Laws of Physics effecting gait Ground Reaction Forces Friction Stored
Intoeing: When to Worry? Sukhdeep K. Dulai SPORC 2018
 Intoeing: When to Worry? Sukhdeep K. Dulai SPORC 2018 What is it? Intoeing: When to worry? Why isn t it always cause for worry? What are the benign causes of intoeing? What are the pathologic causes of
Intoeing: When to Worry? Sukhdeep K. Dulai SPORC 2018 What is it? Intoeing: When to worry? Why isn t it always cause for worry? What are the benign causes of intoeing? What are the pathologic causes of
Instructional Course Lecture 2011
 Instructional Course Lecture 2011 Yoon Hae Kwak Dept. of Orthopaedic Surgery Hallym University Sacred Heart Hospital Hallym University Medical Center Rotational and Angular variations of the lower extremities
Instructional Course Lecture 2011 Yoon Hae Kwak Dept. of Orthopaedic Surgery Hallym University Sacred Heart Hospital Hallym University Medical Center Rotational and Angular variations of the lower extremities
LECTURE 8: DEVELOPMENTAL ORTHOPAEDICS. Paediatric MS History o Reason for referral o Past history
 LECTURE 8: DEVELOPMENTAL ORTHOPAEDICS Paediatric MS History o Reason for referral o Past history Antenatal history Birth history (term? Premmy? Breech? Complications?). Medical history/investigations/tests
LECTURE 8: DEVELOPMENTAL ORTHOPAEDICS Paediatric MS History o Reason for referral o Past history Antenatal history Birth history (term? Premmy? Breech? Complications?). Medical history/investigations/tests
BORGinsole Measurement devices
 BORGinsole Measurement devices BORGinsole Angle-Finder Dorsal Flexion of the first Metatarsophalangeal joint - P. is sitting up on the examination table, with legs straight. - T. is sitting at the end
BORGinsole Measurement devices BORGinsole Angle-Finder Dorsal Flexion of the first Metatarsophalangeal joint - P. is sitting up on the examination table, with legs straight. - T. is sitting at the end
Balanced Body Movement Principles
 Balanced Body Movement Principles How the Body Works and How to Train it. Module 3: Lower Body Strength and Power Developing Strength, Endurance and Power The lower body is our primary source of strength,
Balanced Body Movement Principles How the Body Works and How to Train it. Module 3: Lower Body Strength and Power Developing Strength, Endurance and Power The lower body is our primary source of strength,
Lower Extremity Malalignment: When to Refer and When to Reassure?
 Lower Extremity Malalignment: When to Refer and When to Reassure? Mary Aschenbrener, PA-C Minnesota Academy of Physician Assistants 03/18/16 Cary H. Mielke, MD Chief of Staff Orthopaedic Burn Spinal cord
Lower Extremity Malalignment: When to Refer and When to Reassure? Mary Aschenbrener, PA-C Minnesota Academy of Physician Assistants 03/18/16 Cary H. Mielke, MD Chief of Staff Orthopaedic Burn Spinal cord
Pediatric Orthopedics: ``To Refer or Not to Refer``
 Pediatric Orthopedics: ``To Refer or Not to Refer`` Thierry E. Benaroch, MD, FRCS(C) McGill University Health Centre Intoeing Knock knees Bowlegs Flatfeet Toe walking Knee pain Hip click Intoeing Objectives
Pediatric Orthopedics: ``To Refer or Not to Refer`` Thierry E. Benaroch, MD, FRCS(C) McGill University Health Centre Intoeing Knock knees Bowlegs Flatfeet Toe walking Knee pain Hip click Intoeing Objectives
A Patient s Guide to Rotational Deformities in Children
 A Patient s Guide to Rotational Deformities in Children 2350 Royal Boulevard Suite 200 Elgin, IL 60123 Phone: 847.931.5300 Fax: 847.931.9072 DISCLAIMER: The information in this booklet is compiled from
A Patient s Guide to Rotational Deformities in Children 2350 Royal Boulevard Suite 200 Elgin, IL 60123 Phone: 847.931.5300 Fax: 847.931.9072 DISCLAIMER: The information in this booklet is compiled from
Copyright 2004, Yoshiyuki Shiratori. All right reserved.
 Ankle and Leg Evaluation 1. History Chief Complaint: A. What happened? B. Is it a sharp or dull pain? C. How long have you had the pain? D. Can you pinpoint the pain? E. Do you have any numbness or tingling?
Ankle and Leg Evaluation 1. History Chief Complaint: A. What happened? B. Is it a sharp or dull pain? C. How long have you had the pain? D. Can you pinpoint the pain? E. Do you have any numbness or tingling?
ChiroCredit.com Presents Biomechanics: Focus on
 ChiroCredit.com Presents Biomechanics: Focus on the Knee Presented by: Ivo Waerlop, DC Shawn Allen, DC 1 Focus on The Knee 2 Pertinent Anatomy Femur Tibia Fibula Patella Prepatellar bursa Infrapatellar
ChiroCredit.com Presents Biomechanics: Focus on the Knee Presented by: Ivo Waerlop, DC Shawn Allen, DC 1 Focus on The Knee 2 Pertinent Anatomy Femur Tibia Fibula Patella Prepatellar bursa Infrapatellar
Who, What, Where, When & Why s of The Pediatric Forefoot
 Essential Pediatric Biomechanics Who, What, Where, When & Why s of The Pediatric Forefoot Louis J. DeCaro, DPM President, ACFAP APMA 2018 drlouisjames@aol.com The APMA's only recognized clinical interest
Essential Pediatric Biomechanics Who, What, Where, When & Why s of The Pediatric Forefoot Louis J. DeCaro, DPM President, ACFAP APMA 2018 drlouisjames@aol.com The APMA's only recognized clinical interest
Running Injuries in Children and Adolescents
 Running Injuries in Children and Adolescents Cook Children s SPORTS Symposium July 2, 2014 Running Injuries Overuse injuries Acute injuries Anatomic conditions 1 Overuse Injuries Pain that cannot be tied
Running Injuries in Children and Adolescents Cook Children s SPORTS Symposium July 2, 2014 Running Injuries Overuse injuries Acute injuries Anatomic conditions 1 Overuse Injuries Pain that cannot be tied
What Happens to the Paediatric Flat Foot? Peter J Briggs Freeman Hospital Newcastle upon Tyne
 What Happens to the Paediatric Flat Foot? Peter J Briggs Freeman Hospital Newcastle upon Tyne We don t know!! Population Studies 2300 children aged 4-13 years Shoe wearers Flat foot 8.6% Non-shoe wearers
What Happens to the Paediatric Flat Foot? Peter J Briggs Freeman Hospital Newcastle upon Tyne We don t know!! Population Studies 2300 children aged 4-13 years Shoe wearers Flat foot 8.6% Non-shoe wearers
Running Athlete: Part C. Case Analysis Materials
 Running Athlete: Part C Case Analysis Materials Case 1 Subjective Examination (performed offcamera) Runs very sporadically, but generally 2-3 x per week around 2-4 miles Play recreational soccer Denies
Running Athlete: Part C Case Analysis Materials Case 1 Subjective Examination (performed offcamera) Runs very sporadically, but generally 2-3 x per week around 2-4 miles Play recreational soccer Denies
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Abductor hallucis tendon procedures, for hallux varus, 536 537 Acetabular disorders, intoeing in, 551 553 Akron dome osteotomy, for cavus deformities,
Note: Page numbers of article titles are in boldface type. A Abductor hallucis tendon procedures, for hallux varus, 536 537 Acetabular disorders, intoeing in, 551 553 Akron dome osteotomy, for cavus deformities,
A Patient s Guide to Flatfoot Deformity (Pes Planus) in Children
 in Children") A Patient s Guide to Flatfoot Deformity (Pes Planus) in Children 2350 Royal Boulevard Suite 200 Elgin, IL 60123 Phone: 847.931.5300 Fax: 847.931.9072 DISCLAIMER: The information in this booklet is compiled
A Patient s Guide to Flatfoot Deformity (Pes Planus) in Children 2350 Royal Boulevard Suite 200 Elgin, IL 60123 Phone: 847.931.5300 Fax: 847.931.9072 DISCLAIMER: The information in this booklet is compiled
Recognizing common injuries to the lower extremity
 Recognizing common injuries to the lower extremity Bones Femur Patella Tibia Tibial Tuberosity Medial Malleolus Fibula Lateral Malleolus Bones Tarsals Talus Calcaneus Metatarsals Phalanges Joints - Knee
Recognizing common injuries to the lower extremity Bones Femur Patella Tibia Tibial Tuberosity Medial Malleolus Fibula Lateral Malleolus Bones Tarsals Talus Calcaneus Metatarsals Phalanges Joints - Knee
DAVID LIDDLE PODIATRIST PAEDIATRIC FLATFOOT PODIATRY.
 DAVID LIDDLE PODIATRIST PAEDIATRIC FLATFOOT PODIATRY To treat or not to treat Angela Evans PhD The paediatric flat foot proforma (p-ffp): improved and abridged following a reproducibility study Angela
DAVID LIDDLE PODIATRIST PAEDIATRIC FLATFOOT PODIATRY To treat or not to treat Angela Evans PhD The paediatric flat foot proforma (p-ffp): improved and abridged following a reproducibility study Angela
Dorsal surface-the upper area or top of the foot. Terminology
 It is important to learn the terminology as it relates to feet to properly communicate with referring physicians when necessary and to identify the relationship between the anatomical structure of the
It is important to learn the terminology as it relates to feet to properly communicate with referring physicians when necessary and to identify the relationship between the anatomical structure of the
Biomechanical Explanations for Selective Sport Injuries of the Lower Extremity
 Biomechanical Explanations for Selective Sport Injuries of the Lower Extremity American Osteopathic Academy of Sports Medicine Presentation April 23, 2015 Understanding Normalcy What is Normal? Rearfoot/heel
Biomechanical Explanations for Selective Sport Injuries of the Lower Extremity American Osteopathic Academy of Sports Medicine Presentation April 23, 2015 Understanding Normalcy What is Normal? Rearfoot/heel
Managing Tibialis Posterior Tendon Injuries
 Managing Tibialis Posterior Tendon Injuries by Thomas C. Michaud, DC Published April 1, 2015 by Dynamic Chiropractic Magazine Tibialis posterior is the deepest, strongest, and most central muscle of the
Managing Tibialis Posterior Tendon Injuries by Thomas C. Michaud, DC Published April 1, 2015 by Dynamic Chiropractic Magazine Tibialis posterior is the deepest, strongest, and most central muscle of the
Redirect GRF to Affect Mobility, Stability or Load? Increase/Decrease Joint Moments to Reduce Stress Strain Relationships?
 5-1 SECTION 5 CRITICAL DECISION MAKING IN ORTHOTIC THERAPY QUESTIONS Answering the some critical (as in choosing between criteria) questions should help as a guide to selecting an appropriate orthosis,
5-1 SECTION 5 CRITICAL DECISION MAKING IN ORTHOTIC THERAPY QUESTIONS Answering the some critical (as in choosing between criteria) questions should help as a guide to selecting an appropriate orthosis,
Exam of the Knee and Ankle I HAVE NO FINANCIAL DISCLOSURES RELEVANT TO THIS PRESENTATION
 Exam of the Knee and Ankle I HAVE NO FINANCIAL DISCLOSURES RELEVANT TO THIS PRESENTATION Disclosures I have no relevant financial relationships with the manufacturers of any commercial products and or
Exam of the Knee and Ankle I HAVE NO FINANCIAL DISCLOSURES RELEVANT TO THIS PRESENTATION Disclosures I have no relevant financial relationships with the manufacturers of any commercial products and or
In-toeing and Out-toeing
 In-toeing and Out-toeing What is all the fuss about? Natalie Stork, MD Assistant Professor University of Missouri-Kansas City School of Medicine, Department of Orthopaedic Surgery and Department of Pediatrics
In-toeing and Out-toeing What is all the fuss about? Natalie Stork, MD Assistant Professor University of Missouri-Kansas City School of Medicine, Department of Orthopaedic Surgery and Department of Pediatrics
Anterior knee pain.
 Anterior knee pain What are the symptoms? Anterior knee pain is very common amongst active adolescents and athletes participating in contact sports. It is one of the most common problems/injuries seen
Anterior knee pain What are the symptoms? Anterior knee pain is very common amongst active adolescents and athletes participating in contact sports. It is one of the most common problems/injuries seen
Servers Disease (Calcaneal Apophysitis ) 101
 101") Servers Disease (Calcaneal Apophysitis ) 101 Servers Disease Causes a disturbance to the growing area at the back of the heel bone (calcaneus) where the strong Achilles tendon attaches to it. It is most
Servers Disease (Calcaneal Apophysitis ) 101 Servers Disease Causes a disturbance to the growing area at the back of the heel bone (calcaneus) where the strong Achilles tendon attaches to it. It is most
Other Congenital and Developmental Diseases of the Foot. Department of Orthopedic Surgery St. Vincent s s Hospital, The Catholic University
 Other Congenital and Developmental Diseases of the Foot Department of Orthopedic Surgery St. Vincent s s Hospital, The Catholic University Contents Metatarsus Adductus Skewfoot Hallux Valgus Hallux Valgus
Other Congenital and Developmental Diseases of the Foot Department of Orthopedic Surgery St. Vincent s s Hospital, The Catholic University Contents Metatarsus Adductus Skewfoot Hallux Valgus Hallux Valgus
RN(EC) ENC(C) GNC(C) MN ACNP *** MECHANISM OF INJURY.. MOST IMPORTANT *** - Useful in determining mechanism of injury / overuse
 ENC(C) GNC(C) MN ACNP *** MECHANISM OF INJURY.. MOST IMPORTANT *** - Useful in determining mechanism of injury / overuse") HISTORY *** MECHANISM OF INJURY.. MOST IMPORTANT *** Age of patient Sport / Occupation - Certain conditions are more prevalent in particular age groups (Osgood Schlaters in youth / Degenerative Joint Disease
HISTORY *** MECHANISM OF INJURY.. MOST IMPORTANT *** Age of patient Sport / Occupation - Certain conditions are more prevalent in particular age groups (Osgood Schlaters in youth / Degenerative Joint Disease
Trainers. Anne-Marie O Connor Musculoskeletal Podiatrist
 Trainers Anne-Marie O Connor Musculoskeletal Podiatrist Agenda Background Tarso-navicular stress fractures Case Study Interventions and research Further Research Anatomy Anatomically, wedged between the
Trainers Anne-Marie O Connor Musculoskeletal Podiatrist Agenda Background Tarso-navicular stress fractures Case Study Interventions and research Further Research Anatomy Anatomically, wedged between the
ANTERIOR KNEE PAIN. Explanation. Causes. Symptoms
 ANTERIOR KNEE PAIN Explanation Anterior knee pain is most commonly caused by irritation and inflammation of the patellofemoral joint of the knee (where the patella/kneecap connects to the femur/thigh bone).
ANTERIOR KNEE PAIN Explanation Anterior knee pain is most commonly caused by irritation and inflammation of the patellofemoral joint of the knee (where the patella/kneecap connects to the femur/thigh bone).
right Initial examination established that you have 'flat feet'. Additional information left Left foot is more supinated possibly due to LLD
 Motion analysis report for Feet In Focus at 25/01/2013 Personal data: Mathew Vaughan DEMO REPORT, 20 Churchill Way CF10 2DY Cardiff - United Kingdom Birthday: 03/01/1979 Telephone: 02920 644900 Email:
Motion analysis report for Feet In Focus at 25/01/2013 Personal data: Mathew Vaughan DEMO REPORT, 20 Churchill Way CF10 2DY Cardiff - United Kingdom Birthday: 03/01/1979 Telephone: 02920 644900 Email:
BOW LEGS (GENU VARUM)
") BOW LEGS (GENU VARUM) By Dr John Ebnezar INTRODUCTION Have you noticed how your knees look like? If you observe carefully you will see that both your knees are not parallel but deviated slightly outwards
BOW LEGS (GENU VARUM) By Dr John Ebnezar INTRODUCTION Have you noticed how your knees look like? If you observe carefully you will see that both your knees are not parallel but deviated slightly outwards
Musculoskeletal Examination
 Musculoskeletal Examination Statement of Goals Know how to perform a complete musculoskeletal examination. Learning Objectives A. Describe the anatomy of the musculoskeletal system including the bony structures,
Musculoskeletal Examination Statement of Goals Know how to perform a complete musculoskeletal examination. Learning Objectives A. Describe the anatomy of the musculoskeletal system including the bony structures,
Functional Movement Screen (Cook, 2001)
") Functional Movement Screen (Cook, 2001) TEST 1 DEEP SQUAT Purpose - The Deep Squat is used to assess bilateral, symmetrical, mobility of the hips, knees, and ankles. The dowel held overhead assesses bilateral,
Functional Movement Screen (Cook, 2001) TEST 1 DEEP SQUAT Purpose - The Deep Squat is used to assess bilateral, symmetrical, mobility of the hips, knees, and ankles. The dowel held overhead assesses bilateral,
International Journal of Biological & Medical Research
 Int J Biol Med Res. 2013; 4(1): 2986-2990 Int J Biol Med Res Volume 3, Issue 1, Jan 2012 www.biomedscidirect.com BioMedSciDirect Publications Contents lists available at BioMedSciDirect Publications International
Int J Biol Med Res. 2013; 4(1): 2986-2990 Int J Biol Med Res Volume 3, Issue 1, Jan 2012 www.biomedscidirect.com BioMedSciDirect Publications Contents lists available at BioMedSciDirect Publications International
Therapeutic Foot Care Certificate Program Part I: Online Home Study Program
 Therapeutic Foot Care Certificate Program Part I: Online Home Study Program 1 Anatomy And Terminology Of The Lower Extremity Joan E. Edelstein, MA, PT, FISPO Associate Professor of Clinical Physical Therapy
Therapeutic Foot Care Certificate Program Part I: Online Home Study Program 1 Anatomy And Terminology Of The Lower Extremity Joan E. Edelstein, MA, PT, FISPO Associate Professor of Clinical Physical Therapy
Functional Hallux Limitus Orthotic Therapy for Hallux Valgus and Hallux Rigidus
 Pathology Specific Orthoses Evidence Based Orthotic Therapy: Functional Hallux Limitus Orthotic Therapy for Hallux Valgus and Hallux Rigidus Lawrence Z. Huppin, DPM California School of Podiatric Medicine
Pathology Specific Orthoses Evidence Based Orthotic Therapy: Functional Hallux Limitus Orthotic Therapy for Hallux Valgus and Hallux Rigidus Lawrence Z. Huppin, DPM California School of Podiatric Medicine
Functional biomechanics of the lower limb
 Functional biomechanics of the lower limb Ben and Matt. 24th July 2011 Principles of function Gravity Ground reaction Eco-concentric eccentric loading (preload) of a muscle (or group) is essential for
Functional biomechanics of the lower limb Ben and Matt. 24th July 2011 Principles of function Gravity Ground reaction Eco-concentric eccentric loading (preload) of a muscle (or group) is essential for
RN(EC) ENC(C) GNC(C) MN ACNP *** MECHANISM OF INJURY.. MOST IMPORTANT ***
 ENC(C) GNC(C) MN ACNP *** MECHANISM OF INJURY.. MOST IMPORTANT ***") HISTORY *** MECHANISM OF INJURY.. MOST IMPORTANT *** Age of patient - Certain conditions are more prevalent in particular age groups (Hip pain in children may refer to the knee from Legg-Calve-Perthes
HISTORY *** MECHANISM OF INJURY.. MOST IMPORTANT *** Age of patient - Certain conditions are more prevalent in particular age groups (Hip pain in children may refer to the knee from Legg-Calve-Perthes
Overuse Injuries & special skeletal injuries Dr M.Taghavi Director of sport medicine center of olympic academy
 Overuse Injuries & special skeletal injuries Dr M.Taghavi Director of sport medicine center of olympic academy Prevalence of Overuse Injuries 30 to 50% of all sport injuries are from overuse In some sports
Overuse Injuries & special skeletal injuries Dr M.Taghavi Director of sport medicine center of olympic academy Prevalence of Overuse Injuries 30 to 50% of all sport injuries are from overuse In some sports
THE FOOT S CONNECTED TOO... Evaluation Procedures for Orthotic Therapy Prescription 2005
 THE FOOT S CONNECTED TOO... Evaluation Procedures for Orthotic Therapy Prescription 2005 Unpublished Copyright Biomechanical Services, Inc. 2003 Biomechanical Services, Inc. 1050 Central Ave., Suite D
THE FOOT S CONNECTED TOO... Evaluation Procedures for Orthotic Therapy Prescription 2005 Unpublished Copyright Biomechanical Services, Inc. 2003 Biomechanical Services, Inc. 1050 Central Ave., Suite D
Are you suffering from heel pain? We can help you!
 Are you suffering from heel pain? We can help you! STOP THE PAIN! Heel pain can be effectively combated with the proven Body Armor Night Splint. Heel spurs and heel pain Why? Heel pain is among the most
Are you suffering from heel pain? We can help you! STOP THE PAIN! Heel pain can be effectively combated with the proven Body Armor Night Splint. Heel spurs and heel pain Why? Heel pain is among the most
Physical Examination of the Foot & Ankle
 Inspection Standing, feet straight forward facing toward examiner Swelling Deformity Flatfoot (pes planus and hindfoot valgus) High arch (pes cavus and hindfoot varus) Peek-a-boo heel Varus Too many toes
Inspection Standing, feet straight forward facing toward examiner Swelling Deformity Flatfoot (pes planus and hindfoot valgus) High arch (pes cavus and hindfoot varus) Peek-a-boo heel Varus Too many toes
Leg Posture in Children
 Leg Posture in Children Exceptional healthcare, personally delivered Leg Posture in Children A guide for parents This leaflet has been produced to provide information on the normal postural variation of
Leg Posture in Children Exceptional healthcare, personally delivered Leg Posture in Children A guide for parents This leaflet has been produced to provide information on the normal postural variation of
Financial Disclosure. Turf Toe
 Seth O Brien, CP, LP Financial Disclosure Mr. Seth O'Brien has no relevant financial relationships with commercial interests to disclose. Turf Toe Common in athletes playing on firm, artificial turf Forceful
Seth O Brien, CP, LP Financial Disclosure Mr. Seth O'Brien has no relevant financial relationships with commercial interests to disclose. Turf Toe Common in athletes playing on firm, artificial turf Forceful
Common Apophyseal Problems in the Athlete
 Disclosure Common Apophyseal Problems in the Athlete Mark Halstead, MD November 19, 2009 Faculty Disclosure Information In the past 12 months, I have no relevant financial relationships with the manufacturer
Disclosure Common Apophyseal Problems in the Athlete Mark Halstead, MD November 19, 2009 Faculty Disclosure Information In the past 12 months, I have no relevant financial relationships with the manufacturer
RUNNING MECHANICS AND INJURIES AN OVERVIEW DR. DAVID O BRIAN
 RUNNING MECHANICS AND INJURIES AN OVERVIEW DR. DAVID O BRIAN THIS IS REALLY ABOUT BIOMECHANICS OR THE MECHANICS OF OUR MUSCLES, JOINTS AND TENDONS THAT ENABLE US TO MOVE. BAD MECHANICS LEAD TO INEFFICIENCY
RUNNING MECHANICS AND INJURIES AN OVERVIEW DR. DAVID O BRIAN THIS IS REALLY ABOUT BIOMECHANICS OR THE MECHANICS OF OUR MUSCLES, JOINTS AND TENDONS THAT ENABLE US TO MOVE. BAD MECHANICS LEAD TO INEFFICIENCY
5/14/2013. Acute vs Chronic Mechanism of Injury:
 Third Annual Young Athlete Conference: The Lower Extremity February 22, 2013 Audrey Lewis, DPT Acute vs Chronic Mechanism of Injury: I. Direct: blow to the patella II. Indirect: planted foot with a valgus
Third Annual Young Athlete Conference: The Lower Extremity February 22, 2013 Audrey Lewis, DPT Acute vs Chronic Mechanism of Injury: I. Direct: blow to the patella II. Indirect: planted foot with a valgus
Multiapical Deformities p. 97 Osteotomy Concepts and Frontal Plane Realignment p. 99 Angulation Correction Axis (ACA) p. 99 Bisector Lines p.
 p. 99 Bisector Lines p.") Normal Lower Limb Alignment and Joint Orientation p. 1 Mechanical and Anatomic Bone Axes p. 1 Joint Center Points p. 5 Joint Orientation Lines p. 5 Ankle p. 5 Knee p. 5 Hip p. 8 Joint Orientation Angles
Normal Lower Limb Alignment and Joint Orientation p. 1 Mechanical and Anatomic Bone Axes p. 1 Joint Center Points p. 5 Joint Orientation Lines p. 5 Ankle p. 5 Knee p. 5 Hip p. 8 Joint Orientation Angles
Chapter Seven. Foot and ankle CHAPTER 7
 CHAPTER 7 Chapter Seven 7 c0007 Foot and ankle CHAPTER CONTENTS Overview........................ 330 Gait........................... 330 Conditions resulting in an inturned foot....... 331 Calcaneus varus/inverted
CHAPTER 7 Chapter Seven 7 c0007 Foot and ankle CHAPTER CONTENTS Overview........................ 330 Gait........................... 330 Conditions resulting in an inturned foot....... 331 Calcaneus varus/inverted
Plantar Fasciitis and Heel Pain
 PATIENT INFORMATION Plantar Fasciitis and Heel Pain What is plantar fasciitis? Heel pain and plantar fasciitis Plantar fasciitis causes pain under your heel. It usually goes in time. Treatment may speed
PATIENT INFORMATION Plantar Fasciitis and Heel Pain What is plantar fasciitis? Heel pain and plantar fasciitis Plantar fasciitis causes pain under your heel. It usually goes in time. Treatment may speed
Normal lower limb variants in children
 Link to this article online for CPD/CME credits The Royal London & Barts and The London Children s Hospitals, Barts Health NHS Trust, London E1 1BB, UK Correspondence to: A Yeo andreayeo@doctors.org.uk
Link to this article online for CPD/CME credits The Royal London & Barts and The London Children s Hospitals, Barts Health NHS Trust, London E1 1BB, UK Correspondence to: A Yeo andreayeo@doctors.org.uk
Hyperpronation of the foot causes many different
 IMMEDIATE CHANGES IN THE QUADRICEPS FEMORIS ANGLE AFTER INSERTION OF AN ORTHOTIC DEVICE D. Robert Kuhn, DC, a Terry R. Yochum, DC, b Anton R. Cherry, c and Sean S. Rodgers c ABSTRACT Objective: To measure
IMMEDIATE CHANGES IN THE QUADRICEPS FEMORIS ANGLE AFTER INSERTION OF AN ORTHOTIC DEVICE D. Robert Kuhn, DC, a Terry R. Yochum, DC, b Anton R. Cherry, c and Sean S. Rodgers c ABSTRACT Objective: To measure
AAP Boot Camp KNEE AND ANKLE EXAM
 AAP Boot Camp KNEE AND ANKLE EXAM Disclosures I have no relevant financial relationships with the manufacturers of any commercial products and or providers of commercial services discussed in this CME
AAP Boot Camp KNEE AND ANKLE EXAM Disclosures I have no relevant financial relationships with the manufacturers of any commercial products and or providers of commercial services discussed in this CME
ANKLE JOINT ANATOMY 3. TALRSALS = (FOOT BONES) Fibula. Frances Daly MSc 1 CALCANEUS 2. TALUS 3. NAVICULAR 4. CUBOID 5.
 Fibula. Frances Daly MSc 1 CALCANEUS 2. TALUS 3. NAVICULAR 4. CUBOID 5.") ANKLE JOINT ANATOMY The ankle joint is a synovial joint of the hinge type. The joint is formed by the distal end of the tibia and medial malleolus, the fibula and lateral malleolus and talus bone. It is
ANKLE JOINT ANATOMY The ankle joint is a synovial joint of the hinge type. The joint is formed by the distal end of the tibia and medial malleolus, the fibula and lateral malleolus and talus bone. It is
CHRONIC FOOT PROBLEMS FOOT and ANKLE BASICS
 CHRONIC FOOT PROBLEMS FOOT and ANKLE BASICS ABC s of Comprehensive Musculoskeletal Care December 1 st, 2007 Stephen Pinney MD Chief, UCSF Foot and Ankle Service Chronic problems typically occur gradually
CHRONIC FOOT PROBLEMS FOOT and ANKLE BASICS ABC s of Comprehensive Musculoskeletal Care December 1 st, 2007 Stephen Pinney MD Chief, UCSF Foot and Ankle Service Chronic problems typically occur gradually
Metatarsus adductus, Skew foot, Club foot 성균관대학교삼성창원병원 장현정
 Metatarsus adductus, Skew foot, Club foot 성균관대학교삼성창원병원 장현정 Metatarsus adductus Epidemiology and Etiology 0.1-12% with higher number for multiple birth Deformation and compression from intrauterine crowding
Metatarsus adductus, Skew foot, Club foot 성균관대학교삼성창원병원 장현정 Metatarsus adductus Epidemiology and Etiology 0.1-12% with higher number for multiple birth Deformation and compression from intrauterine crowding
SMALL GROUP SESSION 16 January 8 th or 10 th Shoulder pain case/ Touch workshop/ Upper and Lower Extremity Examination
 SMALL GROUP SESSION 16 January 8 th or 10 th Shoulder pain case/ Touch workshop/ Upper and Lower Extremity Examination Suggested Readings: Opatrny L. The Healing Touch. Ann Int Med 2002; 137:1003. http://www.annals.org/cgi/reprint/137/12/1003.pdf
SMALL GROUP SESSION 16 January 8 th or 10 th Shoulder pain case/ Touch workshop/ Upper and Lower Extremity Examination Suggested Readings: Opatrny L. The Healing Touch. Ann Int Med 2002; 137:1003. http://www.annals.org/cgi/reprint/137/12/1003.pdf
Could this Research Change the Way You Treat Hallux Limitus?
 Could this Research Change the Way You Treat Hallux Limitus? Lawrence Z. Huppin, D.P.M. Assistant Clinical Professor, Western University of Health Sciences, College of Podiatric Medicine Disclosure: Medical
Could this Research Change the Way You Treat Hallux Limitus? Lawrence Z. Huppin, D.P.M. Assistant Clinical Professor, Western University of Health Sciences, College of Podiatric Medicine Disclosure: Medical
Improving the Functional Strategy of the Volleyball Athlete Ron Hruska, MPA, PT
 Improving the Functional Strategy of the Volleyball Athlete Ron Hruska, MPA, PT PREPARATION PHASE Individual examination, mechanical testing and tri-planar assessment. Frontal Plane Tests: Adduction Lift
Improving the Functional Strategy of the Volleyball Athlete Ron Hruska, MPA, PT PREPARATION PHASE Individual examination, mechanical testing and tri-planar assessment. Frontal Plane Tests: Adduction Lift
Scar Engorged veins. Size of the foot [In clubfoot, small foot]
![Scar Engorged veins. Size of the foot [In clubfoot, small foot]](/thumbs/78/77722241.jpg "Scar Engorged veins. Size of the foot [In clubfoot, small foot]") 6. FOOT HISTORY Pain: Walking, Running Foot wear problem Swelling; tingly feeling Deformity Stiffness Disability: At work; recreation; night; walk; ADL, Sports Previous Rx Comorbidities Smoke, Sugar, Steroid
6. FOOT HISTORY Pain: Walking, Running Foot wear problem Swelling; tingly feeling Deformity Stiffness Disability: At work; recreation; night; walk; ADL, Sports Previous Rx Comorbidities Smoke, Sugar, Steroid
5 minutes: Attendance and Breath of Arrival. 50 minutes: Problem Solving Ankles and Feet
 5 minutes: Attendance and Breath of Arrival 50 minutes: Problem Solving Ankles and Feet Punctuality- everybody's time is precious: o o Be ready to learn by the start of class, we'll have you out of here
5 minutes: Attendance and Breath of Arrival 50 minutes: Problem Solving Ankles and Feet Punctuality- everybody's time is precious: o o Be ready to learn by the start of class, we'll have you out of here
Assessment of the Feet Handbook
 Assessment of the Feet Handbook The content of this handbook has been adapted from the assessment methods designed by Simon J. Wikler, Doctor of Surgical Chiropody Step Forward to Better Health Reflexology
Assessment of the Feet Handbook The content of this handbook has been adapted from the assessment methods designed by Simon J. Wikler, Doctor of Surgical Chiropody Step Forward to Better Health Reflexology
A Patient s Guide to Osgood-Schlatter Lesion of the Knee
 A Patient s Guide to Osgood-Schlatter Lesion of the Knee Anatomy What part of the knee is affected? Introduction An Osgood-Schlatter lesion involves pain and swelling in the small bump of bone on the front
A Patient s Guide to Osgood-Schlatter Lesion of the Knee Anatomy What part of the knee is affected? Introduction An Osgood-Schlatter lesion involves pain and swelling in the small bump of bone on the front
Patella Instability in Children and Adolescents
 Patella Instability in Children and Adolescents Description Patella Instability is an injury to the kneecap (patella) affecting the joint it forms with the thigh bone (femur) Patella Instability can occur
Patella Instability in Children and Adolescents Description Patella Instability is an injury to the kneecap (patella) affecting the joint it forms with the thigh bone (femur) Patella Instability can occur
Juvenile Osteochondroses
 Juvenile Osteochondroses Nathalie Gaulier, MD Sports Medicine Physician Cook Children s Medical Center Definition General term for disorders that affect one or more ossification centers in children Encompasses
Juvenile Osteochondroses Nathalie Gaulier, MD Sports Medicine Physician Cook Children s Medical Center Definition General term for disorders that affect one or more ossification centers in children Encompasses
A patient s guide to. Inferior Heel Pain
 A patient s guide to Inferior Heel Pain The Foot & Ankle Unit at the Royal National Orthopaedic Hospital is made up of a multi-disciplinary team. The team consists of four specialist orthopaedic foot and
A patient s guide to Inferior Heel Pain The Foot & Ankle Unit at the Royal National Orthopaedic Hospital is made up of a multi-disciplinary team. The team consists of four specialist orthopaedic foot and
Warm-Up and Stretching Exercises
 Warm-Up and Stretching Exercises Most athletes (swimmers included) use a combination of controlled movement exercises and specific joint/muscle stretching to improve performance potential. The proposed
Warm-Up and Stretching Exercises Most athletes (swimmers included) use a combination of controlled movement exercises and specific joint/muscle stretching to improve performance potential. The proposed
ANKLE PLANTAR FLEXION
 ANKLE PLANTAR FLEXION Evaluation and Measurements By Isabelle Devreux 1 Ankle Plantar Flexion: Gastrocnemius and Soleus ROM: 0 to 40-45 A. Soleus: Origin: Posterior of head of fibula and proximal1/3 of
ANKLE PLANTAR FLEXION Evaluation and Measurements By Isabelle Devreux 1 Ankle Plantar Flexion: Gastrocnemius and Soleus ROM: 0 to 40-45 A. Soleus: Origin: Posterior of head of fibula and proximal1/3 of
BIOMECHANICAL INFLUENCES ON THE SOCCER PLAYER. Planes of Lumbar Pelvic Femoral (Back, Pelvic, Hip) Muscle Function
 Muscle Function") BIOMECHANICAL INFLUENCES ON THE SOCCER PLAYER Functional performance of the soccer player reflects functional capability of certain specific muscle and muscle groups of the back, pelvis and hip to work
BIOMECHANICAL INFLUENCES ON THE SOCCER PLAYER Functional performance of the soccer player reflects functional capability of certain specific muscle and muscle groups of the back, pelvis and hip to work
Knee Pain Solutions. Assess Your Pain. Make a Plan. Take Action
 Knee Pain Solutions Assess Your Pain Make a Plan Take Action By Jared Evans Certified Strength and Conditioning Specialist Giammalva Fitness Director There are many different causes of knee pain and understanding
Knee Pain Solutions Assess Your Pain Make a Plan Take Action By Jared Evans Certified Strength and Conditioning Specialist Giammalva Fitness Director There are many different causes of knee pain and understanding
19 LEG LENGTH DISCREPANCY
 19 LEG LENGTH DISCREPANCY What is Leg Length Discrepancy? A leg length discrepancy (LLD) exists when one leg is longer than the other with respect to the same individual. Such discrepancies are relatively
19 LEG LENGTH DISCREPANCY What is Leg Length Discrepancy? A leg length discrepancy (LLD) exists when one leg is longer than the other with respect to the same individual. Such discrepancies are relatively
Chapter 10: Flexibility
 Chapter 10: Flexibility Lesson 10.1: Flexibility Facts Self-Assessment 10: Arm, Leg, and Trunk Flexibility Lesson Objectives: Describe the characteristics of flexibility. Explain how you benefit from good
Chapter 10: Flexibility Lesson 10.1: Flexibility Facts Self-Assessment 10: Arm, Leg, and Trunk Flexibility Lesson Objectives: Describe the characteristics of flexibility. Explain how you benefit from good
2. Iliotibial Band syndrome
 2. Iliotibial Band syndrome Iliotibial band (ITB) syndrome (so called runners knee although often seen in other sports e.g. cyclists and hill walkers). It is usually an overuse injury with pain felt on
2. Iliotibial Band syndrome Iliotibial band (ITB) syndrome (so called runners knee although often seen in other sports e.g. cyclists and hill walkers). It is usually an overuse injury with pain felt on
2/24/2014. Outline. Anterior Orthotic Management for the Chronic Post Stroke Patient. Terminology. Terminology ROM. Physical Evaluation
 Outline Anterior Orthotic Management for the Chronic Post Stroke Patient Physical Evaluation Design Considerations Orthotic Design Jason M. Jennings CPO, LPO, FAAOP jajennings@hanger.com Primary patterning
Outline Anterior Orthotic Management for the Chronic Post Stroke Patient Physical Evaluation Design Considerations Orthotic Design Jason M. Jennings CPO, LPO, FAAOP jajennings@hanger.com Primary patterning
PRIMARY CARE EXAMINATION OF KEY JOINTS. Thomas M. Howard, MD, FACSM FFPC Sports Medicine
 PRIMARY CARE EXAMINATION OF KEY JOINTS Thomas M. Howard, MD, FACSM FFPC Sports Medicine General exam principles: Expose entire joint and opposite limb for comparison Have a Differential Diagnosis Exam
PRIMARY CARE EXAMINATION OF KEY JOINTS Thomas M. Howard, MD, FACSM FFPC Sports Medicine General exam principles: Expose entire joint and opposite limb for comparison Have a Differential Diagnosis Exam
Conservative management of idiopathic clubfoot: Kite versus Ponseti method
 Journal of Orthopaedic Surgery 2009;17(1):67-71 Conservative management of idiopathic clubfoot: Kite versus Ponseti method AV Sanghvi, 1 VK Mittal 2 1 Department of Orthopaedics, Government Medical College
Journal of Orthopaedic Surgery 2009;17(1):67-71 Conservative management of idiopathic clubfoot: Kite versus Ponseti method AV Sanghvi, 1 VK Mittal 2 1 Department of Orthopaedics, Government Medical College
CHAPTER 8: THE BIOMECHANICS OF THE HUMAN LOWER EXTREMITY
 CHAPTER 8: THE BIOMECHANICS OF THE HUMAN LOWER EXTREMITY _ 1. The hip joint is the articulation between the and the. A. femur, acetabulum B. femur, spine C. femur, tibia _ 2. Which of the following is
CHAPTER 8: THE BIOMECHANICS OF THE HUMAN LOWER EXTREMITY _ 1. The hip joint is the articulation between the and the. A. femur, acetabulum B. femur, spine C. femur, tibia _ 2. Which of the following is
Common Injuries & Ailments
 Common Injuries & Ailments Basic Understanding Tendonitis/ Soft tissue injuries Tendonitis is an inflammation of a tendon. It typically has a pattern of pain when it s cool, improves when it warms up,
Common Injuries & Ailments Basic Understanding Tendonitis/ Soft tissue injuries Tendonitis is an inflammation of a tendon. It typically has a pattern of pain when it s cool, improves when it warms up,
My Technique for Adjusting the Excessively Pronated Foot
 My Technique for Adjusting the Excessively Pronated Foot by Mark N. Charrette, DC One can think of Chiropractic in terms of science, art, and philosophy. The art or application of Chiropractic technique
My Technique for Adjusting the Excessively Pronated Foot by Mark N. Charrette, DC One can think of Chiropractic in terms of science, art, and philosophy. The art or application of Chiropractic technique
AACPDM IC#21 DFEO+PTA 1
 Roles of Distal Femoral Extension Osteotomy and Patellar Tendon Advancement in the Treatment of Severe Persistent Crouch Gait in Adolescents and Young Adults with Cerebral Palsy Instructional Course #21
Roles of Distal Femoral Extension Osteotomy and Patellar Tendon Advancement in the Treatment of Severe Persistent Crouch Gait in Adolescents and Young Adults with Cerebral Palsy Instructional Course #21
Practical advice when treating feet
 Practical advice when treating feet Helen Mandic Clinical Lead Podiatrist in Health Promotion and Student Mentor Department of Podiatry and Foot Health Dawlish Hospital Falls Prevention The Role of the
Practical advice when treating feet Helen Mandic Clinical Lead Podiatrist in Health Promotion and Student Mentor Department of Podiatry and Foot Health Dawlish Hospital Falls Prevention The Role of the
Functional Movement Test. Deep Squat
 Functional Movement Test Put simply, the FMS is a ranking and grading system that documents movement patterns that are key to normal function. By screening these patterns, the FMS readily identifies functional
Functional Movement Test Put simply, the FMS is a ranking and grading system that documents movement patterns that are key to normal function. By screening these patterns, the FMS readily identifies functional
LEG LENGTH INEQUALITY: Sports Medicine Perspective
 LEG LENGTH INEQUALITY: Sports Medicine Perspective Debra A. Zillmer, M.D. M&M Orthopaedics, Ltd 18 Year Old Experienced Cross Country Runner: Sept Sr Year Pain in left lower leg with running Pain now prevents
LEG LENGTH INEQUALITY: Sports Medicine Perspective Debra A. Zillmer, M.D. M&M Orthopaedics, Ltd 18 Year Old Experienced Cross Country Runner: Sept Sr Year Pain in left lower leg with running Pain now prevents
Patellofemoral Pain Syndrome
 What is patellofemoral pain syndrome? Patellofemoral Pain Syndrome Patellofemoral pain syndrome is pain behind the kneecap. It has been given many names, including patellofemoral disorder, patellar malalignment,
What is patellofemoral pain syndrome? Patellofemoral Pain Syndrome Patellofemoral pain syndrome is pain behind the kneecap. It has been given many names, including patellofemoral disorder, patellar malalignment,
Richie Brace Treatment Guide: Tips for Evaluation, Casting, Prescription, Modifications and Troubleshooting
 Richie Brace Treatment Guide: Tips for Evaluation, Casting, Prescription, Modifications and Troubleshooting TABLE OF CONTENTS PAGES General Considerations 1-2 Conditions Adult Acquired Flatfoot (PTTD)
Richie Brace Treatment Guide: Tips for Evaluation, Casting, Prescription, Modifications and Troubleshooting TABLE OF CONTENTS PAGES General Considerations 1-2 Conditions Adult Acquired Flatfoot (PTTD)
METATARSAL FRACTURE (Including Jones and Dancer s Fractures)
") METATARSAL FRACTURE (Including Jones and Dancer s Fractures) Description Possible Complications Metatarsal fracture is a broken bone (fracture) in the middle Nonunion (fracture does not heal, particularly
METATARSAL FRACTURE (Including Jones and Dancer s Fractures) Description Possible Complications Metatarsal fracture is a broken bone (fracture) in the middle Nonunion (fracture does not heal, particularly
Foot and Ankle Natalie Stork, MD
 Foot and Ankle Natalie Stork, MD Assistant Professor University of Missouri-Kansas City School of Medicine, Department of Orthopaedic Surgery and Department of Pediatrics Children s Mercy Kansas City,
Foot and Ankle Natalie Stork, MD Assistant Professor University of Missouri-Kansas City School of Medicine, Department of Orthopaedic Surgery and Department of Pediatrics Children s Mercy Kansas City,
Theuseofgaitanalysisin orthopaedic surgical treatment in children with cerebral palsy
 Theuseofgaitanalysisin orthopaedic surgical treatment in children with cerebral palsy Aim of treatment Correction of functional disorder Requires analysis of function Basis for decision making Basis for
Theuseofgaitanalysisin orthopaedic surgical treatment in children with cerebral palsy Aim of treatment Correction of functional disorder Requires analysis of function Basis for decision making Basis for
Arthritic history is similar to that of the hip. Add history of give way and locking, swelling
 KNEE VASU PAI Arthritic history is similar to that of the hip. Add history of give way and locking, swelling INJURY MECHANISM When How Sequence Progress Disability IKDC Activity I - Strenuous activity
KNEE VASU PAI Arthritic history is similar to that of the hip. Add history of give way and locking, swelling INJURY MECHANISM When How Sequence Progress Disability IKDC Activity I - Strenuous activity
ILIOTIBIAL BAND SYNDROME
 Dr. S. Matthew Hollenbeck, MD Kansas Orthopaedic Center, PA 7550 West Village Circle, Wichita, KS 67205 2450 N Woodlawn, Wichita, KS 67220 Phone: (316) 838-2020 Fax: (316) 838-7574 Description ILIOTIBIAL
Dr. S. Matthew Hollenbeck, MD Kansas Orthopaedic Center, PA 7550 West Village Circle, Wichita, KS 67205 2450 N Woodlawn, Wichita, KS 67220 Phone: (316) 838-2020 Fax: (316) 838-7574 Description ILIOTIBIAL
Four weeks of Intrauterine life
 Objective Congenital & Developmental Malformation Overview of Musculoskeletal dev. Abnormal pattern of dev. Common upper & lower ext. abnormalities READ : SPINE and more information in text book Definition
Objective Congenital & Developmental Malformation Overview of Musculoskeletal dev. Abnormal pattern of dev. Common upper & lower ext. abnormalities READ : SPINE and more information in text book Definition
ANKLE SPRAINS. Explanation. Causes. Symptoms
 ANKLE SPRAINS Explanation Ankle sprains occur when ligaments in the ankle are partially or completely torn due to sudden stretching, either laterally or medially, or when the ankle is suddenly twisted
ANKLE SPRAINS Explanation Ankle sprains occur when ligaments in the ankle are partially or completely torn due to sudden stretching, either laterally or medially, or when the ankle is suddenly twisted
MEDIAL TIBIAL STRESS SYNDROME (Shin Splints)
") MEDIAL TIBIAL STRESS SYNDROME (Shin Splints) Description Expected Outcome Shin splints is a term broadly used to describe pain in the lower extremity brought on by exercise or athletic activity. Most commonly
MEDIAL TIBIAL STRESS SYNDROME (Shin Splints) Description Expected Outcome Shin splints is a term broadly used to describe pain in the lower extremity brought on by exercise or athletic activity. Most commonly
Nicky Schmidt PT, C/NDT 1
 Preparing the foot for third rocker and initial contact Nicky Schmidt PT, C/NDT copyright 2012 References Laboratory Strategies developed and taught by Nicky Schmidt, P.T. in the NDTA Approved Advanced
Preparing the foot for third rocker and initial contact Nicky Schmidt PT, C/NDT copyright 2012 References Laboratory Strategies developed and taught by Nicky Schmidt, P.T. in the NDTA Approved Advanced