Case Presentation MATT WORONCZAK ADVANCED MUSCULOSKELETAL PHYSIOTHERAPIST DANDENONG HOSPITAL VICTORIA
|
|
|
- Tracey Riley
- 5 years ago
- Views:
Transcription
1 Case Presentation MATT WORONCZAK ADVANCED MUSCULOSKELETAL PHYSIOTHERAPIST DANDENONG HOSPITAL VICTORIA
2 Scenario Supervising an intern 22 year old male playing soccer yesterday, rolled ankle and unable to weightbear due to pain in lateral ankle and foot. Pt noticed loss of sensation, active dorsiflexion Swollen lateral ankle and foot, unable to actively dorsiflex toes or foot. Absent sensation on foot with exception of little toe side. Neurovascular function normal otherwise

3 Scenario Pictures are NOT of the patient, but purely for illustration of point

4 Scenario Pictures are NOT of the patient, but purely for illustration of point
5 More information needed Patient had knee fully extended and sustained inversion injury to ankle while changing directions at soccer (which would have likely resulted in a varus / hyperextension force to the knee) No PHx of knee or significant ankle problems
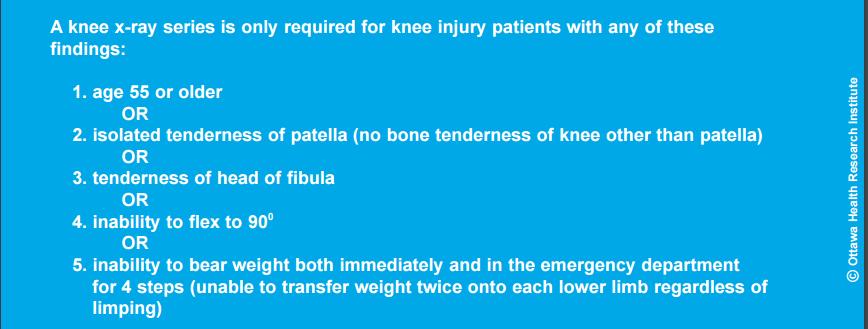
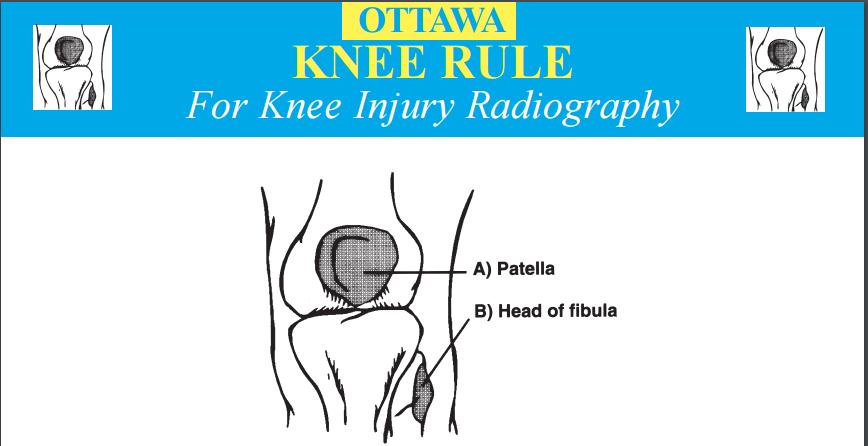
6 Assessment Knee Moderate effusion to knee AROM 0 to 90 = pain limited at either extreme Valgus 0,30 = Mild pain, not lax Varus 0,30 = at least 15 degrees of laxity in each, with guarding limiting accurate assessment Lachman s = unable to relax Tender around lateral hamstrings and posterolateral knee, as well as LCL
7
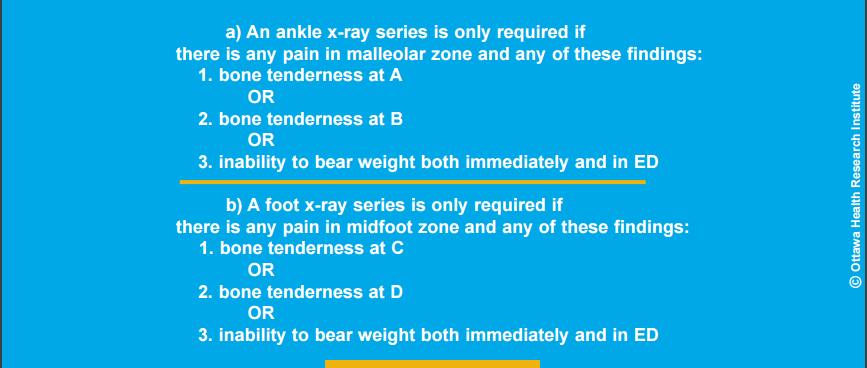
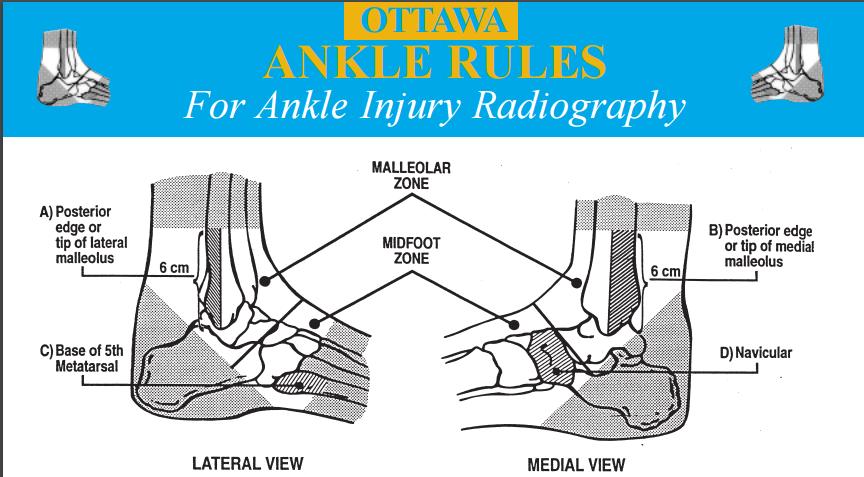
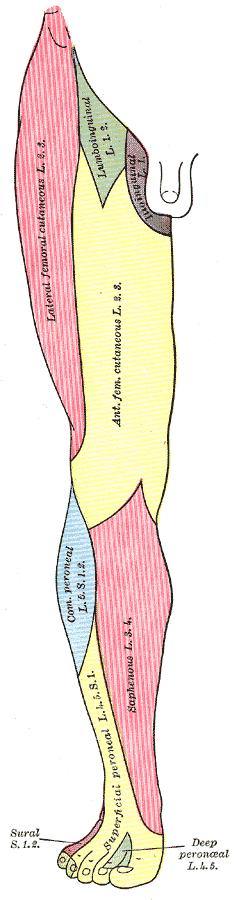
8 Assessment Ankle / Foot Moderate swelling to lateral ankle and foot Absent sensation to anterolateral shin and dorsum of foot with exception of 5 th ray Otherwise NV function normal AROM Dorsiflexion = nil active of ankle or toes Plantarflexion = normal ROM and power Eversion = minimal power / active movement Inversion = painful, but normal ROM and power Tender distal fibula, including posteriorly over the distal 6cm Tender 5 th metatarsal base
9

10


11



12


13

14
15 Muscle Biceps Femoris (short head) Extensor Digitorum Brevis Extensor Digitorum Longus Extensor Hallucis Brevis Extensor Hallucis Longus Peroneus Tertius Tibialis Anterior Peroneus Brevis Peroneus Longus Nerve Supply Common Peroneal Nerve Deep Peroneal Nerve Deep Peroneal Nerve Deep Peroneal Nerve Deep Peroneal Nerve Deep Peroneal Nerve Deep Peroneal Nerve Superficial Peroneal Nerve Superficial Peroneal Nerve

16 Movement Segment Hip Flexion L2/3 Knee Extension L3/4 Ankle Dorsiflexion L4/5 Great Toe Extension L5 Ankle Eversion L5/S1 Ankle Plantarflexion S1/S2 Reflex Segment Knee Jerk L3/4 Ankle Jerk S1/2

17

18 Ankle Brachial Index ABI = P Leg P Arm P Leg = Highest of the dorsalis pedis and posterior tibial systolic pressure P Arm = Highest of the left and right brachial systolic pressure ABI Interpretation <0.90 Abnormal: Arterial Blockage Borderline Abnormal 1.0 to 1.4 Normal >1.40 Abnormal: Hardened Arteries


19




20 MRI ACL Rupture LCL Rupture MCL Grade I-II High Grade Posterolateral Corner Injury Lateral Capsule Disruption Common Peroneal Nerve Avulsion Discharged
21 Clinic Followup and Progress 10/7 post injury Still no active dorsiflexion Not for surgery straight away 3/52 post injury Still no active dorsiflexion 7/52 post injury Still no active dorsiflexion 3/12 post injury Out of knee brace, continuing with physio Still no active dorsiflexion For review in another 3/12
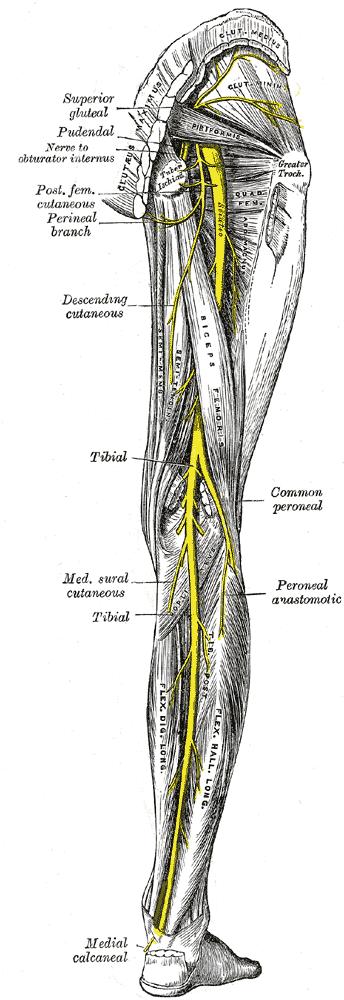
22 Neuroanatomy
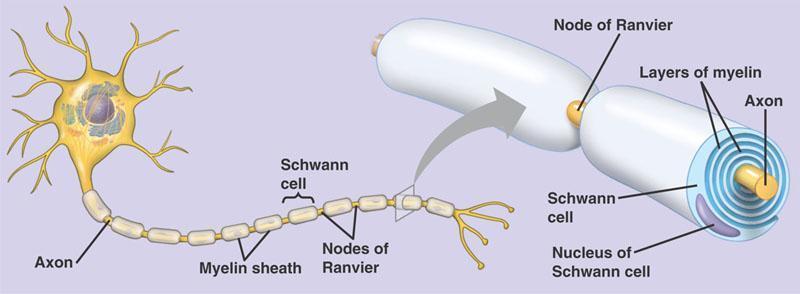
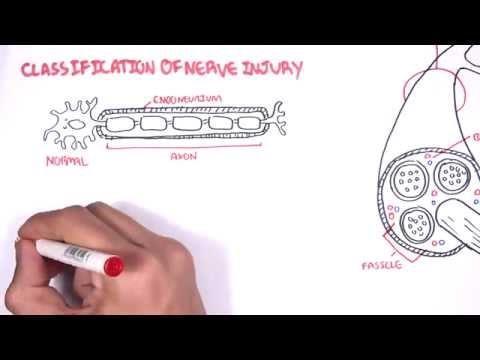
23 Peripheral Nerve Injury Seddon Classification For Nerve Injury 1. Neuropraxia Mild stretch or contusion no significant damage Endoneurium Axon 2. Axonotmesis Axon disruption with an intact endoneurium Myelin 3. Neurotomesis Complete peripheral nerve rupture

24 Peripheral Nerve Injury 1. Neuropraxia Mild stretch or secondary contusion resulting in transient nerve dysfunction secondary to local ischaemia and demyelination Usually caused by blunt injury No significant damage to axon or endoneurium No Wallerian degeneration Conduction occurs proximal and distal to the injury, but not at the site of injury Profound motor loss +/- mild sensory changes Recovery in days to weeks
 does not")
25 Peripheral Nerve Injury Wallerian Degeneration Where there has been significant disruption to a nerve, there will be degeneration distal to the lesion Begins within hours of a lesion Prior to this, distal axon stump remains electrically excitable The axon degenerates, followed by the degradation of the myelin sheath The nerve fibre s neurilemma (outer lining of myelin sheath) does not degenerate and remains as a hollow tube. Within 4 days of the injury, the distal end of the portion of the nerve fibre proximal to the lesion sends out sprouts towards those tubes. If a sprout reaches the tube, it grows into it and advances about 1 mm per day, eventually reaching and reinnervating the target tissue. If the sprouts cannot reach the tube, for instance because the gap is too wide or scar tissue has formed, surgery can help to guide the sprouts into the tubes.

26 Peripheral Nerve Injury Axonotmesis Axon disruption with an intact endoneurium Complete motor loss +/- sensory changes Wallerian Degeneration Regeneration 0.5-1mm per day after a 1 month delay Recovery

27 Peripheral Nerve Injury 3. Neurotomesis Complete peripheral nerve rupture Involves both axonal disruption and: 3a Involves ENDONEURIUM fair regrowth 3b Involves PERINEURIUM poor regrowth 3c Involves EPINEURIUM no regrowth Complete motor and sensory loss Wallerian Degeneration No nerve conduction distal to the injury after 3-4 days
 (Goitz & Tomaino,")
28 Nerve Conduction Studies Needle Electromyography Changes of axonal degeneration may not appear in muscle for 2-3 weeks after injury, EMG not indicated within this time (typically suggested at 4-6 weeks if no signs of improvement) (Goitz & Tomaino, 2003)
 Higher correlation with knee dislocation and associated Posterolateral corner injuries (26/27 in a study by Krych et al,")
29 Common Peroneal Nerve Injury Associated with Knee Injury Associated with ankle inversion injuries and also commonly associated with knee dislocations 10-42% incidence of common peroneal nerve injury with knee dislocation / bicruciate ligament injury (Goitz & Tomaino, 2003) Higher correlation with knee dislocation and associated Posterolateral corner injuries (26/27 in a study by Krych et al, 2014) Fibular head fracture (39% vs 21%) Vascular injury (15% vs 5%) Higher BMI Male (all from Peskun et al 2011) Multiple anatomical factors Has limited excursion (only about 0.5cm) at the fibular head during knee motion, where it is tethered by its branches Relative thickness of epineural to axonal tissue is low compared to other similarly sized nerves Less protection from stretch injuries (Goitz & Tomaino, 2003)

30 Common Peroneal Nerve Injury Associated with Knee Injury
31 Common Peroneal Nerve Injury Associated with Knee Injury Management Incomplete nerve palsies generally have excellent recovery without intervention With complete nerve palsies, there is little consensus regarding treatment: Conservative Treatment 0-50% have at chance of functional return without surgery
32 Common Peroneal Nerve Injury Associated with Knee Injury Operative repair Surgical repair usually necessitates immobilisation in excessive flexion (in contradiction to the management of the ligamentous injuries sustained / repaired) Primary Repair (rarely done nerve frayed) Neurolysis alone (releasing the nerve from its neuroma and surrounding scar tissue; epineurium still intact) Neuroma excision and grafting Graft length affects prognosis <6cm = 75% at least grade 3 strength 6-12cm = 35% at least grade 3 strength >12cm = 14% at least grade 3 strength
33 Common Peroneal Nerve Injury Associated with Knee Injury Timing important (especially with increased length of graft) 20cm = 200mm = > 200 days for regeneration! In closed injuries, operative treatment advised if there is no spontaneous regeneration at 3-4 months post injury (Garozzo et al, 2004) Irreversible muscle atrophy, fibrosis and disappearance of functional neural endplates occurs by 9-12 months after denervation Birch et al (1998) reported 48% good recovery if nerve repaired at 6/12, but only 9% at 12/12
34 Common Peroneal Nerve Injury Associated with Knee Injury Operative CPN repair has a poorer prognosis compared to other peripheral nerves Excessive length of nerve Abundance of connective tissue Force imbalance between intact plantarflexors and the passively stretched denervated foot extensors. Early AFO to avoid contracture Tibialis posterior tendon transfer

35 Common Peroneal Nerve Injury Associated with Knee Injury Always look up! If has had knee dislocation, be wary of damage to the popliteal artery Ankle Brachial Index CPN commonly injured in knee dislocations / bicruciate ligament injuries Need AFO early to prevent contracture Nerve Conduction Studies if no improvement at 4-6/52 If no improvement by 3-4/12, consider operative Mx as poor prognosis for operative Mx > 12/12
36 Bibliography Birch R, Pascher A, Schwarzl F, Pierer G, Fellinger M, Passler JM (1998). Surgical disorders of the peripheral nerves. London: Churchill Liviingstone; 1998 p Garozzo D, Ferraresi P & Buffatti P (2004). Surgical treatment of common peroneal nerve injuries: indications and results. Journal of Neurosurgical Sciences 43,3: Krych AJ, Giuseffi SA, Kuzma SA, Stuart MJ, Levy BA (2014). Is peroneal nerve injury associated with worse function after knee dislocation? Clinical Orthopaedics and Related Research 472: Peskun CJ, Chahal J, Steinfeld ZY & Whelan DB (2012). Risk factors for peroneal nerve injury and recovery in knee dislocation. Clinical Orthopaedics and Related Research 470:
37
The Lower Limb VI: The Leg. Anatomy RHS 241 Lecture 6 Dr. Einas Al-Eisa
 The Lower Limb VI: The Leg Anatomy RHS 241 Lecture 6 Dr. Einas Al-Eisa Muscles of the leg Posterior compartment (superficial & deep): primary plantar flexors of the foot flexors of the toes Anterior compartment:
The Lower Limb VI: The Leg Anatomy RHS 241 Lecture 6 Dr. Einas Al-Eisa Muscles of the leg Posterior compartment (superficial & deep): primary plantar flexors of the foot flexors of the toes Anterior compartment:
BLUE SKY SCHOOL OF PROFESSIONAL MASSAGE AND THERAPEUTIC BODYWORK Musculoskeletal Anatomy & Kinesiology KNEE & ANKLE MUSCLES
 BLUE SKY SCHOOL OF PROFESSIONAL MASSAGE AND THERAPEUTIC BODYWORK Musculoskeletal Anatomy & Kinesiology KNEE & ANKLE MUSCLES MSAK201-I Session 3 1) REVIEW a) THIGH, LEG, ANKLE & FOOT i) Tibia Medial Malleolus
BLUE SKY SCHOOL OF PROFESSIONAL MASSAGE AND THERAPEUTIC BODYWORK Musculoskeletal Anatomy & Kinesiology KNEE & ANKLE MUSCLES MSAK201-I Session 3 1) REVIEW a) THIGH, LEG, ANKLE & FOOT i) Tibia Medial Malleolus
The Leg. Prof. Oluwadiya KS
 The Leg Prof. Oluwadiya KS www.oluwadiya.sitesled.com Compartments of the leg 4 Four Compartments: 1. Anterior compartment Deep fibular nerve Dorsiflexes the foot and toes 2. Lateral Compartment Superficial
The Leg Prof. Oluwadiya KS www.oluwadiya.sitesled.com Compartments of the leg 4 Four Compartments: 1. Anterior compartment Deep fibular nerve Dorsiflexes the foot and toes 2. Lateral Compartment Superficial
ANKLE PLANTAR FLEXION
 ANKLE PLANTAR FLEXION Evaluation and Measurements By Isabelle Devreux 1 Ankle Plantar Flexion: Gastrocnemius and Soleus ROM: 0 to 40-45 A. Soleus: Origin: Posterior of head of fibula and proximal1/3 of
ANKLE PLANTAR FLEXION Evaluation and Measurements By Isabelle Devreux 1 Ankle Plantar Flexion: Gastrocnemius and Soleus ROM: 0 to 40-45 A. Soleus: Origin: Posterior of head of fibula and proximal1/3 of
Leg. Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology
 Leg Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology Skin of the Leg Cutaneous Nerves Medially: The saphenous nerve, a branch of the femoral nerve supplies the skin on the medial surface
Leg Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology Skin of the Leg Cutaneous Nerves Medially: The saphenous nerve, a branch of the femoral nerve supplies the skin on the medial surface
Management of Multi-ligament Knee Sports Injuries
 Management of Multi-ligament Knee Sports Injuries Aimee S. Klapach, MD Sports and Orthopaedic Specialists Allina Health Sports Medicine Conference June 15, 2018 Objectives Background On field assessment
Management of Multi-ligament Knee Sports Injuries Aimee S. Klapach, MD Sports and Orthopaedic Specialists Allina Health Sports Medicine Conference June 15, 2018 Objectives Background On field assessment
Tibial and Common Peroneal Nerve Compression in The Popliteal Fossa: A Case Report and Literature Review
 ISPUB.COM The Internet Journal of Plastic Surgery Volume 2 Number 1 Tibial and Common Peroneal Nerve Compression in The Popliteal Fossa: A Case Report and Literature D Reichner, G Evans Citation D Reichner,
ISPUB.COM The Internet Journal of Plastic Surgery Volume 2 Number 1 Tibial and Common Peroneal Nerve Compression in The Popliteal Fossa: A Case Report and Literature D Reichner, G Evans Citation D Reichner,
Anatomy MCQs Week 13
 Anatomy MCQs Week 13 1. Posterior to the medial malleolus of the ankle: The neurovascular bundle lies between Tibialis Posterior and Flexor Digitorum Longus The tendon of Tibialis Posterior inserts into
Anatomy MCQs Week 13 1. Posterior to the medial malleolus of the ankle: The neurovascular bundle lies between Tibialis Posterior and Flexor Digitorum Longus The tendon of Tibialis Posterior inserts into
1. A worker falls from a height and lands on his feet. Radiographs reveal a fracture of the sustentaculum tali. The muscle passing immediately
 1. A worker falls from a height and lands on his feet. Radiographs reveal a fracture of the sustentaculum tali. The muscle passing immediately beneath it that would be adversely affected is the: fibularis
1. A worker falls from a height and lands on his feet. Radiographs reveal a fracture of the sustentaculum tali. The muscle passing immediately beneath it that would be adversely affected is the: fibularis
Recognizing common injuries to the lower extremity
 Recognizing common injuries to the lower extremity Bones Femur Patella Tibia Tibial Tuberosity Medial Malleolus Fibula Lateral Malleolus Bones Tarsals Talus Calcaneus Metatarsals Phalanges Joints - Knee
Recognizing common injuries to the lower extremity Bones Femur Patella Tibia Tibial Tuberosity Medial Malleolus Fibula Lateral Malleolus Bones Tarsals Talus Calcaneus Metatarsals Phalanges Joints - Knee
Copyright 2004, Yoshiyuki Shiratori. All right reserved.
 Ankle and Leg Evaluation 1. History Chief Complaint: A. What happened? B. Is it a sharp or dull pain? C. How long have you had the pain? D. Can you pinpoint the pain? E. Do you have any numbness or tingling?
Ankle and Leg Evaluation 1. History Chief Complaint: A. What happened? B. Is it a sharp or dull pain? C. How long have you had the pain? D. Can you pinpoint the pain? E. Do you have any numbness or tingling?
Review relevant anatomy of the foot and ankle. Learn the approach to examining the foot and ankle
 Objectives Review relevant anatomy of the foot and ankle Learn the approach to examining the foot and ankle Learn the basics of diagnosis and treatment of ankle sprains Overview of other common causes
Objectives Review relevant anatomy of the foot and ankle Learn the approach to examining the foot and ankle Learn the basics of diagnosis and treatment of ankle sprains Overview of other common causes
Therapeutic Foot Care Certificate Program Part I: Online Home Study Program
 Therapeutic Foot Care Certificate Program Part I: Online Home Study Program 1 Anatomy And Terminology Of The Lower Extremity Joan E. Edelstein, MA, PT, FISPO Associate Professor of Clinical Physical Therapy
Therapeutic Foot Care Certificate Program Part I: Online Home Study Program 1 Anatomy And Terminology Of The Lower Extremity Joan E. Edelstein, MA, PT, FISPO Associate Professor of Clinical Physical Therapy
Year 2004 Paper one: Questions supplied by Megan
 QUESTION 47 A 58yo man is noted to have a right foot drop three days following a right total hip replacement. On examination there is weakness of right ankle dorsiflexion and toe extension (grade 4/5).
QUESTION 47 A 58yo man is noted to have a right foot drop three days following a right total hip replacement. On examination there is weakness of right ankle dorsiflexion and toe extension (grade 4/5).
Where should you palpate the pulse of different arteries in the lower limb?
 Where should you palpate the pulse of different arteries in the lower limb? The femoral artery In the femoral triangle, its pulse is easily felt just inferior to the inguinal ligament midway between the
Where should you palpate the pulse of different arteries in the lower limb? The femoral artery In the femoral triangle, its pulse is easily felt just inferior to the inguinal ligament midway between the
Lower Limb Nerves. Clinical Anatomy
 Lower Limb Nerves Clinical Anatomy Lumbar Plexus Ventral rami L1 L4 Supplies: Abdominal wall External genitalia Anteromedial thigh Major nerves.. Lumbar Plexus Nerves relation to psoas m. : Obturator n.
Lower Limb Nerves Clinical Anatomy Lumbar Plexus Ventral rami L1 L4 Supplies: Abdominal wall External genitalia Anteromedial thigh Major nerves.. Lumbar Plexus Nerves relation to psoas m. : Obturator n.
Considerations in Multiligament Knee Injuries
 Considerations in Multiligament Knee Injuries ERIC BERKSON, MD MGH SPORTS MEDICINE TEAM PHYSICIAN, BOSTON RED SOX ASSISTANT PROFESSOR, HARVARD MEDICAL SCHOOL JULY 26, 2018 Disclosures Neither I nor my
Considerations in Multiligament Knee Injuries ERIC BERKSON, MD MGH SPORTS MEDICINE TEAM PHYSICIAN, BOSTON RED SOX ASSISTANT PROFESSOR, HARVARD MEDICAL SCHOOL JULY 26, 2018 Disclosures Neither I nor my
musculoskeletal system anatomy muscles of foot sheet done by: dina sawadha & mohammad abukabeer
 musculoskeletal system anatomy muscles of foot sheet done by: dina sawadha & mohammad abukabeer Extensor retinaculum : A- superior extensor retinaculum (SER) : originates from the distal ends of the tibia
musculoskeletal system anatomy muscles of foot sheet done by: dina sawadha & mohammad abukabeer Extensor retinaculum : A- superior extensor retinaculum (SER) : originates from the distal ends of the tibia
Section Three: The Leg, Ankle, and Foot Lecture: Review of Clinical Anatomy, Patterns of Dysfunction and Injury, and
 Section Three: The Leg, Ankle, and Foot Lecture: Review of Clinical Anatomy, Patterns of Dysfunction and Injury, and Treatment Implications for the Leg, Ankle, and Foot Levels I and II Demonstration and
Section Three: The Leg, Ankle, and Foot Lecture: Review of Clinical Anatomy, Patterns of Dysfunction and Injury, and Treatment Implications for the Leg, Ankle, and Foot Levels I and II Demonstration and
musculoskeletal system anatomy nerves of the lower limb 2 done by: Dina sawadha & mohammad abukabeer
 musculoskeletal system anatomy nerves of the lower limb 2 done by: Dina sawadha & mohammad abukabeer #Sacral plexus : emerges from the ventral rami of the spinal segments L4 - S4 and provides motor and
musculoskeletal system anatomy nerves of the lower limb 2 done by: Dina sawadha & mohammad abukabeer #Sacral plexus : emerges from the ventral rami of the spinal segments L4 - S4 and provides motor and
Financial Disclosure. Medial Collateral Ligament
 Matthew Murray, M.D. UTHSCSA Sports Medicine Financial Disclosure Dr. Matthew Murray has no relevant financial relationships with commercial interests to disclose. Medial Collateral Ligament Most commonly
Matthew Murray, M.D. UTHSCSA Sports Medicine Financial Disclosure Dr. Matthew Murray has no relevant financial relationships with commercial interests to disclose. Medial Collateral Ligament Most commonly
Mohammad Ayati,M.D Department of Orthopaedics, Yazd University of Medical Science.
 IN THE NAME OF GOD Mohammad Ayati,M.D Department of Orthopaedics, Yazd University of Medical Science. Devastating injury resulting from : high-energy usually from MVC or fall from height commonly a dashboard
IN THE NAME OF GOD Mohammad Ayati,M.D Department of Orthopaedics, Yazd University of Medical Science. Devastating injury resulting from : high-energy usually from MVC or fall from height commonly a dashboard
HUMAN BODY COURSE LOWER LIMB NERVES AND VESSELS
 HUMAN BODY COURSE LOWER LIMB NERVES AND VESSELS October 22, 2010 D. LOWER LIMB MUSCLES 2. Lower limb compartments ANTERIOR THIGH COMPARTMENT General lfunction: Hip flexion, knee extension, other motions
HUMAN BODY COURSE LOWER LIMB NERVES AND VESSELS October 22, 2010 D. LOWER LIMB MUSCLES 2. Lower limb compartments ANTERIOR THIGH COMPARTMENT General lfunction: Hip flexion, knee extension, other motions
On Field Assessment and Management of Acute Knee Injuries: A Physiotherapist s Perspective
 On Field Assessment and Management of Acute Knee Injuries: A Physiotherapist s Perspective Jessica Condliffe Physiotherapist / Clinic Manager TBI Health Wellington Presentation Outline Knee anatomy review
On Field Assessment and Management of Acute Knee Injuries: A Physiotherapist s Perspective Jessica Condliffe Physiotherapist / Clinic Manager TBI Health Wellington Presentation Outline Knee anatomy review
Treatment of Acute Traumatic Knee Dislocations
 Treatment of Acute Traumatic Knee Dislocations Angelo J. Colosimo, MD Head Orthopaedic Surgeon University of Cincinnati Athletics Director of Sports Medicine University of Cincinnati Medical Center Associate
Treatment of Acute Traumatic Knee Dislocations Angelo J. Colosimo, MD Head Orthopaedic Surgeon University of Cincinnati Athletics Director of Sports Medicine University of Cincinnati Medical Center Associate
Treatment of Acute Traumatic Knee Dislocations
 Treatment of Acute Traumatic Knee Dislocations Angelo J. Colosimo, MD Head Orthopaedic Surgeon University of Cincinnati Athletics Director of Sports Medicine University of Cincinnati Medical Center Associate
Treatment of Acute Traumatic Knee Dislocations Angelo J. Colosimo, MD Head Orthopaedic Surgeon University of Cincinnati Athletics Director of Sports Medicine University of Cincinnati Medical Center Associate
SURGICAL AND APPLIED ANATOMY
 Página 1 de 9 Copyright 2001 Lippincott Williams & Wilkins Bucholz, Robert W., Heckman, James D. Rockwood & Green's Fractures in Adults, 5th Edition SURGICAL AND APPLIED ANATOMY Part of "47 - ANKLE FRACTURES"
Página 1 de 9 Copyright 2001 Lippincott Williams & Wilkins Bucholz, Robert W., Heckman, James D. Rockwood & Green's Fractures in Adults, 5th Edition SURGICAL AND APPLIED ANATOMY Part of "47 - ANKLE FRACTURES"
~, /' ~::'~ EXTENSOR HALLUCIS LONGUS. Leg-anterolateral :.:~ / ~\,
 TIBIALIS ANTERIOR Lateral condyle of tibia, upper half of lateral surface of tibia, interosseous membrane Medial side and plantar surface of medial cuneiform bone, and base of first metatarsal bone Dorsiflexes
TIBIALIS ANTERIOR Lateral condyle of tibia, upper half of lateral surface of tibia, interosseous membrane Medial side and plantar surface of medial cuneiform bone, and base of first metatarsal bone Dorsiflexes
Muscles of the Hip 1. Tensor Fasciae Latae O: iliac crest I: lateral femoral condyle Action: abducts the thigh Nerve: gluteal nerve
 Muscles of the Hip 1. Tensor Fasciae Latae O: iliac crest I: lateral femoral condyle Action: abducts the thigh Nerve: gluteal nerve 2. Gluteus Maximus O: ilium I: femur Action: abduct the thigh Nerve:
Muscles of the Hip 1. Tensor Fasciae Latae O: iliac crest I: lateral femoral condyle Action: abducts the thigh Nerve: gluteal nerve 2. Gluteus Maximus O: ilium I: femur Action: abduct the thigh Nerve:
موسى صالح عبد الرحمن الحنبلي أحمد سلمان
 8 موسى صالح عبد الرحمن الحنبلي أحمد سلمان 1 P a g e Today we will talk about a new region, which is the leg. And as always, we will start with studying the sensory innervation of the leg. What is the importance
8 موسى صالح عبد الرحمن الحنبلي أحمد سلمان 1 P a g e Today we will talk about a new region, which is the leg. And as always, we will start with studying the sensory innervation of the leg. What is the importance
The Lower Limb II. Anatomy RHS 241 Lecture 3 Dr. Einas Al-Eisa
 The Lower Limb II Anatomy RHS 241 Lecture 3 Dr. Einas Al-Eisa Tibia The larger & medial bone of the leg Functions: Attachment of muscles Transfer of weight from femur to skeleton of the foot Articulations
The Lower Limb II Anatomy RHS 241 Lecture 3 Dr. Einas Al-Eisa Tibia The larger & medial bone of the leg Functions: Attachment of muscles Transfer of weight from femur to skeleton of the foot Articulations
Knee Dislocation: Spectrum of Injury, Evolution of Treatment & Modern Outcomes
 Knee Dislocation: Spectrum of Injury, Evolution of Treatment & Modern Outcomes William M Weiss, MD MSc FRCSC Orthopedic Surgery & Rehabilitation Sports Medicine, Arthroscopy & Extremity Reconstruction
Knee Dislocation: Spectrum of Injury, Evolution of Treatment & Modern Outcomes William M Weiss, MD MSc FRCSC Orthopedic Surgery & Rehabilitation Sports Medicine, Arthroscopy & Extremity Reconstruction
Knee Injuries. PSK 4U Mr. S. Kelly North Grenville DHS. Medial Collateral Ligament Sprain
 Knee Injuries PSK 4U Mr. S. Kelly North Grenville DHS Medial Collateral Ligament Sprain Result from either a direct blow from the lateral side in a medial direction or a severe outward twist Greater injury
Knee Injuries PSK 4U Mr. S. Kelly North Grenville DHS Medial Collateral Ligament Sprain Result from either a direct blow from the lateral side in a medial direction or a severe outward twist Greater injury
COMMON PERONEAL NERVE INJURIES: GUIDELINES FOR SURGICAL TREATMENT IN OUR EXPERIENCE
 COMMON PERONEAL NERVE INJURIES: GUIDELINES FOR SURGICAL TREATMENT IN OUR EXPERIENCE Debora Garozzo Brachial Plexus and Peripheral Nerve Surgery Unit Neurospinal Hospital Dubai, United Arab Emirates Common
COMMON PERONEAL NERVE INJURIES: GUIDELINES FOR SURGICAL TREATMENT IN OUR EXPERIENCE Debora Garozzo Brachial Plexus and Peripheral Nerve Surgery Unit Neurospinal Hospital Dubai, United Arab Emirates Common
Imaging the Athlete s Knee. Peter Lowry, MD Musculoskeletal Radiology University of Colorado
 Imaging the Athlete s Knee Peter Lowry, MD Musculoskeletal Radiology University of Colorado None Disclosures Knee Imaging: Radiographs Can be performed weight-bearing or non-weight-bearing View options
Imaging the Athlete s Knee Peter Lowry, MD Musculoskeletal Radiology University of Colorado None Disclosures Knee Imaging: Radiographs Can be performed weight-bearing or non-weight-bearing View options
Prevention and Treatment of Injuries. Anatomy. Anatomy. Tibia: the second longest bone in the body
 Prevention and Treatment of Injuries The Ankle and Lower Leg Westfield High School Houston, Texas Anatomy Tibia: the second longest bone in the body Serves as the principle weight-bearing bone of the leg.
Prevention and Treatment of Injuries The Ankle and Lower Leg Westfield High School Houston, Texas Anatomy Tibia: the second longest bone in the body Serves as the principle weight-bearing bone of the leg.
بسم هللا الرحمن الرحيم
 بسم هللا الرحمن الرحيم Laboratory RHS 221 Manual Muscle Testing Theory 1 hour practical 2 hours Dr. Ali Aldali, MS, PT Department of Physical Therapy King Saud University Talocrural and Subtalar Joint
بسم هللا الرحمن الرحيم Laboratory RHS 221 Manual Muscle Testing Theory 1 hour practical 2 hours Dr. Ali Aldali, MS, PT Department of Physical Therapy King Saud University Talocrural and Subtalar Joint
Gait Improvements After Peroneal or Tibial Nerve Transfer in Patients with Foot Drop: A Retrospective Study
 Gait Improvements After Peroneal or Tibial Nerve Transfer in Patients with Foot Drop: A Retrospective Study Rahul K. Nath, MD, and Chandra Somasundaram, PhD Texas Nerve and Paralysis Institute, Houston
Gait Improvements After Peroneal or Tibial Nerve Transfer in Patients with Foot Drop: A Retrospective Study Rahul K. Nath, MD, and Chandra Somasundaram, PhD Texas Nerve and Paralysis Institute, Houston
Treatment of Acute Traumatic Knee Dislocations
 Treatment of Acute Traumatic Knee Dislocations Angelo J. Colosimo, MD Head Orthopaedic Surgeon University of Cincinnati Athletics Director of Sports Medicine University of Cincinnati Medical Center Associate
Treatment of Acute Traumatic Knee Dislocations Angelo J. Colosimo, MD Head Orthopaedic Surgeon University of Cincinnati Athletics Director of Sports Medicine University of Cincinnati Medical Center Associate
Lateral knee injuries
 Created as a free resource by Clinical Edge Based on Physio Edge podcast episode 051 with Matt Konopinski Get your free trial of online Physio education at Orthopaedic timeframes Traditionally Orthopaedic
Created as a free resource by Clinical Edge Based on Physio Edge podcast episode 051 with Matt Konopinski Get your free trial of online Physio education at Orthopaedic timeframes Traditionally Orthopaedic
Musculoskeletal Examination Benchmarks
 Musculoskeletal Examination Benchmarks _ The approach to examining the musculoskeletal system is the same no matter what joint or limb is being examined. The affected and contralateral region should both
Musculoskeletal Examination Benchmarks _ The approach to examining the musculoskeletal system is the same no matter what joint or limb is being examined. The affected and contralateral region should both
Management of Brachial Plexus & Peripheral Nerves Blast Injuries. First Global Conflict Medicine Congress
 Management of Brachial Plexus & Peripheral Nerves Blast Injuries Joseph BAKHACH First Global Conflict Medicine Congress Hand & Microsurgery Department American University of Beirut Medical Centre Brachial
Management of Brachial Plexus & Peripheral Nerves Blast Injuries Joseph BAKHACH First Global Conflict Medicine Congress Hand & Microsurgery Department American University of Beirut Medical Centre Brachial
Cavus Foot: Subtle and Not-So-Subtle AOFAS Resident Review Course September 28, 2013
 Cavus Foot: Subtle and Not-So-Subtle Course September 28, 2013 Matthew M. Roberts, MD Associate Professor of Clinical Orthopaedic Surgery Co-Chief, Foot and Ankle Service Hospital for Special Surgery Disclosure
Cavus Foot: Subtle and Not-So-Subtle Course September 28, 2013 Matthew M. Roberts, MD Associate Professor of Clinical Orthopaedic Surgery Co-Chief, Foot and Ankle Service Hospital for Special Surgery Disclosure
DR SHRENIK M SHAH SHREY HOSPITAL AHMEDABAD
 DR SHRENIK M SHAH SHREY HOSPITAL AHMEDABAD Surgical anatomy Physiology of healing Classification Pre-operative evaluation OVERVIEW Ultrastructure of the nerve Fragile handle with care Damaged by pressure,
DR SHRENIK M SHAH SHREY HOSPITAL AHMEDABAD Surgical anatomy Physiology of healing Classification Pre-operative evaluation OVERVIEW Ultrastructure of the nerve Fragile handle with care Damaged by pressure,
THE LOWER EXTREMITY EXAM FOR THE FAMILY PRACTITIONER
 THE LOWER EXTREMITY EXAM FOR THE FAMILY PRACTITIONER Melinda A. Scott, D.O. Orthopedic Associates of Dayton Board Certified in Primary Care Sports Medicine GOALS Identify landmarks necessary for exam of
THE LOWER EXTREMITY EXAM FOR THE FAMILY PRACTITIONER Melinda A. Scott, D.O. Orthopedic Associates of Dayton Board Certified in Primary Care Sports Medicine GOALS Identify landmarks necessary for exam of
Gross Anatomy Coloring Book Series. Lower Extremity Arteries
 Gross Anatomy Coloring Book Series Lower Extremity Arteries 1 Femoral Artery and Associated Branches For the life of the flesh is in the blood. Leviticus 17:11 Femoral Artery and Associated Branches After
Gross Anatomy Coloring Book Series Lower Extremity Arteries 1 Femoral Artery and Associated Branches For the life of the flesh is in the blood. Leviticus 17:11 Femoral Artery and Associated Branches After
Understanding Leg Anatomy and Function THE UPPER LEG
 Understanding Leg Anatomy and Function THE UPPER LEG The long thigh bone is the femur. It connects to the pelvis to form the hip joint and then extends down to meet the tibia (shin bone) at the knee joint.
Understanding Leg Anatomy and Function THE UPPER LEG The long thigh bone is the femur. It connects to the pelvis to form the hip joint and then extends down to meet the tibia (shin bone) at the knee joint.
Yoshihisa Masakado, Michiyuki Kawakami, Kanjiro Suzuki, Leon Abe, Tetsuo Ota, and Akio Kimura
 REVIEW Clinical Neurophysiology in the Diagnosis of Peroneal Nerve Palsy Yoshihisa Masakado, Michiyuki Kawakami, Kanjiro Suzuki, Leon Abe, Tetsuo Ota, and Akio Kimura Keio University Tsukigase Rehabilitation
REVIEW Clinical Neurophysiology in the Diagnosis of Peroneal Nerve Palsy Yoshihisa Masakado, Michiyuki Kawakami, Kanjiro Suzuki, Leon Abe, Tetsuo Ota, and Akio Kimura Keio University Tsukigase Rehabilitation
Differential Diagnosis
 Case 31yo M who sustained an injury to L knee while playing Basketball approximately 2 weeks ago. He describes pivoting and hyperextending his knee, which swelled over the next few days. He now presents
Case 31yo M who sustained an injury to L knee while playing Basketball approximately 2 weeks ago. He describes pivoting and hyperextending his knee, which swelled over the next few days. He now presents
fig fig For the following diagrams
 fig. 1271 For the following diagrams Please draw small circles at the following points (pts in bold are main syllabus pts): Liver-1 Liver-2 Liver-3 Liver-4 Spleen-4 Spleen-5 Stomach-41 Stomach-42 Stomach-43
fig. 1271 For the following diagrams Please draw small circles at the following points (pts in bold are main syllabus pts): Liver-1 Liver-2 Liver-3 Liver-4 Spleen-4 Spleen-5 Stomach-41 Stomach-42 Stomach-43
Anatomy and evaluation of the ankle.
 Anatomy and evaluation of the ankle www.fisiokinesiterapia.biz Ankle Anatomical Structures Tibia Fibular Talus Tibia This is the strongest largest bone of the lower leg. It bears weight and the bone creates
Anatomy and evaluation of the ankle www.fisiokinesiterapia.biz Ankle Anatomical Structures Tibia Fibular Talus Tibia This is the strongest largest bone of the lower leg. It bears weight and the bone creates
Knee Multiligament Rehabilitation
 Knee Multiligament Rehabilitation Orlando Valle, PT, MSPT, SCS, CSCS Director Ironman Sports Medicine Institute TMC Orlando.Valle@memorialhermann.org 4 Major Ligaments ACL PCL MCL LCL (PLC) Anatomy Function
Knee Multiligament Rehabilitation Orlando Valle, PT, MSPT, SCS, CSCS Director Ironman Sports Medicine Institute TMC Orlando.Valle@memorialhermann.org 4 Major Ligaments ACL PCL MCL LCL (PLC) Anatomy Function
Introduction to Anatomy. Dr. Maher Hadidi. Laith Al-Hawajreh. Mar/25 th /2013
 Introduction to Anatomy Dr. Maher Hadidi Laith Al-Hawajreh 22 Mar/25 th /2013 Lower limb - The leg The skeleton of the leg is formed by two bones: 1) Medial: Tibia 2) Lateral: Fibula The two bones are
Introduction to Anatomy Dr. Maher Hadidi Laith Al-Hawajreh 22 Mar/25 th /2013 Lower limb - The leg The skeleton of the leg is formed by two bones: 1) Medial: Tibia 2) Lateral: Fibula The two bones are
Overview Ligament Injuries. Anatomy. Epidemiology Very commonly injured joint. ACL Injury 20/06/2016. Meniscus Tears. Patellofemoral Problems
 Overview Ligament Injuries Meniscus Tears Pankaj Sharma MBBS, FRCS (Tr & Orth) Consultant Orthopaedic Surgeon Manchester Royal Infirmary Patellofemoral Problems Knee Examination Anatomy Epidemiology Very
Overview Ligament Injuries Meniscus Tears Pankaj Sharma MBBS, FRCS (Tr & Orth) Consultant Orthopaedic Surgeon Manchester Royal Infirmary Patellofemoral Problems Knee Examination Anatomy Epidemiology Very
Peripheral nerve injury
 Peripheral nerve injury Classification of peripheral nerve injury: I. Seddon classification: 1. Neurapraxia: conduction block with or without demyelination (the axon, endoneurium, perineurium and epineurium
Peripheral nerve injury Classification of peripheral nerve injury: I. Seddon classification: 1. Neurapraxia: conduction block with or without demyelination (the axon, endoneurium, perineurium and epineurium
This presentation is the intellectual property of the author. Contact them for permission to reprint and/or distribute.
 Introduction Compartment Syndromes of the Leg Related to Athletic Activity Mark M. Casillas, M.D. Consequences of a misdiagnosis persistence of a performance limitation loss of function/compartment loss
Introduction Compartment Syndromes of the Leg Related to Athletic Activity Mark M. Casillas, M.D. Consequences of a misdiagnosis persistence of a performance limitation loss of function/compartment loss
Lecture 09. Popliteal Fossa. BY Dr Farooq Khan Aurakzai
 Lecture 09 Popliteal Fossa BY Dr Farooq Khan Aurakzai Dated: 14.02.2018 What is popliteus? Introduction Anything relating to, or near the part of the leg behind the knee. From New Latin popliteus the muscle
Lecture 09 Popliteal Fossa BY Dr Farooq Khan Aurakzai Dated: 14.02.2018 What is popliteus? Introduction Anything relating to, or near the part of the leg behind the knee. From New Latin popliteus the muscle
VENOUS DRAINAGE OF THE LOWER LIMB
 Anatomy of the lower limb Superficial veins & nerve injuries Dr. Hayder VENOUS DRAINAGE OF THE LOWER LIMB The venous drainage of the lower limb is of huge clinical & surgical importance. Since the venous
Anatomy of the lower limb Superficial veins & nerve injuries Dr. Hayder VENOUS DRAINAGE OF THE LOWER LIMB The venous drainage of the lower limb is of huge clinical & surgical importance. Since the venous
Clarification of Terms
 Clarification of Terms The plantar aspect of the foot refers to the role or its bottom The dorsal aspect refers to the top or its superior portion The ankle and foot perform three main functions: 1. shock
Clarification of Terms The plantar aspect of the foot refers to the role or its bottom The dorsal aspect refers to the top or its superior portion The ankle and foot perform three main functions: 1. shock
A Patient s Guide to Ankle Anatomy
 A Patient s Guide to Ankle Anatomy 245 North College Lafayette, LA 70506 Phone: 337.232.5301 Fax: 337.237.6504 DISCLAIMER: The information in this booklet is compiled from a variety of sources. It may
A Patient s Guide to Ankle Anatomy 245 North College Lafayette, LA 70506 Phone: 337.232.5301 Fax: 337.237.6504 DISCLAIMER: The information in this booklet is compiled from a variety of sources. It may
5.1 Identify, describe the attachments of and deduce the actions of the muscles of the thigh:
 5.1 Identify, describe the attachments of and deduce the actions of the muscles of the thigh: Anterior group Proximal attachment Distal attachment Sartorius ASIS» Upper part of shaft tibia (middle surface)»
5.1 Identify, describe the attachments of and deduce the actions of the muscles of the thigh: Anterior group Proximal attachment Distal attachment Sartorius ASIS» Upper part of shaft tibia (middle surface)»
ACL Athletic Career. ACL Rupture - Warning Features Intensive pain Immediate swelling Locking Feel a Pop Dead leg Cannot continue to play
 FIMS Ambassador Tour to Eastern Europe, 2004 Belgrade, Serbia Montenegro Acute Knee Injuries - Controversies and Challenges Professor KM Chan OBE, JP President of FIMS Belgrade ACL Athletic Career ACL
FIMS Ambassador Tour to Eastern Europe, 2004 Belgrade, Serbia Montenegro Acute Knee Injuries - Controversies and Challenges Professor KM Chan OBE, JP President of FIMS Belgrade ACL Athletic Career ACL
SOFT TISSUE KNEE INJURIES
 SOFT TISSUE KNEE INJURIES Soft tissue injuries of the knee commonly occur in all sports or in any activity that requires sudden changes in activity or movement. The knee is a complex joint and any injury
SOFT TISSUE KNEE INJURIES Soft tissue injuries of the knee commonly occur in all sports or in any activity that requires sudden changes in activity or movement. The knee is a complex joint and any injury
North of England Bone and Soft Tissue Tumour Service
 North of England Bone and Soft Tissue Tumour Service Guidelines for rehabilitation after proximal tibial replacement Proximal tibial replacement surgery is usually carried out as part of treatment for
North of England Bone and Soft Tissue Tumour Service Guidelines for rehabilitation after proximal tibial replacement Proximal tibial replacement surgery is usually carried out as part of treatment for
The Foot. Dr. Wegdan Moh.Mustafa Medicine Faculty Assistant Professor Mob:
 The Foot Dr. Wegdan Moh.Mustafa Medicine Faculty Assistant Professor Mob: 0127155717 The skeleton of the foot Cutaneous innervations Sole of foot layers of muscles First layer -Abductor hallucis -Flexor
The Foot Dr. Wegdan Moh.Mustafa Medicine Faculty Assistant Professor Mob: 0127155717 The skeleton of the foot Cutaneous innervations Sole of foot layers of muscles First layer -Abductor hallucis -Flexor
MUSCLES OF THE LOWER LIMBS
 MUSCLES OF THE LOWER LIMBS Naming, location and general function Dr. Nabil khouri ROLES THAT SHOULD NOT BE FORGOTTEN Most anterior compartment muscles of the hip and thigh Flexor of the femur at the hip
MUSCLES OF THE LOWER LIMBS Naming, location and general function Dr. Nabil khouri ROLES THAT SHOULD NOT BE FORGOTTEN Most anterior compartment muscles of the hip and thigh Flexor of the femur at the hip
ALGORITHM IN EMERGENCIES
 ALGORITHM IN EMERGENCIES S. ZAFFAGNINI T. ROBERTI DI SARSINA, A. GRASSI CLINICA ORTOPEDICA II LAB. di BIOMECCANICA e INNOVAZIONE TECNOLOGICA Dir. Prof. S. Zaffagnini UNIVERSITA di BOLOGNA ISTITUTO ORTOPEDICO
ALGORITHM IN EMERGENCIES S. ZAFFAGNINI T. ROBERTI DI SARSINA, A. GRASSI CLINICA ORTOPEDICA II LAB. di BIOMECCANICA e INNOVAZIONE TECNOLOGICA Dir. Prof. S. Zaffagnini UNIVERSITA di BOLOGNA ISTITUTO ORTOPEDICO
Physical Examination of the Foot & Ankle
 Inspection Standing, feet straight forward facing toward examiner Swelling Deformity Flatfoot (pes planus and hindfoot valgus) High arch (pes cavus and hindfoot varus) Peek-a-boo heel Varus Too many toes
Inspection Standing, feet straight forward facing toward examiner Swelling Deformity Flatfoot (pes planus and hindfoot valgus) High arch (pes cavus and hindfoot varus) Peek-a-boo heel Varus Too many toes
Sports Injuries of the Ankle and Ankle Arthritis. Mr Amit Amin Consultant Foot and Ankle Surgeon Parkside Hospital
 Sports Injuries of the Ankle and Ankle Arthritis Mr Amit Amin Consultant Foot and Ankle Surgeon Parkside Hospital Impingement Painful mechanical limitation of full ankle movement secondary to osseous
Sports Injuries of the Ankle and Ankle Arthritis Mr Amit Amin Consultant Foot and Ankle Surgeon Parkside Hospital Impingement Painful mechanical limitation of full ankle movement secondary to osseous
MUSCULOSKELETAL LOWER LIMB
 MUSCULOSKELETAL LOWER LIMB Spinal Cord Lumbar and Sacral Regions Spinal cord Dorsal root ganglion Conus medullaris Cauda equina Dorsal root ganglion of the fifth lumbar nerve End of subarachnoid space
MUSCULOSKELETAL LOWER LIMB Spinal Cord Lumbar and Sacral Regions Spinal cord Dorsal root ganglion Conus medullaris Cauda equina Dorsal root ganglion of the fifth lumbar nerve End of subarachnoid space
Scar Engorged veins. Size of the foot [In clubfoot, small foot]
![Scar Engorged veins. Size of the foot [In clubfoot, small foot]](/thumbs/78/77722241.jpg "Scar Engorged veins. Size of the foot [In clubfoot, small foot]") 6. FOOT HISTORY Pain: Walking, Running Foot wear problem Swelling; tingly feeling Deformity Stiffness Disability: At work; recreation; night; walk; ADL, Sports Previous Rx Comorbidities Smoke, Sugar, Steroid
6. FOOT HISTORY Pain: Walking, Running Foot wear problem Swelling; tingly feeling Deformity Stiffness Disability: At work; recreation; night; walk; ADL, Sports Previous Rx Comorbidities Smoke, Sugar, Steroid
Muscles of the lower extremities. Dr. Nabil khouri MD, MSc, Ph.D
 Muscles of the lower extremities Dr. Nabil khouri MD, MSc, Ph.D Posterior leg Popliteal fossa Boundaries Biceps femoris (superior-lateral) Semitendinosis and semimembranosis (superior-medial) Gastrocnemius
Muscles of the lower extremities Dr. Nabil khouri MD, MSc, Ph.D Posterior leg Popliteal fossa Boundaries Biceps femoris (superior-lateral) Semitendinosis and semimembranosis (superior-medial) Gastrocnemius
Located Deep to Flexor Retinaculum on medial aspect of ankle. Posterior to Posterior Tibial Artery. Tom, Dick, and Very Nervous Harry
 ANKLE BLOCK ANESTHESIA GREGORY CLARK D.P.M. HEAD, SECTION OF PODIATRY SCRIPPS CLINIC LA JOLLA, CALIFORNIA A METHOD BY WHICH ONE MAY PROVIDE AN ANESTHETIC BLOCK TO THE FOOT OR ANKLE WITH A MINIMUM OF PATIENT
ANKLE BLOCK ANESTHESIA GREGORY CLARK D.P.M. HEAD, SECTION OF PODIATRY SCRIPPS CLINIC LA JOLLA, CALIFORNIA A METHOD BY WHICH ONE MAY PROVIDE AN ANESTHETIC BLOCK TO THE FOOT OR ANKLE WITH A MINIMUM OF PATIENT
CASE ONE CASE ONE. RADIAL HEAD FRACTURE Mason Classification. RADIAL HEAD FRACTURE Mechanism of Injury. RADIAL HEAD FRACTURE Imaging
 CASE ONE An eighteen year old female falls during a basketball game, striking her elbow on the court. She presents to your office that day with a painful, swollen elbow that she is unable to flex or extend
CASE ONE An eighteen year old female falls during a basketball game, striking her elbow on the court. She presents to your office that day with a painful, swollen elbow that she is unable to flex or extend
First & second layers of muscles of the sole
 The FOOT First & second layers of muscles of the sole introduction The muscles acting on the foot can be divided into two distinct groups; extrinsic and intrinsic muscles. The extrinsic muscles arise from
The FOOT First & second layers of muscles of the sole introduction The muscles acting on the foot can be divided into two distinct groups; extrinsic and intrinsic muscles. The extrinsic muscles arise from
17 FibulA FlAP Tor Chiu fibula flap 153
 17 Fibula Flap Tor Chiu Fibula Flap 153 Fibula Flap FLAP TERRITORY This flap includes a segment of the fibular bone with or without the overlying skin island on the peroneal/ lateral aspect of the calf.
17 Fibula Flap Tor Chiu Fibula Flap 153 Fibula Flap FLAP TERRITORY This flap includes a segment of the fibular bone with or without the overlying skin island on the peroneal/ lateral aspect of the calf.
A Patient s Guide to Ankle Anatomy
 A Patient s Guide to Ankle Anatomy 1436 Exchange Street Middlebury, VT 05753 Phone: 802-388-3194 Fax: 802-388-4881 cvo@champlainvalleyortho.com DISCLAIMER: The information in this booklet is compiled from
A Patient s Guide to Ankle Anatomy 1436 Exchange Street Middlebury, VT 05753 Phone: 802-388-3194 Fax: 802-388-4881 cvo@champlainvalleyortho.com DISCLAIMER: The information in this booklet is compiled from
KNEE EXAMINATION. Tips & Tricks from an Emergency Physician Perspective. EM Physicians Less Exposed to MSK Medicine
 KNEE EXAMINATION Tips & Tricks from an Emergency Physician Perspective Dr P O CONNOR Emergency Medicine Physician EUSEM 10/09/2018 EM Physicians Less Exposed to MSK Medicine Musculoskeletal Medicine becoming
KNEE EXAMINATION Tips & Tricks from an Emergency Physician Perspective Dr P O CONNOR Emergency Medicine Physician EUSEM 10/09/2018 EM Physicians Less Exposed to MSK Medicine Musculoskeletal Medicine becoming
Anatomy of Foot and Ankle
 Anatomy of Foot and Ankle Surface anatomy of the ankle & foot Surface anatomy of the ankle & foot Medial orientation point medial malleous sustentaculum tali tuberosity of navicular TA muscle TP muscle
Anatomy of Foot and Ankle Surface anatomy of the ankle & foot Surface anatomy of the ankle & foot Medial orientation point medial malleous sustentaculum tali tuberosity of navicular TA muscle TP muscle
Muscles of the Gluteal Region
 Muscles of the Gluteal Region 1 Some of the most powerful in the body Extend the thigh during forceful extension Stabilize the iliotibial band and thoracolumbar fascia Related to shoulders and arms because
Muscles of the Gluteal Region 1 Some of the most powerful in the body Extend the thigh during forceful extension Stabilize the iliotibial band and thoracolumbar fascia Related to shoulders and arms because
Lumbar Plexus. Ventral rami L1 L4 Supplies: Major nerves.. Abdominal wall External genitalia Anteromedial thigh
 Lower Limb Nerves Lectures Objectives Describe the structure and relationships of the plexuses of the lower limb. Describe the course, relationships and structures supplied for the major nerves of the
Lower Limb Nerves Lectures Objectives Describe the structure and relationships of the plexuses of the lower limb. Describe the course, relationships and structures supplied for the major nerves of the
Organization of the Lower Limb Audrone Biknevicius, Ph.D. Dept. Biomedical Sciences, OU HCOM at Dublin Clinical Anatomy Immersion 2014
 Organization of the Lower Limb Audrone Biknevicius, Ph.D. Dept. Biomedical Sciences, OU HCOM at Dublin Clinical Anatomy Immersion 2014 www.thestudio1.co.za LIMB FUNCTION choco-locate.com blog.coolibar.com
Organization of the Lower Limb Audrone Biknevicius, Ph.D. Dept. Biomedical Sciences, OU HCOM at Dublin Clinical Anatomy Immersion 2014 www.thestudio1.co.za LIMB FUNCTION choco-locate.com blog.coolibar.com
Compartment Syndrome
 Compartment Syndrome Chapter 34 Compartment Syndrome Introduction Compartment syndrome may occur with an injury to any fascial compartment. The fascial defect caused by the injury may not be adequate to
Compartment Syndrome Chapter 34 Compartment Syndrome Introduction Compartment syndrome may occur with an injury to any fascial compartment. The fascial defect caused by the injury may not be adequate to
Musculoskeletal Ultrasound of the Knee, Foot and ankle
 Musculoskeletal Ultrasound of the Knee, Foot and ankle ADVANCED TEAM PHYSICIAN COURSE SAN DIEGO, CALIFORNIA DECEMBER 11TH 2016 Jonathan S. Halperin MD Learning objec-ves: Understand the basics of knee,
Musculoskeletal Ultrasound of the Knee, Foot and ankle ADVANCED TEAM PHYSICIAN COURSE SAN DIEGO, CALIFORNIA DECEMBER 11TH 2016 Jonathan S. Halperin MD Learning objec-ves: Understand the basics of knee,
Anatomy and Sports Injuries of the Knee
 Anatomy and Sports Injuries of the Knee I. Anatomy II. Assessment III. Treatment IV. Case Study V. Dissection Anatomy Not a hinge joint 6 degrees of freedom Flexion/Extension Rotation Translation Anatomy
Anatomy and Sports Injuries of the Knee I. Anatomy II. Assessment III. Treatment IV. Case Study V. Dissection Anatomy Not a hinge joint 6 degrees of freedom Flexion/Extension Rotation Translation Anatomy
Main Menu. Ankle and Foot Joints click here. The Power is in Your Hands
 1 The Ankle and Foot Joints click here Main Menu Copyright HandsOn Therapy Schools 2009 K.8 http://www.handsonlineeducation.com/classes/k8/k8entry.htm[3/27/18, 1:40:03 PM] Ankle and Foot Joint 26 bones
1 The Ankle and Foot Joints click here Main Menu Copyright HandsOn Therapy Schools 2009 K.8 http://www.handsonlineeducation.com/classes/k8/k8entry.htm[3/27/18, 1:40:03 PM] Ankle and Foot Joint 26 bones
Management of Knee Dislocations
 Management of Knee Dislocations Thomas J. Gill, MD Chief, Sports Medicine Service Massachusetts General Hospital Associate Professor of Orthopedic Surgery Harvard Medical School Complex Challenging Multi-Ligament
Management of Knee Dislocations Thomas J. Gill, MD Chief, Sports Medicine Service Massachusetts General Hospital Associate Professor of Orthopedic Surgery Harvard Medical School Complex Challenging Multi-Ligament
The Muscular System. Chapter 10 Part D. PowerPoint Lecture Slides prepared by Karen Dunbar Kareiva Ivy Tech Community College
 Chapter 10 Part D The Muscular System Annie Leibovitz/Contact Press Images PowerPoint Lecture Slides prepared by Karen Dunbar Kareiva Ivy Tech Community College Table 10.14: Muscles Crossing the Hip and
Chapter 10 Part D The Muscular System Annie Leibovitz/Contact Press Images PowerPoint Lecture Slides prepared by Karen Dunbar Kareiva Ivy Tech Community College Table 10.14: Muscles Crossing the Hip and
Leo Kormanik DC, MS, CCSP Ohio Sports Chiropractic
 Leo Kormanik DC, MS, CCSP Ohio Sports Chiropractic ! Been running at a high level for 15 years.! 2012 Olympics Trials qualifier in the marathon and 6-time All-American in college! Owner of Ohio Sports
Leo Kormanik DC, MS, CCSP Ohio Sports Chiropractic ! Been running at a high level for 15 years.! 2012 Olympics Trials qualifier in the marathon and 6-time All-American in college! Owner of Ohio Sports
Reconstruction of the Ligaments of the Knee
 Reconstruction of the Ligaments of the Knee Contents ACL reconstruction Evaluation Selection Evolution Graft issues Notchplasty Tunnel issues MCL PCL Posterolateral ligament complex Combined injuries Evaluation
Reconstruction of the Ligaments of the Knee Contents ACL reconstruction Evaluation Selection Evolution Graft issues Notchplasty Tunnel issues MCL PCL Posterolateral ligament complex Combined injuries Evaluation
DISSECTION SCHEDULE. Session I - Hip (Front) & Thigh (Superficial)
 & Thigh (Superficial)") DISSECTION SCHEDULE Session I - Hip (Front) & Thigh (Superficial) Surface anatomy Inguinal region Gluteal region Thigh Leg Foot bones Hip bone Femur Superficial fascia Great saphenous vein Superficial
DISSECTION SCHEDULE Session I - Hip (Front) & Thigh (Superficial) Surface anatomy Inguinal region Gluteal region Thigh Leg Foot bones Hip bone Femur Superficial fascia Great saphenous vein Superficial
FACTS 1. Most need only Gastro aponeurotic release [in positive Silverskiold test]
![FACTS 1. Most need only Gastro aponeurotic release [in positive Silverskiold test]](/thumbs/83/88335212.jpg "FACTS 1. Most need only Gastro aponeurotic release [in positive Silverskiold test]") FOOT IN CEREBRAL PALSY GAIT IN CEREBRAL PALSY I True Equinus II Jump gait III Apparent Equinus IV Crouch gait Group I True Equinus Extended hip and knee Equinus at ankle II Jump Gait [commonest] Equinus
FOOT IN CEREBRAL PALSY GAIT IN CEREBRAL PALSY I True Equinus II Jump gait III Apparent Equinus IV Crouch gait Group I True Equinus Extended hip and knee Equinus at ankle II Jump Gait [commonest] Equinus
Rehabilitation of an ACL injury in a 29 year old male with closed kinetic chain exercises: A case study
 Abstract Objective: This paper will examine a rehabilitation program for a healthy 29 year old male who sustained an incomplete tear of the left ACL. Results: Following a 9 week treatment plan focusing
Abstract Objective: This paper will examine a rehabilitation program for a healthy 29 year old male who sustained an incomplete tear of the left ACL. Results: Following a 9 week treatment plan focusing
How to Triage Orthopaedic Care. David W. Gray, M.D.
 How to Triage Orthopaedic Care David W. Gray, M.D. OBJECTIVES: Define basic assessments skills needed to identify orthopedic injuries Differentiate when an orthopedic injury is a medical emergency Determine
How to Triage Orthopaedic Care David W. Gray, M.D. OBJECTIVES: Define basic assessments skills needed to identify orthopedic injuries Differentiate when an orthopedic injury is a medical emergency Determine
FUNCTIONAL ANATOMY: Knee and Leg
 ACSM Team Physician Course San Antonio Feb 2015 FUNCTIONAL ANATOMY: Knee and Leg Marlene DeMaio, MD Professor, Orthopaedic Surgery Marshall University VAMC Huntington, WV Mary Lloyd Ireland, MD Professor
ACSM Team Physician Course San Antonio Feb 2015 FUNCTIONAL ANATOMY: Knee and Leg Marlene DeMaio, MD Professor, Orthopaedic Surgery Marshall University VAMC Huntington, WV Mary Lloyd Ireland, MD Professor
A Patient s Guide to Ankle Anatomy
 A Patient s Guide to Ankle Anatomy Pond View Professional Park 301 Professional View Drive Freehold, NJ 07728 Phone: 732-720-2555 DISCLAIMER: The information in this booklet is compiled from a variety
A Patient s Guide to Ankle Anatomy Pond View Professional Park 301 Professional View Drive Freehold, NJ 07728 Phone: 732-720-2555 DISCLAIMER: The information in this booklet is compiled from a variety
Dupuytrens contracture
 OA Wrist Ganglion/Cysts Dupuytrens contracture Carpal Tunnel Syndrome Carpal Tunnel pathway For advice on management of CTS please follow link to Map of Medicine Trigger Finger Trigger finger pathway For
OA Wrist Ganglion/Cysts Dupuytrens contracture Carpal Tunnel Syndrome Carpal Tunnel pathway For advice on management of CTS please follow link to Map of Medicine Trigger Finger Trigger finger pathway For
Clinical Characteristics of Peroneal Nerve Palsy by Posture
 www.jkns.or.kr http://dx.doi.org/10.3340/jkns.2013.53.5.269 J Korean Neurosurg Soc 53 : 269-273, 2013 Print ISSN 2005-3711 On-line ISSN 1598-7876 Copyright 2013 The Korean Neurosurgical Society Clinical
www.jkns.or.kr http://dx.doi.org/10.3340/jkns.2013.53.5.269 J Korean Neurosurg Soc 53 : 269-273, 2013 Print ISSN 2005-3711 On-line ISSN 1598-7876 Copyright 2013 The Korean Neurosurgical Society Clinical
Ganglion of the peroneal nerve. CULLY A. COBB, III, M.D., AND RICHARD H. MoIr4 M.D.
 Ganglion of the peroneal nerve Report of two cases CULLY A. COBB, III, M.D., AND RICHARD H. MoIr4 M.D. Division of Neurological Surgery, Baylor College of Medicine, Houston, Texas ~" Peroneal nerve ganglion
Ganglion of the peroneal nerve Report of two cases CULLY A. COBB, III, M.D., AND RICHARD H. MoIr4 M.D. Division of Neurological Surgery, Baylor College of Medicine, Houston, Texas ~" Peroneal nerve ganglion
Human Anatomy Biology 255
 Human Anatomy Biology 255 Exam #4 Please place your name and I.D. number on the back of the last page of this exam. You must answer all questions on this exam. Because statistics demonstrate that, on average,
Human Anatomy Biology 255 Exam #4 Please place your name and I.D. number on the back of the last page of this exam. You must answer all questions on this exam. Because statistics demonstrate that, on average,