SEP-1 CHALLENGING CASES WITH DR. TOWNSEND
|
|
|
- Cameron Hancock
- 5 years ago
- Views:
Transcription
1 UW MEDICINE PATIENTS ARE FIRST SEP-1 CHALLENGING CASES WITH DR. TOWNSEND AMADAE AREVALO RN, MSN, CCRN KATIE MEHRING RN, BSN, CCDS AMANDA SIGALA, RN, BSN, MPH, CPHQ JUNE 12, 2018
2 OBJECTIVES 1. Summarize the discussions with Dr. Townsend regarding challenging cases for SEP Recognize role of Clinical Documentation Specialists in improving documentation and efforts in insurance denials 3. Apply new and enhanced knowledge to their respective areas (abstraction, Sepsis committees & working groups, leadership) in regards to SEP-1 Specs Version 5.4 (discharge 2

3 DISCLOSURES WE DO NOT have any financial relationship with industry or commercial supporters to disclose. 3


 Level 1 Cardiac")
4 NORTHWEST HOSPITAL & MEDICAL CENTER Not-for-Profit Community Hospital 281 Licensed Beds 1775 Employees 679 Medical Staff, mostly independent Level 4 Trauma Designation Level 2 Special Care Nursery Level 1 Stroke Categorization (WA-DOH) Level 1 Cardiac Categorization (WA-DOH) 4




5 HARBORVIEW MEDICAL CENTER Academic Medical Center UW Medicine includes Northwest Hospital & Medical Center, Valley Medical Center, Harborview Medical Center, UW Medical Center, UW Neighborhood Clinics, UW Physicians, UW School of Medicine and Airlift Northwest 413 Licensed beds 5200 Employees Level 1 adult and pediatric trauma and burn center and regional referral center serving Washington, Wyoming,Alaska, Montana and Idaho. Emergency Medicine and Disaster Management Comprehensive Stroke Center Specialty Care including neurosciences, HIV/AIDS, psychiatric, substance abuse, eye care, vascular surgery, rehabilitation, sleep medicine and spine care 5

6 NORTHWEST HOSPITAL SEP SEP-1 Overall Compliance % Reasons for Failure % % 42% Failed Passed 6

7 HARBORVIEW MEDICAL CENTER SEP SEP-1 Overall Compliance % Reasons for Failure % % 48% Passed Failed
8 CRYSTALLOID FLUID ADMINISTRATION HMC Case Study #1 8
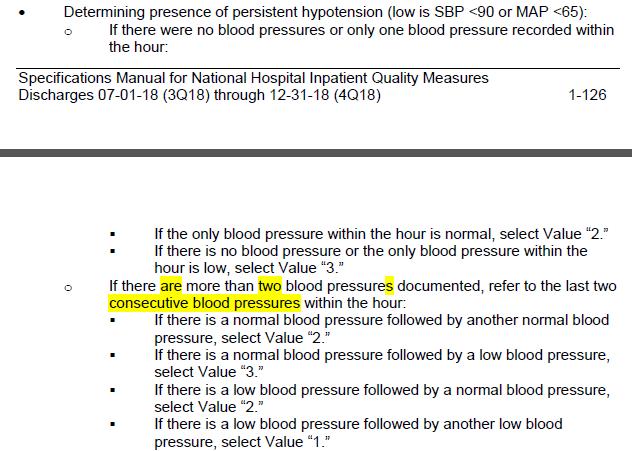
9 CMS V. 5.4 (DISCHARGE PERIOD 7/1/18 12/31/18) Crystalloid Fluids: For the presence of Initial Hypotension, only abstract crystalloid fluids that were started in the timeframe of 6 hrs. prior through 3 hrs. after the initial hypotension. A single order for the target volume initiated within 6 hrs. prior through 3 hrs. after initial hypotension is acceptable. If crystalloid fluids are initiated via multiple physician/apn/pa orders, only abstract crystalloid fluids initiated within 6 hrs. prior to 3 hrs. after. Initial Hypotension: Use the earliest date of the second hypotensive blood pressure documented within the time period of 6 hrs. prior to or within 6 hrs. following Severe Sepsis Presentation date and time 9
10 TIME FRAME FOR FLUID ADMINISTRATION 49F had acute apneic event & PEA arrest in the field while being evaluated by paramedics for SOB. Intubated in the field. 19:30 Arrived at ED, CPR ongoing. 19:34 Triage Vitals HR 154, BP 140/109 20:24 Initial lactate (13.3) 21:40 Time Zero in Admit Note: Septic shock, Highest suspicion would be pulmonary process, anticipate aspiration event in the setting of arrest. Ground glass opacities on imaging raise concern for atypical infection, viral infection. 21:51 WBC Initial Hypotension 22:30 SBP 83 02:00 SBP 80 10
11 TIME FRAME FOR FLUID ADMINISTRATION Fluid requirement ml (Pt. weight = 70 kg x 30 ml/kg = 2100) (within 6 hrs. prior & 3 hrs. after Initial 02:00, between 20:00 to 05:00) 18:58 in ambulance 500mL LR 22:36 in ED 500mL NS 23:34 in ED 100 ml diluent c/ abx. 02:30 in ICU 500 ml LR 04:55 in ICU 500mL LR 05:58 in ICU 1000 ml LR 11
12 MD REVIEW Received 1600 ml within appropriate time frame (20:00 to 05:00 ). Needed ml. Patient care improvement opportunity as the ICU faculty mention volume resuscitation for her shock, but the patient only got a small portion within appropriate time frame. Fails measure in both V. 5.3 and 5.4 Avoid this fallout by ordering fluid as one order instead of multiple orders. 12
13 ROLE OF THE CLINICAL DOCUMENTATION SPECIALIST RN (CDS) Concurrently reviews the medical record to ensure accurate reporting of medical diagnoses. Notifies the QI sepsis abstractor of current sepsis admissions. Concurrently requests documentation clarification and/or clinical validation as needed. 13
14 CDS REVIEW Consider the diagnostic criteria used for the diagnosis of Septic Shock Consider the entire clinical picture Potentially conflicting documentation Seek clarification 14
15 CRYSTALLOID FLUID ADMINISTRATION NWH Case Study #1 15
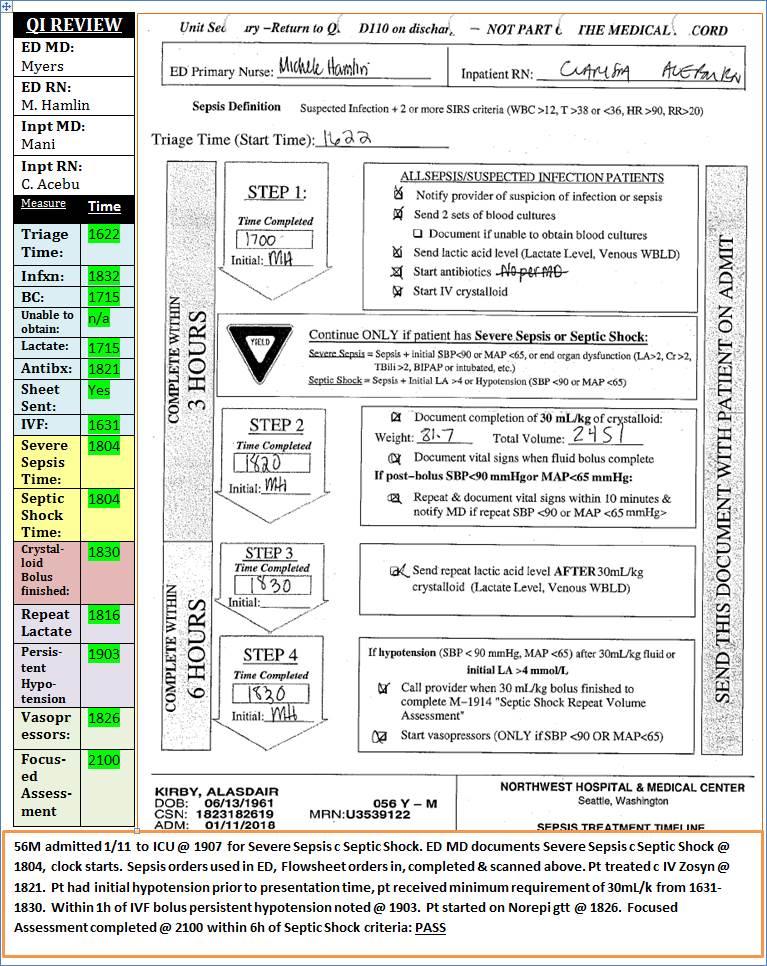
16 BP POST BOLUS ADMINISTRATION 56M admitted for Severe Sepsis with Septic Shock; documentation by ED 1804 Weight: 81.7kg 30mL/kg= IVF orders: 1. IV LR 250mL Administered IV NS 1000mL & again
17 VITALS Systolic Diastolic MAP
18 18
19 19
20 Calculated 10% of 30mL/k required volume = 2206mL Calculated the rate of which the volume infused as well as when 2206mL would have finished infusing
21 VITALS Systolic Diastolic MAP

22 QUESTIONS? 22
23 SEVERE SEPSIS PRESENTATION Documentation Challenges 23
24 IMMEDIATE FEEDBACK & CONCURRENT REVIEWS 1. Cases from Clinical Documentation Specialists (CDS) 2. Manual Abstraction 3. Immediate Feedback sent to Providers 24
25 25
26 SEVERE SEPSIS DOCUMENTATION NWH Case Study #2 26
27 SEVERE SEPSIS DOCUMENTATION 100F in ED dx & treated for UTI + Influenza on 2/5 H&P states pt did not met sepsis criteria - VS normal. First documentation of Severe Sepsis was on 2/ in progress note. No initial lactate within 6h of presentation. 27

28 28
29 29
30 CRITICAL CARE MD REVIEW: So far as I can tell, this is in the category of "chart hygiene" failure. Docs should be encouraged to document sepsis after admission if they deem something to be "missed sepsis" based on the data for purposes of improving care, but should be discouraged from using the "s" word in any other circumstance in subsequent follow up notes (unless new sepsis develops). Similarly, coders should not leave notes eliciting sepsis documentation for same reason. Can't tell which was the case here. 30
31 INPATIENT MD REVIEW Agree with [Critical Care MD above] that "chart hygiene" is important. I think the MD who picked this patient up felt that patient did meet severe sepsis on admission given WBC of 15 and lactic acid of 2.6 and clear source of infection. However, all vitals signs were stable. 31
32 CDS REVIEW This chart was not concurrently reviewed by a CDS. There was not a coder query on this chart Clinical Validation Needed Provide vital signs, lab values, documentation for provider review Clinical Validation Clarification: Please provide documentation of how/why this clinical presentation is out of proportion to what would be expected for a localized infection alone 32
33 SEVERE SEPSIS DOCUMENTATION HMC Case Study #2 33
34 SEVERE SEPSIS PRESENT 50M with 1 day of acute onset LUQ abdominal pain which started abruptly this morning. 18:55 Triage Vitals HR 120, RR 24, BP 140/74 19:27 Initial Lactate (3.0) 19:27 WBC :40 ED "Intra-abdominal free air, concern for bowel perforation, Acute CHF 20:40 Met Severe Sepsis Criteria No BC obtained, went urgently to OR for ex lap & got abx. in OR. Hypotensive in OR, but vitals in OR should not be used per CMS. 34


35 SEVERE SEPSIS PRESENT V. 5.4 SPECS 35

36 ED 20:40: DOCUMENTATION OF SUSPECTED INFECTION 36

37 SEVERE SEPSIS PRESENT V

38 ADMIT NOTE 01:35:?NEGATION OF SUSPECTED INFECTION 38
39 MD REVIEW The perforated ulcer is a source for infection. After repair, the clinician felt that continued instability was due to heart failure, but the initial concern for infection was accurate. 39
40 CDS REVIEW Complicated clinical case Possible potential for documentation clarification of appropriate diagnosis at time of presentation vs. postoperatively. Reminder of necessity for providers to understand the role of the CDS and the background of why documentation clarification is being requested 40

41 QUESTIONS? 41

42 42






43 Amadae Arevalo Catherine Mehring nwhsea.org Phone URL Amanda Sigala Sean Townsend Phone URL
Core Measures SEPSIS UPDATES
 Patricia Walker, RN-BC, BSN Evidence Based Practice Manager Quality Management Services UCLA Health System, Ronald Reagan Medical Center Core Measures SEPSIS UPDATES Severe Sepsis and Septic Shock Based
Patricia Walker, RN-BC, BSN Evidence Based Practice Manager Quality Management Services UCLA Health System, Ronald Reagan Medical Center Core Measures SEPSIS UPDATES Severe Sepsis and Septic Shock Based
Sepsis Early Recognition and Management. Therese Hughes, PhD, MPA, RN
 Sepsis Early Recognition and Management Therese Hughes, PhD, MPA, RN 1 Sepsis a Deadly Progression Affects millions around the world each year, killing one in four Contributes to approximately 50% of all
Sepsis Early Recognition and Management Therese Hughes, PhD, MPA, RN 1 Sepsis a Deadly Progression Affects millions around the world each year, killing one in four Contributes to approximately 50% of all
Inpatient Quality Reporting Program
 SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock Part III: Measure updates and Abstraction Guidance Questions and Answers Moderator: Candace Jackson, RN Inpatient Quality Reporting (IQR) Program
SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock Part III: Measure updates and Abstraction Guidance Questions and Answers Moderator: Candace Jackson, RN Inpatient Quality Reporting (IQR) Program
Inpatient Quality Reporting (IQR) Program
 Program") Hypotension Inpatient Quality Reporting (IQR) Program SEP-1 Early Management Bundle, Severe Sepsis/ Septic Shock: v5.1 Measure Updates Questions and Answers Moderator: Candace Jackson, RN Project Lead,
Hypotension Inpatient Quality Reporting (IQR) Program SEP-1 Early Management Bundle, Severe Sepsis/ Septic Shock: v5.1 Measure Updates Questions and Answers Moderator: Candace Jackson, RN Project Lead,
Inpatient Quality Reporting Program
 SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock Part II Questions and Answers Moderator: Candace Jackson, RN Inpatient Quality Reporting (IQR) Program Lead Hospital Inpatient Value, Incentives,
SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock Part II Questions and Answers Moderator: Candace Jackson, RN Inpatient Quality Reporting (IQR) Program Lead Hospital Inpatient Value, Incentives,
Inpatient Quality Reporting (IQR) Program
 Program") The Clinician Perspective on Sepsis Care: Early Management Bundle for Severe Sepsis/Septic Shock Questions & Answers Moderator Candace Jackson, RN Project Lead, Hospital Inpatient Quality Reporting (IQR)
The Clinician Perspective on Sepsis Care: Early Management Bundle for Severe Sepsis/Septic Shock Questions & Answers Moderator Candace Jackson, RN Project Lead, Hospital Inpatient Quality Reporting (IQR)
NYSDOH Sepsis Q&A Session from February 2018 Data Abstraction Meetings Table of Content
 NYSDOH Sepsis Q&A Session from February 2018 Data Abstraction Meetings Table of Content Adherence variables Q: within 3 hours of the start datetime. How can we document that monotherapy was started before
NYSDOH Sepsis Q&A Session from February 2018 Data Abstraction Meetings Table of Content Adherence variables Q: within 3 hours of the start datetime. How can we document that monotherapy was started before
Sepsis 3 & Early Identification. Disclosures. Objectives 9/19/2016. David Carlbom, MD Medical Director, HMC Sepsis Program
 Sepsis 3 & Early Identification David Carlbom, MD Medical Director, HMC Sepsis Program Disclosures I have no relevant financial relationships with a commercial interest and will not discuss off-label use
Sepsis 3 & Early Identification David Carlbom, MD Medical Director, HMC Sepsis Program Disclosures I have no relevant financial relationships with a commercial interest and will not discuss off-label use
Hospital Inpatient Quality Reporting (IQR) Program
 Program") SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock: v5.4 Measure Updates Presentation Transcript Speakers Noel Albritton, RN, BS Lead Solutions Specialist Hospital Inpatient and Outpatient Process
SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock: v5.4 Measure Updates Presentation Transcript Speakers Noel Albritton, RN, BS Lead Solutions Specialist Hospital Inpatient and Outpatient Process
SEPSIS: IT ALL BEGINS WITH INFECTION. Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft.
 SEPSIS: IT ALL BEGINS WITH INFECTION Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft. Worth 1 2 3 OBJECTIVES Review the new Sepsis 3 definitions of sepsis
SEPSIS: IT ALL BEGINS WITH INFECTION Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft. Worth 1 2 3 OBJECTIVES Review the new Sepsis 3 definitions of sepsis
Troubleshooting Audio
 Welcome! Audio for this event is available via ReadyTalk Internet Streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines
Welcome! Audio for this event is available via ReadyTalk Internet Streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines
IDENTIFYING SEPSIS IN THE PREHOSPITAL SETTING
 IDENTIFYING SEPSIS IN THE PREHOSPITAL SETTING Christopher Hunter, MD, PhD, FACEP Director, Health Services Department Associate Medical Director, Orange County EMS System Medical Director, Orlando Health
IDENTIFYING SEPSIS IN THE PREHOSPITAL SETTING Christopher Hunter, MD, PhD, FACEP Director, Health Services Department Associate Medical Director, Orange County EMS System Medical Director, Orlando Health
Hospital Inpatient Quality Reporting (IQR) Program
 Program") SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock: v5.5a Measure FAQs Presentation Transcript Noel Albritton, MSN, RN Lead Solutions Specialist, Hospital Inpatient and Outpatient Process and Structural
SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock: v5.5a Measure FAQs Presentation Transcript Noel Albritton, MSN, RN Lead Solutions Specialist, Hospital Inpatient and Outpatient Process and Structural
Rapid Response Teams. January 17, Safe Table Webinar
 Rapid Response Teams January 17, 2017 Safe Table Webinar Christin Gordanier, MSN, RN, Inpatient Nursing Director at Virginia Mason Medical Center in Seattle, Washington. Alice Ferguson, BSN, RN, Project
Rapid Response Teams January 17, 2017 Safe Table Webinar Christin Gordanier, MSN, RN, Inpatient Nursing Director at Virginia Mason Medical Center in Seattle, Washington. Alice Ferguson, BSN, RN, Project
Staging Sepsis for the Emergency Department: Physician
 Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
SEPSIS: GETTING STARTED
 SEPSIS: GETTING STARTED Ohio Sepsis Initiative July 15, 2015 SEPSIS INCIDENCE Definition: the number of severe sepsis or septic shock encounters using the following ICD-9 codes (995.91 Sepsis, 995.92 severe
SEPSIS: GETTING STARTED Ohio Sepsis Initiative July 15, 2015 SEPSIS INCIDENCE Definition: the number of severe sepsis or septic shock encounters using the following ICD-9 codes (995.91 Sepsis, 995.92 severe
Sepsis Bundle Project (SEP) Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: April 2015 Most recent Revision: December 2018
 Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: April 2015 Most recent Revision: December 2018") Sepsis Bundle Project (SEP) Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: April 2015 Most recent Revision: December 2018 Objectives 1. To identify the symptom of severe sepsis and septic shock syndrome.
Sepsis Bundle Project (SEP) Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: April 2015 Most recent Revision: December 2018 Objectives 1. To identify the symptom of severe sepsis and septic shock syndrome.
Hospital Inpatient Quality Reporting (IQR) Program
 Program") SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock: v5.3a Measure Updates Questions and Answers Speaker Noel Albritton, RN, BS Lead Solutions Specialist Hospital Inpatient and Outpatient Process
SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock: v5.3a Measure Updates Questions and Answers Speaker Noel Albritton, RN, BS Lead Solutions Specialist Hospital Inpatient and Outpatient Process
Wait, is this sepsis?
 Wait, is this sepsis? Reconciling Disparate Sepsis Definitions LAURA QUINNAN, M.D. NWH SEPSIS COMMITTEE CO-CHAIR, CHIEF OF MEDICINE AND MEDICAL DIRECTOR OF HOSPITALIST TEAM Goals Describe Sepsis-3 definitions
Wait, is this sepsis? Reconciling Disparate Sepsis Definitions LAURA QUINNAN, M.D. NWH SEPSIS COMMITTEE CO-CHAIR, CHIEF OF MEDICINE AND MEDICAL DIRECTOR OF HOSPITALIST TEAM Goals Describe Sepsis-3 definitions
2016 Sepsis Update: Pearls, Pitfalls, and Core Measure Quicksand
 2016 Sepsis Update: Pearls, Pitfalls, and Core Measure Quicksand Jack Perkins, MD FACEP, FAAEM, FACP Assistant Professor of Emergency and Internal Medicine Virginia Tech Carilion School of Medicine Why
2016 Sepsis Update: Pearls, Pitfalls, and Core Measure Quicksand Jack Perkins, MD FACEP, FAAEM, FACP Assistant Professor of Emergency and Internal Medicine Virginia Tech Carilion School of Medicine Why
Applicable to. Team Members Performing MD House Staff APRN/PA RN LPN
 Protocol: Adult Burn Fluid Resuscitation Category Clinical Practice Protocol Number Approval Date vember 1, 2016 Due for review vember 1, 2018 Applicable to VUH Children s DOT VMG Off-site locations VMG
Protocol: Adult Burn Fluid Resuscitation Category Clinical Practice Protocol Number Approval Date vember 1, 2016 Due for review vember 1, 2018 Applicable to VUH Children s DOT VMG Off-site locations VMG
Sepsis Care and the New Core Measures. Daniel S. Hagg, MD January 15, 2016
 Sepsis Care and the New Core Measures Daniel S. Hagg, MD January 15, 2016 Outline What is sepsis? A brief history of sepsis care How should we take care of septic patients now? Core measures What strategies
Sepsis Care and the New Core Measures Daniel S. Hagg, MD January 15, 2016 Outline What is sepsis? A brief history of sepsis care How should we take care of septic patients now? Core measures What strategies
John Park, MD Assistant Professor of Medicine
 John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
SUCCESS IN SEPSIS MORTALITY REDUCTION. Maryanne Whitney RN MSN CNS Improvement Advisor, Cynosure Health HRET HEN AK Webinar
 SUCCESS IN SEPSIS MORTALITY REDUCTION Maryanne Whitney RN MSN CNS Improvement Advisor, Cynosure Health HRET HEN AK Webinar Got Sepsis? Now What?- Alerts & Bundles Maryanne Whitney RN, MS, CNS Improvement
SUCCESS IN SEPSIS MORTALITY REDUCTION Maryanne Whitney RN MSN CNS Improvement Advisor, Cynosure Health HRET HEN AK Webinar Got Sepsis? Now What?- Alerts & Bundles Maryanne Whitney RN, MS, CNS Improvement
Sepsis Story At Intermountain Healthcare Intensive Medicine Clinical Program
 Sepsis Story At Intermountain Healthcare 2004-2012 Intensive Medicine Clinical Program The International Surviving Sepsis Campaign Was Organized In 2002 During The ESICM International Meeting In Barcelona,
Sepsis Story At Intermountain Healthcare 2004-2012 Intensive Medicine Clinical Program The International Surviving Sepsis Campaign Was Organized In 2002 During The ESICM International Meeting In Barcelona,
Cambia Palliative Care Metrics: Where are we and where are we going?
 Cambia Palliative Care Metrics: Where are we and where are we going? J. Randall Curtis, MD, MPH Director, Cambia Palliative Care Center of Excellence www.uwpalliativecarecenter.com Overview of System-Wide
Cambia Palliative Care Metrics: Where are we and where are we going? J. Randall Curtis, MD, MPH Director, Cambia Palliative Care Center of Excellence www.uwpalliativecarecenter.com Overview of System-Wide
Sepsis Update: Focus on Early Recognition and Intervention. Disclosures
 Sepsis Update: Focus on Early Recognition and Intervention Jessie Roske, MD October 2017 Disclosures I have no actual or potential conflict of interest in relation to this program/presentation. I will
Sepsis Update: Focus on Early Recognition and Intervention Jessie Roske, MD October 2017 Disclosures I have no actual or potential conflict of interest in relation to this program/presentation. I will
Objectives. Epidemiology of Sepsis. Review Guidelines for Resuscitation. Tx: EGDT, timing/choice of abx, activated
 Update on Surviving Sepsis 2008 Objectives Epidemiology of Sepsis Definition of Sepsis and Septic Shock Review Guidelines for Resuscitation Dx: Lactate, t cultures, SVO2 Tx: EGDT, timing/choice of abx,
Update on Surviving Sepsis 2008 Objectives Epidemiology of Sepsis Definition of Sepsis and Septic Shock Review Guidelines for Resuscitation Dx: Lactate, t cultures, SVO2 Tx: EGDT, timing/choice of abx,
MBSAQIP Complex Clinical Scenarios & Variable Review
 MBSAQIP Complex Clinical Scenarios & Variable Review Disclosure The following planners, speakers, moderators, and/or panelists of the CME/CEU activity have no relevant financial relationships with commercial
MBSAQIP Complex Clinical Scenarios & Variable Review Disclosure The following planners, speakers, moderators, and/or panelists of the CME/CEU activity have no relevant financial relationships with commercial
Sepsis care and the new core measures
 Sepsis care and the new core measures Daniel S. Hagg, MD January 15, 2016 Outline What is sepsis? A brief history of sepsis care How should we take care of septic patients now? Core measures What strategies
Sepsis care and the new core measures Daniel S. Hagg, MD January 15, 2016 Outline What is sepsis? A brief history of sepsis care How should we take care of septic patients now? Core measures What strategies
Troubleshooting Audio
 Welcome! Audio for this event is available via ReadyTalk Internet Streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines
Welcome! Audio for this event is available via ReadyTalk Internet Streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines
Physician's Core Measure Pocket Guide AMI
 Physician's Core Measure Pocket Guide Core Measure Hotline: Ext. 4448 http://centegramedsource.com Indicator: AMI AMI VER. 9/2018 MUST document WHY no ASA unless there is documentation of contraindication
Physician's Core Measure Pocket Guide Core Measure Hotline: Ext. 4448 http://centegramedsource.com Indicator: AMI AMI VER. 9/2018 MUST document WHY no ASA unless there is documentation of contraindication
Early Goal Directed Therapy in 2015: What Did the Big Trials Teach us?
 Early Goal Directed Therapy in 2015: What Did the Big Trials Teach us? Mitchell M. Levy MD, FCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care Warren Alpert Medical School
Early Goal Directed Therapy in 2015: What Did the Big Trials Teach us? Mitchell M. Levy MD, FCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care Warren Alpert Medical School
McHenry Western Lake County EMS System CE for Paramedics, EMT-B and PHRN s Sepsis Patients. November/December 2017
 McHenry Western Lake County EMS System CE for Paramedics, EMT-B and PHRN s Sepsis Patients November/December 2017 This month we are going to take a look at the patient with Sepsis. Webster s defines septic
McHenry Western Lake County EMS System CE for Paramedics, EMT-B and PHRN s Sepsis Patients November/December 2017 This month we are going to take a look at the patient with Sepsis. Webster s defines septic
SEPSIS UPDATE WHY DO WE NEED A CORE MEASURE CHAD M. KOVALA DO, FACOEP, FACEP
 SEPSIS UPDATE WHY DO WE NEED A CORE MEASURE CHAD M. KOVALA DO, FACOEP, FACEP OBJECTIVES Arise, ProMISE, ProCESS Key points in sepsis management The CMS sepsis core measure COST OF SEPSIS CARE IN US Most
SEPSIS UPDATE WHY DO WE NEED A CORE MEASURE CHAD M. KOVALA DO, FACOEP, FACEP OBJECTIVES Arise, ProMISE, ProCESS Key points in sepsis management The CMS sepsis core measure COST OF SEPSIS CARE IN US Most
Pneumonia (PN) Frequently Asked Questions (FAQs) 2Q09 and 3Q09. Adult Smoking History. Another Suspected Source of Infection
 Frequently Asked Questions (FAQs) 2Q09 and 3Q09. Adult Smoking History. Another Suspected Source of Infection") Pneumonia (PN) Frequently Asked Questions (FAQs) Adult Smoking History The nurse wrote patient smoker for 15 years but does not indicate when or if he quit. The physician in the H&P wrote "The patient
Pneumonia (PN) Frequently Asked Questions (FAQs) Adult Smoking History The nurse wrote patient smoker for 15 years but does not indicate when or if he quit. The physician in the H&P wrote "The patient
Effect of post-intubation hypotension on outcomes in major trauma patients
 Effect of post-intubation hypotension on outcomes in major trauma patients Dr. Robert S. Green Professor, Emergency Medicine and Critical Care Dalhousie University Medical Director, Trauma Nova Scotia
Effect of post-intubation hypotension on outcomes in major trauma patients Dr. Robert S. Green Professor, Emergency Medicine and Critical Care Dalhousie University Medical Director, Trauma Nova Scotia
Critical Care Treatment Guidelines
 Critical Care Treatment Guidelines West Virginia Office of Emergency Medical Services CCT Guidelines CCT Guidelines TABLE OF CONTENTS Preface Acknowledgments Using the Guidelines INITIAL TREATMENT / UNIVERSAL
Critical Care Treatment Guidelines West Virginia Office of Emergency Medical Services CCT Guidelines CCT Guidelines TABLE OF CONTENTS Preface Acknowledgments Using the Guidelines INITIAL TREATMENT / UNIVERSAL
Increased female mortality after ICU admission and its potential causes.
 Increased female mortality after ICU admission and its potential causes. L. Mardini, J. Lipes, D. Jayaraman McGill University CCCF 2012 Oral presentations session October 29 th 2012 Increased female mortality
Increased female mortality after ICU admission and its potential causes. L. Mardini, J. Lipes, D. Jayaraman McGill University CCCF 2012 Oral presentations session October 29 th 2012 Increased female mortality
Harborview Medical Center. Presenting: Celeste Sather Clinic Practice Manager
 Harborview Medical Center Presenting: Celeste Sather Clinic Practice Manager Objectives Overview of Harborview Medical Center Division of Gerontology and Geriatric Medicine Long-Term Care Service Medicine
Harborview Medical Center Presenting: Celeste Sather Clinic Practice Manager Objectives Overview of Harborview Medical Center Division of Gerontology and Geriatric Medicine Long-Term Care Service Medicine
Presented by: Indah Dwi Pratiwi
 Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
Frank Sebat, MD - June 29, 2006
 Types of Shock Hypovolemic Shock Low blood volume decreasing cardiac output. AN INTEGRATED SYSTEM OF CARE FOR PATIENTS AT RISK SHOCK TEAM and RAPID RESPONSE TEAM Septic or Distributive Shock Decrease in
Types of Shock Hypovolemic Shock Low blood volume decreasing cardiac output. AN INTEGRATED SYSTEM OF CARE FOR PATIENTS AT RISK SHOCK TEAM and RAPID RESPONSE TEAM Septic or Distributive Shock Decrease in
Troubleshooting Audio
 Welcome Audio for this event is available via ReadyTalk Internet streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines
Welcome Audio for this event is available via ReadyTalk Internet streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines
AMI Talking Points. Provide appropriate treatment to Acute MI patients with these core measures:
 AMI Provide appropriate treatment to Acute MI patients with these core measures: Aspirin received within 24 hours of arrival or contraindication documented Primary PCI Received Within 90 Minutes of Hospital
AMI Provide appropriate treatment to Acute MI patients with these core measures: Aspirin received within 24 hours of arrival or contraindication documented Primary PCI Received Within 90 Minutes of Hospital
Saving Lives: Focusing on Severe Sepsis and Septic Shock
 Saving Lives: Focusing on Severe Sepsis and Septic Shock Deborah Cameron, RN, CPHQ Paul Pratt, RN Glenn Russ, RN Providence Little Company of Mary Medical Center San Pedro January 18, 2011 Objectives 1.
Saving Lives: Focusing on Severe Sepsis and Septic Shock Deborah Cameron, RN, CPHQ Paul Pratt, RN Glenn Russ, RN Providence Little Company of Mary Medical Center San Pedro January 18, 2011 Objectives 1.
Acute Coronary Syndrome (Code Patient) Anney Hall
 Anney Hall") Scenario Title Patient Name Acute Coronary Syndrome (Code Patient) Anney Hall Medical Record # DOB: Age: Level (year 2, last term of program) Course: Nur 212 Author, w/email Doris Jepson RN, BSN, CCRN
Scenario Title Patient Name Acute Coronary Syndrome (Code Patient) Anney Hall Medical Record # DOB: Age: Level (year 2, last term of program) Course: Nur 212 Author, w/email Doris Jepson RN, BSN, CCRN
National Emergency Laparotomy Audit. Help Box Text
 National Emergency Laparotomy Audit Help Box Text Version Control Version 1.1 06/12/13 1.2 13/12/13 1.3 20/12/13 1.4 20/01/14 1.5 30/01/14 1.6 13/03/14 1.7 07/04/14 1.8 01/12/14 1.9 05/05/15 1.10 02/07/15
National Emergency Laparotomy Audit Help Box Text Version Control Version 1.1 06/12/13 1.2 13/12/13 1.3 20/12/13 1.4 20/01/14 1.5 30/01/14 1.6 13/03/14 1.7 07/04/14 1.8 01/12/14 1.9 05/05/15 1.10 02/07/15
PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT
 PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT Melanie Sanchez, RN, MSNE, OCN, CCRN Clinical Nurse III City of Hope National Medical Center HOW THE EXPERTS TREAT HEMATOLOGIC MALIGNANCIES LAS VEGAS, NV
PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT Melanie Sanchez, RN, MSNE, OCN, CCRN Clinical Nurse III City of Hope National Medical Center HOW THE EXPERTS TREAT HEMATOLOGIC MALIGNANCIES LAS VEGAS, NV
Are Patients Hypoperfused in the ED? Rapid Perfusion Assessment in the Emergency Department
 Are Patients Hypoperfused in the ED? Rapid Perfusion Assessment in the Emergency Department R. Benjamin Saldaña DO, FACEP Associate Medical Director Methodist Emergency Care Center, Houston TX Disclosure
Are Patients Hypoperfused in the ED? Rapid Perfusion Assessment in the Emergency Department R. Benjamin Saldaña DO, FACEP Associate Medical Director Methodist Emergency Care Center, Houston TX Disclosure
PIN BENCHMARKING DATA DEFINITIONS DICTIONARY
 CORE MEASURES PIN BENCHMARKING DATA DEFINITIONS DICTIONARY 1 Total number of CAH acute care patient admissions. Report all CAH acute care only patient admissions for the quarter. Exclude CAH swing bed,
CORE MEASURES PIN BENCHMARKING DATA DEFINITIONS DICTIONARY 1 Total number of CAH acute care patient admissions. Report all CAH acute care only patient admissions for the quarter. Exclude CAH swing bed,
Who Moved My Sepsis? Understanding Sepsis Changes in Terry P. Clemmer, MD
 Who Moved My Sepsis? Understanding Sepsis Changes in 2015 Terry P. Clemmer, MD Danny R. Probst, MS, BSN, RN Data Manager, Intensive Medicine Clinical Program, Objectives: Identify the continued need to
Who Moved My Sepsis? Understanding Sepsis Changes in 2015 Terry P. Clemmer, MD Danny R. Probst, MS, BSN, RN Data Manager, Intensive Medicine Clinical Program, Objectives: Identify the continued need to
Sepsis Awareness and Education
 Sepsis Awareness and Education Meets the updated New York State Department of Health (NYSDOH) requirements for Infection Control and Barrier Precautions coursework Element VII: Sepsis Awareness and Education
Sepsis Awareness and Education Meets the updated New York State Department of Health (NYSDOH) requirements for Infection Control and Barrier Precautions coursework Element VII: Sepsis Awareness and Education
Emergency Department Guideline. Anaphylaxis
 Emergency Department Guideline Inclusion criteria: 1. Acute onset of an illness (minutes to hours) with a AND (b OR c): a. Skin and/or mucosa (pruritus, flushing, hives, angioedema) b. Respiratory compromise
Emergency Department Guideline Inclusion criteria: 1. Acute onset of an illness (minutes to hours) with a AND (b OR c): a. Skin and/or mucosa (pruritus, flushing, hives, angioedema) b. Respiratory compromise
The syndrome formerly known as. Severe Sepsis. James Rooks MD. Coordinator of critical care education OU College of Medicine, Tulsa
 The syndrome formerly known as Severe Sepsis James Rooks MD Coordinator of critical care education OU College of Medicine, Tulsa Disclosures I have no actual or practical conflicts of interest in relation
The syndrome formerly known as Severe Sepsis James Rooks MD Coordinator of critical care education OU College of Medicine, Tulsa Disclosures I have no actual or practical conflicts of interest in relation
Sepsis Denials. Presented by James Donaher, RHIA, CDIP, CCS, CCS-P
 Sepsis Denials Presented by James Donaher, RHIA, CDIP, CCS, CCS-P Sepsis-1 2 From the first Sepsis Definition Conference in 1991 Defined sepsis as systemic response syndrome (SIRS) due to infection SIRS
Sepsis Denials Presented by James Donaher, RHIA, CDIP, CCS, CCS-P Sepsis-1 2 From the first Sepsis Definition Conference in 1991 Defined sepsis as systemic response syndrome (SIRS) due to infection SIRS
Transfusion Requirements and Management in Trauma RACHEL JACK
 Transfusion Requirements and Management in Trauma RACHEL JACK Overview Haemostatic resuscitation Massive Transfusion Protocol Overview of NBA research guidelines Haemostatic resuscitation Permissive hypotension
Transfusion Requirements and Management in Trauma RACHEL JACK Overview Haemostatic resuscitation Massive Transfusion Protocol Overview of NBA research guidelines Haemostatic resuscitation Permissive hypotension
Hospital Inpatient Quality Reporting (IQR) Program
 Program") SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock: v5.2a Commonly Asked Questions & v5.3 Measure Updates Presentation Transcript Moderator Candace Jackson, RN Project Lead Hospital Inpatient Quality
SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock: v5.2a Commonly Asked Questions & v5.3 Measure Updates Presentation Transcript Moderator Candace Jackson, RN Project Lead Hospital Inpatient Quality
No conflicts of interest
 Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF No conflicts of interest Major Points Most ICU patients start in ED Chain of critical care starting in field and
Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF No conflicts of interest Major Points Most ICU patients start in ED Chain of critical care starting in field and
Surviving Sepsis Campaign Guidelines 2012 & Update for David E. Tannehill, DO Critical Care Medicine Mercy Hospital St.
 Surviving Sepsis Campaign Guidelines 2012 & Update for 2015 David E. Tannehill, DO Critical Care Medicine Mercy Hospital St. Louis Be appropriately aggressive the longer one delays aggressive metabolic
Surviving Sepsis Campaign Guidelines 2012 & Update for 2015 David E. Tannehill, DO Critical Care Medicine Mercy Hospital St. Louis Be appropriately aggressive the longer one delays aggressive metabolic
Sepsis - A Year in Transition
 Sepsis - A Year in Transition Todd L. Allen, MD, FACEP Chair, Emergency Department Development Team; Assistant Quality Officer, Institute for Healthcare Leadership Russell R. Miller, III, MD, MPH, FCCM
Sepsis - A Year in Transition Todd L. Allen, MD, FACEP Chair, Emergency Department Development Team; Assistant Quality Officer, Institute for Healthcare Leadership Russell R. Miller, III, MD, MPH, FCCM
Sepsis Surveillance at a Rural Critical Access Hospital
 Sepsis Surveillance at a Rural Critical Access Hospital Pacific Northwest Sepsis Conference University of Washington, 3/21/2017 Jonathan Hibbs MD Kittitas Valley Hospital jhibbs@kvhealthcare.org Background
Sepsis Surveillance at a Rural Critical Access Hospital Pacific Northwest Sepsis Conference University of Washington, 3/21/2017 Jonathan Hibbs MD Kittitas Valley Hospital jhibbs@kvhealthcare.org Background
SURVIVING SEPSIS: Early Management Saves Lives
 SURVIVING SEPSIS: Early Management Saves Lives Pat Posa RN, BSN, MSA System Performance Improvement Leader St. Joseph Mercy Health System Ann Arbor, MI Patricia.posa@stjoeshealth.org Objectives a. Understand
SURVIVING SEPSIS: Early Management Saves Lives Pat Posa RN, BSN, MSA System Performance Improvement Leader St. Joseph Mercy Health System Ann Arbor, MI Patricia.posa@stjoeshealth.org Objectives a. Understand
FLUID MANAGEMENT AND BLOOD COMPONENT THERAPY
 Manual: Section: Protocol #: Approval Date: Effective Date: Revision Due Date: 10/2019 LifeLine Patient Care Protocols Adult/Pediatrics AP1-011 10/2018 10/2018 FLUID MANAGEMENT AND BLOOD COMPONENT THERAPY
Manual: Section: Protocol #: Approval Date: Effective Date: Revision Due Date: 10/2019 LifeLine Patient Care Protocols Adult/Pediatrics AP1-011 10/2018 10/2018 FLUID MANAGEMENT AND BLOOD COMPONENT THERAPY
Chris Fox, MD Professor and Interim Chair Department of Emergency
 Close Calls with the Executioner: Where POCUS Avoided Misdiagnosis Chris Fox, MD Professor and Interim Chair Department of Emergency Medicine En route with 22 year old female Asthma attack witnessed by
Close Calls with the Executioner: Where POCUS Avoided Misdiagnosis Chris Fox, MD Professor and Interim Chair Department of Emergency Medicine En route with 22 year old female Asthma attack witnessed by
Nurse Driven Fluid Optimization Using Dynamic Assessments
 Nurse Driven Fluid Optimization Using Dynamic Assessments 2016 1 WHAT WE BELIEVE We believe that clinicians make vital fluid and drug decisions every day with limited and inconclusive information Cheetah
Nurse Driven Fluid Optimization Using Dynamic Assessments 2016 1 WHAT WE BELIEVE We believe that clinicians make vital fluid and drug decisions every day with limited and inconclusive information Cheetah
Appendix. Supplementary figures and tables
 This appendix was part of the submitted manuscript and has been peer reviewed. It is posted as supplied by the authors. Appendix. Supplementary figures and tables Figure A1. Flowchart describing patient
This appendix was part of the submitted manuscript and has been peer reviewed. It is posted as supplied by the authors. Appendix. Supplementary figures and tables Figure A1. Flowchart describing patient
Pragmatic Sepsis Care For Providers: Aligning evidence, guidelines, mandates and policy to inform your daily practice.
 Sepsis: Acute Care Part 2 Pragmatic Sepsis Care For Providers: Aligning evidence, guidelines, mandates and policy to inform your daily practice. June 15, 2017 Webinar Month 103 For resource downloads go
Sepsis: Acute Care Part 2 Pragmatic Sepsis Care For Providers: Aligning evidence, guidelines, mandates and policy to inform your daily practice. June 15, 2017 Webinar Month 103 For resource downloads go
Troubleshooting Audio
 Welcome! Audio for this event is available via ReadyTalk Internet Streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines
Welcome! Audio for this event is available via ReadyTalk Internet Streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines
Should Roids Be the Rage in Septic Shock? Lauren Powell, MSN, RN, CCRN, AGACNP-BC CHI Baylor St. Luke s Medical Center, Houston, TX
 Should Roids Be the Rage in Septic Shock? Lauren Powell, MSN, RN, CCRN, AGACNP-BC CHI Baylor St. Luke s Medical Center, Houston, TX Learning Objectives 1. Review the mechanism of action for the use of
Should Roids Be the Rage in Septic Shock? Lauren Powell, MSN, RN, CCRN, AGACNP-BC CHI Baylor St. Luke s Medical Center, Houston, TX Learning Objectives 1. Review the mechanism of action for the use of
9/25/2017. Nothing to disclose
 Nothing to disclose Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Explain
Nothing to disclose Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Explain
Nothing to disclose 9/25/2017
 Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Nothing to disclose 1 Explain
Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Nothing to disclose 1 Explain
Sepsis in primary care. what is good care?
 Sepsis in primary care @SepsisUK what is good care? Emmanuel Nsutebu Consultant Infectious Disease Physician & Clinical lead for sepsis Tropical and Infectious Disease Unit Royal Liverpool Hospital Do
Sepsis in primary care @SepsisUK what is good care? Emmanuel Nsutebu Consultant Infectious Disease Physician & Clinical lead for sepsis Tropical and Infectious Disease Unit Royal Liverpool Hospital Do
Sepsis Update Allina Critical Care Conference February 28, 2018
 Sepsis Update Allina Critical Care Conference February 28, 2018 Sandy Fritzlar, MD Medical Director of the Allina Sepsis Program Emergency Care Consultants OBJECTIVES A brief HISTORY of Sepsis Understand
Sepsis Update Allina Critical Care Conference February 28, 2018 Sandy Fritzlar, MD Medical Director of the Allina Sepsis Program Emergency Care Consultants OBJECTIVES A brief HISTORY of Sepsis Understand
What the ED clinician needs to know about SEPSIS - 3. Anna Morgan Consultant EM Barts Health
 What the ED clinician needs to know about SEPSIS - 3 Anna Morgan Consultant EM Barts Health Aims: (1) To review the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3) (2)
What the ED clinician needs to know about SEPSIS - 3 Anna Morgan Consultant EM Barts Health Aims: (1) To review the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3) (2)
Canadian Stroke Best Practices Initial ED Evaluation of Acute Stroke and Transient Ischemic Attack (TIA) Order Set (Order Set 1)
 Order Set (Order Set 1)") Canadian Best Practice Recommendations for Stroke Care: All patients presenting to an emergency department with suspected stroke or transient ischemic attack must have an immediate clinical evaluation
Canadian Best Practice Recommendations for Stroke Care: All patients presenting to an emergency department with suspected stroke or transient ischemic attack must have an immediate clinical evaluation
Discussion of Complex Clinical Scenarios and Variable Review ACS NSQIP Clinical Support Team
 Discussion of Complex Clinical Scenarios and Variable Review CS NSQIP Clinical Support Team SCR Open Q& Calls The CS NSQIP Clinical Team is trialing Open format Q& calls for NSQIP SCRs Participation in
Discussion of Complex Clinical Scenarios and Variable Review CS NSQIP Clinical Support Team SCR Open Q& Calls The CS NSQIP Clinical Team is trialing Open format Q& calls for NSQIP SCRs Participation in
R2R: Severe sepsis/septic shock. Surat Tongyoo Critical care medicine Siriraj Hospital
 R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
SARASOTA MEMORIAL HOSPITAL NURSING DEPARTMENT POLICY
 PS1070 SARASOTA MEMORIAL HOSPITAL NURSING DEPARTMENT POLICY TITLE: ADMISSION/DISCHARGE CRITERIA: CARDIOVASCULAR INTENSIVE Job Title of Reviewer: Director, CVICU EFFECTIVE DATE: REVIEWED/REVISED DATE: POLICY
PS1070 SARASOTA MEMORIAL HOSPITAL NURSING DEPARTMENT POLICY TITLE: ADMISSION/DISCHARGE CRITERIA: CARDIOVASCULAR INTENSIVE Job Title of Reviewer: Director, CVICU EFFECTIVE DATE: REVIEWED/REVISED DATE: POLICY
Where Emergency Medicine Meets Critical Care: Next Level Resuscitation
 Where Emergency Medicine Meets Critical Care: Next Level Resuscitation Rob Green, BSc, MD, DABEM, FRCPC, FRCP(Edin) Professor, Dalhousie University Departments of Emergency Medicine,Critical Care Medicine
Where Emergency Medicine Meets Critical Care: Next Level Resuscitation Rob Green, BSc, MD, DABEM, FRCPC, FRCP(Edin) Professor, Dalhousie University Departments of Emergency Medicine,Critical Care Medicine
Understand the scope of sepsis morbidity and mortality Identify risk factors that predispose a patient to development of sepsis Define and know the
 Understand the scope of sepsis morbidity and mortality Identify risk factors that predispose a patient to development of sepsis Define and know the differences between sepsis, severe sepsis and septic
Understand the scope of sepsis morbidity and mortality Identify risk factors that predispose a patient to development of sepsis Define and know the differences between sepsis, severe sepsis and septic
Stroke in the Rural Setting: How You Can Make A Difference. Susie Fisher, RN, BSN Program Manager Providence Stroke Center Portland, OR
 Stroke in the Rural Setting: How You Can Make A Difference. Susie Fisher, RN, BSN Program Manager Providence Stroke Center Portland, OR Outline State Statistics The Oregon Problem Time & Treatments Steps
Stroke in the Rural Setting: How You Can Make A Difference. Susie Fisher, RN, BSN Program Manager Providence Stroke Center Portland, OR Outline State Statistics The Oregon Problem Time & Treatments Steps
Sepsis Update: Early Identification and Management
 Sepsis Update: Early Identification and Management Q&A From the Live Webinar Presenter: Tom Ahrens, RN, PhD, FAAN Live webinar: Thursday, May 09, 2013 The AACN Critical Care Webinar Series is not only
Sepsis Update: Early Identification and Management Q&A From the Live Webinar Presenter: Tom Ahrens, RN, PhD, FAAN Live webinar: Thursday, May 09, 2013 The AACN Critical Care Webinar Series is not only
SEPSIS: Seeing Through the. W. Graham Carlos MD, MSCR, ATSF, FACP
 SEPSIS: Seeing Through the W. Graham Carlos MD, MSCR, ATSF, FACP Objectives Forget everything you have known about sepsis Learn new things Objectives Define sepsis Explain why Early Goal Directed Therapy
SEPSIS: Seeing Through the W. Graham Carlos MD, MSCR, ATSF, FACP Objectives Forget everything you have known about sepsis Learn new things Objectives Define sepsis Explain why Early Goal Directed Therapy
Northwest Community EMS System August 2018 CE: Sepsis and Septic Shock Credit Questions
 Northwest Community EMS System August 2018 CE: Sepsis and Septic Shock Credit Questions Name: EMS Agency/hospital: EMSC/Educator reviewer: Date submitted: Credit awarded (date): Returned for revisions:
Northwest Community EMS System August 2018 CE: Sepsis and Septic Shock Credit Questions Name: EMS Agency/hospital: EMSC/Educator reviewer: Date submitted: Credit awarded (date): Returned for revisions:
DESIGNER RESUSCITATION: TITRATING TO TISSUE NEEDS
 DESIGNER RESUSCITATION: TITRATING TO TISSUE NEEDS R. Phillip Dellinger MD, MSc, MCCM Professor and Chair of Medicine Cooper Medical School of Rowan University Chief of Medicine Cooper University Hospital
DESIGNER RESUSCITATION: TITRATING TO TISSUE NEEDS R. Phillip Dellinger MD, MSc, MCCM Professor and Chair of Medicine Cooper Medical School of Rowan University Chief of Medicine Cooper University Hospital
Civilian Hospital Response to Mass Casualty Events The Israeli Experience
 Civilian Hospital Response to Mass Casualty Events The Israeli Experience William Schecter, MD Professor of Clinical Surgery University of California, San Francisco Chief of Surgery San Francisco General
Civilian Hospital Response to Mass Casualty Events The Israeli Experience William Schecter, MD Professor of Clinical Surgery University of California, San Francisco Chief of Surgery San Francisco General
Form 1: Demographics
 Form 1: Demographics Case Number: *LMRN: *DOB: / / *Gender: Male Female *Race: White Native Hawaiian/Other Pacific Islander Black or African American Asian American Indian or Alaska Native Unknown *Hispanic
Form 1: Demographics Case Number: *LMRN: *DOB: / / *Gender: Male Female *Race: White Native Hawaiian/Other Pacific Islander Black or African American Asian American Indian or Alaska Native Unknown *Hispanic
Psychotropic Medication
 FOM 802-1 1 of 10 OVERVIEW The use of psychotropic medication as part of a child s comprehensive mental health treatment plan may be beneficial and should include consideration of all alternative interventions.
FOM 802-1 1 of 10 OVERVIEW The use of psychotropic medication as part of a child s comprehensive mental health treatment plan may be beneficial and should include consideration of all alternative interventions.
The ABC s of Chest Trauma
 The ABC s of Chest Trauma J Bradley Pickhardt MD, FACS Providence St Patrick Hospital What s the Problem? 2/3 of trauma patients have chest trauma Responsible for 25% of all trauma deaths Most injuries
The ABC s of Chest Trauma J Bradley Pickhardt MD, FACS Providence St Patrick Hospital What s the Problem? 2/3 of trauma patients have chest trauma Responsible for 25% of all trauma deaths Most injuries
Guidebook for ED and Inpatient Sepsis Order Set Initiatives 2018
 Background The leadership of the Surviving Sepsis Campaign (SSC) believes, since its inception, that both the SSC Guidelines and the SSC performance improvement indicators (1) will evolve as new evidence
Background The leadership of the Surviving Sepsis Campaign (SSC) believes, since its inception, that both the SSC Guidelines and the SSC performance improvement indicators (1) will evolve as new evidence
Guidelines are the Future of Sepsis Management Pro
 Guidelines are the Future of Sepsis Management Pro R. Phillip Dellinger MD, MCCM Professor and Chair of Medicine Director Adult Health Institute Senior Critical Care Attending Camden NJ USA Objectives
Guidelines are the Future of Sepsis Management Pro R. Phillip Dellinger MD, MCCM Professor and Chair of Medicine Director Adult Health Institute Senior Critical Care Attending Camden NJ USA Objectives
Resident At Risk. The National Early Warning Score (NEWS) and Monitoring Vital Signs
 and Monitoring Vital Signs") Resident At Risk The National Early Warning Score (NEWS) and Monitoring Vital Signs Schein et al 64 consecutive ward patients requiring CPR 84% clinical deterioration 8 hours before arrest Pathophysiology
Resident At Risk The National Early Warning Score (NEWS) and Monitoring Vital Signs Schein et al 64 consecutive ward patients requiring CPR 84% clinical deterioration 8 hours before arrest Pathophysiology
Chapter 2 Triage. Introduction. The Trauma Team
 Chapter 2 Triage Chapter 2 Triage Introduction Existing trauma courses focus on a vertical or horizontal approach to the ABCDE assessment of an injured patient: A - Airway B - Breathing C - Circulation
Chapter 2 Triage Chapter 2 Triage Introduction Existing trauma courses focus on a vertical or horizontal approach to the ABCDE assessment of an injured patient: A - Airway B - Breathing C - Circulation
Tailored Volume Resuscitation in the Critically Ill is Achievable. Objectives. Clinical Case 2/16/2018
 Tailored Volume Resuscitation in the Critically Ill is Achievable Heath E Latham, MD Associate Professor Fellowship Program Director Pulmonary and Critical Care Objectives Describe the goal of resuscitation
Tailored Volume Resuscitation in the Critically Ill is Achievable Heath E Latham, MD Associate Professor Fellowship Program Director Pulmonary and Critical Care Objectives Describe the goal of resuscitation
5 Key EMS Articles for 2012
 5 Key EMS Articles for 2012 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN 5 Key Topics Cardiac Arrest Trauma
5 Key EMS Articles for 2012 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN 5 Key Topics Cardiac Arrest Trauma
A Multidisciplinary Approach to Falls Prevention. Ross Ehrmantraut, RN, CCRN Patient Safety Officer Harborview Medical Center UW Medicine Seattle, WA
 A Multidisciplinary Approach to Falls Prevention Ross Ehrmantraut, RN, CCRN Patient Safety Officer Harborview Medical Center UW Medicine Seattle, WA Harborview Medical Center Harborview Medical Center
A Multidisciplinary Approach to Falls Prevention Ross Ehrmantraut, RN, CCRN Patient Safety Officer Harborview Medical Center UW Medicine Seattle, WA Harborview Medical Center Harborview Medical Center
Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014
 December 17, 2014") Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014 Presenters Mark Blaney, RN Regional Nurse Educator CHI Franciscan Health Karen Lautermilch Director, Quality & Performance
Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014 Presenters Mark Blaney, RN Regional Nurse Educator CHI Franciscan Health Karen Lautermilch Director, Quality & Performance
MANAGEMENT OF DENGUE INFECTION IN ADULTS (Revised 2 nd Edition) QUICK REFERENCE FOR HEALTHCARE PROVIDERS
 QUICK REFERENCE FOR HEALTHCARE PROVIDERS") 1 KEY MESSAGES Dengue is a dynamic disease and presented in three phases - febrile phase, critical phase and recovery phase. Clinical deterioration often occurs in the critical phase and is marked by plasma
1 KEY MESSAGES Dengue is a dynamic disease and presented in three phases - febrile phase, critical phase and recovery phase. Clinical deterioration often occurs in the critical phase and is marked by plasma