Techniques for Reduction of Larger Breasts
|
|
|
- Olivia Lambert
- 5 years ago
- Views:
Transcription
1 Techniques for Reduction of Larger Breasts Tolbert S. Wilkinson s discussed earlier, circumareolar surgery was initially performed only for smaller mastopexies; in time its use gradually expanded to include smaller and moderate size breast reductions. Steps were taken to prevent an ultimately flat ("pancake") appearance, as well as areolar expansion. This is particularly important in large breast reduction, because the swelling of the tissues following the reduction puts extra pressure on the areola-skin junction. My method of breast reduction is essentially a subcutaneous Pitanguy wedge with resetting of the mammary mound at a higher position. During the presentation of our teaching course at the annual meeting of the merican Society for Plastic and Reconstructive Surgeons, Louis Benelli commented that he uses a superior pedicle technique with his circumareolar "round block" procedure. I believe the Pitanguy wedge, described in detail below, is probably safer, and certainly easier to create. The addition of liposuction must be viewed with some concern. In the past year one of my patients s u f ~ ea rpartial e d areolar loss; this occurred on the side I had liposuctioned to reduce the bulk to match the opposite side. lthough it is possible that a hemorrhage occurred, because the change in areolar perfusion color became apparent by the twelfth hour postsurgery, it may be wise to defer liposuction for a later date in the patients with very large breasts who request a significant tissue mass reduction. When describing the circumareolar reduction to my younger patients, I emphasize that the advantages outweigh the disadvantages. Since scars on the skin of the chest are even more unpredictable in younger than in older patients, and because clothing styles have changed (with patients having an aversion to scars far greater today than when I first entered practice), our patients are usually ready to accept a longer period of remodeling and healing in the periareolar area to avoid the discomfort and possible hypertrophy of the inferior and vertical scars of standard breast reduction. There are certain patients in whom circumareolar mastopexy should not be considered. These include older patients, patients with poor-quality skin, and those impatient individuals who demand that the breast be "presentable" in a short period of time. For these individuals a standard breast reduction is employed. s shown in Fig- 133



2 134 -:- CIRCUMREOLR TECHNIQUES FOR BREST SURGERY Figure 9.1. McKissock reduction. Because it is as easy to do a double pedicle as it is to do a superiorly or inferiorly based single pedicle, I prefer the security of the double pedicle procedure, particularly in patients such as this one. t this breast length, a free nipple graft is not the best choice. Neither is a circumareolar reduction because of the quality of the skin and the size of the circle that would require deepithelialization, although we are now approaching more of this category of patient () with the circle procedure. In (B), the excellent elevation of the areola is shown. Note, however, that even with careful multilayered approximation, thick scars are present in the circumareolar area at 2 years. Experiences such as this one have led me to apply the technique of "internal" reduction with the circumareolar technique to more patients with this degree of breast hypertrophy. If the best bipedicle reduction still requires "touchup" surgery of the periareolar incision, why not avoid incisions elsewhere if one can obtain this degree of projection? B ures 9.1 and 9.2, I prefer a McKissock double pedicle technique, leaving a "thick" pedicle. This preserves a larger number of ducts. On the other hand, the circumareolar technique protects the ducts from injury because the reduction is a lower one-third wedge removal. In older patients the decision must be made between standard reduction and free nipple grafting. Surprisingly, many authors have reported that patients recover sensation in free nipple grafts, and this has been my experience as well. Nevertheless, there remain the possibilities of loss of color and even loss of the graft. In many older patients, recovery of only a portion of sensation is more than adequate; for them the breast is no longer a sexual organ and nipple sensation plays a lesser role in their lifestyle than in the younger patient. Free grafts, therefore, are less risky. The second of my two complications of partial nipple loss occurred 5 days following a circumareolar reduction in a young patient with an extremely long and ptotic breast. In an older patient I would have recommended free nipple grafting. The fact that the partial necrosis occurred after discharge from the hospital and may be attributed to compression or other outside factors is not important at this point; we must strive to make all procedures as complication free
3 9: TECHNIQUES FOR REDUCTION OF LRGER BRESTS -:- 135 as possible. Fortunately, in younger patients, the remaining areola will expand after the debridement and it is easy enough to create a rounded nipple of 4 cm at the appropriate postoperative time. nother argument for the circumareolar reduction technique in the younger patient is the relative security of the nerve supply, because the circumareolar area is deepithelialized only superficially. Our patients have recovered sensation in all cases to date. Preservation of the ducts for later breast feeding is a concern for many modern women. The circumareolar technique by the Pitanguy wedge procedure preserves most of the ductal system. In addition, ducts are not transsected when the nipple is lifted onto the mass of the breast as it is coned and moved upward. The general principles of breast reduction for larger breasts are similar to those of mastopexy and smaller reductions. The measurements first are for a nipple position at the ideal level, some 18 to 19 cm from the sternal notch. When the areola is elevated (Toledo triangle or Texas diamond excision above the areola) the nipple is secure at this position. s noted in Chapter I, I now make the nipple less than 4 cm because there is inevitably some expansion. diameter of 3.8 cm seems to work best. The second measurement from areola to inframammary fold, is also the same as for mastopexy. Because of the greater length involved from the new areolar edge to t h inframammary fold, one leaves additional skin ~ length. In the classic McKissock procedure, one draws the lower limb to be 5 to 6 cm in length. No skin retraction is involved. In the circumareolar technique for large breasts the skin is undermined widely and will retract into the newly elevated inframammary fold, and will shrink as well. For this reason I leave a distance of 8 to 9 cm between the current inframammary fold and the lower edge of the circle. The two points are then joined with an estimate of the amount of skin that must be resected laterally and medially. This circle or oval is then deepithelialized. s noted in Chapter 4, when freeing the breast skin, it is important to dissect in the subcutaneous tissue rather than beneath the dermis. The extra layer of fatty tissue provides a cushion for contour and protects the blood supply in the skin. Once the dissection is carried out to the inframammary fold it is continued medially until the area is reached where the breast begins to join into the sternum. This must be preserved so that the patient does not have an exaggerated separation of the new breasts. The lateral dissection can be carried out all the way to the nine o'clock position. fter removing the Texas triangle and setting the areola, my assistant holds the breast skin away so that the Pitanguy excision can be carried out. This is not only a central wedge, which is varied according to the size, wishes, and requirements of the patient, but a lateral wedge at the inframammary fold to shorten the length of the inverted V. The limbs should be shortened to between 5 and 6 cm to create a proper cone. In contrast to the infolding or overlapping procedure required by other patients, the large breast reduction patient can be corrected by simple closure of the V in layers. Carefullateralliposuction, rather than the direct debulking performed in the McKissock or other pedicle procedures, is usually required. The bottom points of the inverted V are joined and sutured to the underlying pectoralis fascia at an overcorrected position, usually some 2 to 3 cm above the original inframammary fold. dditional inverted and figure-eight sutures of #1 Vicryl continue the coning. Once it is complete, scissors are used to trim any surface irregularities so that a rounded, tall breast mound is left in its new elevated position. t this point we are ready to begin the circumareolar closure. It is certainly more difficult to obtain a smoother contour in these larger patients and one is often tempted to take a "lollipop" wedge of skin. To test the limits of this procedure, I avoided this temptation in the cases that are presented. Taking the wedge will certainly ensure a quicker resolution of the crumpling, but I have found that it is not necessary in the longterm appearance of the nipple, areola, and surrounding skin. Larger breast reduction patients must be prepared to wait 6 to 18 months while this infolded tissue slowly resolves. When the closure is done as described in Chapters 3 and 4, care is taken that the majority of the folded tissue is placed in the lower part of the circle, between the five and seven o'clock positions. The weight

, the horizontal incisions were kept underneath the fold of the breast both medially")

, an area of direct pressure from")
4 136 -:- CIRCUMREOLR TECHNIQUES FOR BREST SURGERY B c Figure 9.2. Standard reduction mammoplasty. The results for standard mastopexy are immediate, predictable, and quite satisfactory. For the younger patient, however, even the shortened horizontal scar as shown will be distressing. In this McKissock bipedicle reduction (, B), the horizontal incisions were kept underneath the fold of the breast both medially and laterally. Unfortunately, this patient is typical in that the scars are still hypertrophic and angry in appearance, despite a regimen of skin care, topical steroids, and occasional scar injections. The circum areolar approach eliminates all but the scars in the center of the breast (C, D), an area of direct pressure from the brassiere (E). Pressure is important in controlling scar hypertrophy, yet it is our experience that the medial and lateral ends of the standard mastopexy scars often require scar revisions, and frequently multiple revisions until a more satisfactory appearance is obtained. D


5 9: TECHNIQUES FOR REDUCTION OF LRGER BRESTS -:- 137 E of the breasts against the brassiere acts as a pressure mechanism to hasten resolution in this area. It is also a less visible zone. Only a minimal amount of skin folding should be visible in the upper circle, between the ten o'clock and two 0' clock positions. s shown in Figure 9. 3, the wedge has been removed and the lateral limbs have been shortened in preparation for suturing. In Figure 9.3B one or two layers of inverted sutures have been placed in the midline and the anchoring sutures horizontally are holding the new cone in its elevated position. Because of natural asymmetries and the vagaries of planning the degree of wedge to be excised, I have often found it necessary to reintroduce a 3-mm liposuction cannula, this time through the drain site, for further reduction on one side or another. s noted above, this must be done carefully. Drains are always necessary and these patients require continued postoperative support. n example of moderate reduction of large breasts is described in Figure 9.4. In closing the area around the areola in the McKissock or other "standard" breast reductions, I place a series of Dexon 4-0 sutures in the deep subcutaneous tissue to bring the edges together. Because there is no deepithelialized ring, a circle Benelli-type double suture is not necessary and would not help. Tacking stitches are used more frequently than with circle closures, and are usually of the half-buried variety tied loosely on the areolar skin. If a stitch mark should result, it mimicks the appearance of the Montgomery gland. There is still drainage from the edges, however, and the Mesh tape described in the caption to Figure 9.2E is useful. This tape may be applied 24 hr after the breast reduction to immobilize the skin and the areola and yet allow drainage into the overlying dressing. I commonly leave this tape in place for 10 to 12 days. In 1969, when I was a resident in plastic surgery at St. Louis University (St. Louis, MO), I developed Mesh tape as a means of immobilizing skin grafts. With a grant from the 3M Company a commercial preparation of Mesh tape followed and it was made available to other surgeons for
 The deepithelialized area is designed so that the nipple-areolar complex may be brought upward to its new position.")
6 138 -:- CIRCUMREOLR TECHNIQUES FOR BREST SURGERY Figure 9.3. Reduction of the large breast is essentially the same as for the smaller breast. () The deepithelialized area is designed so that the nipple-areolar complex may be brought upward to its new position. This is only a partial-thickness soft tissue excision, leaving the majority of the blood supply intact over the upper two thirds of the breast. With the skin reflected, a Pitanguy wedge is excised. In (B), the left and right sides have been trimmed to an appropriate length based on the position of the now secured nippleareolar complex. This distance should measure 5 to 6 cm. nchoring sutures are then used to secure the lower edges to the pectoralis fascia and a series of imbricating sutures are used to secure the cone shape beneath the skin.

 anesthesia.")
7 9: TECHNIQUES FOR REDUCTION OF LRGER BRESTS -:- 139 Figure 9.4. Major breast reduction in an older patient. Fortunately, this patient requested that her breasts be reduced only moderately. Because of her large bone structure and perhaps as a response to her recent abdominoplasty and major liposuction of the lower body, she had requested that her breasts be left in a fairly large state. () Note the extreme width of the deepitheialization and the wide Texas diamond that will be removed from each areola. This patient's reduction was performed as a demonstration surgery under ketaminediazepam (Valium) anesthesia. One error was made in that we did not drain and a seroma developed on the left side some 10 days postoperatively, resulting in extrusion of the Mersilene suture and a moderate amount of swelling medially. The patient was so pleased with the results (B) that she would not allow the final adjustment, which would include minor liposuction and a revision of the left-side scar. B




8 140 -:- CIRCUMREOLR TECHNIQUES FOR BREST SURGERY B Figure 9.5. Markings for large breast reduction. See text for details. c mobilization of skin grafts and finger tip replacements, where it has proved its worth. Markings for Larger Breast Reductions The markings for breast reduction are essentially the same as for smaller reductions and mastopexy, with the addition of a marking for liposuction of the axilla and the area posterior to the anterior axillary line. s shown in Figure 9.5-C, the initial measurements from the sternal notch and the midclavicle are made and then a visual adjustment is considered. On this patient's left side this resulted in lowering the new nipple position below the measured position. Notice also the differences to account for asymmetry and that the areolar size has been reduced to less than 4.0cm. The second marking is made at a distance 9 cm from the inframammary fold in the midline. These points are then connected with either an ellipse, as shown on the patient's left (Figure 9.5C), or circle, as shown on the patient's right (Figure 9.5B). This is the area that will be deepithelialized. The distance between the top of the circle and the edge of the new areola will be




9 9: TECHNIQUES FOR REDUCTION OF LRGER BRESTS -:- 141 Figure 9.6. Moderate reduction of larger breasts, using the circumareolar technique. (, B) Patient c.y.; (C, D) patient C.S. B C
10 142 -:- CIRCUMREOLR TECHNIQUES FOR BREST SURGERY excised to a depth of 1 cm so that the new areola will be fixed at this preferred position. s described, I now make this nipple position exactly the same as would be selected for a McKissock or other pedicle flap reduction, because the danger of "star gazing" has not materialized in this series of circumareolar reductions. Moderate Circumareolar Reductions in Young Women With Large Breasts Our experience with large reductions, using the circumareolar technique, came as a result of requests from patients; these patients wanted breast reduction without scars that would rub on brassieres or bikini tops. Patients c.y. and c.s. (Figure 9.6), who typify these patients, desired initially only a modest reduction in volume. Because their skin quality was excellent, I decided to try the circumareolar technique with only a moderate amount of liposuction adjustment (liposuction has made this technique even more effective). Patient c.y. is shown preoperatively in 1989 (Figure 9.6) and 5 months postoperatively (Figure 9.6B). The shape conformed to her wishes for a modest reduction. We have received reports that the shape has remained the same and that the wrinkling has since disappeared. Notice in her lateral view (Figure 9.6B) that the breast retains a cone shape, from the internal wedge resection and cone formation with resetting of the inframammary fold. In this initial group of moderate circumareolar reductions, I was more concerned with subsequent areolar lifting to an unacceptable position and purposely placed the areola at a somewhat lower spot. Note the difference in patient C. S., who had a modest reduction in 1990 (Figure 9.6C and D), and for whom a higher areolar position was chosen (Figure 9.6D). When Not to Use a Circumareolar Reduction I am not comfortable with circumareolar reduction of massively enlarged breasts (e.g., Figure 9.7) or of breasts that have multiple stretch marks, which indicate a poor quality of skin retraction and dermal blood supply. In 1983, the patient L.S. (Figure 9.7) asked for a premarital breast reduction. t age 23, her breasts had reached a size that caused her considerable symptomatology. Notice the strap marks on her shoulders and the relative symmetry of the breast enlargement. We used a standard McKissock reduction and changed her to a small C cup. Nine years later, she presented with the problem shown in Figure 9.7F-G. Her breasts had continued to enlarge almost from the day of the operation. When this amount of tissue has regenerated, it is advisable to remove the nipple and replace it as a free nipple graft, and completely remove the ductal system at the same time. This is not a 100% guarantee against recurrence of virginal hypertrophy but it certainly should reduce the risk. t 6 months, her breasts have retained the size and shape that we recreated. Note in the preoperative drawings (Figures 9.7D and E) that liposuction will be used in the anterior axillary line area. The long incision is placed to meet the original long incision from Today, we keep these incisions shorter, even in the larger patients, because the "dog ear" that is located beneath the breast fold will flatten nicely with time.
 Patient J.S.")
 The same patient in 1992.")
11 9: TECHNIQUES FOR REDUCTION OF LRGER BRESTS -:- 143 B c Figure 9.7. (-C) Patient J.S. in 1988; her breasts were reduced using the standard McKissock technique. (D-G) The same patient in See text for details. D
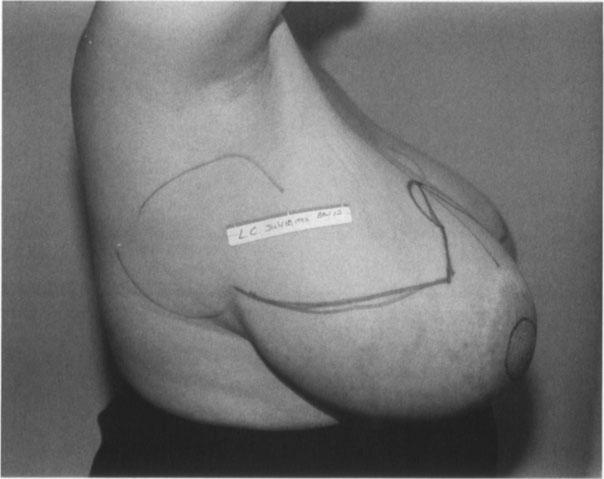
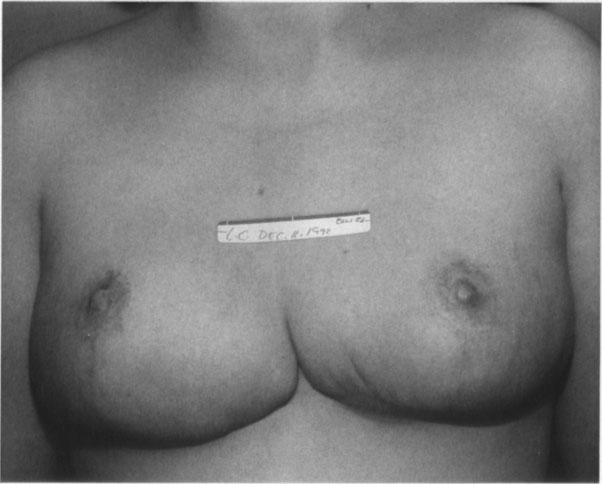
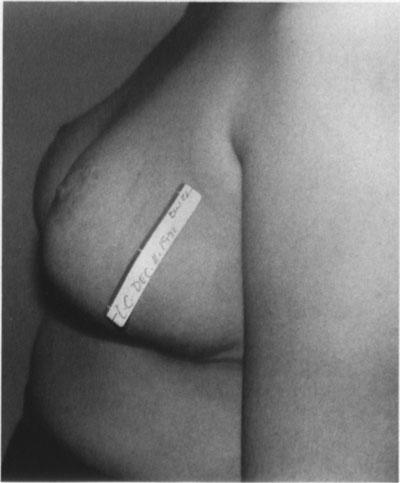
12 144 -:- CIRCUMREOLR TECHNIQUES FOR BREST SURGERY Figure 9.7. Continued E F ;;.;::... G
Circumareolar Mastopexy
 Circumareolar Mastopexy and Moderate Reduction drien iache n mastopexy the problems created by the doughnut-type excision and scarring are relatively minimal, because the breast tissue is not excised and
Circumareolar Mastopexy and Moderate Reduction drien iache n mastopexy the problems created by the doughnut-type excision and scarring are relatively minimal, because the breast tissue is not excised and
The Circumareolar Procedures
 The Circumareolar Procedures Tolbert S. Wilkinson Like most American surgeons, my interest in the circumareolar technique was stimulated by the presentation and then publication on a new mastopexy operation
The Circumareolar Procedures Tolbert S. Wilkinson Like most American surgeons, my interest in the circumareolar technique was stimulated by the presentation and then publication on a new mastopexy operation
AESTHETIC SURGERY OF THE BREAST: MASTOPEXY, AUGMENTATION & REDUCTION
 CHAPTER 18 AESTHETIC SURGERY OF THE BREAST: MASTOPEXY, AUGMENTATION & REDUCTION Ali A. Qureshi, MD and Smita R. Ramanadham, MD Aesthetic surgery of the breast aims to either correct ptosis with a mastopexy,
CHAPTER 18 AESTHETIC SURGERY OF THE BREAST: MASTOPEXY, AUGMENTATION & REDUCTION Ali A. Qureshi, MD and Smita R. Ramanadham, MD Aesthetic surgery of the breast aims to either correct ptosis with a mastopexy,
Breast Reduction By Dr. Tarek Ahmed Said Professor of Plastic Surgery Cairo University 2017
 Breast Reduction By Dr. Tarek Ahmed Said Professor of Plastic Surgery Cairo University 2017 Reduction Mammaplasty SAFE Good Size Reduction Minimal Scar Aesthetic & Long Lasting Breast Shape Reduction Mammaplasty
Breast Reduction By Dr. Tarek Ahmed Said Professor of Plastic Surgery Cairo University 2017 Reduction Mammaplasty SAFE Good Size Reduction Minimal Scar Aesthetic & Long Lasting Breast Shape Reduction Mammaplasty
Breast Lift
 Breast Lift Changes to the breasts can be dissatisfying and make a woman feel as if she is losing her femininity and youthfulness. Over time, factors such as age, genetics, pregnancy and breast feeding,
Breast Lift Changes to the breasts can be dissatisfying and make a woman feel as if she is losing her femininity and youthfulness. Over time, factors such as age, genetics, pregnancy and breast feeding,
ONCOPLASTIC SURGERY. Dr. Sadir Alrawi Director of Surgical Oncology Services. Dr. Humaa Darr Surgical Oncology Fellow
 Hessa St ONCOPLASTIC SURGERY Dr. Sadir Alrawi Director of Surgical Oncology Services Dr. Humaa Darr Surgical Oncology Fellow Al Sufouh Rd AL SUFOUH AL SUFOUH Sharaf DG Mall of the Emirates Mall Of the
Hessa St ONCOPLASTIC SURGERY Dr. Sadir Alrawi Director of Surgical Oncology Services Dr. Humaa Darr Surgical Oncology Fellow Al Sufouh Rd AL SUFOUH AL SUFOUH Sharaf DG Mall of the Emirates Mall Of the
Superior Pedicle Vertical Scar Mammaplasty: Surgical Technique
 Superior Pedicle Vertical Scar Mammaplasty: Surgical Technique 4 Foad Nahai A man honours himself by not displaying all the knowledge he has acquired. Folk Tradition Introduction I first tried the vertical
Superior Pedicle Vertical Scar Mammaplasty: Surgical Technique 4 Foad Nahai A man honours himself by not displaying all the knowledge he has acquired. Folk Tradition Introduction I first tried the vertical
Vertical mammaplasty has been developed
 BREAST Y-Scar Vertical Mammaplasty David A. Hidalgo, M.D. New York, N.Y. Background: Vertical mammaplasty is an effective alternative to inverted-t methods. Among other benefits, it results in a significantly
BREAST Y-Scar Vertical Mammaplasty David A. Hidalgo, M.D. New York, N.Y. Background: Vertical mammaplasty is an effective alternative to inverted-t methods. Among other benefits, it results in a significantly
Breast Reduction
 Breast Reduction Breasts that are excessively large in proportion to body size are a frequent cause of back and neck pain as well as shoulder irritation from bra straps. Additionally, sleep and participation
Breast Reduction Breasts that are excessively large in proportion to body size are a frequent cause of back and neck pain as well as shoulder irritation from bra straps. Additionally, sleep and participation
Augmentation of the Ptotic Breast: Simultaneous Periareolar Mastopexy/Breast Augmentation By: Laurence Kirwan, M.D., F.R.C.S
 Augmentation of the Ptotic Breast: Simultaneous Periareolar Mastopexy/Breast Augmentation By: Laurence Kirwan, M.D., F.R.C.S Background: Submusculofascial augmentation of the ptotic breast can result in
Augmentation of the Ptotic Breast: Simultaneous Periareolar Mastopexy/Breast Augmentation By: Laurence Kirwan, M.D., F.R.C.S Background: Submusculofascial augmentation of the ptotic breast can result in
Breast Reconstruction Postmastectomy. Using DermaMatrix Acellular Dermis in breast reconstruction with tissue expander.
 Breast Reconstruction Postmastectomy. Using DermaMatrix Acellular Dermis in breast reconstruction with tissue expander. Strong and flexible Bacterially inactivated Provides implant support Breast Reconstruction
Breast Reconstruction Postmastectomy. Using DermaMatrix Acellular Dermis in breast reconstruction with tissue expander. Strong and flexible Bacterially inactivated Provides implant support Breast Reconstruction
Cosmetic Surgery: Breast Reduction
 PROCEDURE FACT SHEET PLASTIC SURGERY Cosmetic Surgery: Breast Reduction This guide is for women who are considering having an operation to lift their breasts. We advise that you talk to a plastic surgeon
PROCEDURE FACT SHEET PLASTIC SURGERY Cosmetic Surgery: Breast Reduction This guide is for women who are considering having an operation to lift their breasts. We advise that you talk to a plastic surgeon
Breast reduction surgery reduction mammaplasty Is it right for me? What to expect during your consultation Be prepared to discuss:
 This guide is for women who are considering having an operation to lift their breasts. We advise that you talk to a plastic surgeon and only use this information as a guide to the procedure. Breast reduction
This guide is for women who are considering having an operation to lift their breasts. We advise that you talk to a plastic surgeon and only use this information as a guide to the procedure. Breast reduction
Superomedial Pedicle Reduction with Short Scar
 Superomedial Pedicle Reduction with Short Scar Scott L. Spear, M.D., F.A.C.S., 1 Steven P. Davison, M.D., D.D.S., F.A.C.S., 1 and Ivan Ducic, M.D., Ph.D. 1 ABSTRACT Reduction mammaplasty combining a superomedial
Superomedial Pedicle Reduction with Short Scar Scott L. Spear, M.D., F.A.C.S., 1 Steven P. Davison, M.D., D.D.S., F.A.C.S., 1 and Ivan Ducic, M.D., Ph.D. 1 ABSTRACT Reduction mammaplasty combining a superomedial
Despite breast reduction being one of the BREAST. Does Knowledge of the Initial Technique Affect Outcomes after Repeated Breast Reduction?
 BREAST Does Knowledge of the Initial Technique Affect Outcomes after Repeated Breast Reduction? Jamil Ahmad, M.D. Sarah M. McIsaac, M.D. Frank Lista, M.D. Mississauga and Ottawa, Ontario, Canada Background:
BREAST Does Knowledge of the Initial Technique Affect Outcomes after Repeated Breast Reduction? Jamil Ahmad, M.D. Sarah M. McIsaac, M.D. Frank Lista, M.D. Mississauga and Ottawa, Ontario, Canada Background:
COSMETIC SURGERY: BREAST LIFT (MASTOPEXY)
") PROCEDURE FACT SHEET PLASTIC SURGERY COSMETIC SURGERY: BREAST LIFT (MASTOPEXY) This guide is for women who are considering having an operation to lift their breasts. We advise that you talk to a plastic
PROCEDURE FACT SHEET PLASTIC SURGERY COSMETIC SURGERY: BREAST LIFT (MASTOPEXY) This guide is for women who are considering having an operation to lift their breasts. We advise that you talk to a plastic
BREAST AUGMENTATION TECHNIQUES
 BREAST AUGMENTATION TECHNIQUES Breast Augmentation Top Surgical Procedure in 2015 (Worldwide) Surgical Procedure : Breast Augmentation Rank : 1 Total : 1,488,992 Percent of Total Surgical Procedures :
BREAST AUGMENTATION TECHNIQUES Breast Augmentation Top Surgical Procedure in 2015 (Worldwide) Surgical Procedure : Breast Augmentation Rank : 1 Total : 1,488,992 Percent of Total Surgical Procedures :
Evolution of the Vertical Reduction Mammaplasty
 CME Evolution of the Vertical Reduction Mammaplasty Scott L. Spear, M.D., and Michael A. Howard, M.D. Washington, D.C. Learning Objectives: After studying this article, the participant should be able to:
CME Evolution of the Vertical Reduction Mammaplasty Scott L. Spear, M.D., and Michael A. Howard, M.D. Washington, D.C. Learning Objectives: After studying this article, the participant should be able to:
Oncoplastic Breast Surgery
 Disclosures Oncoplastic Breast Surgery Newfoundlander OAGS 2016 Dr Renee Hanrahan General Surgeon Oncologic and Reconstructive Breast Surgeon Objectives What is Oncoplastic Surgery Define Oncoplastic Surgery
Disclosures Oncoplastic Breast Surgery Newfoundlander OAGS 2016 Dr Renee Hanrahan General Surgeon Oncologic and Reconstructive Breast Surgeon Objectives What is Oncoplastic Surgery Define Oncoplastic Surgery
Modified ''Lejour Technique'': A Safe Option for Large Breasts Reductions
 Egypt, J. Plast. Reconstr. Surg., Vol. 34, No. 1, January: 1-7, 2010 Modified ''Lejour Technique'': A Safe Option for Large Breasts Reductions KARIM KHALIL EL-LAMIE, M.D. The Department of Plastic Surgery,
Egypt, J. Plast. Reconstr. Surg., Vol. 34, No. 1, January: 1-7, 2010 Modified ''Lejour Technique'': A Safe Option for Large Breasts Reductions KARIM KHALIL EL-LAMIE, M.D. The Department of Plastic Surgery,
Frederick J. Duffy, Jr., MD, FACS and Brice W. McKane, MD, FACS BREAST RECONSTRUCTION
 Frederick J. Duffy, Jr., MD, FACS and Brice W. McKane, MD, FACS BREAST RECONSTRUCTION BREAST RECONSTRUCTION: A WOMAN S DECISION Options and Information Our approach to breast reconstruction entails a very
Frederick J. Duffy, Jr., MD, FACS and Brice W. McKane, MD, FACS BREAST RECONSTRUCTION BREAST RECONSTRUCTION: A WOMAN S DECISION Options and Information Our approach to breast reconstruction entails a very
The ideal reduction mammaplasty should produce. Eliminating the Vertical Scar in Breast Reduction Boston Modification of the Robertson Technique
 Eliminating the Vertical Scar in Breast Reduction Boston Modification of the Robertson Technique Kiya Movassaghi, MD, DMD; Eric C. Liao, MD, PhD; Vivian Ting, MD; Evan Matros, MD; Donald J. Morris, MD;
Eliminating the Vertical Scar in Breast Reduction Boston Modification of the Robertson Technique Kiya Movassaghi, MD, DMD; Eric C. Liao, MD, PhD; Vivian Ting, MD; Evan Matros, MD; Donald J. Morris, MD;
Tips for using shaped implants in breast augmentation
 Tips for using shaped implants in breast augmentation Sientra would like to thank Dr. Patricia McGuire of St. Louis, MO for her significant contributions to Sientra s educational efforts. Dr. McGuire has
Tips for using shaped implants in breast augmentation Sientra would like to thank Dr. Patricia McGuire of St. Louis, MO for her significant contributions to Sientra s educational efforts. Dr. McGuire has
Breast Augmentation - Silicone Implants
 Breast Augmentation - Silicone Implants Breast augmentation, or augmentation mammoplasty, is one of the most common plastic surgery procedures performed today. Over time, factors such as age, genetics,
Breast Augmentation - Silicone Implants Breast augmentation, or augmentation mammoplasty, is one of the most common plastic surgery procedures performed today. Over time, factors such as age, genetics,
Breast Reduction Surgery Houston
 Breast Houston Reduction Surgery Breast Reduction Surgery by Houston Board Certified Plastic Surgeon Breast Reduction Surgery Houston Breast Reduction surgery is a very satisfying procedure. Heavy, large,
Breast Houston Reduction Surgery Breast Reduction Surgery by Houston Board Certified Plastic Surgeon Breast Reduction Surgery Houston Breast Reduction surgery is a very satisfying procedure. Heavy, large,
Strattice Reconstructive Tissue Matrix used in the repair of rippling
 Clinical case study Strattice Tissue Matrix Strattice Reconstructive Tissue Matrix used in the repair of rippling Steven Teitelbaum, MD* Santa Monica, CA Case summary A 48-year-old woman with a history
Clinical case study Strattice Tissue Matrix Strattice Reconstructive Tissue Matrix used in the repair of rippling Steven Teitelbaum, MD* Santa Monica, CA Case summary A 48-year-old woman with a history
COSMETIC SURGERY: BREAST REDUCTION FOR MEN (GYNAECOMASTIA)
") PROCEDURE FACT SHEET PLASTIC SURGERY COSMETIC SURGERY: BREAST REDUCTION FOR MEN (GYNAECOMASTIA) This is a guide for men who are considering having a breast reduction operation. We advise that you talk
PROCEDURE FACT SHEET PLASTIC SURGERY COSMETIC SURGERY: BREAST REDUCTION FOR MEN (GYNAECOMASTIA) This is a guide for men who are considering having a breast reduction operation. We advise that you talk
Autoaugmentation Mastopexy with an Inferior-Based Pedicle
 Aesth Plast Surg (2009) 33:302 307 DOI 10.1007/s00266-009-9310-7 ORIGINAL ARTICLE Autoaugmentation Mastopexy with an Inferior-Based Pedicle Johannes Franz Hönig Æ Hans Peter Frey Æ Frank Michael Hasse
Aesth Plast Surg (2009) 33:302 307 DOI 10.1007/s00266-009-9310-7 ORIGINAL ARTICLE Autoaugmentation Mastopexy with an Inferior-Based Pedicle Johannes Franz Hönig Æ Hans Peter Frey Æ Frank Michael Hasse
Breast Reduction. Multimedia Health Education
 This movie is an educational resource only and should not be used to make a decision on Breast Reduction. All decisions about Breast Reduction and management of Breast Conditions must be made in conjunction
This movie is an educational resource only and should not be used to make a decision on Breast Reduction. All decisions about Breast Reduction and management of Breast Conditions must be made in conjunction
An estimated 40,000 breast reduction procedures were performed in the United. The Common Principles of Effective Breast Reduction Techniques
 Special Topic Alexandre de Souza, MD; and Renato Saltz, MD Background: The evolution of breast reduction surgery is discussed to shed light on the various principles and techniques used in this 4-step
Special Topic Alexandre de Souza, MD; and Renato Saltz, MD Background: The evolution of breast reduction surgery is discussed to shed light on the various principles and techniques used in this 4-step
Intra-Capsular Versus Extra-Capsular Breast Mastopexy of Previously Augmented Breast
 Original Hela Article et al. 301 Intra-Capsular Versus Extra-Capsular Breast Mastopexy of Previously Augmented Breast Hesham A. Helal*, Asser El-Hilaly, Nahed Samir Boughdadi Department of Plastic and
Original Hela Article et al. 301 Intra-Capsular Versus Extra-Capsular Breast Mastopexy of Previously Augmented Breast Hesham A. Helal*, Asser El-Hilaly, Nahed Samir Boughdadi Department of Plastic and
Your comprehensive guide to BREAST LIFT SURGERY. (07) cosmedic.com.au
 cosmedic.com.au") Your comprehensive guide to BREAST LIFT SURGERY (07) 5588 4777 cosmedic.com.au Breast Lift Surgery Breast lift, or Mastopexy, is designed to recreate the appearance of firm and more youthful breasts. Whether
Your comprehensive guide to BREAST LIFT SURGERY (07) 5588 4777 cosmedic.com.au Breast Lift Surgery Breast lift, or Mastopexy, is designed to recreate the appearance of firm and more youthful breasts. Whether
Mommy Makeover
 Mommy Makeover Many women experience significant physical changes following pregnancy and breast-feeding, many of which can be persistent and difficult to correct with diet and exercise alone. Changes
Mommy Makeover Many women experience significant physical changes following pregnancy and breast-feeding, many of which can be persistent and difficult to correct with diet and exercise alone. Changes
INFORMATION SHEET MODIFIED (MINI) ABDOMINOPLASTY
 ABDOMINOPLASTY") INFORMATION SHEET MODIFIED (MINI) ABDOMINOPLASTY INTRODUCTION There is not much which is mini about a mini-abdominoplasty because it can take as long and can be as complicated as a standard abdominoplasty
INFORMATION SHEET MODIFIED (MINI) ABDOMINOPLASTY INTRODUCTION There is not much which is mini about a mini-abdominoplasty because it can take as long and can be as complicated as a standard abdominoplasty
Lancashire Teaching Hospitals NHS Foundation Trust Information for Patients having a Breast Reduction Operation
 Lancashire Teaching Hospitals NHS Foundation Trust Information for Patients having a Breast Reduction Operation Plastic Surgery Department Leaflet Number 2 Produced: October 2007 Review date: October 2010
Lancashire Teaching Hospitals NHS Foundation Trust Information for Patients having a Breast Reduction Operation Plastic Surgery Department Leaflet Number 2 Produced: October 2007 Review date: October 2010
Breast Augmentation - Saline Implants
 Breast Augmentation - Saline Implants Breast augmentation, or augmentation mammoplasty, is one of the most common plastic surgery procedures performed today. Over time, factors such as age, genetics, pregnancy,
Breast Augmentation - Saline Implants Breast augmentation, or augmentation mammoplasty, is one of the most common plastic surgery procedures performed today. Over time, factors such as age, genetics, pregnancy,
No Drain Abdominoplasty: No More Excuses. Karol A Gutowski, MD, FACS
 No Drain Abdominoplasty: No More Excuses Karol A Gutowski, MD, FACS Disclosures NO financial interests in any suture company Will use brand names due to lack of distinguishing generic names Objectives
No Drain Abdominoplasty: No More Excuses Karol A Gutowski, MD, FACS Disclosures NO financial interests in any suture company Will use brand names due to lack of distinguishing generic names Objectives
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 4,100 116,000 120M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 4,100 116,000 120M Open access books available International authors and editors Downloads Our
CONSENT FOR GYNECOMASTIA
 CONSENT FOR GYNECOMASTIA Gynecomastia surgery is a procedure to remove excess fat, glandular tissue and/or skin from overdeveloped or enlarged male breasts. In severe cases of gynecomastia, the weight
CONSENT FOR GYNECOMASTIA Gynecomastia surgery is a procedure to remove excess fat, glandular tissue and/or skin from overdeveloped or enlarged male breasts. In severe cases of gynecomastia, the weight
Application of the Lalonde (horizontal-only scar) breast reduction technique for correction of gynaecomastia in dark skinned patients
 breast reduction technique for correction of gynaecomastia in dark skinned patients") Case Report Application of the Lalonde (horizontal-only scar) breast reduction technique for correction of gynaecomastia in dark skinned patients Fawz Kazzazi 1, Charles M. Malata 2,3,4 1 School of Clinical
Case Report Application of the Lalonde (horizontal-only scar) breast reduction technique for correction of gynaecomastia in dark skinned patients Fawz Kazzazi 1, Charles M. Malata 2,3,4 1 School of Clinical
Breast conservation surgery and sentinal node biopsy: Dr R Botha Moderator: Dr E Osman
 Breast conservation surgery and sentinal node biopsy: Dr R Botha Moderator: Dr E Osman Breast anatomy: Breast conserving surgery: The aim of wide local excision is to remove all invasive and in situ
Breast conservation surgery and sentinal node biopsy: Dr R Botha Moderator: Dr E Osman Breast anatomy: Breast conserving surgery: The aim of wide local excision is to remove all invasive and in situ
Barbed Sutures in Progressive Tension Suture Technique Abdominoplasty. Karol A Gutowski, MD
 Barbed Sutures in Progressive Tension Suture Technique Abdominoplasty Karol A Gutowski, MD 1 Disclosures Speakers Bureau for AngioTech since April 2011 (Makers of Quill bi-directional barbed sutures) Technique
Barbed Sutures in Progressive Tension Suture Technique Abdominoplasty Karol A Gutowski, MD 1 Disclosures Speakers Bureau for AngioTech since April 2011 (Makers of Quill bi-directional barbed sutures) Technique
Reconstruction of the Breast after Cancer An Overview of Procedures and Options by Karen M. Horton, MD, MSc, FRCSC
 Downloaded from Reconstruction of the Breast after Cancer An Overview of Procedures and Options by Karen M. Horton, MD, MSc, FRCSC What is Breast Reconstruction? Reconstruction of the breast involves recreating
Downloaded from Reconstruction of the Breast after Cancer An Overview of Procedures and Options by Karen M. Horton, MD, MSc, FRCSC What is Breast Reconstruction? Reconstruction of the breast involves recreating
Breast Augmentation and Mastopexy Using a Pectoral Muscle Loop
 Aesth Plast Surg (2011) 35:333 340 DOI 10.1007/s00266-010-9612-9 ORIGINAL ARTICLE Breast Augmentation and Mastopexy Using a Pectoral Muscle Loop André Auersvald Luiz Augusto Auersvald Received: 28 April
Aesth Plast Surg (2011) 35:333 340 DOI 10.1007/s00266-010-9612-9 ORIGINAL ARTICLE Breast Augmentation and Mastopexy Using a Pectoral Muscle Loop André Auersvald Luiz Augusto Auersvald Received: 28 April
The vertical reduction mammaplasty was first
 Special Topic Technical Refinements of the Vertical Mammaplasty: A Modified Lejour Approach Steven G. Wallach, MD Dr. Wallach is Assistant Clinical Professor of Plastic Surgery, Albert Einstein College
Special Topic Technical Refinements of the Vertical Mammaplasty: A Modified Lejour Approach Steven G. Wallach, MD Dr. Wallach is Assistant Clinical Professor of Plastic Surgery, Albert Einstein College
INFORMED CONSENT-BREAST RECONSTRUCTION WITH TRAM ABDOMINAL MUSCLE FLAP
 INFORMED CONSENT-BREAST RECONSTRUCTION WITH TRAM ABDOMINAL MUSCLE FLAP 2000 American Society of Plastic Surgeons. Purchasers of the Patient Consultation Resource Book are given a limited license to modify
INFORMED CONSENT-BREAST RECONSTRUCTION WITH TRAM ABDOMINAL MUSCLE FLAP 2000 American Society of Plastic Surgeons. Purchasers of the Patient Consultation Resource Book are given a limited license to modify
What are the different techniques used for chest surgery?
 Chest Surgery Chest surgery is a gender-affirming, masculinizing, top surgery that removes breast* tissue and forms remaining tissue into a shape that is typically considered to be more masculine. What
Chest Surgery Chest surgery is a gender-affirming, masculinizing, top surgery that removes breast* tissue and forms remaining tissue into a shape that is typically considered to be more masculine. What
No Drain Abdominoplasty: No More Excuses. Karol A Gutowski, MD, FACS Instructional Course
 No Drain Abdominoplasty: No More Excuses Karol A Gutowski, MD, FACS Instructional Course Disclosures Angiotech/Surgical Specialties - Advisory Board AxcelRx Pharmacuticals - Advisory Board Suneva Medical
No Drain Abdominoplasty: No More Excuses Karol A Gutowski, MD, FACS Instructional Course Disclosures Angiotech/Surgical Specialties - Advisory Board AxcelRx Pharmacuticals - Advisory Board Suneva Medical
cally, a distinct superior crease of the forehead marks this spot. The hairline and
 4 Forehead The anatomical boundaries of the forehead unit are the natural hairline (in patients without alopecia), the zygomatic arch, the lower border of the eyebrows, and the nasal root (Fig. 4.1). The
4 Forehead The anatomical boundaries of the forehead unit are the natural hairline (in patients without alopecia), the zygomatic arch, the lower border of the eyebrows, and the nasal root (Fig. 4.1). The
Medial Pedicle Reduction Mammaplasty for Severe Mammary Hypertrophy
 Medial Pedicle Reduction Mammaplasty for Severe Mammary Hypertrophy Maurice Y. Nahabedian, M.D., Bernard M. McGibbon, M.D., and Paul N. Manson, M.D. Baltimore, Md. Current options in reduction mammaplasty
Medial Pedicle Reduction Mammaplasty for Severe Mammary Hypertrophy Maurice Y. Nahabedian, M.D., Bernard M. McGibbon, M.D., and Paul N. Manson, M.D. Baltimore, Md. Current options in reduction mammaplasty
No Drain Abdominoplasty with Progressive Tension Sutures. Karol A Gutowski, MD, FACS
 No Drain Abdominoplasty with Progressive Tension Sutures Karol A Gutowski, MD, FACS Disclosures Suneva Medical Instructor Merz Advisory Board NO financial interests in any suture company Will use brand
No Drain Abdominoplasty with Progressive Tension Sutures Karol A Gutowski, MD, FACS Disclosures Suneva Medical Instructor Merz Advisory Board NO financial interests in any suture company Will use brand
Reduction Mammoplasty Operative Techniques for Improved Outcomes in the Treatment of Gigantomastia
 Reduction Mammoplasty Operative Techniques for Improved Outcomes in the Treatment of Gigantomastia Brent R. DeGeorge, Jr., MD, PhD, David L. Colen, MD, Alexander F. Mericli, MD, and David B. Drake, MD
Reduction Mammoplasty Operative Techniques for Improved Outcomes in the Treatment of Gigantomastia Brent R. DeGeorge, Jr., MD, PhD, David L. Colen, MD, Alexander F. Mericli, MD, and David B. Drake, MD
Acta Medica Okayama OCTOBER Mastectomy in Female-to-male Transsexuals. Yuzaburo Namba Toshiyuki Watanabe Yoshihiro Kimata
 Acta Medica Okayama Volume 63, Issue 5 2009 Article 4 OCTOBER 2009 Mastectomy in Female-to-male Transsexuals Yuzaburo Namba Toshiyuki Watanabe Yoshihiro Kimata Department of Plastic and Reconstructive
Acta Medica Okayama Volume 63, Issue 5 2009 Article 4 OCTOBER 2009 Mastectomy in Female-to-male Transsexuals Yuzaburo Namba Toshiyuki Watanabe Yoshihiro Kimata Department of Plastic and Reconstructive
Breast Reconstruction Options
 Breast Reconstruction Options Natural reconstruction using your ABDOMINAL tissue: TRAM Flap (Transverse Rectus Abdominis Myocutaneous) There are various forms of TRAM flap reconstruction that are commonly
Breast Reconstruction Options Natural reconstruction using your ABDOMINAL tissue: TRAM Flap (Transverse Rectus Abdominis Myocutaneous) There are various forms of TRAM flap reconstruction that are commonly
CONSENT FOR MASTOPEXY / BREAST REDUCTION SURGERY
 CONSENT FOR MASTOPEXY / BREAST REDUCTION SURGERY Breast Reduction or Reduction Mammoplasty Surgery is performed for both functional and cosmetic reasons. Women who have large breasts may experience a variety
CONSENT FOR MASTOPEXY / BREAST REDUCTION SURGERY Breast Reduction or Reduction Mammoplasty Surgery is performed for both functional and cosmetic reasons. Women who have large breasts may experience a variety
Essential Anatomy for oncoplastic surgery. Omar Z. Youssef M.D Professor of surgical oncology NCI- Cairo University
 Essential Anatomy for oncoplastic surgery Omar Z. Youssef M.D Professor of surgical oncology NCI- Cairo University Introduction Rationale for anatomical basis for OPS Anatomical considerations: 1. Surface
Essential Anatomy for oncoplastic surgery Omar Z. Youssef M.D Professor of surgical oncology NCI- Cairo University Introduction Rationale for anatomical basis for OPS Anatomical considerations: 1. Surface
Kevin T. Kavanagh, MD
 Kevin T. Kavanagh, MD Axial Based upon a named artery. Survival length depends upon the artery not the width of the flap. Random Has random unnamed vessels supplying it. Survival length is directly proportional
Kevin T. Kavanagh, MD Axial Based upon a named artery. Survival length depends upon the artery not the width of the flap. Random Has random unnamed vessels supplying it. Survival length is directly proportional
Selective salvage of zones 2 and 4 in the pedicled TRAM flap: a focus on reducing fat necrosis and improving aesthetic outcomes
 DOI 10.1186/s40064-016-1714-7 RESEARCH Open Access Selective salvage of zones 2 and 4 in the pedicled TRAM flap: a focus on reducing fat necrosis and improving aesthetic outcomes Chi Sun Yoon and Kyu Nam
DOI 10.1186/s40064-016-1714-7 RESEARCH Open Access Selective salvage of zones 2 and 4 in the pedicled TRAM flap: a focus on reducing fat necrosis and improving aesthetic outcomes Chi Sun Yoon and Kyu Nam
Breast Reconstruction. Westmead Breast Cancer Institute
 Breast Reconstruction Westmead Breast Cancer Institute What is breast reconstruction? Breast reconstruction is a surgical procedure that creates a shape on the chest wall following a mastectomy. Occasionally,
Breast Reconstruction Westmead Breast Cancer Institute What is breast reconstruction? Breast reconstruction is a surgical procedure that creates a shape on the chest wall following a mastectomy. Occasionally,
The posterolateral thoracotomy is still probably the
 Posterolateral Thoracotomy Jean Deslauriers and Reza John Mehran The posterolateral thoracotomy is still probably the most commonly used incision in general thoracic surgery. It provides not only excellent
Posterolateral Thoracotomy Jean Deslauriers and Reza John Mehran The posterolateral thoracotomy is still probably the most commonly used incision in general thoracic surgery. It provides not only excellent
Modified Radical Mastectomy
 Modified Radical Mastectomy Valerie L. Staradub, MD, and Monica Morrow, MD S urgical management options for breast cancer include modified radical mastectomy (MRM), MRM with immediate reconstruction, and
Modified Radical Mastectomy Valerie L. Staradub, MD, and Monica Morrow, MD S urgical management options for breast cancer include modified radical mastectomy (MRM), MRM with immediate reconstruction, and
BREAST AUGMENTATION. everything you ever wanted to know about. Cosmetic breast specialist Dr Michael Miroshnik uses. breasts.
 everything you ever wanted to know about BREAST AUGMENTATION Actual patient of Dr Miroshnik ACCORDING TO SYDNEY PLASTIC SURGEON DR MICHAEL MIROSHNIK, ADVANCES IN SURGICAL TECHNIQUE AND IMPLANT TECHNOLOGY
everything you ever wanted to know about BREAST AUGMENTATION Actual patient of Dr Miroshnik ACCORDING TO SYDNEY PLASTIC SURGEON DR MICHAEL MIROSHNIK, ADVANCES IN SURGICAL TECHNIQUE AND IMPLANT TECHNOLOGY
Therapeutic Mammoplasty. Breast Care
 Therapeutic Mammoplasty Breast Care We put our patients first by working as one team; leading and listening, and striving for the best. Together, we make the difference. Patient information Musgrove Park
Therapeutic Mammoplasty Breast Care We put our patients first by working as one team; leading and listening, and striving for the best. Together, we make the difference. Patient information Musgrove Park
The Vertical Scar Reduction Mammaplasty: a Review of 50 Cases Using Hall Findlay s Technique
 The Vertical Scar Reduction Mammaplasty: a Review of 50 Cases Using Hall Findlay s Technique Waleed Haddaden MD*, Muhammad Abo-Samin MD*, Maher Al-Khateeb MD*, Awni Abo-Lail MD*, Khalid El-Maaytah MD*,
The Vertical Scar Reduction Mammaplasty: a Review of 50 Cases Using Hall Findlay s Technique Waleed Haddaden MD*, Muhammad Abo-Samin MD*, Maher Al-Khateeb MD*, Awni Abo-Lail MD*, Khalid El-Maaytah MD*,
What is involved with breast reduction surgery
 1 Breast reduction is an operation in which your breasts are remodeled to reduce their size whilst maintaining an aesthetic breast shape. At the same time it is possible to lift the position of the nipple
1 Breast reduction is an operation in which your breasts are remodeled to reduce their size whilst maintaining an aesthetic breast shape. At the same time it is possible to lift the position of the nipple
Abdominal Wall Modification for the Difficult Ostomy
 Abdominal Wall Modification for the Difficult Ostomy David E. Beck, M.D. 1 ABSTRACT A select group of patients with major stomal problems may benefit from operative modification of the abdominal wall.
Abdominal Wall Modification for the Difficult Ostomy David E. Beck, M.D. 1 ABSTRACT A select group of patients with major stomal problems may benefit from operative modification of the abdominal wall.
Review Article Oncoplastic Approaches to Breast Conservation
 SAGE-Hindawi Access to Research International Journal of Breast Cancer Volume 2011, Article ID 303879, 16 pages doi:10.4061/2011/303879 Review Article Oncoplastic Approaches to Breast Conservation Dennis
SAGE-Hindawi Access to Research International Journal of Breast Cancer Volume 2011, Article ID 303879, 16 pages doi:10.4061/2011/303879 Review Article Oncoplastic Approaches to Breast Conservation Dennis
Breast augmentation (enlargement)
") Breast augmentation is a surgical procedure that uses breast implants to enhance shape or increase the size of a woman s breast after body changes such as pregnancy, weight loss or from natural ageing.
Breast augmentation is a surgical procedure that uses breast implants to enhance shape or increase the size of a woman s breast after body changes such as pregnancy, weight loss or from natural ageing.
Nipple-Areolar Complex Reconstruction: A Review of the Literature and Introduction of the Rectangle-to-Cube Nipple Flap
 Nipple-Areolar Complex Reconstruction: A Review of the Literature and Introduction of the Rectangle-to-Cube Nipple Flap Joshua T. Henderson, BA, a ThomasJ.Lee,MD, b Andrew M. Swiergosz, BS, a Andrea R.
Nipple-Areolar Complex Reconstruction: A Review of the Literature and Introduction of the Rectangle-to-Cube Nipple Flap Joshua T. Henderson, BA, a ThomasJ.Lee,MD, b Andrew M. Swiergosz, BS, a Andrea R.
INFORMED-CONSENT-SKIN GRAFT SURGERY
 INFORMED-CONSENT-SKIN GRAFT SURGERY 2000 American Society of Plastic Surgeons. Purchasers of the Patient Consultation Resource Book are given a limited license to modify documents contained herein and
INFORMED-CONSENT-SKIN GRAFT SURGERY 2000 American Society of Plastic Surgeons. Purchasers of the Patient Consultation Resource Book are given a limited license to modify documents contained herein and
A long term review of augmentation mastopexy in muscle splitting biplane
 Topic: Aesthetic Surgery of the Breast A long term review of augmentation mastopexy in muscle splitting biplane Umar Daraz Khan Aesthetic Plastic Surgeon, Reshape House, West Malling, Kent ME19 6QR, UK.
Topic: Aesthetic Surgery of the Breast A long term review of augmentation mastopexy in muscle splitting biplane Umar Daraz Khan Aesthetic Plastic Surgeon, Reshape House, West Malling, Kent ME19 6QR, UK.
Breast Pedicle Protector
 Pedicle 1 Breast Pedicle Protector BME 201 University of Wisconsin Madison March 14, 2007 Team: Kuya Takami, Team Leader Nathan Werbeckes, Communications Joseph Yuen, BSAC Laura Bagley, BWIG Client: Michael
Pedicle 1 Breast Pedicle Protector BME 201 University of Wisconsin Madison March 14, 2007 Team: Kuya Takami, Team Leader Nathan Werbeckes, Communications Joseph Yuen, BSAC Laura Bagley, BWIG Client: Michael
Breast Reduction / Mastopexy (Uplift)
") Breast Reduction / Mastopexy (Uplift) This information booklet will support what you have heard in the consultation. It may help answer any questions you have, and give you and your family some understanding
Breast Reduction / Mastopexy (Uplift) This information booklet will support what you have heard in the consultation. It may help answer any questions you have, and give you and your family some understanding
Mastectomy. Brought to you in association with EIDO Healthcare and endorsed by the Royal College of Surgeons England.
 Mastectomy Brought to you in association with EIDO Healthcare and endorsed by the Royal College of Surgeons England. Discovery has made every effort to ensure that we obtained the information in this brochure
Mastectomy Brought to you in association with EIDO Healthcare and endorsed by the Royal College of Surgeons England. Discovery has made every effort to ensure that we obtained the information in this brochure
B11 Breast Reconstruction with Abdominal Tissue Flap
 B11 Breast Reconstruction with Abdominal Tissue Flap Issued March 2011 You can get more information about this procedure from www.aboutmyhealth.org Tell us how useful you found this document at www.patientfeedback.org
B11 Breast Reconstruction with Abdominal Tissue Flap Issued March 2011 You can get more information about this procedure from www.aboutmyhealth.org Tell us how useful you found this document at www.patientfeedback.org
Mons Pubis Ptosis: Classification and Strategy for Treatment
 Aesth Plast Surg (2011) 35:24 30 DOI 10.1007/s00266-010-9552-4 ORIGINAL ARTICLE Mons Pubis Ptosis: Classification and Strategy for Treatment Hamdy A. El-Khatib Received: 2 April 2010 / Accepted: 25 June
Aesth Plast Surg (2011) 35:24 30 DOI 10.1007/s00266-010-9552-4 ORIGINAL ARTICLE Mons Pubis Ptosis: Classification and Strategy for Treatment Hamdy A. El-Khatib Received: 2 April 2010 / Accepted: 25 June
Latissimus Dorsi Flap reconstruction Breast reconstruction
 Latissimus Dorsi Flap reconstruction Breast reconstruction 01935 384 352 yeovilhospital.nhs.uk Introduction Lots of women have surgery to reconstruct the breast after mastectomy. There are a variety of
Latissimus Dorsi Flap reconstruction Breast reconstruction 01935 384 352 yeovilhospital.nhs.uk Introduction Lots of women have surgery to reconstruct the breast after mastectomy. There are a variety of
Periareolar Extra-Glandular Breast Augmentation
 Original Article 93 Periareolar Extra-Glandular Breast Augmentation Muhammad Humayun Mohmand 1 *, Muhammad Ahmad 2 1. Cosmetic Plastic Surgeon, La Chirurgie, Islamabad Cosmetic Surgery Centre, Islamabad,
Original Article 93 Periareolar Extra-Glandular Breast Augmentation Muhammad Humayun Mohmand 1 *, Muhammad Ahmad 2 1. Cosmetic Plastic Surgeon, La Chirurgie, Islamabad Cosmetic Surgery Centre, Islamabad,
Drains are Not Needed in Body Contouring Procedures. Karol A Gutowski, MD, FACS
 Drains are Not Needed in Body Contouring Procedures Karol A Gutowski, MD, FACS Drains are Not Needed in Body Contouring Procedures Karol A Gutowski, MD, FACS Disclosures The Doctors Company - Advisory
Drains are Not Needed in Body Contouring Procedures Karol A Gutowski, MD, FACS Drains are Not Needed in Body Contouring Procedures Karol A Gutowski, MD, FACS Disclosures The Doctors Company - Advisory
Breast Lift (Mastopexy) Breast Lift (Mastopexy) Houston
 Breast Lift (Mastopexy) Houston") Breast Lift (Mastopexy) Houston Breast Lift (Mastopexy) Breast Lift (Mastopexy) Houston Breast Lift (Mastopexy) is a procedure that tightens firms and lifts the breasts. Patients who are satisfied with
Breast Lift (Mastopexy) Houston Breast Lift (Mastopexy) Breast Lift (Mastopexy) Houston Breast Lift (Mastopexy) is a procedure that tightens firms and lifts the breasts. Patients who are satisfied with
Colorectal procedure guide
 Colorectal procedure guide Illustrations by Lisa Clark Biodesign ADVANCED TISSUE REPAIR cookmedical.com 2 INDEX Anal fistula repair Using the Biodesign plug with no button.... 4 Anal fistula repair Using
Colorectal procedure guide Illustrations by Lisa Clark Biodesign ADVANCED TISSUE REPAIR cookmedical.com 2 INDEX Anal fistula repair Using the Biodesign plug with no button.... 4 Anal fistula repair Using
Aesthetic Subunits of the Breast
 Aesthetic Subunits of the Breast Scott L. Spear, M.D., and Steven P. Davison, D.D.S., M.D. Washington, D.C. Surgery for breast cancer has traditionally addressed the breast as if it were a geometric circle
Aesthetic Subunits of the Breast Scott L. Spear, M.D., and Steven P. Davison, D.D.S., M.D. Washington, D.C. Surgery for breast cancer has traditionally addressed the breast as if it were a geometric circle
B02 Mastectomy. Expires end of November Write questions or notes here:
 Practice Locations: St John of God Consulting Suites, 117 Anstruther Road, Mandurah Suite 50, Murdoch Medical Centre, 100 Murdoch Drive, Murdoch Tel: 08 6333 2800 Web: saudhamza.com.au B02 Mastectomy Expires
Practice Locations: St John of God Consulting Suites, 117 Anstruther Road, Mandurah Suite 50, Murdoch Medical Centre, 100 Murdoch Drive, Murdoch Tel: 08 6333 2800 Web: saudhamza.com.au B02 Mastectomy Expires
Thyroidectomy. Siu Kwan Ng. Modified Radical Neck Dissection Type II 47
 06 Thyroidectomy Siu Kwan Ng Modified Radical Neck Dissection Type II 47 Thyroidectomy STEP 1. EXPOSING THE THYROID GLAND The collar incision Figure 1 (curvilinear skin crease incision) is made at 1.5-2
06 Thyroidectomy Siu Kwan Ng Modified Radical Neck Dissection Type II 47 Thyroidectomy STEP 1. EXPOSING THE THYROID GLAND The collar incision Figure 1 (curvilinear skin crease incision) is made at 1.5-2
FIG The inferior and posterior peritoneal reflection is easily
 PSOAS HITCH, BOARI FLAP, AND COMBINATION OF PSOAS 7 HITCH AND BOARI FLAP The psoas hitch procedure, Boari flap, and transureteroureterostomy are useful operative procedures for reestablishing continuity
PSOAS HITCH, BOARI FLAP, AND COMBINATION OF PSOAS 7 HITCH AND BOARI FLAP The psoas hitch procedure, Boari flap, and transureteroureterostomy are useful operative procedures for reestablishing continuity
Gynecomastia Consent. Gynecomastia Surgery (Male Breast Reduction)
") Gynecomastia Consent 1. I hereby authorize Dr. Stratis and such assistants as may be selected to perform the following procedure or treatment: Gynecomastia Surgery (Male Breast Reduction) I have received
Gynecomastia Consent 1. I hereby authorize Dr. Stratis and such assistants as may be selected to perform the following procedure or treatment: Gynecomastia Surgery (Male Breast Reduction) I have received
INFORMED-CONSENT-THIGH LIFT INSTRUCTIONS
 INFORMED-CONSENT-THIGH LIFT INSTRUCTIONS This is an informed-consent document that has been prepared to help the Doctor inform you of thigh lift surgery, its risks, as well as alternative treatments. At
INFORMED-CONSENT-THIGH LIFT INSTRUCTIONS This is an informed-consent document that has been prepared to help the Doctor inform you of thigh lift surgery, its risks, as well as alternative treatments. At
The Case FOR Oncoplastic Surgery in Small Breasts. Barbara L. Smith, MD, PhD Massachusetts General Hospital Harvard Medical School Boston, MA USA
 The Case FOR Oncoplastic Surgery in Small Breasts Barbara L. Smith, MD, PhD Massachusetts General Hospital Harvard Medical School Boston, MA USA Changing issues in breast cancer management Early detection
The Case FOR Oncoplastic Surgery in Small Breasts Barbara L. Smith, MD, PhD Massachusetts General Hospital Harvard Medical School Boston, MA USA Changing issues in breast cancer management Early detection
MOHS MICROGRAPHIC SURGERY: AN OVERVIEW
 MOHS MICROGRAPHIC SURGERY: AN OVERVIEW SKIN CANCER: Skin cancer is far and away the most common malignant tumor found in humans. The most frequent types of skin cancer are basal cell carcinoma, squamous
MOHS MICROGRAPHIC SURGERY: AN OVERVIEW SKIN CANCER: Skin cancer is far and away the most common malignant tumor found in humans. The most frequent types of skin cancer are basal cell carcinoma, squamous
Transfemoral Amputation
 Transfemoral Amputation Pre-Op: 42 year old male who sustained severe injuries in a motorcycle accident. Note: he is a previous renal transplant recipient and is on immunosuppressive treatments. His injuries
Transfemoral Amputation Pre-Op: 42 year old male who sustained severe injuries in a motorcycle accident. Note: he is a previous renal transplant recipient and is on immunosuppressive treatments. His injuries
Procedure Information Guide
 Procedure Information Guide Breast reconstruction with abdominal tissue flap Brought to you in association with EIDO and endorsed by the The Royal College of Surgeons of England Discovery has made every
Procedure Information Guide Breast reconstruction with abdominal tissue flap Brought to you in association with EIDO and endorsed by the The Royal College of Surgeons of England Discovery has made every
CASE REPORT An Innovative Solution to Complex Inguinal Defect: Deepithelialized SIEA Flap With Mini Abdominoplasty
 CASE REPORT An Innovative Solution to Complex Inguinal Defect: Deepithelialized SIEA Flap With Mini Abdominoplasty Augustine Reid Wilson, MS, Justin Daggett, MD, Michael Harrington, MD, MPH, and Deniz
CASE REPORT An Innovative Solution to Complex Inguinal Defect: Deepithelialized SIEA Flap With Mini Abdominoplasty Augustine Reid Wilson, MS, Justin Daggett, MD, Michael Harrington, MD, MPH, and Deniz
INFORMED CONSENT GYNECOMASTIA SURGERY
 Purchasers of the Patient Consultation Resource Book are given a limited license to modify documents contained herein and reproduce the modified version for use in the Purchaser's own practice only. All
Purchasers of the Patient Consultation Resource Book are given a limited license to modify documents contained herein and reproduce the modified version for use in the Purchaser's own practice only. All
How To Make a Good Mastectomy for Reconstruction Based on the Anatomy. Zhang Jin, Ph.D MD
 How To Make a Good Mastectomy for Reconstruction Based on the Anatomy Zhang Jin, Ph.D MD Deputy Director and Professor Tianjin Medical University Cancer Institute and Hospital People s Republic of China
How To Make a Good Mastectomy for Reconstruction Based on the Anatomy Zhang Jin, Ph.D MD Deputy Director and Professor Tianjin Medical University Cancer Institute and Hospital People s Republic of China
h a n d s o m e reduction & an overview
 BREAST reduction & Breast lift an overview b r e a s t r e d u c t i o n Having been since ancient times an outstanding symbol for femininity and fertility the female breast has always been a central part
BREAST reduction & Breast lift an overview b r e a s t r e d u c t i o n Having been since ancient times an outstanding symbol for femininity and fertility the female breast has always been a central part
Kettering Breast Service. Advice and Arm Exercises Following Breast Surgery. Information
 Kettering Breast Service Advice and Arm Exercises Following Breast Surgery Information Exercises following breast surgery are an important part of post-operative care. The gentle exercises contained in
Kettering Breast Service Advice and Arm Exercises Following Breast Surgery Information Exercises following breast surgery are an important part of post-operative care. The gentle exercises contained in
Breast uplift. Brought to you in association with EIDO Healthcare and endorsed by the Royal College of Surgeons England.
 Breast uplift Brought to you in association with EIDO Healthcare and endorsed by the Royal College of Surgeons England. Discovery has made every effort to ensure that we obtained the information in this
Breast uplift Brought to you in association with EIDO Healthcare and endorsed by the Royal College of Surgeons England. Discovery has made every effort to ensure that we obtained the information in this
Jordan University Faculty Of Medicine. Breast. Dr. Ahmed Salman. Assistant professor of anatomy & embryology
 Jordan University Faculty Of Medicine Breast Dr. Ahmed Salman Assistant professor of anatomy & embryology The breasts are specialized accessory glands of the skin that secretes milk. They are situated
Jordan University Faculty Of Medicine Breast Dr. Ahmed Salman Assistant professor of anatomy & embryology The breasts are specialized accessory glands of the skin that secretes milk. They are situated