VA/DoD Clinical Practice Guideline for Management of Post Traumatic Stress. Core Module
|
|
|
- Erik Higgins
- 5 years ago
- Views:
Transcription

1 VA/DoD Clinical Practice Guideline for Management of Post Traumatic Stress Core Module

2 Module A Acute Stress Continue Treatment for ASD
3 Treatment for ACUTE Stress Disorder

4 Module B PTSD Continue Treatment PTSD

5 Treatment for PTSD Continue Reassessment and Follow-up
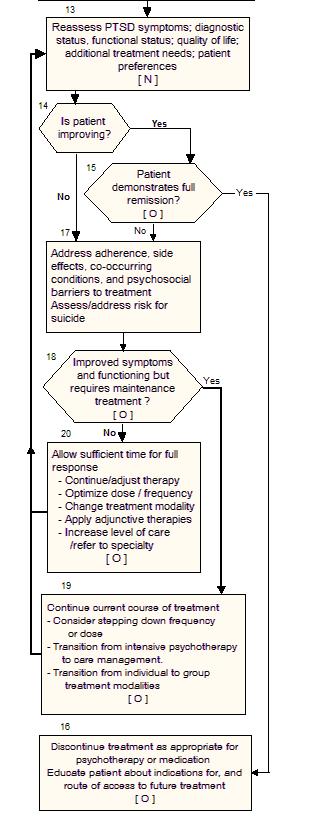
6 Reassessment/Follow-up PTSD
7 Table 1: Common Symptoms After Exposure to Trauma or Loss Physical * Chest pain * Chills * Difficulty breathing * Dizziness * Elevated blood pressure * Fainting * Nausea * Fatigue * Grinding teeth * Headaches * Muscle tremors * Profuse sweating * Rapid heart rate * Shock symptoms * Thirst * Twitches * Visual difficulties * Vomiting * Weakness Cognitive/Mental * Blaming someone * Change in alertness * Confusion * Difficulty identifying familiar objects or people * Hyper-vigilance * Increased or decreased awareness of surroundings * Intrusive images * Loss of orientation to time, place, person * Memory problems * Nightmares * Poor abstract thinking * Poor attention * Poor concentration * Poor decisions * Poor problem solving Emotional * Agitation * Anxiety * Apprehension * Denial * Depression * Emotional shock * Fear * Feeling overwhelmed * Grief * Guilt * Inappropriate emotional response * Irritability * Loss of emotional control * Severe pain * Uncertainty Behavioral * Alcohol consumption * Antisocial acts * Change in activity * Change in communication * Change in sexual functioning * Change in speech pattern * Emotional outbursts * Erratic movements * Hyper-alert to environment * Inability to rest * Loss or increased appetite * Pacing * Somatic complaints * Startle reflex intensified * Suspiciousness * Withdrawal Symptoms Presentation Physical - chronic pain, migraines, or vague somatic complaints Mental - substance abuse, MDD, anxiety, or depression Behavior - irritability, avoidance, anger or non-compliance, self risk behavior (HIV), evokes aversion or fear in provider Change in function
8 Key Elements of Psychological First Aid (PFA) Contact and Engagement - Respond to contacts initiated by affected persons, or initiate contacts in a non-intrusive, compassionate, and helpful manner Safety and Comfort - Enhance immediate and ongoing safety, and provide physical and emotional comfort Stabilization (if needed) - Calm and orient emotionally overwhelmed or distraught survivors Information Gathering - Current Needs and Concerns - Identify immediate needs and concerns, gather additional information, and tailor PFA interventions Practical Assistance - Offer practical help to the survivor in addressing immediate needs and concerns Connection with Social Supports - Help establish opportunities for brief or ongoing contacts with primary support persons or other sources of support, including family members, friends, and community helping resources Information on Coping - Provide information (about stress reactions and coping) to reduce distress and promote adaptive functioning Linkage to Collaborative Services - Link survivors with needed services and inform them about available services that may be needed in the future. Risk Factors for Devloping ASD/PTSD Pre-traumatic factors 1. Onoing life stress 2. Lack of social support 3. Young age at time of trauma 4. Pre-existing psychiatric disorders, or substance misuse 5. History of traumatic events (e.g., MVA) 6. History of post-traumatic stress disorder (PTSD) 7. Other pre-traumatic factors, including: female gender, low socioeconomic status, lower level of education, lower level of intelligence, race (e.g., Hispanic, African-American, American Indian, and Pacific Islander), reported abuse in childhood, report of other previous traumatization, report of other adverse childhood factors, family history of psychiatric disorders, and poor training or preparation for the traumatic event. Peri-traumatic or trauma related factors 1. Severe trauma 2. Physical injury to self or other 3. Type of trauma (combat, interpersonal traumas, such as killing another person, torture, rape, or assault, convey high risk of PTSD) 4. High perceived threat to life of self or others 5. Community (mass) trauma 6. Other peri-traumatic factors, including: history of peri-traumatic dissociation and interpersonal trauma. Post-traumatic factors 1. Ongoing life stress 2. Lack of positive social support 3. Bereavement or traumatic grief 4. Major loss of resources 5. Negative social support (shaming or blaming environment) 6. Poor coping skills 7. Other post-traumatic factors, including: children at home and/or a distressed spouse.
9 Early Interventions after Exposure to Trauma (<4 days after exposure) Balance of Benefit and Harm SR Significant Benefit Some Benefit Unknown Benefit No Benefit Potential Harm I - Psychological First Aid - Psychoeducation and normalization - Social support Spiritual support D Psychological debriefing Early Interventions after Exposure to Trauma (4 to 30 days after exposure) Balance of Benefit and Harm SR Significant Benefit Some Benefit Unknown Benefit No Benefit A - Brief Cognitive Behavioral Therapy (4-5 sessions) C - Social support D - Individual psychological debriefing - Formal psychotherapy for asymptomatic survivors - Benzodiazepines - Typical Antipsychotics I - Psychoeducation and normalization - Imipramine - Propranolol - Prazosin - Other Antidepressants - Group psychological debriefing Anticonvulsants - Atypical Antipsychotics - Spiritual support - Psychological First Aid
10 Psychotherapy Intervention for Treatment of PTSD Balance Benefit and Harm S R Significant Benefit Some Benefit Unknown Benefit - Trauma-focused psychotherapy that includes components of exposure and/or cognitive A restructuring; or, - Stress inoculation training C I Patient Education - Imagery Rehearsal Therapy - Psychodynamic Therapy - Hypnosis - Relaxation Techniques - Group Therapy - Family Therapy - WEB-Based CBT - Acceptance and Commitment Therapy - Dialectical Behavioral Therapy Strongly recommend that patients who are diagnosed with PTSD should be offered one of the evidence-based trauma-focused psychotherapeutic interventions that include components of exposure and/or cognitive restructuring; or stress inoculation training. [A] The choice of a specific approach should be based on the severity of the symptoms, clinician expertise in one or more of these treatment methods and patient preference, and may include : - Exposure-based therapy (e.g., Prolonged Exposure), - Cognitive-based therapy (e.g., Cognitive Processing Therapy), - Stress management therapy (e.g., SIT) or - Eye Movement Desensitization and Reprocessing (EMDR).
11 Pharmacotherapy Interventions for Treatment of PTSD S R A B C D I Significant SSRIs SNRIs Balance of Benefit and Harm Some Benefit Unknown No Benefit - Mirtazapine - Atypical antipsychotics (as adjunct) - Prazosin (for sleep/ nightmares) - TCAs - Nefazodone [Caution] MAOIs (phenelzine) - Prazosin (for global PTSD) - Atypical antipsychotic (monotherapy) - Conventional antipsychotics - Buspirone - Non-benzodiazepine hypnotics - Bupropion - Trazodone (adjunctive) - Gabapentin - Lamotrigine - Propranolol - Clonidine - Benzodiazepines [Harm] - Tiagabine - Guanfacine - Valproate - Topiramate General Recommendations: Risks and benefits of long-term pharmacotherapy should be discussed prior to starting medication and should be a continued discussion item during treatment. Monotherapy therapeutic trial should be optimized before proceeding to subsequent strategies by monitoring outcomes, maximizing dosage (medication or psychotherapy), and allowing sufficient response time (for at least 8 weeks). [C] If there is some response and patient is tolerating the drug, continue for at least another 4 weeks. If the drug is not tolerated, discontinue the current agent and switch to another effective medication. If no improvement is observed at 8 weeks consider: - Increasing the dose of the initial drug to maximum tolerated - Discontinuing the current agent and switching to another effective medication - Augmenting with additional agents. Recommend assessment of adherence, side effects and management to minimize or alleviate adverse effects. Assess for treatment burden (e.g., medication adverse effects, attending appointments) after initiating or changing treatment when the patient is non-adherent to treatment or when the patient is not responding to treatment.
12 PHARAMCOTHERAPY FOR PTSD Monotherapy: Strongly recommend that patients diagnosed with PTSD should be offered selective serotonin reuptake inhibitors (SSRIs), for which fluoxetine, paroxetine, or sertraline have the strongest support, or serotonin norepinephrine reuptake inhibitors (SNRIs), for which venlafaxine has the strongest support, for the treatment of PTSD. [A] Recommend mirtazapine, nefazodone, tricyclic antidepressants (TCAs), amitriptyline and imipramine, or monoamine oxidase inhibitors (phenelzine) for the treatments for PTSD. [B] Recommend against the use of guanfacine, anticonvulsants (tiagabine, topiramate, or valproate) as monotherapy in the management of PTSD. [D] The existing evidence does not support the use of bupropion, buspirone, and trazodone, anticonvulsants (lamotrigine or gabapentin) or atypical antipsychotics as monotherapy in the management of PTSD. [I] There is evidence against the use of benzodiazepines in the management of PTSD. [D] There is insufficient evidence to support the use of prazosin as monotherapy in the management of PTSD. [I] Augmented Therapy for PTSD: Recommend atypical antipsychotics as adjunctive therapy: risperidone or olanzapine [B] or, quetiapine [C]. Recommend adjunctive treatment with prazosin for sleep/nightmares. [B] There is insufficient evidence to recommend a sympatholytic or an anticonvulsant as an adjunctive therapy for the treatment of PTSD. [I] Adjunctive Problem-Focused Method/Services for PTSD If the client and clinician together conclude that the patient with PTSD: 1 Is not fully informed about aspects of health needs and does not avoid high -risk behaviors (e.g., PTSD, substance use) 2 Does not have sufficient self-care and independent living skills 3 Does not have safe, decent, affordable, stable housing that is consistent with treatment goals 4 Does not have a family that is actively supportive and/or knowledgeable about treatment for PTSD Service/Training Provide patient education Refer to self-care/independent living skills training services Use and/or refer to supported housing services Implement family skills training 5 Is not socially active Implement social skills training 6 Does not have a job that provides adequate income and/or fully uses his or her training and skills 7 Is unable to locate and coordinate access to services such as those listed above Implement vocational rehabilitation training Use case management services 8 Does request spiritual support Provide access to religious/ spiritual advisors and/or other resources OTHER CONDITIONS 9 Does have a borderline personality disorder typified by parasuicidal behaviors Consider Dialectical Behavioral Therapy 1 0 Does have concurrent substance abuse problem Integrated PTSD substance abuse treatment (e.g., Seeking Safety)
REMAINING RESILIENT AFTER TRAUMATIC EVENTS
 REMAINING RESILIENT AFTER TRAUMATIC EVENTS www.humanrightsatsea.org A post incident guide for you, your family and friends SUPPORTED BY REMAINING RESILIENT AFTER TRAUMATIC EVENTS A post incident guide
REMAINING RESILIENT AFTER TRAUMATIC EVENTS www.humanrightsatsea.org A post incident guide for you, your family and friends SUPPORTED BY REMAINING RESILIENT AFTER TRAUMATIC EVENTS A post incident guide
Conflict of Interest Slide
 The Trials, Tribulations, and Treatment of PTSD Douglas L Boggs, PharmD., MS, BCPP Douglas.Boggs@yale.edu VISN 1 Academic Detailer Clinical Pharmacy Specialist-Mental Health VA Connecticut Healthcare System
The Trials, Tribulations, and Treatment of PTSD Douglas L Boggs, PharmD., MS, BCPP Douglas.Boggs@yale.edu VISN 1 Academic Detailer Clinical Pharmacy Specialist-Mental Health VA Connecticut Healthcare System
Psychological and Pharmacological Treatments for Adults with Posttraumatic Stress Disorder (PTSD)
") 1 Psychological and Pharmacological Treatments for Adults with Posttraumatic Stress Disorder (PTSD) This continuing education monograph examines the results of a comparative effectiveness review to assess
1 Psychological and Pharmacological Treatments for Adults with Posttraumatic Stress Disorder (PTSD) This continuing education monograph examines the results of a comparative effectiveness review to assess
Implementing the 2010 VA/DoD Clinical Practice Guideline for Post-traumatic Stress: A Guide for Clinic Leaders
 Implementing the 2010 VA/DoD Clinical Practice Guideline for Post-traumatic Stress: A Guide for Clinic Leaders This tool is intended for use in conjunction with other essential resources including: 2010
Implementing the 2010 VA/DoD Clinical Practice Guideline for Post-traumatic Stress: A Guide for Clinic Leaders This tool is intended for use in conjunction with other essential resources including: 2010
Depression: selective serotonin reuptake inhibitors
 Depression: selective serotonin reuptake inhibitors Selective serotonin reuptake inhibitors (SSRIs) are considered first-line treatment for the majority of patients with depression. citalopram and fluoxetine
Depression: selective serotonin reuptake inhibitors Selective serotonin reuptake inhibitors (SSRIs) are considered first-line treatment for the majority of patients with depression. citalopram and fluoxetine
COMMON SIGNS AND SIGNALS OF A STRESS REACTION
 COMMON SIGNS AND SIGNALS OF A STRESS REACTION PHYSICAL SIGNS Fatigue Nausea (upset stomach) Twitches Muscle tremors (lips, hands) Thirst Vomiting Elevated blood pressure Headaches Chills Dizziness Grinding
COMMON SIGNS AND SIGNALS OF A STRESS REACTION PHYSICAL SIGNS Fatigue Nausea (upset stomach) Twitches Muscle tremors (lips, hands) Thirst Vomiting Elevated blood pressure Headaches Chills Dizziness Grinding
Posttraumatic Stress Disorder (PTSD) Marshall E. Cates, Pharm.D., BCPP, FASHP Professor of Pharmacy Practice McWhorter School of Pharmacy
 Marshall E. Cates, Pharm.D., BCPP, FASHP Professor of Pharmacy Practice McWhorter School of Pharmacy") Posttraumatic Stress Disorder (PTSD) Marshall E. Cates, Pharm.D., BCPP, FASHP Professor of Pharmacy Practice McWhorter School of Pharmacy Samford University it Learning Objectives 1. Describe the epidemiology,
Posttraumatic Stress Disorder (PTSD) Marshall E. Cates, Pharm.D., BCPP, FASHP Professor of Pharmacy Practice McWhorter School of Pharmacy Samford University it Learning Objectives 1. Describe the epidemiology,
When to Call our District Critical Incident Stress Management Team. Rev. Dr. William W. Wagner South Wisconsin District Disaster coordinator
 WELCOME When to Call our District Critical Incident Stress Management Team Rev. Dr. William W. Wagner South Wisconsin District Disaster coordinator CISM WHAT IS IT? SWD Compassionate Believers Rev. Dr.
WELCOME When to Call our District Critical Incident Stress Management Team Rev. Dr. William W. Wagner South Wisconsin District Disaster coordinator CISM WHAT IS IT? SWD Compassionate Believers Rev. Dr.
Guidelines MANAGEMENT OF MAJOR DEPRESSIVE DISORDER (MDD)
") MANAGEMENT OF MAJOR DEPRESSIVE DISORDER (MDD) Guidelines CH Lim, B Baizury, on behalf of Development Group Clinical Practice Guidelines Management of Major Depressive Disorder A. Introduction Major depressive
MANAGEMENT OF MAJOR DEPRESSIVE DISORDER (MDD) Guidelines CH Lim, B Baizury, on behalf of Development Group Clinical Practice Guidelines Management of Major Depressive Disorder A. Introduction Major depressive
KEY MESSAGES. It is often under-recognised and 30-50% of MDD cases in primary care and medical settings are not detected.
 KEY MESSAGES Major depressive disorder (MDD) is a significant mental health problem that disrupts a person s mood and affects his psychosocial and occupational functioning. It is often under-recognised
KEY MESSAGES Major depressive disorder (MDD) is a significant mental health problem that disrupts a person s mood and affects his psychosocial and occupational functioning. It is often under-recognised
Charles Schroeder EMS Program Manager NM EMS Bureau
 Charles Schroeder EMS Program Manager NM EMS Bureau Objectives Understand the nature of stress, emotional and psychological distress Understand how it affects people and why Help you to recognize the stressors
Charles Schroeder EMS Program Manager NM EMS Bureau Objectives Understand the nature of stress, emotional and psychological distress Understand how it affects people and why Help you to recognize the stressors
TRAUMA AND STRESSOR RELATED DISORDERS WILBUR DATTILO, MD ASSISTANT PROFESSOR OF PSYCHIATRY UNIVERSITY OF UTAH
 TRAUMA AND STRESSOR RELATED DISORDERS WILBUR DATTILO, MD ASSISTANT PROFESSOR OF PSYCHIATRY UNIVERSITY OF UTAH THE RELATIONSHIP BETWEEN TRAUMA AND PSYCHOPATHOLOGY This has been debated at least since the
TRAUMA AND STRESSOR RELATED DISORDERS WILBUR DATTILO, MD ASSISTANT PROFESSOR OF PSYCHIATRY UNIVERSITY OF UTAH THE RELATIONSHIP BETWEEN TRAUMA AND PSYCHOPATHOLOGY This has been debated at least since the
Panic disorder is a chronic and recurrent illness associated
 CLINICAL PRACTICE GUIDELINES Management of Anxiety Disorders. Panic Disorder, With or Without Agoraphobia Epidemiology Panic disorder is a chronic and recurrent illness associated with significant functional
CLINICAL PRACTICE GUIDELINES Management of Anxiety Disorders. Panic Disorder, With or Without Agoraphobia Epidemiology Panic disorder is a chronic and recurrent illness associated with significant functional
Definition. Objectives. PTSD: The Unrecognized Symptom Jorge I. Ramirez, MD, FAAHPM Caroline Schauer, RN, BSN, CHPN
 PTSD: The Unrecognized Symptom Jorge I. Ramirez, MD, FAAHPM Caroline Schauer, RN, BSN, CHPN VISN 23 Hospice and Palliative Care Objectives Describe Post Traumatic Stress Disorder (PTSD) and the population
PTSD: The Unrecognized Symptom Jorge I. Ramirez, MD, FAAHPM Caroline Schauer, RN, BSN, CHPN VISN 23 Hospice and Palliative Care Objectives Describe Post Traumatic Stress Disorder (PTSD) and the population
Anxiety Disorders. Fear & Anxiety. Anxiety Disorder? 26/5/2014. J. H. Atkinson, M.D. Fear. Anxiety. An anxiety disorder is present when
 Anxiety s J. H. Atkinson, M.D. HIV Neurobehavioral Research Center University of California, San Diego Department of Psychiatry & Veterans Affairs Healthcare System, San Diego Materials courtesy of Dr.
Anxiety s J. H. Atkinson, M.D. HIV Neurobehavioral Research Center University of California, San Diego Department of Psychiatry & Veterans Affairs Healthcare System, San Diego Materials courtesy of Dr.
Critical incident stress
 CAMPUS WELLBEING AND SUPPORT SERVICE Critical incident stress INFORMATION SHEET You have experienced a traumatic event or a critical incident (any incident that causes emergency service personnel to experience
CAMPUS WELLBEING AND SUPPORT SERVICE Critical incident stress INFORMATION SHEET You have experienced a traumatic event or a critical incident (any incident that causes emergency service personnel to experience
Comorbidity Rates. Comorbidity Rates. Males: Females:
 Comorbidity Rates Males: Any Diagnosis: 88% Alcoholism 52% Depression 48% Conduct Disorder 43% Drug Abuse 35% Phobia 31% Kessler, et al. (1995) Comorbidity Rates Females: Any Diagnosis 78% Depression 49%
Comorbidity Rates Males: Any Diagnosis: 88% Alcoholism 52% Depression 48% Conduct Disorder 43% Drug Abuse 35% Phobia 31% Kessler, et al. (1995) Comorbidity Rates Females: Any Diagnosis 78% Depression 49%
Strike out: PTSD TODD LANGUS PSY.D.
 Strike out: PTSD TODD LANGUS PSY.D. A STRATEGIC PLAN FOR CAREER SURVIVAL HOW RESPONDERS ARE TRAINED TO THINK Probability Versus Possibility Behaviors Developed for Job Survival All or Nothing thinking
Strike out: PTSD TODD LANGUS PSY.D. A STRATEGIC PLAN FOR CAREER SURVIVAL HOW RESPONDERS ARE TRAINED TO THINK Probability Versus Possibility Behaviors Developed for Job Survival All or Nothing thinking
SURREY FIRE SERVICE CRITICAL INCIDENT STRESS MANAGEMENT TEAM
 CISM DEFUSING/ DEBRIEFING HANDOUTS Common Signs and Symptoms During a CIS Event You have experienced a traumatic event, or a critical incident. Even though the event may be over, you may now be experiencing,
CISM DEFUSING/ DEBRIEFING HANDOUTS Common Signs and Symptoms During a CIS Event You have experienced a traumatic event, or a critical incident. Even though the event may be over, you may now be experiencing,
MICHELE BEDARD-GILLIGAN, PH.D. ASSISTANT PROFESSOR DEPARTMENT OF PSYCHIATRY AND BEHAVIORAL SCIENCES UNIVERSITY OF WASHINGTON
 Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences PTSD IN PRIMARY CARE MICHELE BEDARD-GILLIGAN, PH.D. ASSISTANT PROFESSOR DEPARTMENT OF PSYCHIATRY AND BEHAVIORAL
Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences PTSD IN PRIMARY CARE MICHELE BEDARD-GILLIGAN, PH.D. ASSISTANT PROFESSOR DEPARTMENT OF PSYCHIATRY AND BEHAVIORAL
Prepared by: Elizabeth Vicens-Fernandez, LMHC, Ph.D.
 Prepared by: Elizabeth Vicens-Fernandez, LMHC, Ph.D. Sources: National Institute of Mental Health (NIMH), the National Alliance on Mental Illness (NAMI), and from the American Psychological Association
Prepared by: Elizabeth Vicens-Fernandez, LMHC, Ph.D. Sources: National Institute of Mental Health (NIMH), the National Alliance on Mental Illness (NAMI), and from the American Psychological Association
Clinical Guideline for the Management of Bipolar Disorder in Adults
 Clinical Guideline for the Management of Bipolar Disorder in Adults Goal: To improve the quality of life of adults with bipolar disorder Identification and Treatment of Bipolar Disorder Criteria for Diagnosis:
Clinical Guideline for the Management of Bipolar Disorder in Adults Goal: To improve the quality of life of adults with bipolar disorder Identification and Treatment of Bipolar Disorder Criteria for Diagnosis:
Treatment Options for Bipolar Disorder Contents
 Keeping Your Balance Treatment Options for Bipolar Disorder Contents Medication Treatment for Bipolar Disorder 2 Page Medication Record 5 Psychosocial Treatments for Bipolar Disorder 6 Module Summary 8
Keeping Your Balance Treatment Options for Bipolar Disorder Contents Medication Treatment for Bipolar Disorder 2 Page Medication Record 5 Psychosocial Treatments for Bipolar Disorder 6 Module Summary 8
Pharmacological Treatment of Anxiety & Depressive Disorders
 Pharmacological Treatment of Anxiety & Depressive Disorders Dr Gary Jackson (MB BCh FRCPsych) Consultant Psychiatrist The Priory Hospital Chelmsford Wellesley Hospital Southend-on-Sea Medical Secretary:
Pharmacological Treatment of Anxiety & Depressive Disorders Dr Gary Jackson (MB BCh FRCPsych) Consultant Psychiatrist The Priory Hospital Chelmsford Wellesley Hospital Southend-on-Sea Medical Secretary:
Presentation is Being Recorded
 Integrated Care for Depression & Anxiety Psychotropic Medication Management for Primary Care Providers Los Angeles County Department of Mental Health September 20, 2011 Presentation is Being Recorded Please
Integrated Care for Depression & Anxiety Psychotropic Medication Management for Primary Care Providers Los Angeles County Department of Mental Health September 20, 2011 Presentation is Being Recorded Please
Major Depressive Disorder (MDD) in Children under Age 6
 in Children under Age 6") in Children under Age 6 Level 0 Comprehensive assessment. Refer to Principles of Practice on page 6. Level 1 Psychotherapeutic intervention (e.g., dyadic therapy) for 6 to 9 months; assessment of parent/guardian
in Children under Age 6 Level 0 Comprehensive assessment. Refer to Principles of Practice on page 6. Level 1 Psychotherapeutic intervention (e.g., dyadic therapy) for 6 to 9 months; assessment of parent/guardian
9/20/2011. Integrated Care for Depression & Anxiety: Psychotropic Medication Management for PCPs. Presentation is Being Recorded
 Integrated Care for Depression & Anxiety Psychotropic Medication Management for Primary Care Providers Los Angeles County Department of Mental Health September 20, 2011 Presentation is Being Recorded Please
Integrated Care for Depression & Anxiety Psychotropic Medication Management for Primary Care Providers Los Angeles County Department of Mental Health September 20, 2011 Presentation is Being Recorded Please
Antidepressant Medication Therapy in Primary Care July 25, 2013
 New York State Collaborative Care Initiative Antidepressant Medication Therapy in Primary Care July 25, 2013 http://uwaims.org Presenter Building on 25 years of Research and Practice in Integrated Mental
New York State Collaborative Care Initiative Antidepressant Medication Therapy in Primary Care July 25, 2013 http://uwaims.org Presenter Building on 25 years of Research and Practice in Integrated Mental
Reducing the Anxiety of Pediatric Anxiety Part 2: Treatment
 Reducing the Anxiety of Pediatric Anxiety Part 2: Treatment Lisa Lloyd Giles, MD Medical Director, Behavioral Consultation, Crisis, and Community Services Primary Children s Hospital Associate Professor,
Reducing the Anxiety of Pediatric Anxiety Part 2: Treatment Lisa Lloyd Giles, MD Medical Director, Behavioral Consultation, Crisis, and Community Services Primary Children s Hospital Associate Professor,
1/7/2013. An unstable or crucial time or state of affairs whose outcome will make a decisive difference for better or worse.
 B7 Responding to a Crisis Understanding a crisis Tools for assessing a crisis Understanding the phases of a crisis Understanding the types of crises Actions to take following a crisis Ways to cope with
B7 Responding to a Crisis Understanding a crisis Tools for assessing a crisis Understanding the phases of a crisis Understanding the types of crises Actions to take following a crisis Ways to cope with
Antidepressant Selection in Primary Care
 Antidepressant Selection in Primary Care Rebecca D. Lewis, DO OOA Summer CME Oklahoma City, OK 6 August 2017 Objectives Understand the epidemiology of depression. Recognize factors to help choose antidepressants.
Antidepressant Selection in Primary Care Rebecca D. Lewis, DO OOA Summer CME Oklahoma City, OK 6 August 2017 Objectives Understand the epidemiology of depression. Recognize factors to help choose antidepressants.
PTSD: Treatment Opportunities
 PTSD: Treatment Opportunities Professor Malcolm Hopwood Department of Psychiatry University of Melbourne Professorial Psychiatry Unit, Albert Road Clinic DSM 5: PTSD CRITERION A exposure to: actual or
PTSD: Treatment Opportunities Professor Malcolm Hopwood Department of Psychiatry University of Melbourne Professorial Psychiatry Unit, Albert Road Clinic DSM 5: PTSD CRITERION A exposure to: actual or
Antidepressant Selection in Primary Care
 Antidepressant Selection in Primary Care R E B E C C A D. L E W I S, D O O O A S U M M E R C M E B R A N S O N, M O 1 5 A U G U S T 2 0 1 5 Objectives Understand the epidemiology of depression. Recognize
Antidepressant Selection in Primary Care R E B E C C A D. L E W I S, D O O O A S U M M E R C M E B R A N S O N, M O 1 5 A U G U S T 2 0 1 5 Objectives Understand the epidemiology of depression. Recognize
Complex Trauma in Children and Adolescents
 Complex Trauma in Children and Adolescents Sara Coffey, D.O. Assistant Professor Department of Psychiatry and Behavioral Sciences Oklahoma State University Center for Health Sciences Overview of trauma
Complex Trauma in Children and Adolescents Sara Coffey, D.O. Assistant Professor Department of Psychiatry and Behavioral Sciences Oklahoma State University Center for Health Sciences Overview of trauma
PTSD Guide for Veterans, Civilians, Patients and Family
 PTSD Guide for Veterans, Civilians, Patients and Family Overview There are a variety of PTSD booklets available, so with ours we wanted to hand-pick the content we felt our audience could use most. We
PTSD Guide for Veterans, Civilians, Patients and Family Overview There are a variety of PTSD booklets available, so with ours we wanted to hand-pick the content we felt our audience could use most. We
In Memory of the American Tragedy
 Evolving Pharmacologic Strategies in the Treatment of PTSD John J. Miller, M.D. Medical Director Brain Health Exeter, NH In Memory of the American Tragedy September 11, 2001 jjm@brain-health.co 1 Overview
Evolving Pharmacologic Strategies in the Treatment of PTSD John J. Miller, M.D. Medical Director Brain Health Exeter, NH In Memory of the American Tragedy September 11, 2001 jjm@brain-health.co 1 Overview
PSYCHOTROPIC MEDICATION AND THE WORKPLACE. Dr. Marty Ewer 295 Fullarton Road Parkside
 PSYCHOTROPIC MEDICATION AND THE WORKPLACE Dr. Marty Ewer 295 Fullarton Road Parkside 5063 82999281 Introduction Depression and anxiety commonly occur in people who work. The World Health Organization has
PSYCHOTROPIC MEDICATION AND THE WORKPLACE Dr. Marty Ewer 295 Fullarton Road Parkside 5063 82999281 Introduction Depression and anxiety commonly occur in people who work. The World Health Organization has
Mental illness A Broad Overview. Dr H Pathmanandam March 2017
 Mental illness A Broad Overview Dr H Pathmanandam March 2017 Introduction Mental disorders are common in primary and secondary care Many are not recognised and not treated Some receive unnecessary or inappropriate
Mental illness A Broad Overview Dr H Pathmanandam March 2017 Introduction Mental disorders are common in primary and secondary care Many are not recognised and not treated Some receive unnecessary or inappropriate
Augmentation and Combination Strategies in Antidepressants treatment of Depression
 Augmentation and Combination Strategies in Antidepressants treatment of Depression Byung-Joo Ham, M.D. Department of Psychiatry Korea University College of Medicine Background The response rates reported
Augmentation and Combination Strategies in Antidepressants treatment of Depression Byung-Joo Ham, M.D. Department of Psychiatry Korea University College of Medicine Background The response rates reported
Identification and Management of Posttraumatic Stress Disorder after Traumatic Brain Injury
 Identification and Management of Posttraumatic Stress Disorder after Traumatic Brain Injury Curtis McKnight, MD Saturday March 23 rd, 2019 @DrCaMcKnight 2019 Barrow Traumatic Brain Injury Symposium Creighton
Identification and Management of Posttraumatic Stress Disorder after Traumatic Brain Injury Curtis McKnight, MD Saturday March 23 rd, 2019 @DrCaMcKnight 2019 Barrow Traumatic Brain Injury Symposium Creighton
PRACTICAL MANAGEMENT OF DEPRESSION IN OLDER ADULTS. Lee A. Jennings, MD MSHS Assistant Professor Division of Geriatrics, UCLA
 CASE #1 PRACTICAL MANAGEMENT OF DEPRESSION IN OLDER ADULTS Lee A. Jennings, MD MSHS Assistant Professor Division of Geriatrics, UCLA OBJECTIVES Epidemiology Presentation in older adults Assessment Treatment
CASE #1 PRACTICAL MANAGEMENT OF DEPRESSION IN OLDER ADULTS Lee A. Jennings, MD MSHS Assistant Professor Division of Geriatrics, UCLA OBJECTIVES Epidemiology Presentation in older adults Assessment Treatment
Introduction into Psychiatric Disorders. Dr Jon Spear- Psychiatrist
 Introduction into Psychiatric Disorders Dr Jon Spear- Psychiatrist Content Stress Major depressive disorder Adjustment disorder Generalised anxiety disorder Post traumatic stress disorder Borderline personality
Introduction into Psychiatric Disorders Dr Jon Spear- Psychiatrist Content Stress Major depressive disorder Adjustment disorder Generalised anxiety disorder Post traumatic stress disorder Borderline personality
Answer Key for Case Studies. Grading for each case study. All Case Studies
 Answer Key for Case Studies Grading for each case study All Case Studies *give 5 points for listing at least four accurate symptoms of the disorder *give 3 points for listing 2 symptoms of the disorder
Answer Key for Case Studies Grading for each case study All Case Studies *give 5 points for listing at least four accurate symptoms of the disorder *give 3 points for listing 2 symptoms of the disorder
CHILD & ADOLESCENT PSYCHIATRY ALERTS, VOLUME XIV, 2012 INDEX
 A Adderall Counterfeit, 31 addiction, internet CBT, 55 ADHD Adjunctive Guanfacine, 11 Counterfeit Adderall, 31 Developmental Trajectory and Risk Factors, 5 Dopamine Transporter Alterations, 14 Extended-Release
A Adderall Counterfeit, 31 addiction, internet CBT, 55 ADHD Adjunctive Guanfacine, 11 Counterfeit Adderall, 31 Developmental Trajectory and Risk Factors, 5 Dopamine Transporter Alterations, 14 Extended-Release
INDIVIDUALS ARE COPING ALL THE TIME.
 Coping Strategies INDIVIDUALS ARE COPING ALL THE TIME. COPING (CONTENDING) Coping: Is the behavior that protects us from becoming psychologically and physiologically disorganized. Usually incorporates
Coping Strategies INDIVIDUALS ARE COPING ALL THE TIME. COPING (CONTENDING) Coping: Is the behavior that protects us from becoming psychologically and physiologically disorganized. Usually incorporates
Post-traumatic stress disorder
 National Institute for Health and Care Excellence Final Post-traumatic stress disorder [F] Evidence reviews for pharmacological interventions for the prevention and treatment of PTSD in adults NICE guideline
National Institute for Health and Care Excellence Final Post-traumatic stress disorder [F] Evidence reviews for pharmacological interventions for the prevention and treatment of PTSD in adults NICE guideline
POST-TRAUMATIC STRESS DISORDER Comorbidity and Treatment
 POST-TRAUMATIC STRESS DISORDER Comorbidity and Treatment Thomas A. Mellman, M.D. Kathleen T. Brady, M.D., Ph.D. R. Bruce Lydiard, M.D., Ph.D. Howard University, Washington DC and Medical University of
POST-TRAUMATIC STRESS DISORDER Comorbidity and Treatment Thomas A. Mellman, M.D. Kathleen T. Brady, M.D., Ph.D. R. Bruce Lydiard, M.D., Ph.D. Howard University, Washington DC and Medical University of
Depression in Late Life
 Depression in Late Life Robert Madan MD FRCPC Geriatric Psychiatrist Key Learnings Robert Madan MD FRCPC Key Learnings By the end of the session, participants will be able to List the symptoms of depression
Depression in Late Life Robert Madan MD FRCPC Geriatric Psychiatrist Key Learnings Robert Madan MD FRCPC Key Learnings By the end of the session, participants will be able to List the symptoms of depression
Post-Traumatic Stress Disorder
 Post-Traumatic Stress Disorder Teena Jain 2017 Post-Traumatic Stress Disorder What is post-traumatic stress disorder, or PTSD? PTSD is a disorder that some people develop after experiencing a shocking,
Post-Traumatic Stress Disorder Teena Jain 2017 Post-Traumatic Stress Disorder What is post-traumatic stress disorder, or PTSD? PTSD is a disorder that some people develop after experiencing a shocking,
TREATING PATIENTS WITH ACUTE STRESS DISORDER AND POSTTRAUMATIC STRESS DISORDER
 TREATING PATIENTS WITH ACUTE STRESS DISORDER AND POSTTRAUMATIC STRESS DISORDER A Quick Reference Guide Based on Practice Guideline for the Treatment of Patients With Acute Stress Disorder and Posttraumatic
TREATING PATIENTS WITH ACUTE STRESS DISORDER AND POSTTRAUMATIC STRESS DISORDER A Quick Reference Guide Based on Practice Guideline for the Treatment of Patients With Acute Stress Disorder and Posttraumatic
PTSD & Stress Responses After Individual and Mass Injury Trauma. Trauma Survivors Outcomes & Support (TSOS) Trauma Survivors Outcomes & Support (TSOS)
 Trauma Survivors Outcomes & Support (TSOS)") PTSD & Stress Responses After Individual and Mass Injury Trauma Douglas Zatzick, MD Professor Department of Psychiatry & Behavioral Sciences Research Faculty Harborview Injury Prevention & Research Center
PTSD & Stress Responses After Individual and Mass Injury Trauma Douglas Zatzick, MD Professor Department of Psychiatry & Behavioral Sciences Research Faculty Harborview Injury Prevention & Research Center
Posttraumatic stress disorder in combat veterans Nicole R. Lawson, MS, PA-C
 Posttraumatic stress disorder in combat veterans Nicole R. Lawson, MS, PA-C ABSTRACT Posttraumatic stress disorder (PTSD) affects up to 18% of combat veterans, many of whom will seek care from clinicians
Posttraumatic stress disorder in combat veterans Nicole R. Lawson, MS, PA-C ABSTRACT Posttraumatic stress disorder (PTSD) affects up to 18% of combat veterans, many of whom will seek care from clinicians
Treatments for PTSD: A brief overview
 Treatments for PTSD: A brief overview Dr Jasmine Pang DPsych(Clin) Snr Clinical Psychologist Psychotraumatology Service Department of Psychological Medicine Changi General Hospital, Singapore Outline Brief
Treatments for PTSD: A brief overview Dr Jasmine Pang DPsych(Clin) Snr Clinical Psychologist Psychotraumatology Service Department of Psychological Medicine Changi General Hospital, Singapore Outline Brief
Post Traumatic Stress Disorder (PTSD) (PTSD)
 (PTSD)") Post Traumatic Stress Disorder (PTSD) (PTSD) Reference: http://www.psychiatry.org/military Prevalence of PTSD One in five veterans of the Iraq and Afghanistan wars is diagnosed with PTSD. (http://www.psychiatry.org/military
Post Traumatic Stress Disorder (PTSD) (PTSD) Reference: http://www.psychiatry.org/military Prevalence of PTSD One in five veterans of the Iraq and Afghanistan wars is diagnosed with PTSD. (http://www.psychiatry.org/military
Introduction to Drug Treatment
 Introduction to Drug Treatment LPT Gondar Mental Health Group www.le.ac.uk Introduction to Psychiatric Drugs Drugs and Neurotransmitters 5 Classes of Psychotropic medications Mechanism of action Clinical
Introduction to Drug Treatment LPT Gondar Mental Health Group www.le.ac.uk Introduction to Psychiatric Drugs Drugs and Neurotransmitters 5 Classes of Psychotropic medications Mechanism of action Clinical
Optimal Treatment of Anxiety Disorders
 Optimal Treatment of Anxiety Disorders Franklin R. Schneier, MD Co-Director, Anxiety Disorders Clinic Research Psychiatrist New York State Psychiatric Institute Special Lecturer in Psychiatry Columbia
Optimal Treatment of Anxiety Disorders Franklin R. Schneier, MD Co-Director, Anxiety Disorders Clinic Research Psychiatrist New York State Psychiatric Institute Special Lecturer in Psychiatry Columbia
Mental Health Nursing: Mood Disorders. By Mary B. Knutson, RN, MS, FCP
 Mental Health Nursing: Mood Disorders By Mary B. Knutson, RN, MS, FCP A Definition of Mood Prolonged emotional state that influences the person s whole personality and life functioning Adaptive Functions
Mental Health Nursing: Mood Disorders By Mary B. Knutson, RN, MS, FCP A Definition of Mood Prolonged emotional state that influences the person s whole personality and life functioning Adaptive Functions
Best Practices in Prescribing Benzodiazepines. Michael Carlisle, DO Medical Director University Hospitals Geauga Medical Center
 Best Practices in Prescribing Benzodiazepines Michael Carlisle, DO Medical Director University Hospitals Geauga Medical Center Objectives To review current practice guidelines in benzodiazepine prescribing
Best Practices in Prescribing Benzodiazepines Michael Carlisle, DO Medical Director University Hospitals Geauga Medical Center Objectives To review current practice guidelines in benzodiazepine prescribing
Index. Note: Page numbers of article titles are in boldface type. A ADHD. See Attention-deficit/hyperactivity disorder (ADHD) b-adrenergic blockers
 b-adrenergic blockers") Note: Page numbers of article titles are in boldface type. A ADHD. See Attention-deficit/hyperactivity disorder (ADHD) a-adrenergic blockers for PTSD, 798 b-adrenergic blockers for PTSD, 798 Adrenergic
Note: Page numbers of article titles are in boldface type. A ADHD. See Attention-deficit/hyperactivity disorder (ADHD) a-adrenergic blockers for PTSD, 798 b-adrenergic blockers for PTSD, 798 Adrenergic
8/22/2016. Contemporary Psychiatric-Mental Health Nursing Third Edition. Theories: Anxiety Disorders. Theories: Anxiety Disorders (cont'd)
") Contemporary Psychiatric-Mental Health Nursing Third Edition CHAPTER 18 Anxiety Disorders Theories: Anxiety Disorders Biological changes in the brain Noradrenergic system is sensitive to norepinephrine;
Contemporary Psychiatric-Mental Health Nursing Third Edition CHAPTER 18 Anxiety Disorders Theories: Anxiety Disorders Biological changes in the brain Noradrenergic system is sensitive to norepinephrine;
This initial discovery led to the creation of two classes of first generation antidepressants:
 Antidepressants - TCAs, MAOIs, SSRIs & SNRIs First generation antidepressants TCAs and MAOIs The discovery of antidepressants could be described as a lucky accident. During the 1950s, while carrying out
Antidepressants - TCAs, MAOIs, SSRIs & SNRIs First generation antidepressants TCAs and MAOIs The discovery of antidepressants could be described as a lucky accident. During the 1950s, while carrying out
First Responders and PTSD
 First Responders and PTSD DR. KENNETH J. COOPER MD, MHSC, FRCPC DR. DION GOODLAND PHD OEMAC CONFERENCE ST. JOHN S NEWFOUNDLAND JUNE 13, 2017 Faculty/Presenter Disclosure Faculty: Dr. Dion Goodland Dr.
First Responders and PTSD DR. KENNETH J. COOPER MD, MHSC, FRCPC DR. DION GOODLAND PHD OEMAC CONFERENCE ST. JOHN S NEWFOUNDLAND JUNE 13, 2017 Faculty/Presenter Disclosure Faculty: Dr. Dion Goodland Dr.
Contemporary Psychiatric-Mental Health Nursing Third Edition. Theories: Anxiety Disorders. Theories: Anxiety Disorders (cont'd) 10/2/2014
 10/2/2014") Contemporary Psychiatric-Mental Health Nursing Third Edition CHAPTER 18 Anxiety Disorders Theories: Anxiety Disorders Biological changes in the brain Neurotransmitters are associated with anxiety. low
Contemporary Psychiatric-Mental Health Nursing Third Edition CHAPTER 18 Anxiety Disorders Theories: Anxiety Disorders Biological changes in the brain Neurotransmitters are associated with anxiety. low
ACUTE STRESS DISORDER
 ACUTE STRESS DISORDER BEHAVIORAL DEFINITIONS 1. Has been exposed to actual death of another or perceived death or serious injury to self or another that resulted in an intense emotional response of fear,
ACUTE STRESS DISORDER BEHAVIORAL DEFINITIONS 1. Has been exposed to actual death of another or perceived death or serious injury to self or another that resulted in an intense emotional response of fear,
They are updated regularly as new NICE guidance is published. To view the latest version of this NICE Pathway see:
 bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published. To view the latest
bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published. To view the latest
Treatment of Anxiety (without benzos)
") Treatment of Anxiety (without benzos) Alison C. Lynch MD MS Clinical Professor Departments of Psychiatry and Family Medicine University of Iowa Health Care None Disclosures Overview/objectives Review common
Treatment of Anxiety (without benzos) Alison C. Lynch MD MS Clinical Professor Departments of Psychiatry and Family Medicine University of Iowa Health Care None Disclosures Overview/objectives Review common
Guilt Suicidality. Depression Co-Occurs with Medical Illness The rate of major depression among those with medical illness is significant.
 1-800-PSYCH If you are obsessive-compulsive, dial 1 repeatedly If you are paranoid-delusional, dial 2 and wait, your call is being traced If you are schizophrenic, a little voice will tell you what number
1-800-PSYCH If you are obsessive-compulsive, dial 1 repeatedly If you are paranoid-delusional, dial 2 and wait, your call is being traced If you are schizophrenic, a little voice will tell you what number
Depression in adults: treatment and management
 1 2 3 4 Depression in adults: treatment and management 5 6 7 8 Appendix V3: recommendations that have been deleted of changed from 2009 guideline Depression in adults: Appendix V3 1 of 22 1 Recommendations
1 2 3 4 Depression in adults: treatment and management 5 6 7 8 Appendix V3: recommendations that have been deleted of changed from 2009 guideline Depression in adults: Appendix V3 1 of 22 1 Recommendations
Kari A. Stephens, PhD & Wayne Bentham, MD Psychiatry & Behavioral Sciences University of Washington. Approach for doing differential diagnosis of PTSD
 IN PRIMARY CARE June 17, 2010 Kari A. Stephens, PhD & Wayne Bentham, MD Psychiatry & Behavioral Sciences University of Washington Defining and assessing Approach for doing differential diagnosis of Best
IN PRIMARY CARE June 17, 2010 Kari A. Stephens, PhD & Wayne Bentham, MD Psychiatry & Behavioral Sciences University of Washington Defining and assessing Approach for doing differential diagnosis of Best
Depression. University of Illinois at Chicago College of Nursing
 Depression University of Illinois at Chicago College of Nursing 1 Learning Objectives Upon completion of this session, participants will be better able to: 1. Recognize depression, its symptoms and behaviors
Depression University of Illinois at Chicago College of Nursing 1 Learning Objectives Upon completion of this session, participants will be better able to: 1. Recognize depression, its symptoms and behaviors
Major Depressive Disorder (MDD) in Children under Age 6
 in Children under Age 6") in Children under Age 6 Level 0 Comprehensive assessment. Refer to Principles of Practice on page 5. Level 1 Psychotherapeutic intervention (e.g., dyadic therapy) for 6 to 9 months; assessment of parent/guardian
in Children under Age 6 Level 0 Comprehensive assessment. Refer to Principles of Practice on page 5. Level 1 Psychotherapeutic intervention (e.g., dyadic therapy) for 6 to 9 months; assessment of parent/guardian
A Family s Guide to Posttraumatic Stress Disorder
 A Family s Guide to Posttraumatic Stress Disorder Department of Veterans Affairs and Department of Defense (DoD) employees who use this information are responsible for considering all applicable regulations
A Family s Guide to Posttraumatic Stress Disorder Department of Veterans Affairs and Department of Defense (DoD) employees who use this information are responsible for considering all applicable regulations
Post-Traumatic Stress Disorder (PTSD) Among People Living with HIV
 Among People Living with HIV") Post-Traumatic Stress Disorder (PTSD) Among People Living with HIV Milton L. Wainberg, M.D. Associate Clinical Professor of Psychiatry College of Physicians and Surgeons Columbia University mlw35@columbia.edu
Post-Traumatic Stress Disorder (PTSD) Among People Living with HIV Milton L. Wainberg, M.D. Associate Clinical Professor of Psychiatry College of Physicians and Surgeons Columbia University mlw35@columbia.edu
Fortunately, panic disorder is one of the most treatable anxiety disorders. The illness can be controlled with medication and focused psychotherapy.
 Anxiety Disorders Anxiety disorders are the most common mental illness in America. More than 19 million Americans suffer from anxiety disorders, which include panic disorder, obsessive-compulsive disorder,
Anxiety Disorders Anxiety disorders are the most common mental illness in America. More than 19 million Americans suffer from anxiety disorders, which include panic disorder, obsessive-compulsive disorder,
MEDICATION ALGORITHM FOR ANXIETY DISORDERS
 Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences MEDICATION ALGORITHM FOR ANXIETY DISORDERS RYAN KIMMEL, MD MEDICAL DIRECTOR HOSPITAL PSYCHIATRY UNIVERSITY OF WASHINGTON
Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences MEDICATION ALGORITHM FOR ANXIETY DISORDERS RYAN KIMMEL, MD MEDICAL DIRECTOR HOSPITAL PSYCHIATRY UNIVERSITY OF WASHINGTON
Anti-Depressant Medications
 Anti-Depressant Medications A Introduction: This topic may be a little bit underestimated here in Jordan, while in western countries it has more significance. The function of anti-depressants is to change
Anti-Depressant Medications A Introduction: This topic may be a little bit underestimated here in Jordan, while in western countries it has more significance. The function of anti-depressants is to change
TREATING MAJOR DEPRESSIVE DISORDER
 TREATING MAJOR DEPRESSIVE DISORDER A Quick Reference Guide Based on Practice Guideline for the Treatment of Patients With Major Depressive Disorder, Second Edition, originally published in April 2000.
TREATING MAJOR DEPRESSIVE DISORDER A Quick Reference Guide Based on Practice Guideline for the Treatment of Patients With Major Depressive Disorder, Second Edition, originally published in April 2000.
Post-Traumatic Stress Disorder (PTSD) in the military and veterans
 in the military and veterans") Post-Traumatic Stress Disorder (PTSD) in the military and veterans When people think of mental illness in the military it is unsurprising that many of them think of Post-Traumatic Stress Disorder (PTSD),
Post-Traumatic Stress Disorder (PTSD) in the military and veterans When people think of mental illness in the military it is unsurprising that many of them think of Post-Traumatic Stress Disorder (PTSD),
Anxiety Disorders.
 Anxiety Disorders Shamim Nejad, MD Medical Director, Psycho-Oncology Services Swedish Cancer Institute Swedish Medical Center Seattle, Washington Shamim.Nejad@swedish.org Disclosures Neither I nor my spouse/partner
Anxiety Disorders Shamim Nejad, MD Medical Director, Psycho-Oncology Services Swedish Cancer Institute Swedish Medical Center Seattle, Washington Shamim.Nejad@swedish.org Disclosures Neither I nor my spouse/partner
Trauma FIRST RESPONDERS JADA B. HUDSON M.S., LCPC, CADC
 JADA B. HUDSON M.S., LCPC, CADC Trauma FIRST RESPONDERS Jada B. Hudson, M.S. Licensed Clinical Professional Counselor Certified Alcohol and Drug Abuse Counselor Operation Shattered Stars Clinical Consultant
JADA B. HUDSON M.S., LCPC, CADC Trauma FIRST RESPONDERS Jada B. Hudson, M.S. Licensed Clinical Professional Counselor Certified Alcohol and Drug Abuse Counselor Operation Shattered Stars Clinical Consultant
PTSD Overview and Psychopharmacology Update. September 16, 2017
 PTSD Overview and Psychopharmacology Update September 16, 2017 Medical Director, OEF/OIF Program VA Medical Center Durham, NC Disclosures I am employed by the U.S. Department of Veterans Affairs Except
PTSD Overview and Psychopharmacology Update September 16, 2017 Medical Director, OEF/OIF Program VA Medical Center Durham, NC Disclosures I am employed by the U.S. Department of Veterans Affairs Except
A Patient s Guide: Understanding Posttraumatic Stress Disorder and Acute Stress Disorder
 A Patient s Guide: Understanding Posttraumatic Stress Disorder and Acute Stress Disorder Department of Veterans Affairs and Department of Defense (DoD) employees who use this information are responsible
A Patient s Guide: Understanding Posttraumatic Stress Disorder and Acute Stress Disorder Department of Veterans Affairs and Department of Defense (DoD) employees who use this information are responsible
Running Head: Counseling for Grieving families of Violence. Counseling for Grieving Families of Violence. Andrea Simmons. Tulane School of Social Work
 Grief 1 Running Head: Counseling for Grieving families of Violence Counseling for Grieving Families of Violence Andrea Simmons Tulane School of Social Work SOWK 745 Professor Jamey Boudreaux April 23,
Grief 1 Running Head: Counseling for Grieving families of Violence Counseling for Grieving Families of Violence Andrea Simmons Tulane School of Social Work SOWK 745 Professor Jamey Boudreaux April 23,
Review of Psychotrophic Medications. (An approved North Carolina Division of Health Services Regulation Continuing Education Course)
") Review of Psychotrophic Medications (An approved North Carolina Division of Health Services Regulation Continuing Education Course) Common Psychiatric Disorders *Schizophrenia *Depression *Bipolar Disorder
Review of Psychotrophic Medications (An approved North Carolina Division of Health Services Regulation Continuing Education Course) Common Psychiatric Disorders *Schizophrenia *Depression *Bipolar Disorder
PTS(D): The Invisible Wound
: The Invisible Wound") PTS(D): The Invisible Wound Julie Rake, MS, PA C Fellow, Integrative Medicine The intelligent combination of conventional and evidence based alternative medicine. It aims to restore the focus of medicine
PTS(D): The Invisible Wound Julie Rake, MS, PA C Fellow, Integrative Medicine The intelligent combination of conventional and evidence based alternative medicine. It aims to restore the focus of medicine
Post-traumatic Stress Disorder
 Parkland College A with Honors Projects Honors Program 2012 Post-traumatic Stress Disorder Nicole Smith Parkland College Recommended Citation Smith, Nicole, "Post-traumatic Stress Disorder" (2012). A with
Parkland College A with Honors Projects Honors Program 2012 Post-traumatic Stress Disorder Nicole Smith Parkland College Recommended Citation Smith, Nicole, "Post-traumatic Stress Disorder" (2012). A with
10/3/2018 FIRE IN THE BASEMENT: Raised by a Combat Veteran. Disclosures. None TRAUMA AND TREATMENT STRATEGIES. Aaron Wilson, MD
 FIRE IN THE BASEMENT: TRAUMA AND TREATMENT STRATEGIES Aaron Wilson, MD Raised by a Combat Veteran Disclosures None 1 Objectives Formulate a practical, working understanding of trauma neurobiology Identify
FIRE IN THE BASEMENT: TRAUMA AND TREATMENT STRATEGIES Aaron Wilson, MD Raised by a Combat Veteran Disclosures None 1 Objectives Formulate a practical, working understanding of trauma neurobiology Identify
Diagnosis and Management of Anxiety Disorders
 Diagnosis and Management of Anxiety Disorders V International Symposium on HIV Neuropsychiatry Barcelona - Spain Milton L. Wainberg, MD Columbia University May 24, 2012 Anxiety Normal reaction to a stressor
Diagnosis and Management of Anxiety Disorders V International Symposium on HIV Neuropsychiatry Barcelona - Spain Milton L. Wainberg, MD Columbia University May 24, 2012 Anxiety Normal reaction to a stressor
Primary Care Provider & Psychiatric Consultant Roles. PC/PCP Role Session Objectives. Working as a Team. Joseph Cerimele Anna Ratzliff
 Primary Care Provider & Psychiatric Consultant Roles Joseph Cerimele Anna Ratzliff PC/PCP Role Session Objectives By the end of the session, participants will: 1. Understand the role of the psychiatric
Primary Care Provider & Psychiatric Consultant Roles Joseph Cerimele Anna Ratzliff PC/PCP Role Session Objectives By the end of the session, participants will: 1. Understand the role of the psychiatric
Session outline. Introduction to depression Assessment of depression Management of depression Follow-up Review
 Depression 1 Session outline Introduction to depression Assessment of depression Management of depression Follow-up Review 2 Activity 1: Person s story followed by group discussion Present the first person
Depression 1 Session outline Introduction to depression Assessment of depression Management of depression Follow-up Review 2 Activity 1: Person s story followed by group discussion Present the first person
ANTI-DEPRESSANT MEDICATIONS
 ANTI-DEPRESSANT MEDICATIONS This information is not intended to be a substitute for medical advice. It s purpose is solely informative. If your client or yourself are taking antidepressants, do not change
ANTI-DEPRESSANT MEDICATIONS This information is not intended to be a substitute for medical advice. It s purpose is solely informative. If your client or yourself are taking antidepressants, do not change
Responding to Traumatic Reactions in Children and Adolescents. Steve Minick Vice President of Programs
 Responding to Traumatic Reactions in Children and Adolescents Steve Minick Vice President of Programs stevem@fsnwpa.org 814 866-4500 TF-CBT at Family Services Trauma Types Served 760 Documented Physical
Responding to Traumatic Reactions in Children and Adolescents Steve Minick Vice President of Programs stevem@fsnwpa.org 814 866-4500 TF-CBT at Family Services Trauma Types Served 760 Documented Physical
Psychobiology Handout
 Nsg 85A / Psychiatric Page 1 of 7 Psychobiology Handout STRUCTURE AND FUNCTION OF THE BRAIN Psychiatric illness and the treatment of psychiatric illness alter brain functioning. Some examples of this are
Nsg 85A / Psychiatric Page 1 of 7 Psychobiology Handout STRUCTURE AND FUNCTION OF THE BRAIN Psychiatric illness and the treatment of psychiatric illness alter brain functioning. Some examples of this are
Treating Anxiety Disorders. Adil Virani, BSc (Pharm), Pharm D, FCSHP
, Pharm D, FCSHP") Treating Anxiety Disorders Adil Virani, BSc (Pharm), Pharm D, FCSHP Outline! Michelle s Case! Types of anxiety disorders! Goals of therapy! Treatment options and guidelines! Pharmacological options! Benzodiazepines
Treating Anxiety Disorders Adil Virani, BSc (Pharm), Pharm D, FCSHP Outline! Michelle s Case! Types of anxiety disorders! Goals of therapy! Treatment options and guidelines! Pharmacological options! Benzodiazepines
Lesson 16: Disaster Psychology
 Community Emergency Response Team (CERT) Training IS-317 Module 4: Disaster Medical Operations Lesson 16: Disaster Psychology Self-Study Guide March 2004 Lesson Overview Overview Lesson Objectives Estimated
Community Emergency Response Team (CERT) Training IS-317 Module 4: Disaster Medical Operations Lesson 16: Disaster Psychology Self-Study Guide March 2004 Lesson Overview Overview Lesson Objectives Estimated
The work of a Clinical Psychologist in Major Trauma
 The work of a Clinical Psychologist in Major Trauma 10 th November 2016 Dr Becky Coles-Gale Senior Clinical Psychologist (Major Trauma) Rebecca.Coles-Gale@sussexpartnership.nhs.uk Royal Sussex County Hospital
The work of a Clinical Psychologist in Major Trauma 10 th November 2016 Dr Becky Coles-Gale Senior Clinical Psychologist (Major Trauma) Rebecca.Coles-Gale@sussexpartnership.nhs.uk Royal Sussex County Hospital
Psychiatric Consultant Role in Collaborative Care Sept 12, 2013
 New York State Collaborative Care Initiative Psychiatric Consultant Role in Collaborative Care Sept 12, 2013 http://uwaims.org Presenter Building on 25 years of Research and Practice in Integrated Mental
New York State Collaborative Care Initiative Psychiatric Consultant Role in Collaborative Care Sept 12, 2013 http://uwaims.org Presenter Building on 25 years of Research and Practice in Integrated Mental
Other significant mental health complaints
 Other significant mental health complaints 2 Session outline Introduction to other significant mental health complaints Assessment of other significant mental health complaints Management of other significant
Other significant mental health complaints 2 Session outline Introduction to other significant mental health complaints Assessment of other significant mental health complaints Management of other significant
Medications for Anxiety & Behavior in Williams Syndrome. Disclosure of Potential Conflicts. None 9/22/2016. Evaluation
 Medications for Anxiety & Behavior in Williams Syndrome Christopher J. McDougle, M.D. Director, Lurie Center for Autism Professor of Psychiatry and Pediatrics Massachusetts General Hospital and MassGeneral
Medications for Anxiety & Behavior in Williams Syndrome Christopher J. McDougle, M.D. Director, Lurie Center for Autism Professor of Psychiatry and Pediatrics Massachusetts General Hospital and MassGeneral
Antidepressants. Dr Malek Zihlif
 Antidepressants The optimal use of antidepressant required a clear understanding of their mechanism of action, pharmacokinetics, potential drug interaction and the deferential diagnosis of psychiatric
Antidepressants The optimal use of antidepressant required a clear understanding of their mechanism of action, pharmacokinetics, potential drug interaction and the deferential diagnosis of psychiatric