Review Article Primary and Posttraumatic Arthritis of the Elbow
|
|
|
- Clementine McGee
- 5 years ago
- Views:
Transcription
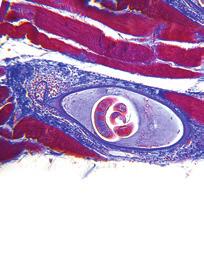
1 Arthritis Volume 2013, Article ID , 6 pages Review Article Primary and Posttraumatic Arthritis of the Elbow Debdut Biswas, Robert W. Wysocki, and Mark S. Cohen Section of Hand and Elbow Surgery, Department of Orthopaedic Surgery, Rush University Medical Center, 1611 W. Harrison Street, Chicago, IL 60612, USA Correspondence should be addressed to Mark S. Cohen; mark s cohen@rush.edu Received 2 January 2013; Revised 31 March 2013; Accepted 8 April 2013 Academic Editor: Changhai Ding Copyright 2013 Debdut Biswas et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Whether degenerative joint disease of the elbow may be the result of primary or posttraumatic etiologies, arthritis of the elbow commonly leads to pain, loss of motion, and functional disability. A detailed history and focused physical examination, in combination with imaging modalities, can help localize the origin of symptoms and help direct treatment. Although nonoperative treatment is the initial therapy for arthritis of the elbow, surgical interventions may provide substantial relief to the appropriately selected patient. 1. Introduction Degenerative joint disease of the elbow may be a painful condition for a majority of patients. Although primary osteoarthritis is less common than posttraumatic arthritis of the elbow, both conditions result in symptoms which affect the quality of life. The health care provider encountering these conditions must carefully tailor treatments, both nonoperative and operative, to account for the patient s age, personal preferences, functional demands, and severity of arthritic changes. This paper will review the pathogenesis of both primary and posttraumatic arthritis of the elbow. The principles of nonoperative management will be presented as well as the indications and considerations for operative treatment. 2. Background/Pathogenesis 2.1. Primary Osteoarthritis. Primary osteoarthritis of the elbow is an uncommon condition which occurs predominantly within the ulnohumeral joint of the dominant extremity of patientswhoengageinheavysportorlabor.theintrinsic congruity of the ulnohumeral articulation preserves a majority of the articular cartilage, with degenerative changes and osteophytes initially affecting the tips of the olecranon and coronoid processes as well as their respective fossae within the distal humerus. Accordingly, the most common complaint of patients in our practice with early stages of primary osteoarthritis of the elbow is pain at terminal flexion and extension, as the osteophytes of the coronoid and olecranon engage their fossae. As the degenerative process involves more of the articular surface, pain is encountered throughout the arc of motion, and enlarging osteophytes coupled with anterior and posterior capsular contracture may provide further mechanical impediments to motion and result in measurable loss of motion in terminal flexion and extension. The majority of articular surface involvement is confined to the ulnohumeral joint. Isolated primary osteoarthritis is uncommon within the radiocapitellar articulation. Accordingly, the practitioner should carry out a detailed history and meticulous physical examination in order to localize the origin of symptoms in the patient with primary osteoarthritis of the elbow. Ulnohumeral arthrosis typically results in pain and diminished range of motion in flexion and extension, while radiocapitellar arthrosis predominantly manifests as focal lateral-sided pain over the radiocapitellar joint during forearm rotation (Figure 1) Posttraumatic Arthritis. A variety of traumatic insults may ultimately result in specific forms of posttraumatic arthritis to the elbow joint. Radiocapitellar incongruity may result following malunion of an intraarticular radial head fracture (Figure 2); patientswill typically reportlateral-sided



2 2 Arthritis Figure 1: Lateral radiograph demonstrates idiopathic arthritis with osteophytes on the radial head as well as anterior and posterior ulnohumeral joints. Figure 2: Oblique and lateral radiographs of a patient who sustained a radial head fracture treated nonoperatively; this patient later developed lateral elbow pain with forearm rotation. Radiographs demonstrate anterolateral osteophytes noted at the radial head and decreased joint space in the radiocapitellar joint. pain and crepitus exacerbated during rotation of the forearm rather than flexion and extension. Conversely, malunion of distal humerus or olecranon fractures which extend intraarticularly into the ulnohumeral joint typically result in arthritis which is symptomatic during flexion and extension. Although malignments in the geometry of the articular surface alter contact pressures and expedite the development of arthritis, ligamentous instability about the elbow may also result in abnormal joint kinematics and the potential for degenerative changes. These potential injuries should be carefully evaluated, as the presence of elbow instability dramatically alters the treatment objectives in the setting of elbow arthritis, particularly when surgical intervention is considered. 3. Evaluation 3.1. History. The most common complaints of patients with either primary or posttraumatic arthritis of the elbow are pain and/or loss of motion; it is important for the practitioner to precisely characterize the principal complaint. Complaints of pain should be localized when possible, particularly when attempting to discern between symptomatic arthrosis of the radiocapitellar or ulnohumeral joint. Pain may be associated at the extremes of motion in earlier forms of ulnohumeral arthritis but may be experienced throughout the arc of elbow flexion and extension in more advanced disease [1, 2]. Although loss of extension is most common, loss of motion may manifest itself as a loss in elbow flexion or forearm rotation depending on the site of arthritis, and it is important to determine if there is true functional disability from the condition, or if the symptoms represent simply a subtle asymmetry when compared to the contralateral side. Forpatientswhoreportapriorepisodeofsignificant elbow trauma, the details surrounding the initial injury as well as mechanism of trauma are important aspects of the history, as any previous treatments including operative reports from previous surgeries and therapy reports to elicit what treatments have been undertaken. Ulnar neuropathy is a frequent finding in patients presenting with degenerative joint disease of the elbow and is frequently subtle and not part of the patient s chief complaint. The examiner should specifically inquire about sensations of numbness and tingling in the ring and small finger, loss of dexterity, and soreness over theulnarnerveintheposteromedialelbow,inordertocomprehensively evaluate for cubital tunnel syndrome. Although uncommon, any suggestion or suspicion of infection in the setting of previous open trauma, surgery, or septic arthritis requires a thorough evaluation, including serologic markers and aspiration of the joint to be analyzed for synovial fluid cell count, culture, and gram stain. Finally, the demand level of the patient must be carefully considered, as certain patients may desire nearly full motion for specific lifestyle and employment demands, which would lower the threshold for motion-preserving debridement, while others may require heavy lifting which would preclude treatment with a total elbow arthroplasty. It should be noted that loss of flexion tends to be much more functionally limiting than loss of extension, as the latter can be compensated for simply by moving closer to an object to reach it. A loss of flexion, however, cannot be compensated for. A loss of pronation can be accommodated for by abducting the shoulder, whereas a loss of supination cannot be accommodated for. The willingness of the patient to comply with the required extensive programs of therapy must also be considered, as treatment outcomes depend on diligent participation in a structured rehabilitation program Physical Examination. Physical examination begins with inspection of the entire upper extremity, specifically evaluating for deformity, swelling, and muscle atrophy, while noting the location of any previous surgical incisions that would influence further surgical planning. Range-of-motion evaluationshouldincludethehand,wrist,forearm,andelbow and should be compared with the contralateral, unaffected extremity. In the posttraumatic setting, loss of extension is

3 Arthritis 3 more common than loss of flexion, whereas in osteoarthritis the loss in motion is quite variable depending on the location of impinging osteophytes. A careful neurovascular examination is important, especiallyduringtheevaluationofulnarnervefunction.residing in the cubital tunnel and adjacent to the medial joint capsule, the ulnar nerve may become compressed either from scar tissue along the medial elbow following trauma or from thickened capsule, osteophytes, or synovitis. Traction ulnar neuritisoftheelbowmaymanifestasmedialelbowpain and patients may complain of sensory changes in an ulnar nerve distribution, particularly with elbow flexion. Patients with posttraumatic ulnar neuropathy may present simply with loss of flexion and medial elbow pain in the absence of overt symptoms of ulnar neuropathy; thus, a meticulous neurovascular evaluation, including two-point discrimination, pinch strength, and intrinsic muscle function are essential to document the preoperative function of the ulnar nerve. Electrodiagnostic testing may be considered in the setting of provocative symptoms of ulnar neuropathy. Evaluation of elbow stability is essential in order to exclude ligamentous insufficiency as a potential diagnosis. Varus and valgus stresses are applied to the affected elbow with the contralateral elbow serving as a normal comparison. Posterolateral rotatory stability is evaluated with the lateral pivot-shift maneuver; this test is performed by applying a valgus stress and axial load to the partially flexed elbow with the forearm fully supinated. Posterior subluxation of the radial head is pathogonomic for posterolateral rotatory instability;alternatively,painwithoutsubluxationissuggestiveof instability [3] Imaging. Plain radiographs of the elbow are typically obtained and include anteroposterior, lateral, and oblique projections; diligent efforts should be made to review previous imaging for patients presenting with posttraumatic arthritis. Stress radiographs should be considered if elbow instability is suspected. Radiographs typically demonstrate preservation of joint space centrally with osteophytes along the anterior and posterior aspects of the joint which may cause impingement (Figure 1). Radiographs should be carefullyexaminedintheposttraumaticelbow,specificallyevaluating for malalignment, incongruency of the ulnohumeral or radiocapitellar joints, or the development of heterotopic ossification (HO). Rettig et al. have suggested that surgical debridement may be less effective for more advanced arthrosis of the elbow joint as visualized on diagnostic imaging [4]. Computerized tomography (CT) is frequently useful, especially when HO or intra-articular loose bodies are suspected, or if bony deformity or malunion is suspected in the setting of previous fracture. CT reconstruction is typically helpful in further delineating bony and articular anatomy (Figure 3). Advanced imaging is important in documenting ulnohumeral joint congruency as well as any osseous impingement secondary to overgrowth in the olecranon or coronoid fossae that would directly serve to limit motion. Magnetic resonance imaging (MRI) has a very limited role except to potentially workup subtle posttraumatic instability. Figure 3: Sagittal CT image demonstrating osteophytes within the olecranon and coronoid fossae of the distal humerus. 4. Nonoperative Treatment Nonoperative management remains the mainstay of initial treatment for both primary osteoarthritis of the elbow and posttraumatic arthritis of the elbow and typically includes elbow sleeves, nonsteroidal anti-inflammatory medications, and intra-articular corticosteroid injections. For early-stage primary arthritis, symptoms are strongly associated with specific activities (weight-lifting, boxing, etc.), and counseling patients on avoidance of aggressive terminal flexion and extension exercises can result in substantial relief of pain. A course of supervised rehabilitation by a certified therapist is reserved typically for patients presenting with an acute-onchronic presentation of symptoms with an associated effusion and limitations in motion. Few reports have evaluated the role of hyaluronic acid as nonoperative management of elbow arthritis. A limited report on 18 patients demonstrated modest relief of pain at 3 months but no long-term benefit following the intraarticular injection of hyaluronic acid in the arthritic elbow [5]. 5. Operative Treatment Surgical management is indicated for patients with elbow pain or significant loss of mobility with resultant impairment of upper extremity function and limitation with daily activities. Careful consideration of patients primary complaints is important in selecting the appropriate surgical intervention. Patients who continue to experience stiffness rather than pain despite nonoperative management may experience improvements in upper extremity function by surgical treatment, either open or arthroscopic debridement and capsular release. Similarly, patients with pain only the extremes of terminal flexion and/or extension but not in the midarc of elbow motion may benefit most from debridement as opposed to those with pain throughout the motion arc, which suggests arthritic involvement of the entire ulnohumeral joint.
4 4 Arthritis 5.1. Surgical Debridement. Fromapurelymechanicalstandpoint, to improve elbow extension, posterior impingement must be removed between the olecranon tip and the olecranon fossa. Anteriorly, tethering soft tissues such as the anterior joint capsule and any adhesions between the brachialis and the humerus must be released. Similarly, to improve elbow flexion, the surgeon must release any posterior soft tissue structures that may be tethering the joint. They include the posterior joint capsule and the triceps muscle, which can becomeadherenttothehumerus.thesurgeonmustremove any bony or soft-tissue impingement anteriorly, including anysoft-tissueovergrowthinthecoronoidandradialfossae. There must be a concavity above the humeral trochlea and capitellum to accept the coronoid centrally and the radial head laterally for full flexion to occur. These principles may be applied in the treatment of patients with the majority of their articular surfaces preserved but still complain of pain at the extremes of motion, as they will respond favorably to debridement of osteophytes anteriorly and/or posteriorly but with much of the articular surface well preserved. Although a flexion contracture of at least 25 to 30 degrees and/or less than 110 to 115 degrees of active flexion was historically reported as an indication for surgical contracture release, surgical management may still be offered to certain patients who may desire full or nearly full motion for specific lifestyle and employment demands. Posttraumatic patients typicallymustbeatleast3to4monthsremovedfrominjury toallowthemtoachieve tissueequilibrium, withmaximal resolution of posttraumatic swelling and inflammation. Most importantly, patients must be willing to comply with the required extensive program of postoperative therapy, as operative outcomes depend on diligent participation in a structured rehabilitation program. Advances in elbow arthroscopy have resulted in favorable outcomes. Arthroscopic debridement of the elbow, particularly in a younger patient population, has excellent results with improvements in pain and range of motion [6 9]when the procedures are performed by surgeons with substantial experience with safe, meticulous techniques in elbow arthroscopy. Open debridement should be considered in cases featuring severe elbow contractures with minimal joint motion, with ulnar nerve transposition surgery, and the presence of significant heterotopic bone. These patients are more reliably treated with extensive open surgery rather than arthroscopic debridement of the elbow to restore motion and protect the ulnar nerve. Open debridement, when required, is now commonly performed using medial and lateral exposures that provide adequate access for debridement and capsular release of the anterior and posterior elbow [10, 11]. Prior surgical exposure of the radial head might result in scarring and adhesions of the radial nerve to the anterior capsule, rendering the nerve susceptible to iatrogenic injury during arthroscopy. Open debridement is also indicated in this scenario. If the ulnohumeral joint shows marked degenerative changes, a simple release of the joint may not lead to improved motion and may exacerbate pain in an arthritic joint. If advanced posttraumatic arthritis is observed in the ulnohumeral articulation, salvage-type procedures are often required such as total elbow arthroplasty or soft-tissue interposition arthroplasty if surgery is undertaken [12]. Open ulnar nerve decompression with or without transposition should be considered along with open or arthroscopic elbow debridement if the patient has positive provocative neuropathic symptoms signs (i.e., a positive Tinel s test) or if the patient cannot flex past 100 to 110 degrees before surgery. Increased postoperative flexion following debridement theoretically should place the nerve at elevated risk of traction neuropathy [11]. Subtle elbow instability can commonly manifest as loss of motion after elbow fracture-dislocation; accordingly, specialattentionshouldbedevotedtowardsevaluatingelbow stability either with stability testing on physical examination or with stress radiographs. When instability is present, then treatment typically would include ligament reconstruction with or without capsular release if there is no arthritis present. In the setting of concomitant degenerative changes from long-standing instability, however, salvage arthroplasty options are considered. The stiff and unstable elbow is a particularly challenging condition to treat Advanced Ulnohumeral Arthritis. Although the outcomes following arthroscopic and open debridement for elbowarthritisandstiffnessarepromising,theseoutcomes predominantly occurred in patients with moderate disease. Individuals with diffuse joint space narrowing and pain throughoutthearcofmotionaresuggestiveofmoreadvanced arthrosis, which might not respond favorably to either arthroscopic or open elbow debridement. Forpatientswithadvanceddiseasewhohavefailednonoperative management, the primary surgical considerations includetheageanddemandlevelofthepatient.younger, high-demand patients with inflammatory arthropathy or severe posttraumatic or primary arthritis which affects the majority of the ulnohumeral articular surfaces are candidates for interposition arthroplasty or elbow arthrodesis. These procedures do not require postoperative lifting restrictions ( kg) as total elbow arthroplasty and are best suited for a younger, high-demand cohort of patients. If the surgeon is considering interposition arthroplasty, elbow stability and adequate bone stock should be confirmed preoperatively, as this procedure may place the elbow at increased risk of postoperative instability [13]. Total elbow arthroplasty is most appropriate for the lowdemand, elderly patient (>60 year-old) with inflammatory, posttraumatic, or primary elbow arthritis. It is paramount that these patients understand and are compliant with the substantial postoperative lifting restrictions following total elbow arthroplasty (Figure 4) [14]. Total elbow arthroplasty is rarely applied in the setting of elbow osteoarthritis which occurs in a younger and typically male population. This procedure is most commonly applied for rheumatoid arthritis and comminuted distal humerus fractures in the elderly Radiocapitellar Arthritis. For the patients with symptomatic radiocapitellar arthritis who require surgical management, favorable outcomes following both open and




5 Arthritis 5 of comminuted radial head fracture, it is not effective in the setting of radiocapitellar arthritis since the capitellum has already degenerated. Radiocapitellar arthroplasty, including both radial head and capitellar replacement, is in the early stages of development to address this shortcoming but is not yet widely available. Innovations in implant design and surgical technique continue to evolve and outcomes are being more widely reported as surgical experience with these implants expands for use in treating radiocapitellar arthrosis [17, 18]. 6. Summary Figure 4: AP and lateral radiographs of a patient who underwent total elbow arthroplasty. Figure 5: A young male laborer with symptomatic arthrosis of the radiocapitellar joint (A) underwent radial head resection; follow-up radiographs demonstrate progressive ulnohumeral arthritis approximately 18 months following the surgical procedure. arthroscopic radial head resection have been reported. Lateral elbow pain localized to the radiocapitellar joint with forearm rotation helps the practitioner identify patients with symptomatic arthritis of the radiocapitellar joint, and several authors have reported favorable outcomes of radial head resection [15, 16]. In asymptomaticpatientswho radiographically demonstrate radiocapitellar arthrosis but do not have lateral elbow pain localized to the radiocapitellar joint, the surgical results are less favorable as axial load across the joint is transferred to the ulnohumeral joint following radial head resection [9]. Although radial head resection does demonstrate favorable results in the appropriately selected patient, proximal migration of the radius may occur or progressive ulnohumeral arthritis may develop at the medial joint line owing to increased valgus forces at the elbow in younger higher demand patients (Figure 5). Radial head resection also predictably leads to decreased grip strength and can only be performed when there is no ligamentous elbow instability. While radial head replacement is widely utilized in the setting The evaluation of posttraumatic and primary osteoarthritis of the elbow requires a thorough, systematic approach to help accurately characterize the primary complaint and formulate a carefully considered treatment plan which accounts for the activity level and functional requirements of a given patient. Nonoperative treatment is almost always initiated although surgical treatment may be indicated in cases refractory to conservative management. Younger patients who experience pain or loss of motion in early stage ulnohumeral arthritis have experienced favorable outcomes following both arthroscopic and open elbow debridement although arthroscopic debridement should only be performed by surgeons who possess the advanced technical skills necessary for safe elbow arthroscopy. Patients with more advanced arthrosis of the elbow commonly require salvage reconstructive procedures. Although total elbow arthroplasty may be performed in the older, low-demand patient, the procedure may not be appropriate for younger, active patients who may not comply with substantial lifting restrictions required for longevity of the implants. For high-demand patients with advanced elbow arthritis, interposition arthroplasty or arthrodesis may provide acceptable functional outcomes while avoiding activity restrictions required by arthroplasty. Conflict of Interests The authors report no conflict of interests related to the publication of this paper. References [1] E.V.Cheung,R.Adams,andB.F.Morrey, Primaryosteoarthritis of the elbow: current treatment options, the American Academy of Orthopaedic Surgeons, vol.16,no.2,pp , [2]R.A.Gallo,A.Payatakes,andD.G.Sotereanos, Surgical Options for the Arthritic Elbow, JournalofHandSurgery,vol. 33,no.5,pp ,2008. [3] S. W. O Driscoll, Classification and evaluation of recurrent instability of the elbow, Clinical Orthopaedics and Related Research, no. 370, pp , [4]L.A.Rettig,H.Hastings,andJ.R.Feinberg, Primaryosteoarthritis of the elbow: lack of radiographic evidence for morphologic predisposition, results of operative debridement at intermediate follow-up, and basis for a new radiographic classification system, Shoulder and Elbow Surgery,vol.17, no. 1, pp , 2008.
6 6 Arthritis [5] R. W. van Brakel and D. Eygendaal, Intra-articular injection of hyaluronic acid is not effective for the treatment of posttraumatic osteoarthritis of the elbow, Arthroscopy, vol.22,no. 11, pp , [6] F. H. Savoie, P. D. Nunley, and L. D. Field, Arthroscopic management of the arthritic elbow: indications, technique, and results, Shoulder and Elbow Surgery, vol. 8, no. 3, pp , [7] C. M. Ball, M. Meunier, L. M. Galatz, R. Calfee, and K. Yamaguchi, Arthroscopic treatment of post-traumatic elbow contracture, Shoulder and Elbow Surgery, vol. 11, no. 6, pp , [8]D.Nguyen,S.I.W.Proper,J.C.MacDermid,G.J.W.King, and K. J. Faber, Functional outcomes of arthroscopic capsular release of the elbow, Arthroscopy, vol. 22, no. 8, pp , [9]E.W.Kelly,R.Bryce,J.Coghlan,andS.Bell, Arthroscopic debridement without radial head excision of the osteoarthritic elbow, Arthroscopy,vol.23,no.2,pp ,2007. [10] S. A. Antuña,B.F.Morrey,R.A.Adams,andS.W.O Driscoll, Ulnohumeral arthroplasty for primary degenerative arthritis of the elbow: long-term outcome and complications, Bone and Joint Surgery A,vol.84,no.12,pp ,2002. [11] N. J. Phillips, A. Ali, and D. Stanley, Treatment of primary degenerative arthritis of the elbow by ulnohumeral arthroplasty. Along-termfollow-up, Bone and Joint Surgery B,vol. 85,no.3,pp ,2003. [12] J. B. Jupiter, S. W. O Driscoll, and M. S. Cohen, The assessment and management of the stiff elbow, Instructional Course Lectures, vol. 52, pp , [13] A.N.LarsonandB.F.Morrey, Interpositionarthroplastywith an achilles tendon allograft as a salvage procedure for the elbow, Bone and Joint Surgery A, vol.90,no.12,pp , [14] C.P.Little,A.J.Graham,andA.J.Carr, Totalelbowarthroplasty: a systematic review of the literature in the English language until the end of 2003, Bone and Joint Surgery, vol.87,no.4,pp ,2005. [15] M. A. Broberg and B. F. Morrey, Results of delayed excision of the radial head after fracture, Bone and Joint Surgery A, vol. 68, no. 5, pp , [16] R. E. McLaughlin, F. H. Savoie, L. D. Field, and J. R. Ramsey, Arthroscopic treatment of the arthritic elbow due to primary radiocapitellar arthritis, Arthroscopy, vol. 22, no. 1, pp , [17] M. R. Zunkiewicz, J. S. Clemente, M. C. Miller et al., Radial head replacement with a bipolar system: a minimum 2-year follow-up, JournalofShoulderandElbowSurgery, vol. 21, no. 1, pp , [18] B. J. Shore, J. B. Mozzon, J. C. MacDermid, K. J. Faber, and G. J. W. King, Chronic posttraumatic elbow disorders treated with metallic radial head arthroplasty, Bone and Joint Surgery A,vol.90,no.2,pp ,2008.











7 MEDIATORS of INFLAMMATION The Scientific World Journal Gastroenterology Research and Practice Diabetes Research International Endocrinology Immunology Research Disease Markers Submit your manuscripts at BioMed Research International PPAR Research Obesity Ophthalmology Evidence-Based Complementary and Alternative Medicine Stem Cells International Oncology Parkinson s Disease Computational and Mathematical Methods in Medicine AIDS Behavioural Neurology Research and Treatment Oxidative Medicine and Cellular Longevity
Rehabilitation after Total Elbow Arthroplasty
 Rehabilitation after Total Elbow Arthroplasty Total Elbow Atrthroplasty Total elbow arthroplasty (TEA) Replacement of the ulnohumeral articulation with a prosthetic device. Goal of TEA is to provide pain
Rehabilitation after Total Elbow Arthroplasty Total Elbow Atrthroplasty Total elbow arthroplasty (TEA) Replacement of the ulnohumeral articulation with a prosthetic device. Goal of TEA is to provide pain
ELBOW ARTHROSCOPY WHERE ARE WE NOW?
 ELBOW ARTHROSCOPY WHERE ARE WE NOW? Christian Veillette M.D., M.Sc., FRCSC Assistant Professor, University of Toronto Shoulder & Elbow Reconstructive Surgery Toronto Western Hospital @ University Health
ELBOW ARTHROSCOPY WHERE ARE WE NOW? Christian Veillette M.D., M.Sc., FRCSC Assistant Professor, University of Toronto Shoulder & Elbow Reconstructive Surgery Toronto Western Hospital @ University Health
Elbow. Chapter 2 LISTEN. Mechanism of Injury (If Applicable) Pain
 Pain") Chapter 2 Elbow LISTEN Mechanism of Injury (If Applicable) Patient usually remembers their position at the time of injury Certain mechanisms of injury result in characteristic patterns Fall on outstretched
Chapter 2 Elbow LISTEN Mechanism of Injury (If Applicable) Patient usually remembers their position at the time of injury Certain mechanisms of injury result in characteristic patterns Fall on outstretched
Case Report Successful Closed Reduction of a Lateral Elbow Dislocation
 Case Reports in Orthopedics Volume 2016, Article ID 5934281, 5 pages http://dx.doi.org/10.1155/2016/5934281 Case Report Successful Closed Reduction of a Lateral Elbow Dislocation Kenya Watanabe, Takuma
Case Reports in Orthopedics Volume 2016, Article ID 5934281, 5 pages http://dx.doi.org/10.1155/2016/5934281 Case Report Successful Closed Reduction of a Lateral Elbow Dislocation Kenya Watanabe, Takuma
Inspection. Physical Examination of the Elbow. Anterior Elbow 2/14/2017. Inspection. Carrying angle. Lateral dimple. Physical Exam of the Elbow
 of the Elbow Anthony A. Romeo, MD Professor, Department of Orthopedics Head, Section of Shoulder and Elbow Surgery Rush University President-Elect, American Shoulder Elbow Surgeons Team Physician, Chicago
of the Elbow Anthony A. Romeo, MD Professor, Department of Orthopedics Head, Section of Shoulder and Elbow Surgery Rush University President-Elect, American Shoulder Elbow Surgeons Team Physician, Chicago
MANAGEMENT OF INTRAARTICULAR FRACTURES OF ELBOW JOINT. By Dr B. Anudeep M. S. orthopaedics Final yr pg
 MANAGEMENT OF INTRAARTICULAR FRACTURES OF ELBOW JOINT By Dr B. Anudeep M. S. orthopaedics Final yr pg INTRAARTICULAR FRACTURES Intercondyar fracture Elbow dislocation Capitellum # Trochlea # Radial head
MANAGEMENT OF INTRAARTICULAR FRACTURES OF ELBOW JOINT By Dr B. Anudeep M. S. orthopaedics Final yr pg INTRAARTICULAR FRACTURES Intercondyar fracture Elbow dislocation Capitellum # Trochlea # Radial head
Recurrent subluxation or dislocation after surgical
 )263( COPYRIGHT 2017 BY THE ARCHIVES OF BONE AND JOINT SURGERY CASE REPORT Persistent Medial Subluxation of the Ulna with Radiotrochlear Articulation Amir R. Kachooei, MD; David Ring, MD, PhD Research
)263( COPYRIGHT 2017 BY THE ARCHIVES OF BONE AND JOINT SURGERY CASE REPORT Persistent Medial Subluxation of the Ulna with Radiotrochlear Articulation Amir R. Kachooei, MD; David Ring, MD, PhD Research
Elbow. Chapter 2 LISTEN. Mechanism of Injury (If Applicable) Pain
 Pain") Preface The first decade of the twenty-first century has witnessed the continuation of an explosion in our knowledge and understanding of all aspects of disease. Accompanying this has been the increasing
Preface The first decade of the twenty-first century has witnessed the continuation of an explosion in our knowledge and understanding of all aspects of disease. Accompanying this has been the increasing
Debridement arthroplasty for osteoarthritis of the elbow (Outerbridge-Kashiwagi procedure)
") Acta Orthop. Belg., 2004, 70, 306-310 ORIGINAL STUDIES Debridement arthroplasty for osteoarthritis of the elbow (Outerbridge-Kashiwagi procedure) Bart VINGERHOEDS, Ilse DEGREEF, Luc DE SMET From the University
Acta Orthop. Belg., 2004, 70, 306-310 ORIGINAL STUDIES Debridement arthroplasty for osteoarthritis of the elbow (Outerbridge-Kashiwagi procedure) Bart VINGERHOEDS, Ilse DEGREEF, Luc DE SMET From the University
Slide 1. Slide 2. Slide 3. The Thrower s Elbow: When to Operate. Medial Elbow Pain in the Athlete. Goal of This Talk
 Slide 1 The Thrower s Elbow: When to Operate Luke S. Oh, MD Massachusetts General Hospital Team Physician, Boston Red Sox Team Physician, New England Revolution Consultant, Harvard University Athletics
Slide 1 The Thrower s Elbow: When to Operate Luke S. Oh, MD Massachusetts General Hospital Team Physician, Boston Red Sox Team Physician, New England Revolution Consultant, Harvard University Athletics
Case Report Intra-Articular Entrapment of the Medial Epicondyle following a Traumatic Fracture Dislocation of the Elbow in an Adult
 Hindawi Case Reports in Orthopedics Volume 2018, Article ID 5401634, 6 pages https://doi.org/10.1155/2018/5401634 Case Report Intra-Articular Entrapment of the Medial Epicondyle following a Traumatic Fracture
Hindawi Case Reports in Orthopedics Volume 2018, Article ID 5401634, 6 pages https://doi.org/10.1155/2018/5401634 Case Report Intra-Articular Entrapment of the Medial Epicondyle following a Traumatic Fracture
Long-term sequel of posterolateral rotatory instability of the elbow: a case report
 CASE REPORT Open Access Long-term sequel of posterolateral rotatory instability of the elbow: a case report Chun-Ying Cheng * Abstract The natural course of untreated posterior lateral rotatory instability
CASE REPORT Open Access Long-term sequel of posterolateral rotatory instability of the elbow: a case report Chun-Ying Cheng * Abstract The natural course of untreated posterior lateral rotatory instability
Arthroscopic Treatment of Posttraumatic
 Arthroscopic Treatment of Posttraumatic Elbow Pain and Stiffness* Laura A. Timmerman, MD, and James R. Andrews, MD From the American Sports Medicine Institute, Birmingham, Alabama ABSTRACT Nineteen consecutive
Arthroscopic Treatment of Posttraumatic Elbow Pain and Stiffness* Laura A. Timmerman, MD, and James R. Andrews, MD From the American Sports Medicine Institute, Birmingham, Alabama ABSTRACT Nineteen consecutive
Management of Chronic Elbow Pain
 Mr. Nashat Siddiqui Consultant Upper Limb Orthopaedic Surgeon Management of Chronic Elbow Pain Patients presenting with elbow pain can pose a diagnostic challenge, especially if there is no obvious recent
Mr. Nashat Siddiqui Consultant Upper Limb Orthopaedic Surgeon Management of Chronic Elbow Pain Patients presenting with elbow pain can pose a diagnostic challenge, especially if there is no obvious recent
OCCUPATIONAL INJURIES OF THE ELBOW
 PLEASE STAND BY WEBINAR WILL BEGIN AT 12:00 PM PST FOR AUDIO: CALL 866-740-1260 / ACCESS CODE: 764-4915# JAMES VAN DEN BOGAERDE, MD OCCUPATIONAL INJURIES OF THE ELBOW Conflict of Interest Disclosure I,
PLEASE STAND BY WEBINAR WILL BEGIN AT 12:00 PM PST FOR AUDIO: CALL 866-740-1260 / ACCESS CODE: 764-4915# JAMES VAN DEN BOGAERDE, MD OCCUPATIONAL INJURIES OF THE ELBOW Conflict of Interest Disclosure I,
Elbow Anatomy, Growth and Physical Exam. Donna M. Pacicca, MD Section of Sports Medicine Division of Orthopaedic Surgery Children s Mercy Hospital
 Elbow Anatomy, Growth and Physical Exam Donna M. Pacicca, MD Section of Sports Medicine Division of Orthopaedic Surgery Children s Mercy Hospital Contributing Factors to Elbow Injury The elbow is affected
Elbow Anatomy, Growth and Physical Exam Donna M. Pacicca, MD Section of Sports Medicine Division of Orthopaedic Surgery Children s Mercy Hospital Contributing Factors to Elbow Injury The elbow is affected
Case Report Intra-Articular Osteotomy for Distal Humerus Malunion
 Volume 2009, Article ID 631306, 4 pages doi:10.1155/2009/631306 Case Report Intra-Articular Osteotomy for Distal Humerus Malunion RenéK.Marti 1 and Job Doornberg 2 1 Department of Orthopaedic Surgery,
Volume 2009, Article ID 631306, 4 pages doi:10.1155/2009/631306 Case Report Intra-Articular Osteotomy for Distal Humerus Malunion RenéK.Marti 1 and Job Doornberg 2 1 Department of Orthopaedic Surgery,
Case Report Combined Isolated Laugier s Fracture and Distal Radial Fracture: Management and Literature Review on the Mechanism of Injury
 Case Reports in Orthopedics Volume 2016, Article ID 7631425, 6 pages http://dx.doi.org/10.1155/2016/7631425 Case Report Combined Isolated Laugier s Fracture and Distal Radial Fracture: Management and Literature
Case Reports in Orthopedics Volume 2016, Article ID 7631425, 6 pages http://dx.doi.org/10.1155/2016/7631425 Case Report Combined Isolated Laugier s Fracture and Distal Radial Fracture: Management and Literature
Common Elbow Problems
 Common Elbow Problems Duncan Ferguson FRACS Knee and Shoulder Specialist Elbow Instability Common 10-25% of elbow injuries Median age 30 yrs Most simple dislocations are stable after reduction recurrence
Common Elbow Problems Duncan Ferguson FRACS Knee and Shoulder Specialist Elbow Instability Common 10-25% of elbow injuries Median age 30 yrs Most simple dislocations are stable after reduction recurrence
Posterolateral elbow dislocation with entrapment of the medial epicondyle in children: a case report Juan Rodríguez Martín* and Juan Pretell Mazzini
 Open Access Case report Posterolateral elbow dislocation with entrapment of the medial epicondyle in children: a case report Juan Rodríguez Martín* and Juan Pretell Mazzini Address: Department of Orthopaedic
Open Access Case report Posterolateral elbow dislocation with entrapment of the medial epicondyle in children: a case report Juan Rodríguez Martín* and Juan Pretell Mazzini Address: Department of Orthopaedic
Bipolar Radial Head System
 Bipolar Radial Head System Katalyst Surgical Technique DESCRIPTION The Katalyst Telescoping Bipolar Radial Head implant restores the support and bearing surface of the radial head in the face of fracture,
Bipolar Radial Head System Katalyst Surgical Technique DESCRIPTION The Katalyst Telescoping Bipolar Radial Head implant restores the support and bearing surface of the radial head in the face of fracture,
Case Report Medial Radial Head Dislocation Associated with a Proximal Olecranon Fracture: A Bado Type V?
 Case Reports in Surgery, Article ID 723756, 4 pages http://dx.doi.org/10.1155/2014/723756 Case Report Medial Radial Head Dislocation Associated with a Proximal Olecranon Fracture: A Bado Type V? Neil Segaren,
Case Reports in Surgery, Article ID 723756, 4 pages http://dx.doi.org/10.1155/2014/723756 Case Report Medial Radial Head Dislocation Associated with a Proximal Olecranon Fracture: A Bado Type V? Neil Segaren,
Case Report Elbow Arthroscopy: Review of the Literature and Case Reports
 Hindawi Publishing Corporation Case Reports in Orthopedics Volume 2012, Article ID 478214, 5 pages doi:10.1155/2012/478214 Case Report Elbow Arthroscopy: Review of the Literature and Case Reports Prakash
Hindawi Publishing Corporation Case Reports in Orthopedics Volume 2012, Article ID 478214, 5 pages doi:10.1155/2012/478214 Case Report Elbow Arthroscopy: Review of the Literature and Case Reports Prakash
Ankle Replacement Surgery
 Ankle Replacement Surgery Ankle replacement surgery is performed to replace the damaged articular surfaces of the three bones of the ankle joint with artificial implants. This procedure is now being preferred
Ankle Replacement Surgery Ankle replacement surgery is performed to replace the damaged articular surfaces of the three bones of the ankle joint with artificial implants. This procedure is now being preferred
Elbow Elbow Anatomy. Flexion extension. Pronation Supination. Anatomy. Anatomy. Romina Astifidis, MS., PT., CHT
 Elbow Elbow Anatomy Romina Astifidis, MS., PT., CHT Curtis National Hand Center Baltimore, MD October 6-8, 2017 Link between the arm and forearm to position the hand in space Not just a hinge Elbow = 70%
Elbow Elbow Anatomy Romina Astifidis, MS., PT., CHT Curtis National Hand Center Baltimore, MD October 6-8, 2017 Link between the arm and forearm to position the hand in space Not just a hinge Elbow = 70%
Case Report Bone Resection for Isolated Ulnar Head Fracture
 Hindawi Case Reports in Orthopedics Volume 2017, Article ID 3519146, 4 pages https://doi.org/10.1155/2017/3519146 Case Report Bone Resection for Isolated Ulnar Head Fracture Hiromasa Akino, Shunpei Hama,
Hindawi Case Reports in Orthopedics Volume 2017, Article ID 3519146, 4 pages https://doi.org/10.1155/2017/3519146 Case Report Bone Resection for Isolated Ulnar Head Fracture Hiromasa Akino, Shunpei Hama,
Management of arthritis of the shoulder. Omar Haddo Consultant Orthopaedic Surgeon
 Management of arthritis of the shoulder Omar Haddo Consultant Orthopaedic Surgeon Diagnosis Pain - with activity initially. As disease progresses night pain is common and sleep difficult Stiffness trouble
Management of arthritis of the shoulder Omar Haddo Consultant Orthopaedic Surgeon Diagnosis Pain - with activity initially. As disease progresses night pain is common and sleep difficult Stiffness trouble
Fractures and dislocations around elbow in adult
 Lec: 3 Fractures and dislocations around elbow in adult These include fractures of distal humerus, fracture of the capitulum, fracture of the radial head, fracture of the olecranon & dislocation of the
Lec: 3 Fractures and dislocations around elbow in adult These include fractures of distal humerus, fracture of the capitulum, fracture of the radial head, fracture of the olecranon & dislocation of the
I (and/or my co-authors) have something to disclose.
 have something to disclose.") Elbow Anatomy And Biomechanics Nikhil N Verma, MD Director, Division of Sports Medicine Professor, Department of Orthopedics Rush University Medical Center Team Physician, Chicago White Sox and Bulls I
Elbow Anatomy And Biomechanics Nikhil N Verma, MD Director, Division of Sports Medicine Professor, Department of Orthopedics Rush University Medical Center Team Physician, Chicago White Sox and Bulls I
Proximal radioulnar translocation associated with elbow dislocation and radial neck fracture in child: a case report and review of literature
 DOI 10.1007/s00402-013-1820-8 TRAUMA SURGERY Proximal radioulnar translocation associated with elbow dislocation and radial neck fracture in child: a case report and review of literature Hong Kee Yoon
DOI 10.1007/s00402-013-1820-8 TRAUMA SURGERY Proximal radioulnar translocation associated with elbow dislocation and radial neck fracture in child: a case report and review of literature Hong Kee Yoon
Shoulder and Elbow ORTHOPAEDIC SYPMPOSIUM APRIL 8, 2017 DANIEL DOTY MD
 Shoulder and Elbow ORTHOPAEDIC SYPMPOSIUM APRIL 8, 2017 DANIEL DOTY MD Shoulder Articulations Glenohumeral Joint 2/3 total arc of motion Shallow Ball and Socket Joint Allows for excellent ROM Requires
Shoulder and Elbow ORTHOPAEDIC SYPMPOSIUM APRIL 8, 2017 DANIEL DOTY MD Shoulder Articulations Glenohumeral Joint 2/3 total arc of motion Shallow Ball and Socket Joint Allows for excellent ROM Requires
Sports Medicine Unit 16 Elbow
 Sports Medicine Unit 16 Elbow I. Bones a. b. c. II. What movements does the elbow perform? a. Flexion b. c. Pronation d. III. Muscles in motion a. FLEXION (supinated) i Brachialis (pronated) ii (neutral)
Sports Medicine Unit 16 Elbow I. Bones a. b. c. II. What movements does the elbow perform? a. Flexion b. c. Pronation d. III. Muscles in motion a. FLEXION (supinated) i Brachialis (pronated) ii (neutral)
Open surgical treatment of post-traumatic elbow contractures in adolescent patients
 Open surgical treatment of post-traumatic elbow contractures in adolescent patients Nickolaos A. Darlis, MD, Robert W. Kaufmann, MD, Dean G. Sotereanos, MD, Pittsburgh, PA The results of surgical treatment
Open surgical treatment of post-traumatic elbow contractures in adolescent patients Nickolaos A. Darlis, MD, Robert W. Kaufmann, MD, Dean G. Sotereanos, MD, Pittsburgh, PA The results of surgical treatment
Integra. Katalyst Bipolar Radial Head System SURGICAL TECHNIQUE
 Integra Katalyst Bipolar Radial Head System SURGICAL TECHNIQUE Surgical Technique As the manufacturer of this device, Integra does not practice medicine and does not recommend this or any other surgical
Integra Katalyst Bipolar Radial Head System SURGICAL TECHNIQUE Surgical Technique As the manufacturer of this device, Integra does not practice medicine and does not recommend this or any other surgical
Case Report Bilateral Distal Femoral Nailing in a Rare Symmetrical Periprosthetic Knee Fracture
 Case Reports in Orthopedics, Article ID 745083, 4 pages http://dx.doi.org/10.1155/2014/745083 Case Report Bilateral Distal Femoral Nailing in a Rare Symmetrical Periprosthetic Knee Fracture Marcos Carvalho,
Case Reports in Orthopedics, Article ID 745083, 4 pages http://dx.doi.org/10.1155/2014/745083 Case Report Bilateral Distal Femoral Nailing in a Rare Symmetrical Periprosthetic Knee Fracture Marcos Carvalho,
Elbow dislocations represent 10% to 25% of all injuries. Elbow Fracture-Dislocations. The Role of Hinged External Fixation
 33 Elbow Fracture-Dislocations The Role of Hinged External Fixation Nader Paksima, D.O., M.P.H., and Anand Panchal, B.S. Abstract Fracture-dislocations of the elbow remain a complex problem in orthopaedics.
33 Elbow Fracture-Dislocations The Role of Hinged External Fixation Nader Paksima, D.O., M.P.H., and Anand Panchal, B.S. Abstract Fracture-dislocations of the elbow remain a complex problem in orthopaedics.
Hand and wrist emergencies
 Chapter1 Hand and wrist emergencies Carl A. Germann Distal radius and ulnar injuries PEARL: Fractures of the distal radius and ulna are the most common type of fractures in patients younger than 75 years.
Chapter1 Hand and wrist emergencies Carl A. Germann Distal radius and ulnar injuries PEARL: Fractures of the distal radius and ulna are the most common type of fractures in patients younger than 75 years.
Open versus Arthroscopic Treatment of Post-Traumatic Stiff Elbow
 Open Journal of Orthopedics, 2014, 4, 304-312 Published Online November 2014 in SciRes. http://www.scirp.org/journal/ojo http://dx.doi.org/10.4236/ojo.2014.411047 Open versus Arthroscopic Treatment of
Open Journal of Orthopedics, 2014, 4, 304-312 Published Online November 2014 in SciRes. http://www.scirp.org/journal/ojo http://dx.doi.org/10.4236/ojo.2014.411047 Open versus Arthroscopic Treatment of
Case Report An Undescribed Monteggia Type 3 Equivalent Lesion: Lateral Dislocation of Radial Head with Both-Bone Forearm Fracture
 Case Reports in Orthopedics Volume 2016, Article ID 8598139, 5 pages http://dx.doi.org/10.1155/2016/8598139 Case Report An Undescribed Monteggia Type 3 Equivalent Lesion: Lateral Dislocation of Radial
Case Reports in Orthopedics Volume 2016, Article ID 8598139, 5 pages http://dx.doi.org/10.1155/2016/8598139 Case Report An Undescribed Monteggia Type 3 Equivalent Lesion: Lateral Dislocation of Radial
Contracture of the elbow is a common problem
 24 The Stiff Elbow Mitchell T. Keschner, M.D., and Nader Paksima, D.O., M.P.H. Contracture of the elbow is a common problem that can be associated with significant morbidity. Elbow contractures may be
24 The Stiff Elbow Mitchell T. Keschner, M.D., and Nader Paksima, D.O., M.P.H. Contracture of the elbow is a common problem that can be associated with significant morbidity. Elbow contractures may be
Other Elbow Concerns in Overhead Athletes
 Other Elbow Concerns in Overhead Athletes John A. Steubs, M.D. Team Physician, Minnesota Twins TRIA Orthopaedic Center Disclosures None relevant to this presentation. Other Elbow Problems Valgus extension
Other Elbow Concerns in Overhead Athletes John A. Steubs, M.D. Team Physician, Minnesota Twins TRIA Orthopaedic Center Disclosures None relevant to this presentation. Other Elbow Problems Valgus extension
Adam J. Seidl, MD Assistant Professor University of Colorado School of Medicine Shoulder & Elbow Surgery Division of Sports Medicine and Shoulder
 Adam J. Seidl, MD Assistant Professor University of Colorado School of Medicine Shoulder & Elbow Surgery Division of Sports Medicine and Shoulder Surgery Division of Hand, Wrist, and Elbow Surgery Anatomy
Adam J. Seidl, MD Assistant Professor University of Colorado School of Medicine Shoulder & Elbow Surgery Division of Sports Medicine and Shoulder Surgery Division of Hand, Wrist, and Elbow Surgery Anatomy
Case Report A Case of Nonunion Avulsion Fracture of the Anterior Tibial Eminence
 Case Reports in Orthopedics Volume 2016, Article ID 9648473, 5 pages http://dx.doi.org/10.1155/2016/9648473 Case Report A Case of Nonunion Avulsion Fracture of the Anterior Tibial Eminence Satoru Atsumi,
Case Reports in Orthopedics Volume 2016, Article ID 9648473, 5 pages http://dx.doi.org/10.1155/2016/9648473 Case Report A Case of Nonunion Avulsion Fracture of the Anterior Tibial Eminence Satoru Atsumi,
D Degenerative joint disease, rotator cuff deficiency with, 149 Deltopectoral approach component removal with, 128
 Index A Abduction exercise, outpatient with, 193, 194 Acromioclavicular arthritis, with, 80 Acromiohumeral articulation, with, 149 Acromio-humeral interval (AHI), physical examination with, 9, 10 Active
Index A Abduction exercise, outpatient with, 193, 194 Acromioclavicular arthritis, with, 80 Acromiohumeral articulation, with, 149 Acromio-humeral interval (AHI), physical examination with, 9, 10 Active
The Elbow Scanning Protocol
 The Elbow Scanning Protocol Diagnostic Imaging of the Elbow: Introduction The elbow maybe considered as consisting of four quadrants, anterior, medial, lateral and posterior. Ultrasound would normally
The Elbow Scanning Protocol Diagnostic Imaging of the Elbow: Introduction The elbow maybe considered as consisting of four quadrants, anterior, medial, lateral and posterior. Ultrasound would normally
Kanji Mori, Kazuya Nishizawa, Akira Nakamura, and Shinji Imai. 1. Introduction. 2. Case Presentation
 Case Reports in Orthopedics Volume 2015, Article ID 301858, 4 pages http://dx.doi.org/10.1155/2015/301858 Case Report Atraumatic Occult Odontoid Fracture in Patients with Osteoporosis-Associated Thoracic
Case Reports in Orthopedics Volume 2015, Article ID 301858, 4 pages http://dx.doi.org/10.1155/2015/301858 Case Report Atraumatic Occult Odontoid Fracture in Patients with Osteoporosis-Associated Thoracic
Nearly all of these fractures are displaced, given the paucity of soft tissue attachments.
 CAPITELLAR FRACTURE Vasu Pai Nearly all of these fractures are displaced, given the paucity of soft tissue attachments. Nonsurgical management is fraught with complications including chronic pain, mechanical
CAPITELLAR FRACTURE Vasu Pai Nearly all of these fractures are displaced, given the paucity of soft tissue attachments. Nonsurgical management is fraught with complications including chronic pain, mechanical
Case Presentation: Comminuted Fractures of the Proximal Ulna 11/28/2017. Disclosures. Surgical Strategy. Implant Choice. Melvin P.
 Current Solutions in Orthopaedic Trauma Case Presentation: Comminuted Fracture of the Proximal Ulna Melvin P. Rosenwasser, MD Robert E. Carroll Professor of Surgery of the Hand Chief, Orthopaedic Hand
Current Solutions in Orthopaedic Trauma Case Presentation: Comminuted Fracture of the Proximal Ulna Melvin P. Rosenwasser, MD Robert E. Carroll Professor of Surgery of the Hand Chief, Orthopaedic Hand
Case Report Combined Posterior and Anterior Ankle Arthroscopy
 Case Reports in Orthopedics Volume 2012, Article ID 693124, 4 pages doi:10.1155/2012/693124 Case Report Combined Posterior and Anterior Ankle Arthroscopy Peter E. Scholten 1, 2 andc.niekvandijk 2 1 Department
Case Reports in Orthopedics Volume 2012, Article ID 693124, 4 pages doi:10.1155/2012/693124 Case Report Combined Posterior and Anterior Ankle Arthroscopy Peter E. Scholten 1, 2 andc.niekvandijk 2 1 Department
FAI syndrome with or without labral tear.
 Case This 16-year-old female, soccer athlete was treated for pain in the right groin previously. Now has acute onset of pain in the left hip. The pain was in the groin that was worse with activities. Diagnosis
Case This 16-year-old female, soccer athlete was treated for pain in the right groin previously. Now has acute onset of pain in the left hip. The pain was in the groin that was worse with activities. Diagnosis
Terrible triad of the elbow
 Terrible triad of the elbow Vasu Pai ? Terrible triad of the elbow" Posterior dislocation of the elbow + Fractures of the radial head + Fracture of coronoid process Uncommon injury 5% of dislocation Problems
Terrible triad of the elbow Vasu Pai ? Terrible triad of the elbow" Posterior dislocation of the elbow + Fractures of the radial head + Fracture of coronoid process Uncommon injury 5% of dislocation Problems
Orthopaedic and Spine Institute 21 Spurs Lane, Suite 245, San Antonio, TX Tel#
 Orthopaedic and Spine Institute 21 Spurs Lane, Suite 245, San Antonio, TX 78240 www.saspine.com Tel# 210-487-7463 PATIENT GUIDE TO SHOULDER INSTABILITY LABRAL (BANKART) REPAIR / CAPSULAR SHIFT WHAT IS
Orthopaedic and Spine Institute 21 Spurs Lane, Suite 245, San Antonio, TX 78240 www.saspine.com Tel# 210-487-7463 PATIENT GUIDE TO SHOULDER INSTABILITY LABRAL (BANKART) REPAIR / CAPSULAR SHIFT WHAT IS
Surgical Complications
 Surgical Complications Complications are common even with ideal management. Recently, Bashyal performed a retrospective review of 622 patients treated for supracondylar fractures and evaluated the complications
Surgical Complications Complications are common even with ideal management. Recently, Bashyal performed a retrospective review of 622 patients treated for supracondylar fractures and evaluated the complications
Anterior Elbow Capsulodesis
 7(1):72 76, 2006 m R E V I E W m Anterior Elbow Capsulodesis Donald H. Lee, MD, Douglas R. Weikert, and Jeffry T. Watson Department of Orthopaedic Surgery Vanderbilt Orthopaedic Institute Nashville, TN
7(1):72 76, 2006 m R E V I E W m Anterior Elbow Capsulodesis Donald H. Lee, MD, Douglas R. Weikert, and Jeffry T. Watson Department of Orthopaedic Surgery Vanderbilt Orthopaedic Institute Nashville, TN
Case Report Multiple Giant Cell Tumors of Tendon Sheath Found within a Single Digit of a 9-Year-Old
 Case Reports in Orthopedics Volume 2016, Article ID 1834740, 4 pages http://dx.doi.org/10.1155/2016/1834740 Case Report Multiple Giant Cell Tumors of Tendon Sheath Found within a Single Digit of a 9-Year-Old
Case Reports in Orthopedics Volume 2016, Article ID 1834740, 4 pages http://dx.doi.org/10.1155/2016/1834740 Case Report Multiple Giant Cell Tumors of Tendon Sheath Found within a Single Digit of a 9-Year-Old
Disclaimer. Evaluation & Treatment of Shoulder and Elbow Pain in the Adult Patient. Objectives. Anatomy
 Evaluation & Treatment of Shoulder and Elbow Pain in the Adult Patient William T. Crowe, RN-C, FNP, MSN, MBA Disclaimer! I, William T Crowe, have relevant financial relationships to be discussed, directly
Evaluation & Treatment of Shoulder and Elbow Pain in the Adult Patient William T. Crowe, RN-C, FNP, MSN, MBA Disclaimer! I, William T Crowe, have relevant financial relationships to be discussed, directly
Functional Anatomy of the Elbow
 Functional Anatomy of the Elbow Orthopedic Institute Daryl C. Osbahr, M.D. Chief of Sports Medicine, Orlando Health Chief Medical Officer, Orlando City Soccer Club Orthopedic Consultant, Washington Nationals
Functional Anatomy of the Elbow Orthopedic Institute Daryl C. Osbahr, M.D. Chief of Sports Medicine, Orlando Health Chief Medical Officer, Orlando City Soccer Club Orthopedic Consultant, Washington Nationals
Elbow Fractures ORIF VS Arthroplasty
 Elbow Fractures ORIF VS Arthroplasty Oke Anakwenze, M.D. Olympus Orthopedics No disclosures Disclosures Distal humerus fractures 0.5-0.7% of all fractures 30% of all elbow fractures Bimodal etiology Young
Elbow Fractures ORIF VS Arthroplasty Oke Anakwenze, M.D. Olympus Orthopedics No disclosures Disclosures Distal humerus fractures 0.5-0.7% of all fractures 30% of all elbow fractures Bimodal etiology Young
Clinical Study Rate of Improvement following Volar Plate Open Reduction and Internal Fixation of Distal Radius Fractures
 SAGE-Hindawi Access to Research Advances in Orthopedics Volume 2011, Article ID 565642, 4 pages doi:10.4061/2011/565642 Clinical Study Rate of Improvement following Volar Plate Open Reduction and Internal
SAGE-Hindawi Access to Research Advances in Orthopedics Volume 2011, Article ID 565642, 4 pages doi:10.4061/2011/565642 Clinical Study Rate of Improvement following Volar Plate Open Reduction and Internal
Elbow arthroscopy has become a commonly practiced
 Technical Note The Joint Jack: Report of a New Technique Essential for Elbow Arthroscopy Ronald M. Selby, M.D., Stephen J. O Brien, M.D., Anne M. Kelly, M.D., and Mark Drakos Abstract: Visualization and
Technical Note The Joint Jack: Report of a New Technique Essential for Elbow Arthroscopy Ronald M. Selby, M.D., Stephen J. O Brien, M.D., Anne M. Kelly, M.D., and Mark Drakos Abstract: Visualization and
A Patient s Guide to Elbow Dislocation
 A Patient s Guide to Elbow Dislocation 2 Introduction When the joint surfaces of an elbow are forced apart, the elbow is dislocated. The elbow is the second most commonly dislocated joint in adults (after
A Patient s Guide to Elbow Dislocation 2 Introduction When the joint surfaces of an elbow are forced apart, the elbow is dislocated. The elbow is the second most commonly dislocated joint in adults (after
Arthroscopy of the Stiff Elbow
 Techniques in Orthopaedics 21(4):331 339 2006 Lippincott Williams & Wilkins, Inc. Arthroscopy of the Stiff Elbow John P. Peden, M.D.* and Felix H. Savoie, III, M.D. Summary: The pathology of elbow stiffness
Techniques in Orthopaedics 21(4):331 339 2006 Lippincott Williams & Wilkins, Inc. Arthroscopy of the Stiff Elbow John P. Peden, M.D.* and Felix H. Savoie, III, M.D. Summary: The pathology of elbow stiffness
Case Report Double-Layered Lateral Meniscus in an 8-Year-Old Child: Report of a Rare Case
 Case Reports in Orthopedics Volume 2016, Article ID 5263248, 4 pages http://dx.doi.org/10.1155/2016/5263248 Case Report Double-Layered Lateral Meniscus in an 8-Year-Old Child: Report of a Rare Case Susumu
Case Reports in Orthopedics Volume 2016, Article ID 5263248, 4 pages http://dx.doi.org/10.1155/2016/5263248 Case Report Double-Layered Lateral Meniscus in an 8-Year-Old Child: Report of a Rare Case Susumu
Other Upper Extremity Trauma. Inje University Sanggye Paik Hospital Yong-Woon Shin
 Other Upper Extremity Trauma Inje University Sanggye Paik Hospital Yong-Woon Shin Forearm Fractures Forearm fractures - the most common orthopaedic injuries in children - 30-50% of all pediatric fractures
Other Upper Extremity Trauma Inje University Sanggye Paik Hospital Yong-Woon Shin Forearm Fractures Forearm fractures - the most common orthopaedic injuries in children - 30-50% of all pediatric fractures
Arthritis of the Shoulder
 Arthritis of the Shoulder Simply defined, arthritis is inflammation of one or more of your joints. In a diseased shoulder, inflammation causes pain and stiffness. Although there is no cure for arthritis
Arthritis of the Shoulder Simply defined, arthritis is inflammation of one or more of your joints. In a diseased shoulder, inflammation causes pain and stiffness. Although there is no cure for arthritis
WHAT YOU IS BACK WITHIN ARM S REACH
 YOUR TOTAL SHOULDER REPLACEMENT SURGERY STEPS TO RETURNING TO A LIFESTYLE YOU DESERVE WHAT YOU IS BACK WITHIN ARM S REACH Nathan Richardson, MD Orthopedics, Shoulder & Elbow Surgeon Board Certified in
YOUR TOTAL SHOULDER REPLACEMENT SURGERY STEPS TO RETURNING TO A LIFESTYLE YOU DESERVE WHAT YOU IS BACK WITHIN ARM S REACH Nathan Richardson, MD Orthopedics, Shoulder & Elbow Surgeon Board Certified in
Joints of the upper limb II
 Joints of the upper limb II Prof. Abdulameer Al-Nuaimi E-mail: a.al-nuaimi@sheffield.ac.uk E. mail: abdulameerh@yahoo.com Elbow joint The elbow joint is connecting the upper arm to the forearm. It is classed
Joints of the upper limb II Prof. Abdulameer Al-Nuaimi E-mail: a.al-nuaimi@sheffield.ac.uk E. mail: abdulameerh@yahoo.com Elbow joint The elbow joint is connecting the upper arm to the forearm. It is classed
Nursing Management: Musculoskeletal Trauma and Orthopedic Surgery. By: Aun Lauriz E. Macuja SAC_SN4
 Nursing Management: Musculoskeletal Trauma and Orthopedic Surgery By: Aun Lauriz E. Macuja SAC_SN4 The most common cause of musculoskeletal injuries is a traumatic event resulting in fracture, dislocation,
Nursing Management: Musculoskeletal Trauma and Orthopedic Surgery By: Aun Lauriz E. Macuja SAC_SN4 The most common cause of musculoskeletal injuries is a traumatic event resulting in fracture, dislocation,
Research Article Relationship between Pain and Medial Meniscal Extrusion in Knee Osteoarthritis
 Advances in Orthopedics Volume 2015, Article ID 210972, 4 pages http://dx.doi.org/10.1155/2015/210972 Research Article Relationship between Pain and Medial Meniscal Extrusion in Knee Osteoarthritis Hiroaki
Advances in Orthopedics Volume 2015, Article ID 210972, 4 pages http://dx.doi.org/10.1155/2015/210972 Research Article Relationship between Pain and Medial Meniscal Extrusion in Knee Osteoarthritis Hiroaki
E ORIGINAL ARTICLE Elbow dislocation and articular fracture of the distal humerus
 Shoulder & Elbow. ISSN 1758-5732 E ORIGINAL ARTICLE Elbow dislocation and articular fracture of the distal humerus Thierry G. Guitton,AndrewD.Duckworth, Margaret M. McQueen, Peter Kloen &DavidRing Harvard
Shoulder & Elbow. ISSN 1758-5732 E ORIGINAL ARTICLE Elbow dislocation and articular fracture of the distal humerus Thierry G. Guitton,AndrewD.Duckworth, Margaret M. McQueen, Peter Kloen &DavidRing Harvard
UDHT08.1.qxd:UDHT /03/08 17:14 Page 1. Surgical. Technique. Elbow Prosthesis. RHS Radial Head System.
 UDHT08.1.qxd:UDHT08.1 13/03/08 17:14 Page 1 Surgical Technique Elbow Prosthesis RHS Radial Head System www.tornier.com UDHT08.1.qxd:UDHT08.1 13/03/08 17:14 Page 2 TABLE OF CONTENTS DESIGN RATIONALE INDICATIONS
UDHT08.1.qxd:UDHT08.1 13/03/08 17:14 Page 1 Surgical Technique Elbow Prosthesis RHS Radial Head System www.tornier.com UDHT08.1.qxd:UDHT08.1 13/03/08 17:14 Page 2 TABLE OF CONTENTS DESIGN RATIONALE INDICATIONS
Case Report Double-Layered Lateral Meniscus Accompanied by Meniscocapsular Separation
 Case Reports in Orthopedics Volume 2015, Article ID 357463, 5 pages http://dx.doi.org/10.1155/2015/357463 Case Report Double-Layered Lateral Meniscus Accompanied by Meniscocapsular Separation Aki Fukuda,
Case Reports in Orthopedics Volume 2015, Article ID 357463, 5 pages http://dx.doi.org/10.1155/2015/357463 Case Report Double-Layered Lateral Meniscus Accompanied by Meniscocapsular Separation Aki Fukuda,
Ulnar Collateral Ligament Reconstruction in Posttraumatic Elbow Release
 Feature Article Ulnar Collateral Ligament Reconstruction in Posttraumatic Elbow Release KEVIN J. MALONE, MD; PAUL A. MARTINEAU, MD; DOUGLAS P. HANEL, MD abstract Full article available online at ORTHOSuperSite.com.
Feature Article Ulnar Collateral Ligament Reconstruction in Posttraumatic Elbow Release KEVIN J. MALONE, MD; PAUL A. MARTINEAU, MD; DOUGLAS P. HANEL, MD abstract Full article available online at ORTHOSuperSite.com.
A Patient s Guide to Osteoarthritis of the Elbow
 A Patient s Guide to Osteoarthritis of the Elbow 20295 NE 29th Place, Ste 300 Aventura, FL 33180 Phone: (786) 629-0910 Fax: (786) 629-0920 admin@instituteofsports.com DISCLAIMER: The information in this
A Patient s Guide to Osteoarthritis of the Elbow 20295 NE 29th Place, Ste 300 Aventura, FL 33180 Phone: (786) 629-0910 Fax: (786) 629-0920 admin@instituteofsports.com DISCLAIMER: The information in this
Case Report Surgical Treatment of Posttraumatic Radioulnar Synostosis
 Case Reports in Orthopedics Volume 2016, Article ID 5956304, 4 pages http://dx.doi.org/10.1155/2016/5956304 Case Report Surgical Treatment of Posttraumatic Radioulnar Synostosis S. Pfanner, P. Bigazzi,
Case Reports in Orthopedics Volume 2016, Article ID 5956304, 4 pages http://dx.doi.org/10.1155/2016/5956304 Case Report Surgical Treatment of Posttraumatic Radioulnar Synostosis S. Pfanner, P. Bigazzi,
Case Report Reverse Segond Fracture Associated with Anteromedial Tibial Rim and Tibial Attachment of Anterior Cruciate Ligament Avulsion Fractures
 Hindawi Case Reports in Orthopedics Volume 2017, Article ID 9637153, 4 pages https://doi.org/10.1155/2017/9637153 Case Report Reverse Segond Fracture Associated with Anteromedial Tibial Rim and Tibial
Hindawi Case Reports in Orthopedics Volume 2017, Article ID 9637153, 4 pages https://doi.org/10.1155/2017/9637153 Case Report Reverse Segond Fracture Associated with Anteromedial Tibial Rim and Tibial
Clinical Evaluation and Imaging of the Patellofemoral Joint Common clinical syndromes
 Clinical Evaluation and Imaging of the Patellofemoral Joint Common clinical syndromes A. Panagopoulos Lecturer in Orthopaedics Medical School, Patras University Objectives Anatomy of patellofemoral joint
Clinical Evaluation and Imaging of the Patellofemoral Joint Common clinical syndromes A. Panagopoulos Lecturer in Orthopaedics Medical School, Patras University Objectives Anatomy of patellofemoral joint
Radial head fractures; ORIF radial head; radial head arthroplasty; coronoid process fracture; ligament repair Elbow Anatomy Spectrum of injuries
 Radial head fractures; ORIF radial head; radial head arthroplasty; coronoid process fracture; ligament repair This information aims to help you understand your condition and gain maximum benefit from your
Radial head fractures; ORIF radial head; radial head arthroplasty; coronoid process fracture; ligament repair This information aims to help you understand your condition and gain maximum benefit from your
Case Report Unusual Bilateral Rim Fracture in Femoroacetabular Impingement
 Case Reports in Orthopedics Volume 2015, Article ID 210827, 4 pages http://dx.doi.org/10.1155/2015/210827 Case Report Unusual Bilateral Rim Fracture in Femoroacetabular Impingement Claudio Rafols, Juan
Case Reports in Orthopedics Volume 2015, Article ID 210827, 4 pages http://dx.doi.org/10.1155/2015/210827 Case Report Unusual Bilateral Rim Fracture in Femoroacetabular Impingement Claudio Rafols, Juan
ADHESIVE CAPSULITIS (FROZEN SHOULDER)
") ADHESIVE CAPSULITIS (FROZEN SHOULDER) Frozen shoulder, or adhesive capsulitis is a condition that generally begins with the gradual onset of pain followed by a limitation of shoulder motion. The discomfort
ADHESIVE CAPSULITIS (FROZEN SHOULDER) Frozen shoulder, or adhesive capsulitis is a condition that generally begins with the gradual onset of pain followed by a limitation of shoulder motion. The discomfort
Shoulder Joint Replacement
 Shoulder Joint Replacement Although shoulder joint replacement is less common than knee or hip replacement, it is just as successful in relieving joint pain. Shoulder replacement surgery was first performed
Shoulder Joint Replacement Although shoulder joint replacement is less common than knee or hip replacement, it is just as successful in relieving joint pain. Shoulder replacement surgery was first performed
Fumiaki Takase, Atsuyuki Inui, Yutaka Mifune, Tomoyuki Muto, Yoshifumi Harada, Takeshi Kokubu, and Masahiro Kurosaka
 Case Reports in Orthopedics, Article ID 312968, 4 pages http://dx.doi.org/10.1155/2014/312968 Case Report Concurrent Rotator Cuff Tear and Axillary Nerve Palsy Associated with Anterior Dislocation of the
Case Reports in Orthopedics, Article ID 312968, 4 pages http://dx.doi.org/10.1155/2014/312968 Case Report Concurrent Rotator Cuff Tear and Axillary Nerve Palsy Associated with Anterior Dislocation of the
Arthritis of the Shoulder
 Arthritis of the Shoulder In 2011, more than 50 million people in the United States reported that they had been diagnosed with some form of arthritis, according to the National Health Interview Survey.
Arthritis of the Shoulder In 2011, more than 50 million people in the United States reported that they had been diagnosed with some form of arthritis, according to the National Health Interview Survey.
Elbow Joint Anatomy ELBOW ANATOMY, BIOMECHANICS. Bone Anatomy. Bone Anatomy. Property of VOMPTI, LLC
 ELBOW ANATOMY, BIOMECHANICS AND PATHOLOGY Kristin Kelley, DPT, OCS, FAAOMPT Elbow Joint Anatomy Joint articulations Humeroulnar Radiohumeral Radioulnar (proximal and distal) Orthopaedic Manual Physical
ELBOW ANATOMY, BIOMECHANICS AND PATHOLOGY Kristin Kelley, DPT, OCS, FAAOMPT Elbow Joint Anatomy Joint articulations Humeroulnar Radiohumeral Radioulnar (proximal and distal) Orthopaedic Manual Physical
Cubital Tunnel Syndrome
 Disclaimer This movie is an educational resource only and should not be used to manage Orthopaedic Health. All decisions about must be made in conjunction with your Physician or a licensed healthcare provider.
Disclaimer This movie is an educational resource only and should not be used to manage Orthopaedic Health. All decisions about must be made in conjunction with your Physician or a licensed healthcare provider.
Index. orthopedic.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Acetabular fractures pediatric, 494 498 classification of, 494 diagnostic imaging of, 494, 496 497 epidemiology of, 494 treatment of, 494 498
Note: Page numbers of article titles are in boldface type. A Acetabular fractures pediatric, 494 498 classification of, 494 diagnostic imaging of, 494, 496 497 epidemiology of, 494 treatment of, 494 498
Elbow arthroscopy has increased in popularity for
 Arthroscopic Ulnar Nerve Identification During Posterior Elbow Arthroscopy Srinath Kamineni, M.D., F.R.C.S.(Orth), and David Anthony Hamilton Jr., M.D., M.B.A. Abstract: Elbow arthroscopy has increased
Arthroscopic Ulnar Nerve Identification During Posterior Elbow Arthroscopy Srinath Kamineni, M.D., F.R.C.S.(Orth), and David Anthony Hamilton Jr., M.D., M.B.A. Abstract: Elbow arthroscopy has increased
Unstable elbow dislocations: a case report of a new surgical technique
 SICOT J 2016, 2, 15 Ó The Authors, published by EDP Sciences, 2016 DOI: 10.1051/sicotj/2016010 Available online at: www.sicot-j.org CASE REPORT OPEN ACCESS Unstable elbow dislocations: a case report of
SICOT J 2016, 2, 15 Ó The Authors, published by EDP Sciences, 2016 DOI: 10.1051/sicotj/2016010 Available online at: www.sicot-j.org CASE REPORT OPEN ACCESS Unstable elbow dislocations: a case report of
Elbow Pain. Lateral Elbow Pain. Lateral Elbow Pain. tennis elbow lateral epicondylitis extensor tendinopathy
 Elbow Pain Peter Brukner OAM, FACSP Associate Professor in Sports Medicine Centre for Health, Exercise and Sports Medicine University of Melbourne Lateral Elbow Pain tennis elbow lateral epicondylitis
Elbow Pain Peter Brukner OAM, FACSP Associate Professor in Sports Medicine Centre for Health, Exercise and Sports Medicine University of Melbourne Lateral Elbow Pain tennis elbow lateral epicondylitis
The Elbow and the cubital fossa. Prof Oluwadiya Kehinde
 The Elbow and the cubital fossa Prof Oluwadiya Kehinde www.oluwadiya.com Elbow and Forearm Anatomy The elbow joint is formed by the humerus, radius, and the ulna Bony anatomy of the elbow Distal Humerus
The Elbow and the cubital fossa Prof Oluwadiya Kehinde www.oluwadiya.com Elbow and Forearm Anatomy The elbow joint is formed by the humerus, radius, and the ulna Bony anatomy of the elbow Distal Humerus
11/15/2017. Biceps Lesions. Highgate Private Hospital (Whittington Health NHS Trust) E: LHB Anatomy.
 E: LHB Anatomy.") Biceps Lesions Mr Omar Haddo (Consultant Orthopaedic Surgeon MBBS, BmedSci, FRCS(Orth) ) Highgate Private Hospital (Whittington Health NHS Trust) E: admin@denovomedic.co.uk LHB Anatomy Arise from superior
Biceps Lesions Mr Omar Haddo (Consultant Orthopaedic Surgeon MBBS, BmedSci, FRCS(Orth) ) Highgate Private Hospital (Whittington Health NHS Trust) E: admin@denovomedic.co.uk LHB Anatomy Arise from superior
Terrible Triad: Tricks for Dealing with the Unstable Elbow
 Terrible Triad: Tricks for Dealing with the Unstable Elbow Mark A. Mighell, MD Kaitlyn N. Christmas, BS Disclosure Paid Consultation Research Support Speakers Bureau Paid Consultation Speakers Bureau The
Terrible Triad: Tricks for Dealing with the Unstable Elbow Mark A. Mighell, MD Kaitlyn N. Christmas, BS Disclosure Paid Consultation Research Support Speakers Bureau Paid Consultation Speakers Bureau The
The Upper Limb. Elbow Rotation 4/25/18. Dr Peter Friis
 The Upper Limb Dr Peter Friis Elbow Rotation Depending upon the sport, the elbow moves through an arc of approximately 75⁰ to 100⁰ in about 20 to 35 msec. The resultant angular velocity is between 1185
The Upper Limb Dr Peter Friis Elbow Rotation Depending upon the sport, the elbow moves through an arc of approximately 75⁰ to 100⁰ in about 20 to 35 msec. The resultant angular velocity is between 1185
WEEKEND 2 Elbow. Elbow Range of Motion Assessment
 Virginia Orthopedic Manual Physical Therapy Institute - 2016 Technique Manual WEEKEND 2 Elbow Elbow Range of Motion Assessment - Patient Positioning: Sitting or supine towards the edge of the bed - Indications:
Virginia Orthopedic Manual Physical Therapy Institute - 2016 Technique Manual WEEKEND 2 Elbow Elbow Range of Motion Assessment - Patient Positioning: Sitting or supine towards the edge of the bed - Indications:
The posterior Monteggia lesion with associated ulnohumeral instability
 The posterior Monteggia lesion with associated ulnohumeral instability E. J. Strauss, N. C. Tejwani, C. F. Preston, K. A. Egol From the New York Universty Hospital for Joint Diseases, New York, New York,
The posterior Monteggia lesion with associated ulnohumeral instability E. J. Strauss, N. C. Tejwani, C. F. Preston, K. A. Egol From the New York Universty Hospital for Joint Diseases, New York, New York,
P.O. Box Sierra Park Road Mammoth Lakes, CA Orthopedic Surgery & Sports Medicine
 P.O. Box 660 85 Sierra Park Road Mammoth Lakes, CA 93546 SHOULDER: Instability Dislocation Labral Tears The shoulder is the most mobile joint in the body, but to have this amount of motion, it is also
P.O. Box 660 85 Sierra Park Road Mammoth Lakes, CA 93546 SHOULDER: Instability Dislocation Labral Tears The shoulder is the most mobile joint in the body, but to have this amount of motion, it is also