Chapter 16: Using Therapeutic Exercise in Rehabilitation
|
|
|
- Camilla Parrish
- 5 years ago
- Views:
Transcription
1 Chapter 16: Using Therapeutic Exercise in Rehabilitation
2 Athletic Trainer s Approach to Rehabilitation Begins immediately after injury Initial first aid has a substantial impact on the injury One of ATC s primary responsibilities is to design, implement and supervise rehab plans Easy part is designing the program based on short and long term goals
3
4 Short term goals Control pain and inflammation Maintain or improve ROM Restore and increase strength Re-establish neuromuscular control Maintain levels of cardiorespiratory fitness Long term goals Return athlete to practice and competition quickly and safely Difficult part is knowing when and how to progress relative to the injury Progress should be based on specific criteria Return to play must be based on functional outcomes
5 Due to competitive nature of sports, rehab must be aggressive Must return to competition quickly and safely Rehab should be based on framework of healing process Understand time and sequence of healing and physiological principals Provide optimal healing environment ATC must have broad theoretical knowledge base of rehab techniques in order to select appropriately for each case No cookbook approach to rehab
6 Therapeutic Exercise Versus Conditioning Exercise Basic principle of strength training apply to rehabilitation Use conditioning to prevent injury and also to recover from injury Training and conditioning limit and minimize possibility of injury just as rehab works to return to play and prevent re-injury
7 Sudden Physical Inactivity and Injury Immobilization Body requires physical activity to maintain proper physical functioning When injury occurs Generalized loss of physical fitness due to loss of activity Specific inactivity of injured part resulting from immobilization or splinting of soft tissue Effects of General Inactivity Highly conditioned athlete will experience rapid generalized loss of fitness
8 Loss of muscle strength, endurance and coordination Athlete must continue to work entire body w/out aggravating the injury Effects of Immobilization Cause a number of disuse problems that impact muscle, joints, ligaments, bones, neuromuscular efficiency and cardiorespiratory system
9 Muscle Immobilization Atrophy and fiber conversion Loss of muscle mass - greatest atrophy occurring in Type I fibers Immobilization in a lengthened or neutral position tends to atrophy less Can be prevented through isometric contractions and electrical stimulation As unused muscle decreases in size, protein is also lost W/ normal activity protein synthesis is reestablished Decreased neuromuscular efficiency Motor nerves become less efficient in recruiting and stimulating individual fibers w/in a given motor unit After immobilization, function returns w/in 1 week
10 Joints and Immobilization Loss of normal compression leads to decreased lubrication, subsequently causing degeneration Cartilage is deprived of normal nutrition Continuous passive motion, electrical muscle stimulation or hinged casts help to retard loss of articular cartilage Ligaments and Bone and Immobilization Both adapt to normal stress - becoming or maintaining their strength W/out stress ligaments and bone become weaker High frequency, short duration endurance activity positively enhance collagen hypertrophy Full remodeling of ligament can take 12 months or more following immobilization
11 Cardiorespiratory System and Immobilization Resting heart rate increases approximately 1/2 beat per minute each day of immobilization Stroke volume, maximum oxygen uptake and vital capacity decrease concurrently w/ increased HR
12 Major Components of a Rehabilitation Program Well-designed rehab program should routinely address several key components before the athlete can return to pre-injury competitive levels Minimizing Initial Swelling Swelling is caused by many factors and must be controlled immediately after injury Minimizing swelling significantly speeds the healing process RICE!!!
13 Controlling Pain Some degree of pain will be experienced Pain will be dependent on the severity of the injury, athlete s response, perception of pain and the circumstances RICE, analgesics and medication can be used to modify pain Pain can interfere w/ rehab and therefore must be addressed throughout the rehab process Restoring Range of Motion Injury to a joint will always be associated w/ some loss of motion Due to contracture of connective tissue or resistance to stretch of musculotendinous unit
14 Physiological versus Accessory Movements Both occur simultaneously and ultimately work together Physiological movement results from active voluntary muscle contraction - moving an extremity through a ROM Accessory motion refers to the manner in which one articulating surface moves relative to another Must be normal to allow for full range of physiological movement If restricted, normal physiological cardinal plane movement will not occur
15 Rehab plans tend to concentrate on passive physiological movements If physiological movement is restricted, a stretching program designed to increase flexibility should be engaged If accessory motion is restricted, joint mobilization techniques should be used to address capsular and ligamentous dysfunction Restoring Muscular Strength, Endurance and Power Must work through a full pain free range of motion when working on strength
16 Isometrics Performed in early part of rehab following period of immobilization Used when resistance through full range could make injury worse Increase static strength, work to decrease/limit atrophy, create a muscle pump to decrease swelling Strength gains are limited primarily to angle at which joint is exercised, no functional force or eccentric work developed Difficult to motivate and measure force being applied
17 Progressive Resistance Exercise (PRE) Can be performed using a variety of equipment Utilizes isotonic contractions to generate force while muscle changes length Concentric and eccentric muscle contractions Traditionally focus on concentric exercises Eccentrics involved in deceleration of limbs Facilitate concentric contractions for plyometrics & incorporated w/ functional PNF strengthening exercises Both forms are contraction can be created using a variety of equipment Machines tend to limit movement in functional planes Machines and free weights are difficult to operate at functional speeds w/out injury

18 Tubing allows for a variety exercises Not encumbered by design of the machine Wide variety at low cost
19 Isokinetic Exercise Incorporated in later stage of rehabilitation process Uses fixed speeds w/ accommodating resistance to provide maximal resistance throughout ROM Isokinetic units allow for calculation of torque, force, average power, and work ratios which can be used by the clinician diagnostically Allows for work at more functional speeds Work at higher speeds tends to reduce joint compressive forces Can be used to develop neuromuscular pattern for functional speed and movements
20 Testing Strength, Endurance and Power Can be performed through Manual muscle tests Isotonic resistance Isokinetic dynamometers Isokinetic testing generally provides the most reliable and objective measures of change in strength

21
22 Re-establishing Neuromuscular Control, Proprioception, Kinesthesia and Joint Position Sense Following injury, body forgets how to integrate information coming in from multiple biological sources Neuromuscular control is mind s attempt to teach the body conscious control of a specific movement Re-establishing neuromuscular control requires repetition of same movement, step by step until it becomes automatic (progression from simple to difficult task Closed kinetic chain (CKC) exercises are essential for re-establishing control but can be difficult
23 Must regain established sensory pattern CNS constantly compares intent and production of specific movement w/ stored information, constantly modifying until discrepancy in movement is corrected Four key elements Proprioception and kinesthetic awareness Dynamic stability Preparatory and reactive muscle characteristics Conscious and unconscious functional and motor patterns Must relearn normal functional movement and timing after injury - may require several months Critical throughout rehab - most critical early in process to avoid reinjury
24 Reestablishing proprioception and kinesthesia should be of primary concern Proprioception is joint position sense (determine position of joint in space) Kinesthesia is the ability to detect movement Kinesthesia and proprioception are mediated by mechanoreceptors in muscle and joints, cutaneous, visual, and vestibular input Neuromuscular control relies on CNS to integrate all areas to produce coordinated movement
25 Joint Mechanoreceptors Found in ligaments, capsules, menisci, labra, and fat pads Ruffini s endings Pacinian corpuscles Free nerve endings Sensitive to changes in shape of structure and rate/direction of movement Most active at end of ranges of motion Muscle Mechanoreceptors Muscle spindles - sensitive to changes in length of muscle Golgi tendon organs - sensitive to changes in tissue tension
26 Regaining Balance Involves complex integration of muscular forces, neurological sensory information from mechanoreceptors and biomechanical information Entails positioning center of gravity (CoG) w/in the base of support If CoG extends beyond this base, the limits of stability have been exceeded and a corrective step or stumble will be necessary to prevent Even when motionless body is constantly undergoing constant postural sway w/ reflexive muscle contractions which correct and maintain dynamic equilibrium in an upright posture
27 When balanced is challenged the response is reflexive and automatic The primary mechanism for controlling balance occurs in the joints of the lower extremity The ability to balance and maintain it is critical for athletes If an athlete lacks balance or postural stability following injury, they may also lack proprioceptive and kinesthetic information or muscular strength which may limit their ability to generate an adequate response to disequilibrium A rehabilitation plan must incorporate functional activities that incorporate balance and proprioceptive training

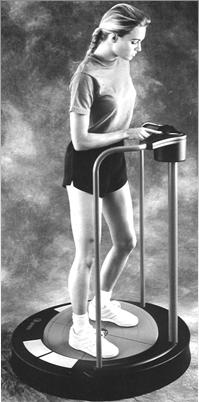

28 Balance Equipment
29 Maintaining Cardiorespiratory Fitness When injury occurs athlete is forced to miss training time which results in decreased cardiorespiratory endurance unless training occurs to help maintain it Alternative activities must be substituted that allow athlete to maintain fitness
30 Incorporating Functional Progressions Involves a series of gradually progressive activities designed to prepare the individual for return to a specific sport/activity Should be incorporated into treatment as early as possible Adequate program will gradually assist athlete regain pain free ROM, restoration of strength, and neuromuscular control Progression moves from simple to complex, slow to fast, short to long, light to heavy
31 New activities must be monitored closely to assure proper mechanics and form If pain and swelling do not arise, the activity can be advanced -- new activities should be added as quickly as possible As progress is made, the athlete should be returned to sports specific activity The optimal functional progression would be designed to allow opportunity for practice of every skill that is required for the sport This program will minimize the normal anxiety and apprehension experienced by the athlete upon return to the competitive environment Functional progression activities should be done during team practice - integrate athlete w/ team and coaches
32 Functional Testing Uses functional progression drills for the purpose of assessing the athlete s ability to perform a specific activity Entails a single maximal effort to gauge how close the athlete is to full return Variety of tests Shuttle runs Agility runs Figure 8 s Cariocca tests -Vertical jumps -Balance -Hopping for distance -Co-contraction test
33 Developing a Rehabilitative Plan Must be carefully designed Must have complete understanding of the injury: how it was sustained major anatomical structures involved the grade of trauma stage or phase of healing
34 Preoperative Exercise Phase Only applies to those requiring injury Exercise may be used as a means to improve outcome By allowing inflammation to subside, increasing strength, flexibility, cardiovascular fitness and neuromuscular control the athlete may be better prepared to continue rehab after surgery
35 Phase I - Acute Inflammatory Response Phase May last up to 4 days Immobility for the first 2 days is necessary to control inflammation Primary focus is to control swelling and modulate pain w/ RICE Early mobility during rehab is critical, however, being overly aggressive during the first 48 hours may not allow inflammatory process to accomplish its purpose Rest should be active - avoiding aggravating injury, but working to maintain other areas
36 By day 3 or 4 swelling begins to subside While it may be painful to the touch w/ some discoloration, gradual mobility exercises may be started (pain free ROM) If it is the lower extremity, athlete should be encouraged to bear weight The use of NSAID s may also be used to control swelling and inflammation
37 Phase 2: Repair Phase Repair is underway and pain is less Pain control is still critical The addition of cardio, strengthening, flexibility and neuromuscular activities should be gradually added Phase 3: The Maturation/Remodeling Phase Longest of 3 phases Pain is minimal (none to the touch) and collagen must be realigned according to tensile strength applied to them during functional activities
38 Focus is on regaining sport-specific skills Functional training - repeated performance of athletic skill for purpose of perfecting that skill Strengthening exercises should be used to place athlete under stresses and strains normally associated w/ athletic participation Plyometrics can be used to improve power and explosiveness Functional testing should be done to determine specific skill weaknesses that need to be addressed prior to full return Thermal modalities should be used to enhance tissue environment (reduce spasm, increase circulation, waste removal and reduce pain)
39 Exercise that is too intense or prolonged can be detrimental to progress Increases in swelling, pain, a loss or plateau in strength/rom, an increase in laxity or exacerbation of other symptoms indicates too great a load
40 Adherence to a Rehabilitation Program Athlete must comply to be successful To enhance adherence Provide encouragement Be creative Support from peers and coaches Provide a positive attitude Design clear plan and instructions Coach must support the rehabilitation process Make an effort to fit the program to the athlete s schedule Rehabilitation should be pain free
41 Criteria for Full Return to Activity Rehab plan must determine what is meant by complete recovery Athlete is fully reconditioned, achieved full ROM, strength, neuromuscular control, cardiovascular fitness and sports specific functional skills Athlete is mentally prepared The decision to return to play should be a group decision (sports medicine team) Team physician is ultimately responsible
42 Decision should address the following concerns Physiological healing constraints Pain status Swelling ROM, strength, neuromuscular control, proprioception, kinesthesia, cardiovascular fitness Sports-specific demands Functional testing Prophylactic strapping, bracing, padding Responsibility of the athlete Predisposition of the athlete Psychological factors Athlete education and preventative maintenance program
43 Additional Approaches to Therapeutic Exercise Open versus Closed Kinetic Chain Exercises Anatomical functional relationship in upper and lower extremities Open kinetic chain exists when foot or hand is not in contact w/ ground or other surface Closed kinetic chain = foot or hand is weight bearing Forces begin at ground and work their way up -- forces must be absorbed by various tissues and structures, rather than just dissipating
44 Most activities involve some degree of weight bearing, therefore CKC exercise are more functional than open chain activities Isolation exercise typically make use of one specific muscular contraction to produce or control movement CKC exercises integrate a combination of contractions in different muscle groups w/in the chain There are a variety of popular exercises Mini-squats, leg presses, step-ups, terminal knee extension w/ tubing, push-ups and weight shifting exercises on a medicine ball
45 Core Stabilization Training Important component of all strengthening and comprehensive injury prevention program Core is defined as the lumbo-pelvic complex, area where CoG is located Will improve dynamic postural control, ensure appropriate muscular balance, allow for expression of dynamic functional strength, improve neuromuscular efficiency Body s stabilization system has to function optimally to effectively utilize the strength of prime movers
46 A weak core is a fundamental problem of inefficient movements which leads to injury Facilitates balanced muscular functioning of the entire kinetic chain - offers biomechanically efficient position for the entire kinetic chain, allowing optimal neuromuscular efficiency Program should be systematic, progressive and functional Program should be safe, challenging, stress multiple planes and incorporate a variety of resistance equipment, be derived from fundamental movement skills, and be activity specific

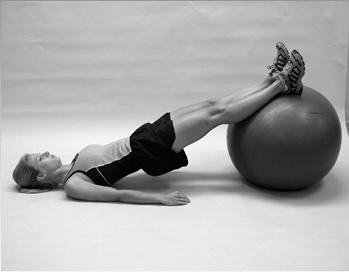
47 Core Stabilization Exercises
48 Aquatic Exercise Water submersion offers an excellent environment for beginning a program of exercise therapy or it can compliment all phases of rehab Buoyancy and hydrostatic pressure present versatile exercise environment Assistive Supportive Resistive Can engage in sports skills, restore functional capacities, perform a variety of upper and lower extremity exercises Full weight bearing activities can also be performed



49 Aquatic Exercises
50 Proprioceptive Neuromuscular Facilitation Technique Exercise that uses proprioceptive, cutaneous, and auditory input to produce functional improvement in motor output Used to increase strength, flexibility and coordination Based on the physiological properties of the stretch reflex Strengthening Techniques Rhythmic initiation Progressive series, first of passive movement then active assistive movements, followed by active movement through an agonist pattern Helps athlete w/ limited movement progressively regain strength through ROM
51 Repeated Contraction Used for general weakness at one specific point Move isotonically against maximum resistance of the ATC until fatigue is experienced At point of fatigue, stretch is applied at that point in range to facilitate greater strength production Must be accommodated resistance Slow Reversal Movement through a complete range against maximal resistance Promotes normal reciprocal coordination Reversal of movement pattern is initiated before previous pattern completed
52 Slow-reversal-hold Part is moved isotonically using agonists, immediately followed by and isometric contraction Used to develop strength at a specific point in the ROM Rhythmic stabilization Uses isometric contraction of agonists and antagonists - repeated contraction to strengthen at a particular point Stretching techniques Contract-relax Passively moved until resistance is felt; athlete contracts antagonist isotonically against resistance for 10 seconds or until fatigue; athlete relaxes for 10 seconds and then the limb is pushed to a new stretch Repeated 3 times
53 Hold-relax The athlete moves until resistance is felt; athlete contracts isometrically against resistance for 10 seconds; athlete relaxes for 10 seconds and then the limb is pushed to a new stretch actively by the athlete or passively by the clinician Repeated 3 times Slow-reversal-hold-relax Athlete moves until resistance is felt; athlete contracts isometrically against resistance for 10 seconds; athlete relaxes for 10 seconds, relaxing the antagonist while the agonist is contracted moving the limb to a new limit Repeated 3 times
54 Basic Principles for Using PNF Technique Athlete must be taught through brief, simple descriptions (starting to terminal positions) Athlete should look at limb for feedback on directional and positional control when learning Verbal commands should be firm and simple Manual contact will facilitate the motions ATC must use correct body mechanics Resistance should facilitate a maximal response that allows smooth, coordinated motion Rotational movement is critical
55 Distal movement should occur first and should be completed no later than halfway through pattern The stronger components are emphasized to facilitate weaker components of movement Pressing the joint together causes increased stability, while traction facilitates movement Giving a quick stretch causes a reflex contraction of that muscle


56 PNF Patterns Involves 3 components Flexion/extension Abduction/adduction Internal/External rotation Distinct diagonal patterns w/ rotational movements of upper & lower extremities, upper & lower trunk and neck D1 and D2 patterns for each body part Named according to movement occurring at hip or shoulder
57 Muscle Energy Technique Manually applied stretching techniques that utilize principles of neurophysiology to relax overactive muscles and/or stretch chronically shortened muscles Variation of PNF contract-relax and hold-relax techniques Based on stretch reflex Voluntary contraction of muscle in a specifically controlled direction at varied levels of intensity against a distinctly executed counterforce applied by the clinician
58 Athlete provides intrinsic corrective force and controls intensity of muscular contraction while clinician controls precision and localization of procedure 5 components necessary for MET Active muscle contraction by the athlete A muscle contraction oriented in a specific direction Some patient control of contraction intensity Athletic trainer controlled joint position Athletic trainer applied appropriate counterforce Procedure Locate resistance barrier; athlete contracts antagonist isometrically for 10 seconds, relaxes, inhales and exhales maximally while body part is moved to new resistance barrier (repeat 3-5 times or until full ROM achieved
59 Joint Mobilization and Traction Used to improve joint mobility or decrease pain by restoring accessory motion -allowing for nonrestricted pain free ROM Mobilization may be used to Reduce pain Decrease muscle guarding Stretch or lengthen tissue surrounding a joint Produce reflexogenic effects that either inhibit or facilitate muscle tone or stretch reflex For proprioceptive effects that improve postural and kinesthetic awareness
60 Mobilization Techniques Used to increase accessory motion about a joint Involve small amplitude movements (glides) w/in a specific range Should be performed w/ athlete and athletic trainer in comfortable position Joint should be stabilized as near one articulating surface as possible; other should be held firmly Treatment occurs in parallel treatment plane Maitland Grading System Grade I (for pain) - small amplitude at beginning of range Grade II (for pain) - large range at midrange Grade III (treating stiffness) - large amplitude to pathological limit Grade IV (treating stiffness) - small amplitude at end range Grade V (manipulation) - quick, short thrust
61 Mobilization based on concave-convex rule When concave surface is stationary, convex surfaces is glided in opposite direction of bone movement When convex surface is stationary, concave surface is glided in direction of movement Mobilization can also be used in conjunction w/ traction Traction Pull articulating segments apart (joint separation) Occurs in perpendicular treatment plane Used to treat pain or joint hypomobility
62 Treatment Planes




63 Joint Mobilization Techniques
64 Myofascial Release Group of techniques used to relief soft tissue from abnormal grip of tight fascia Specialized form of stretching Fascia is essentially a continuous connective tissue network that runs throughout the body, encapsulating muscles tendon, nerves, bone, and organs If damage occurs in one section it can impact fascia in sites away from the affected area
65 Form of soft tissue mobilization Locate restriction and move into the direction of the restriction More subjective and relies heavily on experience of the clinician Focuses on large areas Can have a significant impact on joint mobility Progression, working from superficial to deep restrictions As extensibility increases in tissue should be stretched
66 Strengthening should also occur to enhance neuromuscular reeducation to promote new more efficient movement patterns Acute cases resolve in a few treatments, while longer conditions take longer to resolve Sometimes treatments result in dramatic results Recommended that treatment occur 3 times/wk
67 Strain/Counterstrain Technique used to decrease muscle tension and normalize muscle function Passive technique that places body in a position of comfort - thereby relieving pain Locate tender points (tense, tender, edematous spots, <1cm in diameter, may run few centimeters long in muscle, may fall w/in a line, or have multiple points for one specific joint) Tender points monitored as athlete placed in position of comfort (shorten muscle)
68 When position is found, tender point is no longer tense After being held for 90 seconds, point should be clear Patient should then be returned to neutral position Physiological rationale based on stretch reflex Muscle relaxed instead of stretched Muscle spindle input is reduced allowing for decreasing in tension and pain
69 Positional Release Therapy PRT is based on the strain/counterstrain technique Difference is the use of a facilitating force (compression) to enhance the effect of positioning Osteopathic mobilization technique Technique follows same procedure as strain/counterstrain however, contact is maintained and pressure is exerted Maintaining contact has therapeutic effect

70 Positional Release Therapy
71 Active Release Therapy ART is relatively new type of therapy used to correct soft tissue problems caused by formation of fibrotic adhesions Result of acute injury and repetitive overuse injuries or constant pressure/tension Disrupt normal muscle function affecting biomechanics of joint complex leading to pain and dysfunction Way to diagnose and treat underlying causes of cumulative trauma disorders
72 Deep tissue technique used for breaking down scarring and adhesions Locate point and trap affected muscle by applying pressure over lesion Athlete actively moves body part to elongate muscle Repeat 3-5 times/treatment Uncomfortable treatment but will gradually soften and stretch scar tissue, increase ROM, strength, and improve circulation, optimizing healing Must follow up w/ activity modification, stretching and exercise


73 Active Release Therapy
74 Purchasing and Maintaining Therapeutic Exercise Equipment Price can range from $2 for surgical tubing to $80,000 for computer driven isokinetic and balance units Debate on effectiveness and availability of expensive equipment versus hands of clinician Must consider budget restraints when purchasing
75 Must consider usefulness and durability of equipment Will equipment facilitate athlete reaching goals of rehabilitative program Must be sure to maintain equipment once purchased, use correctly and for intended purpose Apply manufacturers guidelines for periodic inspection and maintenance to ensure safe operating conditions
Re-establishing establishing Neuromuscular
 Re-establishing establishing Neuromuscular Control Why is NMC Critical? What is NMC? Physiology of Mechanoreceptors Elements of NMC Lower-Extremity Techniques Upper-Extremity Techniques Readings Chapter
Re-establishing establishing Neuromuscular Control Why is NMC Critical? What is NMC? Physiology of Mechanoreceptors Elements of NMC Lower-Extremity Techniques Upper-Extremity Techniques Readings Chapter
Strength and conditioning? Chapter 4 Training Techniques. Weight gain (24yr, 73kg, 177cm, takes 18% protein) Guidelines.
 Guidelines.") Strength and conditioning? Chapter 4 Training Techniques Minimise the probability of injury Maximise performance Athletic Training Spring 2014 Jihong Park Guidelines Safety: environment, technique, nutrition
Strength and conditioning? Chapter 4 Training Techniques Minimise the probability of injury Maximise performance Athletic Training Spring 2014 Jihong Park Guidelines Safety: environment, technique, nutrition
Performance Enhancement. Strength Training
 Performance Enhancement Strength Training Muscle Fiber type & Performance Slow twitch More efficient using oxygen to generate fuel for continuous extended muscle contractions Contract slowly, but continue
Performance Enhancement Strength Training Muscle Fiber type & Performance Slow twitch More efficient using oxygen to generate fuel for continuous extended muscle contractions Contract slowly, but continue
Restoring Range of Motion and Improving Flexibility.
 Restoring Range of Motion and Improving Flexibility www.fisiokinesiterapia.biz Importance of Flexibility Important Goal: Restore or improve to normal pre-injury range of motion With injury there is generally
Restoring Range of Motion and Improving Flexibility www.fisiokinesiterapia.biz Importance of Flexibility Important Goal: Restore or improve to normal pre-injury range of motion With injury there is generally
Manual Therapy Techniques
 Manual Therapy Techniques manual therapy: the use of hands-on techniques to evaluate, treat, and improve the status of neuromusculoskeletal conditions massage: the systematic and scientific manipulation
Manual Therapy Techniques manual therapy: the use of hands-on techniques to evaluate, treat, and improve the status of neuromusculoskeletal conditions massage: the systematic and scientific manipulation
Vivekananda University Free Lance Language Editor. Ghoshal
 C14 M 6.1: Introduction and Classification of Therapeutic Exercise Role Name Affiliation Principal Investigator Dr. Asis Goswami Ramakrishna Mission Vivekananda University Co-Principal Investigator Dr.
C14 M 6.1: Introduction and Classification of Therapeutic Exercise Role Name Affiliation Principal Investigator Dr. Asis Goswami Ramakrishna Mission Vivekananda University Co-Principal Investigator Dr.
2006 Back to The Basics Strength and Conditioning Clinic. Warm Ups and Flexibility
 2006 Back to The Basics Strength and Conditioning Clinic Warm Ups and Flexibility Building the complete athlete Strength Training and Core Development Plyometric Training Speed and Agility Flexibility
2006 Back to The Basics Strength and Conditioning Clinic Warm Ups and Flexibility Building the complete athlete Strength Training and Core Development Plyometric Training Speed and Agility Flexibility
ACE Personal Trainer Manual, 4 th edition. Chapter 10: Resistance Training: Programming and Progressions
 ACE Personal Trainer Manual, 4 th edition Chapter 10: Resistance Training: Programming and Progressions 1 Learning Objectives This session, which is based on Chapter 10 of the ACE Personal Trainer Manual,
ACE Personal Trainer Manual, 4 th edition Chapter 10: Resistance Training: Programming and Progressions 1 Learning Objectives This session, which is based on Chapter 10 of the ACE Personal Trainer Manual,
NATURAL DEVELOPMENT AND TRAINABILITY OF PLYOMETRIC ABILITY DURING CHILDHOOD BY KIRSTY QUERL SPORT SCIENTIST STRENGTH AND CONDITIONING COACH
 NATURAL DEVELOPMENT AND TRAINABILITY OF PLYOMETRIC ABILITY DURING CHILDHOOD BY KIRSTY QUERL SPORT SCIENTIST STRENGTH AND CONDITIONING COACH The truth... Youth are not as active as they used to be, Decline
NATURAL DEVELOPMENT AND TRAINABILITY OF PLYOMETRIC ABILITY DURING CHILDHOOD BY KIRSTY QUERL SPORT SCIENTIST STRENGTH AND CONDITIONING COACH The truth... Youth are not as active as they used to be, Decline
Hands on Sports Therapy KNOWLEDGE REVIEW QUESTIONS 2004 Thomson Learning. Q1:From the following list of acronyms, write down the full title of each
 CHAPTER 09 Knowledge Review Q1:From the following list of acronyms, write down the full title of each treatment technique: NMT; PRT; SCS; FT; MET; PNF; PIR; RI; CRAC; INIT; ICT; ICCT. A1: NMT: Neuromuscular
CHAPTER 09 Knowledge Review Q1:From the following list of acronyms, write down the full title of each treatment technique: NMT; PRT; SCS; FT; MET; PNF; PIR; RI; CRAC; INIT; ICT; ICCT. A1: NMT: Neuromuscular
PROGRESSION OF EXERCISE
 PROGRESSION OF EXERCISE PLANNING YOUR TREATMENT Evaluation guides your treatment How? IRRITABILITY Pain level Linger Sleep How quickly does the pain come on? Consistency or behavior STAGE Acute Chemical
PROGRESSION OF EXERCISE PLANNING YOUR TREATMENT Evaluation guides your treatment How? IRRITABILITY Pain level Linger Sleep How quickly does the pain come on? Consistency or behavior STAGE Acute Chemical
DEVELOPING PHYSICAL CAPACITIES IV - STRENGTH MUSCLE TYPES
 DEVELOPING PHYSICAL CAPACITIES IV - STRENGTH The muscular system is made up of around 650 muscles and account for around half of the weight of our body. The muscular system of the body is what allows humans
DEVELOPING PHYSICAL CAPACITIES IV - STRENGTH The muscular system is made up of around 650 muscles and account for around half of the weight of our body. The muscular system of the body is what allows humans
REHABILITATION FOLLOWING ACL RECONSTRUCTION PROTOCOL. WEEK 1: Knee immobilizer locked in extension. WBAT with bilateral crutches.
 REHABILITATION FOLLOWING ACL RECONSTRUCTION PROTOCOL IMMEDIATE POST OPERATIVE PHASE Week 1: WEEK 1: Knee immobilizer locked in extension. WBAT with bilateral crutches. Ankle Pumps Passive knee extension
REHABILITATION FOLLOWING ACL RECONSTRUCTION PROTOCOL IMMEDIATE POST OPERATIVE PHASE Week 1: WEEK 1: Knee immobilizer locked in extension. WBAT with bilateral crutches. Ankle Pumps Passive knee extension
Diagnosis: ( LEFT / RIGHT ) Shoulder Instability / SLAP Tear
 Shoulder Instability / SLAP Tear") UCLA OUTPATIENT REHABILITATION SERVICES! SANTA MONICA! WESTWOOD 1000 Veteran Ave., A level Phone: (310) 794-1323 Fax: (310) 794-1457 1260 15 th St, Ste. 900 Phone: (310) 319-4646 Fax: (310) 319-2269 FOR
UCLA OUTPATIENT REHABILITATION SERVICES! SANTA MONICA! WESTWOOD 1000 Veteran Ave., A level Phone: (310) 794-1323 Fax: (310) 794-1457 1260 15 th St, Ste. 900 Phone: (310) 319-4646 Fax: (310) 319-2269 FOR
Chapter 4. Muscular Strength and Endurance KIN 217 3/28/18 1
 Chapter 4 Muscular Strength and Endurance KIN 217 1 Functions of Muscle Tissues Functions: provide stability and postural tone, allow purposeful movement, heat production. Muscle mass constitutes: 40 to
Chapter 4 Muscular Strength and Endurance KIN 217 1 Functions of Muscle Tissues Functions: provide stability and postural tone, allow purposeful movement, heat production. Muscle mass constitutes: 40 to
Anterior Cruciate Ligament Hamstring Rehabilitation Protocol
 Anterior Cruciate Ligament Hamstring Rehabilitation Protocol Focus on exercise quality avoid overstressing the donor area while it heals. Typically, isolated hamstring strengthening begins after the 6
Anterior Cruciate Ligament Hamstring Rehabilitation Protocol Focus on exercise quality avoid overstressing the donor area while it heals. Typically, isolated hamstring strengthening begins after the 6
Exploring the Rotator Cuff
 Exploring the Rotator Cuff Improving one s performance in sports and daily activity is a factor of neuromuscular efficiency and metabolic enhancements. To attain proficiency, reaction force must be effectively
Exploring the Rotator Cuff Improving one s performance in sports and daily activity is a factor of neuromuscular efficiency and metabolic enhancements. To attain proficiency, reaction force must be effectively
CSEP-Certified Certified Personal Trainer (CSEP-CPT) CPT) Musculoskeletal Fitness Theory
 CPT) Musculoskeletal Fitness Theory") CSEP-Certified Certified Personal Trainer (CSEP-CPT) CPT) Musculoskeletal Fitness Theory 1 Basic Anatomy Key Concepts: 3.23-3.25 3.25 2 Force & Levers 1 st class» seesaw» muscles that extend neck R F AF
CSEP-Certified Certified Personal Trainer (CSEP-CPT) CPT) Musculoskeletal Fitness Theory 1 Basic Anatomy Key Concepts: 3.23-3.25 3.25 2 Force & Levers 1 st class» seesaw» muscles that extend neck R F AF
Sports Rehabilitation & Performance Center Medial Patellofemoral Ligament Reconstruction Guidelines * Follow physician s modifications as prescribed
 The following MPFL guidelines were developed by the Sports Rehabilitation and Performance Center team at Hospital for Special Surgery. Progression is based on healing constraints, functional progression
The following MPFL guidelines were developed by the Sports Rehabilitation and Performance Center team at Hospital for Special Surgery. Progression is based on healing constraints, functional progression
Dr. Huff Modified Brostrom Repair Rehabilitation Protocol:
 Dr. Huff Modified Brostrom Repair Rehabilitation Protocol: The intent of this protocol is to provide the clinician with a guideline of the post-operative rehabilitation course of a patient who has undergone
Dr. Huff Modified Brostrom Repair Rehabilitation Protocol: The intent of this protocol is to provide the clinician with a guideline of the post-operative rehabilitation course of a patient who has undergone
Chapter 8: Muscular Strength & Endurance. ACE Personal Trainer Manual Third Edition
 Chapter 8: Muscular Strength & Endurance ACE Personal Trainer Manual Third Edition Introduction Muscles are unique in their ability to relax, contract, and produce force. In addition, this metabolically
Chapter 8: Muscular Strength & Endurance ACE Personal Trainer Manual Third Edition Introduction Muscles are unique in their ability to relax, contract, and produce force. In addition, this metabolically
1-Apley scratch test.
 1-Apley scratch test. The patient attempts to touch the opposite scapula to test range of motion of the shoulder. 1-Testing abduction and external rotation( +ve sign touch the opposite scapula, -ve sign
1-Apley scratch test. The patient attempts to touch the opposite scapula to test range of motion of the shoulder. 1-Testing abduction and external rotation( +ve sign touch the opposite scapula, -ve sign
Anterior Cruciate Ligament (ACL) Reconstruction Protocol. Hamstring Autograft, Allograft, or Revision
 Reconstruction Protocol. Hamstring Autograft, Allograft, or Revision") Anterior Cruciate Ligament (ACL) Reconstruction Protocol Hamstring Autograft, Allograft, or Revision As tolerated should be understood to perform with safety for the reconstruction/repair. Pain, limp,
Anterior Cruciate Ligament (ACL) Reconstruction Protocol Hamstring Autograft, Allograft, or Revision As tolerated should be understood to perform with safety for the reconstruction/repair. Pain, limp,
Chapter 5. Joint Classifications. Synarthroses. Amphiarthroses Slightly movable joints such as: Synchondroses 1 st sternocostal
 Chapter 5 Joint Classifications Synarthroses immovable Amphiarthroses slightly movable Diarthroses (synovial) freely movable Biomechanics of Human Skeletal Articulations Synarthroses Immovable joints such
Chapter 5 Joint Classifications Synarthroses immovable Amphiarthroses slightly movable Diarthroses (synovial) freely movable Biomechanics of Human Skeletal Articulations Synarthroses Immovable joints such
THERMAL - ASSISTED CAPSULORRAPHY With or without SLAP Repair
 THERMAL - ASSISTED CAPSULORRAPHY With or without SLAP Repair **It is important for the clinician to determine the capsular response to the heat probe. Patients that have excessive ROM early in the rehab
THERMAL - ASSISTED CAPSULORRAPHY With or without SLAP Repair **It is important for the clinician to determine the capsular response to the heat probe. Patients that have excessive ROM early in the rehab
OSTEOCHONDRAL AUTOGRAFT TRANSPLANTATION
 OSTEOCHONDRAL AUTOGRAFT TRANSPLANTATION FEMORAL CONDYLE REHABILITATION PROGRAM PHASE I - PROTECTION PHASE (WEEKS 0-6) Protection of healing tissue from load and shear forces Decrease pain and effusion
OSTEOCHONDRAL AUTOGRAFT TRANSPLANTATION FEMORAL CONDYLE REHABILITATION PROGRAM PHASE I - PROTECTION PHASE (WEEKS 0-6) Protection of healing tissue from load and shear forces Decrease pain and effusion
9180 KATY FREEWAY, STE. 200 (713)
") OSTEOCHONDRAL AUTOGRAFT TRANSPLANTATION Patella/Trochlea Rehabilitation Guidelines PHASE I - PROTECTION PHASE (WEEKS 0-6) Goals: - Protection of healing tissue from load and shear forces - Decrease pain
OSTEOCHONDRAL AUTOGRAFT TRANSPLANTATION Patella/Trochlea Rehabilitation Guidelines PHASE I - PROTECTION PHASE (WEEKS 0-6) Goals: - Protection of healing tissue from load and shear forces - Decrease pain
Chapter 10: Flexibility. ACE Personal Trainer Manual Third Edition
 Chapter 10: Flexibility ACE Personal Trainer Manual Third Edition Flexibility: A Definition Flexibility is the range of motion (ROM) within a joint along the various planes of motion. A number of factors
Chapter 10: Flexibility ACE Personal Trainer Manual Third Edition Flexibility: A Definition Flexibility is the range of motion (ROM) within a joint along the various planes of motion. A number of factors
Fitness Intro. Freshmen PE
 Fitness Intro Freshmen PE Physical Fitness Are you able to get through your day easily without tiring? Does your body respond quickly when it needs to? Are you mentally alert in class? Do you feel good
Fitness Intro Freshmen PE Physical Fitness Are you able to get through your day easily without tiring? Does your body respond quickly when it needs to? Are you mentally alert in class? Do you feel good
Phase I : Immediate Postoperative Phase- Protected Motion. (0-2 Weeks)
") Phase I : Immediate Postoperative Phase- Protected Motion (0-2 Weeks) Appointments Progression Criteria 2 weeks after surgery Rehabilitation appointments begin within 7-10 days of surgery, continue 1-2
Phase I : Immediate Postoperative Phase- Protected Motion (0-2 Weeks) Appointments Progression Criteria 2 weeks after surgery Rehabilitation appointments begin within 7-10 days of surgery, continue 1-2
CHAPTER 15: KINESIOLOGY OF FITNESS AND EXERCISE
 CHAPTER 15: KINESIOLOGY OF FITNESS AND EXERCISE KINESIOLOGY Scientific Basis of Human Motion, 12th edition Hamilton, Weimar & Luttgens Presentation Created by TK Koesterer, Ph.D., ATC Humboldt State University
CHAPTER 15: KINESIOLOGY OF FITNESS AND EXERCISE KINESIOLOGY Scientific Basis of Human Motion, 12th edition Hamilton, Weimar & Luttgens Presentation Created by TK Koesterer, Ph.D., ATC Humboldt State University
Training Methods. Remember : FRCIFCP. Fartlek. Resistance Circuit Interval Flexibility Continuous Plyometrics Pilates / Fitball
 Remember : FRCIFCP Fartlek Resistance Circuit Interval Flexibility Continuous Plyometrics Pilates / Fitball Fartlek: A variation of continuous training with bursts of speed so the anaerobic system is also
Remember : FRCIFCP Fartlek Resistance Circuit Interval Flexibility Continuous Plyometrics Pilates / Fitball Fartlek: A variation of continuous training with bursts of speed so the anaerobic system is also
Medial Patellofemoral Ligament Reconstruction Guidelines Brian Grawe Protocol
 Medial Patellofemoral Ligament Reconstruction Guidelines Brian Grawe Protocol Progression is based on healing constraints, functional progression specific to the patient. Phases and time frames are designed
Medial Patellofemoral Ligament Reconstruction Guidelines Brian Grawe Protocol Progression is based on healing constraints, functional progression specific to the patient. Phases and time frames are designed
Rehabilitation Following Unilateral Patellar Tendon Repair
 Rehabilitation Following Unilateral Patellar Tendon Repair I. Immediate Postoperative Phase (Days 1-7) Restore full passive knee extension Diminish pain and joint swelling Restore patellar mobility Initiate
Rehabilitation Following Unilateral Patellar Tendon Repair I. Immediate Postoperative Phase (Days 1-7) Restore full passive knee extension Diminish pain and joint swelling Restore patellar mobility Initiate
Small Rotator Cuff Repair
 Small Rotator Cuff Repair 1. Defined a. Surgical repair of the rotator cuff (most commonly supraspinatus muscle) utilizing sutures b. May be done arthroscopically or open. c. May be done in conjunction
Small Rotator Cuff Repair 1. Defined a. Surgical repair of the rotator cuff (most commonly supraspinatus muscle) utilizing sutures b. May be done arthroscopically or open. c. May be done in conjunction
Large/Massive Rotator Cuff Repair
 Large/Massive Rotator Cuff Repair 1. Defined a. Suturing of tears within the rotator cuff (most commonly supraspinatus muscle). Massive RCR usually involve more than the supraspinatus. b. May be done arthroscopically
Large/Massive Rotator Cuff Repair 1. Defined a. Suturing of tears within the rotator cuff (most commonly supraspinatus muscle). Massive RCR usually involve more than the supraspinatus. b. May be done arthroscopically
REHABILITATION PROTOCOL FOLLOWING PCL RECONSTRUCTION USING A TWO TUNNEL GRAFT. Brace E-Z Wrap locked at zero degree extension, sleep in Brace
 Therapist Phone REHABILITATION PROTOCOL FOLLOWING PCL RECONSTRUCTION USING A TWO TUNNEL GRAFT I. IMMEDIATE POST-OPERATIVE PHASE (Week 1) Control Swelling and Inflammation Obtain Full Passive Knee Extension
Therapist Phone REHABILITATION PROTOCOL FOLLOWING PCL RECONSTRUCTION USING A TWO TUNNEL GRAFT I. IMMEDIATE POST-OPERATIVE PHASE (Week 1) Control Swelling and Inflammation Obtain Full Passive Knee Extension
MSc in Athletic Therapy
 NATIONAL UNIVERSITY OF MEDICAL SCIENCES MSc in Athletic Therapy Research Paper: Sports Strength and Conditioning in conjunction with Therapy Arun Kumar 6/22/2015 Student Number: S140212 Topic: Sports Strength
NATIONAL UNIVERSITY OF MEDICAL SCIENCES MSc in Athletic Therapy Research Paper: Sports Strength and Conditioning in conjunction with Therapy Arun Kumar 6/22/2015 Student Number: S140212 Topic: Sports Strength
Accelerated Rehabilitation Following ACL-PTG Reconstruction & PCL Reconstruction with Medial Collateral Ligament Repair
 Page 1 of 7 Accelerated Rehabilitation Following ACL-PTG Reconstruction & PCL Reconstruction with Medial Collateral Ligament Repair PREOPERATIVE PHASE Goals: Diminish inflammation, swelling, and pain Restore
Page 1 of 7 Accelerated Rehabilitation Following ACL-PTG Reconstruction & PCL Reconstruction with Medial Collateral Ligament Repair PREOPERATIVE PHASE Goals: Diminish inflammation, swelling, and pain Restore
CENTER FOR ORTHOPAEDICS AND SPINE CARE PHYSICAL THERAPY PROTOCOL ARTHROSCOPIC SLAP LESION REPAIR (TYPE II) BENJAMIN J. DAVIS, MD
 BENJAMIN J. DAVIS, MD") I. Phase I Immediate Postoperative Phase Restrictive Motion (Day 1 to Week 6) Goals: Protect the anatomic repair Prevent negative effects of immobilization Promote dynamic stability Diminish pain and inflammation
I. Phase I Immediate Postoperative Phase Restrictive Motion (Day 1 to Week 6) Goals: Protect the anatomic repair Prevent negative effects of immobilization Promote dynamic stability Diminish pain and inflammation
Athletic Preparation ACL Reconstruction - Accelerated Rehabilitation. Autologous Bone-Tendon-Bone, Patella Tendon Graft
 Orthopaedic Sports Specialists, P.C. Michael E. Joyce, M.D. 84 Glastonbury Blvd., Suite 101, Glastonbury, Connecticut 06033 Voice: 860-652-8883, Fax: 860-652-8887 Athletic Preparation ACL Reconstruction
Orthopaedic Sports Specialists, P.C. Michael E. Joyce, M.D. 84 Glastonbury Blvd., Suite 101, Glastonbury, Connecticut 06033 Voice: 860-652-8883, Fax: 860-652-8887 Athletic Preparation ACL Reconstruction
Hip Arthroscopy Rehabilitation Protocol
 Hip Arthroscopy Rehabilitation Protocol 1. Concepts: a. Range of motion and weight bearing restrictions must be adhered to during the initial rehab process (4 total weeks of ROM and weight bearing restrictions)
Hip Arthroscopy Rehabilitation Protocol 1. Concepts: a. Range of motion and weight bearing restrictions must be adhered to during the initial rehab process (4 total weeks of ROM and weight bearing restrictions)
chapter Exercise Technique for Alternative Modes and Nontraditional Implement Training
 chapter 16 Exercise Technique for Alternative Modes and Nontraditional Implement Training Chapter Objectives Understand the basic guidelines for performing resistance exercise with alternative modes and
chapter 16 Exercise Technique for Alternative Modes and Nontraditional Implement Training Chapter Objectives Understand the basic guidelines for performing resistance exercise with alternative modes and
Rehabilitation Guidelines for Anterior Cruciate Ligament (ACL) Reconstruction
 Reconstruction") Rehabilitation Guidelines for Anterior Cruciate Ligament (ACL) Reconstruction The knee is the body's largest joint, and the place where the femur, tibia, and patella meet to form a hinge-like joint. These
Rehabilitation Guidelines for Anterior Cruciate Ligament (ACL) Reconstruction The knee is the body's largest joint, and the place where the femur, tibia, and patella meet to form a hinge-like joint. These
ULNAR COLLATERAL LIGAMENT (UCL) RECONSTRUCTION REHABILITATION PROTOCOL
 RECONSTRUCTION REHABILITATION PROTOCOL") General Notes As tolerated should be understood to include with safety for the surgical procedure; a sudden increase in pain, swelling, or other undesirable factors are indicators that you are doing too
General Notes As tolerated should be understood to include with safety for the surgical procedure; a sudden increase in pain, swelling, or other undesirable factors are indicators that you are doing too
VO2MAX TEST.
 AEROBIC CAPACITY Aerobic capacity refers to the maximum amount of oxygen that the body can utilize in an exercise session It is possible to improve aerobic capacity over time, and it is also possible to
AEROBIC CAPACITY Aerobic capacity refers to the maximum amount of oxygen that the body can utilize in an exercise session It is possible to improve aerobic capacity over time, and it is also possible to
Hip Arthroscopy Femoroacetabular Impingement (FAI) Ryan W. Hess, MD Tracey Pederson, PCC Office: (763) Fax: (763)
 Ryan W. Hess, MD Tracey Pederson, PCC Office: (763) Fax: (763)") Hip Arthroscopy Femoroacetabular Impingement (FAI) Ryan W. Hess, MD Tracey Pederson, PCC Office: (763) 302-2223 Fax: (763) 302-2401 GENERAL GUIDELINES: Despite the minimally invasive nature of hip arthroscopy,
Hip Arthroscopy Femoroacetabular Impingement (FAI) Ryan W. Hess, MD Tracey Pederson, PCC Office: (763) 302-2223 Fax: (763) 302-2401 GENERAL GUIDELINES: Despite the minimally invasive nature of hip arthroscopy,
Arthroscopic Anterior Stabilization Rehab
 Arthroscopic Anterior Stabilization Rehab Phase I (0-3weeks) Sling immobilization-md directed Codmans/Pendulum exercises Wrist/Elbow ROM Gripping exercises FF-AAROM (supine)-limit to 90 o ER to 0 o Sub
Arthroscopic Anterior Stabilization Rehab Phase I (0-3weeks) Sling immobilization-md directed Codmans/Pendulum exercises Wrist/Elbow ROM Gripping exercises FF-AAROM (supine)-limit to 90 o ER to 0 o Sub
Introduction. Anatomy
 the patella is called the quadriceps mechanism. Though we think of it as a single device, the quadriceps mechanism has two separate tendons, the quadriceps tendon on top of the patella and the patellar
the patella is called the quadriceps mechanism. Though we think of it as a single device, the quadriceps mechanism has two separate tendons, the quadriceps tendon on top of the patella and the patellar
The Purpose of Training
 The Purpose of Training Training improves the physiological capacity of athletes to bring out the best performance possible. The demands of the sport can be identified by undertaking an activity analysis.
The Purpose of Training Training improves the physiological capacity of athletes to bring out the best performance possible. The demands of the sport can be identified by undertaking an activity analysis.
ANTERIOR KNEE PAIN. Explanation. Causes. Symptoms
 ANTERIOR KNEE PAIN Explanation Anterior knee pain is most commonly caused by irritation and inflammation of the patellofemoral joint of the knee (where the patella/kneecap connects to the femur/thigh bone).
ANTERIOR KNEE PAIN Explanation Anterior knee pain is most commonly caused by irritation and inflammation of the patellofemoral joint of the knee (where the patella/kneecap connects to the femur/thigh bone).
Physical fitness : ability of the body to respond to physical. Skill-related fitness : ability to perform specific leisure or sport
 Chapter 6: Fitness What Is Fitness? Physical fitness : ability of the body to respond to physical demands Skill-related fitness : ability to perform specific leisure or sport skills Health-related fitness:
Chapter 6: Fitness What Is Fitness? Physical fitness : ability of the body to respond to physical demands Skill-related fitness : ability to perform specific leisure or sport skills Health-related fitness:
Post-op / Pre-op Page (ALREADY DONE)
") Post-op / Pre-op Page (ALREADY DONE) We offer individualized treatment plans based on your physician's recommendations, our evaluations, and your feedback. Most post-operative and preoperative rehabilitation
Post-op / Pre-op Page (ALREADY DONE) We offer individualized treatment plans based on your physician's recommendations, our evaluations, and your feedback. Most post-operative and preoperative rehabilitation
Chinese Proverb. He who asks a question is a fool for five minutes; he who does not ask a question remains a fool forever. What do we Fix?
 Robert H. Rowe, PT, DPT, DMT, MHS, FAAOMPT Director Brooks Institute of Higher Learning Chinese Proverb He who asks a question is a fool for five minutes; he who does not ask a question remains a fool
Robert H. Rowe, PT, DPT, DMT, MHS, FAAOMPT Director Brooks Institute of Higher Learning Chinese Proverb He who asks a question is a fool for five minutes; he who does not ask a question remains a fool
Rehabilitation Guidelines for Labral/Bankert Repair
 Rehabilitation Guidelines for Labral/Bankert Repair The true shoulder joint is called the glenohumeral joint and consists humeral head and the glenoid. It is a ball and socket joint. Anatomy of the Shoulder
Rehabilitation Guidelines for Labral/Bankert Repair The true shoulder joint is called the glenohumeral joint and consists humeral head and the glenoid. It is a ball and socket joint. Anatomy of the Shoulder
CENTER FOR ORTHOPAEDICS AND SPINE CARE PHYSICAL THERAPY PROTOCOL ORIF PATELLA BENJAMIN J. DAVIS, MD
 I. Immediate Postoperative Phase (Days 1-7) Restore full passive knee extension Diminish pain and joint swelling Restore patellar mobility Initiate early controlled motion *Controlled forces on repair
I. Immediate Postoperative Phase (Days 1-7) Restore full passive knee extension Diminish pain and joint swelling Restore patellar mobility Initiate early controlled motion *Controlled forces on repair
REHABILITATION FOLLOWING ACL PTG RECONSTRUCTION
 REHABILITATION FOLLOWING ACL PTG RECONSTRUCTION I. IMMEDIATE POST OPERATIVE PHASE POD 1 POD 2 to 3 Brace: EZ Wrap brace locked at zero degrees extension or Protonics Rehab System (PRS) as directed by physician
REHABILITATION FOLLOWING ACL PTG RECONSTRUCTION I. IMMEDIATE POST OPERATIVE PHASE POD 1 POD 2 to 3 Brace: EZ Wrap brace locked at zero degrees extension or Protonics Rehab System (PRS) as directed by physician
Rehabilitation Guidelines for Meniscal Repair
 Rehabilitation Guidelines for Meniscal Repair The knee is the body's largest joint, and the place where the femur, tibia, and patella meet to form a hinge-like joint. These bones are supported by a large
Rehabilitation Guidelines for Meniscal Repair The knee is the body's largest joint, and the place where the femur, tibia, and patella meet to form a hinge-like joint. These bones are supported by a large
Manual Therapy Techniques: Joint Mobilization and PNF Diagonal Patterns. Linda Gazzillo Diaz, Ed.D., ATC William Paterson University
 Manual Therapy Techniques: Joint Mobilization and PNF Diagonal Patterns Linda Gazzillo Diaz, Ed.D., ATC William Paterson University Assist in restoring joint motion by decreasing pain and stiffness Arthrokinematics
Manual Therapy Techniques: Joint Mobilization and PNF Diagonal Patterns Linda Gazzillo Diaz, Ed.D., ATC William Paterson University Assist in restoring joint motion by decreasing pain and stiffness Arthrokinematics
Meniscus Repair Rehabilitation Protocol
 Brian E. Camilleri, DO 2610 Enterprise Dr Anderson, IN 46013 Phone: (765) 683-4400 Fax: (765) 642-7903 www.ciocenter.com Meniscus Repair Rehabilitation Protocol The intent of this protocol is to provide
Brian E. Camilleri, DO 2610 Enterprise Dr Anderson, IN 46013 Phone: (765) 683-4400 Fax: (765) 642-7903 www.ciocenter.com Meniscus Repair Rehabilitation Protocol The intent of this protocol is to provide
Chapter 14 Training Muscles to Become Stronger
 Chapter 14 Training Muscles to Become Stronger Slide Show developed by: Richard C. Krejci, Ph.D. Professor of Public Health Columbia College 11.22.11 Objectives 1. Describe the following four methods to
Chapter 14 Training Muscles to Become Stronger Slide Show developed by: Richard C. Krejci, Ph.D. Professor of Public Health Columbia College 11.22.11 Objectives 1. Describe the following four methods to
POST-OPERATIVE REHABILITATION PROTOCOL FOLLOWING ULNAR COLLATERAL LIGAMENT RECONSTRUCTION USING AUTOGENOUS GRACILIS GRAFT
 Therapist POST-OPERATIVE REHABILITATION PROTOCOL FOLLOWING ULNAR COLLATERAL LIGAMENT RECONSTRUCTION USING AUTOGENOUS GRACILIS GRAFT I. IMMEDIATE POST-OPERATIVE PHASE (0-3 weeks) Protect healing tissue
Therapist POST-OPERATIVE REHABILITATION PROTOCOL FOLLOWING ULNAR COLLATERAL LIGAMENT RECONSTRUCTION USING AUTOGENOUS GRACILIS GRAFT I. IMMEDIATE POST-OPERATIVE PHASE (0-3 weeks) Protect healing tissue
Molecular-level benefits of stabilizing blood glucose levels. Copyright 2015 McGraw-Hill Education. All rights reserved.
 Fitness Chapter 6 No reproduction or distribution without the prior written consent of McGraw-Hill Education. 1 What Is Fitness? Physical fitness: ability of the body to respond to physical demands Skill-related
Fitness Chapter 6 No reproduction or distribution without the prior written consent of McGraw-Hill Education. 1 What Is Fitness? Physical fitness: ability of the body to respond to physical demands Skill-related
ARTHROSCOPIC SLAP LESION REPAIR (TYPE II) WITH THERMAL CAPSULAR SHRINKAGE
 WITH THERMAL CAPSULAR SHRINKAGE") ARTHROSCOPIC SLAP LESION REPAIR (TYPE II) WITH THERMAL CAPSULAR SHRINKAGE I. Phase I Immediate Postoperative Phase Restrictive Motion (Day 1 to Week 6) Goals: Protect the anatomic repair Prevent negative
ARTHROSCOPIC SLAP LESION REPAIR (TYPE II) WITH THERMAL CAPSULAR SHRINKAGE I. Phase I Immediate Postoperative Phase Restrictive Motion (Day 1 to Week 6) Goals: Protect the anatomic repair Prevent negative
REHABILITATION PROTOCOL FOLLOWING PCL RECONSTRUCTION USING Allograft
 Sports Medicine and Rehabilitation Center Therapist Phone REHABILITATION PROTOCOL FOLLOWING PCL RECONSTRUCTION USING Allograft I. IMMEDIATE POST-OPERATIVE PHASE (Week 1) Control Swelling and Inflammation
Sports Medicine and Rehabilitation Center Therapist Phone REHABILITATION PROTOCOL FOLLOWING PCL RECONSTRUCTION USING Allograft I. IMMEDIATE POST-OPERATIVE PHASE (Week 1) Control Swelling and Inflammation
Chapter 20: Muscular Fitness and Assessment
 Chapter 20: Muscular Fitness and Assessment American College of Sports Medicine. (2010). ACSM's resource manual for guidelines for exercise testing and prescription (6th ed.). New York: Lippincott, Williams
Chapter 20: Muscular Fitness and Assessment American College of Sports Medicine. (2010). ACSM's resource manual for guidelines for exercise testing and prescription (6th ed.). New York: Lippincott, Williams
Femoral Condyle Rehabilitation Guidelines
 Femoral Condyle Rehabilitation Guidelines PHASE I - PROTECTION PHASE (WEEKS 0-6) Brace: Protect healing tissue from load and shear forces Decrease pain and effusion Restore full passive knee extension
Femoral Condyle Rehabilitation Guidelines PHASE I - PROTECTION PHASE (WEEKS 0-6) Brace: Protect healing tissue from load and shear forces Decrease pain and effusion Restore full passive knee extension
SUMMARY OF MEDICAL TREATMENT GUIDELINE FOR CARPAL TUNNEL SYNDROME AS IT RELATES TO PHYSICAL THERAPY
 SUMMARY OF MEDICAL TREATMENT GUIDELINE FOR CARPAL TUNNEL SYNDROME AS IT RELATES TO PHYSICAL THERAPY Effective March 1, 2013, the New York State Workers Compensation System will implement Medical Treatment
SUMMARY OF MEDICAL TREATMENT GUIDELINE FOR CARPAL TUNNEL SYNDROME AS IT RELATES TO PHYSICAL THERAPY Effective March 1, 2013, the New York State Workers Compensation System will implement Medical Treatment
Accelerated Rehabilitation Following ACL-PTG Reconstruction with Medial Collateral Ligament Repair
 Page 1 of 7 Accelerated Rehabilitation Following ACL-PTG Reconstruction with Medial Collateral Ligament Repair PREOPERATIVE PHASE Goals: Diminish inflammation, swelling, and pain Restore normal range of
Page 1 of 7 Accelerated Rehabilitation Following ACL-PTG Reconstruction with Medial Collateral Ligament Repair PREOPERATIVE PHASE Goals: Diminish inflammation, swelling, and pain Restore normal range of
Anterior Cruciate Ligament (ACL)
") Anterior Cruciate Ligament (ACL) The anterior cruciate ligament (ACL) is one of the 4 major ligament stabilizers of the knee. ACL tears are among the most common major knee injuries in active people of
Anterior Cruciate Ligament (ACL) The anterior cruciate ligament (ACL) is one of the 4 major ligament stabilizers of the knee. ACL tears are among the most common major knee injuries in active people of
AquaStretch: Intuition &Accenting
 International Aquatic Therapy Symposium June 28, 2012 Jessica Huss PT, DPT, CCI Aquatic Rehab &Wellness Center AT Still University Manual Techniques Stretching Dynamic vs. Static Manual Techniques Myofascial
International Aquatic Therapy Symposium June 28, 2012 Jessica Huss PT, DPT, CCI Aquatic Rehab &Wellness Center AT Still University Manual Techniques Stretching Dynamic vs. Static Manual Techniques Myofascial
Sheena Black, MD. Orthopaedic Surgery, Sports Medicine PHYSICAL THERAPY PRESCRIPTION ACL RECONSTRUCTION HAMSTRING TENDON TECHNIQUE
 PHYSICAL THERAPY PRESCRIPTION ACL RECONSTRUCTION HAMSTRING TENDON TECHNIQUE Name: Date: Post-Operative Diagnosis: Right Left ACL Reconstruction Graft: BTB Hamstring Allograft Additional Procedures: Lateral
PHYSICAL THERAPY PRESCRIPTION ACL RECONSTRUCTION HAMSTRING TENDON TECHNIQUE Name: Date: Post-Operative Diagnosis: Right Left ACL Reconstruction Graft: BTB Hamstring Allograft Additional Procedures: Lateral
l. Initiate early proprioceptive activity and progress by means of distraction techniques: i. eyes open to eyes closed ii. stable to unstable m.
 Meniscus Repair 1. Defined a. Sutures or bioabsorbable fixation devices (arrows, darts, screws, etc.) bring together and fixate the edges of a tear in the meniscus in order to maintain the shock absorption
Meniscus Repair 1. Defined a. Sutures or bioabsorbable fixation devices (arrows, darts, screws, etc.) bring together and fixate the edges of a tear in the meniscus in order to maintain the shock absorption
Proximal Hamstring Rupture: Physical Therapy Protocol
 Proximal Hamstring Rupture: Physical Therapy Protocol The intent of this protocol is to provide guidelines for your patient s therapy progression. It is not intended to serve as a recipe for treatment.
Proximal Hamstring Rupture: Physical Therapy Protocol The intent of this protocol is to provide guidelines for your patient s therapy progression. It is not intended to serve as a recipe for treatment.
Labral Repair with a Microfracture
 Labral Repair with a Microfracture This protocol should be used as a guideline for progression and should be tailored to the needs of the individual patient. Strict protective weight bearing status for
Labral Repair with a Microfracture This protocol should be used as a guideline for progression and should be tailored to the needs of the individual patient. Strict protective weight bearing status for
chapter Plyometric Training
 chapter 18 Plyometric Training Chapter Objectives Explain the physiology of plyometric exercise. Identify the phases of the stretch-shortening cycle. Identify components of a plyometric training program.
chapter 18 Plyometric Training Chapter Objectives Explain the physiology of plyometric exercise. Identify the phases of the stretch-shortening cycle. Identify components of a plyometric training program.
Benefits of Weight bearing increased awareness of the involved side decreased fear improved symmetry regulation of muscle tone
 From the information we have gathered during our Evaluation, the Clinical Reasoning we used to identify key problem areas and the Goals Established with functional outcomes we now have enough information
From the information we have gathered during our Evaluation, the Clinical Reasoning we used to identify key problem areas and the Goals Established with functional outcomes we now have enough information
THERAPEUTIC EXERCISE BASICS..
 THERAPEUTIC EXERCISE BASICS.. 97750, 97110, 97530, 97535, 97112, 97140, 97150, 97802, 97803, A9150 GUIDELINES FOR THERAPEUTIC EXERCISE Supervised exercise is an essential component of Chiropractic Rehabilitation
THERAPEUTIC EXERCISE BASICS.. 97750, 97110, 97530, 97535, 97112, 97140, 97150, 97802, 97803, A9150 GUIDELINES FOR THERAPEUTIC EXERCISE Supervised exercise is an essential component of Chiropractic Rehabilitation
SHOULDER ARTHROSCOPY WITH ANTERIOR STABILIZATION / CAPSULORRHAPHY REHABILITATION PROTOCOL
 General Notes As tolerated should be understood to include with safety for the surgical procedure; a sudden increase in pain, swelling, or other undesirable factors are indicators that you are doing too
General Notes As tolerated should be understood to include with safety for the surgical procedure; a sudden increase in pain, swelling, or other undesirable factors are indicators that you are doing too
Rehabilitation and Reconditioning
 Rehabilitation and Reconditioning Rehabilitation and Reconditioning Principles Healing tissues must not be overstressed. The athlete must fulfill specific criteria to progress from one phase to another
Rehabilitation and Reconditioning Rehabilitation and Reconditioning Principles Healing tissues must not be overstressed. The athlete must fulfill specific criteria to progress from one phase to another
Superior Labrum Repair Protocol - SLAP
 Superior Labrum Repair Protocol - SLAP Stage I (0-4 weeks): Key Goals: Protect the newly repaired shoulder. Allow for decreased inflammation and healing. Maintain elbow, wrist and hand function. Maintain
Superior Labrum Repair Protocol - SLAP Stage I (0-4 weeks): Key Goals: Protect the newly repaired shoulder. Allow for decreased inflammation and healing. Maintain elbow, wrist and hand function. Maintain
ACL REHABILITATION PROTOCOL
 Name: ID: Date Of Surgery :DD / MM / YYYY Procedure: ACL REHABILITATION PROTOCOL Note :If another procedure like meniscus repair or OATS (Osteochondralautograft transfer) has been done along with ACL reconstruction
Name: ID: Date Of Surgery :DD / MM / YYYY Procedure: ACL REHABILITATION PROTOCOL Note :If another procedure like meniscus repair or OATS (Osteochondralautograft transfer) has been done along with ACL reconstruction
This presentation is the intellectual property of the author. Contact them for permission to reprint and/or distribute.
 The Stiff Hand: Manual Therapy Sylvia Dávila, PT, CHT San Antonio, Texas Orthopedic Manual Therapy Common Applications Passive stretch Tensile force to tissue to increase extensibility of length & ROM
The Stiff Hand: Manual Therapy Sylvia Dávila, PT, CHT San Antonio, Texas Orthopedic Manual Therapy Common Applications Passive stretch Tensile force to tissue to increase extensibility of length & ROM
Acute Achilles Tendon Repair Protocol
 Acute Achilles Tendon Repair Protocol As tolerated should be understood to perform with safety for the reconstruction/repair. Pain, limp, swelling, or other undesirable factors are indicators that you
Acute Achilles Tendon Repair Protocol As tolerated should be understood to perform with safety for the reconstruction/repair. Pain, limp, swelling, or other undesirable factors are indicators that you
Nursing Management: Musculoskeletal Trauma and Orthopedic Surgery. By: Aun Lauriz E. Macuja SAC_SN4
 Nursing Management: Musculoskeletal Trauma and Orthopedic Surgery By: Aun Lauriz E. Macuja SAC_SN4 The most common cause of musculoskeletal injuries is a traumatic event resulting in fracture, dislocation,
Nursing Management: Musculoskeletal Trauma and Orthopedic Surgery By: Aun Lauriz E. Macuja SAC_SN4 The most common cause of musculoskeletal injuries is a traumatic event resulting in fracture, dislocation,
NONOPERATIVE REHABILITATION FOLLOWING ACL INJURY ( Program)
") Therapist: Phone: NONOPERATIVE REHABILITATION FOLLOWING ACL INJURY (3-3-4-4 Program) IMMEDIATE INJURY PHASE (Day 1 to Day 7) Restore full passive knee extension Diminish joint swelling and pain Restore
Therapist: Phone: NONOPERATIVE REHABILITATION FOLLOWING ACL INJURY (3-3-4-4 Program) IMMEDIATE INJURY PHASE (Day 1 to Day 7) Restore full passive knee extension Diminish joint swelling and pain Restore
CENTER FOR ORTHOPAEDICS AND SPINE CARE PHYSICAL THERAPY PROTOCOL REHABILITATION FOLLOWING UNILATERAL PETELLAR TENDON REPAIR BENJAMIN J.
 I. Immediate Postoperative Phase (Days 1-7) Restore full passive knee extension Diminish pain and joint swelling Restore patellar mobility Initiate early controlled motion *Controlled forces on repair
I. Immediate Postoperative Phase (Days 1-7) Restore full passive knee extension Diminish pain and joint swelling Restore patellar mobility Initiate early controlled motion *Controlled forces on repair
Shoulder Arthroscopy with Rotator Cuff Repair Rehabilitation Protocol
 General Notes: As tolerated should be understood to include with safety for the surgical procedure; a sudden increase in pain, swelling, or other undesirable factors are indicators that you are doing too
General Notes: As tolerated should be understood to include with safety for the surgical procedure; a sudden increase in pain, swelling, or other undesirable factors are indicators that you are doing too
9180 KATY FREEWAY, STE. 200 (713)
") AUTOLOGOUS CHONDROCYTE IMPLANTATION Femoral Condyle Rehabilitation Guidelines PHASE I - PROTECTION PHASE (WEEKS 0-6) Goals: - Protect healing tissue from load and shear forces - Decrease pain and effusion
AUTOLOGOUS CHONDROCYTE IMPLANTATION Femoral Condyle Rehabilitation Guidelines PHASE I - PROTECTION PHASE (WEEKS 0-6) Goals: - Protect healing tissue from load and shear forces - Decrease pain and effusion
Sheena Black, MD PHYSICAL THERAPY PRESCRIPTION MCL RECONSTRUCTION. Orthopaedic Surgery, Sports Medicine.
 PHYSICAL THERAPY PRESCRIPTION Name: Date: Post-Operative Diagnosis: Right Left MCL Reconstruction Graft: BTB Hamstring Allograft Additional Procedures: Lateral Menisectomy Medial Menisectomy Lateral Meniscal
PHYSICAL THERAPY PRESCRIPTION Name: Date: Post-Operative Diagnosis: Right Left MCL Reconstruction Graft: BTB Hamstring Allograft Additional Procedures: Lateral Menisectomy Medial Menisectomy Lateral Meniscal
EVALUATION AND MEASUREMENTS. I. Devreux
 EVALUATION AND MEASUREMENTS I. Devreux To determine the extent and degree of muscular weakness resulting from disease, injury or disuse. The records obtained from these tests provide a base for planning
EVALUATION AND MEASUREMENTS I. Devreux To determine the extent and degree of muscular weakness resulting from disease, injury or disuse. The records obtained from these tests provide a base for planning
Shoulder Arthroscopy with Posterior Labral Repair Rehabilitation Protocol
 General Notes: As tolerated should be understood to include with safety for the surgical procedure; a sudden increase in pain, swelling, or other undesirable factors are indicators that you are doing too
General Notes: As tolerated should be understood to include with safety for the surgical procedure; a sudden increase in pain, swelling, or other undesirable factors are indicators that you are doing too
Chapter 1: Exercise Physiology. ACE Personal Trainer Manual Third Edition
 Chapter 1: Exercise Physiology ACE Personal Trainer Manual Third Edition Introduction Physiology is the study of the myriad functions in a living organism. Exercise physiology is the study of the ways
Chapter 1: Exercise Physiology ACE Personal Trainer Manual Third Edition Introduction Physiology is the study of the myriad functions in a living organism. Exercise physiology is the study of the ways
Training For The Triple Jump. The Aston Moore Way
 Training For The Triple Jump The Aston Moore Way Establish Your Technical Style/Model Go anywhere in the world, the triple jumps is still just a hop, step and a jump So, what do I mean by technical style
Training For The Triple Jump The Aston Moore Way Establish Your Technical Style/Model Go anywhere in the world, the triple jumps is still just a hop, step and a jump So, what do I mean by technical style
Sheena Black, MD. Orthopaedic Surgery, Sports Medicine PHYSICAL THERAPY PRESCRIPTION ACL RECONSTRUCTION PATELLAR TENDON/ BTB TECHNIQUE
 PHYSICAL THERAPY PRESCRIPTION ACL RECONSTRUCTION PATELLAR TENDON/ BTB TECHNIQUE Name: Date: Post-Operative Diagnosis: Right Left ACL Reconstruction Graft: BTB Hamstring Allograft Additional Procedures:
PHYSICAL THERAPY PRESCRIPTION ACL RECONSTRUCTION PATELLAR TENDON/ BTB TECHNIQUE Name: Date: Post-Operative Diagnosis: Right Left ACL Reconstruction Graft: BTB Hamstring Allograft Additional Procedures:
Nonoperative Rehabilitation for Multi-Directional Instability
 Nonoperative Rehabilitation for Multi-Directional Instability This multi-phased program is designed to allow the patient/athlete to return to their previous functional level as quickly and safely as possible.
Nonoperative Rehabilitation for Multi-Directional Instability This multi-phased program is designed to allow the patient/athlete to return to their previous functional level as quickly and safely as possible.
Hip Arthroscopy with CAM resection/labral Repair Protocol
 Hip Arthroscopy with CAM resection/labral Repair Protocol As tolerated should be understood to perform with safety for the reconstruction/repair. Pain, limp, swelling, or other undesirable factors are
Hip Arthroscopy with CAM resection/labral Repair Protocol As tolerated should be understood to perform with safety for the reconstruction/repair. Pain, limp, swelling, or other undesirable factors are