Ian Kitai TB Specialist. Division of Infectious Diseases Sickkids
|
|
|
- Gordon Gilmore
- 6 years ago
- Views:
Transcription



1 Ian Kitai TB Specialist Division of Infectious Diseases Sickkids
2 Review Clinical presentation of TB disease childhood How to assess risk for TB infection How to assess risk for disease if infected TST s and IGRA s benefits Discuss monitoring during therapy, side effects and reactions to treatment
3 Canadian TB Standards 2007 Google it Excellent resource especially diagnosis section excellent summary of literature. Some of this talk with audio Webber training course Frances Curry Center excellent resources, drug information
4 TB in the world 1 new case every 3 seconds 1 TB death every 19 seconds Global statistics as based on smear positive individuals: underestimate pediatric TB World Health Statistics
5 7 week old Aunt visiting from endemic country Cough marked History of TB treatment in past Taken to walk in clinic, X rayed, abnormal Mom concerned re exposure of infant Sees pediatrician
6 11 year old, Born Congo Crohns, growth Failure Failing Methotrexate Being considered for Infliximab Evaluation?
7 16 year old Volunteer at hospital Born Canada moved to Dubai, Lived in Pakistan: Returned 10 years ago. Had BCG at 18 months of age No known TB contact TST 10mm Normal Chest X ray

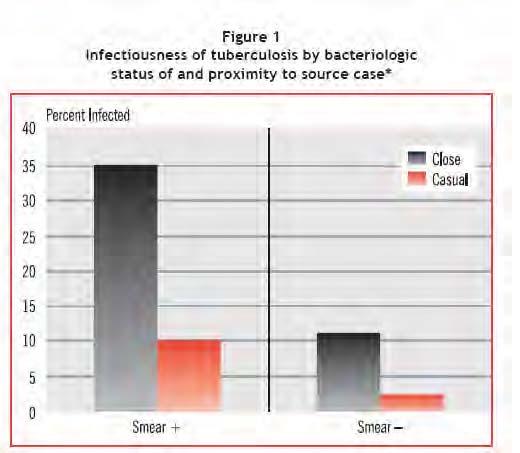
8 1. Close contacts with multibacillary and cavitary disease and cough-adults or ADOLESCENTS 2. Less often: smear negative culture positive patients
9 Standard response Young children (approx <10) do not spread TB to others Childhood Tb is paucibacillary Children do not generate cough to spread TB Little role for isolation This message is largely true- BUT there ARE a FEW exceptions which can be anticipated from the clinical circumstances
10 Munoz et al- Texas children s Screened adult visitors of 59 consecutive children admitted with TB Isolation if thought have potential to be airborne 8 children required isolation 16/105 (15%) screened adult visitors -- previously undetected pulmonary TB. Risk- mainly from adults accompanying child Infect Control Hosp Epidemiol :
11
12 Very young < 1 Miliary, pulmonary, extrapulmonary, TB meningitis Young child Primary complex and its complications Overlap Older child and adolescent Pulmonary and extrapulmonary protean.
13 3 month old Hx pertussis like cough Fever Canadian Born Unwell
14 Unwell Hemophagocytosis Hepatosplenomegaly ICU admission Cavitary disease infected close contacts.


15 Age at Primary Infection Manifestations of Disease Risk of Disease (%) < 12 months No disease Pulmonary disease TB meningitis or miliary disease months No disease Pulmonary disease TB meningitis or miliary disease years No disease Pulmonary disease TB meningitis or miliary disease years No disease Pulmonary disease TB meningitis or miliary disease 98 2 < 0.5 > 10 years No disease Pulmonary disease TB meningitis or miliary disease < 0.5 Marais BJ, et al. The natural history of childhood intra-thoracic tuberculosis: a critical review of literature from the pre-chemotherapy era. Int J Tuberc Lung Dis 2004;8(4):
16 7 week old Aunt visiting from endemic country Cough marked History of TB treatment in past Taken to walk in clinic, X rayed, abnormal Mom concerned re exposure of infant Sees pediatrician
17 Referred to TB clinic Physical exam normal Chest X ray normal TB skin test 0mm at 48 hours What to do next??
18 GET SOURCE CASE DETAILS Xray- extensive upper lobe disease Positive skin test No sputum sent Public health in clinic notified home follow up Aunt- sputum smear numerous, AMTD positive What next?
19 Window prophylaxis INH (10mg/kg/day) in young infants use mg/kg to allow for rapid growth and adjust monthly based on weight Available as suspension Pyridoxine in breastfed- 1-2mg/kg/day is plenty (crushed tabs) What follow up?
20 High risk of drug resistance Need to get source case sensitivities Turnaround typically 1-2 weeks for culture 2-3 weeks or sensitivities INH resistant--? INH and rifampin resistant?
21 Rapid progression to TB disease Often disseminated May be miliary, TB meningitis TB EXPOSURES: The younger child the more urgent the need for prophylaxis.
22 X ray and PPD all children PPD negative: clinically well Preventive Rx to all < 5 (varies) Repeat TST 10 weeks (8-12 weeks) after break in contact D/c Rx if repeat ve. Infant<6months treat until age 6 months And ppd negative
23 PPD positive: Rule out disease If clinically well, Normal chest X ray Preventive Rx INH sensitive: INH 10-15mg/kg/d for 9 months Pyridoxine 1-2mg/kg. Adults 25-50mg/kg
24 INH resistant contacts: Refer if possible EXCLUDE DISEASE!! Rifampin 10mg/kg/day until proven negative If LTBI --for 4 to 6 months No RCT but theoretically better drug than INH MultiDrug resistant contacts no data, need referral/discussion.
25 A few bacilli Sequestered somewhere Undetectable clinically Able to reactivate Vey cunning strategy to sustain an epidemic over centuries.





26 EXPOSURE Child exposed to bacilli from adult or adolescent More TB meningitis common in the No infection Primary complex Miliary TB young child Heals -- latent infection Progresses
27 ONTARIO TB: SITES OF DISEASE BY AGE 100% 80% % 60% 40% 20% 0% Both Extrapulmonary Pulmonary Age
28 precx natural history 100% 90% 80% 70% 60% 50% 40% Meningitis/Miliary Pulmonary No disease 30% 20% 10% 0% < 12 months 12-23mo
29 1 st Step to disease Lifetime risk of developing TB 1:10-1:20 Prevent TB by reducing pool of infectious adults who transmit to the next generation Young children, immunocompromised, at high risk of rapid progression to severe disease
30 Approximately 10% Lifetime risk of developing disease. UPHS trial 1957 Most disease (about 40%) occurs within first 2 years of infection Several factors increase risk of disease.
31 Well patient- asymptomatic Poor tests No gold standards Outcome if not treated usually curable Sequelae/fatalities especially in young and immunocompromised Rare but serious toxicity of treatment
32 How likely is the child to have been infected? Close contact Endemic country
33 What might happen if the patient really is infected? Immunocompromised HIV infection Renal failure Diabetes 2 fold risk but very prevelant risk factor Young age
 15x Age<6")
34 AIDS x HIV infection x Transplantation 20 74x CRF hemodialysis 10 15x Recent TB infection (<2yrs) 15x Age<6 months?
 2.0 3.6x Underweight (90% <IBW); 2.0-3x Age < 4 2.")
35 Risk Rx with glucocorticoids 4.9x TNF-alpha inhibitors 1.5 4x Diabetes mellitus (all types) x Underweight (90% <IBW); 2.0-3x Age < x Abnormal CxR granuloma 2x
36 Treatment is for the patient s benefit. Patient needs to understand the risks, benefits and intention of treatment In their own language. And accept treatment Young infants with significant exposures or LTBI may be exception If for the public good- where s the no fault compensation and legislation?
37 TST: 200 antigens Developed early 20 th century Administered intradermally Requires reading at timed intervals Inter and intraobserver variability For standardisation see Canadian TB Standards page 55
38 Induration > 5 mm Close contact with infectious TB Suspected TB disease immunosuppressive Rx immunocompromised (including HIV)
39 Induration > 10 mm (including BCG) increased risk of disseminated disease < 4 years of age medical risk factors: malnutrition, malignancy increased environmental TB exposure Child/parents born in high prevalence area travel to high prevalence area Adult contact is HIV positive/ homeless/ IVDU/ institutionalized
40 False negatives: very young children, Immunocompromised malnutrition, concurrent chronic medical conditions, other viral and parasitic infections. Sensitivity in active and or disseminated TB only 77% recent meta-analysis. - Deil CHEST 2010: 137:
41 Unknown: PPV a real problem for low risk populations Size matters (>20mm more significant than >10mm) BCG given at birth: most lose reactivity by 10 years BUT great variability different BCG strains, Influence of environmental mycobacteria BCG in later life: approx 25% positive for life Positive second step tests correlate with BCG better than with disease states
42 Variable sensitivity in immunocompromised patients and in active disease Poor/variable specificity in BCG vaccinated populations Poor standardization Inter and intra-observer variability Need for a return visit within 48-72hrs for interpretation...reluctance to look for and screen for LTBI
43 Validated as marker for progression to active disease USPHS trials from 1957 showed about 5-10% risk of developing TB disease over a lifetime in TST positive (and marked reduction in risk with 6-12 months INH) Controlled chemoprophylaxis trials in tuberculosis. A general review. Ferebee SH - Bibl Tuberc - 01-JAN-1970; 26:

44 measure the in vitro production of interferon gamma by sensitized lymphocytes in response to M. TB specific antigens. Antigens USED DO NOT OCCUR not in BCG or in the majority of non-tuberculous mycobacteria.
45 No gold standard for latent TB infection active disease used as a surrogate when quantifying specificity IGRA specificity (93-99%) consistently >> TST (60%) in BCG vaccinated populations IGRA correlates better with gradients of exposure to infectious source cases that the TST in low incidence settings
46 A positive IGRA may be indicative of TB infection however low level positives that revert and convert are described and are of uncertain significance
47 Sensitivity of the IGRA is variable across studies, high vs. low incidence settings, pediatric vs. adult data, active vs. LTBI In active TB, the sensitivity of the IGRA 75-90% (QFT less sensitive than T-SPOT TB) In clinical LTBI, overall agreement between TST and IGRA in children is 55-95%, Majority of discordant values TST+/IGRA-
48 To date no longitudinal studies on the predictive value of a negative IGRA on children who do not receive chemoprophylaxis as a result. A negative IGRA does not rule out TB disease Many reports of IGRA s failing to detect TB in children and adults Very Limited data in children<5: Redbook- don t use <5 but can use >5 in most situations where TST is used.
49 Few data No longitudinal data Reasonable agreement with TST Less influenced by BCG Sensitivity--? Seem fairly specific Low level positives may be false positives
50 In children may be used in addition to TST to support diagnosis of infection which is sometimes used to help support diagnosis of disease. Does NOT take the place of collection of clinical specimens.

51 May increase sensitivity in immunocompromised when combined with the TST: T spot better than QFT Confirmatory rule out test for patients not thought to be at high risk for TB infection. Research tool for population surveys Not recommended for staff, immigration screening. but this is under review
52 Alberta PHL does them Ontario- not routine Commercial Laboratory: 2 sites; $90 per test
53 2 year old Mother found to have smear positive cavitary disease Well child N CxR USE TST AND IGRA (if available). Any positive=positive and needs treatment for LTBI. Repeat TST + IGRA 8-12 weeks after break in contact
54 16 year old Volunteer at hospital Born Dubai, Lived in Pakistan: Immigrated 10 years ago. Had BCG No known TB contact TST 10mm Normal Chest X ray Low risk. May use negative IGRA to help decide against prophylaxis.
55 11 year old Crohns, Growth Failure Failing Metotrexate, NSAID s Being considered for Infliximab Evaluation? Immunocompromised and at high risk USE TST AND IGRA. Any positive=positive and needs treatment for LTBI.
56 Interferes with mycolic acid production Keep at room temperature Fatty meal- 50% less absorption Penetrates well into inflamed meninges B6 important in adults S/E Hepatic, CNS, Peripheral neuropathy. Validated in RCFT s to prevent TB disease in infected. 9 months standard Rx - 80%+protection
57 Inform patient of S/E and to D/C if Anorexia, Nausea, Jaundice, Abdominal Pain, Vomiting. Provide contact numbers and plan See monthly Ask about side effects Routine LFT s not considered necessary but do if ANY S/E Is this enough?
58 Case 10 Female LTBI CLOSE CONTACT 12 MM MANTOUX Normal Baseline LFT s On INH for 7 months Seen monthly Discussion of side effects and what to do x3 2 weeks after last clinic visit c/o pain and vomiting Thought to be wanting to avoid school
59 Continued to c/pain Presented jaundiced Very lively and active No hepatic tenderness HIGH bilirubin. AST 3000 s ALT 3000 INR 1.6 Admitted. Listed for liver transplant Ultimately recovered A VERY near miss
60 All US pediatric transplant centers cases severe liver disease 4 recovered 6 died awaiting OLT 10 transplanted Estimated incidence 3.2/ INH courses 14% of drug induced liver disease needing Tx Wu Transplantation 2007
61 4 year old no risk factors Kindergarten entry tested INH Information sheet. Well at 3 weeks 10 weeks- vomiting, thought to have stomach flu 11 weeks jaundice, AST 4200, Liver transplant
62 MMWR State health departments about patients start therpy per year 17 cases 2-9 months after initiating therapy Most followed according to guidelines 5 transplants 5deaths (1Tx) 8 recovered Taking INH while symptomatic risk factor
63 What are the public health implications for public health practice? Patients receiving INH therapy for LTBI should be told categorically by medical providers to stop taking their medication immediately if they have symptoms such as nausea, vomiting, abdominal discomfort, or unexplained fatigue and to contact their providers for further evaluation.
64 Your child has been prescribed a drug called Isoniazid to prevent Tuberculosis disease from developing. This medicine usually has few or no side effects. Very rarely the medicine can affect the liver. If this occurs your child may: Vomit Complain of tummy ache Not want to eat Feel very tired Become yellow around the white part of the eyes If these symptoms or signs occur STOP GIVING THE MEDICINE and call us. Patricia Malloy can be reached at and the clinic nurse can be reached at Otherwise call and ask to speak to the infectious diseases fellow on call. Don t start the medicine again until the child has been checked.
65 1. Children generally acquire TB from adolescents and adults. Most children are not infectious to others 2. Risks of and presentation of TB disease changes with age. 3. The younger child the more urgent the need for evaluation and prophylaxis 4. Extrapulmonary disease is common in children and adolescents in Canada and North America 5. INH toxicity is rare but can be fatal. Counsel patients carefully and accurately in patient s language. Always monitor according to guidelines. D/C if any side effects
66 Public Health gives all/ almost all the info! Source case: Smear and culture results PHL specimen # helpful. Update sensitivities when they become available Break in contact date NBB.
67 Local epidemiology helpful- how many contacts are positive and # tested Ongoing smear results from index case: Break in Contact Use smear negative plus 2 weeks.
Tuberculosis in Children and Adolescents Dr. Ian Kitai, Hospital for Sick Children, Toronto A Webber Training Teleclass
 TB in Children and Adolescents - Problems in Diagnosis and Infection Control Dr. Ian Kitai Division of Infectious Diseases Hospital for Sick Children Hosted by Paul Webber paul@webbertraining.com www.webbertraining.com
TB in Children and Adolescents - Problems in Diagnosis and Infection Control Dr. Ian Kitai Division of Infectious Diseases Hospital for Sick Children Hosted by Paul Webber paul@webbertraining.com www.webbertraining.com
Contact Investigation and Prevention in the USA
 Contact Investigation and Prevention in the USA George D. McSherry, MD Division of Infectious Disease Penn State Children s Hospital Pediatric Section TB Center of Excellence Rutgers Global Tuberculosis
Contact Investigation and Prevention in the USA George D. McSherry, MD Division of Infectious Disease Penn State Children s Hospital Pediatric Section TB Center of Excellence Rutgers Global Tuberculosis
Treatment of TB Infection Lisa Y. Armitige, MD, PhD April 7, 2015
 Treatment of TB Infection Lisa Y. Armitige, MD, PhD April 7, 2015 Tuberculosis Infection Diagnosis and Treatment April 7, 2015 El Paso, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has
Treatment of TB Infection Lisa Y. Armitige, MD, PhD April 7, 2015 Tuberculosis Infection Diagnosis and Treatment April 7, 2015 El Paso, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has
TB Nurse Case Management San Antonio, Texas July 18 20, 2012
 TB Nurse Case Management San Antonio, Texas July 18 20, 2012 Pediatric TB Kim Smith, MD, MPH July 19, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
TB Nurse Case Management San Antonio, Texas July 18 20, 2012 Pediatric TB Kim Smith, MD, MPH July 19, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
Fundamentals of Tuberculosis (TB)
") TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
PREVENTION OF TUBERCULOSIS. Dr Amitesh Aggarwal
 PREVENTION OF TUBERCULOSIS Dr Amitesh Aggarwal 25 to 50 % of persons exposed to intimate contact with active PTB - latent infection with TB. Exposure to index case for 12 hours - high risk of infection.
PREVENTION OF TUBERCULOSIS Dr Amitesh Aggarwal 25 to 50 % of persons exposed to intimate contact with active PTB - latent infection with TB. Exposure to index case for 12 hours - high risk of infection.
Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017
 Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has the following disclosures
Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has the following disclosures
Tuberculosis in Primary Care COC GTA Spring Symposium Dr Elizabeth Rea April 2013
 Tuberculosis in Primary Care COC GTA Spring Symposium Dr Elizabeth Rea April 2013 1 TB in Toronto - risk groups Diagnosis of active TB LTBI diagnosis and management Infection control 2 TB in Toronto Case
Tuberculosis in Primary Care COC GTA Spring Symposium Dr Elizabeth Rea April 2013 1 TB in Toronto - risk groups Diagnosis of active TB LTBI diagnosis and management Infection control 2 TB in Toronto Case
TB Nurse Case Management San Antonio, Texas March 7 9, Pediatric TB Kim Connelly Smith, MD, MPH March 8, 2012
 TB Nurse Case Management San Antonio, Texas March 7 9, 2012 Pediatric TB Kim Connelly Smith, MD, MPH March 8, 2012 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict of interests
TB Nurse Case Management San Antonio, Texas March 7 9, 2012 Pediatric TB Kim Connelly Smith, MD, MPH March 8, 2012 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict of interests
Tuberculosis Tools: A Clinical Update
 Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
Latent Tuberculosis Infection (LTBI) Questions and Answers for Health Care Providers
 Questions and Answers for Health Care Providers") Latent Tuberculosis Infection (LTBI) Questions and Answers for Health Care Providers Who Should Be Screened for Latent Tuberculosis Infection (LTBI)?... 2 What tests are used to screen for LTBI?... 2 How
Latent Tuberculosis Infection (LTBI) Questions and Answers for Health Care Providers Who Should Be Screened for Latent Tuberculosis Infection (LTBI)?... 2 What tests are used to screen for LTBI?... 2 How
Pediatric TB Lisa Armitige, MD, PhD September 28, 2011
 TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Pediatric TB Lisa Armitige, MD, PhD September 28, 2011 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interest.
TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Pediatric TB Lisa Armitige, MD, PhD September 28, 2011 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interest.
CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT]
![CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT]](/thumbs/89/99628771.jpg "CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT]") CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT] QUESTION: : Which children in the United States should get a tuberculin skin test? Do questionnaires really work? Jeffrey
CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT] QUESTION: : Which children in the United States should get a tuberculin skin test? Do questionnaires really work? Jeffrey
Management of Pediatric Tuberculosis in New Jersey
 Management of Pediatric Tuberculosis in New Jersey Helen Aguila, MD NJMS Global TB Institute December 15, 2011 This presentation is in part adapted from Pediatric Tuberculosis by Ann Loeffler, MD : Francis
Management of Pediatric Tuberculosis in New Jersey Helen Aguila, MD NJMS Global TB Institute December 15, 2011 This presentation is in part adapted from Pediatric Tuberculosis by Ann Loeffler, MD : Francis
TUBERCULOSIS. Presented By: Public Health Madison & Dane County
 TUBERCULOSIS Presented By: Public Health Madison & Dane County What is Tuberculosis? Tuberculosis, or TB, is a disease caused by a bacteria called Mycobacterium tuberculosis. The bacteria can attack any
TUBERCULOSIS Presented By: Public Health Madison & Dane County What is Tuberculosis? Tuberculosis, or TB, is a disease caused by a bacteria called Mycobacterium tuberculosis. The bacteria can attack any
Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010
 Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 What is Latent TB Infection (LTBI)? Traci Hadley, RN October 5, 2010 LTBI or TB Disease? Presented by : Traci Hadley, RN
Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 What is Latent TB Infection (LTBI)? Traci Hadley, RN October 5, 2010 LTBI or TB Disease? Presented by : Traci Hadley, RN
Tuberculosis Intensive
 Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Childhood Tuberculosis Kim Smith, MD, MPH April 6, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Childhood Tuberculosis Kim Smith, MD, MPH April 6, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
CHAPTER 3: DEFINITION OF TERMS
 CHAPTER 3: DEFINITION OF TERMS NOTE: TB bacteria is used in place of Mycobacterium tuberculosis and Mycobacterium tuberculosis complex in most of the definitions presented here. 3.1 Acid-fast bacteria
CHAPTER 3: DEFINITION OF TERMS NOTE: TB bacteria is used in place of Mycobacterium tuberculosis and Mycobacterium tuberculosis complex in most of the definitions presented here. 3.1 Acid-fast bacteria
TB Skin Test Practicum Houston, Texas Region 6/5 South September 23, 2014
 TB Skin Test Practicum Houston, Texas Region 6/5 South September 23, 2014 Catalina Navarro, BSN, RN has the following disclosures to make: No conflict of interests No relevant financial relationships with
TB Skin Test Practicum Houston, Texas Region 6/5 South September 23, 2014 Catalina Navarro, BSN, RN has the following disclosures to make: No conflict of interests No relevant financial relationships with
TB in Corrections Phoenix, Arizona
 TB in Corrections Phoenix, Arizona March 24, 2011 Treatment of Latent TB Infection Renuka Khurana MD, MPH March 24, 2011 Renuka Khurana, MD, MPH has the following disclosures to make: No conflict of interests
TB in Corrections Phoenix, Arizona March 24, 2011 Treatment of Latent TB Infection Renuka Khurana MD, MPH March 24, 2011 Renuka Khurana, MD, MPH has the following disclosures to make: No conflict of interests
LATENT TUBERCULOSIS. Robert F. Tyree, MD
 LATENT TUBERCULOSIS Robert F. Tyree, MD 1 YK TB OFFICERS Ron Bowerman Elizabeth Roll Mien Chyi (Pediatrics) Cindi Mondesir (Pediatrics) The new guys: Philip Johnson Robert Tyree 2009 CDC TB CASE DEFINITION
LATENT TUBERCULOSIS Robert F. Tyree, MD 1 YK TB OFFICERS Ron Bowerman Elizabeth Roll Mien Chyi (Pediatrics) Cindi Mondesir (Pediatrics) The new guys: Philip Johnson Robert Tyree 2009 CDC TB CASE DEFINITION
TB Intensive Houston, Texas. Childhood Tuberculosis Kim Connelly Smith. November 12, 2009
 TB Intensive Houston, Texas November 10-12, 12 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 1 OUTLINE Stages
TB Intensive Houston, Texas November 10-12, 12 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 1 OUTLINE Stages
Diagnosis and Medical Management of Latent TB Infection
 Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Tuberculosis and Diabetes Mellitus. Lana Kay Tyer, RN MSN WA State Department of Health TB Nurse Consultant
 Tuberculosis and Diabetes Mellitus Lana Kay Tyer, RN MSN WA State Department of Health TB Nurse Consultant Learning Objectives Understand the impact of uncontrolled diabetes mellitus (DM) on TB infection
Tuberculosis and Diabetes Mellitus Lana Kay Tyer, RN MSN WA State Department of Health TB Nurse Consultant Learning Objectives Understand the impact of uncontrolled diabetes mellitus (DM) on TB infection
DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE
 DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH Assistant Professor University of Texas Health Science Center Staff Physician, Texas Center for Infectious Diseases TB Nurse Case
DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH Assistant Professor University of Texas Health Science Center Staff Physician, Texas Center for Infectious Diseases TB Nurse Case
TB is Global. Latent TB Infection (LTBI) Sharing the Care: Working Together. September 24, 2014
 Sharing the Care: Working Together. September 24, 2014") Sharing the Care: Working Together to Meet the Challenge of TB Presented by: Barbara Cole, RN, PHN, MSN Director, Disease Control County of Riverside Department of Public Health Curry International TB
Sharing the Care: Working Together to Meet the Challenge of TB Presented by: Barbara Cole, RN, PHN, MSN Director, Disease Control County of Riverside Department of Public Health Curry International TB
ESCMID Online Lecture Library. by author
 Tuberculosis prevention in immunodepressed patients M. Carmen Fariñas Álvarez Infectious Diseases.H.U.Marqués de Valdecilla University of Cantabria, Spain DISCLOSURES I have no potential conflicts with
Tuberculosis prevention in immunodepressed patients M. Carmen Fariñas Álvarez Infectious Diseases.H.U.Marqués de Valdecilla University of Cantabria, Spain DISCLOSURES I have no potential conflicts with
Latent Tuberculosis Best Practices
 Latent Tuberculosis Best Practices Last Updated September 7, 2016 LTBI Demographics in the US o 13million people in the US with LTBI (estimate) o In 2014, approximately 66% of TB cases in the United States
Latent Tuberculosis Best Practices Last Updated September 7, 2016 LTBI Demographics in the US o 13million people in the US with LTBI (estimate) o In 2014, approximately 66% of TB cases in the United States
Chapter 5 Treatment for Latent Tuberculosis Infection
 Chapter 5 Treatment for Latent Tuberculosis Infection Table of Contents Chapter Objectives.... 109 Introduction.... 111 Candidates for the Treatment of LTBI... 112 LTBI Treatment Regimens.... 118 LTBI
Chapter 5 Treatment for Latent Tuberculosis Infection Table of Contents Chapter Objectives.... 109 Introduction.... 111 Candidates for the Treatment of LTBI... 112 LTBI Treatment Regimens.... 118 LTBI
Diagnosis and Treatment of Tuberculosis, 2011
 Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
What the Primary Physician Should Know about Tuberculosis. Topics for Discussion. Life Cycle of M. tuberculosis
 What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Microbiology Epidemiology Common disease presentations Diagnosis of active
What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Microbiology Epidemiology Common disease presentations Diagnosis of active
Diagnosis and Medical Management of TB Infection Lisa Y. Armitige, MD, PhD September 12, TB Nurse Case Management September 12 14, 2017
 Diagnosis and Medical Management of TB Infection Lisa Y. Armitige, MD, PhD September 12, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has
Diagnosis and Medical Management of TB Infection Lisa Y. Armitige, MD, PhD September 12, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has
TB: Management in an era of multiple drug resistance. Bob Belknap M.D. Denver Public Health November 2012
 TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
Communicable Disease Control Manual Chapter 4: Tuberculosis
 Provincial TB Services 655 West 12th Avenue Vancouver, BC V5Z 4R4 www.bccdc.ca Communicable Disease Control Manual Definitions Page 1 2.0 DEFINITIONS Many of the definitions that follow are taken from
Provincial TB Services 655 West 12th Avenue Vancouver, BC V5Z 4R4 www.bccdc.ca Communicable Disease Control Manual Definitions Page 1 2.0 DEFINITIONS Many of the definitions that follow are taken from
Isoniazid Preventive Therapy (IPT)
") Isoniazid Preventive Therapy (IPT) Josefina Cadorna-Carlos, M.D. Professor of Pediatrics U E R M M M C Objectives 1. Define IPT. 2. Discuss the indications for IPT. 3. Present RCT s for IPT (6H vs 9H).
Isoniazid Preventive Therapy (IPT) Josefina Cadorna-Carlos, M.D. Professor of Pediatrics U E R M M M C Objectives 1. Define IPT. 2. Discuss the indications for IPT. 3. Present RCT s for IPT (6H vs 9H).
Contact Investigation
 Tuberculosis Ann Raftery, RN, PHN, MSc GHS Learning Objectives Upon completion of this session, participants will be able to: Describe the criteria used and method for determining the infectious period
Tuberculosis Ann Raftery, RN, PHN, MSc GHS Learning Objectives Upon completion of this session, participants will be able to: Describe the criteria used and method for determining the infectious period
Tuberculosis Update. Topics to be Addressed
 Tuberculosis Update Robert M. Jasmer, M.D. University of California, San Francisco TB Control Section, San Francisco Department of Public Health Topics to be Addressed TB in the USA Screening recommendations
Tuberculosis Update Robert M. Jasmer, M.D. University of California, San Francisco TB Control Section, San Francisco Department of Public Health Topics to be Addressed TB in the USA Screening recommendations
has the following disclosures to make:
 CLINICAL DIAGNOSIS AND MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH September 22, 2015 TB Nurse Case Management September 22 24, 2015 San Antonio. TX EXCELLENCE EXPERTISE INNOVATION Annie Kizilbash
CLINICAL DIAGNOSIS AND MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH September 22, 2015 TB Nurse Case Management September 22 24, 2015 San Antonio. TX EXCELLENCE EXPERTISE INNOVATION Annie Kizilbash
Interferon Gamma Release Assay Testing for Latent Tuberculosis Infection: Physician Guidelines
 Interferon Gamma Release Assay Testing for Latent Tuberculosis Infection: Physician Guidelines Historically, Latent Tuberculosis Infection (LTBI) diagnosis was based on risk assessment, chest x-ray (CXR)
Interferon Gamma Release Assay Testing for Latent Tuberculosis Infection: Physician Guidelines Historically, Latent Tuberculosis Infection (LTBI) diagnosis was based on risk assessment, chest x-ray (CXR)
Tuberculosis (TB) Fundamentals for School Nurses
 Fundamentals for School Nurses") Tuberculosis (TB) Fundamentals for School Nurses June 9, 2015 Kristin Gall, RN, MSN/Pat Infield, RN-TB Program Manager Marsha Carlson, RN, BSN Two Rivers Public Health Department Nebraska Department of
Tuberculosis (TB) Fundamentals for School Nurses June 9, 2015 Kristin Gall, RN, MSN/Pat Infield, RN-TB Program Manager Marsha Carlson, RN, BSN Two Rivers Public Health Department Nebraska Department of
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016
 Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
What the Primary Physician Should Know about Tuberculosis. Topics for Discussion. Global Impact of TB
 What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Common disease presentations Diagnosis of active TB Screening
What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Common disease presentations Diagnosis of active TB Screening
Latent TB Infection (LTBI) Strategies for Detection and Management
 Strategies for Detection and Management") Latent TB Infection (LTBI) Strategies for Detection and Management Patrick T. Dowling MD,MPH Professor and Chair Dept of Family Medicine David Geffen School of Medicine at UCLA Pri-Med March 29 2014 Pdowling@mednet.ucla.edu
Latent TB Infection (LTBI) Strategies for Detection and Management Patrick T. Dowling MD,MPH Professor and Chair Dept of Family Medicine David Geffen School of Medicine at UCLA Pri-Med March 29 2014 Pdowling@mednet.ucla.edu
Let s Talk TB A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year
 A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Madhukar Pai, MD, PhD Author and Series Editor Camilla Rodrigues, MD co-author Abstract Most individuals who get exposed
A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Madhukar Pai, MD, PhD Author and Series Editor Camilla Rodrigues, MD co-author Abstract Most individuals who get exposed
Pediatric TB Basics and Evaluation and Management of Exposed Neonates
 Pediatric TB Basics and Evaluation and Management of Exposed Neonates Ann M. Loeffler, MD Randall Children s Hospital, Portland OR & Curry International TB Center, Oakland CA September, 2017 No Disclosures
Pediatric TB Basics and Evaluation and Management of Exposed Neonates Ann M. Loeffler, MD Randall Children s Hospital, Portland OR & Curry International TB Center, Oakland CA September, 2017 No Disclosures
At the end of this session, participants will be able to:
 Advanced Concepts in Pediatric Tuberculosis: Infection Control, Source Case and Contact Investigation Ana M. Alvarez, M.D. Associate Professor Division of Pediatric Infectious Diseases and Immunology University
Advanced Concepts in Pediatric Tuberculosis: Infection Control, Source Case and Contact Investigation Ana M. Alvarez, M.D. Associate Professor Division of Pediatric Infectious Diseases and Immunology University
Approaches to LTBI Diagnosis
 Approaches to LTBI Diagnosis Focus on LTBI October 8 th, 2018 Michelle Haas, M.D. Associate Director Denver Metro Tuberculosis Program Denver Public Health DISCLOSURES I have no disclosures or conflicts
Approaches to LTBI Diagnosis Focus on LTBI October 8 th, 2018 Michelle Haas, M.D. Associate Director Denver Metro Tuberculosis Program Denver Public Health DISCLOSURES I have no disclosures or conflicts
Screening and Treatment Recommendations for Persons Exposed to MDR TB
 Screening and Treatment Recommendations for Persons Exposed to MDR TB Although all persons at increased risk of tuberculosis (TB) infection should be screened for TB infection per USPTF/CDC guidelines
Screening and Treatment Recommendations for Persons Exposed to MDR TB Although all persons at increased risk of tuberculosis (TB) infection should be screened for TB infection per USPTF/CDC guidelines
10/3/2017. Updates in Tuberculosis. Global Tuberculosis, WHO 2015 report. Objectives. Disclosures. I have nothing to disclose
 Disclosures Updates in Tuberculosis I have nothing to disclose Chris Keh, MD Assistant Clinical Professor, Division of Infectious Diseases, UCSF TB Controller, TB Prevention and Control Program, Population
Disclosures Updates in Tuberculosis I have nothing to disclose Chris Keh, MD Assistant Clinical Professor, Division of Infectious Diseases, UCSF TB Controller, TB Prevention and Control Program, Population
LTBI Videos-Treatment
 LTBI Videos-Treatment This program is presented by the Global Tuberculosis Institute and is based on recommendations from the Centers for Disease Control and Prevention. This is the third in a series of
LTBI Videos-Treatment This program is presented by the Global Tuberculosis Institute and is based on recommendations from the Centers for Disease Control and Prevention. This is the third in a series of
Didactic Series. Latent TB Infection in HIV Infection
 Didactic Series Latent TB Infection in HIV Infection Jacqueline Peterson Tulsky, MD UCSF Positive Health Program at SFGH Medical Director, SF and North Coast AETC March 13, 2014 ACCREDITATION STATEMENT:
Didactic Series Latent TB Infection in HIV Infection Jacqueline Peterson Tulsky, MD UCSF Positive Health Program at SFGH Medical Director, SF and North Coast AETC March 13, 2014 ACCREDITATION STATEMENT:
Barbara J Seaworth MD Medical Director, Heartland National TB Center Professor, Internal Medicine and Infectious Disease UT Health Northeast
 Practical Aspects for Using the Interferon Gamma Release Assay (IGRA) Test Live Webinar July 14, 2017 Barbara J Seaworth MD Medical Director, Heartland National TB Center Professor, Internal Medicine and
Practical Aspects for Using the Interferon Gamma Release Assay (IGRA) Test Live Webinar July 14, 2017 Barbara J Seaworth MD Medical Director, Heartland National TB Center Professor, Internal Medicine and
TB Prevention Who and How to Screen
 TB Prevention Who and How to Screen 4.8.07. IUATLD 1st Asia Pacific Region Conference 2007 Dr Cynthia Chee Dept of Respiratory Medicine / TB Control Unit Tan Tock Seng Hospital, Singapore Cycle of Infection
TB Prevention Who and How to Screen 4.8.07. IUATLD 1st Asia Pacific Region Conference 2007 Dr Cynthia Chee Dept of Respiratory Medicine / TB Control Unit Tan Tock Seng Hospital, Singapore Cycle of Infection
Tuberculosis: A Provider s Guide to
 Tuberculosis: A Provider s Guide to Diagnosis and Treatment of Active Tuberculosis (TB) Disease and Screening and Treatment of Latent Tuberculosis Infection (LTBI) Alameda County Health Care Services Agency
Tuberculosis: A Provider s Guide to Diagnosis and Treatment of Active Tuberculosis (TB) Disease and Screening and Treatment of Latent Tuberculosis Infection (LTBI) Alameda County Health Care Services Agency
Errors in Dx and Rx of TB
 Errors in Dx and Rx of TB David Schlossberg, MD, FACP Professor of Medicine Temple University School of Medicine Medical Director, TB Control Program Philadelphia Department of Public Health TB Still a
Errors in Dx and Rx of TB David Schlossberg, MD, FACP Professor of Medicine Temple University School of Medicine Medical Director, TB Control Program Philadelphia Department of Public Health TB Still a
Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis
 Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Diagnosis of active TB Screening
Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Diagnosis of active TB Screening
Diagnosis and Management of Latent TB Infection Douglas Hornick, MD September 27, 2011
 TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Diagnosis and Management of Latent TB Infection Douglas Hornick, MD September 27, 2011 Douglas Hornick, MD has the following disclosures to
TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Diagnosis and Management of Latent TB Infection Douglas Hornick, MD September 27, 2011 Douglas Hornick, MD has the following disclosures to
LATENT TUBERCULOSIS SCREENING AND TREATMENT:
 LATENT TUBERCULOSIS SCREENING AND TREATMENT: TB or not TB Christopher Kwong, MD and William Rifkin, MD Week 14 Educational Objectives: 1. Understand who should be screened for latent TB infection and why
LATENT TUBERCULOSIS SCREENING AND TREATMENT: TB or not TB Christopher Kwong, MD and William Rifkin, MD Week 14 Educational Objectives: 1. Understand who should be screened for latent TB infection and why
Latent Tuberculosis Infection Reporting Instructions for Civil Surgeons Using CalREDIE Provider Portal
 Latent Tuberculosis Infection Reporting Instructions for Civil Surgeons Using CalREDIE Provider Portal Civil surgeons are required to report tuberculosis (TB) screening outcomes that result in latent TB
Latent Tuberculosis Infection Reporting Instructions for Civil Surgeons Using CalREDIE Provider Portal Civil surgeons are required to report tuberculosis (TB) screening outcomes that result in latent TB
TB In Detroit 2011* Early TB: Smudge Sign. Who is at risk for exposure to or infection with TB? Who is at risk for TB after exposure or infection?
 Those oral antibiotics are just not working! Inpatient Standards of Care & Discharge Planning S/He s in the Hospital: Now What Do I Do? Dana G. Kissner, MD TB Intensive Workshop, Lansing, MI 2012 Objectives:
Those oral antibiotics are just not working! Inpatient Standards of Care & Discharge Planning S/He s in the Hospital: Now What Do I Do? Dana G. Kissner, MD TB Intensive Workshop, Lansing, MI 2012 Objectives:
Latent TB, TB and the Role of the Health Department
 Latent TB, TB and the Role of the Health Department Elaine Darnall, RN, BSN, CIC TB Nurse Consultant Illinois Dept of Public Health March 21, 2018 Elaine Darnall has disclosed that there is no actual or
Latent TB, TB and the Role of the Health Department Elaine Darnall, RN, BSN, CIC TB Nurse Consultant Illinois Dept of Public Health March 21, 2018 Elaine Darnall has disclosed that there is no actual or
Latent TB Infection Treatment
 Latent TB Infection Treatment Douglas B. Hornick, MD Pulmonologist w/ Infectious Attitude Division of Pulmonary/Critical Care/Occ Med UI Carver College of Medicine 2014 MFMER slide-1 Disclosures: None
Latent TB Infection Treatment Douglas B. Hornick, MD Pulmonologist w/ Infectious Attitude Division of Pulmonary/Critical Care/Occ Med UI Carver College of Medicine 2014 MFMER slide-1 Disclosures: None
Targeted Testing and the Diagnosis of. Latent Tuberculosis. Infection and Tuberculosis Disease
 Self-Study Study Modules on Tuberculosis Targeted Testing and the Diagnosis of Latent Tuberculosis Infection and Tuberculosis Disease 1 Module 3: Objectives At completion of this module, learners will
Self-Study Study Modules on Tuberculosis Targeted Testing and the Diagnosis of Latent Tuberculosis Infection and Tuberculosis Disease 1 Module 3: Objectives At completion of this module, learners will
Advanced Management of Patients with Tuberculosis Little Rock, Arkansas August 13 14, 2014
 Advanced Management of Patients with Tuberculosis Little Rock, Arkansas August 13 14, 2014 Tuberculosis Pathogenesis and Treatment of Latent TB Infection Lisa Armitige, MD, PhD August 13, 2014 Lisa Armitige,
Advanced Management of Patients with Tuberculosis Little Rock, Arkansas August 13 14, 2014 Tuberculosis Pathogenesis and Treatment of Latent TB Infection Lisa Armitige, MD, PhD August 13, 2014 Lisa Armitige,
Latent Tuberculosis in Adults: From Testing TO Treatment
 Latent Tuberculosis in Adults: From Testing TO Treatment Sergio M. Borgia, MD, MSc., FRCP(C) Infectious Diseases Consultant, WOHS Medical Director, WOHS Tuberculosis Clinic Assistant Clinical Professor,
Latent Tuberculosis in Adults: From Testing TO Treatment Sergio M. Borgia, MD, MSc., FRCP(C) Infectious Diseases Consultant, WOHS Medical Director, WOHS Tuberculosis Clinic Assistant Clinical Professor,
Latent tuberculosis infection
 EXECUTIVE SUMMARY Latent tuberculosis infection Updated and consolidated guidelines for programmatic management Executive summary Latent tuberculosis infection (LTBI) is defined as a state of persistent
EXECUTIVE SUMMARY Latent tuberculosis infection Updated and consolidated guidelines for programmatic management Executive summary Latent tuberculosis infection (LTBI) is defined as a state of persistent
What you need to know about diagnosing and treating TB: a preventable, fatal disease. Bob Belknap M.D. Denver Public Health November 2014
 What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2014 The Critical First Step Consider TB in the Differential 1. Risks
What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2014 The Critical First Step Consider TB in the Differential 1. Risks
Tuberculosis Elimination: The Role of the Infection Preventionist
 Tuberculosis Elimination: The Role of the Infection Preventionist Preface: What Happens when Health Care Professionals are not familiar with TB? A 15 year old student was diagnosed with highly infectious
Tuberculosis Elimination: The Role of the Infection Preventionist Preface: What Happens when Health Care Professionals are not familiar with TB? A 15 year old student was diagnosed with highly infectious
TB Intensive San Antonio, Texas August 7-10, 2012
 TB Intensive San Antonio, Texas August 7-10, 2012 An Introduction to Childhood Tuberculosis Kim Smith, MD, MPH August 10, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests
TB Intensive San Antonio, Texas August 7-10, 2012 An Introduction to Childhood Tuberculosis Kim Smith, MD, MPH August 10, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests
Diagnosis & Medical Case Management of TB Disease. Lisa Armitige, MD, PhD October 22, 2015
 Diagnosis & Medical Case Management of TB Disease Lisa Armitige, MD, PhD October 22, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
Diagnosis & Medical Case Management of TB Disease Lisa Armitige, MD, PhD October 22, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
Disclosures. Updates in TB for the PCP: Opportunities for Prevention. Objectives PART 1: WHY TEST? 4/14/2016. None
 Disclosures Updates in TB for the PCP: Opportunities for Prevention None Pennan Barry, MD, MPH Chief, Surveillance and Epidemiology, California TB Control Branch Assistant Clinical Professor, Division
Disclosures Updates in TB for the PCP: Opportunities for Prevention None Pennan Barry, MD, MPH Chief, Surveillance and Epidemiology, California TB Control Branch Assistant Clinical Professor, Division
11/1/2017. Disclosures. Update In Tuberculosis, Indiana Outline/Objectives. Pathogenesis of M.tb Global/U.S. TB Burden, 2016
 Disclosures Update In Tuberculosis, Indiana 2017 Bradley Allen, MD, PhD, FACP, FIDSA Indiana University School of Medicine Division of Infectious Diseases Roudebush VAMC Indianapolis Medical Consultant,
Disclosures Update In Tuberculosis, Indiana 2017 Bradley Allen, MD, PhD, FACP, FIDSA Indiana University School of Medicine Division of Infectious Diseases Roudebush VAMC Indianapolis Medical Consultant,
Tuberculosis. Impact of TB. Infectious Disease Epidemiology BMTRY 713 (A. Selassie, DrPH)
") Infectious Disease Epidemiology BMTRY 713 (A. Selassie, DrPH) Lecture 20 Tuberculosis Learning Objectives 1. Describe the biologic characteristics of the agent 2. Determine the epidemiologic characteristics
Infectious Disease Epidemiology BMTRY 713 (A. Selassie, DrPH) Lecture 20 Tuberculosis Learning Objectives 1. Describe the biologic characteristics of the agent 2. Determine the epidemiologic characteristics
Northwestern Polytechnic University
 Clinical Tuberculosis Assessment by Health Care Provider Clinicians should review and verify the information in the Tuberculosis (TB) Screening Questionnaire (attached). Persons answering YES to any questions
Clinical Tuberculosis Assessment by Health Care Provider Clinicians should review and verify the information in the Tuberculosis (TB) Screening Questionnaire (attached). Persons answering YES to any questions
TUBERCULOSIS IN HEALTHCARE SETTINGS Diana M. Nilsen, MD, FCCP Director of Medical Affairs, Bureau of Tuberculosis Control New York City Department of
 TUBERCULOSIS IN HEALTHCARE SETTINGS Diana M. Nilsen, MD, FCCP Director of Medical Affairs, Bureau of Tuberculosis Control New York City Department of Health and Mental Hygiene TODAY S PRESENTATION Epidemiology
TUBERCULOSIS IN HEALTHCARE SETTINGS Diana M. Nilsen, MD, FCCP Director of Medical Affairs, Bureau of Tuberculosis Control New York City Department of Health and Mental Hygiene TODAY S PRESENTATION Epidemiology
TUBERCULOSIS CONTACT INVESTIGATION
 TB CASE MANAGEMENT AND CONTACT INVESTIGATION INTENSIVE TUBERCULOSIS CONTACT INVESTIGATION LEARNING OBJECTIVES Upon completion of this session, participants will be able to: 1. Describe the criteria used
TB CASE MANAGEMENT AND CONTACT INVESTIGATION INTENSIVE TUBERCULOSIS CONTACT INVESTIGATION LEARNING OBJECTIVES Upon completion of this session, participants will be able to: 1. Describe the criteria used
Targeted Tuberculin Testing and Treatment of Latent Tuberculosis Infection (LTBI) Lloyd Friedman, M.D. Milford Hospital Yale University
 Lloyd Friedman, M.D. Milford Hospital Yale University") Targeted Tuberculin Testing and Treatment of Latent Tuberculosis Infection (LTBI) Lloyd Friedman, M.D. Milford Hospital Yale University Tuberculosis Estimates USA World Infection 15,000,000 2,000,000,000
Targeted Tuberculin Testing and Treatment of Latent Tuberculosis Infection (LTBI) Lloyd Friedman, M.D. Milford Hospital Yale University Tuberculosis Estimates USA World Infection 15,000,000 2,000,000,000
Michael J. Huey, MD. NYSCHA Annual Meeting WE-2, October 19, 2016
 Michael J. Huey, MD Assistant Vice President and Executive Director Emory University Student Health Services Associate Professor, Family and Preventive Medicine Emory University School of Medicine President-elect
Michael J. Huey, MD Assistant Vice President and Executive Director Emory University Student Health Services Associate Professor, Family and Preventive Medicine Emory University School of Medicine President-elect
Diagnosis & Management of Latent TB Infection
 Diagnosis & Management of Latent TB Infection Prof. Ashok Rattan, MD, MAMS, INSA DFG, WHO Lab Director Academics, Industry: Research, Diagnosis, Public Health, Academics Adviser: Laboratory Operations,
Diagnosis & Management of Latent TB Infection Prof. Ashok Rattan, MD, MAMS, INSA DFG, WHO Lab Director Academics, Industry: Research, Diagnosis, Public Health, Academics Adviser: Laboratory Operations,
Diagnosis and Medical Management of TB Disease. Quratulian Annie Kizilbash, MD, MPH March 17, 2015
 Diagnosis and Medical Management of TB Disease Quratulian Annie Kizilbash, MD, MPH March 17, 2015 TB Nurse Case Management March 17 19, 2015 San Antonio, Texas EXCELLENCE EXPERTISE INNOVATION Quratulian
Diagnosis and Medical Management of TB Disease Quratulian Annie Kizilbash, MD, MPH March 17, 2015 TB Nurse Case Management March 17 19, 2015 San Antonio, Texas EXCELLENCE EXPERTISE INNOVATION Quratulian
Tuberculosis Screening Protocol For Use In Marin County School Settings
 Tuberculosis Screening Protocol For Use In Marin County School Settings New Student no known history of positive skin test Kindergarten or First Grade entry (whichever comes first) All students, countywide,
Tuberculosis Screening Protocol For Use In Marin County School Settings New Student no known history of positive skin test Kindergarten or First Grade entry (whichever comes first) All students, countywide,
Interpretation of TST & IGRA results. Objectives
 Interpretation of TST & IGRA results Randall Reves, MD, MSc Volunteer Clinician Denver Metro TB Program and Division of Infectious Diseases, Department of Medicine University of Colorado Denver Objectives
Interpretation of TST & IGRA results Randall Reves, MD, MSc Volunteer Clinician Denver Metro TB Program and Division of Infectious Diseases, Department of Medicine University of Colorado Denver Objectives
LTBI: Who to Test & When to Treat
 LTBI: Who to Test & When to Treat TB Intensive May 10 th, 2016 David Horne, MD, MPH Harborview Medical Center University of Washington DISCLOSURES I have no disclosures or conflicts of interest to report
LTBI: Who to Test & When to Treat TB Intensive May 10 th, 2016 David Horne, MD, MPH Harborview Medical Center University of Washington DISCLOSURES I have no disclosures or conflicts of interest to report
Core Curriculum on Tuberculosis: What the Clinician Should Know
 Core Curriculum on Tuberculosis: What the Clinician Should Know Sixth Edition 2013 National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention Division of Tuberculosis Elimination 1 Chapters
Core Curriculum on Tuberculosis: What the Clinician Should Know Sixth Edition 2013 National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention Division of Tuberculosis Elimination 1 Chapters
PEDIATRIC TUBERCULOSIS. Objectives. Children are not just small adults. Pediatric Tuberculosis 1
 PEDIATRIC TUBERCULOSIS Ann M. Loeffler, M.D. Faculty Consultant Curry International Tuberculosis Center Objectives At the end of this session, participants will be able to describe: how pediatric patients
PEDIATRIC TUBERCULOSIS Ann M. Loeffler, M.D. Faculty Consultant Curry International Tuberculosis Center Objectives At the end of this session, participants will be able to describe: how pediatric patients
Santa Clara County Tuberculosis Screening Requirement for School Entrance Effective June 1, 2014
 Guidelines to Revisions to the School Mandate and Requirements 1) What are the tuberculosis (TB) screening requirements for school entrance in Santa Clara County? Students must undergo a TB risk assessment
Guidelines to Revisions to the School Mandate and Requirements 1) What are the tuberculosis (TB) screening requirements for school entrance in Santa Clara County? Students must undergo a TB risk assessment
PEDIATRIC TUBERCULOSIS
 PEDIATRIC TUBERCULOSIS Ann M. Loeffler, M.D. Faculty Consultant Curry International Tuberculosis Center Objectives At the end of this session, participants will be able to describe: how pediatric patients
PEDIATRIC TUBERCULOSIS Ann M. Loeffler, M.D. Faculty Consultant Curry International Tuberculosis Center Objectives At the end of this session, participants will be able to describe: how pediatric patients
HEALTH SERVICES POLICY & PROCEDURE MANUAL
 PAGE 1 of 7 References Related ACA Standards 4 th Edition Standards for Adult Correctional Institutions 4-4350, 4-4355 These guidelines are based on the recommendations of the American Thoracic Society
PAGE 1 of 7 References Related ACA Standards 4 th Edition Standards for Adult Correctional Institutions 4-4350, 4-4355 These guidelines are based on the recommendations of the American Thoracic Society
TUBERCULOSIS. Pathogenesis and Transmission
 TUBERCULOSIS Pathogenesis and Transmission TUBERCULOSIS Pathogenesis and Transmission Infection to Disease Diagnostic & Isolation Updates Treatment Updates Pathogenesis Droplet nuclei of 5µm or less are
TUBERCULOSIS Pathogenesis and Transmission TUBERCULOSIS Pathogenesis and Transmission Infection to Disease Diagnostic & Isolation Updates Treatment Updates Pathogenesis Droplet nuclei of 5µm or less are
TB Contact Investigation
 Ann Raftery, RN, PHN, MS Curry International TB Center Overview Contact investigation as a core TB control and elimination activity Components of TB Contact Investigation TB Control Priority Strategies.
Ann Raftery, RN, PHN, MS Curry International TB Center Overview Contact investigation as a core TB control and elimination activity Components of TB Contact Investigation TB Control Priority Strategies.
Tuberculosis Education for the Medical Professional
 Tuberculosis Education for the Medical Professional North Dakota Diagnosis and Medical Management of Latent TB Infection Dawn Farrell, RN, BSN, PHN Maria Robles, BSN July 10, 2007 Tuberculosis Education
Tuberculosis Education for the Medical Professional North Dakota Diagnosis and Medical Management of Latent TB Infection Dawn Farrell, RN, BSN, PHN Maria Robles, BSN July 10, 2007 Tuberculosis Education
Evaluation and Treatment of TB Contacts Tyler, Texas April 11, 2014
 Evaluation and Treatment of TB Contacts Tyler, Texas April 11, 2014 Interferon Gamma Release Assays: Understanding the Test David Griffith, BA, MD April 11, 2014 David Griffith, BA, MD has the following
Evaluation and Treatment of TB Contacts Tyler, Texas April 11, 2014 Interferon Gamma Release Assays: Understanding the Test David Griffith, BA, MD April 11, 2014 David Griffith, BA, MD has the following
Case 1: Clinical Presentation
 Impostors and Preconceived Notions: Lessons Learned in TB Diagnosis & Treatment Tuberculosis Nursing Workshop June 1, 2015 Christopher Spitters, MD, MPH Tuberculosis Clinic Public Health Seattle & King
Impostors and Preconceived Notions: Lessons Learned in TB Diagnosis & Treatment Tuberculosis Nursing Workshop June 1, 2015 Christopher Spitters, MD, MPH Tuberculosis Clinic Public Health Seattle & King
2017/2018 Annual Volunteer Tuberculosis Notice
 Lewis Center for Educational Research Academy for Academic Excellence Norton Science and Language Academy Business Offices 17500 Mana Road Apple Valley, CA 92307 E-mail: hr@lcer.org 760-946-5414 Fax 760-946-9193
Lewis Center for Educational Research Academy for Academic Excellence Norton Science and Language Academy Business Offices 17500 Mana Road Apple Valley, CA 92307 E-mail: hr@lcer.org 760-946-5414 Fax 760-946-9193
TB & HIV CO-INFECTION IN CHILDREN. Reené Naidoo Paediatric Infectious Diseases Broadreach Healthcare 19 April 2012
 TB & HIV CO-INFECTION IN CHILDREN Reené Naidoo Paediatric Infectious Diseases Broadreach Healthcare 19 April 2012 Introduction TB & HIV are two of the leading causes of morbidity & mortality in children
TB & HIV CO-INFECTION IN CHILDREN Reené Naidoo Paediatric Infectious Diseases Broadreach Healthcare 19 April 2012 Introduction TB & HIV are two of the leading causes of morbidity & mortality in children
TB the basics. (Dr) Margaret (DHA) and John (INZ)
 Margaret (DHA) and John (INZ)") TB the basics (Dr) Margaret (DHA) and John (INZ) Question 1 The scientist who discovered M. tuberculosis was: A: Louis Pasteur B: Robert Koch C: Jean-Antoine Villemin D: Calmette and Guerin Question 2
TB the basics (Dr) Margaret (DHA) and John (INZ) Question 1 The scientist who discovered M. tuberculosis was: A: Louis Pasteur B: Robert Koch C: Jean-Antoine Villemin D: Calmette and Guerin Question 2
LTBI in Special Populations John Nava, MD October 5, 2010
 Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 LTBI in Special Populations John Nava, MD October 5, 2010 2 Treatment of Latent TB Infection in Special Populations John
Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 LTBI in Special Populations John Nava, MD October 5, 2010 2 Treatment of Latent TB Infection in Special Populations John
Didactic Series. Latent TB Infection in HIV Infection
 Didactic Series Latent TB Infection in HIV Infection Jacqueline Peterson Tulsky, MD UCSF Positive Health Program at SFGH Medical Director SF, North Coast and East Bay AETC January 8, 2015 ACCREDITATION
Didactic Series Latent TB Infection in HIV Infection Jacqueline Peterson Tulsky, MD UCSF Positive Health Program at SFGH Medical Director SF, North Coast and East Bay AETC January 8, 2015 ACCREDITATION
Contact Follow-Up and Treatment of LTBI in Households of Infectious Cases in Pakistan
 Contact Follow-Up and Treatment of LTBI in Households of Infectious Cases in Pakistan 17 th Annual Conference, The Union-North American Region, Vancouver, Canada. 28 February 2013 Farhana Amanullah Director
Contact Follow-Up and Treatment of LTBI in Households of Infectious Cases in Pakistan 17 th Annual Conference, The Union-North American Region, Vancouver, Canada. 28 February 2013 Farhana Amanullah Director