Assessing and Managing the Patient with Cognitive Decline
|
|
|
- Gervase Curtis
- 6 years ago
- Views:
Transcription
1 Assessing and Managing the Patient with Cognitive Decline Center of Excellence For Alzheimer s Disease for State of NY Capital Region Alzheimer s Center of Albany Medical Center Earl A. Zimmerman, MD Professor of Neurology
2 Support Grant support from NYS Department of Health for Center of Excellence in Alzheimer s disease for the NY Capital region IDMC member (Independent Monitoring Board) for vtv Therapeutics phase 3 trial of TTP488 (alzeliragon) in mild AD PI at AMC for Biogen phase 3 trial of monoclonal antibody aducanumab in MCI/early AD

3 Objectives *Learn simple methods to detect early dementia, or recognize even if not so early. *Be aware of tools to measure dementia in the patient in the office. *When to refer to neuropsychology or a specialist. *What imaging techniques are better? *What treatments and when?

4 Common Progressive Cognitive Disorders Alzheimer s disease more than 70%; presents usually with short term memory loss for years Frontotemporal dementias different disorders most often presenting with frontal behaviors: poor judgment, disinhibition early and language problems Lewy Body disease presents often with early hallucinations, parkinsonism, REM sleep disorder Vascular dementia: Multi-infarct; lacunar strokes; less common nowadays
5 Why Bother? Pathologies are different and treatments differ. Discovery the earlier the better for AD: MCI, mild cognitive/early AD can be slowed by aerobic exercise; treatment of diabetes and hypertension ameliorates AD Diagnosis of FTD often missed as psychiatric or poor judgement unrecognized may result in financial and other disasters Tighter control of BP and HbA1C may prevent lacunar stroke/dementia
6

7
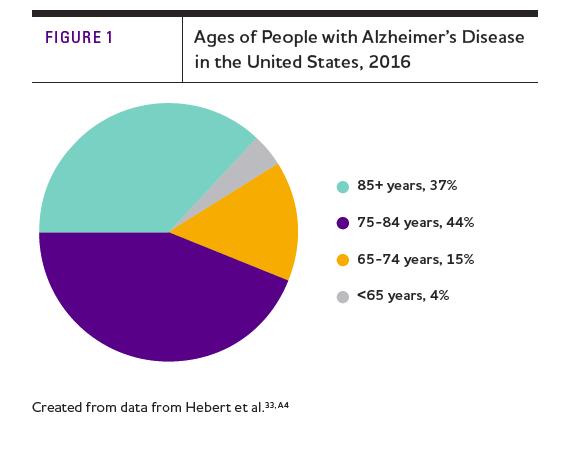
8 AD Statistics AD is the most common cause of dementia among people age 65 and older. Scientists estimate that around 4.5 million people now have AD. This number is expected to rise to 13 million by The national cost of caring for people with AD is approximately $100 billion per year More than 70% of patients with AD live at home with care provided by family and friends
9 Definition of Dementia: Impairment of short and long term memory in addition to abnormalities in at least one area of mental function: o o o o o o Abstract thinking Judgment Praxis Visual recognition Constructional abilities Personality
10 Causes of Dementia (Progressive Mental Decline) Alzheimer s disease (50-75%) Frontotemporal dementia (FTD) (Picks complex) (10-15%) Lewy body dementia (LBD) (5-10%) Parkinson's disease CJD (Creutzfeldt-Jakob/ prion disease) (rapid, rare) Cerebrovascular dementia (multi-infarct) (10%) Dementia with Multiple Sclerosis (MS) Dementia with treatable cause Pseudo dementia (depression often coexists with AD) Normal pressure hydrocephalus Brain tumor Hypothyroidism Vitamin B12 deficiency Infection: AIDS, syphilis
11 Different Presentations of Dementia Short term memory loss is the most common Visual spatial issues Language issues

12 Tau support for microtubule integrity and function is lost in AD due to A-beta amyloid or in FTD due to Genetic or other defects


13 Alzheimer s disease timeline Genetic risk Factors? Mis-folding & aggregation of aβ & tau, followed by sps & nfts Oxidative, nitrative & inflammatory Damage Cell death Clinical Diagnosis Autopsy MCI Probable AD Yrs Preventative Modifying Symptomatic
14 Stages of Alzheimer s Disease Clinical Dementia Rating Scale (CDR) MCI (Mild Cognitive Impairment) Mild Stage (CDR1) Moderate Stage (CDR 2) Severe Stage (CDR3)
15
 When tested, memory is slightly")

16 MCI (Mild Cognitive Impairment) New research category- not a disease Usually people with memory complaints and sometimes other things like word finding Function normally in Activities of Daily Living (ADL s) When tested, memory is slightly abnormal for age and education The memory type of MCI (amnestic) are more likely to progress to AD (rate of 10%/year) This is the subject of intense research interest for determining who with MCI has early AD and what might be done to stop progression
17 Clinical Progression of AD Early Stage (Mild) Pre mild - MCI: short term memory loss beyond normal aging; not demented (no loss of ability) Mild, stage 1: short term memory loss due to degeneration in hippocampus; mild visual-spatial difficulty (drawing intersecting pentagons on MMSE) due to parietal cortical dysfunction; independent except for forgetting medications, appointments Word finding trouble Often depressed (apathy, loss of interest)

18 Dennis Selkoe, Scientific American, Plaque distribution in red dots
19 Stages of AD (Moderate) More extensive memory loss More visual-spatial difficulty (visual agnosia): wandering, lost in space; need guidance in ambulation; some become delusional and others become agitated ( sundowning ) May become hypersexual and may crave sweets due to involvement of amygdala More trouble with language (aphasia) Parkinsonism in 25%

20 Stages of AD (Severe) Develop gait apraxia due to frontal cortex loss ( feet stuck to the floor ) forget walking Exhibit grasp reflexes Lose all language Become bedridden and need total care Later have trouble swallowing Die from aspiration pneumonia Hospice for last 6 months
21

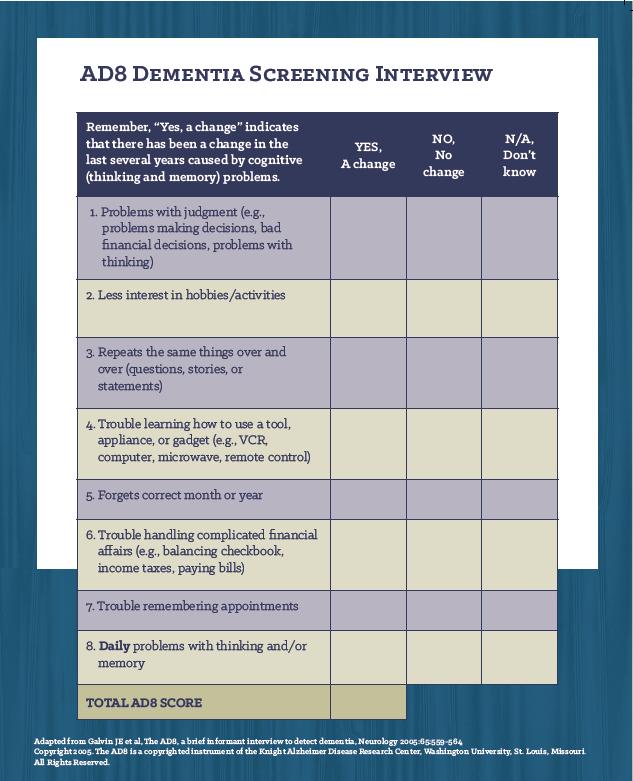
22 AD8 Scale Quick, easy, and reliable for early detection of dementia Takes a few minutes Can be done by patient, but less desirable Score of two or greater suggests dementia Highly recommended for screening
23
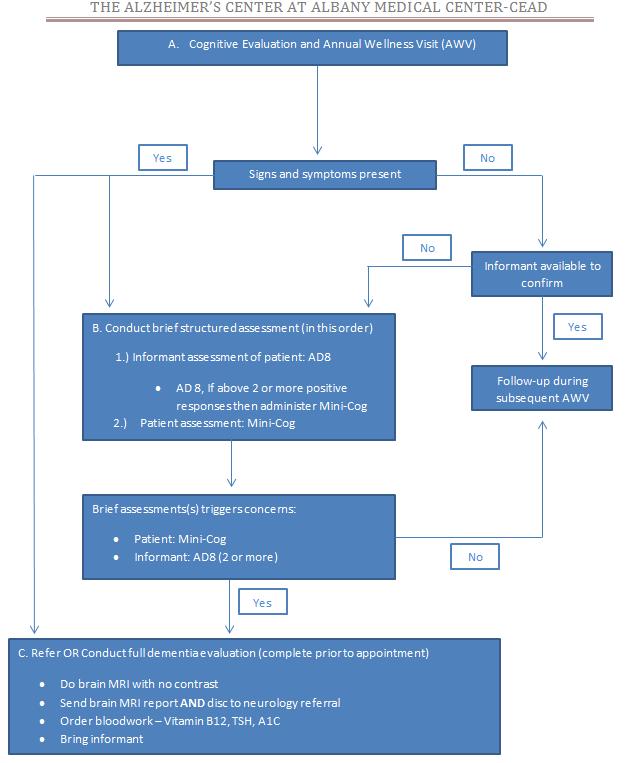
24 Next Steps Administer the MMSE or MiniCog
25
26 MMSE Scoring Score of 26 or less out of 30 may suggest dementia Score of our of 30 c/w moderate stage AD Score less than 10 c/w severe stage and test is not reliable due to language loss Not sensitive in early stage AD (MCI or very early AD)-Suggest performing MoCA
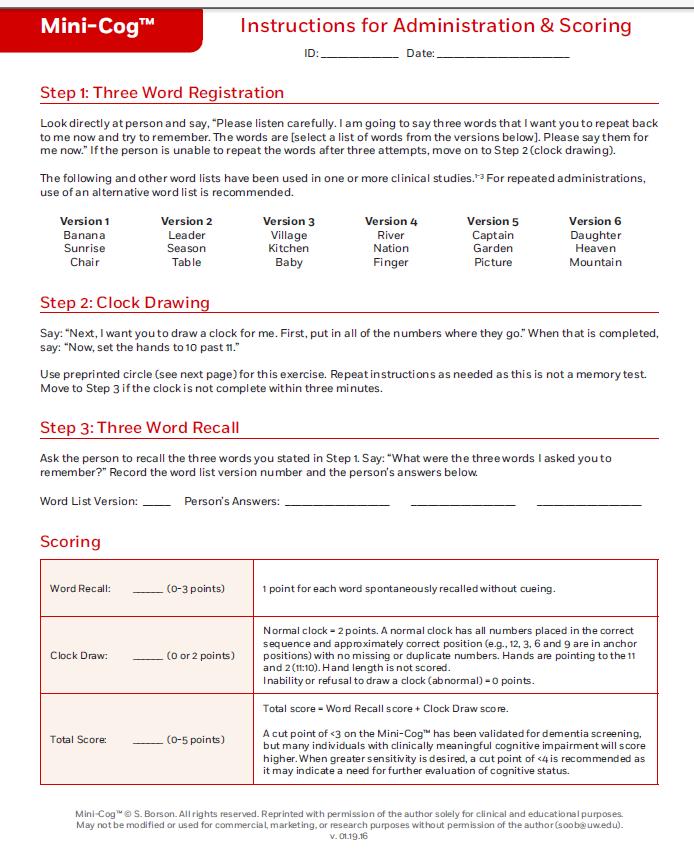

27 Mini COG
28 Imaging MRI of the brain (without contrast) if possible is preferable to CT scan o Better detail to detect atrophy and vascular disease Actual scan should be provided to consulting neurologist at first visit as well as report Caregiver/informant is critical for assessment
29 Advanced Imaging Metabolic PET/CT o To look at glucose metabolism loss. o May be useful in MCI or very early AD. Determining AD from FTD o Expensive and generally not needed (insurance may not cover) Amyloid PET o Useful especially in early diagnosis but CMS not paying for it o Research tool at present
30 Initial Management Complete evaluation before using medication Depression usually apathy is typically part of the presentation even in MCI and early AD o Patient benefit more from an SSRI than Aricept/Namenda. Both SSRI and Aricept (donepezil) can cause diarrhea o Don t start both at the same time Cholinesterase inhibitors and memantine both can cause agitation and DO NOT slow progression Aerobic exercise does o I recommend 30min/day, five times/week if possible in early stage AD
31 When to Order a Formal Neuropsychological Evaluation? The diagnosis of AD is clinical and not by neuropsychological testing The clinical testing should be done first most like by a neurosciences clinician expert in the diagnosis: evidence for progressive change from an informant, formalized office testing of patient, family history, clinical examination: r/o stroke, evidence for apraxia, parkinsonism, atrophy on the MRI Generally neruopsych should be ordered for very early AD (MCI) or differential diagnosis: AD vs FTD or LBD or for year repeat for advanced progression
32 What can our center do for you, primary care? Fully evaluate/diagnose dementia and its causes Educate the caregiver and family. Social work services are present from the initial visit Recommend a treatment course in collaboration with your general management of the diseases of aging. o Example: Maximize BP and diabetes control Follow patients longitudinally and help manage the behaviors and care issues long term.
33 Tools/Scales MMSE (Mini Mental Status Exam) MoCA (Montreal Cognitive Assessment) o o Much more sensitive especially in MCI/early AD; Takes experience and longer time ADL/IADL (Activities and Instrumental Activities of Daily Living) o Completed by caregiver CDR (Clinical Dementia Rating Scale) o o o o Useful tool in explaining to family the stage of the disease and in what is expected in 10 years CDR: 1 Mild stage, 5 years CDR: 2 - Moderate stage and more dependent, 3 years CDR: 3 - Severe stage, about 2 years. Neuropsychiatric inventory o Excellent way to understand behaviors. Mores useful than Geriatric depression scale
34
35
36
37
38 Common Mistakes in AD Failure to recognize memory loss resulting in medication mix-ups Unrecognized depression in early management Patient drifts into moderate AD and has an auto accident or wanders off Develops psychosis and goes after his wife with a butcher knife in unrecognized moderate AD Financial disasters due to poor judgment even in fairly early AD
39 Psychosis in Moderate AD Occurs to some degree in up to 40% of our patients Agitation most common and hallucinations in some and sometimes combativeness especially at dinner time ( sundowning ) We explain to family the use and risks of atypical antipsychotics and titrate them and monitor them. Can allow patient to stay at home. Quetiapine is more sedating but has less side effects and tends to be more effective.

40 End of Life Issues Educate family on the dying process Recruit palliative/hospice care for late stage Death Certificate o o Put Alzheimer s disease as the first diagnosis (the underlying disease process Highly under reported Second diagnosis: pneumonia or cardiopulmonary arrest.
41 Alzheimer's Center of Albany Medical Center NYS Center of Excellence for Alzheimer s Disease (CEAD) Diagnosis and Care Plan Case Management with Goldberg Alzheimer s Resource Research in Biomarkers and Drug Trials of industry and NIH, e.g. The ADNI imaging project; Biogen phase 3 trial of monoclonal antibody zimmere@mail.amc.edu; (518)
Evaluations. Alzheimer s Disease A Public Health Response. Viewer Call-In. July 19, Guest Speakers. Thanks to our Sponsors:
 Alzheimer s Disease A Public Health Response July 19, 2007 1 2 Guest Speakers Thanks to our Sponsors: Earl A. Zimmerman, M.D. Bender Endowed Chair of Neurology and Director of the Alzheimer s Center at
Alzheimer s Disease A Public Health Response July 19, 2007 1 2 Guest Speakers Thanks to our Sponsors: Earl A. Zimmerman, M.D. Bender Endowed Chair of Neurology and Director of the Alzheimer s Center at
DEMENTIA? 45 Million. What is. WHAT IS DEMENTIA Dementia is a disturbance in a group of mental processes including: 70% Dementia is not a disease
 What is PRESENTS DEMENTIA? WHAT IS DEMENTIA Dementia is a disturbance in a group of mental processes including: Memory Reasoning Planning Learning Attention Language Perception Behavior AS OF 2013 There
What is PRESENTS DEMENTIA? WHAT IS DEMENTIA Dementia is a disturbance in a group of mental processes including: Memory Reasoning Planning Learning Attention Language Perception Behavior AS OF 2013 There
WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient
 DEMENTIA WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient Progressive and disabling Not an inherent aspect of
DEMENTIA WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient Progressive and disabling Not an inherent aspect of
ALZHEIMER S DISEASE. Mary-Letitia Timiras M.D. Overlook Hospital Summit, New Jersey
 ALZHEIMER S DISEASE Mary-Letitia Timiras M.D. Overlook Hospital Summit, New Jersey Topics Covered Demography Clinical manifestations Pathophysiology Diagnosis Treatment Future trends Prevalence and Impact
ALZHEIMER S DISEASE Mary-Letitia Timiras M.D. Overlook Hospital Summit, New Jersey Topics Covered Demography Clinical manifestations Pathophysiology Diagnosis Treatment Future trends Prevalence and Impact
Diagnosis and Treatment of Alzhiemer s Disease
 Diagnosis and Treatment of Alzhiemer s Disease Roy Yaari, MD, MAS Director, Memory Disorders Clinic, Banner Alzheimer s Institute 602-839-6900 Outline Introduction Alzheimer s disease (AD)Guidelines -revised
Diagnosis and Treatment of Alzhiemer s Disease Roy Yaari, MD, MAS Director, Memory Disorders Clinic, Banner Alzheimer s Institute 602-839-6900 Outline Introduction Alzheimer s disease (AD)Guidelines -revised
ALZHEIMER S DISEASE OVERVIEW. Jeffrey Cummings, MD, ScD Cleveland Clinic Lou Ruvo Center for Brain Health
 ALZHEIMER S DISEASE OVERVIEW Jeffrey Cummings, MD, ScD Cleveland Clinic Lou Ruvo Center for Brain Health Prevalence AD: DEMOGRAPHY AND CLINICAL FEATURES Risk and protective factors Clinical features and
ALZHEIMER S DISEASE OVERVIEW Jeffrey Cummings, MD, ScD Cleveland Clinic Lou Ruvo Center for Brain Health Prevalence AD: DEMOGRAPHY AND CLINICAL FEATURES Risk and protective factors Clinical features and
GERIATRIC MENTAL HEALTH AND MEDICATION TREATMENT
 Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences GERIATRIC MENTAL HEALTH AND MEDICATION TREATMENT RUTH KOHEN ASSOCIATE PROFESSOR UW DEPARTMENT OF PSYCHIATRY 5-4-2017
Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences GERIATRIC MENTAL HEALTH AND MEDICATION TREATMENT RUTH KOHEN ASSOCIATE PROFESSOR UW DEPARTMENT OF PSYCHIATRY 5-4-2017
Alzheimer s disease dementia: a neuropsychological approach
 Alzheimer s disease dementia: a neuropsychological approach Dr. Roberta Biundo, PhD Neuropsychology Coordinator at Parkinson s disease and movement disorders unit of San Camillo rehabilitation hospital
Alzheimer s disease dementia: a neuropsychological approach Dr. Roberta Biundo, PhD Neuropsychology Coordinator at Parkinson s disease and movement disorders unit of San Camillo rehabilitation hospital
Dementia is not normal aging!
 The Future of Alzheimer s Disease Treatment Adam L. Boxer, MD, PhD Director, Alzheimer s Disease Clinical Trials Program Memory and Aging Center Assistant Professor of Neurology University of California,
The Future of Alzheimer s Disease Treatment Adam L. Boxer, MD, PhD Director, Alzheimer s Disease Clinical Trials Program Memory and Aging Center Assistant Professor of Neurology University of California,
Evaluation and Treatment of Dementia
 Evaluation and Treatment of Dementia Jeffrey M. Burns, MD Edward H. Hashinger Professor of Neurology Co-Director, KU Alzheimer s Disease Center Director, Clinical and Translational Science Unit Disclosures
Evaluation and Treatment of Dementia Jeffrey M. Burns, MD Edward H. Hashinger Professor of Neurology Co-Director, KU Alzheimer s Disease Center Director, Clinical and Translational Science Unit Disclosures
Memory Loss, Dementia and Alzheimer's Disease: The Basics
 Memory Loss, Dementia and Alzheimer's Disease: The Basics What is memory loss? What is age-related memory loss? Typical changes Typical age-related changes involve: Making a bad decision once in a while
Memory Loss, Dementia and Alzheimer's Disease: The Basics What is memory loss? What is age-related memory loss? Typical changes Typical age-related changes involve: Making a bad decision once in a while
Dementia: It s Not Always Alzheimer s
 Dementia: It s Not Always Alzheimer s A Caregiver s Perspective Diane E. Vance, Ph.D. Mid-America Institute on Aging and Wellness 2017 My Background Caregiver for my husband who had Lewy Body Dementia
Dementia: It s Not Always Alzheimer s A Caregiver s Perspective Diane E. Vance, Ph.D. Mid-America Institute on Aging and Wellness 2017 My Background Caregiver for my husband who had Lewy Body Dementia
Form D1: Clinician Diagnosis
 Initial Visit Packet Form D: Clinician Diagnosis NACC Uniform Data Set (UDS) ADC name: Subject ID: Form date: / / Visit #: Examiner s initials: INSTRUCTIONS: This form is to be completed by the clinician.
Initial Visit Packet Form D: Clinician Diagnosis NACC Uniform Data Set (UDS) ADC name: Subject ID: Form date: / / Visit #: Examiner s initials: INSTRUCTIONS: This form is to be completed by the clinician.
Dementia. Stephen S. Flitman, MD Medical Director 21st Century Neurology
 Dementia Stephen S. Flitman, MD Medical Director 21st Century Neurology www.neurozone.org Dementia is a syndrome Progressive memory loss, plus Progressive loss of one or more cognitive functions: Language
Dementia Stephen S. Flitman, MD Medical Director 21st Century Neurology www.neurozone.org Dementia is a syndrome Progressive memory loss, plus Progressive loss of one or more cognitive functions: Language
Dementia Basics. Welcome! What to expect and how to handle a dementia diagnosis. In partnership with Scripps Health.
 Dementia Basics What to expect and how to handle a dementia diagnosis March 18, 2017 In partnership with Scripps Health Welcome! 1 Welcome Kristin Gaspar San Diego County Supervisor District 3 2 Our Mission:
Dementia Basics What to expect and how to handle a dementia diagnosis March 18, 2017 In partnership with Scripps Health Welcome! 1 Welcome Kristin Gaspar San Diego County Supervisor District 3 2 Our Mission:
Understanding Dementia
 Understanding Dementia Dr. Dallas Seitz MD FRCPC Assistant Professor, Department of Psychiatry, Queen s University, Kingston, Ontario, Canada What s Next Information about Dementia, Elder Care and Supports
Understanding Dementia Dr. Dallas Seitz MD FRCPC Assistant Professor, Department of Psychiatry, Queen s University, Kingston, Ontario, Canada What s Next Information about Dementia, Elder Care and Supports
P20.2. Characteristics of different types of dementia and challenges for the clinician
 P20.2. Characteristics of different types of dementia and challenges for the clinician, professor Danish Dementia Research Center Rigshospitalet, University of Copenhagen (Denmark) This project has received
P20.2. Characteristics of different types of dementia and challenges for the clinician, professor Danish Dementia Research Center Rigshospitalet, University of Copenhagen (Denmark) This project has received
3/6/2019 DIAGNOSIS OF DEMENTIA IN THE OUTPATIENT SETTING FINANCIAL DISCLOSURES LEARNING OBJECTIVES
 DIAGNOSIS OF DEMENTIA IN THE OUTPATIENT SETTING MILTA LITTLE, DO, CMD DUKE UNIVERSITY SCHOOL OF MEDICINE FINANCIAL DISCLOSURES Dr. Little has no relevant financial disclosures to report Dr. Little will
DIAGNOSIS OF DEMENTIA IN THE OUTPATIENT SETTING MILTA LITTLE, DO, CMD DUKE UNIVERSITY SCHOOL OF MEDICINE FINANCIAL DISCLOSURES Dr. Little has no relevant financial disclosures to report Dr. Little will
Dementia and Alzheimer s disease
 Since 1960 Medicine Korat โรงพยาบาลมหาราชนครราชส มา Dementia and Alzheimer s disease Concise Reviews PAWUT MEKAWICHAI MD DEPARTMENT of MEDICINE MAHARAT NAKHON RATCHASIMA HOSPITAL 1 Prevalence Increase
Since 1960 Medicine Korat โรงพยาบาลมหาราชนครราชส มา Dementia and Alzheimer s disease Concise Reviews PAWUT MEKAWICHAI MD DEPARTMENT of MEDICINE MAHARAT NAKHON RATCHASIMA HOSPITAL 1 Prevalence Increase
OLD AGE PSYCHIATRY. Dementia definition TYPES OF DEMENTIA. Other causes. Psychiatric disorders of the elderly. Dementia.
 Psychiatric disorders of the elderly OLD AGE PSYCHIATRY Dementia Depression Delusional disorder/late onset schizophrenia Delirium Dementia definition LOCALISATION OF CEREBRAL FUNCTION Impairment of multiple
Psychiatric disorders of the elderly OLD AGE PSYCHIATRY Dementia Depression Delusional disorder/late onset schizophrenia Delirium Dementia definition LOCALISATION OF CEREBRAL FUNCTION Impairment of multiple
Part 2: Early detection, assessment and treatment in relation to the new guidelines. Christopher Patterson McMaster University
 Part 2: Early detection, assessment and treatment in relation to the new guidelines Christopher Patterson McMaster University C. Patterson MD, FRCPC Division of Geriatric Medicine, McMaster University
Part 2: Early detection, assessment and treatment in relation to the new guidelines Christopher Patterson McMaster University C. Patterson MD, FRCPC Division of Geriatric Medicine, McMaster University
The ABCs of Dementia Diagnosis
 The ABCs of Dementia Diagnosis Dr. Robin Heinrichs, Ph.D., ABPP Board Certified Clinical Neuropsychologist Associate Professor, Psychiatry & Behavioral Sciences Director of Neuropsychology Training What
The ABCs of Dementia Diagnosis Dr. Robin Heinrichs, Ph.D., ABPP Board Certified Clinical Neuropsychologist Associate Professor, Psychiatry & Behavioral Sciences Director of Neuropsychology Training What
The Person: Dementia Basics
 The Person: Dementia Basics Objectives 1. Discuss how expected age related changes in the brain might affect an individual's cognition and functioning 2. Discuss how changes in the brain due to Alzheimer
The Person: Dementia Basics Objectives 1. Discuss how expected age related changes in the brain might affect an individual's cognition and functioning 2. Discuss how changes in the brain due to Alzheimer
Alzheimer s Disease without Dementia
 Alzheimer s Disease without Dementia Dr Emer MacSweeney CEO & Consultant Neuroradiologist Re:Cognition Health London Osteopathic Society 13 September 2016 Early diagnosis of Alzheimer s Disease How and
Alzheimer s Disease without Dementia Dr Emer MacSweeney CEO & Consultant Neuroradiologist Re:Cognition Health London Osteopathic Society 13 September 2016 Early diagnosis of Alzheimer s Disease How and
A BRIEF LOOK AT DEMENTIA
 Dementia A BRIEF LOOK AT DEMENTIA David Kaufman, MD Neurology Consultants of Bellin Health November 2, 2017 Defined as a progressive decline in cognitive function that impairs daily activities. Always
Dementia A BRIEF LOOK AT DEMENTIA David Kaufman, MD Neurology Consultants of Bellin Health November 2, 2017 Defined as a progressive decline in cognitive function that impairs daily activities. Always
What if it s not Alzheimer s? Update on Lewy body dementia and frontotemporal dementia
 What if it s not Alzheimer s? Update on Lewy body dementia and frontotemporal dementia Dementia: broad term for any acquired brain condition impairing mental function such that ADLs are impaired. Includes:
What if it s not Alzheimer s? Update on Lewy body dementia and frontotemporal dementia Dementia: broad term for any acquired brain condition impairing mental function such that ADLs are impaired. Includes:
Overview. Case #1 4/20/2012. Neuropsychological assessment of older adults: what, when and why?
 Neuropsychological assessment of older adults: what, when and why? Benjamin Mast, Ph.D. Associate Professor & Vice Chair, Psychological & Brain Sciences Associate Clinical Professor, Family & Geriatric
Neuropsychological assessment of older adults: what, when and why? Benjamin Mast, Ph.D. Associate Professor & Vice Chair, Psychological & Brain Sciences Associate Clinical Professor, Family & Geriatric
Common Forms of Dementia Handout Package
 Common Forms of Dementia Handout Package Common Forms of Dementia 1 Learning Objectives As a result of working through this module, you should be better able to: 1. Describe clinical features of 4 major
Common Forms of Dementia Handout Package Common Forms of Dementia 1 Learning Objectives As a result of working through this module, you should be better able to: 1. Describe clinical features of 4 major
Dementia. Assessing Brain Damage. Mental Status Examination
 Dementia Assessing Brain Damage Mental status examination Information about current behavior and thought including orientation to reality, memory, and ability to follow instructions Neuropsychological
Dementia Assessing Brain Damage Mental status examination Information about current behavior and thought including orientation to reality, memory, and ability to follow instructions Neuropsychological
What APS Workers Need to Know about Frontotemporal, Lewy Body and Vascular Dementias
 What APS Workers Need to Know about Frontotemporal, Lewy Body and Vascular Dementias Presenter: Kim Bailey, MS Gerontology, Program & Education Specialist, Alzheimer s Orange County 1 1 Facts About Our
What APS Workers Need to Know about Frontotemporal, Lewy Body and Vascular Dementias Presenter: Kim Bailey, MS Gerontology, Program & Education Specialist, Alzheimer s Orange County 1 1 Facts About Our
Approach to Cognitive Disorders in Primary Care
 Approach to Cognitive Disorders in Primary Care What can reasonably be done in an office visit? What about screening for cognitive disorders? USPSTF (2014) doesn t recommend screening: magnitude of clinically
Approach to Cognitive Disorders in Primary Care What can reasonably be done in an office visit? What about screening for cognitive disorders? USPSTF (2014) doesn t recommend screening: magnitude of clinically
FTD basics! Etienne de Villers-Sidani, MD!
 FTD basics! Etienne de Villers-Sidani, MD! Frontotemporal lobar degeneration (FTLD) comprises 3 clinical syndromes! Frontotemporal dementia (behavioral variant FTD)! Semantic dementia (temporal variant
FTD basics! Etienne de Villers-Sidani, MD! Frontotemporal lobar degeneration (FTLD) comprises 3 clinical syndromes! Frontotemporal dementia (behavioral variant FTD)! Semantic dementia (temporal variant
Fact Sheet Alzheimer s disease
 What is Alzheimer s disease Fact Sheet Alzheimer s disease Alzheimer s disease, AD, is a progressive brain disorder that gradually destroys a person s memory and ability to learn, reason, make judgements,
What is Alzheimer s disease Fact Sheet Alzheimer s disease Alzheimer s disease, AD, is a progressive brain disorder that gradually destroys a person s memory and ability to learn, reason, make judgements,
Understanding Symptoms, Causes, and Risks for Alzheimer s Disease
 Understanding Symptoms, Causes, and Risks for Alzheimer s Disease Gene E. Alexander, Ph.D., Professor of Psychology, Neuroscience, and Physiological Sciences; Director, Brain Imaging, Behavior & Aging
Understanding Symptoms, Causes, and Risks for Alzheimer s Disease Gene E. Alexander, Ph.D., Professor of Psychology, Neuroscience, and Physiological Sciences; Director, Brain Imaging, Behavior & Aging
Differentiating Dementia Diagnoses
 Differentiating Dementia Diagnoses Waitemata PHO 21 October 2014 Dr Michal Boyd, RN, NP, ND Nurse Practitioner Older Adults School of Nursing & Freemasons Dept. of Geriatric Medicine The University of
Differentiating Dementia Diagnoses Waitemata PHO 21 October 2014 Dr Michal Boyd, RN, NP, ND Nurse Practitioner Older Adults School of Nursing & Freemasons Dept. of Geriatric Medicine The University of
Non Alzheimer Dementias
 Non Alzheimer Dementias Randolph B Schiffer Department of Neuropsychiatry and Behavioral Science Texas Tech University Health Sciences Center 9/11/2007 Statement of Financial Disclosure Randolph B Schiffer,,
Non Alzheimer Dementias Randolph B Schiffer Department of Neuropsychiatry and Behavioral Science Texas Tech University Health Sciences Center 9/11/2007 Statement of Financial Disclosure Randolph B Schiffer,,
Latest Methods to Early Detection for Alzheimer's: Cognitive Assessments and Diagnostic Tools in Practice
 Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/alzheimers-disease-towards-earlier-detection/latest-methods-earlydetection-alzheimers-cognitive-assessments-and-diagnostic-tools-practice/8321/
Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/alzheimers-disease-towards-earlier-detection/latest-methods-earlydetection-alzheimers-cognitive-assessments-and-diagnostic-tools-practice/8321/
A Fresh View of Cognitive Disorders in Older Adults: New Classification and Screening Strategies
 A Fresh View of Cognitive Disorders in Older Adults: New Classification and Screening Strategies Lynda Mackin, PhD, AGPCNP-BC, CNS University of California San Francisco School of Nursing 1 Alzheimer s
A Fresh View of Cognitive Disorders in Older Adults: New Classification and Screening Strategies Lynda Mackin, PhD, AGPCNP-BC, CNS University of California San Francisco School of Nursing 1 Alzheimer s
4/11/2017. The impact of Alzheimer s disease. Typical changes. The impact of Alzheimer s disease. Problematic changes. Problematic changes
 The impact of Alzheimer s disease Ron Petersen, MD, PhD, is Director of the Mayo Alzheimer's Disease Research Center. 2 The impact of Alzheimer s disease Typical changes Typical age-related changes involve:
The impact of Alzheimer s disease Ron Petersen, MD, PhD, is Director of the Mayo Alzheimer's Disease Research Center. 2 The impact of Alzheimer s disease Typical changes Typical age-related changes involve:
Alzheimer s Disease - Dementia
 - Dementia Neurocognitive disorder with dysfunction or loss of " Memory " Orientation " Attention " Language " Judgment " Reasoning Other characteristics that can manifest " Personality changes " Behavioral
- Dementia Neurocognitive disorder with dysfunction or loss of " Memory " Orientation " Attention " Language " Judgment " Reasoning Other characteristics that can manifest " Personality changes " Behavioral
Introduction to Dementia: Diagnosis & Evaluation. Created in March 2005 Duration: about 15 minutes
 Introduction to Dementia: Diagnosis & Evaluation Created in March 2005 Duration: about 15 minutes Axel Juan, MD The Geriatrics Institute axel.juan@med.va.gov 305-575-3388 Credits Principal medical contributor:
Introduction to Dementia: Diagnosis & Evaluation Created in March 2005 Duration: about 15 minutes Axel Juan, MD The Geriatrics Institute axel.juan@med.va.gov 305-575-3388 Credits Principal medical contributor:
Pharmacological Treatments for Neuropsychiatric Symptoms in Dementia 3/22/2018
 Pharmacological Treatments for Neuropsychiatric Symptoms in Dementia 3/22/2018 Mary Ellen Quiceno, MD, FAAN Associate Professor of Neurology UNTHSC Center for Geriatrics 855 Montgomery Street, PCC 4, Ft.
Pharmacological Treatments for Neuropsychiatric Symptoms in Dementia 3/22/2018 Mary Ellen Quiceno, MD, FAAN Associate Professor of Neurology UNTHSC Center for Geriatrics 855 Montgomery Street, PCC 4, Ft.
Alzheimer s Disease. Pathophysiology: Alzheimer s disease (AD) is a progressive dementia affecting cognition, behavior,
 is a progressive dementia affecting cognition, behavior,") 2 Alzheimer s Disease Alzheimer s disease (AD) is a progressive dementia affecting cognition, behavior, and functional status with no known cause or cure. Patients eventually lose cognitive, analytical,
2 Alzheimer s Disease Alzheimer s disease (AD) is a progressive dementia affecting cognition, behavior, and functional status with no known cause or cure. Patients eventually lose cognitive, analytical,
The Basics of Alzheimer s Disease
 2017 Memory Loss Conference The Basics of Alzheimer s Disease Tom Ala, MD Center for Alzheimer s Disease and Related Disorders Southern Illinois University School of Medicine Springfield, Illinois SIU
2017 Memory Loss Conference The Basics of Alzheimer s Disease Tom Ala, MD Center for Alzheimer s Disease and Related Disorders Southern Illinois University School of Medicine Springfield, Illinois SIU
Alzheimer Disease and Related Dementias. Alzheimer Society of Manitoba Dr. David Strang
 Alzheimer Disease and Related Dementias Alzheimer Society of Manitoba Dr. David Strang What is Dementia? Dementia is a syndrome symptoms include loss of memory, judgment and reasoning, and changes in mood
Alzheimer Disease and Related Dementias Alzheimer Society of Manitoba Dr. David Strang What is Dementia? Dementia is a syndrome symptoms include loss of memory, judgment and reasoning, and changes in mood
What is dementia? What is dementia?
 What is dementia? What is dementia? What is dementia? Dementia is an umbrella term for a range of progressive conditions that affect the brain. It has been identified that there are over 200 subtypes of
What is dementia? What is dementia? What is dementia? Dementia is an umbrella term for a range of progressive conditions that affect the brain. It has been identified that there are over 200 subtypes of
Alzheimer s Disease Update: From Treatment to Prevention
 Alzheimer s Disease Update: From Treatment to Prevention Jeffrey M. Burns, MD Edward H. Hashinger Professor of Medicine Co-Director, KU Alzheimer s Disease Center Director, Clinical and Translational Science
Alzheimer s Disease Update: From Treatment to Prevention Jeffrey M. Burns, MD Edward H. Hashinger Professor of Medicine Co-Director, KU Alzheimer s Disease Center Director, Clinical and Translational Science
Dementia and Fall Geriatric Interprofessional Training. Wael Hamade, MD, FAAFP
 Dementia and Fall Geriatric Interprofessional Training Wael Hamade, MD, FAAFP Prevalence of Dementia Age range 65-74 5% % affected 75-84 15-25% 85 and older 36-50% 5.4 Million American have AD Dementia
Dementia and Fall Geriatric Interprofessional Training Wael Hamade, MD, FAAFP Prevalence of Dementia Age range 65-74 5% % affected 75-84 15-25% 85 and older 36-50% 5.4 Million American have AD Dementia
Dr. Michael Lobatz Dr. Michael Jackson Dr. James Brewer Dr. Paul Aisen. Dr. Michael Plopper. Dr. Guerry Peavy
 1 Anne State 2 3 Dr. Michael Lobatz Dr. Michael Jackson Dr. James Brewer Dr. Paul Aisen Dr. Michael Plopper Dr. Guerry Peavy 4 Michael Lobatz, MD Medical Director, Neurosciences Medical Director, Rehabilitation
1 Anne State 2 3 Dr. Michael Lobatz Dr. Michael Jackson Dr. James Brewer Dr. Paul Aisen Dr. Michael Plopper Dr. Guerry Peavy 4 Michael Lobatz, MD Medical Director, Neurosciences Medical Director, Rehabilitation
DISCLOSURES. Objectives. THE EPIDEMIC of 21 st Century. Clinical Assessment of Cognition: New & Emerging Tools for Diagnosing Dementia NONE TO REPORT
 Clinical Assessment of Cognition: New & Emerging Tools for Diagnosing Dementia DISCLOSURES NONE TO REPORT Freddi Segal Gidan, PA, PhD USC Keck School of Medicine Rancho/USC California Alzheimers Disease
Clinical Assessment of Cognition: New & Emerging Tools for Diagnosing Dementia DISCLOSURES NONE TO REPORT Freddi Segal Gidan, PA, PhD USC Keck School of Medicine Rancho/USC California Alzheimers Disease
The Aging Brain The Aging Brain
 The Aging Brain The Aging Brain R. Scott Turner, MD, PhD Director, Memory Disorders Program Professor, Department of Neurology Georgetown University Washington, DC memory.georgetown.edu rst36@georgetown.edu
The Aging Brain The Aging Brain R. Scott Turner, MD, PhD Director, Memory Disorders Program Professor, Department of Neurology Georgetown University Washington, DC memory.georgetown.edu rst36@georgetown.edu
Mild Cognitive Impairment (MCI)
") October 19, 2018 Mild Cognitive Impairment (MCI) Yonas E. Geda, MD, MSc Professor of Neurology and Psychiatry Consultant, Departments of Psychiatry & Psychology, and Neurology Mayo Clinic College of Medicine
October 19, 2018 Mild Cognitive Impairment (MCI) Yonas E. Geda, MD, MSc Professor of Neurology and Psychiatry Consultant, Departments of Psychiatry & Psychology, and Neurology Mayo Clinic College of Medicine
Clinical Differences Among Four Common Dementia Syndromes. a program of Morningside Ministries
 Clinical Differences Among Four Common Dementia Syndromes a program of Morningside Ministries Introduction Four clinical dementia syndromes account for 90% of all cases after excluding reversible causes
Clinical Differences Among Four Common Dementia Syndromes a program of Morningside Ministries Introduction Four clinical dementia syndromes account for 90% of all cases after excluding reversible causes
Dementia Update. October 1, 2013 Dylan Wint, M.D. Cleveland Clinic Lou Ruvo Center for Brain Health Las Vegas, Nevada
 Dementia Update October 1, 2013 Dylan Wint, M.D. Cleveland Clinic Lou Ruvo Center for Brain Health Las Vegas, Nevada Outline New concepts in Alzheimer disease Biomarkers and in vivo diagnosis Future trends
Dementia Update October 1, 2013 Dylan Wint, M.D. Cleveland Clinic Lou Ruvo Center for Brain Health Las Vegas, Nevada Outline New concepts in Alzheimer disease Biomarkers and in vivo diagnosis Future trends
What is dementia? What is dementia?
 What is dementia? What is dementia? What is dementia? Dementia is an umbrella term for a range of progressive conditions that affect the brain. There are over 200 subtypes of dementia, but the five most
What is dementia? What is dementia? What is dementia? Dementia is an umbrella term for a range of progressive conditions that affect the brain. There are over 200 subtypes of dementia, but the five most
Dr Georgina Train Consultant Psychiatrist EMDASS service and Continuing Care.
 Dr Georgina Train Consultant Psychiatrist EMDASS service and Continuing Care. Consultant Psychiatrist of both General adult and Old Age Psychiatry. Work with Memory Service and a Continuing Care ward.
Dr Georgina Train Consultant Psychiatrist EMDASS service and Continuing Care. Consultant Psychiatrist of both General adult and Old Age Psychiatry. Work with Memory Service and a Continuing Care ward.
DEMENTIA 101: WHAT IS HAPPENING IN THE BRAIN? Philip L. Rambo, PhD
 DEMENTIA 101: WHAT IS HAPPENING IN THE BRAIN? Philip L. Rambo, PhD OBJECTIVES Terminology/Dementia Basics Most Common Types Defining features Neuro-anatomical/pathological underpinnings Neuro-cognitive
DEMENTIA 101: WHAT IS HAPPENING IN THE BRAIN? Philip L. Rambo, PhD OBJECTIVES Terminology/Dementia Basics Most Common Types Defining features Neuro-anatomical/pathological underpinnings Neuro-cognitive
NEUROPSYCHOMETRIC TESTS
 NEUROPSYCHOMETRIC TESTS CAMCOG It is the Cognitive section of Cambridge Examination for Mental Disorders of the Elderly (CAMDEX) The measure assesses orientation, language, memory, praxis, attention, abstract
NEUROPSYCHOMETRIC TESTS CAMCOG It is the Cognitive section of Cambridge Examination for Mental Disorders of the Elderly (CAMDEX) The measure assesses orientation, language, memory, praxis, attention, abstract
Diagnosis and management of non-alzheimer dementias. Melissa Yu, M.D. Department of Neurology
 Diagnosis and management of non-alzheimer dementias Melissa Yu, M.D. Department of Neurology AGENDA Introduction When to think of alternate diagnoses Other forms of dementia Other reasons for confusion
Diagnosis and management of non-alzheimer dementias Melissa Yu, M.D. Department of Neurology AGENDA Introduction When to think of alternate diagnoses Other forms of dementia Other reasons for confusion
Improving diagnosis of Alzheimer s disease and lewy body dementia. Brain TLC October 2018
 Improving diagnosis of Alzheimer s disease and lewy body dementia Brain TLC October 2018 Plan for this discussion: Introduction to AD and LBD Why do we need to improve diagnosis? What progress has been
Improving diagnosis of Alzheimer s disease and lewy body dementia Brain TLC October 2018 Plan for this discussion: Introduction to AD and LBD Why do we need to improve diagnosis? What progress has been
Is PET/CT really helpful in diagnosing Alzheimer s Disease?
 Is PET/CT really helpful in diagnosing Alzheimer s Disease? J. Rudolf MD Ph.D. Consultant in Neurology, Dept. of Neurology, General Hospital Papageorgiou Thessaloniki, Greece Conflict of Interest PET/CT
Is PET/CT really helpful in diagnosing Alzheimer s Disease? J. Rudolf MD Ph.D. Consultant in Neurology, Dept. of Neurology, General Hospital Papageorgiou Thessaloniki, Greece Conflict of Interest PET/CT
Forgetfulness: Knowing When to Ask for Help
 National Institute on Aging AgePage Forgetfulness: Knowing When to Ask for Help Maria has been a teacher for 35 years. Teaching fills her life and gives her a sense of accomplishment, but recently she
National Institute on Aging AgePage Forgetfulness: Knowing When to Ask for Help Maria has been a teacher for 35 years. Teaching fills her life and gives her a sense of accomplishment, but recently she
Memory Matters: Learning Objectives: Synapses, Age, and Health. Neuronal Synapses DISCLOSURE DECLARATION. Cognition and Normal Aging
 Standard Deviations from Mean Memory Matters: Preventing and Treating Late-Life, Cognitive Decline Daniel L. Murman, MD, MS Director, Behavioral and Geriatric Neurology Program Professor & Vice Chair,
Standard Deviations from Mean Memory Matters: Preventing and Treating Late-Life, Cognitive Decline Daniel L. Murman, MD, MS Director, Behavioral and Geriatric Neurology Program Professor & Vice Chair,
Alzheimer s Disease and Related Disorders: The Public Health Call to Action
 Levine Alzheimer s Disease and Related Disorders: The Public Health Call to Action Jed A. Levine, M.A. Executive Vice President Director of Programs and Services Alzheimer s Association, New York City
Levine Alzheimer s Disease and Related Disorders: The Public Health Call to Action Jed A. Levine, M.A. Executive Vice President Director of Programs and Services Alzheimer s Association, New York City
DEMENTIA ANDREA BERG, MD
 DEMENTIA ANDREA BERG, MD What Is Dementia? Decline in memory, language, problem-solving and other cognitive skills that affects a persons ability to perform everyday activities Progressive and disabling
DEMENTIA ANDREA BERG, MD What Is Dementia? Decline in memory, language, problem-solving and other cognitive skills that affects a persons ability to perform everyday activities Progressive and disabling
PROJECTION: Worlds dementia population is expected to triple by 2050
 DEMENTIA C L I S K C O N S U LTA N T P H Y S I C I A N I N A C U T E M E D I C I N E A N D G E R I AT R I C M E D I C I N E, B A R N E T H O S P I TA L, R O YA L F R E E N H S F O U N D AT I O N T R U
DEMENTIA C L I S K C O N S U LTA N T P H Y S I C I A N I N A C U T E M E D I C I N E A N D G E R I AT R I C M E D I C I N E, B A R N E T H O S P I TA L, R O YA L F R E E N H S F O U N D AT I O N T R U
Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE
 Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE Objectives At the conclusion of the session, participants will be
Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE Objectives At the conclusion of the session, participants will be
Roger E. Kelley, M.D. Professor and Chairman Department of Neurology Tulane University School of Medicine New Orleans, Louisiana
 Roger E. Kelley, M.D. Professor and Chairman Department of Neurology Tulane University School of Medicine New Orleans, Louisiana FINANCIAL DISCLOSURE No potential conflict of interest to disclose. OBJECTIVES
Roger E. Kelley, M.D. Professor and Chairman Department of Neurology Tulane University School of Medicine New Orleans, Louisiana FINANCIAL DISCLOSURE No potential conflict of interest to disclose. OBJECTIVES
Overview of neurological changes in Alzheimer s disease. Eric Karran
 Overview of neurological changes in Alzheimer s disease Eric Karran Alzheimer s disease Alois Alzheimer 1864-1915 Auguste D. 1850-1906 Case presented November 26 th 1906 Guildford Talk.ppt 20 th March,
Overview of neurological changes in Alzheimer s disease Eric Karran Alzheimer s disease Alois Alzheimer 1864-1915 Auguste D. 1850-1906 Case presented November 26 th 1906 Guildford Talk.ppt 20 th March,
Palliative Approach to the Person with Advanced Dementia
 Mid North Coast Rural Palliative Care Project Link Nurse Education 2004 Palliative Approach to the Person with Advanced Dementia Anne Sneesby CNC - ACAT To care for the dying is a very human opportunity
Mid North Coast Rural Palliative Care Project Link Nurse Education 2004 Palliative Approach to the Person with Advanced Dementia Anne Sneesby CNC - ACAT To care for the dying is a very human opportunity
DRUG THERAPY CHOICES FOR THE DEMENTED PATIENT Past, Present and Future
 DRUG THERAPY CHOICES FOR THE DEMENTED PATIENT Past, Present and Future Daniel S. Sitar Professor Emeritus University of Manitoba Email: Daniel.Sitar@umanitoba.ca March 6, 2018 INTRODUCTION EPIDEMIOLOGY
DRUG THERAPY CHOICES FOR THE DEMENTED PATIENT Past, Present and Future Daniel S. Sitar Professor Emeritus University of Manitoba Email: Daniel.Sitar@umanitoba.ca March 6, 2018 INTRODUCTION EPIDEMIOLOGY
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017.
 DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
Caring Sheet #11: Alzheimer s Disease:
 CARING SHEETS: Caring Sheet #11: Alzheimer s Disease: A Summary of Information and Intervention Suggestions with an Emphasis on Cognition By Shelly E. Weaverdyck, PhD Introduction This caring sheet focuses
CARING SHEETS: Caring Sheet #11: Alzheimer s Disease: A Summary of Information and Intervention Suggestions with an Emphasis on Cognition By Shelly E. Weaverdyck, PhD Introduction This caring sheet focuses
Dementia. Aetiology, pathophysiology and the role of neuropsychological testing. Dr Sheng Ling Low Geriatrician
 Dementia Aetiology, pathophysiology and the role of neuropsychological testing Dr Sheng Ling Low Geriatrician Topics to cover Why is dementia important What is dementia Differentiate between dementia,
Dementia Aetiology, pathophysiology and the role of neuropsychological testing Dr Sheng Ling Low Geriatrician Topics to cover Why is dementia important What is dementia Differentiate between dementia,
Yin-Hui Siow MD, FRCPC Director of Nuclear Medicine Southlake Regional Health Centre
 Yin-Hui Siow MD, FRCPC Director of Nuclear Medicine Southlake Regional Health Centre Today Introduction to CT Introduction to MRI Introduction to nuclear medicine Imaging the dementias The Brain ~ 1.5
Yin-Hui Siow MD, FRCPC Director of Nuclear Medicine Southlake Regional Health Centre Today Introduction to CT Introduction to MRI Introduction to nuclear medicine Imaging the dementias The Brain ~ 1.5
4/28/2017. Aging with Down Syndrome. Second Annual USC UCEDD Community Education Conference May 19, 2017
 Aging with Down Syndrome Second Annual USC UCEDD Community Education Conference May 19, 2017 Linda D. Nelson, M.Ed., Ed.S., Ph.D., ABN Board Certified Clinical Neuropsychologist Professor, Emerita, of
Aging with Down Syndrome Second Annual USC UCEDD Community Education Conference May 19, 2017 Linda D. Nelson, M.Ed., Ed.S., Ph.D., ABN Board Certified Clinical Neuropsychologist Professor, Emerita, of
Objectives. My Patient: The story 10/6/2017
 Objectives Our Grey Matter Matters: A Case in Point Vivien Brown MDCM, CCFP,FCFP, NCMP Assistant Professor, University of Toronto Vice President, Medical Affairs, Medisys Healthy Group Past President,
Objectives Our Grey Matter Matters: A Case in Point Vivien Brown MDCM, CCFP,FCFP, NCMP Assistant Professor, University of Toronto Vice President, Medical Affairs, Medisys Healthy Group Past President,
Prof Tim Anderson. Neurologist University of Otago Christchurch
 Prof Tim Anderson Neurologist University of Otago Christchurch Tim Anderson Christchurch Insidious cognitive loss From subjective memory complaints (SMC) to dementia Case 1. AR. 64 yrs Male GP referral
Prof Tim Anderson Neurologist University of Otago Christchurch Tim Anderson Christchurch Insidious cognitive loss From subjective memory complaints (SMC) to dementia Case 1. AR. 64 yrs Male GP referral
SECTION 1: as each other, or as me. THE BRAIN AND DEMENTIA. C. Boden *
 I read all the available books by other [people with] Alzheimer s disease but they never had quite the same problems as each other, or as me. I t s not like other diseases, where there is a standard set
I read all the available books by other [people with] Alzheimer s disease but they never had quite the same problems as each other, or as me. I t s not like other diseases, where there is a standard set
Alzheimer s disease is an
 Alzheimer s Disease FACT SHEET Alzheimer s disease is an irreversible, progressive brain disease that slowly destroys memory and thinking skills, and eventually even the ability to carry out the simplest
Alzheimer s Disease FACT SHEET Alzheimer s disease is an irreversible, progressive brain disease that slowly destroys memory and thinking skills, and eventually even the ability to carry out the simplest
Dementia: Diagnosis and Treatment
 Dementia: Diagnosis and Treatment Outline 1. Risk factors and definition of dementia 2. Types of Dementias 3. MMSE and testing 4. Treatment options Cognitive decline with aging Mild changes in memory and
Dementia: Diagnosis and Treatment Outline 1. Risk factors and definition of dementia 2. Types of Dementias 3. MMSE and testing 4. Treatment options Cognitive decline with aging Mild changes in memory and
Cognitive Screening in Risk Assessment. Geoffrey Tremont, Ph.D. Rhode Island Hospital & Alpert Medical School of Brown University.
 Cognitive Screening in Risk Assessment Geoffrey Tremont, Ph.D. Rhode Island Hospital & Alpert Medical School of Brown University Outline of Talk Definition of Dementia and MCI Incidence and Prevalence
Cognitive Screening in Risk Assessment Geoffrey Tremont, Ph.D. Rhode Island Hospital & Alpert Medical School of Brown University Outline of Talk Definition of Dementia and MCI Incidence and Prevalence
Dementia Update. Daniel Drubach, M.D. Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota
 Dementia Update Daniel Drubach, M.D. Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota Nothing to disclose Dementia Progressive deterioration in mental function
Dementia Update Daniel Drubach, M.D. Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota Nothing to disclose Dementia Progressive deterioration in mental function
Dementia and Delirium: A Neurologist s Approach to Altered Mental Status. Case 1 4/7/11. Which of the following evaluations is your next step?
 Dementia and Delirium: A Neurologist s Approach to Altered Mental Status S. Andrew Josephson, MD Director, Neurohospitalist Program Medical Director, Inpatient Neurology University of California San Francisco
Dementia and Delirium: A Neurologist s Approach to Altered Mental Status S. Andrew Josephson, MD Director, Neurohospitalist Program Medical Director, Inpatient Neurology University of California San Francisco
GENI Jeopardy: Geriatric Mental Health. Part of the brain responsible for executive functioning
 GENI Jeopardy: Geriatric Mental Health Part of the brain responsible for executive functioning Dementia: It is not just forgetfulness GENI February 20, 2008 Marcia Carr - CNS Dementia Dementia means brain
GENI Jeopardy: Geriatric Mental Health Part of the brain responsible for executive functioning Dementia: It is not just forgetfulness GENI February 20, 2008 Marcia Carr - CNS Dementia Dementia means brain
Michael A. Lobatz MD The Neurology Center Scripps Rehabilitation Center
 Michael A. Lobatz MD The Neurology Center Scripps Rehabilitation Center Dementia an acquired syndrome consisting of a decline in memory and other cognitive functions Alzheimer s Disease Fronto temporal
Michael A. Lobatz MD The Neurology Center Scripps Rehabilitation Center Dementia an acquired syndrome consisting of a decline in memory and other cognitive functions Alzheimer s Disease Fronto temporal
Diagnosis and management of Dementia
 Diagnosis and management of Dementia Dr. Jahnavi Kedare Associate Professor Dept. of Psychiatry, T. N. Medical College B. Y. L. Nair Hospital, Mumbai Prevalence of Dementia Lower than developed countries
Diagnosis and management of Dementia Dr. Jahnavi Kedare Associate Professor Dept. of Psychiatry, T. N. Medical College B. Y. L. Nair Hospital, Mumbai Prevalence of Dementia Lower than developed countries
Form A3: Subject Family History
 Initial Visit Packet NACC Uniform Data Set (UDS) Form A: Subject Family History ADC name: Subject ID: Form date: / / Visit #: Examiner s initials: INSTRUCTIONS: This form is to be completed by a clinician
Initial Visit Packet NACC Uniform Data Set (UDS) Form A: Subject Family History ADC name: Subject ID: Form date: / / Visit #: Examiner s initials: INSTRUCTIONS: This form is to be completed by a clinician
Mild cognitive impairment A view on grey areas of a grey area diagnosis
 Mild cognitive impairment A view on grey areas of a grey area diagnosis Dr Sergi Costafreda Senior Lecturer Division of Psychiatry, UCL Islington Memory Service, C&I NHS FT s.costafreda@ucl.ac.uk London
Mild cognitive impairment A view on grey areas of a grey area diagnosis Dr Sergi Costafreda Senior Lecturer Division of Psychiatry, UCL Islington Memory Service, C&I NHS FT s.costafreda@ucl.ac.uk London
DEMENTIA NEWSLETTER for PHYSICIANS
 DEMENTIA NEWSLETTER for PHYSICIANS Vol. 6, No. 4 OTTAWA AND RENFREW COUNTY Winter 2008 In This Issue... Mild Cognitive Impairment Monitoring Patient Response to Cognitive Enhancers CDN Diagnostic Assessment
DEMENTIA NEWSLETTER for PHYSICIANS Vol. 6, No. 4 OTTAWA AND RENFREW COUNTY Winter 2008 In This Issue... Mild Cognitive Impairment Monitoring Patient Response to Cognitive Enhancers CDN Diagnostic Assessment
Comments to this discussion are invited on the Alzforum Webinar page. Who Should Use the New Diagnostic Guidelines? The Debate Continues
 Comments to this discussion are invited on the Alzforum Webinar page. Who Should Use the New Diagnostic s? The Debate Continues Ever since new criteria came out for a research diagnosis of prodromal/preclinical
Comments to this discussion are invited on the Alzforum Webinar page. Who Should Use the New Diagnostic s? The Debate Continues Ever since new criteria came out for a research diagnosis of prodromal/preclinical
Clinical Diagnosis. Step 1: Dementia or not? Diagnostic criteria for dementia (DSM-IV)
") Step 1: Dementia or not? Diagnostic criteria for dementia (DSM-IV) A. The development of multiple cognitive deficits manifested by both 1 and 2 1 1. Memory impairment 2. One (or more) of the following
Step 1: Dementia or not? Diagnostic criteria for dementia (DSM-IV) A. The development of multiple cognitive deficits manifested by both 1 and 2 1 1. Memory impairment 2. One (or more) of the following
Carol Manning, PhD, ABPP-CN Director, Memory Disorders Clinic University of Virginia
 Carol Manning, PhD, ABPP-CN Director, Memory Disorders Clinic University of Virginia Case Study Mr. S. is a 74 year old man who has smoked for 20 years. He is overweight, has high cholesterol and high
Carol Manning, PhD, ABPP-CN Director, Memory Disorders Clinic University of Virginia Case Study Mr. S. is a 74 year old man who has smoked for 20 years. He is overweight, has high cholesterol and high
7/3/2013 ABNORMAL PSYCHOLOGY SEVENTH EDITION CHAPTER FOURTEEN CHAPTER OUTLINE. Dementia, Delirium, and Amnestic Disorders. Oltmanns and Emery
 ABNORMAL PSYCHOLOGY SEVENTH EDITION Oltmanns and Emery PowerPoint Presentations Prepared by: Ashlea R. Smith, Ph.D. This multimedia and its contents are protected under copyright law. The following are
ABNORMAL PSYCHOLOGY SEVENTH EDITION Oltmanns and Emery PowerPoint Presentations Prepared by: Ashlea R. Smith, Ph.D. This multimedia and its contents are protected under copyright law. The following are
Dementia. Dr Maria Foundas Consultant Physician. Training support Skills development Competency Assessment Scholarships Education
 Dementia Dr Maria Foundas Consultant Physician Training support Skills development Competency Assessment Scholarships Education Preamble and disclaimer These slides are made available by the Western Australian
Dementia Dr Maria Foundas Consultant Physician Training support Skills development Competency Assessment Scholarships Education Preamble and disclaimer These slides are made available by the Western Australian
10 Facts We All Need to Know About Dementia (MNCD) in Old Age
 in Old Age") 10 Facts We All Need to Know About Dementia (MNCD) in Old Age DUNCAN ROBERTSON FRCP (LOND & EDIN) FRCPC MEDICAL ADVISOR TO ADVANCING DEMENTIA DIAGNOSIS AND MANAGEMENT IN ALBERTA AND PRIMARY HEALTH CARE
10 Facts We All Need to Know About Dementia (MNCD) in Old Age DUNCAN ROBERTSON FRCP (LOND & EDIN) FRCPC MEDICAL ADVISOR TO ADVANCING DEMENTIA DIAGNOSIS AND MANAGEMENT IN ALBERTA AND PRIMARY HEALTH CARE
Alzheimer's Disease. Dementia
 Alzheimer's Disease Victor W. Henderson, MD, MS Departments of Health Research & Policy (Epidemiology) and of Neurology & Neurological Sciences Stanford University Director, Stanford Alzheimer s Disease
Alzheimer's Disease Victor W. Henderson, MD, MS Departments of Health Research & Policy (Epidemiology) and of Neurology & Neurological Sciences Stanford University Director, Stanford Alzheimer s Disease
Mild Cognitive Impairment
 Mild Cognitive Impairment Victor W. Henderson, MD, MS Departments of Health Research & Policy (Epidemiology) and of Neurology & Neurological Sciences Stanford University Director, Stanford Alzheimer s
Mild Cognitive Impairment Victor W. Henderson, MD, MS Departments of Health Research & Policy (Epidemiology) and of Neurology & Neurological Sciences Stanford University Director, Stanford Alzheimer s
Dementia the A,B,Cs. Dr. Frank Molnar. Associate Professor of Medicine, University of Ottawa Division of Geriatric Medicine, the Ottawa Hospital
 Dementia the A,B,Cs Dr. Frank Molnar Associate Professor of Medicine, University of Ottawa Division of Geriatric Medicine, the Ottawa Hospital Implications for Practice Dementia the A,B,Cs (Dr. Frank Molnar)
Dementia the A,B,Cs Dr. Frank Molnar Associate Professor of Medicine, University of Ottawa Division of Geriatric Medicine, the Ottawa Hospital Implications for Practice Dementia the A,B,Cs (Dr. Frank Molnar)
2016 Programs & Information
 Mayo Alzheimer s Disease Research Clinic Education Center 2016 Programs & Information BROCHURE TITLE FLUSH RIGHT for Persons & Families impacted by Mild Cognitive Impairment Alzheimer s Disease Dementia
Mayo Alzheimer s Disease Research Clinic Education Center 2016 Programs & Information BROCHURE TITLE FLUSH RIGHT for Persons & Families impacted by Mild Cognitive Impairment Alzheimer s Disease Dementia