Endocrine Hypertension
|
|
|
- Georgina French
- 5 years ago
- Views:
Transcription
1 Endocrine Hypertension 1
2 No Disclosures
3 Endocrine Hypertension Objectives: 1. Understand Endocrine disorders causing hypertension 2. Understand clinical presentation of Pheochromocytoma and Hyperaldosteronism 3. Understand clinical detection testing for Pheochromocytoma and hyperaldosteronism
4 Principle Centered Medicine Framework for patient care centered in the whole patient Consider body, mind, spirit in the pathway to health Seeking the full health potential of the patient For this lecture: focus on getting the the bottom of the problem of Hypertension, looking for an endocrine cause Seeking a diagnosis to apply Rational Therapy based in scientific endocrine principles
5 Resistant Hypertension Blood pressure above goal on 3 medi-cations of different classes as per ACC/AHA 2017 One of these medications should be a diuretic If control on 4 drugs, this is also resistant hypertension 5
6 Pseudoresistant Hypertension Insufficient treatment Incorrect measurement Poor adherence to medications Poor adherence to dietary & lifestyle measures White coat hypertension 6
7
8 Factors that could be adjusted in Resistant Hypertension Medications/herbals Diet & Lifestyle Insufficient treatment Volume expansion Secondary etiologies 8
9 Endocrine Etiologies Pheochromocytoma & Paraganglioma Primary Aldosteronism Mineralocorticoid Excess Secondary hyperaldosteronism and Renovascular Cushing syndrome Hypothyroidism Hyperthyroidism Hyperparathyroidism & hypercalcemis Acromegaly 9
10
11 Pheochromocytoma & Paraganglioma (PPargls) In addition to hypertension, Headache Diaphoresis Palpitations Sometimes no symptoms, particularly paragangliomas 11
12 Pheochromocytoma & Paraganglioma (PPargls) Tumors produce Metanephrines But, only intermittent exocytotic parent values Poorly diagnostic results: urine VMA, Catecholamines, Chromogranin A Arise from adrenal medulla up to 85 % and otherwise arise from sympathetic paraganglia 1.6 per 10,000 people, But at autopsy 5 per 10,000 people Incidental adrenal lesion 500 per 10,000 people 12
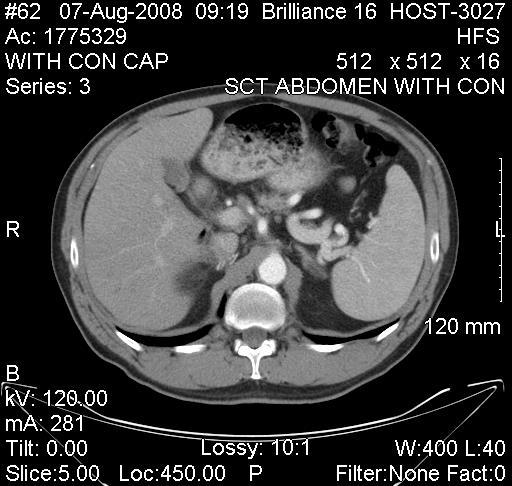
13 Imaging last Not first Common endocrine rule. Incidentalomas are common, and, finding a lesion, may result in inappropriate testing or procedures
14 PPargls measurement parameters Serum testing positional, supine 30 minutes at rest, cannula in place, no dietary requirement Urine 24 hour test; Detail to pt how to collect 14
15
16 Case detection testing High sensitivity labs Serum free metanephrines Urine 24 hour fractionated metanephrines Liquid chromatography with Tandem mass spect abnormal values 2 to 3 X normal
17


18


19
20
21
22 Primary Hyperaldosteronism Increased aldosterone Decrease renin Urine potassium loss Hypokalemia with cramps, paresthesia, weakness But, Hypokalemia is not predominate 5 to 10 % of hypertension 20 % resistent hypertension patients Obstructive sleep apnea common 22
23 Primary Hyperaldosteronism Increases CV events over essential hypertension Non blood pressure effects reversed with aldosterone directed treatment Only 20 % hypokalemia Hypokalemia provokes aldosterone Screen most patients with hypertension Case detection for 1st degree hypertensive relatives 23
24 Primary Hyperaldosteronism Case Detection Many patients are Not hypokalemic, normal electrolytes do not exclude diagnosis Aldosterone/Renin ratio (ARR) is the preferred screen No diuretics for 4 weeks prior to ARR testing Normalize potassium, hypokalemia provokes potassium Liberal sodium diet 24
25 Primary Hyperaldosteronism Case Detection Plasma aldosterone > 10 ng/ml with Plasma renin < 1 ng/ml This values indicate a positive screen Then, proceed to confirmation testing 25
26 Adrenal Venous Sampling Summary RE: Male DOB: 1942 Aldosterone (ng/dl) Cortisol (ug/dl) Basal: Right adrenal vein Left adrenal vein Peripheral Arm POST ACTH: Right adrenal vein Left adrenal vein >150 Peripheral Vena Cava Peripheral Femoral Vein
27 Other Mineralocorticoid Excess
28 Congenital Adrenal Hyperplasia Adrenal enzyme defect ACTH drives precursors Not in deficiency 21 hydroxylase = not htn Low Renin and Aldosterone in hypertension 28
29
30
31
32 Enzymatic defects in steroidogensis that yield androgen over cortisol Most common cases are 21-hydroxylase deficiency If this is complete enzymatic block, the result is ambiguous genitalia in infant girls This presents a crisis of Adrenal Insufficiency, which can be unrecognized in male infants with screening for 17-OH progesterone Variations include late onset CAH in which adult women present with hirsutism
33 CAH and Hypertension 11 beta hydroxylase deficiency 2/3 with Hypertension Hypokalemia Aldosterone low and Renin Low Girls = ambiguous genitalia Boys = precocious puberty 1 in 100,000 caucasian, 5% of CAH
34 Case Detection in 11 beta hydroxylase deficiency Deoxycorticosterone increased Increased 11-deoxycortisol Other steroidogenesis precursors If abnormal, germline mutation testing
35
36 CAH and Hypertension 17 alpha hydroxylase deficiency Hypertension Estimated 1 in 1,000,000 live births Decreased cortisol and sex hormones Girls primary amenorrhea Boys present female body habitus or pseudohermaphrodite
37 Case Detection in 17 alpha hydroxylase deficiency Low blood testing for cortisol, aldosterone, DHEAS, 17-hydroxyprogesterone and others High DOC and corticosterone These labs with hypertension and hypokalemia should have genetic testing, additional diagnostic testing to confirm this deficiency
38 Renovascular Hypertension Renin angiotensin aldosterone system associated Abnormally high aldosterone 1 to 5 % of hypertensives Case detection by renal artery duplex ultrasound and CT angiography highly sensitive Peripheral renin, aldosterone and renal vein renin vary as per conditions of testing Focus for endovascular stents is less on BP and more on saving kidney function and treating pulmonary edema 38
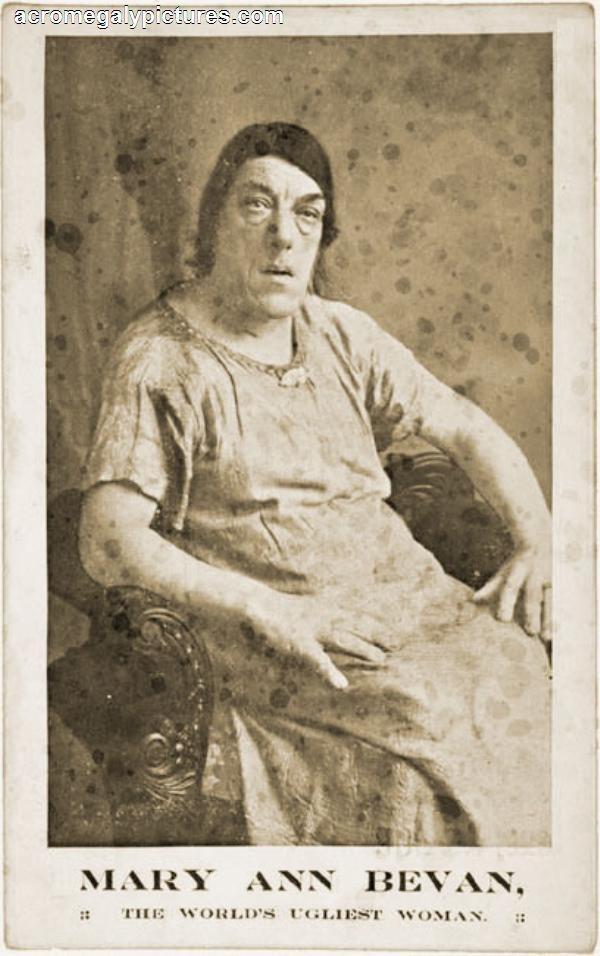
39 Other endocrine HTN presentations Cushing Syndrome: Urine 24 hr free cortisol, 1 mg overnight dexamethasone suppression, midnight salivary cortisol Hyperthyroidism: TSH, Free T4 Hypothyroidism: TSH, Free T4 Hypercalcemia/hyperparathyroidism: PTH, urine 24 hr calcium Acromegaly: IGF-1 Obstructive sleep apnea: Sleep study


40

41

42 42

43

44

45

46 46

47 47

48

49 49

50 50

51 51
52 52

53 53

54 54

55

56
57 References Endocrine Hypertension: I: Clinical disorders of hypertension Chapter 298 Online Harrisons: Kotchen, Theodore A.. "Hypertensive Vascular Disease." Harrison's Principles of Internal Medicine, 19e Eds. Dennis Ka II: Endocrine Reviews Endocrine hypertension screening: William F. Young, David A. Calhoun, Jacques W.M. Lenders, Michael Stowasser, Stephen C. Textor; Screening for Endo III: Endocrine Society Guidelines for Primary Hyperaldosteronism: John W. Funder, Robert M. Carey, Franco Mantero, M. Hassan Murad, Martin Reincke, Hirotaka Shibata, Michael Stow IV: Endocrine Society Guidelines for Pheochromocytoma and Paraganglioma: Jacques W. M. Lenders, Quan-Yang Duh, Graeme Eisenhofer, Anne-Paule Gimenez-Roqueplo, Stefan K. G. Grebe, Moh
58 John Sutton, DO, FACOI, FACE, CCD Carson Tahoe Endocrinology Carson City, NV Phone:
Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone
 Disease of the Adrenals 1 Zona Glomerulosa Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone leads to salt
Disease of the Adrenals 1 Zona Glomerulosa Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone leads to salt
Endocrine. Endocrine as it relates to the kidney. Sarah Elfering, MD University of Minnesota
 Endocrine Sarah Elfering, MD University of Minnesota Endocrine as it relates to the kidney Parathyroid gland Vitamin D Endocrine causes of HTN Adrenal adenoma PTH Bone Kidney Intestine 1, 25 OH Vitamin
Endocrine Sarah Elfering, MD University of Minnesota Endocrine as it relates to the kidney Parathyroid gland Vitamin D Endocrine causes of HTN Adrenal adenoma PTH Bone Kidney Intestine 1, 25 OH Vitamin
John Sutton, DO, FACOI, FACE, CCD. Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989
 John Sutton, DO, FACOI, FACE, CCD Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989 Gonadal Physiology and Disease 3 No Disclosures Gonadal Axis Hypothalamic-pituitary-gonadal Feedback mechanisms
John Sutton, DO, FACOI, FACE, CCD Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989 Gonadal Physiology and Disease 3 No Disclosures Gonadal Axis Hypothalamic-pituitary-gonadal Feedback mechanisms
Secondary Hypertension: A Real World Approach
 Secondary Hypertension: A Real World Approach Evan Brittain, MD December 7, 2012 Kingston, Jamaica Disclosures None Real World Causes Renovascular Hypertension Endocrine Obstructive Sleep Apnea Pseudosecondary
Secondary Hypertension: A Real World Approach Evan Brittain, MD December 7, 2012 Kingston, Jamaica Disclosures None Real World Causes Renovascular Hypertension Endocrine Obstructive Sleep Apnea Pseudosecondary
Screening for Endocrine Hypertension: An Endocrine Society Scientific Statement
 SCIENTIFIC STATEMENT Screening for Endocrine Hypertension: An Endocrine Society Scientific Statement William F. Young Jr., 1 David A. Calhoun, 3 Jacques W.M. Lenders, 4,5 Michael Stowasser, 6,7,8 and Stephen
SCIENTIFIC STATEMENT Screening for Endocrine Hypertension: An Endocrine Society Scientific Statement William F. Young Jr., 1 David A. Calhoun, 3 Jacques W.M. Lenders, 4,5 Michael Stowasser, 6,7,8 and Stephen
SECONDARY HYPERTENSION
 SECONDARY HYPERTENSION Grand round for Medical student 25 October 2013 By Rungnapa Laortanakul, MD. OUTLINE Overview of HT Secondary HT Resistance HT Primary aldosteronism Pheochromocytoma Cushing s syndrome
SECONDARY HYPERTENSION Grand round for Medical student 25 October 2013 By Rungnapa Laortanakul, MD. OUTLINE Overview of HT Secondary HT Resistance HT Primary aldosteronism Pheochromocytoma Cushing s syndrome
How to Recognize Adrenal Disease
 How to Recognize Adrenal Disease CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi
How to Recognize Adrenal Disease CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi
Case Based Urology Learning Program
 Case Based Urology Learning Program Resident s Corner: UROLOGY Case Number 4 CBULP 2010 004 Case Based Urology Learning Program Editor: Associate Editors: Manager: Case Contributors: Steven C. Campbell,
Case Based Urology Learning Program Resident s Corner: UROLOGY Case Number 4 CBULP 2010 004 Case Based Urology Learning Program Editor: Associate Editors: Manager: Case Contributors: Steven C. Campbell,
The Work-up and Treatment of Adrenal Nodules
 The Work-up and Treatment of Adrenal Nodules Lawrence Andrew Drew Shirley, MD, MS, FACS Assistant Professor of Surgical-Clinical Department of Surgery Division of Surgical Oncology The Ohio State University
The Work-up and Treatment of Adrenal Nodules Lawrence Andrew Drew Shirley, MD, MS, FACS Assistant Professor of Surgical-Clinical Department of Surgery Division of Surgical Oncology The Ohio State University
Approach to Adrenal Incidentaloma. Alice Y.Y. Cheng, MD, FRCP
 Approach to Adrenal Incidentaloma Alice Y.Y. Cheng, MD, FRCP Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form
Approach to Adrenal Incidentaloma Alice Y.Y. Cheng, MD, FRCP Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form
SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES DISCIPLINE OF BIOCHEMISTRY & MOLECULAR BIOLOGY
 1 SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES DISCIPLINE OF BIOCHEMISTRY & MOLECULAR BIOLOGY PBL SEMINAR: SEX HORMONES PART 1 An Overview What are steroid hormones? Steroid
1 SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES DISCIPLINE OF BIOCHEMISTRY & MOLECULAR BIOLOGY PBL SEMINAR: SEX HORMONES PART 1 An Overview What are steroid hormones? Steroid
How to approach resistant hypertension. Teh-Li Huo, M.D., Ph.D.
 How to approach resistant hypertension Teh-Li Huo, M.D., Ph.D. BP goals No risk factors:
How to approach resistant hypertension Teh-Li Huo, M.D., Ph.D. BP goals No risk factors:
ADRENAL GLANDS. G M Kellerman. Hunter Area Pathology Service
 ADRENAL GLANDS G M Kellerman Hunter Area Pathology Service ADRENAL FUNCTIONS THE ADRENAL GLANDS ACTUALLY HAVE 4 QUITE SEPARATE FUNCTIONS 1. MINERALOCORTICOID SECRETION BY THE ZONA GLOMERULOSA OF THE CORTEX
ADRENAL GLANDS G M Kellerman Hunter Area Pathology Service ADRENAL FUNCTIONS THE ADRENAL GLANDS ACTUALLY HAVE 4 QUITE SEPARATE FUNCTIONS 1. MINERALOCORTICOID SECRETION BY THE ZONA GLOMERULOSA OF THE CORTEX
Spectrum of Hypertension & Hypokalemia
 Spectrum of Hypertension & Hypokalemia Farheen K. Dojki, PGY-6 Hypertension Fellow, ASH Hypertension Center Dr. Dojki does not have any relevant financial relationships with any commercial interests. OBJECTIVES:
Spectrum of Hypertension & Hypokalemia Farheen K. Dojki, PGY-6 Hypertension Fellow, ASH Hypertension Center Dr. Dojki does not have any relevant financial relationships with any commercial interests. OBJECTIVES:
RESISTENT HYPERTENSION. Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University
 RESISTENT HYPERTENSION Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University Resistant Hypertension Blood pressure remaining above goal in spite of concurrent use of 3 antihypertensive
RESISTENT HYPERTENSION Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University Resistant Hypertension Blood pressure remaining above goal in spite of concurrent use of 3 antihypertensive
CHOLESTEROL IS THE PRECURSOR OF STERIOD HORMONES
 HORMONES OF ADRENAL CORTEX R. Mohammadi Biochemist (Ph.D.) Faculty member of Medical Faculty CHOLESTEROL IS THE PRECURSOR OF STERIOD HORMONES CONVERSION OF CHOLESTROL TO PREGNENOLONE MINERALOCORTICOCOIDES
HORMONES OF ADRENAL CORTEX R. Mohammadi Biochemist (Ph.D.) Faculty member of Medical Faculty CHOLESTEROL IS THE PRECURSOR OF STERIOD HORMONES CONVERSION OF CHOLESTROL TO PREGNENOLONE MINERALOCORTICOCOIDES
Adrenal incidentaloma guideline for Northern Endocrine Network
 Adrenal incidentaloma guideline for Northern Endocrine Network Definition of adrenal incidentaloma Adrenal mass detected on an imaging study done for indications that are not related to an adrenal problem
Adrenal incidentaloma guideline for Northern Endocrine Network Definition of adrenal incidentaloma Adrenal mass detected on an imaging study done for indications that are not related to an adrenal problem
Upon completion, participants should be able to:
 Learning Objectives Upon completion, participants should be able to: Describe the causes of secondary hypertension and the prevalence of primary aldosteronism Discuss the diagnostic approach to primary
Learning Objectives Upon completion, participants should be able to: Describe the causes of secondary hypertension and the prevalence of primary aldosteronism Discuss the diagnostic approach to primary
Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical Sciences. Endocrinology. (Review) Year 5 Internal Medicine
 Year 5 Internal Medicine") Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical Sciences Endocrinology (Review) Year 5 Internal Medicine Presented by: Dr. Mona Arekat Prepared by: Ali Jassim Alhashli Case (1):
Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical Sciences Endocrinology (Review) Year 5 Internal Medicine Presented by: Dr. Mona Arekat Prepared by: Ali Jassim Alhashli Case (1):
Primary Aldosteronism: screening, diagnosis and therapy
 Primary Aldosteronism: screening, diagnosis and therapy Jacques W.M. Lenders, internist DEPT. OF INTERNAL MEDICINE, RADBOUD UNIVERSITY NIJMEGEN MEDICAL CENTER, NIJMEGEN,THE NETHERLANDS DEPT. OF INTERNAL
Primary Aldosteronism: screening, diagnosis and therapy Jacques W.M. Lenders, internist DEPT. OF INTERNAL MEDICINE, RADBOUD UNIVERSITY NIJMEGEN MEDICAL CENTER, NIJMEGEN,THE NETHERLANDS DEPT. OF INTERNAL
Endocrine MR. Jan 30, 2015 Michael LaFata, MD
 Endocrine MR Jan 30, 2015 Michael LaFata, MD Brief case 55-year-old female in ED PMH: HTN, DM2, HLD, GERD CC: Epigastric/LUQ abdominal pain, N/V x2 days AF, HR 103, BP 155/85, room air CMP: Na 133, K 3.6,
Endocrine MR Jan 30, 2015 Michael LaFata, MD Brief case 55-year-old female in ED PMH: HTN, DM2, HLD, GERD CC: Epigastric/LUQ abdominal pain, N/V x2 days AF, HR 103, BP 155/85, room air CMP: Na 133, K 3.6,
Endocrine Surgery When to Refer and What We Do
 Endocrine Surgery When to Refer and What We Do None Disclosures W. Heath Giles, M.D., F.A.C.S. Surgery Residency Program Director Assistant Professor of Surgery What is Endocrine Surgery? Who performs
Endocrine Surgery When to Refer and What We Do None Disclosures W. Heath Giles, M.D., F.A.C.S. Surgery Residency Program Director Assistant Professor of Surgery What is Endocrine Surgery? Who performs
4/23/2015. Objectives DISCLOSURES
 2015 PENS Conference Savannah, GA Novel Cases of Congenital Hyperreninemic Hypaldosteronism Jan M. Foote DISCLOSURES I have no actual or potential conflicts of interest in relation to this presentation.
2015 PENS Conference Savannah, GA Novel Cases of Congenital Hyperreninemic Hypaldosteronism Jan M. Foote DISCLOSURES I have no actual or potential conflicts of interest in relation to this presentation.
Year 2004 Paper two: Questions supplied by Megan 1
 Year 2004 Paper two: Questions supplied by Megan 1 QUESTION 96 A 32yo woman if found to have high blood pressure (180/105mmHg) at an insurance medical examination. She is asymptomatic. Clinical examination
Year 2004 Paper two: Questions supplied by Megan 1 QUESTION 96 A 32yo woman if found to have high blood pressure (180/105mmHg) at an insurance medical examination. She is asymptomatic. Clinical examination
ENDOCRINE FORMS OF HYPERTENSION. Michael Stowasser
 ENDOCRINE FORMS OF HYPERTENSION Michael Stowasser Hypertension Unit, University Department of Medicine, Princess Alexandra Hospital, Brisbane 4102, Australia. ENDOCRINE FORMS OF HYPERTENSION Mineralocorticoid
ENDOCRINE FORMS OF HYPERTENSION Michael Stowasser Hypertension Unit, University Department of Medicine, Princess Alexandra Hospital, Brisbane 4102, Australia. ENDOCRINE FORMS OF HYPERTENSION Mineralocorticoid
Primary aldosteronism clinical practice guidelines: a re-appraisal The Management of Primary Aldosteronism
 Primary aldosteronism clinical practice guidelines: a re-appraisal The Management of Primary Aldosteronism Prof. FRANCO MANTERO Division of Endocrinology University of Padua Italy Case Detection, Diagnosis
Primary aldosteronism clinical practice guidelines: a re-appraisal The Management of Primary Aldosteronism Prof. FRANCO MANTERO Division of Endocrinology University of Padua Italy Case Detection, Diagnosis
Hormones. Introduction to Endocrine Disorders. Hormone actions. Modulation of hormone levels. Modulation of hormone levels
 Introduction to Endocrine Disorders Hormones Self-regulating system (homeostasis) Affect: Growth Metabolism Reproduction Fluid and electrolyte balance Hormone actions Endocrine gland Hormone synthesis
Introduction to Endocrine Disorders Hormones Self-regulating system (homeostasis) Affect: Growth Metabolism Reproduction Fluid and electrolyte balance Hormone actions Endocrine gland Hormone synthesis
ULTIMATE BEAUTY OF BIOCHEMISTRY. Dr. Veena Bhaskar S Gowda Dept of Biochemistry 30 th Nov 2017
 ULTIMATE BEAUTY OF BIOCHEMISTRY Dr. Veena Bhaskar S Gowda Dept of Biochemistry 30 th Nov 2017 SUSPECTED CASE OF CUSHING S SYNDROME Clinical features Moon face Obesity Hypertension Hunch back Abdominal
ULTIMATE BEAUTY OF BIOCHEMISTRY Dr. Veena Bhaskar S Gowda Dept of Biochemistry 30 th Nov 2017 SUSPECTED CASE OF CUSHING S SYNDROME Clinical features Moon face Obesity Hypertension Hunch back Abdominal
27 F with new onset hypertension and weight gain. Rajesh Jain Endorama 10/01/2015
 27 F with new onset hypertension and weight gain Rajesh Jain Endorama 10/01/2015 HPI 27 F with hypertension x 1 year BP 130-140/90 while on amlodipine 5 mg daily She also reports weight gain, 7 LB, mainly
27 F with new onset hypertension and weight gain Rajesh Jain Endorama 10/01/2015 HPI 27 F with hypertension x 1 year BP 130-140/90 while on amlodipine 5 mg daily She also reports weight gain, 7 LB, mainly
Secondary hypertension How to approach?
 Secondary hypertension How to approach? Tomáš Seeman Department of Pediatrics and Transplantation Center, University Hospital Motol, 2 nd Faculty of Medicine, Charles University Prague, Czech Republic
Secondary hypertension How to approach? Tomáš Seeman Department of Pediatrics and Transplantation Center, University Hospital Motol, 2 nd Faculty of Medicine, Charles University Prague, Czech Republic
The endocrine system is made up of a complex group of glands that secrete hormones.
 1 10. Endocrinology I MEDCHEM 535 Diagnostic Medicinal Chemistry Endocrinology The endocrine system is made up of a complex group of glands that secrete hormones. These hormones control reproduction, metabolism,
1 10. Endocrinology I MEDCHEM 535 Diagnostic Medicinal Chemistry Endocrinology The endocrine system is made up of a complex group of glands that secrete hormones. These hormones control reproduction, metabolism,
Endocrine hypertensionmolecules. Marie Freel Caledonian Endocrine Society Meeting 29 th November 2015
 Endocrine hypertensionmolecules and genes Marie Freel Caledonian Endocrine Society Meeting 29 th November 2015 Plan Mineralocorticoid hypertension Myths surrounding Primary Aldosteronism (PA) New developments
Endocrine hypertensionmolecules and genes Marie Freel Caledonian Endocrine Society Meeting 29 th November 2015 Plan Mineralocorticoid hypertension Myths surrounding Primary Aldosteronism (PA) New developments
PITUITARY: JUST THE BASICS PART 2 THE PATIENT
 PITUITARY: JUST THE BASICS PART 2 THE PATIENT DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none Steps taken to review and
PITUITARY: JUST THE BASICS PART 2 THE PATIENT DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none Steps taken to review and
Adrenal gland Incidentaloma
 Adrenal gland Incidentaloma Topic review 17 sep 2008 Anatomy 1 Anatomical consideration Blood supply Artery: small branches from Inf. phrenic, renal artery and aorta Vein: Rt : medial aspect to IVC Lt
Adrenal gland Incidentaloma Topic review 17 sep 2008 Anatomy 1 Anatomical consideration Blood supply Artery: small branches from Inf. phrenic, renal artery and aorta Vein: Rt : medial aspect to IVC Lt
Assistant Professor of Endocrinology
 Pathophysiology Of Adrenal Disorder Dr.Rezvan Salehidoost Assistant Professor of Endocrinology Pathophysiology Of Adrenal Disorder The adrenal glands lie at the superior pole of each kidney and are composed
Pathophysiology Of Adrenal Disorder Dr.Rezvan Salehidoost Assistant Professor of Endocrinology Pathophysiology Of Adrenal Disorder The adrenal glands lie at the superior pole of each kidney and are composed
Dr Doris M. W Kinuthia
 Dr Doris M. W Kinuthia Objectives Normal blood pressures in children Measurement of blood pressure in children Aetiology of Hypertension in children Evaluation of children with hypertension Treatment of
Dr Doris M. W Kinuthia Objectives Normal blood pressures in children Measurement of blood pressure in children Aetiology of Hypertension in children Evaluation of children with hypertension Treatment of
Diseases of the Adrenal gland
 Diseases of the Adrenal gland Adrenal insufficiency Cushing disease vs syndrome Pheochromocytoma Hyperaldostronism What are the layers of the adrenal gland?? And what does each layer produce?? What are
Diseases of the Adrenal gland Adrenal insufficiency Cushing disease vs syndrome Pheochromocytoma Hyperaldostronism What are the layers of the adrenal gland?? And what does each layer produce?? What are
Adrenal Mass. Cynthia Kwong SUNY Downstate Medical Center Grand Rounds October 13, 2016
 Adrenal Mass Cynthia Kwong SUNY Downstate Medical Center Grand Rounds October 13, 2016 Case Presentation 65F found to have a 4cm left adrenal mass in 2012 now presents with 6.7cm left adrenal mass PMHx:
Adrenal Mass Cynthia Kwong SUNY Downstate Medical Center Grand Rounds October 13, 2016 Case Presentation 65F found to have a 4cm left adrenal mass in 2012 now presents with 6.7cm left adrenal mass PMHx:
AVS and IPSS: The Basics and the Pearls
 AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2018 Mayo Foundation for Medical Education and Research.
AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2018 Mayo Foundation for Medical Education and Research.
A case of DYSELECTROLYTEMIA. Dr. Prathyusha Dr. Lalitha janakiraman s unit
 A case of DYSELECTROLYTEMIA Dr. Prathyusha Dr. Lalitha janakiraman s unit CASE SUMMARY 4 month old, female infant 1 st born to NC parents, term, b.wt: 3.25kg No neonatal hospitalization Attained head control
A case of DYSELECTROLYTEMIA Dr. Prathyusha Dr. Lalitha janakiraman s unit CASE SUMMARY 4 month old, female infant 1 st born to NC parents, term, b.wt: 3.25kg No neonatal hospitalization Attained head control
ADRENAL INCIDENTALOMA. Jamii St. Julien
 ADRENAL INCIDENTALOMA Jamii St. Julien Outline Definition Differential Evaluation Treatment Follow up Questions Case Definition The phenomenon of detecting an otherwise unsuspected adrenal mass on radiologic
ADRENAL INCIDENTALOMA Jamii St. Julien Outline Definition Differential Evaluation Treatment Follow up Questions Case Definition The phenomenon of detecting an otherwise unsuspected adrenal mass on radiologic
Approach to patient with hypertension. Dr. Amitesh Aggarwal
 Approach to patient with hypertension Dr. Amitesh Aggarwal Definition A systolic blood pressure ( SBP) >139 mmhg and/or A diastolic (DBP) >89 mmhg. Based on the average of two or more properly measured,
Approach to patient with hypertension Dr. Amitesh Aggarwal Definition A systolic blood pressure ( SBP) >139 mmhg and/or A diastolic (DBP) >89 mmhg. Based on the average of two or more properly measured,
Incidental Adrenal Nodules Differential Diagnosis
 Adrenal Stuff Richard J. Auchus, MD, PhD, FACE Division of Metabolism, Endocrinology & Diabetes Departments of Internal Medicine & Pharmacology University of Michigan/VA Ann Arbor Incidental Adrenal Nodules
Adrenal Stuff Richard J. Auchus, MD, PhD, FACE Division of Metabolism, Endocrinology & Diabetes Departments of Internal Medicine & Pharmacology University of Michigan/VA Ann Arbor Incidental Adrenal Nodules
A CASE OF HYPERTENSION AND ACUTE RENAL FAILURE OBJECTIVES
 A CASE OF HYPERTENSION AND ACUTE RENAL FAILURE Maricel Pilapil-Pureza WLA Nephrology OBJECTIVES After the presentation, the attendee will be able to: 1. Discuss when to suspect for secondary causes of
A CASE OF HYPERTENSION AND ACUTE RENAL FAILURE Maricel Pilapil-Pureza WLA Nephrology OBJECTIVES After the presentation, the attendee will be able to: 1. Discuss when to suspect for secondary causes of
Checking the Right Box at the Right Age: the Art of Pediatric Endocrine Testing
 Checking the Right Box at the Right Age: the Art of Pediatric Endocrine Testing Jean-Pierre Chanoine, MD Endocrinology and Diabetes Unit British Columbia s Children s Hospital Objectives 1. Interpret the
Checking the Right Box at the Right Age: the Art of Pediatric Endocrine Testing Jean-Pierre Chanoine, MD Endocrinology and Diabetes Unit British Columbia s Children s Hospital Objectives 1. Interpret the
Table of Contents Section I Pituitary and Hypothalamus 1. Development of the Pituitary Gland 2. Divisions of the Pituitary Gland and Relationship to
 Table of Contents Section I Pituitary and Hypothalamus 1. Development of the Pituitary Gland 2. Divisions of the Pituitary Gland and Relationship to the Hypothalamus 3. Blood Supply of the Pituitary Gland
Table of Contents Section I Pituitary and Hypothalamus 1. Development of the Pituitary Gland 2. Divisions of the Pituitary Gland and Relationship to the Hypothalamus 3. Blood Supply of the Pituitary Gland
When testes make no testosterone: Identifying a rare cause of 46, XY female phenotype in adulthood
 When testes make no testosterone: Identifying a rare cause of 46, XY female phenotype in adulthood Gardner DG, Shoback D. Greenspan's Basic & Clinical Endocrinology, 10e; 2017 Sira Korpaisarn, MD Endocrinology
When testes make no testosterone: Identifying a rare cause of 46, XY female phenotype in adulthood Gardner DG, Shoback D. Greenspan's Basic & Clinical Endocrinology, 10e; 2017 Sira Korpaisarn, MD Endocrinology
ADRENAL GLANDS HORMONES
 ADRNAL GLANDS HORMONS Glands Cortex 80% mesoderm Mineralococorticoids Glucocorticoids (phenylethanolamine N- methyl transferase) A Sex Hormones Catecholamines Medulla 20% PNMT, N neuroectoderm N PNMT V
ADRNAL GLANDS HORMONS Glands Cortex 80% mesoderm Mineralococorticoids Glucocorticoids (phenylethanolamine N- methyl transferase) A Sex Hormones Catecholamines Medulla 20% PNMT, N neuroectoderm N PNMT V
New Hypertension Guidelines. Kofi Osei, MD
 New Hypertension Guidelines Kofi Osei, MD None Disclosures Objectives The new blood pressure definitions and cardiovascular risk The role to time and location in the diagnosis of hypertension Apply evidence-based
New Hypertension Guidelines Kofi Osei, MD None Disclosures Objectives The new blood pressure definitions and cardiovascular risk The role to time and location in the diagnosis of hypertension Apply evidence-based
Systemic Hypertension Dr ahmed almutairi Assistant professor Internal medicine dept
 Systemic Hypertension Dr ahmed almutairi Assistant professor Internal medicine dept Continents 1- introduction 2- classification/definition 3- classification/etiology 4-etiology in both categories 5- complications
Systemic Hypertension Dr ahmed almutairi Assistant professor Internal medicine dept Continents 1- introduction 2- classification/definition 3- classification/etiology 4-etiology in both categories 5- complications
SEX STERIOD HORMONES I: An Overview. University of PNG School of Medicine & Health Sciences Division of Basic Medical Sciences PBL MBBS III VJ Temple
 SEX STERIOD HORMONES I: An Overview University of PNG School of Medicine & Health Sciences Division of Basic Medical Sciences PBL MBBS III VJ Temple 1 What are the Steroid hormones? Hormones synthesized
SEX STERIOD HORMONES I: An Overview University of PNG School of Medicine & Health Sciences Division of Basic Medical Sciences PBL MBBS III VJ Temple 1 What are the Steroid hormones? Hormones synthesized
Adrenal disease Real and Unreal. Objectives. Real
 Adrenal disease Real and Unreal J R Minkoff MD, FACP Endocrinology Clinical Professor of Family and Community Medicine UCSF Objectives Participants will: 1) understand the signs, symptoms, diagnosis and
Adrenal disease Real and Unreal J R Minkoff MD, FACP Endocrinology Clinical Professor of Family and Community Medicine UCSF Objectives Participants will: 1) understand the signs, symptoms, diagnosis and
A 64 year old man referred for evaluation of suspected hyperaldosteronism
 A 64 year old man referred for evaluation of suspected hyperaldosteronism Dr. Dickens does not have any relevant financial relationships with any commercial interests. ENDORAMA: 64 year old man referred
A 64 year old man referred for evaluation of suspected hyperaldosteronism Dr. Dickens does not have any relevant financial relationships with any commercial interests. ENDORAMA: 64 year old man referred
301 S. Westfield Rd., Suite 250 Madison, WI See inside for information about our Endocrine Surgery Referral Program
 301 S. Westfield Rd., Suite 250 Madison, WI 53717 See inside for information about our Endocrine Surgery Referral Program December 2017 Dear Colleague, Thank you for referring your patient(s) to UW Health
301 S. Westfield Rd., Suite 250 Madison, WI 53717 See inside for information about our Endocrine Surgery Referral Program December 2017 Dear Colleague, Thank you for referring your patient(s) to UW Health
Aldosterone synthase inhibitors. John McMurray BHF Cardiovascular Research Centre University of Glasgow
 Aldosterone synthase inhibitors John McMurray BHF Cardiovascular Research Centre University of Glasgow Inhibition of aldosterone synthesis is hypothesized to be of benefit to patients with cardiovascular
Aldosterone synthase inhibitors John McMurray BHF Cardiovascular Research Centre University of Glasgow Inhibition of aldosterone synthesis is hypothesized to be of benefit to patients with cardiovascular
in Primary Care (Part 2) Jonathan R. Anolik, MD, FACP, FACE Lewis Katz School of Medicine at Temple University
 Jonathan R. Anolik, MD, FACP, FACE Lewis Katz School of Medicine at Temple University") Common Endocrine Problems Seen in Primary Care (Part 2) Lecture #34 Jonathan R. Anolik, MD, FACP, FACE Lewis Katz School of Medicine at Temple University None Conflict of Interest Topics to be Covered
Common Endocrine Problems Seen in Primary Care (Part 2) Lecture #34 Jonathan R. Anolik, MD, FACP, FACE Lewis Katz School of Medicine at Temple University None Conflict of Interest Topics to be Covered
Pathophysiology of Adrenal Disorders
 Pathophysiology of Adrenal Disorders PHCL 415 Hadeel Alkofide April 2010 Some slides adapted from Rania Aljizani MSc 1 Learning Objectives Describe the roles of the various zones of the adrenal cortex
Pathophysiology of Adrenal Disorders PHCL 415 Hadeel Alkofide April 2010 Some slides adapted from Rania Aljizani MSc 1 Learning Objectives Describe the roles of the various zones of the adrenal cortex
Biochemistry past year s questions.
 Biochemistry past year s questions. Q1) A random blood sample for GH assessment in a suspected deficiency state is useless because it is commonly undetectable, so there are several " tricks " to collect
Biochemistry past year s questions. Q1) A random blood sample for GH assessment in a suspected deficiency state is useless because it is commonly undetectable, so there are several " tricks " to collect
The most current assessment of this problem can be found in the Apex note dated
 Him andpcos Smartphrase:.REFENDOPCOS NOTE: patients with suspected PCOS are welcomed to endocrine clinic. There is also a PCOS clinic is available in the Ob/Gyn Department. I am referring @name@, a @age@
Him andpcos Smartphrase:.REFENDOPCOS NOTE: patients with suspected PCOS are welcomed to endocrine clinic. There is also a PCOS clinic is available in the Ob/Gyn Department. I am referring @name@, a @age@
Pituitary Gland Disorders
 Pituitary Gland Disorders 1 2 (GH-RH) (CRH) (TRH) (TRH) (GTRH) (GTRH) 3 Classification of pituitary disorders: 1. Hypersecretory diseases: a. Acromegaly and gigantism: Usually caused by (GH)-secreting
Pituitary Gland Disorders 1 2 (GH-RH) (CRH) (TRH) (TRH) (GTRH) (GTRH) 3 Classification of pituitary disorders: 1. Hypersecretory diseases: a. Acromegaly and gigantism: Usually caused by (GH)-secreting
Subclinical Cushing s Syndrome
 Subclinical Cushing s Syndrome AACE 26th Annual Scientific & Clinical Congress Associate Clinical Professor of Medicine and Clinical Chief University of Miami Miller Scholl of Medicine Miami, Florida aayala2@miami.edu
Subclinical Cushing s Syndrome AACE 26th Annual Scientific & Clinical Congress Associate Clinical Professor of Medicine and Clinical Chief University of Miami Miller Scholl of Medicine Miami, Florida aayala2@miami.edu
Southern Derbyshire Shared Care Pathology Guidelines. Secondary Hypertension
 Southern Derbyshire Shared Care Pathology Guidelines Secondary Hypertension Purpose of Guideline This guideline covers the investigation and referral criteria of patients with suspected secondary causes
Southern Derbyshire Shared Care Pathology Guidelines Secondary Hypertension Purpose of Guideline This guideline covers the investigation and referral criteria of patients with suspected secondary causes
Primary Aldosteronism
 Primary Aldosteronism Odelia Cooper, MD Assistant Professor of Medicine Division of Endocrinology, Diabetes, and Metabolism Cedars-Sinai Medical Center HYPERTENSION CENTER Barriers to diagnosing primary
Primary Aldosteronism Odelia Cooper, MD Assistant Professor of Medicine Division of Endocrinology, Diabetes, and Metabolism Cedars-Sinai Medical Center HYPERTENSION CENTER Barriers to diagnosing primary
The Case of the Adrenal Mass
 The Case of the Adrenal Mass Functional Adrenal Tumors Patricia Leung 10.2.14 Kings County Hospital Case presentation 62 year old F PMH: HTN, DM, arthritis PSH: none Meds: Metoprolol, Nifedipine, Losartan,
The Case of the Adrenal Mass Functional Adrenal Tumors Patricia Leung 10.2.14 Kings County Hospital Case presentation 62 year old F PMH: HTN, DM, arthritis PSH: none Meds: Metoprolol, Nifedipine, Losartan,
Case Based Urology Learning Program
 Case Based Urology Learning Program Resident s Corner: UROLOGY Case Number 3 CBULP 2011 019 Case Based Urology Learning Program Editor: Associate Editors: Manager: Case Contributors: Steven C. Campbell,
Case Based Urology Learning Program Resident s Corner: UROLOGY Case Number 3 CBULP 2011 019 Case Based Urology Learning Program Editor: Associate Editors: Manager: Case Contributors: Steven C. Campbell,
MILD HYPERCORTISOLISM DUE TO ADRENAL ADENOMA: IS IT REALLY SUBCLINICAL?
 MILD HYPERCORTISOLISM DUE TO ADRENAL ADENOMA: IS IT REALLY SUBCLINICAL? Alice C. Levine, MD Professor of Medicine Division of Endocrinology, Diabetes and Bone Diseases Georgia-AACE 2017 Annual Meeting
MILD HYPERCORTISOLISM DUE TO ADRENAL ADENOMA: IS IT REALLY SUBCLINICAL? Alice C. Levine, MD Professor of Medicine Division of Endocrinology, Diabetes and Bone Diseases Georgia-AACE 2017 Annual Meeting
Treating Hypertension from
 Treating Hypertension from Initiation to Resistance: A Case Study Approach Michelle Krause, MD Division of Nephrology University of Arkansas for Medical Sciences Central Arkansas Veteran s Healthcare System
Treating Hypertension from Initiation to Resistance: A Case Study Approach Michelle Krause, MD Division of Nephrology University of Arkansas for Medical Sciences Central Arkansas Veteran s Healthcare System
2402 : Anatomy/Physiology
 Dr. Chris Doumen Lecture 4 2402 : Anatomy/Physiology Major Endocrine Organs Calci u m H o me os t asis TextBook Readings Pages 624 through 632. Make use of the figures in your textbook ; a picture is worth
Dr. Chris Doumen Lecture 4 2402 : Anatomy/Physiology Major Endocrine Organs Calci u m H o me os t asis TextBook Readings Pages 624 through 632. Make use of the figures in your textbook ; a picture is worth
AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA
 AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2016 Mayo Foundation for Medical Education and Research.
AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2016 Mayo Foundation for Medical Education and Research.
COPYRIGHTED MATERIAL. Adrenal Imaging. 1.1 Introduction. Khaled M. Elsayes 1, Isaac R. Francis 1, Melvyn Korobkin 1 and Gerard M.
 1 Adrenal Imaging Khaled M. Elsayes 1, Isaac R. Francis 1, Melvyn Korobkin 1 and Gerard M. Doherty 2 1 Department of Radiology, University of Michigan 2 Department of Radiology and Surgery, University
1 Adrenal Imaging Khaled M. Elsayes 1, Isaac R. Francis 1, Melvyn Korobkin 1 and Gerard M. Doherty 2 1 Department of Radiology, University of Michigan 2 Department of Radiology and Surgery, University
THE HIGHS AND LOWS OF ADRENAL GLAND PATHOLOGY
 THE HIGHS AND LOWS OF ADRENAL GLAND PATHOLOGY Symptoms of Adrenal Gland Disorders 2 Depends on whether it is making too much or too little hormone And on what you Google! Symptoms include obesity, skin
THE HIGHS AND LOWS OF ADRENAL GLAND PATHOLOGY Symptoms of Adrenal Gland Disorders 2 Depends on whether it is making too much or too little hormone And on what you Google! Symptoms include obesity, skin
Pediatric Endocrine Dysfunction
 Pediatric Endocrine Dysfunction Chapter 52 Debra Mercer BSN, RN, RRT Mechanisms of Hormonal Regulation The endocrine system is composed of various glands located throughout the body. These glands can synthesize
Pediatric Endocrine Dysfunction Chapter 52 Debra Mercer BSN, RN, RRT Mechanisms of Hormonal Regulation The endocrine system is composed of various glands located throughout the body. These glands can synthesize
Endocrine Testing. Alice Y.Y. Cheng, MD, FRCP October 14, 2015
 Endocrine Testing Alice Y.Y. Cheng, MD, FRCP October 14, 2015 Disclosure No disclosures relevant to the content of this workshop Learning Objectives By the end of this workshop, you will be able to: 1.
Endocrine Testing Alice Y.Y. Cheng, MD, FRCP October 14, 2015 Disclosure No disclosures relevant to the content of this workshop Learning Objectives By the end of this workshop, you will be able to: 1.
Stelios Mantis, MD DuPage Medical Group Pediatric Endocrinology
 Stelios Mantis, MD DuPage Medical Group Pediatric Endocrinology 4 11 13 Initial Presentation Pt initially presented to pediatrician for school physical in fall 2012. Pt was found to be overweight (BMI:
Stelios Mantis, MD DuPage Medical Group Pediatric Endocrinology 4 11 13 Initial Presentation Pt initially presented to pediatrician for school physical in fall 2012. Pt was found to be overweight (BMI:
How do I investigate suspected secondary hypertension? Marie Freel RCP Update in Medicine 23 rd November 2016
 How do I investigate suspected secondary hypertension? Marie Freel RCP Update in Medicine 23 rd November 2016 World beaters..! Michel Joffres et al. BMJ Open 2013;3:e003423 Hypertension often poorly controlled
How do I investigate suspected secondary hypertension? Marie Freel RCP Update in Medicine 23 rd November 2016 World beaters..! Michel Joffres et al. BMJ Open 2013;3:e003423 Hypertension often poorly controlled
Special Lecture 11/08/2013. Hypertension Dr. HN Mayrovitz
 Special Lecture 11/08/2013 Hypertension Dr. HN Mayrovitz Arterial Blood Pressure (ABP) Major Factors Summarized Sympathetic Hormones Arteriole MAP ~ Q x TPR + f (V / C) SV x HR Renal SBP Hypertension =
Special Lecture 11/08/2013 Hypertension Dr. HN Mayrovitz Arterial Blood Pressure (ABP) Major Factors Summarized Sympathetic Hormones Arteriole MAP ~ Q x TPR + f (V / C) SV x HR Renal SBP Hypertension =
Il Carcinoma Surrenalico
 Il Carcinoma Surrenalico Massimo Terzolo Medicina Interna I AOU San Luigi Orbassano (TO) Italy AGENDA DIAGNOSIS CLINICAL PRESENTATION IMPACT ON PROGNOSIS TREATMENT DIAGNOSIS 23-yr-old lady October 2010,
Il Carcinoma Surrenalico Massimo Terzolo Medicina Interna I AOU San Luigi Orbassano (TO) Italy AGENDA DIAGNOSIS CLINICAL PRESENTATION IMPACT ON PROGNOSIS TREATMENT DIAGNOSIS 23-yr-old lady October 2010,
Pituitary Adenomas: Evaluation and Management. Fawn M. Wolf, MD 10/27/17
 Pituitary Adenomas: Evaluation and Management Fawn M. Wolf, MD 10/27/17 Over 18,000 pituitaries examined at autopsy: -10.6% contained adenomas (1.5-27%) -Frequency similar for men and women and across
Pituitary Adenomas: Evaluation and Management Fawn M. Wolf, MD 10/27/17 Over 18,000 pituitaries examined at autopsy: -10.6% contained adenomas (1.5-27%) -Frequency similar for men and women and across
ظظظ/ Omar Sami. Hussam Twaissi. Mousa Abbadi
 ظظظ/ 5 Omar Sami Hussam Twaissi Mousa Abbadi The doctor started this lecture by revising what we have taken in lecture number four, I won t re-write these stuff as it becomes boring so often. This sheet
ظظظ/ 5 Omar Sami Hussam Twaissi Mousa Abbadi The doctor started this lecture by revising what we have taken in lecture number four, I won t re-write these stuff as it becomes boring so often. This sheet
Case Questions. Polycystic Ovarian Syndrome: Treatment Goals and Options. Differential Diagnosis of Hyperandrogenic Anovulation
 Polycystic Ovarian Syndrome: Treatment Goals and Options Marc Cornier, MD Division of Endocrinology, Metabolism and Diabetes Colorado Center for Health and Wellness University of Colorado School of Medicine
Polycystic Ovarian Syndrome: Treatment Goals and Options Marc Cornier, MD Division of Endocrinology, Metabolism and Diabetes Colorado Center for Health and Wellness University of Colorado School of Medicine
Jared Moore, MD, FACP
 Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Hyperandrogenism. Dr Jack Biko. MB. BCh (Wits), MMED O & G (Pret), FCOG (SA), Dip Advanced Endoscopic Surgery(Kiel, Germany)
, MMED O & G (Pret), FCOG (SA), Dip Advanced Endoscopic Surgery(Kiel, Germany)") Hyperandrogenism Dr Jack Biko MB. BCh (Wits), MMED O & G (Pret), FCOG (SA), Dip Advanced Endoscopic Surgery(Kiel, Germany) 2012 Hyperandrogenism Excessive production of androgens Adrenal glands main source
Hyperandrogenism Dr Jack Biko MB. BCh (Wits), MMED O & G (Pret), FCOG (SA), Dip Advanced Endoscopic Surgery(Kiel, Germany) 2012 Hyperandrogenism Excessive production of androgens Adrenal glands main source
AMBIGUOUS GENITALIA & CONGENITAL ADRENALHYPERPLASIA
 AMBIGUOUS GENITALIA & CONGENITAL ADRENALHYPERPLASIA BY Dr Numair Ali sheikh FCPS PGT I Department Of Pediatrics BBH RWP AMBIGUOUS GENITALIA Children born with ambiguous genitalia may be subdivided in to
AMBIGUOUS GENITALIA & CONGENITAL ADRENALHYPERPLASIA BY Dr Numair Ali sheikh FCPS PGT I Department Of Pediatrics BBH RWP AMBIGUOUS GENITALIA Children born with ambiguous genitalia may be subdivided in to
The Management of adrenal incidentaloma
 The Management of adrenal incidentaloma Dimitrios Linos, MD Director of Surgery, Hygeia Hospital, Athens, Greece Consultant in Surgery, Massachusetts General Hospital, Boston, USA 8 th Postgraduate Course
The Management of adrenal incidentaloma Dimitrios Linos, MD Director of Surgery, Hygeia Hospital, Athens, Greece Consultant in Surgery, Massachusetts General Hospital, Boston, USA 8 th Postgraduate Course
THE FACTS YOU NEED TO KNOW
 PHEOCHROMOCYTOMA THE FACTS YOU NEED TO KNOW Pheochromocytoma is a part of the pheochromocytoma and paraganglioma group of syndromes. A pheochromocytoma is a tumor arising in the adrenal gland medulla.
PHEOCHROMOCYTOMA THE FACTS YOU NEED TO KNOW Pheochromocytoma is a part of the pheochromocytoma and paraganglioma group of syndromes. A pheochromocytoma is a tumor arising in the adrenal gland medulla.
Updates in primary hyperaldosteronism and the rule
 Updates in primary hyperaldosteronism and the 20-50 rule I. David Weiner, M.D. C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University of
Updates in primary hyperaldosteronism and the 20-50 rule I. David Weiner, M.D. C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University of
Morbidity & Mortality. Mark H. Tseng MD SUNY Downstate Medical Center Lutheran Medical Center December 16, 2005
 Morbidity & Mortality Mark H. Tseng MD SUNY Downstate Medical Center Lutheran Medical Center December 16, 2005 Case presentation Pt is a xx year old Asian woman who present to the ED with cc of epigastric
Morbidity & Mortality Mark H. Tseng MD SUNY Downstate Medical Center Lutheran Medical Center December 16, 2005 Case presentation Pt is a xx year old Asian woman who present to the ED with cc of epigastric
Updates in primary hyperaldosteronism and the rule
 Updates in primary hyperaldosteronism and the 20-50 rule I. David Weiner, M.D. Professor of Medicine and Physiology and Functional Genomics University of Florida College of Medicine and NF/SGVHS The 20-50
Updates in primary hyperaldosteronism and the 20-50 rule I. David Weiner, M.D. Professor of Medicine and Physiology and Functional Genomics University of Florida College of Medicine and NF/SGVHS The 20-50
An easily missed diagnosis: 17-alpha-hydroxylase/17,20-lyase deficiency
 The Turkish Journal of Pediatrics 2015; 57: 277-281 Case Report An easily missed diagnosis: 17-alpha-hydroxylase/17,20-lyase deficiency Banu Küçükemre-Aydın 1, Özlem Öğrendil-Yanar 1, Ilmay Bilge 2, Firdevs
The Turkish Journal of Pediatrics 2015; 57: 277-281 Case Report An easily missed diagnosis: 17-alpha-hydroxylase/17,20-lyase deficiency Banu Küçükemre-Aydın 1, Özlem Öğrendil-Yanar 1, Ilmay Bilge 2, Firdevs
Adrenal incidentaloma
 Adrenal incidentaloma Prevalence 5% post-mortem series 4% CT series 6-20% CT series in patients with Hx extra-adrenal malignancy Commoner with increasing age Associated with adrenal hyperfunction in 15%
Adrenal incidentaloma Prevalence 5% post-mortem series 4% CT series 6-20% CT series in patients with Hx extra-adrenal malignancy Commoner with increasing age Associated with adrenal hyperfunction in 15%
Adrenal Disorders for the USMLE, Step One: Abnormalities of the Fasciculata: Hypercortisolism
 Adrenal Disorders for the USMLE, Step One: Abnormalities of the Fasciculata: Hypercortisolism Howard Sachs, MD Patients Course, 2017 Associate Professor of Clinical Medicine UMass Medical School Adrenal
Adrenal Disorders for the USMLE, Step One: Abnormalities of the Fasciculata: Hypercortisolism Howard Sachs, MD Patients Course, 2017 Associate Professor of Clinical Medicine UMass Medical School Adrenal
Laura Stewart, MD, FRCPC Clinical Associate Professor Division of Pediatric Endocrinology University of British Columbia
 Precocious Puberty Laura Stewart, MD, FRCPC Clinical Associate Professor Division of Pediatric Endocrinology University of British Columbia Faculty Disclosure Faculty: Laura Stewart No relationships with
Precocious Puberty Laura Stewart, MD, FRCPC Clinical Associate Professor Division of Pediatric Endocrinology University of British Columbia Faculty Disclosure Faculty: Laura Stewart No relationships with
Hypertension Update. Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy
 Hypertension Update Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy Introduction 1/3 of US adults have HTN More prevalent in non-hispanic
Hypertension Update Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy Introduction 1/3 of US adults have HTN More prevalent in non-hispanic
Spironolactone has not been demonstrated to elevate serum uric acid, to precipitate gout or to alter carbohydrate metabolism.
 SPIRONE Composition Each tablet contains Spironolactone 100 mg. Tablets Action Spironolactone is a specific pharmacologic antagonist of aldosterone, acting primarily through competitive binding of receptors
SPIRONE Composition Each tablet contains Spironolactone 100 mg. Tablets Action Spironolactone is a specific pharmacologic antagonist of aldosterone, acting primarily through competitive binding of receptors
74. Hormone synthesis in the adrenal cortex. The glucocorticoids: biosynthesis, regulation, effects. Adrenal cortex is vital for life!
 74. Hormone synthesis in the adrenal cortex. The glucocorticoids: biosynthesis, regulation, effects. Adrenal cortex is vital for life! 5 g each Zona glomerulosa : Mineralocorticoids ALDOSTERON Zona fasciculata:
74. Hormone synthesis in the adrenal cortex. The glucocorticoids: biosynthesis, regulation, effects. Adrenal cortex is vital for life! 5 g each Zona glomerulosa : Mineralocorticoids ALDOSTERON Zona fasciculata:
Pheochromocytoma AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGY ILLINOIS CHAPTER OCTOBER 13, 2018
 Pheochromocytoma AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGY ILLINOIS CHAPTER OCTOBER 13, 2018 Steven A. De Jong, M.D., FACS, FACE Professor and Vice Chair of Surgery Chief, Division of General Surgery
Pheochromocytoma AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGY ILLINOIS CHAPTER OCTOBER 13, 2018 Steven A. De Jong, M.D., FACS, FACE Professor and Vice Chair of Surgery Chief, Division of General Surgery
9. Congenital Adrenal Hyperplasia (CAH)
") 9. Congenital Adrenal Hyperplasia (CAH) 9.0 Introduction Screening for congenital adrenal hyperplasia (CAH) has only been included in U.S. screening programs since 1987. The screening technique used is
9. Congenital Adrenal Hyperplasia (CAH) 9.0 Introduction Screening for congenital adrenal hyperplasia (CAH) has only been included in U.S. screening programs since 1987. The screening technique used is
Hypertension Update Background
 Hypertension Update Background Overview Aaron J. Friedberg, MD Assistant Professor, Clinical Division of General Internal Medicine The Ohio State University Wexner Medical Center Management Guideline Comparison
Hypertension Update Background Overview Aaron J. Friedberg, MD Assistant Professor, Clinical Division of General Internal Medicine The Ohio State University Wexner Medical Center Management Guideline Comparison
Secondary hypertension is defined as being
 Canadian Coalation for High Blood Pressure Prevention and Control Coalition Canadienne pour la Prévention et le Contrôle de l Hypertension Artérielle Secondary Hypertension: Diagnosis and Management Options
Canadian Coalation for High Blood Pressure Prevention and Control Coalition Canadienne pour la Prévention et le Contrôle de l Hypertension Artérielle Secondary Hypertension: Diagnosis and Management Options
Adrenal Incidentalomas. G Stephen DeCherney, MD, MPH Clinical Professor of Medicine Division of Endocrinology UNC School of Medicine
 Adrenal Incidentalomas G Stephen DeCherney, MD, MPH Clinical Professor of Medicine Division of Endocrinology UNC School of Medicine Disclosures No financial, investment, or consulting relationship with
Adrenal Incidentalomas G Stephen DeCherney, MD, MPH Clinical Professor of Medicine Division of Endocrinology UNC School of Medicine Disclosures No financial, investment, or consulting relationship with