Palliative Care Emergencies. Additional module if needed
|
|
|
- Amice Charles
- 5 years ago
- Views:
Transcription
1 Palliative Care Emergencies Additional module if needed
2 Learning objectives Understand emergency /urgent / important Describe common emergencies in PC Explore principles of essential management Outline management for specific common emergencies in PC
3 Questions In any given situation we must use knowledge know what we could do skill know what we should do attitude know how we should do diplomacy know what the patient wants us to do / not do judgement make an active/ negotiated decision
4 Emergencies severe pain confusion spinal cord compression fractures metabolic - hypercalcaemia seizures haemorrhage superior vena cava obstruction respiratory obstruction

5 Total Pain PHYSICAL EMOTIONAL SOCIAL SPIRITUAL
6 Confusion confusion up to 75% patients advanced illness often fluctuates terminal restlessness (mild) terminal delerium (severe)
7 Confusion Causes biochemical / drugs pain cerebral irritation infection constipation / retention hypoxia / respiratory distress anxiety / spiritual distress
8 Confusion Management treat reversible causes stop medications / insert catheter / start antibiotics / treat constipation adjust environment familiar voices, music, soft lighting, avoid loud noise / don t use restraints explain / support family needs pharmacological intervention
9 Confusion Management use sedatives symptom relief neuroleptics - anxiolyic /antipsychotic haloperidol / olanzepine / chlorpromazine haloperidol 5mg po/sc as required and repeat benzodiazepines - anxiolytic / sedative midazolam / lorazepam / diazepam midazolam 2.5mg sc / diazepam 5mg od
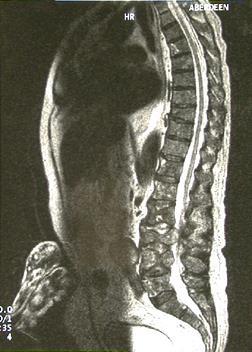
10 Spinal Cord Compression Incidence 3% patients advanced cancer > one level 20% common breast bronchus prostate
11 Spinal Cord Compression Mechanism metastatic spread to bone 85% direct tumour extension 10% intramedullary primary 4% haematogenous spread to epidural space 1%
12 Spinal Cord Compression Presentation pain >90% weakness >75% sensory level >50% sphincter dysfunction >40% nb. pain usually predates other symptoms
13 Spinal Cord Compression Diagnosis history and clinical findings plain x-ray?bone scan?mri?ct / myelogram
14
15 Spinal Cord Compression Management corticosteroids dexamethasone 16-32mg radiotherapy as soon as possible surgery
16 Spinal Cord Compression Outcome poor prognosis loss of sphincter control rapid onset complete paraplegia better prognosis early detection and treatment cauda equina lesion incompete paraplegia

17

18
19
20 Fracture common with metastatic bone disease may be terminal event management anticipate radiotherapy surgery neuraxial therapies

21

22

23
24 Hypercalcaemia commonest metabolic complication rate of rise determines emergency common up to 50% breast and myeloma lung / renal / cervix / head and neck diagnosis thirst / polyuria / confusion / pain / nausea and vomiing / constipation / dehydration / coma
25 Hypercalcaemia investigation serum calcium / albumin / renal function management rehydrate bisphosphonates pamidronate 60mg treat underlying disease
26 Seizures Causes cerebral metastases cerebral infection / oedema cerebral haemorrhage biochemical derangement premorbid epilepsy
27 Seizures Treatment emergency maintain airway pharmacology diazepam 10mg pr midazolam 5-10mg sc/iv phenobarbitol 100mg sc or in 100mls saline over 30mins consider steroids
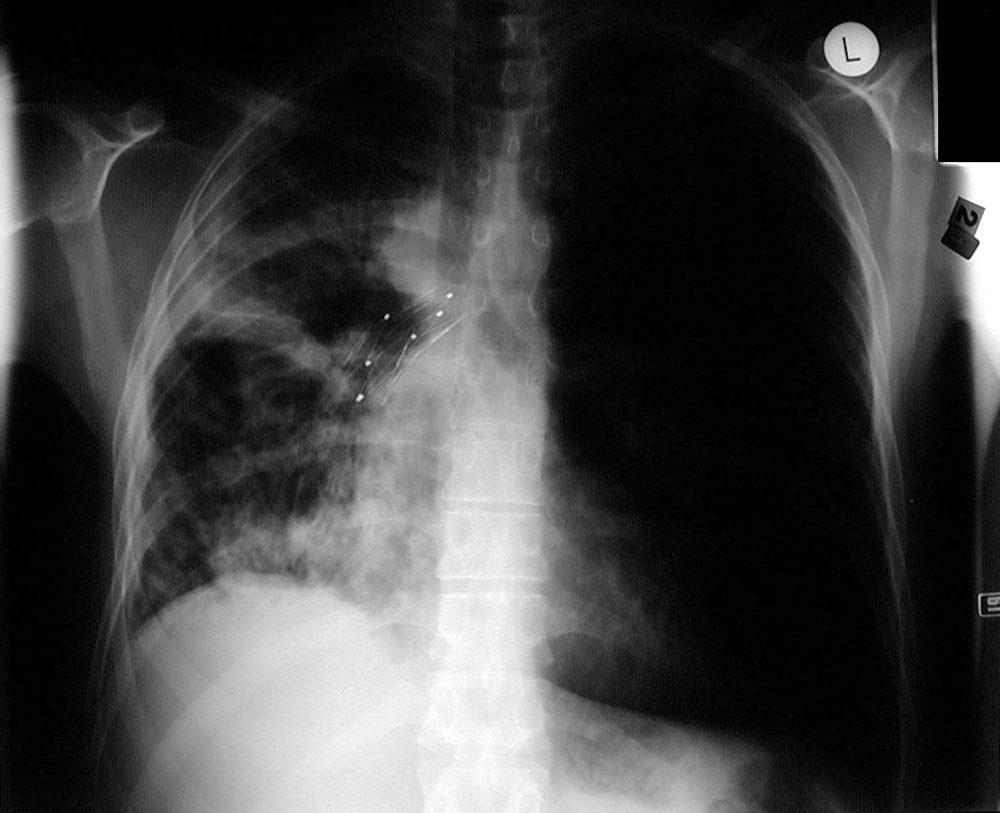
28 Haemorrhage fear often worse than reality more common GI / lung / pelvic / head and neck management radiotherapy surgery
29 Haemorrhage Management topical mild oozing topical sucralfate moderate oozing dilute hemloc (adrenaline 1:1000 soaked swab)
30 Haemorrhage Management oral ethamsylate 500mg QID (tranexamic acid) sucralfate 1g bd-qds 1% alum bladder irrigation
31 Massive Haemorrhage Management anticipate prevent (if possible) keep calm skilled person (if available) sedation (if possible) benzodiazepine / morphine vaginal pack / local measures / surgery
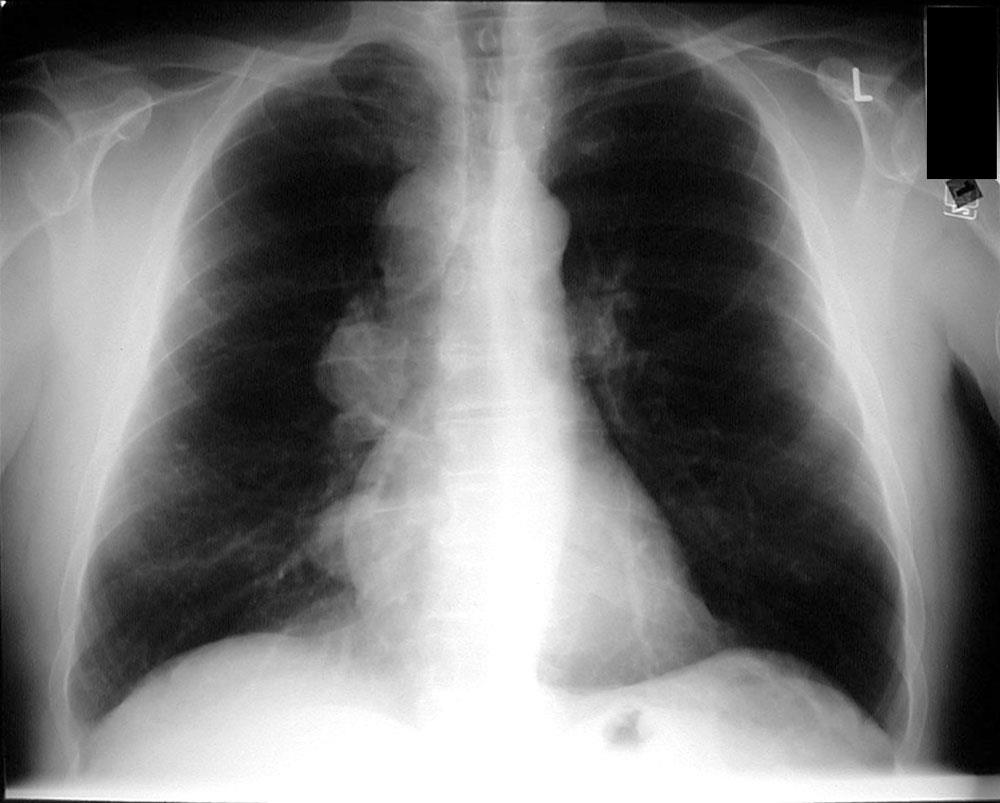
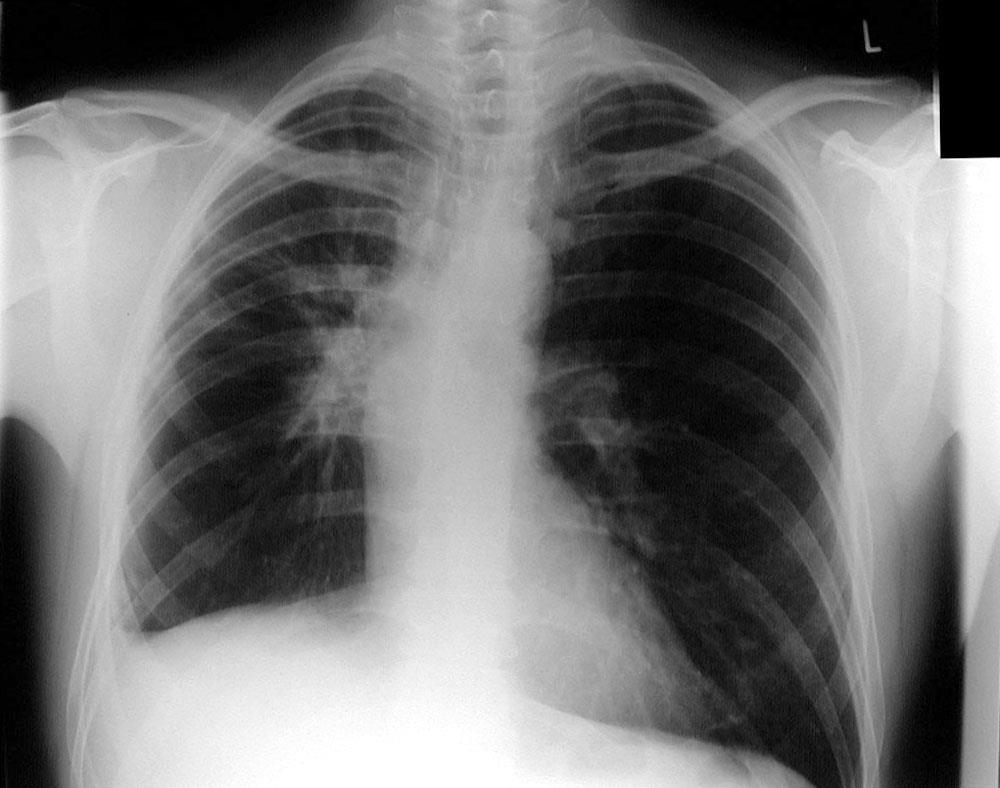
32 SVCO Superior venal cava obstruction 75% SVCO is in lung carcinoma extrinsic compression / mediastinum symptoms/signs depend on extent and speed of development symptoms worse on lying flat facial +/- arm swelling engorged neck and chest wall veins
33 SVCO Management stat iv dexamethasone 8-16mg then po?urgent referral for radiotherapy stent?chemotherapy
34 Respiratory Obstruction acute reversible or irreversible? relieve symptoms regardless of cause Pharmacological parenteral morphine s/l lorazepam mg PRN / parenteral midazolam?steroids - dexamethasone Non-pharmacological fan, presence
35 Stridor acute stridor is very rare iv dexamethasone stat iv midazolam, if severe agitation? referral for stent /DXT
36
37
38
39 Conclusions can be physical, social, spiritual, psychological can cause team tension challenge opportunity bridges specialties teamwork

40 These resources are developed as part of the THET multi-country project whose goal is to strengthen and integrate palliative care into national health systems through a public health primary care approach Acknowledgement given to Cairdeas International Palliative Care Trust and MPCU for their preparation and adaptation part of the teaching materials for the Palliative Care Toolkit training with modules as per the Training Manual can be used as basic PC presentations when facilitators are encouraged to adapt and make contextual
Palliative Care Emergencies
 Palliative Care Emergencies LAURA BARNFIELD What might constitute an emergency in Palliative Care? 1 Palliative Care Emergencies Major haemorrhage Metastatic Spinal Cord Compression (MSCC) Superior Vena
Palliative Care Emergencies LAURA BARNFIELD What might constitute an emergency in Palliative Care? 1 Palliative Care Emergencies Major haemorrhage Metastatic Spinal Cord Compression (MSCC) Superior Vena
Palliative Care Emergencies. Dr Debbie Quinn Associate Specialist in Palliative Medicine, Isabel Hospice
 Palliative Care Emergencies Dr Debbie Quinn Associate Specialist in Palliative Medicine, Isabel Hospice Factors in dealing with emergencies in palliative care The general physical condition of the patient
Palliative Care Emergencies Dr Debbie Quinn Associate Specialist in Palliative Medicine, Isabel Hospice Factors in dealing with emergencies in palliative care The general physical condition of the patient
Emergencies in Palliative Medicine
 Emergencies in Palliative Medicine Objectives Recognise palliative care emergencies Be aware of their existence Recognise signs and symptoms of common emergencies Anticipate occurrence of emergencies Manage
Emergencies in Palliative Medicine Objectives Recognise palliative care emergencies Be aware of their existence Recognise signs and symptoms of common emergencies Anticipate occurrence of emergencies Manage
Palliative Care Emergencies
 Palliative Care Emergencies Dr. T. Thirukkumaran Palliative Care Services Northwest Tasmania What are the emergencies in Palliative Medicine? Palliative Emergencies (a) Disease related or Symptom related
Palliative Care Emergencies Dr. T. Thirukkumaran Palliative Care Services Northwest Tasmania What are the emergencies in Palliative Medicine? Palliative Emergencies (a) Disease related or Symptom related
Palliative Emergencies. Ken Stakiw
 Palliative Emergencies Ken Stakiw Disclosure None to disclose for this lecture Have received honoraria from a number of agencies and companies previously Intend to discuss some off label use of medications
Palliative Emergencies Ken Stakiw Disclosure None to disclose for this lecture Have received honoraria from a number of agencies and companies previously Intend to discuss some off label use of medications
Regional Breathlessness Audit - Case Note Survey. 1. Introduction. Regional Breathlessness Audit - Case Note Survey. 2.
 Regional Breathlessness Audit - Case te Survey 1. Introduction Please complete this form for your case note review. Cases used may be PROSPECTIVE AND/OR RETROSPECTIVE. Please log as many cases as you can.
Regional Breathlessness Audit - Case te Survey 1. Introduction Please complete this form for your case note review. Cases used may be PROSPECTIVE AND/OR RETROSPECTIVE. Please log as many cases as you can.
FACTSHEET 16 ON PALLIATIVE CARE EMERGENCIES IN PALLIATIVE CARE
 FACTSHEET 16 ON PALLIATIVE CARE EMERGENCIES IN PALLIATIVE CARE See also Cambridgeshire Community Services policy for anticipatory prescribing for patients with a terminal illness ( Just in Case ) http://www.cambridgeshireandpeterboroughccg.nhs.uk/downloads/catch/just_in_case_
FACTSHEET 16 ON PALLIATIVE CARE EMERGENCIES IN PALLIATIVE CARE See also Cambridgeshire Community Services policy for anticipatory prescribing for patients with a terminal illness ( Just in Case ) http://www.cambridgeshireandpeterboroughccg.nhs.uk/downloads/catch/just_in_case_
SYMPTOM MANAGEMENT GUIDANCE FOR PATIENTS RECEIVING PALLIATIVE CARE AT ROYAL DERBY HOSPITAL
 SYMPTOM MANAGEMENT GUIDANCE FOR PATIENTS RECEIVING PALLIATIVE CARE AT ROYAL DERBY HOSPITAL If a patient is believed to be approaching the end of their life, medication should be prescribed in anticipation
SYMPTOM MANAGEMENT GUIDANCE FOR PATIENTS RECEIVING PALLIATIVE CARE AT ROYAL DERBY HOSPITAL If a patient is believed to be approaching the end of their life, medication should be prescribed in anticipation
In our patients the cause of seizures can be broadly divided into structural and systemic causes.
 Guidelines for the management of Seizures Amalgamation and update of previous policies 7 (Seizure guidelines, ND, 2015) and 9 (Status epilepticus, KJ, 2011) Seizures can occur in up to 15% of the Palliative
Guidelines for the management of Seizures Amalgamation and update of previous policies 7 (Seizure guidelines, ND, 2015) and 9 (Status epilepticus, KJ, 2011) Seizures can occur in up to 15% of the Palliative
F I O N A F I N L A Y C O N S U L T A N T I N P A L L I A T I V E M E D I C I N E Q U E E N E L I Z A B E T H U N I V E R S I T Y H O S P I T A L F I
 F I O N A F I N L A Y C O N S U L T A N T I N P A L L I A T I V E M E D I C I N E Q U E E N E L I Z A B E T H U N I V E R S I T Y H O S P I T A L F I O N A F I N L A Y @ N H S. N E T Clinical focus, case
F I O N A F I N L A Y C O N S U L T A N T I N P A L L I A T I V E M E D I C I N E Q U E E N E L I Z A B E T H U N I V E R S I T Y H O S P I T A L F I O N A F I N L A Y @ N H S. N E T Clinical focus, case
Agitation. Susan Emmens Palliative Care Clinical Nurse Specialist
 Agitation Susan Emmens Palliative Care Clinical Nurse Specialist Definitions Restlessness finding or affording no rest, uneasy, agitated. Constantly in motion fidgeting Agitation shaking, moving, mental
Agitation Susan Emmens Palliative Care Clinical Nurse Specialist Definitions Restlessness finding or affording no rest, uneasy, agitated. Constantly in motion fidgeting Agitation shaking, moving, mental
PAIN MANAGEMENT Person established taking oral morphine or opioid naive.
 PAIN MANAGEMENT Person established taking oral morphine or opioid naive. Important; it is the responsibility of the prescriber to ensure that guidelines are followed when prescribing opioids. Every member
PAIN MANAGEMENT Person established taking oral morphine or opioid naive. Important; it is the responsibility of the prescriber to ensure that guidelines are followed when prescribing opioids. Every member
PAIN MANAGEMENT Patient established on oral morphine or opioid naive.
 PAIN MANAGEMENT Patient established on oral morphine or opioid naive. Important; It is the responsibility of the prescriber to ensure that guidelines are followed when prescribing opioids. Every member
PAIN MANAGEMENT Patient established on oral morphine or opioid naive. Important; It is the responsibility of the prescriber to ensure that guidelines are followed when prescribing opioids. Every member
Breathlessness in advanced disease. February 2017
 Breathlessness in advanced disease February 2017 Breathlessness Managing breathlessness in primary care Chronic breathlessness Acute exacerbation of breathlessness Breathlessness at end of life Breathlessness
Breathlessness in advanced disease February 2017 Breathlessness Managing breathlessness in primary care Chronic breathlessness Acute exacerbation of breathlessness Breathlessness at end of life Breathlessness
Oncologic Emergencies: When to call the Radiation Oncologist
 Oncologic Emergencies: When to call the Radiation Oncologist Dr. Shrinivas Rathod Radiation Oncologist Radiation Oncology Program CancerCare Manitoba and University of Manitoba Disclosures Speaker s name:
Oncologic Emergencies: When to call the Radiation Oncologist Dr. Shrinivas Rathod Radiation Oncologist Radiation Oncology Program CancerCare Manitoba and University of Manitoba Disclosures Speaker s name:
Symptom Management Guidelines for End of Life Care
 Symptom Management Guidelines for End of Life Care The following pages are guidelines for the management of common symptoms in the last few days of life. General principles: 1. Consider how symptoms can
Symptom Management Guidelines for End of Life Care The following pages are guidelines for the management of common symptoms in the last few days of life. General principles: 1. Consider how symptoms can
Symptom Management Pocket Guides: DELIRIUM
 Symptom Management Pocket Guides: DELIRIUM August 2010 DELIRIUM Page Considerations. 1 Assessment 2 Diagnosis. 3 Non-Pharmacological treatment 3 Pharmacological treatment. 5 Mild Delirium... 6 Moderate
Symptom Management Pocket Guides: DELIRIUM August 2010 DELIRIUM Page Considerations. 1 Assessment 2 Diagnosis. 3 Non-Pharmacological treatment 3 Pharmacological treatment. 5 Mild Delirium... 6 Moderate
Spinal Cord Compression Diagnosis and Management. Information for Shared Care Centres and Community Staff
 Reference: CG1412 Written by: Dr Daniel Yeomanson Peer reviewer Dr Jeanette Payne Approved: August 2016 Approved by D&TC: 10 th June 2016 Review Due: August 2019 Intended Audience This document contains
Reference: CG1412 Written by: Dr Daniel Yeomanson Peer reviewer Dr Jeanette Payne Approved: August 2016 Approved by D&TC: 10 th June 2016 Review Due: August 2019 Intended Audience This document contains
BREATHLESSNESS MANAGEMENT
 Guideline Name: Breathlessness BACKGROUND Breathlessness is a common symptom in patients with cancer, end-stage heart failure and end-stage chronic obstructive pulmonary disease (COPD). There are many
Guideline Name: Breathlessness BACKGROUND Breathlessness is a common symptom in patients with cancer, end-stage heart failure and end-stage chronic obstructive pulmonary disease (COPD). There are many
PRESCRIBING GUIDELINES FOR SYMPTOM MANAGEMENT IN THE DYING PATIENT
 PRESCRIBING GUIDELINES FOR SYMPTOM MANAGEMENT IN THE DYING PATIENT A collaboration between: St. Rocco s Hospice, Bridgewater Community Healthcare NHS Trust, NHS Warrington Clinical Commissioning Group,
PRESCRIBING GUIDELINES FOR SYMPTOM MANAGEMENT IN THE DYING PATIENT A collaboration between: St. Rocco s Hospice, Bridgewater Community Healthcare NHS Trust, NHS Warrington Clinical Commissioning Group,
Managing Respiratory Symptoms - Breathlessness, Cough and Secretions. Dr Laura Healy. Palliative Medicine Registrar, Beaumont Hospital.
 Managing Respiratory Symptoms - Breathlessness, Cough and Secretions. Dr Laura Healy. Palliative Medicine Registrar, Beaumont Hospital. Things to consider: 1. Very common symptoms. 2. Can occur in any
Managing Respiratory Symptoms - Breathlessness, Cough and Secretions. Dr Laura Healy. Palliative Medicine Registrar, Beaumont Hospital. Things to consider: 1. Very common symptoms. 2. Can occur in any
Palliative care for patients with brain cancer
 Palliative care for patients with brain cancer Lyn Cave Clinical Nurse Specialist Palliative Care Hospital2Home (H2H) Dr Jayne Wood Clinical Lead Palliative Care The Royal Marsden and Royal Brompton Palliative
Palliative care for patients with brain cancer Lyn Cave Clinical Nurse Specialist Palliative Care Hospital2Home (H2H) Dr Jayne Wood Clinical Lead Palliative Care The Royal Marsden and Royal Brompton Palliative
Approach to symptom control near the end-of-life
 Approach to symptom control near the end-of-life 18 Sept 2011 Dr Alethea Yee Senior Consultant, Department of Palliative Medicine National Cancer Centre,Singapore What is end of life? No precise definition
Approach to symptom control near the end-of-life 18 Sept 2011 Dr Alethea Yee Senior Consultant, Department of Palliative Medicine National Cancer Centre,Singapore What is end of life? No precise definition
Malignant Spinal cord Compression. Dr. Thiru Thirukkumaran Palliative Care Services - Northwest Tasmania
 Malignant Spinal cord Compression Dr. Thiru Thirukkumaran Palliative Care Services - Northwest Tasmania Background Statistics of SCC -1 Incidence of SCC Vertebral body metastases 85 % Para-vertebral (Lymphoma)
Malignant Spinal cord Compression Dr. Thiru Thirukkumaran Palliative Care Services - Northwest Tasmania Background Statistics of SCC -1 Incidence of SCC Vertebral body metastases 85 % Para-vertebral (Lymphoma)
1. GUIDELINES FOR THE MANAGEMENT OF AGITATION IN ADVANCED CANCER
 1. GUIDELINES FOR THE MANAGEMENT OF AGITATION IN ADVANCED CANCER 1.1 GENERAL PRINCIPLES There are many causes of agitation in palliative care patients, which makes recommendations for treatment difficult.
1. GUIDELINES FOR THE MANAGEMENT OF AGITATION IN ADVANCED CANCER 1.1 GENERAL PRINCIPLES There are many causes of agitation in palliative care patients, which makes recommendations for treatment difficult.
MMG035 Symptom Management Guidelines for a Person thought to be in the Last Few Days and Hours of Life
 MMG035 Symptom Management Guidelines for a Person thought to be in the Last Few Days and Hours of Life The following pages are guidelines for the management of common symptoms for a person thought to be
MMG035 Symptom Management Guidelines for a Person thought to be in the Last Few Days and Hours of Life The following pages are guidelines for the management of common symptoms for a person thought to be
Waterloo Wellington (WW) Symptom Management Guideline for the End of Life (EOL) Medication Order Set for Long Term Care (LTC)
 Symptom Management Guideline for the End of Life (EOL) Medication Order Set for Long Term Care (LTC)") Waterloo Wellington (WW) Symptom Management Guideline for the End of Life (EOL) Medication Order Set for Long Term Care (LTC) May 2018 THE WATERLOO WELLINGTON SYMPTOM MANAGEMENT GUIDELINE FOR THE END OF
Waterloo Wellington (WW) Symptom Management Guideline for the End of Life (EOL) Medication Order Set for Long Term Care (LTC) May 2018 THE WATERLOO WELLINGTON SYMPTOM MANAGEMENT GUIDELINE FOR THE END OF
Management of Severe Agitation
 Management of Severe Agitation Key Points 1. The management of the severely agitated or violent patient embraces psychological, physical and pharmacological approaches. 2. Psychological methods focus on
Management of Severe Agitation Key Points 1. The management of the severely agitated or violent patient embraces psychological, physical and pharmacological approaches. 2. Psychological methods focus on
Palliative RT. Jiraporn Setakornnukul, M.D. Radiation Oncology Division Siriraj Hospital, Mahidol University
 Palliative RT Jiraporn Setakornnukul, M.D. Radiation Oncology Division Siriraj Hospital, Mahidol University Scope Brain metastasis Metastasis epidural spinal cord compression SVC obstruction Bone pain
Palliative RT Jiraporn Setakornnukul, M.D. Radiation Oncology Division Siriraj Hospital, Mahidol University Scope Brain metastasis Metastasis epidural spinal cord compression SVC obstruction Bone pain
 The last days of life Linda Magann CNC Palliative Care St George Hospital I m not afraid of dying, I just don t want to be there when it happens Woody Allen Palliative Care is an approach that improves
The last days of life Linda Magann CNC Palliative Care St George Hospital I m not afraid of dying, I just don t want to be there when it happens Woody Allen Palliative Care is an approach that improves
Emergency Control of the Acutely Disturbed Adult Patient GUIDELINES ON EMERGENCY CONTROL OF THE ACUTELY DISTURBED ADULT PATIENT... 2 ACTION...
 Delirium Toolkit Emergency Control of the Acutely Disturbed Adult Patient Table of Contents GUIDELINES ON EMERGENCY CONTROL OF THE ACUTELY DISTURBED ADULT PATIENT... 2 ACTION... 2 AFTERCARE... 3 NOTES...
Delirium Toolkit Emergency Control of the Acutely Disturbed Adult Patient Table of Contents GUIDELINES ON EMERGENCY CONTROL OF THE ACUTELY DISTURBED ADULT PATIENT... 2 ACTION... 2 AFTERCARE... 3 NOTES...
Delirium. Assessment and Management
 Delirium Assessment and Management Goals and Objectives Participants will: 1. be able to recognize and diagnose the syndrome of delirium. 2. understand the causes of delirium. 3. become knowledgeable about
Delirium Assessment and Management Goals and Objectives Participants will: 1. be able to recognize and diagnose the syndrome of delirium. 2. understand the causes of delirium. 3. become knowledgeable about
Emergencies in Palliative Care. Dr Alison Landon October 2018
 Emergencies in Palliative Care Dr Alison Landon October 2018 Learning Objectives Identify the major emergencies that can occur in palliative care and the causes Identify and discuss the signs and symptoms
Emergencies in Palliative Care Dr Alison Landon October 2018 Learning Objectives Identify the major emergencies that can occur in palliative care and the causes Identify and discuss the signs and symptoms
survey Parenteral anti-epileptics What is your experience? May July 2015
 Parenteral anti-epileptics What is your experience? May July 2015 Number of responses = 99 1a) In patients with pre-existing epilepsy controlled by PO medication that are imminently dying (prognosis
Parenteral anti-epileptics What is your experience? May July 2015 Number of responses = 99 1a) In patients with pre-existing epilepsy controlled by PO medication that are imminently dying (prognosis
Care in the Last Days of Life
 Care in the Last Days of Life Introduction This guideline is an aid to clinical decision making and good practice in person-centred care for patients who are deteriorating and at risk of dying. The patient
Care in the Last Days of Life Introduction This guideline is an aid to clinical decision making and good practice in person-centred care for patients who are deteriorating and at risk of dying. The patient
Learning Objectives. Delirium. Delirium. Delirium. Terminal Restlessness 3/28/2016
 Terminal Restlessness Dr. Christopher Churchill St. Cloud VA Health Care System EC&R Service Line Director & Medical Director Hospice & Palliative Care March 31, 2016 Learning Objectives Different Terminology
Terminal Restlessness Dr. Christopher Churchill St. Cloud VA Health Care System EC&R Service Line Director & Medical Director Hospice & Palliative Care March 31, 2016 Learning Objectives Different Terminology
Dyspnea: The top things you need to you know! Dr. Megan Sellick & Dr. Lawrence Lee Edmonton Zone Palliative Care Program
 : The top things you need to you know! Dr. Megan Sellick & Dr. Lawrence Lee Edmonton Zone Palliative Care Program Faculty / Presenter Disclosure Faculty: Dr. Lawrence Lee Relationships with commercial
: The top things you need to you know! Dr. Megan Sellick & Dr. Lawrence Lee Edmonton Zone Palliative Care Program Faculty / Presenter Disclosure Faculty: Dr. Lawrence Lee Relationships with commercial
Management of Delirium in Hospice Patients
 Presentation Objectives Management of Delirium in Hospice Patients Lynn Williams, BSPharm Clinical Pharmacist Hospice Pharmacy Solutions Identify the clinical features of delirium Understand the underlying
Presentation Objectives Management of Delirium in Hospice Patients Lynn Williams, BSPharm Clinical Pharmacist Hospice Pharmacy Solutions Identify the clinical features of delirium Understand the underlying
PAIN AND SYMPTOM MANAGEMENT GUIDANCE IN THE LAST DAYS OF LIFE
 PAIN AND SYMPTOM MANAGEMENT GUIDANCE IN THE LAST DAYS OF LIFE Reference: DCM029 Version: 1.1 This version issued: 07/06/18 Result of last review: Minor changes Date approved by owner (if applicable): N/A
PAIN AND SYMPTOM MANAGEMENT GUIDANCE IN THE LAST DAYS OF LIFE Reference: DCM029 Version: 1.1 This version issued: 07/06/18 Result of last review: Minor changes Date approved by owner (if applicable): N/A
Supporting Last Days of Life Symptom Control Medication Guidance: Algorithm. Agitation & Anxiety
 Agitation & Anxiety (Exclude or treat REVERSIBLE causes*) Patient is anxious / frightened, but lucid Patient is confused, agitated and / or hallucinating MIDAZOLAM 2.5-5mg s/c (Max total 24 hour dose of
Agitation & Anxiety (Exclude or treat REVERSIBLE causes*) Patient is anxious / frightened, but lucid Patient is confused, agitated and / or hallucinating MIDAZOLAM 2.5-5mg s/c (Max total 24 hour dose of
Nausea and Vomiting. Principles and Practice in End of Life Care November 2018
 Nausea and Vomiting Principles and Practice in End of Life Care November 2018 Overview Aims and Objectives Why is managing nausea and vomiting important? Definitions Causes Interventions pharmacological
Nausea and Vomiting Principles and Practice in End of Life Care November 2018 Overview Aims and Objectives Why is managing nausea and vomiting important? Definitions Causes Interventions pharmacological
Professor Dr. Saiyeedur Rahman Professor and Head Department of Medicine SBMCH, Barisal
 Professor Dr. Saiyeedur Rahman Professor and Head Department of Medicine SBMCH, Barisal What is Oncologic Emergency? An oncologic emergency is an acute, potentially life-threatening event resulting from
Professor Dr. Saiyeedur Rahman Professor and Head Department of Medicine SBMCH, Barisal What is Oncologic Emergency? An oncologic emergency is an acute, potentially life-threatening event resulting from
Management of Dyspnea and Cough in Lung Cancer
 Management of Dyspnea and Cough in Lung Cancer Dr. Chris Ogaranko Lung Cancer Educational Event November 2013 Presenter Disclosure Faculty: Dr. Chris Ogaranko Relationships with commercial interests: Grants/Research
Management of Dyspnea and Cough in Lung Cancer Dr. Chris Ogaranko Lung Cancer Educational Event November 2013 Presenter Disclosure Faculty: Dr. Chris Ogaranko Relationships with commercial interests: Grants/Research
Gastrointestinal obstruction Dr Iain Lawrie
 Gastrointestinal obstruction Dr Iain Lawrie Consultant and Honorary Clinical Senior Lecturer in Palliative Medicine The Pennine Acute Hospitals NHS Trust / The University of Manchester iain.lawrie@pat.nhs.uk
Gastrointestinal obstruction Dr Iain Lawrie Consultant and Honorary Clinical Senior Lecturer in Palliative Medicine The Pennine Acute Hospitals NHS Trust / The University of Manchester iain.lawrie@pat.nhs.uk
Hospice and Palliative Medicine
 Hospice and Palliative Medicine Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the
Hospice and Palliative Medicine Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the
Update on Management of Malignant Spinal Cord Compression. Heino Hugel Consultant in Palliative Medicine University Hospital Aintree
 Update on Management of Malignant Spinal Cord Compression Heino Hugel Consultant in Palliative Medicine University Hospital Aintree Current Guidelines The symptoms of MSCC may be subtle and therefore careful
Update on Management of Malignant Spinal Cord Compression Heino Hugel Consultant in Palliative Medicine University Hospital Aintree Current Guidelines The symptoms of MSCC may be subtle and therefore careful
Health Learning Partnership End of Life Care 29 th June 2016
 Health Learning Partnership End of Life Care 29 th June 2016 Beth Wright Consultant in Palliative Medicine Case 1 Malignant bowel obstruction Sarah is a 43 year old woman colon cancer, diagnosed in 2014.
Health Learning Partnership End of Life Care 29 th June 2016 Beth Wright Consultant in Palliative Medicine Case 1 Malignant bowel obstruction Sarah is a 43 year old woman colon cancer, diagnosed in 2014.
Cancer of Unknown Primary (CUP) Protocol
 Protocol") 1 Department of Oncology. Cancer of Unknown Primary (CUP) Protocol Version: Document type: Document sponsor Designation Document author [ s] Designation[s] Approving committee / Group Ratified by: Date
1 Department of Oncology. Cancer of Unknown Primary (CUP) Protocol Version: Document type: Document sponsor Designation Document author [ s] Designation[s] Approving committee / Group Ratified by: Date
Symptom Management in the Non-Verbal Patient at the End of Life Laura Carmon, ANP-BC
 Symptom Management in the Non-Verbal Patient at the End of Life Laura Carmon, ANP-BC 2017 NPSS Asheville, NC Objectives The learner will recognize non-verbal signs and symptoms commonly seen at the EOL.
Symptom Management in the Non-Verbal Patient at the End of Life Laura Carmon, ANP-BC 2017 NPSS Asheville, NC Objectives The learner will recognize non-verbal signs and symptoms commonly seen at the EOL.
Delirium and Nausea. Delirium - definition. Delirium Incidence. Predisposing Risk Factors for Delirium. Impact. Delirium Types 10/14/2016
 Delirium - definition Delirium and Nausea Etiologically non-specific global cerebral dysfunction associated with changes in LOC, attention, thinking, perception, memory, psychomotor behavior, emotion and
Delirium - definition Delirium and Nausea Etiologically non-specific global cerebral dysfunction associated with changes in LOC, attention, thinking, perception, memory, psychomotor behavior, emotion and
CLINICAL GUIDELINES FOR END OF LIFE CARE MEDICATIONS IN LONG TERM CARE HOMES
 CLINICAL GUIDELINES F END OF LIFE CARE MEDICATIONS IN LONG TERM CARE HOMES OPENING STATEMENT: Insert Facility Name is committed to providing effective end-of-life symptom management to all residents. Symptom
CLINICAL GUIDELINES F END OF LIFE CARE MEDICATIONS IN LONG TERM CARE HOMES OPENING STATEMENT: Insert Facility Name is committed to providing effective end-of-life symptom management to all residents. Symptom
Learn about Leptomeningeal Disease
 Learn about Leptomeningeal Disease Information for patients and caregivers Princess Margaret Read this resource to learn: What is leptomeningeal disease What are the symptoms of leptomeningeal disease
Learn about Leptomeningeal Disease Information for patients and caregivers Princess Margaret Read this resource to learn: What is leptomeningeal disease What are the symptoms of leptomeningeal disease
Management of the complications of myeloma and side-effects of treatment Christine Morris Clinical Nurse Specialist in Myeloma Royal Derby Hospital
 Management of the complications of myeloma and side-effects of treatment Christine Morris Clinical Nurse Specialist in Myeloma Royal Derby Hospital Common problems in myeloma Myeloma-related complications/symptoms
Management of the complications of myeloma and side-effects of treatment Christine Morris Clinical Nurse Specialist in Myeloma Royal Derby Hospital Common problems in myeloma Myeloma-related complications/symptoms
Palliative Prescribing - Pain
 Palliative Prescribing - Pain LAURA BARNFIELD 21/2/17 Aims To understand the classes of painkillers available in palliative care To gain confidence in counselling regarding opiates To gain confidence prescribing
Palliative Prescribing - Pain LAURA BARNFIELD 21/2/17 Aims To understand the classes of painkillers available in palliative care To gain confidence in counselling regarding opiates To gain confidence prescribing
For patients and their carers this means smoother symptom control, better support in a crisis, and avoidance of admission if that is their choice.
 Bedfordshire Palliative Care Palliative Care Medicines Guidance This folder has been produced to support professionals providing palliative care in any setting. Its aim is to make best practice in palliative
Bedfordshire Palliative Care Palliative Care Medicines Guidance This folder has been produced to support professionals providing palliative care in any setting. Its aim is to make best practice in palliative
Bone Metastases. Sukanda Denjanta, M.Sc., BCOP Pharmacy Department, Chiangrai Prachanukroh Hospital
 Bone Metastases Sukanda Denjanta, M.Sc., BCOP Pharmacy Department, Chiangrai Prachanukroh Hospital 1 Outline Pathophysiology Signs & Symptoms Diagnosis Treatment Spinal Cord Compression 2 General Information
Bone Metastases Sukanda Denjanta, M.Sc., BCOP Pharmacy Department, Chiangrai Prachanukroh Hospital 1 Outline Pathophysiology Signs & Symptoms Diagnosis Treatment Spinal Cord Compression 2 General Information
Bleeding Emergencies in Palliative Medicine. Dr. Julia Ridley CCFP(PC) / Fraser Health (RCH/BH) / UBC Asst Clin Professor / July 27, 2016
 / Fraser Health (RCH/BH) / UBC Asst Clin Professor / July 27, 2016") Bleeding Emergencies in Palliative Medicine Dr. Julia Ridley CCFP(PC) / Fraser Health (RCH/BH) / UBC Asst Clin Professor / July 27, 2016 Objectives Consider possible sites of bleeding Discuss general principles
Bleeding Emergencies in Palliative Medicine Dr. Julia Ridley CCFP(PC) / Fraser Health (RCH/BH) / UBC Asst Clin Professor / July 27, 2016 Objectives Consider possible sites of bleeding Discuss general principles
The last days of life in hospital and at home
 The last days of life in hospital and at home Beaumont Multi-disciplinary Palliative Care Study Day 28/9/2017 Dr Sarah McLean Consultant in Palliative Medicine St Francis Hospice Beaumont Hospital Overview
The last days of life in hospital and at home Beaumont Multi-disciplinary Palliative Care Study Day 28/9/2017 Dr Sarah McLean Consultant in Palliative Medicine St Francis Hospice Beaumont Hospital Overview
End of Life with Dementia Sue Quist RN, CHPN
 End of Life with Dementia Sue Quist RN, CHPN Objectives: Describe the Medicare hospice benefit and services. Discuss the Medicare admission criteria for hospice patients with dementia due to Alzheimer
End of Life with Dementia Sue Quist RN, CHPN Objectives: Describe the Medicare hospice benefit and services. Discuss the Medicare admission criteria for hospice patients with dementia due to Alzheimer
Palliative Care. Pocketbook 4
 Nottinghamshire STP EOL Programme Board 2019 Review 2022 Palliative Care Pocketbook 4 Contents Pain Guidelines page 2 Nausea and Vomiting page 9 Inoperable Bowel Obstruction page 10 Constipation page 11
Nottinghamshire STP EOL Programme Board 2019 Review 2022 Palliative Care Pocketbook 4 Contents Pain Guidelines page 2 Nausea and Vomiting page 9 Inoperable Bowel Obstruction page 10 Constipation page 11
Pain. Christine Illingworth. Community Nurse St Luke s Hospice 17/5/17
 Pain Christine Illingworth Community Nurse St Luke s Hospice 17/5/17 What is pain? Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damage Pain is whatever
Pain Christine Illingworth Community Nurse St Luke s Hospice 17/5/17 What is pain? Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damage Pain is whatever
Care of the Deteriorating Patient in Recovery NADIA TICEHURST : CLINICAL NURSE EDUCATOR PERI ANAESTHETICS BENDIGO HEALTH
 Care of the Deteriorating Patient in Recovery NADIA TICEHURST : CLINICAL NURSE EDUCATOR PERI ANAESTHETICS BENDIGO HEALTH Intended learning outcomes Describe the components of a comprehensive clinician
Care of the Deteriorating Patient in Recovery NADIA TICEHURST : CLINICAL NURSE EDUCATOR PERI ANAESTHETICS BENDIGO HEALTH Intended learning outcomes Describe the components of a comprehensive clinician
Clatterbridge Centre for Oncology
 Clatterbridge Centre for Oncology CONTENTS 1. Why and when to use a syringe driver 2. Siting the syringe driver 3. Mixing and measuring 4. Setting up the syringe driver 5. Drug information 6. Common problems
Clatterbridge Centre for Oncology CONTENTS 1. Why and when to use a syringe driver 2. Siting the syringe driver 3. Mixing and measuring 4. Setting up the syringe driver 5. Drug information 6. Common problems
Management of complications and side-effects of myeloma. Jackie Quinn Myeloma CNS Belfast Trust
 Management of complications and side-effects of myeloma Jackie Quinn Myeloma CNS Belfast Trust Common problems in myeloma Myeloma-related complications/symptoms Treatment-related side-effects Myeloma bone
Management of complications and side-effects of myeloma Jackie Quinn Myeloma CNS Belfast Trust Common problems in myeloma Myeloma-related complications/symptoms Treatment-related side-effects Myeloma bone
Metastatic Spinal Cord Compression (MSCC) Clinical guidelines and pathway
 Clinical guidelines and pathway") Metastatic Spinal Cord Compression (MSCC) Clinical guidelines and pathway Version 2: May 2012 To be read in conjunction with NICE CG75 Developed by consensus by: Dr Peter Robson, Consultant Oncologist,
Metastatic Spinal Cord Compression (MSCC) Clinical guidelines and pathway Version 2: May 2012 To be read in conjunction with NICE CG75 Developed by consensus by: Dr Peter Robson, Consultant Oncologist,
STEROID GUIDELINES AUDIT RESULTS
 STEROID GUIDELINES AUDIT RESULTS 27 patients were under active follow up between the audit dates. Notes for all these were audited. 59% (163) were not on steroids during this time 21% (57) were already
STEROID GUIDELINES AUDIT RESULTS 27 patients were under active follow up between the audit dates. Notes for all these were audited. 59% (163) were not on steroids during this time 21% (57) were already
End of life prescribing guidance
 End of life prescribing guidance Introduction This guidance has been prepared to ASSIST IN DECISION MAKING for the prescribing and monitoring of medicines useful in the management of symptoms commonly
End of life prescribing guidance Introduction This guidance has been prepared to ASSIST IN DECISION MAKING for the prescribing and monitoring of medicines useful in the management of symptoms commonly
Suspected spinal cord compression form
 Suspected spinal cord compression form Enter this form into the notes at the appropriate date in the Progress / Evaluation sheets. Please copy this form to Lisa Lewis, Medical PA (ext 4551), for audit
Suspected spinal cord compression form Enter this form into the notes at the appropriate date in the Progress / Evaluation sheets. Please copy this form to Lisa Lewis, Medical PA (ext 4551), for audit
Guidelines: EOLC Symptom Control for Patients with Normal Renal Function (in Wandsworth)
") Guidelines: EOLC Symptom Control for Patients with Normal Renal Function (in Wandsworth) Policy Number : DC020 Issue Date: October 2014 Review date: October 2016 Policy Owner: Head Community Services Monitor:
Guidelines: EOLC Symptom Control for Patients with Normal Renal Function (in Wandsworth) Policy Number : DC020 Issue Date: October 2014 Review date: October 2016 Policy Owner: Head Community Services Monitor:
Delirium in Palliative Care. Case Studies 2015
 Delirium in Palliative Care Case Studies 2015 Case 1 - Alex 35 yo M with metastatic melanoma Decreased LOC, unilateral hearing loss and bilateral vision loss, back pain, lower extremity weakness,? confusion/hallucinations
Delirium in Palliative Care Case Studies 2015 Case 1 - Alex 35 yo M with metastatic melanoma Decreased LOC, unilateral hearing loss and bilateral vision loss, back pain, lower extremity weakness,? confusion/hallucinations
Sam H Ahmedzai Academic Unit of Supportive Care Department of Oncology The University of Sheffield & Sheffield Teaching Hospitals NHS Foundation
 Sam H Ahmedzai Academic Unit of Supportive Care Department of Oncology The University of Sheffield & Sheffield Teaching Hospitals NHS Foundation Trust Overview Which drugs? How much? How to give? Adverse
Sam H Ahmedzai Academic Unit of Supportive Care Department of Oncology The University of Sheffield & Sheffield Teaching Hospitals NHS Foundation Trust Overview Which drugs? How much? How to give? Adverse
Symptom Control in the Community Setting. Dr Andrew Tysoe-Calnon
 Symptom Control in the Community Setting Dr Andrew Tysoe-Calnon Lead Consultant t Common symptoms Pain Agitation Shortness of breath Nausea and vomiting Intestinal obstruction Confusion Pain Occurs in
Symptom Control in the Community Setting Dr Andrew Tysoe-Calnon Lead Consultant t Common symptoms Pain Agitation Shortness of breath Nausea and vomiting Intestinal obstruction Confusion Pain Occurs in
Palliative Care Impact Survey
 September 2018 Contents Introduction...3 Headlines...3 Approach...4 Findings...4 Which guideline are used...4 How and where the guidelines are used...6 Alternative sources of information...7 Use of the
September 2018 Contents Introduction...3 Headlines...3 Approach...4 Findings...4 Which guideline are used...4 How and where the guidelines are used...6 Alternative sources of information...7 Use of the
SYMPTOM CONTROL IN THE LAST DAYS OF LIFE. Bradford, Airedale, Wharfedale & Craven
 Bradford, Airedale, Wharfedale & Craven Managed Clinical Network SYMPTOM CONTROL IN THE LAST DAYS OF LIFE Guidelines for Healthcare Professionals Bradford, Airedale, Wharfedale & Craven Signs and symptoms
Bradford, Airedale, Wharfedale & Craven Managed Clinical Network SYMPTOM CONTROL IN THE LAST DAYS OF LIFE Guidelines for Healthcare Professionals Bradford, Airedale, Wharfedale & Craven Signs and symptoms
Metastatic Spinal Disease
 Metastatic Spinal Disease Mr Neil Chiverton Consultant Spinal Surgeon, Sheffield Objectives The scale and nature of the problem NICE recommendations Surgical decision making Case illustrations Incidence
Metastatic Spinal Disease Mr Neil Chiverton Consultant Spinal Surgeon, Sheffield Objectives The scale and nature of the problem NICE recommendations Surgical decision making Case illustrations Incidence
Syringe driver in Palliative Care
 Syringe driver in Palliative Care Introduction: Syringe drivers are portable, battery operated devices widely used in palliative care to deliver medication as a continuous subcutaneous infusion over 24
Syringe driver in Palliative Care Introduction: Syringe drivers are portable, battery operated devices widely used in palliative care to deliver medication as a continuous subcutaneous infusion over 24
Current Management of Metastatic Bone Disease
 Current Management of Metastatic Bone Disease Evaluation and Medical Management Dr. Sara Rask Head, Medical Oncology Simcoe Muskoka Regional Cancer Centre www.rvh.on.ca Objectives 1. Outline an initial
Current Management of Metastatic Bone Disease Evaluation and Medical Management Dr. Sara Rask Head, Medical Oncology Simcoe Muskoka Regional Cancer Centre www.rvh.on.ca Objectives 1. Outline an initial
Oncologic Emergencies
 Oncologic Emergencies Peter Bjerkerot RN, OCN 1339 Normandy Drive Atlanta, GA 30306-2574 404.754.5952 WebPage http://boyrn.com peter.bjerkerot@mindspring.com Full Disclosure Statement Celgene Nurse Advisory
Oncologic Emergencies Peter Bjerkerot RN, OCN 1339 Normandy Drive Atlanta, GA 30306-2574 404.754.5952 WebPage http://boyrn.com peter.bjerkerot@mindspring.com Full Disclosure Statement Celgene Nurse Advisory
Renal Palliative Care Last Days of Life
 Renal Palliative Care Last Days of Life Introduction This guideline is an aid to clinical decision-making and good practice for patients with stage 4-5 chronic kidney disease (egfr
Renal Palliative Care Last Days of Life Introduction This guideline is an aid to clinical decision-making and good practice for patients with stage 4-5 chronic kidney disease (egfr
Zerlinda (MRP DK/H/2265/001)
") Zerlinda (MRP DK/H/2265/001) VI.2 Elements for a Public Summary VI.2.1 Overview of disease epidemiology Prevention of bone complications, e.g. fractures, in adult patients with bone metastases (spread
Zerlinda (MRP DK/H/2265/001) VI.2 Elements for a Public Summary VI.2.1 Overview of disease epidemiology Prevention of bone complications, e.g. fractures, in adult patients with bone metastases (spread
Faculty of Clinical Forensic Medicine Committee 1/2018
 Guideline Subject: Clinical Forensic Assessment and Management of Non-Fatal Strangulation Approval Date: January 2018 Review Date: January 2021 Review By: Number: Faculty of Clinical Forensic Medicine
Guideline Subject: Clinical Forensic Assessment and Management of Non-Fatal Strangulation Approval Date: January 2018 Review Date: January 2021 Review By: Number: Faculty of Clinical Forensic Medicine
Delirium. A Plan to Reduce Use of Restraints. David Wensel DO, FAAHPM Medical Director Midland Care
 Delirium A Plan to Reduce Use of Restraints David Wensel DO, FAAHPM Medical Director Midland Care Objectives Define delirium Describe pathophysiology of delirium Understand most common etiologies Define
Delirium A Plan to Reduce Use of Restraints David Wensel DO, FAAHPM Medical Director Midland Care Objectives Define delirium Describe pathophysiology of delirium Understand most common etiologies Define
AND CHEMOTHERAPY IN PALLIATIVE CARE
 THE ROLE OF RADIOTHERAPY AND CHEMOTHERAPY IN PALLIATIVE CARE Top Ten Cancers in Public Hospital KNH 2008 (CTC) Multidisciplinary Approach Radiotherapist Radiologist Medical Oncologist PALLIATIVE CARE/ONCOLOGY
THE ROLE OF RADIOTHERAPY AND CHEMOTHERAPY IN PALLIATIVE CARE Top Ten Cancers in Public Hospital KNH 2008 (CTC) Multidisciplinary Approach Radiotherapist Radiologist Medical Oncologist PALLIATIVE CARE/ONCOLOGY
The Quebec Palliative Sedation Guidelines. Rose DeAngelis, N, MSc(A), CHPCN (C)
, CHPCN (C)") The Quebec Palliative Sedation Guidelines Rose DeAngelis, N, MSc(A), CHPCN (C) CHPCA Conference September 2017 Conflict of Interest Statements There is no financial or in-kind support for this presentation.
The Quebec Palliative Sedation Guidelines Rose DeAngelis, N, MSc(A), CHPCN (C) CHPCA Conference September 2017 Conflict of Interest Statements There is no financial or in-kind support for this presentation.
Developing spinal cord compression care guidelines at WPH
 Developing spinal cord compression care guidelines at WPH Spinal cord compression team: Sue Banks, Jean Buchanan, Bernie Foran, Suzanne Hodson, Jane Mason, Rebecca Mills, Jan Siddall, Rebecca Walsh, Clare
Developing spinal cord compression care guidelines at WPH Spinal cord compression team: Sue Banks, Jean Buchanan, Bernie Foran, Suzanne Hodson, Jane Mason, Rebecca Mills, Jan Siddall, Rebecca Walsh, Clare
Symptom Management Challenges at End-of-Life
 Symptom Management Challenges at End-of-Life Amanda Lovell, PharmD, BCGP Clinical Pharmacist- Inpatient Units Optum Hospice Pharmacy Services February 15, 2018 Hospice Pharmacy Services Objectives Identify
Symptom Management Challenges at End-of-Life Amanda Lovell, PharmD, BCGP Clinical Pharmacist- Inpatient Units Optum Hospice Pharmacy Services February 15, 2018 Hospice Pharmacy Services Objectives Identify
BRAIN. Tumor byproducts. Autonomic nerves. Somatic nerves. Host immune cells. Cytokines
 Patient s Problems Pain (80%) Fatigue (90%) Weight Loss (80%) Lack of Appetite (80%) Nausea, Vomiting (90%) Anxiety (25%) Shortness of Breath (50%) Confusion-Agitation (80%) Tumor Mass Tumor Function Somatic
Patient s Problems Pain (80%) Fatigue (90%) Weight Loss (80%) Lack of Appetite (80%) Nausea, Vomiting (90%) Anxiety (25%) Shortness of Breath (50%) Confusion-Agitation (80%) Tumor Mass Tumor Function Somatic
Symptom control, essentials: delirium, dyspnoea and recurrent ascites
 Symptom control, essentials: delirium, dyspnoea and recurrent ascites Dr Jayne Wood Consultant Palliative Medicine, Clinical Lead NHS Foundation Trust, London ESMO Preceptorship Supportive and Palliative
Symptom control, essentials: delirium, dyspnoea and recurrent ascites Dr Jayne Wood Consultant Palliative Medicine, Clinical Lead NHS Foundation Trust, London ESMO Preceptorship Supportive and Palliative
Delirium in Cancer: Psychopharmacologic Management
 Delirium in Cancer: Psychopharmacologic Management William Breitbart, MD Professor and Chief, Psychiatry Service Memorial Sloan-Kettering Cancer Center New York, New York Delirium in Patients with Cancer
Delirium in Cancer: Psychopharmacologic Management William Breitbart, MD Professor and Chief, Psychiatry Service Memorial Sloan-Kettering Cancer Center New York, New York Delirium in Patients with Cancer
Supportive Care. End of Life Phase
 Supportive Care End of Life Phase Guidelines for Health Care Professionals In the care of patients with established renal failure who are in the last days of life References: Chambers E J (2004) End of
Supportive Care End of Life Phase Guidelines for Health Care Professionals In the care of patients with established renal failure who are in the last days of life References: Chambers E J (2004) End of
10/4/2017. Rationale symptom management. Satisfactory. NCCN Palliative Care Guidelines. Respiratory Symptoms. Dyspnea: Overview and Incidence
 Rationale symptom management Core Curriculum MODULE 3 PART II: SYMPTOM MANAGEMENT CARLA JOLLEY MN, ARNP, AOCN, ACHPN WHIDBEYHEALTH PALLIATIVE CARE Just because we can..doesn t mean we need to.. Assessment
Rationale symptom management Core Curriculum MODULE 3 PART II: SYMPTOM MANAGEMENT CARLA JOLLEY MN, ARNP, AOCN, ACHPN WHIDBEYHEALTH PALLIATIVE CARE Just because we can..doesn t mean we need to.. Assessment
MSCC CARE PATHWAYS & CASE STUDIES. By Michael Balloch Spine CNS
 MSCC CARE PATHWAYS & CASE STUDIES By Michael Balloch Spine CNS Aims To be familiar with the routes of MSCC prentaion How the guidelines work in practice Routes of presentation Generic intervention Managing
MSCC CARE PATHWAYS & CASE STUDIES By Michael Balloch Spine CNS Aims To be familiar with the routes of MSCC prentaion How the guidelines work in practice Routes of presentation Generic intervention Managing
Index. Surg Clin N Am 85 (2005) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Surg Clin N Am 85 (2005) 393 398 Index Note: Page numbers of article titles are in boldface type. A Acetaminophen, for chronic pain, in surgical patients, 219 a2 Adrenergic agonists, for neuropathic pain,
Surg Clin N Am 85 (2005) 393 398 Index Note: Page numbers of article titles are in boldface type. A Acetaminophen, for chronic pain, in surgical patients, 219 a2 Adrenergic agonists, for neuropathic pain,
FREQUENTLY ASKED QUESTIONS
 FREQUENTLY ASKED QUESTIONS The following questions are representative of questions that patients and family members ask when they visit the Bone and Cancer Foundation website or contact the Foundation
FREQUENTLY ASKED QUESTIONS The following questions are representative of questions that patients and family members ask when they visit the Bone and Cancer Foundation website or contact the Foundation
Formulary and Clinical Guideline Document Pharmacy Department Medicines Management Services
 Formulary and Clinical Guideline Document Pharmacy Department Medicines Management Services VIOLENCE, AGGRESSION OR SEVERE BEHAVIOURAL DISTURBANCE Introduction During an acute episode or illness, some
Formulary and Clinical Guideline Document Pharmacy Department Medicines Management Services VIOLENCE, AGGRESSION OR SEVERE BEHAVIOURAL DISTURBANCE Introduction During an acute episode or illness, some
Delirium. Delirium. Delirium Etiology and Pathophysiology. Fall 2018
 Three most common cognitive problems in adults 1. (acute confusion) 2. Dementia 3. Depression These problems often occur together Can you think of common stimuli for each? 1 1 State of temporary but acute
Three most common cognitive problems in adults 1. (acute confusion) 2. Dementia 3. Depression These problems often occur together Can you think of common stimuli for each? 1 1 State of temporary but acute
North Wales Critical Care Network
 North Wales Critical Care Network SEDATION GUIDELINES FOR ADULTS IN CRITICAL CARE Approved 6.9.12 1 Sedation guidelines for intensive care Betsi Cadwaladr University Health Board (Adapted from guidelines
North Wales Critical Care Network SEDATION GUIDELINES FOR ADULTS IN CRITICAL CARE Approved 6.9.12 1 Sedation guidelines for intensive care Betsi Cadwaladr University Health Board (Adapted from guidelines
This talk will cover. Myeloma kidney disease, pain and fatigue: complications of myeloma and side-effects of treatment. Pain.
 This talk will cover Myeloma kidney disease, pain and fatigue: complications of myeloma and side-effects of treatment Shirley Crofts Myeloma Clinical Nurse Specialist University Hospital Southampton NHS
This talk will cover Myeloma kidney disease, pain and fatigue: complications of myeloma and side-effects of treatment Shirley Crofts Myeloma Clinical Nurse Specialist University Hospital Southampton NHS
Palliative Care Out-of-hours. A resource pack for West Dorset. Contents:
 Palliative Care Out-of-hours. A resource pack for West Dorset Contents: Section 1 Supply of drugs DCH Pharmacy hours and arrangements How to contact a community pharmacist out of hours Palliative care
Palliative Care Out-of-hours. A resource pack for West Dorset Contents: Section 1 Supply of drugs DCH Pharmacy hours and arrangements How to contact a community pharmacist out of hours Palliative care
Benefits of Radiation Therapy in the Palliative Cancer Patient
 Benefits of Radiation Therapy in the Palliative Cancer Patient Dr Joshua Sappiatzer Radiation Oncologist Page 1 Overview Why we should aim for better palliative radiotherapy treatment Bone metastases Rapid
Benefits of Radiation Therapy in the Palliative Cancer Patient Dr Joshua Sappiatzer Radiation Oncologist Page 1 Overview Why we should aim for better palliative radiotherapy treatment Bone metastases Rapid