REHABILITATION FOR SHOULDER FRACTURES & SURGERIES. Clavicle fractures Proximal head of humerus fractures
|
|
|
- Nancy Jennings
- 5 years ago
- Views:
Transcription


1 REHABILITATION FOR SHOULDER FRACTURES & SURGERIES Clavicle fractures Proximal head of humerus fractures


2 By Dr. Mohamed Behiry Lecturer Department of physical therapy for Orthopaedic and its surgery. Delta University for science and technology
3 Objectives At the completion of this lecture the student will be able to : 1. Describe the classification of clavicle and proximal humeral head fractures. 2. Describe the mechanism of injury. 3. Summarize the rehabilitation goals of these fractures. 4. Plan an effective rehabilitation prescription for these fractures management. 5. Plan an effective home program and instruct the patient in its use.
 Group II-fracture of the lateral")
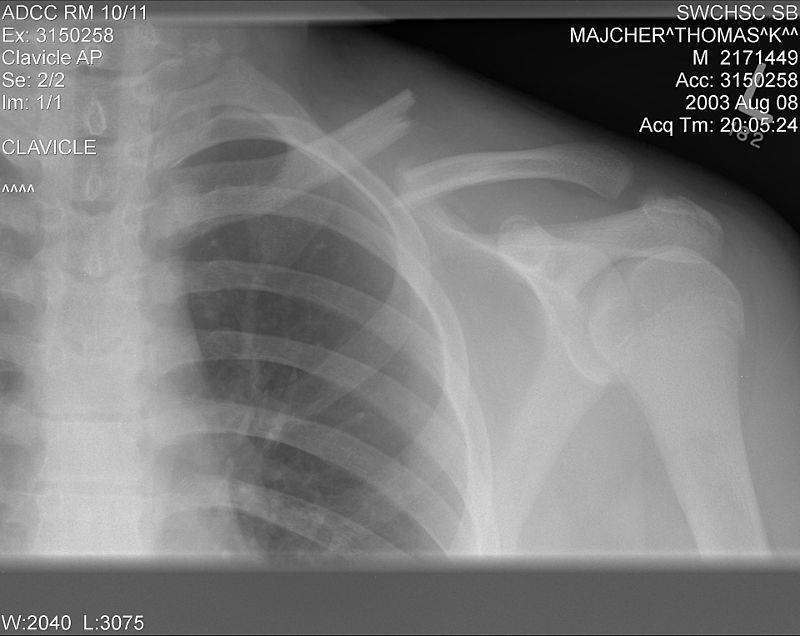
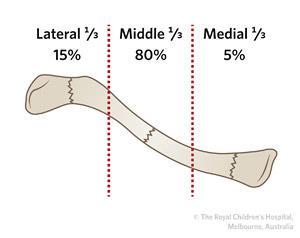
4 Clavicle Fractures Classification There is more than one accepted classification for clavicle fractures. The following is Craig's classification: Group I-fracture of the middle one third (most clavicular fractures are group I fractures) Group II-fracture of the lateral or distal one third Group III-fracture of the medial one third
5
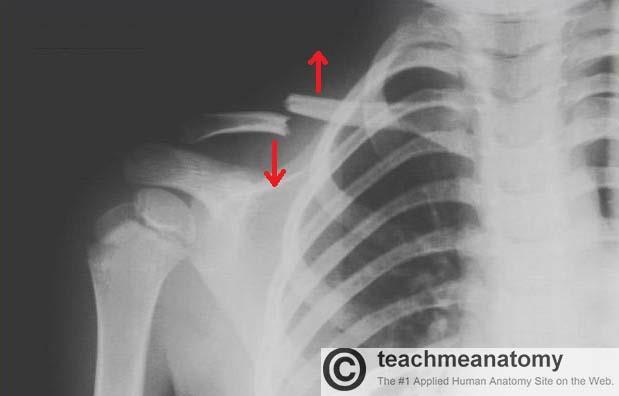
6 Mechanism of Injury Most clavicle fractures are caused by a fall or other direct trauma to the shoulder Falls on an outstretched hand (FOOSH), although commonly cited, account for a smaller percentage of clavicle fractures.

7
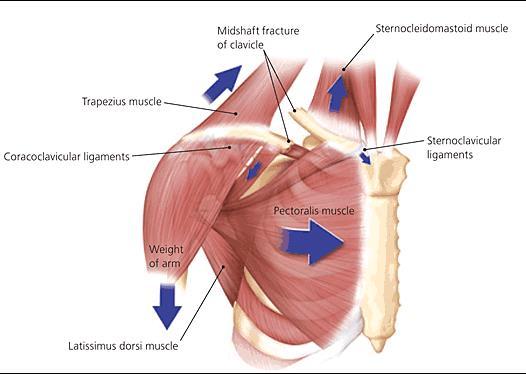
8 Treatment Goals Rehabilitation Objectives 1-Restore and improve the range of motion of the shoulder 2-Improve the strength of the following muscles: Sternocleidomastoid (neck rotation) Pectoralis major (arm adduction) Deltoid (arm abduction) 3-Improve and restore the function of the shoulder for activities of daily living and sports activities. Expected Time of Bone Healing Six to 12 weeks. Expected Duration of Rehabilitation Ten to 12 weeks.
9 Methods of Treatment Sling or Supportive Immobilization This is the method of choice for most clavicle fractures. Many comparisons of plain sling treatment to figure-of-eight bracing in adults have shown no difference. Open Reduction and Internal Fixation Open reduction and internal fixation is the method of choice for open fractures


10 Arm sling figure-of-eight bracing
11 TREATMENT Treatment: Early to Immediate (Day of Injury to One Week) BONE HEALING Stability at fracture site: None. Stage of bone healing: Inflammatory phase. X-ray: No callus.
12 Prescription Precautions: Shoulder is held in adduction and internal rotation. Elbow is maintained at 90 degrees of flexion. Range of Motion: No range of motion to the shoulder. Full, active range of motion is encouraged to the wrist, hand, and digits. Muscle Strength: No strengthening exercises to the shoulder, Begin isometric exercises to elbow arm and wrist 3 to 4 days after the fracture, once the pain subsides. Functional Activities: The uninvolved extremity is used in self-care and personal hygiene. Weight bearing : None.
13 Treatment: Two Weeks BONE HEALING Stability at fracture site: None to minimal Stage of bone healing: begin to reparative phase. X-ray: No to early callus. (Visible fracture line)
14 Prescription Precautions: Shoulder is held in adduction and internal rotation. Elbow is maintained at 90 degrees of flexion. Range of Motion: Gentle pendulum exercises to the shoulder in the sling as pain permits. Muscle Strength: No strengthening exercises to the shoulder. Start gentle isometric exercises to the deltoid. Functional Activities: The uninvolved extremity is used in self-care and personal hygiene. Weight bearing: None.


15 Shoulder is held in adduction and internal rotation. Elbow is maintained at 90 degrees of flexion. Gentle pendulum exercises
16 Treatment: Four to Six Weeks BONE HEALING Stability at fracture site: with bridging callus the fracture is usually stable. Stage of bone healing: Reparative phase. X-ray: Bridging callus is visible.
17 Prescription Precautions: At the end of 6 weeks, once there is good callus formation and the fracture site is stable, the sling or brace is removed, Limit abduction. Range of Motion: At the end of 6 weeks, gentle active range of motion to the shoulder is allowed. Abduction is limited to 80 degrees. Muscle Strength: Start isometric exercises to the rotator cuff and deltoids. Functional Activities: The patient uses the affected extremity for some self-care and personal hygiene. Weight bearing: None.


18 A, Isometric shoulder internal rotation. B, Isometric shoulder external rotation. C, Isometric shoulder abduction. D, Isometric shoulder flexion. E, Isometric shoulder extension.
19 Treatment: Six to Eight Weeks BONE HEALING Stability at fracture site: with bridging callus the fracture is usually stable. Stage of bone healing: Reparative phase. X-ray: Bridging callus more apparent.
20 Prescription Precautions: None. Avoid contact sports. Range of Motion: Active to active-assistive range of motion in all planes. Muscle Strength: Resistive exercises to the shoulder girdle muscles. Functional Activities: The patient uses the affected extremity for personal hygiene, self-care, stabilization, and light activities. Weight bearing: Gradual weight bearing is allowed (when pushing off from a chair or bed or using axillary crutches or a cane).
21 Treatment: Eight to Twelve Weeks Stability at fracture site: Stable. BONE HEALING Stage of bone healing: Remodeling phase. X-ray: Bridging callus is very visible. N.B frequently, it takes years for the large callus to remodel and be less visible cosmetically.
22 Prescription Precautions: None. Avoid contact sports. Range of Motion: Gentle stretching may be necessary. Active range of motion to the shoulder. Abduction is encouraged. Muscle Strength: Isometric and isotonic exercises are prescribed to the shoulder girdle muscles. Resistive exercises are prescribed. The resistance is gradually increased. Functional Activities: The involved extremity is used in self-care and functional activities. Weight bearing: Full weight bearing. N.B Contact sports should be avoided for approximately 2 months.
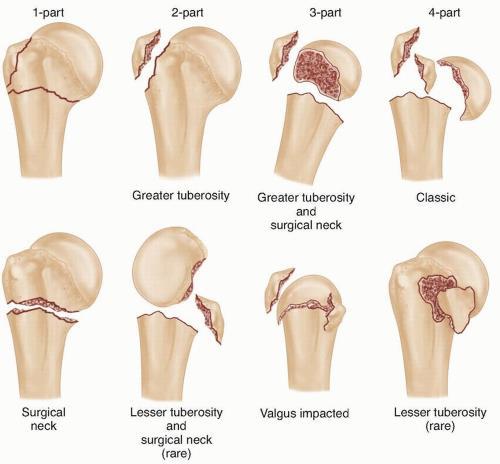
23 Proximal Humeral Fractures Definition Fractures of the proximal end of the humerus involve the humeral head, anatomic neck, and surgical neck of the humerus. Neer's classification system categorizes these fractures as one-, two-, three-, or four-part fractures based on the displacement and angulation of the parts, which are the head, shaft, greater tuberosity, and lesser tuberosity in the proximal humerus. Fractures may have associated dislocations.
24
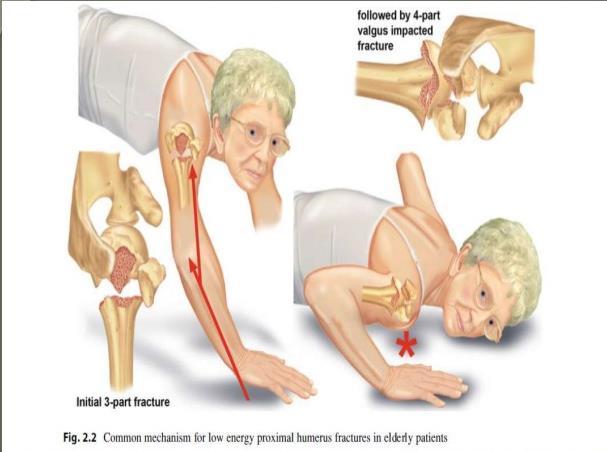
25 Mechanism of Injury Proximal humeral fractures can be caused by a fall on an elbow or an outstretched hand, especially in an elderly patient, or by trauma to the lateral aspects of the shoulder. Seizures can occasionally result in fracture/ dislocation of the shoulder.
26
27 Treatment Goals Rehabilitation Objectives 1-Restore the full range of motion of the shoulder in all planes. Frequently, there may be residual loss of range of motion secondary to the fracture 2-Improve the strength of the shoulder muscles and attempt to regain full strength against maximum resistance. Residual loss of strength, especially of the deltoid muscles, 4/5 (5/5 is full strength), may occur frequently 3-Improve and restore the function of the shoulder for activities of daily living and sports activities.
28 Methods of Treatment Sling Indications: Nondisplaced, impacted, or minimally displaced proximal humeral fractures usually are immobilized for 2 to 3 weeks until the patient's pain subsides. 85 % of proximal humeral fractures are minimally displaced. Open Reduction and Internal Fixation Indications: Open reduction and internal fixation is indicated for two- and three-part fractures and those that may also require repair of the rotator cuff External Fixator Indications: External fixation is used for open and severely comminuted fractures.
29 Expected Time of Bone Healing Six to 8 weeks. Expected Duration of Rehabilitation Twelve weeks to 1 year. Associated Injury Rotator Cuff Tears are associated with displacement of either tuberosity and require repair. Neurovascular Injuries axillary nerve or posterior cord of the brachial plexus.
30 TREATMENT Treatment: Early (Day of Injury to One Week) BONE HEALING Stability at fracture site: None. Stage of bone healing: Inflammatory phase. X-ray: No callus.
31 Prescription Precautions: Avoid shoulder motion. Range of Motion: None at the shoulder and elbow. Gentle pendulum exercises are allowed for nondisplaced fractures and hemiarthroplasty. Muscle Strength: No strengthening exercises to the elbow or shoulder are permitted. Functional Activities: One-handed activities with the uninvolved extremity. The patient needs assistance in dressing, grooming, and preparing meals. Weight Bearing: None on affected extremity.
32 Treatment: Two to Four Weeks BONE HEALING Stability at fracture site: None to minimal. Stage of bone healing: Beginning of reparative phase. X-ray: No callus; fracture line is still visible. Prescription Precautions: Avoid internal/external rotation of the shoulder because they displace the fracture. Range of Motion: Patients treated conservatively with a sling can continue with pendulum exercises.
33 Active to gentle passive exercises to the shoulder to decrease or prevent shoulder tightness and contracture e.g. lying supine, the patient can try to flex the shoulder up to 180 degrees using the other arm. Patients treated surgically should start passive range of motion in supine position. No active range of motion to the shoulder. Muscle Strength: Isometric shoulder exercises in patients treated with sling only. No strengthening exercises for patients treated with surgical intervention. Functional Activities: Patient continues with one handed activities and needs assistance in dressing, grooming, and preparing meals. Weight Bearing: None on affected extremity.


34 Active-assisted shoulder abduction. passive-assistive exercises
35 Applying moist heat before and ice after exercises minimizes swelling. The patient should do ball-squeezing exercises to maintain the strength of the intrinsic muscles of the hand. Sling At the end of 2 weeks, the sling is removed The sling is replaced at night for support or during the day when the patient feels a need for it. Open Reduction and Internal Fixation Remove sutures or staples from the operative site at 2 weeks and check for evidence of superficial infection (erythema, drainage)
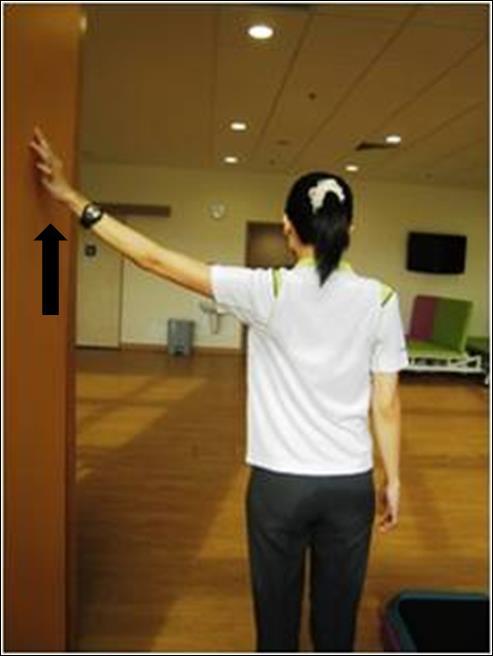
36 Range of Motion: Shoulder-limited range Flexion/abduction up to 100 to 110 degrees e.g. wall-climbing exercises (fingers against the wall and reaching up) Treatment: Four to Six Weeks BONE HEALING Stability at fracture site: With bridging callus, the fracture is usually stable. Stage of bone healing: reparative phase. X-ray: Bridging callus is visible. Prescription Precautions: Do not apply force in attempting to regain the full range of motion.
37 Internal/external rotation-limited Elbow-full range of motion in flexion, extension, supination, and pronation Surgically treated patients may continue with passive assistive range-of-motion exercises Muscle Strength: Shoulder-avoid exercises to the deltoid if it is incised during surgery Elbow-isometric and isotonic exercises
38 Functional Activities: Involved extremity used for dressing and grooming as tolerated. Patient still needs assistance in house cleaning and preparing meals. Weight Bearing: None on affected extremity. Check for early evidence of adhesive capsulitis (frozen shoulder), especially if the patient is not compliant with the rehabilitation program.


39 wall-climbing exercises Codman s pendulum.
40 Treatment: Six to Eight Weeks BONE HEALING Stability at fracture site: With bridging callus, the fracture is usually stable. Stage of bone healing: reparative phase. X-ray: Bridging callus is visible.
41 Prescription Precautions: Avoid forced range of motion. Range of Motion: Active, active-assistive, and passive range of motion to the shoulder and elbow in all planes, to tolerance. Muscle Strength: Continue isometric exercises to the shoulder. Continue with isometric and isotonic exercises to the elbow. Start progressive resistive exercises for patients treated with a sling. Functional Activities: The involved extremity is used for self-care and feeding. Weight Bearing: Weight bearing as tolerated.
42 Treatment: Eight to Twelve Weeks BONE HEALING Stability at fracture site: stable. Stage of bone healing: Remodeling phase. X-ray: Abundant callus; fracture line begins to disappear.
43 Prescription Precautions: None. Range of Motion: Active and passive range of motion to the shoulder and elbow in all planes. Muscle Strength: Resistive exercises to the shoulder with gradual increases in weights. Functional Activities: Patient should be able to use the affected extremity without significant limitations in activities of daily living and self-care. Weight Bearing: full Weight bearing.
44 References David J. Magee, Pathology and Intervention in Musculoskeletal Rehabilitation, 2nd ed Rehabilitation for the Postsurgical Orthopedic Patient, 3 rd Edition Treatment and Rehabilitation of Fractures David J. Magee, Orthopedic Physical Assessments Atlas And Video: Selected Special Testes and Movements, 5th ed James Wyss, Therapeutic programs for musculoskeletal disorders.2013
45 Thanks Dr. Mohamed Behiry Lecturer Department of physical therapy for Orthopaedic and its surgery. Delta University for science and technology
Charlotte Shoulder Institute
 Charlotte Shoulder Institute Patient Centered. Research Driven. Outcome Maximized. James R. Romanowski, M.D. Novant Health Perry & Cook Orthopedics and Sports Medicine 2826 Randolph Rd. Charlotte, NC 28211
Charlotte Shoulder Institute Patient Centered. Research Driven. Outcome Maximized. James R. Romanowski, M.D. Novant Health Perry & Cook Orthopedics and Sports Medicine 2826 Randolph Rd. Charlotte, NC 28211
Charlotte Shoulder Institute
 Charlotte Shoulder Institute Patient Centered. Research Driven. Outcome Maximized. James R. Romanowski, M.D. Novant Health Perry & Cook Orthopedics and Sports Medicine 2826 Randolph Rd. Charlotte, NC 28211
Charlotte Shoulder Institute Patient Centered. Research Driven. Outcome Maximized. James R. Romanowski, M.D. Novant Health Perry & Cook Orthopedics and Sports Medicine 2826 Randolph Rd. Charlotte, NC 28211
I have no relevant disclosures pertaining to this talk.
 Bryan Houseman, D.O., ATC Orthopaedic Trauma and Fracture Surgeon New Hampshire Orthopaedic Center September 10, 2016 I have no relevant disclosures pertaining to this talk. From Rockwood & Green, 8 th
Bryan Houseman, D.O., ATC Orthopaedic Trauma and Fracture Surgeon New Hampshire Orthopaedic Center September 10, 2016 I have no relevant disclosures pertaining to this talk. From Rockwood & Green, 8 th
Charlotte Shoulder Institute
 Charlotte Shoulder Institute Patient Centered. Research Driven. Outcome Maximized. James R. Romanowski, M.D. Gill Orthopaedic Midtown Medical Plaza 1918 Randolph Rd., Suite 700 Charlotte, NC 28211 704-342-3544
Charlotte Shoulder Institute Patient Centered. Research Driven. Outcome Maximized. James R. Romanowski, M.D. Gill Orthopaedic Midtown Medical Plaza 1918 Randolph Rd., Suite 700 Charlotte, NC 28211 704-342-3544
Orthopedics - Dr. Ahmad - Lecture 2 - Injuries of the Upper Limb
 The shoulder and the upper arm Fractures of the clavicle 1. Fall on the shoulder. 2. Fall on outstretched hand. In mid shaft fractures, the outer fragment is pulled down by the weight of the arm and the
The shoulder and the upper arm Fractures of the clavicle 1. Fall on the shoulder. 2. Fall on outstretched hand. In mid shaft fractures, the outer fragment is pulled down by the weight of the arm and the
Reverse Total Shoulder Arthroplasty Protocol Shawn Hennigan, MD
 General Information: Reverse Total Shoulder Arthroplasty Protocol Shawn Hennigan, MD Reverse or Inverse Total Shoulder Arthroplasty (rtsa) is designed specifically for the treatment of glenohumeral (GH)
General Information: Reverse Total Shoulder Arthroplasty Protocol Shawn Hennigan, MD Reverse or Inverse Total Shoulder Arthroplasty (rtsa) is designed specifically for the treatment of glenohumeral (GH)
Reverse Total Shoulder Arthroplasty Protocol
 General Information: Reverse Total Shoulder Arthroplasty Protocol Reverse or Inverse Total Shoulder Arthroplasty (rtsa) is designed specifically for the treatment of glenohumeral (GH) arthritis when it
General Information: Reverse Total Shoulder Arthroplasty Protocol Reverse or Inverse Total Shoulder Arthroplasty (rtsa) is designed specifically for the treatment of glenohumeral (GH) arthritis when it
Rehabilitation after Total Elbow Arthroplasty
 Rehabilitation after Total Elbow Arthroplasty Total Elbow Atrthroplasty Total elbow arthroplasty (TEA) Replacement of the ulnohumeral articulation with a prosthetic device. Goal of TEA is to provide pain
Rehabilitation after Total Elbow Arthroplasty Total Elbow Atrthroplasty Total elbow arthroplasty (TEA) Replacement of the ulnohumeral articulation with a prosthetic device. Goal of TEA is to provide pain
Shoulder and Elbow ORTHOPAEDIC SYPMPOSIUM APRIL 8, 2017 DANIEL DOTY MD
 Shoulder and Elbow ORTHOPAEDIC SYPMPOSIUM APRIL 8, 2017 DANIEL DOTY MD Shoulder Articulations Glenohumeral Joint 2/3 total arc of motion Shallow Ball and Socket Joint Allows for excellent ROM Requires
Shoulder and Elbow ORTHOPAEDIC SYPMPOSIUM APRIL 8, 2017 DANIEL DOTY MD Shoulder Articulations Glenohumeral Joint 2/3 total arc of motion Shallow Ball and Socket Joint Allows for excellent ROM Requires
Biceps Tenodesis Protocol
 Biceps Tenodesis Protocol A biceps tenodesis procedure involves cutting of the long head of the biceps just prior to its insertion on the superior labrum and then anchoring the tendon along its anatomical
Biceps Tenodesis Protocol A biceps tenodesis procedure involves cutting of the long head of the biceps just prior to its insertion on the superior labrum and then anchoring the tendon along its anatomical
TALLGRASS ORTHOPEDIC & SPORTS MEDICINE. Phase I Immediate Post-Surgical Phase (Weeks 0-2) Date: Maintain/protect integrity of the repair
 Date: Maintain/protect integrity of the repair") TALLGRASS ORTHOPEDIC & SPORTS MEDICINE Name: Date of Surgery: Patient Flow Sheet Arthroscopic Rotator Cuff Repair Small to Medium Tears Benedict Figuerres, MD Phase I Immediate Post-Surgical Phase (Weeks
TALLGRASS ORTHOPEDIC & SPORTS MEDICINE Name: Date of Surgery: Patient Flow Sheet Arthroscopic Rotator Cuff Repair Small to Medium Tears Benedict Figuerres, MD Phase I Immediate Post-Surgical Phase (Weeks
HUMERAL SHAFT FRACTURES. Fractures of the shaft of the humerus are common, especially in the elderly.
 HUMERAL SHAFT FRACTURES Introduction Fractures of the shaft of the humerus are common, especially in the elderly. The majority can be treated conservatively but patient coping issues may be significant.
HUMERAL SHAFT FRACTURES Introduction Fractures of the shaft of the humerus are common, especially in the elderly. The majority can be treated conservatively but patient coping issues may be significant.
Charlotte Shoulder Institute
 Charlotte Shoulder Institute Patient Centered. Research Driven. Outcome Maximized. James R. Romanowski, M.D. Novant Health Perry & Cook Orthopedics and Sports Medicine 2826 Randolph Rd. Charlotte, NC 28211
Charlotte Shoulder Institute Patient Centered. Research Driven. Outcome Maximized. James R. Romanowski, M.D. Novant Health Perry & Cook Orthopedics and Sports Medicine 2826 Randolph Rd. Charlotte, NC 28211
Reverse Total Shoulder Protocol
 Marion Herring, M.D. OrthoVirginia PH: (804) 270-1305 FX: (804) 273-9294 www.orthovirginia.com Reverse Total Shoulder Protocol General Information: Reverse Total Shoulder Arthroplasty (rtsa) is designed
Marion Herring, M.D. OrthoVirginia PH: (804) 270-1305 FX: (804) 273-9294 www.orthovirginia.com Reverse Total Shoulder Protocol General Information: Reverse Total Shoulder Arthroplasty (rtsa) is designed
PROM is not stretching!
 Dx: o Right o Left Shoulder Replacement/Hemiarthroplasty Rehab Date of Surgery: Patient Name: PT/OT: Please evaluate and treat. Follow attached protocol. 2-3 x per week x 6 weeks. Signature/Date: The intent
Dx: o Right o Left Shoulder Replacement/Hemiarthroplasty Rehab Date of Surgery: Patient Name: PT/OT: Please evaluate and treat. Follow attached protocol. 2-3 x per week x 6 weeks. Signature/Date: The intent
Ms. Ruth A. Delaney, MB BCh BAO, MMedSc, MRCS
 Ms. Ruth A. Delaney, MB BCh BAO, MMedSc, MRCS Consultant Orthopaedic Surgeon, Shoulder Specialist. +353 1 5262335 ruthdelaney@sportssurgeryclinic.com Modified from the protocol developed at Boston Shoulder
Ms. Ruth A. Delaney, MB BCh BAO, MMedSc, MRCS Consultant Orthopaedic Surgeon, Shoulder Specialist. +353 1 5262335 ruthdelaney@sportssurgeryclinic.com Modified from the protocol developed at Boston Shoulder
Type Three Rotator Cuff Repair Arthroscopic Assisted with SAD Large to Massive Tears (Greater than 4 cm)
") Type Three Rotator Cuff Repair Arthroscopic Assisted with SAD Large to Massive Tears (Greater than 4 cm) Therapist Phone I. Phase I - Immediate Post-Surgical Phase (Day 1-10) Goals: Maintain Integrity
Type Three Rotator Cuff Repair Arthroscopic Assisted with SAD Large to Massive Tears (Greater than 4 cm) Therapist Phone I. Phase I - Immediate Post-Surgical Phase (Day 1-10) Goals: Maintain Integrity
Reverse Total Shoulder
 Rehabilitation Protocol: Reverse Total Shoulder Department of Orthopaedic Surgery Lahey Hospital & Medical Center, Burlington 781-744-8650 Lahey Outpatient Center, Lexington 781-372-7020 Lahey Medical
Rehabilitation Protocol: Reverse Total Shoulder Department of Orthopaedic Surgery Lahey Hospital & Medical Center, Burlington 781-744-8650 Lahey Outpatient Center, Lexington 781-372-7020 Lahey Medical
Charlotte Shoulder Institute
 Charlotte Shoulder Institute Patient Centered. Research Driven. Outcome Maximized. James R. Romanowski, M.D. Novant Health Perry & Cook Orthopedics and Sports Medicine 2826 Randolph Rd. Charlotte, NC 28211
Charlotte Shoulder Institute Patient Centered. Research Driven. Outcome Maximized. James R. Romanowski, M.D. Novant Health Perry & Cook Orthopedics and Sports Medicine 2826 Randolph Rd. Charlotte, NC 28211
Rehabilitation Guidelines for Labral/Bankert Repair
 Rehabilitation Guidelines for Labral/Bankert Repair The true shoulder joint is called the glenohumeral joint and consists humeral head and the glenoid. It is a ball and socket joint. Anatomy of the Shoulder
Rehabilitation Guidelines for Labral/Bankert Repair The true shoulder joint is called the glenohumeral joint and consists humeral head and the glenoid. It is a ball and socket joint. Anatomy of the Shoulder
Goals. Initial management skeletal trauma. Physical Exam ABC OF PRIMARY CARE MEDICINE FRACTURE MANAGEMENT 12/4/2010
 ABC OF PRIMARY CARE MEDICINE FRACTURE MANAGEMENT Brian Feeley, MD UCSF Sports Medicine and Shoulder Surgery Goals Discuss common fractures and initial management, treatment guidelines Let your patients
ABC OF PRIMARY CARE MEDICINE FRACTURE MANAGEMENT Brian Feeley, MD UCSF Sports Medicine and Shoulder Surgery Goals Discuss common fractures and initial management, treatment guidelines Let your patients
2778 N. Webb Road Shoulder, Elbow, Wrist, Hand Wichita, KS and Arthroscopic Surgery Phone: Fax:
 Phase I: Protection Phase (Weeks 0-5) FOCUS: Passive range of motion (ROM). Minimize pain and inflammation. Maintain integrity of the repair. Regain full passive foward flexion of operated shoulder. Use
Phase I: Protection Phase (Weeks 0-5) FOCUS: Passive range of motion (ROM). Minimize pain and inflammation. Maintain integrity of the repair. Regain full passive foward flexion of operated shoulder. Use
Orthopedic Surgery and Sports Medicine FL License:
 Reverse Shoulder Arthroplasty Protocol: The intent of this protocol is to provide the therapist with a guideline for the post-operative rehabilitation course of a patient that has undergone a Reverse Shoulder
Reverse Shoulder Arthroplasty Protocol: The intent of this protocol is to provide the therapist with a guideline for the post-operative rehabilitation course of a patient that has undergone a Reverse Shoulder
Bradley C. Carofino, M.D. Shoulder Specialist 230 Clearfield Avenue, Suite 124 Virginia Beach, Virginia Phone
 Subpectoral Bicep Tenodesis Protocol (Spreadsheet) Weeks 1-2 Modalities Treatment Restrictions Goals No active elbow flexion (6weeks) Full PROM shoulder and elbow PROM: Shoulder, elbow, forearm No active
Subpectoral Bicep Tenodesis Protocol (Spreadsheet) Weeks 1-2 Modalities Treatment Restrictions Goals No active elbow flexion (6weeks) Full PROM shoulder and elbow PROM: Shoulder, elbow, forearm No active
Jennifer L. Cook, MD Stephen A. Hanff, MD. Rotator Cuff Type I Repair (Small Large Tear)
") Jennifer L. Cook, MD Stephen A. Hanff, MD Florida Joint Care Institute 2165 Little Road, Trinity, Florida 34655 PH: (727) 372 6637 FAX: (727) 375 5044 Rotator Cuff Type I Repair (Small Large Tear) This
Jennifer L. Cook, MD Stephen A. Hanff, MD Florida Joint Care Institute 2165 Little Road, Trinity, Florida 34655 PH: (727) 372 6637 FAX: (727) 375 5044 Rotator Cuff Type I Repair (Small Large Tear) This
TOTAL SHOULDER ARTHROPLASTY / HEMIARTHROPLASTY
 Teodoro P. Nissen, M.D., Q.M.E. Fellowship Trained Board Certified Joseph M. Centeno, M.D. Fellowship Trained Board Certified TOTAL SHOULDER ARTHROPLASTY / HEMIARTHROPLASTY Protocol: The intent of this
Teodoro P. Nissen, M.D., Q.M.E. Fellowship Trained Board Certified Joseph M. Centeno, M.D. Fellowship Trained Board Certified TOTAL SHOULDER ARTHROPLASTY / HEMIARTHROPLASTY Protocol: The intent of this
Rehabilitation Guidelines for Large Rotator Cuff Repair
 Rehabilitation Guidelines for Large Rotator Cuff Repair The true shoulder joint is called the glenohumeral joint and consists humeral head and the glenoid. It is a ball and socket joint. Anatomy of the
Rehabilitation Guidelines for Large Rotator Cuff Repair The true shoulder joint is called the glenohumeral joint and consists humeral head and the glenoid. It is a ball and socket joint. Anatomy of the
Anterior Labrum Repair Protocol
 Anterior Labrum Repair Protocol Stage I (0-4 weeks): Key Goals: Protect the newly repaired shoulder. Allow for decreased inflammation and healing. Maintain elbow, wrist and hand function. Maintain scapular
Anterior Labrum Repair Protocol Stage I (0-4 weeks): Key Goals: Protect the newly repaired shoulder. Allow for decreased inflammation and healing. Maintain elbow, wrist and hand function. Maintain scapular
DISCHARGE INSTRUCTIONS & PHYSICAL THERAPY PROTOCOL: Arthroscopic Rotator Cuff Repair With or Without Biceps Tenodesis
 DISCHARGE INSTRUCTIONS & PHYSICAL THERAPY PROTOCOL: Arthroscopic Rotator Cuff Repair With or Without Biceps Tenodesis Initial recovery after shoulder surgery entails healing, controlling swelling and discomfort
DISCHARGE INSTRUCTIONS & PHYSICAL THERAPY PROTOCOL: Arthroscopic Rotator Cuff Repair With or Without Biceps Tenodesis Initial recovery after shoulder surgery entails healing, controlling swelling and discomfort
Phase I : Immediate Postoperative Phase- Protected Motion. (0-2 Weeks)
") Phase I : Immediate Postoperative Phase- Protected Motion (0-2 Weeks) Appointments Progression Criteria 2 weeks after surgery Rehabilitation appointments begin within 7-10 days of surgery, continue 1-2
Phase I : Immediate Postoperative Phase- Protected Motion (0-2 Weeks) Appointments Progression Criteria 2 weeks after surgery Rehabilitation appointments begin within 7-10 days of surgery, continue 1-2
Total Shoulder Arthroplasty / Hemiarthroplasty Therapy Protocol
 Total Shoulder Arthroplasty / Hemiarthroplasty Therapy Protocol The intent of this protocol is to provide the therapist with a guideline of the postoperative rehabilitation course of a patient that has
Total Shoulder Arthroplasty / Hemiarthroplasty Therapy Protocol The intent of this protocol is to provide the therapist with a guideline of the postoperative rehabilitation course of a patient that has
The Four Phases of Healing During Rehabilitation Following Rotator Cuff Surgery. Phase 1: Immediate postoperative period (weeks 0-6) Goals
 Goals") The Four Phases of Healing During Rehabilitation Following Rotator Cuff Surgery Phase 1: Immediate postoperative period (weeks 0-6) Maintain/protect integrity of repair Gradually increase PROM Diminish
The Four Phases of Healing During Rehabilitation Following Rotator Cuff Surgery Phase 1: Immediate postoperative period (weeks 0-6) Maintain/protect integrity of repair Gradually increase PROM Diminish
After Arthroscopic Subacromial Decompression Intact Rotator Cuff (Distal Clavicle Resection)
") After Arthroscopic Subacromial Decompression Intact Rotator Cuff (Distal Clavicle Resection) Rehabilitation Protocol Phase 1: Weeks 0-4 Restrictions ROM 140 degrees of forward flexion 40 degrees of external
After Arthroscopic Subacromial Decompression Intact Rotator Cuff (Distal Clavicle Resection) Rehabilitation Protocol Phase 1: Weeks 0-4 Restrictions ROM 140 degrees of forward flexion 40 degrees of external
Superior Labrum Repair Protocol - SLAP
 Superior Labrum Repair Protocol - SLAP Stage I (0-4 weeks): Key Goals: Protect the newly repaired shoulder. Allow for decreased inflammation and healing. Maintain elbow, wrist and hand function. Maintain
Superior Labrum Repair Protocol - SLAP Stage I (0-4 weeks): Key Goals: Protect the newly repaired shoulder. Allow for decreased inflammation and healing. Maintain elbow, wrist and hand function. Maintain
Total Shoulder Rehab Protocol Dr. Payne
 Total Shoulder Rehab Protocol Dr. Payne Phase I Immediate Post Surgical Phase (0-4 weeks): Allow healing of soft tissue Maintain integrity of replaced joint Gradually increase passive range of motion (PROM)
Total Shoulder Rehab Protocol Dr. Payne Phase I Immediate Post Surgical Phase (0-4 weeks): Allow healing of soft tissue Maintain integrity of replaced joint Gradually increase passive range of motion (PROM)
Total Shoulder Arthroplasty / Hemiarthroplasty Protocol
 Adam N. Whatley, M.D. 6550 Main St., STE. 2300 Zachary, LA 70791 Phone(225)658-1808 Fax(225)658-5299 Total Shoulder Arthroplasty / Hemiarthroplasty Protocol The intent of this protocol is to provide the
Adam N. Whatley, M.D. 6550 Main St., STE. 2300 Zachary, LA 70791 Phone(225)658-1808 Fax(225)658-5299 Total Shoulder Arthroplasty / Hemiarthroplasty Protocol The intent of this protocol is to provide the
Rehabilitation Protocol: Massive Rotator Cuff Tear Repair
 Rehabilitation Protocol: Massive Rotator Cuff Tear Repair Department of Orthopaedic Surgery Lahey Hospital & Medical Center, Burlington 781-744-8650 Lahey Outpatient Center, Lexington 781-372-7020 Lahey
Rehabilitation Protocol: Massive Rotator Cuff Tear Repair Department of Orthopaedic Surgery Lahey Hospital & Medical Center, Burlington 781-744-8650 Lahey Outpatient Center, Lexington 781-372-7020 Lahey
Rotator Cuff Repair +/- Acromioplasty/Mumford. Phase I: 0 to 2 weeks after surgery
 Rotator Cuff Repair +/- Acromioplasty/Mumford 2. Ensure wound healing Phase I: 0 to 2 weeks after surgery 1. Sling: Use your sling all of the time. 2. Use of the affected arm: You may use your hand on
Rotator Cuff Repair +/- Acromioplasty/Mumford 2. Ensure wound healing Phase I: 0 to 2 weeks after surgery 1. Sling: Use your sling all of the time. 2. Use of the affected arm: You may use your hand on
Bradley C. Carofino, M.D. Shoulder Specialist 230 Clearfield Avenue, Suite 124 Virginia Beach, Virginia Phone
 Rehabilitation following Arthroscopic Rotator Cuff Repair: Medium Tears Phase I: Immediate Postsurgical Phase (Days 10-14) Precautions: No lifting of objects; No excessive arm motions; No excessive external
Rehabilitation following Arthroscopic Rotator Cuff Repair: Medium Tears Phase I: Immediate Postsurgical Phase (Days 10-14) Precautions: No lifting of objects; No excessive arm motions; No excessive external
Progression to the next phase based on Clinic Criteria and or Time Frames as Appropriate
 Bicep Tenodesis D. WATTS, M.D. Progression to the next phase based on Clinic Criteria and or Time Frames as Appropriate PHASE I PASSIVE RANG OF MOTION PHASE (STARTS APPROXIMATELY POST OP WEEKS 1-2) Minimize
Bicep Tenodesis D. WATTS, M.D. Progression to the next phase based on Clinic Criteria and or Time Frames as Appropriate PHASE I PASSIVE RANG OF MOTION PHASE (STARTS APPROXIMATELY POST OP WEEKS 1-2) Minimize
Biceps Tenodesis Protocol
 Robert K. Fullick, MD 6400 Fannin Street, Suite 1700 Houston, Texas 77030 Ph.: 713-486-7543 / Fx.: 713-486-5549 Biceps Tenodesis Protocol The intent of this protocol is to provide the clinician with a
Robert K. Fullick, MD 6400 Fannin Street, Suite 1700 Houston, Texas 77030 Ph.: 713-486-7543 / Fx.: 713-486-5549 Biceps Tenodesis Protocol The intent of this protocol is to provide the clinician with a
Diagnosis: s/p ( LEFT / RIGHT ) AC Joint Reconstruction -- Surgery Date:
 AC Joint Reconstruction -- Surgery Date:") UCLA OUTPATIENT REHABILITATION SERVICES! SANTA MONICA! WESTWOOD 1000 Veteran Ave., A level Phone: (310) 794-1323 Fax: (310) 794-1457 1260 15 th St, Ste. 900 Phone: (310) 319-4646 Fax: (310) 319-2269 FOR
UCLA OUTPATIENT REHABILITATION SERVICES! SANTA MONICA! WESTWOOD 1000 Veteran Ave., A level Phone: (310) 794-1323 Fax: (310) 794-1457 1260 15 th St, Ste. 900 Phone: (310) 319-4646 Fax: (310) 319-2269 FOR
Avon Office 2 Simsbury Rd. Avon, CT Office: (860) Fax: (860) REHABILITATION AFTER REVERSE SHOULDER ARTHROPLASTY
 Fax: (860) REHABILITATION AFTER REVERSE SHOULDER ARTHROPLASTY") Katherine J. Coyner, MD UCONN Musculoskeletal Institute Medical Arts & Research Building 263 Farmington Ave. Farmington, CT 06030 Office: (860) 679-6600 Fax: (860) 679-6649 www.drcoyner.com Avon Office
Katherine J. Coyner, MD UCONN Musculoskeletal Institute Medical Arts & Research Building 263 Farmington Ave. Farmington, CT 06030 Office: (860) 679-6600 Fax: (860) 679-6649 www.drcoyner.com Avon Office
Christopher K. Jones, MD Colorado Springs Orthopaedic Group
 Christopher K. Jones, MD Colorado Springs Orthopaedic Group 719-632-7669 Total Shoulder Replacement You have undergone a shoulder replacement procedure. The performance of the procedure is complete, but
Christopher K. Jones, MD Colorado Springs Orthopaedic Group 719-632-7669 Total Shoulder Replacement You have undergone a shoulder replacement procedure. The performance of the procedure is complete, but
(PROTOCOL #18) REVERSE TOTAL SHOULDER ARTHROPLASTY PROTOCOL
 REVERSE TOTAL SHOULDER ARTHROPLASTY PROTOCOL") The following is a set of general guidelines. It is important to remember that each patient is different. The progression of the patient depends on many factors including age and medical health of the
The following is a set of general guidelines. It is important to remember that each patient is different. The progression of the patient depends on many factors including age and medical health of the
Reverse Geometry Shoulder Arthroplasty
 1.0 Policy Statement... 2 2.0 Purpose... 2 3.0 Scope... 2 4.0 Health & Safety... 2 5.0 Responsibilities... 2 6.0 Definitions and Abbreviations... 3 7.0 Guideline... 3 7.1 Pre-Operative... 3 7.2 Post-Operative...
1.0 Policy Statement... 2 2.0 Purpose... 2 3.0 Scope... 2 4.0 Health & Safety... 2 5.0 Responsibilities... 2 6.0 Definitions and Abbreviations... 3 7.0 Guideline... 3 7.1 Pre-Operative... 3 7.2 Post-Operative...
Arthroscopic Rotator Cuff Repair Protocol:
 Arthroscopic Rotator Cuff Repair Protocol: The intent of this protocol is to provide the therapist and patient with guidelines for the post-operative rehabilitation course after arthroscopic SLAP repair.
Arthroscopic Rotator Cuff Repair Protocol: The intent of this protocol is to provide the therapist and patient with guidelines for the post-operative rehabilitation course after arthroscopic SLAP repair.
Rotator Cuff Repair Small Tear with possible: Subacromial Decompression, Distal Clavicle Excision, Biceps Tenodesis, Biceps Tenotomy
 Rotator Cuff Repair Small Tear with possible: Subacromial Decompression, Distal Clavicle Excision, Biceps Tenodesis, Biceps Tenotomy As tolerated should be understood to perform with safety for the repair.
Rotator Cuff Repair Small Tear with possible: Subacromial Decompression, Distal Clavicle Excision, Biceps Tenodesis, Biceps Tenotomy As tolerated should be understood to perform with safety for the repair.
Rehabilitation Guidelines for Total Shoulder Arthroplasty and Hemi-arthroplasty
 Rehabilitation Guidelines for Total Shoulder Arthroplasty and Hemi-arthroplasty Josef K. Eichinger, MD General Information Total Recovery time is between 4-6 months depending on factors such as injury
Rehabilitation Guidelines for Total Shoulder Arthroplasty and Hemi-arthroplasty Josef K. Eichinger, MD General Information Total Recovery time is between 4-6 months depending on factors such as injury
Rotator Cuff Repair Protocol for tear involving Subscapularis Tendon with or without Pectoralis Major Tendon Transfer
 Rotator Cuff Repair Protocol for tear involving Subscapularis Tendon with or without Pectoralis Major Tendon Transfer D. WATTS, MD Precautions: BASIS Tendon healing back to bone is a slow process that
Rotator Cuff Repair Protocol for tear involving Subscapularis Tendon with or without Pectoralis Major Tendon Transfer D. WATTS, MD Precautions: BASIS Tendon healing back to bone is a slow process that
Title Protocol for the Management of Shoulder Injuries in MIUs and WICs
 Document Control Title in MIUs and WICs Author Author s job title Professional Lead, Minor Injuries Unit Directorate, Logistics and Resilience Department Emergency Department Version Date Issued Status
Document Control Title in MIUs and WICs Author Author s job title Professional Lead, Minor Injuries Unit Directorate, Logistics and Resilience Department Emergency Department Version Date Issued Status
Ms. Ruth A. Delaney, MB BCh BAO, MMedSc, MRCS
 Ms. Ruth A. Delaney, MB BCh BAO, MMedSc, MRCS Consultant Orthopaedic Surgeon, Shoulder Specialist. +353 1 5262335 ruthdelaney@sportssurgeryclinic.com Modified from the protocol developed at Boston Shoulder
Ms. Ruth A. Delaney, MB BCh BAO, MMedSc, MRCS Consultant Orthopaedic Surgeon, Shoulder Specialist. +353 1 5262335 ruthdelaney@sportssurgeryclinic.com Modified from the protocol developed at Boston Shoulder
Anterior Stabilization of the Shoulder: Distal Tibial Allograft
 Anterior Stabilization of the Shoulder: Distal Tibial Allograft Name: Diagnosis: Date: Date of Surgery: Phase I Immediate Post Surgical Phase (approximately Weeks 1-3) Minimize shoulder pain and inflammatory
Anterior Stabilization of the Shoulder: Distal Tibial Allograft Name: Diagnosis: Date: Date of Surgery: Phase I Immediate Post Surgical Phase (approximately Weeks 1-3) Minimize shoulder pain and inflammatory
Distal Biceps Repair/Reconstruction Protocol
 SPORTS & ORTHOPAEDIC SPECIALISTS Distal Biceps Repair/Reconstruction Protocol 6-10 visits over 4-6 months Maintain shoulder ROM while immobilized during early phase of healing During recovery, pulling
SPORTS & ORTHOPAEDIC SPECIALISTS Distal Biceps Repair/Reconstruction Protocol 6-10 visits over 4-6 months Maintain shoulder ROM while immobilized during early phase of healing During recovery, pulling
REHABILITATION GUIDELINES FOR ROTATOR CUFF REPAIR FOR TYPE II TEARS (MASSIVE)(+/- SUBACROMIAL DECOMPRESSION)
(+/- SUBACROMIAL DECOMPRESSION)") REHABILITATION GUIDELINES FOR ROTATOR CUFF REPAIR FOR TYPE II TEARS (MASSIVE)(+/- SUBACROMIAL DECOMPRESSION) The rehabilitation guidelines are presented in a criterion based progression. General time frames
REHABILITATION GUIDELINES FOR ROTATOR CUFF REPAIR FOR TYPE II TEARS (MASSIVE)(+/- SUBACROMIAL DECOMPRESSION) The rehabilitation guidelines are presented in a criterion based progression. General time frames
POST-SURGICAL POSTERIOR GLENOHUMERAL STABILIZATION REHABILITATION PROTOCOL (Capsulolabral Repair)
") Gregory N. Lervick, MD Andrew Anderson, PA-C 952-456-7111 POST-SURGICAL POSTERIOR GLENOHUMERAL STABILIZATION REHABILITATION PROTOCOL (Capsulolabral Repair) Open Arthroscopic Phase 1: Weeks 0-4 No shoulder
Gregory N. Lervick, MD Andrew Anderson, PA-C 952-456-7111 POST-SURGICAL POSTERIOR GLENOHUMERAL STABILIZATION REHABILITATION PROTOCOL (Capsulolabral Repair) Open Arthroscopic Phase 1: Weeks 0-4 No shoulder
SHOULDER ARTHROSCOPY WITH ANTERIOR STABILIZATION / CAPSULORRHAPHY REHABILITATION PROTOCOL
 General Notes As tolerated should be understood to include with safety for the surgical procedure; a sudden increase in pain, swelling, or other undesirable factors are indicators that you are doing too
General Notes As tolerated should be understood to include with safety for the surgical procedure; a sudden increase in pain, swelling, or other undesirable factors are indicators that you are doing too
SHOULDER INSTABILITY
 Disclaimer This movie is an educational resource only and should not be used to manage Orthopaedic health. All decisions about the management of Shoulder Instability must be made in conjunction with your
Disclaimer This movie is an educational resource only and should not be used to manage Orthopaedic health. All decisions about the management of Shoulder Instability must be made in conjunction with your
REVERSE SHOULDER REPLACEMENT
 REVERSE SHOULDER REPLACEMENT The Reverse Shoulder Replacement is designed specifically for the use in shoulders with a deficient rotator cuff and arthritis, as well as other difficult shoulder reconstructive
REVERSE SHOULDER REPLACEMENT The Reverse Shoulder Replacement is designed specifically for the use in shoulders with a deficient rotator cuff and arthritis, as well as other difficult shoulder reconstructive
Shoulder Arthroscopy with Posterior Labral Repair Rehabilitation Protocol
 General Notes: As tolerated should be understood to include with safety for the surgical procedure; a sudden increase in pain, swelling, or other undesirable factors are indicators that you are doing too
General Notes: As tolerated should be understood to include with safety for the surgical procedure; a sudden increase in pain, swelling, or other undesirable factors are indicators that you are doing too
Protocol S8 Physical Therapy Protocol for Arthroscopic Reverse Bankart Repair or Open Posterior Capsulorrhaphy
 Phase I: Protection Phase (0-5 weeks) Allow time for labral repair to heal. Gradually increase shoulder passive range of motion (ROM) Use pain medications as needed. Wear shoulder immobilizer for 5 weeks.
Phase I: Protection Phase (0-5 weeks) Allow time for labral repair to heal. Gradually increase shoulder passive range of motion (ROM) Use pain medications as needed. Wear shoulder immobilizer for 5 weeks.
Shoulder Arthroscopy with Rotator Cuff Repair Rehabilitation Protocol
 General Notes: As tolerated should be understood to include with safety for the surgical procedure; a sudden increase in pain, swelling, or other undesirable factors are indicators that you are doing too
General Notes: As tolerated should be understood to include with safety for the surgical procedure; a sudden increase in pain, swelling, or other undesirable factors are indicators that you are doing too
Fractures of the shoulder girdle, elbow and fractures of the humerus. H. Sithebe 2012
 Fractures of the shoulder girdle, elbow and fractures of the humerus H. Sithebe 2012 Fractures of the Clavicle (mid-shaft). Fractures of the clavicle Fractures of the clavicle Treatment- conservative.
Fractures of the shoulder girdle, elbow and fractures of the humerus H. Sithebe 2012 Fractures of the Clavicle (mid-shaft). Fractures of the clavicle Fractures of the clavicle Treatment- conservative.
Proximal Humerus Fractures
 Proximal Humerus Fractures Trafford General Hospital, June 2010 Nehmat Singh, Jawad Sultan Anatomy of the Proximal Humerus Consists of four parts: humeral head, surgical neck and greater and lesser tubercles
Proximal Humerus Fractures Trafford General Hospital, June 2010 Nehmat Singh, Jawad Sultan Anatomy of the Proximal Humerus Consists of four parts: humeral head, surgical neck and greater and lesser tubercles
Shoulder Arthroplasty
 Shoulder Arthroplasty Nathan G. Everding, MD Specializing in Hand, Wrist, Elbow & Shoulder Surgery Syracuse Orthopedic Specialists SJH Family Practice Refresher course 3/8/19 Shoulder Arthroplasty Rate
Shoulder Arthroplasty Nathan G. Everding, MD Specializing in Hand, Wrist, Elbow & Shoulder Surgery Syracuse Orthopedic Specialists SJH Family Practice Refresher course 3/8/19 Shoulder Arthroplasty Rate
ROTATOR CUFF TEAR, SURGERY FOR
 ROTATOR CUFF TEAR, SURGERY FOR Indications (Who Needs Surgery, When, electricity is used to cauterize small capillaries. Electricity or Why, and Goals) a motorized shaver is used to remove the bursa and
ROTATOR CUFF TEAR, SURGERY FOR Indications (Who Needs Surgery, When, electricity is used to cauterize small capillaries. Electricity or Why, and Goals) a motorized shaver is used to remove the bursa and
SUPERIOR LABRAL REPAIRS
 LOURDES MEDICAL ASSOCIATES Sean Mc Millan, DO Director of Orthopaedic Sports Medicine & Arthroscopy 2103 Burlington-Mount Holly Rd Burlington, NJ 08016 (609) 747-9200 (office) (609) 747-1408 (fax) http://orthodoc.aaos.org/drmcmillan
LOURDES MEDICAL ASSOCIATES Sean Mc Millan, DO Director of Orthopaedic Sports Medicine & Arthroscopy 2103 Burlington-Mount Holly Rd Burlington, NJ 08016 (609) 747-9200 (office) (609) 747-1408 (fax) http://orthodoc.aaos.org/drmcmillan
Rotator Cuff Repair Protocol
 Rotator Cuff Repair Protocol Overview a. Begin passive shoulder ROM after surgery (beginning week 1) b. Active assist ROM beginning week 7 after surgery (weeks 7-8) c. Active ROM beginning week 9 after
Rotator Cuff Repair Protocol Overview a. Begin passive shoulder ROM after surgery (beginning week 1) b. Active assist ROM beginning week 7 after surgery (weeks 7-8) c. Active ROM beginning week 9 after
Latarjet Repair Rehabilitation Protocol
 General Notes: As tolerated should be understood to include with safety for the reconstruction/repair; a sudden increase in pain, swelling, or other undesirable factors are indicators that you are doing
General Notes: As tolerated should be understood to include with safety for the reconstruction/repair; a sudden increase in pain, swelling, or other undesirable factors are indicators that you are doing
Frozen Shoulder Syndrome Rehabilitation Using the Resistance Chair
 Frozen Shoulder Syndrome Rehabilitation Using the Resistance Chair General Information Frozen shoulder is a condition where the shoulder joint (glenohumeral joint) gradually becomes stiff, resulting in
Frozen Shoulder Syndrome Rehabilitation Using the Resistance Chair General Information Frozen shoulder is a condition where the shoulder joint (glenohumeral joint) gradually becomes stiff, resulting in
ROTATOR CUFF REPAIR REHAB PROTOCOL
 Jayesh K. Patel, M.D. Trinity Clinic Orthopaedic and Sports Medicine 1327 Troup Hwy Tyler, TX 75701 (903) 510-8840 ROTATOR CUFF REPAIR REHAB PROTOCOL This rehabilitation protocol has been developed for
Jayesh K. Patel, M.D. Trinity Clinic Orthopaedic and Sports Medicine 1327 Troup Hwy Tyler, TX 75701 (903) 510-8840 ROTATOR CUFF REPAIR REHAB PROTOCOL This rehabilitation protocol has been developed for
TOTAL SHOULDER ARTHROPLASTY, HEMIARTHROPLASTY OR REVERSE ARTHROPLASTY
 TOTAL SHOULDER ARTHROPLASTY, HEMIARTHROPLASTY OR REVERSE ARTHROPLASTY Philosophy The following is an outline of the standard post-operative rehabilitation program following total shoulder arthroplasty.
TOTAL SHOULDER ARTHROPLASTY, HEMIARTHROPLASTY OR REVERSE ARTHROPLASTY Philosophy The following is an outline of the standard post-operative rehabilitation program following total shoulder arthroplasty.
ADHESIVE CAPSULITIS (FROZEN SHOULDER)
") ADHESIVE CAPSULITIS (FROZEN SHOULDER) Frozen shoulder, or adhesive capsulitis is a condition that generally begins with the gradual onset of pain followed by a limitation of shoulder motion. The discomfort
ADHESIVE CAPSULITIS (FROZEN SHOULDER) Frozen shoulder, or adhesive capsulitis is a condition that generally begins with the gradual onset of pain followed by a limitation of shoulder motion. The discomfort
Phase I: 0 to 3 weeks after surgery
 Dx: Right Left RTC (Massive) Repair Date of Surgery: Patient Name: PT/OT: Please evaluate and treat. Follow attached protocol. 2-3 x per week x 6 weeks. Signature/Date: 2. Ensure wound healing Phase I:
Dx: Right Left RTC (Massive) Repair Date of Surgery: Patient Name: PT/OT: Please evaluate and treat. Follow attached protocol. 2-3 x per week x 6 weeks. Signature/Date: 2. Ensure wound healing Phase I:
Dr. Denard s Rehabilitation Protocols Arthroscopic Shoulder Surgery
 2780 E. Barnett Rd Medford, OR 97530 541-779-6250 Dr. Denard s Rehabilitation Protocols Arthroscopic Shoulder Surgery These rehabilitation protocols are based on current studies detailing healing time
2780 E. Barnett Rd Medford, OR 97530 541-779-6250 Dr. Denard s Rehabilitation Protocols Arthroscopic Shoulder Surgery These rehabilitation protocols are based on current studies detailing healing time
Rehab protocol. Phase I: Immediate Post-Surgical Phase: Typically 0-4 weeks; 2 PT visits. Goals:
 Reverse Total shoulder arthroplasty Rehab protocol Phase I: Immediate Post-Surgical Phase: Typically 0-4 weeks; 2 PT visits Allow healing of soft tissue Maintain integrity of replaced joint Gradually increase
Reverse Total shoulder arthroplasty Rehab protocol Phase I: Immediate Post-Surgical Phase: Typically 0-4 weeks; 2 PT visits Allow healing of soft tissue Maintain integrity of replaced joint Gradually increase
Anterior Stabilization of the Shoulder: Latarjet Protocol
 Robert K. Fullick, MD 6400 Fannin Street, Suite 1700 Houston, Texas 77030 Ph.: 713-486-7543 / Fx.: 713-486-5549 Anterior Stabilization of the Shoulder: Latarjet Protocol The intent of this protocol is
Robert K. Fullick, MD 6400 Fannin Street, Suite 1700 Houston, Texas 77030 Ph.: 713-486-7543 / Fx.: 713-486-5549 Anterior Stabilization of the Shoulder: Latarjet Protocol The intent of this protocol is
ACROMIO- CLAVICULAR (A/C) JOINT SPRAIN An IPRS Guide to provide you with exercises and advice to ease your condition
 JOINT SPRAIN An IPRS Guide to provide you with exercises and advice to ease your condition") Contents What causes an A/C joint sprain?..................................3 What treatment can I receive?.....................................4 YOUR GUIDE TO ACROMIO- CLAVICULAR (A/C) JOINT SPRAIN An
Contents What causes an A/C joint sprain?..................................3 What treatment can I receive?.....................................4 YOUR GUIDE TO ACROMIO- CLAVICULAR (A/C) JOINT SPRAIN An
Biceps Tenotomy Protocol
 Biceps Tenotomy Protocol A biceps tenotomy procedure involves cutting of the long head of the biceps just prior to its insertion on the superior labrum. A biceps tenotomy is typically done when there is
Biceps Tenotomy Protocol A biceps tenotomy procedure involves cutting of the long head of the biceps just prior to its insertion on the superior labrum. A biceps tenotomy is typically done when there is
Post-Operative Instructions Glenoid Reconstruction using Fresh Distal Tibial Allograft
 Day of Surgery Post-Operative Instructions Glenoid Reconstruction using Fresh Distal Tibial Allograft A. Relax. Diet as tolerated. B. Icing is important for the first 5-7 days post-op. While the post-op
Day of Surgery Post-Operative Instructions Glenoid Reconstruction using Fresh Distal Tibial Allograft A. Relax. Diet as tolerated. B. Icing is important for the first 5-7 days post-op. While the post-op
Page 2 of 13 Fig. E-2A Fig. E-2B Fig. E-2C Fig. E-2D Figs. E-2A through E-2D Treatment to relax the upper part of the trapezius muscle. Fig. E-2A Pati
 Page 1 of 13 Fig. E-1A Fig. E-1B Figs. E-1A through E-1C Correction of the sitting position to increase the patient s awareness for the correct sitting position and the interscapular muscles. Fig. E-1A
Page 1 of 13 Fig. E-1A Fig. E-1B Figs. E-1A through E-1C Correction of the sitting position to increase the patient s awareness for the correct sitting position and the interscapular muscles. Fig. E-1A
AC reconstruction Protocol: Dr. Rolf
 AC reconstruction Protocol: Dr. Rolf The intent of this protocol is to provide the clinician with a guideline of the post-operative rehabilitation course of a patient that has undergone a AC reconstruction
AC reconstruction Protocol: Dr. Rolf The intent of this protocol is to provide the clinician with a guideline of the post-operative rehabilitation course of a patient that has undergone a AC reconstruction
DISCHARGE INSTRUCTIONS & PHYSICAL THERAPY PROTOCOL: Biceps Tenodesis
 DISCHARGE INSTRUCTIONS & PHYSICAL THERAPY PROTOCOL: Biceps Tenodesis Initial recovery after shoulder surgery entails healing, controlling swelling and discomfort and regaining some shoulder motion. The
DISCHARGE INSTRUCTIONS & PHYSICAL THERAPY PROTOCOL: Biceps Tenodesis Initial recovery after shoulder surgery entails healing, controlling swelling and discomfort and regaining some shoulder motion. The
Rotator Cuff Repair Protocol
 Protocol This rehabilitation protocol has been developed for the patient following a rotator cuff surgical procedure. This protocol will vary in length and aggressiveness depending on factors such as:
Protocol This rehabilitation protocol has been developed for the patient following a rotator cuff surgical procedure. This protocol will vary in length and aggressiveness depending on factors such as:
Rehabilitation Guidelines for Shoulder Arthroscopy
 Rehabilitation Guidelines for Shoulder Arthroscopy The true shoulder joint is called the glenohumeral joint and consists humeral head and the glenoid. It is a ball and socket joint. Anatomy of the Shoulder
Rehabilitation Guidelines for Shoulder Arthroscopy The true shoulder joint is called the glenohumeral joint and consists humeral head and the glenoid. It is a ball and socket joint. Anatomy of the Shoulder
WILLIAM M. ISBELL, MD Jeremy R. Stinson PA-C
 WILLIAM M. ISBELL, MD Jeremy R. Stinson PA-C Post-Operative Rehabilitation Guidelines for Total Shoulder Arthroplasty (TSA) The intent of this protocol is to provide the physical therapist with a guideline/treatment
WILLIAM M. ISBELL, MD Jeremy R. Stinson PA-C Post-Operative Rehabilitation Guidelines for Total Shoulder Arthroplasty (TSA) The intent of this protocol is to provide the physical therapist with a guideline/treatment
1/19/2018. Winter injuries to the shoulder and elbow. Highgate Private Hospital (Whittington Health NHS Trust)
") Winter injuries to the shoulder and elbow Omar Haddo Consultant Orthopaedic Surgeon, Shoulder, Elbow, Hand & Wrist Specialist MBBS, BmedSci, FRCS(Orth) Highgate Private Hospital (Whittington Health NHS
Winter injuries to the shoulder and elbow Omar Haddo Consultant Orthopaedic Surgeon, Shoulder, Elbow, Hand & Wrist Specialist MBBS, BmedSci, FRCS(Orth) Highgate Private Hospital (Whittington Health NHS
Pectorlais Major Tendon Repair
 Dr. Mark Price MGH Sports Medicine Center 175 Cambridge Street, 4th floor Boston, MA 02114 www.massgeneral.org/ortho-sports-medicine/dr-price Pectorlais Major Tendon Repair The pectoralis major muscle
Dr. Mark Price MGH Sports Medicine Center 175 Cambridge Street, 4th floor Boston, MA 02114 www.massgeneral.org/ortho-sports-medicine/dr-price Pectorlais Major Tendon Repair The pectoralis major muscle
REVERSE TOTAL SHOULDER ARTHROPLASTY PROTOCOL
 Jennifer L. Cook, MD Stephen A. Hanff, MD Florida Joint Care Institute 2165 Little Road, Trinity, Florida 34655 PH: (727) 372 6637 FAX: (727) 375 5044 REVERSE TOTAL SHOULDER ARTHROPLASTY PROTOCOL Shoulder
Jennifer L. Cook, MD Stephen A. Hanff, MD Florida Joint Care Institute 2165 Little Road, Trinity, Florida 34655 PH: (727) 372 6637 FAX: (727) 375 5044 REVERSE TOTAL SHOULDER ARTHROPLASTY PROTOCOL Shoulder
S p o r t s & O r t h o p a e d i c S p e c i a l i s t s M A S S I V E R O T A T O R C U F F R E P A I R P R O T O C O L
 S p o r t s & O r t h o p a e d i c S p e c i a l i s t s M A S S I V E R O T A T O R C U F F R E P A I R P R O T O C O L This protocol provides appropriate guidelines for the rehabilitation of patients
S p o r t s & O r t h o p a e d i c S p e c i a l i s t s M A S S I V E R O T A T O R C U F F R E P A I R P R O T O C O L This protocol provides appropriate guidelines for the rehabilitation of patients
Ms. Ruth A. Delaney, MB BCh BAO, MMedSc, MRCS
 Ms. Ruth A. Delaney, MB BCh BAO, MMedSc, MRCS Consultant Orthopaedic Surgeon, Shoulder Specialist. +353 1 5262335 ruthdelaney@sportssurgeryclinic.com Modified from the protocol developed at Boston Shoulder
Ms. Ruth A. Delaney, MB BCh BAO, MMedSc, MRCS Consultant Orthopaedic Surgeon, Shoulder Specialist. +353 1 5262335 ruthdelaney@sportssurgeryclinic.com Modified from the protocol developed at Boston Shoulder
St Mary Orthopaedic Conference. Steven A. Caruso, MD Trenton Orthopaedic Group Trauma and Complex Fracture Surgeon October 25, 2014
 St Mary Orthopaedic Conference Steven A. Caruso, MD Trenton Orthopaedic Group Trauma and Complex Fracture Surgeon October 25, 2014 Nothing to disclose Goals To discuss common orthopaedic pathologies and
St Mary Orthopaedic Conference Steven A. Caruso, MD Trenton Orthopaedic Group Trauma and Complex Fracture Surgeon October 25, 2014 Nothing to disclose Goals To discuss common orthopaedic pathologies and
Reverse Total Shoulder Arthroplasty with Latissimus dorsi tendon transfer Protocol:
 Adam N. Whatley, M.D. 6550 Main St., STE. 2300 Zachary, LA 70791 Phone(225)658-1808 Fax(225)658-5299 Reverse Total Shoulder Arthroplasty with Latissimus dorsi tendon transfer Protocol: General Information:
Adam N. Whatley, M.D. 6550 Main St., STE. 2300 Zachary, LA 70791 Phone(225)658-1808 Fax(225)658-5299 Reverse Total Shoulder Arthroplasty with Latissimus dorsi tendon transfer Protocol: General Information:
The Shoulder Complex. Anatomy. Articulations 12/11/2017. Oak Ridge High School Conroe, Texas. Clavicle Collar Bone Scapula Shoulder Blade Humerus
 The Shoulder Complex Oak Ridge High School Conroe, Texas Anatomy Clavicle Collar Bone Scapula Shoulder Blade Humerus Articulations Sternoclavicular SC joint. Sternum and Clavicle. Acromioclavicular AC
The Shoulder Complex Oak Ridge High School Conroe, Texas Anatomy Clavicle Collar Bone Scapula Shoulder Blade Humerus Articulations Sternoclavicular SC joint. Sternum and Clavicle. Acromioclavicular AC
Arthroscopic SLAP Repair Protocol
 SPORTS & ORTHOPAEDIC SPECIALISTS Arthroscopic SLAP Repair Protocol 6-8 visits over 12 weeks Emphasis is on AAROM and a high repetition, low weight free weight program Address posterior capsular tightness
SPORTS & ORTHOPAEDIC SPECIALISTS Arthroscopic SLAP Repair Protocol 6-8 visits over 12 weeks Emphasis is on AAROM and a high repetition, low weight free weight program Address posterior capsular tightness
IP: Sling for 6 weeks Week 0-6: Immobilisation + Pendulum exercise Week 6-4 Months: Active ROM 4 Months-on: Strengthening exercises
 Supplemental material 5 Table 1. Summary of rehabilitation programs postoperative. Author (year) Early Rehabilitation Conservative Rehabilitation Arndt et al., 2012 [35] First day postoperative-week 6:
Supplemental material 5 Table 1. Summary of rehabilitation programs postoperative. Author (year) Early Rehabilitation Conservative Rehabilitation Arndt et al., 2012 [35] First day postoperative-week 6: