Geriatric syndromes and. of geriatric medicine. Pavel Weber
|
|
|
- Jemima Blake
- 5 years ago
- Views:
Transcription
1 Geriatric syndromes and frailty - the crucial points of geriatric medicine Pavel Weber Department of Internal Medicine, Geriatrics and Practical Medicine; Faculty Hospital and Masaryk University; Brno; Czech Republic 1
2 Ageing- definition Inevitable physiological process, which is the last ontogenetic period of life. Over 75 y. break point of ontogenesis. 2
3 Old Age and Illness According to rising age the spectra of morbidity is changing risk of chronical and degenerative illnesses and death An old organism adapts badly to varying conditions of internal and external environment 3
4 European Population Age Structure (Baltes: Gerontology 2003;49:123) 100% 80% 60% 40% % 0% Year 4

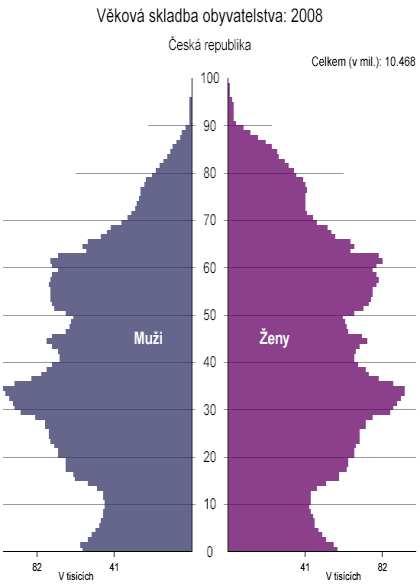

5 Population of the Czech Republic
6 CR and prognosis osis 2060 (ČSÚ ročenka) y. 14,6% 80 y. 3,4% 85 y. 1,2% LE: 73,5 y. 79,7 y y. 33% 80 y. 14% 85 y. 7,5% LE: 85,5 y. 90,1 y. 6
7 Age Categories New Division y. young seniors y. old seniors adaptability vulnerability 85 + y. oldest old frailty dependance 7
8 Functional Categorization 1. Fit seniors 2. Independent fail only due to stress (illness, injury, surgery etc.) 3. Frail risk even in normal conditions (falls, cognition, mobility, etc.) 4. Bedridden immobile Weber P. et al.: Adv. Gerontol., 21, 2008, No 1, pp
9 Who is a geriatric patient? Biologically older patient Multi - morbid Disabled with functional limitations Need - specific geriatric mode Weber P.: Vnitř. Lék, 51, 2005, č.2, s
10 Difficulties of modern medicine in the care of seniors Atomization of medicine Absence of holistic approach Multi-morbidity seemingly doesn t belong anywhere socialization of health problems Weber P., Svačinová J.: Chapter X, s In: Reece, Steve M.; NOVA Publisher, New York USA, 2005, 233s. ISBN:
11 The Main Aim of Geriatrics 1. To preserve the health of seniors 2. To live a high-quality and independent life as long as possible 3. Sustaining and protection of self-sufficiency 4. To minimize the period with sy of FTT Weber P.: Vnitřní Lékařství. 47, 2001, č.2, s
12 What is frailty? Medical syndrome sarcopenia Neither multimorbidity nor disability Multidimensional phenomenon Prognostic negative factor 65y. 7%; 85y. 25% Handicapping at least in 2 of 4 areas: somatic, cognitive, nutritional, social. Weber P., et al.: Čas. Lék. Čes., 143, 2004, č. 8, s
13 Disregulation HPA axis 13
14 Illnesses and Age vs. frailty THYREOPAT. DEMENTIA DEPRESSION SENSORY ORGANS Muscle strenght Physical activity CVD MULTI- MORBIDITY OSTEOPOR. Frailty Falls Sarcopenia TUMORS DM Disability 14
15 Frailty characterist teristicsics physical, mental and social capacities rise or deterioration of disability multimorbidity adverse effect of the drugs (AED) social izolation risk of institutionalization risk of death (>80 y. one of the main) Weber P., P. Crome: Ageing & Health. 13, 2005, s
16 Frailty relations to FD, FTT AGE ILLNESS ENVIR. SOCIAL Adaptability Physical capacity cognition nutrition CLINICALLY EVALUABLE deterioration FUNCTIONAL DECREASE - FD Frailty (disability) GERIATRIC SYNDROMS FTT - DEVELOPMENT 16
17 Transition to frailty (Tinetti, Wolf) < 80y. sight cognition regular exercise FRAILTY sight disorders weakness LE ROBUSTNESS TRANSITION REVERSI SIBILITY? > 80y. standing and walk disorders depression sedativeses ZD: <2F a >3Z FR: >4F a <1Z 17
18 1. Instability 2. Immobility 3. Incontinence Geriatric giants 4. Intellectual disorders 5. Iatrogenia? Weber P.: Postgraduální medicína, 6, 2004, č. 3, příloha, s
19 Characteristi teristics sy 5I5 Multicausality Chronical process Decline of independence Impossibility of ordinary treatment Weber P.: Euro J Ger, 4, 2002, č. 4, s
20 Instability Closely related to such symptoms as: balance, standing, walk, vertigo and their consequences falls. 20
21 Mobility Disorders Over 65 yrs. 15 to 20 % persons slow and difficult walk Over 75 yrs. 40 % walk: less than 1 mile 1/3 difficulties with walking the stairs % need stick or assistance 5 % confined to bed 21
22 Falls - characteristics cteristics 65+ y % persons once a year at home 1/3 of them: repeated falls with age,, maximum in 7 th 8 th decade With risk factors 50% Only 1/4 of falls are registered by paramedics Elderly people don t mention them falls remind them of their helplessness Women: : more frequently ( muscles, home activity) 22
23 Falls - reasons 1. Mechanic falls (external reasons) % slipping, tripping, etc. 2. Symptomatic falls (internal reasons) 70-75% 75% - somatic illness consequence Neurological, cardiovascular and psychiatric illnesses; musculoskeletal system disorders, sight and hearing; drugs, alcohol 23
24 Immobility Syndrom Long-term or permanent confinement to bed (contingently wheelchair) consequences. Main symptoms: decubitus, muscular atrophy, decondition, walking stereotype disruption, dehydration, etc. 24
25 Urinary incontinence introduct. Def.: inability to control the flow of urine and involuntary provable urination, which causes hygienical and social problems to the involved Prevalence over 60 yrs % persons in very old - > 40% Consequences life interference mental deprivation incontinence tools costs The Standardisation of Terminology of Lower 25 Urinary Tract Function, I.C.S. 2002)
26 Incontinence Occurrence 26
27 Specifics cs of Incontinence in the Elderly The oldest old is ashamed of talking about incontinence, more than 1/2 persons conceal it The physician has to ask the patient actively 27
28 Dementia tia- characteris teristics The most common diagnosis in the elderly heterogeneous group of illnesses with the global intellect disorder deterioration of some cognitive functions (memory, talk, thought, orientation, discretion) personality changes, affectivity, behaviour disorders 28
29 Dementia Classification (based on etiology) Primarily degenerative dementia 50-70% Alzheimer senile and presenile 50-60%; others (m. Parkinson, etc.) 5-10% Vascular dementia 15-30% Mixed dementia 10-20% Lewy body dementia 10-20% Frontotemporal dem. 3-5% Secondary dementia 3-5% 29
30 Delirium - characterist teristicsics Def.: Unspecified reaction of the brain on various noxas Alterations of the mental state acute and temporary connected with inability to identify and react to environmental changes adequately. Consciousness is blured and the reduced quality of perception may fluctuate between the extrems from total vigility to coma. 30
31 Epidemiology of delirium at home - 65 yrs. old - 1-2% at home - over 85 yrs. old % acute dept. >75 yrs. on admission 10-15% acute dept. >75 yrs. during the hospitalization 20-30% gerontopsych. and institute for long-term patients (ILP) 30-60% after general surgeries-10%; heart-30% and hip up to 50% 31
32 Polyph pharmacotherapy (PPT) definition Use of 3 or more drugs regardless of the age In CR especially in diagnosis: heart failure; atrial fibrilation; DM; stroke and TIA; chr. bronchitis 32
33 Pharmacotherapy in the elderly - specifics 1. hanged reaction to drugs Changes of pharmacodynamics and -kinetics 2. AED in the elderly generally 3. non-compliance of seniors 4. appearance of pharmaceutical interactions 33
34 Iatrogenia 30% AED are predictable Up to 70% AED are dose dependent The treatment should be considered individually ( tailor made ) AED reactions remind unspecific geriatric syndroms 34
35 Other geriatric syndroms Sy decondition and hypomobility (sarcopenia) Sy anorexia and malnutrition, dehydration Sy of dual deficit (sight, hearing) Geriatric maladaptive sy Sy of mistreatment, neglect and elder abuse Sy of the terminal geriatric deterioration - FTT Weber P.: Euro J Ger, 4, 2002, č. 4, s
36 Sy decondition and hypomobility (sarcopenia) The principle is the limitation of kinetic activity due to sitting or lying, muscle atrophy of the lower extremities. The cause may be the loss of motivation, depression, nutrition disorders, kinetic dyscomfort. 36
37 Sy anorexia and malnutrition Causes of anorexia: tumors, depression, constipation, inadequate form of food Causes of malnutrition: bad denture or dysphagia, absorption disorders, poverty, immobility, dementia or neglect sy 37
38 Sy of dual sensory deficit (sight( sight, hearing) r. at home: 0,5% 85 r. at home: 6% With cognitive dysfunction: 6 13% In nursing institutions: 7 25% SLAETS, JP. The prevalence of combined vision impairment and hearing loss: the importace of comorbidity studies. Ned. Tijdschr. Geneetikol., 2007, 151 (26), p
39 Geriatric maladaptive syndrom Psycho-social maladaptation Maladjustment to new living conditions (e.g. nursing home admission, etc.). Somatization of difficulties (vertigo, heart palpitation, sweat, etc.). Drugs often worsen the situation. 39
40 Sy of elder abuse, neglect and mistreatment sy EAN Intentional use or threat of use of physical powers or other instrument against himself, other person, against some group etc. All kinds of physical, mental and sexual mistreatment and abuse, acts of neglect and suicides and other forms of self-mutilation 5-20% seniors 40
41 Risk Factors of Sy of EAN Old age Disability Loneliness Intellectual dysfunction: dementia, depression (> 50%) Poverty Minorities; Ethnically different races 41
42 Sy terminal geriatric deterioration tion - FTT medical and functional status without an explicit pathological reason, refractory to the treatment loss of appetite, slimming, fatigue, activity limitation, apathy - immobility, confusion Heading for death up to ¾ cases over 85 yrs. it lasts 3-6 months in average 42
43 How to get old in a healthy manner? GUIDE- LINES Physical activity Mental activity Nutrition Social activity 30min./d. exercise Optimum BMI Osteoporosis prevention Sarkopenia prevention Brain gymnastics Reminiscences therapy FFA, chol. Na Fruits, vegetables, cal. Vitamins, trace elements Loneliness Socialization (communication) Weber P.: Euro Rehab, 12, 2002, č. 2, s
44 Conclusion Not to underestimate the ability to recover and live independent life in an acceptable condition. 44
45 THM A geriatric patient during the hospitalization or Out-patient check-up at GP s or somewhere else CGA (incl( incl.. MMSE, ADL, etc.) Geriatric consultation multidisciplinary approach 45

46 add life to years not years to life 46
Longevity - loneliness, dependency, malnutrition and geriatric giants in 12,210 elderly hospitalized people
 Longevity - loneliness, dependency, malnutrition and geriatric giants in 12,210 elderly hospitalized people Pavel Weber, Hana Meluzínová, Hana Matějovská-Kubešová, Vlasta Polcarová, Dana Weberová, Katarina
Longevity - loneliness, dependency, malnutrition and geriatric giants in 12,210 elderly hospitalized people Pavel Weber, Hana Meluzínová, Hana Matějovská-Kubešová, Vlasta Polcarová, Dana Weberová, Katarina
Continence, falls and the frailty syndrome. Anne Foley - BGS Bladders and Bowel Health 2012
 Continence, falls and the frailty syndrome Outline Frailty Geriatric syndromes and giants Aetiology What can be done? The future Frailty Frailty Frailty (noun): The state of being weak in health or body
Continence, falls and the frailty syndrome Outline Frailty Geriatric syndromes and giants Aetiology What can be done? The future Frailty Frailty Frailty (noun): The state of being weak in health or body
Family Medicine for English language students of Medical University of Lodz. Seminar 12. Elderly care. Przemysław Kardas MD PhD
 Family Medicine for English language students of Medical University of Lodz Seminar 12 Elderly care Przemysław Kardas MD PhD Europe is facing demographic challenge 2014 2080 2 3 Old vs young: major differences
Family Medicine for English language students of Medical University of Lodz Seminar 12 Elderly care Przemysław Kardas MD PhD Europe is facing demographic challenge 2014 2080 2 3 Old vs young: major differences
The Industry s Views on Older Old Patients
 The Industry s Views on Older Old Patients Susanna Del Signore and Philippe Guillet Global Regulatory Policy and Ageing Therapeutic Strategic Unit SANOFI R&D 1 Outline Introduction EFPIA Survey: Overview
The Industry s Views on Older Old Patients Susanna Del Signore and Philippe Guillet Global Regulatory Policy and Ageing Therapeutic Strategic Unit SANOFI R&D 1 Outline Introduction EFPIA Survey: Overview
Chapter 01 Introduction
 Chapter 01 Introduction Defining the Elderly There is no universally accepted age cut-off defining elderly. This reflects the fact that chronological age itself is less important than biological events
Chapter 01 Introduction Defining the Elderly There is no universally accepted age cut-off defining elderly. This reflects the fact that chronological age itself is less important than biological events
Geriatrics and Cancer Care
 Geriatrics and Cancer Care Roger Wong, BMSc, MD, FRCPC, FACP Postgraduate Dean of Medical Education Clinical Professor, Division of Geriatric Medicine UBC Faculty of Medicine Disclosure No competing interests
Geriatrics and Cancer Care Roger Wong, BMSc, MD, FRCPC, FACP Postgraduate Dean of Medical Education Clinical Professor, Division of Geriatric Medicine UBC Faculty of Medicine Disclosure No competing interests
WEBINAR SERIES: AGING IN INDIVIDUALS WITH INTELLECTUAL AND DEVELOPMENTAL DISABILITIES
 WEBINAR SERIES: AGING IN INDIVIDUALS WITH INTELLECTUAL AND DEVELOPMENTAL DISABILITIES 1 CMS Medicare-Medicaid Coordination Office (MMCO) Established by Section 2602 of the Affordable Care Act Purpose:
WEBINAR SERIES: AGING IN INDIVIDUALS WITH INTELLECTUAL AND DEVELOPMENTAL DISABILITIES 1 CMS Medicare-Medicaid Coordination Office (MMCO) Established by Section 2602 of the Affordable Care Act Purpose:
Understanding and Assessing for Frailty
 Understanding and Assessing for Frailty Dr Gloria Yu Clinical Head of Bexley Integrated Care Consultant Physician in Elderly, General and Stroke Medicine 8 July 2015 Learning objectives What is frailty?
Understanding and Assessing for Frailty Dr Gloria Yu Clinical Head of Bexley Integrated Care Consultant Physician in Elderly, General and Stroke Medicine 8 July 2015 Learning objectives What is frailty?
UNTHSC TCOM Geriatric Competencies Curriculum Mapping Document
 INSTRUCTIONS: Place a "B" (Basic), "I" (Intermediate), or "A" (Advanced) in the box next to the Geriatric Competency to indicate the Geraitaric Competency being taught, the corresponding Method of Subject
INSTRUCTIONS: Place a "B" (Basic), "I" (Intermediate), or "A" (Advanced) in the box next to the Geriatric Competency to indicate the Geraitaric Competency being taught, the corresponding Method of Subject
Delirium. Quick reference guide. Issue date: July Diagnosis, prevention and management
 Issue date: July 2010 Delirium Diagnosis, prevention and management Developed by the National Clinical Guideline Centre for Acute and Chronic Conditions About this booklet This is a quick reference guide
Issue date: July 2010 Delirium Diagnosis, prevention and management Developed by the National Clinical Guideline Centre for Acute and Chronic Conditions About this booklet This is a quick reference guide
Geriatric Medicine I) OBJECTIVES
 OBJECTIVES") Geriatric Medicine I) OBJECTIVES 1 To provide a broad training and in-depth experience at a level sufficient for trainees to acquire competence and professionalism required of a specialist in Geriatric
Geriatric Medicine I) OBJECTIVES 1 To provide a broad training and in-depth experience at a level sufficient for trainees to acquire competence and professionalism required of a specialist in Geriatric
Aging. Objectives 13/02/2013
 Deirdre Gillespie RN MN AHEADD (Assessment, Health, Education and Developmental Disabilities) dgillespie1@cogeco.ca 613-985-6154 Objectives Discussion about aging Aging and Developmental Disabilities Supporting
Deirdre Gillespie RN MN AHEADD (Assessment, Health, Education and Developmental Disabilities) dgillespie1@cogeco.ca 613-985-6154 Objectives Discussion about aging Aging and Developmental Disabilities Supporting
Geriatric Alterations Associated with Neurological Conditions
 Geriatric Alterations Associated with Neurological Conditions I have no conflicts of interest. Julie Bronson The Older Adult According to the World Health Organization Africa 50-55 or 50-65 United Nations
Geriatric Alterations Associated with Neurological Conditions I have no conflicts of interest. Julie Bronson The Older Adult According to the World Health Organization Africa 50-55 or 50-65 United Nations
Frailty in Older Adults
 Frailty in Older Adults John Puxty puxtyj@providencecare Geriatrics 20/20: Bringing Current Issues into Perspective Session Overview Definition of Frailty Strategies for identifying frail older adults
Frailty in Older Adults John Puxty puxtyj@providencecare Geriatrics 20/20: Bringing Current Issues into Perspective Session Overview Definition of Frailty Strategies for identifying frail older adults
Dysphagia as a Geriatric Syndrome Braca Cantor, M.D.
 Dysphagia as a Geriatric Syndrome Braca Cantor, M.D. March 3, 2018 Braca B. Cantor, MD Indiana University School of Medicine, Class of 2014 St. Vincent Internal Medicine Residency, Class of 2017 Current
Dysphagia as a Geriatric Syndrome Braca Cantor, M.D. March 3, 2018 Braca B. Cantor, MD Indiana University School of Medicine, Class of 2014 St. Vincent Internal Medicine Residency, Class of 2017 Current
Communication with Cognitively Impaired Clients For CNAs
 Communication with Cognitively Impaired Clients For CNAs This course has been awarded one (1.0) contact hour. This course expires on August 31, 2017. Copyright 2005 by RN.com. All Rights Reserved. Reproduction
Communication with Cognitively Impaired Clients For CNAs This course has been awarded one (1.0) contact hour. This course expires on August 31, 2017. Copyright 2005 by RN.com. All Rights Reserved. Reproduction
Quality Care for the Hospitalized Older Adult
 Quality Care for the Hospitalized Older Adult Quality Care for the Hospitalized Older Adult Shelley R McDonald, DO, PhD May 19 th, 2018 Objectives To define why the hospital is a dangerous place for older
Quality Care for the Hospitalized Older Adult Quality Care for the Hospitalized Older Adult Shelley R McDonald, DO, PhD May 19 th, 2018 Objectives To define why the hospital is a dangerous place for older
Recommended Geropsychiatric Competency Enhancements for Gerontological Nurse Practitioners
 Recommended Geropsychiatric Competency Enhancements for Gerontological Nurse Practitioners These recommended competency enhancement statements draw attention to the special needs of older adults with mental
Recommended Geropsychiatric Competency Enhancements for Gerontological Nurse Practitioners These recommended competency enhancement statements draw attention to the special needs of older adults with mental
Table to Demonstrate a method of working through Triggered CAPs.
 CAP Problem Goals Triggers Guidelines Physical Activities increase hours of exercises Reports less than 2 hours Personal choice Promotion and physical activity activity in last 3 days Instrumental Activities
CAP Problem Goals Triggers Guidelines Physical Activities increase hours of exercises Reports less than 2 hours Personal choice Promotion and physical activity activity in last 3 days Instrumental Activities
Fall Risk Assessment and Prevention in the Post-Acute Setting A Road Map
 Fall Risk Assessment and Prevention in the Post-Acute Setting A Road Map Cora M. Butler, JD, RN, CHC HealthCore Value Advisors, Inc. Juli A. James, RN Primaris Holdings, Inc. Objectives Explore the burden
Fall Risk Assessment and Prevention in the Post-Acute Setting A Road Map Cora M. Butler, JD, RN, CHC HealthCore Value Advisors, Inc. Juli A. James, RN Primaris Holdings, Inc. Objectives Explore the burden
FRAILTY SYNDROME. dr. Rose Dinda Martini, Sp.PD, K-Ger
 FRAILTY SYNDROME dr. Rose Dinda Martini, Sp.PD, K-Ger Geriatric Division, Internal Medicine Department M. Djamil Hospital Padang Faculty of Medicine, Andalas University, 2018 Medical syndrome Multiple
FRAILTY SYNDROME dr. Rose Dinda Martini, Sp.PD, K-Ger Geriatric Division, Internal Medicine Department M. Djamil Hospital Padang Faculty of Medicine, Andalas University, 2018 Medical syndrome Multiple
Chapter Goal. Learning Objectives 9/12/2012. Chapter 36. Geriatrics. Use assessment findings to formulate management plan for geriatric patients
 Chapter 36 Geriatrics Chapter Goal Use assessment findings to formulate management plan for geriatric patients Learning Objectives Describe dependent & independent living environments Identify local resources
Chapter 36 Geriatrics Chapter Goal Use assessment findings to formulate management plan for geriatric patients Learning Objectives Describe dependent & independent living environments Identify local resources
Course Handouts & Post Test
 Abuse, Neglect, Mistreatment and Exploitation What You Need to Know and Do Course Handouts & Post Test To download presentation handouts, click on the attachment icon Course evaluation and post test are
Abuse, Neglect, Mistreatment and Exploitation What You Need to Know and Do Course Handouts & Post Test To download presentation handouts, click on the attachment icon Course evaluation and post test are
Comprehensive Geriatric Assessment: what s it all about? Deborah Mayne, City Hospitals Sunderland Clinical Lead for Frailty
 Comprehensive Geriatric Assessment: what s it all about? Deborah Mayne, City Hospitals Sunderland Clinical Lead for Frailty What is Comprehensive Geriatric Assessment (CGA)? Gold standard for management
Comprehensive Geriatric Assessment: what s it all about? Deborah Mayne, City Hospitals Sunderland Clinical Lead for Frailty What is Comprehensive Geriatric Assessment (CGA)? Gold standard for management
Delirium and Falls. Julia Poole CNC Aged Care RNSH
 Delirium and Falls Julia Poole CNC Aged Care RNSH Falls Risk Screening Tool Ontario STRATIFY NORTHERN SYDNEY CENTRAL COAST HEALTH Falls Risk Screening - Ontario STRATIFY Please read instructions for use
Delirium and Falls Julia Poole CNC Aged Care RNSH Falls Risk Screening Tool Ontario STRATIFY NORTHERN SYDNEY CENTRAL COAST HEALTH Falls Risk Screening - Ontario STRATIFY Please read instructions for use
Mental Health Counseling for mood, aging, and coping with life transitions and chronic illness.
 Mental Health Counseling for mood, aging, and coping with life transitions and chronic illness. Silver Linings for Seniors Silver Linings for Seniors, Inc. offers on-site confidential Mental Health Counseling
Mental Health Counseling for mood, aging, and coping with life transitions and chronic illness. Silver Linings for Seniors Silver Linings for Seniors, Inc. offers on-site confidential Mental Health Counseling
Blueprint Schwerpunktprüfung Geriatrie (Version 2011) Medical Content Category
 Medical Content Category") Blueprint Schwerpunktprüfung Geriatrie (Version 2011) A A1 A2 Gerontology Demography and epidemiology Psychology and sociology of aging Demographic development in Switzerland, Europe and USA Life expectancy
Blueprint Schwerpunktprüfung Geriatrie (Version 2011) A A1 A2 Gerontology Demography and epidemiology Psychology and sociology of aging Demographic development in Switzerland, Europe and USA Life expectancy
Welcome to the Routine frailty identification in the GP contract webinar presented by Dawn Moody
 Welcome to the Routine frailty identification in the GP contract webinar presented by Dawn Moody The presentation will begin at 12.00pm. Attendees will be muted during the presentation to avoid interference.
Welcome to the Routine frailty identification in the GP contract webinar presented by Dawn Moody The presentation will begin at 12.00pm. Attendees will be muted during the presentation to avoid interference.
Pre- Cardiac intervention. Dr. Victor Sim 16 th Oct 2014
 Pre- Cardiac intervention Frailty assessment Dr. Victor Sim 16 th Oct 2014 Topics to cover Defining frailty Pathophysiology of frailty Are current pre-cardiac surgery assessment tools adequate? Why do
Pre- Cardiac intervention Frailty assessment Dr. Victor Sim 16 th Oct 2014 Topics to cover Defining frailty Pathophysiology of frailty Are current pre-cardiac surgery assessment tools adequate? Why do
Community and Mental Health Services. Palliative Care. Criteria and
 Community and Mental Health Services Specialist Palliative Care Service Referral Criteria and Guidance November 2018 Specialist Palliative Care Service Referrals These guidelines cover referrals for patients
Community and Mental Health Services Specialist Palliative Care Service Referral Criteria and Guidance November 2018 Specialist Palliative Care Service Referrals These guidelines cover referrals for patients
How to prevent delirium in nursing home. Dr. Sophie ALLEPAERTS Geriatric department CHU-Liège Belgium
 How to prevent delirium in nursing home Dr. Sophie ALLEPAERTS Geriatric department CHU-Liège Belgium 1 CONFLICT OF INTEREST DISCLOSURE I have no potential conflict of interest to report 2 Outline 1. Introduction
How to prevent delirium in nursing home Dr. Sophie ALLEPAERTS Geriatric department CHU-Liège Belgium 1 CONFLICT OF INTEREST DISCLOSURE I have no potential conflict of interest to report 2 Outline 1. Introduction
Hospitalization- Associated Disability
 Hospitalization- Associated Disability Deborah Villarreal, MD Assistant Professor Geriatric and Palliative Medicine An Unfortunately Common Scenario Mrs.G 70 y/o BF DM type II, HTN, s/p CVA, OA, OP admitted
Hospitalization- Associated Disability Deborah Villarreal, MD Assistant Professor Geriatric and Palliative Medicine An Unfortunately Common Scenario Mrs.G 70 y/o BF DM type II, HTN, s/p CVA, OA, OP admitted
Behavioral Interventions
 Behavioral Interventions Linda K. Shumaker, R.N.-BC, MA Pennsylvania Behavioral Health and Aging Coalition Behavioral Management is the key in taking care of anyone with a Dementia! Mental Health Issues
Behavioral Interventions Linda K. Shumaker, R.N.-BC, MA Pennsylvania Behavioral Health and Aging Coalition Behavioral Management is the key in taking care of anyone with a Dementia! Mental Health Issues
The Geriatrician in the Trauma Service. Trauma Quality Improvement Program (TQIP) Annual Scientific Meeting and Training 2013
 Annual Scientific Meeting and Training 2013") The Geriatrician in the Trauma Service Trauma Quality Improvement Program (TQIP) Annual Scientific Meeting and Training 2013 Challenges of the Geriatric Trauma Patient Challenges of the Geriatric Patient
The Geriatrician in the Trauma Service Trauma Quality Improvement Program (TQIP) Annual Scientific Meeting and Training 2013 Challenges of the Geriatric Trauma Patient Challenges of the Geriatric Patient
Death by Bedrest: The Perils of The Hospital
 Death by Bedrest: The Perils of The Hospital Mindy Fain, MD Professor of Clinical Medicine Director, Arizona Reynolds Program of Applied Geriatrics Section Head, Geriatrics & Gerontology University of
Death by Bedrest: The Perils of The Hospital Mindy Fain, MD Professor of Clinical Medicine Director, Arizona Reynolds Program of Applied Geriatrics Section Head, Geriatrics & Gerontology University of
Frailty and falls assessment and intervention tool
 Frailty and falls assessment and intervention tool Contents Frailty and falls 4 Social circumstances 5 Mental health 6 Environment 7 Nutrition 8 Dizziness or blackout 9 Medications 10 Mobility and balance
Frailty and falls assessment and intervention tool Contents Frailty and falls 4 Social circumstances 5 Mental health 6 Environment 7 Nutrition 8 Dizziness or blackout 9 Medications 10 Mobility and balance
Delirium. Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta
 Delirium Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta Overview A. Delirium - the nature of the beast B. Significance of delirium C. An approach
Delirium Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta Overview A. Delirium - the nature of the beast B. Significance of delirium C. An approach
Frailty. Nicholas Butler MD, MBA Department of Family Medicine University of Iowa
 Frailty Nicholas Butler MD, MBA Department of Family Medicine University of Iowa Doris 84 yo female who comes into your clinic with her daughter. She complains of feeling increasingly fatigued and just
Frailty Nicholas Butler MD, MBA Department of Family Medicine University of Iowa Doris 84 yo female who comes into your clinic with her daughter. She complains of feeling increasingly fatigued and just
Specialist Palliative Care Service Referral Criteria and Guidance
 Specialist Palliative Care Service Referral Criteria and Guidance Specialist Palliative Care Service Referrals These guidelines cover referrals for patients with progressive terminal illness, whether
Specialist Palliative Care Service Referral Criteria and Guidance Specialist Palliative Care Service Referrals These guidelines cover referrals for patients with progressive terminal illness, whether
Frailty and Aging Managing from a Community Perspective. Dr. John Puxty
 Frailty and Aging Managing from a Community Perspective Dr. John Puxty puxtyj@providencecare.ca Presenter Disclosure No commercial support received or potential conflicts Learning Objectives The participant
Frailty and Aging Managing from a Community Perspective Dr. John Puxty puxtyj@providencecare.ca Presenter Disclosure No commercial support received or potential conflicts Learning Objectives The participant
Dr Cameron Mitchell Liggins Institute University of Auckland
 Dr Cameron Mitchell Liggins Institute University of Auckland 14:00-14:55 WS #46: Aging Health and Nutrition 15:05-16:00 WS #58: Aging Health and Nutrition (Repeated) Aging Health and Nutrition Cameron
Dr Cameron Mitchell Liggins Institute University of Auckland 14:00-14:55 WS #46: Aging Health and Nutrition 15:05-16:00 WS #58: Aging Health and Nutrition (Repeated) Aging Health and Nutrition Cameron
Mental Health Problems in Older Adults: Signs & Symptoms Addressing Illness, Injury, & Loss
 Mental Health Problems in Older Adults: Signs & Symptoms Addressing Illness, Injury, & Loss Tobi A. Abramson, PhD September 22, 2013 Myths, Misperceptions, & Stereotypes Questions to consider Who has misperceptions
Mental Health Problems in Older Adults: Signs & Symptoms Addressing Illness, Injury, & Loss Tobi A. Abramson, PhD September 22, 2013 Myths, Misperceptions, & Stereotypes Questions to consider Who has misperceptions
Define frailty Recognise the consequences of frailty Know why CGA important and what are the main components of a CGA that can be done in an initial
 Dr Kyra Neubauer Define frailty Recognise the consequences of frailty Know why CGA important and what are the main components of a CGA that can be done in an initial assessment Understand what are potential
Dr Kyra Neubauer Define frailty Recognise the consequences of frailty Know why CGA important and what are the main components of a CGA that can be done in an initial assessment Understand what are potential
Ageing Well. Avoiding falls in older people. Prof Martin Vernon NCD Older People. Find Recognise Assess Intervene Long-term.
 Ageing Well Avoiding falls in older people Prof Martin Vernon NCD Older People 21 October 2016 1 Its not how old we are, but how we are old 2 Key points 1. Demography 2. Frailty & falls 3. Routine frailty
Ageing Well Avoiding falls in older people Prof Martin Vernon NCD Older People 21 October 2016 1 Its not how old we are, but how we are old 2 Key points 1. Demography 2. Frailty & falls 3. Routine frailty
5 Negative Effects of Loneliness on Physical and Mental Health
 5 Negative Effects of Loneliness on Physical and Mental Health Devi Gajendran Disorders The feeling of loneliness or being detached from others is not just a human emotion; it is a complex emotional response
5 Negative Effects of Loneliness on Physical and Mental Health Devi Gajendran Disorders The feeling of loneliness or being detached from others is not just a human emotion; it is a complex emotional response
Understand the Process and Experience of Dementia
 Unit 33: Understand the Process and Experience of Dementia Unit code: DEM 301 Unit reference number: J/601/3538 QCF level: 3 Credit value: 3 Guided learning hours: 22 Unit summary This unit provides the
Unit 33: Understand the Process and Experience of Dementia Unit code: DEM 301 Unit reference number: J/601/3538 QCF level: 3 Credit value: 3 Guided learning hours: 22 Unit summary This unit provides the
Delirium, Depression and Dementia
 Delirium, Depression and Dementia Martha Watson, MS, APRN, GCNS Some material included in this presentation is adapted from: NICHE (2009). Geriatric Resource Nurse Core Curriculum [Power Point presentation].
Delirium, Depression and Dementia Martha Watson, MS, APRN, GCNS Some material included in this presentation is adapted from: NICHE (2009). Geriatric Resource Nurse Core Curriculum [Power Point presentation].
Acoustic neuroma s/p removal BPPV (Crystals)- 50% of people over 65 y/ o with dizziness will have this as main reason for dizziness
- 50% of people over 65 y/ o with dizziness will have this as main reason for dizziness") Dizziness and the Heart Mended Hearts Inservice Karen Hansen, PT, DPT, Cert Vestibular Rehab, CEAS Tennessee Therapy & Balance Center, LLC July 21, 2016 Balance We maintain balance with input from our
Dizziness and the Heart Mended Hearts Inservice Karen Hansen, PT, DPT, Cert Vestibular Rehab, CEAS Tennessee Therapy & Balance Center, LLC July 21, 2016 Balance We maintain balance with input from our
Pre- Cardiac intervention. Dr. Victor Sim 26 th Sept 2014
 Pre- Cardiac intervention Frailty assessment Dr. Victor Sim 26 th Sept 2014 Defining frailty Lacks consensus (Rockwood CMAJ 2005;173(5):489-95 Introduction) Some consider symptoms, signs, diseases and
Pre- Cardiac intervention Frailty assessment Dr. Victor Sim 26 th Sept 2014 Defining frailty Lacks consensus (Rockwood CMAJ 2005;173(5):489-95 Introduction) Some consider symptoms, signs, diseases and
Evolutions in Geriatric Fracture Care Preparing for the Silver Tsunami
 Evolutions in Geriatric Fracture Care Preparing for the Silver Tsunami James Holstine, DO Medical Director for the Joint Replacement Center, Geriatric Fracture Center, Orthopedic Surgeon PeaceHealth Whatcom
Evolutions in Geriatric Fracture Care Preparing for the Silver Tsunami James Holstine, DO Medical Director for the Joint Replacement Center, Geriatric Fracture Center, Orthopedic Surgeon PeaceHealth Whatcom
Aging and Mental Health Current Challenges in Long Term Care
 Aging and Mental Health Current Challenges in Long Term Care Stephanie Saur & Christina Pacheco Acute Care Behavioural Consultants Alzheimer Society Peel What is Mental Health? Mental health includes our
Aging and Mental Health Current Challenges in Long Term Care Stephanie Saur & Christina Pacheco Acute Care Behavioural Consultants Alzheimer Society Peel What is Mental Health? Mental health includes our
Interprofessional Care for Elders through 48/5
 Interprofessional Care for Elders through 48/5 Janet E. McElhaney, MD, FRCPC, FACP HSN Volunteer Association Chair in Geriatric Research Professor of Medicine, Northern Ontario School of Medicine Health
Interprofessional Care for Elders through 48/5 Janet E. McElhaney, MD, FRCPC, FACP HSN Volunteer Association Chair in Geriatric Research Professor of Medicine, Northern Ontario School of Medicine Health
Frailty: what s it all about?
 Frailty: what s it all about? What is frailty? 1. an inevitable consequence of aging 2. A state due to multiple long term conditions 3. A condition in which the person becomes fragile 4. A state associated
Frailty: what s it all about? What is frailty? 1. an inevitable consequence of aging 2. A state due to multiple long term conditions 3. A condition in which the person becomes fragile 4. A state associated
Coding For Dementia & Other Unspecified Conditions
 Coding For Dementia & Other Unspecified Conditions Judy Adams, RN, BSN, HCS-D, HCS-O AHIMA Approved ICD-10-CM Trainer Transmittal 3022 CMS released Transmittal 3022, Hospice Manual Update for Diagnosis
Coding For Dementia & Other Unspecified Conditions Judy Adams, RN, BSN, HCS-D, HCS-O AHIMA Approved ICD-10-CM Trainer Transmittal 3022 CMS released Transmittal 3022, Hospice Manual Update for Diagnosis
Elder Abuse: Forensic Pathology Perspective. Dr Linda Iles Forensic Pathology Services VIFM
 Elder Abuse: Forensic Pathology Perspective Dr Linda Iles Forensic Pathology Services VIFM Medico-legal death investigation Integration of: Circumstantial information: police reports Scene attendance/photographs
Elder Abuse: Forensic Pathology Perspective Dr Linda Iles Forensic Pathology Services VIFM Medico-legal death investigation Integration of: Circumstantial information: police reports Scene attendance/photographs
Living well with frailty. JOHN YOUNG National Clinical Director for the Frail Elderly & Integration, NHS England
 Living well with frailty JOHN YOUNG National Clinical Director for the Frail Elderly & Integration, NHS England A LTC rarely travels alone Kent Whole Population Dataset: Interim Report 2014 The burden
Living well with frailty JOHN YOUNG National Clinical Director for the Frail Elderly & Integration, NHS England A LTC rarely travels alone Kent Whole Population Dataset: Interim Report 2014 The burden
Dementia. Assessing Brain Damage. Mental Status Examination
 Dementia Assessing Brain Damage Mental status examination Information about current behavior and thought including orientation to reality, memory, and ability to follow instructions Neuropsychological
Dementia Assessing Brain Damage Mental status examination Information about current behavior and thought including orientation to reality, memory, and ability to follow instructions Neuropsychological
Specialist Palliative Care Referral for Patients
 Specialist Palliative Care Referral for Patients This guideline covers referrals for patients with progressive terminal illness, whether due to cancer or other disease. For many patients in the late stages
Specialist Palliative Care Referral for Patients This guideline covers referrals for patients with progressive terminal illness, whether due to cancer or other disease. For many patients in the late stages
Healthcare, hospitals and the challenges of an ageing population
 Healthcare, hospitals and the challenges of an ageing population Prof David Oliver Vice President, RCP, London Past President, British Geriatrics Society Senior Visiting Fellow, King s Fund Consultant
Healthcare, hospitals and the challenges of an ageing population Prof David Oliver Vice President, RCP, London Past President, British Geriatrics Society Senior Visiting Fellow, King s Fund Consultant
Charles Bernick, MD, MPH Cleveland Clinic Lou Ruvo Center for Brain Health June 2, 2018
 Charles Bernick, MD, MPH Cleveland Clinic Lou Ruvo Center for Brain Health June 2, 2018 Delirium common Prolongs hospitalization Worsens dementia ( if you survive) Increased risk of institutionalization
Charles Bernick, MD, MPH Cleveland Clinic Lou Ruvo Center for Brain Health June 2, 2018 Delirium common Prolongs hospitalization Worsens dementia ( if you survive) Increased risk of institutionalization
Psychosocial Problems In Reproductive Health Of Elders
 Psychosocial Problems In Reproductive Health Of Elders Dr. Sonia Oveisi Maternity and Child Health Assistant Professor of Qazvin University of Medical Science 6/2/2014 1 Goals 1. Definition 2. Epidemiology
Psychosocial Problems In Reproductive Health Of Elders Dr. Sonia Oveisi Maternity and Child Health Assistant Professor of Qazvin University of Medical Science 6/2/2014 1 Goals 1. Definition 2. Epidemiology
Frailty and relationship centred care in dementia
 Frailty and relationship centred care in dementia Dr Karen Harrison Dening Head of Research & Publications Dementia UK I will consider Frailty, Comorbidity, Multi morbidity & Dementia Older, spousal carers
Frailty and relationship centred care in dementia Dr Karen Harrison Dening Head of Research & Publications Dementia UK I will consider Frailty, Comorbidity, Multi morbidity & Dementia Older, spousal carers
Frailty in Older Adults. Frailty
 Frailty in Older Adults Nancy Stiles, MD Associate Professor Geriatrics i Sanders-Brown Center on Aging University of Kentucky Frailty Global impairment of physiological reserves involving i multiple l
Frailty in Older Adults Nancy Stiles, MD Associate Professor Geriatrics i Sanders-Brown Center on Aging University of Kentucky Frailty Global impairment of physiological reserves involving i multiple l
DISCLAIMER: ECHO Nevada emphasizes patient privacy and asks participants to not share ANY Protected Health Information during ECHO clinics.
 DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
Falls and Mobility. Katherine Berg, PhD, PT and Arielle Berger, MD. Presented by: Ontario s Geriatric Steering Committee
 Falls and Mobility Katherine Berg, PhD, PT and Arielle Berger, MD Key Learnings Arielle Berger, MD Key Learnings Learn approaches to falls assessment Understand inter-relationship between promoting safe
Falls and Mobility Katherine Berg, PhD, PT and Arielle Berger, MD Key Learnings Arielle Berger, MD Key Learnings Learn approaches to falls assessment Understand inter-relationship between promoting safe
4/26/2012. Laura Grooms, MD Assistant Professor Geriatric Medicine Department of Family and Geriatric Medicine University of Louisville April 20, 2012
 Laura Grooms, MD Assistant Professor Geriatric Medicine Department of Family and Geriatric Medicine University of Louisville April 20, 2012 Laura Grooms, MD Assistant Professor Geriatric Medicine Department
Laura Grooms, MD Assistant Professor Geriatric Medicine Department of Family and Geriatric Medicine University of Louisville April 20, 2012 Laura Grooms, MD Assistant Professor Geriatric Medicine Department
Delirium in the Elderly
 Delirium in the Elderly ELITE 2017 Liza Genao, MD Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity Very much under-recognized
Delirium in the Elderly ELITE 2017 Liza Genao, MD Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity Very much under-recognized
GUIDELINES: Referral Guidelines to Nelson Tasman Hospice Service including Clinical Criteria for Patients
 GUIDELINES: Referral Guidelines to Nelson Tasman Hospice Service including Clinical Criteria for Patients Overview Admission to the hospice service is NOT diagnosis specific and includes all patients with
GUIDELINES: Referral Guidelines to Nelson Tasman Hospice Service including Clinical Criteria for Patients Overview Admission to the hospice service is NOT diagnosis specific and includes all patients with
Depression and Suicidal Ideation among Institutionalized and Non-Institutionalized Elders. Godishala Sridevi. GEMS Health Care, Masabtank, Hyderabad
 International International Multidisciplinary Multidisciplinary e-journal e Journal/ Godishala Sridevi (213-224) ISSN 2277-4262 Depression and Suicidal Ideation among Institutionalized and Non-Institutionalized
International International Multidisciplinary Multidisciplinary e-journal e Journal/ Godishala Sridevi (213-224) ISSN 2277-4262 Depression and Suicidal Ideation among Institutionalized and Non-Institutionalized
Changing care systems for people with frailty. John Young
 Changing care systems for people with frailty John Young Geriatrician, Bradford Hospitals Trust, UK National Clinical Director for Integration & the Frail Elderly, NHS England (john.young@bthft.nhs.uk)
Changing care systems for people with frailty John Young Geriatrician, Bradford Hospitals Trust, UK National Clinical Director for Integration & the Frail Elderly, NHS England (john.young@bthft.nhs.uk)
HOMES AND SENIORS SERVICES. APPROVAL DATE: February 2011 REVISION DATE: July 2018
 Page 1 of 7 POLICY: Each resident s level of nutrition and hydration risk will be identified by the Registered Dietitian during the RAI-MDS Admission Assessment and thereafter during the quarterly, significant
Page 1 of 7 POLICY: Each resident s level of nutrition and hydration risk will be identified by the Registered Dietitian during the RAI-MDS Admission Assessment and thereafter during the quarterly, significant
Appendix 1: Service self-assessment
 Appendix 1: Service self-assessment Frailty Screening Are we delivering high-quality care for frail older people? We are assessing for frailty in people aged 65+ at every entry into the service using a
Appendix 1: Service self-assessment Frailty Screening Are we delivering high-quality care for frail older people? We are assessing for frailty in people aged 65+ at every entry into the service using a
When and How to Screen for Common Geriatric Conditions Among Older Adults in Primary Care -
 When and How to Screen for Common Geriatric Conditions Among Older Adults in Primary Care - Randall W. Rupper, MD, MPH Rocky Mountain Geriatrics Conference August 29, 2016 When to screen? Tailoring to
When and How to Screen for Common Geriatric Conditions Among Older Adults in Primary Care - Randall W. Rupper, MD, MPH Rocky Mountain Geriatrics Conference August 29, 2016 When to screen? Tailoring to
Practical Management of the Delirious Patient with Mental Retardation by the Nurse Anesthetist
 Practical Management of the Delirious Patient with Mental Retardation by the Nurse Anesthetist 1. Basic Facts on Delirium The nurse anesthetist plays an important role in prevention of delirium among surgical
Practical Management of the Delirious Patient with Mental Retardation by the Nurse Anesthetist 1. Basic Facts on Delirium The nurse anesthetist plays an important role in prevention of delirium among surgical
Evaluation of fragility and factors influencing falls in nursing homes. Dr Marie-Laure Seux Geriatrics Broca Hospital May 2013
 Evaluation of fragility and factors influencing falls in nursing homes Dr Marie-Laure Seux Geriatrics Broca Hospital May 2013 Epidemiological data Among the over 65s: 1/3 present at least one fall per
Evaluation of fragility and factors influencing falls in nursing homes Dr Marie-Laure Seux Geriatrics Broca Hospital May 2013 Epidemiological data Among the over 65s: 1/3 present at least one fall per
homeinstead.com Each Home Instead Senior Care franchise office is independently owned and operated Home Instead, Inc.
 Each Home Instead Senior Care franchise office is independently owned and operated. 2010 Home Instead, Inc. homeinstead.com Many of us may joke about having old timers disease, but when cognitive impairment
Each Home Instead Senior Care franchise office is independently owned and operated. 2010 Home Instead, Inc. homeinstead.com Many of us may joke about having old timers disease, but when cognitive impairment
Biological theory for the construct of intrinsic capacity to be used in clinical settings Matteo Cesari, MD, PhD
 Biological theory for the construct of intrinsic capacity to be used in clinical settings Matteo Cesari, MD, PhD World Health Organization Geneva (Switzerland) December 1, 2016 World Health Organization.
Biological theory for the construct of intrinsic capacity to be used in clinical settings Matteo Cesari, MD, PhD World Health Organization Geneva (Switzerland) December 1, 2016 World Health Organization.
Delirium in the Elderly
 Delirium in the Elderly ELITE 2015 Mamata Yanamadala M.B.B.S, MS Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity
Delirium in the Elderly ELITE 2015 Mamata Yanamadala M.B.B.S, MS Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity
Comprehensive Assessment of the Frail Older Patient
 Comprehensive Assessment of the Frail Older Patient Executive Summary Comprehensive geriatric assessment (CGA) is a multidimensional and usually interdisciplinary diagnostic process designed to determine
Comprehensive Assessment of the Frail Older Patient Executive Summary Comprehensive geriatric assessment (CGA) is a multidimensional and usually interdisciplinary diagnostic process designed to determine
MOVE ON: Mobilization Of Vulnerable Elders In Ontario. How Can We Keep Our Patients Moving?
 MOVE ON: Mobilization Of Vulnerable Elders In Ontario Or How Can We Keep Our Patients Moving? Objectives After participating in this educational session, interprofessional team members will be able to:
MOVE ON: Mobilization Of Vulnerable Elders In Ontario Or How Can We Keep Our Patients Moving? Objectives After participating in this educational session, interprofessional team members will be able to:
20th June Integrated Care in Sunderland: Guide to Risk Stratification
 20th June 2017 Integrated Care in Sunderland: Guide to Risk Stratification Table of Contents Integrated Care in Sunderland:... 1 Guide to Risk Stratification... 1 Table of Contents... 2 Background... 3
20th June 2017 Integrated Care in Sunderland: Guide to Risk Stratification Table of Contents Integrated Care in Sunderland:... 1 Guide to Risk Stratification... 1 Table of Contents... 2 Background... 3
What is Frailty? National Background and Local Pathways
 What is Frailty? National Background and Local Pathways Learning Outcomes At the end of the session you will be able to :Know where to go to look at key national resources on frailty. Define frailty. Screen
What is Frailty? National Background and Local Pathways Learning Outcomes At the end of the session you will be able to :Know where to go to look at key national resources on frailty. Define frailty. Screen
Nutrition to prevent and treat sarcopenia in older people
 1 Nutrition to prevent and treat sarcopenia in older people Alfonso J. Cruz-Jentoft Hospital Universitario Ramón y Cajal Madrid, Spain Roma, 17 dicembre 2014 + The objective of Gerontology is not to increase
1 Nutrition to prevent and treat sarcopenia in older people Alfonso J. Cruz-Jentoft Hospital Universitario Ramón y Cajal Madrid, Spain Roma, 17 dicembre 2014 + The objective of Gerontology is not to increase
Frailty: Challenges and Possible Solutions
 Frailty: Challenges and Possible Solutions EMA Workshop: Ensuring safe and effective medicines for an ageing population Niccolò Marchionni Professor of Geriatrics University of Florence, Italy 22-23 March
Frailty: Challenges and Possible Solutions EMA Workshop: Ensuring safe and effective medicines for an ageing population Niccolò Marchionni Professor of Geriatrics University of Florence, Italy 22-23 March
Depression among Older Adults. Prevalence & Intervention Strategies
 Depression among Older Adults Prevalence & Intervention Strategies Definition Depression is a complex syndrome complex characterized by mood disturbance plus variety of cognitive, psychological, and vegetative
Depression among Older Adults Prevalence & Intervention Strategies Definition Depression is a complex syndrome complex characterized by mood disturbance plus variety of cognitive, psychological, and vegetative
ME/CFS : stakeholder engagement meeting. Issues for people with severe ME/CFS
 People s experiences of living with ME/CFS or caring for people with ME/CFS Stakeholders discussed their experience of ME/CFS. The condition is characterised by great variability of severity and with symptoms
People s experiences of living with ME/CFS or caring for people with ME/CFS Stakeholders discussed their experience of ME/CFS. The condition is characterised by great variability of severity and with symptoms
Frailty in Older Adults. Farshad Sharifi, MD, MPH Elderly Health Research Center
 Frailty in Older Adults Farshad Sharifi, MD, MPH Elderly Health Research Center 1 Outlines Definition of frailty Significance of frailty Conceptual Frailty Models Pathogenesis of frailty Management of
Frailty in Older Adults Farshad Sharifi, MD, MPH Elderly Health Research Center 1 Outlines Definition of frailty Significance of frailty Conceptual Frailty Models Pathogenesis of frailty Management of
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative
 Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Atypical Presentation. Atypical Presentation Part II
 Atypical Presentation Part II Atypical Presentation in Acutely Ill Older Adults Head to Toe Assessment General Weakness/FTT The Frailty Syndrome/Phenotype Dr. Peter O Connor Geriatrician Feb 2008 Physical
Atypical Presentation Part II Atypical Presentation in Acutely Ill Older Adults Head to Toe Assessment General Weakness/FTT The Frailty Syndrome/Phenotype Dr. Peter O Connor Geriatrician Feb 2008 Physical
Test and Learn Community Frailty Service for frail housebound patients and those living in care homes in South Gloucestershire
 Test and Learn Community Frailty Service for frail housebound patients and those living in care homes in South Gloucestershire Introduction This document introduces South Gloucestershire Clinical Commissioning
Test and Learn Community Frailty Service for frail housebound patients and those living in care homes in South Gloucestershire Introduction This document introduces South Gloucestershire Clinical Commissioning
The webinar, Multimorbidity in Canada, will begin shortly.
 The webinar, Multimorbidity in Canada, will begin shortly. For first-time WebEx users: Follow the instructions that appear on your screen and choose your audio preference (phone or computer). To change
The webinar, Multimorbidity in Canada, will begin shortly. For first-time WebEx users: Follow the instructions that appear on your screen and choose your audio preference (phone or computer). To change
DELIRIUM DR S A R A H A B D E L A T I S A S DR H I L A R Y W O L F E N D A L E S T 4
 DELIRIUM DR S A R A H A B D E L A T I S A S DR H I L A R Y W O L F E N D A L E S T 4 AIMS Define delirium Identify: Different types of delirium Risk factors Preventable causes Screening tools Management
DELIRIUM DR S A R A H A B D E L A T I S A S DR H I L A R Y W O L F E N D A L E S T 4 AIMS Define delirium Identify: Different types of delirium Risk factors Preventable causes Screening tools Management
Fall Prevention is Everyone s Business. Types of Falls. What is a Fall 7/8/2016
 Fall Prevention is Everyone s Business Part 1 Prof (Col) Dr RN Basu Adviser, Quality & Academics Medica Superspecilalty Hospital & Executive Director Academy of Hospital Administration Kolkata Chapter
Fall Prevention is Everyone s Business Part 1 Prof (Col) Dr RN Basu Adviser, Quality & Academics Medica Superspecilalty Hospital & Executive Director Academy of Hospital Administration Kolkata Chapter
Mental and Physical Health and Abuse. Presented by Dr. Sally MacDonald Reagan Gale, PhD, R. Psych.
 Mental and Physical Health and Abuse Presented by Dr. Sally MacDonald Reagan Gale, PhD, R. Psych. October 28 2014 Overview Introduction 3 D s of aging Substance use disorder in older adults Elder abuse
Mental and Physical Health and Abuse Presented by Dr. Sally MacDonald Reagan Gale, PhD, R. Psych. October 28 2014 Overview Introduction 3 D s of aging Substance use disorder in older adults Elder abuse
Frailty and Sarcopenia
 Frailty and Sarcopenia Hans Hobbelen Professor in Healthy lifestyle, Ageing and Health Care Hanze University of Applied Sciences Groningen Lotte Kunst Master Geriatric physical therapist Careyn Utrecht
Frailty and Sarcopenia Hans Hobbelen Professor in Healthy lifestyle, Ageing and Health Care Hanze University of Applied Sciences Groningen Lotte Kunst Master Geriatric physical therapist Careyn Utrecht
CARE OF SPINAL CORD INJURY VICTIMS
 CARE OF SPINAL CORD INJURY VICTIMS Dr THIERRY ALBERT Centre de Rééducation et de Réadaptation pour Adulte de COUBERT Route de Liverdy, Coubert 77257 Brie comte robert, cedex talbert@ugecamif.fr Spinal
CARE OF SPINAL CORD INJURY VICTIMS Dr THIERRY ALBERT Centre de Rééducation et de Réadaptation pour Adulte de COUBERT Route de Liverdy, Coubert 77257 Brie comte robert, cedex talbert@ugecamif.fr Spinal
Past Surgical History
 Name: DOB: Check All That Apply Past Medical History o Anemia o Aneurysm o Asthma o Bipolar o Bleeding Disorder o Blood Clot o Brain Tumor o Bronchitis o Cancer o Crohn s Disease/Ulcerative Colitis o Depression
Name: DOB: Check All That Apply Past Medical History o Anemia o Aneurysm o Asthma o Bipolar o Bleeding Disorder o Blood Clot o Brain Tumor o Bronchitis o Cancer o Crohn s Disease/Ulcerative Colitis o Depression
Integrating Geriatrics into Oncology Care
 Integrating Geriatrics into Oncology Care William Dale, MD, PhD Chief, Geriatrics & Palliative Medicine Director, Specialized Oncology Care & Research in the Elderly (SOCARE) Clinic University of Chicago
Integrating Geriatrics into Oncology Care William Dale, MD, PhD Chief, Geriatrics & Palliative Medicine Director, Specialized Oncology Care & Research in the Elderly (SOCARE) Clinic University of Chicago
Alison Burton-Shepherd PGCAP (ed) FHEA R Nutr (Scientist) MSc BSc (Hons) RGN Queens Nurse
 FHEA R Nutr (Scientist) MSc BSc (Hons) RGN Queens Nurse") Alison Burton-Shepherd PGCAP (ed) FHEA R Nutr (Scientist) MSc BSc (Hons) RGN Queens Nurse 3 million individuals in the UK are at risk of developing malnutrition 93% of these individuals live alone in the
Alison Burton-Shepherd PGCAP (ed) FHEA R Nutr (Scientist) MSc BSc (Hons) RGN Queens Nurse 3 million individuals in the UK are at risk of developing malnutrition 93% of these individuals live alone in the