TB Nurse Case Management Waukesha, Wisconsin March 31 April 2, Pediatric TB Michelle Hulse, MD April 1, 2009
|
|
|
- Eric Lamb
- 5 years ago
- Views:
Transcription


1 TB Nurse Case Management Waukesha, Wisconsin March 31 April 2, 2009 Pediatric TB Michelle Hulse, MD April 1, 2009 Pediatric Tuberculosis HNTC Nurse Case Management Course April 1, 2009 Waukesha, Wisconsin Michelle Hulse, MD Medical Director Infectious Disease/Immunology/Rheumatology Children s Hospital s and Clinics of Minnesota Pediatric Tuberculosis consultant St. Paul-Ramsey County Public Health Department Minnesota Department of Health Tuberculosis Control Program 1
2 Pediatric TB Defined by WHO and CDC TB in children less than 15 years old historically WHO only reports AFB smear positive cases by age WHO will now report cases <5 yrs, 5-14 yrs, >/= 15 yrs In contrast to adults Clinical manifestations are usually related to primary tuberculosis rather than reactivation tuberculosis Stages of Tuberculosis Exposure to contagious adult with pulmonary disease Household contacts 20-30% Latent TB infection LTBI 5-10% 5-50% Disease Active TB Adult Disease Active TB Child 2
3 Percentage of Household and Close Contacts Who Have a Positive Tuberculin Skin Test after Exposure to a Patient with Smear-Positive, Culture-Positive, or Culture-Negative Tuberculosis Musher DM. N Engl J Med 2003;348: Epidemiology of Childhood TB Percent Positive PPD Household contacts 0-14 yrs of age England,1954 Canada, contacts 1876 contacts Smear+ 65% 45% Culture+ Smear- 27% 26% Culture+ 3
4 Pediatric TB Diagnostic and therapeutic challenges Less specific signs and symptoms of disease Paucibacillary resulting in fewer positive cultures Increased risk of progression of disease once infected Increased risk of dissemination Age Related Risk for TB Risk of progression to active disease in first year after infection <12 months 43% 1-5 years 24% 6-10 years 2% years 15% Healthy adults 5-10% lifetime risk HIV infected adult 30-50% lifetime risk 4

5 Age Related Risk for TB Disease manifestations vary Immunocompetent, <2 yrs of age Highest rate of disease of any age group Experience most of the disseminated disease 2-5 yr olds Disease rate is the same as those <2yrs Less risk for meningeal or disseminated disease School age children have the lowest disease rate of any age Exposure Household contact with contagious teen or adult Usually > 4 hours of contact Chest 2 view PAandLat* TWO VIEW CHEST: IMPRESSION: Airway disease. No infiltrate, adenopathy or evidence of active pulmonary tuberculosis. Pt: 2 week old infant Adult index case: father, incarcerated during gestation, ill for several months prior to hospitalization Cavitary, smear + pulmonary disease, pericarditis, osteomyelitis MTB pansenstive isolated 5
6 Pediatric Exposure Treatment Window prophylaxis Window period for TST conversion: 2-12 weeks Indicated for those </=4 years Baseline TST / CXR normal INH prophylaxis recommended Children </= 4yrs Immunosuppressed pts Pts on TNF alpha blockers Follow up TST done weeks after last exposure to infectious contact induration less than 5 mm stop prophylaxis, induration greater than 5 mm treat for LTBI TB diagnosis Risk assessment important Diagnosis in children more often based on epidemiology and clinical findings than on smear or culture 6

7 TST and pediatric disease Positive TST with TB disease Pediatrics 89% Adults 54% Up to 20% of children with TB disease will have a negative TST at diagnosis Approximately 5% will be persistently negative TST and BCG BCG prevents infection in approximately 50% of vaccine recipients BCG may prevent severe forms of TB disease in young children BCG influence on TST results depends on: Age at immunization (less effect if at birth) Time since immunization Exposure to nontuberculous mycobacteria (false positives) Prevalence of LTBI (if prevalence high then PPV better) Type of vaccine used (higher # of bacilli= greater effect) 7
8 TST and BCG Study of children given BCG at birth: <50% of infants will have a positive TST at 6-12 mos of age Most children will have nonreactive TSTs by 5 years of age Previous BCG is not a contraindication for TST TST positivity in BCG vaccinated children from TB endemic countries is more likely related to LTBI than BCG BCG vaccination status should be disregarded in interpreting TSTs TB disease Clinical and radiographic findings ( ,480 US cases) Pulmonary 76.9% Primary Progressive Chronic/reactivation Extra-pulmonary Lymphatic 15.5% Meningeal 2.1% Miliary 1.1% Pleural 1.1% Bone/joint 1.4% TB in newborns 8

9 Pediatric TB disease Laboratory diagnosis Adult source isolate can direct treatment Cultures need to be obtained from the child if: source case is unknown several possible source cases with different susceptibility patterns if the likely source has drug resistant TB extrapulmonary disease Pediatric TB disease Laboratory diagnosis Childhood pulmonary disease Inpatient early morning gastric aspirate x3 (cx + ~40%) Induced sputum x 3 in cooperative older children-first morning best Bronchoscopy: culture yield is lower than properly obtained gastric aspirate (cx + ~20%) Newer testing modalities are not used for various reasons: PCR sensitivity only slightly better than culture, specificity less, so not widely used in pediatrics NAA and IGRAs not approved for use Extrapulmonary disease Culture from affected body site (cx +~40%) 9
10 TB disease Clinical and radiographic findings Pulmonary primary TB Most common presenting symptoms: cough, fever, wheeze, decreased appetite, and fatigue 50% are asymptomatic Usually not infectious Lack cavities Cough not strong enough to produce airborne bacilli TB disease Clinical and radiographic findings Pulmonary primary TB Radiographic findings Intrathoracic lymphadenopathy (hilar, mediastinal, subcarinal) Parenchymal changes Segmental hyperinflation and atelectasis due to bronchial obstruction Alveolar consolidation Interstitial densities Bronchiectasis 10
11 Primary Pulmonary Hilar adenopathy 13 yo asymptomatic, identified as part of contact investigation PPD 20mm Primary Pulmonary Hilar adenopathy + 6 yo PPD 15 mm Contact investigation CXR hilar and infrahilar fullness Chest CT : Multiple pulmonary nodules in the lung bases bilaterally, in the right lower lobe, one in the posterolateral right middle lobe and two in the left lower lobe. Also present is extensive adenopathy. 11
12 Primary Pulmonary LLL infiltrate Contact investigation 8 yo PPD 18 mm CXR LLL opacity pneumonia vs atelectasis Asymptomatic Sputum smear negative TB disease Clinical and radiographic findings Progressive pulmonary primary TB Associated with weight loss or FTT, anorexia, fatigue, low grade temp, intermittent cough May cause cavitation or endobronchial disease 12
13 TB disease Clinical and radiographic findings Chronic pulmonary/ reactivation disease Most common in adolescents with primary infection after 7 years of age Present with fever, weight loss, productive cough, hemoptysis, night sweats Xray findings include cavitations, typically upper lobe TB disease Clinical and radiographic findings Chronic pulmonary/ reactivation disease US data Cavitary disease Sputum smear positive Sputum culture positive <10 years of age 3.5% 1.7% % years of age 11.8% (p<0.001) 10.3% (p<0.001) 21.3% (p<
14 TB disease Clinical and radiographic findings Superficial lymphadenitis Usually the anterior cervical and submandibular nodes Usually presents within 6 months of infection Affects children with median age months Nodes are firm, nontender or minimally so No systemic symptoms Chest radiographic findings may be present TB disease Clinical and radiographic findings Pleural effusion Most occur 3 months after primary infection Usually affect older children (mean 13.5 years) Present with fever, fatigue, respiratory distress, chest pain CXR shows unilateral pleural effusion Associated parenchymal abnormalities in about half of pts Excellent prognosis 14




15 TB meningitis SA, 8 month old East Indian girl RUL pneumonia, possible abscess or Loculated pleural fluid SA, 8 month old with pulmonary TB and TB meningitis. Chest CT with RUL dense Consolidation with multiple Cavitations. Superior mediastinum findings Consistent with abscess 15
16 TB disease Clinical and radiographic findings Meningeal disease Most within 3-6 months of primary infection Often associated with miliary disease, esp in < 5 yr olds Median age affected months Most severe form of disease TB disease Clinical and radiographic findings Meningeal disease Indolent with symptoms present 1-4 weeks before diagnosis Most common symptoms are fever, vomiting, lethargy, headache, seizure (esp in < 2 year olds) Hydrocephalus common on presentation Brain parenchymal disease (tuberculoma) in 20-37% CXR abnormal in 40-86% 16
17 TB disease Clinical and radiographic findings Meningeal disease Outcome depends on age and severity of symptoms at presentation Mortality <10% with effective therapy Long term sequelae are common Mental retardation Seizures hemiparesis TB disease Clinical and radiographic findings YY 18 mo Hmong male Micronodular infiltrates Hilar fullness Miliary disease Similar to meningitis in pathogenesis, time of onset after infection, indolent presentation, and severity Median age affected is 6 11 months Often present with weeks of fever, cough, weight loss, anorexia, and malaise 17


18 TB disease Clinical and radiographic findings Miliary disease 50-70% have generalized lymphadenopathy and hepatosplenomegaly 90% have diffuse micronodular pulmonary consolidations YY 21 mo Hmong male F/U CXR 3mos: improving micronodular infiltrates and hilar fullness 18

19 TB disease Clinical and radiographic findings Bone/joint disease Onset 6-18 months after primary infection Median age of onset 6 years Affect vertebrae, knee, hip, and elbow most commonly Present with localized inflammation, pain, swelling, decreased range of motion, and fever Xrays may show spondylitis, arthritis, and osteomyelitis 50% will have abnormal CXR LH 7 yo Hmong refugee Pott s disease spine MRI Destruction and collapse of L3 and L4 along with inferior L2 and Superior L5. Kyphosis and gibbus formation, mild Central stenosis 19
20 Pediatric TB disease Treatment Well established adult regimens used (ATS/IDSA/CDC 2002) Emphasis on number of doses in given time period DOT DOT DOT DOT DOT DOT DOT DOT Empiric regimens require 4 drugs in initial phase in Minnesota Pediatric TB disease Treatment Pulmonary TB 6 mos Isolated hilar adenopathy 6 mos INH+Rifampin Extrapulmonary TB adenitis Bone and joint TB TB meningitis Miliary/severe disseminated 6 mos 6-9 months 12 months 9-12 months Durations listed are for drug susceptible TB disease 20
 0.")
21 Pediatric TB disease Treatment First line drugs INH rifampin pyrazinamide ethambutol streptomycin (im) Pills preferred over suspensions <1% of children develop adverse effects (rash, N/V/D) Hypersensitivity reaction causing MP or morbiliform rash can occur and occasionally require D/C of INH 8% of 965 children: transient increase in LFTs (Palusci el al) 0.4% discontinued INH Check LFTs and monitor in those with risk factors for hepatitis Inhibits metabolism of some drugs resulting in increased levels (ie anticonvulsants) Table from: Francis J Curry National Tuberculosis Center and California Dept of Public Health, 2008: Drug Resistant Tuberculosis: A Survival Guide for Clinicians, 2 nd Ed 21
22 Pediatric TB disease Treatment INH and peripheral neuropathy Caused by vitamin B6 deficiency Caused by increased excretion Manifests as tingling of fingers and toes Rare in children Predisposition in: diabetes uremia milk/meat deficient diet malnutrition symptomatic HIV ETOH use pregnancy breastfeeding Can result in orange discoloration of urine, tears, sweat Increases metabolism of many drugs (OCPs, HIV protease inhibitors and NNRTIs, corticosteroids, phenytoin) Adverse effects: Rash, GI upset Flu-like symptoms (intermittent therapy) Hepatotoxicity Severe immunologic reaction (rare) Table from: Francis J Curry National Tuberculosis Center and California Dept of Public Health, 2008: Drug Resistant Tuberculosis: A Survival Guide for Clinicians, 2 nd Ed 22


23 Adverse effects Fever GI upset Transient increase in uric acid Hepatotoxicity rare Not recommended with underlying liver disease or INH induced hepatotoxicity Table from: Francis J Curry National Tuberculosis Center and California Dept of Public Health, 2008: Drug Resistant Tuberculosis: A Survival Guide for Clinicians, 2 nd Ed Adverse effects GI, hypersensitivity, and visual Retrobulbar neuritis Reversible in most Dose and renal function dependent Manifests as decreased visual acuity or red-green color discrimination Two reviews on use in children did not find evidence for visual toxicity Monitor monthly Table from: Francis J Curry National Tuberculosis Center and California Dept of Public Health, 2008: Drug Resistant Tuberculosis: A Survival Guide for Clinicians, 2 nd Ed 23
24 Medication delivery Expect resistance! Prepare the family for the challenge! Give medications all at once and at same time each day Incent the child Rewards Praise Choices Medication delivery INH Commercial suspension in sorbitol High osmotic load can cause GI upset and diarrhea Poorly tolerated in older children Other meds can be compounded into suspensions Recommend pill/capsules over suspensions 24
25 Medication delivery Pill and capsules taken intact or halves is easiest Tip head back to swallow pills, forward for capsules Place crushed tabs in empty capsule if capsules are easier Crushed pills can be given in soft food or liquid Medication delivery Soft vehicle ideas Chocolate sauce, pudding, fudge sauce, ice cream Jelly or marmalade (texture can hide granularity) Apple sauce or berry sauce (can hide red rifampin color) Nutella or peanut butter Cream cheese or chili Oreo cookie cream 25




26 Case presentation #1 20 mo old Somali refugee with 8 mo hx of fever, cough, chronic otitis media, constitutional symptoms +PPD Chest imaging with miliary opacities and extensive mediastinal and hilar adenopathy CNS tuberculomas Splenomegaly, retroperitoneal, and peri-portal adenopathy Mildly increased aminotransferases and inflammatory markers JO 20 months, Somali Refugee from Kenya 2 m prior 8 m hx cough, fever, Poor appetite No interest in play


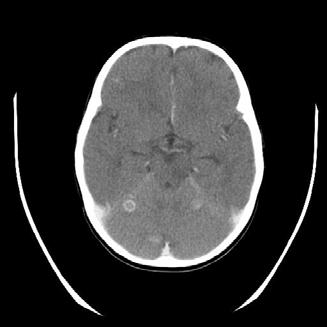
27 Chest CT Head CT 27
28 Case presentation #1 Gastric washings X3 1/3 + MTB pansensitive Induced sputum X3 all neg Left ear drainage cx +MTB Blood culture neg Urine culture neg Case presentation #1 Started therapy INH Rifampin PZA EMB B6 Steroids Ranitidine Dilantin NG feeds 28


29 Case presentation #1 Rapid improvement in symptoms Defervesced More interactive and playful Improved appetite Discharged home on directly observed therapy on hospital day 11 Follow up CT one month after start of therapy IMPRESSION: Improved findings of miliary tuberculosis compared to Mild cylindrical bronchiectasis right upper and middle lobes. 3. Very slight improvement in extensive necrotic mediastinal and right hilar lymphadenopathy. 4. Improved aeration right upper lobe 29
30 Case presentation #1 Follow up chest CT: improvement in all findings except mediastinal and hilar adenopathy Head CT: marked improvement in tuberculomas Pt had been seen in clinic prior with verification that all meds were being given, TB meds by TB clinic staff, others by mom Case presentation #1 On repeat questioning steroids were not being given, and had not been given after the pt was discharged from the hospital Steroids are an important part of treatment in miliary disease Reduce adenopathy and potential for further airway compression and late pulmonary complications such and collapse-consolidation Bronchial erosion and endobronchial disease Reduce risk of broncho- or tracheo- esophogeal fisutala Reduce CNS inflammation 30
31 Case presentation #1 Steroids were started again, with one dose by DOT and the other verified each day Treatment for 4 weeks with 3 week taper Prolonged rx and taper reduce risk of rebound Pt did well thereafter Case presentation #1 Pt had 6 sibs: 4 yrs-12 yrs 5/6 with +PPD 4/5 with pulmonary disease 1/4 had normal CXR on initial screen and presented 2 ½ weeks later with unilateral pleural effusion, not responsive to antibacterial therapy 1/6 PPD and CXR (4 yr old), remains PPD neg 31




32 WO, 5 yo PPD +, CXR L hilar fullness, retrocardiac LLL infiltrate, medial RUL infil vs atelectasis; GW 1/3 + MTB; induced sputum + MTB pansensitive IO, 11 yo Somali refugee PPD 18 mm 11/18/06 CXR normal 12/10/06 admit with chest pain, fever CXR unilateral effusion 32



33 IO Chest CT on admit with unilateral pleural effusion Persistent fever and rising CRP on parenteral antibiotics, BC neg, pleural fluid cx neg CXR 3 months after starting antimycobacterial meds LO 6 yo Somali refugee PPD 16 mm, poor appetite 11/18/06 CXR bilat hilar prominence L>R Interstitial prominence Medial RUL infiltrate 33

34 Case Presentation #2 Miliary TB Chest 2 view PAandLat* FINDINGS: Normal cardiothymic silhouette. There is diffuse reticulonodular density of the lungs suspicious for possible disseminated miliary tuberculosis in patient with positive skin test. No focal air space opacity or effusion. Hilar shadows are mildly prominent and hilar adenopathy is not excluded. IMPRESSION: Suspicious for disseminated miliary TB. 34


35 TCS 12 mo miliary TB Pansensitive Endobronchial lesion with collapse-consolidation 4 mos into therapy Initial steroid therapy non-compliance Neck CT showing large necrotic left cervical nodes 4 months into DOT therapy Immune reconstitution phenomenon in 14 month old HIV negative with miliary TB 35

36 Case Presentation #3 TB disease Left hilar fullness Gastric washing cx INH resistant MTB N.L., 15 mo Indian female FUO presenting chest x-ray 36


37 TB disease N.L. FUO Chest CT Pulmonary TB Necrotic perihilar adenopathy and peripheral nodular infiltrate 37
Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017
 Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has the following disclosures
Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has the following disclosures
Pediatric TB Lisa Armitige, MD, PhD September 28, 2011
 TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Pediatric TB Lisa Armitige, MD, PhD September 28, 2011 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interest.
TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Pediatric TB Lisa Armitige, MD, PhD September 28, 2011 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interest.
TB Nurse Case Management San Antonio, Texas July 18 20, 2012
 TB Nurse Case Management San Antonio, Texas July 18 20, 2012 Pediatric TB Kim Smith, MD, MPH July 19, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
TB Nurse Case Management San Antonio, Texas July 18 20, 2012 Pediatric TB Kim Smith, MD, MPH July 19, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
TB Intensive Houston, Texas. Childhood Tuberculosis Kim Connelly Smith. November 12, 2009
 TB Intensive Houston, Texas November 10-12, 12 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 1 OUTLINE Stages
TB Intensive Houston, Texas November 10-12, 12 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 1 OUTLINE Stages
TB Nurse Case Management San Antonio, Texas March 7 9, Pediatric TB Kim Connelly Smith, MD, MPH March 8, 2012
 TB Nurse Case Management San Antonio, Texas March 7 9, 2012 Pediatric TB Kim Connelly Smith, MD, MPH March 8, 2012 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict of interests
TB Nurse Case Management San Antonio, Texas March 7 9, 2012 Pediatric TB Kim Connelly Smith, MD, MPH March 8, 2012 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict of interests
Tuberculosis Intensive
 Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Childhood Tuberculosis Kim Smith, MD, MPH April 6, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Childhood Tuberculosis Kim Smith, MD, MPH April 6, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
Diagnosis and Medical Management of Latent TB Infection
 Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
TB: Management in an era of multiple drug resistance. Bob Belknap M.D. Denver Public Health November 2012
 TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
Tuberculosis Tools: A Clinical Update
 Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
PEDIATRIC TUBERCULOSIS
 PEDIATRIC TUBERCULOSIS Ann M. Loeffler, M.D. Faculty Consultant Curry International Tuberculosis Center Objectives At the end of this session, participants will be able to describe: how pediatric patients
PEDIATRIC TUBERCULOSIS Ann M. Loeffler, M.D. Faculty Consultant Curry International Tuberculosis Center Objectives At the end of this session, participants will be able to describe: how pediatric patients
TB Intensive Houston, Texas
 TB Intensive Houston, Texas October 15-17, 17 2013 Diagnosis of TB: Radiology Rosa M Estrada-Y-Martin, MD MSc FCCP October 16, 2013 Rosa M Estrada-Y-Martin, MD MSc FCCP, has the following disclosures to
TB Intensive Houston, Texas October 15-17, 17 2013 Diagnosis of TB: Radiology Rosa M Estrada-Y-Martin, MD MSc FCCP October 16, 2013 Rosa M Estrada-Y-Martin, MD MSc FCCP, has the following disclosures to
PEDIATRIC TUBERCULOSIS. Objectives. Children are not just small adults. Pediatric Tuberculosis 1
 PEDIATRIC TUBERCULOSIS Ann M. Loeffler, M.D. Faculty Consultant Curry International Tuberculosis Center Objectives At the end of this session, participants will be able to describe: how pediatric patients
PEDIATRIC TUBERCULOSIS Ann M. Loeffler, M.D. Faculty Consultant Curry International Tuberculosis Center Objectives At the end of this session, participants will be able to describe: how pediatric patients
TB Intensive San Antonio, Texas August 7-10, 2012
 TB Intensive San Antonio, Texas August 7-10, 2012 An Introduction to Childhood Tuberculosis Kim Smith, MD, MPH August 10, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests
TB Intensive San Antonio, Texas August 7-10, 2012 An Introduction to Childhood Tuberculosis Kim Smith, MD, MPH August 10, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests
Pediatric TB Radiology: It s Not Black and White Part 2
 Experiencing technical difficulties? Please call Adobe Connect for technical assistance at 1-800-422-3623 Pediatric TB Radiology: It s Not Black and White Part 2 June 18, 2018 A National Webinar June 18,
Experiencing technical difficulties? Please call Adobe Connect for technical assistance at 1-800-422-3623 Pediatric TB Radiology: It s Not Black and White Part 2 June 18, 2018 A National Webinar June 18,
Contact Investigation and Prevention in the USA
 Contact Investigation and Prevention in the USA George D. McSherry, MD Division of Infectious Disease Penn State Children s Hospital Pediatric Section TB Center of Excellence Rutgers Global Tuberculosis
Contact Investigation and Prevention in the USA George D. McSherry, MD Division of Infectious Disease Penn State Children s Hospital Pediatric Section TB Center of Excellence Rutgers Global Tuberculosis
TUBERCULOSIS. Pathogenesis and Transmission
 TUBERCULOSIS Pathogenesis and Transmission TUBERCULOSIS Pathogenesis and Transmission Infection to Disease Diagnostic & Isolation Updates Treatment Updates Pathogenesis Droplet nuclei of 5µm or less are
TUBERCULOSIS Pathogenesis and Transmission TUBERCULOSIS Pathogenesis and Transmission Infection to Disease Diagnostic & Isolation Updates Treatment Updates Pathogenesis Droplet nuclei of 5µm or less are
DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE
 DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH Assistant Professor University of Texas Health Science Center Staff Physician, Texas Center for Infectious Diseases TB Nurse Case
DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH Assistant Professor University of Texas Health Science Center Staff Physician, Texas Center for Infectious Diseases TB Nurse Case
Diagnosis and Treatment of Tuberculosis, 2011
 Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
TB Radiology for Nurses Garold O. Minns, MD
 TB Nurse Case Management Salina, Kansas March 31-April 1, 2010 TB Radiology for Nurses Garold O. Minns, MD April 1, 2010 TB Radiology for Nurses Highway Patrol Training Center Salina, KS April 1, 2010
TB Nurse Case Management Salina, Kansas March 31-April 1, 2010 TB Radiology for Nurses Garold O. Minns, MD April 1, 2010 TB Radiology for Nurses Highway Patrol Training Center Salina, KS April 1, 2010
Treatment of TB Infection Lisa Y. Armitige, MD, PhD April 7, 2015
 Treatment of TB Infection Lisa Y. Armitige, MD, PhD April 7, 2015 Tuberculosis Infection Diagnosis and Treatment April 7, 2015 El Paso, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has
Treatment of TB Infection Lisa Y. Armitige, MD, PhD April 7, 2015 Tuberculosis Infection Diagnosis and Treatment April 7, 2015 El Paso, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has
Interpretation of Chest Radiographs Paul Christensen, MD 10/21/09. Diagnostic Evaluation. Medical Evaluation & CXR Interpretation.
 Diagnostic Evaluation Medical Evaluation & CXR Interpretation University of Michigan TB Consultant Washtenaw County Medical history Physical examination Testing for TB exposure (previously covered) Radiologic
Diagnostic Evaluation Medical Evaluation & CXR Interpretation University of Michigan TB Consultant Washtenaw County Medical history Physical examination Testing for TB exposure (previously covered) Radiologic
Pediatric Tuberculosis: The Essentials October 8, 2014
 Pediatric Tuberculosis: The Essentials Ann M Loeffler, MD Randall Children s Hospital at Legacy Emanuel Portland, Oregon Curry International TB Center Disclosures Nothing to disclose Learning Objectives
Pediatric Tuberculosis: The Essentials Ann M Loeffler, MD Randall Children s Hospital at Legacy Emanuel Portland, Oregon Curry International TB Center Disclosures Nothing to disclose Learning Objectives
3/25/2012. numerous micro-organismsorganisms
 Congenital & Neonatal TB A Case of Tuberculosis Congenital or Acquired? Felicia Dworkin, MD NYC DOHMH Bureau TB Control World TB Day March 23, 2012 Congenital TB: acquired by the fetus during pregnancy
Congenital & Neonatal TB A Case of Tuberculosis Congenital or Acquired? Felicia Dworkin, MD NYC DOHMH Bureau TB Control World TB Day March 23, 2012 Congenital TB: acquired by the fetus during pregnancy
Diagnosis & Medical Case Management of TB Disease. Lisa Armitige, MD, PhD October 22, 2015
 Diagnosis & Medical Case Management of TB Disease Lisa Armitige, MD, PhD October 22, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
Diagnosis & Medical Case Management of TB Disease Lisa Armitige, MD, PhD October 22, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
Errors in Dx and Rx of TB
 Errors in Dx and Rx of TB David Schlossberg, MD, FACP Professor of Medicine Temple University School of Medicine Medical Director, TB Control Program Philadelphia Department of Public Health TB Still a
Errors in Dx and Rx of TB David Schlossberg, MD, FACP Professor of Medicine Temple University School of Medicine Medical Director, TB Control Program Philadelphia Department of Public Health TB Still a
has the following disclosures to make:
 CLINICAL DIAGNOSIS AND MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH September 22, 2015 TB Nurse Case Management September 22 24, 2015 San Antonio. TX EXCELLENCE EXPERTISE INNOVATION Annie Kizilbash
CLINICAL DIAGNOSIS AND MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH September 22, 2015 TB Nurse Case Management September 22 24, 2015 San Antonio. TX EXCELLENCE EXPERTISE INNOVATION Annie Kizilbash
An Introduction to Radiology for TB Nurses
 An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
Fundamentals of Tuberculosis (TB)
") TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
TUBERCULOSIS. By Dr. Najaf Masood Assistant Prof Pediatrics Benazir Bhutto Hospital Rawalpindi
 TUBERCULOSIS By Dr. Najaf Masood Assistant Prof Pediatrics Benazir Bhutto Hospital Rawalpindi Tuberculosis Infectious, Systemic, Chronic granulomatous disease caused by mycobacterium tuberculosis DEFINITION
TUBERCULOSIS By Dr. Najaf Masood Assistant Prof Pediatrics Benazir Bhutto Hospital Rawalpindi Tuberculosis Infectious, Systemic, Chronic granulomatous disease caused by mycobacterium tuberculosis DEFINITION
Tuberculosis (TB) Fundamentals for School Nurses
 Fundamentals for School Nurses") Tuberculosis (TB) Fundamentals for School Nurses June 9, 2015 Kristin Gall, RN, MSN/Pat Infield, RN-TB Program Manager Marsha Carlson, RN, BSN Two Rivers Public Health Department Nebraska Department of
Tuberculosis (TB) Fundamentals for School Nurses June 9, 2015 Kristin Gall, RN, MSN/Pat Infield, RN-TB Program Manager Marsha Carlson, RN, BSN Two Rivers Public Health Department Nebraska Department of
TB In Detroit 2011* Early TB: Smudge Sign. Who is at risk for exposure to or infection with TB? Who is at risk for TB after exposure or infection?
 Those oral antibiotics are just not working! Inpatient Standards of Care & Discharge Planning S/He s in the Hospital: Now What Do I Do? Dana G. Kissner, MD TB Intensive Workshop, Lansing, MI 2012 Objectives:
Those oral antibiotics are just not working! Inpatient Standards of Care & Discharge Planning S/He s in the Hospital: Now What Do I Do? Dana G. Kissner, MD TB Intensive Workshop, Lansing, MI 2012 Objectives:
Pediatric TB Basics and Evaluation and Management of Exposed Neonates
 Pediatric TB Basics and Evaluation and Management of Exposed Neonates Ann M. Loeffler, MD Randall Children s Hospital, Portland OR & Curry International TB Center, Oakland CA September, 2017 No Disclosures
Pediatric TB Basics and Evaluation and Management of Exposed Neonates Ann M. Loeffler, MD Randall Children s Hospital, Portland OR & Curry International TB Center, Oakland CA September, 2017 No Disclosures
At the end of this session, participants will be able to:
 Advanced Concepts in Pediatric Tuberculosis: Infection Control, Source Case and Contact Investigation Ana M. Alvarez, M.D. Associate Professor Division of Pediatric Infectious Diseases and Immunology University
Advanced Concepts in Pediatric Tuberculosis: Infection Control, Source Case and Contact Investigation Ana M. Alvarez, M.D. Associate Professor Division of Pediatric Infectious Diseases and Immunology University
Pediatric TB Theresa Barton, MD
 TB Nurse Case Management San Antonio, Texas December 8-10, 2009 Pediatric TB Theresa Barton, MD December 9, 2009 Pediatric Tuberculosis Tess Barton, MD Assistant Professor of Pediatrics UT Southwestern
TB Nurse Case Management San Antonio, Texas December 8-10, 2009 Pediatric TB Theresa Barton, MD December 9, 2009 Pediatric Tuberculosis Tess Barton, MD Assistant Professor of Pediatrics UT Southwestern
Diagnosis of TB: Radiology David Finlay, MD
 TB Intensive Tyler, Texas June 2-4, 2010 Diagnosis of TB: Radiology David Finlay, MD June 3, 2010 2stages stages- Tuberculosis 1. primary infection 2. reactivation, or post primary disease 2 1 Primary
TB Intensive Tyler, Texas June 2-4, 2010 Diagnosis of TB: Radiology David Finlay, MD June 3, 2010 2stages stages- Tuberculosis 1. primary infection 2. reactivation, or post primary disease 2 1 Primary
Managing the Patients Response to TB Treatment
 Managing the Patients Response to TB Treatment Barbarah Martinez, RN, BSN September 13, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Barbarah Martinez, RN, BSN has
Managing the Patients Response to TB Treatment Barbarah Martinez, RN, BSN September 13, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Barbarah Martinez, RN, BSN has
Diagnosis and Medical Management of TB Disease. Quratulian Annie Kizilbash, MD, MPH March 17, 2015
 Diagnosis and Medical Management of TB Disease Quratulian Annie Kizilbash, MD, MPH March 17, 2015 TB Nurse Case Management March 17 19, 2015 San Antonio, Texas EXCELLENCE EXPERTISE INNOVATION Quratulian
Diagnosis and Medical Management of TB Disease Quratulian Annie Kizilbash, MD, MPH March 17, 2015 TB Nurse Case Management March 17 19, 2015 San Antonio, Texas EXCELLENCE EXPERTISE INNOVATION Quratulian
9 month old with stridor, cough, low-grade fever, mild hypoxia
 9 month old with stridor, cough, low-grade fever, mild hypoxia 3 months of age CXR normal Scenarios: Pregnant woman with + PPD Next steps? CXR negative, asymptomatic: treat for LTBI after delivery (INH
9 month old with stridor, cough, low-grade fever, mild hypoxia 3 months of age CXR normal Scenarios: Pregnant woman with + PPD Next steps? CXR negative, asymptomatic: treat for LTBI after delivery (INH
Management of Pediatric Tuberculosis in New Jersey
 Management of Pediatric Tuberculosis in New Jersey Helen Aguila, MD NJMS Global TB Institute December 15, 2011 This presentation is in part adapted from Pediatric Tuberculosis by Ann Loeffler, MD : Francis
Management of Pediatric Tuberculosis in New Jersey Helen Aguila, MD NJMS Global TB Institute December 15, 2011 This presentation is in part adapted from Pediatric Tuberculosis by Ann Loeffler, MD : Francis
Tuberculosis - clinical forms. Dr. A.Torossian,, M.D., Ph. D. Department of Respiratory Diseases
 Tuberculosis - clinical forms Dr. A.Torossian,, M.D., Ph. D. Department of Respiratory Diseases 1 TB DISEASE Primary Post-primary (Secondary) Common primary forms Primary complex Tuberculosis of the intrathoracic
Tuberculosis - clinical forms Dr. A.Torossian,, M.D., Ph. D. Department of Respiratory Diseases 1 TB DISEASE Primary Post-primary (Secondary) Common primary forms Primary complex Tuberculosis of the intrathoracic
TB Intensive Houston, Texas October 15-17, 2013
 TB Intensive Houston, Texas October 15-17, 2013 Tuberculosis in Children Kim Connelly Smith, MD, MPH October 16, 2013 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict of interests
TB Intensive Houston, Texas October 15-17, 2013 Tuberculosis in Children Kim Connelly Smith, MD, MPH October 16, 2013 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict of interests
Pediatric TB Intensive Houston, Texas October 14, Extrapulmonary TB in Children Kim Connelly Smith, MD, MPH October 14, 2013
 Pediatric TB Intensive Houston, Texas October 14, 2013 Extrapulmonary TB in Children Kim Connelly Smith, MD, MPH October 14, 2013 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict
Pediatric TB Intensive Houston, Texas October 14, 2013 Extrapulmonary TB in Children Kim Connelly Smith, MD, MPH October 14, 2013 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict
Pediatric Tuberculosis
 Pediatric Tuberculosis Kim Connelly Smith, MD, MPH April 7, 2016 TB Intensive April 5 8, 2016 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Kim Connelly Smith, MD, MPH has the following disclosures to
Pediatric Tuberculosis Kim Connelly Smith, MD, MPH April 7, 2016 TB Intensive April 5 8, 2016 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Kim Connelly Smith, MD, MPH has the following disclosures to
LTBI Videos-Treatment
 LTBI Videos-Treatment This program is presented by the Global Tuberculosis Institute and is based on recommendations from the Centers for Disease Control and Prevention. This is the third in a series of
LTBI Videos-Treatment This program is presented by the Global Tuberculosis Institute and is based on recommendations from the Centers for Disease Control and Prevention. This is the third in a series of
Communicable Disease Control Manual Chapter 4: Tuberculosis
 Provincial TB Services 655 West 12th Avenue Vancouver, BC V5Z 4R4 www.bccdc.ca Communicable Disease Control Manual Definitions Page 1 2.0 DEFINITIONS Many of the definitions that follow are taken from
Provincial TB Services 655 West 12th Avenue Vancouver, BC V5Z 4R4 www.bccdc.ca Communicable Disease Control Manual Definitions Page 1 2.0 DEFINITIONS Many of the definitions that follow are taken from
Tuberculosis: The Essentials
 Tuberculosis: The Essentials Kendra L. Fisher, MD, PhD THORACIC TUBERCULOSIS: THE BARE ESSENTIALS Kendra Fisher MD, FRCP (C) Department of Radiology Loma Linda University Medical Center TUBERCULOSIS ()
Tuberculosis: The Essentials Kendra L. Fisher, MD, PhD THORACIC TUBERCULOSIS: THE BARE ESSENTIALS Kendra Fisher MD, FRCP (C) Department of Radiology Loma Linda University Medical Center TUBERCULOSIS ()
TB in Children. Rene De Gama Block 10 Lectures 2012
 TB in Children Rene De Gama Block 10 Lectures 2012 Contents Epidemiology Transmission and pathogenesis Diagnosis of TB TB and HIV Management Epidemiology The year 2000 8.3 million new TB cases diagnosed
TB in Children Rene De Gama Block 10 Lectures 2012 Contents Epidemiology Transmission and pathogenesis Diagnosis of TB TB and HIV Management Epidemiology The year 2000 8.3 million new TB cases diagnosed
Northwestern Polytechnic University
 Clinical Tuberculosis Assessment by Health Care Provider Clinicians should review and verify the information in the Tuberculosis (TB) Screening Questionnaire (attached). Persons answering YES to any questions
Clinical Tuberculosis Assessment by Health Care Provider Clinicians should review and verify the information in the Tuberculosis (TB) Screening Questionnaire (attached). Persons answering YES to any questions
What you need to know about diagnosing and treating TB: a preventable, fatal disease. Bob Belknap M.D. Denver Public Health November 2014
 What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2014 The Critical First Step Consider TB in the Differential 1. Risks
What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2014 The Critical First Step Consider TB in the Differential 1. Risks
Dr Francis Ogaro MTRH ELDORET
 Dr Francis Ogaro MTRH ELDORET TB in children often severe, disseminated and can progress rapidly and with poor outcome TB diagnosis in children has relied on clinical, imaging, microscopy and TST findings.
Dr Francis Ogaro MTRH ELDORET TB in children often severe, disseminated and can progress rapidly and with poor outcome TB diagnosis in children has relied on clinical, imaging, microscopy and TST findings.
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016
 Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
Tuberculosis: A Provider s Guide to
 Tuberculosis: A Provider s Guide to Diagnosis and Treatment of Active Tuberculosis (TB) Disease and Screening and Treatment of Latent Tuberculosis Infection (LTBI) Alameda County Health Care Services Agency
Tuberculosis: A Provider s Guide to Diagnosis and Treatment of Active Tuberculosis (TB) Disease and Screening and Treatment of Latent Tuberculosis Infection (LTBI) Alameda County Health Care Services Agency
PULMONARY TUBERCULOSIS RADIOLOGY
 PULMONARY TUBERCULOSIS RADIOLOGY RADIOLOGICAL MODALITIES Medical radiophotography Radiography Fluoroscopy Linear (conventional) tomography Computed tomography Pulmonary angiography, bronchography Ultrasonography,
PULMONARY TUBERCULOSIS RADIOLOGY RADIOLOGICAL MODALITIES Medical radiophotography Radiography Fluoroscopy Linear (conventional) tomography Computed tomography Pulmonary angiography, bronchography Ultrasonography,
TB & HIV CO-INFECTION IN CHILDREN. Reené Naidoo Paediatric Infectious Diseases Broadreach Healthcare 19 April 2012
 TB & HIV CO-INFECTION IN CHILDREN Reené Naidoo Paediatric Infectious Diseases Broadreach Healthcare 19 April 2012 Introduction TB & HIV are two of the leading causes of morbidity & mortality in children
TB & HIV CO-INFECTION IN CHILDREN Reené Naidoo Paediatric Infectious Diseases Broadreach Healthcare 19 April 2012 Introduction TB & HIV are two of the leading causes of morbidity & mortality in children
Diagnosis and Management of TB Disease Lisa Armitige, MD, PhD September 27, 2011
 TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Diagnosis and Management of TB Disease Lisa Armitige, MD, PhD September 27, 2011 Lisa Armitige, MD, PhD has the following disclosures to make:
TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Diagnosis and Management of TB Disease Lisa Armitige, MD, PhD September 27, 2011 Lisa Armitige, MD, PhD has the following disclosures to make:
What the Primary Physician Should Know about Tuberculosis. Topics for Discussion. Global Impact of TB
 What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Common disease presentations Diagnosis of active TB Screening
What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Common disease presentations Diagnosis of active TB Screening
Pediatric TB Intensive Houston, Texas October 14, 2013
 Pediatric TB Intensive Houston, Texas October 14, 2013 Diagnosis and Management of Tuberculosis in Adolescents Andrea T. Cruz, MD, MPH Sections of Infectious Diseases & Emergency Medicine October 14, 2013
Pediatric TB Intensive Houston, Texas October 14, 2013 Diagnosis and Management of Tuberculosis in Adolescents Andrea T. Cruz, MD, MPH Sections of Infectious Diseases & Emergency Medicine October 14, 2013
What you need to know about diagnosing and treating TB: a preventable, fatal disease. Bob Belknap M.D. Denver Public Health November 2013
 What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2013 Case 1: 52 y/o male Born in the Pacific Islands; some travel in
What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2013 Case 1: 52 y/o male Born in the Pacific Islands; some travel in
HEALTH SERVICES POLICY & PROCEDURE MANUAL
 PAGE 1 of 7 References Related ACA Standards 4 th Edition Standards for Adult Correctional Institutions 4-4350, 4-4355 These guidelines are based on the recommendations of the American Thoracic Society
PAGE 1 of 7 References Related ACA Standards 4 th Edition Standards for Adult Correctional Institutions 4-4350, 4-4355 These guidelines are based on the recommendations of the American Thoracic Society
Radiological Aspects of Pulmonary Tuberculosis in Immunocompetent Hosts
 Nov 2003 Radiological Aspects of Pulmonary Tuberculosis in Immunocompetent Hosts Josh Rempell, Harvard Medical School Year III Tuberculosis: the captain of all (wo)men of death Overall, one third of the
Nov 2003 Radiological Aspects of Pulmonary Tuberculosis in Immunocompetent Hosts Josh Rempell, Harvard Medical School Year III Tuberculosis: the captain of all (wo)men of death Overall, one third of the
David E. Griffith, MD has the following disclosures to make:
 Diagnosis of TB: Radiology David E. Griffith, MD March 13, 2015 TB for Pulmonologist March 13, 2015 Phoenix, AZ EXCELLENCE EXPERTISE INNOVATION David E. Griffith, MD has the following disclosures to make:
Diagnosis of TB: Radiology David E. Griffith, MD March 13, 2015 TB for Pulmonologist March 13, 2015 Phoenix, AZ EXCELLENCE EXPERTISE INNOVATION David E. Griffith, MD has the following disclosures to make:
Pediatric TB Intensive Houston, Texas
 Pediatric TB Intensive Houston, Texas November 13, 2009 Treatment of Pediatric TB Jeffrey R. Starke, M.D. November 13, 2009 MANAGEMENT OF CHILDHOOD TUBERCULOSIS Jeffrey R. Starke, M.D. Professor of Pediatrics
Pediatric TB Intensive Houston, Texas November 13, 2009 Treatment of Pediatric TB Jeffrey R. Starke, M.D. November 13, 2009 MANAGEMENT OF CHILDHOOD TUBERCULOSIS Jeffrey R. Starke, M.D. Professor of Pediatrics
What the Primary Physician Should Know about Tuberculosis. Topics for Discussion. Life Cycle of M. tuberculosis
 What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Microbiology Epidemiology Common disease presentations Diagnosis of active
What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Microbiology Epidemiology Common disease presentations Diagnosis of active
Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012
 Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 LTBI and TB Disease Treatment Cara Christ, MD, MS May 8, 2012 Cara Christ, MD, MS has the following disclosures to make: No conflict
Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 LTBI and TB Disease Treatment Cara Christ, MD, MS May 8, 2012 Cara Christ, MD, MS has the following disclosures to make: No conflict
Supplemental Figure 1. Gating strategies for flow cytometry and intracellular cytokinestaining
 Supplemental Figure 1. Gating strategies for flow cytometry and intracellular cytokinestaining of PBMCs. Forward scatter area (FSC-A) versus side scatter area (SSC-A) was used to select lymphocytes followed
Supplemental Figure 1. Gating strategies for flow cytometry and intracellular cytokinestaining of PBMCs. Forward scatter area (FSC-A) versus side scatter area (SSC-A) was used to select lymphocytes followed
CHAPTER:1 TUBERCULOSIS. BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY
 CHAPTER:1 TUBERCULOSIS BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY GLOBAL EMERGENCY: * Tuberculosis kills 5,000 people a day! * 2.3 million die each year!
CHAPTER:1 TUBERCULOSIS BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY GLOBAL EMERGENCY: * Tuberculosis kills 5,000 people a day! * 2.3 million die each year!
MANAGEMENT OF TUBERCULOSIS IN NEONATES AND YOUNG INFANTS
 MANAGEMENT OF TUBERCULOSIS IN NEONATES AND YOUNG INFANTS A Bekker FIDSSA Conference, 2017 OUTLINE Case Perinatal TB Approach to the TB-exposed newborn MOM AND BABY S Born by NVD at peripheral hospital
MANAGEMENT OF TUBERCULOSIS IN NEONATES AND YOUNG INFANTS A Bekker FIDSSA Conference, 2017 OUTLINE Case Perinatal TB Approach to the TB-exposed newborn MOM AND BABY S Born by NVD at peripheral hospital
PEDIATRIC TB. Modified PPT from group A seminar (F)
") PEDIATRIC TB Modified PPT from group A seminar (F) objectives the epidemiology of pediatric TB. TB Mycobacteriology. pediatric TB presentations compared to adults TB. Know the differences between, and
PEDIATRIC TB Modified PPT from group A seminar (F) objectives the epidemiology of pediatric TB. TB Mycobacteriology. pediatric TB presentations compared to adults TB. Know the differences between, and
LTBI in Special Populations John Nava, MD October 5, 2010
 Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 LTBI in Special Populations John Nava, MD October 5, 2010 2 Treatment of Latent TB Infection in Special Populations John
Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 LTBI in Special Populations John Nava, MD October 5, 2010 2 Treatment of Latent TB Infection in Special Populations John
Chapter 22. Pulmonary Infections
 Chapter 22 Pulmonary Infections Objectives State the incidence of pneumonia in the United States and its economic impact. Discuss the current classification scheme for pneumonia and be able to define hospital-acquired
Chapter 22 Pulmonary Infections Objectives State the incidence of pneumonia in the United States and its economic impact. Discuss the current classification scheme for pneumonia and be able to define hospital-acquired
PREVENTION OF TUBERCULOSIS. Dr Amitesh Aggarwal
 PREVENTION OF TUBERCULOSIS Dr Amitesh Aggarwal 25 to 50 % of persons exposed to intimate contact with active PTB - latent infection with TB. Exposure to index case for 12 hours - high risk of infection.
PREVENTION OF TUBERCULOSIS Dr Amitesh Aggarwal 25 to 50 % of persons exposed to intimate contact with active PTB - latent infection with TB. Exposure to index case for 12 hours - high risk of infection.
CLINICAL DIAGNOSIS AND MANAGEMENT OF TB Disease
 CLINICAL DIAGNOSIS AND MANAGEMENT OF TB Disease Barbara J Seaworth MD Medical Director Heartland National TB Center Professor of Medicine University of Texas Health Center Tyler Barbara J Seaworth MD has
CLINICAL DIAGNOSIS AND MANAGEMENT OF TB Disease Barbara J Seaworth MD Medical Director Heartland National TB Center Professor of Medicine University of Texas Health Center Tyler Barbara J Seaworth MD has
TB Classification (ATS/CDC)
") bits and pieces Lisa Chen, MD UCSF Pulmonary/Critical Care Curry International Tuberculosis Center 10/2017 TB Classification (ATS/CDC) TB0 No tuberculosis exposure, not infected TB1 Tuberculosis exposure,
bits and pieces Lisa Chen, MD UCSF Pulmonary/Critical Care Curry International Tuberculosis Center 10/2017 TB Classification (ATS/CDC) TB0 No tuberculosis exposure, not infected TB1 Tuberculosis exposure,
Patient History 1. Patient History 2. Social History. The Role of Surgery in the Management of TB. Reynard McDonald, MD & Paul Bolanowski, MD
 Patient History 1 The Role of Surgery in the Management of TB Reynard McDonald, MD & Paul Bolanowski, MD September 16, 2010 42 y/o AA male was initially diagnosed with pansensitive pulmonary TB in 1986
Patient History 1 The Role of Surgery in the Management of TB Reynard McDonald, MD & Paul Bolanowski, MD September 16, 2010 42 y/o AA male was initially diagnosed with pansensitive pulmonary TB in 1986
Diagnosis of tuberculosis in children
 Diagnosis of tuberculosis in children H Simon Schaaf Desmond Tutu TB Centre Department of Paediatrics and Child Health, Stellenbosch University, and Tygerberg Children s Hospital (TCH) Estimated TB incidence
Diagnosis of tuberculosis in children H Simon Schaaf Desmond Tutu TB Centre Department of Paediatrics and Child Health, Stellenbosch University, and Tygerberg Children s Hospital (TCH) Estimated TB incidence
Chapter 5 Treatment for Latent Tuberculosis Infection
 Chapter 5 Treatment for Latent Tuberculosis Infection Table of Contents Chapter Objectives.... 109 Introduction.... 111 Candidates for the Treatment of LTBI... 112 LTBI Treatment Regimens.... 118 LTBI
Chapter 5 Treatment for Latent Tuberculosis Infection Table of Contents Chapter Objectives.... 109 Introduction.... 111 Candidates for the Treatment of LTBI... 112 LTBI Treatment Regimens.... 118 LTBI
Tuberculosis in Primary Care COC GTA Spring Symposium Dr Elizabeth Rea April 2013
 Tuberculosis in Primary Care COC GTA Spring Symposium Dr Elizabeth Rea April 2013 1 TB in Toronto - risk groups Diagnosis of active TB LTBI diagnosis and management Infection control 2 TB in Toronto Case
Tuberculosis in Primary Care COC GTA Spring Symposium Dr Elizabeth Rea April 2013 1 TB in Toronto - risk groups Diagnosis of active TB LTBI diagnosis and management Infection control 2 TB in Toronto Case
Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis
 Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Diagnosis of active TB Screening
Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Diagnosis of active TB Screening
TB, or NOT TB? A Tough Question in Kids!
 TB, or NOT TB? A Tough Question in Kids! Brian Lee, MD Pediatric Tuberculosis Program Division of Infectious Diseases Ken Martin, MD Division of Radiology Overview Illustrate the range of clinical scenarios
TB, or NOT TB? A Tough Question in Kids! Brian Lee, MD Pediatric Tuberculosis Program Division of Infectious Diseases Ken Martin, MD Division of Radiology Overview Illustrate the range of clinical scenarios
INDEX CASE INFORMATION
 Instructions for Completing the MDH Tuberculosis Contact Investigation Report Form Please provide as much information as possible. Each field represents information that is important to the contact investigation.
Instructions for Completing the MDH Tuberculosis Contact Investigation Report Form Please provide as much information as possible. Each field represents information that is important to the contact investigation.
TB in the Patient with HIV
 TB in the Patient with HIV Lisa Y. Armitige, MD, PhD May 11, 2017 TB Intensive May 9 12, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD, has the following disclosures to
TB in the Patient with HIV Lisa Y. Armitige, MD, PhD May 11, 2017 TB Intensive May 9 12, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD, has the following disclosures to
Targeted Testing and the Diagnosis of. Latent Tuberculosis. Infection and Tuberculosis Disease
 Self-Study Study Modules on Tuberculosis Targeted Testing and the Diagnosis of Latent Tuberculosis Infection and Tuberculosis Disease 1 Module 3: Objectives At completion of this module, learners will
Self-Study Study Modules on Tuberculosis Targeted Testing and the Diagnosis of Latent Tuberculosis Infection and Tuberculosis Disease 1 Module 3: Objectives At completion of this module, learners will
CHAPTER 3: DEFINITION OF TERMS
 CHAPTER 3: DEFINITION OF TERMS NOTE: TB bacteria is used in place of Mycobacterium tuberculosis and Mycobacterium tuberculosis complex in most of the definitions presented here. 3.1 Acid-fast bacteria
CHAPTER 3: DEFINITION OF TERMS NOTE: TB bacteria is used in place of Mycobacterium tuberculosis and Mycobacterium tuberculosis complex in most of the definitions presented here. 3.1 Acid-fast bacteria
Rehuka Khurana, MD, MPH has the following disclosures to make:
 Case Presentation Steps to a Systematic Approach to Diagnosis of TB Case Presentation Steps to a Systematic Approach to Diagnosis of TB Renuka Khurana, MD, MPH March 13, 2015 TB for Pulmonologist March
Case Presentation Steps to a Systematic Approach to Diagnosis of TB Case Presentation Steps to a Systematic Approach to Diagnosis of TB Renuka Khurana, MD, MPH March 13, 2015 TB for Pulmonologist March
5. HIV-positive individuals treated with INH should receive Pyridoxine (B6) 25 mg daily or 50 mg twice/thrice weekly on the same schedule as INH
 25 mg daily or 50 mg twice/thrice weekly on the same schedule as INH") V. TB and HIV/AIDS A. Standards of Treatment and Management The majority of TB treatment principles apply to persons with HIV/AIDS who require treatment for TB disease. The following points are either
V. TB and HIV/AIDS A. Standards of Treatment and Management The majority of TB treatment principles apply to persons with HIV/AIDS who require treatment for TB disease. The following points are either
Gary Reubenson 16 October 2012 PAEDIATRIC TUBERCULOSIS: AN OVERVIEW IN 40 MINUTES!!
 Gary Reubenson 16 October 2012 PAEDIATRIC TUBERCULOSIS: AN OVERVIEW IN 40 MINUTES!! DECLARATION No relevant conflicts of interest to declare OVERVIEW Burden of disease & epidemiology Pathogenesis (not
Gary Reubenson 16 October 2012 PAEDIATRIC TUBERCULOSIS: AN OVERVIEW IN 40 MINUTES!! DECLARATION No relevant conflicts of interest to declare OVERVIEW Burden of disease & epidemiology Pathogenesis (not
Pediatric TB Intensive Houston, Texas October 14, 2013
 Pediatric TB Intensive Houston, Texas October 14, 2013 Radiologic Presentation of Childhood TB Susan D. John, MD, FACR October 14, 2013 Disclosures I have no disclosures or conflicts of interest to report
Pediatric TB Intensive Houston, Texas October 14, 2013 Radiologic Presentation of Childhood TB Susan D. John, MD, FACR October 14, 2013 Disclosures I have no disclosures or conflicts of interest to report
TB Nurse Case Management
 TB Nurse Case Management San Antonio, Texas March 2-4, 2011 Pediatric TB Andrea T. Cruz, MD, MPH March 2, 2011 Andrea Cruz, MD, MPH has the following disclosures to make: No conflict of interests No relevant
TB Nurse Case Management San Antonio, Texas March 2-4, 2011 Pediatric TB Andrea T. Cruz, MD, MPH March 2, 2011 Andrea Cruz, MD, MPH has the following disclosures to make: No conflict of interests No relevant
Pediatric Tuberculosis
 Pediatric Tuberculosis Rafael E. Hernandez, MD PhD Attending Physician, Instructor Pediatric Infectious Diseases Seattle Children s Hospital & University of Washington Disclosures No financial conflicts
Pediatric Tuberculosis Rafael E. Hernandez, MD PhD Attending Physician, Instructor Pediatric Infectious Diseases Seattle Children s Hospital & University of Washington Disclosures No financial conflicts
The Diagnosis of Active TB. Deborah McMahan, MD TB Intensive September 28, 2017
 The Diagnosis of Active TB Deborah McMahan, MD TB Intensive September 28, 2017 Agenda Epidemiology Big picture Conditions that Should Make You Suspicious Which test? Eeenie meenie miny mo Radiographic
The Diagnosis of Active TB Deborah McMahan, MD TB Intensive September 28, 2017 Agenda Epidemiology Big picture Conditions that Should Make You Suspicious Which test? Eeenie meenie miny mo Radiographic
TB Intensive San Antonio, Texas
 TB Intensive San Antonio, Texas August 2-5, 2011 Pediatric TB Jeffrey Starke, MD August 5, 2011 Jeffrey Starke, MD has the following disclosures to make: Is on a data safety monitoring board for Hoffman
TB Intensive San Antonio, Texas August 2-5, 2011 Pediatric TB Jeffrey Starke, MD August 5, 2011 Jeffrey Starke, MD has the following disclosures to make: Is on a data safety monitoring board for Hoffman
Diagnosis of tuberculosis in children H Simon Schaaf
 Diagnosis of tuberculosis in children H Simon Schaaf Desmond Tutu TB Centre Department of Paediatrics and Child Health, Stellenbosch University, and Tygerberg Children s Hospital (TCH) Estimated TB incidence
Diagnosis of tuberculosis in children H Simon Schaaf Desmond Tutu TB Centre Department of Paediatrics and Child Health, Stellenbosch University, and Tygerberg Children s Hospital (TCH) Estimated TB incidence
TB is Global. Latent TB Infection (LTBI) Sharing the Care: Working Together. September 24, 2014
 Sharing the Care: Working Together. September 24, 2014") Sharing the Care: Working Together to Meet the Challenge of TB Presented by: Barbara Cole, RN, PHN, MSN Director, Disease Control County of Riverside Department of Public Health Curry International TB
Sharing the Care: Working Together to Meet the Challenge of TB Presented by: Barbara Cole, RN, PHN, MSN Director, Disease Control County of Riverside Department of Public Health Curry International TB
Bronchial syndrome. Atelectasis Draining bronchus Bronchiectasis
 Bronchial syndrome Atelectasis Draining bronchus Bronchiectasis Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology Atelectasis Consequence
Bronchial syndrome Atelectasis Draining bronchus Bronchiectasis Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology Atelectasis Consequence
10/3/2017. Updates in Tuberculosis. Global Tuberculosis, WHO 2015 report. Objectives. Disclosures. I have nothing to disclose
 Disclosures Updates in Tuberculosis I have nothing to disclose Chris Keh, MD Assistant Clinical Professor, Division of Infectious Diseases, UCSF TB Controller, TB Prevention and Control Program, Population
Disclosures Updates in Tuberculosis I have nothing to disclose Chris Keh, MD Assistant Clinical Professor, Division of Infectious Diseases, UCSF TB Controller, TB Prevention and Control Program, Population
Tuberculosis and Diabetes Dec. 10, 2009 Dean Schillinger, M.D. and Gisela Schecter, M.D., M.P.H. 1 of 18
 Screening, Diagnosis, and Treatment of TB in Persons with Diabetes Dean Schillinger, M.D. University of California San Francisco CA Diabetes Program Gisela Schecter, M.D., M.P.H. TB Control Branch CA Department
Screening, Diagnosis, and Treatment of TB in Persons with Diabetes Dean Schillinger, M.D. University of California San Francisco CA Diabetes Program Gisela Schecter, M.D., M.P.H. TB Control Branch CA Department
Drug Interactions Lisa Armitige, MD, PhD November 17, 2010
 Substance Abuse and Tuberculosis Oklahoma City, Oklahoma November 17, 2010 Drug Interactions Lisa Armitige, MD, PhD November 17, 2010 Drug Interactions Lisa Y. Armitige, M.D., Ph.D. Medical Consultant
Substance Abuse and Tuberculosis Oklahoma City, Oklahoma November 17, 2010 Drug Interactions Lisa Armitige, MD, PhD November 17, 2010 Drug Interactions Lisa Y. Armitige, M.D., Ph.D. Medical Consultant