Medications Contributing to Falls. Kate Niemann, PharmD BCGP AuBurn Pharmacy
|
|
|
- Leslie Little
- 5 years ago
- Views:
Transcription




1 Medications Contributing to Falls Kate Niemann, PharmD BCGP AuBurn Pharmacy
2 Why Are Falls Important? Leading cause of injury in elders Costs to the system (CDC, 2008) ER Visits: 2.2 million $28.2 billion in healthcare costs Mortality 19,700 Hospitalizations 581,000 Falls reduce quality of life Issues with mobility, self care Anxiety / depression
3 Risk Factors for Falls Advanced age Postural hypotension Female gender Depression Previous fall history Urinary incontinence Impaired mobility Stroke Arthritis / joint disorder Cardiovascular disease Parkinson s disease Dizziness Vision impairment Chronic disease Hearing impairment Pain Cognitive impairment Low level of activity
4 Some Ways Medications May Contribute Adverse CNS Effects Dizziness, Drowsiness Numerous medications have this potential side effect Bladder and Bowel Changes Particularly, diarrhea and increased urination Increased trips to bathroom and sense of urgency may result in falls Gait disturbances / pseudoparkinsonism Muscle rigidity and abnormal movements may make ambulation difficult
5 Adverse CNS Effects Dizziness and Drowsiness
6 Dizziness and Drowsiness Medications that can cause these side effects are TNTC (too numerous to count). Some main of concern: Antidepressants Antipsychotics Sedative hypnotics Anxiolytics, especially benzodiazepines Pain medications, particularly opioids 1 st generation antihistamines Anticholinergic medications All of the above we try to reduce use!
7 Sedative Hypnotics Class includes: Zolpidem, Zaleplon, Triazolam, Temazepam, Eszopiclone, Suvorexant Used to promote sleep and combat insomnia Drawbacks: Tolerance Addictive potential / Dependence Side effects Potential relationship with dementia
8 Sedative Hypnotics - Alternatives Melatonin Natural chemical used by the body in the regulation of sleep (circadian rhythm) Does not lead to dependence Bedtime routines Warm milk or decaffeinated tea before bed Warm blanket Soothing music Foot / hand treatments before bed Environmental Factors Quiet environment Lights reduced Appropriate temperature for resident
9 Anxiolytics Examples: clonazepam, alprazolam, lorazepam, diazepam Anxiolytics, particularly benzodiazepines, can contribute to falls Also carry risks of tolerance and dependence Consider, for chronic anxiety: Antidepressants should be attempted first These do carry a fall risk as well If antidepressant monotherapy fails, then adjunctive agent could be added for anxiety, BUT be sure we have attempted non-pharmacologic methods first Address boredom Make use of home routines Address environmental factors
10 Drugs with Anticholinergic Side Effects Anticholinergic side effects include urinary retention, blurred vision, constipation, dizziness, and drowsiness Numerous medications have anticholinergic side effect potential, some examples: Benzodiazepines 1 st generation antihistamines Tricyclic antidepressants (TCAs) Some antidepressants Urinary anticholinergics Benztropine, Amantadine Antipsychotics (Ox)Carbamazepine Valproic acid Metoclopramide Muscle relaxants Opioids
11 Beers Criteria and STOPP/START These listings attempt to identify potentially inappropriate medications in the elderly Not surprisingly, there is considerable overlap Numerous anticholinergic drugs listed Some differences between In the U.S., it seems Beers Criteria better known and more popular Beers Criteria will itemize potentially problematic drugs and give a recommendation, rationale, quality of evidence and strength of recommendation If resident is on a Beers listed med, be sure: Medication is truly needed Alternatives have been considered (possibly attempted) Lowest effective dose of the medication is in use


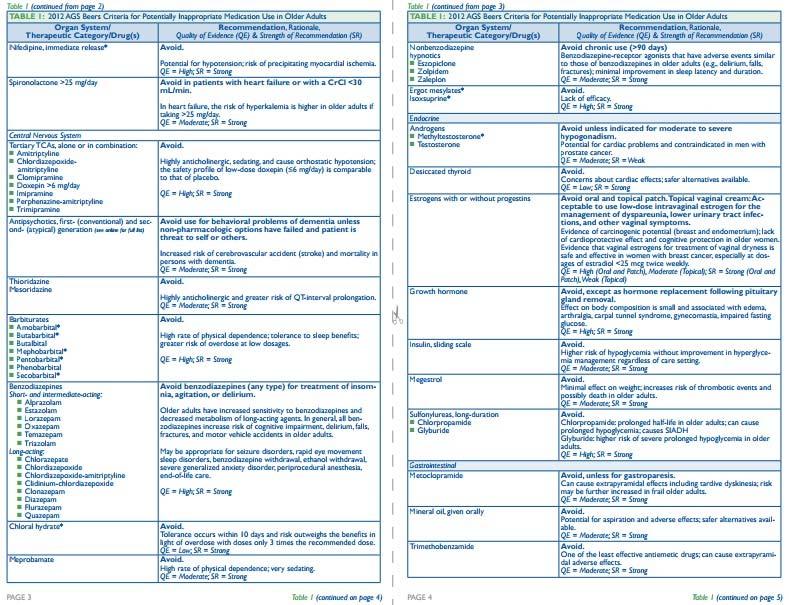
12 Beers, Snapshot
13 Reducing Anticholinergic Burden, Examples If urinary anticholinergic is needed, consider solifenacin or trospium, rather than oxybutynin Mirabegron? If antihistamine is needed, consider a second generation (cetirizine, loratadine, fexofenadine) rather than first (diphenhydramine, chlorpheniramine) If antidepressant is needed, avoid tricyclic antidepressants (nortriptyline, desipramine, etc.) and paroxetine (SSRI) and use SSRIs with lower anticholinergic burden (e.g. escitalopram, sertraline) or SNRIs
14 Bowel & Bladder Changes
15 Bowel & Bladder Changes Cause Diarrhea Proton Pump Inhibitors (PPIs) Cause Inc. Urination Diuretics Antacids Antibiotics! Antidepressants Lithium Alpha blockers (e.g. doxazosin, prazosin, terazosin) Bethanechol Chemotherapy Metformin, Victoza, Trulicity, etc. Colchicine ACE Inhibitors NSAIDs Overuse / too high of a dose of laxative
16 Bowel & Bladder Changes Constipation also needs to be addressed Numerous agents can cause constipation Opioids Medications with anticholinergic side effects Antidepressants the list goes on. Constipation can put pressure on the bladder and reduce its ability to expand, in turn leading to increased urgency and frequency.
17 Drug Induced Parkinsonism, Abnormal Movements, Gait Abnormalities
18 Drugs With Abnormal Muscle Movements, Parkinsonism, Gait Disturbances Antipsychotics Seroquel and Clozaril less so than others in class These are your preferred agents for Parkinsons psychosis if traditional antipsychotic must be used, or, Nuplazid has different mechanism of action no worsening of Parkinson motor symptoms Metoclopramide More of an effect on serotonin than dopamine Depakote (valproic acid) Lithium




19 Drugs With Abnormal Muscle Movements, Parkinsonism, Gait Disturbances Table from Journal of Clinical Neurology
20 Drugs With Abnormal Muscle Movements, Parkinsonism, Gait Disturbances Drug-induced parkinsonism usually resolves within weeks to months after stopping the offending drug; however, parkinsonism may persist or progress in 10-50% of patients. Further argument against antipsychotic use for inappropriate indications Drug Induced Parkinsonism, Journal of Clinical Neurology, 2012 March 31. Hae-Won Shin, Sun Ju Chung
21 Other Factors to Consider
22 Unaddressed Needs Pain Is the patient in pain, and is getting up or moving in bed, attempting to find comfort Is pain limiting the patient s range of motion, thereby increasing fall risk Is neuropathy in feet impairing patient s ability to walk NOTE: If patient is in chronic pain, they ll be more likely to limit motion and exercise, which could lead to weakness and functional decline
23 Unaddressed Needs Physical & Occupational Therapy PT/OT should be considered Restore strength, balance and coordination Safe transfer techniques Appropriate footwear Medicare will cover diabetic shoes given proper documentation Environmental considerations Provide good lighting Clean spills immediately To the best of your ability, keep floors clutter free Consider bed position
24 Unaddressed Needs Boredom Activities Try to schedule activities around peak fall times Diet Ensure diet is appropriate for patient Weight loss may be associated with weakness Toileting Programs More to come
25 Recapping Falls and Meds
26 Agency for Healthcare Research & Quality The AHRQ has a tool for hospitals to evaluate fall risk Point Value (Risk Level) Drug Class Comments 3 (High) Analgesics,* antipsychotics, anticonvulsants, benzodiazepines 2 (Medium) Antihypertensives, cardiac drugs, antiarrhythmics, antidepressants Sedation, dizziness, postural disturbances, altered gait and balance, impaired cognition Induced orthostasis, impaired cerebral perfusion, poor health status 1 (Low) Diuretics Increased ambulation, induced orthostasis Score 6 Higher risk for fall; evaluate patient
27 Overall Medication Concerns Reduce anticholinergic burden Find alternatives Find lowest effective dose Evaluate all psychotropic medications periodically for potential reduction Reserve antipsychotic use for truly needed conditions Consider alternatives to hypnotics and benzodiazepines Reduce any routine pain medications to the minimum effective dose Employ any/all means of pain control possible to reduce systemic pain medication use Ensure bowel and bladder function is where it should be Are med changes needed?
28 Beers and STOPP/START American Geriatric Society (AGS): To purchase a Beers list pocket card or other publication through AGS: -criteria-pocketcard/pc001 STOPP/START Many articles regarding this topic out there, one source:



29 Kate Niemann, (office) (cell)
30 Bibliography Drug-related falls in older patients: implicated drugs, consequences and possible prevention strategies, Therapeutic Advances in Drug Safety, 2013 Aug; 4(4): Marlies R de Jong, Maarten Van der Elst, and Klaas A. Hartholt Alternative Medications to High-Risk Medications in the Elderly; Harmful Drug-Disease Interactions in the Elderly; Quality Measures, Journal of American Geriatrics Society, Joseph T Hanlon, Todd Semla, Kenneth Schmader, 8 Oct 2015 (Beer s Criteria Update) Agency for Healthcare Research and Equality, Preventing Falls in Hospitals, Tool 3I: Medication Fall Risk Score and Evaluation Tools Drug Induced Parkinsonism, Journal of Clinical Neurology, 2012 March 31. Hae-Won Shin, Sun Ju Chung. Are Your Medications Causing or Increasing Incontinence? Cleveland Clinic, Urinary and Kidney Team, health.clevelandclinic.org/are-your-medications-causing-orincreasing-incontinence/amp/
Katee Kindler, PharmD, BCACP
 Speaker Introduction Katee Kindler, PharmD, BCACP Current Practice: Clinical Pharmacy Specialist Ambulatory Care, St. Vincent Indianapolis Assistant Professor of Pharmacy Practice, Manchester University,
Speaker Introduction Katee Kindler, PharmD, BCACP Current Practice: Clinical Pharmacy Specialist Ambulatory Care, St. Vincent Indianapolis Assistant Professor of Pharmacy Practice, Manchester University,
Falls most commonly seen in RACFs are due to tripping, slipping and stumbling (21.6%). Falling down stairs is relatively uncommon in
. Falling down stairs is relatively uncommon in") This Presentation Medications and Falls Dr Peter Tenni M Pharm (Curtin), PhD (UTAS) AACPA Director, CPS A fall is an event which results in a person coming to rest inadvertently on the ground or floor
This Presentation Medications and Falls Dr Peter Tenni M Pharm (Curtin), PhD (UTAS) AACPA Director, CPS A fall is an event which results in a person coming to rest inadvertently on the ground or floor
Fall Prevention in Hospice (A pharmacologic and nonpharmacologic approach)
") Fall Prevention in Hospice (A pharmacologic and nonpharmacologic approach) Chinenye Emereole, Pharm.D. Clinical Pharmacist Hospice Pharmacy Solutions Objectives Assess and identify hospice patients who
Fall Prevention in Hospice (A pharmacologic and nonpharmacologic approach) Chinenye Emereole, Pharm.D. Clinical Pharmacist Hospice Pharmacy Solutions Objectives Assess and identify hospice patients who
1/21/2016 UPDATE ON THE AMERICAN GERIATRICS SOCIETY 2015 BEERS CRITERIA DISCLOSURE OBJECTIVES AGING GOALS BEERS CRITERIA
 UPDATE ON THE AMERICAN GERIATRICS SOCIETY 2015 BEERS CRITERIA DISCLOSURE I have no financial conflict of interest to disclose. Lacey Charbonneau, Pharm.D. PGY-1 Community Practice Resident Baptist Medical
UPDATE ON THE AMERICAN GERIATRICS SOCIETY 2015 BEERS CRITERIA DISCLOSURE I have no financial conflict of interest to disclose. Lacey Charbonneau, Pharm.D. PGY-1 Community Practice Resident Baptist Medical
Geri-PARDY! (2015 Beers Criteria) Pharmacology Edition
 Pharmacology Edition") Geri-PARDY! Pharmacology Edition (2015 Beers Criteria) Aurelio Muyot, MD, AGSF, FACP Assistant Professor College of Osteopathic Medicine Touro University Nevada Objectives Review the 2015 Beers Criteria
Geri-PARDY! Pharmacology Edition (2015 Beers Criteria) Aurelio Muyot, MD, AGSF, FACP Assistant Professor College of Osteopathic Medicine Touro University Nevada Objectives Review the 2015 Beers Criteria
COMMON DRUG RELATED PROBLEMS SEEN IN PACE AND MECHANISMS TO MITIGATE RISK
 COMMON DRUG RELATED PROBLEMS SEEN IN PACE AND MECHANISMS TO MITIGATE RISK Robert L Alesiani, PharmD, CGP Chief Pharmacotherapy Officer CareKinesis, Inc. (a Tabula Rasa Healthcare Company) 2 3 4 5 Pharmacogenomics
COMMON DRUG RELATED PROBLEMS SEEN IN PACE AND MECHANISMS TO MITIGATE RISK Robert L Alesiani, PharmD, CGP Chief Pharmacotherapy Officer CareKinesis, Inc. (a Tabula Rasa Healthcare Company) 2 3 4 5 Pharmacogenomics
Insomnia: Updates in Medical Management. Michael Newnam M.D.
 Insomnia: Updates in Medical Management Michael Newnam M.D. Sleep Neurobiology Delicate balance of excitatory and inhibitory neurotransmitters that control the switch between wakefulness and sleep Circadian
Insomnia: Updates in Medical Management Michael Newnam M.D. Sleep Neurobiology Delicate balance of excitatory and inhibitory neurotransmitters that control the switch between wakefulness and sleep Circadian
Primary Care Approach for Evaluating the Risk of Falls with Elderly Patients. Danielle Hansen, DO, MS (Med Ed), MHSA
, MHSA") Primary Care Approach for Evaluating the Risk of Falls with Elderly Patients Danielle Hansen, DO, MS (Med Ed), MHSA Clinical Assistant Professor, LECOM Associate Director, LECOM Institute for Successful
Primary Care Approach for Evaluating the Risk of Falls with Elderly Patients Danielle Hansen, DO, MS (Med Ed), MHSA Clinical Assistant Professor, LECOM Associate Director, LECOM Institute for Successful
Medication Use in Older Adults
 Medication Use in Older Adults F. Michael Gloth, III, MD, AGSF, FACP, CMD Clinical Professor Department of Geriatrics, Florida State University College of Medicine Associate Professor of Medicine Division
Medication Use in Older Adults F. Michael Gloth, III, MD, AGSF, FACP, CMD Clinical Professor Department of Geriatrics, Florida State University College of Medicine Associate Professor of Medicine Division
Black holes taped on floor Redirection Music and activities Yellow straps across the door Remind other residents to use call bell when she comes in
 Intrusive Wandering Case study........................................... A 97 year old woman with dementia lives in a mixed 23 bed LTC unit. She is independently mobile in her wheelchair and goes in and
Intrusive Wandering Case study........................................... A 97 year old woman with dementia lives in a mixed 23 bed LTC unit. She is independently mobile in her wheelchair and goes in and
Using the ASCP-NCOA Falls Risk Reduction Toolkit Part 1: A Companion to CDC's STEADI Toolkit
 Using the ASCP-NCOA Falls Risk Reduction Toolkit Part 1: A Companion to CDC's STEADI Toolkit Target Audience: Pharmacists ACPE#: 0202-9999-18-056-L01-P Activity Type: Application-based Disclosures Kathleen
Using the ASCP-NCOA Falls Risk Reduction Toolkit Part 1: A Companion to CDC's STEADI Toolkit Target Audience: Pharmacists ACPE#: 0202-9999-18-056-L01-P Activity Type: Application-based Disclosures Kathleen
STOPP and START criteria October 2011
 # START and STOPP are newer criteria to identify potentially inappropriate medications in elderly, including drug drug and drug disease interactions, drugs which increase risk of falls and drugs which
# START and STOPP are newer criteria to identify potentially inappropriate medications in elderly, including drug drug and drug disease interactions, drugs which increase risk of falls and drugs which
Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016
 Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016 Disclosures: Drugs in Older Adults: Beers Criteria Heather Sakely,
Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016 Disclosures: Drugs in Older Adults: Beers Criteria Heather Sakely,
Friend or Foe? Review of the Regulations & Benefits: Risk Profiles of the Benzodiazepines
 Friend or Foe? Review of the Regulations & Benefits: Risk Profiles of the Benzodiazepines Program Learning Objectives At the conclusion of the activity, participants should be able to: Have a basic understanding
Friend or Foe? Review of the Regulations & Benefits: Risk Profiles of the Benzodiazepines Program Learning Objectives At the conclusion of the activity, participants should be able to: Have a basic understanding
Psychotropic Medication Use in Dementia
 Psychotropic Medication Use in Dementia Marie A DeWitt, MD Diplomate of the American Board of Psychiatry and Neurology, Specialization in Psychiatry & Subspecialization in Geriatric Psychiatry Staff Physician,
Psychotropic Medication Use in Dementia Marie A DeWitt, MD Diplomate of the American Board of Psychiatry and Neurology, Specialization in Psychiatry & Subspecialization in Geriatric Psychiatry Staff Physician,
INSOMNIA IN THE GERIATRIC POPULATION. Shannon Bush, MS4
 INSOMNIA IN THE GERIATRIC POPULATION Shannon Bush, MS4 CHANGES IN SLEEP ARCHITECTURE 2 Reduction in slow wave sleep (stage 3 and 4) Increase in lighter stages of sleep (stage 1 and 2) Decrease in REM sleep
INSOMNIA IN THE GERIATRIC POPULATION Shannon Bush, MS4 CHANGES IN SLEEP ARCHITECTURE 2 Reduction in slow wave sleep (stage 3 and 4) Increase in lighter stages of sleep (stage 1 and 2) Decrease in REM sleep
Prevention of Medication-Related Falls Through Appropriate Medication Use. Clay Sprouse, MEd., CPhT Piedmont Technical College
 Prevention of Medication-Related Falls Through Appropriate Medication Use Clay Sprouse, MEd., CPhT Piedmont Technical College Disclosure I have no relevant financial or nonfinancial relationships to disclose
Prevention of Medication-Related Falls Through Appropriate Medication Use Clay Sprouse, MEd., CPhT Piedmont Technical College Disclosure I have no relevant financial or nonfinancial relationships to disclose
A Step Forward: Promoting Independence through Falls Prevention
 A Step Forward: Promoting Independence through Falls Prevention 2014 Geriatric Update Meharry Consortium Geriatric Education Center A Step Forward: Promoting Independence through Falls Prevention Moderator:
A Step Forward: Promoting Independence through Falls Prevention 2014 Geriatric Update Meharry Consortium Geriatric Education Center A Step Forward: Promoting Independence through Falls Prevention Moderator:
Rational prescribing in the older adult. Assoc Prof Craig Whitehead
 Rational prescribing in the older adult Assoc Prof Craig Whitehead Introduction Physioloical ageing and frailty Medication risks in older adults Drug Burden Anticholinergic and sedative drug burden Cascade
Rational prescribing in the older adult Assoc Prof Craig Whitehead Introduction Physioloical ageing and frailty Medication risks in older adults Drug Burden Anticholinergic and sedative drug burden Cascade
Caring for a Patient or Family Member with Alzheimer s Disease or Related Dementia
 Caring for a Patient or Family Member with Alzheimer s Disease or Related Dementia Tiffany D. Long, MS4 UNC School of Medicine MD Candidate Class of 2018 Disclaimers A portion of this project is/was supported
Caring for a Patient or Family Member with Alzheimer s Disease or Related Dementia Tiffany D. Long, MS4 UNC School of Medicine MD Candidate Class of 2018 Disclaimers A portion of this project is/was supported
Workshop 4: Preventing Falls through Medication Vigilance
 Workshop 4: Preventing Falls through Medication Vigilance Nancy L. Losben, R.Ph., CCP, FASCP, CG Chief Quality Officer Omnicare, Inc. & Diane C. Vaughn, RN, C-DONA/LTC, LNHA VP, Clinical Services Benedictine
Workshop 4: Preventing Falls through Medication Vigilance Nancy L. Losben, R.Ph., CCP, FASCP, CG Chief Quality Officer Omnicare, Inc. & Diane C. Vaughn, RN, C-DONA/LTC, LNHA VP, Clinical Services Benedictine
PRESCRIBING IN THE ELDERLY. CARE HOME PHARMACY TEAM Bhavini Shah, Eleesha Pentiah & Puja Vyas
 PRESCRIBING IN THE ELDERLY CARE HOME PHARMACY TEAM Bhavini Shah, Eleesha Pentiah & Puja Vyas LEARNING OUTCOMES Medicines Optimisation The effects of aging on health and medicines. Polypharmacy Acute Kidney
PRESCRIBING IN THE ELDERLY CARE HOME PHARMACY TEAM Bhavini Shah, Eleesha Pentiah & Puja Vyas LEARNING OUTCOMES Medicines Optimisation The effects of aging on health and medicines. Polypharmacy Acute Kidney
Anxiety Pharmacology UNIVERSITY OF HAWAI I HILO PRE -NURSING PROGRAM
 Anxiety Pharmacology UNIVERSITY OF HAWAI I HILO PRE NURSING PROGRAM NURS 203 GENERAL PHARMACOLOGY DANITA NARCISO PHARM D Learning Objectives Understand the normal processing of fear vs fear processing
Anxiety Pharmacology UNIVERSITY OF HAWAI I HILO PRE NURSING PROGRAM NURS 203 GENERAL PHARMACOLOGY DANITA NARCISO PHARM D Learning Objectives Understand the normal processing of fear vs fear processing
Assessing the impact of medicine on falls risk
 Medicines and falls Assessing the impact of medicine on falls risk This presentation is designed for registered nurses, but may be applicable to all nursing staff at the aged care facility. It is part
Medicines and falls Assessing the impact of medicine on falls risk This presentation is designed for registered nurses, but may be applicable to all nursing staff at the aged care facility. It is part
Potentially Inappropriate Medication Use in Older Adults 2015 Latest Research
 Home Resources Potentially Inappropriate Medication Use in Older Adults 2015 Resources Potentially Inappropriate Medication Use in Older Adults 2015 Latest Research Drugs and Categories of Drugs What these
Home Resources Potentially Inappropriate Medication Use in Older Adults 2015 Resources Potentially Inappropriate Medication Use in Older Adults 2015 Latest Research Drugs and Categories of Drugs What these
Geriatric Pharmacology
 Geriatric Pharmacology Janice Scheufler R.Ph.,PharmD, FASCP Clinical Pharmacist Hospice of the Western Reserve Objectives List three risk factors for adverse drug events in the elderly Discuss two physiological
Geriatric Pharmacology Janice Scheufler R.Ph.,PharmD, FASCP Clinical Pharmacist Hospice of the Western Reserve Objectives List three risk factors for adverse drug events in the elderly Discuss two physiological
Causes of Transient Incontinence. Geriatrics: Urinary Incontinence, Dementia, and Delirium. Classification of Established Incontinence
 Causes of Transient Geriatrics: Urinary, Dementia, and Delirium Carla Zeilmann, PharmD, BCPS St. Louis College of Pharmacy Therapeutics 3 Fall 2003 D delirium I infection A atrophic urethritis and vaginitis
Causes of Transient Geriatrics: Urinary, Dementia, and Delirium Carla Zeilmann, PharmD, BCPS St. Louis College of Pharmacy Therapeutics 3 Fall 2003 D delirium I infection A atrophic urethritis and vaginitis
DRUGS THAT ACT IN THE CNS
 DRUGS THAT ACT IN THE CNS Anxiolytic and Hypnotic Drugs Dr Karamallah S. Mahmood PhD Clinical Pharmacology 1 OTHER ANXIOLYTIC AGENTS/ A. Antidepressants Many antidepressants are effective in the treatment
DRUGS THAT ACT IN THE CNS Anxiolytic and Hypnotic Drugs Dr Karamallah S. Mahmood PhD Clinical Pharmacology 1 OTHER ANXIOLYTIC AGENTS/ A. Antidepressants Many antidepressants are effective in the treatment
Mentoring Session: Participant Cases
 Handout for the Neuroscience Education Institute (NEI) online activity: Mentoring Session: Participant Cases The Case: 55-year-old patient with depression and anxiety The Question: What to do when antidepressants
Handout for the Neuroscience Education Institute (NEI) online activity: Mentoring Session: Participant Cases The Case: 55-year-old patient with depression and anxiety The Question: What to do when antidepressants
Meds and Falls: Keep in Step with your Meds
 Meds and Falls: Keep in Step with your Meds Donna Bartlett PharmD, CGP, RPh Associate Professor-Pharmacy Practice MCPHS University Clinical Pharmacist-MCPHS University- Pharmacy Outreach Program donna.bartlett@mcphs.edu
Meds and Falls: Keep in Step with your Meds Donna Bartlett PharmD, CGP, RPh Associate Professor-Pharmacy Practice MCPHS University Clinical Pharmacist-MCPHS University- Pharmacy Outreach Program donna.bartlett@mcphs.edu
Residents Who Don t Sleep
 Residents Who Don t Sleep Case study........................................... An 86 yr. old woman has diagnoses of Alzheimer s disease, congestive heart failure, constipation, depression, hypertension
Residents Who Don t Sleep Case study........................................... An 86 yr. old woman has diagnoses of Alzheimer s disease, congestive heart failure, constipation, depression, hypertension
risk factors for falling
 Resource # 10 Page 1 of 8 1. Dizziness- What Can Cause Dizziness? Not eating regularly Change in body position (e.g. from sitting to standing) Low blood pressure High blood pressure Medication side effects
Resource # 10 Page 1 of 8 1. Dizziness- What Can Cause Dizziness? Not eating regularly Change in body position (e.g. from sitting to standing) Low blood pressure High blood pressure Medication side effects
Anti-Depressant Medications
 Anti-Depressant Medications A Introduction: This topic may be a little bit underestimated here in Jordan, while in western countries it has more significance. The function of anti-depressants is to change
Anti-Depressant Medications A Introduction: This topic may be a little bit underestimated here in Jordan, while in western countries it has more significance. The function of anti-depressants is to change
Anxiolytic, Sedative and Hypnotic Drugs. Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia
 Anxiolytic, Sedative and Hypnotic Drugs Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Anxiolytics: reduce anxiety Sedatives: decrease activity, calming
Anxiolytic, Sedative and Hypnotic Drugs Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Anxiolytics: reduce anxiety Sedatives: decrease activity, calming
Nortriptyline vs amitriptyline in elderly
 Nortriptyline vs amitriptyline in elderly Amitriptyline (Elavil ) vs other antidepressants - comparative analysis amitriptyline vs divalproate, amitriptyline vs trazodone. Learn what other patients are
Nortriptyline vs amitriptyline in elderly Amitriptyline (Elavil ) vs other antidepressants - comparative analysis amitriptyline vs divalproate, amitriptyline vs trazodone. Learn what other patients are
Use of Psychotropic Medications in Older Adults with Dementia!
 Use of Psychotropic Medications in Older Adults with Dementia! Deepa Pattani, PharmD, RPh Owner: PrevInteract Health Deepa.Pattani@PrevInteract.com 972-372-9775 About Me Deepa Pattani, PharmD, RPh with
Use of Psychotropic Medications in Older Adults with Dementia! Deepa Pattani, PharmD, RPh Owner: PrevInteract Health Deepa.Pattani@PrevInteract.com 972-372-9775 About Me Deepa Pattani, PharmD, RPh with
Medicine Related Falls Risk Assessment Tool (MRFRAT)
") Medicine Related Falls Risk Assessment Tool (MRFRAT) The Medicine Related Falls Risk Assessment tool (MRFRAT) in Appendix 1 is designed to help identify patients at risk of falls due to their current medicine
Medicine Related Falls Risk Assessment Tool (MRFRAT) The Medicine Related Falls Risk Assessment tool (MRFRAT) in Appendix 1 is designed to help identify patients at risk of falls due to their current medicine
Learning Objectives. Delirium. Delirium. Delirium. Terminal Restlessness 3/28/2016
 Terminal Restlessness Dr. Christopher Churchill St. Cloud VA Health Care System EC&R Service Line Director & Medical Director Hospice & Palliative Care March 31, 2016 Learning Objectives Different Terminology
Terminal Restlessness Dr. Christopher Churchill St. Cloud VA Health Care System EC&R Service Line Director & Medical Director Hospice & Palliative Care March 31, 2016 Learning Objectives Different Terminology
Inappropriate Medication Use in the Elderly
 Inappropriate Medication Use in the Elderly Amanda Ilenin, Pharm.D. OhioHealth Dublin Methodist Hospital & OhioHealth Grady Memorial Hospital Kristian Navickas, Pharm.D. OhioHealth McConnell Heart Health
Inappropriate Medication Use in the Elderly Amanda Ilenin, Pharm.D. OhioHealth Dublin Methodist Hospital & OhioHealth Grady Memorial Hospital Kristian Navickas, Pharm.D. OhioHealth McConnell Heart Health
BEHAVIORAL PROBLEMS IN DEMENTIA
 BEHAVIORAL PROBLEMS IN DEMENTIA CLINICAL FEATURES Particularly as dementia progresses, psychiatric symptoms may develop that resemble discrete mental disorders such as depression or mania The course and
BEHAVIORAL PROBLEMS IN DEMENTIA CLINICAL FEATURES Particularly as dementia progresses, psychiatric symptoms may develop that resemble discrete mental disorders such as depression or mania The course and
Disclosures. Geriatric Incontinence and Voiding Dysfunction. Agenda. Agenda. UI: a Geriatric Syndrome. Geriatric Syndromes 9/7/2018.
 Disclosures Geriatric Incontinence and Voiding Dysfunction None Shachi Tyagi MD, MS Assistant Professor Division of Geriatric Medicine University of Pittsburgh Medical Center UI: a Geriatric Syndrome Geriatric
Disclosures Geriatric Incontinence and Voiding Dysfunction None Shachi Tyagi MD, MS Assistant Professor Division of Geriatric Medicine University of Pittsburgh Medical Center UI: a Geriatric Syndrome Geriatric
4/2/13 COMMON CLASSES OF MEDICATIONS. Child & Adolescent Behavioral Medicine & Medication Therapies. Behavioral Medicine & Medication Therapies
 Child & Adolescent Behavioral Medicine & Medication Therapies Brian J Cowles, PharmD Associate Professor of Pharmacy Practice Albany College of Pharmacy & Health Sciences; Vermont Campus Behavioral Medicine
Child & Adolescent Behavioral Medicine & Medication Therapies Brian J Cowles, PharmD Associate Professor of Pharmacy Practice Albany College of Pharmacy & Health Sciences; Vermont Campus Behavioral Medicine
Treating sleep disorders
 Treating sleep disorders Sue Wilson Centre for Neuropsychopharmacology Imperial College London sue.wilson@imperial.ac.uk Suggested algorithm for treatment of insomnia Diagnosis of insomnia Associated with
Treating sleep disorders Sue Wilson Centre for Neuropsychopharmacology Imperial College London sue.wilson@imperial.ac.uk Suggested algorithm for treatment of insomnia Diagnosis of insomnia Associated with
STOPP START Toolkit Supporting Medication Review in the Older Person
 STOPP START Toolkit Supporting Medication Review in the Older Person STOPP: Screening Tool of Older People s potentially inappropriate Prescriptions START: Screening Tool to Alert doctors to Right (appropriate,
STOPP START Toolkit Supporting Medication Review in the Older Person STOPP: Screening Tool of Older People s potentially inappropriate Prescriptions START: Screening Tool to Alert doctors to Right (appropriate,
Psychotropic Medications Archana Jhawar, PharmD, BCPP Clinical Faculty of UIC Pharmacy Practice Clinical Psychiatric Pharmacist Jesse Brown VA
 Psychotropic Medications Archana Jhawar, PharmD, BCPP Clinical Faculty of UIC Pharmacy Practice Clinical Psychiatric Pharmacist Jesse Brown VA Goals of Medications Use least number at lowest dose to get
Psychotropic Medications Archana Jhawar, PharmD, BCPP Clinical Faculty of UIC Pharmacy Practice Clinical Psychiatric Pharmacist Jesse Brown VA Goals of Medications Use least number at lowest dose to get
Pharmaceutical Interventions. Collaborative Model of Mental Health Care for Older Iowans Des Moines May 18, 2007
 Pharmaceutical Interventions Collaborative Model of Mental Health Care for Older Iowans Des Moines May 18, 2007 Outline Overview Overview of initial workup and decisions in elderly depressed individual
Pharmaceutical Interventions Collaborative Model of Mental Health Care for Older Iowans Des Moines May 18, 2007 Outline Overview Overview of initial workup and decisions in elderly depressed individual
Tai Chi for Prevention of Falls in Older Adults. Yolanda Suarez, DO Geriatrics Fellow University of Reno School of Medicine June 20, 2018
 Tai Chi for Prevention of Falls in Older Adults Yolanda Suarez, DO Geriatrics Fellow University of Reno School of Medicine June 20, 2018 Through this interactive presentation you will learn to Identify
Tai Chi for Prevention of Falls in Older Adults Yolanda Suarez, DO Geriatrics Fellow University of Reno School of Medicine June 20, 2018 Through this interactive presentation you will learn to Identify
You May Be at Risk. You are currently taking a sedative-hypnotic drug. Please Bring This Information With You To Your Next Medical Appointment
 You are currently taking a sedative-hypnotic drug Alprazolam Chlordiazepoxide Clonazepam Diazepam Estazolam Flurazepam Lorazepam Oxazepam Temazepam Triazolam Eszopiclone Zaleplon Zolpidem Please Bring
You are currently taking a sedative-hypnotic drug Alprazolam Chlordiazepoxide Clonazepam Diazepam Estazolam Flurazepam Lorazepam Oxazepam Temazepam Triazolam Eszopiclone Zaleplon Zolpidem Please Bring
Managing Insomnia Disorder A Review of the Research for Adults
 Managing Insomnia Disorder A Review of the Research for Adults e Is This Information Right for Me? This information is right for you if: Your health care professional said you have insomnia disorder (said
Managing Insomnia Disorder A Review of the Research for Adults e Is This Information Right for Me? This information is right for you if: Your health care professional said you have insomnia disorder (said
Cell Phones and Pagers
 FALLS Cell Phones and Pagers Please turn your cell phones off or turn the ringer down during the session. If you must answer a call, please be considerate of other attendees and leave the room before you
FALLS Cell Phones and Pagers Please turn your cell phones off or turn the ringer down during the session. If you must answer a call, please be considerate of other attendees and leave the room before you
START, STOPP, Beers Oh My! Navigating the World of Geriatric Pharmacy
 START, STOPP, Beers Oh My! Navigating the World of Geriatric Pharmacy Jessica DiLeo, PharmD Kate Murphy, PharmD OBJECTIVES Identify pharmacodynamic and pharmacokinetic parameters that may influence treatment
START, STOPP, Beers Oh My! Navigating the World of Geriatric Pharmacy Jessica DiLeo, PharmD Kate Murphy, PharmD OBJECTIVES Identify pharmacodynamic and pharmacokinetic parameters that may influence treatment
Review of Psychotrophic Medications. (An approved North Carolina Division of Health Services Regulation Continuing Education Course)
") Review of Psychotrophic Medications (An approved North Carolina Division of Health Services Regulation Continuing Education Course) Common Psychiatric Disorders *Schizophrenia *Depression *Bipolar Disorder
Review of Psychotrophic Medications (An approved North Carolina Division of Health Services Regulation Continuing Education Course) Common Psychiatric Disorders *Schizophrenia *Depression *Bipolar Disorder
9/6/2017 DEPRESCRIBING SAFELY IN THE OLDER ADULT. What is Deprescribing??? What leads to overmedication?
 DEPRESCRIBING SAFELY IN THE OLDER ADULT Pennsylvania Coalition of Nurse Practitioners State Conference November 4, 2017 Cynthia Blevins, DNP CRNP General Internal Medicine of Lancaster What is Deprescribing???
DEPRESCRIBING SAFELY IN THE OLDER ADULT Pennsylvania Coalition of Nurse Practitioners State Conference November 4, 2017 Cynthia Blevins, DNP CRNP General Internal Medicine of Lancaster What is Deprescribing???
What are you trying to achieve? Falls Prevention, Assessment and Management Strategies. Falls can be classified into four main groups:
 What are you trying to achieve? Falls Prevention, Assessment and Management Strategies Dr Adam Darowski Community: Falls risk assessment: Falls risk is 50% per year in 80yr population and higher in those
What are you trying to achieve? Falls Prevention, Assessment and Management Strategies Dr Adam Darowski Community: Falls risk assessment: Falls risk is 50% per year in 80yr population and higher in those
Dementia and Fall Geriatric Interprofessional Training. Wael Hamade, MD, FAAFP
 Dementia and Fall Geriatric Interprofessional Training Wael Hamade, MD, FAAFP Prevalence of Dementia Age range 65-74 5% % affected 75-84 15-25% 85 and older 36-50% 5.4 Million American have AD Dementia
Dementia and Fall Geriatric Interprofessional Training Wael Hamade, MD, FAAFP Prevalence of Dementia Age range 65-74 5% % affected 75-84 15-25% 85 and older 36-50% 5.4 Million American have AD Dementia
Deconstructing Polypharmacy. Alan B. Douglass, M.D. Director
 Deconstructing Polypharmacy Alan B. Douglass, M.D. Director Recognize this patient? Mrs. Brown- 82 years young Active Medical Problems Hypertension Hyperlipidemia Type 2 Diabetes Peripheral edema Osteoarthritis
Deconstructing Polypharmacy Alan B. Douglass, M.D. Director Recognize this patient? Mrs. Brown- 82 years young Active Medical Problems Hypertension Hyperlipidemia Type 2 Diabetes Peripheral edema Osteoarthritis
Maximizing Medication Safety UNIVERSITY OF HAWAII AUGUST 31, 2016
 Maximizing Medication Safety UNIVERSITY OF HAWAII AUGUST 31, 2016 Adverse Drug Events (ADE s) RISK FACTORS FOR Adverse Drug Events (ADEs) 6 or more concurrent chronic conditions 12 or more doses of drugs/day
Maximizing Medication Safety UNIVERSITY OF HAWAII AUGUST 31, 2016 Adverse Drug Events (ADE s) RISK FACTORS FOR Adverse Drug Events (ADEs) 6 or more concurrent chronic conditions 12 or more doses of drugs/day
MANAGEMENT OF VISCERAL PAIN
 MANAGEMENT OF VISCERAL PAIN William D. Chey, MD, FACG Professor of Medicine University of Michigan 52 year old female with abdominal pain 5 year history of persistent right sided burning/sharp abdominal
MANAGEMENT OF VISCERAL PAIN William D. Chey, MD, FACG Professor of Medicine University of Michigan 52 year old female with abdominal pain 5 year history of persistent right sided burning/sharp abdominal
Behavioral Issues in Dementia. March 27, 2014 Dylan Wint, M.D.
 Behavioral Issues in Dementia March 27, 2014 Dylan Wint, M.D. OVERVIEW Key points Depression Definitions and detection Treatment Psychosis Definitions and detection Treatment Agitation SOME KEY POINTS
Behavioral Issues in Dementia March 27, 2014 Dylan Wint, M.D. OVERVIEW Key points Depression Definitions and detection Treatment Psychosis Definitions and detection Treatment Agitation SOME KEY POINTS
Making Sense of the Long Term Care Mega Rule: Unnecessary Drugs & Psychotropics. Session Objectives. January 2018
 Making Sense of the Long Term Care Mega Rule: Unnecessary Drugs & Psychotropics Bridget McCrate Protus, PharmD, MLIS, BCGP, CDP Director of Drug Information Optum Hospice Pharmacy Services Session Objectives
Making Sense of the Long Term Care Mega Rule: Unnecessary Drugs & Psychotropics Bridget McCrate Protus, PharmD, MLIS, BCGP, CDP Director of Drug Information Optum Hospice Pharmacy Services Session Objectives
Managing falls in the elderly: real world approach DR PRISCILLA NG
 Managing falls in the elderly: real world approach DR PRISCILLA NG A fall is defined as an event which results in a person coming to rest inadvertently on the ground or floor or other lower level. FALL:
Managing falls in the elderly: real world approach DR PRISCILLA NG A fall is defined as an event which results in a person coming to rest inadvertently on the ground or floor or other lower level. FALL:
FALLS PREVENTION. S H I R L E Y H U A N G, M S c, M D, F R C P C
 FALLS PREVENTION S H I R L E Y H U A N G, M S c, M D, F R C P C S T A F F G E R I A T R I C I A N T H E O T T A W A H O S P I T A L B R U Y E R E C O N T I N U I N G C A R E W I N C H E S T E R D I S T
FALLS PREVENTION S H I R L E Y H U A N G, M S c, M D, F R C P C S T A F F G E R I A T R I C I A N T H E O T T A W A H O S P I T A L B R U Y E R E C O N T I N U I N G C A R E W I N C H E S T E R D I S T
Learning Objectives 2/4/2016. Patrick Leung, Pharm.D., BCPS, PhC. Patrick Leung, Pharm.D., BCPS, PhC Davena Norris, Pharm.D., BCPS, PhC 2/20/2016
 Patrick Leung, Pharm.D., BCPS, PhC Davena Norris, Pharm.D., BCPS, PhC 2/20/2016 Learning Objectives Identify age-related pharmacokinetic and pharmacodynamic changes in older adults. Utilization the START/STOPP
Patrick Leung, Pharm.D., BCPS, PhC Davena Norris, Pharm.D., BCPS, PhC 2/20/2016 Learning Objectives Identify age-related pharmacokinetic and pharmacodynamic changes in older adults. Utilization the START/STOPP
Safe Prescribing in Dementia
 Safe Prescribing in Dementia Dr Daniel Harwood Consultant Psychiatrist and Clinical Director, London Strategic Clinical Network Gurdeep Kaur Major Rapid Access Team Senior Pharmacist, Camden CNWL NHS Trust
Safe Prescribing in Dementia Dr Daniel Harwood Consultant Psychiatrist and Clinical Director, London Strategic Clinical Network Gurdeep Kaur Major Rapid Access Team Senior Pharmacist, Camden CNWL NHS Trust
COMMONLY PRESCRIBED PSYCHOTROPIC MEDICATIONS NAME Generic (Trade) DOSAGE KEY CLINICAL INFORMATION Antidepressant Medications*
 DOSAGE KEY CLINICAL INFORMATION Antidepressant Medications*") COMMONLY PRESCRIBED PSYCHOTROPIC MEDICATIONS NAME Generic (Trade) DOSAGE KEY CLINICAL INFORMATION Antidepressant Medications* Bupropion (Wellbutrin) Start: IR-100 mg bid X 4d then to 100 mg tid; SR-150
COMMONLY PRESCRIBED PSYCHOTROPIC MEDICATIONS NAME Generic (Trade) DOSAGE KEY CLINICAL INFORMATION Antidepressant Medications* Bupropion (Wellbutrin) Start: IR-100 mg bid X 4d then to 100 mg tid; SR-150
Multifactorial risk assessments and evidence-based interventions to address falls in primary care. Objectives. Importance
 Multifactorial risk assessments and evidence-based interventions to address falls in primary care Sarah Ross, DO, MS Assistant Professor Internal Medicine, Geriatrics Nicoleta Bugnariu, PT, PhD Associate
Multifactorial risk assessments and evidence-based interventions to address falls in primary care Sarah Ross, DO, MS Assistant Professor Internal Medicine, Geriatrics Nicoleta Bugnariu, PT, PhD Associate
Sleep and Parkinson's Disease
 Parkinson s Disease Clinic and Research Center University of California, San Francisco 505 Parnassus Ave., Rm. 795-M, Box 0114 San Francisco, CA 94143-0114 (415) 476-9276 http://pdcenter.neurology.ucsf.edu
Parkinson s Disease Clinic and Research Center University of California, San Francisco 505 Parnassus Ave., Rm. 795-M, Box 0114 San Francisco, CA 94143-0114 (415) 476-9276 http://pdcenter.neurology.ucsf.edu
Letter from Home for Direct Care Providers Fall Risk Identification and Prevention
 Letter from Home for Direct Care Providers Fall Risk Identification and Prevention Each year, thousands of older adults will have a fall in their home. Falls are more common than strokes and can have just
Letter from Home for Direct Care Providers Fall Risk Identification and Prevention Each year, thousands of older adults will have a fall in their home. Falls are more common than strokes and can have just
Objectives. 0 Identify medicines which increase the risk of falls and secondary injury on the farm/ranch.
 Objectives 0 Identify medicines which increase the risk of falls and secondary injury on the farm/ranch. 0 Examine the impact of a medication assessment service on Missouri AgrAbility clients confidence
Objectives 0 Identify medicines which increase the risk of falls and secondary injury on the farm/ranch. 0 Examine the impact of a medication assessment service on Missouri AgrAbility clients confidence
Chitra Fernando, MD March 18, 2008
 Chitra Fernando, MD March 18, 2008 Definition Statistics Risk factors Why older adults are more prone to ADE Manifestations Inappropriate medications for older adults What can be done to minimize adverse
Chitra Fernando, MD March 18, 2008 Definition Statistics Risk factors Why older adults are more prone to ADE Manifestations Inappropriate medications for older adults What can be done to minimize adverse
Antidepressants: Prof. Riyadh Al_Azzawi F.R.C.Psych
 Antidepressants: Prof. Riyadh Al_Azzawi F.R.C.Psych A. Heterocyclic antidepressants: (tricyclic and tetracyclic ), e.g.amitryptaline,imipramine. B. Monoamine oxidase inhibitors(m.a.o.i), e.g.phenelzine.
Antidepressants: Prof. Riyadh Al_Azzawi F.R.C.Psych A. Heterocyclic antidepressants: (tricyclic and tetracyclic ), e.g.amitryptaline,imipramine. B. Monoamine oxidase inhibitors(m.a.o.i), e.g.phenelzine.
University of Hawaii Center on Aging
 University of Hawaii Center on Aging. Supported in part by a cooperative agreement No. 90AL0011-01-00 from the Administration on Aging, Administration for Community Living, U.S. Department of Health and
University of Hawaii Center on Aging. Supported in part by a cooperative agreement No. 90AL0011-01-00 from the Administration on Aging, Administration for Community Living, U.S. Department of Health and
2/12/2016. Drugs and Dementia in the Hospice Patient. Jim Joyner, Pharm.D., C.G.P. Director of Clinical Operations Outcome Resources
 Drugs and Dementia in the Hospice Patient Jim Joyner, Pharm.D., C.G.P. Director of Clinical Operations Outcome Resources 1 Drug Therapy: Targeted at Symptoms Cognitive: Impaired abstract thinking Impaired
Drugs and Dementia in the Hospice Patient Jim Joyner, Pharm.D., C.G.P. Director of Clinical Operations Outcome Resources 1 Drug Therapy: Targeted at Symptoms Cognitive: Impaired abstract thinking Impaired
Antidepressants and Sedatives. David G. Standaert, M.D., Ph.D. Massachusetts General Hospital Harvard Medical School
 Antidepressants and Sedatives David G. Standaert, M.D., Ph.D. Massachusetts General Hospital Harvard Medical School Depression A frequent problem, affecting up to 5% of the population Common presentations
Antidepressants and Sedatives David G. Standaert, M.D., Ph.D. Massachusetts General Hospital Harvard Medical School Depression A frequent problem, affecting up to 5% of the population Common presentations
A Geriatrician s Perspective on Successful Aging. Ariel Green, MD, MPH Assistant Professor of Medicine
 A Geriatrician s Perspective on Successful Aging Ariel Green, MD, MPH Assistant Professor of Medicine 1 Disclosures Johns Hopkins Clinical Research Scholars Program American College of Cardiology Foundation
A Geriatrician s Perspective on Successful Aging Ariel Green, MD, MPH Assistant Professor of Medicine 1 Disclosures Johns Hopkins Clinical Research Scholars Program American College of Cardiology Foundation
PROCEDURE REF NO SABP/EXECUTIVE BOARD/0017
 PROCEDURE REF NO SABP/EXECUTIVE BOARD/0017 NAME OF GUIDELINE REASON FOR GUIDELINE WHAT THE GUIDELINE WILL ACHIEVE? WHO NEEDS TO KNOW ABOUT IT? Medicines Guideline: Hypnotic Medication Compliance with NICE
PROCEDURE REF NO SABP/EXECUTIVE BOARD/0017 NAME OF GUIDELINE REASON FOR GUIDELINE WHAT THE GUIDELINE WILL ACHIEVE? WHO NEEDS TO KNOW ABOUT IT? Medicines Guideline: Hypnotic Medication Compliance with NICE
Insomnia. Learning Objectives. Disclosure 6/7/11. Research funding: NIH, Respironics, Embla Consulting: Elsevier
 Insomnia Teofilo Lee-Chiong MD Professor of Medicine National Jewish Health University of Colorado Denver School of Medicine Learning Objectives Learn about the causes of transient and chronic Learn how
Insomnia Teofilo Lee-Chiong MD Professor of Medicine National Jewish Health University of Colorado Denver School of Medicine Learning Objectives Learn about the causes of transient and chronic Learn how
Medicine Related Falls Risk Assessment Tool (MrFRAT) User Guide for Age Related Residential Care Facility Staff in Hawke s Bay
 User Guide for Age Related Residential Care Facility Staff in Hawke s Bay") Medicine Related Falls Risk Assessment Tool (MrFRAT) User Guide for Age Related Residential Care Facility Staff in Hawke s Bay (Revised edition November 2015) The Medicine Related Falls Risk Assessment
Medicine Related Falls Risk Assessment Tool (MrFRAT) User Guide for Age Related Residential Care Facility Staff in Hawke s Bay (Revised edition November 2015) The Medicine Related Falls Risk Assessment
Polypharmacy: Guidance for Prescribing in Frail Adults
 Polypharmacy: Guidance for Prescribing in Frail Adults Why is reviewing polypharmacy important? Medication is by far the most common form of medical intervention. Four out of five people aged over 75 years
Polypharmacy: Guidance for Prescribing in Frail Adults Why is reviewing polypharmacy important? Medication is by far the most common form of medical intervention. Four out of five people aged over 75 years
Treatments for Alzheimer s Disease A Quick Guide for Patients and Caregivers
 Treatments for Alzheimer s Disease A Quick Guide for Patients and Caregivers By Kelsey F. Lee, PharmD candidate 2011 Preceptor: Demetra Antimisiaris, PharmD University of Louisvlle Dept. Family Medicine
Treatments for Alzheimer s Disease A Quick Guide for Patients and Caregivers By Kelsey F. Lee, PharmD candidate 2011 Preceptor: Demetra Antimisiaris, PharmD University of Louisvlle Dept. Family Medicine
KEY MESSAGES. It is often under-recognised and 30-50% of MDD cases in primary care and medical settings are not detected.
 KEY MESSAGES Major depressive disorder (MDD) is a significant mental health problem that disrupts a person s mood and affects his psychosocial and occupational functioning. It is often under-recognised
KEY MESSAGES Major depressive disorder (MDD) is a significant mental health problem that disrupts a person s mood and affects his psychosocial and occupational functioning. It is often under-recognised
From MCI to Dementia DR YU- MIN LIN GERIATRICIAN AUG 2018
 From MCI to Dementia DR YU- MIN LIN GERIATRICIAN AUG 2018 Overview What is dementia? Common causes Normal cognitive decline Abnormal decline and mild cognitive impairment How do we manage dementia Can
From MCI to Dementia DR YU- MIN LIN GERIATRICIAN AUG 2018 Overview What is dementia? Common causes Normal cognitive decline Abnormal decline and mild cognitive impairment How do we manage dementia Can
How to Manage Insomnia with and without medications
 How to Manage Insomnia with and without medications Tatyana Gurvich, Pharm.D. USC School of Pharmacy UC Irvine SeniorHealth Center Insomnia: How common is it? 26-50% of adult population complain of insomnia
How to Manage Insomnia with and without medications Tatyana Gurvich, Pharm.D. USC School of Pharmacy UC Irvine SeniorHealth Center Insomnia: How common is it? 26-50% of adult population complain of insomnia
Dr Alex Bartle. Sleep Well Clinic
 Dr Alex Bartle Sleep Well Clinic Overview of Sleep Disorders Sleep: Why bother. Effect of Poor Quality or reduced Quantity of Sleep Common Sleep Disorders Management of Insomnia Medication vs CBTi Conclusion
Dr Alex Bartle Sleep Well Clinic Overview of Sleep Disorders Sleep: Why bother. Effect of Poor Quality or reduced Quantity of Sleep Common Sleep Disorders Management of Insomnia Medication vs CBTi Conclusion
Anxiolytic & Hypnotic Drugs. Asst Prof Dr Inam S Arif
 Anxiolytic & Hypnotic Drugs Asst Prof Dr Inam S Arif isamalhaj@yahoo.com Anxiolytic & Hpnotic Agents Anxiety: unpleasant state of tension, apprehension or uneasiness, characterised by, tachycardia, sweating,
Anxiolytic & Hypnotic Drugs Asst Prof Dr Inam S Arif isamalhaj@yahoo.com Anxiolytic & Hpnotic Agents Anxiety: unpleasant state of tension, apprehension or uneasiness, characterised by, tachycardia, sweating,
DISCLAIMER: ECHO Nevada emphasizes patient privacy and asks participants to not share ANY Protected Health Information during ECHO clinics.
 DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
Addressing the Multiple Causes and Lifestyle Impacts of Insomnia: A Guide for Patient Counseling
 Addressing the Multiple Causes and Lifestyle Impacts of Insomnia: A Guide for Patient Counseling Educational Objectives: At the completion of this knowledge-based activity, participants will be able to:
Addressing the Multiple Causes and Lifestyle Impacts of Insomnia: A Guide for Patient Counseling Educational Objectives: At the completion of this knowledge-based activity, participants will be able to:
Preventing Falls in Older Adults A Matter of Safety
 Preventing Falls in Older Adults A Matter of Safety Roger Tam, BSc. Pharm. Wal-Mart Clinical Designated Pharmacist Falls Prevention Pharmacist Specialist NCCHC-Pre/Post Test Educator Q.U.I.T Educator Overview
Preventing Falls in Older Adults A Matter of Safety Roger Tam, BSc. Pharm. Wal-Mart Clinical Designated Pharmacist Falls Prevention Pharmacist Specialist NCCHC-Pre/Post Test Educator Q.U.I.T Educator Overview
Any interventions, where RCTs in PD are not available, are not included in the tables.
 Tables Interventions where new studies have been published are indicated in bold italics. Changes in conclusions are indicated in italics and are highlighted in yellow. Any interventions, where RCTs in
Tables Interventions where new studies have been published are indicated in bold italics. Changes in conclusions are indicated in italics and are highlighted in yellow. Any interventions, where RCTs in
Antipsychotic Use in the Elderly
 Antipsychotic Use in the Elderly Presented by: Fatima M. Ali, PharmD, RPh, BCPS Clinical Consultant Pharmacist MediSystem Pharmacy, Kingston Originally Prepared by: Nicole Tisi BScPhm, RPh ACPR Disclosure
Antipsychotic Use in the Elderly Presented by: Fatima M. Ali, PharmD, RPh, BCPS Clinical Consultant Pharmacist MediSystem Pharmacy, Kingston Originally Prepared by: Nicole Tisi BScPhm, RPh ACPR Disclosure
Benzodiazepines: Comparative Effectiveness and Strategies for Discontinuation. Ann M. Hamer, PharmD, BCPP Rural Oregon Academic Detailing Project
 Benzodiazepines: Comparative Effectiveness and Strategies for Discontinuation Ann M. Hamer, PharmD, BCPP Rural Oregon Academic Detailing Project This project is funded through a grant from the Pew Charitable
Benzodiazepines: Comparative Effectiveness and Strategies for Discontinuation Ann M. Hamer, PharmD, BCPP Rural Oregon Academic Detailing Project This project is funded through a grant from the Pew Charitable
The Basics of Psychoactive/Psychotropic Medications Tina Sanchez, RN, SMQT New Mexico Department of Health Division of Health Improvement State
 The Basics of Psychoactive/Psychotropic Medications Tina Sanchez, RN, SMQT New Mexico Department of Health Division of Health Improvement State RAI/MDS Coordinator Objectives Upon completion of this training,
The Basics of Psychoactive/Psychotropic Medications Tina Sanchez, RN, SMQT New Mexico Department of Health Division of Health Improvement State RAI/MDS Coordinator Objectives Upon completion of this training,
Medicines save lives
 Optimizing Aging Collaborative Disclosures Too much of a good thing: No financial interests to disclose John Newman, MD, PhD Assistant Professor Division of Geriatrics, UCSF Kirby Lee, PharmD, MAS Associate
Optimizing Aging Collaborative Disclosures Too much of a good thing: No financial interests to disclose John Newman, MD, PhD Assistant Professor Division of Geriatrics, UCSF Kirby Lee, PharmD, MAS Associate
Pregnancy. General Principles of Prescribing in Pregnancy (The Maudsley, 12 th Edition)
") Pregnancy General Principles of Prescribing in Pregnancy (The Maudsley, 12 th Edition) In all women of child bearing potential Always discuss the possibility of pregnancy; half of all pregnancies are unplanned
Pregnancy General Principles of Prescribing in Pregnancy (The Maudsley, 12 th Edition) In all women of child bearing potential Always discuss the possibility of pregnancy; half of all pregnancies are unplanned
Geriatric Pharmacology. Kwi Bulow, M.D. Clinical Professor of Medicine Director, Academic Geriatric Resource Center
 Geriatric Pharmacology Kwi Bulow, M.D. Clinical Professor of Medicine Director, Academic Geriatric Resource Center Silver Tsunami 2010: 40 million (13%) 2030: 72 million (20%) Baby Boomers (1946-1964)
Geriatric Pharmacology Kwi Bulow, M.D. Clinical Professor of Medicine Director, Academic Geriatric Resource Center Silver Tsunami 2010: 40 million (13%) 2030: 72 million (20%) Baby Boomers (1946-1964)
Anxiolytic and Hypnotic drugs
 Anxiolytic and Hypnotic drugs Anxiolytic and Hypnotic drugs Anxiety is unpleasant state of tension and fear that seems to arise from unknown source. The symptoms of severe anxiety are similar to those
Anxiolytic and Hypnotic drugs Anxiolytic and Hypnotic drugs Anxiety is unpleasant state of tension and fear that seems to arise from unknown source. The symptoms of severe anxiety are similar to those
ENSURING EXCELLENCE IN PRESCRIBING FOR OLDER ADULTS
 ENSURING EXCELLENCE IN PRESCRIBING FOR OLDER ADULTS Philip J. Schneider, MS, FASHP The University of Arizona College of Pharmacy Learning Objectives: Describe the medication-use system and all interdependent
ENSURING EXCELLENCE IN PRESCRIBING FOR OLDER ADULTS Philip J. Schneider, MS, FASHP The University of Arizona College of Pharmacy Learning Objectives: Describe the medication-use system and all interdependent
Predicting which medication classes interfere with allergy skin testing
 Predicting which medication classes interfere with allergy skin testing Kunal M. Shah, M.D, 1 Matthew A. Rank, M.D., 1 Shoban A. Davé, M.D., 2 Corrine L. Oslie, R.N., 1 and Joseph H. Butterfield, M.D.
Predicting which medication classes interfere with allergy skin testing Kunal M. Shah, M.D, 1 Matthew A. Rank, M.D., 1 Shoban A. Davé, M.D., 2 Corrine L. Oslie, R.N., 1 and Joseph H. Butterfield, M.D.