DEMENTIA (Major Neurocognitive Disorder) SUSAN BEHNAWA, M.D. DIVISION OF GERIATRIC MEDICINE AND GERONTOLOGY UC IRVINE HEALTH SCHOOL OF MEDICINE
|
|
|
- Blake Andrews
- 6 years ago
- Views:
Transcription
 SUSAN BEHNAWA, M.D.")

1 DEMENTIA (Major Neurocognitive Disorder) SUSAN BEHNAWA, M.D. DIVISION OF GERIATRIC MEDICINE AND GERONTOLOGY UC IRVINE HEALTH SCHOOL OF MEDICINE
2 Objectives Review the epidemiology and social impact of Dementia Discuss the definition of Dementia Recognize the clinical presentation of Dementia Outline the diagnostic approach to patients Differentiate Mild Cognitive Impairment vs. Dementia Characterize the Major Dementia Syndromes Review Treatment and Management Approaches Discuss possible Prevention Strategies
3

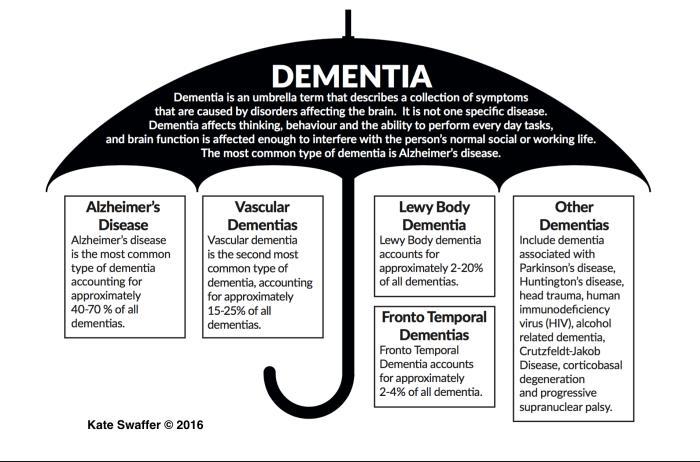
4 Types of Dementia Alzheimer s Disease (AD) is the most common type, accounting for ~2/3 of all cases and affecting 6-8% of those 65 years old Disease prevalence doubles every 5 years after age 60 yrs, 45%+ who are 85 yrs old have AD DLB now thought to be 2 nd MCC dementia FTD smaller percentage with younger age of onset Neurodegenerative diseases such as Huntington disease, Parkinson disease, head injury, alcoholism account for other
5 Epidemiology and Social Impact of AD An estimated 5.4 million Americans have Alzheimer's disease. By mid-century, the number of people living with Alzheimer's disease in the United States is projected to grow to 13.8 million, fueled in large part by the aging baby boom generation. Today, someone in the country develops Alzheimer's disease every 66 seconds. By 2050, one new case of Alzheimer's is expected to develop every 33 seconds, resulting in nearly 1 million new cases per year. In 2013, official death certificates recorded 84,767 deaths from Alzheimer's disease, making it the sixth leading cause of death in the United States and the fifth leading cause of death in Americans age 65 years. Between 2000 and 2013, deaths resulting from stroke, heart disease, and prostate cancer decreased 23%, 14%, and 11%, respectively, whereas deaths from Alzheimer's disease increased 71% (actual number of deaths likely much larger) In 2016, an estimated 700,000 Americans age 65 years will die with Alzheimer's disease, and many of them will die because of the complications caused by Alzheimer's disease.

6 Epidemiology and Social Impact of AD In 2015, more than 15 million family members and other unpaid caregivers provided an estimated 18.1 billion hours of care to people with Alzheimer's and other dementias, a contribution valued at more than $221 billion. Average per-person Medicare payments for services to beneficiaries age 65 years with Alzheimer's disease/other dementias are more than two and a half times as great as payments for all beneficiaries without these conditions, and Medicaid payments are 19 times as great. Total payments in 2016 for health care, long-term care and hospice services for people age 65 years with dementia are estimated to be $236 billion. The costs of Alzheimer's care may place a substantial financial burden on families, who often have to take money out of their retirement savings, cut back on buying food, and reduce their own trips to the doctor. In addition, many family members incorrectly believe that Medicare pays for nursing home care and other types of long-term care.

7 DSM-V Criteria: Major Neurocognitive Disorder (previously known as Dementia) 2013 Evidence from history and clinical assessment that indicates significant cognitive impairment in at least one of the following cognitive domains: Learning and Memory Language Executive Function Complex Attention Perceptual-Motor Function Social Cognition Impairment is acquired and represents a significant decline from previous level of functioning Cognitive deficits must interfere with independence in everyday activities In neurodegenerative dementias (i.e. Alzheimer s), the onset is insidious and progressive Disturbances are not occurring exclusively during the course of delirium Disturbances are not better accounted for by another mental disorder (e.g. Major Depressive Disorder, Schizophrenia)


8 Cognitive Domains Complex Attention Sustained, divided, and selective attention as well as processing speed Executive Functioning Planning, decision making, working memory error detection and correction, inhibition, and mental flexibility Learning and Memory All memory registers (e.g. short-term, semantic, autobiographical) and implicit learning Language Expressive and Receptive Language Perceptual-Motor Includes visual perception, visuo-constructional abilities, perceptual-motor, praxis, and gnosis Social Cognition Recognition of emotions and theory of mind

9 Normal Aging vs. Dementia Normal Cognitive Decline of aging is primarily mild changes in memory and rate of information processing; these are not progressive and do not affect daily function New learning is slower but still occurs, is usually well compensated with memory supports (e.g. lists) Self-reported memory loss does not appear to correlate with subsequent development of dementia; Informant-reported memory loss is much better predictor of current presence and future development of dementia In community-dwelling, cognitively normal individuals ages 62 to 100 years, learning or acquisition performance declined uniformly with increasing age. In contrast, delayed recall or forgetting remained relatively stable. Aging is associated with decline in learning of new information but not in memory retention. Patients with dementia may have difficulty with one or more of the following: Retaining new information (eg, trouble remembering events) Handling complex tasks (eg, balancing a checkbook) Reasoning (eg, unable to cope with unexpected events) Spatial ability and orientation (eg, getting lost in familiar places) Language (eg, word finding) Behavior
10 Normal Memory Changes vs Dementia TYPICAL AGING Complains about memory loss but able to provide detailed examples of forgetfulness Occasionally searches for words May have to pause to remember directions but doesn t get lost in familiar places Remembers recent important events; conversations are not impaired Interpersonal social skills are at the same level Able to function independently despite occasional memory lapses Losing things from time to time SYMPTOMS OF DEMENTIA May complain of memory loss only if asked; unable to recall specific instances Frequent word-finding pauses, substitutions Gets lost in familiar places; takes excessive time to return home Notable decline in memory for recent events and ability to converse Loss of interest in social activities; may behave in socially inappropriate ways Difficulty performing simple tasks; forgetting how to do things that have been done many times before Misplacing items and not being able to retrace steps to find them

11 Clinical Evaluation for Suspected Dementia Informant interview, patient interview, and office-based clinical assessment are most important Current condition, medical history, medications, substance use, living arrangements Onset and nature of symptoms Cognitive performance will be influenced by number of years of formal education Some tests are affected by language performance or cultural differences Improve accuracy by performing serial assessments to determine presence of a decline and using a medical interpreter when needed Assess ADLs and iadls Routine labs: CBC, Na, Ca, Bun/Cr, FBG, RPR, TSH, B12 If indicated: LFTs, Folic Acid, Homocysteine, MMA, UA, Utox, CSF, HIV, EKG, CXR In general, the diagnosis of dementia is clinical

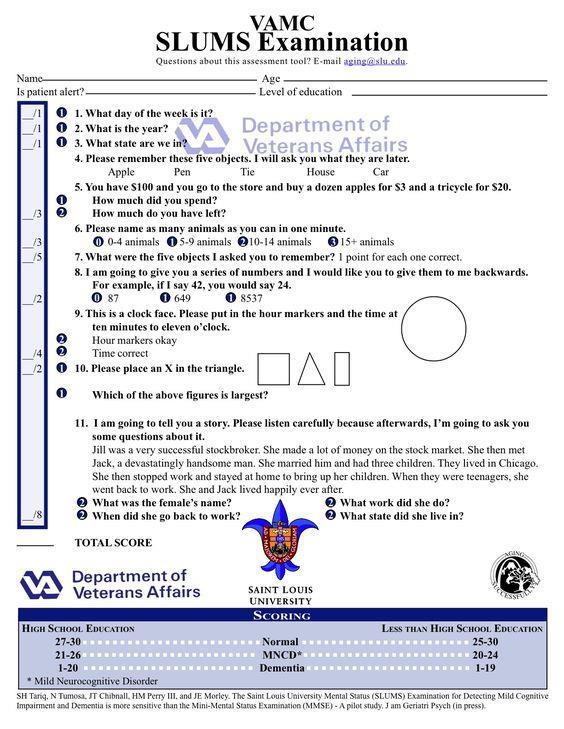
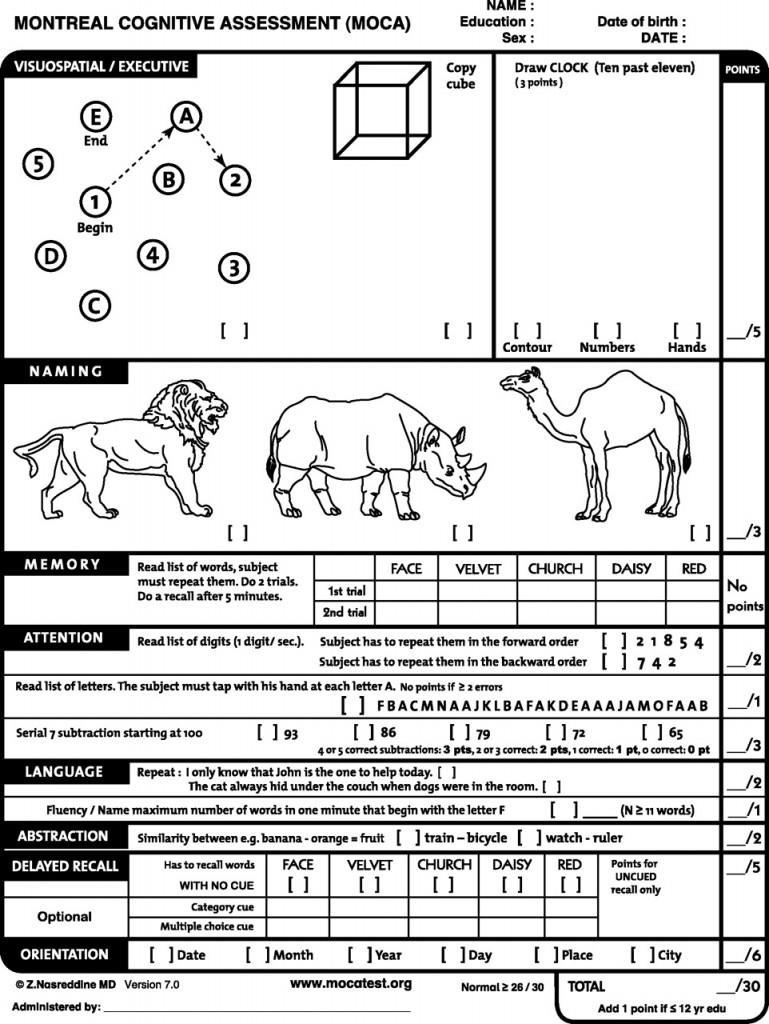
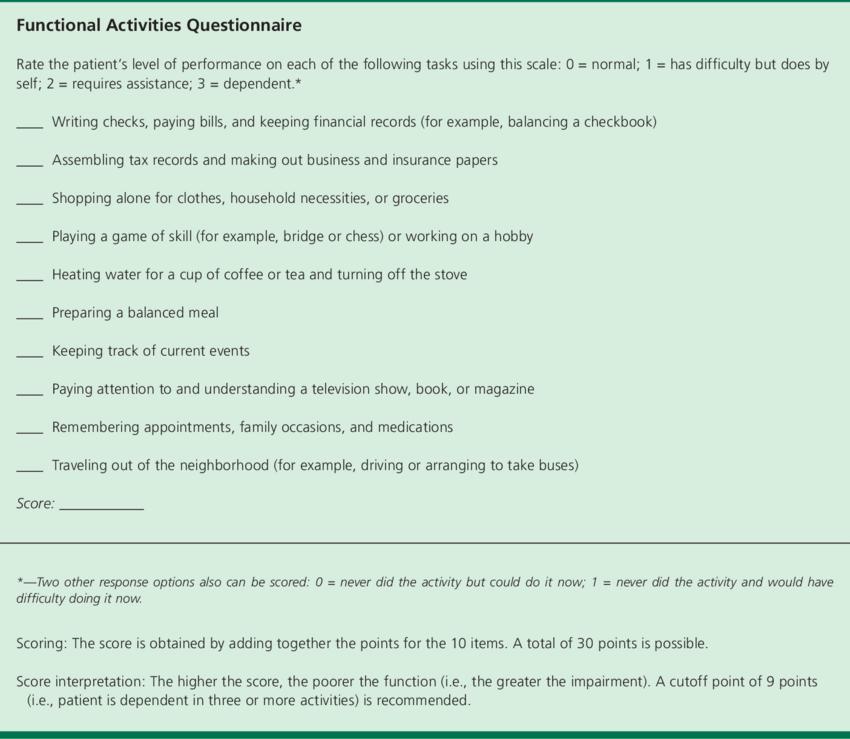
12 Cognition Screening Instruments Mini-Cog Visuospatial, Executive Function, Recall St. Louis University Mental Status Exam Orientation, Recall, Calculation, Naming, Attention, Executive Function Montreal Cognitive Assessment Orientation, Recall, Attention, Naming, Repetition, Verbal Fluency, Abstraction, Executive Function, Visuospatial Folstein Mini-Mental Status Exam* Orientation, Registration, Attention, Recall, Naming, Repetition, 3-step Command, Language, Visuospatial (*licensed version of MMSE should be purchased from Psychological Assessment Resources (PAR) for $1.23 per test) Functional Activities Questionnaire Informant Based, Executive Functioning, ADLs, Attention, Concentration, Memory, Home Safety

13
14
15 Brain Imaging Studies Helpful in the following situations: Onset <65 yrs of age, sudden onset or rapidly progressing symptoms, evidence of focal or asymmetrical neurologic deficits; clinical picture suggestive of NPH (onset within last year, gait disorder, unexplained incontinence is present); hx of recent fall or trauma Non-contrast CT head scan adequate to exclude intracranial bleeding, space-occupying lesions, and hydrocephalus; will see characteristic parietal and temporal deficits in AD or the widespread irregular deficits in vascular dementia MRI is often performed if vascular dementia is suspected, but white matter changes in T2 weighted MRI should not be overinterpreted Functional brain imaging studies such as PET may be useful when the diagnosis remains uncertain FDA has approved PET scanning with florbetapir, which binds brain amyloid, but few insurers provide payment, and guideless from NIA and AA still recommend limited use by specialists CSF analysis of beta-amyloid and phosphorylated tau has limited availability and interpretation is challenging
16 Delirium Disturbance of consciousness with reduced ability to focus, sustain, or shift attention A change in cognition or a perceptual disturbance not better explained by a preexisting, established, or evolving dementia Disturbance develops over a short period of time (usually hours to days) Disturbance tends to fluctuate during the course of the day Evidence suggesting cognitive disturbance caused by the direct physiological consequences of a medical condition Causes of Delirium D - drug use E - electrolyte and physiologic abnormalities L - lack of drugs (withdrawal, e.g. Etoh) I - infection R - reduced sensory input I - intracranial problems (stroke, bleeding, meningitis, post-ictal) U - urinary retention and fecal impaction M - myocardial problems (e.g. MI, arrhythmia, CHF) *Almost any acute illness may cause delirium*
17 Depression Depression and dementia may occur in the same patient. Patients with depression are more likely to complain about memory loss than those with dementia Patients with depression may have signs of psychomotor slowing and give poor effort on testing ("I just can t do this"), while those with dementia often try hard but respond with incorrect answers. People with history of depression/affective disorder may become demented Prevalence of older adults with depression ~ 10% People with dementia frequently become depressed - Perhaps as many as 25% of patients will experience depression during their course Apathy and affective (sad or anxious) presentations may also occur that may present differently than textbook depression Cognitive behavioral therapy limited with dementia SSRI s a good choice for medication, especially Celexa (Citalopram), Lexapro (Escitalopram), or Zoloft (Sertraline) Start low dose, and realize that will take longer to respond, watch for side effects, especially anorexia Avoid tricyclics due to anticholinergic effects Trazadone or Mirtazapine if sleep disturbances prominent

18 15 questions, may be self-administered 5 or more positive responses suggestive of clinically significant depression More severe cognitive impairment may limit effectiveness of screen If cognitive impairment mild, and depression severe, consider treating depression before making AD diagnosis
19 Neurocognitive Disorder (Dementia) Mild Neurocognitive Disorders (similar to MCI): Measurable decline in one or more cognitive domains causing the individual to use compensatory strategies in their management of iadls Major Neurocognitive Disorders: Measurable decline in one or more cognitive domains to a degree impairing his or her ability to manage iadls or ADLs independently. Subcategorized according to presumed etiology Primary Diagnosis would be Major or Mild NCD, followed by etiological subtype DSM-V has also added specifiers Behavioral Disturbances (with or without) Degree of severity in Major NCDs (Mild, Moderate, Severe) Possible versus Probable (when designating a specific dementia)
20 Mild Cognitive Impairment (MCI) Individuals who have a subjective complaint of cognitive decline in at least one domain (complex attention, executive function, learning and memory, language, perceptual-motor or social cognition) to a degree that is noticeable and measurable, but not to a degree that causes impairment in independent living. MCI as a diagnostic entity allows for identification and possible early treatment of individuals who may convert to AD (9-14/1,000 person-years) For individuals with MCI whose single domain of impairment is memory (amnestic MCI versus nonamnestic MCI), the rate of conversion to AD is predictably higher but not wholly predictive of AD or other dementias Nearly half of individuals with amnestic MCI maintain a stable degree of impairment or return to a state of normal cognition over 3-5 years DSM-V terminology oof 'mild neurocognitive disorder (mncd)' defined by a noticeable decrement in cognitive functioning that goes beyond normal changes seen in aging. It is a disorder that may progress to dementia - importantly, it may not. Presently, our understanding of mncd is derived from research on mild cognitive impairment (MCI).

21 Cognitive Impairment as a Spectrum



22 Alzheimer s Disease Most common; major risk factors are family history, genetic factors, head injury Gradual Onset, Progressive Decline in cognitive functioning Memory impairment is typically the core feature present in the earliest stages Pathology is associated with parietal and temporal regions of the brain Motor and sensory functions are spared until middle or late stages Autopsy findings of Beta-Amyloid plaques and Neurofibrillary Tangles (Tau protein) Difficulty learning and retaining new information early, later compromised ability to learn and retrieve information and pts are unable to access older, more distant memories Aphasia, apraxia, disorientation, visuospatial dysfunction, impaired judgement, and executive dysfunction are also present Probability of AD is amplified by presence of a biomarker in addition to clear decline in memory and learning Auguste Deter ( May April 1906). Nationality: German. Her maiden name is unknown. She married Karl Deter in the 1880s or so and together they had one daughter. Auguste had a normal life. However, during the late 1890s, she started showing symptoms of dementia. After many years, she became completely mindless, muttering to herself. She was the first person diagnosed with Alzheimer's Disease (named after Dr. Alois Alzheimer).
23 Biomarkers in Alzheimer s Disease Biomarkers of brain amyloid-beta (Aβ) protein deposition: low cerebrospinal fluid Aβ42 and positive PET amyloid imaging 3 major biomarkers of downstream neuronal degeneration or injury are: elevated CSF tau, [both total tau and phosphorylated tau (p-tau)]; decreased 18fluorodeoxyglucose (FDG) uptake on PET in temporo parietal cortex; disproportionate atrophy on structural magnetic resonance imaging in medial, basal, and lateral temporal lobe, and medial parietal cortex
24
25 Vascular Dementia Cognitive deficits most often associated with vascular damage (micro or macro) in nature Risk factors: HTN, DM, Age, CVA, EtOH, CV RFs May see focal neurologic deficits that accompany cognitive loss Abrupt onset, fluctuating course, stepwise decline Cognitive/Neurologic impairments correlate anatomically with area of ischemia More likely than AD to have depression, affective changes, disturbance of gait, and confusion Relatively high mixed etiology found in AD Temporal association of CV events, genetic predispositions, and/or neuroimaging date increase probability of a diagnosis of vascular dementia

26 Dementia with Lewy Bodies Both dementia and at least one of the following core features must be present: Recurrent and detailed visual hallucinations Parkinsonian signs Fluctuating changes in alertness/attention Poor visuospatial abilities are often out of proportion to other cognitive deficits Additional suggestive features may include autonomic dysfunction, sleep disorder, severe neuroleptic sensitivity, and psychiatric misidentification syndromes This diagnosis may overlap with AD and the dementia associated with Parkinson disease but having at least 2 core features raises the probability of dementia with Lewy bodies If Parkinson disease has been diagnosed or has been present for 1 yr before cognitive symptoms are seen, the diagnosis is more c/w Parkinson disease dementia If parkinsonian symptoms are present at the same time as cognitive symptoms, dementia with Lewy bodies should be considered

27 Frontotemporal Dementia Often seen in patients with onset of cognitive symptoms at a younger age Shrinking of the frontal and temporal regions; most common in men Executive and language dysfunction and significant behavioral changes Disinhibition and Hyperorality before significant memory decline Often have a profound effect on patient s social functioning Memory deficits are not as pronounced in the early stage Language impairment in FTD may progress much faster than other domains FTD probability increased by presence of known genetic marker and/or evidence of disproportionate frontal and/or temporal lobe involvement from neuroimaging
28 Treatment and Management of Dementia Goal is to enhance QOL and maximize functional performance Emphasis on non-pharmacological treatment Behavioral symptoms challenge both family members and professional caregivers Pharmacological treatment for behavioral problems recommended only after nonpharmacological treatments prove ineffective, or when there is an emergent need such as extreme patient distress or risk of physical violence Schedule regular appointments with PCP 3-6 months, screen for behavioral disturbance and proper sleep hygiene, caregiver well-being Family and Caregiver Education and support Environmental modification with attention to safety
29 Pharmacological Considerations Decreased renal clearance and hepatic impairment Drug interactions and adverse effects likely Anticholinergic side effects are a particular problem for patients with dementia because they can worsen cognitive impairment and lead to delirium Any nonessential medications with CNS adverse effects should be considered carefully
30 Cholinesterase Inhibitors Primary medications available for stabilizing cognitive function in Alzheimer s Dementia Currently approved by the FDA: Donepezil, Rivastigmine, and Galantamine By slowing the breakdown of the NT Acetylcholine, these medications are thought to facilitate memory function because of the association of acetylcholine and memory In clinical trials, these meds demonstrate a modest delay in cognitive decline compared with placebo Onset of behavioral problems and decline in ADLs is modestly delayed compared to placebo Widespread treatment in vascular dementia not currently recommended because of limited cognitive benefit and lack of sufficient data ChIs may be helpful in managing attention and behavioral disturbances/hallucinations associated in Dementia with Lewy Bodies
31 Cholinesterase Inhibitors Rivastigmine is approved by the FDA for use in Parkinson disease No role for ChIs in treating Frontotemporal Dementia; evidence suggests they may worsen agitation Effects are modest in all disorders Patients and Family should be counseled to have realistic expectations Discontinuation of the medication should be considered after a reasonable time period if decline continues at the rate expected without treatment In long-term therapy with initial positive responses to treatment but continued advancement of cognitive decline, unclear what effect discontinuation will have on cognition When cognitive decline persists despite maximum treatment with ChIs, tapering the medication over time may be considered Abrupt discontinuation is not recommended
32 Cholinesterase Inhibitors Dosed once daily, either in oral form (Donepezil and Galantamine) or as a 24-hr patch (Rivastigmine) Follow slow titration curve to maximize tolerable dosage while avoiding adverse effects Nausea, Diarrhea, Insomnia, Headaches, Dizziness, Orthostasis, Nightmares, Bradycardia
33 Aricept (Donepezil) Approved for mild-moderate-severe AD Begin 5 mg daily for four weeks Titrate up to 10 mg daily 23 mg dose available for severe dementia Common side effects: Upset stomach or poor appetite Sleep disturbances Syncope/Orthostasis/ Bradycardia
34 Exelon (Rivastigmine) Approved for mild to moderate AD and Parkinsons Dementia Pills Begin 1.5 mg orally twice a day Titrate up by 1.5 mg dose to target of 6 mg bid Titrate every 2 weeks to target Patches may have less GI side effects Begin 4.6 mg patch, change daily Titrate up in four weeks to 9.5 mg patch, then 13.3mg Common side effects same, with addition of rash from patches
35 Razadyne (Galantamine ) Approved for mild to moderate dementia DO NOT USE FOR MCI (Black Box Warning Increased Death) Available in short acting or long acting forms Goal daily doses are the same (16-24 mg) Begin 8 mg per day (either 4mg BID, or 8mgER once daily) 4 weeks between dosage titration
36 Memantine NMDA Antagonist Thought to have neuroprotective effects by reducing glutamate-mediated excitotoxicity Clinical trials support the efficacy of memantine in moderate to severe stages of AD Trials have yet to establish efficacy in other dementias Most common adverse effects are constipation, dizziness, and headache Can be used safely as a single agent and in conjunction with ChIs for moderate to severe AD
37 Namenda (Memantine) Namenda Titration Pack: Begin 5mg daily for one week, then 5 mg twice daily for one week, then 10mg in the morning and 5mg in the evening for one week, then 10mg twice daily Target dose is 10 mg bid but once/day may be adequate (long half life - hrs). (May need to dose adjust for renal failure). Very well tolerated. May reduce GI side effects of cholinesterase inhibitors (can start before or with).
38 Other Cognitive Enhancers Antioxidants Gingko Biloba Vitamin E B vitamins Omega 3 fatty acids Medium chain triglycerides Other OTC supplements
39 Antidepressants Consider for AD patients with Depressive symptoms, including depressed mood, appetite loss, insomnia, fatigue, irritability, agitations SSRIs can be helpful in managing disinhibitions and compulsive behaviors associated with FTDs However SSRIs and SNRIs can possibly exacerbate risk of fall, especially those with greater anticholinergic tone (e.g. Paroxetine)
40 Behavioral and Psychological Symptoms of Dementia (BPSD) Very common problem, ranging from sundowning, to anger, to oppositional behavior, to wandering. Hallucinations, Delusions, Affective syndrome, Depression, Anxiety, Irritability, Agitation, Behavioral Syndrome, Euphoria, Disinhibition, Apathy, Aberrant Motor behaviors, Sleep disturbances Prevalence 60-80% depending on setting Incidence over any patient s course >80% Frequent cause of hospitalization, nursing home placement, caregiver burden (and burnout) No easy answers Caregiver education Safe environments Activities focused on giving patients satisfaction, adapted to current capabilities When considering medications, ask: Are you treating the patient or the caregiver?
41 Psychoactive Medications Paranoia, agitation, and irritability are best managed by non-pharmacologic strategies Reduce overstimulation, distraction, redirection, physical activity 1 st and 2 nd generation antipsychotics help control behavioral and psychological sx of dementia All antipsychotics increase risk of all-cause mortality in setting of dementia ALL carry risk of death/black box warning. Consider written informed consent. Frequently attempt to taper Avoid use of BZDs and meds with anticholinergic effects Antidepressants with sedating effects (Mirtazapine, Trazodone) can be considered in management of insomnia
42 Sleep Disturbance in Dementia Day/night reversal hard on caregivers Overall sleep and quality of sleep impaired Treat the patient, support the caregiver Daytime activity Melatonin 1-3mg before bedtime Trazadone, Remeron sometimes helpful Avoid benzo s, z-drugs
43 Concomitant Medical Problems Err on the side of safety. DM: hypoglycemia more dangerous than modestly elevated glucose HTN: orthostatic hypotension and risks of falls are substantial Medications that impair food intake increase risks Meds that impair cognition to be avoided Often necessary to compromise with once daily regimens to improve compliance Nutrition and SafetyConditions Especially important to focus on prognosis and goals of care
44 Caregiver Burnout The Caregiver Burden Inventory (CBI) 22 items, with 5 possible responses per item Never, Rarely, Sometimes, Quite Frequently, Nearly Always Composite numeric score and five subscale scores (0-4) Scores of 36 or higher indicative of significant burden May be used as self-report or via interview A strategy for self-report during an office visit




45 Supporting the Caregiver During the past month have you often been bothered by feeling down, depressed, or hopeless? During the past month have you often been bothered by little interest or pleasure in doing things? If concerned about significant depression, considering asking about thoughts of self-harm, or harm directed at care reciever. A delicate issue if not the provider for caregiver. Just asking about burden is helpful. Validate the caregiving experience/role. People want to know if they are doing enough or what they are supposed to be doing? Community support resources Alzheimer s Association support groups

46 Dementia is a Terminal Disease POLST Form Timely discussions with patients and families Recognition of decline and poor prognosis Adequate diagnosis and treatment of pain Restricted use of feeding tubes: No improved survival, No improved nutritional status, No improved functional status, No prevention of aspiration Careful hand feeding is much more beneficial, for patient and caregiver, and safer. Late stage: people become bedfast, have swallowing difficulties, lose the ability to communicate basic information and needs, have increased risk for infections and death Referral to Hospice in a timely manner
47
WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient
 DEMENTIA WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient Progressive and disabling Not an inherent aspect of
DEMENTIA WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient Progressive and disabling Not an inherent aspect of
Diagnosis and Treatment of Alzhiemer s Disease
 Diagnosis and Treatment of Alzhiemer s Disease Roy Yaari, MD, MAS Director, Memory Disorders Clinic, Banner Alzheimer s Institute 602-839-6900 Outline Introduction Alzheimer s disease (AD)Guidelines -revised
Diagnosis and Treatment of Alzhiemer s Disease Roy Yaari, MD, MAS Director, Memory Disorders Clinic, Banner Alzheimer s Institute 602-839-6900 Outline Introduction Alzheimer s disease (AD)Guidelines -revised
ALZHEIMER S DISEASE. Mary-Letitia Timiras M.D. Overlook Hospital Summit, New Jersey
 ALZHEIMER S DISEASE Mary-Letitia Timiras M.D. Overlook Hospital Summit, New Jersey Topics Covered Demography Clinical manifestations Pathophysiology Diagnosis Treatment Future trends Prevalence and Impact
ALZHEIMER S DISEASE Mary-Letitia Timiras M.D. Overlook Hospital Summit, New Jersey Topics Covered Demography Clinical manifestations Pathophysiology Diagnosis Treatment Future trends Prevalence and Impact
Dementia. Aetiology, pathophysiology and the role of neuropsychological testing. Dr Sheng Ling Low Geriatrician
 Dementia Aetiology, pathophysiology and the role of neuropsychological testing Dr Sheng Ling Low Geriatrician Topics to cover Why is dementia important What is dementia Differentiate between dementia,
Dementia Aetiology, pathophysiology and the role of neuropsychological testing Dr Sheng Ling Low Geriatrician Topics to cover Why is dementia important What is dementia Differentiate between dementia,
The Person: Dementia Basics
 The Person: Dementia Basics Objectives 1. Discuss how expected age related changes in the brain might affect an individual's cognition and functioning 2. Discuss how changes in the brain due to Alzheimer
The Person: Dementia Basics Objectives 1. Discuss how expected age related changes in the brain might affect an individual's cognition and functioning 2. Discuss how changes in the brain due to Alzheimer
Assessing and Managing the Patient with Cognitive Decline
 Assessing and Managing the Patient with Cognitive Decline Center of Excellence For Alzheimer s Disease for State of NY Capital Region Alzheimer s Center of Albany Medical Center Earl A. Zimmerman, MD Professor
Assessing and Managing the Patient with Cognitive Decline Center of Excellence For Alzheimer s Disease for State of NY Capital Region Alzheimer s Center of Albany Medical Center Earl A. Zimmerman, MD Professor
Dementia. Assessing Brain Damage. Mental Status Examination
 Dementia Assessing Brain Damage Mental status examination Information about current behavior and thought including orientation to reality, memory, and ability to follow instructions Neuropsychological
Dementia Assessing Brain Damage Mental status examination Information about current behavior and thought including orientation to reality, memory, and ability to follow instructions Neuropsychological
Michael A. Lobatz MD The Neurology Center Scripps Rehabilitation Center
 Michael A. Lobatz MD The Neurology Center Scripps Rehabilitation Center Dementia an acquired syndrome consisting of a decline in memory and other cognitive functions Alzheimer s Disease Fronto temporal
Michael A. Lobatz MD The Neurology Center Scripps Rehabilitation Center Dementia an acquired syndrome consisting of a decline in memory and other cognitive functions Alzheimer s Disease Fronto temporal
Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE
 Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE Objectives At the conclusion of the session, participants will be
Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE Objectives At the conclusion of the session, participants will be
The ABCs of Dementia Diagnosis
 The ABCs of Dementia Diagnosis Dr. Robin Heinrichs, Ph.D., ABPP Board Certified Clinical Neuropsychologist Associate Professor, Psychiatry & Behavioral Sciences Director of Neuropsychology Training What
The ABCs of Dementia Diagnosis Dr. Robin Heinrichs, Ph.D., ABPP Board Certified Clinical Neuropsychologist Associate Professor, Psychiatry & Behavioral Sciences Director of Neuropsychology Training What
DEMENTIA? 45 Million. What is. WHAT IS DEMENTIA Dementia is a disturbance in a group of mental processes including: 70% Dementia is not a disease
 What is PRESENTS DEMENTIA? WHAT IS DEMENTIA Dementia is a disturbance in a group of mental processes including: Memory Reasoning Planning Learning Attention Language Perception Behavior AS OF 2013 There
What is PRESENTS DEMENTIA? WHAT IS DEMENTIA Dementia is a disturbance in a group of mental processes including: Memory Reasoning Planning Learning Attention Language Perception Behavior AS OF 2013 There
Alzheimer s Disease. Pathophysiology: Alzheimer s disease (AD) is a progressive dementia affecting cognition, behavior,
 is a progressive dementia affecting cognition, behavior,") 2 Alzheimer s Disease Alzheimer s disease (AD) is a progressive dementia affecting cognition, behavior, and functional status with no known cause or cure. Patients eventually lose cognitive, analytical,
2 Alzheimer s Disease Alzheimer s disease (AD) is a progressive dementia affecting cognition, behavior, and functional status with no known cause or cure. Patients eventually lose cognitive, analytical,
Dementia Medications Acetylcholinesterase Inhibitors (AChEIs) and Glutamate (NMDA) Receptor Antagonist
 and Glutamate (NMDA) Receptor Antagonist") Dementia Medications Acetylcholinesterase Inhibitors (AChEIs) and Glutamate (NMDA) Receptor Antagonist Medication Dosage Indication for Use Aricept (donepezil) Exelon (rivastigmine) 5mg 23mg* ODT 5mg Solution
Dementia Medications Acetylcholinesterase Inhibitors (AChEIs) and Glutamate (NMDA) Receptor Antagonist Medication Dosage Indication for Use Aricept (donepezil) Exelon (rivastigmine) 5mg 23mg* ODT 5mg Solution
Alzheimer's disease (AD), also known as Senile Dementia of the Alzheimer Type (SDAT) or simply Alzheimer s is the most common form of dementia.
, also known as Senile Dementia of the Alzheimer Type (SDAT) or simply Alzheimer s is the most common form of dementia.") CHAPTER 3 Alzheimer's disease (AD), also known as Senile Dementia of the Alzheimer Type (SDAT) or simply Alzheimer s is the most common form of dementia. This incurable, degenerative, terminal disease
CHAPTER 3 Alzheimer's disease (AD), also known as Senile Dementia of the Alzheimer Type (SDAT) or simply Alzheimer s is the most common form of dementia. This incurable, degenerative, terminal disease
Dementia: It s Not Always Alzheimer s
 Dementia: It s Not Always Alzheimer s A Caregiver s Perspective Diane E. Vance, Ph.D. Mid-America Institute on Aging and Wellness 2017 My Background Caregiver for my husband who had Lewy Body Dementia
Dementia: It s Not Always Alzheimer s A Caregiver s Perspective Diane E. Vance, Ph.D. Mid-America Institute on Aging and Wellness 2017 My Background Caregiver for my husband who had Lewy Body Dementia
PROJECTION: Worlds dementia population is expected to triple by 2050
 DEMENTIA C L I S K C O N S U LTA N T P H Y S I C I A N I N A C U T E M E D I C I N E A N D G E R I AT R I C M E D I C I N E, B A R N E T H O S P I TA L, R O YA L F R E E N H S F O U N D AT I O N T R U
DEMENTIA C L I S K C O N S U LTA N T P H Y S I C I A N I N A C U T E M E D I C I N E A N D G E R I AT R I C M E D I C I N E, B A R N E T H O S P I TA L, R O YA L F R E E N H S F O U N D AT I O N T R U
Significance A Busy Clinician's Guide to Seniors with Memory Loss
 Significance A Busy Clinician's Guide to Seniors with Memory Loss Victoria Braund MD FACP CMD Division of Geriatrics. NorthShore University HealthSystem Alzheimer's disease is the sixth leading cause of
Significance A Busy Clinician's Guide to Seniors with Memory Loss Victoria Braund MD FACP CMD Division of Geriatrics. NorthShore University HealthSystem Alzheimer's disease is the sixth leading cause of
The Basics of Alzheimer s Disease
 2017 Memory Loss Conference The Basics of Alzheimer s Disease Tom Ala, MD Center for Alzheimer s Disease and Related Disorders Southern Illinois University School of Medicine Springfield, Illinois SIU
2017 Memory Loss Conference The Basics of Alzheimer s Disease Tom Ala, MD Center for Alzheimer s Disease and Related Disorders Southern Illinois University School of Medicine Springfield, Illinois SIU
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017.
 DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
Memory Loss, Dementia and Alzheimer's Disease: The Basics
 Memory Loss, Dementia and Alzheimer's Disease: The Basics What is memory loss? What is age-related memory loss? Typical changes Typical age-related changes involve: Making a bad decision once in a while
Memory Loss, Dementia and Alzheimer's Disease: The Basics What is memory loss? What is age-related memory loss? Typical changes Typical age-related changes involve: Making a bad decision once in a while
A BRIEF LOOK AT DEMENTIA
 Dementia A BRIEF LOOK AT DEMENTIA David Kaufman, MD Neurology Consultants of Bellin Health November 2, 2017 Defined as a progressive decline in cognitive function that impairs daily activities. Always
Dementia A BRIEF LOOK AT DEMENTIA David Kaufman, MD Neurology Consultants of Bellin Health November 2, 2017 Defined as a progressive decline in cognitive function that impairs daily activities. Always
Alzheimer s Disease - Dementia
 - Dementia Neurocognitive disorder with dysfunction or loss of " Memory " Orientation " Attention " Language " Judgment " Reasoning Other characteristics that can manifest " Personality changes " Behavioral
- Dementia Neurocognitive disorder with dysfunction or loss of " Memory " Orientation " Attention " Language " Judgment " Reasoning Other characteristics that can manifest " Personality changes " Behavioral
WHEN THE GOING GETS TOUGH: Working Through the Challenges of Dementia Together. Presented by
 WHEN THE GOING GETS TOUGH: Working Through the Challenges of Dementia Together Presented by Our agenda for today Understanding behavioral symptoms in people living with dementia Briefly review key strategies
WHEN THE GOING GETS TOUGH: Working Through the Challenges of Dementia Together Presented by Our agenda for today Understanding behavioral symptoms in people living with dementia Briefly review key strategies
Caring Sheet #11: Alzheimer s Disease:
 CARING SHEETS: Caring Sheet #11: Alzheimer s Disease: A Summary of Information and Intervention Suggestions with an Emphasis on Cognition By Shelly E. Weaverdyck, PhD Introduction This caring sheet focuses
CARING SHEETS: Caring Sheet #11: Alzheimer s Disease: A Summary of Information and Intervention Suggestions with an Emphasis on Cognition By Shelly E. Weaverdyck, PhD Introduction This caring sheet focuses
Understanding Dementia
 Dementia Handbook for Carers Essex Understanding Dementia What is dementia? 1 Summary of dementia symptoms 4 Medication and treatment 5 1 Dementia is the name for several conditions that lead to the progressive
Dementia Handbook for Carers Essex Understanding Dementia What is dementia? 1 Summary of dementia symptoms 4 Medication and treatment 5 1 Dementia is the name for several conditions that lead to the progressive
Overview. Case #1 4/20/2012. Neuropsychological assessment of older adults: what, when and why?
 Neuropsychological assessment of older adults: what, when and why? Benjamin Mast, Ph.D. Associate Professor & Vice Chair, Psychological & Brain Sciences Associate Clinical Professor, Family & Geriatric
Neuropsychological assessment of older adults: what, when and why? Benjamin Mast, Ph.D. Associate Professor & Vice Chair, Psychological & Brain Sciences Associate Clinical Professor, Family & Geriatric
Evaluation and Treatment of Dementia
 Evaluation and Treatment of Dementia Jeffrey M. Burns, MD Edward H. Hashinger Professor of Neurology Co-Director, KU Alzheimer s Disease Center Director, Clinical and Translational Science Unit Disclosures
Evaluation and Treatment of Dementia Jeffrey M. Burns, MD Edward H. Hashinger Professor of Neurology Co-Director, KU Alzheimer s Disease Center Director, Clinical and Translational Science Unit Disclosures
DISCLOSURES. Objectives. THE EPIDEMIC of 21 st Century. Clinical Assessment of Cognition: New & Emerging Tools for Diagnosing Dementia NONE TO REPORT
 Clinical Assessment of Cognition: New & Emerging Tools for Diagnosing Dementia DISCLOSURES NONE TO REPORT Freddi Segal Gidan, PA, PhD USC Keck School of Medicine Rancho/USC California Alzheimers Disease
Clinical Assessment of Cognition: New & Emerging Tools for Diagnosing Dementia DISCLOSURES NONE TO REPORT Freddi Segal Gidan, PA, PhD USC Keck School of Medicine Rancho/USC California Alzheimers Disease
4/11/2017. The impact of Alzheimer s disease. Typical changes. The impact of Alzheimer s disease. Problematic changes. Problematic changes
 The impact of Alzheimer s disease Ron Petersen, MD, PhD, is Director of the Mayo Alzheimer's Disease Research Center. 2 The impact of Alzheimer s disease Typical changes Typical age-related changes involve:
The impact of Alzheimer s disease Ron Petersen, MD, PhD, is Director of the Mayo Alzheimer's Disease Research Center. 2 The impact of Alzheimer s disease Typical changes Typical age-related changes involve:
Addressing Difficult Behaviors in Dementia
 Addressing Difficult Behaviors in Dementia GEORGE SCHOEPHOERSTER, MD GERIATRICIAN GENEVIVE/CENTRACARE CLINIC Objectives By the end of the session, you will be able to: 1) Explain the role of pain management
Addressing Difficult Behaviors in Dementia GEORGE SCHOEPHOERSTER, MD GERIATRICIAN GENEVIVE/CENTRACARE CLINIC Objectives By the end of the session, you will be able to: 1) Explain the role of pain management
DEMENTIA ANDREA BERG, MD
 DEMENTIA ANDREA BERG, MD What Is Dementia? Decline in memory, language, problem-solving and other cognitive skills that affects a persons ability to perform everyday activities Progressive and disabling
DEMENTIA ANDREA BERG, MD What Is Dementia? Decline in memory, language, problem-solving and other cognitive skills that affects a persons ability to perform everyday activities Progressive and disabling
OLD AGE PSYCHIATRY. Dementia definition TYPES OF DEMENTIA. Other causes. Psychiatric disorders of the elderly. Dementia.
 Psychiatric disorders of the elderly OLD AGE PSYCHIATRY Dementia Depression Delusional disorder/late onset schizophrenia Delirium Dementia definition LOCALISATION OF CEREBRAL FUNCTION Impairment of multiple
Psychiatric disorders of the elderly OLD AGE PSYCHIATRY Dementia Depression Delusional disorder/late onset schizophrenia Delirium Dementia definition LOCALISATION OF CEREBRAL FUNCTION Impairment of multiple
Dementia Basics. Welcome! What to expect and how to handle a dementia diagnosis. In partnership with Scripps Health.
 Dementia Basics What to expect and how to handle a dementia diagnosis March 18, 2017 In partnership with Scripps Health Welcome! 1 Welcome Kristin Gaspar San Diego County Supervisor District 3 2 Our Mission:
Dementia Basics What to expect and how to handle a dementia diagnosis March 18, 2017 In partnership with Scripps Health Welcome! 1 Welcome Kristin Gaspar San Diego County Supervisor District 3 2 Our Mission:
Dementia and Alzheimer s disease
 Since 1960 Medicine Korat โรงพยาบาลมหาราชนครราชส มา Dementia and Alzheimer s disease Concise Reviews PAWUT MEKAWICHAI MD DEPARTMENT of MEDICINE MAHARAT NAKHON RATCHASIMA HOSPITAL 1 Prevalence Increase
Since 1960 Medicine Korat โรงพยาบาลมหาราชนครราชส มา Dementia and Alzheimer s disease Concise Reviews PAWUT MEKAWICHAI MD DEPARTMENT of MEDICINE MAHARAT NAKHON RATCHASIMA HOSPITAL 1 Prevalence Increase
DSM-5 MAJOR AND MILD NEUROCOGNITIVE DISORDERS (PAGE 602)
") SUPPLEMENT 2 RELEVANT EXTRACTS FROM DSM-5 The following summarizes the neurocognitive disorders in DSM-5. For the complete DSM-5 see Diagnostic and Statistical Manualof Mental Disorders, 5th edn. 2013,
SUPPLEMENT 2 RELEVANT EXTRACTS FROM DSM-5 The following summarizes the neurocognitive disorders in DSM-5. For the complete DSM-5 see Diagnostic and Statistical Manualof Mental Disorders, 5th edn. 2013,
Dementia NICE Guidelines Update. Key points for primary care - NICE guideline (June 2018 update ) 26 September 2018
 26 September 2018") Dementia NICE Guidelines Update Key points for primary care - NICE guideline (June 2018 update ) 26 September 2018 How NICE guidelines are reviewed Multidisciplinary guideline committee established Review
Dementia NICE Guidelines Update Key points for primary care - NICE guideline (June 2018 update ) 26 September 2018 How NICE guidelines are reviewed Multidisciplinary guideline committee established Review
Clinical Diagnosis. Step 1: Dementia or not? Diagnostic criteria for dementia (DSM-IV)
") Step 1: Dementia or not? Diagnostic criteria for dementia (DSM-IV) A. The development of multiple cognitive deficits manifested by both 1 and 2 1 1. Memory impairment 2. One (or more) of the following
Step 1: Dementia or not? Diagnostic criteria for dementia (DSM-IV) A. The development of multiple cognitive deficits manifested by both 1 and 2 1 1. Memory impairment 2. One (or more) of the following
PRACTICAL MANAGEMENT OF DEPRESSION IN OLDER ADULTS. Lee A. Jennings, MD MSHS Assistant Professor Division of Geriatrics, UCLA
 CASE #1 PRACTICAL MANAGEMENT OF DEPRESSION IN OLDER ADULTS Lee A. Jennings, MD MSHS Assistant Professor Division of Geriatrics, UCLA OBJECTIVES Epidemiology Presentation in older adults Assessment Treatment
CASE #1 PRACTICAL MANAGEMENT OF DEPRESSION IN OLDER ADULTS Lee A. Jennings, MD MSHS Assistant Professor Division of Geriatrics, UCLA OBJECTIVES Epidemiology Presentation in older adults Assessment Treatment
GERIATRIC MENTAL HEALTH AND MEDICATION TREATMENT
 Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences GERIATRIC MENTAL HEALTH AND MEDICATION TREATMENT RUTH KOHEN ASSOCIATE PROFESSOR UW DEPARTMENT OF PSYCHIATRY 5-4-2017
Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences GERIATRIC MENTAL HEALTH AND MEDICATION TREATMENT RUTH KOHEN ASSOCIATE PROFESSOR UW DEPARTMENT OF PSYCHIATRY 5-4-2017
Dementia and Delirium: A Neurologist s Approach to Altered Mental Status. Case 1 4/7/11. Which of the following evaluations is your next step?
 Dementia and Delirium: A Neurologist s Approach to Altered Mental Status S. Andrew Josephson, MD Director, Neurohospitalist Program Medical Director, Inpatient Neurology University of California San Francisco
Dementia and Delirium: A Neurologist s Approach to Altered Mental Status S. Andrew Josephson, MD Director, Neurohospitalist Program Medical Director, Inpatient Neurology University of California San Francisco
Dementia and Fall Geriatric Interprofessional Training. Wael Hamade, MD, FAAFP
 Dementia and Fall Geriatric Interprofessional Training Wael Hamade, MD, FAAFP Prevalence of Dementia Age range 65-74 5% % affected 75-84 15-25% 85 and older 36-50% 5.4 Million American have AD Dementia
Dementia and Fall Geriatric Interprofessional Training Wael Hamade, MD, FAAFP Prevalence of Dementia Age range 65-74 5% % affected 75-84 15-25% 85 and older 36-50% 5.4 Million American have AD Dementia
Dementia Facts and Resources Dementia Warning Signs Getting a Diagnosis Dementia Communication Tips Dementia Risk Reduction.
 Dementia Facts and Resources Dementia Warning Signs Getting a Diagnosis Dementia Communication Tips Dementia Risk Reduction Intermission Dementia Stages and Behaviors Caregiving and Self-Care Overview
Dementia Facts and Resources Dementia Warning Signs Getting a Diagnosis Dementia Communication Tips Dementia Risk Reduction Intermission Dementia Stages and Behaviors Caregiving and Self-Care Overview
Dementia: Diagnosis and Treatment
 Dementia: Diagnosis and Treatment Outline 1. Risk factors and definition of dementia 2. Types of Dementias 3. MMSE and testing 4. Treatment options Cognitive decline with aging Mild changes in memory and
Dementia: Diagnosis and Treatment Outline 1. Risk factors and definition of dementia 2. Types of Dementias 3. MMSE and testing 4. Treatment options Cognitive decline with aging Mild changes in memory and
What is dementia? What is dementia?
 What is dementia? What is dementia? What is dementia? Dementia is an umbrella term for a range of progressive conditions that affect the brain. It has been identified that there are over 200 subtypes of
What is dementia? What is dementia? What is dementia? Dementia is an umbrella term for a range of progressive conditions that affect the brain. It has been identified that there are over 200 subtypes of
Clinical Differences Among Four Common Dementia Syndromes. a program of Morningside Ministries
 Clinical Differences Among Four Common Dementia Syndromes a program of Morningside Ministries Introduction Four clinical dementia syndromes account for 90% of all cases after excluding reversible causes
Clinical Differences Among Four Common Dementia Syndromes a program of Morningside Ministries Introduction Four clinical dementia syndromes account for 90% of all cases after excluding reversible causes
EARLY DEMENTIA. University of Hawaii Geriatric Medicine Department
 EARLY DEMENTIA University of Hawaii Geriatric Medicine Department INTRODUCTION Dementia is very prevalent Screening and early diagnosis is important Evaluation Dementia Management DEMENTIA IS VERY PREVALENT
EARLY DEMENTIA University of Hawaii Geriatric Medicine Department INTRODUCTION Dementia is very prevalent Screening and early diagnosis is important Evaluation Dementia Management DEMENTIA IS VERY PREVALENT
A Fresh View of Cognitive Disorders in Older Adults: New Classification and Screening Strategies
 A Fresh View of Cognitive Disorders in Older Adults: New Classification and Screening Strategies Lynda Mackin, PhD, AGPCNP-BC, CNS University of California San Francisco School of Nursing 1 Alzheimer s
A Fresh View of Cognitive Disorders in Older Adults: New Classification and Screening Strategies Lynda Mackin, PhD, AGPCNP-BC, CNS University of California San Francisco School of Nursing 1 Alzheimer s
Medications for Alzheimer s disease: are they right for you?
 Medications for Alzheimer s disease: are they right for you? There are no medications today that can cure Alzheimer s disease. But there are currently four medications approved by Health Canada which can
Medications for Alzheimer s disease: are they right for you? There are no medications today that can cure Alzheimer s disease. But there are currently four medications approved by Health Canada which can
If you have dementia, you may have some or all of the following symptoms.
 About Dementia Dementia may be caused by a number of illnesses that affect the brain. Dementia typically leads to memory loss, inability to do everyday things, difficulty in communication, confusion, frustration,
About Dementia Dementia may be caused by a number of illnesses that affect the brain. Dementia typically leads to memory loss, inability to do everyday things, difficulty in communication, confusion, frustration,
Understanding Alzheimer s Disease
 Understanding Alzheimer s Disease Alzheimer s disease is an irreversible, progressive brain disorder that slowly impacts memory, thinking, skills and, eventually, the ability to carry out the simplest
Understanding Alzheimer s Disease Alzheimer s disease is an irreversible, progressive brain disorder that slowly impacts memory, thinking, skills and, eventually, the ability to carry out the simplest
Common Forms of Dementia Handout Package
 Common Forms of Dementia Handout Package Common Forms of Dementia 1 Learning Objectives As a result of working through this module, you should be better able to: 1. Describe clinical features of 4 major
Common Forms of Dementia Handout Package Common Forms of Dementia 1 Learning Objectives As a result of working through this module, you should be better able to: 1. Describe clinical features of 4 major
DISCLAIMER: ECHO Nevada emphasizes patient privacy and asks participants to not share ANY Protected Health Information during ECHO clinics.
 DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
Dementia the A,B,Cs. Dr. Frank Molnar. Associate Professor of Medicine, University of Ottawa Division of Geriatric Medicine, the Ottawa Hospital
 Dementia the A,B,Cs Dr. Frank Molnar Associate Professor of Medicine, University of Ottawa Division of Geriatric Medicine, the Ottawa Hospital Implications for Practice Dementia the A,B,Cs (Dr. Frank Molnar)
Dementia the A,B,Cs Dr. Frank Molnar Associate Professor of Medicine, University of Ottawa Division of Geriatric Medicine, the Ottawa Hospital Implications for Practice Dementia the A,B,Cs (Dr. Frank Molnar)
Dementia: How to explain the diagnosis to patients and relatives
 GPHot Topics (April 2017): Dementia: How to explain the diagnosis to patients and relatives mohammad somauroo Consultant Physician with specialist interest in Community Geriatrics Royal Liverpool and Broadgreen
GPHot Topics (April 2017): Dementia: How to explain the diagnosis to patients and relatives mohammad somauroo Consultant Physician with specialist interest in Community Geriatrics Royal Liverpool and Broadgreen
BEHAVIORAL PROBLEMS IN DEMENTIA
 BEHAVIORAL PROBLEMS IN DEMENTIA CLINICAL FEATURES Particularly as dementia progresses, psychiatric symptoms may develop that resemble discrete mental disorders such as depression or mania The course and
BEHAVIORAL PROBLEMS IN DEMENTIA CLINICAL FEATURES Particularly as dementia progresses, psychiatric symptoms may develop that resemble discrete mental disorders such as depression or mania The course and
The Psychopharmacology of Alzheimer s Disease. Bruce Kaster, MD Instructor in Psychiatry Harvard Medical school
 The Psychopharmacology of Alzheimer s Disease Bruce Kaster, MD Instructor in Psychiatry Harvard Medical school Overview of Alzheimer s Disease Alzheimer s is a progressive degenerative disease Prevalence
The Psychopharmacology of Alzheimer s Disease Bruce Kaster, MD Instructor in Psychiatry Harvard Medical school Overview of Alzheimer s Disease Alzheimer s is a progressive degenerative disease Prevalence
Alzheimer s disease dementia: a neuropsychological approach
 Alzheimer s disease dementia: a neuropsychological approach Dr. Roberta Biundo, PhD Neuropsychology Coordinator at Parkinson s disease and movement disorders unit of San Camillo rehabilitation hospital
Alzheimer s disease dementia: a neuropsychological approach Dr. Roberta Biundo, PhD Neuropsychology Coordinator at Parkinson s disease and movement disorders unit of San Camillo rehabilitation hospital
SECTION 1: as each other, or as me. THE BRAIN AND DEMENTIA. C. Boden *
 I read all the available books by other [people with] Alzheimer s disease but they never had quite the same problems as each other, or as me. I t s not like other diseases, where there is a standard set
I read all the available books by other [people with] Alzheimer s disease but they never had quite the same problems as each other, or as me. I t s not like other diseases, where there is a standard set
Imaging of Alzheimer s Disease: State of the Art
 July 2015 Imaging of Alzheimer s Disease: State of the Art Neir Eshel, Harvard Medical School Year IV Outline Our patient Definition of dementia Alzheimer s disease Epidemiology Diagnosis Stages of progression
July 2015 Imaging of Alzheimer s Disease: State of the Art Neir Eshel, Harvard Medical School Year IV Outline Our patient Definition of dementia Alzheimer s disease Epidemiology Diagnosis Stages of progression
Cognitive enhancers PINCH ME. Anticholinergic burden BPSD. Agitation, Aggression and antipsychotics
 Cognitive enhancers PINCH ME Anticholinergic burden BPSD Agitation, Aggression and antipsychotics 2 types Cholinesterase inhibitors licensed for mild to moderate AD Donepezil Galantamine Rivastigmine also
Cognitive enhancers PINCH ME Anticholinergic burden BPSD Agitation, Aggression and antipsychotics 2 types Cholinesterase inhibitors licensed for mild to moderate AD Donepezil Galantamine Rivastigmine also
Objectives. Prevalence of AD by age. Diagnosing and Managing Dementia in Ambulatory Practice
 Diagnosing and Managing Dementia in Ambulatory Practice 35 th Annual Nurse Practitioners of Oregon Education Conference Elizabeth Eckstrom, MD, MPH Oregon Health & Science University Objectives Review
Diagnosing and Managing Dementia in Ambulatory Practice 35 th Annual Nurse Practitioners of Oregon Education Conference Elizabeth Eckstrom, MD, MPH Oregon Health & Science University Objectives Review
Comments to this discussion are invited on the Alzforum Webinar page. Who Should Use the New Diagnostic Guidelines? The Debate Continues
 Comments to this discussion are invited on the Alzforum Webinar page. Who Should Use the New Diagnostic s? The Debate Continues Ever since new criteria came out for a research diagnosis of prodromal/preclinical
Comments to this discussion are invited on the Alzforum Webinar page. Who Should Use the New Diagnostic s? The Debate Continues Ever since new criteria came out for a research diagnosis of prodromal/preclinical
Delirium & Dementia. Nicholas J. Silvestri, MD
 Delirium & Dementia Nicholas J. Silvestri, MD Outline Delirium vs. Dementia Neural pathways relating to consciousness Encephalopathy Stupor Coma Dementia Delirium vs. Dementia Delirium Abrupt onset Lasts
Delirium & Dementia Nicholas J. Silvestri, MD Outline Delirium vs. Dementia Neural pathways relating to consciousness Encephalopathy Stupor Coma Dementia Delirium vs. Dementia Delirium Abrupt onset Lasts
Alzheimer Disease and Related Dementias
 Alzheimer Disease and Related Dementias Defining Generic Key Terms and Concepts Mild cognitive impairment: (MCI) is a state of progressive memory loss after the age of 50 that is beyond what would be expected
Alzheimer Disease and Related Dementias Defining Generic Key Terms and Concepts Mild cognitive impairment: (MCI) is a state of progressive memory loss after the age of 50 that is beyond what would be expected
Fact Sheet Alzheimer s disease
 What is Alzheimer s disease Fact Sheet Alzheimer s disease Alzheimer s disease, AD, is a progressive brain disorder that gradually destroys a person s memory and ability to learn, reason, make judgements,
What is Alzheimer s disease Fact Sheet Alzheimer s disease Alzheimer s disease, AD, is a progressive brain disorder that gradually destroys a person s memory and ability to learn, reason, make judgements,
DRUG THERAPY CHOICES FOR THE DEMENTED PATIENT Past, Present and Future
 DRUG THERAPY CHOICES FOR THE DEMENTED PATIENT Past, Present and Future Daniel S. Sitar Professor Emeritus University of Manitoba Email: Daniel.Sitar@umanitoba.ca March 6, 2018 INTRODUCTION EPIDEMIOLOGY
DRUG THERAPY CHOICES FOR THE DEMENTED PATIENT Past, Present and Future Daniel S. Sitar Professor Emeritus University of Manitoba Email: Daniel.Sitar@umanitoba.ca March 6, 2018 INTRODUCTION EPIDEMIOLOGY
Alzheimer s disease is an
 Alzheimer s Disease FACT SHEET Alzheimer s disease is an irreversible, progressive brain disease that slowly destroys memory and thinking skills, and eventually even the ability to carry out the simplest
Alzheimer s Disease FACT SHEET Alzheimer s disease is an irreversible, progressive brain disease that slowly destroys memory and thinking skills, and eventually even the ability to carry out the simplest
Sorting Out the Three D s:
 Sorting Out the Three D s: Delirium, Depression & Dementia Teepa Snow, Positive Approach, LLC to be reused only with permission. Dementia Delirium Depression What s What? What s What For Each D Onset Hx
Sorting Out the Three D s: Delirium, Depression & Dementia Teepa Snow, Positive Approach, LLC to be reused only with permission. Dementia Delirium Depression What s What? What s What For Each D Onset Hx
7/3/2013 ABNORMAL PSYCHOLOGY SEVENTH EDITION CHAPTER FOURTEEN CHAPTER OUTLINE. Dementia, Delirium, and Amnestic Disorders. Oltmanns and Emery
 ABNORMAL PSYCHOLOGY SEVENTH EDITION Oltmanns and Emery PowerPoint Presentations Prepared by: Ashlea R. Smith, Ph.D. This multimedia and its contents are protected under copyright law. The following are
ABNORMAL PSYCHOLOGY SEVENTH EDITION Oltmanns and Emery PowerPoint Presentations Prepared by: Ashlea R. Smith, Ph.D. This multimedia and its contents are protected under copyright law. The following are
Diagnosis and management of non-alzheimer dementias. Melissa Yu, M.D. Department of Neurology
 Diagnosis and management of non-alzheimer dementias Melissa Yu, M.D. Department of Neurology AGENDA Introduction When to think of alternate diagnoses Other forms of dementia Other reasons for confusion
Diagnosis and management of non-alzheimer dementias Melissa Yu, M.D. Department of Neurology AGENDA Introduction When to think of alternate diagnoses Other forms of dementia Other reasons for confusion
Cal MediConnect Dementia Awareness CMC Annual Training
 Cal MediConnect 2017 Dementia Awareness 2017 CMC Annual Training Definition Overview of Dementia Training Diagnosis of Dementia Signs and Symptoms Risk Factors Stages of Dementia Types of Dementia: Reversible/Irreversible
Cal MediConnect 2017 Dementia Awareness 2017 CMC Annual Training Definition Overview of Dementia Training Diagnosis of Dementia Signs and Symptoms Risk Factors Stages of Dementia Types of Dementia: Reversible/Irreversible
What APS Workers Need to Know about Frontotemporal, Lewy Body and Vascular Dementias
 What APS Workers Need to Know about Frontotemporal, Lewy Body and Vascular Dementias Presenter: Kim Bailey, MS Gerontology, Program & Education Specialist, Alzheimer s Orange County 1 1 Facts About Our
What APS Workers Need to Know about Frontotemporal, Lewy Body and Vascular Dementias Presenter: Kim Bailey, MS Gerontology, Program & Education Specialist, Alzheimer s Orange County 1 1 Facts About Our
3/6/2019 DIAGNOSIS OF DEMENTIA IN THE OUTPATIENT SETTING FINANCIAL DISCLOSURES LEARNING OBJECTIVES
 DIAGNOSIS OF DEMENTIA IN THE OUTPATIENT SETTING MILTA LITTLE, DO, CMD DUKE UNIVERSITY SCHOOL OF MEDICINE FINANCIAL DISCLOSURES Dr. Little has no relevant financial disclosures to report Dr. Little will
DIAGNOSIS OF DEMENTIA IN THE OUTPATIENT SETTING MILTA LITTLE, DO, CMD DUKE UNIVERSITY SCHOOL OF MEDICINE FINANCIAL DISCLOSURES Dr. Little has no relevant financial disclosures to report Dr. Little will
Understanding dementia
 Dementia handbook for carers Essex Understanding dementia About this handbook 1 What is dementia 3 Summary of dementia symptoms 6 Medication and treatment 7 About this handbook This handbook aims to summarise
Dementia handbook for carers Essex Understanding dementia About this handbook 1 What is dementia 3 Summary of dementia symptoms 6 Medication and treatment 7 About this handbook This handbook aims to summarise
Alzheimer s Disease. Fact Sheet. Fact Sheet. Fact Sheet. What Causes AD?
 2 Alzheimer s Disease Dementia is a brain disorder that seriously affects a person s ability to carry out daily activities. The most common form of dementia among older people is Alzheimer s disease (AD),
2 Alzheimer s Disease Dementia is a brain disorder that seriously affects a person s ability to carry out daily activities. The most common form of dementia among older people is Alzheimer s disease (AD),
Getting Help for Patients with Dementia and their Caregivers. Erica Salamida Associate Director of Programs and Services Alzheimer s Association-NENY
 Getting Help for Patients with Dementia and their Caregivers Erica Salamida Associate Director of Programs and Services Alzheimer s Association-NENY In this session you will learn about: Symptoms of dementia,
Getting Help for Patients with Dementia and their Caregivers Erica Salamida Associate Director of Programs and Services Alzheimer s Association-NENY In this session you will learn about: Symptoms of dementia,
As a general cognitive screening tool or as part of an annual exam (Medicare Annual Wellness Visit).
.") EMR DECISION SUPPORT TOOLS FOR ALZHEIMER S AND RELATED DEMENTIAS 1. Screening Tool Criteria For When to Use: As a general cognitive screening tool or as part of an annual exam (Medicare Annual Wellness
EMR DECISION SUPPORT TOOLS FOR ALZHEIMER S AND RELATED DEMENTIAS 1. Screening Tool Criteria For When to Use: As a general cognitive screening tool or as part of an annual exam (Medicare Annual Wellness
10/17/2017. Causes of Dementia Alzheimer's Disease Vascular Dementia Diffuse Lewy Body Disease Alcoholic Dementia Fronto-Temporal Dementia Others
 1 Dementia Dementia comes from the Latin word demens, meaning out of mind. It is the permanent loss of multiple intellectual functions. It is progressive deterioration of mental powers accompanied by changes
1 Dementia Dementia comes from the Latin word demens, meaning out of mind. It is the permanent loss of multiple intellectual functions. It is progressive deterioration of mental powers accompanied by changes
P20.2. Characteristics of different types of dementia and challenges for the clinician
 P20.2. Characteristics of different types of dementia and challenges for the clinician, professor Danish Dementia Research Center Rigshospitalet, University of Copenhagen (Denmark) This project has received
P20.2. Characteristics of different types of dementia and challenges for the clinician, professor Danish Dementia Research Center Rigshospitalet, University of Copenhagen (Denmark) This project has received
FRONTOTEMPORAL DEGENERATION: OVERVIEW, TRENDS AND DEVELOPMENTS
 FRONTOTEMPORAL DEGENERATION: OVERVIEW, TRENDS AND DEVELOPMENTS Norman L. Foster, M.D. Director, Center for Alzheimer s Care, Imaging and Research Chief, Division of Cognitive Neurology, Department of Neurology
FRONTOTEMPORAL DEGENERATION: OVERVIEW, TRENDS AND DEVELOPMENTS Norman L. Foster, M.D. Director, Center for Alzheimer s Care, Imaging and Research Chief, Division of Cognitive Neurology, Department of Neurology
Non Alzheimer Dementias
 Non Alzheimer Dementias Randolph B Schiffer Department of Neuropsychiatry and Behavioral Science Texas Tech University Health Sciences Center 9/11/2007 Statement of Financial Disclosure Randolph B Schiffer,,
Non Alzheimer Dementias Randolph B Schiffer Department of Neuropsychiatry and Behavioral Science Texas Tech University Health Sciences Center 9/11/2007 Statement of Financial Disclosure Randolph B Schiffer,,
Alzheimer Disease and Related Dementias. Alzheimer Society of Manitoba Dr. David Strang
 Alzheimer Disease and Related Dementias Alzheimer Society of Manitoba Dr. David Strang What is Dementia? Dementia is a syndrome symptoms include loss of memory, judgment and reasoning, and changes in mood
Alzheimer Disease and Related Dementias Alzheimer Society of Manitoba Dr. David Strang What is Dementia? Dementia is a syndrome symptoms include loss of memory, judgment and reasoning, and changes in mood
DEMENTIA Dementia is NOT a normal part of aging Symptoms of dementia can be caused by different diseases Some symptoms of dementia may include:
 DEMENTIA Dementia is NOT a normal part of aging Symptoms of dementia can be caused by different diseases Some symptoms of dementia may include: 1. Memory loss The individual may repeat questions or statements,
DEMENTIA Dementia is NOT a normal part of aging Symptoms of dementia can be caused by different diseases Some symptoms of dementia may include: 1. Memory loss The individual may repeat questions or statements,
Alzheimer's Disease. Dementia
 Alzheimer's Disease Victor W. Henderson, MD, MS Departments of Health Research & Policy (Epidemiology) and of Neurology & Neurological Sciences Stanford University Director, Stanford Alzheimer s Disease
Alzheimer's Disease Victor W. Henderson, MD, MS Departments of Health Research & Policy (Epidemiology) and of Neurology & Neurological Sciences Stanford University Director, Stanford Alzheimer s Disease
Recognizing Signs and Symptoms of Alzheimer's Disease in Earlier Stages Can Lead to Diagnosis
 A joint publication of the Illinois Health Care Association and CE Solutions November 2015 Recognizing Signs and Symptoms of Alzheimer's Disease in Earlier Stages Can Lead to Diagnosis Early diagnosis
A joint publication of the Illinois Health Care Association and CE Solutions November 2015 Recognizing Signs and Symptoms of Alzheimer's Disease in Earlier Stages Can Lead to Diagnosis Early diagnosis
Dementia Update. October 1, 2013 Dylan Wint, M.D. Cleveland Clinic Lou Ruvo Center for Brain Health Las Vegas, Nevada
 Dementia Update October 1, 2013 Dylan Wint, M.D. Cleveland Clinic Lou Ruvo Center for Brain Health Las Vegas, Nevada Outline New concepts in Alzheimer disease Biomarkers and in vivo diagnosis Future trends
Dementia Update October 1, 2013 Dylan Wint, M.D. Cleveland Clinic Lou Ruvo Center for Brain Health Las Vegas, Nevada Outline New concepts in Alzheimer disease Biomarkers and in vivo diagnosis Future trends
UNDERSTANDING ALZHEIMER S AND DEMENTIA
 UNDERSTANDING ALZHEIMER S AND DEMENTIA Geri T., living with Alzheimer's, and her husband and care partner, Jim T. THE IMPACT OF ALZHEIMER S AND DEMENTIA Currently, an estimated 50 million people worldwide
UNDERSTANDING ALZHEIMER S AND DEMENTIA Geri T., living with Alzheimer's, and her husband and care partner, Jim T. THE IMPACT OF ALZHEIMER S AND DEMENTIA Currently, an estimated 50 million people worldwide
Objectives. My Patient: The story 10/6/2017
 Objectives Our Grey Matter Matters: A Case in Point Vivien Brown MDCM, CCFP,FCFP, NCMP Assistant Professor, University of Toronto Vice President, Medical Affairs, Medisys Healthy Group Past President,
Objectives Our Grey Matter Matters: A Case in Point Vivien Brown MDCM, CCFP,FCFP, NCMP Assistant Professor, University of Toronto Vice President, Medical Affairs, Medisys Healthy Group Past President,
Understanding Dementia
 Understanding Dementia Dr. Dallas Seitz MD FRCPC Assistant Professor, Department of Psychiatry, Queen s University, Kingston, Ontario, Canada What s Next Information about Dementia, Elder Care and Supports
Understanding Dementia Dr. Dallas Seitz MD FRCPC Assistant Professor, Department of Psychiatry, Queen s University, Kingston, Ontario, Canada What s Next Information about Dementia, Elder Care and Supports
Recognition and Management of Behavioral Disturbances in Dementia
 Recognition and Management of Behavioral Disturbances in Dementia Danielle Hansen, DO, MS (Med Ed), MHSA INTRODUCTION 80% 90% of patients with dementia develop at least one behavioral disturbances or psychotic
Recognition and Management of Behavioral Disturbances in Dementia Danielle Hansen, DO, MS (Med Ed), MHSA INTRODUCTION 80% 90% of patients with dementia develop at least one behavioral disturbances or psychotic
Medications and Non-Pharma Approaches to Treatment. David J. Irwin, MD Penn Frontotemporal Degeneration Center
 Medications and Non-Pharma Approaches to Treatment David J. Irwin, MD Penn Frontotemporal Degeneration Center Outline Non-Pharmacological Treatment Strategies Behavior Language Motor Supportive Care Check-points
Medications and Non-Pharma Approaches to Treatment David J. Irwin, MD Penn Frontotemporal Degeneration Center Outline Non-Pharmacological Treatment Strategies Behavior Language Motor Supportive Care Check-points
DEMENTIA, THE BRAIN AND HOW IT WORKS AND WHY YOU MATTER
 OVERCOMING THE CHALLENGES OF MANAGING CHRONIC DISEASES IN PERSONS WITH DEMENTIA DEMENTIA, THE BRAIN AND HOW IT WORKS AND WHY YOU MATTER LEARNING OBJECTIVES Be familiar with the diagnostic criteria for
OVERCOMING THE CHALLENGES OF MANAGING CHRONIC DISEASES IN PERSONS WITH DEMENTIA DEMENTIA, THE BRAIN AND HOW IT WORKS AND WHY YOU MATTER LEARNING OBJECTIVES Be familiar with the diagnostic criteria for
Dementia Update. Daniel Drubach, M.D. Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota
 Dementia Update Daniel Drubach, M.D. Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota Nothing to disclose Dementia Progressive deterioration in mental function
Dementia Update Daniel Drubach, M.D. Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota Nothing to disclose Dementia Progressive deterioration in mental function
What is dementia? What is dementia?
 What is dementia? What is dementia? What is dementia? Dementia is an umbrella term for a range of progressive conditions that affect the brain. There are over 200 subtypes of dementia, but the five most
What is dementia? What is dementia? What is dementia? Dementia is an umbrella term for a range of progressive conditions that affect the brain. There are over 200 subtypes of dementia, but the five most
Behavioral Interventions
 Behavioral Interventions Linda K. Shumaker, R.N.-BC, MA Pennsylvania Behavioral Health and Aging Coalition Behavioral Management is the key in taking care of anyone with a Dementia! Mental Health Issues
Behavioral Interventions Linda K. Shumaker, R.N.-BC, MA Pennsylvania Behavioral Health and Aging Coalition Behavioral Management is the key in taking care of anyone with a Dementia! Mental Health Issues
Introduction to Dementia: Diagnosis & Evaluation. Created in March 2005 Duration: about 15 minutes
 Introduction to Dementia: Diagnosis & Evaluation Created in March 2005 Duration: about 15 minutes Axel Juan, MD The Geriatrics Institute axel.juan@med.va.gov 305-575-3388 Credits Principal medical contributor:
Introduction to Dementia: Diagnosis & Evaluation Created in March 2005 Duration: about 15 minutes Axel Juan, MD The Geriatrics Institute axel.juan@med.va.gov 305-575-3388 Credits Principal medical contributor:
Resources: Types of dementia
 1/5 Dementia is an umbrella term for a number of progressive conditions affecting the functioning of the brain. Different types of dementia have different causes. There are a great number of rare forms.
1/5 Dementia is an umbrella term for a number of progressive conditions affecting the functioning of the brain. Different types of dementia have different causes. There are a great number of rare forms.
Dr. Michael Lobatz Dr. Michael Jackson Dr. James Brewer Dr. Paul Aisen. Dr. Michael Plopper. Dr. Guerry Peavy
 1 Anne State 2 3 Dr. Michael Lobatz Dr. Michael Jackson Dr. James Brewer Dr. Paul Aisen Dr. Michael Plopper Dr. Guerry Peavy 4 Michael Lobatz, MD Medical Director, Neurosciences Medical Director, Rehabilitation
1 Anne State 2 3 Dr. Michael Lobatz Dr. Michael Jackson Dr. James Brewer Dr. Paul Aisen Dr. Michael Plopper Dr. Guerry Peavy 4 Michael Lobatz, MD Medical Director, Neurosciences Medical Director, Rehabilitation
Cognitive Evaluation in Primary Care. Scott T. Larson, MD Clinical Assistant Professor University of Iowa
 Cognitive Evaluation in Primary Care Scott T. Larson, MD Clinical Assistant Professor University of Iowa scott-larson@uiowa.edu Objectives Understand the subtypes of dementia, and the DSM-5 categorization
Cognitive Evaluation in Primary Care Scott T. Larson, MD Clinical Assistant Professor University of Iowa scott-larson@uiowa.edu Objectives Understand the subtypes of dementia, and the DSM-5 categorization
Mild Cognitive Impairment (MCI)
") October 19, 2018 Mild Cognitive Impairment (MCI) Yonas E. Geda, MD, MSc Professor of Neurology and Psychiatry Consultant, Departments of Psychiatry & Psychology, and Neurology Mayo Clinic College of Medicine
October 19, 2018 Mild Cognitive Impairment (MCI) Yonas E. Geda, MD, MSc Professor of Neurology and Psychiatry Consultant, Departments of Psychiatry & Psychology, and Neurology Mayo Clinic College of Medicine