Sagittal balance is important for biomechanical optimization
|
|
|
- Eugene Gerard Lewis
- 5 years ago
- Views:
Transcription
1 SPINE Volume 36, Number 3, pp E186 E , Lippincott Williams & Wilkins Quality Control of Reconstructed Sagittal Balance for Sagittal Imbalance Kao-Wha Chang, MD, PhD,* Xiangyang Leng, MD, Wenhai Zhao, MD, Ching-Wei Cheng, PhD, Tsung-Chein Chen, MD,* Ku-I Chang, MD,* and Yin-Yu Chen, MD* Study Design. Prospective radiographic study. Objective. To investigate the feasibility of controlling quality of reconstructed sagittal balance for sagittal imbalance. Summary of Background Data. Patients with sagittal imbalance cannot walk or stand erect without overwork of musculature because of compromised biomechanical advantage. The result is muscle fatigue and activity-related pain. During reconstructive surgery, restoration of optimal sagittal balance is crucial for obtaining satisfactory clinical results. However, there is no way to control quality of reconstructed sagittal balance before or during surgery. Methods. A method was developed to determine the lumbosacral curve in a way that theoretically would bring sagittal balance to an ideal state by calculation and simulation for each patient before surgery and then template rods of the curve and a blueprint were made accordingly for operative procedures. Ninety-four consecutive patients with sagittal imbalance due to lumbar kyphosis were treated for intractable pain and then followed up for a mean of 4.3 years. Radiographs were analyzed before surgery, 2 months after surgery, and at most recent follow-up. Results. The mean estimated values of L1 S1 lordosis, sacral inclination angle, sacrofemoral distance, and distribution of L1 S1 lordosis at the closing-opening wedge osteotomy site and L4 S1 segments were 30.8, 24.6, 0 mm, 16.1% ( 5 ), and 62% ( 19 ), respectively. The mean reconstructed values were 41.1, 23.3, 3.9 mm, 41% ( 17 ), and 46% ( 19 ), respectively. There were significant differences between estimated and reconstructed values of L1 S1 lordosis and the percentage of distributions; however, there was no significant difference between the estimated and reconstructed magnitude of L4 S1 lordosis, sacral inclination angle, and sacrofemoral distance. A properly oriented pelvis can be brought nearly directly above the hip axis. The mean sagittal global balance, represented by the distance between the vertical line through the hip axis and sacral promontory, improved from 61.4 mm before surgery to 3.9 mm 2 months after surgery, and 1.3 mm at final follow-up. Normal sagittal global balance was reconstructed and maintained. The mean sagittal spinal balance measured as the horizontal distance between the C7 sagittal plumb line and the posterior superior corner of S1 improved from 97.4 mm before surgery to 11 mm 2 months after surgery. However, there was significant loss of sagittal spinal balance to 25.4 mm at the final visit. Normal sagittal spinal balance was reconstructed and appeared to be maintained. The magnitude of T1 T12 kyphosis compensated from 13 before surgery to months after surgery and 34.5 at final follow-up. Conclusions. Quality control of the reconstructed sagittal balance for sagittal imbalance is possible. Correctly orienting the pelvis, reconstructed by the restoration of enough L1 S1 lordosis with adequate distribution at L4 S1 segments, is a matter of critical importance for optimizing reconstructed sagittal balance. The correctly oriented pelvis can be determined before surgery. Preventing junctional fracture and persistent rehabilitation of surgically injured lumbar extensor musculature are crucial for maintaining the reconstructed sagittal balance. Key words: pelvic orientation, sacral inclination angle, sagittal balance, sagittal imbalance. Spine 2011;36:E186 E197 Sagittal balance is important for biomechanical optimization of forces at segmental interspaces. Sagittal spinal balance has been historically quantified by measuring a vertical line from the center of the C7 vertebral body with respect to the posterior superior corner of S1. There is significant normal variation of lumbar lordosis and thoracic kyphosis in maintaining overall sagittal balance. 1 Jackson and From the *Taiwan Spine Center, Jen-Ai Hospital, Taichung, Taiwan, Republic Hales 2 described a congruent spinopelvic alignment, which of China; Department of Bio-Industrial Mechatronics Engineering, National Chung Hsing University, Taichung, Taiwan, Republic of China; and Affiliated defines the relationship among thoracic kyphosis, lumbar lordosis, and pelvic position. Sagittal plane malalignment is most Hospital of Changchun University of Chinese medicine, Changchun, Jilin, People s Republic of China. often clinically significant when there is loss of normal lordosis Acknowledgment date: March 30, Revision date: May 26, Acceptance date: June 29, of the lumbar spine. Excessive kyphosis across these mobile, unsupported segments increases intradiscal pressures and compromises the mechanical advantage of the erector spinae mus- The manuscript submitted does not contain information about medical device(s)/drug(s). No funds were received in support of this work. No benefits in any form have culature. 3 Clinically, the patient with sagittal imbalance presents with intractable pain, early fatigue, a subjective sense of been or will be received from a commercial party related directly or indirectly to the subject of this manuscript. imbalance and leaning forward, and difficulty with horizontal Address correspondence and reprint requests to Kao-Wha Chang, MD, PhD, gaze. Compensation can be gained by extension of the hips and Taiwan Spine Center, Jen-Ai Hospital, No. 483 Dong Rong Rd, Tali, Taichung, Taiwan, Republic of China; admin_c@taiwanspinecenter.com.tw flexion of the knees, although this causes increased fatigue. As DOI: /BRS.0b013e3181ef6828 patients age, muscular weakness, adjacent-disc degeneration, E186 February 2011
2 and hip and pelvic disease may decrease compensation and increase disability. Restoration of normal and economical sagittal balance reduces the work of the erector spinae and hamstring muscles to achieve balance during normal activity. During reconstructive surgery, restoration of optimal sagittal balance is crucial for obtaining satisfactory clinical results. 4 6 However, there is no way to control the quality of the reconstructed sagittal balance before or during surgery. We developed a method to determine the lumbosacral curve that theoretically would bring sagittal balance to an ideal state by calculation and simulation for each patient before surgery and made template rods of the curve and a blueprint accordingly for operative procedures to follow. The objective of this study was to evaluate the feasibility of the control quality of reconstructed sagittal balance for patients with sagittal imbalance by using this method. MATERIALS AND METHODS The medical records of 103 consecutive patients who underwent surgery according to the blueprints and with the utilization of the template rods for correction of sagittal imbalance by the same surgeon from 2003 to 2007 were reviewed. Three patients died of unrelated causes and six were lost to follow-up. The remaining 94 patients (73 women, 21 men; mean age, 64.7 years; range, years) were followed up for 2 to 6 years. Diagnoses included degenerative lumbar kyphosis (n 41), degenerative lumbar kyphoscoliosis (n 16), posttraumatic lumbar kyphosis (including osteoporotic compression fracture) (n 27), and iatrogenic lumbar kyphosis resulted from extensive neurologic decompression without instrumentation and fusion (n 10). We excluded patients with neuromuscular disease, ankylosing spondylitis, or flat-back syndrome with instrumented lumbar fusion and patients with lumbar kyphosis combined with weakness of lumbar extensors proved by inability to lift their trunk from the floor by the contraction of the extensor muscles in the prone position with their legs being fixed. The efficacy of a method to correct sagittal imbalance can be assessed by radiographic parameters and absolute correction. Preoperative, 2-month postoperative, and final followup radiographs were analyzed. One of the authors, who was independent of the surgical team, made all the radiographic measurements. Sagittal measurements were made on 36-inch standing lateral views of the entire spine and upper femur obtained with the hips and knees fully extended. Thoracic kyphosis was measured from the upper end plate of T1 to the lower end plate of T12, and lumbar lordosis was measured from the upper end plate of L1 to the upper end plate of S1. Positive values were used to denote kyphosis, and negative values were used to indicate lordosis. Sagittal global balance was measured as the horizontal distance between vertical lines through the hip axis (HA) and sacral promontory and was represented as sacrofemoral distance (SFD, positive values for femoral anterior to the promontory). The acceptable range of the reconstructed sagittal global balance was 2 to 2 cm (HA nearly under the promontory). Sagittal spinal balance was measured as the horizontal distance between the C7 sagittal plumb line and the posterior superior corner of S1. Because the posterosuperior aspect of the S1 body was Spine the reference, the normal neutral range for sagittal spinal balance was 3 cm or less from this point (plumb line through or behind the L5 S1 disc). Sacral inclination angle (SIA) was defined as the angle subtended by the sacral end plate and horizontal reference line (positive for anterior inclination). The proximal junctional angle was defined as the angle of the inferior end plate of the upper instrumented vertebrae (UIV) to the superior end plate of one suprajacent vertebra above the UIV. Abnormal proximal junctional kyphosis was defined by the proximal junction sagittal Cobb angle 10 or more and proximal junction sagittal Cobb angle being at least 10 higher than the preoperative measurement. Fracture of the UIV or one suprajacent vertebra above the UIV was noted as a junctional fracture. Segmental lordosis from L1 to S1 was measured by the Cobb method from the superior end plates of adjacent vertebrae and was used to distribute segmental lordosis of the determined lumbosacral curve. Closing-opening wedge osteotomy (COWO) angle was the segmental lordosis of the segment with COWO. L4 S1 lordosis was the Cobb angle between the superior end plates between L4 and S1. Magnetic resonance imaging was used to confirm spinal stenosis and identify neural compression (retropulsed bone or disc). All patients received the standard method of measuring bone density via dura-energy radiographic absorptiometry. Thirtyfour patients were osteopenic (T scores between 1.0 and 2.5) and 43 patients were osteoporotic (T scores 2.5). Seventeen patients had normal bone stock (T scores between 1 and 1). Paired t tests were used for continuous variables between time points and between estimated and reconstructed values. Statistical significance was set at P MAKING TEMPLATE RODS AND BLUEPRINT FOR SURGERY Identify the Center of Gravity Line The center of gravity (CG) is over the HA and normally directly under the promontory of the sacrum. 7 The CG line is a vertical line through the CG, and it was used as a guideline for the reconstruction of optimal sagittal balance in this study. The ideal sagittal balance to be reconstructed was to have a sagittal global balance with the CG directly under the promontory with SFD 0 (Figure 1A). Determine Pelvic Orientation Each person has a unique posture and spinopelvic balance with a particular set of sagittal alignment. Pelvic morphology has been shown to affect standing lumbosacral lordosis and pelvic balance significantly around the hips in studies involving both adult volunteers and patients with spinal disorders Measurements of pelvic morphology have been made by determining the approximate centers of the hip joints on lateral radiographs. 2 Jackson and Hales 2 described a specific pelvic radius technique, which involved locating a midpoint between the hip centers called the pelvic hip axis and drew a line from this axis to the posterior superior corner of S1. This line segment was named the pelvic radius (PR) because the sacrum rotated around the HA along an arc that can be E187



3 B A C D E188 February 2011 BRS indd 188 1/6/11 4:56 AM
, sacrofemoral distance (SFD), and sagittal spinal balance were 35, 9, 41 mm, and 150 mm, respectively.")

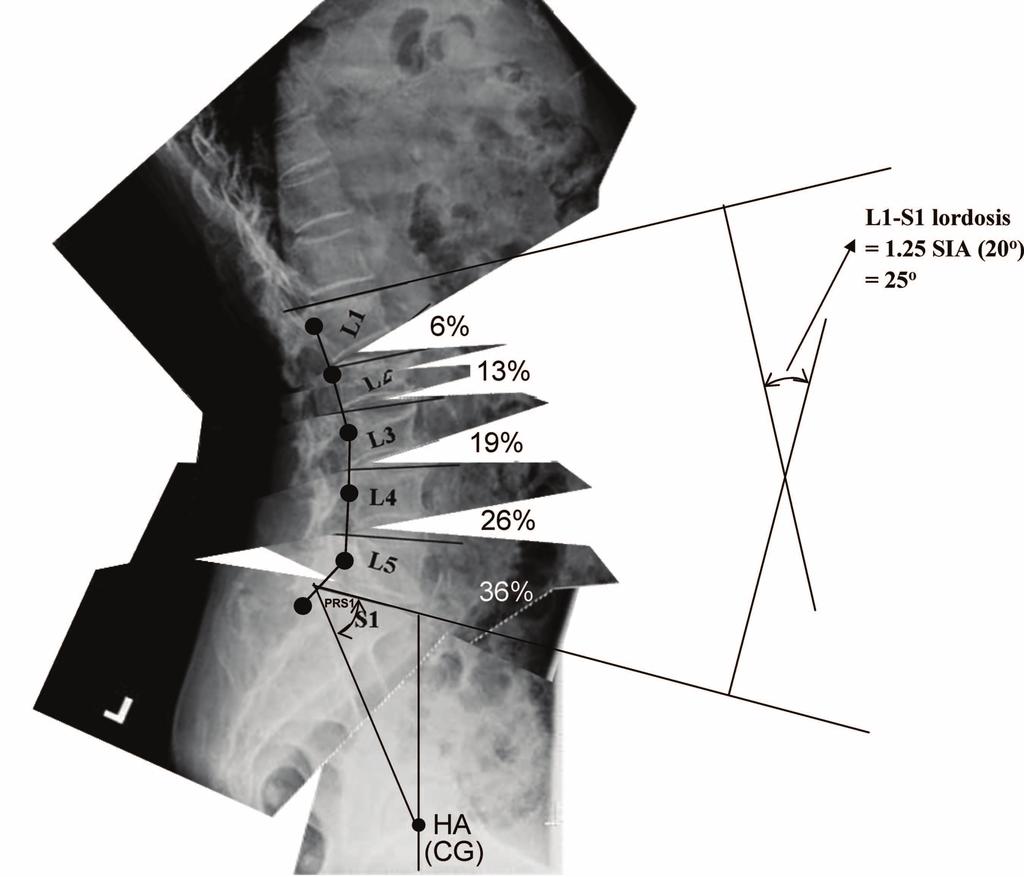
4 E F Figure 1. A representative example. A 67-year-old woman with iatrogenic lumbar kyphosis. The preoperative value of L1 S1 lordosis, sacral inclination angle (SIA), sacrofemoral distance (SFD), and sagittal spinal balance were 35, 9, 41 mm, and 150 mm, respectively. A, Identify the center of gravity line (CGL). Hip axis (HA) is the midpoint between the hip centers. The center of gravity (CG) is over the HA. The CGL is a vertical line through the CG and is a guideline for reconstruction of optimal sagittal balance. B, Determine pelvic orientation. The lumbopelvic portion of the standing radiograph was magnified to life size and the values of pelvic-radius length and pelvic radius-s1 angle were measured, which are constants for each patient. The lumbopelvic portion was divided into the hips and spinopelvic portion. Given the two anatomic constants and 0-mm SFD, pelvic orientation can be determined by translating and rotating the paper with the spinopelvic portion to a position with the values. C, Determine the lumbosacral curve. The Cobb angle between L1 and S1 is equal to the estimated L1 S1 lordosis. The lumbosacral curve was made approximately according to the reported distribution by simulation of operative procedures and motion behavior of vertebral segments. D, The template, a rod positioned 15 mm (the average length of the patient's lumbar pedicles) posterior to the curve and contoured to match the lumbosacral curve. The two marks on the rod would be connected to the pedicle screw of L1 and S1. The blueprint is for operative procedures to follow. E, After instrumentation-assisted correction with the template rod. The estimated values of L1 S1 lordosis, SIA, SFD, closing-opening wedge osteotomy angle, and L4 S1 lordosis were 25, 20, 0 mm, 3.3, and 15.5, respectively, as compared with the reconstructed values 27, 19, 0 mm, 11, and 14. F, Sagittal spinal and global balance improved from 150 mm and 41 mm before surgery to 0 mm and 0 mm 2 months after surgery. defined by this radial line. Intraobserver and interobserver assessments for lumbopelvic lordosis and sacropelvic alignment, as well as for pelvic morphology, have been reported as very reliable and reproducible by the PR technique. 2,12 Spine Individual pelvic anatomy should be constant in the adult and therefore not changing much over time. PR lengths and PRS1 angles are constants for each person 12 and should not change with pelvic rotation or sagittal translation. In adult volunteers E189
5 and in patients with spinal disorders, pelvic morphology and lumbosacral lordosis are strongly correlated and complementary in determining lumbopelvic lordosis, 12 which are strongly correlated with pelvic balance around the HA. The SFD determines pelvic balance. Therefore, given the two anatomic constants and 0-mm SFD, pelvic orientation can be determined. The lumbopelvic portion of the standing lateral radiograph was magnified to life size and printed on transparent paper, which was divided into the hips and spinopelvic portions. We located the HA and rotated and translated the paper, with the spinopelvic portion to a position with the original PR length and PRS1 angle (constants for each individual) 12 and with an SFD value of 0 mm. (The CG line normally is directly under the promontory 7 ). Pelvic orientation and the SIA could thus be identified (Figure 1B). Determine Lumbosacral Lordosis Spinal balance is conceived as the result of an optimal lordotic positioning of the vertebrae above a correctly oriented pelvis. 13 Kobayashi et al 11 substantiated their previous results showing that the strongest determinant of lumbar lordosis is sacral alignment. Appropriate lumbar lordosis was estimated to be 80% of sacral inclination by using standing radiographs. The study provides practical data for the assessment of sagittal spinal alignment. For L1 L5 lordosis, 40% are at L4 L5 in the aging spine. 14 L5 S1 lordosis/l4 L5 lordosis ave aged Total L1 S1 lordosis was estimated accordingly: L1 S1 lordosis ([SIA 0.8] 0.4) 1.4 SIA SIA. Determine the Lumbosacral Curve that Can Bring the Promontory Directly Above the Center of Gravity COWO 16 (Figure 2) and Smith-Peterson osteotomy (SPO) 17 were performed in this study to provide adequate release and flexibility for optimal correction. The apex of the lumbar kyphosis was usually between L2 and L4. The site of COWO for three-column release was as close to the apex as possible (usually L2 or L3) and also allowed enough segments below for rigid fixation. The site of COWO was located and marked on the paper of the spinopelvic portion. The spinopelvic portion was divided at the site of COWO and at each disc to simulate release provided by COWO and SPO. Each divided portion of the paper was rotated and translated with correction hinges, either at the pedicular base of the COWO vertebra to simulate closing and opening wedge of COWO or at the posterior border of each divided disc to simulate lordotic correction until the angle between superior end plate of L1 and S1 was equal to the estimated L1 S1 lordosis. For L1 L5 lordosis, the distribution of lordosis had been reported to be approximately 10% at L1 L2, 20% at L2 L3, 30% at L3 L4, and 40% at L4 L5 and L5 S1 lordosis/l4 L5 lordosis averaged Therefore, the distribution of L1 S1 lordosis was approximately 6% at L1 L2, 13% at L2 L3, 19% at L3 L4, 26% at L4 L5, and 36% at L5 S1. The estimated distribution of lordosis at the COWO segment of the determined lumbosacral curve would be either 13% if COWO was at L2 or 19% if COWO was at L3. The estimated distribution of lordosis at L4 S1 segments would be 62%. The lumbosacral curve connecting each pedicle base of L1 S1 was approximately made (Figure 1C). Make Template Rod and Blueprint for Reconstruction of Optimal Sagittal Balance The template, a rod, positioned at the distance of the average length of the patient's lumbar pedicles posterior to the curve and contoured to match the lumbosacral curve, was marked on points L1 and S1, which would be connected with pedicle Figure 2. Diagram of closing-opening wedge osteotomy. A, Lateral view outlines the bone block to be resected. B, Postoperative view shows that the correction is achieved by hinging on the closed middle column, closing the intravertebral osteotomy and creating an open wedge of the anterior column. E190 February 2011
6 screws of L1 and S1 (Figure 1D). In theory, the promontory of the sacrum could be brought near to the CG line if the lumbosacral curve could be reconstructed accordingly. Through simulation, the site of osteotomy was noted, and what corrective forces, such as translation, compression, distraction, or rotation, were required during correction was noted on the paper as a blueprint for operative procedures to follow (Figure 1D). The previously mentioned method of template generation can also be done on a computerized model instead of paper cutouts. (Figure 1) Surgery Patients were placed in the prone position with padding at the iliac crests, knees, shoulders, and chest. The abdomen was left free to reduce intraoperative bleeding. The osteotomy site (L2 or L3) was kept over the hinge in the table so that as the osteotomy was closed and the table could be moved from the neutral to V position. A standard posterior midline incision was made (usually from T10 to the sacrum). The spine was bilaterally exposed to the tip of the transverse processes with a strictly subperiosteal approach to reduce bleeding. Pedicle screws were inserted (usually from T10 to the sacrum and ilium except at the COWO level). Intraoperative lateral radiographs were used to adjust the length between the bases of the pedicle and screw head to be the average length of the patient's lumbar pedicles. Wide posterior decompression and formal lateral-recess decompression and foraminotomy of the involved stenotic levels were usually necessary to treat neurogenic claudication and pain. According to the blueprint, COWO 16 for threecolumn release was performed as close to the apical vertebra of the deformity as possible (either L2 or L3). Laminectomy and facetectomy at the level of osteotomy were performed. After both pedicles to be resected were identified, holes were made through them to the vertebral body and curettes were used to enlarge the holes. The transverse processes were excised at their bases. With angled curettes, the cancellous bone was pushed anteriorly into the body to create a cavity. The anterior, posterior, and lateral cortexes of the body were thinned with angled curettes, and both pedicles were enucleated with a small osteotome. The posterior cortex was then pushed down into the body. A rongeur was used to resect the appropriate lateral cortex bilaterally. The anterior cortex was weakened by bilateral penetration with a blunt-end cage trial to facilitate its fracture and opening during corrective procedures for patients with sagittal imbalance requiring large magnitude of correction. Correction was achieved by hinging on the closed middle column, closing the intravertebral osteotomy, and creating an open wedge of the anterior column of the osteotomized vertebra. Before correction, abundant autogenous bones from laminectomy and facetectomy were pushed into the anterior portion of intravertebral osteotomy as bone grafts for the open wedge of the anterior column created by correction. SPO was performed at the other levels for posterior release. These osteotomies provide enough flexibility for optimal correction. A template rod was connected to the pedicle screws with mark S1 connected to the S1 pedicle Spine screw and mark L1 connected to the L1 pedicle screw. The pedicle screws were long-arm pedicle screws. The ample space within the screw head and the flexibility of the rod allow the rod to connect to the screw heads. The operating table was slowly moved to a V position to facilitate correction and provide space for sagittal translation and rotation around the site of COWO and the HA. The rod was rotated to correct any scoliosis. The surgeon and assistant pushed the rod against the lumbosacral spine to transform kyphosis into lordosis and compressed the pedicle screws to each other to create lordosis between segments and thus create the lordotic lumbosacral curve (Figure 1E, F). The sacrum of the properly oriented pelvis, which had been brought above the HA, needed to be confirmed by intraoperative lateral radiographs. Wake-up tests were performed. Iliac screws were used for all arthrodeses. Anterior bone grafts were not routinely used for segments added to the arthrodesis. However, interbody fusion with wedge-shaped cages placed posteriorly for anterior-column support and fusion at L5 S1 were performed along with neurologic decompression procedures for 32 patients combined with spinal stenosis at L5 S1 because of the known difficulty of obtaining a long fusion to the sacrum. For patients with T scores less than 1.0, we augmented the UIV and its one suprajacent level with polymethylmethacrylate (PMMA) bone cement to prevent the junctional fracture (Figure 3). Patients ambulated 48 hours later and used custom-made thoracolumbar orthoses for 6 months. Rehabilitation of lumbar extensor musculature by standing straight as much as possible for 15 to 30 minutes every 2 hours during day time began 1 week after the operation. RESULTS The average preoperative T1 T12 kyphosis was 13. This increased to months after surgery and to 34.5 at the most recent follow-up. The average preoperative L1 S1 lordosis was The curve was corrected to months after surgery and to 40.4 at the most recent follow-up. Mean sagittal spinal balance improved from 97.4 mm before surgery to 11 mm 2 months after surgery. Normal sagittal spinal balances ( 3 mm) were reconstructed in 85 of the 94 patients. At the final postoperative visit, the mean sagittal balance increased to 25.4 mm, and there was a significant loss of the reconstructed sagittal spinal balance (P 0.01); however, the normal sagittal spinal balance appeared to be maintained. Mean SFD improved from 61.4 mm before surgery to 3.9 mm 2 months after surgery and to 1.3 mm at the final visit. Acceptable sagittal global balances (SFD 2 to 2 cm) were reconstructed in all patients. There were no significant differences in the mean value between the 2-month and most recent postoperative visits (P 0.3). Mean SIA improved from 5.4 before surgery to months after surgery and to 25.7 at final follow-up. There was no significant change of SIA at the final postoperative visit (P 0.4). COWO was performed at L2 in 46 patients and at L3 in 48 patients. The mean lordosis at the COWO site was 17 and 41% of the reconstructed L1 S1 lordosis 2 months after surgery. The mean estimated lordosis at the COWO site was E191

7 Figure 3. A 69-year-old woman with degenerative lumbar kyphosis. The preoperative values of L1 S1 lordosis, sacral inclination angle, sacrofemoral distance, and sagittal spinal balance were 17, 10, 74 mm, and 75 mm, respectively, compared with postoperative values 48, 30, 10 mm, and 0 mm. The upper instrumented vertebrae and its one suprajacent vertebra were augmented with polymethylmethacrylate bone cement to prevent junctional fracture. 5 and 16.1% of the reconstructed L1 S1 lordosis, which was significantly different from the reconstructed value. The mean postoperative L4 S1 lordosis was 19 and 46% of the reconstructed L1 S1 lordosis. The mean estimated lordosis at the L4 S1 segment was 19 and 62% of the reconstructed L1 S1 lordosis. The magnitude was not significantly different from the reconstructed value; however, the percentage of distribution was significantly different from the reconstructed value (P 0.01). The estimated L1 S1 lordosis was 30.8, which was significantly less than the reconstructed L1 S1 lordosis. The estimated values of SIA and SFD were 24.6 and 0 mm, respectively, which were not significantly different from the reconstructed values (23.3 and 3.9 mm). (Tables 1, 2) Only three patients developed junctional kyphosis. No junctional fracture occurred. DISCUSSION Patients with sagittal imbalance cannot stand erect without compensatory hip extension, knee flexion, and overwork of the erector spinae musculature because reduced moment arm compromises the mechanical advantage. The results are muscle fatigue and activity-related pain. As patients age, muscular weakness, adjacent-disc degeneration, and hip and pelvic disease may decrease compensation and increase disability. During reconstructive surgery, restoration of optimal sagittal balance is crucial for obtaining satisfactory clinical results. The spine should be fused in a balanced position, that is, as close to the normal configuration as possible, because insufficient deformity correction involving posterior instrumentation alone may lead to lost correction, pseudarthrosis, increased reoperation rates, or poor clinical results. 18,19 TABLE 1. Summary of Radiographic Data Measurement Preoperative Postoperative 2 Mo Last Follow-up Correction Loss of Correction T1 T12 kyphosis ( ) ( 13 to 22) (11 to 34) (18 to 41) (3 to 14)* (5.1 to 11.1)* L1 S1 lordosis ( ) ( 7 to 42) 41.1 ± 15 ( 21 to 51) 40.4 ± 13 ( 20 to 51) (31 to 78)* (0.3 to 2.5) Sagittal balance (mm) 97.4 ± 24.3 (23 to 193) ( 34 to 43) 25.4 ± 7.3 ( 31 to 51.3) (23 to 161)* (7.4 to 37.2) * SIA ( ) ( 12 to 13) (14 to 34) (13 to 34) (19 to 37)* (0.1 to 3.5) SFD (mm) 61.4 ± 17 (25 to 83) 3.9 ± 2.1 ( 13 to 19) ( 11 to 24) (25 to 83)* 2.6 ± 0.3 (0 to 5.1) Data are presented as the mean standard deviation (range). *P SFD indicates sacrofemoral distance or the distance between the plumb line through the hip axis and the sacral promontory; SIA, sacral inclination angle or the angle between the upper surface of the sacrum and the horizontal line. E192 February 2011
* Distribution COWO angle ( ) 5 ± 2.6 ( 3 to 7) 17 ± 5.7 ( 9 to 20) 12 ± 4.7 (8 to 18)* % of L1 S1 lordosis 16.1 41 ± 13.1 (33 to 57) 24.9 8 (16.9 to 40.9)* L4 S1 lordosis ( ) 19 ± 5.")
8 TABLE 2. Summary of Estimated and Reconstructed Data Estimated Value Postoperative 2 Mo Difference L1-S1 lordosis ( ) ( 19 to 43) ( 21 to 49) (1 to 18.3)* Distribution COWO angle ( ) 5 ± 2.6 ( 3 to 7) 17 ± 5.7 ( 9 to 20) 12 ± 4.7 (8 to 18)* % of L1 S1 lordosis ± 13.1 (33 to 57) (16.9 to 40.9)* L4 S1 lordosis ( ) 19 ± 5.8 ( 12 to 27) 19 ± 4.9 ( 10 to 23) 0 ± 1.1 ( 3 to 5) % of L1 S1 lordosis (39 to 52) (10 to 23)* SIA ( ) (15 to 34) (14 to 34) ( 2 to 2.5) SFD (mm) ( 13 to 19) ( 13 to 19) Data are presented as the mean ± standard deviation (range). *P COWO indicates closing-opening wedge osteotomy; SFD, sacrofemoral distance or the distance between the plumb line through the hip axis and the sacral promontory; SIA, sacral inclination angle or the angle between the upper surface of the sacrum and the horizontal line. Global sagittal spinal alignment has been historically quantified by measuring a vertical line from the center of the C7 vertebral body with respect to the posterior superior corner of S This sagittal vertical axis describes the cumulative balance of the sagittal spinal curves of the trunk but not the entire body, which occurs at the CG. Assessment of the gravity line is gaining interest among spine surgeons in the evaluation of sagittal global balance in normal subjects and in patients with spinal deformity The CG is near the axis through the hip for pelvic rotation and normally is directly under the promotory. 7 Some patients in this study presented with a lumbar kyphosis and a compensatory thoracic lordosis had a normal sagittal spinal balance and a severely abnormal sagittal global balance (Figure 4). Improved association of the spine, pelvis, and CG or economical sagittal balance reduces the work of the erector spinae and hamstring muscles to achieve balance during normal activity. According to normal standards, 2,7,11 all patients in this study had decreased inclination in the upper sacral surface, or backward rotation, which can be explained by compensated lumbar kyphosis. The line connecting both hip joints was far in front of the promontory, increasing the SFD. Even in natural standing, the lumbar extensors overworked to secure balance against a CG located far in front of the lumbosacral junction. Muscle fatigue, spasm, and pain are the clinical symptoms of attempted correction of truncal and whole-body imbalance. Correction of lumbar kyphosis and improvement of sagittal spinal balance without relocating the promontory close to the CG line do not relieve myogenic pain in lumbar kyphosis. Adult pelvic anatomy is stable, and the PR length and PRS1 angle are considered to be constant 12 and should not change with pelvic rotation or sagittal translation. In adult volunteers and in patients with spinal disorders, pelvic morphology and lumbosacral lordosis are strongly correlated and complementary in determining lumbopelvic lordosis, 12 which is strongly correlated with pelvic balance around the HA. The SFD determines pelvic balance and sacral inclination, which determines L1 S1 lordosis. Therefore, given the two anatomic Spine constants and 0-mm SFD, and simulated motion behavior of the kyphotic lumbar spine, which is adequately released by osteotomies during correction, a lumbosacral curve with reported distributions to bring the promontory close to the CG line theoretically could be approximately simulated. Because the caudal end of the construct was sacral and ilial, and because correction of lumbar kyphosis and restoration of lumbosacral lordosis were accomplished by pushing the template rods toward the V position of the operating table, the lumbar spine around the apex, which had been three-column Figure 4. A 57-year-old woman presented with a lumbar kyphosis and a compensatory thoracic lordosis had a normal sagittal spinal balance and a severely abnormal sagittal global balance. E193
9 released by COWO, translated anteriorly and the lumbopelvic segment caudal to the apex rotated around the HA. When the pelvis rotated anteriorly, the distance from the promontory to the CG line decreased and inclination of the upper sacral surface increased. Therefore, the SFD decreased and the SIA increased. All patients obtained significant decrease in SFDs and increase in the SIA. Because of the rigidity of the deformities, proper release is needed to provide adequate flexibility before posterior instrumentation-augmented correction can be successful. COWO is a three-column release procedure and is responsible for transforming kyphosis into lordosis by lengthening of the anterior column and shortening of the middle and posterior columns. SPO is a posterior column-only release procedure. The flexibility of a segment with COWO is more than the flexibility of the other segments provided by SPO. It is reasonable that the magnitude of correction obtained at the segment with COWO is the largest (41%) among all segmental lordoses of the reconstructed L1 S1 lordosis. Spinal balance is conceived as the result of an optimal lordotic positioning of the vertebral column above a correctly oriented pelvis. 13 Anatomically, the L4 S1 angle is an important source of lordosis in the lumbosacral spine and about two-thirds of an L1 S1 lordosis are distributed below L4 to maintain a correctly oriented pelvis. Correction by pushing the template rod, with 62% of the estimated L1 S1 lordosis being contoured into the portion of template rod connected to L4 S1 segments, obtained only 46% lordosis of the reconstructed L1 S1 lordosis at L4 S1 segments. This is 16% less than the before-surgery estimated distribution at L4 S1 segments. However, the reconstructed L1 S1 lordosis was 33% larger than the estimated L1 S1 lordosis. We believe that this was because of pushing the flexible and deformable template rod during correction. The magnitude of reconstructed L4 S1 lordosis was not significantly different from the estimated value of L4 S1 lordosis ( 19 vs. 19 ). Therefore, a properly oriented pelvis can be reconstructed according to the before-surgery made template and blueprint. We reconstructed a lumbosacral curve with L1 S1 lordosis of 41.1 and properly oriented pelvis with an SIA of 23.3, which improved sagittal spinal balance from 97.4 mm to 11 mm and improved sagittal global balance by decreasing the SFD from 61.4 to 3.9 mm. We approximated lumbopelvic and sagittal balance to the physiologic state. Although the method was approximate, the results demonstrated that it was efficient. We compared the estimated and reconstructed values of L1 S1 lordosis, L4 S1 lordosis, and the SIA. The reconstructed L1 S1 lordosis was 33% larger than the estimated L1 S1 lordosis, and the reconstructed L4 S1 lordosis was 16% less than the estimated L4 S1 lordosis, so the reconstructed L4 S1 lordosis and SIA were not significantly different from the estimated value. Evidently, the lumbar spine was comparatively overlordosed; however, optimal sagittal spinal and global balance were obtained. Sagittal balance is conceived as the result of an optimal lordotic positioning of the vertebrae above a correctly oriented pelvis. 30 On the basis of this study, a correctly oriented pelvis is probably more crucial than optimal lordotic positioning for quality control of optimal sagittal balance reconstruction. It is necessary to create enough L1 S1 lordosis with adequate distribution at L4 S1 segments to obtain a correctly oriented pelvis and optimal sagittal balance, sometimes at the expense of overcorrection of the lumbar spine. In this study, we excluded patients with ankylosing spondylitis or flat-back syndrome with instrumented lumbar fusion, because the fused L4 S1 segments, unlike motion behavior at L4 S1 segments in this series, would not accept enough distribution from reconstructed L1 S1 lordosis to obtain a correctly oriented pelvis during reconstructive surgery. However, the exclusion does not mean that this study is not helpful for these patients who represent a challenging group of patients that constitute a significant proportion of adult spinal deformity surgeons' practices. Additional release procedures at L4 S1 levels to provide adequate flexibility allow L4 S1 segments to accept enough lordosis for obtaining a correctly oriented pelvis and optimal sagittal balance. Of course, all these additional procedures would increase operation time, blood loss, and complications. Overlordosating the lumbar spine to distribute enough lordosis at L4 S1 segments is another option for these patients. However, more-severe proximal junctional problems and compensatory changes of the thoracic spine might compromise the reconstructed sagittal balance. The pelvic incidence 13 (PI) is defined as the angle between the line perpendicular to the sacral plate at its midpoint and the line connecting this point to the axis of the femoral heads. It is an anatomic parameter, unique to each individual, independent of the spatial orientation of the pelvis. This parameter can be considered as a constant because it is an anatomic one, independent of the position of the pelvis, and independent of the age, once growth is completed. PI is an important component of assessing and reconstructing the sagittal alignment. In fact, it determines it. In this study, we used PRS1 angle (the angle between PR and sacral plate) instead of PI, because PRS1 angle is much easier to be identified and measured than PI. Jackson and Hales 2 demonstrated that PRS1 angle was one of the most reliable radiographic measurements of pelvic morphology. PRS1 angle can be utilized in place of PI and is based on the following mathematical calculation (A) and mechanic analysis (B). A. Mathematical Calculation 1. According to the law of sine, principle of trigonometry states that the lengths of the sides of any triangle are proportional to the sines of the opposite angles, when a, b, and c are the sides and A, B, and C are the opposite angles. 2. Refer to Figure 5 and the triangle OAB, OBA BOA OBA 180, the angle (i.e., PI) is a constant, because AD is perpendicular to BC, so the angle OAB 90 is a constant. The length of AB 1 2 BC is a constant, angle BOA is a constant, the angle BOA 180 OBA OAB, the angle OAB is E194 February 2011
10 Figure 5. Point O is the hip axis. Point B is the posterosuperior corner of sacrum. Point A is the midpoint of sacral plate. Point C is promontory of sacrum. BC is sacral plate. AD is perpendicular to BC. OB is pelvic radius. Angle is pelvic incidence. Angle is PRS1 angle. constant, and the angle OBA (i.e., PRS1 angle) is a constant. The previous calculation demonstrates that because PI is a constant, PRS1 angle is a constant. B. Mechanic Analysis The PI (angle ) is an anatomic parameter. The anatomic components involved in the make-up of this parameter were the first three sacral vertebrae, the sacroiliac joints, and the posterior segment of the iliac bone. HA was considered to be a fixed or stationary reference point as the hinge of motion. The mobility of sacroiliac joint is considered negligible. According to this characteristic property, we can assume that it is a rigid-body; any rigid-body displacement can be considered to be a combination of a rigid-body translation and a rigid-body rotation. The resulting displacements are such that there is no change in the distance between any two points in the body and in any way of moving in rigid-body motion in a fixed axis or plane; all the points maintain the relative distance, and the relative position between points stays the same. 31 In this case, the angle (i.e., PI) and angle (i.e., PRS1 angle) are constants and the distance between any two arbitrary points of the body is constant and should not change with pelvic rotation or sagittal translation (Figure 6). On the basis of the above calculation and analysis, both PI and PRS1 are constants and should not change with pelvis rotation or sagittal translation. The ideal sagittal balance to be reconstructed was to have a sagittal global balance with the CG directly under the promontory, with SFD 0 (Figure 1A). Given the two anatomic constants (PR and PRS1 angle instead of PI) and 0-mm SFD, pelvic orientation to be reconstructed could be determined before surgery. The results of this study demonstrated that optimal sagittal balance could be reconstructed for sagittal imbalance if the pelvic orientation could be reconstructed accordingly. There was no significant loss of correction of the reconstructed lumbosacral curve. With the aid of abundant bone grafting the anterior portion of intravertebral osteotomy before correction as bone grafts for the open wedge of the anterior column of the osteomized vertebra created by correction, the union of the anterior open wedge of the anterior column is like the union of a close fracture with rigid fixation, which is fast and definite. During union period, there might be some loss of correction; we believe that it should be minimal. At the level of L5 S1, anterior-column support and anterior bone grafting reduced but did not eliminate the complications Figure 6. The anatomic construct of pelvic incidence can be considered as a rigid body. Pelvic incidence (angle ) and PRS1 angle (angle ) stay the same, no matter pelvis moves around the hinge (Point O, the hip axis). The illustrations show that angle and angle stay the same while the pelvis is rotating 15 and translating posteriorly, staying in neutral position, or rotating 15 and translating anteriorly. Spine E195
11 such as pseudarthrosis and rods breakage. So, it was not our routine practice to perform structural grafting at L5 S1 through anterior approach. Interbody fusion, with wedge-shaped cages placed posteriorly for anterior-column support, and grafting with high concentrations of autogenous bone and bone morphogenetic protein anteriorly and posteriorly at L5 S1 were performed along with neurologic decompression procedures for patients combined with spinal stenosis at L5 S1 because of the known difficulty of obtaining a long fusion to the sacrum. For patients with fusion of long segments, and especially for osteoporotic patients, increased motion and stress concentration at a junctional area can induce junctional failure at or above the UIV and adjacent-disc degeneration, leading to junctional kyphosis. Junctional fracture and kyphosis may result in catastrophic neurologic injury, significant loss of sagittal balance, and require reoperation for progressive junctional kyphosis or neurologic deficit. In this study, the lumbar spine was overlordosed; hence, more-severe proximal segmental junctional problems might occur. Preventing the occurrence of junctional problems is crucial for maintaining the reconstructed sagittal balance. DeWald and Stanley 32 believe that the occurrence of junctional kyphosis is an inevitable consequence of multilevel instrumentation in patients with poor bone stock. They suggested that a potential approach to this problem was to perform limited fusion with the intention of staging proximal extension as the junctional kyphosis progresses. On the basis of our observation of 33 osteoporotic patients who were older than 65 years, had a T score less than 2.5, had a fusion of long segments, and were followed up for an average of 3.7 years, 26% developed junctional fracture and 29% developed junctional kyphosis, whereas among 46 patients who were older than 65 years, had a T score less than 2.5, had long-segment fusion with PMMA augmentation of UIV and its one suprajacent vertebra to prevent junctional fracture, and were followed up for 4.7 years, none had junctional fracture and nine (20%) developed junctional kyphosis. The cause of junctional kyphosis was suprajacent disc degeneration rather than junctional fracture, so the severity of junctional kyphosis was diminished. We also observed 43 patients older than 65 year who had osteopenia (T score 0.1) with fusion of long segments and found that 8% developed junctional fracture and 11% developed junctional kyphosis. In this study, PMMA augmentation of UIV (usually T10) and its one suprajacent vertebra was performed to prevent junctional fracture for osteopenia or osteoporotic patients with a T score less than 1. No junctional failure occurred, and 13 (14%) patients developed junctional kyphosis because of suprajacent disc degeneration. This technique could effectively prevent junctional failure and minimize the severity of junctional kyphosis and the risk of jeopardizing the reconstructed sagittal balance. The primary cause of lumbar kyphosis might be the following: (1) decline of the anterior elements, multiple disc narrowing, and vertebral wedging or collapse; (2) weakness and loosening of the posterior elements and atrophy of the extensor muscles; (3) combined factors. 7 Spinal alignment can be reconstructed surgically; however, sagittal balance cannot be restored in the presence of weak and atrophic extensor spinal musculature. Therefore, in this study, we excluded patients with neuromuscular disease and those with lumbar kyphosis who could not lift their trunks from the floor by contraction of the extensor muscles in the prone position with legs being fixed. Undoubtedly, the severe reconditioning of the lumbar extensor musculature that occurs as the result of the posterior exposure influences the patient's ability to stand erect. Postoperative rehabilitation of the lumbar extensor muscles is crucial for maintaining the reconstructed sagittal balance and should be started as early as possible and continued. The average increase of the thoracic sagittal Cobb angle between T1 and T12 at 2 months after surgery was 25.2 and at final follow-up was Although how the thoracic spine would change above was unpredictable and there were significant compensatory changes of the thoracic spine above and significant loss of sagittal spinal balance, the optimal reconstructed sagittal global and spinal balance appeared to be maintained by effective prevention of occurrence of junctional failure and persistent rehabilitation of extensor spinal musculature. CONCLUSION Quality control of the reconstructed sagittal balance for surgical treatment of sagittal imbalance is possible. A correctly oriented pelvis, which can be determined before surgery, reconstructed by restoration of enough L1 S1 lordosis with adequate distribution at L4 S1 segments is a matter of critical importance for optimizing reconstructed sagittal balance. Prevention of junctional fracture and persistent rehabilitation of surgically injured lumbar extensor musculature are crucial for maintaining reconstructed sagittal balance. Key Points The lumbosacral curve that theoretically would bring sagittal balance to an ideal state for each patient with sagittal imbalance due to lumbar kyphosis can be determined before surgery by calculation and simulation. Optimal sagittal balance can be reconstructed by using the template rod of the lumbosacral curve. A correctly oriented pelvis, which can be determined before surgery, reconstructed by restoration of enough L1 S1 lordosis with adequate distribution at L4 S1 segments is a matter of critical importance for optimizing reconstructed sagittal balance. Quality control of the reconstructed sagittal balance for sagittal imbalance is feasible. References 1. Bernhardt M, Bridwell KI. Segmental analysis of the sagittal plane alignment of the normal thoracic and lumbar spines and thoracolumbar junction. Spine 1989;14: Jackson RP, Hales C. Congruent spinopelvic alignment on standing lateral radiographs of adult volunteers. Spine 2000;25: White AA, Panjabi MM. Practical biomechanics of scoliosis and kyphosis. In: White AA, Panjabi MM, eds. Clinical biomechanics of the spine. Philadelphia, PA: Lippincott-Raven; 1990: E196 February 2011
12 4. Mac-Thiong JM, Transfeldt EE, Mehbod AA, et al. Can C7 plumbline and gravity line predict health related quality of life in adult scoliosis? Spine 2009;34:E Glassman SD, Berven S, Bridwell K, et al. Correlation of radiographic parameters and clinical symptoms in adult scoliosis. Spine 2005;30: Glassman SD, Bridwell K, Dimar JR, et al. The impact of positive sagittal balance in adult spinal deformity. Spine 2005;30: Takemitsu Y, Harada Y, Iwahava T, et al. Lumbar degenerative kyphosis. Clinical, radiological and epidemiological studies. Spine 1988;13: Jackson PR, Peterson MD, McManus AC, et al. Compensatory spinopelvic balance over the hip axis and better reliability in measuring lordotic to the pelvic radius on standing lateral radiographs of adult volunteers and patients. Spine 1998;16: During J, Goudfrooij H, Keessen W, et al. Toward standards for posture. Postural characteristics of the lower back system in normal and pathologic conditions. Spine 1985;10: Jackson PR. Spinal balance, lumbopelvic alignments around the hip axis and positioning for surgery. Spine State Art Rev 1997;11: Kobayashi T, Atsuta Y, Matsuno T, et al. A longitudinal study of congruent sagittal spinal alignment in an adult cohort. Spine 2004;29: Jackson RP, Kanemura T, Kawakami N, et al. Lumbopelvic lordosis and pelvic balance on repeated standing lateral radiographs of adult volunteers and untreated patients with constant low back pain. Spine 2000;25: Legaye J, Duval-Beaupere G, Hecquct J, et al. Pelvic incidence: a fundamental pelvic parameter three-dimensional regulation of spinal sagittal curves. Eur Spine J 1998:7; Hammerberg EM, Wood KB. Sagittal profile of the elderly. J Spinal Disord Tech 2003;16: Jackson RP, McManus AC. Radiographic analysis of sagittal plane alignment and balance in standing volunteers and patients with low back pain matched for age, sex, and size: a prospective controlled clinical study. Spine 1994;19: Chang KW, Cheng CW, Chen HC, et al. Closing-opening wedge osteotomy for the treatment of sagittal imbalance. Spine 2008;33: Smith-Peterson MN, Larson CB, Aufranc OE. Osteotomy of the spine for correction of flexion deformity in rheumatoid arthritis. Clin Orthop Relat Res 1969;66: Grubb SA, Lipscomb HJ. Diagnostic findings in painful adult scoliosis. Spine 1992;17: Bradford DS, Tay BK, Hu SS. Adult scoliosis: surgical indications, operative management, complications, and outcomes. Spine 1999;24: Gelb DE, Lenke LG, Bridwell KH, et al. An analysis of sagittal spinal alignment in 100 asymptomatic middle and older aged volunteers. Spine 1995;20: Van Royen BJ, Toussaint HM, Kingma I, et al. Accuracy of the sagittal vertical axis in a standing lateral radiograph as a measurement of balance in spinal deformities. Eur Spine J 1998;7: Vedantam R, Lenke LG, Bridwell KH, et al. The effect of variation in arm position on sagittal spinal alignment. Spine 2000;25: Roussouly P, Gollogly S. Noseda O, et al. The vertical projection of the sum of the ground reactive forces of a standing patient is not the same as the C7 plumb line: a radiographic study of the sagittal alignment of 153 asymptomatic volunteers. Spine 2006;31:E Gangnet N, Pornero V, Dumas R, et al. Variability of the spine and pelvis location with respect to the gravity line: a three-dimensional stereoradiographic study using force platform. Surg Radiol Anat 2003;25: Legaye J, Duval-Beaupere G. Gravitational forces and sagittal shape of the spine. Clinical estimation of their relations. Int Orthop 2008;32: Schwab F, Lafage V, Boyce R, et al. Gravity line analysis in adult volunteers: age-related correlation with spinal parameters, pelvic parameters, and foot position. Spine 2006;31:E Allard P, Chavet P, Barbier F, et al. Effect of body morphology on standing balance in adolescent idiopathic scoliosis. Am J Phys Med Rebabil 2004;83: El Fegoun AB, Schwab F, Gamez L, et al. Center of gravity and radiographic posture analysis: a preliminary review of adult volunteers and adult patients affected by scoliosis. Spine 2005;30: Geiger EV, Müller O, Niemeyer T, et al. Adjustment of pelvispinal parameters preserves the constant gravity line position. Int Orthop 2007;31: Nash ML, Allard P, Hinse S, et al. Relations between standing stability and body posture parameters in adolescent idiopathic scoliosis. Spine 2002;27: Jansson PA, Grahn R. Engineering Mechanics: Vol. 2, Dynamics. Hemel Hempstead, Hertfordshire, United Kingdom: Prentice Hall International;1995: DeWald CJ, Stanley T. Instrumentation-related complications of multilevel fusions for adult spinal deformity patients over age 65. Spine 2006;31:S Spine E197
Quality Control of Reconstructed Sagittal Balance for Sagittal Imbalance
 Quality Control of Reconstructed Sagittal Balance for Sagittal Imbalance 3 Kao-Wha Chang Taiwan Spine Center, Taichung Jen-Ai Hospital, Taiwan, Republic of China 1. Introduction Sagittal balance is important
Quality Control of Reconstructed Sagittal Balance for Sagittal Imbalance 3 Kao-Wha Chang Taiwan Spine Center, Taichung Jen-Ai Hospital, Taiwan, Republic of China 1. Introduction Sagittal balance is important
Spinal deformities, such as increased thoracic
 An Original Study Clinical and Radiographic Evaluation of Sagittal Imbalance: A New Radiographic Assessment Hossein Elgafy, MD, MCh, FRCS Ed, FRCSC, Rick Bransford, MD, Hassan Semaan, MD, and Theodore
An Original Study Clinical and Radiographic Evaluation of Sagittal Imbalance: A New Radiographic Assessment Hossein Elgafy, MD, MCh, FRCS Ed, FRCSC, Rick Bransford, MD, Hassan Semaan, MD, and Theodore
Closing-Opening Wedge Osteotomy for the Treatment of Sagittal Imbalance
 Input-gn SPINE Volume 33, Number 13, pp 000 000 2008, Lippincott Williams & Wilkins Closing-Opening Wedge Osteotomy for the Treatment of Sagittal Imbalance Kao-Wha Chang, MD,* Ching-Wei Cheng, PhD, Hung-Chang
Input-gn SPINE Volume 33, Number 13, pp 000 000 2008, Lippincott Williams & Wilkins Closing-Opening Wedge Osteotomy for the Treatment of Sagittal Imbalance Kao-Wha Chang, MD,* Ching-Wei Cheng, PhD, Hung-Chang
Flatback Syndrome. Pathologic Loss of Lumbar Lordosis
 Flatback Syndrome Pathologic Loss of Lumbar Lordosis Robert P. Norton, MD Florida Spine Specialists Orthopaedic Spine Surgery Clinical Associate Professor, FAU College of Medicine Boca Raton, FL Courtesy
Flatback Syndrome Pathologic Loss of Lumbar Lordosis Robert P. Norton, MD Florida Spine Specialists Orthopaedic Spine Surgery Clinical Associate Professor, FAU College of Medicine Boca Raton, FL Courtesy
5/27/2016. Sagittal Balance What is It and How Did We Get Here? Sagittal Balance. Steven J. Tresser, MD Tampa, FL. Concept:
 Sagittal Balance What is It and How Did We Get Here? Steven J. Tresser, MD Tampa, FL Number of Articles Published on Sagittal Balance/Alignment by Year 350 300 250 200 150 100 50 0 Sagittal Balance Concept:
Sagittal Balance What is It and How Did We Get Here? Steven J. Tresser, MD Tampa, FL Number of Articles Published on Sagittal Balance/Alignment by Year 350 300 250 200 150 100 50 0 Sagittal Balance Concept:
Sagittal balance analysis after pedicle subtraction osteotomy in ankylosing spondylitis
 DOI 10.1007/s00586-011-1929-9 ORIGINAL ARTICLE Sagittal balance analysis after pedicle subtraction osteotomy in ankylosing spondylitis Romain Debarge Guillaume Demey Pierre Roussouly Received: 11 July
DOI 10.1007/s00586-011-1929-9 ORIGINAL ARTICLE Sagittal balance analysis after pedicle subtraction osteotomy in ankylosing spondylitis Romain Debarge Guillaume Demey Pierre Roussouly Received: 11 July
Idiopathic scoliosis Scoliosis Deformities I 06
 What is Idiopathic scoliosis? 80-90% of all scolioses are idiopathic, the rest are neuromuscular or congenital scolioses with manifest primary diseases responsible for the scoliotic pathogenesis. This
What is Idiopathic scoliosis? 80-90% of all scolioses are idiopathic, the rest are neuromuscular or congenital scolioses with manifest primary diseases responsible for the scoliotic pathogenesis. This
Surgical treatment for adult spinal deformity: Conceptual approach and surgical strategy
 REVIEW ARTICLE SPINE SURGERY AND RELATED RESEARCH Surgical treatment for adult spinal deformity: Conceptual approach and surgical strategy Yukihiro Matsuyama Department of Orthopedic Surgery, Hamamatsu
REVIEW ARTICLE SPINE SURGERY AND RELATED RESEARCH Surgical treatment for adult spinal deformity: Conceptual approach and surgical strategy Yukihiro Matsuyama Department of Orthopedic Surgery, Hamamatsu
Postoperative Change of Thoracic Kyphosis after Corrective Surgery for Adult Spinal Deformity
 ORIGINAL ARTICLE SPINE SURGERY AND RELATED RESEARCH Postoperative Change of Thoracic Kyphosis after Corrective Surgery for Adult Spinal Deformity Tatsuya Yasuda 1), Tomohiko Hasegawa 2), Yu Yamato 2),
ORIGINAL ARTICLE SPINE SURGERY AND RELATED RESEARCH Postoperative Change of Thoracic Kyphosis after Corrective Surgery for Adult Spinal Deformity Tatsuya Yasuda 1), Tomohiko Hasegawa 2), Yu Yamato 2),
Proximal junctional kyphosis in adult spinal deformity with long spinal fusion from T9/T10 to the ilium
 Original Study Proximal junctional kyphosis in adult spinal deformity with long spinal fusion from T9/T10 to the ilium Tatsuya Yasuda, Tomohiko Hasegawa, Yu Yamato, Sho Kobayashi, Daisuke Togawa, Shin
Original Study Proximal junctional kyphosis in adult spinal deformity with long spinal fusion from T9/T10 to the ilium Tatsuya Yasuda, Tomohiko Hasegawa, Yu Yamato, Sho Kobayashi, Daisuke Togawa, Shin
The Influence of Spinal Deformities on Acetabular Orientation in Total Hip Arthroplasty
 The Influence of Spinal Deformities on Acetabular Orientation in Total Hip Arthroplasty S. SAMUEL BEDERMAN MD PhD FRCSC Scoliosis & Spine Tumor Center S. SAMUEL BEDERMAN MD PhD FRCSC disclosures October
The Influence of Spinal Deformities on Acetabular Orientation in Total Hip Arthroplasty S. SAMUEL BEDERMAN MD PhD FRCSC Scoliosis & Spine Tumor Center S. SAMUEL BEDERMAN MD PhD FRCSC disclosures October
The Kickstand Rod technique for correction of coronal imbalance in patients with adult spinal deformity: theory and technical considerations
 Case Report The Kickstand Rod technique for correction of coronal imbalance in patients with adult spinal deformity: theory and technical considerations Melvin C. Makhni 1, Meghan Cerpa 2, James D. Lin
Case Report The Kickstand Rod technique for correction of coronal imbalance in patients with adult spinal deformity: theory and technical considerations Melvin C. Makhni 1, Meghan Cerpa 2, James D. Lin
Long lumbar instrumented fusions have been described
 SPINE Volume 37, Number 16, pp 1407 1414 2012, Lippincott Williams & Wilkins SURGERY Upper Instrumented Vertebral Fractures in Long Lumbar Fusions What Are the Associated Risk Factors? Stephen J. Lewis,
SPINE Volume 37, Number 16, pp 1407 1414 2012, Lippincott Williams & Wilkins SURGERY Upper Instrumented Vertebral Fractures in Long Lumbar Fusions What Are the Associated Risk Factors? Stephen J. Lewis,
Implementation of Pre-operative Planning:
 Implementation of Pre-operative Planning: 1-Year Results Using Patient-Specific UNiD Rods in Adult Deformity C.J. Kleck, MD 06/16/2017 Pre-operative Planning In the fields of observation chance favors
Implementation of Pre-operative Planning: 1-Year Results Using Patient-Specific UNiD Rods in Adult Deformity C.J. Kleck, MD 06/16/2017 Pre-operative Planning In the fields of observation chance favors
ASJ. Characteristics of Sagittal Spino-Pelvic Alignment in Japanese Young Adults. Asian Spine Journal. Introduction
 Asian Spine Journal Asian Spine Clinical Journal Study Asian Spine J 2014;8(5):599-604 Sagittal http://dx.doi.org/10.4184/asj.2014.8.5.599 spino-pelvic alignment 599 Characteristics of Sagittal Spino-Pelvic
Asian Spine Journal Asian Spine Clinical Journal Study Asian Spine J 2014;8(5):599-604 Sagittal http://dx.doi.org/10.4184/asj.2014.8.5.599 spino-pelvic alignment 599 Characteristics of Sagittal Spino-Pelvic
Could Structural and Noncompensatory Lenke 3 and 4C Lumbar Curves Be Nonstructural and Compensatory?
 SPINE Volume 39, Number 22, pp 1850-1859 2014, Lippincott Williams & Wilkins DEFORMITY Could Structural and Noncompensatory Lenke 3 and 4C Lumbar Curves Be Nonstructural and Compensatory? Lenke 1, 2, 3,
SPINE Volume 39, Number 22, pp 1850-1859 2014, Lippincott Williams & Wilkins DEFORMITY Could Structural and Noncompensatory Lenke 3 and 4C Lumbar Curves Be Nonstructural and Compensatory? Lenke 1, 2, 3,
Original Article Clinics in Orthopedic Surgery 2018;10:
 Original Article Clinics in Orthopedic Surgery 2018;10:322-327 https://doi.org/10.4055/cios.2018.10.3.322 Spinopelvic Orientation on Radiographs in Various Body Postures: Upright Standing, Chair Sitting,
Original Article Clinics in Orthopedic Surgery 2018;10:322-327 https://doi.org/10.4055/cios.2018.10.3.322 Spinopelvic Orientation on Radiographs in Various Body Postures: Upright Standing, Chair Sitting,
Changes of Sagittal Spinopelvic Parameters in Normal Koreans with Age over 50
 Asian Spine Journal Vol. 4, No. 2, pp 96~101, 2010 doi:10.4184/asj.2010.4.2.96 Changes of Sagittal Spinopelvic Parameters in Normal Koreans with Age over 50 Kyu-Bok Kang 1, Youngjung J Kim 2, Nasir Muzaffar
Asian Spine Journal Vol. 4, No. 2, pp 96~101, 2010 doi:10.4184/asj.2010.4.2.96 Changes of Sagittal Spinopelvic Parameters in Normal Koreans with Age over 50 Kyu-Bok Kang 1, Youngjung J Kim 2, Nasir Muzaffar
Selective fusion in adolescent idiopathic scoliosis: a radiographic evaluation of risk factors for imbalance
 J Child Orthop (2015) 9:153 160 DOI 10.1007/s11832-015-0653-0 ORIGINAL CLINICAL ARTICLE Selective fusion in adolescent idiopathic scoliosis: a radiographic evaluation of risk factors for imbalance D. Studer
J Child Orthop (2015) 9:153 160 DOI 10.1007/s11832-015-0653-0 ORIGINAL CLINICAL ARTICLE Selective fusion in adolescent idiopathic scoliosis: a radiographic evaluation of risk factors for imbalance D. Studer
Posture. Kinesiology RHS 341 Lecture 10 Dr. Einas Al-Eisa
 Posture Kinesiology RHS 341 Lecture 10 Dr. Einas Al-Eisa Posture = body alignment = the relative arrangement of parts of the body Changes with the positions and movements of the body throughout the day
Posture Kinesiology RHS 341 Lecture 10 Dr. Einas Al-Eisa Posture = body alignment = the relative arrangement of parts of the body Changes with the positions and movements of the body throughout the day
The effect of body mass index on lumbar lordosis on the Mizuho OSI Jackson spinal table
 35 35 40 The effect of body mass index on lumbar lordosis on the Mizuho OSI Jackson spinal table Authors Justin Bundy, Tommy Hernandez, Haitao Zhou, Norman Chutkan Institution Orthopaedic Department, Medical
35 35 40 The effect of body mass index on lumbar lordosis on the Mizuho OSI Jackson spinal table Authors Justin Bundy, Tommy Hernandez, Haitao Zhou, Norman Chutkan Institution Orthopaedic Department, Medical
Department of Neurosurgery, St. Elisabeth Hospital, Warsaw, Poland 3
 Signature: Pol J Radiol, 2017; 82: 287-292 DOI: 10.12659/PJR.899975 CASE REPORT Received: 2016.06.08 Accepted: 2016.09.05 Published: 2017.05.28 Authors Contribution: A Study Design B Data Collection C
Signature: Pol J Radiol, 2017; 82: 287-292 DOI: 10.12659/PJR.899975 CASE REPORT Received: 2016.06.08 Accepted: 2016.09.05 Published: 2017.05.28 Authors Contribution: A Study Design B Data Collection C
ASSESSMENT OF SPINO-PELVIC MORPHOMETRY, A PREDICTOR OF LUMBOSACRAL INSTABILITY
 Research article 45 East African Orthopaedic Journal ASSESSMENT OF SPINO-PELVIC MORPHOMETRY, A PREDICTOR OF LUMBOSACRAL INSTABILITY J.M. Muthuuri, MBChB, MMed (Surg), H.Dip.Orth (SA), FCS (ECSA), Consultant
Research article 45 East African Orthopaedic Journal ASSESSMENT OF SPINO-PELVIC MORPHOMETRY, A PREDICTOR OF LUMBOSACRAL INSTABILITY J.M. Muthuuri, MBChB, MMed (Surg), H.Dip.Orth (SA), FCS (ECSA), Consultant
Update on Assessment of Normal Sagittal Spinal Alignment
 3 rd Annual International Spinal Deformity Symposium November 3-4, 2017 Update on Assessment of Normal Sagittal Spinal Alignment Justin S. Smith, MD, PhD Harrison Distinguished Professor Department of
3 rd Annual International Spinal Deformity Symposium November 3-4, 2017 Update on Assessment of Normal Sagittal Spinal Alignment Justin S. Smith, MD, PhD Harrison Distinguished Professor Department of
When is Degenerative Disease Really Deformity
 When is Degenerative Disease Really Deformity Cabo State of Spine Surgery Think Tank June 2017 Gurvinder S. Deol, MD Wake Orthopaedics/WakeMed Health and Hospitals Clinical Assistant Professor Department
When is Degenerative Disease Really Deformity Cabo State of Spine Surgery Think Tank June 2017 Gurvinder S. Deol, MD Wake Orthopaedics/WakeMed Health and Hospitals Clinical Assistant Professor Department
Adolescent Idiopathic Scoliosis
 Adolescent Idiopathic Scoliosis Surgical Treatment Comparisons By: Dr. Alex Rabinovich and Dr. Devin Peterson Options 1. Pedicle Screws versus Hooks 2. Posterior versus Anterior Instrumentation 3. Open
Adolescent Idiopathic Scoliosis Surgical Treatment Comparisons By: Dr. Alex Rabinovich and Dr. Devin Peterson Options 1. Pedicle Screws versus Hooks 2. Posterior versus Anterior Instrumentation 3. Open
Adult Spinal Deformity: Principles of Surgical Correction
 Adult Spinal Deformity: Principles of Surgical Correction S. Samuel Bederman, MD PhD FRCSC Department of Orthopaedic Surgery California Orthopaedic Association, Indian Wells, CA April 25, 2015 2 3 4 Adult
Adult Spinal Deformity: Principles of Surgical Correction S. Samuel Bederman, MD PhD FRCSC Department of Orthopaedic Surgery California Orthopaedic Association, Indian Wells, CA April 25, 2015 2 3 4 Adult
Degenerative spondylolisthesis at the L4 L5 in a 32-year-old female with previous fusion for idiopathic scoliosis: A case report
 Journal of Orthopaedic Surgery 2003: 11(2): 202 206 Degenerative spondylolisthesis at the L4 L5 in a 32-year-old female with previous fusion for idiopathic scoliosis: A case report RB Winter Clinical Professor,
Journal of Orthopaedic Surgery 2003: 11(2): 202 206 Degenerative spondylolisthesis at the L4 L5 in a 32-year-old female with previous fusion for idiopathic scoliosis: A case report RB Winter Clinical Professor,
Simultaneous anterior vertebral column resection-distraction and posterior rod contouring for restoration of sagittal balance: report of a technique
 Case Report Simultaneous anterior vertebral column resection-distraction and posterior rod contouring for restoration of sagittal balance: report of a technique Shaishav Bhagat 1, Alexander Z. E. Durst
Case Report Simultaneous anterior vertebral column resection-distraction and posterior rod contouring for restoration of sagittal balance: report of a technique Shaishav Bhagat 1, Alexander Z. E. Durst
ASJ. Radiologic and Clinical Courses of Degenerative Lumbar Scoliosis (10 25 ) after a Short-Segment Fusion. Asian Spine Journal.
 after a Short-Segment Fusion. Asian Spine Journal.") Asian Spine Journal 570 Kyu Yeol Clinical Lee et al. Study Asian Spine J 2017;11(4):570-579 https://doi.org/10.4184/asj.2017.11.4.570 Asian Spine J 2017;11(4):570-579 Radiologic and Clinical Courses of
Asian Spine Journal 570 Kyu Yeol Clinical Lee et al. Study Asian Spine J 2017;11(4):570-579 https://doi.org/10.4184/asj.2017.11.4.570 Asian Spine J 2017;11(4):570-579 Radiologic and Clinical Courses of
Raymond Wiegand, D.C. Spine Rehabilitation Institute of Missouri
 2D Pattern matching of frontal plane radiograph to 3D model identifies structural and functional deficiencies of the spinal pelvic system in consideration of mechanical spine pain (AKA Spine distortion
2D Pattern matching of frontal plane radiograph to 3D model identifies structural and functional deficiencies of the spinal pelvic system in consideration of mechanical spine pain (AKA Spine distortion
Louis Boissière Anouar Bourghli Jean-Marc Vital Olivier Gille Ibrahim Obeid. Introduction
 Eur Spine J (2013) 22:1339 1345 DOI 10.1007/s00586-013-2711-y ORIGINAL ARTICLE The lumbar lordosis index: a new ratio to detect spinal malalignment with a therapeutic impact for sagittal balance correction
Eur Spine J (2013) 22:1339 1345 DOI 10.1007/s00586-013-2711-y ORIGINAL ARTICLE The lumbar lordosis index: a new ratio to detect spinal malalignment with a therapeutic impact for sagittal balance correction
Correlation of Radiographic Parameters and Clinical Symptoms in Adult Scoliosis
 Correlation of Radiographic Parameters and Clinical Symptoms in Adult Scoliosis SPINE Volume 30, Number 6, pp 682 688 2005, Lippincott Williams & Wilkins, Inc. Steven D. Glassman, MD,* Sigurd Berven, MD,
Correlation of Radiographic Parameters and Clinical Symptoms in Adult Scoliosis SPINE Volume 30, Number 6, pp 682 688 2005, Lippincott Williams & Wilkins, Inc. Steven D. Glassman, MD,* Sigurd Berven, MD,
Focal Correction of Severe Fixed Kyphosis with Single Level Posterior Ponte Osteotomy and Interbody Fusion
 Open Access Case Report DOI: 10.7759/cureus.653 Focal Correction of Severe Fixed Kyphosis with Single Level Posterior Ponte Osteotomy and Interbody Fusion Seth S. Molloy 1, Faiz U. Ahmad 2, Griffin R.
Open Access Case Report DOI: 10.7759/cureus.653 Focal Correction of Severe Fixed Kyphosis with Single Level Posterior Ponte Osteotomy and Interbody Fusion Seth S. Molloy 1, Faiz U. Ahmad 2, Griffin R.
Spinal Deformity Pathologies and Treatments
 Spinal Deformity Pathologies and Treatments Scoliosis Spinal Deformity 3-dimensional deformity affecting all 3 planes Can be difficult to visualize with 2-dimensional radiographs Kyphosis Deformity affecting
Spinal Deformity Pathologies and Treatments Scoliosis Spinal Deformity 3-dimensional deformity affecting all 3 planes Can be difficult to visualize with 2-dimensional radiographs Kyphosis Deformity affecting
Adult degenerative scoliosis: Is it worth the risk?
 3 rd Annual UCSF Techniques in Complex Spine Surgery Las Vegas, NV Nov 8-9 th 2013 Adult degenerative scoliosis: Is it worth the risk? Jens R. Chapman, M.D. HansJörg Wyss Professor and Chair Department
3 rd Annual UCSF Techniques in Complex Spine Surgery Las Vegas, NV Nov 8-9 th 2013 Adult degenerative scoliosis: Is it worth the risk? Jens R. Chapman, M.D. HansJörg Wyss Professor and Chair Department
LIV selection in selective thoracic fusions
 Russian Research Institute for Traumatology and Orthopedics named after R.R.Vreden, St.Petersburg LIV selection in selective thoracic fusions Ptashnikov D. Professor, The chief of spine surgery & oncology
Russian Research Institute for Traumatology and Orthopedics named after R.R.Vreden, St.Petersburg LIV selection in selective thoracic fusions Ptashnikov D. Professor, The chief of spine surgery & oncology
ACE s Essentials of Exercise Science for Fitness Professionals TRUNK
 ACE s Essentials of Exercise Science for Fitness Professionals TRUNK Posture and Balance Posture refers to the biomechanical alignment of the individual body parts and the orientation of the body to the
ACE s Essentials of Exercise Science for Fitness Professionals TRUNK Posture and Balance Posture refers to the biomechanical alignment of the individual body parts and the orientation of the body to the
Change of Sagittal Spinopelvic Parameters after Selective and Non-Selective Fusion in Lenke Type 1 Adolescent Idiopathic Scoliosis Patients
 DOI: 10.5137/1019-5149.JTN.22557-18.2 Received: 13.01.2018 / Accepted: 09.04.2018 Published Online: 24.04.2018 Turk Neurosurg, 2018 Original Investigation Change of Sagittal Spinopelvic Parameters after
DOI: 10.5137/1019-5149.JTN.22557-18.2 Received: 13.01.2018 / Accepted: 09.04.2018 Published Online: 24.04.2018 Turk Neurosurg, 2018 Original Investigation Change of Sagittal Spinopelvic Parameters after
Prevention and management of iatrogenic flatback deformity
 Washington University School of Medicine Digital Commons@Becker Open Access Publications 8-1-2004 Prevention and management of iatrogenic flatback deformity Benjamin K. Potter Walter Reed Army Medical
Washington University School of Medicine Digital Commons@Becker Open Access Publications 8-1-2004 Prevention and management of iatrogenic flatback deformity Benjamin K. Potter Walter Reed Army Medical
Posture and balance. Center of gravity. Dynamic nature of center of gravity. John Milton BIO-39 November 7, 2017
 Posture and balance John Milton BIO-39 November 7, 2017 Center of gravity The center of gravity (COG) of the human body lies approximately at the level of the second sacral vertebrae (S2), anterior to
Posture and balance John Milton BIO-39 November 7, 2017 Center of gravity The center of gravity (COG) of the human body lies approximately at the level of the second sacral vertebrae (S2), anterior to
The normal standing posture with least energy expenditure
 CLINICAL ARTICLE J Neurosurg Spine 27:74 80, 2017 The impact of spinopelvic morphology on the short-term outcome of pedicle subtraction osteotomy in 104 patients Karin Eskilsson, MD, 1 Deep Sharma, MS,
CLINICAL ARTICLE J Neurosurg Spine 27:74 80, 2017 The impact of spinopelvic morphology on the short-term outcome of pedicle subtraction osteotomy in 104 patients Karin Eskilsson, MD, 1 Deep Sharma, MS,
Original Article Selection of proximal fusion level for degenerative scoliosis and the entailing proximal-related late complications
 Int J Clin Exp Med 2015;8(4):5731-5738 www.ijcem.com /ISSN:1940-5901/IJCEM0006438 Original Article Selection of proximal fusion level for degenerative scoliosis and the entailing proximal-related late
Int J Clin Exp Med 2015;8(4):5731-5738 www.ijcem.com /ISSN:1940-5901/IJCEM0006438 Original Article Selection of proximal fusion level for degenerative scoliosis and the entailing proximal-related late
Pedicle subtraction osteotomy for the treatment of fixed sagittal imbalance: Surgical technique.
 Washington University School of Medicine Digital Commons@Becker Open Access Publications 3-1-2004 Pedicle subtraction osteotomy for the treatment of fixed sagittal imbalance: Surgical technique. Keith
Washington University School of Medicine Digital Commons@Becker Open Access Publications 3-1-2004 Pedicle subtraction osteotomy for the treatment of fixed sagittal imbalance: Surgical technique. Keith
Management of fractures of the pedicle after instrumentation with transpedicular screws
 Management of fractures of the pedicle after instrumentation with transpedicular screws A REPORT OF THREE PATIENTS F. Lattig, T. F. Fekete, D. Jeszenszky From the Schulthess Clinic, Zürich, Switzerland
Management of fractures of the pedicle after instrumentation with transpedicular screws A REPORT OF THREE PATIENTS F. Lattig, T. F. Fekete, D. Jeszenszky From the Schulthess Clinic, Zürich, Switzerland
Catastrophic Dropped Head Syndrome Requiring Multiple Reconstruction Surgeries after Cervical Laminoplasty
 CASE REPORT SPINE SURGERY AND RELATED RESEARCH Catastrophic Dropped Head Syndrome Requiring Multiple Reconstruction Surgeries after Cervical Laminoplasty Seiichi Odate, Jitsuhiko Shikata and Tsunemitsu
CASE REPORT SPINE SURGERY AND RELATED RESEARCH Catastrophic Dropped Head Syndrome Requiring Multiple Reconstruction Surgeries after Cervical Laminoplasty Seiichi Odate, Jitsuhiko Shikata and Tsunemitsu
Screws versus hooks: implant cost and deformity correction in adolescent idiopathic scoliosis
 J Child Orthop (2012) 6:137 143 DOI 10.1007/s11832-012-0400-8 ORIGINAL CLINICAL ARTICLE Screws versus hooks: implant cost and deformity correction in adolescent idiopathic scoliosis Bradley P. Jaquith
J Child Orthop (2012) 6:137 143 DOI 10.1007/s11832-012-0400-8 ORIGINAL CLINICAL ARTICLE Screws versus hooks: implant cost and deformity correction in adolescent idiopathic scoliosis Bradley P. Jaquith
Prevention of PJF: Surgical Strategies to Reduce PJF. Robert Hart, MD Professor OHSU Orthopaedics Portland OR. Conflicts
 Prevention of PJF: Surgical Strategies to Reduce PJF Robert Hart, MD Professor OHSU Orthopaedics Portland OR Conflicts Consultant Depuy Spine, Medtronic Royalties Seaspine, Depuy Research/Fellowship Support
Prevention of PJF: Surgical Strategies to Reduce PJF Robert Hart, MD Professor OHSU Orthopaedics Portland OR Conflicts Consultant Depuy Spine, Medtronic Royalties Seaspine, Depuy Research/Fellowship Support
Sagittal Balance 5/19/2017. Disclosures. Radiographic Assessment And Surgical Goals
 Sagittal Balance Radiographic Assessment And Surgical Goals Steven J. Tresser, MD Disclosures Nuvasive consultant, royalties, speaking K2M consultant, royalties Centinel Spine consultant, speaking CTL
Sagittal Balance Radiographic Assessment And Surgical Goals Steven J. Tresser, MD Disclosures Nuvasive consultant, royalties, speaking K2M consultant, royalties Centinel Spine consultant, speaking CTL
Respecting and restoring the sagittal. profile in spinal surgery
 Respecting and restoring the sagittal profile in spinal surgery Jwalant S. Mehta MBBS, D Orth, MCh (Orth), FRCS (Tr & Orth) Consultant Spine Surgeon Swansea Spinal Unit ABMU Health Board Outline Why this
Respecting and restoring the sagittal profile in spinal surgery Jwalant S. Mehta MBBS, D Orth, MCh (Orth), FRCS (Tr & Orth) Consultant Spine Surgeon Swansea Spinal Unit ABMU Health Board Outline Why this
Clinical Biomechanics in Spinal Surgery
 Disclosure Clinical Biomechanics in Spinal Surgery Joseph S. Cheng, M.D., M.S. Associate Professor of Neurological Surgery and Orthopedic Surgery Director, Neurosurgery Spine Program I have no relevant
Disclosure Clinical Biomechanics in Spinal Surgery Joseph S. Cheng, M.D., M.S. Associate Professor of Neurological Surgery and Orthopedic Surgery Director, Neurosurgery Spine Program I have no relevant
Lumbar degenerative spinemodalities
 Lumbar degenerative spinemodalities of treatment Prof. dr Mirza Bišćević Spine department, Orthopedics What should we accept as normal siutuation? - morphologic abnormalities in the lumbar spine are common
Lumbar degenerative spinemodalities of treatment Prof. dr Mirza Bišćević Spine department, Orthopedics What should we accept as normal siutuation? - morphologic abnormalities in the lumbar spine are common
Patient Information. ADULT SCOLIOSIS Information About Adult Scoliosis, Symptoms, and Treatment Options
 Patient Information ADULT SCOLIOSIS Information About Adult Scoliosis, Symptoms, and Treatment Options Table of Contents Anatomy of the Spine...2 What is Adult Scoliosis...4 What are the Causes of Adult
Patient Information ADULT SCOLIOSIS Information About Adult Scoliosis, Symptoms, and Treatment Options Table of Contents Anatomy of the Spine...2 What is Adult Scoliosis...4 What are the Causes of Adult
There is No Remarkable Difference Between Pedicle Screw and Hybrid Construct in the Correction of Lenke Type-1 Curves
 DOI: 10.5137/1019-5149.JTN.20522-17.1 Received: 11.04.2017 / Accepted: 12.07.2017 Published Online: 21.09.2017 Original Investigation There is No Remarkable Difference Between Pedicle Screw and Hybrid
DOI: 10.5137/1019-5149.JTN.20522-17.1 Received: 11.04.2017 / Accepted: 12.07.2017 Published Online: 21.09.2017 Original Investigation There is No Remarkable Difference Between Pedicle Screw and Hybrid
Can pelvic tilt be restored by spinal osteotomy in ankylosing spondylitis patients with thoracolumbar kyphosis? A minimum follow-up of 2 years
 Wang et al. Journal of Orthopaedic Surgery and Research (2018) 13:172 https://doi.org/10.1186/s13018-018-0874-2 RESEARCH ARTICLE Can pelvic tilt be restored by spinal osteotomy in ankylosing spondylitis
Wang et al. Journal of Orthopaedic Surgery and Research (2018) 13:172 https://doi.org/10.1186/s13018-018-0874-2 RESEARCH ARTICLE Can pelvic tilt be restored by spinal osteotomy in ankylosing spondylitis
Lumbosacral Fixation Using the Diagonal S2 Screw for Long Fusion in Degenerative Lumbar Deformity: Technical Note Involving 13 Cases
 Technical Note Clinics in Orthopedic Surgery 2013;5:225-229 http://dx.doi.org/10.4055/cios.2013.5.3.225 Lumbosacral Fixation Using the Diagonal S2 Screw for Long Fusion in Degenerative Lumbar Deformity:
Technical Note Clinics in Orthopedic Surgery 2013;5:225-229 http://dx.doi.org/10.4055/cios.2013.5.3.225 Lumbosacral Fixation Using the Diagonal S2 Screw for Long Fusion in Degenerative Lumbar Deformity:
FUNDAMENTAL SEATING PRINCIPLES Power Point PDF Bengt Engström Physiotherapist. Concept ENGSTRÖM
 FUNDAMENTAL SEATING PRINCIPLES Power Point PDF Bengt Engström Physiotherapist Starting with a few questions! How are your clients sitting? What kind of problems do you see? How long time are your clients
FUNDAMENTAL SEATING PRINCIPLES Power Point PDF Bengt Engström Physiotherapist Starting with a few questions! How are your clients sitting? What kind of problems do you see? How long time are your clients
Spinal Terminology Basics
 Spinal Terminology Basics Anterior The front portion of the body. It is often used to indicate the position of one structure relative to another. Annulus Fibrosus The outer, fibrous, ring like portion
Spinal Terminology Basics Anterior The front portion of the body. It is often used to indicate the position of one structure relative to another. Annulus Fibrosus The outer, fibrous, ring like portion
Biomechanics of compensatory mechanisms in spinal-pelvic complex
 Journal of Physics: Conference Series PAPER OPEN ACCESS Biomechanics of compensatory mechanisms in spinal-pelvic complex To cite this article: D V Ivanov et al 2018 J. Phys.: Conf. Ser. 991 012036 View
Journal of Physics: Conference Series PAPER OPEN ACCESS Biomechanics of compensatory mechanisms in spinal-pelvic complex To cite this article: D V Ivanov et al 2018 J. Phys.: Conf. Ser. 991 012036 View
Patient Information MIS LLIF. Lateral Lumbar Interbody Fusion Using Minimally Invasive Surgical Techniques
 Patient Information MIS LLIF Lateral Lumbar Interbody Fusion Using Minimally Invasive Surgical Techniques Table of Contents Anatomy of Spine...2 General Conditions of the Spine....4 What is Spondylolisthesis....5
Patient Information MIS LLIF Lateral Lumbar Interbody Fusion Using Minimally Invasive Surgical Techniques Table of Contents Anatomy of Spine...2 General Conditions of the Spine....4 What is Spondylolisthesis....5
Vertebral column decancellation for the management of sharp angular spinal deformity
 Eur Spine J (2011) 20:1703 1710 DOI 10.1007/s00586-011-1771-0 ORIGINAL ARTICLE Vertebral column decancellation for the management of sharp angular spinal deformity Yan Wang Lawrence G. Lenke Received:
Eur Spine J (2011) 20:1703 1710 DOI 10.1007/s00586-011-1771-0 ORIGINAL ARTICLE Vertebral column decancellation for the management of sharp angular spinal deformity Yan Wang Lawrence G. Lenke Received:
ASJ. Surgical Treatment of Adult Degenerative Scoliosis. Asian Spine Journal. Introduction. Classification of Adult Scoliosis
 Asian Spine Journal Asian Spine Review Journal Article Asian Spine J Surgical 2014;8(3):371-381 treatment of http://dx.doi.org/10.4184/asj.2014.8.3.371 adult degenerative scoliosis 371 Surgical Treatment
Asian Spine Journal Asian Spine Review Journal Article Asian Spine J Surgical 2014;8(3):371-381 treatment of http://dx.doi.org/10.4184/asj.2014.8.3.371 adult degenerative scoliosis 371 Surgical Treatment
Fixed Sagittal Plane Imbalance
 Global Spine Journal Review Article 287 Jason W. Savage 1 Alpesh A. Patel 1 1 Department of Orthopaedic Surgery, Northwestern University Feinberg School of Medicine, Chicago, Illinois, United States Global
Global Spine Journal Review Article 287 Jason W. Savage 1 Alpesh A. Patel 1 1 Department of Orthopaedic Surgery, Northwestern University Feinberg School of Medicine, Chicago, Illinois, United States Global
Adult Spinal Deformity Robert Hart. Dept. Orthopaedics and Rehab OHSU
 Adult Spinal Deformity 2010 Robert Hart Dept. Orthopaedics and Rehab OHSU What is Adult Spinal Deformity? Untreated Idiopathic Scoliosis Flat Back Syndrome Adjacent Segment Stenosis Non-Union Degenerative
Adult Spinal Deformity 2010 Robert Hart Dept. Orthopaedics and Rehab OHSU What is Adult Spinal Deformity? Untreated Idiopathic Scoliosis Flat Back Syndrome Adjacent Segment Stenosis Non-Union Degenerative
J. C. Le Huec, S. Aunoble, Leijssen Philippe & Pellet Nicolas
 Pelvic parameters: origin and significance J. C. Le Huec, S. Aunoble, Leijssen Philippe & Pellet Nicolas European Spine Journal ISSN 0940-6719 Volume 20 Supplement 5 Eur Spine J (2011) 20:564-571 DOI 10.1007/s00586-011-1940-1
Pelvic parameters: origin and significance J. C. Le Huec, S. Aunoble, Leijssen Philippe & Pellet Nicolas European Spine Journal ISSN 0940-6719 Volume 20 Supplement 5 Eur Spine J (2011) 20:564-571 DOI 10.1007/s00586-011-1940-1
SKELETAL AWARENESS & DEXTERITY. Update, Misnomers & Insights for Non-Specific Low Back Pain
 SKELETAL AWARENESS & DEXTERITY Spondylolisthesis I: Update, Misnomers & Insights for Non-Specific Low Back Pain Robert Burgess BEd, PT, PhD, Huggins Hospital Newsletter# 7 January 2015 Isthmic Spondylolisthesis
SKELETAL AWARENESS & DEXTERITY Spondylolisthesis I: Update, Misnomers & Insights for Non-Specific Low Back Pain Robert Burgess BEd, PT, PhD, Huggins Hospital Newsletter# 7 January 2015 Isthmic Spondylolisthesis
Using Biomechanical Principles in the Management of Complex Postural Deviations in Sitting
 Using Biomechanical Principles in the Management of Complex Postural Deviations in Sitting ISS 2016 / Part 2 Managing Complex Postures KELLY WAUGH, PT, MAPT, ATP S E N I O R I N S T R U C TO R / C L I
Using Biomechanical Principles in the Management of Complex Postural Deviations in Sitting ISS 2016 / Part 2 Managing Complex Postures KELLY WAUGH, PT, MAPT, ATP S E N I O R I N S T R U C TO R / C L I
Analysis of instrumentation failures after three column osteotomies of the spine
 Kavadi et al. Scoliosis and Spinal Disorders (2017) 12:19 DOI 10.1186/s13013-017-0127-x RESEARCH Open Access Analysis of instrumentation failures after three column osteotomies of the spine Niranjan Kavadi
Kavadi et al. Scoliosis and Spinal Disorders (2017) 12:19 DOI 10.1186/s13013-017-0127-x RESEARCH Open Access Analysis of instrumentation failures after three column osteotomies of the spine Niranjan Kavadi
Asymmetric T5 Pedicle Subtraction Osteotomy (PSO) for complex posttraumatic deformity
 for complex posttraumatic deformity") Eur Spine J (2013) 22:2130 2135 DOI 10.1007/s00586-013-2942-y OPEN OPERATING THEATRE (OOT) Asymmetric T5 Pedicle Subtraction Osteotomy (PSO) for complex posttraumatic deformity Ibrahim Obeid Fethi Laouissat
Eur Spine J (2013) 22:2130 2135 DOI 10.1007/s00586-013-2942-y OPEN OPERATING THEATRE (OOT) Asymmetric T5 Pedicle Subtraction Osteotomy (PSO) for complex posttraumatic deformity Ibrahim Obeid Fethi Laouissat
Maintenance of sagittal and coronal balance has
 Neurosurg Focus 36 (5):E14, 2014 AANS, 2014 Limitations and ceiling effects with circumferential minimally invasive correction techniques for adult scoliosis: analysis of radiological outcomes over a 7-year
Neurosurg Focus 36 (5):E14, 2014 AANS, 2014 Limitations and ceiling effects with circumferential minimally invasive correction techniques for adult scoliosis: analysis of radiological outcomes over a 7-year
Royal Oak IBFD System Surgical Technique Posterior Lumbar Interbody Fusion (PLIF)
") Royal Oak IBFD System Surgical Technique Posterior Lumbar Interbody Fusion (PLIF) Preoperative Planning Preoperative planning is necessary for the correct selection of lumbar interbody fusion devices.
Royal Oak IBFD System Surgical Technique Posterior Lumbar Interbody Fusion (PLIF) Preoperative Planning Preoperative planning is necessary for the correct selection of lumbar interbody fusion devices.
Pelvic Evaluation in Thoracolumbar Corrective Spine Surgery: How I Do It 1
 This copy is for personal use only. To order printed copies, contact reprints@rsna.org REVIEWS AND COMMENTARY n HOW I DO IT Ryan D. Murtagh, MD, MBA Robert M. Quencer, MD Juan Uribe, MD Pelvic Evaluation
This copy is for personal use only. To order printed copies, contact reprints@rsna.org REVIEWS AND COMMENTARY n HOW I DO IT Ryan D. Murtagh, MD, MBA Robert M. Quencer, MD Juan Uribe, MD Pelvic Evaluation
Induction and Maintenance of Lordosis in MultiLevel ACDF Using Allograft. Saad Khairi, MD Jennifer Murphy Robert S. Pashman, MD
 Induction and Maintenance of Lordosis in MultiLevel ACDF Using Allograft Saad Khairi, MD Jennifer Murphy Robert S. Pashman, MD Purpose Is lordosis induced by multilevel cortical allograft ACDF placed on
Induction and Maintenance of Lordosis in MultiLevel ACDF Using Allograft Saad Khairi, MD Jennifer Murphy Robert S. Pashman, MD Purpose Is lordosis induced by multilevel cortical allograft ACDF placed on
Don t turn your back on Scheuermann s Kyphosis
 Don t turn your back on Scheuermann s Kyphosis Stefan Parent, MD, PhD Ste-Justine Hospital Université de Montréal Academic Chair in Pediatric Spinal Deformities Disclosures Depuy Synthes spine (a), Canadian
Don t turn your back on Scheuermann s Kyphosis Stefan Parent, MD, PhD Ste-Justine Hospital Université de Montréal Academic Chair in Pediatric Spinal Deformities Disclosures Depuy Synthes spine (a), Canadian
Outcomes in Adult Scoliosis Patients Who Undergo Spinal Fusion Stopping at L5 Compared with Extension to the Sacrum
 96 Systematic Review Outcomes in Adult Scoliosis Patients Who Undergo Spinal Fusion Stopping at L5 Compared with Extension to the Sacrum Zeeshan M. Sardar 1 Jean A. Ouellet 1 Dena J. Fischer 2 Andrea C.
96 Systematic Review Outcomes in Adult Scoliosis Patients Who Undergo Spinal Fusion Stopping at L5 Compared with Extension to the Sacrum Zeeshan M. Sardar 1 Jean A. Ouellet 1 Dena J. Fischer 2 Andrea C.
3D titanium interbody fusion cages sharx. White Paper
 3D titanium interbody fusion cages sharx (SLM selective laser melted) Goal of the study: Does the sharx intervertebral cage due to innovative material, new design, and lordotic shape solve some problems
3D titanium interbody fusion cages sharx (SLM selective laser melted) Goal of the study: Does the sharx intervertebral cage due to innovative material, new design, and lordotic shape solve some problems
AOSpine Advances Symposium Spinal Deformity
 AOSpine Advances Symposium Spinal Deformity December 03-04, 2010 Istanbul, Türkiye Proper radiographic evaluation, parameters, clinical relevance and importance Dr. Alpaslan Şenköylü Session: Sagittal
AOSpine Advances Symposium Spinal Deformity December 03-04, 2010 Istanbul, Türkiye Proper radiographic evaluation, parameters, clinical relevance and importance Dr. Alpaslan Şenköylü Session: Sagittal
Disclosures. Outline. General Guideline 6/4/2011. Consultant Medtronic, Stryker, Depuy. Osteotomy Planning and the Impact of Reciprocal Changes
 Disclosures Consultant Medtronic, Stryker, Depuy Osteotomy Planning and the Impact of Reciprocal Changes Christopher Ames MD Associate Professor Director of Spine Tumor and Deformity Surgery UCSF Department
Disclosures Consultant Medtronic, Stryker, Depuy Osteotomy Planning and the Impact of Reciprocal Changes Christopher Ames MD Associate Professor Director of Spine Tumor and Deformity Surgery UCSF Department
factor for identifying unstable thoracolumbar fractures. There are clinical and radiological criteria
 NMJ-Vol :2/ Issue:1/ Jan June 2013 Case Report Medical Sciences Progressive subluxation of thoracic wedge compression fracture with unidentified PLC injury Dr.Thalluri.Gopala krishnaiah* Dr.Voleti.Surya
NMJ-Vol :2/ Issue:1/ Jan June 2013 Case Report Medical Sciences Progressive subluxation of thoracic wedge compression fracture with unidentified PLC injury Dr.Thalluri.Gopala krishnaiah* Dr.Voleti.Surya
Low Res SAMPLE SPINAL CURVES THE SPINE
 THE SPINE The normal healthy spine has a naturally curved shape. Like a coiled spring, these curves help to absorb some of the forces that are placed on your spine while standing erect. When looking at
THE SPINE The normal healthy spine has a naturally curved shape. Like a coiled spring, these curves help to absorb some of the forces that are placed on your spine while standing erect. When looking at
Original Date: October 2015 LUMBAR SPINAL FUSION FOR
 National Imaging Associates, Inc. Clinical guidelines Original Date: October 2015 LUMBAR SPINAL FUSION FOR Page 1 of 9 INSTABILITY AND DEGENERATIVE DISC CONDITIONS FOR CMS (MEDICARE) MEMBERS ONLY CPT4
National Imaging Associates, Inc. Clinical guidelines Original Date: October 2015 LUMBAR SPINAL FUSION FOR Page 1 of 9 INSTABILITY AND DEGENERATIVE DISC CONDITIONS FOR CMS (MEDICARE) MEMBERS ONLY CPT4
Pedicle Subtraction Osteotomy. Case JB. Antonio Castellvi 5/19/2017
 Pedicle Subtraction Osteotomy John M. Small MD Florida Orthopedic Institute University South Florida Department Orthopedic Surgery Castellvi Spine May 11, 2017 Case JB 66 y/o male 74 235 lbs Retired police
Pedicle Subtraction Osteotomy John M. Small MD Florida Orthopedic Institute University South Florida Department Orthopedic Surgery Castellvi Spine May 11, 2017 Case JB 66 y/o male 74 235 lbs Retired police
18th International Scientific Meeting of the VCFS Educational Foundation Steven M. Reich, MD. July 15-17, 2011 New Brunswick, New Jersey USA
 18th International Scientific Meeting of the VCFS Educational Foundation Steven M. Reich, MD July 15-17, 2011 New Brunswick, New Jersey USA SCOLIOSIS AND ITS TREATMENT Steven M. Reich, MD Assistant Clinical
18th International Scientific Meeting of the VCFS Educational Foundation Steven M. Reich, MD July 15-17, 2011 New Brunswick, New Jersey USA SCOLIOSIS AND ITS TREATMENT Steven M. Reich, MD Assistant Clinical
LUMBAR SPINAL STENOSIS
 LUMBAR SPINAL STENOSIS Always occurs in the mobile segment. Factors play role in Stenosis Pre existing congenital or developmental narrowing of the lumbar spinal canal Translation of one anatomic segment
LUMBAR SPINAL STENOSIS Always occurs in the mobile segment. Factors play role in Stenosis Pre existing congenital or developmental narrowing of the lumbar spinal canal Translation of one anatomic segment
Module: #15 Lumbar Spine Fusion. Author(s): Jenni Buckley, PhD. Date Created: March 27 th, Last Updated:
: Jenni Buckley, PhD. Date Created: March 27 th, Last Updated:") Module: #15 Lumbar Spine Fusion Author(s): Jenni Buckley, PhD Date Created: March 27 th, 2011 Last Updated: Summary: Students will perform a single level lumbar spine fusion to treat lumbar spinal stenosis.
Module: #15 Lumbar Spine Fusion Author(s): Jenni Buckley, PhD Date Created: March 27 th, 2011 Last Updated: Summary: Students will perform a single level lumbar spine fusion to treat lumbar spinal stenosis.
Solitaire Anterior Spinal System
 Surgical Technique Solitaire Anterior Spinal System Independent Stabilization for the Anterior Column Available in Titanium and Contents Introduction... Page 1 Design Features... Page 2 Instruments...
Surgical Technique Solitaire Anterior Spinal System Independent Stabilization for the Anterior Column Available in Titanium and Contents Introduction... Page 1 Design Features... Page 2 Instruments...
Sacropelvic Fixation. Ahmet Alanay M.D. Professor. Acıbadem Maslak Hospital Comprehensive Spine Center Istanbul TURKEY
 Sacropelvic Fixation Ahmet Alanay M.D. Professor Acıbadem Maslak Hospital Comprehensive Spine Center Istanbul TURKEY Conflict of Interest Grant Depuy & Synthes Definition Sacropelvic fixation Long spinal
Sacropelvic Fixation Ahmet Alanay M.D. Professor Acıbadem Maslak Hospital Comprehensive Spine Center Istanbul TURKEY Conflict of Interest Grant Depuy & Synthes Definition Sacropelvic fixation Long spinal
Clinical Study Acute Reciprocal Changes Distant from the Site of Spinal Osteotomies Affect Global Postoperative Alignment
 SAGE-Hindawi Access to Research Advances in Orthopedics Volume 2011, Article ID 415946, 7 pages doi:10.4061/2011/415946 Clinical Study Acute Reciprocal Changes Distant from the Site of Spinal Osteotomies
SAGE-Hindawi Access to Research Advances in Orthopedics Volume 2011, Article ID 415946, 7 pages doi:10.4061/2011/415946 Clinical Study Acute Reciprocal Changes Distant from the Site of Spinal Osteotomies
It consist of two components: the outer, laminar fibrous container (or annulus), and the inner, semifluid mass (the nucleus pulposus).
, and the inner, semifluid mass (the nucleus pulposus).") Lumbar Spine The lumbar vertebrae are the last five vertebrae of the vertebral column. They are particularly large and heavy when compared with the vertebrae of the cervical or thoracicc spine. Their bodies
Lumbar Spine The lumbar vertebrae are the last five vertebrae of the vertebral column. They are particularly large and heavy when compared with the vertebrae of the cervical or thoracicc spine. Their bodies
Departement of Neurosurgery A.O.R.N A. Cardarelli- Naples.
 Percutaneous posterior pedicle screw fixation in the treatment of thoracic, lumbar and thoraco-lumbar junction (T12-L1) traumatic and pathological spine fractures. Report of 45 cases. G. Vitale, A. Punzo,
Percutaneous posterior pedicle screw fixation in the treatment of thoracic, lumbar and thoraco-lumbar junction (T12-L1) traumatic and pathological spine fractures. Report of 45 cases. G. Vitale, A. Punzo,
Axial Skeleton: Vertebrae and Thorax
 Axial Skeleton: Vertebrae and Thorax Function of the vertebral column (spine or backbone): 1) 2) 3) Composition of Vertebral column The vertebral column is formed by 33 individual vertebrae (some of which
Axial Skeleton: Vertebrae and Thorax Function of the vertebral column (spine or backbone): 1) 2) 3) Composition of Vertebral column The vertebral column is formed by 33 individual vertebrae (some of which
The importance of the sagittal profile in spinal deformity surgery
 The importance of the sagittal profile in spinal deformity surgery FRCS (Orth), MCh (Orth), D (Orth), MS (Orth) Consultant Spine Deformity Surgeon The Royal Orthopaedic Hospital, Birmingham Childrens Hospital
The importance of the sagittal profile in spinal deformity surgery FRCS (Orth), MCh (Orth), D (Orth), MS (Orth) Consultant Spine Deformity Surgeon The Royal Orthopaedic Hospital, Birmingham Childrens Hospital
Current status of managing pediatric kyphosis deformity Papers divided into 3 categories
 Biomechanical and Clinical Evaluation of Rib Anchors Richard H. Gross, MD Research Professor, Clemson University Clemson-MUSC Bioengineering Consortium Charleston, SC Staff surgeon, Shriners Hospital,
Biomechanical and Clinical Evaluation of Rib Anchors Richard H. Gross, MD Research Professor, Clemson University Clemson-MUSC Bioengineering Consortium Charleston, SC Staff surgeon, Shriners Hospital,
Postoperative standing posteroanterior spine
 )376( COPYRIGHT 2016 BY THE ARCHIVES OF BONE AND JOINT SURGERY RESEARCH ARTICLE Assessment of Coronal Radiographic Parameters of the Spine in the Treatment of Adolescent Idiopathic Scoliosis Abstract Mohsen
)376( COPYRIGHT 2016 BY THE ARCHIVES OF BONE AND JOINT SURGERY RESEARCH ARTICLE Assessment of Coronal Radiographic Parameters of the Spine in the Treatment of Adolescent Idiopathic Scoliosis Abstract Mohsen
Functional Movement Test. Deep Squat
 Functional Movement Test Put simply, the FMS is a ranking and grading system that documents movement patterns that are key to normal function. By screening these patterns, the FMS readily identifies functional
Functional Movement Test Put simply, the FMS is a ranking and grading system that documents movement patterns that are key to normal function. By screening these patterns, the FMS readily identifies functional
Author's response to reviews
 Author's response to reviews Title: Scoliotic posture as the initial symptom in adolescents with lumbar disc herniation: its curve pattern and natural history after lumbar discectomy Authors: Zezhang Zhu
Author's response to reviews Title: Scoliotic posture as the initial symptom in adolescents with lumbar disc herniation: its curve pattern and natural history after lumbar discectomy Authors: Zezhang Zhu
Lowest instrumented vertebra selection in Lenke 3C and 6C scoliosis: what if we choose lumbar apical vertebra as distal fusion end?
 Eur Spine J (2012) 21:1053 1061 DOI 10.1007/s00586-011-2058-1 ORIGINAL ARTICLE Lowest instrumented vertebra selection in Lenke 3C and 6C scoliosis: what if we choose lumbar apical vertebra as distal fusion
Eur Spine J (2012) 21:1053 1061 DOI 10.1007/s00586-011-2058-1 ORIGINAL ARTICLE Lowest instrumented vertebra selection in Lenke 3C and 6C scoliosis: what if we choose lumbar apical vertebra as distal fusion
Effect of direct vertebral body derotation on the sagittal profile in adolescent idiopathic scoliosis
 Eur Spine J (2012) 21:31 39 DOI 10.1007/s00586-011-1991-3 ORIGINAL ARTICLE Effect of direct vertebral body derotation on the sagittal profile in adolescent idiopathic scoliosis Steven W. Hwang Amer F.
Eur Spine J (2012) 21:31 39 DOI 10.1007/s00586-011-1991-3 ORIGINAL ARTICLE Effect of direct vertebral body derotation on the sagittal profile in adolescent idiopathic scoliosis Steven W. Hwang Amer F.