Pediatric Tuberculosis
|
|
|
- Stephen Bridges
- 5 years ago
- Views:
Transcription

1 Pediatric Tuberculosis Kim Connelly Smith, MD, MPH April 7, 2016 TB Intensive April 5 8, 2016 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant financial relationships with any commercial companies pertaining to this educational activity 1


2 PEDIATRIC TUBERCULOSIS Kim Connelly Smith, MD, MPH OUTLINE Stages of tuberculosis Differences of disease in children and adults Diagnostic challenges of pediatric TB Treatment of TB in children Clinical cases 2
3 STAGES OF TUBERCULOSIS Exposure to Contagious Adult with Pulmonary Disease Household contacts 20-30% Latent TB Infection LTBI 5-10% Adult Active TB Disease Risk varies by age 5-50% Child Active TB Disease RISK OF DISEASE WITH NO TREATMENT BY AGE INFECTED OR MEDICAL CONDITION 60% 50% 50% 50% 40% 30% 30% 20% 24% 10% 15% 0% Birth-12 months 5% 7% 1-3 years 4-11 years years Healthy Adults Diabetes HIV Infected 3
4 RISK OF PROGRESSION TO TB DISEASE BY AGE primary infection Birth-12months Risk of Disease Disease 50% Pulmonary Dis 30-40% Miliary or TBM 10-20% 1-2 years Disease 20-25% Pulmonary Dis 75% Miliary or TBM 2-5% Marais BJ. Int J Tuberc Lung Dis 2004;8: Stages of TB Exposure Child < 4 years of age Household contact with adult with active pulmonary disease TREATMENT OF TUBERCULOSIS IN CHILDREN Skin Test or CXR SXs Treatment IGRA TST Negative Normal None Meds: INH or Rif window prophylaxis Duration: 8-10 weeks Repeat skin test: 8-10 wks after exp if positive > 5mm, see LTBI Latent TB infection (LTBI) Positive Normal None Treatment Options: INH x 9 months or RIF x 4-6 months or 3HP wkly x 12 wks, DOT only Disease Pulmonary and extrapulmonary (except disseminated disease and meningitis, see below) Disease Disseminated including miliary, bone/joint and multi-site disease 90% positive Abnormal +/- 50% of children with no symptoms TST may be negative early in disseminated TB, 90% positive by end of treatment Meds: INH, RIF, PZA, EMB (or an aminoglycoside) Duration: 6 mo total, Stop PZA after 2 mo, continue INH & RIF for susceptible disease +/- Yes Meds: INH, RIF, PZA and EMB or an aminoglycoside Duration: 9-12 mo total Stop PZA and EMB or aminoglycoside after 2 mo for susceptible disease Disease Meningitis Often negative early in meningitis and miliary disease 90% positive by end of tx +/- Yes Meds: INH, RIF, PZA and Ethionamide, or an aminoglycoside or EMB daily for 2 mo, then INH and RIF for 7-10 mo Duration: 9-12 mo total for drug susceptible disease Steroids recommended for first 1-2 months for meningitis 4

5 STAGES OF TB IN CHILDREN Stages of TB TST/IGRA CXR/Lab Physical Symptoms Treatment Exposure Child <4yrs (adult source) Negative Normal None Window CPX INH or Rif 8-10 wks Repeat TST 8-10 wks after last contact LTBI Positive Normal None INH x 9 mo or Rif x 4-6 mo or 3HP wkly x 12 wks, DOT only Disease 90% Positive 50% false neg with miliary and TBM Abnormal CXR, PE or labs 50% of children have symptoms RIPE x 6-12 months, duration depends on site Daycare Exposure 5
6 DAYCARE EXPOSURE Index case, teacher assistant with AFB smear positive pulmonary disease and cough for 6 weeks 135 children < 4 years of age, plus adult staff members exposed Smith, KC. Southern Medical Journal 93(9): , 2000 DAYCARE EXPOSURE MANAGEMENT o Who needs TST? o Everyone with significant contact with source case o Who needs CXR? o All children less than 4 years of age even if TST negative o Any contacts with positive TST (> 5mm) o Who needs treatment? o LTBI (positive TST >5mm and normal CXR) INH for 9 months or Rif x 4-6 months o Exposed children less than 4 years of age (window prophylaxis) o Follow up: o Skin test conversions: 4 adults and 3 children 6
 CXR and physical exam normal INH or Rifampin prophylaxis")

7 WINDOW PROPHYLAXIS FOR EXPOSURE Household contact with contagious person Teen or adult with pulmonary TB disease Usually > 4 hours of contact Initial TST negative Window period for TST conversion (8-10 weeks) CXR and physical exam normal INH or Rifampin prophylaxis recommended: For children <4 yrs of age Immunosuppressed patients May prevent progression to disease during window period Repeat TST 8-10 wks after exposure May stop CPX if 2 nd TST negative <5mm in immunocompetent patients Timetable of T Tuberculosis *Feigin & Cherry, Text of Pedi ID 7


8 PREVENTABLE CASE PREVENTABLE CASE 6 month old hospitalized March week history of fever (Tmax 101), vomiting and diarrhea, daily cold sweats CXR with miliary infiltrates Developed respiratory failure, seizure and AMS Family history Father, uncle and mother with history of incarceration Father hospitalized 7 weeks prior with cavitary pneumonia, AFB smears negative, no TB treatment Sputum cultures grew TB at 4 weeks but Health Department unable to locate family 8
, 46%L, Protein 130 (<40) Complications SIADH, hyponatremia, seizures Hydrocephalus, VP shunt and developmental delay OUTCOME")

9 HOSPITAL COURSE Respiratory failure, intubation Deterioration, AMS and focal neurologic exam MRI brain Acute hydrocephalus, leptomeningeal enhancement, diffuse nodular parenchymal enhancements CSF RBC 300, WBC46 (<7), 46%L, Protein 130 (<40) Complications SIADH, hyponatremia, seizures Hydrocephalus, VP shunt and developmental delay OUTCOME All family members tested positive for TB Patient grew TB from tracheal aspirate Neurologic: hydrocephalus, VP shunt, seizure disorder, developmental delay How could this have been prevented? Report to HD and start treatment when TB suspected (cavitary pneumonia) Timely Contact Investigation when suspect reported Window prophylaxis for children < 4 years 9
10 TB MENINGITIS Youssef FG, et al. Diagn Microbiol Infect Dis 2006;55(4):275-8 TB MENINGITIS TREATMENT AND CLINICAL COURSE 9-12 months RIPE therapy Steroids for 1-2 month with 2-3 week taper decreases CNS inflammation Fever common for first month, symptoms may initially worsen followed by gradual improvement Possible complications Seizures Hydrocephalus CNS tuberculoma, stroke, mental disabilities, CP Mortality high (>90%) if not diagnosed and treated 10
 Usually symptomatic and contagious")
11 DIFFERENCES IN ADULT AND PEDIATRIC TB REACTIVATION DISEASE Occurs years after primary infection Typical of adult disease Occasionally seen in teens Often cavitary disease High numbers of organisms (AFB +) Usually symptomatic and contagious 11

")
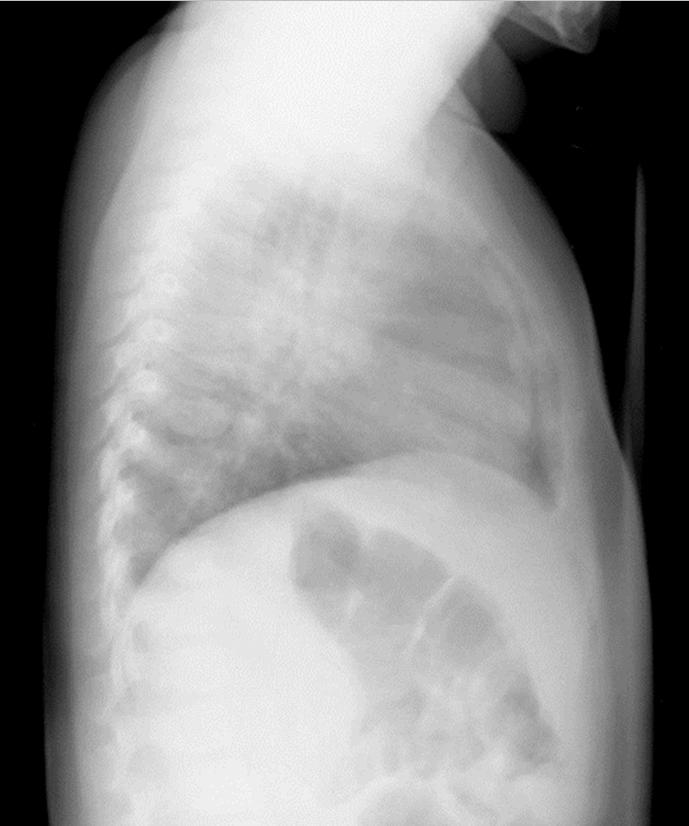
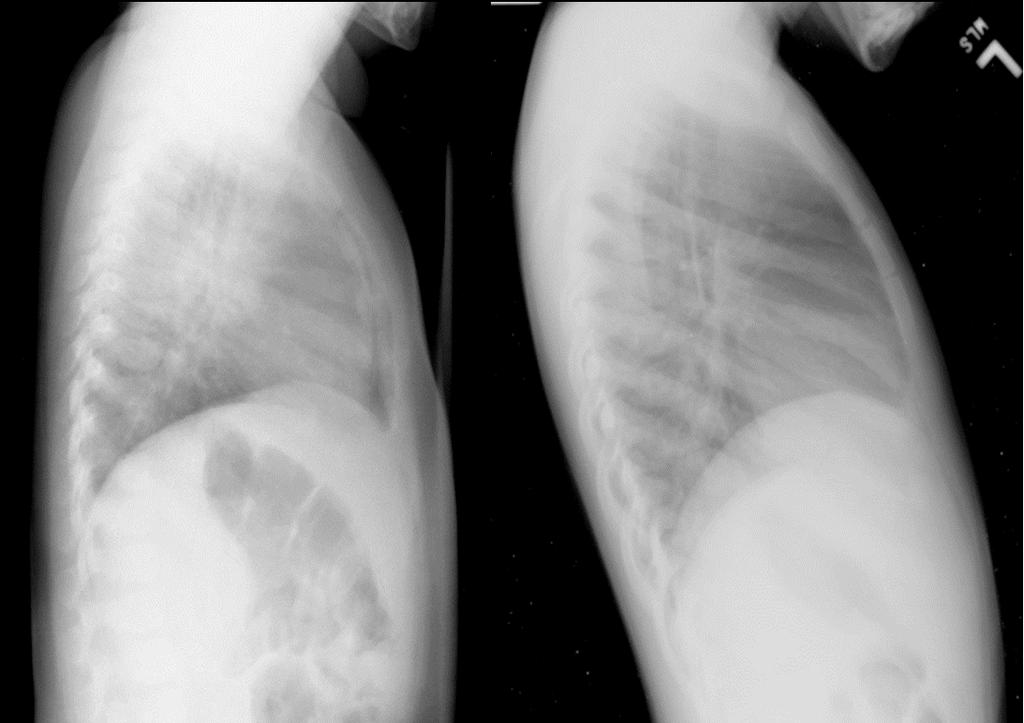
12 PRIMARY TB DISEASE Typical of childhood TB Usually not cavitary Classic x-ray: Hilar lymphadenopathy +/- infiltrates or Miliary pattern Low numbers of organisms AFB smears negative (95%) Cultures negative in 60% of cases Most children <12 yrs not contagious Often asymptomatic (50%) 12
13 13

14 RADIOGRAPHIC FINDINGS IN PEDIATRIC TB DISEASE Typical of TB Hilar and interthoracic lymphadenopathy Miliary pattern Basilar enhancement on brain imaging Not specific but common Lobar pneumonia Pleural effusion in adults and teens Apical cavitary lesions in adults and teens 14
 Other 13% Bone/Joint 10% Meningeal 4% Miliary 9% GU 16% Lymphatic 25% Pleural 23% Lymphatic Pleural GU Meningeal Bone/Joint Miliary Other")
15 TB DISEASE Adult TB Disease Pediatric TB Disease 15% 85% 25% 75% Pulmonary Extrapulm Pulmonary Extrapulmonary Adult Extrapulmonary TB Disease (15%) Other 13% Bone/Joint 10% Meningeal 4% Miliary 9% GU 16% Lymphatic 25% Pleural 23% Lymphatic Pleural GU Meningeal Bone/Joint Miliary Other 15
16 Miliary 5% Extrapulmonary TB Disease in Children (25%) Other 5% Bone/Joint 5% Pleural 6% Meningeal 14% Lymphatic 65% Lymphatic Meningeal Pleural Miliary Other Bone/Joint COMMON SYMPTOMS OF TB DISEASE IN CHILDREN (NONSPECIFIC) Cough and/or respiratory distress Pulmonary findings on examination Lymphadenopathy or lymphadenitis S/Sx of meningitis including seizures Persistent fever (FUO) Weight loss or failure to thrive Unlike adults, up to 50% of children with TB disease have no symptoms 16



17 DIAGNOSIS OF TB IN CHILDREN Gold Standard Positive TB Culture OR, Clinical Diagnosis: Abnormal CXR, laboratory, or physical examination consistent with TB AND 1 or more of the following: Positive tuberculin skin test or IGRA Contagious adult source case identified Clinical course consistent with TB disease, or Improvement on TB therapy DIAGNOSTIC TRIAD PEDI TB DISEASE 1. Positive TST 2. Abnormal CXR 3. Infectious source case 17

 Nasopharynx suctioned One specimen sufficient Minimal costs Yield equivalent to GA s Lancet.")
18 GASTRIC ASPIRATES Inpatient procedure Overnight fasting Lavage with normal saline Collected in morning x 3 days Inpatient costs substantial AFB smear yield: <5% Sensitivity of culture 20-50% Future: possible use of NAAT s in children INDUCED SPUTUM Outpatient procedure 2-3h fasting period Pretreatment: Nebulized bronchodilator and hypertonic saline Chest physiotherapy (CPT) Nasopharynx suctioned One specimen sufficient Minimal costs Yield equivalent to GA s Lancet. 2005;365:130 18

 Nucleic acid amplification tests (NAAT) in children Data limited especially from U.S.")
19 TB CULTURES FROM CHILDREN Bronchoalveolar lavage (BAL) Single specimen with similar yield to 3 GA s Sensitivity 40% (20-50% range) Lymph nodes Biopsy or FNA for path and culture Sensitivity 30-70% on culture CSF in TB meningitis High volume (> 6 ml) improves yield Sensitivity 20% average (12-50% range) Nucleic acid amplification tests (NAAT) in children Data limited especially from U.S. Sensitivity estimated at 60-85% Bottom line Negative test does not rule out disease TUBERCULIN SKIN TEST AND INTERFERON GAMA RELEASE ASSAYS (IGRA) Tuberculin Skin Test Sensitivity 90% 50% in disseminated TB Specificity 85% Lower in BCG vaccinated Cross reacts with BCG vaccine Many NTM IGRA (QFT or TSPOT) Sensitivity 75-90% Children 90% Lower in developing countries and children <5 years of age (50-90%) Specificity 90-99% Cross reactions None with BCG Only 3 NTM M. kansasii, M. marinum, M. szulgai Both TST and IGRA tests may be helpful in difficult cases 19
20 Quantiferon and TST in Children Machingaidze et al. PIDJ 2011; 30: epub IGRA SENSITIVITY IN CHILDREN < 5 YRS OF AGE INSUFFICIENT TO REPLACE TST Test Sensitivity <5 years (CI) Sensitivity >5 years (CI) Specificity TST 90% (79-100) 98% (93-100) NA, ref standard QFT-G-IT 73% (58-89) 93% (84-100) 93% (88-99) T-SPOT.TB 63% (46-80) 83% (75-90) 92% (87-99) Chiappini E. PIDJ. 2014:33: children total, 210 not infected, 58 LTBI, 42 probable TB disease by clinical criteria, 28 culture confirmed disease 20
21 Algorithm for TB Testing in Children TB Risk Questionnaire positive? Yes Age < 5 years? No Yes Screening Complete TST Preferred No BCG Vaccinated? Yes IGRA Preferred No TST or IGRA Acceptable Consider Cost Confidence in test Ability to return WHAT TO DO WITH DISCORDANT IGRA AND TST RESULTS? For healthy patients (5 yrs or older) with low risk for disease Choose the more specific test (IGRA) If the patient is sick, under 5 years of age or at high risk of disease Consider either test positive for highest sensitivity Indeterminate results means the control failed Repeat the test 21
 Monitor and reinforce adherence When to follow up CXR s for pulmonary TB Beginning and end of therapy Anytime if clinical change")
22 MONITORING CHILDREN ON TB TREATMENT Risk of drug toxicity very low Monitor clinical signs regular clinical visits (4-6 wks) patient education Routine blood work not necessary unless symptoms risk factors for toxicity (obesity, other hepatotoxic medications) Monitor and reinforce adherence When to follow up CXR s for pulmonary TB Beginning and end of therapy Anytime if clinical change Completion of therapy certificate TB MEDICATIONS IN KIDS Hepatotoxicity rare INH liquid vs tablets Medication refusal in children Crush tablets, medication sandwich Vitamin B6 Not needed for all kids Important for Breastfed infants Teens and/or picky eaters Patients with symptoms of peripheral neuropathy Going back to school Children <12 yrs of age are not contagious 22



23 CENTRAL NERVOUS SYSTEM TB DRUG PENETRATION Drug Isoniazid Rifampin PZA Ethambutol Ethionamide Aminoglycosides Fluoroquinolones CNS Penetration Good Inflamed meninges only Good Inflamed meninges only Good Inflamed meninges only Good except Cipro poor ETHAMBUTOL IN CHILDREN Risk of optic neuritis: Visual acuity Color perception Dose related Usually reversible Risk around 1-3% in adults Risk in children about the same EMB safe in children with monitoring Monitor vision on treatment Infants visual evoked potentials (VEP) 23
24 Ethambutol in Children Table 2. Studies that have specifically sought optical toxicity in children treated with Ethambutol Reference Patients (n) Age range Method of evaluation Length of follow up Number with (months) toxicity Fox* years 4 months to 16 years 1-15 years 4-5 years 5-15 years 9-16 years Visual evoked responses Acuity/field/colour Acuity/field/colour Acuity/field/colour Acuity/field/colour Computerized visual field examination *Fox W, unpublished data quoted in Tubercle 1986; 67:27. SM Graham. Arch Dis child 1998; 79: FLUOROQUINOLONES IN CHILDREN Initial clinical trials in children not done Some children have been treated without problems: CF, chronic UTI, shigellosis and TB Most consider safe in children: Some case series and RCT with good results Germany study: 2030 patients treated, 31 (1.5%) with self resolving arthralgia* Not indicated for routine infections in children Consider risks and benefits Monitor clinically for joint and tendon problems *B Hampel. Pediatr Inf Dis J, 1997;16:
25 Comparison of Side Effects with Ciprofloxacin vs Ceftazidime/Tobramycin in Children No. of Patients Event Ciprofloxacin N = 67 (%) Ceftazidime/ Tobramycin N = 62 (%) P Any 52 (78) 43 (69) Abnormal liver function tests 17 (25) 13 (21) Injection 16 (24) 5 (8) Injection site pain 13 (19) 7 (11) Rash 10 (15) 5 (8) Phlebitis 7 (10) 1 (2) Vomiting 11(16) 4 (6) Central nervous system, any 1 (1) 6 (10) Respiratory, any 7 (10) 3 (5) Musculoskeletal, any 15 (22) 13 (21) Joint Disorder 8 (12) 10 (16) Arthralgia 7 (10) 7 (11) Arthritis 1 (1) 0 (0) 1.0 Leg cramps 0 (0) 1 (2) Myalgia 1 (1) 0 (0) DA Church. Pediatr Infec Dis J 1997 Jan; 16 (1): PEDIATRIC TB CASES 25


26 LYMPHADENOPATHY CLINICAL CASE CERVICAL LYMPHADENOPATHY 8 yr old with cervical lymphadenopathy History: LAN for 3 months PMHx: Healthy BCG vaccine at birth TB skin test 10 mm Physical Exam: 3 cm anterior cervical LAN 1.5 cm supraclavicular lymphadenopathy CXR: Hilar LAN, no infiltrates Is this TB disease? What else could it be? 26

27 HILAR & CERVICAL LYMPHADENOPATHY Differential Dx Tuberculosis Non TB mycobacteria (NTM) Lymphoma/Leukemia HIV Other causes Diagnostic tests Biopsy (FNA or surgical for culture and path) Interferon blood test for TB infection RESULTS Fine needle aspirate of node: Pathology: lymphoma, no TB by culture or microscopy Interferon Blood test for TB T-SPOT Positive Diagnoses: Hodgkin s Lymphoma LTBI Treatment: Chemotherapy for lymphoma Treatment for LTBI (INH, Rif or 3HP) 27

28 Skin Test in Foreign Born SKIN TEST IN FOREIGN BORN 6 year old with positive TST for school entry Born in Asia BCG documented on vaccination records at birth and BCG scar present TST measures 12mm 28
29 CXR NORMAL How do you interpret the 12 mm skin test? Is this BCG effect or LTBI? Are there any other tests that may help? TREATMENT OF LATENT TB INFECTION (LTBI) Traditional INH for 9 months Clinically monitor for hepatitis and peripheral neuropathy Supplement Vit B6 if breastfed, poor diet or symptoms Caution: liquid INH causes diarrhea Crushed tablets preferred Dose: daily or twice weekly (DOT) Newer option Rifampin daily for 4-6 months Potential drug interactions (OCA s, protease inhibitors) Discolors urine and tears Cost 5-8 x higher than INH Capsules or can be compounded into liquid formulation Health Department Only INH-Rifapentine (3HP) once weekly for 12 doses Must be DOT Not approved for children < 2 years DOT = Directly Observed Therapy 29
 12 weeks NA INH 15 mg/kg RPT 20-30 mg/kg INH 900 mg RPT 900 mg INH $5-$9 RPT")
30 LTBI TREATMENT OPTIONS AND DRUG COST Drug Duration Daily Dose Intermittent Dose Max Dose Drug Cost only Not DOT INH 9 months mg/kg mg/kg 300 mg daily 900 mg BIW $45-$180/daily $13-$55/BIW Rifampin 4-6 months mg/kg Not recommended for LTBI 600 mg daily $190-$500/4 mo $290-$730/6 mo INH/RPT (3HP) 12 weeks NA INH 15 mg/kg RPT mg/kg INH 900 mg RPT 900 mg INH $5-$9 RPT $100-$300 Nicholson EG. J Pediatr Health Care. (2015) 29, BABY EXPOSED TO TB DISEASE 2 month old infant Mother with pulmonary TB Cavitary disease on CXR AFB smear positive Mother s CXR 30


31 BABY EXPOSED TO TB DISEASE Baby with cough and respiratory distress TST 0 mm What would you do next? CXR Diagnosis? Lumbar puncture? CSF normal Treatment? TB IN NEWBORN NURSERY 31
32 NEW MOTHER WITH POSITIVE TST Newborn infant in hospital nursery Mother with 15 mm TST CXR: calcified granuloma no active disease Not on treatment What is mother s diagnosis? Do mother or baby need isolation? May baby breast feed and room with mother? 32
33 Maternal TB disease or LTBI during pregnancy Is mother contagious? If no exposure to contagious household TB contacts: No treatment for baby Okay to breastfeed No Yes Exposure to contagious household TB contact: Window prophylaxis for baby Multivitamin for baby Okay to breastfeed If MDR-TB, separate baby from source PREVENTION OF TB DISEASE IN CHILDREN Contact Investigation Window Prophylaxis Treatment of LTBI 33

34 RESOURCES HNTC Pedi TB Toolbox Guidelines and clinical tools Reference materials Patient education materials TB Testing in Children Brochure Pediatric Radiology for Clinicians 34
TB Intensive Houston, Texas October 15-17, 2013
 TB Intensive Houston, Texas October 15-17, 2013 Tuberculosis in Children Kim Connelly Smith, MD, MPH October 16, 2013 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict of interests
TB Intensive Houston, Texas October 15-17, 2013 Tuberculosis in Children Kim Connelly Smith, MD, MPH October 16, 2013 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict of interests
Tuberculosis Intensive
 Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Childhood Tuberculosis Kim Smith, MD, MPH April 6, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Childhood Tuberculosis Kim Smith, MD, MPH April 6, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
TB Nurse Case Management San Antonio, Texas July 18 20, 2012
 TB Nurse Case Management San Antonio, Texas July 18 20, 2012 Pediatric TB Kim Smith, MD, MPH July 19, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
TB Nurse Case Management San Antonio, Texas July 18 20, 2012 Pediatric TB Kim Smith, MD, MPH July 19, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
TB Intensive San Antonio, Texas August 7-10, 2012
 TB Intensive San Antonio, Texas August 7-10, 2012 An Introduction to Childhood Tuberculosis Kim Smith, MD, MPH August 10, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests
TB Intensive San Antonio, Texas August 7-10, 2012 An Introduction to Childhood Tuberculosis Kim Smith, MD, MPH August 10, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests
TB Nurse Case Management San Antonio, Texas March 7 9, Pediatric TB Kim Connelly Smith, MD, MPH March 8, 2012
 TB Nurse Case Management San Antonio, Texas March 7 9, 2012 Pediatric TB Kim Connelly Smith, MD, MPH March 8, 2012 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict of interests
TB Nurse Case Management San Antonio, Texas March 7 9, 2012 Pediatric TB Kim Connelly Smith, MD, MPH March 8, 2012 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict of interests
TB Intensive Houston, Texas. Childhood Tuberculosis Kim Connelly Smith. November 12, 2009
 TB Intensive Houston, Texas November 10-12, 12 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 1 OUTLINE Stages
TB Intensive Houston, Texas November 10-12, 12 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 1 OUTLINE Stages
Pediatric TB Lisa Armitige, MD, PhD September 28, 2011
 TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Pediatric TB Lisa Armitige, MD, PhD September 28, 2011 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interest.
TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Pediatric TB Lisa Armitige, MD, PhD September 28, 2011 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interest.
Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017
 Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has the following disclosures
Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has the following disclosures
Diagnosis and Medical Management of Latent TB Infection
 Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Pediatric TB Intensive Houston, Texas October 14, Extrapulmonary TB in Children Kim Connelly Smith, MD, MPH October 14, 2013
 Pediatric TB Intensive Houston, Texas October 14, 2013 Extrapulmonary TB in Children Kim Connelly Smith, MD, MPH October 14, 2013 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict
Pediatric TB Intensive Houston, Texas October 14, 2013 Extrapulmonary TB in Children Kim Connelly Smith, MD, MPH October 14, 2013 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict
Treatment of TB Infection Lisa Y. Armitige, MD, PhD April 7, 2015
 Treatment of TB Infection Lisa Y. Armitige, MD, PhD April 7, 2015 Tuberculosis Infection Diagnosis and Treatment April 7, 2015 El Paso, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has
Treatment of TB Infection Lisa Y. Armitige, MD, PhD April 7, 2015 Tuberculosis Infection Diagnosis and Treatment April 7, 2015 El Paso, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has
DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE
 DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH Assistant Professor University of Texas Health Science Center Staff Physician, Texas Center for Infectious Diseases TB Nurse Case
DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH Assistant Professor University of Texas Health Science Center Staff Physician, Texas Center for Infectious Diseases TB Nurse Case
TB: Management in an era of multiple drug resistance. Bob Belknap M.D. Denver Public Health November 2012
 TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
Contact Investigation and Prevention in the USA
 Contact Investigation and Prevention in the USA George D. McSherry, MD Division of Infectious Disease Penn State Children s Hospital Pediatric Section TB Center of Excellence Rutgers Global Tuberculosis
Contact Investigation and Prevention in the USA George D. McSherry, MD Division of Infectious Disease Penn State Children s Hospital Pediatric Section TB Center of Excellence Rutgers Global Tuberculosis
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016
 Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
Management of Pediatric Tuberculosis in New Jersey
 Management of Pediatric Tuberculosis in New Jersey Helen Aguila, MD NJMS Global TB Institute December 15, 2011 This presentation is in part adapted from Pediatric Tuberculosis by Ann Loeffler, MD : Francis
Management of Pediatric Tuberculosis in New Jersey Helen Aguila, MD NJMS Global TB Institute December 15, 2011 This presentation is in part adapted from Pediatric Tuberculosis by Ann Loeffler, MD : Francis
has the following disclosures to make:
 CLINICAL DIAGNOSIS AND MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH September 22, 2015 TB Nurse Case Management September 22 24, 2015 San Antonio. TX EXCELLENCE EXPERTISE INNOVATION Annie Kizilbash
CLINICAL DIAGNOSIS AND MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH September 22, 2015 TB Nurse Case Management September 22 24, 2015 San Antonio. TX EXCELLENCE EXPERTISE INNOVATION Annie Kizilbash
Diagnosis & Medical Case Management of TB Disease. Lisa Armitige, MD, PhD October 22, 2015
 Diagnosis & Medical Case Management of TB Disease Lisa Armitige, MD, PhD October 22, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
Diagnosis & Medical Case Management of TB Disease Lisa Armitige, MD, PhD October 22, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
PEDIATRIC TUBERCULOSIS. Objectives. Children are not just small adults. Pediatric Tuberculosis 1
 PEDIATRIC TUBERCULOSIS Ann M. Loeffler, M.D. Faculty Consultant Curry International Tuberculosis Center Objectives At the end of this session, participants will be able to describe: how pediatric patients
PEDIATRIC TUBERCULOSIS Ann M. Loeffler, M.D. Faculty Consultant Curry International Tuberculosis Center Objectives At the end of this session, participants will be able to describe: how pediatric patients
Tuberculosis Tools: A Clinical Update
 Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
PEDIATRIC TUBERCULOSIS
 PEDIATRIC TUBERCULOSIS Ann M. Loeffler, M.D. Faculty Consultant Curry International Tuberculosis Center Objectives At the end of this session, participants will be able to describe: how pediatric patients
PEDIATRIC TUBERCULOSIS Ann M. Loeffler, M.D. Faculty Consultant Curry International Tuberculosis Center Objectives At the end of this session, participants will be able to describe: how pediatric patients
What the Primary Physician Should Know about Tuberculosis. Topics for Discussion. Global Impact of TB
 What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Common disease presentations Diagnosis of active TB Screening
What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Common disease presentations Diagnosis of active TB Screening
Diagnosis and Treatment of Tuberculosis, 2011
 Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
What the Primary Physician Should Know about Tuberculosis. Topics for Discussion. Life Cycle of M. tuberculosis
 What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Microbiology Epidemiology Common disease presentations Diagnosis of active
What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Microbiology Epidemiology Common disease presentations Diagnosis of active
TB Intensive San Antonio, Texas
 TB Intensive San Antonio, Texas August 2-5, 2011 Pediatric TB Jeffrey Starke, MD August 5, 2011 Jeffrey Starke, MD has the following disclosures to make: Is on a data safety monitoring board for Hoffman
TB Intensive San Antonio, Texas August 2-5, 2011 Pediatric TB Jeffrey Starke, MD August 5, 2011 Jeffrey Starke, MD has the following disclosures to make: Is on a data safety monitoring board for Hoffman
TB in the Patient with HIV
 TB in the Patient with HIV Lisa Y. Armitige, MD, PhD May 11, 2017 TB Intensive May 9 12, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD, has the following disclosures to
TB in the Patient with HIV Lisa Y. Armitige, MD, PhD May 11, 2017 TB Intensive May 9 12, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD, has the following disclosures to
Tuberculosis: A Provider s Guide to
 Tuberculosis: A Provider s Guide to Diagnosis and Treatment of Active Tuberculosis (TB) Disease and Screening and Treatment of Latent Tuberculosis Infection (LTBI) Alameda County Health Care Services Agency
Tuberculosis: A Provider s Guide to Diagnosis and Treatment of Active Tuberculosis (TB) Disease and Screening and Treatment of Latent Tuberculosis Infection (LTBI) Alameda County Health Care Services Agency
TUBERCULOSIS. Pathogenesis and Transmission
 TUBERCULOSIS Pathogenesis and Transmission TUBERCULOSIS Pathogenesis and Transmission Infection to Disease Diagnostic & Isolation Updates Treatment Updates Pathogenesis Droplet nuclei of 5µm or less are
TUBERCULOSIS Pathogenesis and Transmission TUBERCULOSIS Pathogenesis and Transmission Infection to Disease Diagnostic & Isolation Updates Treatment Updates Pathogenesis Droplet nuclei of 5µm or less are
Diagnosis and Medical Management of TB Disease. Quratulian Annie Kizilbash, MD, MPH March 17, 2015
 Diagnosis and Medical Management of TB Disease Quratulian Annie Kizilbash, MD, MPH March 17, 2015 TB Nurse Case Management March 17 19, 2015 San Antonio, Texas EXCELLENCE EXPERTISE INNOVATION Quratulian
Diagnosis and Medical Management of TB Disease Quratulian Annie Kizilbash, MD, MPH March 17, 2015 TB Nurse Case Management March 17 19, 2015 San Antonio, Texas EXCELLENCE EXPERTISE INNOVATION Quratulian
5. HIV-positive individuals treated with INH should receive Pyridoxine (B6) 25 mg daily or 50 mg twice/thrice weekly on the same schedule as INH
 25 mg daily or 50 mg twice/thrice weekly on the same schedule as INH") V. TB and HIV/AIDS A. Standards of Treatment and Management The majority of TB treatment principles apply to persons with HIV/AIDS who require treatment for TB disease. The following points are either
V. TB and HIV/AIDS A. Standards of Treatment and Management The majority of TB treatment principles apply to persons with HIV/AIDS who require treatment for TB disease. The following points are either
Pediatric TB Theresa Barton, MD
 TB Nurse Case Management San Antonio, Texas December 8-10, 2009 Pediatric TB Theresa Barton, MD December 9, 2009 Pediatric Tuberculosis Tess Barton, MD Assistant Professor of Pediatrics UT Southwestern
TB Nurse Case Management San Antonio, Texas December 8-10, 2009 Pediatric TB Theresa Barton, MD December 9, 2009 Pediatric Tuberculosis Tess Barton, MD Assistant Professor of Pediatrics UT Southwestern
TB Update: March 2012
 TB Update: March 2012 David Schlossberg, MD, FACP Medical Director, TB Control Program Philadelphia Department of Public Health 1 TB Update: March 2012 IGRAs vs TST LTBI A New Regimen NAATs What is Their
TB Update: March 2012 David Schlossberg, MD, FACP Medical Director, TB Control Program Philadelphia Department of Public Health 1 TB Update: March 2012 IGRAs vs TST LTBI A New Regimen NAATs What is Their
Diagnosis of tuberculosis in children
 Diagnosis of tuberculosis in children H Simon Schaaf Desmond Tutu TB Centre Department of Paediatrics and Child Health, Stellenbosch University, and Tygerberg Children s Hospital (TCH) Estimated TB incidence
Diagnosis of tuberculosis in children H Simon Schaaf Desmond Tutu TB Centre Department of Paediatrics and Child Health, Stellenbosch University, and Tygerberg Children s Hospital (TCH) Estimated TB incidence
TB Nurse Case Management
 TB Nurse Case Management San Antonio, Texas March 2-4, 2011 Pediatric TB Andrea T. Cruz, MD, MPH March 2, 2011 Andrea Cruz, MD, MPH has the following disclosures to make: No conflict of interests No relevant
TB Nurse Case Management San Antonio, Texas March 2-4, 2011 Pediatric TB Andrea T. Cruz, MD, MPH March 2, 2011 Andrea Cruz, MD, MPH has the following disclosures to make: No conflict of interests No relevant
TB & HIV CO-INFECTION IN CHILDREN. Reené Naidoo Paediatric Infectious Diseases Broadreach Healthcare 19 April 2012
 TB & HIV CO-INFECTION IN CHILDREN Reené Naidoo Paediatric Infectious Diseases Broadreach Healthcare 19 April 2012 Introduction TB & HIV are two of the leading causes of morbidity & mortality in children
TB & HIV CO-INFECTION IN CHILDREN Reené Naidoo Paediatric Infectious Diseases Broadreach Healthcare 19 April 2012 Introduction TB & HIV are two of the leading causes of morbidity & mortality in children
Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis
 Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Diagnosis of active TB Screening
Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Diagnosis of active TB Screening
Tuberculosis in Primary Care COC GTA Spring Symposium Dr Elizabeth Rea April 2013
 Tuberculosis in Primary Care COC GTA Spring Symposium Dr Elizabeth Rea April 2013 1 TB in Toronto - risk groups Diagnosis of active TB LTBI diagnosis and management Infection control 2 TB in Toronto Case
Tuberculosis in Primary Care COC GTA Spring Symposium Dr Elizabeth Rea April 2013 1 TB in Toronto - risk groups Diagnosis of active TB LTBI diagnosis and management Infection control 2 TB in Toronto Case
TB in Children. Rene De Gama Block 10 Lectures 2012
 TB in Children Rene De Gama Block 10 Lectures 2012 Contents Epidemiology Transmission and pathogenesis Diagnosis of TB TB and HIV Management Epidemiology The year 2000 8.3 million new TB cases diagnosed
TB in Children Rene De Gama Block 10 Lectures 2012 Contents Epidemiology Transmission and pathogenesis Diagnosis of TB TB and HIV Management Epidemiology The year 2000 8.3 million new TB cases diagnosed
Diagnosis and Management of TB Disease Lisa Armitige, MD, PhD September 27, 2011
 TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Diagnosis and Management of TB Disease Lisa Armitige, MD, PhD September 27, 2011 Lisa Armitige, MD, PhD has the following disclosures to make:
TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Diagnosis and Management of TB Disease Lisa Armitige, MD, PhD September 27, 2011 Lisa Armitige, MD, PhD has the following disclosures to make:
Northwestern Polytechnic University
 Clinical Tuberculosis Assessment by Health Care Provider Clinicians should review and verify the information in the Tuberculosis (TB) Screening Questionnaire (attached). Persons answering YES to any questions
Clinical Tuberculosis Assessment by Health Care Provider Clinicians should review and verify the information in the Tuberculosis (TB) Screening Questionnaire (attached). Persons answering YES to any questions
Disclosures. Current Issues and Controversies in Child and Adolescent Tuberculosis 02/24/2016. NSTC 2016 Annual Meeting
 Current Issues and Controversies in Child and Adolescent Tuberculosis Jeffrey R. Starke, M.D. Professor of Pediatrics Baylor College of Medicine [With great thanks to Andrea Cruz, M.D.] Disclosures Dr.
Current Issues and Controversies in Child and Adolescent Tuberculosis Jeffrey R. Starke, M.D. Professor of Pediatrics Baylor College of Medicine [With great thanks to Andrea Cruz, M.D.] Disclosures Dr.
New Approaches to the Diagnosis and Management of Tuberculosis Infection in Children and Adolescents
 New Approaches to the Diagnosis and Management of Tuberculosis Infection in Children and Adolescents Jeffrey R. Starke, M.D. Professor of Pediatrics Baylor College of Medicine [With great thanks to Andrea
New Approaches to the Diagnosis and Management of Tuberculosis Infection in Children and Adolescents Jeffrey R. Starke, M.D. Professor of Pediatrics Baylor College of Medicine [With great thanks to Andrea
Pediatric Tuberculosis
 Pediatric Tuberculosis Rafael E. Hernandez, MD PhD Attending Physician, Instructor Pediatric Infectious Diseases Seattle Children s Hospital & University of Washington Disclosures No financial conflicts
Pediatric Tuberculosis Rafael E. Hernandez, MD PhD Attending Physician, Instructor Pediatric Infectious Diseases Seattle Children s Hospital & University of Washington Disclosures No financial conflicts
10/3/2017. Updates in Tuberculosis. Global Tuberculosis, WHO 2015 report. Objectives. Disclosures. I have nothing to disclose
 Disclosures Updates in Tuberculosis I have nothing to disclose Chris Keh, MD Assistant Clinical Professor, Division of Infectious Diseases, UCSF TB Controller, TB Prevention and Control Program, Population
Disclosures Updates in Tuberculosis I have nothing to disclose Chris Keh, MD Assistant Clinical Professor, Division of Infectious Diseases, UCSF TB Controller, TB Prevention and Control Program, Population
Diagnosis and Medical Management of TB Infection Lisa Y. Armitige, MD, PhD September 12, TB Nurse Case Management September 12 14, 2017
 Diagnosis and Medical Management of TB Infection Lisa Y. Armitige, MD, PhD September 12, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has
Diagnosis and Medical Management of TB Infection Lisa Y. Armitige, MD, PhD September 12, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has
What you need to know about diagnosing and treating TB: a preventable, fatal disease. Bob Belknap M.D. Denver Public Health November 2014
 What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2014 The Critical First Step Consider TB in the Differential 1. Risks
What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2014 The Critical First Step Consider TB in the Differential 1. Risks
TB Intensive San Antonio, Texas May 7-10, 2013
 TB Intensive San Antonio, Texas May 7-10, 2013 TB in the HIV Patient Lisa Armitige, MD, PhD May 09, 2013 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interests No relevant
TB Intensive San Antonio, Texas May 7-10, 2013 TB in the HIV Patient Lisa Armitige, MD, PhD May 09, 2013 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interests No relevant
Pediatric Tuberculosis
 Pediatric Tuberculosis Rafael E. Hernandez, MD PhD Attending Physician, Instructor Pediatric Infectious Diseases Seattle Children s Hospital & University of Washington Disclosures No financial conflicts
Pediatric Tuberculosis Rafael E. Hernandez, MD PhD Attending Physician, Instructor Pediatric Infectious Diseases Seattle Children s Hospital & University of Washington Disclosures No financial conflicts
Pediatric TB Intensive Houston, Texas October 14, 2013
 Pediatric TB Intensive Houston, Texas October 14, 2013 Diagnosis and Management of Tuberculosis in Adolescents Andrea T. Cruz, MD, MPH Sections of Infectious Diseases & Emergency Medicine October 14, 2013
Pediatric TB Intensive Houston, Texas October 14, 2013 Diagnosis and Management of Tuberculosis in Adolescents Andrea T. Cruz, MD, MPH Sections of Infectious Diseases & Emergency Medicine October 14, 2013
Pediatric Tuberculosis: The Essentials October 8, 2014
 Pediatric Tuberculosis: The Essentials Ann M Loeffler, MD Randall Children s Hospital at Legacy Emanuel Portland, Oregon Curry International TB Center Disclosures Nothing to disclose Learning Objectives
Pediatric Tuberculosis: The Essentials Ann M Loeffler, MD Randall Children s Hospital at Legacy Emanuel Portland, Oregon Curry International TB Center Disclosures Nothing to disclose Learning Objectives
Pediatric TB Radiology: It s Not Black and White Part 2
 Experiencing technical difficulties? Please call Adobe Connect for technical assistance at 1-800-422-3623 Pediatric TB Radiology: It s Not Black and White Part 2 June 18, 2018 A National Webinar June 18,
Experiencing technical difficulties? Please call Adobe Connect for technical assistance at 1-800-422-3623 Pediatric TB Radiology: It s Not Black and White Part 2 June 18, 2018 A National Webinar June 18,
CLINICAL DIAGNOSIS AND MANAGEMENT OF TB Disease
 CLINICAL DIAGNOSIS AND MANAGEMENT OF TB Disease Barbara J Seaworth MD Medical Director Heartland National TB Center Professor of Medicine University of Texas Health Center Tyler Barbara J Seaworth MD has
CLINICAL DIAGNOSIS AND MANAGEMENT OF TB Disease Barbara J Seaworth MD Medical Director Heartland National TB Center Professor of Medicine University of Texas Health Center Tyler Barbara J Seaworth MD has
Chapter 5 Treatment for Latent Tuberculosis Infection
 Chapter 5 Treatment for Latent Tuberculosis Infection Table of Contents Chapter Objectives.... 109 Introduction.... 111 Candidates for the Treatment of LTBI... 112 LTBI Treatment Regimens.... 118 LTBI
Chapter 5 Treatment for Latent Tuberculosis Infection Table of Contents Chapter Objectives.... 109 Introduction.... 111 Candidates for the Treatment of LTBI... 112 LTBI Treatment Regimens.... 118 LTBI
Pre-Treatment Evaluation. Treatment of Latent TB Infection (LTBI) Initiating Treatment: Patient Education. Before initiating treatment for LTBI:
 Initiating Treatment: Patient Education. Before initiating treatment for LTBI:") Pre-Treatment Evaluation Before initiating treatment for LTBI: Treatment of Latent TB Infection (LTBI) Amee Patrawalla, MD Associate Professor, New Jersey Medical School Attending Physician, NJMS Global
Pre-Treatment Evaluation Before initiating treatment for LTBI: Treatment of Latent TB Infection (LTBI) Amee Patrawalla, MD Associate Professor, New Jersey Medical School Attending Physician, NJMS Global
Diagnosing Tuberculosis in Pediatric Patients Kim Connelly Smith, MD, MPH November 13, 2008
 Tuberculosis Updates for Clinicians San Antonio, Texas November 13, 2008 Diagnosing Tuberculosis in Pediatric Patients Kim Connelly Smith, MD, MPH November 13, 2008 Childhood Tuberculosis Kim Connelly
Tuberculosis Updates for Clinicians San Antonio, Texas November 13, 2008 Diagnosing Tuberculosis in Pediatric Patients Kim Connelly Smith, MD, MPH November 13, 2008 Childhood Tuberculosis Kim Connelly
Latent TB, TB and the Role of the Health Department
 Latent TB, TB and the Role of the Health Department Elaine Darnall, RN, BSN, CIC TB Nurse Consultant Illinois Dept of Public Health March 21, 2018 Elaine Darnall has disclosed that there is no actual or
Latent TB, TB and the Role of the Health Department Elaine Darnall, RN, BSN, CIC TB Nurse Consultant Illinois Dept of Public Health March 21, 2018 Elaine Darnall has disclosed that there is no actual or
TB In Detroit 2011* Early TB: Smudge Sign. Who is at risk for exposure to or infection with TB? Who is at risk for TB after exposure or infection?
 Those oral antibiotics are just not working! Inpatient Standards of Care & Discharge Planning S/He s in the Hospital: Now What Do I Do? Dana G. Kissner, MD TB Intensive Workshop, Lansing, MI 2012 Objectives:
Those oral antibiotics are just not working! Inpatient Standards of Care & Discharge Planning S/He s in the Hospital: Now What Do I Do? Dana G. Kissner, MD TB Intensive Workshop, Lansing, MI 2012 Objectives:
The Origin of Swine Flu
 How the Heck Do You Diagnose Tuberculosis in Children, Anyway? Jeffrey R. Starke, M.D. Professor and Vice Chairman of Pediatrics Baylor College of Medicine Houston, Texas USA The Origin of Swine Flu MAIN
How the Heck Do You Diagnose Tuberculosis in Children, Anyway? Jeffrey R. Starke, M.D. Professor and Vice Chairman of Pediatrics Baylor College of Medicine Houston, Texas USA The Origin of Swine Flu MAIN
Pediatric TB Basics and Evaluation and Management of Exposed Neonates
 Pediatric TB Basics and Evaluation and Management of Exposed Neonates Ann M. Loeffler, MD Randall Children s Hospital, Portland OR & Curry International TB Center, Oakland CA September, 2017 No Disclosures
Pediatric TB Basics and Evaluation and Management of Exposed Neonates Ann M. Loeffler, MD Randall Children s Hospital, Portland OR & Curry International TB Center, Oakland CA September, 2017 No Disclosures
Pediatric TB Intensive Houston, Texas
 Pediatric TB Intensive Houston, Texas November 13, 2009 Treatment of Pediatric TB Jeffrey R. Starke, M.D. November 13, 2009 MANAGEMENT OF CHILDHOOD TUBERCULOSIS Jeffrey R. Starke, M.D. Professor of Pediatrics
Pediatric TB Intensive Houston, Texas November 13, 2009 Treatment of Pediatric TB Jeffrey R. Starke, M.D. November 13, 2009 MANAGEMENT OF CHILDHOOD TUBERCULOSIS Jeffrey R. Starke, M.D. Professor of Pediatrics
Fundamentals of Tuberculosis (TB)
") TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
At the end of this session, participants will be able to:
 Advanced Concepts in Pediatric Tuberculosis: Infection Control, Source Case and Contact Investigation Ana M. Alvarez, M.D. Associate Professor Division of Pediatric Infectious Diseases and Immunology University
Advanced Concepts in Pediatric Tuberculosis: Infection Control, Source Case and Contact Investigation Ana M. Alvarez, M.D. Associate Professor Division of Pediatric Infectious Diseases and Immunology University
INDEX CASE INFORMATION
 Instructions for Completing the MDH Tuberculosis Contact Investigation Report Form Please provide as much information as possible. Each field represents information that is important to the contact investigation.
Instructions for Completing the MDH Tuberculosis Contact Investigation Report Form Please provide as much information as possible. Each field represents information that is important to the contact investigation.
CDC Immigration Requirements: Tuberculosis Screening for Children
 CDC Immigration Requirements: Tuberculosis Screening for Children Ann M. Loeffler, M.D. Curry International TB Center San Francisco, CA March, 2013 Atlanta, Georgia CDC Immigration Requirements: Tuberculosis
CDC Immigration Requirements: Tuberculosis Screening for Children Ann M. Loeffler, M.D. Curry International TB Center San Francisco, CA March, 2013 Atlanta, Georgia CDC Immigration Requirements: Tuberculosis
I. Demographic Information GENDER NUMBER OF CASES PERCENT OF CASES. Male % Female %
 San Joaquin County (SJC) in 03, (N=43) County Rate = 6. Cases per 00,000 Population I. Demographic Information Table I-A: TB cases by gender, SJC, 03 (N=43) GENDER NUMBER OF CASES Male 6 60.5% Female 7
San Joaquin County (SJC) in 03, (N=43) County Rate = 6. Cases per 00,000 Population I. Demographic Information Table I-A: TB cases by gender, SJC, 03 (N=43) GENDER NUMBER OF CASES Male 6 60.5% Female 7
LTBI in Special Populations John Nava, MD October 5, 2010
 Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 LTBI in Special Populations John Nava, MD October 5, 2010 2 Treatment of Latent TB Infection in Special Populations John
Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 LTBI in Special Populations John Nava, MD October 5, 2010 2 Treatment of Latent TB Infection in Special Populations John
TB Intensive San Antonio, Texas. TB/HIV Co-Infection. Lisa Armitige, MD, PhD has the following disclosures to make:
 TB Intensive San Antonio, Texas August 2-5, 2011 TB/HIV Co-Infection Lisa Armitige, MD, PhD August 4, 2011 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interests No relevant
TB Intensive San Antonio, Texas August 2-5, 2011 TB/HIV Co-Infection Lisa Armitige, MD, PhD August 4, 2011 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interests No relevant
Dose Counting Exercise Elizabeth Foy, RN, BSN September 8, 2016
 Dose Counting Exercise Elizabeth Foy, RN, BSN September 8, 2016 TB Nurse Case Management September 7-9, 2016 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Jessica Quintero, M.Ed., has the following disclosures
Dose Counting Exercise Elizabeth Foy, RN, BSN September 8, 2016 TB Nurse Case Management September 7-9, 2016 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Jessica Quintero, M.Ed., has the following disclosures
3/25/2012. numerous micro-organismsorganisms
 Congenital & Neonatal TB A Case of Tuberculosis Congenital or Acquired? Felicia Dworkin, MD NYC DOHMH Bureau TB Control World TB Day March 23, 2012 Congenital TB: acquired by the fetus during pregnancy
Congenital & Neonatal TB A Case of Tuberculosis Congenital or Acquired? Felicia Dworkin, MD NYC DOHMH Bureau TB Control World TB Day March 23, 2012 Congenital TB: acquired by the fetus during pregnancy
Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012
 Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 LTBI and TB Disease Treatment Cara Christ, MD, MS May 8, 2012 Cara Christ, MD, MS has the following disclosures to make: No conflict
Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 LTBI and TB Disease Treatment Cara Christ, MD, MS May 8, 2012 Cara Christ, MD, MS has the following disclosures to make: No conflict
Tuberculosis Intensive
 Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 TB in the HIV Patient Lisa Armitige, MD, PhD April 6, 2012 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interests
Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 TB in the HIV Patient Lisa Armitige, MD, PhD April 6, 2012 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interests
Pediatric Tuberculosis
 Pediatric Tuberculosis Rafael Hernandez, MD PhD Attending Physician, Instructor Pediatric Infectious Diseases Disclosures No financial conflicts Off-label use: Drugs used in typical HZRE regimens are approved
Pediatric Tuberculosis Rafael Hernandez, MD PhD Attending Physician, Instructor Pediatric Infectious Diseases Disclosures No financial conflicts Off-label use: Drugs used in typical HZRE regimens are approved
TUBERCULOSIS. Presented By: Public Health Madison & Dane County
 TUBERCULOSIS Presented By: Public Health Madison & Dane County What is Tuberculosis? Tuberculosis, or TB, is a disease caused by a bacteria called Mycobacterium tuberculosis. The bacteria can attack any
TUBERCULOSIS Presented By: Public Health Madison & Dane County What is Tuberculosis? Tuberculosis, or TB, is a disease caused by a bacteria called Mycobacterium tuberculosis. The bacteria can attack any
TB in Corrections Phoenix, Arizona
 TB in Corrections Phoenix, Arizona March 24, 2011 Treatment of Latent TB Infection Renuka Khurana MD, MPH March 24, 2011 Renuka Khurana, MD, MPH has the following disclosures to make: No conflict of interests
TB in Corrections Phoenix, Arizona March 24, 2011 Treatment of Latent TB Infection Renuka Khurana MD, MPH March 24, 2011 Renuka Khurana, MD, MPH has the following disclosures to make: No conflict of interests
Communicable Disease Control Manual Chapter 4: Tuberculosis
 Provincial TB Services 655 West 12th Avenue Vancouver, BC V5Z 4R4 www.bccdc.ca Communicable Disease Control Manual Definitions Page 1 2.0 DEFINITIONS Many of the definitions that follow are taken from
Provincial TB Services 655 West 12th Avenue Vancouver, BC V5Z 4R4 www.bccdc.ca Communicable Disease Control Manual Definitions Page 1 2.0 DEFINITIONS Many of the definitions that follow are taken from
New Standards for an Old Disease:
 New Standards for an Old Disease: Practical Implications of the TB Standards TB Prevention and Control Saskatchewan September 16, 2015 Practical Implications of the TB Standards Learning Objectives At
New Standards for an Old Disease: Practical Implications of the TB Standards TB Prevention and Control Saskatchewan September 16, 2015 Practical Implications of the TB Standards Learning Objectives At
Tuberculosis in Children and Adolescents 2017
 Tuberculosis in Children and Adolescents 2017 George D. McSherry, MD Division of Infectious Diseases Penn State Children s Hospital and Pediatric Section Northeastern Regional Training and Medical Consultation
Tuberculosis in Children and Adolescents 2017 George D. McSherry, MD Division of Infectious Diseases Penn State Children s Hospital and Pediatric Section Northeastern Regional Training and Medical Consultation
Gary Reubenson 16 October 2012 PAEDIATRIC TUBERCULOSIS: AN OVERVIEW IN 40 MINUTES!!
 Gary Reubenson 16 October 2012 PAEDIATRIC TUBERCULOSIS: AN OVERVIEW IN 40 MINUTES!! DECLARATION No relevant conflicts of interest to declare OVERVIEW Burden of disease & epidemiology Pathogenesis (not
Gary Reubenson 16 October 2012 PAEDIATRIC TUBERCULOSIS: AN OVERVIEW IN 40 MINUTES!! DECLARATION No relevant conflicts of interest to declare OVERVIEW Burden of disease & epidemiology Pathogenesis (not
Santa Clara County Tuberculosis Screening Requirement for School Entrance Effective June 1, 2014
 Guidelines to Revisions to the School Mandate and Requirements 1) What are the tuberculosis (TB) screening requirements for school entrance in Santa Clara County? Students must undergo a TB risk assessment
Guidelines to Revisions to the School Mandate and Requirements 1) What are the tuberculosis (TB) screening requirements for school entrance in Santa Clara County? Students must undergo a TB risk assessment
TB, or NOT TB? A Tough Question in Kids!
 TB, or NOT TB? A Tough Question in Kids! Brian Lee, MD Pediatric Tuberculosis Program Division of Infectious Diseases Ken Martin, MD Division of Radiology Overview Illustrate the range of clinical scenarios
TB, or NOT TB? A Tough Question in Kids! Brian Lee, MD Pediatric Tuberculosis Program Division of Infectious Diseases Ken Martin, MD Division of Radiology Overview Illustrate the range of clinical scenarios
TB in the Correctional Setting Florence, Arizona October 7, 2014
 TB in the Correctional Setting Florence, Arizona October 7, 2014 Diagnosis and Treatment of TB Disease Renuka Khurana, MBBS, MPH October 7, 2014 Renuka Khurana, MSSB, MPH has the following disclosures
TB in the Correctional Setting Florence, Arizona October 7, 2014 Diagnosis and Treatment of TB Disease Renuka Khurana, MBBS, MPH October 7, 2014 Renuka Khurana, MSSB, MPH has the following disclosures
Targeted Testing and the Diagnosis of. Latent Tuberculosis. Infection and Tuberculosis Disease
 Self-Study Study Modules on Tuberculosis Targeted Testing and the Diagnosis of Latent Tuberculosis Infection and Tuberculosis Disease 1 Module 3: Objectives At completion of this module, learners will
Self-Study Study Modules on Tuberculosis Targeted Testing and the Diagnosis of Latent Tuberculosis Infection and Tuberculosis Disease 1 Module 3: Objectives At completion of this module, learners will
TB Nurse Case Management San Antonio, Texas April 9-11, 2013
 TB Nurse Case Management San Antonio, Texas April 9-11, 2013 TB / Dose Counting Rachel Munoz, RN. TB Nurse Case Manager/Nurse Consultant Austin/Travis County Health Department April 10, 2013 Rachel Munoz,
TB Nurse Case Management San Antonio, Texas April 9-11, 2013 TB / Dose Counting Rachel Munoz, RN. TB Nurse Case Manager/Nurse Consultant Austin/Travis County Health Department April 10, 2013 Rachel Munoz,
Drug Interactions Lisa Armitige, MD, PhD November 17, 2010
 Substance Abuse and Tuberculosis Oklahoma City, Oklahoma November 17, 2010 Drug Interactions Lisa Armitige, MD, PhD November 17, 2010 Drug Interactions Lisa Y. Armitige, M.D., Ph.D. Medical Consultant
Substance Abuse and Tuberculosis Oklahoma City, Oklahoma November 17, 2010 Drug Interactions Lisa Armitige, MD, PhD November 17, 2010 Drug Interactions Lisa Y. Armitige, M.D., Ph.D. Medical Consultant
Jeffrey R. Starke, M.D. has the following disclosures to make:
 AAP 2018 Red Book Tuberculosis: IGRAs and Treatment of TB Infection Jeffrey R. Starke, M.D. May 31, 2018 AAP 2018 Red Book Childhood Tuberculosis: IGRAs and Treatment of TB Infection May 31, 2018 WEBINAR
AAP 2018 Red Book Tuberculosis: IGRAs and Treatment of TB Infection Jeffrey R. Starke, M.D. May 31, 2018 AAP 2018 Red Book Childhood Tuberculosis: IGRAs and Treatment of TB Infection May 31, 2018 WEBINAR
Barbara J Seaworth MD Medical Director, Heartland National TB Center Professor, Internal Medicine and Infectious Disease UT Health Northeast
 Practical Aspects for Using the Interferon Gamma Release Assay (IGRA) Test Live Webinar July 14, 2017 Barbara J Seaworth MD Medical Director, Heartland National TB Center Professor, Internal Medicine and
Practical Aspects for Using the Interferon Gamma Release Assay (IGRA) Test Live Webinar July 14, 2017 Barbara J Seaworth MD Medical Director, Heartland National TB Center Professor, Internal Medicine and
The Diagnosis of Active TB. Deborah McMahan, MD TB Intensive September 28, 2017
 The Diagnosis of Active TB Deborah McMahan, MD TB Intensive September 28, 2017 Agenda Epidemiology Big picture Conditions that Should Make You Suspicious Which test? Eeenie meenie miny mo Radiographic
The Diagnosis of Active TB Deborah McMahan, MD TB Intensive September 28, 2017 Agenda Epidemiology Big picture Conditions that Should Make You Suspicious Which test? Eeenie meenie miny mo Radiographic
Tuberculosis (TB) Fundamentals for School Nurses
 Fundamentals for School Nurses") Tuberculosis (TB) Fundamentals for School Nurses June 9, 2015 Kristin Gall, RN, MSN/Pat Infield, RN-TB Program Manager Marsha Carlson, RN, BSN Two Rivers Public Health Department Nebraska Department of
Tuberculosis (TB) Fundamentals for School Nurses June 9, 2015 Kristin Gall, RN, MSN/Pat Infield, RN-TB Program Manager Marsha Carlson, RN, BSN Two Rivers Public Health Department Nebraska Department of
Diagnosis of tuberculosis in children H Simon Schaaf
 Diagnosis of tuberculosis in children H Simon Schaaf Desmond Tutu TB Centre Department of Paediatrics and Child Health, Stellenbosch University, and Tygerberg Children s Hospital (TCH) Estimated TB incidence
Diagnosis of tuberculosis in children H Simon Schaaf Desmond Tutu TB Centre Department of Paediatrics and Child Health, Stellenbosch University, and Tygerberg Children s Hospital (TCH) Estimated TB incidence
LATENT TUBERCULOSIS. Robert F. Tyree, MD
 LATENT TUBERCULOSIS Robert F. Tyree, MD 1 YK TB OFFICERS Ron Bowerman Elizabeth Roll Mien Chyi (Pediatrics) Cindi Mondesir (Pediatrics) The new guys: Philip Johnson Robert Tyree 2009 CDC TB CASE DEFINITION
LATENT TUBERCULOSIS Robert F. Tyree, MD 1 YK TB OFFICERS Ron Bowerman Elizabeth Roll Mien Chyi (Pediatrics) Cindi Mondesir (Pediatrics) The new guys: Philip Johnson Robert Tyree 2009 CDC TB CASE DEFINITION
Dr Francis Ogaro MTRH ELDORET
 Dr Francis Ogaro MTRH ELDORET TB in children often severe, disseminated and can progress rapidly and with poor outcome TB diagnosis in children has relied on clinical, imaging, microscopy and TST findings.
Dr Francis Ogaro MTRH ELDORET TB in children often severe, disseminated and can progress rapidly and with poor outcome TB diagnosis in children has relied on clinical, imaging, microscopy and TST findings.
Treatment of Tuberculosis, 2017
 Treatment of Tuberculosis, 2017 Charles L. Daley, MD National Jewish Health University of Colorado Health Sciences Center Treatment of Tuberculosis Disclosures Advisory Board Horizon, Johnson and Johnson,
Treatment of Tuberculosis, 2017 Charles L. Daley, MD National Jewish Health University of Colorado Health Sciences Center Treatment of Tuberculosis Disclosures Advisory Board Horizon, Johnson and Johnson,
TUBERCULOSIS IN HEALTHCARE SETTINGS Diana M. Nilsen, MD, FCCP Director of Medical Affairs, Bureau of Tuberculosis Control New York City Department of
 TUBERCULOSIS IN HEALTHCARE SETTINGS Diana M. Nilsen, MD, FCCP Director of Medical Affairs, Bureau of Tuberculosis Control New York City Department of Health and Mental Hygiene TODAY S PRESENTATION Epidemiology
TUBERCULOSIS IN HEALTHCARE SETTINGS Diana M. Nilsen, MD, FCCP Director of Medical Affairs, Bureau of Tuberculosis Control New York City Department of Health and Mental Hygiene TODAY S PRESENTATION Epidemiology
Errors in Dx and Rx of TB
 Errors in Dx and Rx of TB David Schlossberg, MD, FACP Professor of Medicine Temple University School of Medicine Medical Director, TB Control Program Philadelphia Department of Public Health TB Still a
Errors in Dx and Rx of TB David Schlossberg, MD, FACP Professor of Medicine Temple University School of Medicine Medical Director, TB Control Program Philadelphia Department of Public Health TB Still a
Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010
 Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 What is Latent TB Infection (LTBI)? Traci Hadley, RN October 5, 2010 LTBI or TB Disease? Presented by : Traci Hadley, RN
Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 What is Latent TB Infection (LTBI)? Traci Hadley, RN October 5, 2010 LTBI or TB Disease? Presented by : Traci Hadley, RN
HIV prevalance in TB cases
 TUBERCULOSIS HIV prevalance in TB cases Top 5 AIDS indicative diseases; EUR, 2003 58% 35% 25% 11% 7% TB HIV wasting s. Candidiasis Rec. pneumonia HIV encephal. 26% 25% 31% 31% 16% 8% 7% 16% 14% 10% TB
TUBERCULOSIS HIV prevalance in TB cases Top 5 AIDS indicative diseases; EUR, 2003 58% 35% 25% 11% 7% TB HIV wasting s. Candidiasis Rec. pneumonia HIV encephal. 26% 25% 31% 31% 16% 8% 7% 16% 14% 10% TB
What you need to know about diagnosing and treating TB: a preventable, fatal disease. Bob Belknap M.D. Denver Public Health November 2013
 What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2013 Case 1: 52 y/o male Born in the Pacific Islands; some travel in
What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2013 Case 1: 52 y/o male Born in the Pacific Islands; some travel in
Evaluation and Management of the Patient with Latent Tuberculosis Infection (LTBI)
") Evaluation and Management of the Patient with Latent Tuberculosis Infection (LTBI) CURTIS FOWLER MPT,PA C ASSISTANT CLINICAL PROFESSOR UNIVERSITY OF THE PACIFIC Learning objectives Recognize the appropriate
Evaluation and Management of the Patient with Latent Tuberculosis Infection (LTBI) CURTIS FOWLER MPT,PA C ASSISTANT CLINICAL PROFESSOR UNIVERSITY OF THE PACIFIC Learning objectives Recognize the appropriate