Course n : (ex: Course 6) Sub-category: (ex: 6.4.) Date: ( ) Language:English/Romanian City:Bucharest Country:Romania Speaker: (Radu T.
|
|
|
- Coleen Cannon
- 5 years ago
- Views:
Transcription
 Date: (9-12-2015) Language:English/Romanian City:Bucharest")
1 Course n : (ex: Course 6) Sub-category: (ex: 6.4.) Date: ( ) Language:English/Romanian City:Bucharest Country:Romania Speaker: (Radu T. Stoica)



2 Dificulties in Pediatric Thoracic Anesthesia Dr. Radu T. Stoica Thoracic Anesthesia and Respiratory ICU

3 Why is so difficult?
4


5 Anathomy
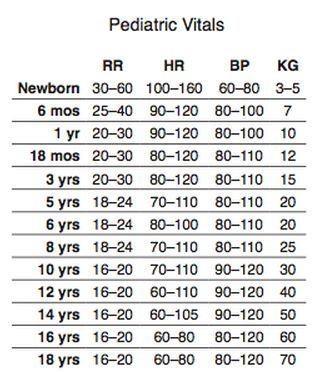
6 Physiology High metabolic rate (5-8 mlo 2 /kg/min) (2-3ml/kg/min adult) Tidal volume (6-7 ml/kg/min) High respiratory rate (40-60 breaths/min) High alveolar ventilation (130 ml/kg/min) Lung compliance is less while chest wall compliance is more than those in adults (reduced FRC and atelectasis) PEEP. Diaphragm has less oxidative type I fibers susceptible for fatigue. The work of breathing is composed of compliance and resistive components. The compliance work relative to tidal volume is nearly the same as in adult. The resistive work increases when breathing through ETT (4 th radius), and through circle system. FAST DESATURATION
7 Preoperative assessment - Clinical status of the child: underlying acute or chronic conditions that may impact the perioperative course - Infants have less specific signs: poor feeding, irritability, or change in sleep habits - Older children: dyspnea, cyanosis, wheezing, coughing, weight loss - If history of previous surgery: the perioperative course - Thoracic examination: asymmetric expansion and use of accessory muscles. auscultate for wheezes, rales, rhonchi, and absent breath sounds - Pulsoximetry - Venous HCO 3, elevated in children with chronic CO 2 Golianu B, Hammer GB, Pediatric thoracic anesthesia, Current Opinion in Anaesthesiology 2005, 18:5 11

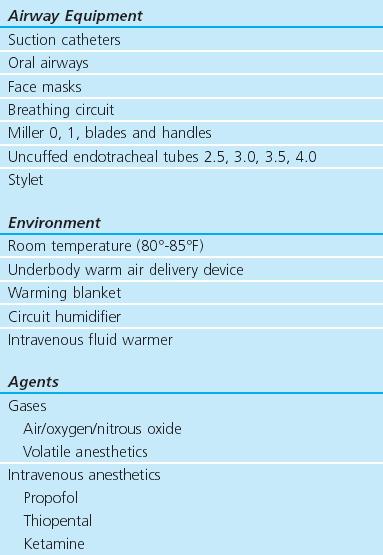
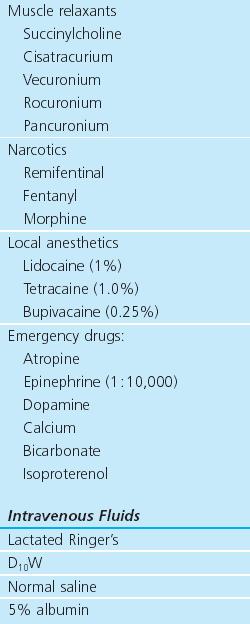
8 Preparing for anesthesia
9 +
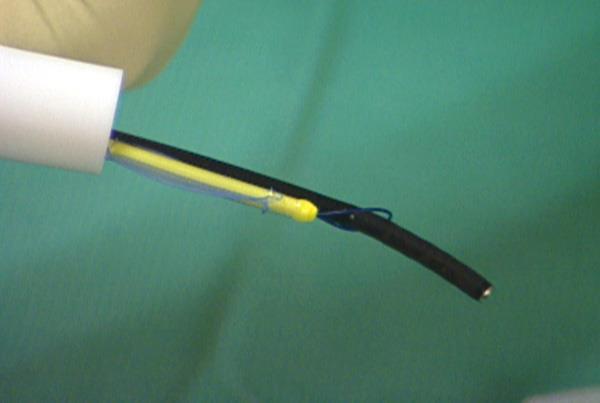
10 Equipment for lung separation Thoracothomy and VATS - Single Lumen Endotracheal Tube (ETT), cuffed or uncuffed intubate a mainstem bronchus - Balloon-Tipped Bronchial Blockers - Univent Tube - Double Lumen Tubes (DLT) Verify with FOB




11 Single lumen Univent Double lumen



12 Bronchial Blockers EZ-Blocker Fuji Cohen Arndt
13 Tube selection for single lung ventilation in children Age ETT (ID) BB (Fr) Univent (ID) DLT cuffed cuffed cuffed cuffed cuffed Golianu B, Hammer GB, Pediatric thoracic anesthesia, Current Opinion in Anaesthesiology 2005, 18:5 11
14 General anesthesia - Monitoring vital signs + Transcutaneous CO 2 monitoring - Induction of anesthesia: intravenous catheter, and tracheal intubation, arterial catheterization for most patients undergoing thoracotomy as well as those with severe lung disease having thoracoscopic surgery - Combination of general anesthesia with regional anesthesia and postoperative analgesia is particularly desirable for thoracotomy Ishibe Y, et al. The effect of thoracic epidural anesthesia on hypoxic pulmonary vasoconstriction in dogs: an analysis of the pressure-flow volume curve. Anesth Analg 1996; 82: General anesthesia: Inhalation an iv anesthesia. Not important interference with HPV. Muscle relaxants Frequent 100% FiO 2
15 Physiology of one-lung ventilation - Adults: oxygenation is optimal in lateral decubitus with the healthy lung dependent due to increased blood flow (gravitational and HPV) BETTER V/Q MACH - Infants: FRC is closer to residual volume. Airway closure likely to occur in the dependent lung even during tidal breathing. Soft, easily compressible rib cage an lower abdominal pressure WORST VENTILATION Low hydrostatic pressure gradient between the nondependent and dependent lung. WORST CIRCULATION WORST V/Q MACH
16 Pain assessment
17 Thoracic epidural - Thoracic epidural placement in infants and young children should be restricted to those experienced in the technique. - The procedure should be abandoned if difficulties are encountered. - In children 2 10 yr of age, the mean distance of the spinal cord from the dura at T9 10 vertebral level is 4.3 mm. - The thoracic vertebral spines are almost horizontal, which allows a midline approach to the thoracic epidural space. A paramedian approach is often required in adolescents. - In neonates and infants, catheters can be easily and consistently threaded to higher segmental levels from lower approaches. Insertion at a lumbar level is often possible and safer in infants compared with a direct thoracic approach. D. Patel, Epidural analgesia for children, Contin Educ Anaesth Crit Care Pain (2006) 6 (2):
18 63 children: 3 months to 18 yr and in weight from 3.2 kg to 78 kg - Intravascular placement was excluded using a test dose that consisted of 1 to 3 ml bupivacaine 0.25% with epinephrine (1:200,000). - Postoperative analgesia was provided by an initial bolus of 0.2 to 0.3 ml. kg - of bupivacaine 0.25% with 0.5 to 1.0 microg/kg -I fentanyl followed by a continuous infusion of bupivacaine 0.1% to 0.125% with 2 microg/ml fentanyl. Tobias JD, Lowe S, Thoracic epidural anesthesia in infants and children, 1993 Can J Anaesth, 40: Ganesh A et al, Efficacy of addition of fentanyl to epidural bupivacaine on postoperative analgesia after thoracotomy for lung resection in infantsanesthesiology. 2008;109:
19 Thoracic epidural HAMMER ANESTH ANALG PEDIATRIC THORACIC ANESTHESIA 2001;92:

20 -Positioning. Sitting or lateral decubitus. -Landmarks. Spinous process. Needle insertion point is 1 to 2 cm lateral to the superior aspect of he spinous process. -Technique.Use a 22-guage Tuohy needle. The insertion point: 0.5 to 1cm past the transverse process. Estimated depth: paravertebral space: 20 + (0.5 wt [kg]) = depth in mm Thoracic Paravertebral
, Extralobar sequestration (< 2years old), Pulmonary hypoplasia, Congenital")
, Esophageal atresia - Mediastinal (childhood) Limphomas, Neuroblastomas -")
21 Thoracic surgery pathology - Lesions of the trachea and bronchi Aquired Congenital - Lung parenchyma Pulmonary sequestrations (childhood or adult), Extralobar sequestration (< 2years old), Pulmonary hypoplasia, Congenital lobar emphysema, Bronchogenic cysts, Dermoid cysts, Cystic adenomatoid malformations, Metastasis - Esophagus Tracheoesophageal fistula (TEF), Esophageal atresia - Mediastinal (childhood) Limphomas, Neuroblastomas - Diaphragm Hernias
22 Tracheal surgery 1. FOB is used to evaluate the severity of the stenosis General anesthesia with spontaneous breathing, Local anesthesia on vocal cords 2. ETI, LAM, Rigid bronhoscopy for ventilation 3. Cricoid split procedure or laryngotracheoplasty (rib, auricular), stent 4. ETT (half size than tracheoscope) left in place 5. May require postoperative ventilation for a period of time 6. Rarely, repair of distal tracheal and bronchial stenosis may require cardiopulmonary bypass.
23 Anterior mediastinal mass (AMM) Danger of respiratory/circulatory colaps at induction!

24 Anterior mediastinal mass Preparing General Anesthesia - Devices and skilled personel! Rigid bronchoscope, FOB available Prepared for tracheostomy - Consider changing patient position Head elevated Lateral decubitus with CPAP for maintaining FRC - Anesthesia: Adequate IV lane Mask induction with spontaneous breathing Intubation without muscle relaxant or succinylcholine LMA if possible for biopsy of AMM! Large and symptomatic AMM may need ECMO or CPB - ICU bed available! Hammer GB Anaesthetic management of children with anterior mediastinal masses, Anaesthesia, 2008;63:
25 Foreign body - Degree of emergency: tracheal or respiratory distress Urgent FOB or rigid bronchoscopy in OR - Rigid bronchoscopy in most cases! - Anesthesia induction: under the fear of foreign body relocation! Spontaneos breathing: cough! IPPV: distal dislogement! under the fear of gastric aspiration in emergency cases! - i.v general anesthesia anesthesia during the procedure - Lateral port ventilation or HFJV - If spontanos ventilation is chosen: + topical anestesia on vocal cords Fidkowski CW, et al, The Anesthetic Considerations of Tracheobronchial Foreign Bodies in Children: A Literature Review of 12,979 Cases Anesth Analg 2010;111:

26 Conclusions - Knowledge of respiratory physiology and anatomy in pediatric patients - Devices and skills: special size FOB, Bronchial blockers, LM, one-lung ventilation - Use of regional anesthetic techniques - Anesthetic management in specific conditions: anterior mediastinal mass, foreign body

27 Children are totaly different!
Thoracic anaesthesia. Simon May
 Thoracic anaesthesia Simon May Contents Indications for lung isolation Ways of isolating lungs Placing a DLT Hypoxia on OLV Suitability for surgery Analgesia Key procedures Indications for lung isolation
Thoracic anaesthesia Simon May Contents Indications for lung isolation Ways of isolating lungs Placing a DLT Hypoxia on OLV Suitability for surgery Analgesia Key procedures Indications for lung isolation
INDEPENDENT LUNG VENTILATION
 INDEPENDENT LUNG VENTILATION Giuseppe A. Marraro, MD Director Anaesthesia and Intensive Care Department Paediatric Intensive Care Unit Fatebenefratelli and Ophthalmiatric Hospital Milan, Italy gmarraro@picu.it
INDEPENDENT LUNG VENTILATION Giuseppe A. Marraro, MD Director Anaesthesia and Intensive Care Department Paediatric Intensive Care Unit Fatebenefratelli and Ophthalmiatric Hospital Milan, Italy gmarraro@picu.it
Index. Note: Page numbers of article titles are in boldface type
 Index Note: Page numbers of article titles are in boldface type A Acute coronary syndrome, perioperative oxygen in, 599 600 Acute lung injury (ALI). See Lung injury and Acute respiratory distress syndrome.
Index Note: Page numbers of article titles are in boldface type A Acute coronary syndrome, perioperative oxygen in, 599 600 Acute lung injury (ALI). See Lung injury and Acute respiratory distress syndrome.
One Lung Ventilation in Obese patients
 One Lung Ventilation in Obese patients YUSNI PUSPITA DEPARTEMEN ANESTESIOLOGI DAN TERAPI INTENSIF FAKULTAS KEDOKTERAN UNIVERSITAS SRIWIJAYA/RSMH PALEMBANG One Lung Ventilation Lung isolation techniques
One Lung Ventilation in Obese patients YUSNI PUSPITA DEPARTEMEN ANESTESIOLOGI DAN TERAPI INTENSIF FAKULTAS KEDOKTERAN UNIVERSITAS SRIWIJAYA/RSMH PALEMBANG One Lung Ventilation Lung isolation techniques
J of Evolution of Med and Dent Sci/ eissn , pissn / Vol. 3/ Issue 65/Nov 27, 2014 Page 13644
 ANAESTHESIA FOR A PAEDIATRICS PATIENT POSTED FOR VIDEO: ASSISTED THORACOSCOPIC EXCISION OF AN ANTERIOR MEDIASTINAL MASS Sahajananda 1, K. T. Venkateshmurthy 2, Madhumala 3, Soumya Rohit 4, Sumaiya Tahseen
ANAESTHESIA FOR A PAEDIATRICS PATIENT POSTED FOR VIDEO: ASSISTED THORACOSCOPIC EXCISION OF AN ANTERIOR MEDIASTINAL MASS Sahajananda 1, K. T. Venkateshmurthy 2, Madhumala 3, Soumya Rohit 4, Sumaiya Tahseen
Fariba Rezaeetalab Associate Professor,Pulmonologist
 Fariba Rezaeetalab Associate Professor,Pulmonologist rezaitalabf@mums.ac.ir Patient related risk factors Procedure related risk factors Preoperative risk assessment Risk reduction strategies Age Obesity
Fariba Rezaeetalab Associate Professor,Pulmonologist rezaitalabf@mums.ac.ir Patient related risk factors Procedure related risk factors Preoperative risk assessment Risk reduction strategies Age Obesity
October Paediatric Respiratory Workbook APCP RESPIRATORY COMMITTEE
 October 2017 Paediatric Respiratory Workbook APCP RESPIRATORY COMMITTEE This workbook is designed to introduce to you the difference between paediatric and adult anatomy and physiology. It will also give
October 2017 Paediatric Respiratory Workbook APCP RESPIRATORY COMMITTEE This workbook is designed to introduce to you the difference between paediatric and adult anatomy and physiology. It will also give
FOREIGN BODY ASPIRATION in children. Dr. Xayyavong Bouathongthip, M.D Emergency department, children s hospital
 FOREIGN BODY ASPIRATION in children Dr. Xayyavong Bouathongthip, M.D Emergency department, children s hospital How common is choking? About 3,000 people die/year from choking Figure remained unchanged
FOREIGN BODY ASPIRATION in children Dr. Xayyavong Bouathongthip, M.D Emergency department, children s hospital How common is choking? About 3,000 people die/year from choking Figure remained unchanged
A neonate is any patient less than 45 weeks post conception regardless of chronological age.
 Case Log Definitions: A Guide for Fellows and Program Directors Recommendations from the Pediatric Anesthesia Program Directors Association Case Log Task Force January 2013 These recommendations represent
Case Log Definitions: A Guide for Fellows and Program Directors Recommendations from the Pediatric Anesthesia Program Directors Association Case Log Task Force January 2013 These recommendations represent
One-lung anaesthesia
 Jo Eastwood FRCA Ravi Mahajan DM FRCA One-lung anaesthesia (OLA) may be indicated in lung, oesophageal, mediastinal and spinal surgery (Table 1). This review examines preoperative considerations, physiology
Jo Eastwood FRCA Ravi Mahajan DM FRCA One-lung anaesthesia (OLA) may be indicated in lung, oesophageal, mediastinal and spinal surgery (Table 1). This review examines preoperative considerations, physiology
Tarek M Sarhan, Assistant professor of Anesthesiology, Faculty of Medicine, Alexandria University
 7 ANALGESIA FOR TRACHEOESOPHAGEAL FISTULA REPAIR IN NEONATES : A COMPARISON OF SINGLE SHOT THORACIC PARAVERTEBRAL BLOCK AND EPIDURAL BLOCK WITH ROPIVACAINE Tarek M Sarhan, Assistant professor of Anesthesiology,
7 ANALGESIA FOR TRACHEOESOPHAGEAL FISTULA REPAIR IN NEONATES : A COMPARISON OF SINGLE SHOT THORACIC PARAVERTEBRAL BLOCK AND EPIDURAL BLOCK WITH ROPIVACAINE Tarek M Sarhan, Assistant professor of Anesthesiology,
Disclosures. Learning Objectives. Coeditor/author. Associate Science Editor, American Heart Association
 Tracheotomy Challenges for airway specialists Elizabeth H. Sinz, MD Professor of Anesthesiology & Neurosurgery Associate Dean for Clinical Simulation Disclosures Coeditor/author Associate Science Editor,
Tracheotomy Challenges for airway specialists Elizabeth H. Sinz, MD Professor of Anesthesiology & Neurosurgery Associate Dean for Clinical Simulation Disclosures Coeditor/author Associate Science Editor,
Subject Index. Bacterial infection, see Suppurative lung disease, Tuberculosis
 Subject Index Abscess, virtual 107 Adenoidal hypertrophy, features 123 Airway bleeding, technique 49, 50 Airway stenosis, see Stenosis, airway Anaesthesia biopsy 47 complications 27, 28 flexible 23 26
Subject Index Abscess, virtual 107 Adenoidal hypertrophy, features 123 Airway bleeding, technique 49, 50 Airway stenosis, see Stenosis, airway Anaesthesia biopsy 47 complications 27, 28 flexible 23 26
Congenital Lung Malformations: Radiologic-Pathologic Correlation
 Acta Radiológica Portuguesa, Vol.XVIII, nº 70, pág. 51-60, Abr.-Jun., 2006 Congenital Lung Malformations: Radiologic-Pathologic Correlation Marilyn J. Siegel Mallinckrodt Institute of Radiology, Washington
Acta Radiológica Portuguesa, Vol.XVIII, nº 70, pág. 51-60, Abr.-Jun., 2006 Congenital Lung Malformations: Radiologic-Pathologic Correlation Marilyn J. Siegel Mallinckrodt Institute of Radiology, Washington
Cricoid pressure: useful or dangerous?
 Cricoid pressure: useful or dangerous? Francis VEYCKEMANS Cliniques Universitaires Saint Luc Bruxelles (2009) Controversial issue - Can J Anaesth 1997 JR Brimacombe - Pediatr Anesth 2002 JG Brock-Utne
Cricoid pressure: useful or dangerous? Francis VEYCKEMANS Cliniques Universitaires Saint Luc Bruxelles (2009) Controversial issue - Can J Anaesth 1997 JR Brimacombe - Pediatr Anesth 2002 JG Brock-Utne
2/3/2015. Anterior Mediastinal Masses and Lower Airway Problems
 es and Lower Airway Problems es and Lower Airway Problems 25 y.o. Female Ant. Mediastinal Mass Cervical Mediastinoscopy + Biopsy Most Important History? A) Dysphagia B) Fever C) Orthopnea D) Chest pain
es and Lower Airway Problems es and Lower Airway Problems 25 y.o. Female Ant. Mediastinal Mass Cervical Mediastinoscopy + Biopsy Most Important History? A) Dysphagia B) Fever C) Orthopnea D) Chest pain
PEMSS PROTOCOLS INVASIVE PROCEDURES
 PEMSS PROTOCOLS INVASIVE PROCEDURES Panhandle Emergency Medical Services System SURGICAL AND NEEDLE CRICOTHYROTOMY Inability to intubate is the primary indication for creating an artificial airway. Care
PEMSS PROTOCOLS INVASIVE PROCEDURES Panhandle Emergency Medical Services System SURGICAL AND NEEDLE CRICOTHYROTOMY Inability to intubate is the primary indication for creating an artificial airway. Care
Surgical Care at the District Hospital. EMERGENCY & ESSENTIAL SURGICAL CARE
 Surgical Care at the District Hospital 1 14 Practical Anesthesia Key Points 2 14.1 General Anesthesia Have a clear plan before starting anesthesia Never use an unfamiliar anesthetic technique in an emergency
Surgical Care at the District Hospital 1 14 Practical Anesthesia Key Points 2 14.1 General Anesthesia Have a clear plan before starting anesthesia Never use an unfamiliar anesthetic technique in an emergency
Tracheal stenosis in infants and children is typically characterized
 Slide Tracheoplasty for Congenital Tracheal Stenosis Peter B. Manning, MD Tracheal stenosis in infants and children is typically characterized by the presence of complete cartilaginous tracheal rings and
Slide Tracheoplasty for Congenital Tracheal Stenosis Peter B. Manning, MD Tracheal stenosis in infants and children is typically characterized by the presence of complete cartilaginous tracheal rings and
TRACHEOSTOMY. Tracheostomy means creation an artificial opening in the trachea with tracheostomy tube insertion
 TRACHEOSTOMY Definition Tracheostomy means creation an artificial opening in the trachea with tracheostomy tube insertion Indications for tracheostomy 1-upper airway obstruction with stridor, air hunger,
TRACHEOSTOMY Definition Tracheostomy means creation an artificial opening in the trachea with tracheostomy tube insertion Indications for tracheostomy 1-upper airway obstruction with stridor, air hunger,
Case Report Complete Obstruction of Endotracheal Tube in an Infant with a Retropharyngeal and Anterior Mediastinal Abscess
 Hindawi Case Reports in Pediatrics Volume 2017, Article ID 1848945, 4 pages https://doi.org/10.1155/2017/1848945 Case Report Complete Obstruction of Endotracheal Tube in an Infant with a Retropharyngeal
Hindawi Case Reports in Pediatrics Volume 2017, Article ID 1848945, 4 pages https://doi.org/10.1155/2017/1848945 Case Report Complete Obstruction of Endotracheal Tube in an Infant with a Retropharyngeal
An anterior mediastinal mass: delayed airway compression and using a double lumen tube for airway patency
 Case Report An anterior mediastinal mass: delayed airway compression and using a double lumen tube for airway patency Jeounghyuk Lee, Yong Chul Rim, Junyong In Department of Anesthesiology and Pain Medicine,
Case Report An anterior mediastinal mass: delayed airway compression and using a double lumen tube for airway patency Jeounghyuk Lee, Yong Chul Rim, Junyong In Department of Anesthesiology and Pain Medicine,
Comparison of the Berman Intubating Airway and the Williams Airway Intubator for fibreoptic orotracheal intubation in anaesthetised patients.
 Title Comparison of the Berman Intubating Airway and the Williams Airway Intubator for fibreoptic orotracheal intubation in anaesthetised patients Author(s) Greenland, KB; Ha, ID; Irwin, MG Citation Anaesthesia,
Title Comparison of the Berman Intubating Airway and the Williams Airway Intubator for fibreoptic orotracheal intubation in anaesthetised patients Author(s) Greenland, KB; Ha, ID; Irwin, MG Citation Anaesthesia,
Respiratory Anesthetic Emergencies in Oral and Maxillofacial Surgery. By: Lillian Han
 Respiratory Anesthetic Emergencies in Oral and Maxillofacial Surgery By: Lillian Han Background: Respiratory anesthetic emergencies are the most common complications during the administration of anesthesia
Respiratory Anesthetic Emergencies in Oral and Maxillofacial Surgery By: Lillian Han Background: Respiratory anesthetic emergencies are the most common complications during the administration of anesthesia
PROFESORES EXTRANJEROS Vol. 32. Supl. 1, Abril-Junio 2009 pp S220-S226. Lung separation techniques for thoracic surgery. Peter Slinger MD, FRCPC*
 medigraphic Artemisa en línea Anestesiología Mexicana de Revista ANTES C COLEGIO MEXICANO DE ANESTESIOLOGÍA A.C. SOCIEDAD MEXICANA DE ANESTESIOLOGÍA PROFESORES EXTRANJEROS Vol. 32. Supl. 1, Abril-Junio
medigraphic Artemisa en línea Anestesiología Mexicana de Revista ANTES C COLEGIO MEXICANO DE ANESTESIOLOGÍA A.C. SOCIEDAD MEXICANA DE ANESTESIOLOGÍA PROFESORES EXTRANJEROS Vol. 32. Supl. 1, Abril-Junio
Airway Management. Teeradej Kuptanon, MD
 Airway Management Teeradej Kuptanon, MD Outline Anatomy Detect difficult airway Rapid sequence intubation Difficult ventilation Difficult intubation Surgical airway access ICU setting Intubation Difficult
Airway Management Teeradej Kuptanon, MD Outline Anatomy Detect difficult airway Rapid sequence intubation Difficult ventilation Difficult intubation Surgical airway access ICU setting Intubation Difficult
According to their anatomical location, an anterior
 Case Report 258 Airway Obstruction by a Metastatic Mediastinal Tumor During Anesthesia Sheng-Huan Chen, MD; Jee-Ching Hsu, MD, PhD; Ping-Wing Lui, MD, PhD; Chih-Hung Chen 1, MD; Ching-Yue Yang, MD A case
Case Report 258 Airway Obstruction by a Metastatic Mediastinal Tumor During Anesthesia Sheng-Huan Chen, MD; Jee-Ching Hsu, MD, PhD; Ping-Wing Lui, MD, PhD; Chih-Hung Chen 1, MD; Ching-Yue Yang, MD A case
Neonatal Airway Disorders, Treatments, and Outcomes. Steven Goudy, MD Pediatric Otolaryngology Emory University Medical Center
 Neonatal Airway Disorders, Treatments, and Outcomes Steven Goudy, MD Pediatric Otolaryngology Emory University Medical Center Disclosure I have nothing to disclose Neonatal and Pediatric Tracheostomy Tracheostomy
Neonatal Airway Disorders, Treatments, and Outcomes Steven Goudy, MD Pediatric Otolaryngology Emory University Medical Center Disclosure I have nothing to disclose Neonatal and Pediatric Tracheostomy Tracheostomy
Jay B. Brodsky, M.D. Professor Department of Anesthesia tel: (650) Stanford University School of Medicine fax: (650)
 Stanford University School of Medicine fax: (650)") Jay B. Brodsky, M.D. Professor Department of Anesthesia tel: (650) 725-5869 Stanford University School of Medicine fax: (650) 725-8544 Stanford, CA, 94305, USA e-mail: jbrodsky@stanford.edu RELIABLE SEPARATION
Jay B. Brodsky, M.D. Professor Department of Anesthesia tel: (650) 725-5869 Stanford University School of Medicine fax: (650) 725-8544 Stanford, CA, 94305, USA e-mail: jbrodsky@stanford.edu RELIABLE SEPARATION
DIFFICULT AIRWAY MANAGMENT. Dr.N.SANTHOSH KUMAR MD ANESTHESIA (2 nd Yr)
") DIFFICULT AIRWAY MANAGMENT Dr.N.SANTHOSH KUMAR MD ANESTHESIA (2 nd Yr) AIRWAY MANAGEMENT AND MAINTAINING OXYGENATION ARE THE FUNDAMENTAL RESPONSIBILITIES OF ANY BASIC DOCTOR. TO MANAGE A DIFFICULT AIRWAY,
DIFFICULT AIRWAY MANAGMENT Dr.N.SANTHOSH KUMAR MD ANESTHESIA (2 nd Yr) AIRWAY MANAGEMENT AND MAINTAINING OXYGENATION ARE THE FUNDAMENTAL RESPONSIBILITIES OF ANY BASIC DOCTOR. TO MANAGE A DIFFICULT AIRWAY,
Unconscious exchange of air between lungs and the external environment Breathing
 Respiration Unconscious exchange of air between lungs and the external environment Breathing Two types External Exchange of carbon dioxide and oxygen between the environment and the organism Internal Exchange
Respiration Unconscious exchange of air between lungs and the external environment Breathing Two types External Exchange of carbon dioxide and oxygen between the environment and the organism Internal Exchange
All bedside percutaneously placed tracheostomies
 Page 1 of 5 Scope: All bedside percutaneously placed tracheostomies Population: All ICU personnel Outcomes: To standardize and outline the steps necessary to safely perform a percutaneous tracheostomy
Page 1 of 5 Scope: All bedside percutaneously placed tracheostomies Population: All ICU personnel Outcomes: To standardize and outline the steps necessary to safely perform a percutaneous tracheostomy
Lung sequestration and Scimitar syndrome
 Lung sequestration and Scimitar syndrome Imaging approaches M. Mearadji International Foundation for Pediatric Imaging Aid Rotterdam, The Netherlands Pulmonary sequestration Pulmonary sequestration (PS)
Lung sequestration and Scimitar syndrome Imaging approaches M. Mearadji International Foundation for Pediatric Imaging Aid Rotterdam, The Netherlands Pulmonary sequestration Pulmonary sequestration (PS)
Endoscopy. Pulmonary Endoscopy
 Pulmonary 1 Direct visualization of TB tree Developed in 1890 s to remove foreign bodies - rigid metal tube Advances added light system, Sx Flexible fiberoptic scopes introduced in early 1960 s 2 Used
Pulmonary 1 Direct visualization of TB tree Developed in 1890 s to remove foreign bodies - rigid metal tube Advances added light system, Sx Flexible fiberoptic scopes introduced in early 1960 s 2 Used
1. Influence of isoflurane exposure in pregnant rats on the learning and memory of offspring
 1. Influence of isoflurane exposure in pregnant rats on the learning and memory of offspring Huang W, Dong Y, Zhao G, et al. BMC Anesthesiology 2018 18:5 Concerns remain about possible effects of general
1. Influence of isoflurane exposure in pregnant rats on the learning and memory of offspring Huang W, Dong Y, Zhao G, et al. BMC Anesthesiology 2018 18:5 Concerns remain about possible effects of general
ISPUB.COM. Acquired Tracheoesophageal Fistula in Infancy: Communication is Key to Successful Outcome. A Reddy, J Iocono, R Brown Jr.
 ISPUB.COM The Internet Journal of Anesthesiology Volume 19 Number 1 Acquired Tracheoesophageal Fistula in Infancy: Communication is Key to Successful Outcome A Reddy, J Iocono, R Brown Jr. Citation A Reddy,
ISPUB.COM The Internet Journal of Anesthesiology Volume 19 Number 1 Acquired Tracheoesophageal Fistula in Infancy: Communication is Key to Successful Outcome A Reddy, J Iocono, R Brown Jr. Citation A Reddy,
Anatomy and Physiology. The airways can be divided in to parts namely: The upper airway. The lower airway.
 Airway management Anatomy and Physiology The airways can be divided in to parts namely: The upper airway. The lower airway. Non-instrumental airway management Head Tilt and Chin Lift Jaw Thrust Advanced
Airway management Anatomy and Physiology The airways can be divided in to parts namely: The upper airway. The lower airway. Non-instrumental airway management Head Tilt and Chin Lift Jaw Thrust Advanced
Chapter 124: Congenital Disorders of the Trachea. Bruce Benjamin
 Chapter 124: Congenital Disorders of the Trachea Bruce Benjamin Investigation of the larynx and pharynx may be incomplete in infants and children with congenital abnormalities without investigation of
Chapter 124: Congenital Disorders of the Trachea Bruce Benjamin Investigation of the larynx and pharynx may be incomplete in infants and children with congenital abnormalities without investigation of
ANESTHESIOLOGY CASE LOG CHANGES 2015
 ANESTHESIOLOGY CASE LOG CHANGES 2015 I. Case Information FORMER: 1. Role removed. 2. Setting removed. 3. Involved Morbidity has been renamed Life-Threatening Pathology. a. All former cases that included
ANESTHESIOLOGY CASE LOG CHANGES 2015 I. Case Information FORMER: 1. Role removed. 2. Setting removed. 3. Involved Morbidity has been renamed Life-Threatening Pathology. a. All former cases that included
Surgical indications: Non-malignant pulmonary diseases. Punnarerk Thongcharoen
 Surgical indications: Non-malignant pulmonary diseases Punnarerk Thongcharoen Non-malignant Malignant as a pathological term: Cancer Non-malignant = not cancer Malignant as an adjective: Disposed to cause
Surgical indications: Non-malignant pulmonary diseases Punnarerk Thongcharoen Non-malignant Malignant as a pathological term: Cancer Non-malignant = not cancer Malignant as an adjective: Disposed to cause
CHAPTER 7 Procedures on Respiratory System
 CHAPTER 7 Propunere noua clasificare proceduri folosind codificarea ICD-10-AM versiunea 3, 30 martie 2004 Procedures on Respiratory System BLOCK 520 Examination procedures on larynx 41764-03 Fibreoptic
CHAPTER 7 Propunere noua clasificare proceduri folosind codificarea ICD-10-AM versiunea 3, 30 martie 2004 Procedures on Respiratory System BLOCK 520 Examination procedures on larynx 41764-03 Fibreoptic
Wheeze. Dr Jo Harrison
 Wheeze Dr Jo Harrison 9.9.14 Wheeze - Physiology a continuous musical sound that lasts longer than 250 msec. can be high-pitched or low-pitched, consist of single or multiple notes, and occur during inspiration
Wheeze Dr Jo Harrison 9.9.14 Wheeze - Physiology a continuous musical sound that lasts longer than 250 msec. can be high-pitched or low-pitched, consist of single or multiple notes, and occur during inspiration
Cuffed Tracheal Tubes in Children - Myths and Facts. PD Dr. Markus Weiss Department of Anaesthesia University Children s Hospital Zurich Switzerland
 Cuffed Tracheal Tubes in Children - Myths and Department of Anaesthesia University Children s Hospital Zurich Switzerland PRO Reduced gas leak, low fresh gas flow Decreased atmospheric pollution Constant
Cuffed Tracheal Tubes in Children - Myths and Department of Anaesthesia University Children s Hospital Zurich Switzerland PRO Reduced gas leak, low fresh gas flow Decreased atmospheric pollution Constant
CASE PRIMERS. Pediatric Anesthesia Fellowship Program. Laryngotracheal Reconstruction (LTR) Tufts Medical Center
 Tufts Medical Center") CASE PRIMERS Pediatric Anesthesia Fellowship Program Tufts Medical Center Department of Anesthesiology and Perioperative Medicine Division of Pediatric Anesthesia 800 Washington Street, Box 298 Boston,
CASE PRIMERS Pediatric Anesthesia Fellowship Program Tufts Medical Center Department of Anesthesiology and Perioperative Medicine Division of Pediatric Anesthesia 800 Washington Street, Box 298 Boston,
A case of a neonate with a congenital laryngeal web: management of a difficult airway and intra-operative complications
 A case of a neonate with a congenital laryngeal web: management of a difficult airway and intra-operative complications Moderators: Marcellene Franzen, MD Fellow in Pediatric Anesthesiology Medical College
A case of a neonate with a congenital laryngeal web: management of a difficult airway and intra-operative complications Moderators: Marcellene Franzen, MD Fellow in Pediatric Anesthesiology Medical College
Equipment: NRP algorithm, MRSOPA table, medication chart, SpO 2 table Warm
 NRP Skills Stations Performance Skills Station OR Integrated Skills Station STATION: Assisting with and insertion of endotracheal tube (ETT) Equipment: NRP algorithm, MRSOPA table, medication chart, SpO
NRP Skills Stations Performance Skills Station OR Integrated Skills Station STATION: Assisting with and insertion of endotracheal tube (ETT) Equipment: NRP algorithm, MRSOPA table, medication chart, SpO
Options for Airway Management During Complex Resection and Reconstruction
 Options for Airway Management During Complex Resection and Reconstruction Brian E. Louie MD, FACS, FRCSC, MHA, MPH Director, Thoracic Research and Education Co-Director, Minimally Invasive Thoracic Surgery
Options for Airway Management During Complex Resection and Reconstruction Brian E. Louie MD, FACS, FRCSC, MHA, MPH Director, Thoracic Research and Education Co-Director, Minimally Invasive Thoracic Surgery
MANAGMENT OF ONE-LUNG VENTILATION
 MANAGMENT OF ONE-LUNG VENTILATION A. NEYRINCK, MD, PhD VERSION MARCH 2013 DOUBLE-LUMEN TUBE (DLT) OR BRONCHIAL BLOCKER (BB) FOR ONE-LUNG VENTILATION (OLV) OLV LUNG ISOLATION LUNG SEPARATION to avoid contamination
MANAGMENT OF ONE-LUNG VENTILATION A. NEYRINCK, MD, PhD VERSION MARCH 2013 DOUBLE-LUMEN TUBE (DLT) OR BRONCHIAL BLOCKER (BB) FOR ONE-LUNG VENTILATION (OLV) OLV LUNG ISOLATION LUNG SEPARATION to avoid contamination
Lung Injury and Protection in the Perioperative Period
 J. Earl Wynands Lung Injury and Protection in the Perioperative Period Non-injured Lungs: Perioperative Experience (Surgeon) Injured Lungs: Anesthesiologist 78 y.o. Male, Chronic Gallstone Pancreatitis,
J. Earl Wynands Lung Injury and Protection in the Perioperative Period Non-injured Lungs: Perioperative Experience (Surgeon) Injured Lungs: Anesthesiologist 78 y.o. Male, Chronic Gallstone Pancreatitis,
REGIONAL/LOCAL ANESTHESIA and OBESITY
 REGIONAL/LOCAL ANESTHESIA and OBESITY Jay B. Brodsky, MD Stanford University School of Medicine Jbrodsky@stanford.edu Potential Advantages Regional compared to General Anesthesia Minimal intra-operative
REGIONAL/LOCAL ANESTHESIA and OBESITY Jay B. Brodsky, MD Stanford University School of Medicine Jbrodsky@stanford.edu Potential Advantages Regional compared to General Anesthesia Minimal intra-operative
CAE Healthcare Human Patient Simulator (HPS)
") CAE Healthcare Human Patient Simulator (HPS) The Human Patient Simulator, HPS, is a tethered simulator that is capable of patient assessment and treatment including mechanical ventilation and anesthesia.
CAE Healthcare Human Patient Simulator (HPS) The Human Patient Simulator, HPS, is a tethered simulator that is capable of patient assessment and treatment including mechanical ventilation and anesthesia.
RESPIRATORY FAILURE. Michael Kelly, MD Division of Pediatric Critical Care Dept. of Pediatrics
 RESPIRATORY FAILURE Michael Kelly, MD Division of Pediatric Critical Care Dept. of Pediatrics What talk is he giving? DO2= CO * CaO2 CO = HR * SV CaO2 = (Hgb* SaO2 * 1.34) + (PaO2 * 0.003) Sound familiar??
RESPIRATORY FAILURE Michael Kelly, MD Division of Pediatric Critical Care Dept. of Pediatrics What talk is he giving? DO2= CO * CaO2 CO = HR * SV CaO2 = (Hgb* SaO2 * 1.34) + (PaO2 * 0.003) Sound familiar??
Therapist Written RRT Examination Detailed Content Outline
 I. PATIENT DATA EVALUATION AND RECOMMENDATIONS 4 7 17 28 A. Review Data in the Patient Record 1 4 0 5 1. Patient history e.g., present illness admission notes respiratory care orders medication history
I. PATIENT DATA EVALUATION AND RECOMMENDATIONS 4 7 17 28 A. Review Data in the Patient Record 1 4 0 5 1. Patient history e.g., present illness admission notes respiratory care orders medication history
Other methods for maintaining the airway (not definitive airway as still unprotected):
:") Page 56 Where anaesthetic skills and drugs are available, endotracheal intubation is the preferred method of securing a definitive airway. This technique comprises: rapid sequence induction of anaesthesia
Page 56 Where anaesthetic skills and drugs are available, endotracheal intubation is the preferred method of securing a definitive airway. This technique comprises: rapid sequence induction of anaesthesia
Recognizing the Difficult Airway in Pediatric Patients. Nancy L. Glass, MD, MBA,
 Recognizing the Difficult Airway in Pediatric Patients Nancy L. Glass, MD, MBA, FAAP nglass@bcm.edu @DrNancyGlass1 None Disclosures Learning Objectives At the end of this presentation, participants will
Recognizing the Difficult Airway in Pediatric Patients Nancy L. Glass, MD, MBA, FAAP nglass@bcm.edu @DrNancyGlass1 None Disclosures Learning Objectives At the end of this presentation, participants will
Collaborating with interventional pulmonology in managing a massive tracheoesophageal fistula that extends from cricoid to carina: a case report
 DOI 10.1186/s40981-017-0133-2 CASE REPORT Collaborating with interventional pulmonology in managing a massive tracheoesophageal fistula that extends from cricoid to carina: a case report Luis E. Tollinche
DOI 10.1186/s40981-017-0133-2 CASE REPORT Collaborating with interventional pulmonology in managing a massive tracheoesophageal fistula that extends from cricoid to carina: a case report Luis E. Tollinche
Author's Accepted Manuscript
 Author's Accepted Manuscript One-lung ventilation via tracheostomy and left endobronchial microlaryngeal tube Stephen Howell MD, Monica Ata MD, Matthew Ellison MD, Colin Wilson MD www.elsevier.com/locate/buildenv
Author's Accepted Manuscript One-lung ventilation via tracheostomy and left endobronchial microlaryngeal tube Stephen Howell MD, Monica Ata MD, Matthew Ellison MD, Colin Wilson MD www.elsevier.com/locate/buildenv
POSTGRADUATE INSTITUTE OF MEDICINE UNIVERSITY OF COLOMBO. MD (ANAESTHESIOLOGY) FINAL EXAMINATION AUGUST 2011 Time : 1.00 p.m p.m.
 FINAL EXAMINATION AUGUST 2011 Time : 1.00 p.m p.m.") POSTGRADUATE INSTITUTE OF MEDICINE UNIVERSITY OF COLOMBO MD (ANAESTHESIOLOGY) FINAL EXAMINATION AUGUST 2011 Date : 5 th August 2011 Time : 1.00 p.m. 4.00 p.m. Answer any three questions. Answer each question
POSTGRADUATE INSTITUTE OF MEDICINE UNIVERSITY OF COLOMBO MD (ANAESTHESIOLOGY) FINAL EXAMINATION AUGUST 2011 Date : 5 th August 2011 Time : 1.00 p.m. 4.00 p.m. Answer any three questions. Answer each question
Unusual presentation of complete tracheal rings in a 15 year old trauma patient
 Unusual presentation of complete tracheal rings in a 15 year old trauma patient B. S. Schmidt 1, E. J. Herschmiller 2, R. J. Jarrah 1, T. A. Nakagawa 1 1 Department of Anesthesiology (Section on Pediatric
Unusual presentation of complete tracheal rings in a 15 year old trauma patient B. S. Schmidt 1, E. J. Herschmiller 2, R. J. Jarrah 1, T. A. Nakagawa 1 1 Department of Anesthesiology (Section on Pediatric
Applied Physiology of One Lung Ventilation
 Applied Physiology of One Lung Ventilation One Lung Ventilation Usual situation Thoracic surgery Lateral decubitus position GA, paralysis, PPV Non-dependant lung collapsed and non-ventilated Chest may
Applied Physiology of One Lung Ventilation One Lung Ventilation Usual situation Thoracic surgery Lateral decubitus position GA, paralysis, PPV Non-dependant lung collapsed and non-ventilated Chest may
A challenging anesthetic management of acquired tracheo-esophageal fistula operation
 CASE REPORT Yazıcıoğlu et al. 1 PEER REVIEWED OPEN ACCESS A challenging anesthetic management of acquired tracheo-esophageal fistula operation Hija Yazıcıoğlu, Bilfer Özler, Büşra Tezcan, Mahmut Subaşı,
CASE REPORT Yazıcıoğlu et al. 1 PEER REVIEWED OPEN ACCESS A challenging anesthetic management of acquired tracheo-esophageal fistula operation Hija Yazıcıoğlu, Bilfer Özler, Büşra Tezcan, Mahmut Subaşı,
Intravascular Ultrasound (IVUS) and Optical Coherence Tomography (OCT)
 and Optical Coherence Tomography (OCT)") Intravascular Ultrasound (IVUS) and Optical Coherence Tomography (OCT) Clare McLaren Great Ormond Street Hospital London Introduction IVUS and OCT supplementary techniques to angiography provide information
Intravascular Ultrasound (IVUS) and Optical Coherence Tomography (OCT) Clare McLaren Great Ormond Street Hospital London Introduction IVUS and OCT supplementary techniques to angiography provide information
Lecture 2: Clinical anatomy of thoracic cage and cavity II
 Lecture 2: Clinical anatomy of thoracic cage and cavity II Dr. Rehan Asad At the end of this session, the student should be able to: Identify and discuss clinical anatomy of mediastinum such as its deflection,
Lecture 2: Clinical anatomy of thoracic cage and cavity II Dr. Rehan Asad At the end of this session, the student should be able to: Identify and discuss clinical anatomy of mediastinum such as its deflection,
I. Subject: Continuous Positive Airway Pressure CPAP by Continuous Flow Device
 I. Subject: Continuous Positive Airway Pressure CPAP by Continuous Flow Device II. Policy: Continuous Positive Airway Pressure CPAP by the Down's system will be instituted by Respiratory Therapy personnel
I. Subject: Continuous Positive Airway Pressure CPAP by Continuous Flow Device II. Policy: Continuous Positive Airway Pressure CPAP by the Down's system will be instituted by Respiratory Therapy personnel
Double-lumen endotracheal tubes (DLTs) are used
 are used") Case Report 503 Tension Pneumothorax Complicated by Double-Lumen Endotracheal Tube Intubation Chia-Chun Huang, MD; An-Hsun Chou, MD; Hung-Pin Liu, MD; Chee-Yueu Ho, MD; Min-Wein Yun, MD Tension pneumothorax
Case Report 503 Tension Pneumothorax Complicated by Double-Lumen Endotracheal Tube Intubation Chia-Chun Huang, MD; An-Hsun Chou, MD; Hung-Pin Liu, MD; Chee-Yueu Ho, MD; Min-Wein Yun, MD Tension pneumothorax
1 Chapter 40 Advanced Airway Management 2 Advanced Airway Management The advanced airway management techniques discussed in this chapter are to
 1 Chapter 40 Advanced Airway Management 2 Advanced Airway Management The advanced airway management techniques discussed in this chapter are to introduce the EMT-B student to these procedures only. In
1 Chapter 40 Advanced Airway Management 2 Advanced Airway Management The advanced airway management techniques discussed in this chapter are to introduce the EMT-B student to these procedures only. In
Milestone Guide. CBD Anesthesia
 Table of Contents Department of Anesthesiology Foundations 1 Airway 1 Pharmacology 1 Physiology 1 Common Uncomplicated Anesthetics Practice 2 Obstetrics 2 Pain 2 Core 3 Perioperative Medicine 3 Complex
Table of Contents Department of Anesthesiology Foundations 1 Airway 1 Pharmacology 1 Physiology 1 Common Uncomplicated Anesthetics Practice 2 Obstetrics 2 Pain 2 Core 3 Perioperative Medicine 3 Complex
Chapter 40 Advanced Airway Management
 1 2 3 4 5 Chapter 40 Advanced Airway Management Advanced Airway Management The advanced airway management techniques discussed in this chapter are to introduce the EMT-B student to these procedures only.
1 2 3 4 5 Chapter 40 Advanced Airway Management Advanced Airway Management The advanced airway management techniques discussed in this chapter are to introduce the EMT-B student to these procedures only.
Advanced Airway Management. University of Colorado Medical School Rural Track
 Advanced Airway Management University of Colorado Medical School Rural Track Advanced Airway Management Basic Airway Management Airway Suctioning Oxygen Delivery Methods Laryngeal Mask Airway ET Intubation
Advanced Airway Management University of Colorado Medical School Rural Track Advanced Airway Management Basic Airway Management Airway Suctioning Oxygen Delivery Methods Laryngeal Mask Airway ET Intubation
ENDOTRACHEAL INTUBATION POLICY
 POLICY Indications: Ineffective ventilation with mask and t-piece, or mask and bag technique Inability to maintain a patent airway Need or anticipation of need for prolonged ventilation Need for endotracheal
POLICY Indications: Ineffective ventilation with mask and t-piece, or mask and bag technique Inability to maintain a patent airway Need or anticipation of need for prolonged ventilation Need for endotracheal
Thoracic Anesthesia Can Be a Pleasure!
 Thoracic Anesthesia Can Be a Pleasure! Tips and Tricks For Maximizing Success Karen Sibert, MD Associate Clinical Professor Department of Anesthesiology & Perioperative Medicine David Geffen School of
Thoracic Anesthesia Can Be a Pleasure! Tips and Tricks For Maximizing Success Karen Sibert, MD Associate Clinical Professor Department of Anesthesiology & Perioperative Medicine David Geffen School of
Overview. The Respiratory System. Chapter 18. Respiratory Emergencies 9/11/2012
 Chapter 18 Respiratory Emergencies Slide 1 Overview Respiratory System Review Anatomy Physiology Breathing Assessment Adequate Breathing Breathing Difficulty Focused History and Physical Examination Emergency
Chapter 18 Respiratory Emergencies Slide 1 Overview Respiratory System Review Anatomy Physiology Breathing Assessment Adequate Breathing Breathing Difficulty Focused History and Physical Examination Emergency
Preoperative Workup for Pulmonary Resection. Kristen Bridges, M.D. Richmond University Medical Center January 21, 2016
 Preoperative Workup for Pulmonary Resection Kristen Bridges, M.D. Richmond University Medical Center January 21, 2016 Patient Presentation 50 yo male with 70 pack year smoking history Large R hilar lung
Preoperative Workup for Pulmonary Resection Kristen Bridges, M.D. Richmond University Medical Center January 21, 2016 Patient Presentation 50 yo male with 70 pack year smoking history Large R hilar lung
External trauma (MVA, surf board, assault, etc.) Internal trauma (Endotracheal intubation, tracheostomy) Other
 Internal trauma (Endotracheal intubation, tracheostomy) Other") Etiology External trauma (MVA, surf board, assault, etc.) Internal trauma (Endotracheal intubation, tracheostomy) Other Systemic diseases (vasculitis, etc.) Chemo/XRT Idiopathic Trans nasal Esophagoscope
Etiology External trauma (MVA, surf board, assault, etc.) Internal trauma (Endotracheal intubation, tracheostomy) Other Systemic diseases (vasculitis, etc.) Chemo/XRT Idiopathic Trans nasal Esophagoscope
Tracheal Trauma: Management and Treatment. Kosmas Iliadis, MD, PhD, FECTS
 Tracheal Trauma: Management and Treatment Kosmas Iliadis, MD, PhD, FECTS Thoracic Surgeon Director of Thoracic Surgery Department Hygeia Hospital, Athens INTRODUCTION Heterogeneous group of injuries mechanism
Tracheal Trauma: Management and Treatment Kosmas Iliadis, MD, PhD, FECTS Thoracic Surgeon Director of Thoracic Surgery Department Hygeia Hospital, Athens INTRODUCTION Heterogeneous group of injuries mechanism
BIOE221. Session 5. Examination of Thorax- Respiratory system. Bioscience Department. Endeavour College of Natural Health endeavour.edu.
 BIOE221 Session 5 Examination of Thorax- Respiratory system Bioscience Department Session Objectives Understand the structure of the thorax and the organs contained in this cavity Understand the importance
BIOE221 Session 5 Examination of Thorax- Respiratory system Bioscience Department Session Objectives Understand the structure of the thorax and the organs contained in this cavity Understand the importance
TRACHEOBRONCHIAL FOREIGN BODY REMOVAL ADVICE IN DOGS AND CATS
 Vet Times The website for the veterinary profession https://www.vettimes.co.uk TRACHEOBRONCHIAL FOREIGN BODY REMOVAL ADVICE IN DOGS AND CATS Author : MIKE STAFFORD-JOHNSON, MIKE MARTIN Categories : Vets
Vet Times The website for the veterinary profession https://www.vettimes.co.uk TRACHEOBRONCHIAL FOREIGN BODY REMOVAL ADVICE IN DOGS AND CATS Author : MIKE STAFFORD-JOHNSON, MIKE MARTIN Categories : Vets
Patient Management Code Blue in the CT Suite
 Patient Management Code Blue in the CT Suite David Stultz, MD November 28, 2001 Case Presentation A 53-year-old woman experienced acute respiratory distress during an IV contrast enhanced CT scan of the
Patient Management Code Blue in the CT Suite David Stultz, MD November 28, 2001 Case Presentation A 53-year-old woman experienced acute respiratory distress during an IV contrast enhanced CT scan of the
Therapeutic Bronchoscopy Etiology - Benign Stenosis Post - intubation Trauma Post - operative Inflammatory Idiopathic
 Endobronchial Palliation of Airway Disease Douglas E. Wood, MD Professor and Chief Division of Cardiothoracic Surgery Vice-Chair, Department of Surgery Endowed Chair in Lung Cancer Research University
Endobronchial Palliation of Airway Disease Douglas E. Wood, MD Professor and Chief Division of Cardiothoracic Surgery Vice-Chair, Department of Surgery Endowed Chair in Lung Cancer Research University
The Pediatric Patient. Morgen Bernius, MD NCEMS Conference February 24, 2007
 The Pediatric Patient Morgen Bernius, MD NCEMS Conference February 24, 2007 Rule #1: Everyone Loves the Pediatric Patient Pediatrics in EMS Approximately 10% of all EMS treatment is for children younger
The Pediatric Patient Morgen Bernius, MD NCEMS Conference February 24, 2007 Rule #1: Everyone Loves the Pediatric Patient Pediatrics in EMS Approximately 10% of all EMS treatment is for children younger
Subspecialty Rotation: Anesthesia
 Subspecialty Rotation: Anesthesia Faculty: John Heaton, M.D. GOAL: Maintenance of Airway Patency and Oxygenation. Recognize and manage upper airway obstruction and desaturation. Recognize and manage upper
Subspecialty Rotation: Anesthesia Faculty: John Heaton, M.D. GOAL: Maintenance of Airway Patency and Oxygenation. Recognize and manage upper airway obstruction and desaturation. Recognize and manage upper
Life-threatening check valve formation due to tracheobronchial aspergillosis
 Matsuura et al. JA Clinical Reports (2015) 1:17 DOI 10.1186/s40981-015-0022-5 CASE REPORT Life-threatening check valve formation due to tracheobronchial aspergillosis Hideki Matsuura, Satoki Inoue *, Kazuaki
Matsuura et al. JA Clinical Reports (2015) 1:17 DOI 10.1186/s40981-015-0022-5 CASE REPORT Life-threatening check valve formation due to tracheobronchial aspergillosis Hideki Matsuura, Satoki Inoue *, Kazuaki
Difficult Airway. Victor M. Gomez, M.D. Pulmonary Critical Care Medicine Medical City Dallas Hospital
 Difficult Airway Victor M. Gomez, M.D. Pulmonary Critical Care Medicine Medical City Dallas Hospital Difficult Airway Definition Predicting a difficult airway Preparing for a difficult airway Extubation
Difficult Airway Victor M. Gomez, M.D. Pulmonary Critical Care Medicine Medical City Dallas Hospital Difficult Airway Definition Predicting a difficult airway Preparing for a difficult airway Extubation
Foundation in Critical Care Nursing. Airway / Respiratory / Workbook
 Foundation in Critical Care Nursing Airway / Respiratory / Workbook Airway Anatomy: Please label the following: Tongue Larynx Epiglottis Pharynx Trachea Vertebrae Oesophagus Where is the ET (endotracheal)
Foundation in Critical Care Nursing Airway / Respiratory / Workbook Airway Anatomy: Please label the following: Tongue Larynx Epiglottis Pharynx Trachea Vertebrae Oesophagus Where is the ET (endotracheal)
Life-Threatening Respiratory Distress from Mediastinal Masses in Infants
 Life-Threatening Respiratory Distress from Mediastinal Masses in Infants J. Alex Haller, Jr., M.D., Dennis W. Shermeta, M.D., James S. Donahoo, M.D., and John J. White, M.D. ABSTRACT From 1972 through
Life-Threatening Respiratory Distress from Mediastinal Masses in Infants J. Alex Haller, Jr., M.D., Dennis W. Shermeta, M.D., James S. Donahoo, M.D., and John J. White, M.D. ABSTRACT From 1972 through
Handling Common Problems & Pitfalls During. Oxygen desaturation in patients receiving mechanical ventilation ACUTE SEVERE RESPIRATORY FAILURE
 Handling Common Problems & Pitfalls During ACUTE SEVERE RESPIRATORY FAILURE Pravit Jetanachai, MD QSNICH Oxygen desaturation in patients receiving mechanical ventilation Causes of oxygen desaturation 1.
Handling Common Problems & Pitfalls During ACUTE SEVERE RESPIRATORY FAILURE Pravit Jetanachai, MD QSNICH Oxygen desaturation in patients receiving mechanical ventilation Causes of oxygen desaturation 1.
1 Chapter 13 Respiratory Emergencies 2 Respiratory Distress Patients often complain about. Shortness of breath Symptom of many different Cause can be
 1 Chapter 13 Respiratory Emergencies 2 Respiratory Distress Patients often complain about. Shortness of breath Symptom of many different Cause can be difficult to determine. Even for physician in hospital
1 Chapter 13 Respiratory Emergencies 2 Respiratory Distress Patients often complain about. Shortness of breath Symptom of many different Cause can be difficult to determine. Even for physician in hospital
Endotracheal Intubation in a Neonate with Esophageal Atresia and Trachea-Esophageal Fistula: Pitfalls and Techniques. Bharti Taneja,* Kirti N Saxena
 Journal of Neonatal Surgery 2014;3(2):18 REVIEW ARTICLE Endotracheal Intubation in a Neonate with Esophageal Atresia and Trachea-Esophageal Fistula: Pitfalls and Bharti Taneja,* Kirti N Saxena Department
Journal of Neonatal Surgery 2014;3(2):18 REVIEW ARTICLE Endotracheal Intubation in a Neonate with Esophageal Atresia and Trachea-Esophageal Fistula: Pitfalls and Bharti Taneja,* Kirti N Saxena Department
Alyssa Brzenski MD May 2, 2012
 Alyssa Brzenski MD May 2, 2012 Overview Background Pre repair bronchoscopy Thorascopic repair To extubate or not? Esophageal atresia treatment of long gap esophageal atresia Complications following TEF/EA
Alyssa Brzenski MD May 2, 2012 Overview Background Pre repair bronchoscopy Thorascopic repair To extubate or not? Esophageal atresia treatment of long gap esophageal atresia Complications following TEF/EA
Waitin In The Wings. Esophageal/Tracheal Double Lumen Airway (Combitube ) Indications and Use for the Pre-Hospital Provider
 Indications and Use for the Pre-Hospital Provider") Waitin In The Wings Esophageal/Tracheal Double Lumen Airway (Combitube ) Indications and Use for the Pre-Hospital Provider 1 CombiTube Kit General Description The CombiTube is A double-lumen tube with
Waitin In The Wings Esophageal/Tracheal Double Lumen Airway (Combitube ) Indications and Use for the Pre-Hospital Provider 1 CombiTube Kit General Description The CombiTube is A double-lumen tube with
COUGH Dr. A m A it i e t sh A g A garwa w l Le L ctu t rer Departm t ent t o f f M e M dic i in i e
 COUGH Dr. Amitesh Aggarwal Lecturer Department of Medicine Cough is an explosive expiration that provides a normal protective mechanism for clearing the tracheobronchial tree of secretions and foreign
COUGH Dr. Amitesh Aggarwal Lecturer Department of Medicine Cough is an explosive expiration that provides a normal protective mechanism for clearing the tracheobronchial tree of secretions and foreign
(ix) Difficult & Failed Intubation Queen Charlotte s Hospital
 Difficult & Failed Intubation Queen Charlotte s Hospital") (ix) Difficult & Failed Intubation Queen Charlotte s Hospital Pre-operative Assessment Clinical assessment of airway and risk of difficult intubation: (can be performed in a matter of seconds): 1. Mouth
(ix) Difficult & Failed Intubation Queen Charlotte s Hospital Pre-operative Assessment Clinical assessment of airway and risk of difficult intubation: (can be performed in a matter of seconds): 1. Mouth
MD (Anaesthesiology) Title (Plan of Thesis) (Session )
 Title (Plan of Thesis) (Session )") S.No. 1. COMPARATIVE STUDY OF CENTRAL VENOUS CANNULATION USING ULTRASOUND GUIDANCE VERSUS LANDMARK TECHNIQUE IN PAEDIATRIC CARDIAC PATIENT. 2. TO EVALUATE THE ABILITY OF SVV OBTAINED BY VIGILEO-FLO TRAC
S.No. 1. COMPARATIVE STUDY OF CENTRAL VENOUS CANNULATION USING ULTRASOUND GUIDANCE VERSUS LANDMARK TECHNIQUE IN PAEDIATRIC CARDIAC PATIENT. 2. TO EVALUATE THE ABILITY OF SVV OBTAINED BY VIGILEO-FLO TRAC
Preoperative assessment for lung resection. RA Dyer
 Preoperative assessment for lung resection RA Dyer 2016 The ideal assessment of operative risk would identify every patient who could safely tolerate surgery. This ideal is probably unattainable... Mittman,
Preoperative assessment for lung resection RA Dyer 2016 The ideal assessment of operative risk would identify every patient who could safely tolerate surgery. This ideal is probably unattainable... Mittman,
4/24/2017. Tracheal Stenosis. Tracheal Stenosis. Tracheal Stenosis. Tracheal Stenosis. Tracheal Stenosis Endoscopic & Surgical Management
 Endoscopic & Surgical Management Pressure ulceration Healing: granulation cicatrization contraction Ann Surg 1969;169:334-348 Gary Schwartz, MD Department of Thoracic Surgery and Lung Transplantation Baylor
Endoscopic & Surgical Management Pressure ulceration Healing: granulation cicatrization contraction Ann Surg 1969;169:334-348 Gary Schwartz, MD Department of Thoracic Surgery and Lung Transplantation Baylor
Educational deputy, Department of Anesthesiology & Pain management, Akhtar Hospital,
 CV Shideh Dabir, M.D., Associatet Professor of Anesthesia, Educational deputy, Department of Anesthesiology & Pain management, Akhtar Hospital, Research council member of Tracheal Diseases Research Center,
CV Shideh Dabir, M.D., Associatet Professor of Anesthesia, Educational deputy, Department of Anesthesiology & Pain management, Akhtar Hospital, Research council member of Tracheal Diseases Research Center,
Semiology of respiratory system in children Simple choice 1. Mark the intrauterine age of lung development onset from the gut: a) 1 week b) 24 days
 1 week b) 24 days") Semiology of respiratory system in children Simple choice 1. Mark the intrauterine age of lung development onset from the gut: a) 1 week b) 24 days c) 6 weeks d) 12 weeks e) 35 weeks 2. Stridor is not
Semiology of respiratory system in children Simple choice 1. Mark the intrauterine age of lung development onset from the gut: a) 1 week b) 24 days c) 6 weeks d) 12 weeks e) 35 weeks 2. Stridor is not
W. J. RUSSELL*, M. F. JAMES
 Anaesth Intensive Care 2004; 32: 644-648 The Effects on Arterial Haemoglobin Oxygen Saturation and on Shunt of Increasing Cardiac Output with Dopamine or Dobutamine During One-lung Ventilation W. J. RUSSELL*,
Anaesth Intensive Care 2004; 32: 644-648 The Effects on Arterial Haemoglobin Oxygen Saturation and on Shunt of Increasing Cardiac Output with Dopamine or Dobutamine During One-lung Ventilation W. J. RUSSELL*,
Awake regional versus general anesthesia in preterms and ex-preterm infants for herniotomy
 Awake regional versus general anesthesia in preterms and ex-preterm infants for herniotomy Department of Anaesthesia University Children s Hospital Zurich Switzerland Epidemiology Herniotomy needed in
Awake regional versus general anesthesia in preterms and ex-preterm infants for herniotomy Department of Anaesthesia University Children s Hospital Zurich Switzerland Epidemiology Herniotomy needed in
Interpreting thoracic x-ray of the supine immobile patient: Syllabus
 Interpreting thoracic x-ray of the supine immobile patient: Syllabus Johannes Godt Dep. of Radiology and Nuclear Medicine Oslo University Hospital Ullevål NORDTER 2017, Helsinki Content - Why bedside chest
Interpreting thoracic x-ray of the supine immobile patient: Syllabus Johannes Godt Dep. of Radiology and Nuclear Medicine Oslo University Hospital Ullevål NORDTER 2017, Helsinki Content - Why bedside chest