January Dear Physician:
|
|
|
- Noah Casey
- 6 years ago
- Views:
Transcription
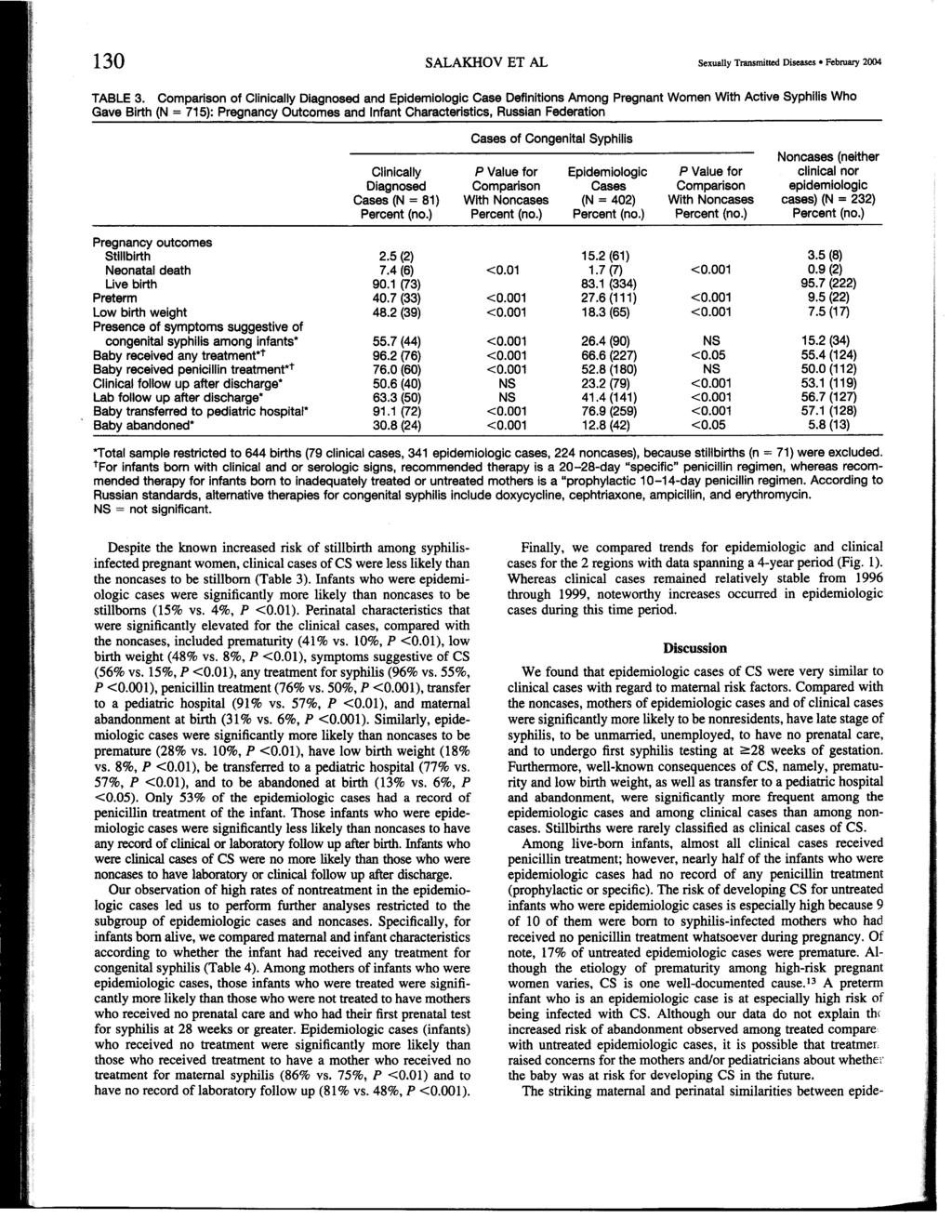
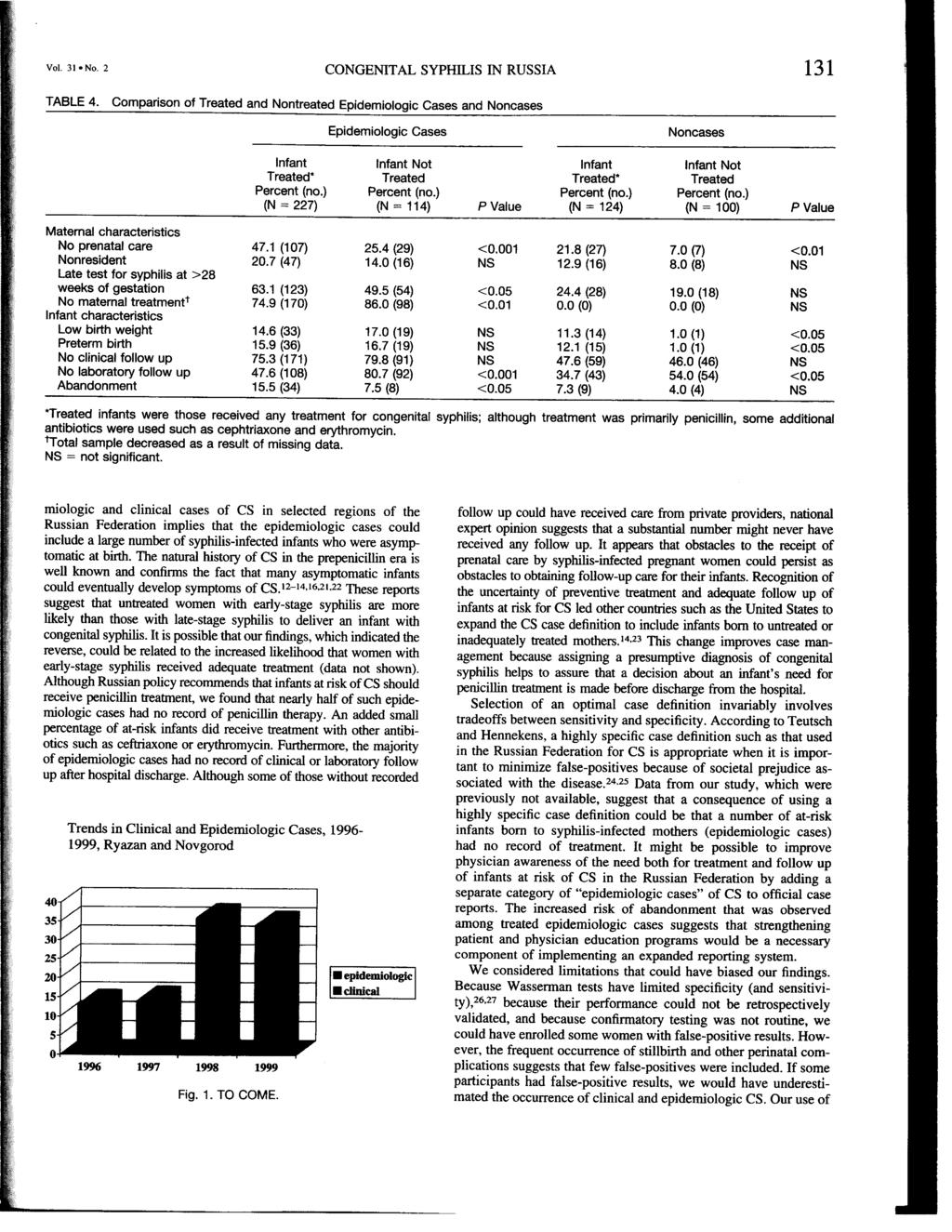
1 Richard F. Daines, M.D. Commissioner Wendy E. Saunders Executive Deputy Commissioner January 2009 Dear Physician: The purpose of this letter is to bring your attention to the significant increase in reported cases of congenital syphilis since 2003 and one important contributing cause: cases among foreign born children placed for adoption in New York State. In 2003, twenty cases of congenital syphilis were reported in New York State (excluding New York City, which is a separate health jurisdiction). Of note, four (20 percent) of these cases occurred among children adopted internationally. In 2004, 2006 and 2007, one additional case of congenital syphilis among international adoptees was reported in each year. Medical screening of these seven adoptees identified reactive syphilis serologies. Based on local health department investigation, no medical record documentation of adequate treatment for syphilis of the biologic mother or of the infant in the home country was provided to the adopting parents or placement agency. Given the lack of documentation of prior adequate treatment and the serologic evidence of treponemal antibody, these adoptees, all of whom were greater than twelve months of age, met the federal Centers for Disease Control and Prevention case definition for congenital syphilis. The New York State Department of Health s Bureau of Sexually Transmitted Disease Control (BSTDC) recommended full medical evaluation and treatment in accordance with the Sexually Transmitted Diseases Treatment Guidelines issued by the CDC. The prevention of congenital syphilis is the number one priority of the BSTDC, as the perinatal consequences of maternal syphilis may be severe, permanent, and potentially fatal. To promote the early identification and treatment of syphilis infection, New York State regulations require serologic screening of pregnant females at the time pregnancy is first diagnosed, and in high risk populations, again during the third trimester. Furthermore, serologic screening of cord blood at delivery is mandated for all live-born infants or stillbirths of at least 20 weeks gestation. This serologic testing is a mainstay of the Bureau s efforts to prevent congenital syphilis as the majority of infected infants are initially asymptomatic. By law, medical providers and laboratories must report reactive syphilis serologies to the health officers of local health departments. Receipt of a reactive syphilis serology in a pregnant woman results in an immediate, priority investigation by local health department staff to determine the infection status of the individual and, if necessary, to make recommendations for medical management and treatment. Recommendations for the evaluation and treatment of congenital syphilis are based on the identification of syphilis in the (biologic) mother; adequacy of maternal treatment; and, presence of clinical, laboratory, or radiographic evidence of syphilis in the infant. A seroreactive infant who is not treated for congenital syphilis during the perinatal period should receive careful follow-up examinations at 1, 2, 3, 6, and 12 months. Nontreponemal antibody titers should decline by three months of age and should be nonreactive at six months of age if the infant was not infected and the titers were the result of passive transfer of antibody from
2 the mother. If titers are found to be stable or increasing, the child should be medically evaluated including a long bone radiograph and cerebrospinal fluid analysis for VDRL, cell count and protein, and receive a full ten-day course of penicillin therapy. In contrast, passively transferred treponemal antibody may persist for as long as 1 year. If they are present after 1 year, the infant is considered to be infected and should receive a baseline medical evaluation and treatment for congenital syphilis. Enclosed with this letter please find BSTDC s addendum to the Centers for Disease Control and Prevention 2006 Sexually Transmitted Diseases Treatment Guidelines (obtain a copy at: as they pertain to the evaluation and management of pregnant women with syphilis and of infants at risk for congenital syphilis. Also enclosed is an article on congenital syphilis in Russia. The article documents study results that found nearly 50% of asymptomatic cases of congenital syphilis did not have a record of any penicillin treatment. Such cases were also less likely to receive clinical or laboratory follow up. The Bureau of Sexually Transmitted Disease Control s public health mission is to control and prevent sexually transmitted diseases among residents of New York State. Accordingly, the Bureau works with medical providers to assure the best management and treatment outcomes for infected patients in compliance with national and State guidelines. Failure to comply with recommendations for the medical evaluation and treatment of infants meeting the federal case definition for congenital syphilis will be reported by the Bureau of Sexually Transmitted Disease Control to the New York State Office of Professional Medical Conduct for further investigation. Further consultation regarding this information or assistance with the epidemiologic investigation may be obtained by contacting local Bureau of STD Control personnel located in area offices or the central office of the New York State Department of Health. Albany Regional Office (Troy) (518) Western Regional Office (Buffalo) (716) Rochester Regional Office: (585) or (800) Syracuse Regional Office (800) Metro New York - Westchester Area (914) Metro New York - Long Island Area (631) Central Office (Albany): (518) In New York City, questions should be directed to the New York City Office of Mental Health and Hygiene s STD Control Program at (212) Sincerely, Enclosures. F. Bruce Coles, D.O. Medical Director Bureau of STD Control
3 New York State Addendum for Congenital Syphilis Treatment Guidelines The New York State Bureau of Sexually Transmitted Disease Control has issued an addendum to the Centers for Disease Control and Prevention, Sexually Transmitted Diseases Treatment Guidelines These modified guidelines, presented below, reflect the Bureau's policy and procedures specifically for the evaluation and management of pregnant women with syphilis, and of infants at risk for congenital syphilis. Clinical providers are encouraged to refer to this addendum for guidance on the evaluation and treatment of syphilis in pregnant women and atrisk infants. The Centers for Disease Control and Prevention, Sexually Transmitted Diseases Treatment Guidelines 2006 are referred to throughout this document. Syphilis During Pregnancy New York State Regulations for Screening During Pregnancy 1. All women must be screened serologically for syphilis at the time pregnancy is first diagnosed. In communities and populations with high syphilis prevalence or for patients at high risk New York State surveillance data indicates that repeat infection and infection acquired late in pregnancy are not uncommon events; therefore, women from these settings should be screened repeatedly throughout pregnancy (perhaps monthly in some instances e.g., high risk women who continue to be sexually active). 2. New York State law mandates screening at delivery for all infants. In addition, any woman who delivers a stillborn infant after 20 weeks gestation must be tested for syphilis. No infant should leave the hospital without the serologic status of the infant's mother having been determined at least once during pregnancy. Diagnostic Considerations Seropositive pregnant women should be considered infected unless treatment history is documented clearly in a medical or health department record and sequential serologic antibody titers have appropriately declined. Serofast low antibody titers might not require treatment; however, persistent higher titer antibody tests might indicate reinfection and require treatment. Treatment Penicillin is effective for preventing transmission to fetuses and for treating established infection among fetuses. Evidence is insufficient, however, to determine whether the specific, recommended penicillin regimens are optimal. Recommended Regimens Treatment during pregnancy should be the penicillin regimen appropriate for the woman's stage of syphilis. Some experts recommend additional therapy (e.g., a second dose of benzathine penicillin 2.4 million units IM) one week after the initial dose, particularly for those women in the third trimester of pregnancy and for women who have secondary syphilis during pregnancy. 1
4 Other Management Considerations Women who are treated for syphilis during the second half of pregnancy are at risk for premature labor or fetal distress, or both, if their treatment precipitates the Jarisch-Herxheimer reaction. These women should be advised to seek medical attention following treatment if they notice any decrease in fetal movements or if they have contractions. Stillbirth is a rare complication of treatment; however, since therapy is necessary to prevent further fetal damage, that concern should not delay treatment. All patients with syphilis should be tested for HIV. Follow-Up Serologic titers should be checked monthly until adequacy of treatment has been assured. The antibody response should be appropriate for the stage of disease. Management of Sex Partners Refer to General Principles, Management of Sex Partners (CDC guidelines, page 24.) Special Considerations Penicillin Allergy There are no proven alternatives to penicillin. A pregnant woman with a history of penicillin allergy should be treated with penicillin, after desensitization, if necessary. Skin testing may be helpful for some patients and in some settings (CDC guidelines, page 33, Management of Patients Who Have a History of Penicillin Allergy). Tetracycline and doxycycline are contraindicated during pregnancy. Erythromycin should not be used because it cannot be relied upon to cure an infected fetus. Data are insufficient to recommend azithromycin or ceftriaxone for treatment of maternal infection and prevention of congenital syphilis. Congenital Syphilis Evaluation and Treatment of Infants During the First Month of Life Who Should Be Evaluated Infants should be evaluated for congenital syphilis if they were born to seropositive (nontreponemal test confirmed by treponemal test) women who meet the following criteria: Have untreated syphilis; or Were treated for syphilis during pregnancy with a non-recommended therapy (including erythromycin, doxycycline, tetracycline or a nonrecommended penicillin regimen); or Were treated for syphilis less than 1 month before delivery; or Were treated for syphilis during pregnancy with the appropriate penicillin regimen, but nontreponemal antibody titers did not decrease sufficiently after therapy to indicate an adequate response (greater than or equal to fourfold decrease); or Do not have a well-documented history of treatment for syphilis; or 2
5 Were treated appropriately before pregnancy but had insufficient serologic follow-up to assure that they had responded appropriately to treatment and are not currently infected (greater than or equal to fourfold decrease for patients treated for early syphilis; stable or declining titers less than or equal to 1:4 for other patients). Note: Serologic tests for the mother and infant can be nonreactive at delivery if the mother was infected late during pregnancy. Treatment Evaluation of the Infant The clinical and laboratory evaluation of infants born to women described above should include the following: A thorough physical examination for evidence of congenital syphilis; A quantitative nontreponemal serologic test for syphilis performed on the infant's sera (not on cord blood); CSF analysis for VDRL, cell count, and protein; Long bone x-rays; Other tests as clinically indicated (e.g., chest x-ray, complete blood count, differential and platelet count, liver function tests, cranial ultrasound, ophthalmologic exam, and auditory brainstem response); For infants who have no evidence of congenital syphilis on the above evaluation, determination of presence of specific antitreponemal IgM antibody by a testing method recognized by CDC as having either provisional or standard status; Pathologic examination of the placenta or amniotic cord using specific fluorescent antitreponemal antibody staining. Therapy Decisions Infants should be treated for presumed congenital syphilis if they were born to mothers who, at delivery, 1) had untreated syphilis; 2) were treated with a nonrecommended antibiotic regimen; 3) were treated less than one month prior to delivery; or 4) had evidence of relapse or reinfection after treatment (CDC guidelines, page 30-32, Congenital Syphilis). Additional criteria for presumptively treating infants with congenital syphilis are as follows: Physical evidence of active disease; X-ray evidence of active disease; A reactive VDRL-CSF or, for infants born to seroreactive mothers, an abnormal CSF white blood cell count or protein, regardless of CSF results; In the immediate newborn period, interpretation of CSF test results may be difficult; normal values vary with gestational age and are higher in preterm infants. Other causes of elevated values also should be considered when an infant is being evaluated for congenital syphilis. Though values as high as 25 white blood cells (WBC) /mm3 and 150 mg protein/dl occur among normal neonates, some experts recommend that lower values (5 WBC/mm3 and 40 mg protein/dl) be considered the upper limits of normal. The infant should be treated if test results cannot exclude infection. 3
6 A serum quantitative nontreponemal serologic titer that is at least fourfold greater than the mother's titer; Specific antitreponemal IgM antibody detected by a testing method that has been given provisional or standard status by CDC; If they meet the previously cited criteria for "Who Should Be Evaluated," but have not been fully evaluated (CDC guidelines, page 30, Congenital Syphilis). NOTE: Infants with clinically evident congenital syphilis should have an ophthalmologic examination. Recommended Regimens Aqueous crystalline penicillin G, 100, ,000 units/kg/day administered as 50,000 units/kg IV every 12 hours during the first 7 days of life and every 8 hours thereafter for a total of 10 days, or Procaine penicillin G, 50,000 units/kg IM daily in a single dose for 10 days. If more than one day of therapy is missed, the entire course should be restarted. When possible, a full 10-day course of penicillin is preferred, even if ampicillin was initially provided for possible sepsis. NOTE: Due to reports of treatment failure of benzathine penicillin among newborns including cases among initially asymptomatic infants, the New York State Department of Health does not recommend use of benzathine penicillin G, 50,000 units/kg IM in a single dose for treatment of congenital syphilis. In some cases, infants with a normal complete evaluation for whom follow-up can be assured can be followed closely without treatment. If the decision is made to treat the baby, the standard 10-day therapy should be given. the absence of a fourfold greater titer for an infant cannot be used as evidence against congenital syphilis. 4
7 Infants of Women Treated in the Third Trimester Although there is uniform agreement that treatment of syphilis in early pregnancy is almost 100% effective in preventing congenital syphilis, the evidence is less certain for treatment in the last trimester. As indicated above (see CDC guidelines, Congenital Syphilis, scenarios page 31-32), if the mother was treated within one month of delivery, treatment of the infant is considered inadequate and the infant must be treated for congenital syphilis. There are cases reported in the literature and to the Department of Health's surveillance system which suggest that treatment of the mother during the seventh and eighth month of pregnancy may also fail to treat the fetus. While this is an uncommon event, at present it is not possible to predict when treatment failure will occur. Therefore, if the mother is treated during the seventh or eighth month of pregnancy, both she and her infant must be followed especially closely. If these infants meet any of the criteria in "Evaluation & Treatment of Infants During the First Month of Life" (CDC guidelines, page 30, Congenital Syphilis), they should be given the standard 10-day therapy. For the baby who does not meet these treatment criteria, the mother should show an expected decrease in serologic titer. If this decrease cannot be documented, these infants should either be followed with repeat serologic testing over a one-year period or empirically treated with the standard 10- day therapy if follow-up cannot be assured. Evaluation and Treatment of Older Infants and Children After the newborn period (i.e., aged > 1 month), children diagnosed with syphilis should have a CSF examination to exclude neurosyphilis and records should be reviewed to assess whether the child has congenital or acquired syphilis (CDC guidelines, page 26, Primary and Secondary Syphilis and Latent Syphilis). Any child who is thought to have congenital syphilis or who has neurologic involvement should be treated with aqueous crystalline penicillin G, 200, ,000 units/kg/day IV administered as 50,000 units/kg every 4-6 hours for 10 days. Follow-Up A seroreactive infant (or an infant whose mother was seroreactive at delivery) who is not treated for congenital syphilis during the perinatal period should receive careful follow-up examinations at 1 month and at 2, 3, 6, and 12 months after therapy. Nontreponemal antibody titers should decline by 3 months of age and should be nonreactive by 6 months of age if the infant was not infected and the titers were the result of passive transfer of antibody from the mother. If these titers are found to be stable or increasing after 6 12 months, the child should be re-evaluated, including CSF examination, and fully treated. Passively transferred maternal treponemal antibodies may be present for as long as 1 year. If they are present greater than 1 year, the infant should be re-evaluated and treated for congenital syphilis. Treated infants also should be followed every 2-3 months to assure that nontreponemal antibody titers decline; these infants should have become nonreactive by 6 months of age (response may be slower for infants treated after the neonatal period). Treponemal tests should not be used to evaluate response to treatment because test results can remain positive despite effective therapy if the child was infected. Infants with CSF pleocytosis should undergo CSF examination every 6 months, or until the cell count is normal. If the cell count is still abnormal after 2 years, or if a downward trend is not present at each examination, the child should be re-treated. The VDRL-CSF also should be checked at 6 months; if still reactive, the infant should be re-treated. 5
8 Follow-up of children treated for congenital syphilis after the newborn period should be the same as that prescribed for congenital syphilis among neonates. Special Considerations Penicillin Allergy Children who require treatment for syphilis after the newborn period (> 30 days), but who have a history of penicillin allergy, should be treated with penicillin after desensitization, if necessary. Skin testing may be helpful in some patients and settings (CDC guidelines, page 33, Management of Patients Who Have a History of Penicillin Allergy). HIV Infection Mothers of infants with congenital syphilis should be tested for HIV. Infants born to mothers who have HIV infection should be referred for evaluation and appropriate follow-up. No data exist to suggest that infants with congenital syphilis whose mothers are coinfected with HIV require different evaluation, therapy, or follow-up for syphilis than is recommended for all infants. Penicillin Shortage During periods when the availability of penicillin is compromised, the following is recommended (see 1. For infants (< 30 days of age) with clinical evidence of congenital syphilis, check local sources for aqueous crystalline penicillin G (potassium or sodium). If IV penicillin G is limited, substitute some or all daily doses with procaine penicillin G (50,000 U/kg/dose IM a day in a single daily dose for 10 days). 2. For infants at risk of congenital syphilis without any clinical evidence of infection, use procaine penicillin G, 50,000 U/kg/dose IM a day in a single dose for 10 days. As stated previously, the New York State Department of Health does not recommend use of benzathine penicillin G, 50,000 units/kg IM in a single dose for treatment of congenital syphilis. Due to the lack of data, procaine penicillin is not recommended for treating infants > 30 days old. 3. For premature infants at risk of congenital syphilis but who have no other clinical evidence of infection and who might not tolerate IM injections because of decreased muscle mass, IV ceftriaxone may be considered only if careful clinical and serologic follow-up can be assured. If aqueous or procaine penicillin G is not available, IV ampicillin (200 mg/kg a day in 4 divided doses for days) or, alternatively, ceftriaxone may be considered with careful clinical and serologic follow-up. Ceftriaxone must be used with caution in 6
9 jaundiced infants and dosed according to age and weight. For infants < 30 days old, use 75 mg/kg IV/IM a day in a single daily dose for days. For older infants, this dose should be 100 mg/kg a day in a single daily dose. Studies that strongly support ampicillin or ceftriaxone for the treatment of congenital syphilis have not been done. As a result, their use requires management in consultation with an expert in the treatment of infants with congenital syphilis. 7

10

11

12
13
14

15
Syphilis Treatment Protocol
 STD, HIV, AND TB SECTION Syphilis Treatment Protocol CLINICAL GUIDANCE FOR PRIMARY AND SECONDARY SYPHILIS AND LATENT SYPHILIS www.lekarzol.com (4/2016) Page 1 of 8 Table of Contents Description... 3 Stages
STD, HIV, AND TB SECTION Syphilis Treatment Protocol CLINICAL GUIDANCE FOR PRIMARY AND SECONDARY SYPHILIS AND LATENT SYPHILIS www.lekarzol.com (4/2016) Page 1 of 8 Table of Contents Description... 3 Stages
Sexually Transmitted Diseases Treatment Guidelines, 2015
 Morbidity and Mortality Weekly Report Recommendations and Reports / Vol. 64 / No. 3 June 5, 2015 Sexually Transmitted Diseases Treatment Guidelines, 2015 U.S. Department of Health and Human Services Centers
Morbidity and Mortality Weekly Report Recommendations and Reports / Vol. 64 / No. 3 June 5, 2015 Sexually Transmitted Diseases Treatment Guidelines, 2015 U.S. Department of Health and Human Services Centers
9/9/2015. Began to see a shift in 2012 Early syphilis cases more than doubled from year before
 George Walton, MPH, CPH, MLS(ASCP) CM STD Program Manager Bureau of HIV, STD, and Hepatitis September 15, 2015 1 1) Discuss the changing epidemiology of syphilis in Iowa; 2) Explore key populations affected
George Walton, MPH, CPH, MLS(ASCP) CM STD Program Manager Bureau of HIV, STD, and Hepatitis September 15, 2015 1 1) Discuss the changing epidemiology of syphilis in Iowa; 2) Explore key populations affected
Use of Treponemal Immunoassays for Screening and Diagnosis of Syphilis
 Use of Treponemal Immunoassays for Screening and Diagnosis of Syphilis Guidance for Medical Providers and Laboratories in California These guidelines were developed by the California Department of Public
Use of Treponemal Immunoassays for Screening and Diagnosis of Syphilis Guidance for Medical Providers and Laboratories in California These guidelines were developed by the California Department of Public
Management of Syphilis in Patients with HIV
 Management of Syphilis in Patients with HIV Adult Clinical Guideline from the New York State Department of Health AIDS Institute www.hivguidelines.org Purpose of the Guideline Increase the numbers of NYS
Management of Syphilis in Patients with HIV Adult Clinical Guideline from the New York State Department of Health AIDS Institute www.hivguidelines.org Purpose of the Guideline Increase the numbers of NYS
Public/Private Partnerships: Intervening in the Spread of Syphilis
 Public/Private Partnerships: Intervening in the Spread of Diana Torres-Burgos MD, MPH Gerard Castaneda, BSN Alana Thomas, BS STD/HIV Update Conference Grand Rapids, MI 3/11/2014 Outline overview Stages
Public/Private Partnerships: Intervening in the Spread of Diana Torres-Burgos MD, MPH Gerard Castaneda, BSN Alana Thomas, BS STD/HIV Update Conference Grand Rapids, MI 3/11/2014 Outline overview Stages
Sex, Sores, Science, and Surveillance: Syphilis in the 21 st Century (U046)
") Sex, Sores, Science, and Surveillance: Syphilis in the 21 st Century (U046) Kenneth A. Katz, MD, MSc, MSCE Dermatologist, Kaiser Permanente, San Francisco, CA AAD Annual Meeting, Orlando, FL March 4, 2017
Sex, Sores, Science, and Surveillance: Syphilis in the 21 st Century (U046) Kenneth A. Katz, MD, MSc, MSCE Dermatologist, Kaiser Permanente, San Francisco, CA AAD Annual Meeting, Orlando, FL March 4, 2017
SYPHILIS. The Great Pretender K. Amen Eguakun, MSN, APRN, AAHIVS
 SYPHILIS The Great Pretender K. Amen Eguakun, MSN, APRN, AAHIVS Learning Objectives At the end of this presentation, the participants will be able to 1. Describe the epidemiology of syphilis in the United
SYPHILIS The Great Pretender K. Amen Eguakun, MSN, APRN, AAHIVS Learning Objectives At the end of this presentation, the participants will be able to 1. Describe the epidemiology of syphilis in the United
Learning Objectives. Syphilis. Lessons. Epidemiology: Disease in the U.S. Syphilis Definition. Transmission. Treponema pallidum
 Learning Objectives Syphilis Treponema pallidum 1 Upon completion of this content, the learner will be able to 1. Describe the epidemiology of syphilis in the U.S. 2. Describe the pathogenesis of T. pallidum.
Learning Objectives Syphilis Treponema pallidum 1 Upon completion of this content, the learner will be able to 1. Describe the epidemiology of syphilis in the U.S. 2. Describe the pathogenesis of T. pallidum.
Replaces: 04/13/17. / Formulated: 7/05 SYPHLIS
 Effective Date: 81017 Replaces: 041317 Page 1 of 7 POLICY: The Texas Department of Criminal Justice (TDCJ) will identify, test, and manage all offenders with suspected or confirmed syphilis with a uniform
Effective Date: 81017 Replaces: 041317 Page 1 of 7 POLICY: The Texas Department of Criminal Justice (TDCJ) will identify, test, and manage all offenders with suspected or confirmed syphilis with a uniform
Learning Objectives. Epidemiology 5/3/2013. Treponema pallidum Diagnosis, Treatment and Prevention. Anne Rompalo, MD, ScM Professor of Medicine
 Treponema pallidum Diagnosis, Treatment and Prevention Anne Rompalo, MD, ScM Professor of Medicine Learning Objectives Describe the epidemiology of syphilis in the U.S.Describe the pathogenesis of Treponema
Treponema pallidum Diagnosis, Treatment and Prevention Anne Rompalo, MD, ScM Professor of Medicine Learning Objectives Describe the epidemiology of syphilis in the U.S.Describe the pathogenesis of Treponema
ALASKA NATIVE MEDICAL CENTER SEXUALLY TRANSMITTED DISEASE SCREENING AND TREATMENT GUIDELINES
 ALASKA NATIVE MEDICAL CENTER SEXUALLY TRANSMITTED DISEASE SCREENING AND TREATMENT GUIDELINES A. Screening Page Chlamydia and Gonorrhea 1 HIV 1 Syphilis 1 Genital Herpes 2 Hepatitis A 2 Hepatitis B 2 Hepatitis
ALASKA NATIVE MEDICAL CENTER SEXUALLY TRANSMITTED DISEASE SCREENING AND TREATMENT GUIDELINES A. Screening Page Chlamydia and Gonorrhea 1 HIV 1 Syphilis 1 Genital Herpes 2 Hepatitis A 2 Hepatitis B 2 Hepatitis
Syphilis Technical Instructions for Civil Surgeons
 National Center for Emerging and Zoonotic Infectious Diseases Syphilis Technical Instructions for Civil Surgeons Joanna J. Regan, MD, MPH, FAAP Medical Officer Medical Assessment and Policy Team Immigrant,
National Center for Emerging and Zoonotic Infectious Diseases Syphilis Technical Instructions for Civil Surgeons Joanna J. Regan, MD, MPH, FAAP Medical Officer Medical Assessment and Policy Team Immigrant,
Michigan Guidelines: HIV, Syphilis, HBV in Pregnancy
 Michigan Guidelines: HIV, Syphilis, HBV in Pregnancy Presenter: Theodore B. Jones, MD Maternal Fetal Medicine Wayne State University School of Medicine Beaumont Dearborn Hospital HIV, Syphilis, HBV in
Michigan Guidelines: HIV, Syphilis, HBV in Pregnancy Presenter: Theodore B. Jones, MD Maternal Fetal Medicine Wayne State University School of Medicine Beaumont Dearborn Hospital HIV, Syphilis, HBV in
Sex, Sores, Science, and Surveillance: Syphilis in the 21 st Century (U046)
") Sex, Sores, Science, and Surveillance: Syphilis in the 21 st Century (U046) Kenneth A. Katz, MD, MSc, MSCE Dermatologist, Kaiser Permanente, San Francisco, CA AAD Annual Meeting, San Diego, CA February
Sex, Sores, Science, and Surveillance: Syphilis in the 21 st Century (U046) Kenneth A. Katz, MD, MSc, MSCE Dermatologist, Kaiser Permanente, San Francisco, CA AAD Annual Meeting, San Diego, CA February
ANNUAL MORBIDITY REPORT
 DUTCHESS COUNTY DEPARTMENT OF HEALTH S ANNUAL MORBIDITY REPORT Marcus J. Molinaro, Dutchess County Executive Kari Reiber, MD, Acting Commissioner of Health Volume 8, Issue FIRST CONGENITAL SYPHILIS CASE
DUTCHESS COUNTY DEPARTMENT OF HEALTH S ANNUAL MORBIDITY REPORT Marcus J. Molinaro, Dutchess County Executive Kari Reiber, MD, Acting Commissioner of Health Volume 8, Issue FIRST CONGENITAL SYPHILIS CASE
Sexually Transmitted Disease Treatment Tables
 Sexually Transmitted Disease Treatment Tables Federal Bureau of Prisons Clinical Practice Guidelines June 2011 Clinical guidelines are made available to the public for informational purposes only. The
Sexually Transmitted Disease Treatment Tables Federal Bureau of Prisons Clinical Practice Guidelines June 2011 Clinical guidelines are made available to the public for informational purposes only. The
STI Treatment Guidelines. Teodora Wi. Training Course in Sexual and Reproductive Health Research
 Teodora Wi Geneva, 28 August 2017 STI Treatment Guidelines Teodora Wi Training Course in Sexual and Reproductive Health Research 2017 Twitter @HRPresearch 1 STI treatment guidelines Neisseria gonorrhoeae
Teodora Wi Geneva, 28 August 2017 STI Treatment Guidelines Teodora Wi Training Course in Sexual and Reproductive Health Research 2017 Twitter @HRPresearch 1 STI treatment guidelines Neisseria gonorrhoeae
Nothing to disclose.
 Update on Diagnosis and Treatment Lisa Winston, MD University of California, San Francisco/ Zuckerberg San Francisco General Nothing to disclose. 1 This talk will be a little depressing Rising incidence
Update on Diagnosis and Treatment Lisa Winston, MD University of California, San Francisco/ Zuckerberg San Francisco General Nothing to disclose. 1 This talk will be a little depressing Rising incidence
Syphilis Update: New Presentations of an Old Disease
 Syphilis Update: New Presentations of an Old Disease Bradley Stoner, MD, PhD Washington University in St. Louis Disclosure: Bradley Stoner, MD, PhD STDs in the United States Where do we stand right now?
Syphilis Update: New Presentations of an Old Disease Bradley Stoner, MD, PhD Washington University in St. Louis Disclosure: Bradley Stoner, MD, PhD STDs in the United States Where do we stand right now?
Lisa Villarroel, MD MPH Medical Director, Division of Public Health Preparedness Arizona Department of Health Services.
 Lisa Villarroel, MD MPH Medical Director, Division of Public Health Preparedness Arizona Department of Health Services Disclosures: None 1 PRIMARY Fitzgerald TJ, Cleveland P, Johnson RC et al: Scanning
Lisa Villarroel, MD MPH Medical Director, Division of Public Health Preparedness Arizona Department of Health Services Disclosures: None 1 PRIMARY Fitzgerald TJ, Cleveland P, Johnson RC et al: Scanning
Sexually Transmitted Diseases. Summary of CDC Treatment Guidelines
 DC 2015 Sexually Transmitted Diseases Summary of CDC Treatment Guidelines These summary guidelines reflect the June 2015 update to the 2010 CDC Guidelines for Treatment of Sexually Transmitted Diseases.
DC 2015 Sexually Transmitted Diseases Summary of CDC Treatment Guidelines These summary guidelines reflect the June 2015 update to the 2010 CDC Guidelines for Treatment of Sexually Transmitted Diseases.
Zika Pregnancy and Birth Defects Surveillance
 Zika Pregnancy and Birth Defects Surveillance Sowmya Adibhatla, MPH Zika Surveillance and Response Coordinator Overview History/Background Zika cases update Zika virus infection Testing guidance Recommendations
Zika Pregnancy and Birth Defects Surveillance Sowmya Adibhatla, MPH Zika Surveillance and Response Coordinator Overview History/Background Zika cases update Zika virus infection Testing guidance Recommendations
Didactic Series. STD Screening & Management: Syphilis. Christian B. Ramers, MD, MPH
 Didactic Series STD Screening & Management: Syphilis Christian B. Ramers, MD, MPH Assistant Medical Director Family Health Centers of San Diego Ciaccio Memorial Clinic 3/26/15 ACCREDITATION STATEMENT:
Didactic Series STD Screening & Management: Syphilis Christian B. Ramers, MD, MPH Assistant Medical Director Family Health Centers of San Diego Ciaccio Memorial Clinic 3/26/15 ACCREDITATION STATEMENT:
CHLAMYDIA, GONORRHEA & SYPHILIS: STDS ON THE RISE
 CHLAMYDIA, GONORRHEA & SYPHILIS: STDS ON THE RISE What are sexually transmitted diseases (STDs)? Sexually transmitted diseases (STDs) are passed from person to person through sexual activity. These infections
CHLAMYDIA, GONORRHEA & SYPHILIS: STDS ON THE RISE What are sexually transmitted diseases (STDs)? Sexually transmitted diseases (STDs) are passed from person to person through sexual activity. These infections
SEXUALLY TRANSMITED DISEASES SYPHILIS ( LUES ) Dr D. Tenea Department of Dermatology University of Pretoria
 Dr D. Tenea Department of Dermatology University of Pretoria") SEXUALLY TRANSMITED DISEASES SYPHILIS ( LUES ) Dr D. Tenea Department of Dermatology University of Pretoria INTRODUCTION Venereal disease = old term STD infections transmitted by sexual contact Sexually
SEXUALLY TRANSMITED DISEASES SYPHILIS ( LUES ) Dr D. Tenea Department of Dermatology University of Pretoria INTRODUCTION Venereal disease = old term STD infections transmitted by sexual contact Sexually
To view an archived recording of this presentation please click the following link:
 To view an archived recording of this presentation please click the following link: http://pho.adobeconnect.com/p16lj8z0qm3/ Please scroll down this file to view a copy of the slides from the session.
To view an archived recording of this presentation please click the following link: http://pho.adobeconnect.com/p16lj8z0qm3/ Please scroll down this file to view a copy of the slides from the session.
Susanne Norris Zanto, MPH, MLS (ASCP) CM, SM Montana Public Health Laboratory
 CM, SM Montana Public Health Laboratory") Susanne Norris Zanto, MPH, MLS (ASCP) CM, SM Montana Public Health Laboratory Describe the challenges in syphilis diagnostics Present two testing algorithms Non-treponemal test as initial screen Treponemal
Susanne Norris Zanto, MPH, MLS (ASCP) CM, SM Montana Public Health Laboratory Describe the challenges in syphilis diagnostics Present two testing algorithms Non-treponemal test as initial screen Treponemal
CHLAMYDIA, GONORRHEA & SYPHILIS: STDS ON THE RISE
 CHLAMYDIA, GONORRHEA & SYPHILIS: STDS ON THE RISE What are sexually transmitted diseases (STDs)? Sexually transmitted diseases (STDs) are passed from person to person through sexual activity. These infections
CHLAMYDIA, GONORRHEA & SYPHILIS: STDS ON THE RISE What are sexually transmitted diseases (STDs)? Sexually transmitted diseases (STDs) are passed from person to person through sexual activity. These infections
Syphilis in the 21 st Century: Sex, Sores, Science, and Surveillance. Syphilis in Men
 Syphilis in the 21 st Century: Sex, Sores, Science, and Surveillance Syphilis in Men Kenneth A. Katz, MD, MSc, MSCE Kaiser Permanente, San Francisco, CA AAD Annual Meeting Washington, D.C. March 2, 2019
Syphilis in the 21 st Century: Sex, Sores, Science, and Surveillance Syphilis in Men Kenneth A. Katz, MD, MSc, MSCE Kaiser Permanente, San Francisco, CA AAD Annual Meeting Washington, D.C. March 2, 2019
Zika Virus. Robert Wittler, MD
 Zika Virus Robert Wittler, MD Disclosure I have no relevant financial relationships with the manufacturers(s) of any commercial products(s) and/or provider of commercial services discussed in this CME
Zika Virus Robert Wittler, MD Disclosure I have no relevant financial relationships with the manufacturers(s) of any commercial products(s) and/or provider of commercial services discussed in this CME
Zika Virus. Disclosure. Zika Virus 8/26/2016
 Zika Virus Robert Wittler, MD Disclosure I have no relevant financial relationships with the manufacturers(s) of any commercial products(s) and/or provider of commercial services discussed in this CME
Zika Virus Robert Wittler, MD Disclosure I have no relevant financial relationships with the manufacturers(s) of any commercial products(s) and/or provider of commercial services discussed in this CME
Update on Sexually Transmitted Infections Jeanne Marrazzo, MD, MPH
 Update on Sexually Transmitted Infections Jeanne Marrazzo, MD, MPH Division of Infectious Diseases University of Alabama at Birmingham School of Medicine Birmingham, Alabama Outline Syphilis in all its
Update on Sexually Transmitted Infections Jeanne Marrazzo, MD, MPH Division of Infectious Diseases University of Alabama at Birmingham School of Medicine Birmingham, Alabama Outline Syphilis in all its
WHAT DO U KNOW ABOUT STIS?
 WHAT DO U KNOW ABOUT STIS? Rattiya Techakajornkeart MD. Bangrak STIs Cluster, Bureau of AIDS, TB and STIs, Department of Disease Control, MOPH, Thailand SEXUALLY TRANSMITTED INFECTIONS? STIs Infections
WHAT DO U KNOW ABOUT STIS? Rattiya Techakajornkeart MD. Bangrak STIs Cluster, Bureau of AIDS, TB and STIs, Department of Disease Control, MOPH, Thailand SEXUALLY TRANSMITTED INFECTIONS? STIs Infections
Edward W. Hook, III, M.D.
 Challenging Cases Edward W. Hook III M.D. Professor and Director Division of Infectious Diseases University of Alabama at Birmingham And PI, Alabama/North Carolina STD PTC Edward W. Hook, III, M.D. Grant/Research
Challenging Cases Edward W. Hook III M.D. Professor and Director Division of Infectious Diseases University of Alabama at Birmingham And PI, Alabama/North Carolina STD PTC Edward W. Hook, III, M.D. Grant/Research
STDs and Hepatitis C
 STDs and Hepatitis C Catherine S. O Neal, MD Assistant Professor of Clinical Medicine, Infectious Diseases Louisiana State University Health Sciences Center March 3, 2018 Objectives Review patient risk
STDs and Hepatitis C Catherine S. O Neal, MD Assistant Professor of Clinical Medicine, Infectious Diseases Louisiana State University Health Sciences Center March 3, 2018 Objectives Review patient risk
Congenital CMV infection. Infectious and Tropical Pediatric Division Department of Child Health Medical Faculty, University of Sumatera Utara
 Congenital CMV infection Infectious and Tropical Pediatric Division Department of Child Health Medical Faculty, University of Sumatera Utara Congenital CMV infection Approximately 0.15 2% of live births
Congenital CMV infection Infectious and Tropical Pediatric Division Department of Child Health Medical Faculty, University of Sumatera Utara Congenital CMV infection Approximately 0.15 2% of live births
26. Screening for Syphilis
 26. Screening for Syphilis RECOMMENDATION Routine serologic screening for syphilis is recommended for all pregnant women and for persons at increased risk of infection (see Clinical Inter - vention). See
26. Screening for Syphilis RECOMMENDATION Routine serologic screening for syphilis is recommended for all pregnant women and for persons at increased risk of infection (see Clinical Inter - vention). See
Current standards for diagnosis and treatment of syphilis: selection of some practical issues, based on the European (IUSTI) and U.S.
 and U.S.") Special paper Current standards for diagnosis and treatment of syphilis: selection of some practical issues, based on the European (IUSTI) and U.S. (CDC) guidelines Maciej Pastuszczak, Anna Wojas-Pelc
Special paper Current standards for diagnosis and treatment of syphilis: selection of some practical issues, based on the European (IUSTI) and U.S. (CDC) guidelines Maciej Pastuszczak, Anna Wojas-Pelc
Con temporary. An OldDisease, a. Pwinatal Problem. ]( ;n PRINCIPLES Q: PRACTICE. Pathogenesis. May/June 1992 J O G N N 209
 ]( ;n PRINCIPLES Q: PRACTICE JILL TILLMAN, RN, MSN An OldDisease, a Con temporary Pwinatal Problem he incidence of syphilis peaked during World War 11, with 600,000 new cases reported per year. Six thousand
]( ;n PRINCIPLES Q: PRACTICE JILL TILLMAN, RN, MSN An OldDisease, a Con temporary Pwinatal Problem he incidence of syphilis peaked during World War 11, with 600,000 new cases reported per year. Six thousand
Revisions to the Syphilis Surveillance Case Definitions, 2018
 National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention Revisions to the Syphilis Surveillance Case Definitions, 2018 Sarah Kidd, MD, MPH Medical Epidemiologist Division of STD Prevention
National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention Revisions to the Syphilis Surveillance Case Definitions, 2018 Sarah Kidd, MD, MPH Medical Epidemiologist Division of STD Prevention
Annals of Internal Medicine. 1991;114:
 Serologic Response to Treatment of Infectious Syphilis Barbara Romanowski, MD; Ruth Sutherland, DPH, RN; Gordon H. Fick, PhD; Debbie Mooney, BSc; and Edgar J. Love, MD, PhD Objective: To evaluate the serologic
Serologic Response to Treatment of Infectious Syphilis Barbara Romanowski, MD; Ruth Sutherland, DPH, RN; Gordon H. Fick, PhD; Debbie Mooney, BSc; and Edgar J. Love, MD, PhD Objective: To evaluate the serologic
Management of infants at risk of congenital syphilis
 Management of infants at risk of congenital syphilis Version: Issued: Review date: Author: Dr Sanjay Patel (Paediatric Infectious Diseases Consultant), Dr Emanuela Pelosi (Consultant Virologist), Dr Mildred
Management of infants at risk of congenital syphilis Version: Issued: Review date: Author: Dr Sanjay Patel (Paediatric Infectious Diseases Consultant), Dr Emanuela Pelosi (Consultant Virologist), Dr Mildred
Standard of Newborn Care in the Age of Birth Plans. Stephanie Deal, MD Tiffany McKee-Garrett, MD
 Standard of Newborn Care in the Age of Birth Plans Stephanie Deal, MD Tiffany McKee-Garrett, MD Disclosure We have no relevant financial relationships with the manufacturers(s) of any commercial products(s)
Standard of Newborn Care in the Age of Birth Plans Stephanie Deal, MD Tiffany McKee-Garrett, MD Disclosure We have no relevant financial relationships with the manufacturers(s) of any commercial products(s)
Alabama Department of Public Health. Sexually Transmitted Diseases
 Alabama Department of Public Health Sexually Transmitted Diseases Annual Report 29 August 16, 21 Dear Alabama Stakeholder: The Division of Sexually Transmitted Disease Prevention and Control of the Alabama
Alabama Department of Public Health Sexually Transmitted Diseases Annual Report 29 August 16, 21 Dear Alabama Stakeholder: The Division of Sexually Transmitted Disease Prevention and Control of the Alabama
Disclosures. STD Screening for Women. Chlamydia & Gonorrhea. I have no disclosures or conflicts of interest to report.
 Disclosures Management of STIs: Challenges in Practice I have no disclosures or conflicts of interest to report. Alison O. Marshall, MSN, FNP-C Associate Professor of Practice & Director of the Family
Disclosures Management of STIs: Challenges in Practice I have no disclosures or conflicts of interest to report. Alison O. Marshall, MSN, FNP-C Associate Professor of Practice & Director of the Family
Elimination of Congenital Syphilis in South Africa Where are we and what needs to be done?
 Elimination of Congenital Syphilis in South Africa Where are we and what needs to be done? Presented by: Dr Saiqa Mullick (Director: Implementation Science, Wits RHI) Co-authors: Diantha Pillay (Researcher:
Elimination of Congenital Syphilis in South Africa Where are we and what needs to be done? Presented by: Dr Saiqa Mullick (Director: Implementation Science, Wits RHI) Co-authors: Diantha Pillay (Researcher:
Centers for Disease Control and Prevention Zika Virus in Pregnancy What Midwives Need To Know
 Centers for Disease Control and Prevention Zika Virus in Pregnancy What Midwives Need To Know Margaret A. Lampe, RN, MPH Pregnancy and Birth Defects Surveillance Team Zika Virus Emergency Response U.S.
Centers for Disease Control and Prevention Zika Virus in Pregnancy What Midwives Need To Know Margaret A. Lampe, RN, MPH Pregnancy and Birth Defects Surveillance Team Zika Virus Emergency Response U.S.
SYPHILIS (Treponema pallidum) IMMEDIATE NOTIFICATION STD PROGRAM
 IMMEDIATE NOTIFICATION STD PROGRAM") SYPHILIS (Treponema pallidum) IMMEDIATE NOTIFICATION STD PROGRAM Event Name: Event Time Period: Clinical Description (CDC 2014) Syphilis 180 days Syphilis is a complex sexually transmitted disease that
SYPHILIS (Treponema pallidum) IMMEDIATE NOTIFICATION STD PROGRAM Event Name: Event Time Period: Clinical Description (CDC 2014) Syphilis 180 days Syphilis is a complex sexually transmitted disease that
Clinical Practice Objectives
 STD Essentials for the Busy Clinician Susan S. Philip, MD, MPH Assistant Professor, Division of Infectious Diseases, UCSF Director, STD Prevention and Control Services San Francisco Department of Public
STD Essentials for the Busy Clinician Susan S. Philip, MD, MPH Assistant Professor, Division of Infectious Diseases, UCSF Director, STD Prevention and Control Services San Francisco Department of Public
Case Report Congenital Syphilis Like Many Years Ago
 Case Reports in Infectious Diseases Volume 2011, Article ID 235059, 4 pages doi:10.1155/2011/235059 Case Report Congenital Syphilis Like Many Years Ago Giulia Brighi, 1 Giorgia Farneti, 1 Antonella Marangoni,
Case Reports in Infectious Diseases Volume 2011, Article ID 235059, 4 pages doi:10.1155/2011/235059 Case Report Congenital Syphilis Like Many Years Ago Giulia Brighi, 1 Giorgia Farneti, 1 Antonella Marangoni,
Obstetric Complications in HIV-Infected Women. Jeanne S. Sheffield, MD Maternal-Fetal Medicine UT Southwestern Medical School
 Obstetric Complications in HIV-Infected Women Jeanne S. Sheffield, MD Maternal-Fetal Medicine UT Southwestern Medical School Obstetric Complications and HIV Obstetric complications are not increased in
Obstetric Complications in HIV-Infected Women Jeanne S. Sheffield, MD Maternal-Fetal Medicine UT Southwestern Medical School Obstetric Complications and HIV Obstetric complications are not increased in
Questions and Answers for Pediatric Healthcare Providers: Infants and Zika Virus Infection
 1 of 5 01/02/2016 20:39 Questions and Answers for Pediatric Healthcare Providers: Infants and Zika Virus Infection Summary CDC has developed interim guidelines for healthcare providers in the United States
1 of 5 01/02/2016 20:39 Questions and Answers for Pediatric Healthcare Providers: Infants and Zika Virus Infection Summary CDC has developed interim guidelines for healthcare providers in the United States
Gonorrhea, Chlamydia, and Syphilis in Alaska
 Department of Health and Social Services Division of Public Health Section of Epidemiology Karen Perdue, Commissioner Karen Pearson, Director John Middaugh, MD, Editor 361 C Street, Suite 54, P.O. Box
Department of Health and Social Services Division of Public Health Section of Epidemiology Karen Perdue, Commissioner Karen Pearson, Director John Middaugh, MD, Editor 361 C Street, Suite 54, P.O. Box
6/11/15. BACTERIAL STDs IN A POST- HIV WORLD. Learning Objectives. How big a problem are STIs in the U.S.?
 BACTERIAL STDs IN A POST- HIV WORLD Tracey Graney, PhD, MT(ASCP) Monroe Community College Learning Objectives Describe the epidemiology and incidence of bacterial STDs in the U.S. Describe current detection
BACTERIAL STDs IN A POST- HIV WORLD Tracey Graney, PhD, MT(ASCP) Monroe Community College Learning Objectives Describe the epidemiology and incidence of bacterial STDs in the U.S. Describe current detection
The Great Imitator Revealed: Syphilis
 The Great Imitator Revealed: Syphilis Jeffrey D. Klausner, MD, MPH Professor of Medicine and Public Health University of California Los Angeles David Geffen School of Medicine Los Angeles, California Learning
The Great Imitator Revealed: Syphilis Jeffrey D. Klausner, MD, MPH Professor of Medicine and Public Health University of California Los Angeles David Geffen School of Medicine Los Angeles, California Learning
STD Essentials for the Busy Clinician. Stephanie E. Cohen, MD, MPH
 STD Essentials for the Busy Clinician Stephanie E. Cohen, MD, MPH Assistant Professor, Division of Infectious Diseases, UCSF Medical Director, City Clinic San Francisco Department of Public Health Disclosures
STD Essentials for the Busy Clinician Stephanie E. Cohen, MD, MPH Assistant Professor, Division of Infectious Diseases, UCSF Medical Director, City Clinic San Francisco Department of Public Health Disclosures
Management of MDR TB in special situations. Dr Sarabjit Chadha The Union
 Management of MDR TB in special situations Dr Sarabjit Chadha The Union MDR TB in special situations Pregnancy Breastfeeding Contraception Renal Insufficiency Diabetes Pregnancy and TB Pregnancy is not
Management of MDR TB in special situations Dr Sarabjit Chadha The Union MDR TB in special situations Pregnancy Breastfeeding Contraception Renal Insufficiency Diabetes Pregnancy and TB Pregnancy is not
1.4.5 SYPHILIS IN PREGNANCY AND THE NEWBORN DIAGNOSIS AND TREATMENT
 WOMEN AND NEWBORN HEALTH SERVICE CLINICAL GUIDELINES SECTION B : GUIDELINES RELEVANT TO OBSTETRICS & MIDWIFERY 1 ANTEPARTUM CARE 1.4 INFECTIONS IN PREGNANCY Authorised by: OGCCU and the Newborn. 1.4.5
WOMEN AND NEWBORN HEALTH SERVICE CLINICAL GUIDELINES SECTION B : GUIDELINES RELEVANT TO OBSTETRICS & MIDWIFERY 1 ANTEPARTUM CARE 1.4 INFECTIONS IN PREGNANCY Authorised by: OGCCU and the Newborn. 1.4.5
in pregnancy Document Review History Version Review Date Reviewed By Approved By
 GYNAECOLOGY/ ANTENATAL CARE WIRRAL WOMEN & CHILDREN S HOSPITAL Guideline No: Hepatitis B management in pregnancy VERSION 1 AMENDMENTS MADE: N/A DATE OF ISSUE: May 2012 DATE OF REVIEW: May 2015 REVIEW INTERVAL:
GYNAECOLOGY/ ANTENATAL CARE WIRRAL WOMEN & CHILDREN S HOSPITAL Guideline No: Hepatitis B management in pregnancy VERSION 1 AMENDMENTS MADE: N/A DATE OF ISSUE: May 2012 DATE OF REVIEW: May 2015 REVIEW INTERVAL:
Neurosyphilis as an Emerging Feature in the HIV Setting. Christina M. Marra, MD University of Washington Seattle, WA, USA
 Neurosyphilis as an Emerging Feature in the HIV Setting Christina M. Marra, MD University of Washington Seattle, WA, USA Syphilis in the Developing World Region 1995 1999 Sub-Saharan 3,530,000 3,828,000
Neurosyphilis as an Emerging Feature in the HIV Setting Christina M. Marra, MD University of Washington Seattle, WA, USA Syphilis in the Developing World Region 1995 1999 Sub-Saharan 3,530,000 3,828,000
12/1/2014 GLOBAL HEALTH CASE STUDY RACHEL LE HISTORY OF PRESENT ILLNESS ANY IDEAS? Location: Vadodara, India Gender: female
 GLOBAL HEALTH CASE STUDY RACHEL LE HISTORY OF PRESENT ILLNESS Location: Vadodara, India Gender: female Age: 14 years Complains: perforation, anterior hard palate, difficulty eating, difficulty speaking
GLOBAL HEALTH CASE STUDY RACHEL LE HISTORY OF PRESENT ILLNESS Location: Vadodara, India Gender: female Age: 14 years Complains: perforation, anterior hard palate, difficulty eating, difficulty speaking
Concerning Testing of Pregnant Women and Newborns for HIV: Sindy M. Paul, MD, MPH, FACPM October 27, 2009
 PL 2007 c 218 An Act Concerning Testing of Pregnant Women and Newborns for HIV: The Regulations Sindy M. Paul, MD, MPH, FACPM October 27, 2009 The Process Legislation signed into law Legislation requires
PL 2007 c 218 An Act Concerning Testing of Pregnant Women and Newborns for HIV: The Regulations Sindy M. Paul, MD, MPH, FACPM October 27, 2009 The Process Legislation signed into law Legislation requires
SYPHILIS (REPORTABLE)
") SYPHILIS (REPORTABLE) PREAMBLE In BC, the diagnosis of syphilis is determined by the BCCDC Provincial STI/HIV Clinic physician directly or in coordination with the*physician or nurse practitioner (NP)
SYPHILIS (REPORTABLE) PREAMBLE In BC, the diagnosis of syphilis is determined by the BCCDC Provincial STI/HIV Clinic physician directly or in coordination with the*physician or nurse practitioner (NP)
Wang Linhong, Deputy Director, Professor National Center for Women and Children s Health, China CDC
 Maternal and Child Health in China Wang Linhong, Deputy Director, Professor National Center for Women and Children s Health, China CDC Table of Contents 1 MCH Development and Situation in China 2 MCH Resources
Maternal and Child Health in China Wang Linhong, Deputy Director, Professor National Center for Women and Children s Health, China CDC Table of Contents 1 MCH Development and Situation in China 2 MCH Resources
Infectious Disease Update
 Infectious Disease Update Karen Rose, RN BSN Communicable Disease Surveillance Nurse; Office of Epidemiology WeArePublicHealth.org twitter.com/maricopahealth facebook.com/mcdph Today s Updates: Influenza
Infectious Disease Update Karen Rose, RN BSN Communicable Disease Surveillance Nurse; Office of Epidemiology WeArePublicHealth.org twitter.com/maricopahealth facebook.com/mcdph Today s Updates: Influenza
Obstetrics and HIV An Update. Jennifer Van Horn MD University of Utah
 Obstetrics and HIV An Update Jennifer Van Horn MD University of Utah Obstetrics and HIV Perinatal transmission Testing Antiretroviral therapy Antepartum management Intrapartum management Postpartum management
Obstetrics and HIV An Update Jennifer Van Horn MD University of Utah Obstetrics and HIV Perinatal transmission Testing Antiretroviral therapy Antepartum management Intrapartum management Postpartum management
Injury Chronic Disease Infant Mortality Maternal & Child Health Infectious Disease Life Expectancy
 Visit WatchUsThrive.org to learn more Welcome to the Community Health Pathway of WeTHRIVE! SM Here you will find a brief Community Health Assessment for your community. This will provide you with health
Visit WatchUsThrive.org to learn more Welcome to the Community Health Pathway of WeTHRIVE! SM Here you will find a brief Community Health Assessment for your community. This will provide you with health
OB Provider Guide to Alaska s Perinatal Hepatitis B Prevention Program
 OB Provider Guide to Alaska s Perinatal Hepatitis B Prevention Program Dear Colleague, This letter is to introduce myself and explain the role I play with the Alaska Perinatal Hepatitis B Program. Alaska
OB Provider Guide to Alaska s Perinatal Hepatitis B Prevention Program Dear Colleague, This letter is to introduce myself and explain the role I play with the Alaska Perinatal Hepatitis B Program. Alaska
STI Indicators by STI
 STI Indicators by STI Table of Contents pg. 2 Sexual History pg. 3-4 Syphilis pg. 5-6 Gonorrhea pg. 7-9 Chlamydia pg. 10 HIV/PrEP 1 Sexual History Comprehensive Sexual History Elements Percentage of patients
STI Indicators by STI Table of Contents pg. 2 Sexual History pg. 3-4 Syphilis pg. 5-6 Gonorrhea pg. 7-9 Chlamydia pg. 10 HIV/PrEP 1 Sexual History Comprehensive Sexual History Elements Percentage of patients
NIH Public Access Author Manuscript Clin Infect Dis. Author manuscript; available in PMC 2009 October 1.
 NIH Public Access Author Manuscript Published in final edited form as: Clin Infect Dis. 2008 October 1; 47(7): 893 899. doi:10.1086/591534. Normalization of Serum Rapid Plasma Reagin Titer Predicts Normalization
NIH Public Access Author Manuscript Published in final edited form as: Clin Infect Dis. 2008 October 1; 47(7): 893 899. doi:10.1086/591534. Normalization of Serum Rapid Plasma Reagin Titer Predicts Normalization
The U.S. Preventive Services Task Force (USPSTF) makes
 makes") Annals of Internal Medicine Clinical Guidelines Screening for Syphilis Infection in Pregnancy: U.S. Preventive Services Task Force Reaffirmation Recommendation Statement U.S. Preventive Services Task Force*
Annals of Internal Medicine Clinical Guidelines Screening for Syphilis Infection in Pregnancy: U.S. Preventive Services Task Force Reaffirmation Recommendation Statement U.S. Preventive Services Task Force*
Invasive Neonatal Group-B Streptococcus (GBS) Disease in Wisconsin,
 Disease in Wisconsin,") Invasive Neonatal Group-B Streptococcus (GBS) Disease in Wisconsin, 2002-2008 2008 Hanne Nissen Bjørnsen RN, MS MPH Candidate 2010 University of Wisconsin - Madison May 7 th 2010 Streptococcus agalactiae
Invasive Neonatal Group-B Streptococcus (GBS) Disease in Wisconsin, 2002-2008 2008 Hanne Nissen Bjørnsen RN, MS MPH Candidate 2010 University of Wisconsin - Madison May 7 th 2010 Streptococcus agalactiae
Epatite B: fertilità, gravidanza ed allattamento, aspetti clinici e terapeutici. Ivana Maida
 Epatite B: fertilità, gravidanza ed allattamento, aspetti clinici e terapeutici Ivana Maida Positivity for HBsAg was found in 0.5% of tested women In the 70s and 80s, Italy was one of the European countries
Epatite B: fertilità, gravidanza ed allattamento, aspetti clinici e terapeutici Ivana Maida Positivity for HBsAg was found in 0.5% of tested women In the 70s and 80s, Italy was one of the European countries
STDs in HIV Clinical Care: New Guidelines on Treatment and Prevention
 STDs in HIV Clinical Care: New Guidelines on Treatment and Prevention Palliative Care Conference Faculty Development Conference August 13, 2015 Steven C. Johnson M.D. Director, University of Colorado HIV/AIDS
STDs in HIV Clinical Care: New Guidelines on Treatment and Prevention Palliative Care Conference Faculty Development Conference August 13, 2015 Steven C. Johnson M.D. Director, University of Colorado HIV/AIDS
GENITAL HERPES. 81.1% of HSV-2 infections are asymptomatic or unrecognized. Figure 14 HSV-2 seroprevalence among persons aged years by sex.
 GENITAL HERPES Genital herpes is a chronic, lifelong, sexually transmitted disease caused by herpes simplex virus type 1 (HSV-1) and type 2 (HSV-2). HSV-1 typically causes small, painful, fluid-filled,
GENITAL HERPES Genital herpes is a chronic, lifelong, sexually transmitted disease caused by herpes simplex virus type 1 (HSV-1) and type 2 (HSV-2). HSV-1 typically causes small, painful, fluid-filled,
Zika Virus Guidance for Medical Providers. Denise Smith, PHN, MPA Director of Disease Control Kern County Public Health Services Department
 Zika Virus Guidance for Medical Providers Denise Smith, PHN, MPA Director of Disease Control Kern County Public Health Services Department Kern Perinatal Symposium March 3, 2017 CME DISCLOSURE The Planners,
Zika Virus Guidance for Medical Providers Denise Smith, PHN, MPA Director of Disease Control Kern County Public Health Services Department Kern Perinatal Symposium March 3, 2017 CME DISCLOSURE The Planners,
Serological screening for syphilis in HIV-infected individuals: is a non-treponemal test adequate in the era of increasing of new syphilis infections?
 Abstract no. WEPE 494 Serological screening for syphilis in HIV-infected individuals: is a non-treponemal test adequate in the era of increasing of new syphilis infections? G.Chrysos 1, D.Karageorgopoulos
Abstract no. WEPE 494 Serological screening for syphilis in HIV-infected individuals: is a non-treponemal test adequate in the era of increasing of new syphilis infections? G.Chrysos 1, D.Karageorgopoulos
Infectious syphilis in Canada:
 30 CCDR 05 February 2015 Volume 41-2 https://doi.org/10.14745/ccdr.v41i02a03 Infectious syphilis in Canada: 2003-2012 Totten S 1,*, MacLean R 1, Payne E 1 1 Centre for Communicable Diseases and Infection
30 CCDR 05 February 2015 Volume 41-2 https://doi.org/10.14745/ccdr.v41i02a03 Infectious syphilis in Canada: 2003-2012 Totten S 1,*, MacLean R 1, Payne E 1 1 Centre for Communicable Diseases and Infection
Lecture-7- Hazem Al-Khafaji 2016
 TOXOPLASMOSIS Lecture-7- Hazem Al-Khafaji 2016 TOXOPLASMOSIS It is a disease caused by Toxoplasma gondii which is a protozoan parasite that is infects a variety of mammals and birds throughout the world.
TOXOPLASMOSIS Lecture-7- Hazem Al-Khafaji 2016 TOXOPLASMOSIS It is a disease caused by Toxoplasma gondii which is a protozoan parasite that is infects a variety of mammals and birds throughout the world.
Congenital syphilis: global trends
 Sex, Sores, Science and Surveillance: Syphilis in the 21 st Century (UO20) Congenital syphilis: global trends Adriana R. Cruz A. Associate professor Universidad del Valle Research associate CIDEIM Cali,
Sex, Sores, Science and Surveillance: Syphilis in the 21 st Century (UO20) Congenital syphilis: global trends Adriana R. Cruz A. Associate professor Universidad del Valle Research associate CIDEIM Cali,
Perinatal Hepatitis b Prevention
 Perinatal Hepatitis b Prevention Purpose 2 The primary goal of the Perinatal Hepatitis b Prevention Program (PHBPP) is to identify all pregnant women who are infected with hepatitis b and prevent perinatal
Perinatal Hepatitis b Prevention Purpose 2 The primary goal of the Perinatal Hepatitis b Prevention Program (PHBPP) is to identify all pregnant women who are infected with hepatitis b and prevent perinatal
transmission (MTCT) of
 of") Training Course in Sexual and Reproductive Health Research 2013 Module: Principles and Practice of Sexually Transmitted Infections Prevention and Care Dual elimination of mother-to-child transmission (MTCT)
Training Course in Sexual and Reproductive Health Research 2013 Module: Principles and Practice of Sexually Transmitted Infections Prevention and Care Dual elimination of mother-to-child transmission (MTCT)
Timby/Smith: Introductory Medical-Surgical Nursing, 9/e
 Timby/Smith: Introductory Medical-Surgical Nursing, 9/e Chapter 62: Caring for Clients With Sexually Transmitted Diseases Slide 1 Epidemiology Introduction Study of the occurrence, distribution, and causes
Timby/Smith: Introductory Medical-Surgical Nursing, 9/e Chapter 62: Caring for Clients With Sexually Transmitted Diseases Slide 1 Epidemiology Introduction Study of the occurrence, distribution, and causes
Changing Provincial Regulations: The Newborn Eye Prophylaxis Story
 Changing Provincial Regulations: The Newborn Eye Prophylaxis Story Janet Walker, RN Director, Provincial Knowledge Transformation & Acute Care Healthy Mothers and Healthy Babies Conference March 12, 2016
Changing Provincial Regulations: The Newborn Eye Prophylaxis Story Janet Walker, RN Director, Provincial Knowledge Transformation & Acute Care Healthy Mothers and Healthy Babies Conference March 12, 2016
Congenital Cytomegalovirus (CMV)
") August 2011 Congenital Cytomegalovirus (CMV) Revision Dates Case Definition Reporting Requirements Remainder of the Guideline (i.e., Etiology to References sections inclusive) August 2011 August 2011 June
August 2011 Congenital Cytomegalovirus (CMV) Revision Dates Case Definition Reporting Requirements Remainder of the Guideline (i.e., Etiology to References sections inclusive) August 2011 August 2011 June
EPIDEMIC OF SYPHILIS
 Brian Sandoval Governor Richard Whitley, MS Director Julie Kotchevar, PhD Administrator Ihsan Azzam, PhD, Md Chief Medical Officer EPIDEMIC OF SYPHILIS Understanding the Clinical & Public Health Need for
Brian Sandoval Governor Richard Whitley, MS Director Julie Kotchevar, PhD Administrator Ihsan Azzam, PhD, Md Chief Medical Officer EPIDEMIC OF SYPHILIS Understanding the Clinical & Public Health Need for
Trends in Reportable Sexually Transmitted Diseases in the United States, 2007
 Trends in Reportable Sexually Transmitted Diseases in the United States, 2007 National Surveillance Data for Chlamydia, Gonorrhea, and Syphilis Sexually transmitted diseases (STDs) remain a major public
Trends in Reportable Sexually Transmitted Diseases in the United States, 2007 National Surveillance Data for Chlamydia, Gonorrhea, and Syphilis Sexually transmitted diseases (STDs) remain a major public
NIDA Rationale Clean 1 09/17/06
 Rationale for Modifications to the 2001 National Institute on Drug Abuse Policy on Counseling and Testing for HIV/AIDS and other Infectious Diseases (NOT-DA-01-001). This document identifies and provides
Rationale for Modifications to the 2001 National Institute on Drug Abuse Policy on Counseling and Testing for HIV/AIDS and other Infectious Diseases (NOT-DA-01-001). This document identifies and provides
Tribal Vector Borne Disease Meeting Inter Tribal Council of Arizona, Inc. Tribal Epidemiology Center February 13-15, 2018 Chandler, AZ
 CDC S Response to Zika Tribal Vector Borne Disease Meeting Inter Tribal Council of Arizona, Inc. Tribal Epidemiology Center February 13-15, 2018 Chandler, AZ Dr. Maleeka Glover Lead, Medical Investigations
CDC S Response to Zika Tribal Vector Borne Disease Meeting Inter Tribal Council of Arizona, Inc. Tribal Epidemiology Center February 13-15, 2018 Chandler, AZ Dr. Maleeka Glover Lead, Medical Investigations
Syphilis Update. roadmap
 AND Nurse Practitioners!!! AND Physician Assistants!!! Oliver Bacon, MD, MPH Physician, SF City Clinic Disease Prevention and Control Branch Population Health Division roadmap 1. Syphilis: diagnosis and
AND Nurse Practitioners!!! AND Physician Assistants!!! Oliver Bacon, MD, MPH Physician, SF City Clinic Disease Prevention and Control Branch Population Health Division roadmap 1. Syphilis: diagnosis and
Learning Objectives. STI Update. Case 1 6/1/2016
 Learning Objectives STI Update June 16 th, 2016 Madhu Choudhary, MD. FIDSA Assoc. Prof of Medicine Albany Medical College Review screening recommendations for STI in different patient populations Describe
Learning Objectives STI Update June 16 th, 2016 Madhu Choudhary, MD. FIDSA Assoc. Prof of Medicine Albany Medical College Review screening recommendations for STI in different patient populations Describe
Clinical Cases from the STD Clinical Consultation Network
 Clinical Cases from the STD Clinical Consultation Network Christine Johnston STD TCG April 24, 2017 Last Updated: uwptc@uw.edu uwptc.org 206-685-9850 STD Clinical Consultation Network (STDCCN) Developed
Clinical Cases from the STD Clinical Consultation Network Christine Johnston STD TCG April 24, 2017 Last Updated: uwptc@uw.edu uwptc.org 206-685-9850 STD Clinical Consultation Network (STDCCN) Developed
2/13/ Graphic photographs or cartoons used during this presentation might be offensive to some; for this I apologize in advance.
 Leon Bullard, MD, MA Medical Consultant, DHEC, DADE The 23 rd Annual APRN Conference Charleston, SC February 24, 2017 1. Provide a brief (very) review of the syphilis story. 2. Define and discuss the stages
Leon Bullard, MD, MA Medical Consultant, DHEC, DADE The 23 rd Annual APRN Conference Charleston, SC February 24, 2017 1. Provide a brief (very) review of the syphilis story. 2. Define and discuss the stages
4/6/17 UNPRECEDENTED HIGH. Shelagh Larson, RNC, WHNP, NCMP
 Shelagh Larson, RNC, WHNP, NCMP UNPRECEDENTED HIGH Total combined cases of chlamydia, gonorrhea, and syphilis reported in 2015 reached the highest number ever, according to the annualmore than 1.5 million
Shelagh Larson, RNC, WHNP, NCMP UNPRECEDENTED HIGH Total combined cases of chlamydia, gonorrhea, and syphilis reported in 2015 reached the highest number ever, according to the annualmore than 1.5 million
Summary Guidelines for the Use of Herpes Simplex Virus (HSV) Type 2 Serologies
 Type 2 Serologies") Summary Guidelines for the Use of Herpes Simplex Virus (HSV) Type 2 Serologies Genital herpes is one of the most prevalent sexually transmitted diseases, affecting more than one in five sexually active
Summary Guidelines for the Use of Herpes Simplex Virus (HSV) Type 2 Serologies Genital herpes is one of the most prevalent sexually transmitted diseases, affecting more than one in five sexually active
Communicable Diseases
 Communicable Diseases Communicable diseases are ones that can be transmitted or spread from one person or species to another. 1 A multitude of different communicable diseases are currently reportable in
Communicable Diseases Communicable diseases are ones that can be transmitted or spread from one person or species to another. 1 A multitude of different communicable diseases are currently reportable in
Yakima Health District BULLETIN
 Yakima Health District BULLETIN Volume 12, Issue 4 December, 2013 Overview Prevention of Perinatal Hepatitis B Transmission Perinatal transmission of hepatitis B virus (HBV) is preventable through universal
Yakima Health District BULLETIN Volume 12, Issue 4 December, 2013 Overview Prevention of Perinatal Hepatitis B Transmission Perinatal transmission of hepatitis B virus (HBV) is preventable through universal
Maternal and Child Health, Substance Abuse Ohio Department of Health, Bureau of Maternal Child and Family Health
 Maternal and Child Health, Substance Abuse Ohio Department of Health, Bureau of Maternal Child and Family Health Columbus, Ohio Assignment Description The rapid advance of the opiate crisis has had far
Maternal and Child Health, Substance Abuse Ohio Department of Health, Bureau of Maternal Child and Family Health Columbus, Ohio Assignment Description The rapid advance of the opiate crisis has had far