Adverse drug reaction (ADR) A specific reaction usually related to a medication s pharmacology
|
|
|
- Noah Booth
- 6 years ago
- Views:
Transcription
1 Differentiate between an adverse drug reaction (ADR) and an adverse drug event (ADE). Identify ADE risk factors in older adults. Apply strategies to ensure safe medication use in older adults. Utilize clinical tools to recognize potential drugrelated problems in older adults. Identify limitations when applying the START, STOPP, and Beers Criteria in patient care. Discuss limitations of herbal and supplement use in older adults. Adverse drug reaction (ADR) A specific reaction usually related to a medication s pharmacology Adverse drug event (ADE) Injury due to a medication May include ADR and events related to medication use Medication error Inappropriate medication use that may or may not result in harm Nebeker J R et al. Ann Intern Med 2004;140:
(4). Nebeker J R et al.")
2 You deliver that bag of fentanyl for CC, a 76 yo female in the Surgical ICU. The nurse starts the infusion. Thirty minutes later, CC is found unresponsive, her BP is reading 72/45, HR of 67. The head nurse come to the room and found that the fentanyl drip is connected to CC s epidural catheter instead of her PICC line Relationships of key terms.(30)(4). Nebeker J R et al. Ann Intern Med 2004;140: Difficult to estimate ADE prevalence in older adult population Emergency Department visits: 5.9% to 12.6% 1-3 Older adults more likely to be hospitalized than younger patients Community dwelling: 5.5% to 33% 4-5 Impact healthcare costs and hospital admission rates 1) JAMA 2006;296: ) Ann Pharmacother 2005;39: ) BMJ 2004;329(7456): ) JAMA 2003;289: ) J Gerontol Med Sci 2006;61A:511-5.
3 Increasing age Female gender Hx prior ADR Prolonged hospitalization Fragmented medical care Multiple disease states/poor health status Polypharmacy Prescribing/Medication Selection Dispensing Administration/Adherence Monitoring Medication without an indication Indication without a medication Duplicate medications Wrong drug Wrong dose Wrong route or formulation Wrong time or frequency Wrong duration Drug interactions Allergies, contraindications DICP. 1990;24(11):
4 Zhan Criteria (2000) Beers Criteria (2003) START/STOPP Criteria (2008) French Consensus Panel List (2007) Norwegian General Practice Criteria (2009) Ann Pharmacother. 2010;44: DD is an 88 y.o. female patient who presents to the geriatric clinic with her daughter. The patient is orientated to self and place. She is able to answer simple commands. The patient c/o left leg pain only. You are asked to evaluate the patient s medications prior to her visit with the medication provider.
5 Social Hx: Widowed; patient moved in with her daughter 3 yrs three years ago secondary to difficulty with ADLs at home MMSE: 18/30 (1 month ago) PMH: Dementia, CHF, Hx Colon CA, COPD, Anxiety, and HTN Labs: BUN: 31 mg/dl, SCr: 1.7mg/dl, Alb: 2.9 g/dl, GFR: 29 ml/min/1.72m 2, BG: 84mg/dl, Electrolytes WNL, LFTs WNL Vital Signs: HR: 82 bpm, RR: 22 breaths/min, O 2 Sat: 96% on RA, BP: 132/70 mmhg, Temp: 98.6 F Ht: 5 4, Wt: 95 lbs Current Medications ASA 81mg PO Daily Lorazepam 1mg PO Q6h Lorazepam 0.5mg PO Q4h prn anxiety (2 doses/day) Miralax Mix 17g in 8 oz water and drink Daily Lactulose 10g/15ml PO Daily HCTZ 25mg PO Daily Lisinopril 10mg PO Daily Megestrol Susp 400mg PO BID Mirtazepine 15mg PO QHS Allergies: Codeine Aricept 10mg PO QHS Benefiber 2 tbsp in 8 oz of water and drink daily Oxycodone/Acetaminophen 5/325mg PO Q4h prn BTP (4 doses/day) Estradiol 0.5mg PO Daily Flonase 1 spray in each nostril BID MVI 1 tab PO Daily Prevacid 30mg PO Daily Ginkgo Biloba 160mg (2tabs) PO Daily
6 Most commonly used criteria on drugs to avoid in older adults Center for Medicare Services (CMS) mandated for nursing home Developed for use in community dwelling and nursing home patients Recommendations compiled by geriatric panel Review of medical literature Expert opinion Arch Intern Med 2003;163: Inappropriate medications for all elderly patients Drugs that should not be prescribed above criteria doses Drug-drug and drug-disease combinations to avoid Distinguishes between high and low severity Arch Intern Med 2003;163: Cyclobenzaprine Carisoprodol Amitriptyline Doxepin Dicyclomine Hydroxyzine Promethazine Fluoxetine Diazepam Amphetamines Naproxen Indomethacin Amiodarone Nitrofurantoin Doxazosin Clonidine Arch Intern Med 2003;163:
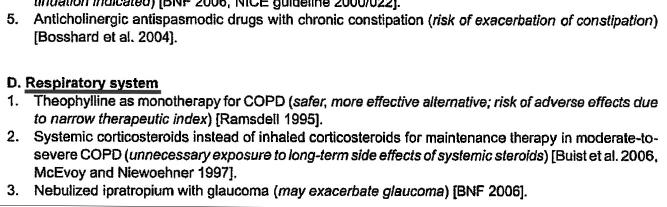
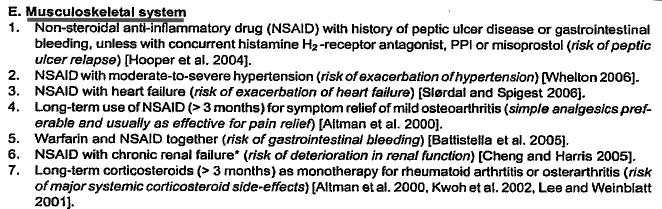
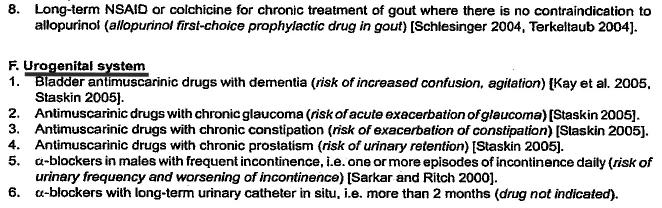
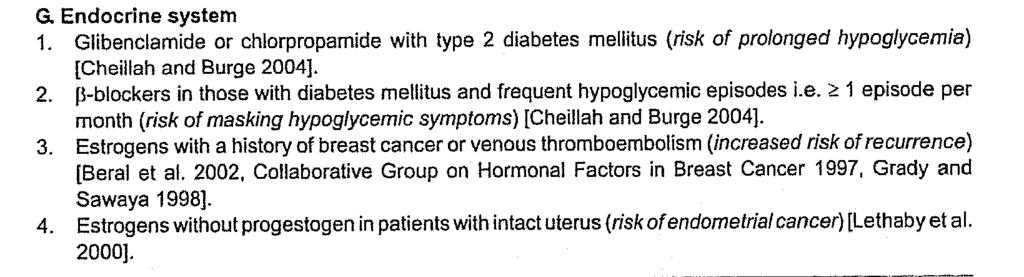
7 Drugs that should not be prescribed above criteria dose in the older adult Lorazepam (3 mg/day) Alprazolam (2 mg/day) Temazepam (15 mg/day) Digoxin (>125 mcg/day) Except when treating atrial arrhythmias Arch Intern Med 2003;163: Not an all inclusive drug list Not updated to reflect changes in clinical practice since 2002 Darvon, Darvocet removed from market NSAIDs and Cardiovascular AEs Increased risk of death in elderly patients taking atypical antipsychotics Evidence of validity is inconclusive Impact on mortality and cost HOWEVER. It is a reasonable starting place According to the Beers Criteria, is DD taking any potentially inappropriate medications? What are the medications severity ratings?
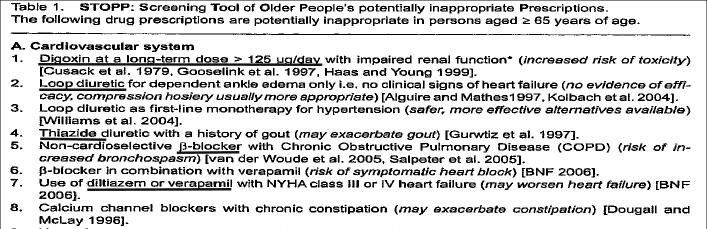
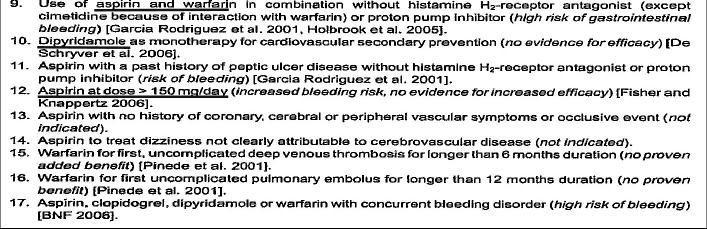
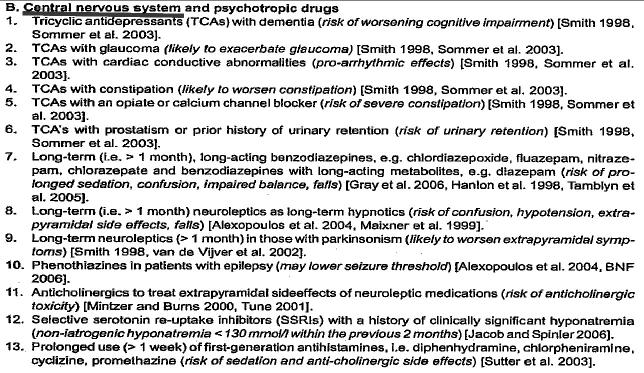
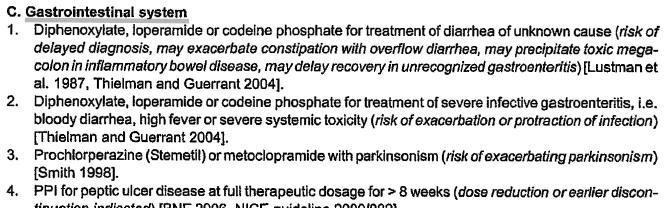
8 Screening Tool to Alert Doctors to the Right Treatment Most medical literature focuses on inappropriate prescribing in older adults Lack of evidence about medication omissions START criteria Evidence- based screening tool to alert prescribers to medications that are not prescribed but indicated Based on body system Developed by academic geriatrician with expert panel review Age and Aging. 2007;36: Endocrine System (i) Metformin with type 2 diabetes +/ Metabolic Syndrome (in the absence of renal impairment present (i.e. blood urea >33.6 mg/dl, ± serum creatinine >2.3 mg/dl). (ii) ACE inhibitor or Angiotension Receptor Blocker in diabetes with nephropathy i.e. overt dipstick proteinuria or microalbuminuria (>30mg/24 h) ± serum biochemical renal impairment (blood urea > 22.4 mg/dl or serum creatinine >1.7 mg/dl). (iii) ASA therapy in diabetes mellitus with well controlled BP (iv) Statin therapy in diabetes mellitus if fasting serum cholesterol >193 mg/dl or additional cardiovascular risk factor(s) present. Central Nervous System (i) L-DOPA in idiopathic Parkinson s disease with definite functional impairment and resultant disability. (ii) Antidepressant in the presence of clear-cut depressive symptoms, lasting at least 3 months. Locomotor System (i) Disease-modifying anti-rheumatic drug (DMARD) with known, moderate severe rheumatoid disease lasting more than 12 wks (ii) Bisphosphonate in patients taking glucocorticoids for more than 1 month (i.e. chronic corticosteroid therapy). (iii) Calcium and vitamin D supplement in patients with known osteoporosis (previous fragility fracture, acquired dorsal kyphosis).
9 Lack of supporting data on primary and secondary prevention outcomes Cost impact for medication omissions New costs for secondary prevention Lack of validation of findings in clinical practice Does not provide for individualization 2nd to shifting on goals of care Limited life expectancy Palliation versus secondary prevention According to the START criteria, are there additional medications that DD should receive? Screening Tool of Older Persons Potentially Inappropriate Prescriptions Evidence- based tool to address clinically significant criteria for potentially inappropriate prescribing Goal: improving limitations of other tools and reflect clinical practice changes Same research group that developed START criteria Expert geriatric panel review Based on body system Int J Clin Pharmacol Ther. 2008;46:72-83.
10
11
12 Lack of validation of findings in clinical practice Lack of outcomes data Cost Clinical efficacy Balance between limitations in START criteria (omission) with STOPP criteria (inappropriate prescribing) According to the STOPP criteria, is DD receiving any potentially inappropriate medications? Age and Aging 2008;37(6):
13 715 consecutive acutely ill, older adults in the emergency department Study investigators determined if PIMs contributed to or caused admission ADE was the cause or contributory factor for admission in 90 pts. (12.5% of all admissions) Age and Aging 2008;37(6): Most common presenting events: Falls, with following injuries: fractures 27% Ischemic Heart Disease (IHD) 12% Respiratory Tract Infection 10% Stroke 7% Cardiac failure 6% Delirium 5% Most prevalent co-morbidities: HTN (40%) IHD (29%) Stroke (16%) DM (16%) AFib (18%) Dementia (10%) STOPP criteria results 336 PIMs (in 247 pts.) detected (from total of 715 pts.) 82 patients (or 1/3) with PMIs presented an associated ADE (11.5% of total admissions) Beer s criteria results 226 PIMs (in 177 pts.) detected (from total of in 715 pts) 43 patients with PMIs presented an associated ADE (6% of total admissions) P<0.001
14 Includes OTC medications, herbals, and supplements Community dwelling patients often utilize these products without appropriate assessment and monitoring by a healthcare provider Use of herbals and dietary supplements has doubled among geriatric patients since 2000 Self-care with herbals, OTC medications, and supplements may contribute to Medications without an indication Duplicate therapy Drug-interactions J Religion Health. 2003;42(4):
15 Beers s Criteria STOPP Criteria Diphenhydramine ASA Chlorpheniramine 1st Generation Bisacodyl Antihistamines Except with chronic opioid use Diphenhydramine, Chlorpheniramine Mineral oil NSAIDs Ibuprofen, Naproxen Cimetidine Naproxen sodium 1) Arch Intern Med 2003;163: ) Loperamide PPIs Lansoprazole, Omeprazole, Zegrid Int J Clin Pharmacol TherOTC 2008;46: Treatment that is not within standard evidencebased medical practice Used instead of conventional medicine eg. breast CA patient who decides to utilize herbals instead of chemotherapy Intended to treat a disease state or improve organ function
16 Alternative therapies are used in combination with conventional medical practices eg. massage therapy in cancer patients receiving chemotherapy eg. Coenzyme Q10 use in patients taking warfarin Coenzyme Q10 improves cardiovascular disease? Decreased warfarin efficacy First Limitation: Unregulated Combination dietary supplement product 227 cases of selenium poisoning in 9 states Tested product selenium content: 40,800 µg/1 oz Labeled selenium content: 200 µg/1 oz RDA: 55 µg/day Arch Intern Med. 2010; 170(3):

17 Reported Symptoms of Selenium Toxicity After Consuming a Misformulated Dietary Supplement MacFarquhar, J. K. et al. Arch Intern Med 2010;170: Copyright restrictions may apply. Conclusions: Toxic concentrations of selenium in a liquid dietary supplement resulted in a widespread outbreak. Had the manufacturers been held to standards used in the pharmaceutical industry, it may have been prevented. Arch Intern Med. 2010; 170(3): Quantity of products listed Contaminants Misidentification or Cost Savings? woman hospitalized with irregular HR after taking what she thought was an herbal laxative. Investigation: product contained digitalis instead of plantain. The supplier had misidentified the herb in its raw form (Washington Post 2006) Plantain laxative Digitalis antiarrhythmic

 most clinical evidence CYP 1A2, 2C9, 2C19, 2D6, 2E1, 3A4 Many clinically significant drug-herbal interactions Warfarin")
18 Unregulated Limited / absent clinical data Efficacy Drug-herbal, drug-supplement, or drug-lab interactions Difficult to distinguish confounders in combination products Adverse effects incidence Reporting Impact of product variability Dose and length of therapy Patient specific factors St. John s Wort (SJW) most clinical evidence CYP 1A2, 2C9, 2C19, 2D6, 2E1, 3A4 Many clinically significant drug-herbal interactions Warfarin Increased metabolism via CYP3A4 induction Decreased metabolism via CYP1A2 inhibition Br J Clin Pharmacol. 2004;57(5):



19 Difficult to recommend widespread supplement use Exception calcium/vitamin D in osteoporosis Counsel patients on lack of evidence Document conversation Discourage use of combination products Encourage use of standardized products Medline Plus US National Library of Medicine and National Institutes of Health (NIH) b_all.html Memorial Sloan Kettering Cancer Center Look for these seals U.S. Pharmacopeia Dietary Supplement Verification Program USP Look for the USP certification Consumerlab.com -

20 Utilizing your clinical judgment What additional information would be beneficial? What additional interventions do you recommend?
STOPP and START criteria October 2011
 # START and STOPP are newer criteria to identify potentially inappropriate medications in elderly, including drug drug and drug disease interactions, drugs which increase risk of falls and drugs which
# START and STOPP are newer criteria to identify potentially inappropriate medications in elderly, including drug drug and drug disease interactions, drugs which increase risk of falls and drugs which
Screening tools for elderly patients in primary care
 Screening tools for elderly patients in primary care Cristín Ryan 1 Prof. Julia Kennedy 1 Dr. Denis O Mahony 2 Dr. Stephen Byrne 1 Co-Investigator: Dr. Paul Gallagher 2 1 Pharmaceutical Care Research Group,
Screening tools for elderly patients in primary care Cristín Ryan 1 Prof. Julia Kennedy 1 Dr. Denis O Mahony 2 Dr. Stephen Byrne 1 Co-Investigator: Dr. Paul Gallagher 2 1 Pharmaceutical Care Research Group,
Geriatric Pharmacology
 Geriatric Pharmacology Janice Scheufler R.Ph.,PharmD, FASCP Clinical Pharmacist Hospice of the Western Reserve Objectives List three risk factors for adverse drug events in the elderly Discuss two physiological
Geriatric Pharmacology Janice Scheufler R.Ph.,PharmD, FASCP Clinical Pharmacist Hospice of the Western Reserve Objectives List three risk factors for adverse drug events in the elderly Discuss two physiological
ROAD TO UNDERSTANDING POLYPHARMACY. Lt Col PHIL L. SAMPLES BS Phr, Pharm. D., BCNSP
 ROAD TO UNDERSTANDING POLYPHARMACY Lt Col PHIL L. SAMPLES BS Phr, Pharm. D., BCNSP Definition occurs when: 1. a medical regimen includes at least one unnecessary medication 2. Medications have not been
ROAD TO UNDERSTANDING POLYPHARMACY Lt Col PHIL L. SAMPLES BS Phr, Pharm. D., BCNSP Definition occurs when: 1. a medical regimen includes at least one unnecessary medication 2. Medications have not been
START, STOPP, Beers Oh My! Navigating the World of Geriatric Pharmacy
 START, STOPP, Beers Oh My! Navigating the World of Geriatric Pharmacy Jessica DiLeo, PharmD Kate Murphy, PharmD OBJECTIVES Identify pharmacodynamic and pharmacokinetic parameters that may influence treatment
START, STOPP, Beers Oh My! Navigating the World of Geriatric Pharmacy Jessica DiLeo, PharmD Kate Murphy, PharmD OBJECTIVES Identify pharmacodynamic and pharmacokinetic parameters that may influence treatment
Geriatric Pharmacology. Kwi Bulow, M.D. Clinical Professor of Medicine Director, Academic Geriatric Resource Center
 Geriatric Pharmacology Kwi Bulow, M.D. Clinical Professor of Medicine Director, Academic Geriatric Resource Center Silver Tsunami 2010: 40 million (13%) 2030: 72 million (20%) Baby Boomers (1946-1964)
Geriatric Pharmacology Kwi Bulow, M.D. Clinical Professor of Medicine Director, Academic Geriatric Resource Center Silver Tsunami 2010: 40 million (13%) 2030: 72 million (20%) Baby Boomers (1946-1964)
POLYPHARMACY IN OLDER ADULTS AND BEERS CRITERIA UPDATE
 POLYPHARMACY IN OLDER ADULTS AND BEERS CRITERIA UPDATE Jeannie Kim Lee, PharmD, BCPS, CGP Clinical Pharmacy Director College of Pharmacy The University of Arizona Learning Objectives: State the risks of
POLYPHARMACY IN OLDER ADULTS AND BEERS CRITERIA UPDATE Jeannie Kim Lee, PharmD, BCPS, CGP Clinical Pharmacy Director College of Pharmacy The University of Arizona Learning Objectives: State the risks of
Transitions of Care & Medication Reconciliation Ashley King, PharmD, BCGP Clinical Pharmacist LECOM Health March 2018
 Transitions of Care & Medication Reconciliation Ashley King, PharmD, BCGP Clinical Pharmacist LECOM Health March 2018 Objectives Identify when to complete medication reconciliation Understand the importance
Transitions of Care & Medication Reconciliation Ashley King, PharmD, BCGP Clinical Pharmacist LECOM Health March 2018 Objectives Identify when to complete medication reconciliation Understand the importance
Strategies to Decrease Medication Errors in Elderly. Abeer Zeitoun, Pharm. D Certified in Medication Safety, MCPHS
 Strategies to Decrease Medication Errors in Elderly Abeer Zeitoun, Pharm. D Certified in Medication Safety, MCPHS Road Map..Outline 1. Introduction A. Definitions B. Geriatrics: High risk population C.
Strategies to Decrease Medication Errors in Elderly Abeer Zeitoun, Pharm. D Certified in Medication Safety, MCPHS Road Map..Outline 1. Introduction A. Definitions B. Geriatrics: High risk population C.
家庭醫業 評估工具. 65 Beer's Criteria 19.1% i m p l i c i t prescribing indicators Akazawa M (1.68 ) (Medication Appropriateness Index, MAI)
 (Medication Appropriateness Index, MAI)") 前言 2001 2004 65 Beer's Criteria 19.1% 2001 Akazawa M (1.68 ) ( 33%) 高雄榮民總醫院家庭醫學部 potentially inappropriate medication; STOPP; START 評估工具 i m p l i c i t prescribing indicators (Medication Appropriateness
前言 2001 2004 65 Beer's Criteria 19.1% 2001 Akazawa M (1.68 ) ( 33%) 高雄榮民總醫院家庭醫學部 potentially inappropriate medication; STOPP; START 評估工具 i m p l i c i t prescribing indicators (Medication Appropriateness
PRESCRIBING IN THE ELDERLY. CARE HOME PHARMACY TEAM Bhavini Shah, Eleesha Pentiah & Puja Vyas
 PRESCRIBING IN THE ELDERLY CARE HOME PHARMACY TEAM Bhavini Shah, Eleesha Pentiah & Puja Vyas LEARNING OUTCOMES Medicines Optimisation The effects of aging on health and medicines. Polypharmacy Acute Kidney
PRESCRIBING IN THE ELDERLY CARE HOME PHARMACY TEAM Bhavini Shah, Eleesha Pentiah & Puja Vyas LEARNING OUTCOMES Medicines Optimisation The effects of aging on health and medicines. Polypharmacy Acute Kidney
Prescribing in the Elderly. Dr Alison Macrae and Dr Debbie Vest GPST2 Drs in Psychiatry
 Prescribing in the Elderly Dr Alison Macrae and Dr Debbie Vest GPST2 Drs in Psychiatry 24 th September 2014 Objectives Understand the significance of polypharmacy in the elderly Become familiar with the
Prescribing in the Elderly Dr Alison Macrae and Dr Debbie Vest GPST2 Drs in Psychiatry 24 th September 2014 Objectives Understand the significance of polypharmacy in the elderly Become familiar with the
Aging and Geriatric Assessment March 31, 2008 Sharon Leigh, Pharm D. BCPS Providence ElderPlace
 Aging and Geriatric Assessment Page 1 Aging and Geriatric Assessment March 31, 2008 Sharon Leigh, Pharm D. BCPS Providence ElderPlace I. Aging A. Demographics Age 65+ population 3.1 million 1900 31.2 million
Aging and Geriatric Assessment Page 1 Aging and Geriatric Assessment March 31, 2008 Sharon Leigh, Pharm D. BCPS Providence ElderPlace I. Aging A. Demographics Age 65+ population 3.1 million 1900 31.2 million
STOPP START Toolkit Supporting Medication Review in the Older Person
 STOPP START Toolkit Supporting Medication Review in the Older Person STOPP: Screening Tool of Older People s potentially inappropriate Prescriptions START: Screening Tool to Alert doctors to Right (appropriate,
STOPP START Toolkit Supporting Medication Review in the Older Person STOPP: Screening Tool of Older People s potentially inappropriate Prescriptions START: Screening Tool to Alert doctors to Right (appropriate,
Disclosures. Use caution in the elderly: review of safe and effective medication use in older patients. Institute of Medicine. Learning Objectives
 Use caution in the elderly: review of safe and effective medication use in older patients Disclosures I have no disclosures or conflicts of interest related to this presentation John T. Holmes, PharmD,
Use caution in the elderly: review of safe and effective medication use in older patients Disclosures I have no disclosures or conflicts of interest related to this presentation John T. Holmes, PharmD,
Case 1. Case 2. What do you think about reducing or discontinuing some of the above now that his LVEF has normalized?
 Case 1 A primary care colleague inquires what to do with a patient (HFrEF in NSR) who has a digoxin level of 2.8ng/ml. Level was obtained at 10am, patient takes all medications at one time upon arising
Case 1 A primary care colleague inquires what to do with a patient (HFrEF in NSR) who has a digoxin level of 2.8ng/ml. Level was obtained at 10am, patient takes all medications at one time upon arising
Pitfalls in Pharmacotherapy of Geriatrics
 Pitfalls in Pharmacotherapy of Geriatrics DR Ali M. Alyami (M Pharm., PhD) Case Study An 85 year old female with a history of atrial fibrillation, stroke, dementia, and hypertension, who is receiving chronic
Pitfalls in Pharmacotherapy of Geriatrics DR Ali M. Alyami (M Pharm., PhD) Case Study An 85 year old female with a history of atrial fibrillation, stroke, dementia, and hypertension, who is receiving chronic
Interdisciplinary detection of potential drug related problems in older people
 Interdisciplinary detection of potential drug related problems in older people Prof. dr. Mirko Petrovic Department of Internal Medicine, Ghent University Department of Geriatrics, Ghent University Hospital,
Interdisciplinary detection of potential drug related problems in older people Prof. dr. Mirko Petrovic Department of Internal Medicine, Ghent University Department of Geriatrics, Ghent University Hospital,
Use caution in the elderly: review of safe and effective medication use in older patients
 Use caution in the elderly: review of safe and effective medication use in older patients John T. Holmes, PharmD, BCPS Assistant Professor of Family Medicine and Pharmacy Practice In support of improving
Use caution in the elderly: review of safe and effective medication use in older patients John T. Holmes, PharmD, BCPS Assistant Professor of Family Medicine and Pharmacy Practice In support of improving
Rebecca Rottman-Sagebiel, Pharm.D., BCPS Sharon Jung Tschirhart, Pharm.D., BCPS Geriatric Clinical Pharmacy Specialists STVHCS, Audie L.
 Rebecca Rottman-Sagebiel, Pharm.D., BCPS Sharon Jung Tschirhart, Pharm.D., BCPS Geriatric Clinical Pharmacy Specialists STVHCS, Audie L. Murphy Division Clinical Assistant Professors, University of Texas/UTHSCSA
Rebecca Rottman-Sagebiel, Pharm.D., BCPS Sharon Jung Tschirhart, Pharm.D., BCPS Geriatric Clinical Pharmacy Specialists STVHCS, Audie L. Murphy Division Clinical Assistant Professors, University of Texas/UTHSCSA
BLCS 1-Clinical Overview. Dr. Chris Rauscher Clinical Lead Shared Care Polypharmacy Risk Reduction Initiative
 BLCS 1-Clinical Overview Dr. Chris Rauscher Clinical Lead Shared Care Polypharmacy Risk Reduction Initiative Fraser Health Guide To Person-Centered Medication Decisions Factors to Consider When Systematically
BLCS 1-Clinical Overview Dr. Chris Rauscher Clinical Lead Shared Care Polypharmacy Risk Reduction Initiative Fraser Health Guide To Person-Centered Medication Decisions Factors to Consider When Systematically
Katee Kindler, PharmD, BCACP
 Speaker Introduction Katee Kindler, PharmD, BCACP Current Practice: Clinical Pharmacy Specialist Ambulatory Care, St. Vincent Indianapolis Assistant Professor of Pharmacy Practice, Manchester University,
Speaker Introduction Katee Kindler, PharmD, BCACP Current Practice: Clinical Pharmacy Specialist Ambulatory Care, St. Vincent Indianapolis Assistant Professor of Pharmacy Practice, Manchester University,
Drug use in long term care. Graziano Onder Centro Medicina Invecchiamento Università Cattolica Sacro Cuore, Rome
 Drug use in long term care Graziano Onder Centro Medicina Invecchiamento Università Cattolica Sacro Cuore, Rome Polypharmacy in nursing home (USA) Concurrent use of 9 medications was reported for 39.7%
Drug use in long term care Graziano Onder Centro Medicina Invecchiamento Università Cattolica Sacro Cuore, Rome Polypharmacy in nursing home (USA) Concurrent use of 9 medications was reported for 39.7%
Intelligent Polypharmacy. Professor Colin P Bradley Department of General Practice University College Cork
 Intelligent Polypharmacy Professor Colin P Bradley Department of General Practice University College Cork Polypharmacy No standard definition 2005 review the use of medications that are not clinically
Intelligent Polypharmacy Professor Colin P Bradley Department of General Practice University College Cork Polypharmacy No standard definition 2005 review the use of medications that are not clinically
Meds and Falls: Keep in Step with your Meds
 Meds and Falls: Keep in Step with your Meds Donna Bartlett PharmD, CGP, RPh Associate Professor-Pharmacy Practice MCPHS University Clinical Pharmacist-MCPHS University- Pharmacy Outreach Program donna.bartlett@mcphs.edu
Meds and Falls: Keep in Step with your Meds Donna Bartlett PharmD, CGP, RPh Associate Professor-Pharmacy Practice MCPHS University Clinical Pharmacist-MCPHS University- Pharmacy Outreach Program donna.bartlett@mcphs.edu
Pharmaceutical Care for Geriatrics
 Continuing Professional Pharmacy Development Program Pharmaceutical Care for Geriatrics Presented by: Alla El-Awaisi; MPharm, MRPharmS, MSc Event Organizer: Dr. Nadir Kheir; PhD Disclaimer: PRESENTING
Continuing Professional Pharmacy Development Program Pharmaceutical Care for Geriatrics Presented by: Alla El-Awaisi; MPharm, MRPharmS, MSc Event Organizer: Dr. Nadir Kheir; PhD Disclaimer: PRESENTING
Overview of Current Quality Measures that can be Impacted by Ambulatory Pharmacists
 Overview of Current Quality Measures that can be Impacted by Ambulatory Pharmacists Measure Name Measure Domain Measure Focus Comment/Explanation CMS Value-based Purchasing Program (CMS VBP) AMI 30-day
Overview of Current Quality Measures that can be Impacted by Ambulatory Pharmacists Measure Name Measure Domain Measure Focus Comment/Explanation CMS Value-based Purchasing Program (CMS VBP) AMI 30-day
Medication Use in Older Adults
 Medication Use in Older Adults F. Michael Gloth, III, MD, AGSF, FACP, CMD Clinical Professor Department of Geriatrics, Florida State University College of Medicine Associate Professor of Medicine Division
Medication Use in Older Adults F. Michael Gloth, III, MD, AGSF, FACP, CMD Clinical Professor Department of Geriatrics, Florida State University College of Medicine Associate Professor of Medicine Division
ASPIRIN MISUSE AT HOME ACCORDING TO START AND STOPP IN FRAIL OLDER PERSONS
 ASPIRIN MISUSE AT HOME ACCORDING TO START AND STOPP IN FRAIL OLDER PERSONS O. Dalleur 1,4, B. Boland 2,3, A. Spinewine 4-5 1 Pharmacy and 2 Geriatric Medicine, St-Luc university Hospital, 3 Institute of
ASPIRIN MISUSE AT HOME ACCORDING TO START AND STOPP IN FRAIL OLDER PERSONS O. Dalleur 1,4, B. Boland 2,3, A. Spinewine 4-5 1 Pharmacy and 2 Geriatric Medicine, St-Luc university Hospital, 3 Institute of
BEERs For the Elderly
 BEERs For the Elderly February 2008 Presented by:carla Ambrosini Seniors First Clinic Pharmacist 12/05/2008 1 Objectives To highlight the overall health care impact of drug related adverse reactions and
BEERs For the Elderly February 2008 Presented by:carla Ambrosini Seniors First Clinic Pharmacist 12/05/2008 1 Objectives To highlight the overall health care impact of drug related adverse reactions and
Polypharmacy 101. Acknowledgements. Disclosure. with special thanks to Jen Lehman, PharmD candidate
 Polypharmacy 101 Kimberly Brand, PharmD Acknowledgements Original presentation by Chris Cawood, PharmD, with special thanks to Jen Lehman, PharmD candidate Content Contributions: Stephanie Powell, PharmD
Polypharmacy 101 Kimberly Brand, PharmD Acknowledgements Original presentation by Chris Cawood, PharmD, with special thanks to Jen Lehman, PharmD candidate Content Contributions: Stephanie Powell, PharmD
Appropriate prescribing and deprescribing for older people getting it right. Alan Davis Northland District Health Board
 Appropriate prescribing and deprescribing for older people getting it right Alan Davis Northland District Health Board Unused returns Potentially inappropriate medication use in the elderly 15% of older
Appropriate prescribing and deprescribing for older people getting it right Alan Davis Northland District Health Board Unused returns Potentially inappropriate medication use in the elderly 15% of older
1/21/2016 UPDATE ON THE AMERICAN GERIATRICS SOCIETY 2015 BEERS CRITERIA DISCLOSURE OBJECTIVES AGING GOALS BEERS CRITERIA
 UPDATE ON THE AMERICAN GERIATRICS SOCIETY 2015 BEERS CRITERIA DISCLOSURE I have no financial conflict of interest to disclose. Lacey Charbonneau, Pharm.D. PGY-1 Community Practice Resident Baptist Medical
UPDATE ON THE AMERICAN GERIATRICS SOCIETY 2015 BEERS CRITERIA DISCLOSURE I have no financial conflict of interest to disclose. Lacey Charbonneau, Pharm.D. PGY-1 Community Practice Resident Baptist Medical
Measure #238 (NQF 0022): Use of High-Risk Medications in the Elderly National Quality Strategy Domain: Patient Safety
: Use of High-Risk Medications in the Elderly National Quality Strategy Domain: Patient Safety") Measure #238 (NQF 0022): Use of High-Risk Medications in the Elderly National Quality Strategy Domain: Patient Safety 2015 PHYSICIAN QUALITY REPTING OPTIONS F INDIVIDUAL MEASURES REGISTRY ONLY DESCRIPTION:
Measure #238 (NQF 0022): Use of High-Risk Medications in the Elderly National Quality Strategy Domain: Patient Safety 2015 PHYSICIAN QUALITY REPTING OPTIONS F INDIVIDUAL MEASURES REGISTRY ONLY DESCRIPTION:
Perfect Endings. Home Alone. Senior Estimate. Staying Alive. Medication Madness
 Senior Estimate Home Alone Staying Alive Perfect Endings Medication Madness 10 10 10 10 10 20 20 20 20 20 30 30 30 30 30 40 40 40 40 40 50 50 50 50 50 Senior Estimate - 10 Patients who have multiple interacting
Senior Estimate Home Alone Staying Alive Perfect Endings Medication Madness 10 10 10 10 10 20 20 20 20 20 30 30 30 30 30 40 40 40 40 40 50 50 50 50 50 Senior Estimate - 10 Patients who have multiple interacting
Polypharmacy & De-prescribing In Older Adults
 Polypharmacy & De-prescribing In Older Adults Maryland Association of Osteopathic Physicians Annual Meeting September 15, 2018 Elizabeth Phung, DO Lead Clinical Associate Physician Beacham Center for Geriatric
Polypharmacy & De-prescribing In Older Adults Maryland Association of Osteopathic Physicians Annual Meeting September 15, 2018 Elizabeth Phung, DO Lead Clinical Associate Physician Beacham Center for Geriatric
Beers Criteria: Practical Considerations. A Clinician Education Tool. Curt Wood, RPh, CGP, FASCP
 Beers Criteria: Practical Considerations A Clinician Education Tool Curt Wood, RPh, CGP, FASCP Objectives: u Explain the purpose of the Beers Criteria u Discuss the key concepts in applying the Beers Criteria
Beers Criteria: Practical Considerations A Clinician Education Tool Curt Wood, RPh, CGP, FASCP Objectives: u Explain the purpose of the Beers Criteria u Discuss the key concepts in applying the Beers Criteria
Safe Medication Use. Holly Divine, PharmD, CGP, CDE. University of Kentucky College of Pharmacy Department of Pharmacy Practice & Science
 Safe Medication Use in the Older Adult Holly Divine, PharmD, CGP, CDE Associate Professor University of Kentucky College of Pharmacy Department of Pharmacy Practice & Science Objectives Know the principles
Safe Medication Use in the Older Adult Holly Divine, PharmD, CGP, CDE Associate Professor University of Kentucky College of Pharmacy Department of Pharmacy Practice & Science Objectives Know the principles
Measure #238 (NQF 0022): Use of High-Risk Medications in the Elderly National Quality Strategy Domain: Patient Safety
: Use of High-Risk Medications in the Elderly National Quality Strategy Domain: Patient Safety") Measure #238 (NQF 0022): Use of High-Risk Medications in the Elderly National Quality Strategy Domain: Patient Safety 2017 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process DESCRIPTION:
Measure #238 (NQF 0022): Use of High-Risk Medications in the Elderly National Quality Strategy Domain: Patient Safety 2017 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process DESCRIPTION:
Disclosure and Acknowledgements
 Greetings from Penn Nursing SOHN 37 TH ANNUAL CONGRESS AND NURSING SYMPOSIUM POLYPHARMACY AND OLDER ADULTS: HIGH RISK MEDS, TOO MANY MEDS, AND TOO FEW MEDS Sarah H. Kagan PhD, RN University of Pennsylvania,
Greetings from Penn Nursing SOHN 37 TH ANNUAL CONGRESS AND NURSING SYMPOSIUM POLYPHARMACY AND OLDER ADULTS: HIGH RISK MEDS, TOO MANY MEDS, AND TOO FEW MEDS Sarah H. Kagan PhD, RN University of Pennsylvania,
Chronic Obstructive Pulmonary Disease (COPD) Care Management Assessment
 Care Management Assessment") The questions in this brochure, based on the 2010 Global Initiative for Chronic Obstructive Lung Disease (GOLD) report, 1 are designed to help healthcare professionals (specifically case/care managers)
The questions in this brochure, based on the 2010 Global Initiative for Chronic Obstructive Lung Disease (GOLD) report, 1 are designed to help healthcare professionals (specifically case/care managers)
There s A Pill For That (But should my patient be on it?) A Review of Tools for the Evaluation of Optimal Prescribing in Geriatric Patients
 A Review of Tools for the Evaluation of Optimal Prescribing in Geriatric Patients") There s A Pill For That (But should my patient be on it?) A Review of Tools for the Evaluation of Optimal Prescribing in Geriatric Patients Marilyn N. Bulloch, PharmD, BCPS Assistant Clinical Professor
There s A Pill For That (But should my patient be on it?) A Review of Tools for the Evaluation of Optimal Prescribing in Geriatric Patients Marilyn N. Bulloch, PharmD, BCPS Assistant Clinical Professor
De-prescribing in Older Adults. Wael Hamade, MD, FAAFP 04/08/2016
 De-prescribing in Older Adults Wael Hamade, MD, FAAFP 04/08/2016 DISCLOSURES None of the faculty, planners, speakers, providers nor CME committee has any relevant financial relationships with commercial
De-prescribing in Older Adults Wael Hamade, MD, FAAFP 04/08/2016 DISCLOSURES None of the faculty, planners, speakers, providers nor CME committee has any relevant financial relationships with commercial
Topic: Chronic Heart Failure Cases for Monday s March 21th lecture.
 1 Phar6122: CV section Date: 3/10/05 Topic: Chronic Heart Failure Cases for Monday s March 21th lecture. Directions: This handout includes three chronic heart failure cases of increasing difficulty. In
1 Phar6122: CV section Date: 3/10/05 Topic: Chronic Heart Failure Cases for Monday s March 21th lecture. Directions: This handout includes three chronic heart failure cases of increasing difficulty. In
Managing medicines in older people. Jane Noble and Caroline Ralph
 Managing medicines in older people Jane Noble and Caroline Ralph Where? Community Hospital Care Home What? Prescribing Dispensing Administering Case 1 84 year old lady Admitted with reduced mobility Recurrent
Managing medicines in older people Jane Noble and Caroline Ralph Where? Community Hospital Care Home What? Prescribing Dispensing Administering Case 1 84 year old lady Admitted with reduced mobility Recurrent
Dementia Pharmacotherapy
 Dementia Pharmacotherapy 1 early therapeutic interventions can maximize pharmacologic efficacy with these agents 2 Selecting a Medication Not enough evidence to recommend one agent over another based on
Dementia Pharmacotherapy 1 early therapeutic interventions can maximize pharmacologic efficacy with these agents 2 Selecting a Medication Not enough evidence to recommend one agent over another based on
Deprescribing Unnecessary Medications: A Four-Part Process
 Deprescribing Unnecessary Medications: A Four-Part Process Scott Endsley, MD Fam Pract Manag. 2018;25(3):28-32. Abstract and Introduction Introduction www.medscape.com Ms. Horatio is a 76-year-old patient
Deprescribing Unnecessary Medications: A Four-Part Process Scott Endsley, MD Fam Pract Manag. 2018;25(3):28-32. Abstract and Introduction Introduction www.medscape.com Ms. Horatio is a 76-year-old patient
Pharmacology in the Elderly
 Pharmacology in the Elderly James Hardy Geriatrician, Royal North Shore Hospital A recent consultation Aspirin Clopidogrel Warfarin Coloxyl with senna Clearlax Methotrexate Paracetamol Pantoprazole Cholecalciferol
Pharmacology in the Elderly James Hardy Geriatrician, Royal North Shore Hospital A recent consultation Aspirin Clopidogrel Warfarin Coloxyl with senna Clearlax Methotrexate Paracetamol Pantoprazole Cholecalciferol
DEPRESCRIBING IN THE ELDERLY
 DEPRESCRIBING IN THE ELDERLY G E R I A T R I C S R E F R E S H E R D A Y W E D N E S D A Y, A P R I L 5 TH, 2 0 1 7 V É R O N I Q U E F R E N C H M E R K L E Y, M D, C C F P ( C O E ) B R U Y È R E C O
DEPRESCRIBING IN THE ELDERLY G E R I A T R I C S R E F R E S H E R D A Y W E D N E S D A Y, A P R I L 5 TH, 2 0 1 7 V É R O N I Q U E F R E N C H M E R K L E Y, M D, C C F P ( C O E ) B R U Y È R E C O
Mucky Meds: A (practical) approach the nightmare med list. Michelle Gibson, MD, CCFP (COE), FCFP and Erin Beattie, MD, CCFP
 approach the nightmare med list. Michelle Gibson, MD, CCFP (COE), FCFP and Erin Beattie, MD, CCFP") Mucky Meds: A (practical) approach the nightmare med list Michelle Gibson, MD, CCFP (COE), FCFP and Erin Beattie, MD, CCFP Faculty/Presenter Disclosure Faculty: Michelle Gibson Relationships with financial
Mucky Meds: A (practical) approach the nightmare med list Michelle Gibson, MD, CCFP (COE), FCFP and Erin Beattie, MD, CCFP Faculty/Presenter Disclosure Faculty: Michelle Gibson Relationships with financial
A Primer on Safe Prescribing to the Elderly. Dr. John Puxty
 A Primer on Safe Prescribing to the Elderly Dr. John Puxty Learning Objectives Describe an approach to safe prescribing for older patients. Appreciate the significance and causes of Polypharmacy. Identify
A Primer on Safe Prescribing to the Elderly Dr. John Puxty Learning Objectives Describe an approach to safe prescribing for older patients. Appreciate the significance and causes of Polypharmacy. Identify
Medication safety in vulnerable patient groups - Elderly patients -
 Woodennature/CC-BY-SA-3.0 http://theintelligence.de Medication safety in vulnerable patient groups - Elderly patients - 20th Congress of EAHP 25-27 March, 2015, Hamburg, Germany Dr. rer. nat. Beate Wickop
Woodennature/CC-BY-SA-3.0 http://theintelligence.de Medication safety in vulnerable patient groups - Elderly patients - 20th Congress of EAHP 25-27 March, 2015, Hamburg, Germany Dr. rer. nat. Beate Wickop
Prescribing Drugs to the Elderly
 Answers to your questions from University of Toronto experts Prescribing Drugs to the Elderly Can drugs do more harm than good? M.A. is a 90-year-old man living at home. He has dementia and due to wandering
Answers to your questions from University of Toronto experts Prescribing Drugs to the Elderly Can drugs do more harm than good? M.A. is a 90-year-old man living at home. He has dementia and due to wandering
Deprescribing in CKD patients: Is less more? Speaker: Dr. Judith G. Marin, PharmD
 2016 Deprescribing in CKD patients: Is less more? Speaker: Dr. Judith G. Marin, PharmD Case Mr. Kid Ney is a 75 y/o patient who has been on dialysis for the last 4 years (PD, then HD). PMHx: HTN, DM,
2016 Deprescribing in CKD patients: Is less more? Speaker: Dr. Judith G. Marin, PharmD Case Mr. Kid Ney is a 75 y/o patient who has been on dialysis for the last 4 years (PD, then HD). PMHx: HTN, DM,
Prescribing and Pharmacokinetic Considerations in the Elderly
 Prescribing and Pharmacokinetic Considerations in the Elderly Melanie A. Dodd, Pharm.D., Ph.C., BCPS Associate Professor of Pharmacy in Geriatrics College of Pharmacy The University of New Mexico OBJECTIVES
Prescribing and Pharmacokinetic Considerations in the Elderly Melanie A. Dodd, Pharm.D., Ph.C., BCPS Associate Professor of Pharmacy in Geriatrics College of Pharmacy The University of New Mexico OBJECTIVES
Deconstructing Polypharmacy. Alan B. Douglass, M.D. Director
 Deconstructing Polypharmacy Alan B. Douglass, M.D. Director Recognize this patient? Mrs. Brown- 82 years young Active Medical Problems Hypertension Hyperlipidemia Type 2 Diabetes Peripheral edema Osteoarthritis
Deconstructing Polypharmacy Alan B. Douglass, M.D. Director Recognize this patient? Mrs. Brown- 82 years young Active Medical Problems Hypertension Hyperlipidemia Type 2 Diabetes Peripheral edema Osteoarthritis
University of Hawaii Center on Aging
 University of Hawaii Center on Aging. Supported in part by a cooperative agreement No. 90AL0011-01-00 from the Administration on Aging, Administration for Community Living, U.S. Department of Health and
University of Hawaii Center on Aging. Supported in part by a cooperative agreement No. 90AL0011-01-00 from the Administration on Aging, Administration for Community Living, U.S. Department of Health and
Session 1: Circuit, Anticoagulation and Monitoring. Ashita Tolwani, MD, MSc Noel Oabel, BSN, RN, CNN 2019
 Session 1: Circuit, Anticoagulation and Monitoring Ashita Tolwani, MD, MSc Noel Oabel, BSN, RN, CNN 2019 Goals n Learn how to set up citrate anticoagulation for CVVH, CVVHD, CVVHDF using Prismaflex n Determine
Session 1: Circuit, Anticoagulation and Monitoring Ashita Tolwani, MD, MSc Noel Oabel, BSN, RN, CNN 2019 Goals n Learn how to set up citrate anticoagulation for CVVH, CVVHD, CVVHDF using Prismaflex n Determine
AGS Annual Meeting May Sponsored by the Polypharmacy Special Interest Group and the Pharmacists Section
 AGS Annual Meeting May 2010 Sponsored by the Polypharmacy Special Interest Group and the Pharmacists Section No financial conflicts of interest Sponsored by the Polypharmacy Special Interest Group Thanks
AGS Annual Meeting May 2010 Sponsored by the Polypharmacy Special Interest Group and the Pharmacists Section No financial conflicts of interest Sponsored by the Polypharmacy Special Interest Group Thanks
Do benzos, opioids, or strong anticholinergics cause delirium? Lisa Burry
 Do benzos, opioids, or strong anticholinergics cause delirium? Lisa Burry Delirium in the ICU Occurs in up to 85% of MICU/SICU MV patients 20-50% of lower severity ICU patients develop delirium Hypoactive
Do benzos, opioids, or strong anticholinergics cause delirium? Lisa Burry Delirium in the ICU Occurs in up to 85% of MICU/SICU MV patients 20-50% of lower severity ICU patients develop delirium Hypoactive
Iatrogenic Delirium. Heather Carey, PharmD, BCPP Clinical Psychiatric Pharmacist University Hospitals Richmond Medical Center
 Iatrogenic Delirium Heather Carey, PharmD, BCPP Clinical Psychiatric Pharmacist University Hospitals Richmond Medical Center Objectives Discuss proposed mechanisms of medication induced delirium Identify
Iatrogenic Delirium Heather Carey, PharmD, BCPP Clinical Psychiatric Pharmacist University Hospitals Richmond Medical Center Objectives Discuss proposed mechanisms of medication induced delirium Identify
Polypharmacy in the Elderly
 Polypharmacy in the Elderly Physiotherapy Alberta Conference September 24 th 2016 Lesley Charles Associate Professor and Program Director Division of Care of the Elderly Department of Family Medicine,
Polypharmacy in the Elderly Physiotherapy Alberta Conference September 24 th 2016 Lesley Charles Associate Professor and Program Director Division of Care of the Elderly Department of Family Medicine,
First, Do No Harm: The Geriatric Patient. Objectives. What is Delirium? 5/3/2011
 First, Do No Harm: The Geriatric Patient Debbie Harrell M.S., DPh Sandy McGill RN, MSN, MBA Laurence Solberg MD Amber Velasquez MSN, ANP BC Objectives The Learner will be able to: Identify the risks for
First, Do No Harm: The Geriatric Patient Debbie Harrell M.S., DPh Sandy McGill RN, MSN, MBA Laurence Solberg MD Amber Velasquez MSN, ANP BC Objectives The Learner will be able to: Identify the risks for
DEPRESCRIBING: A CASE-BASED APPROACH
 DEPRESCRIBING: A CASE-BASED APPROACH Cheryl Atherley- Todd, MD, CMD, FAAFP Assistant Professor Family Medicine/ Geriatrics Nova Southeastern University Andrea Levin, PharmD, BCACP Assistant Professor,
DEPRESCRIBING: A CASE-BASED APPROACH Cheryl Atherley- Todd, MD, CMD, FAAFP Assistant Professor Family Medicine/ Geriatrics Nova Southeastern University Andrea Levin, PharmD, BCACP Assistant Professor,
From medicines reconciliation to medicines review. Dr. Fatma Karapinar Hospital pharmacistepidemiologist
 From medicines reconciliation to medicines review Dr. Fatma Karapinar Hospital pharmacistepidemiologist Conflict of interest Nothing to disclose Questions Medication review is more important than medicines
From medicines reconciliation to medicines review Dr. Fatma Karapinar Hospital pharmacistepidemiologist Conflict of interest Nothing to disclose Questions Medication review is more important than medicines
Diabetes and the Elderly: Medication Considerations When Determining Benefits and Risks
 Diabetes and the Elderly: Medication Considerations When Determining Benefits and Risks Gretchen M. Ray, PharmD, PhC, BCACP, CDE Associate Professor UNM College of Pharmacy September 7 th, 2018 DISCLOSURES
Diabetes and the Elderly: Medication Considerations When Determining Benefits and Risks Gretchen M. Ray, PharmD, PhC, BCACP, CDE Associate Professor UNM College of Pharmacy September 7 th, 2018 DISCLOSURES
Prevention and Treatment of Migraines CAITLIN BARNES, PHARM.D. CANDIDATE AMBULATORY CARE JOE CAMMILLERI, PHARM.D. NATOHYA MALLORY, PHARM.D.
 Prevention and Treatment of Migraines CAITLIN BARNES, PHARM.D. CANDIDATE AMBULATORY CARE JOE CAMMILLERI, PHARM.D. NATOHYA MALLORY, PHARM.D. Objectives Present patient case Review epidemiology/pathophysiology
Prevention and Treatment of Migraines CAITLIN BARNES, PHARM.D. CANDIDATE AMBULATORY CARE JOE CAMMILLERI, PHARM.D. NATOHYA MALLORY, PHARM.D. Objectives Present patient case Review epidemiology/pathophysiology
All rights reserved. For Permissions, please
 Age and Ageing 2008; 37: 673 679 doi: 10.1093/ageing/afn197 Published electronically 1 October 2008 C The Author 2008. Published by Oxford University Press on behalf of the British Geriatrics Society.
Age and Ageing 2008; 37: 673 679 doi: 10.1093/ageing/afn197 Published electronically 1 October 2008 C The Author 2008. Published by Oxford University Press on behalf of the British Geriatrics Society.
Rational prescribing in the older adult. Assoc Prof Craig Whitehead
 Rational prescribing in the older adult Assoc Prof Craig Whitehead Introduction Physioloical ageing and frailty Medication risks in older adults Drug Burden Anticholinergic and sedative drug burden Cascade
Rational prescribing in the older adult Assoc Prof Craig Whitehead Introduction Physioloical ageing and frailty Medication risks in older adults Drug Burden Anticholinergic and sedative drug burden Cascade
Topic: Chronic Heart Failure Cases for Monday s March 21th lecture.
 1 Phar6122: CV section Date: 3/21/05 Topic: Chronic Heart Failure Cases for Monday s March 21th lecture. Directions: This handout includes three chronic heart failure cases of increasing difficulty. In
1 Phar6122: CV section Date: 3/21/05 Topic: Chronic Heart Failure Cases for Monday s March 21th lecture. Directions: This handout includes three chronic heart failure cases of increasing difficulty. In
Measure #238 (NQF 0022): Use of High-Risk Medications in the Elderly National Quality Strategy Domain: Patient Safety
: Use of High-Risk Medications in the Elderly National Quality Strategy Domain: Patient Safety") Measure #238 (NQF 0022): Use of High-Risk Medications in the Elderly National Quality Strategy Domain: Patient Safety 2016 PHYSICIAN QUALITY REPORTING OPTIONS FOR INDIVIDUAL MEASURES REGISTRY ONLY DESCRIPTION:
Measure #238 (NQF 0022): Use of High-Risk Medications in the Elderly National Quality Strategy Domain: Patient Safety 2016 PHYSICIAN QUALITY REPORTING OPTIONS FOR INDIVIDUAL MEASURES REGISTRY ONLY DESCRIPTION:
Update in Geriatrics: Choosing Wisely Primum Non Nocere
 Joseph G. Ouslander, M.D. Professor of Clinical Biomedical Science Senior Associate Dean for Geriatric Programs Chair, Department of Integrated Medical Science Charles E. Schmidt College of Medicine Professor
Joseph G. Ouslander, M.D. Professor of Clinical Biomedical Science Senior Associate Dean for Geriatric Programs Chair, Department of Integrated Medical Science Charles E. Schmidt College of Medicine Professor
Anthony J. Caprio, MD, CMD, AGSF 1
 Objectives 1) Discuss the dangers of polypharmacy 2) Review potentially inappropriate medications for older adults Doc, I think I am taking too many medications! 3) Develop strategies for prioritizing
Objectives 1) Discuss the dangers of polypharmacy 2) Review potentially inappropriate medications for older adults Doc, I think I am taking too many medications! 3) Develop strategies for prioritizing
Chitra Fernando, MD March 18, 2008
 Chitra Fernando, MD March 18, 2008 Definition Statistics Risk factors Why older adults are more prone to ADE Manifestations Inappropriate medications for older adults What can be done to minimize adverse
Chitra Fernando, MD March 18, 2008 Definition Statistics Risk factors Why older adults are more prone to ADE Manifestations Inappropriate medications for older adults What can be done to minimize adverse
TOP 5 DRUGS.. TO AVOID IN THE ELDERLY
 TOP 5 DRUGS.. TO AVOID IN THE ELDERLY Debbie Kwan, BScPhm., MSc., FCSHP Canadian Geriatrics Society, April 20, 2013 Disclosure of Potential for Conflict of Interest: Financial Disclosure: None Mar 26,
TOP 5 DRUGS.. TO AVOID IN THE ELDERLY Debbie Kwan, BScPhm., MSc., FCSHP Canadian Geriatrics Society, April 20, 2013 Disclosure of Potential for Conflict of Interest: Financial Disclosure: None Mar 26,
COMMON DRUG RELATED PROBLEMS SEEN IN PACE AND MECHANISMS TO MITIGATE RISK
 COMMON DRUG RELATED PROBLEMS SEEN IN PACE AND MECHANISMS TO MITIGATE RISK Robert L Alesiani, PharmD, CGP Chief Pharmacotherapy Officer CareKinesis, Inc. (a Tabula Rasa Healthcare Company) 2 3 4 5 Pharmacogenomics
COMMON DRUG RELATED PROBLEMS SEEN IN PACE AND MECHANISMS TO MITIGATE RISK Robert L Alesiani, PharmD, CGP Chief Pharmacotherapy Officer CareKinesis, Inc. (a Tabula Rasa Healthcare Company) 2 3 4 5 Pharmacogenomics
Objectives. Case Ruby. 1- Warfarin. 1- Warfarin. Warfarin discontinuation 8/13/ DRUGS TO STOP GIVING HOSPICE PATIENTS
 Objectives 10 DRUGS TO STOP GIVING HOSPICE PATIENTS Richard E. Allen MD, MPH Hospice Medical Director Family Medicine Residency Director Salt Lake City, Utah 2 Recognize 10 commonly prescribed medications
Objectives 10 DRUGS TO STOP GIVING HOSPICE PATIENTS Richard E. Allen MD, MPH Hospice Medical Director Family Medicine Residency Director Salt Lake City, Utah 2 Recognize 10 commonly prescribed medications
National Medicines Information Centre ST. JAMES S HOSPITAL DUBLIN 8 TEL or FAX
 National Medicines Information Centre ST. JAMES S HOSPITAL DUBLIN 8 TEL 01-4730589 or 1850-727-727 FAX 01-4730596 www.nmic.ie PRESCRIBING IN THE ELDERLY INTRODUCTION According to the most recent census
National Medicines Information Centre ST. JAMES S HOSPITAL DUBLIN 8 TEL 01-4730589 or 1850-727-727 FAX 01-4730596 www.nmic.ie PRESCRIBING IN THE ELDERLY INTRODUCTION According to the most recent census
Fairview Southdale Hospital Total Points: 50 RN/LPN Medication Assessment Passing: 45
 Fairview Southdale Hospital Total Points: 50 RN/LPN Medication Assessment Passing: 45 1. Your diabetic patient is to be started on an insulin drip at 8 units/hour. The insulin is supplied: 100 units in
Fairview Southdale Hospital Total Points: 50 RN/LPN Medication Assessment Passing: 45 1. Your diabetic patient is to be started on an insulin drip at 8 units/hour. The insulin is supplied: 100 units in
DEPRESCRIBING. Phil St John CSIM Workshop
 DEPRESCRIBING Phil St John CSIM Workshop Conflict of Interest Disclosure Consultant for: none Speaker for: none Received grant/research support from: CIHR, MHRC, Riverview Foundation Received honoraria
DEPRESCRIBING Phil St John CSIM Workshop Conflict of Interest Disclosure Consultant for: none Speaker for: none Received grant/research support from: CIHR, MHRC, Riverview Foundation Received honoraria
Polypharmacy and Polymorbid Patients: Practical Tips and Tricks
 Polypharmacy and Polymorbid Patients: Practical Tips and Tricks November 2, 2013 Faculty/Presenter Disclosure Faculty: Chris Fan-Lun, BScPhm, ACPR, CGP Pharmacist - Geriatric Medicine Clinical Practice
Polypharmacy and Polymorbid Patients: Practical Tips and Tricks November 2, 2013 Faculty/Presenter Disclosure Faculty: Chris Fan-Lun, BScPhm, ACPR, CGP Pharmacist - Geriatric Medicine Clinical Practice
The Failing Heart in Primary Care
 The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
Identifying Inappropriate Medications and Deprescribing Strategies ANGELA M. HILL, PHARM.D., RCPH GWEP JUNE 9, 2017
 Identifying Inappropriate Medications and Deprescribing Strategies ANGELA M. HILL, PHARM.D., RCPH GWEP LEARN@LUNCH JUNE 9, 2017 Objectives of Talk Identify inappropriate medications in a medication regimen
Identifying Inappropriate Medications and Deprescribing Strategies ANGELA M. HILL, PHARM.D., RCPH GWEP LEARN@LUNCH JUNE 9, 2017 Objectives of Talk Identify inappropriate medications in a medication regimen
Multidisciplinary Geriatric Trauma Care Guideline
 Multidisciplinary Geriatric Trauma Care Background Traumatic injury in the geriatric population is increasing in prevalence and is associated with higher mortality and complication rates comparted to younger
Multidisciplinary Geriatric Trauma Care Background Traumatic injury in the geriatric population is increasing in prevalence and is associated with higher mortality and complication rates comparted to younger
Reduction of High Risk Medications Using A Quality Initiative Perspective
 Reduction of High Risk Medications Using A Quality Initiative Perspective Richard Mueller PharmD, MBA, MS, Director of Pharmacy Dianne Hempel BSN, RN Quality Improvement Coordinator Objectives Learn what
Reduction of High Risk Medications Using A Quality Initiative Perspective Richard Mueller PharmD, MBA, MS, Director of Pharmacy Dianne Hempel BSN, RN Quality Improvement Coordinator Objectives Learn what
Polypharmacy: So Many Drugs, So Little Time. Shannon O. Smith, MD General Internal Medicine Conference
 Polypharmacy: So Many Drugs, So Little Time Shannon O. Smith, MD General Internal Medicine Conference Objectives 1. Recognize polypharmacy and what it means to your patients 2. Fix it. Patient Susie Q
Polypharmacy: So Many Drugs, So Little Time Shannon O. Smith, MD General Internal Medicine Conference Objectives 1. Recognize polypharmacy and what it means to your patients 2. Fix it. Patient Susie Q
Maximizing Medication Safety UNIVERSITY OF HAWAII AUGUST 31, 2016
 Maximizing Medication Safety UNIVERSITY OF HAWAII AUGUST 31, 2016 Adverse Drug Events (ADE s) RISK FACTORS FOR Adverse Drug Events (ADEs) 6 or more concurrent chronic conditions 12 or more doses of drugs/day
Maximizing Medication Safety UNIVERSITY OF HAWAII AUGUST 31, 2016 Adverse Drug Events (ADE s) RISK FACTORS FOR Adverse Drug Events (ADEs) 6 or more concurrent chronic conditions 12 or more doses of drugs/day
Special Generic Drug Pricing Program
 FREE PICK-UP & DELIVERY Flu-Shots Specialty prescription Compounding Wellness center providing health screenings for hypertension and diabetes $3 Special Generic Prescription Drug Program only offered
FREE PICK-UP & DELIVERY Flu-Shots Specialty prescription Compounding Wellness center providing health screenings for hypertension and diabetes $3 Special Generic Prescription Drug Program only offered
Learning Objectives 2/4/2016. Patrick Leung, Pharm.D., BCPS, PhC. Patrick Leung, Pharm.D., BCPS, PhC Davena Norris, Pharm.D., BCPS, PhC 2/20/2016
 Patrick Leung, Pharm.D., BCPS, PhC Davena Norris, Pharm.D., BCPS, PhC 2/20/2016 Learning Objectives Identify age-related pharmacokinetic and pharmacodynamic changes in older adults. Utilization the START/STOPP
Patrick Leung, Pharm.D., BCPS, PhC Davena Norris, Pharm.D., BCPS, PhC 2/20/2016 Learning Objectives Identify age-related pharmacokinetic and pharmacodynamic changes in older adults. Utilization the START/STOPP
Talking to patients with osteoporosis about initiating therapy
 Talking to patients with osteoporosis about initiating therapy Deborah Sellmeyer, MD Director, Johns Hopkins Metabolic Bone Center Dept of Medicine, Division of Endocrinology Disclosure DSMB member for
Talking to patients with osteoporosis about initiating therapy Deborah Sellmeyer, MD Director, Johns Hopkins Metabolic Bone Center Dept of Medicine, Division of Endocrinology Disclosure DSMB member for
Polypharmacy. Polypharmacy. Suboptimal Prescribing in Older Adults. Kenneth Schmader, MD Professor of Medicine-Geriatrics
 Polypharmacy Kenneth Schmader, MD Professor of Medicine-Geriatrics Polypharmacy Definition Causes Consequences Prevention/management Suboptimal Prescribing in Older Adults Overuse Polypharmacy Underuse
Polypharmacy Kenneth Schmader, MD Professor of Medicine-Geriatrics Polypharmacy Definition Causes Consequences Prevention/management Suboptimal Prescribing in Older Adults Overuse Polypharmacy Underuse
Taking the harm out of Polypharmacy Step by step. Karen Reid and Claire Stein Lead Integrated Care Pharmacist NHS Lothian
 Taking the harm out of Polypharmacy Step by step Karen Reid and Claire Stein Lead Integrated Care Pharmacist NHS Lothian Presentation: Polypharmacy Overview of the 2015 guidelines The Seven Steps Application
Taking the harm out of Polypharmacy Step by step Karen Reid and Claire Stein Lead Integrated Care Pharmacist NHS Lothian Presentation: Polypharmacy Overview of the 2015 guidelines The Seven Steps Application
An approach to prescribing in the elderly. Preamble
 An approach to prescribing in the elderly Dr K Outhoff Preamble Advances in medical technology, surgical procedures, medical practice and innovative drug development An increasing proportion of the population
An approach to prescribing in the elderly Dr K Outhoff Preamble Advances in medical technology, surgical procedures, medical practice and innovative drug development An increasing proportion of the population
Quality ID #238 (NQF 0022): Use of High-Risk Medications in the Elderly National Quality Strategy Domain: Patient Safety
: Use of High-Risk Medications in the Elderly National Quality Strategy Domain: Patient Safety") Quality ID #238 (NQF 0022): Use of High-Risk Medications in the Elderly National Quality Strategy Domain: Patient Safety 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process DESCRIPTION:
Quality ID #238 (NQF 0022): Use of High-Risk Medications in the Elderly National Quality Strategy Domain: Patient Safety 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process DESCRIPTION:
MEDICATION APPROPRIATENESS FOR THE AGING POPULATION. Building Partnerships for Successful Aging
 MEDICATION APPROPRIATENESS FOR THE AGING POPULATION Building Partnerships for Successful Aging Learning objectives Appreciate complexities involved in making appropriate clinical decisions in older adults
MEDICATION APPROPRIATENESS FOR THE AGING POPULATION Building Partnerships for Successful Aging Learning objectives Appreciate complexities involved in making appropriate clinical decisions in older adults
The base of evidence for the relative harm versus benefit
 EDITORIAL Protecting Patients from Adverse Drug Events: Propoxyphene, PIMs, and Drugs to Avoid in Older Adults Frederic R. Curtiss, PhD, RPh, CEBS, and Kathleen A. Fairman, MA The base of evidence for
EDITORIAL Protecting Patients from Adverse Drug Events: Propoxyphene, PIMs, and Drugs to Avoid in Older Adults Frederic R. Curtiss, PhD, RPh, CEBS, and Kathleen A. Fairman, MA The base of evidence for
MEASURING CARE QUALITY
 MEASURING CARE QUALITY Region December 2013 For Clinical Effectiveness of Care Measures of Performance From: Healthcare Effectiveness Data and Information Set (HEDIS ) HEDIS is a set of standardized performance
MEASURING CARE QUALITY Region December 2013 For Clinical Effectiveness of Care Measures of Performance From: Healthcare Effectiveness Data and Information Set (HEDIS ) HEDIS is a set of standardized performance
Stronger together - optimizing pharmacotherapy on geriatric wards?
 Stronger together - optimizing pharmacotherapy on geriatric wards? Clinicamp FOD 27/4/2018 Dr. Jean-Claude Lemper ( Geriater UZ Brussel) Apr. Julie Hias (ziekenhuisapotheker UZ Leuven) Project College
Stronger together - optimizing pharmacotherapy on geriatric wards? Clinicamp FOD 27/4/2018 Dr. Jean-Claude Lemper ( Geriater UZ Brussel) Apr. Julie Hias (ziekenhuisapotheker UZ Leuven) Project College
High Risk Medications: What Can Community Pharmacists Do to Make Patients Safer?
 CONTINUING EDUCATION High Risk Medications: What Can Community Pharmacists Do to Make Patients Safer? by Sean T. Lasota, PharmD Sept. 1, 2015 (expires Sept. 1, 2018) Activity Type: Knowledge-based To earn
CONTINUING EDUCATION High Risk Medications: What Can Community Pharmacists Do to Make Patients Safer? by Sean T. Lasota, PharmD Sept. 1, 2015 (expires Sept. 1, 2018) Activity Type: Knowledge-based To earn