SmartRelease Endoscopic Carpal Tunnel Release (ECTR)
|
|
|
- Dina Terry
- 6 years ago
- Views:
Transcription

")

1 SmartRelease Endoscopic Carpal Tunnel Release (ECTR) Hand Anatomy and Technical Hints




2 Hand Anatomy Hand Topography Hand Anatomical Landmarks 1 SmartRelease Hand Anatomy and Technical Hints

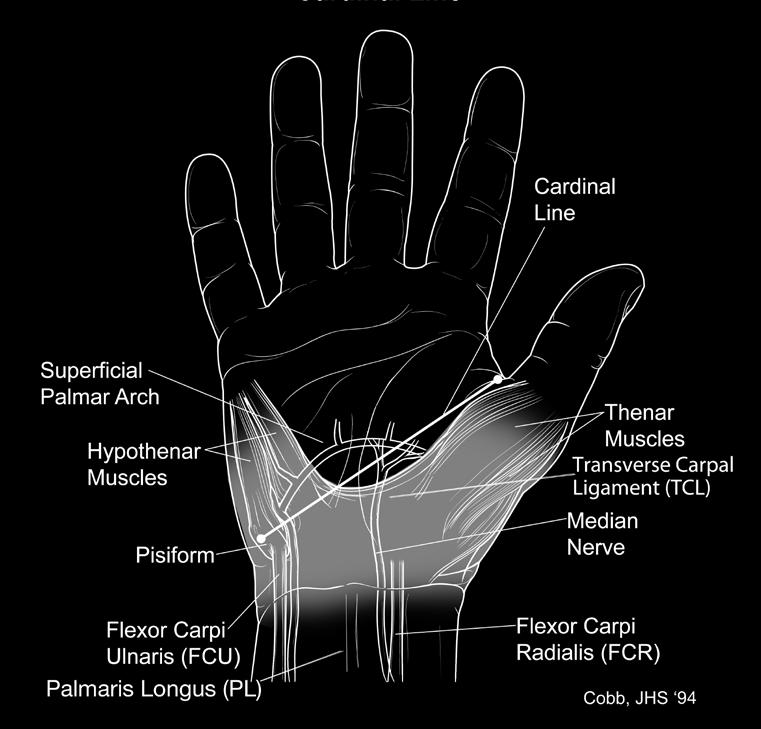
3 Cobb s Line Cardinal Line SmartRelease Hand Anatomy and Technical Hints 2


4 Wrist Cross Section with Device (Left Hand) Anatomy Identification in Cadaver Dissection Create a wrist incision as described in the MicroAire SmartRelease Surgical Technique (LIT-ECTR-TECH). Incise the skin and palmar fascia from the proximal transverse palmar crease to the insertion point in the wrist incision. Excise the fat and remove tissue to obtain a clear view of the important structures. Identify: Median nerve Thenar motor branch Common digital nerve to the third and fourth web Branch of ulnar nerve communicating with median nerve Guyon s canal and ulnar neurovascular bundle Superficial palmar arterial arch Place the blade assembly in the proper position to cut the TCL and observe the relationship between the blade assembly and: The main trunk of the median nerve The common digital nerve to third and fourth finger web Guyon s canal The superficial branch of ulnar artery 3 SmartRelease Hand Anatomy and Technical Hints
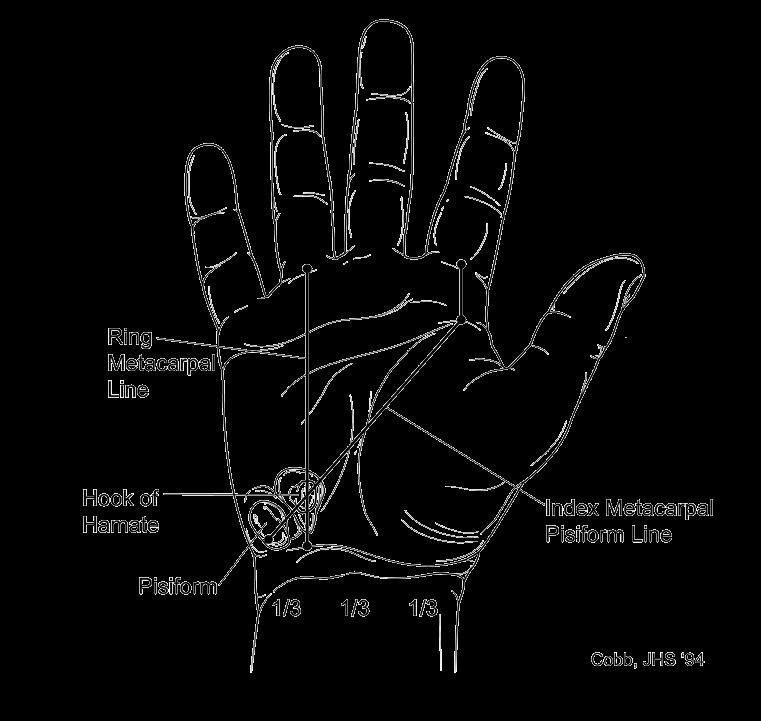
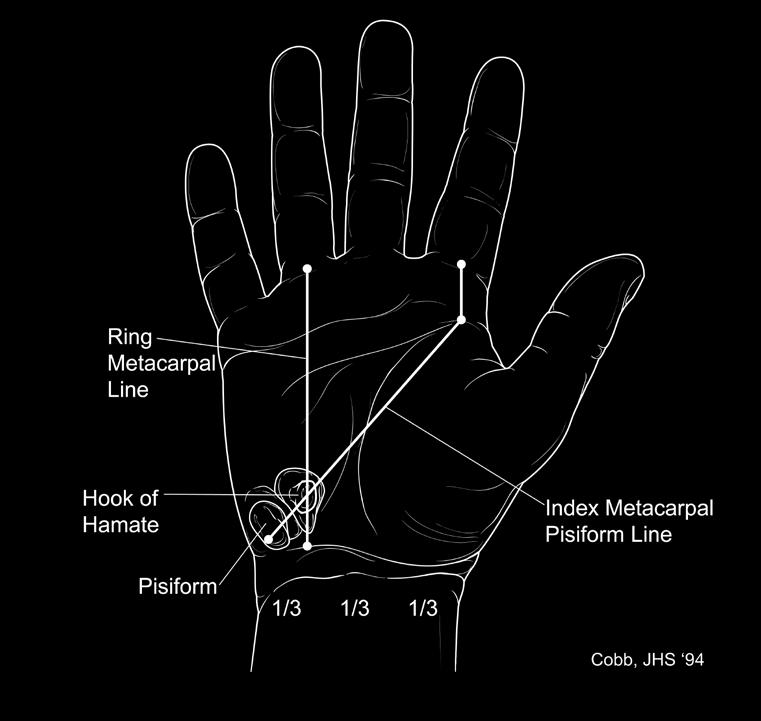
5 Ten Rules to Follow When Using the MicroAire Carpal Tunnel Release System By Edward North, M.D. #1 Know Your Anatomy. This device is not the same as an arthroscope. Many critical structures lie within 1 or 2 mm of the cutting blade. The safe area for ligament transaction is in line with the ring finger. #2 Never, Never Overcommit Yourself. Despite your enthusiasm with this new technique, don t promise the patient an endoscopic release. Technical problems or anatomical abnormalities may prevent endoscopic carpal tunnel release. Your patients should be informed at the pre-op visit that the incidence of conversion to open procedure for their safety is around 5%. #3 Make Certain the Equipment is Working Properly Before You Begin. The light source should be on, a clear image obtained, focus and whiteness adjustment made, the lens defogged, and the blade assembly well secured and properly aligned. This will lessen the chance of technical problems that will obscure your vision which could increase the risk of injury to critical structures. #4 If the Scope Insertion is Obstructed, Abort. You cannot see the source of obstruction through the scope and it could be an aberrant branch of the median nerve. To force the blade assembly into the canal could cause injury to such a nerve branch. Convert to an open procedure if this occurs. #5 Be Certain You Are in the Carpal Canal (or you had better not be in the loge of Guyon). This is when damage to the ulnar nerve occurs. Make your initial window through the forearm fascia beneath the palmaris longus tendon and look for the median nerve beneath the fascia. If you begin your skin incision in one of the more proximal volar wrist creases, it is easier to differentiate the vulgar carpal ligament covering Guyon s canal from the transverse carpal ligament covering the carpal tunnel (although this skin approach leaves a less cosmetic scar). #6 If You Can t See Well, Abort. Nothing will get you into trouble faster than proceeding with division of the ligament without a clear view of the transverse fibers of the ligament. You may have tenosynovium interposed or you may be on the dorsal surface of the median nerve. You absolutely must see the transverse ligament fibers along a strip the entire length of the canal before cutting. #7 Do Not Explore the Carpal Canal with the Scope. In the first place, you can t see anything because the soft tissues collapse over the window and you cannot get far enough away to see things like a median nerve constriction. Secondly, you may cause a neurapraxia or get into the wrong plane by manipulating the scope around the canal. The blade assembly is a retractor used 1) to visualize the ligament to be cut and 2) to exclude the other critical structures. #8 If the View is Not Normal, Abort. There may be unusual anatomy that will prevent clear visualization of the ligament. Or, more commonly, there may be a clear distal demarcation of the ligament due to prolongation of fibers of the palmar fascia. Rather than cutting more distally with the blade assembly, thereby risking injury to the superficial vascular arch and the common digital nerves, convert to an open procedure. #9 Stay in Line with the Ring Finger. Draw a line on the skin and stay along this line in your preparation of the pathway and cutting. This will keep you between the ulnar and median nerves. Since the scope pivots on the hook of the hamate, moving the handle slightly out of line with the ring finger can cause the tip of the blade assembly to swing more out of line with the ring finger. #10 When in Doubt, Get Out. If for any reason, either as described above or a problem not yet reported, you are uncomfortable proceeding, convert to an open release. The morbidity with an open procedure will be much less than with a severed nerve. SmartRelease Hand Anatomy and Technical Hints 4
6 Technical Hints on Performing ECTR Using the MicroAire Carpal Tunnel Release System By Edward Diao, M.D. Chief, Hand and Microsurgery Service, University of California, San Francisco 1. Make sure you re down to the right level. Do not be fooled by dissecting subcutaneous fat. The ante brachial fascia and flexor retinaculum should be a discrete structure, below the level of the subcutaneous vessels, and if a palmaris longus is present, directly deep to that structure. If you have achieved the proper level, there should be fascial layer which is visible. 2. Make the U-shaped flap wide enough to not impinge upon the nosepiece of the endoscopic carpal tunnel device. 3. Use the synovial elevator carefully, but adequately to palpate the transverse striations on the undersurface of the transverse carpal ligament and to remove some of the synovium away from this layer, for better visualization. 4. Make sure you re not in Guyon s canal. If you re in Guyon s canal, the hamate finder or endoscopic device will be subcutaneously palpable, at the proximal one-third of the palm. If, however, you re in the carpal tunnel canal, the device will not be palpable in the proximal one-third of the palm, but will re-emerge at the level of the distal edge of transverse carpal ligament at the junction of the middle and proximal one-third, at or about the level of Kaplan s line. 5. Use bimanual palpation. This is an important guide. 6. Be aware of the axis of the ring finger as your aiming point. 7. Use transillumination, and the difference between the quality of the light as you are passing from underneath the transverse carpal ligament, into the mid-palmar area. 8. Consider rolling the endoscopic carpal tunnel device radially to visualize the median nerve and flexor tendons, and to see how much of a safe zone you have in the undersurface of the transverse carpal ligament. 9. If you perform a partial division of the transverse carpal ligament and the fat is prolapsing from the palmar layers through the cut transverse carpal ligament to obscure your visualization, use a Senn or Ragnell retractor to hold up the fat, at the level of the partially cut transverse carpal ligament. Then you can visualize things well, to perform the remainder of the transverse carpal ligament division. This technique can be used to release the proximal portions, while saving the division of the distal-most portion of the transverse carpal ligament for a second pass. One can alternatively use Dr. Richard Tortsa s suggestion of releasing the distal one-third to one-half of the ligament first, then doing the proximal portion in the second pass. 10. If you have completely divided the transverse carpal ligament, you should not be able to visualize both cut leaflets of the cut transverse carpal ligament simultaneously (see MicroAire SmartRelease Surgical Technique (LIT-ECTR-TECH) for reference). 5 SmartRelease Hand Anatomy and Technical Hints
7 Points to Consider in the MicroAire Carpal Tunnel Release System Surgical Skills Workshop From the MicroAire SmartRelease Surgical Technique (LIT-ECTR-TECH) 1. If you can t see, don t cut. Be sure you and your patient are prepared to abandon the procedure in favor of an open carpal tunnel release. 2. Aim at the ring finger, hug the heel of the hamate, snugly apply the window to the deep side of the ligament, elevate the blade and slowly withdraw the device. 3. Review the ways to stay out of Guyon s canal: review anatomy, note that Guyon s doesn t have synovium in it. 4. Scale on nosepiece: scale is a relative guide allowing you to correlate surface anatomy with what you see in the endoscopic view. Note that scale is in centimeters and starts with point of blade elevation. 5. Control and adjust wrist position in the flexion extension plane with your opposite hand; allows surgeon to accurately use tip of disposable to sweep synovium and fat off of ligament especially distal ligament when making second and third passes. Also, this approach positions surgeon s thumb to palpate course of blade assembly to bounce on soft tissues to help define (endoscopically) how rigid remaining tissues are. In addition, you can use thumb pressure to hold tissue snugly opposed to the window. 6. Be sure to incise fascia proximal to skin incision using tenotomy scissors. 7. Goal of pre-op work up : 1) define patient with carpal tunnel syndrome of severity adequate to deserve surgical decompression, 2) by the overall clinical picture including history, physical and radiographic exam, define that there is no pathology inside the carpal tunnel that needs to be viewed or treated during surgery. THIS SURGICAL SYSTEM IS DESIGNED SOLELY TO VISUALIZE AND CUT THE TRANSVERSE CARPAL LIGAMENT! 8. Local anesthesia: Surgery can usually be performed under local anesthesia supported with sedation and other anesthetic agents as needed. You should attempt surgery under local only after you have gained experience with the operative procedure and has mastered the technical details of the surgical approach and instrumentation under block or general anesthesia. 9. The secret to success requires a careful surgical approach designed to define a plane between the finger flexor synovium and the deep side of the transverse carpal ligament. This surgical plane gives the surgeon a clear unobstructed view of the bundles of collagen of the ligament for their safe endoscopic division. 10. A transverse incision in a wrist flexion crease combined with an intracuticular wound closure produces a scar that is essentially invisible. 11. Post-operatively, use a splint that allows the thumb to fall into opposition. Post-op splinting that forces the thumb into extension and supination (into the plane of the palm of the hand) tends to pull the cut edges of the transverse carpal ligament apart resulting in a weak opposition and flattening of the proximal arch of the palm of the hand. Although important in endoscopic carpal tunnel release, it is critical in conventional open carpal tunnel release as the radial half of the divided transverse carpal ligament is unstable secondary to division of the overlying soft tissues (palmar fascia, etc.). 12. Pre-operative x-rays are important to rule out pathology of the bony canal, especially anomalies and non-unions of the hook of the hamate as well as calcific tendonitis. These patients deserve open carpal tunnel release. 13. Light level: the ideal endoscopic light level allows appreciation of the contour and texture of the collagen bundles of the transverse carpal ligament. Excessive lighting destroys this important definition. This is frequently achieved with manual control of the light level. 14. All instrumentation (the synovium elevator, hamate finders and blade assembly) are introduced down the ulnar side of the carpal tunnel with the wrist in some degree of extension. Care is taken to maintain a ring finger aim, hug the hook of the hamate and keep the instrumentation snugly applied to the deep side of the ligament. 15. Following endoscopic carpal tunnel release, patients should avoid power gripping, especially with the wrist flexed, until soft tissue (ligament) healing is complete. 16. Partial degrees of blade elevation are useful with second passes to release remaining bands of ligament collagen. 17. The surgical goal is to completely divide the transverse carpal ligament as defined by the creation of a trapezoidal defect in the ligament. In a patient, the two halves of the ligament typically retract approximately 5 mm to allow insertion of the blade assembly between the two cut edges of the ligament. Gentle rotation of the blade assembly from side to side will allow visualization of the cut edges of the ligament. 18. Additional cuts of soft tissues superficial to the transverse carpal ligament divide fascial layers that are important in stabilizing the origin of the thenar muscles. This results in a progressive loss of the change in morbidity gained by endoscopic carpal tunnel release. 19. Note that most cadavers lose the elastic properties of their carpal tunnel. You should note two differences between cadavers and patients: 1) the ligament is more difficult to cut in a cadaver because its fibers are under less (or no) resting tension and, 2) the divided ligament is reluctant to retract in a cadaver (it retracts readily in a patient). 20. If you want to get your patient back to work earlier, let them know pre-operatively about the change in morbidity achieved by endoscopic carpal tunnel release. A patient who has not experienced open carpal tunnel release on their opposite hand may not appreciate the decrease in morbidity achieved endoscopically. This helps break the post-operative disability syndrome typical of some workman comp patients. Be positive and reassuring and this will help the patient meet your expectations as well as the potential of endoscopic carpal tunnel release. SmartRelease Hand Anatomy and Technical Hints 6
8 Surgeon Recommended Local Anesthesia Technique for ECTR By Michael J. Wheatley, M.D., Portland, Oregon Equipment 30 gauge 1 inch needle 27 gauge 1.5 inch needle (2) 5 cc syringes 10 cc of 2% lidocaine with epinephrine 8.4% Sodium Bicarbonate A dense median nerve block is essential for comfortable endoscopic carpal tunnel release under local anesthesia. The median nerve is located between the FCR and palmar longus tendons and can extend ulnar to the palmaris longus tendon. Therefore, safer areas for median nerve are through or radial to the FCR tendon and along the axis of the fourth ray. The use of small bore needles greatly minimizes the risk of iatrogenic median nerve injury. Local anesthesia should be administered approximately minutes prior to the procedure to allow for a dense median nerve block. Anesthetizing the ulnar nerve is not necessary, but the transverse carpal ligament must be anesthetized with a palmar block. Median nerve block alone does not reliably anesthetize the transverse carpal ligament. Place 1 cc of 8.4% sodium bicarbonate in 10 cc of 2% lidocaine with epinephrine. This will raise the ph of the lidocaine and significantly decrease the pain with injection. Mark the radial aspect of the FCR tendon at a point 3 cm proximal to the wrist flexion crease. Inject ½ cc of lidocaine with epinephrine at this point using the 30-gauge needle. Then, slowly advance the needle at a 45-degree angle to the FCR tendon. When the needle is inserted to ½ of its length, injection 3 cc of the local anesthesia solution. Advance the needle to ³ ₄ of its length and inject the remaining 2 cc of solution. Next, mark the incision site. From the initial FCR injection point, slowly advance the 27-gauge needle, injecting in the subcutaneous tissue while the needle is advanced. Once the incision is anesthetized, perforate the skin with the 27-gauge needle in the mid-portion of the anesthetized incision and then advance slowly into the palm in the area overlying the transverse carpal ligament. Inject 2 3 cc in the tissues superficial to the transverse carpal ligament. Alternate Technique Mark a point 3 cm proximal to the distal wrist flexion crease along the ulnar side of the axis of the third ray. Using the 30-gauge needle angled in a 45-degree proximal and 45-degree radial direction, injection up to 8 cc at depths of ½ to ³ ₄ the length of the needle. Mark the incision. Starting at the already anesthetized initial point, inject ½ cc of lidocaine with epinephrine into the incision area in the subcutaneous tissue using the 30-gauge needle. Once the incision is anesthetized, perforate the skin with the 27-gauge needle in the mid-portion of the anesthetized incision and then advance slowly into the palm in the area overlying the transverse carpal ligament. Inject 2 3 cc in the tissues superficial to the transverse carpal ligament. The patient should experience paresthesias and numbness in the median nerve distribution. Additional lidocaine can be given if the block is not dense. This may be necessary in men with large hands. Ulnar nerve block is not required for comfortable local only ECTR. MicroAire Surgical Instruments 3590 Grand Forks Boulevard Charlottesville, VA USA or MicroAire Surgical Instruments, LLC All rights reserved. LIT-ECTR-HAND-HINTS REV A
Centerline Carpal Tunnel Release
 Centerline Endoscopic Carpal Tunnel Release Surgical Technique Centerline Carpal Tunnel Release Centerline Endoscopic Carpal Tunnel Release Surgical Set Up The patient is positioned supine on the operating
Centerline Endoscopic Carpal Tunnel Release Surgical Technique Centerline Carpal Tunnel Release Centerline Endoscopic Carpal Tunnel Release Surgical Set Up The patient is positioned supine on the operating
Endoscopic Carpal Tunnel Release System. SafeViewTM Endoscopic Carpal Tunnel Release System
 Endoscopic Carpal Tunnel Release System SafeViewTM Endoscopic Carpal Tunnel Release System Fully Disposable and Sterile Packaged Endoscopic Carpal Tunnel Release System SafeView is packaged sterile with
Endoscopic Carpal Tunnel Release System SafeViewTM Endoscopic Carpal Tunnel Release System Fully Disposable and Sterile Packaged Endoscopic Carpal Tunnel Release System SafeView is packaged sterile with
Endoscopic Carpal Tunnel Release System. SafeViewTM 360 Panoramic Visualization Sterile Packaged Fully Disposable
 U P P E R E X T R E M I T Y T E C H N I Q U E G U I D E Endoscopic Carpal Tunnel Release System SafeViewTM 360 Panoramic Visualization Sterile Packaged Fully Disposable Versatility and Control SafeView
U P P E R E X T R E M I T Y T E C H N I Q U E G U I D E Endoscopic Carpal Tunnel Release System SafeViewTM 360 Panoramic Visualization Sterile Packaged Fully Disposable Versatility and Control SafeView
Table of Contents: CARPAL TUNNEL RELEASE SURGICAL TECHNIQUE Knife Assembly... Page 6 VERSION 2.2
 www.s2ssurgical.com Table of Contents: Preparation... Page 1 Dissection... Page 2 Tunneling... Page 3 Release... Page 4 Closure... Page 6 Knife Assembly... Page 6 CARPAL TUNNEL RELEASE SURGICAL TECHNIQUE
www.s2ssurgical.com Table of Contents: Preparation... Page 1 Dissection... Page 2 Tunneling... Page 3 Release... Page 4 Closure... Page 6 Knife Assembly... Page 6 CARPAL TUNNEL RELEASE SURGICAL TECHNIQUE
SmartRelease Endoscopic Carpal Tunnel
 SmartRelease Endoscopic Carpal Tunnel Endoscopic Carpal Tunnel Release Surgical Technique Traditionally, a patient treated surgically for carpal tunnel syndrome could expect significant recovery time away
SmartRelease Endoscopic Carpal Tunnel Endoscopic Carpal Tunnel Release Surgical Technique Traditionally, a patient treated surgically for carpal tunnel syndrome could expect significant recovery time away
Integra. SafeGuard Mini Carpal Tunnel Release System SURGICAL TECHNIQUE
 SafeGuard Mini Carpal Tunnel Release System SURGICAL TECHNIQUE SafeGuard Mini Carpal Release System Contents Surgical Technique...2 Description...2 The SafeGuard System...2 Indications...2 Contraindications...2
SafeGuard Mini Carpal Tunnel Release System SURGICAL TECHNIQUE SafeGuard Mini Carpal Release System Contents Surgical Technique...2 Description...2 The SafeGuard System...2 Indications...2 Contraindications...2
Initial experience with endoscopic carpal tunnel release surgery
 Initial experience with endoscopic carpal tunnel release surgery Craig H. Rabb, M.D., and Todd Kuether, M.D. Division of Neurosurgery, Oregon Health Sciences University, Portland, Oregon; and Portland
Initial experience with endoscopic carpal tunnel release surgery Craig H. Rabb, M.D., and Todd Kuether, M.D. Division of Neurosurgery, Oregon Health Sciences University, Portland, Oregon; and Portland
Endoscopic Soft Tissue Release System. SafeViewTM 360 Panoramic Visualization Sterile Packaged Fully Disposable
 L O W E R E X T R E M I T Y T E C H N I Q U E G U I D E Endoscopic Soft Tissue Release System SafeViewTM 360 Panoramic Visualization Sterile Packaged Fully Disposable Versatility and Control SafeView is
L O W E R E X T R E M I T Y T E C H N I Q U E G U I D E Endoscopic Soft Tissue Release System SafeViewTM 360 Panoramic Visualization Sterile Packaged Fully Disposable Versatility and Control SafeView is
carpal tunnel get back to life Patient information about Endoscopic Surgery for the treatment of Carpal Tunnel Syndrome
 carpal tunnel get back to life Patient information about Endoscopic Surgery for the treatment of Carpal Tunnel Syndrome what is carpal tunnel syndrome? Carpal Tunnel Syndrome (CTS) is a medical condition
carpal tunnel get back to life Patient information about Endoscopic Surgery for the treatment of Carpal Tunnel Syndrome what is carpal tunnel syndrome? Carpal Tunnel Syndrome (CTS) is a medical condition
Hand Anatomy A Patient's Guide to Hand Anatomy
 Hand Anatomy A Patient's Guide to Hand Anatomy Introduction Few structures of the human anatomy are as unique as the hand. The hand needs to be mobile in order to position the fingers and thumb. Adequate
Hand Anatomy A Patient's Guide to Hand Anatomy Introduction Few structures of the human anatomy are as unique as the hand. The hand needs to be mobile in order to position the fingers and thumb. Adequate
WHAT CAN ULTRASOUND SEE IN THE CARPAL TUNNEL REGION?
 WHAT CAN ULTRASOUND SEE IN THE CARPAL TUNNEL REGION? Jay Smith, M.D. CMO, Sonex Health LLC June 2017 Modern day ultrasound (US) machines provide a powerful combination of submillimeter resolution and dynamic
WHAT CAN ULTRASOUND SEE IN THE CARPAL TUNNEL REGION? Jay Smith, M.D. CMO, Sonex Health LLC June 2017 Modern day ultrasound (US) machines provide a powerful combination of submillimeter resolution and dynamic
Endoscopic Carpal Tunnel Release ECTR
 Endoscopic Carpal Tunnel Release ECTR Christophe MATHOULIN Paris, France Historics Paget, 1854 Putnam, 1893 Hunt, 1909 Marie et Foix, 1913 Recommanded surgical release Learmonth, 1933 First reported release
Endoscopic Carpal Tunnel Release ECTR Christophe MATHOULIN Paris, France Historics Paget, 1854 Putnam, 1893 Hunt, 1909 Marie et Foix, 1913 Recommanded surgical release Learmonth, 1933 First reported release
EndoRelease ENDOSCOPIC CUBITAL TUNNEL RELEASE SYSTEM
 EndoRelease ENDOSCOPIC CUBITAL TUNNEL RELEASE SYSTEM SURGICAL TECHNIQUE Up p e r Ex t r e m i t y So l u t i o n s ENDOSCOPIC CUBITAL TUNNEL RELEASE SYSTEM Description: The EndoRelease Endoscopic Cubital
EndoRelease ENDOSCOPIC CUBITAL TUNNEL RELEASE SYSTEM SURGICAL TECHNIQUE Up p e r Ex t r e m i t y So l u t i o n s ENDOSCOPIC CUBITAL TUNNEL RELEASE SYSTEM Description: The EndoRelease Endoscopic Cubital
Carpal Tunnel Release
 Carpal Tunnel Release Carpal tunnel syndrome is a condition in the hand and wrist caused by excessive pressure on the median nerve in the wrist. Compression of the nerve typically causes numbness and tingling
Carpal Tunnel Release Carpal tunnel syndrome is a condition in the hand and wrist caused by excessive pressure on the median nerve in the wrist. Compression of the nerve typically causes numbness and tingling
Anatomic relationships of an endoscopic carpal tunnel device to surrounding structures
 This is" a reprint of an article in The Journal of Hand Surgery (American Volume) as it was published in its original foi m. Articles in The Journal are not prepared for any company or distributor, and
This is" a reprint of an article in The Journal of Hand Surgery (American Volume) as it was published in its original foi m. Articles in The Journal are not prepared for any company or distributor, and
LECTURE 8 HANDS: BONES AND MUSCLES
 LECTURE 8 HANDS: BONES AND MUSCLES WRIST AND HAND - Human hand can do power grip and precision grip - Thumb is 90 to the rest of the hand can do fine actions - Often able to do power actions o Take tools
LECTURE 8 HANDS: BONES AND MUSCLES WRIST AND HAND - Human hand can do power grip and precision grip - Thumb is 90 to the rest of the hand can do fine actions - Often able to do power actions o Take tools
Endoscopic Carpal Tunnel Release Experience at King Hussein Medical Center
 Endoscopic Carpal Tunnel Release Experience at King Hussein Medical Center Issam A. Dahabra MD* ABSTRACT Objective: To describe the results of the endoscopic carpal tunnel release using the MicroAire Carpal
Endoscopic Carpal Tunnel Release Experience at King Hussein Medical Center Issam A. Dahabra MD* ABSTRACT Objective: To describe the results of the endoscopic carpal tunnel release using the MicroAire Carpal
Manual therapy approach to the Patient with Carpal Tunnel Syndrome.
 Manual therapy approach to the Patient with Carpal Tunnel Syndrome www.fisiokinesiterapia.biz Symptoms and Signs Thumb, index, middle, and radial aspect of ring finger Hand Pain Paresthesia Numbness Pins
Manual therapy approach to the Patient with Carpal Tunnel Syndrome www.fisiokinesiterapia.biz Symptoms and Signs Thumb, index, middle, and radial aspect of ring finger Hand Pain Paresthesia Numbness Pins
EndoBlade Soft Tissue Release System
 Surgical Technique Endoscopic Gastroc Recession Endoscopic Plantar Fascia Release EndoBlade Soft Tissue Release System Endoscopic Gastroc Recession Arthrex has developed a comprehensive, completely disposable
Surgical Technique Endoscopic Gastroc Recession Endoscopic Plantar Fascia Release EndoBlade Soft Tissue Release System Endoscopic Gastroc Recession Arthrex has developed a comprehensive, completely disposable
Trigger Finger and Trigger Thumb A Patient's Guide to Trigger Finger & Trigger Thumb
 Trigger Finger and Trigger Thumb A Patient's Guide to Trigger Finger & Trigger Thumb Introduction Trigger finger and trigger thumb are conditions affecting the movement of the tendons as they bend the
Trigger Finger and Trigger Thumb A Patient's Guide to Trigger Finger & Trigger Thumb Introduction Trigger finger and trigger thumb are conditions affecting the movement of the tendons as they bend the
10/15/2014. Wrist. Clarification of Terms. Clarification of Terms cont
 Wrist Clarification of Terms Palmar is synonymous with anterior aspect of the wrist and hand Ventral is also synonymous with anterior aspect of the wrist and hand Dorsal refers to the posterior aspect
Wrist Clarification of Terms Palmar is synonymous with anterior aspect of the wrist and hand Ventral is also synonymous with anterior aspect of the wrist and hand Dorsal refers to the posterior aspect
Hand and Wrist Editing file. Color Code Important Doctors Notes Notes/Extra explanation
 Hand and Wrist Editing file Color Code Important Doctors Notes Notes/Extra explanation Objectives Describe the anatomy of the deep fascia of the wrist & hand (flexor & extensor retinacula & palmar aponeurosis).
Hand and Wrist Editing file Color Code Important Doctors Notes Notes/Extra explanation Objectives Describe the anatomy of the deep fascia of the wrist & hand (flexor & extensor retinacula & palmar aponeurosis).
Integra. Endoscopic Gastrocnemius Release System SURGICAL TECHNIQUE
 Integra Endoscopic Gastrocnemius Release System SURGICAL TECHNIQUE Table of Contents Indications... 2 Contraindications... 2 System Description... 2 Features and Benefits... 2 Surgical Site Preparation...3
Integra Endoscopic Gastrocnemius Release System SURGICAL TECHNIQUE Table of Contents Indications... 2 Contraindications... 2 System Description... 2 Features and Benefits... 2 Surgical Site Preparation...3
Main Menu. Wrist and Hand Joints click here. The Power is in Your Hands
 1 The Wrist and Hand Joints click here Main Menu K.5 http://www.handsonlineeducation.com/classes/k5/k5entry.htm[3/23/18, 1:40:40 PM] Bones 29 bones, including radius and ulna 8 carpal bones in 2 rows of
1 The Wrist and Hand Joints click here Main Menu K.5 http://www.handsonlineeducation.com/classes/k5/k5entry.htm[3/23/18, 1:40:40 PM] Bones 29 bones, including radius and ulna 8 carpal bones in 2 rows of
Ultrasonography of Peripheral Nerve -upper extremity
 Ultrasonography of Peripheral Nerve -upper extremity Department of Physical Medicine and Rehabilitation Korea University Guro Hospital Korea University College of Medicine Yoon Joon Shik Normal median
Ultrasonography of Peripheral Nerve -upper extremity Department of Physical Medicine and Rehabilitation Korea University Guro Hospital Korea University College of Medicine Yoon Joon Shik Normal median
Levels of the anatomical cuts of the upper extremity RADIUS AND ULNA right
 11 CHAPTER 2 Levels of the anatomical cuts of the upper extremity AND right CUT 1 CUT 4 1 2 3 4 5 6 Isolated fixation of the radius is difficult at this level because of the anterolateral vessels and the
11 CHAPTER 2 Levels of the anatomical cuts of the upper extremity AND right CUT 1 CUT 4 1 2 3 4 5 6 Isolated fixation of the radius is difficult at this level because of the anterolateral vessels and the
Wrist and Hand Anatomy/Biomechanics
 Wrist and Hand Anatomy/Biomechanics Kristin Kelley, DPT, OCS, FAAOMPT Orthopaedic Manual Physical Therapy Series Charlottesville 2017-2018 Orthopaedic Manual Physical Therapy Series 2017-2018 Anatomy -
Wrist and Hand Anatomy/Biomechanics Kristin Kelley, DPT, OCS, FAAOMPT Orthopaedic Manual Physical Therapy Series Charlottesville 2017-2018 Orthopaedic Manual Physical Therapy Series 2017-2018 Anatomy -
Anatomy - Hand. Wrist and Hand Anatomy/Biomechanics. Osteology. Carpal Arch. Property of VOMPTI, LLC
 Wrist and Hand Anatomy/Biomechanics Kristin Kelley, DPT, OCS, FAAOMPT The wrist The metacarpals The Phalanges Digit 1 thumb Digit 5 digiti minimi Anatomy - Hand Orthopaedic Manual Physical Therapy Series
Wrist and Hand Anatomy/Biomechanics Kristin Kelley, DPT, OCS, FAAOMPT The wrist The metacarpals The Phalanges Digit 1 thumb Digit 5 digiti minimi Anatomy - Hand Orthopaedic Manual Physical Therapy Series
Chapter 4: Forearm 4.3 Forearm shaft fractures, transverse (12-D/4)
") AO Manual of ESIN in children s fractures Chapter 4: Forearm 4.3 Forearm shaft fractures, transverse (12-D/4) Title AO Manual of ESIN in children Subtitle Elastic stable intramedullary nailing (ESIN) Author
AO Manual of ESIN in children s fractures Chapter 4: Forearm 4.3 Forearm shaft fractures, transverse (12-D/4) Title AO Manual of ESIN in children Subtitle Elastic stable intramedullary nailing (ESIN) Author
The hand is full with sweat glands, activated at times of stress. In Slide #2 there was a mistake where the doctor mentioned lateral septum twice.
 We should only know: Name, action & nerve supply Layers - Skin - Superficial fascia - Deep fascia The hand is full with sweat glands, activated at times of stress. Deep fascia In Slide #2 there was a mistake
We should only know: Name, action & nerve supply Layers - Skin - Superficial fascia - Deep fascia The hand is full with sweat glands, activated at times of stress. Deep fascia In Slide #2 there was a mistake
Lecture 9: Forearm bones and muscles
 Lecture 9: Forearm bones and muscles Remember, the region between the shoulder and the elbow = brachium/arm, between elbow and wrist = antebrachium/forearm. Forearm bones : Humerus (distal ends) Radius
Lecture 9: Forearm bones and muscles Remember, the region between the shoulder and the elbow = brachium/arm, between elbow and wrist = antebrachium/forearm. Forearm bones : Humerus (distal ends) Radius
ARM Brachium Musculature
 ARM Brachium Musculature Coracobrachialis coracoid process of the scapula medial shaft of the humerus at about its middle 1. flexes the humerus 2. assists to adduct the humerus Blood: muscular branches
ARM Brachium Musculature Coracobrachialis coracoid process of the scapula medial shaft of the humerus at about its middle 1. flexes the humerus 2. assists to adduct the humerus Blood: muscular branches
MCQWeek2. All arise from the common flexor origin. The posterior aspect of the medial epicondyle is the common flexor origin.
 MCQWeek2. 1. Regarding superficial muscles of anterior compartment of the forearm: All arise from the common flexor origin. The posterior aspect of the medial epicondyle is the common flexor origin. Flexor
MCQWeek2. 1. Regarding superficial muscles of anterior compartment of the forearm: All arise from the common flexor origin. The posterior aspect of the medial epicondyle is the common flexor origin. Flexor
Anatomy Workshop Upper Extremity David Ebaugh, PT, PhD Workshop Leader. Lab Leaders: STATION I BRACHIAL PLEXUS
 Anatomy Workshop Upper Extremity David Ebaugh, PT, PhD Workshop Leader Lab Leaders: STATION I BRACHIAL PLEXUS A. Posterior cervical triangle and axilla B. Formation of plexus 1. Ventral rami C5-T1 2. Trunks
Anatomy Workshop Upper Extremity David Ebaugh, PT, PhD Workshop Leader Lab Leaders: STATION I BRACHIAL PLEXUS A. Posterior cervical triangle and axilla B. Formation of plexus 1. Ventral rami C5-T1 2. Trunks
Physical therapy of the wrist and hand
 Physical therapy of the wrist and hand Functional anatomy wrist and hand The wrist includes distal radius, scaphoid, lunate, triquetrum, pisiform, trapezium, trapezoid, capitate, and hamate. The hand includes
Physical therapy of the wrist and hand Functional anatomy wrist and hand The wrist includes distal radius, scaphoid, lunate, triquetrum, pisiform, trapezium, trapezoid, capitate, and hamate. The hand includes
Common Upper Extremity Neuropathies (Not Carpal Tunnel Syndrome)
") Common Upper Extremity Neuropathies (Not Carpal Tunnel Syndrome) Nerve Compressions Common in adults, rare in children Frequently cause missed days of work and sleepless nights CDC 2001 26,794 cases of
Common Upper Extremity Neuropathies (Not Carpal Tunnel Syndrome) Nerve Compressions Common in adults, rare in children Frequently cause missed days of work and sleepless nights CDC 2001 26,794 cases of
The hand. it's the most important subject of the upper limb because it has a clinical importance. the palm of the hand**
 Today at 12:48 AM The hand it's the most important subject of the upper limb because it has a clinical importance. the palm of the hand** -the palmar aponeurosis located in the palm of the hand which is
Today at 12:48 AM The hand it's the most important subject of the upper limb because it has a clinical importance. the palm of the hand** -the palmar aponeurosis located in the palm of the hand which is
divided by the bones ( redius and ulna ) and interosseous membrane into :
 and interosseous membrane into :") fossa Cubital Has: * floor. * roof : - Skin - superficial fasica - deep fascia ( include bicipital aponeurosis ) Structures within the roof : -cephalic and basilic veins -and between them median cubital
fossa Cubital Has: * floor. * roof : - Skin - superficial fasica - deep fascia ( include bicipital aponeurosis ) Structures within the roof : -cephalic and basilic veins -and between them median cubital
Hand and wrist emergencies
 Chapter1 Hand and wrist emergencies Carl A. Germann Distal radius and ulnar injuries PEARL: Fractures of the distal radius and ulna are the most common type of fractures in patients younger than 75 years.
Chapter1 Hand and wrist emergencies Carl A. Germann Distal radius and ulnar injuries PEARL: Fractures of the distal radius and ulna are the most common type of fractures in patients younger than 75 years.
Wrist & Hand Assessment and General View
 Wrist & Hand Assessment and General View Done by; Mshari S. Alghadier BSc Physical Therapy RHPT 366 m.alghadier@sau.edu.sa http://faculty.sau.edu.sa/m.alghadier/ Functional anatomy The hand can be divided
Wrist & Hand Assessment and General View Done by; Mshari S. Alghadier BSc Physical Therapy RHPT 366 m.alghadier@sau.edu.sa http://faculty.sau.edu.sa/m.alghadier/ Functional anatomy The hand can be divided
Chapter 39. Volar surface incisions
 Chapter 39 EXPLORATION OF AN INJURED HAND OR FOREARM KEY FIGURES: Tourniquet Midlateral finger incisions Brunner zigzag incisions Volar surface incisions Dorsal incisions Proximal and distal extension
Chapter 39 EXPLORATION OF AN INJURED HAND OR FOREARM KEY FIGURES: Tourniquet Midlateral finger incisions Brunner zigzag incisions Volar surface incisions Dorsal incisions Proximal and distal extension
Introduction. The wrist contains eight small carpal bones, which as a group act as a flexible spacer between the forearm and hand.
 Wrist Introduction The wrist contains eight small carpal bones, which as a group act as a flexible spacer between the forearm and hand. Distal forearm Distal forearm 4 Distal end of the radius A. anterior
Wrist Introduction The wrist contains eight small carpal bones, which as a group act as a flexible spacer between the forearm and hand. Distal forearm Distal forearm 4 Distal end of the radius A. anterior
Nerves of Upper limb. Dr. Brijendra Singh Professor & Head Department of Anatomy AIIMS Rishikesh
 Nerves of Upper limb Dr. Brijendra Singh Professor & Head Department of Anatomy AIIMS Rishikesh 1 Objectives Origin, course & relation of median & ulnar nerves. Motor & sensory distribution Carpal tunnel
Nerves of Upper limb Dr. Brijendra Singh Professor & Head Department of Anatomy AIIMS Rishikesh 1 Objectives Origin, course & relation of median & ulnar nerves. Motor & sensory distribution Carpal tunnel
Duputytren's Contracture
 Disclaimer This movie is an educational resource only and should not be used to manage Orthopaedic Health. All decisions about must be made in conjunction with your Physician or a licensed healthcare provider.
Disclaimer This movie is an educational resource only and should not be used to manage Orthopaedic Health. All decisions about must be made in conjunction with your Physician or a licensed healthcare provider.
A Patient's Guide to Ganglions of the Wrist
 Introduction A ganglion is a small, harmless cyst, or sac of fluid, that sometimes develops in the wrist. Doctors don't know exactly what causes ganglions, but a ganglion that isn't painful and doesn't
Introduction A ganglion is a small, harmless cyst, or sac of fluid, that sometimes develops in the wrist. Doctors don't know exactly what causes ganglions, but a ganglion that isn't painful and doesn't
CARPAL TUNNEL SYNDROME
 CARPAL TUNNEL SYNDROME Carpal tunnel syndrome results from the pinching or entrapping of the median nerve in the underside of the wrist. The actual pathology in most cases is due to either a decrease in
CARPAL TUNNEL SYNDROME Carpal tunnel syndrome results from the pinching or entrapping of the median nerve in the underside of the wrist. The actual pathology in most cases is due to either a decrease in
The Language of Anatomy. (Anatomical Terminology)
") The Language of Anatomy (Anatomical Terminology) Terms of Position The anatomical position is a fixed position of the body (cadaver) taken as if the body is standing (erect) looking forward with the upper
The Language of Anatomy (Anatomical Terminology) Terms of Position The anatomical position is a fixed position of the body (cadaver) taken as if the body is standing (erect) looking forward with the upper
Injuries to the Hands and Feet
 Injuries to the Hands and Feet Chapter 26 Injuries to the Hands and Feet Introduction Combat injuries to the hands and feet differ from those of the arms and legs in terms of mortality and morbidity. Death
Injuries to the Hands and Feet Chapter 26 Injuries to the Hands and Feet Introduction Combat injuries to the hands and feet differ from those of the arms and legs in terms of mortality and morbidity. Death
CARPAL TUNNEL RELEASE BLOCK Author John Hyndman
 Questions CARPAL TUNNEL RELEASE BLOCK Author John Hyndman Web Editor Kirsten Fehrmann - kirstenfehrmann@hotmail.com 1) Why does a LA solution containing Epinephrine cause pain on injection and what can
Questions CARPAL TUNNEL RELEASE BLOCK Author John Hyndman Web Editor Kirsten Fehrmann - kirstenfehrmann@hotmail.com 1) Why does a LA solution containing Epinephrine cause pain on injection and what can
79b Orthopedic Massage: Technique Demo and Practice! Rotator Cuff and Carpal Tunnel!
 79b Orthopedic Massage: Technique Demo and Practice! Rotator Cuff and Carpal Tunnel! 79b Orthopedic Massage: Technique Demo and Practice! Rotator Cuff and Carpal Tunnel! Class Outline" 5 minutes" "Attendance,
79b Orthopedic Massage: Technique Demo and Practice! Rotator Cuff and Carpal Tunnel! 79b Orthopedic Massage: Technique Demo and Practice! Rotator Cuff and Carpal Tunnel! Class Outline" 5 minutes" "Attendance,
Shoulder Surgery. Gregory M. Behm, MD Ravalli Orthopedics & Sports Medicine
 Shoulder Surgery The purpose of this handout is to help you understand the way I perform shoulder surgeries and to help you plan for the recovery. Below are some general items that apply to most surgeries
Shoulder Surgery The purpose of this handout is to help you understand the way I perform shoulder surgeries and to help you plan for the recovery. Below are some general items that apply to most surgeries
Forearm and Wrist Regions Neumann Chapter 7
 Forearm and Wrist Regions Neumann Chapter 7 REVIEW AND HIGHLIGHTS OF OSTEOLOGY & ARTHROLOGY Radius dorsal radial tubercle radial styloid process Ulna ulnar styloid process ulnar head Carpals Proximal Row
Forearm and Wrist Regions Neumann Chapter 7 REVIEW AND HIGHLIGHTS OF OSTEOLOGY & ARTHROLOGY Radius dorsal radial tubercle radial styloid process Ulna ulnar styloid process ulnar head Carpals Proximal Row
Acu-Loc Wrist Plating System. Surgical Technique
 Acu-Loc Wrist Plating System Surgical Technique Acumed is a global leader of innovative orthopaedic and medical solutions. We are dedicated to developing products, service methods, and approaches that
Acu-Loc Wrist Plating System Surgical Technique Acumed is a global leader of innovative orthopaedic and medical solutions. We are dedicated to developing products, service methods, and approaches that
80b Orthopedic Massage: Technique Review and Practice! Rotator Cuff and Carpal Tunnel!
 80b Orthopedic Massage: Technique Review and Practice! Rotator Cuff and Carpal Tunnel! 80b Orthopedic Massage: Technique Review and Practice! Rotator Cuff and Carpal Tunnel! Class Outline 5 minutes Attendance,
80b Orthopedic Massage: Technique Review and Practice! Rotator Cuff and Carpal Tunnel! 80b Orthopedic Massage: Technique Review and Practice! Rotator Cuff and Carpal Tunnel! Class Outline 5 minutes Attendance,
Kinesiology of The Wrist and Hand. Cuneyt Mirzanli Istanbul Gelisim University
 Kinesiology of The Wrist and Hand Cuneyt Mirzanli Istanbul Gelisim University Bones The wrist and hand contain 29 bones including the radius and ulna. There are eight carpal bones in two rows of four to
Kinesiology of The Wrist and Hand Cuneyt Mirzanli Istanbul Gelisim University Bones The wrist and hand contain 29 bones including the radius and ulna. There are eight carpal bones in two rows of four to
Hand / wrist Injections. MATS. June Condition Symptoms Conservative Treatments Location of injection CBA for surgery
 Hand / wrist Injections. MATS. June 2018. Condition Symptoms Conservative Treatments Location of injection CBA for surgery Carpal Tunnel Tingling / numbness in median nerve distribution (lateral 3 fingers)
Hand / wrist Injections. MATS. June 2018. Condition Symptoms Conservative Treatments Location of injection CBA for surgery Carpal Tunnel Tingling / numbness in median nerve distribution (lateral 3 fingers)
Viorel Nacu. The clinical anatomy of the Hand
 Viorel Nacu The clinical anatomy of the Hand The distal part of the upper limb is divided in to three regions: 1. The wrist (carpus) 2. The hand (metacarpus) 3. The digits (fingers) The landmarks of this
Viorel Nacu The clinical anatomy of the Hand The distal part of the upper limb is divided in to three regions: 1. The wrist (carpus) 2. The hand (metacarpus) 3. The digits (fingers) The landmarks of this
Muscles of the hand Prof. Abdulameer Al-Nuaimi
 Muscles of the hand Prof. Abdulameer Al-Nuaimi a.alnuaimi@sheffield.ac.uk abdulameerh@yahoo.com Thenar Muscles Thenar muscles are three short muscles located at base of the thumb. All are innervated by
Muscles of the hand Prof. Abdulameer Al-Nuaimi a.alnuaimi@sheffield.ac.uk abdulameerh@yahoo.com Thenar Muscles Thenar muscles are three short muscles located at base of the thumb. All are innervated by
Breast conservation surgery and sentinal node biopsy: Dr R Botha Moderator: Dr E Osman
 Breast conservation surgery and sentinal node biopsy: Dr R Botha Moderator: Dr E Osman Breast anatomy: Breast conserving surgery: The aim of wide local excision is to remove all invasive and in situ
Breast conservation surgery and sentinal node biopsy: Dr R Botha Moderator: Dr E Osman Breast anatomy: Breast conserving surgery: The aim of wide local excision is to remove all invasive and in situ
TIE-IN. trapezium IMPLANT. surgical technique. presented by by James H. Calandruccio, MD and Mark T. Jobe, MD
 TRAPEZIUM IMPLANT TIE-IN trapezium IMPLANT surgical technique presented by by James H. Calandruccio, MD and Mark T. Jobe, MD TIE-IN TRAPEZIUM IMPLANT as described by James H. Calandruccio, MD and Mark
TRAPEZIUM IMPLANT TIE-IN trapezium IMPLANT surgical technique presented by by James H. Calandruccio, MD and Mark T. Jobe, MD TIE-IN TRAPEZIUM IMPLANT as described by James H. Calandruccio, MD and Mark
Compartment Syndrome
 Compartment Syndrome Chapter 34 Compartment Syndrome Introduction Compartment syndrome may occur with an injury to any fascial compartment. The fascial defect caused by the injury may not be adequate to
Compartment Syndrome Chapter 34 Compartment Syndrome Introduction Compartment syndrome may occur with an injury to any fascial compartment. The fascial defect caused by the injury may not be adequate to
Nerves of the upper limb Prof. Abdulameer Al-Nuaimi. E. mail:
 Nerves of the upper limb Prof. Abdulameer Al-Nuaimi E-mail: a.al-nuaimi@sheffield.ac.uk E. mail: abdulameerh@yahoo.com Brachial plexus Median nerve After originating from the brachial plexus in the axilla,
Nerves of the upper limb Prof. Abdulameer Al-Nuaimi E-mail: a.al-nuaimi@sheffield.ac.uk E. mail: abdulameerh@yahoo.com Brachial plexus Median nerve After originating from the brachial plexus in the axilla,
Case 1. Your diagnosis
 Case 1 44-year-old midwife presented with intermittent pins and needles in the little and ring fingers with blanching. Symptoms were exacerbated by cold exposure. Your diagnosis Diagnosis Hypothenar syndrome
Case 1 44-year-old midwife presented with intermittent pins and needles in the little and ring fingers with blanching. Symptoms were exacerbated by cold exposure. Your diagnosis Diagnosis Hypothenar syndrome
A Patient s Guide to Elbow Anatomy
 A Patient s Guide to Elbow Anatomy Iain is a specialist in musculoskeletal imaging and the diagnosis of musculoskeletal pain. This information is provided with the hope that you can better understand and
A Patient s Guide to Elbow Anatomy Iain is a specialist in musculoskeletal imaging and the diagnosis of musculoskeletal pain. This information is provided with the hope that you can better understand and
A Patient s Guide to Ganglions of the Wrist
 A Patient s Guide to Ganglions of the Wrist 20295 NE 29th Place, Ste 300 Aventura, FL 33180 Phone: (786) 629-0910 Fax: (786) 629-0920 admin@instituteofsports.com DISCLAIMER: The information in this booklet
A Patient s Guide to Ganglions of the Wrist 20295 NE 29th Place, Ste 300 Aventura, FL 33180 Phone: (786) 629-0910 Fax: (786) 629-0920 admin@instituteofsports.com DISCLAIMER: The information in this booklet
AcUMEDr. FoREARM ROD SYSTEM
 AcUMEDr FoREARM ROD SYSTEM FoREARM ROD SYSTEM Since 1988 Acumed has been designing solutions to the demanding situations facing orthopedic surgeons, hospitals and their patients. Our strategy has been
AcUMEDr FoREARM ROD SYSTEM FoREARM ROD SYSTEM Since 1988 Acumed has been designing solutions to the demanding situations facing orthopedic surgeons, hospitals and their patients. Our strategy has been
[[Sally Leaning Towards Peter To Take Cold Hand]]
![[[Sally Leaning Towards Peter To Take Cold Hand]]](/thumbs/84/91174469.jpg "[[Sally Leaning Towards Peter To Take Cold Hand]]") In this lecture we will talk about the bones of the hand, and the muscles and contents of the forearm. *The hand bones are: - Carpal bones. -Metacarpals. -Phalanges. *The carpal bones (wrist bones): They
In this lecture we will talk about the bones of the hand, and the muscles and contents of the forearm. *The hand bones are: - Carpal bones. -Metacarpals. -Phalanges. *The carpal bones (wrist bones): They
Chapter 24. Arthroscopic Thumb Carpometacarpal Interposition Arthroplasty. Introduction. Operative Technique. Patient Preparation and Positioning
 Chapter 24 Arthroscopic Thumb Carpometacarpal Interposition Arthroplasty Introduction Osteoarthritis in the thumb carpometacarpal (CMC) joint is a common condition, especially in women over 60 years of
Chapter 24 Arthroscopic Thumb Carpometacarpal Interposition Arthroplasty Introduction Osteoarthritis in the thumb carpometacarpal (CMC) joint is a common condition, especially in women over 60 years of
Flexor Tendon Lacerations
 Flexor Tendon Lacerations When a Flexor Tendon Is Cut Tendons are cordlike fibers that connect muscle to bone. The flexor tendons attach muscles in the forearm to bones on the palm side of the fingers.
Flexor Tendon Lacerations When a Flexor Tendon Is Cut Tendons are cordlike fibers that connect muscle to bone. The flexor tendons attach muscles in the forearm to bones on the palm side of the fingers.
EPF Endoscopic Plantar Fasciotomy. Operative technique
 Endoscopic Plantar Fasciotomy Operative technique Endoscopic Plantar Fasciotomy Table of contents Introduction 3 Operative technique 4 This publication sets forth detailed recommended procedures for using
Endoscopic Plantar Fasciotomy Operative technique Endoscopic Plantar Fasciotomy Table of contents Introduction 3 Operative technique 4 This publication sets forth detailed recommended procedures for using
The Muscular System. Chapter 10 Part C. PowerPoint Lecture Slides prepared by Karen Dunbar Kareiva Ivy Tech Community College
 Chapter 10 Part C The Muscular System Annie Leibovitz/Contact Press Images PowerPoint Lecture Slides prepared by Karen Dunbar Kareiva Ivy Tech Community College Table 10.9: Muscles Crossing the Shoulder
Chapter 10 Part C The Muscular System Annie Leibovitz/Contact Press Images PowerPoint Lecture Slides prepared by Karen Dunbar Kareiva Ivy Tech Community College Table 10.9: Muscles Crossing the Shoulder
ULTRASOUND GUIDED NERVE BLOCKS
 2 ULTRASOUND GUIDED NERVE BLOCKS Elizabeth Kwan, MD UCSF High Risk Emergency Medicine 2014 1 Instructors Kristin Berona Reza Danesh Sally Graglia Daniel Kievlan Starr Knight Allison Mulcahy Carmen Partida
2 ULTRASOUND GUIDED NERVE BLOCKS Elizabeth Kwan, MD UCSF High Risk Emergency Medicine 2014 1 Instructors Kristin Berona Reza Danesh Sally Graglia Daniel Kievlan Starr Knight Allison Mulcahy Carmen Partida
 P R E S E N T S Dr. Mufa T. Ghadiali is skilled in all aspects of General Surgery. His General Surgery Services include: General Surgery Advanced Laparoscopic Surgery Surgical Oncology Gastrointestinal
P R E S E N T S Dr. Mufa T. Ghadiali is skilled in all aspects of General Surgery. His General Surgery Services include: General Surgery Advanced Laparoscopic Surgery Surgical Oncology Gastrointestinal
Upper Extremity Fractures
 Upper Extremity Fractures Ranie Whatley, RN,FNP-C David W. Gray, MD Skeletal Trauma 10 to 15 % of all Childhood Injuries Physeal (Growth Plate) Injuries are ~ 15% of all Skeletal Injuries Orthopaedic Assessment
Upper Extremity Fractures Ranie Whatley, RN,FNP-C David W. Gray, MD Skeletal Trauma 10 to 15 % of all Childhood Injuries Physeal (Growth Plate) Injuries are ~ 15% of all Skeletal Injuries Orthopaedic Assessment
Ligaments of Elbow hinge: sagittal plane so need lateral and medial ligaments
 Ligaments of Elbow hinge: sagittal plane so need lateral and medial ligaments Ulnar Collateral ligament on medial side; arising from medial epicondyle and stops excess valgus movement (lateral movement)
Ligaments of Elbow hinge: sagittal plane so need lateral and medial ligaments Ulnar Collateral ligament on medial side; arising from medial epicondyle and stops excess valgus movement (lateral movement)
Carpal Tunnel Release: Analysis of Carpal Tunnel Syndrome and Rehabilitation. Michael Commesso, Nicholas Francisco, and Maritza Rodriguez
 Carpal Tunnel Release: Analysis of Carpal Tunnel Syndrome and Rehabilitation Michael Commesso, Nicholas Francisco, and Maritza Rodriguez PHYT 625: Movement Analysis & Patient/Client Management I Abstract
Carpal Tunnel Release: Analysis of Carpal Tunnel Syndrome and Rehabilitation Michael Commesso, Nicholas Francisco, and Maritza Rodriguez PHYT 625: Movement Analysis & Patient/Client Management I Abstract
Benefits of Aspiration and Injection JOINT INJECTIONS. Injection Indications. Mechanism of Action 1/11/2016
 Benefits of Aspiration and Injection JOINT INJECTIONS Mark Niedfeldt, M.D. Medical College of Wisconsin Decrease or resolution of pain Decrease or resolution of inflammation Decrease or resolution of effusion
Benefits of Aspiration and Injection JOINT INJECTIONS Mark Niedfeldt, M.D. Medical College of Wisconsin Decrease or resolution of pain Decrease or resolution of inflammation Decrease or resolution of effusion
Intrinsic muscles palsies of the hand Management of Thumb Opposition with BURKHALTER s Procedure
 Intrinsic muscles palsies of the hand Management of Thumb Opposition with BURKHALTER s Procedure TRUONG LE DAO, MD, IFAAD 1 Burkhalter W.E, Cristhensen R.C, Brown P.W, Extensor Indicis Proprius opponensplasty
Intrinsic muscles palsies of the hand Management of Thumb Opposition with BURKHALTER s Procedure TRUONG LE DAO, MD, IFAAD 1 Burkhalter W.E, Cristhensen R.C, Brown P.W, Extensor Indicis Proprius opponensplasty
Transfemoral Amputation
 Transfemoral Amputation Pre-Op: 42 year old male who sustained severe injuries in a motorcycle accident. Note: he is a previous renal transplant recipient and is on immunosuppressive treatments. His injuries
Transfemoral Amputation Pre-Op: 42 year old male who sustained severe injuries in a motorcycle accident. Note: he is a previous renal transplant recipient and is on immunosuppressive treatments. His injuries
WEEKEND 2 Elbow. Elbow Range of Motion Assessment
 Virginia Orthopedic Manual Physical Therapy Institute - 2016 Technique Manual WEEKEND 2 Elbow Elbow Range of Motion Assessment - Patient Positioning: Sitting or supine towards the edge of the bed - Indications:
Virginia Orthopedic Manual Physical Therapy Institute - 2016 Technique Manual WEEKEND 2 Elbow Elbow Range of Motion Assessment - Patient Positioning: Sitting or supine towards the edge of the bed - Indications:
Trigger Finger Release
 Trigger Finger Release Trigger finger, also known as stenosing tenosynovitis, occurs when one of the tendons responsible for bending a finger or the thumb develops a thickening, known as a nodule, and
Trigger Finger Release Trigger finger, also known as stenosing tenosynovitis, occurs when one of the tendons responsible for bending a finger or the thumb develops a thickening, known as a nodule, and
Integra. Spider and Mini Spider Limited Wrist Fusion System SURGICAL TECHNIQUE
 Integra Spider and Mini Spider Limited Wrist Fusion System SURGICAL TECHNIQUE Table of contents Description... 02 Indications... 02 Contraindications... 02 Surgical Technique... 03 Spider Introduction-Four
Integra Spider and Mini Spider Limited Wrist Fusion System SURGICAL TECHNIQUE Table of contents Description... 02 Indications... 02 Contraindications... 02 Surgical Technique... 03 Spider Introduction-Four
INTRODUCTION Cubital Tunnel Syndrome
 INTRODUCTION Cubital Tunnel Syndrome Diagram of the ulnar nerve supplying the muscles of forearm and hand Cubital Tunnel is a condition that refers to the ulnar nerve being compressed around the elbow.
INTRODUCTION Cubital Tunnel Syndrome Diagram of the ulnar nerve supplying the muscles of forearm and hand Cubital Tunnel is a condition that refers to the ulnar nerve being compressed around the elbow.
Key Points for Success:
 SELF WRIST & HAND 1 2 All of the stretches described in this chapter are detailed to stretch the right side. Key Points for Success: Sit comfortably in a position where you can straighten or fully extend
SELF WRIST & HAND 1 2 All of the stretches described in this chapter are detailed to stretch the right side. Key Points for Success: Sit comfortably in a position where you can straighten or fully extend
Scaphoid Fracture of the Wrist
 A Patient s Guide to Scaphoid Fracture of the Wrist 651 Old Country Road Plainview, NY 11803 Phone: 5166818822 Fax: 5166813332 p.lettieri@aol.com DISCLAIMER: The information in this booklet is compiled
A Patient s Guide to Scaphoid Fracture of the Wrist 651 Old Country Road Plainview, NY 11803 Phone: 5166818822 Fax: 5166813332 p.lettieri@aol.com DISCLAIMER: The information in this booklet is compiled
Exam of the Injured Hand and Wrist. Christina M. Ward, MD Regions Hospital TRIA Woodbury
 Exam of the Injured Hand and Wrist Christina M. Ward, MD Regions Hospital TRIA Woodbury Disclosures We have no disclosures that are pertinent to this presentation Terminology Ring Long Index Small Thumb
Exam of the Injured Hand and Wrist Christina M. Ward, MD Regions Hospital TRIA Woodbury Disclosures We have no disclosures that are pertinent to this presentation Terminology Ring Long Index Small Thumb
Biceps Brachii. Muscles of the Arm and Hand 4/4/2017 MR. S. KELLY
 Muscles of the Arm and Hand PSK 4U MR. S. KELLY NORTH GRENVILLE DHS Biceps Brachii Origin: scapula Insertion: radius, fascia of forearm (bicipital aponeurosis) Action: supination and elbow flexion Innervation:
Muscles of the Arm and Hand PSK 4U MR. S. KELLY NORTH GRENVILLE DHS Biceps Brachii Origin: scapula Insertion: radius, fascia of forearm (bicipital aponeurosis) Action: supination and elbow flexion Innervation:
ORTHOPAEDIC INJECTION AND ASPIRATION TECHNIQUES
 ORTHOPAEDIC INJECTION AND ASPIRATION TECHNIQUES OAAPN October 20, 2016 David H. Sohn, JD MD Chief, Shoulder and Sports Medicine University of Toledo Medical Center When to aspirate? To rule out infection
ORTHOPAEDIC INJECTION AND ASPIRATION TECHNIQUES OAAPN October 20, 2016 David H. Sohn, JD MD Chief, Shoulder and Sports Medicine University of Toledo Medical Center When to aspirate? To rule out infection
RADIOGRAPHY OF THE WRIST
 RADIOGRAPHY OF THE WRIST Patient Position: WRIST PA Projection, elbow in same plane Part Position: Hand ; fingers centered to IR Central Ray: Structures Shown: NOTE: Optional AP projection best demonstrates
RADIOGRAPHY OF THE WRIST Patient Position: WRIST PA Projection, elbow in same plane Part Position: Hand ; fingers centered to IR Central Ray: Structures Shown: NOTE: Optional AP projection best demonstrates
Rotator Cuff Strain and Carpal Tunnel Syndrome
 Rotator Cuff Strain and Carpal Tunnel Syndrome 5 minutes: Attendance and Breath of Arrival 50 minutes: Problem-Solving: SG, Arms, and Hands Punctuality- everybody's time is precious: o o Be ready to learn
Rotator Cuff Strain and Carpal Tunnel Syndrome 5 minutes: Attendance and Breath of Arrival 50 minutes: Problem-Solving: SG, Arms, and Hands Punctuality- everybody's time is precious: o o Be ready to learn
CARPAL TUNNEL RELEASE VIA MINI-OPEN WRIST CREASE INCISION: PROCEDURE AND RESULTS OF FOUR YEARS CLINICAL EXPERIENCE
 CARPAL TUNNEL RELEASE VIA MINI-OPEN WRIST CREASE INCISION: PROCEDURE AND RESULTS OF FOUR YEARS CLINICAL EXPERIENCE Sudqi A. Hamed 1, Falah Z. Harfoushi 2 ABSTRACT Objective: To evaluate prospectively the
CARPAL TUNNEL RELEASE VIA MINI-OPEN WRIST CREASE INCISION: PROCEDURE AND RESULTS OF FOUR YEARS CLINICAL EXPERIENCE Sudqi A. Hamed 1, Falah Z. Harfoushi 2 ABSTRACT Objective: To evaluate prospectively the
The Elbow and the cubital fossa. Prof Oluwadiya Kehinde
 The Elbow and the cubital fossa Prof Oluwadiya Kehinde www.oluwadiya.com Elbow and Forearm Anatomy The elbow joint is formed by the humerus, radius, and the ulna Bony anatomy of the elbow Distal Humerus
The Elbow and the cubital fossa Prof Oluwadiya Kehinde www.oluwadiya.com Elbow and Forearm Anatomy The elbow joint is formed by the humerus, radius, and the ulna Bony anatomy of the elbow Distal Humerus
The Forearm 2. Extensor & lateral Compartments of the Forearm
 The Forearm 2 Extensor & lateral Compartments of the Forearm 1-Lateral Fascial Compartment (at the lateral side of the forearm ) *Some books mention the lateral compartment contain just the Brachioradialis
The Forearm 2 Extensor & lateral Compartments of the Forearm 1-Lateral Fascial Compartment (at the lateral side of the forearm ) *Some books mention the lateral compartment contain just the Brachioradialis
Wrist and Hand Anatomy
 Wrist and Hand Anatomy Bone Anatomy Scapoid Lunate Triquetrium Pisiform Trapeziod Trapezium Capitate Hamate Wrist Articulations Radiocarpal Joint Proximal portion Distal portion Most surface contact found
Wrist and Hand Anatomy Bone Anatomy Scapoid Lunate Triquetrium Pisiform Trapeziod Trapezium Capitate Hamate Wrist Articulations Radiocarpal Joint Proximal portion Distal portion Most surface contact found
Modular Ulnar Head surgical technique. Transforming Extremities
 First Choice Modular Ulnar Head surgical technique Transforming Extremities instrumentation Head and Collar Trials Assembly Pad Starter Awl Trial Extractor Osteotomy Guide Stem Trials Implant Impactor
First Choice Modular Ulnar Head surgical technique Transforming Extremities instrumentation Head and Collar Trials Assembly Pad Starter Awl Trial Extractor Osteotomy Guide Stem Trials Implant Impactor
In the name of Allah, Most gracious, Most merciful
 In the name of Allah, Most gracious, Most merciful This lecture includes the following: The Palmer Oponeurosis. The Carpel tunnel. The palmaris brevis muscle. The anatomical snuffbox. The Fibrous flexor
In the name of Allah, Most gracious, Most merciful This lecture includes the following: The Palmer Oponeurosis. The Carpel tunnel. The palmaris brevis muscle. The anatomical snuffbox. The Fibrous flexor
Procedure: Chest Tube Placement (Tube Thoracostomy)
") Procedure: Chest Tube Placement (Tube Thoracostomy) Basic Information: The insertion and placement of a chest tube into the pleural cavity for the purpose of removing air, blood, purulent drainage, or
Procedure: Chest Tube Placement (Tube Thoracostomy) Basic Information: The insertion and placement of a chest tube into the pleural cavity for the purpose of removing air, blood, purulent drainage, or
STRUCTURAL BASIS OF MEDICAL PRACTICE EXAMINATION 5. September 30, 2011
 STRUCTURAL BASIS OF MEDICAL PRACTICE EXAMINATION 5 September 30, 2011 PART l. Answer in the space provided. (12 pts) 1. Identify the structures. (2 pts) EXAM NUMBER A. Suprascapular nerve B. Axillary nerve
STRUCTURAL BASIS OF MEDICAL PRACTICE EXAMINATION 5 September 30, 2011 PART l. Answer in the space provided. (12 pts) 1. Identify the structures. (2 pts) EXAM NUMBER A. Suprascapular nerve B. Axillary nerve
Surgical Anatomy of the Hip. Joseph H. Dimon
 Surgical Anatomy of the Hip Joseph H. Dimon The hip joint is a deep joint surrounded by large and powerful muscles necessary for its proper function. Essential neurovascular structures lie in front and
Surgical Anatomy of the Hip Joseph H. Dimon The hip joint is a deep joint surrounded by large and powerful muscles necessary for its proper function. Essential neurovascular structures lie in front and