Parkinsons Disease update. Sindhu R Srivatsal MD MPH Virginia Mason Medical Center
|
|
|
- Daniella Bruce
- 5 years ago
- Views:
Transcription





1 Parkinsons Disease update Sindhu R Srivatsal MD MPH Virginia Mason Medical Center
2 PARKINSONISM Vs PARKINSON S Parkinsonism Bradykinesia: slowness of movements (essential feature) PLUS one of Tremor: resting form (absent 30% of the time) Rigidity Postural instability
3 WHAT IS PARKINSON S DISEASE Spontaneous Parkinsonism without any other etiology (drug/ toxin) With no evidence of red flags Early gait impairment, dementia, autonomic issues With robust medication responsiveness
4 Contd.. Causes for parkinsonism Parkinson s disease (commonest) Parkinson plus (Multiple systems atrophy, dementia with lewy body, Progressive supranuclear palsy) Vascular parkinsonism Drug/ Toxin induced parkinsonism Alzheimer's with parkinsonian features

5 MOTOR FEATURES Bradykinesia Arm swing, dexterity, hypomimia, stooped posture Rigidity Pain, stiffness, shoulder ROMS Tremor Pill rolling rest tremor

6 PARKINSON COMPLEX- Tip of the iceberg anology
7 PREVALENCE: > 1 MILLION people currently diagnosed with PD in USA 1 in 100 Americans over the age of 60 ETIOLOGY: A combination of genetic susceptibility and exposure to environmental toxins and this may vary from person to person Monogenic forms: Autosomal dominant: SNCA, LRRK2 Autosomal recessive: PARKIN, PINK1, DJ-1, rarer < 10% of parkinsons is familial,




8 ENVIRONMENTAL FACTORS Risks: Rural residence X 1.56 Well water X 1.26 Living on a farm X 1.42 Pesticide (rotenone, paraquat) X 1.94 Protective: Smoking X 0.59 Coffee X 0.69
 Olfactory dysfunction in Parkinson disease Nat. Rev.")
9 BRAAK HYPOTHESIS Doty, R. L. (2012) Olfactory dysfunction in Parkinson disease Nat. Rev. Neurol. doi: /nrneurol

10 DIAGNOSIS Essentially a clinical diagnosis, levodopa responsiveness used as a diagnostic tool. Imaging such as MRI BRAIN used to eliminate mimics DAT SPECT used at times to distinguish between essential tremor and Parkinson s/ parkinsonian syndromes

11 STAGES OF PARKINSON S

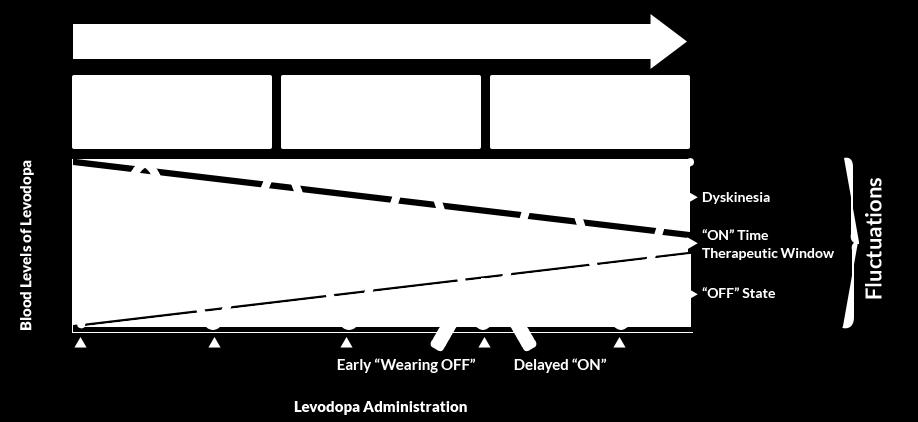
12 CHANGES IN DOPAMINE RESPONSE IN PARKINSON S

13 Rx Motor: Tremor Rigidity bradykinesia Dyskinesias Non Motor Mood disorders, cognitive dysfunction, Sleep disorders, GI issues, GU issues, Autonomic issues

14 MOTOR MAOB-Is Selegiline, rasagiline Safinamide Dopamine agonists Pramipexole, ropinirole, Rotigotine, Apomorphine E F F I C A C Y COMT inhibitors: Entacapone, tolcapone Anticholinergics:Trihexypheni dyl, Amantadine/ ER Carbidopa/levodopa ER/ IR Rytary
15 HOW DO MEDS WORK.. accessed sept 2014
16 CARBIDOPA/LEVODOPA Most Potent PD medication, often used for diagnostic and therapeutic trial Levodopa: 3,4-dihydroxy l-phenylalanine Levodopa- prodrug, converts to Dopamine in brain Carbidopa: blocks peripheral conversion

17 Formulations Sinemet IR (immediate release): 25/100, 25/250 Elimination half life 1.5 hrs Sinemet CR (controlled release): 25/100, 50/

18 RYTARY- Combined immediate and extended release levodopa Elimination half life 5 to 6 hrs, doses tid to qid Microbeads dissolve at different times Less dyskinesias and less wearing off
19 INTERACTIONS & SIDE EFFECTS Dietary protein intake Amino acid transporter competition Protein redistribution vs low protein Side effects: nausea, vomiting, Dizziness/ lightheadedness Drowsiness (peak dose) Rarely hallucinations/ confusion
 Ropinirole: Requip 0.25/0.5/1mg (max dose 20-24 mg) Rotigotine patch : Neupro 2-8 mg/24 hr")
20 DOPAMINE AGONISTS Less potent, less likely to cause motor fluctuations More even response, longer acting, once day possible Pramipexole: Mirapex 0.125/0.25/0.5 mg (max dose 4.5mg) Ropinirole: Requip 0.25/0.5/1mg (max dose mg) Rotigotine patch : Neupro 2-8 mg/24 hr
, but needs to be injected, Subcutaneous infusion being tested")
21 APOMORPHINE (dopamine agonist) Subcutaneous injectable form, for sudden and unpredictable off periods Can cause severe nausea, used with tigan Orthostatic hypotension is a serious side effect Very fast acting (10 min onset), but needs to be injected, Subcutaneous infusion being tested
22 SIDE EFFECTS Nausea, vomiting (worse with Apomorphine) Drowsiness and sleep attacks Impulse control problems: compulsive gambling, shopping (preferential Mesolimbic involvement) Confusion, hallucinations Ankle swelling
23 ANTICHOLINERGICS Trihexyphenidyl (Artane -1-2 mg bid/ tid) or Benztropine (Cogentin 1-2 mg bid/ tid) Can help tremor more than other symptoms Useful as additive therapy Fallen out of favor due to cognitive side effects. Other side effects include dry mouth/ eyes, urinary retention, may worsen gait

24 MAOB-I and COMT Reduce turnover of levodopa and dopamine
25 MAOB-I Monoamine Oxidase B inhibitor Selegiline (Deprenyl 5mg), Rasagiline (Azilect 1mg) Block Monoamine oxidase enzyme, reduces breakdown of dopamine and prolongs effect of levodopa Mild symptomatic effect, useful in reducing need for levodopa, dyskinesias and freezing of gait SE: similar to levodopa except selegiline breakdown produces amphetamine byproducts causing insomnia? Disease modifiers.
26 Unique mechanism MAO B inhibitor SAFINAMIDE new drug NMDA receptor antagonist Approved March 2017 as adjunct for on time without dyskinesia (Xadago)
27 Catechol-O-methyl transferase INHIBITORS Inhibit enzyme COMT enzyme Block peripheral and central (tolcapone) breakdown of levodopa,» Entacapone (comtan 200mg), and in combination with sinemet (Stalevo 50/75/100/125/150/200)» Tolcapone (Tasmar): rarely used due to liver toxicity» Opicapone approved in European union (2016), once a day dose
, once a day")
28 AMANTADINE Blocks NMDA receptor, effects are mild on parkinson symptoms» Reducing dyskinesias, can improve gait» Side effects: ankle swelling, hallucinations, confusion, livedo reticularis» TID dosing, comes as 100 mg dose» Extended release amantadine approved 2017» (Gocovri), once a day dose

29 Early to advanced parkinsons treatment spectrum
30 DEEP BRAIN STIMULATION FDA approved in 2002 Considered in the following situations: motor fluctuations not fully controlled on maximum medical therapy Disabling tremor not controlled by medications Rarely: intolerance of medications Data for early DBS before motor fluctuations is rising

31 BASAL GANGLIA STRUCTURE

32 DBS TARGET Subthalamic nucleus or Globus pallidus interna 94/brain%20implant.PNG



33 TARGETING Mapping, Micro electrode recording, Macro stimulation
34 OUTCOMES Deuschl 2006
35 RISKS AND BENEFITS BENEFITS: Increase on time and improve off state mobility, better than best medical therapy Reduce levodopa dose requirements and dyskinesias RISKS: Infection, bleeding Lead fracture

36 LEVODOPA INTESTINAL GEL Continuous levodopa infusion during waking hours with basal and bolus infusions Mimics natural dopamine release Circumvents gut absorption issues
37 SIDE EFFECTS/ ADVERSE EFFECTS Procedural issues Kinking of tube Invasive, needs G-J tube Abdominal pain and distension Generalized polyneuropathy Other side effects similar to levodopa

38 NON MOTOR SYMPTOMS IN PD
39 DEPRESSION Very common in PD, may precede onset Prevalence of Depression in PD: 20-40% Major depression: 5-10% Rx: Evidence for Amitriptilline (side effects limit use), SSRIs comparable, watch for seratonin syndrome Pramipexole can help sometimes
40 HALLUCINATIONS/ PSYCHOSIS Often a side effect of medications (Dopamine Agonists/ Amantadine > levodopa) Independent risk factor for Nursing home placement Cognitive impairment Visual hallucinations: a predictor for cortical Lewy bodies
41 Rx Consider discontinuing Dopamine Agonist (DA), amantadine Rule out infection Consider lowering total levodopa dose Discontinue other offending drugs including anticholinergics, opiates etc
42 PIMAVANSERIN (new drug) FDA approved specifically for treating pyschosis in PD and DLB (Nuplazid) MOA: Selective 5HT2A blocker, taken once a day Unlike antipsychotics doesn t make PD worse Dose 34 mg taken as two 17 mg tabs together Side effects: nausea, dizziness, constipation, confusion, prolongs QT
43 DEMENTIA Presents after years of PD, but can have Mild cognitive impairment early on Attentional and executive function problems Implicit and explicit memory problems Visuo-spatial dysfunction Fluency and confrontational naming issues Trails B: good paper and pencil test to estimate driving ability
44 PREVALENCE Average is 30-40%, Dementia at onset or within a year of parkinsons = DLB Percentage affected grows over time: 16-21% in 5 years 37% in 10 years 50-80% in 20 years
45 Rx Cholinesterase inhibitors mainstay Rivastigmine only FDA approved medication for treatment of dementia associated with PD. (1.5 to 6 mg bid) Donepezil (5-10 mg qday) and galantamine also used in clinical practice (off-label) Potential for worsening tremors Memantine as an adjunctive option (off-label)
46 SIALORRHEA- DROOLING Due to decreased automatic swallowing resulting in pooling of saliva Flexed posture of neck impairs swallow Rx: Sucking hard candy and chewing Atropine eye drops 1% 4 drops under the tongue every 4 hours (off-label) Ipratropium spray may bypass systemic effects (1-2 sprays up to 4 times a day) (off-label) Botulinum toxin injections to salivary glands (off-label)
47 CONSTIPATION Colon transit time is prolonged in PD Slowing occurs in 80% of PD patients Average CTT in PD is twice as long: 44 hours vs. 20 hours (Edwards et al.) Rx Increase fluid and fiber intake (20-35 grams of fiber/day), prunes Add stool softener, Consider lactulose/miralax, and enemas Lubiprostone effective in a small study (activates Chloride channel),
48 BLADDER ISSUES Urinary frequency, urgency and nocturia Anticholinergics: Oxybutynin ( can cross BBB and cause confusion) Tolterodine, solifenacin and darifenacin preferable Reduce caffeine/ bladder irritants (citrus agents, chocolate) Mirabegron (Myrbetriq) has effects on beta adrenergic system and hence no cognitive side effects Urinary Hesitancy: Less common, rule out other conditions e.g., prostate enlargement May need bethanechol
49 REM BEHAVIOR DISORDER May affect up to 50% of persons with PD, sign of synucleinopathy Talking and shouting while asleep, Intense, and sometimes violent, movements Involves "acting out" dreams, REM Atonia is lost May precede typical motor features of PD by decades
50 Rx Treat when it affects patient s/ partner s sleep, Eliminate potentially offending medications Antidepressants, Cholinesterase inhibitors, Beta blockers, Tramadol, Caffeine Melatonin, Well-tolerated and available OTC (3-9 mg) Clonazepam (0.25 mg) Favorable response in up to 90% of patients Others (e.g., gabapentin, clozapine)
51 VIT D in Parkinsons Disease Cross sectional studies: Vit D levels correlate with mood, UPDRS scores, HY stage, verbal fluency (causation vs reverse causation) Higher Vit D levels associated with milder PD (HY and UPDRS) I small randomized trial in PD patients showed Vit D 1200 units for 12 mo reduced progression of HY scale slightly
, similar results in women not on HRT? can help motor symptoms")
52 CAFFEINE IN PD Shown to reduce LID (levodopa induced dyskinesias Risk for PD less in men drinking coffee (2cups/dy), similar results in women not on HRT? can help motor symptoms
53 QUESTIONS? THANK YOU!!
Scott J Sherman MD, PhD The University of Arizona PARKINSON DISEASE
 Scott J Sherman MD, PhD The University of Arizona PARKINSON DISEASE LEARNING OBJECTIVES The Course Participant will: 1. Be familiar with the pathogenesis of Parkinson s Disease (PD) 2. Understand clinical
Scott J Sherman MD, PhD The University of Arizona PARKINSON DISEASE LEARNING OBJECTIVES The Course Participant will: 1. Be familiar with the pathogenesis of Parkinson s Disease (PD) 2. Understand clinical
Best Medical Treatments for Parkinson s disease
 Best Medical Treatments for Parkinson s disease Bernadette Schöneburg, M.D. June 20 th, 2015 What is Parkinson s Disease (PD)? Progressive neurologic disorder that results from the loss of specific cells
Best Medical Treatments for Parkinson s disease Bernadette Schöneburg, M.D. June 20 th, 2015 What is Parkinson s Disease (PD)? Progressive neurologic disorder that results from the loss of specific cells
10th Medicine Review Course st July Prakash Kumar
 10th Medicine Review Course 2018 21 st July 2018 Drug Therapy for Parkinson's disease Prakash Kumar National Neuroscience Institute Singapore General Hospital Sengkang General Hospital Singhealth Duke-NUS
10th Medicine Review Course 2018 21 st July 2018 Drug Therapy for Parkinson's disease Prakash Kumar National Neuroscience Institute Singapore General Hospital Sengkang General Hospital Singhealth Duke-NUS
Parkinson s Disease WHERE HAVE WE BEEN, WHERE ARE WE HEADING? CHARLECE HUGHES D.O.
 Parkinson s Disease WHERE HAVE WE BEEN, WHERE ARE WE HEADING? CHARLECE HUGHES D.O. Parkinson s Epidemiology AFFECTS 1% OF POPULATION OVER 65 MEAN AGE OF ONSET 65 MEN:WOMEN 1.5:1 IDIOPATHIC:HEREDITARY 90:10
Parkinson s Disease WHERE HAVE WE BEEN, WHERE ARE WE HEADING? CHARLECE HUGHES D.O. Parkinson s Epidemiology AFFECTS 1% OF POPULATION OVER 65 MEAN AGE OF ONSET 65 MEN:WOMEN 1.5:1 IDIOPATHIC:HEREDITARY 90:10
PD: Key Treatment Considerations
 PD: Key Treatment Considerations 2018 Management of Neurologic and Neurosurgical Disorders in Daily Practice Elise Anderson MD Medical Co-Director, PBSI Movement Disorders 11/27/2018 1 Outline Treatment
PD: Key Treatment Considerations 2018 Management of Neurologic and Neurosurgical Disorders in Daily Practice Elise Anderson MD Medical Co-Director, PBSI Movement Disorders 11/27/2018 1 Outline Treatment
Optimizing Clinical Communication in Parkinson s Disease:
 Optimizing Clinical Communication in Parkinson s Disease:,Strategies for improving communication between you and your neurologist PFNCA Symposium March 25, 2017 Pritha Ghosh, MD Assistant Professor of
Optimizing Clinical Communication in Parkinson s Disease:,Strategies for improving communication between you and your neurologist PFNCA Symposium March 25, 2017 Pritha Ghosh, MD Assistant Professor of
Pharmacologic Treatment of Parkinson s Disease. Nicholas J. Silvestri, M.D. Assistant Professor of Neurology
 + Pharmacologic Treatment of Parkinson s Disease Nicholas J. Silvestri, M.D. Assistant Professor of Neurology + Overview n Brief review of Parkinson s disease (PD) n Clinical manifestations n Pathophysiology
+ Pharmacologic Treatment of Parkinson s Disease Nicholas J. Silvestri, M.D. Assistant Professor of Neurology + Overview n Brief review of Parkinson s disease (PD) n Clinical manifestations n Pathophysiology
What s new for diagnosing and treating Parkinson s Disease?
 What s new for diagnosing and treating Parkinson s Disease? Erika Driver-Dunckley, MD Associate Professor of Neurology Program Director Movement Disorders Fellowship Assistant Program Director Neurology
What s new for diagnosing and treating Parkinson s Disease? Erika Driver-Dunckley, MD Associate Professor of Neurology Program Director Movement Disorders Fellowship Assistant Program Director Neurology
Motor Fluctuations Stephen Grill, MD, PHD Parkinson s and Movement Disorders Center of Maryland and Johns Hopkins University
 Motor Fluctuations Stephen Grill, MD, PHD Parkinson s and Movement Disorders Center of Maryland and Johns Hopkins University I have no financial interest with any entity producing marketing, re-selling,
Motor Fluctuations Stephen Grill, MD, PHD Parkinson s and Movement Disorders Center of Maryland and Johns Hopkins University I have no financial interest with any entity producing marketing, re-selling,
Parkinson s Disease Update. Presented by Joanna O Leary, MD Movement disorder neurologist Providence St. Vincent s
 Parkinson s Disease Update Presented by Joanna O Leary, MD Movement disorder neurologist Providence St. Vincent s What is a movement disorder? Neurological disorders that affect ability to move by causing
Parkinson s Disease Update Presented by Joanna O Leary, MD Movement disorder neurologist Providence St. Vincent s What is a movement disorder? Neurological disorders that affect ability to move by causing
Communicating About OFF Episodes With Your Doctor
 Communicating About OFF Episodes With Your Doctor Early in Parkinson s disease (PD), treatment with levodopa and other anti-pd drugs provides continuous benefit. As the disease progresses, however, symptom
Communicating About OFF Episodes With Your Doctor Early in Parkinson s disease (PD), treatment with levodopa and other anti-pd drugs provides continuous benefit. As the disease progresses, however, symptom
Pharmacologic Treatment of Parkinson s Disease. Nicholas J. Silvestri, M.D. Associate Professor of Neurology
 + Pharmacologic Treatment of Parkinson s Disease Nicholas J. Silvestri, M.D. Associate Professor of Neurology + Disclosures n NO SIGNIFICANT FINANCIAL, GENERAL, OR OBLIGATION INTERESTS TO REPORT + Learning
+ Pharmacologic Treatment of Parkinson s Disease Nicholas J. Silvestri, M.D. Associate Professor of Neurology + Disclosures n NO SIGNIFICANT FINANCIAL, GENERAL, OR OBLIGATION INTERESTS TO REPORT + Learning
Medications used to treat Parkinson s disease
 Medications used to treat Parkinson s disease Edwin B. George, M.D., Ph.D. Director of Wayne State University Movement Disorder Clinic University Health Center Neurology Clinic University Health The John
Medications used to treat Parkinson s disease Edwin B. George, M.D., Ph.D. Director of Wayne State University Movement Disorder Clinic University Health Center Neurology Clinic University Health The John
parts of the gastrointenstinal tract. At the end of April 2008, it was temporarily withdrawn from the US Market because of problems related to
 parts of the gastrointenstinal tract. At the end of April 2008, it was temporarily withdrawn from the US Market because of problems related to crystallization of the drug, which caused unreliable drug
parts of the gastrointenstinal tract. At the end of April 2008, it was temporarily withdrawn from the US Market because of problems related to crystallization of the drug, which caused unreliable drug
Evaluation and Management of Parkinson s Disease in the Older Patient
 Evaluation and Management of Parkinson s Disease in the Older Patient David A. Hinkle, MD, PhD Comprehensive Movement Disorders Clinic Pittsburgh Institute for Neurodegenerative Diseases University of
Evaluation and Management of Parkinson s Disease in the Older Patient David A. Hinkle, MD, PhD Comprehensive Movement Disorders Clinic Pittsburgh Institute for Neurodegenerative Diseases University of
Treatment of Parkinson s Disease: Present and Future
 Treatment of Parkinson s Disease: Present and Future Karen Blindauer, MD Professor of Neurology Director of Movement Disorders Program Medical College of Wisconsin Neuropathology: Loss of Dopamine- Producing
Treatment of Parkinson s Disease: Present and Future Karen Blindauer, MD Professor of Neurology Director of Movement Disorders Program Medical College of Wisconsin Neuropathology: Loss of Dopamine- Producing
Parkinson s Disease Medications: Professionals Edition
 Parkinson s Disease Clinic and Research Center University of California, San Francisco 505 Parnassus Ave., Rm. 795-M, Box 0114 San Francisco, CA 94143-0114 (415) 476-9276 http://pdcenter.neurology.ucsf.edu
Parkinson s Disease Clinic and Research Center University of California, San Francisco 505 Parnassus Ave., Rm. 795-M, Box 0114 San Francisco, CA 94143-0114 (415) 476-9276 http://pdcenter.neurology.ucsf.edu
Parkinson s Disease Update
 Parkinson s Disease Update Elise Anderson MD Providence Center for Parkinson s Disease October 26, 2017 11/6/2017 1 Disclosures GE Speaker, DaTSCAN 11/6/2017 2 Outline PD diagnosis Motor and nonmotor symptoms
Parkinson s Disease Update Elise Anderson MD Providence Center for Parkinson s Disease October 26, 2017 11/6/2017 1 Disclosures GE Speaker, DaTSCAN 11/6/2017 2 Outline PD diagnosis Motor and nonmotor symptoms
Parkinson s Disease Current Treatment Options
 Parkinson s Disease Current Treatment Options Daniel Kassicieh, D.O., FAAN Sarasota Neurology, P.A. PD: A Chronic Neurodegenerative Ds. 1 Million in USA Epidemiology 50,000 New Cases per Year Majority
Parkinson s Disease Current Treatment Options Daniel Kassicieh, D.O., FAAN Sarasota Neurology, P.A. PD: A Chronic Neurodegenerative Ds. 1 Million in USA Epidemiology 50,000 New Cases per Year Majority
Medication Management & Strategies When the levodopa honeymoon is over
 Medication Management & Strategies When the levodopa honeymoon is over Eric J Pappert, MD Parkinson s Disease & Movement Disorders Center Neurology Associates Medication Options in Parkinson s Carbidopa/Levodopa
Medication Management & Strategies When the levodopa honeymoon is over Eric J Pappert, MD Parkinson s Disease & Movement Disorders Center Neurology Associates Medication Options in Parkinson s Carbidopa/Levodopa
PD ExpertBriefings: Parkinson s Medications: Today and Tomorrow Led By: Cynthia L. Comella, M.D., F.A.A.N.
 PD ExpertBriefings: Parkinson s Medications: Today and Tomorrow Led By: Cynthia L. Comella, M.D., F.A.A.N. To hear the session live on: Tuesday, April 17, 2012 at 1:00 PM ET. DIAL: 1 (888) 272-8710 and
PD ExpertBriefings: Parkinson s Medications: Today and Tomorrow Led By: Cynthia L. Comella, M.D., F.A.A.N. To hear the session live on: Tuesday, April 17, 2012 at 1:00 PM ET. DIAL: 1 (888) 272-8710 and
The symptoms of the Parkinson s disease may vary from person to person. The symptoms might include the following:
 1 PARKINSON S DISEASE Parkinson's disease is a long term disease related to the central nervous system that mainly affects the motor system, resulting in the loss of dopamine, which helps in producing
1 PARKINSON S DISEASE Parkinson's disease is a long term disease related to the central nervous system that mainly affects the motor system, resulting in the loss of dopamine, which helps in producing
PARKINSON S MEDICATION
 PARKINSON S MEDICATION History 1940 50 s Neurosurgeons operated on basal ganglia. Improved symptoms. 12% mortality 1960 s: Researchers identified low levels of dopamine caused Parkinson s leading to development
PARKINSON S MEDICATION History 1940 50 s Neurosurgeons operated on basal ganglia. Improved symptoms. 12% mortality 1960 s: Researchers identified low levels of dopamine caused Parkinson s leading to development
WHAT DEFINES YOPD? HANDLING UNIQUE CONCERNS REBECCA GILBERT, MD, PHD VICE PRESIDENT, CHIEF SCIENTIFIC OFFICER, APDA MARCH 14, 2019
 WHAT DEFINES YOPD? HANDLING UNIQUE CONCERNS REBECCA GILBERT, MD, PHD VICE PRESIDENT, CHIEF SCIENTIFIC OFFICER, APDA MARCH 14, 2019 YOUNG ONSET PARKINSON S DISEASE Definition: Parkinson s disease diagnosed
WHAT DEFINES YOPD? HANDLING UNIQUE CONCERNS REBECCA GILBERT, MD, PHD VICE PRESIDENT, CHIEF SCIENTIFIC OFFICER, APDA MARCH 14, 2019 YOUNG ONSET PARKINSON S DISEASE Definition: Parkinson s disease diagnosed
What is Parkinson s Disease?
 2018 Update in Parkinson s Disease: Treatments and Future Plans Arita McCoy, MSN, CRNP Johns Hopkins Parkinson s Disease and Movement Disorder Center A National Parkinson Foundation Center of Excellence
2018 Update in Parkinson s Disease: Treatments and Future Plans Arita McCoy, MSN, CRNP Johns Hopkins Parkinson s Disease and Movement Disorder Center A National Parkinson Foundation Center of Excellence
Overview. Overview. Parkinson s disease. Secondary Parkinsonism. Parkinsonism: Motor symptoms associated with impairment in basal ganglia circuits
 Overview Overview Parkinsonism: Motor symptoms associated with impairment in basal ganglia circuits The differential diagnosis of Parkinson s disease Primary vs. Secondary Parkinsonism Proteinopathies:
Overview Overview Parkinsonism: Motor symptoms associated with impairment in basal ganglia circuits The differential diagnosis of Parkinson s disease Primary vs. Secondary Parkinsonism Proteinopathies:
PARKINSON S DISEASE. Nigrostriatal Dopaminergic Neurons 5/11/16 CARDINAL FEATURES OF PARKINSON S DISEASE. Parkinson s disease
 5/11/16 PARKINSON S DISEASE Parkinson s disease Prevalence increases with age (starts 40s60s) Seen in all ethnic groups, M:F about 1.5:1 Second most common neurodegenerative disease Genetics role greater
5/11/16 PARKINSON S DISEASE Parkinson s disease Prevalence increases with age (starts 40s60s) Seen in all ethnic groups, M:F about 1.5:1 Second most common neurodegenerative disease Genetics role greater
Parkinson s Disease: initial diagnosis, initial treatment & non-motor features. J. Timothy Greenamyre, MD, PhD
 Parkinson s Disease: initial diagnosis, initial treatment & non-motor features J. Timothy Greenamyre, MD, PhD Involuntary tremulous motion, with lessened muscular power, in parts not in action and even
Parkinson s Disease: initial diagnosis, initial treatment & non-motor features J. Timothy Greenamyre, MD, PhD Involuntary tremulous motion, with lessened muscular power, in parts not in action and even
Objectives. Emerging Treatments in Parkinson s s Disease. Pathology. As Parkinson s progresses it eventually affects large portions of the brain.
 Objectives Emerging Treatments in Parkinson s s Disease 1) Describe recent developments in the therapies for Parkinson s Disease Jeff Kraakevik MD Assistant Professor OHSU/Portland VAMC Parkinson s Center
Objectives Emerging Treatments in Parkinson s s Disease 1) Describe recent developments in the therapies for Parkinson s Disease Jeff Kraakevik MD Assistant Professor OHSU/Portland VAMC Parkinson s Center
Parkinson s Disease Update. Colleen Peach, RN, MSN, FNP Movement Disorders Clinic Emory University School of Medicine March 7, 2015
 Parkinson s Disease Update Colleen Peach, RN, MSN, FNP Movement Disorders Clinic Emory University School of Medicine March 7, 2015 Parkinson s Disease Progressive, chronic, neurodegenerative disease Slow,
Parkinson s Disease Update Colleen Peach, RN, MSN, FNP Movement Disorders Clinic Emory University School of Medicine March 7, 2015 Parkinson s Disease Progressive, chronic, neurodegenerative disease Slow,
Treatment of Parkinson s Disease and of Spasticity. Satpal Singh Pharmacology and Toxicology 3223 JSMBS
 Treatment of Parkinson s Disease and of Spasticity Satpal Singh Pharmacology and Toxicology 3223 JSMBS singhs@buffalo.edu 716-829-2453 1 Disclosures NO SIGNIFICANT FINANCIAL, GENERAL, OR OBLIGATION INTERESTS
Treatment of Parkinson s Disease and of Spasticity Satpal Singh Pharmacology and Toxicology 3223 JSMBS singhs@buffalo.edu 716-829-2453 1 Disclosures NO SIGNIFICANT FINANCIAL, GENERAL, OR OBLIGATION INTERESTS
History Parkinson`s disease. Parkinson's disease was first formally described in 1817 by a London physician named James Parkinson
 Parkinsonismm History Parkinson`s disease Parkinson's disease was first formally described in 1817 by a London physician named James Parkinson Definition : Parkinsonism: Parkinsonism is a progressive neurological
Parkinsonismm History Parkinson`s disease Parkinson's disease was first formally described in 1817 by a London physician named James Parkinson Definition : Parkinsonism: Parkinsonism is a progressive neurological
Key Concepts and Issues in Parkinson s Disease in 2016
 Key Concepts and Issues in Parkinson s Disease in 2016 Michael Rezak, M.D., Ph.D. Section Chief, Neurosciences Institute Director, Movement Disorders and Neurodegenerative Diseases Center Northwestern
Key Concepts and Issues in Parkinson s Disease in 2016 Michael Rezak, M.D., Ph.D. Section Chief, Neurosciences Institute Director, Movement Disorders and Neurodegenerative Diseases Center Northwestern
Cardinal Features of Parkinson s. Management of Parkinson s Disease. Drug Induced Parkinson s. Other Parkinson s Symptoms.
 Cardinal Features of Parkinson s Management of Parkinson s Disease Kristin S. Meyer, PharmD, CGP, FASHP Assistant Professor of Pharmacy Practice Drake University & Iowa Veterans Home Spring 2009 Tremor
Cardinal Features of Parkinson s Management of Parkinson s Disease Kristin S. Meyer, PharmD, CGP, FASHP Assistant Professor of Pharmacy Practice Drake University & Iowa Veterans Home Spring 2009 Tremor
Parkinson s Disease. Prevalence. Mark S. Baron, M.D. Cardinal Features. Clinical Characteristics. Not Just a Movement Disorder
 Prevalence Parkinson s Disease Mark S. Baron, M.D. Associate Professor of Neurology Movement Disorders Section VCU School of Medicine Common disorder Approaching 1% by 65 yrs of age, 2% by 80 yrs of age
Prevalence Parkinson s Disease Mark S. Baron, M.D. Associate Professor of Neurology Movement Disorders Section VCU School of Medicine Common disorder Approaching 1% by 65 yrs of age, 2% by 80 yrs of age
PARKINSON S PRIMER. Dr. Kathryn Giles MD, MSc, FRCPC Cambridge, Ontario, Canada
 PARKINSON S PRIMER Dr. Kathryn Giles MD, MSc, FRCPC Cambridge, Ontario, Canada COPYRIGHT 2017 BY SEA COURSES INC. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
PARKINSON S PRIMER Dr. Kathryn Giles MD, MSc, FRCPC Cambridge, Ontario, Canada COPYRIGHT 2017 BY SEA COURSES INC. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Advanced Therapies for Motor Symptoms in PD. Matthew Boyce MD
 Advanced Therapies for Motor Symptoms in PD Matthew Boyce MD Medtronic Education Teva Speakers Bureau Acadia Speakers Bureau Disclosures Discuss issues in advanced PD Adjunct therapies to levo-dopa Newer
Advanced Therapies for Motor Symptoms in PD Matthew Boyce MD Medtronic Education Teva Speakers Bureau Acadia Speakers Bureau Disclosures Discuss issues in advanced PD Adjunct therapies to levo-dopa Newer
Program Highlights. Michael Pourfar, MD Co-Director, Center for Neuromodulation New York University Langone Medical Center New York, New York
 Program Highlights David Swope, MD Associate Professor of Neurology Mount Sinai Health System New York, New York Michael Pourfar, MD Co-Director, Center for Neuromodulation New York University Langone
Program Highlights David Swope, MD Associate Professor of Neurology Mount Sinai Health System New York, New York Michael Pourfar, MD Co-Director, Center for Neuromodulation New York University Langone
Parkinson s Disease. Sirilak yimcharoen
 Parkinson s Disease Sirilak yimcharoen EPIDEMIOLOGY ~1% of people over 55 years Age range 35 85 years peak age of onset is in the early 60s ~5% of cases characterized by an earlier age of onset (typically
Parkinson s Disease Sirilak yimcharoen EPIDEMIOLOGY ~1% of people over 55 years Age range 35 85 years peak age of onset is in the early 60s ~5% of cases characterized by an earlier age of onset (typically
9/26/18. Objectives. Disclosures. Parkinson s Disease Update Clinical and Operational Considerations
 Parkinson s Disease Update Clinical and Operational Considerations Dana Saffel, PharmD, BCGP, CPh, FASCP President, CEO PharmaCare Strategies, Inc. September 2018 Objectives Describe epidemiology and pathophysiology
Parkinson s Disease Update Clinical and Operational Considerations Dana Saffel, PharmD, BCGP, CPh, FASCP President, CEO PharmaCare Strategies, Inc. September 2018 Objectives Describe epidemiology and pathophysiology
Recent Advances in the cause and treatment of Parkinson disease. Anthony Schapira Head of Dept. Clinical Neurosciences UCL Institute of Neurology UCL
 Recent Advances in the cause and treatment of Parkinson disease Anthony Schapira Head of Dept. Clinical Neurosciences UCL Institute of Neurology UCL SOME BACKGROUND incidence rate (per 100.000 person years)
Recent Advances in the cause and treatment of Parkinson disease Anthony Schapira Head of Dept. Clinical Neurosciences UCL Institute of Neurology UCL SOME BACKGROUND incidence rate (per 100.000 person years)
Parkinson s Disease. Gillian Sare
 Parkinson s Disease Gillian Sare Outline Reminder about PD Parkinson s disease in the inpatient Surgical patients with PD Patients who cannot swallow End of life care Parkinson s disease PD is the second
Parkinson s Disease Gillian Sare Outline Reminder about PD Parkinson s disease in the inpatient Surgical patients with PD Patients who cannot swallow End of life care Parkinson s disease PD is the second
Issues for Patient Discussion
 onmotor complications radykinesia Screening Tools asked PD micrographia eurodegeneration Designed for Use by Family Practitioners remor on-off opamine agonists tiffness depression ostural instability wearing
onmotor complications radykinesia Screening Tools asked PD micrographia eurodegeneration Designed for Use by Family Practitioners remor on-off opamine agonists tiffness depression ostural instability wearing
Faculty. Joseph Friedman, MD
 Faculty Claire Henchcliffe, MD, DPhil Associate Professor of Neurology Weill Cornell Medical College Associate Attending Neurologist New York-Presbyterian Hospital Director of the Parkinson s Institute
Faculty Claire Henchcliffe, MD, DPhil Associate Professor of Neurology Weill Cornell Medical College Associate Attending Neurologist New York-Presbyterian Hospital Director of the Parkinson s Institute
Non-Motor Symptoms of Parkinson s Disease
 Non-Motor Symptoms of Parkinson s Disease Samantha Holden, MD University of Colorado Movement Disorders MOTOR SYMPTOMS Rigidity Bradykinesia Tremor Gait Imbalance NON-MOTOR SYMPTOMS Dementia Urinary frequency
Non-Motor Symptoms of Parkinson s Disease Samantha Holden, MD University of Colorado Movement Disorders MOTOR SYMPTOMS Rigidity Bradykinesia Tremor Gait Imbalance NON-MOTOR SYMPTOMS Dementia Urinary frequency
8/28/2017. Behind the Scenes of Parkinson s Disease
 BEHIND THE SCENCES IN Parkinson s Disease Behind the Scenes of Parkinson s Disease Anna Marie Wellins DNP, ANP C Objectives Describe prevalence of Parkinson's disease (PD) Describe the hallmark pathologic
BEHIND THE SCENCES IN Parkinson s Disease Behind the Scenes of Parkinson s Disease Anna Marie Wellins DNP, ANP C Objectives Describe prevalence of Parkinson's disease (PD) Describe the hallmark pathologic
Drugs Affecting the Central Nervous System
 Asst Prof Inam S Arif isamalhaj@yahoo.com Drugs Affecting the Central Nervous System Ass Efferent neurons in ANS Neurodegenerative Diseases Parkinson s Disease Multiple Sclerosis Alzheimer s Disease
Asst Prof Inam S Arif isamalhaj@yahoo.com Drugs Affecting the Central Nervous System Ass Efferent neurons in ANS Neurodegenerative Diseases Parkinson s Disease Multiple Sclerosis Alzheimer s Disease
Evaluation of Parkinson s Patients and Primary Care Providers
 Evaluation of Parkinson s Patients and Primary Care Providers 2018 Movement Disorders Half Day Symposium Elise Anderson MD Medical Co-Director, PBSI Movement Disorders 6/28/2018 1 Disclosures GE Speaker,
Evaluation of Parkinson s Patients and Primary Care Providers 2018 Movement Disorders Half Day Symposium Elise Anderson MD Medical Co-Director, PBSI Movement Disorders 6/28/2018 1 Disclosures GE Speaker,
Drugs for Parkinson s Disease
 This Clinical Resource gives subscribers additional insight related to the Recommendations published in July 2017 ~ Resource #330705 Drugs for Parkinson s Disease Parkinson s disease is characterized by
This Clinical Resource gives subscribers additional insight related to the Recommendations published in July 2017 ~ Resource #330705 Drugs for Parkinson s Disease Parkinson s disease is characterized by
Movement Disorders: A Brief Overview
 Movement Disorders: A Brief Overview Albert Hung, MD, PhD Massachusetts General Hospital Harvard Medical School August 17, 2006 Cardinal Features of Parkinsonism Tremor Rigidity Bradykinesia Postural imbalance
Movement Disorders: A Brief Overview Albert Hung, MD, PhD Massachusetts General Hospital Harvard Medical School August 17, 2006 Cardinal Features of Parkinsonism Tremor Rigidity Bradykinesia Postural imbalance
Alison Charleston 1 st September 2016
 Alison Charleston 1 st September 2016 Clinical features of Parkinson s disease Differential diagnosis Management of the motor features Non-motor and neuropsychiatric aspects 100-200 per 100,000 prevalence
Alison Charleston 1 st September 2016 Clinical features of Parkinson s disease Differential diagnosis Management of the motor features Non-motor and neuropsychiatric aspects 100-200 per 100,000 prevalence
475 GERIATRIC PSYCHOPHARMACOLOGY (p.1)
") 475 GERIATRIC PSYCHOPHARMACOLOGY (p.1) I. General Information? Use lower doses? Start low and go slow? Expect prolonged elimination ½ lives? Expect sedative-hypnotics to be dementing, to impair cognitive
475 GERIATRIC PSYCHOPHARMACOLOGY (p.1) I. General Information? Use lower doses? Start low and go slow? Expect prolonged elimination ½ lives? Expect sedative-hypnotics to be dementing, to impair cognitive
With Time, The Pathology of PD Spreads Throughout the Brain
 With Time, The Pathology of PD Spreads Throughout the Brain Braak s staging of Parkinson s disease pathology dm co sn mc hc fc 1 Hubert H. Fernandez, MD, FAAN Professor of Medicine (Neurology) Cleveland
With Time, The Pathology of PD Spreads Throughout the Brain Braak s staging of Parkinson s disease pathology dm co sn mc hc fc 1 Hubert H. Fernandez, MD, FAAN Professor of Medicine (Neurology) Cleveland
10/4/2016. Disclosures. Motor symptoms are Just the tip of the iceberg. Parkinson s Disease for the Primary Care Clinician
 Disclosures Parkinson s Disease for the Primary Care Clinician Maya Katz, M.D. Assistant Professor of Neurology Movement Disorder and Neuromodulation Center UCSF Medical Center Consulting services for
Disclosures Parkinson s Disease for the Primary Care Clinician Maya Katz, M.D. Assistant Professor of Neurology Movement Disorder and Neuromodulation Center UCSF Medical Center Consulting services for
Welcome and Introductions
 Parkinson s Disease Spotlight on Addressing Motor and Non-Motor Symptoms The Changing Landscape Wednesday, March 8, 2017 Welcome and Introductions Stephanie Paul Vice President Development and Marketing
Parkinson s Disease Spotlight on Addressing Motor and Non-Motor Symptoms The Changing Landscape Wednesday, March 8, 2017 Welcome and Introductions Stephanie Paul Vice President Development and Marketing
Update on the Treatment of Parkinson s Disease. Neurotherapeutics for Rehab Professionals November 6 th, 2015
 Brent Bluett, DO Dr. Brent Bluett completed medical school at Touro Unviersity Nevada College of Osteopathic Medicine, neurology residency at the University of Texas Southwestern at Austin, and a Movement
Brent Bluett, DO Dr. Brent Bluett completed medical school at Touro Unviersity Nevada College of Osteopathic Medicine, neurology residency at the University of Texas Southwestern at Austin, and a Movement
Any interventions, where RCTs in PD are not available, are not included in the tables.
 Tables Interventions where new studies have been published are indicated in bold italics. Changes in conclusions are indicated in italics and are highlighted in yellow. Any interventions, where RCTs in
Tables Interventions where new studies have been published are indicated in bold italics. Changes in conclusions are indicated in italics and are highlighted in yellow. Any interventions, where RCTs in
Pharmacy Coverage Guidelines are subject to change as new information becomes available.
 ZELAPAR (selegiline hydrochloride) orally disintegrating tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific
ZELAPAR (selegiline hydrochloride) orally disintegrating tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific
Parkinson s disease. Information for patients and carers. The Leeds Teaching Hospitals NHS Trust
 n The Leeds Teaching Hospitals NHS Trust Parkinson s disease Information for patients and carers in partnership with Leeds Community Healthcare NHS Trust The symptoms of Parkinson s appear when the levels
n The Leeds Teaching Hospitals NHS Trust Parkinson s disease Information for patients and carers in partnership with Leeds Community Healthcare NHS Trust The symptoms of Parkinson s appear when the levels
Welcome and Introductions
 Parkinson s Disease Spotlight on Treatment Advances Tuesday, January 26, 2016 Welcome and Introductions Stephanie Paul Vice President Development and Marketing American Parkinson Disease Association 1
Parkinson s Disease Spotlight on Treatment Advances Tuesday, January 26, 2016 Welcome and Introductions Stephanie Paul Vice President Development and Marketing American Parkinson Disease Association 1
PARKINS ON CENTER. Parkinson s Disease: Diagnosis and Management. Learning Objectives: Recognition of PD OHSU. Disclosure Information
 OHSU PARKINS ON CENTER Parkinson s Disease: Diagnosis and Management for Every MD Disclosure Information Grants/Research Support: National Parkinson Foundation, NIH, Michael J. Fox Foundation Consultant:
OHSU PARKINS ON CENTER Parkinson s Disease: Diagnosis and Management for Every MD Disclosure Information Grants/Research Support: National Parkinson Foundation, NIH, Michael J. Fox Foundation Consultant:
Parkinson s Disease and Treatment Options for the Younger Adult
 Parkinson s Disease and Treatment Options for the Younger Adult David E. Riley, M.D. Chair, Medical Education InMotion April 22, 2016 Case Presentation - 1 A 57-year-old woman had Tremor of her right hand
Parkinson s Disease and Treatment Options for the Younger Adult David E. Riley, M.D. Chair, Medical Education InMotion April 22, 2016 Case Presentation - 1 A 57-year-old woman had Tremor of her right hand
Parkinson s Disease and Treatment Options for the Younger Adult
 The Way CME Should Be Parkinson s Disease and Treatment Options for the Younger Adult David E. Riley, M.D. Chair, Medical Education InMotion April 22, 2016 Case Presentation - 1 A 57-year-old woman had
The Way CME Should Be Parkinson s Disease and Treatment Options for the Younger Adult David E. Riley, M.D. Chair, Medical Education InMotion April 22, 2016 Case Presentation - 1 A 57-year-old woman had
Drugs used in Parkinsonism
 Drugs used in Parkinsonism قادة فريق علم األدوية : لي التميمي & عبدالرحمن ذكري الشكر موصول ألعضاء الفريق املتميزين : جومانة القحطاني ندى الصومالي روان سعد القحطاني pharma436@outlook.com @pharma436 Your
Drugs used in Parkinsonism قادة فريق علم األدوية : لي التميمي & عبدالرحمن ذكري الشكر موصول ألعضاء الفريق املتميزين : جومانة القحطاني ندى الصومالي روان سعد القحطاني pharma436@outlook.com @pharma436 Your
Parkinson Disease. Lorraine Kalia, MD, PhD, FRCPC. Presented by: Ontario s Geriatric Steering Committee
 Parkinson Disease Lorraine Kalia, MD, PhD, FRCPC Key Learnings Parkinson Disease (L. Kalia) Key Learnings Parkinson disease is the most common but not the only cause of parkinsonism Parkinson disease is
Parkinson Disease Lorraine Kalia, MD, PhD, FRCPC Key Learnings Parkinson Disease (L. Kalia) Key Learnings Parkinson disease is the most common but not the only cause of parkinsonism Parkinson disease is
Commonly encountered medications and their side effects - what the generalist needs to know
 Commonly encountered medications and their side effects - what the generalist needs to know Jeremy Cosgrove Consultant Neurologist Leeds Teaching Hospitals NHS Trust Outline: Parkinson s medications and
Commonly encountered medications and their side effects - what the generalist needs to know Jeremy Cosgrove Consultant Neurologist Leeds Teaching Hospitals NHS Trust Outline: Parkinson s medications and
Parkinson's Disease KP Update
 Parkinson's Disease KP Update Andrew Imbus, PA-C Neurology, Movement Disorders Kaiser Permanente, Los Angeles Medical Center No disclosures "I often say now I don't have any choice whether or not I have
Parkinson's Disease KP Update Andrew Imbus, PA-C Neurology, Movement Disorders Kaiser Permanente, Los Angeles Medical Center No disclosures "I often say now I don't have any choice whether or not I have
Advances in Parkinson s Disease Treatment. Ryan J. Uitti, M.D. Professor of Neurology Mayo Clinic, Jacksonville, FL
 Advances in Parkinson s Disease Treatment Ryan J. Uitti, M.D. Professor of Neurology Mayo Clinic, Jacksonville, FL Uitti.ryan@mayo.edu Ryan J. Uitti, MD Disclosure receives research support from NIH/NINDS,
Advances in Parkinson s Disease Treatment Ryan J. Uitti, M.D. Professor of Neurology Mayo Clinic, Jacksonville, FL Uitti.ryan@mayo.edu Ryan J. Uitti, MD Disclosure receives research support from NIH/NINDS,
Parkinson s Disease Initial Clinical and Diagnostic Evaluation. J. Timothy Greenamyre, MD, PhD
 Parkinson s Disease Initial Clinical and Diagnostic Evaluation J. Timothy Greenamyre, MD, PhD Involuntary tremulous motion, with lessened muscular power, in parts not in action and even when supported
Parkinson s Disease Initial Clinical and Diagnostic Evaluation J. Timothy Greenamyre, MD, PhD Involuntary tremulous motion, with lessened muscular power, in parts not in action and even when supported
The Role of Pharmacists in Treating & Managing Parkinson s Disease Author: Mary Jo Carden, RPh, JD Principal, Carden Associates
 The Role of Pharmacists in Treating & Managing Parkinson s Disease Author: Mary Jo Carden, RPh, JD Principal, Carden Associates Editor: Marsha K. Millonig, MBA, RPh President/CEO Catalyst Enterprises,
The Role of Pharmacists in Treating & Managing Parkinson s Disease Author: Mary Jo Carden, RPh, JD Principal, Carden Associates Editor: Marsha K. Millonig, MBA, RPh President/CEO Catalyst Enterprises,
Clinical Features and Treatment of Parkinson s Disease
 Clinical Features and Treatment of Parkinson s Disease Richard Camicioli, MD, FRCPC Cognitive and Movement Disorders Department of Medicine University of Alberta 1 Objectives To review the diagnosis and
Clinical Features and Treatment of Parkinson s Disease Richard Camicioli, MD, FRCPC Cognitive and Movement Disorders Department of Medicine University of Alberta 1 Objectives To review the diagnosis and
Parkinson s disease Therapeutic strategies. Surat Tanprawate, MD Division of Neurology University of Chiang Mai
 Parkinson s disease Therapeutic strategies Surat Tanprawate, MD Division of Neurology University of Chiang Mai 1 Scope Modality of treatment Pathophysiology of PD and dopamine metabolism Drugs Are there
Parkinson s disease Therapeutic strategies Surat Tanprawate, MD Division of Neurology University of Chiang Mai 1 Scope Modality of treatment Pathophysiology of PD and dopamine metabolism Drugs Are there
CE on SUNDAY Newark, NJ October 18, 2009
 CE on SUNDAY Newark, NJ October 18, 2009 Date: Sunday, October 18, 2009 Time: 10:30 AM 11:45 AM Location: Sheraton Newark Airport Hotel Title: Speaker(s): Treating Parkinson s Disease: A Pharmacist s Overview
CE on SUNDAY Newark, NJ October 18, 2009 Date: Sunday, October 18, 2009 Time: 10:30 AM 11:45 AM Location: Sheraton Newark Airport Hotel Title: Speaker(s): Treating Parkinson s Disease: A Pharmacist s Overview
2/20/18. History of Parkinson s. What is happening in the brain? DOPAMINE! Epidemiology. Parkinson s Disease. It s much more than tremor
 Parkinson s Disease History of Parkinson s It s much more than tremor Laura Dixon, DNP, MPA, APRN, FNP-BC University of Louisville Department of Neurology Movement Disorders Division Parkinson s Disease
Parkinson s Disease History of Parkinson s It s much more than tremor Laura Dixon, DNP, MPA, APRN, FNP-BC University of Louisville Department of Neurology Movement Disorders Division Parkinson s Disease
Drug Therapy of Parkinsonism. Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia
 Drug Therapy of Parkinsonism Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Parkinsonism is a progressive neurological disorder of muscle movement, usually
Drug Therapy of Parkinsonism Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Parkinsonism is a progressive neurological disorder of muscle movement, usually
The PD You Don t See: Cognitive and Non-motor Symptoms
 The PD You Don t See: Cognitive and Non-motor Symptoms Benzi M. Kluger, M.D., M.S. Associate Professor of Neurology and Psychiatry Director Movement Disorders Center University of Colorado Denver Goals
The PD You Don t See: Cognitive and Non-motor Symptoms Benzi M. Kluger, M.D., M.S. Associate Professor of Neurology and Psychiatry Director Movement Disorders Center University of Colorado Denver Goals
ARE YOUR LEVODOPA PILLS WORKING LIKE THEY USED TO?
 ARE YOUR LEVODOPA PILLS WORKING LIKE THEY USED TO? You may have noticed a change... Levodopa is a common treatment for Parkinson s, and doctors have relied on it for decades. Over time as Parkinson s progresses,
ARE YOUR LEVODOPA PILLS WORKING LIKE THEY USED TO? You may have noticed a change... Levodopa is a common treatment for Parkinson s, and doctors have relied on it for decades. Over time as Parkinson s progresses,
Faculty Information 2/15/2013
 Timothy Reilly, PharmD, BCPS, CGP, FASCP Clinical Assistant Professor Ernest Mario School of Pharmacy Rutgers, The State University of New Jersey tjreilly@pharmacy.rutgers.edu Faculty Information Presenter:
Timothy Reilly, PharmD, BCPS, CGP, FASCP Clinical Assistant Professor Ernest Mario School of Pharmacy Rutgers, The State University of New Jersey tjreilly@pharmacy.rutgers.edu Faculty Information Presenter:
Prior Authorization with Quantity Limit Program Summary
 Gocovri (amantadine) Prior Authorization with Quantity Limit Program Summary This prior authorization applies to Commercial, NetResults A series, SourceRx and Health Insurance Marketplace formularies.
Gocovri (amantadine) Prior Authorization with Quantity Limit Program Summary This prior authorization applies to Commercial, NetResults A series, SourceRx and Health Insurance Marketplace formularies.
Pharmacy Coverage Guidelines are subject to change as new information becomes available.
 ZELAPAR (selegiline hydrochloride) orally disintegrating tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific
ZELAPAR (selegiline hydrochloride) orally disintegrating tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific
Parkinson s Disease. Medications
 Parkinson s Disease Medications By David Houghton, MD, MPH, Howard Hurtig, MD, and Sharon Metz, RN, MPH, with guest authors Monique Giroux, MD, Giselle Petzinger, MD, Beth Fisher, PT, PhD, Lauren Hawthorne,
Parkinson s Disease Medications By David Houghton, MD, MPH, Howard Hurtig, MD, and Sharon Metz, RN, MPH, with guest authors Monique Giroux, MD, Giselle Petzinger, MD, Beth Fisher, PT, PhD, Lauren Hawthorne,
Dr Barry Snow. Neurologist Auckland District Health Board
 Dr Barry Snow Neurologist Auckland District Health Board Dystonia and Parkinson s disease Barry Snow Gowers 1888: Tetanoid chorea Dystonia a movement disorder characterized by sustained or intermittent
Dr Barry Snow Neurologist Auckland District Health Board Dystonia and Parkinson s disease Barry Snow Gowers 1888: Tetanoid chorea Dystonia a movement disorder characterized by sustained or intermittent
Anticholinergics. COMT* Inhibitors. Dopaminergic Agents. Dopamine Agonists. Combination Product
 Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-945-5220 Fax 503-947-1119 Class Update: Parkinson s Drugs Month/Year of Review:
Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-945-5220 Fax 503-947-1119 Class Update: Parkinson s Drugs Month/Year of Review:
PD ExpertBriefing: What s in the Parkinson s Pipeline
 PD ExpertBriefing: What s in the Parkinson s Pipeline Presented by: David G. Standaert, M.D., Ph.D. Professor of Neurology Director, Center for Neurodegeneration and Experimental Therapeutics University
PD ExpertBriefing: What s in the Parkinson s Pipeline Presented by: David G. Standaert, M.D., Ph.D. Professor of Neurology Director, Center for Neurodegeneration and Experimental Therapeutics University
Parkinson's Disease and how you can make a difference with medication
 Parkinson's Disease and how you can make a difference with medication Alyson Franks Parkinson's and Movement Disorder Nurse Specialist Royal Hallamshire Hospital No treatment all Complementary Therapy
Parkinson's Disease and how you can make a difference with medication Alyson Franks Parkinson's and Movement Disorder Nurse Specialist Royal Hallamshire Hospital No treatment all Complementary Therapy
05-Nov-15. Impact of Parkinson s Disease in Australia. The Nature of Parkinson s disease 21st Century
 Peter Silburn Professor Clinical Neuroscience University of Queensland Queensland Brain Institute Neurosciences Queensland Impact of in Australia Second most common neurodegenerative disorder Up to 64,000
Peter Silburn Professor Clinical Neuroscience University of Queensland Queensland Brain Institute Neurosciences Queensland Impact of in Australia Second most common neurodegenerative disorder Up to 64,000
DRUGS THAT ACT IN THE CNS
 DRUGS THAT ACT IN THE CNS Drugs for Neurodegenerative Diseases 2 Dr Karamallah S. Mahmood PhD Clinical Pharmacology 1 DRUGS USED IN PARKINSON S DISEASE/ B. Selegiline and rasagiline Selegiline, also called
DRUGS THAT ACT IN THE CNS Drugs for Neurodegenerative Diseases 2 Dr Karamallah S. Mahmood PhD Clinical Pharmacology 1 DRUGS USED IN PARKINSON S DISEASE/ B. Selegiline and rasagiline Selegiline, also called
CENTENE PHARMACY AND THERAPEUTICS NEW DRUG REVIEW 3Q17 July August
 BRAND NAME Xadago GENERIC NAME Safinamide MANUFACTURER Newron Pharmaceuticals SpA holds license; granted approval. US WorldMeds, LLC exclusive licensee and distributor in the U.S. DATE OF APPROVAL March
BRAND NAME Xadago GENERIC NAME Safinamide MANUFACTURER Newron Pharmaceuticals SpA holds license; granted approval. US WorldMeds, LLC exclusive licensee and distributor in the U.S. DATE OF APPROVAL March
Welcome and Introductions
 Parkinson s Disease Spotlight on Parkinson s Choices Playing an Active Role in Your Treatment Plan Wednesday, August 17, 2016 Welcome and Introductions Stephanie Paul Vice President Development and Marketing
Parkinson s Disease Spotlight on Parkinson s Choices Playing an Active Role in Your Treatment Plan Wednesday, August 17, 2016 Welcome and Introductions Stephanie Paul Vice President Development and Marketing
Chapter 20. Media Directory. Amyotrophic Lateral Sclerosis. Alzheimer s Disease. Huntington s Chorea. Multiple Sclerosis
 Chapter 20 Drugs for Degenerative Diseases of the Nervous System Slide 18 Media Directory Levadopa Animation Upper Saddle River, New Jersey 07458 All rights reserved. Alzheimer s Disease Amyotrophic Lateral
Chapter 20 Drugs for Degenerative Diseases of the Nervous System Slide 18 Media Directory Levadopa Animation Upper Saddle River, New Jersey 07458 All rights reserved. Alzheimer s Disease Amyotrophic Lateral
10/13/2017. Disclosures. Deep Brain Stimulation in the Treatment of Movement Disorders. Deep Brain Stimulation: Objectives.
 Deep Brain Stimulation in the Treatment of Movement Disorders Disclosures None Eleanor K Orehek, M.D. Movement Disorders Specialist Noran Neurological Clinic 1 2 Objectives To provide an overview of deep
Deep Brain Stimulation in the Treatment of Movement Disorders Disclosures None Eleanor K Orehek, M.D. Movement Disorders Specialist Noran Neurological Clinic 1 2 Objectives To provide an overview of deep
Let s Look at Parkinson s (PD) Sheena Morgan Parkinson s Disease Nurse Specialist Isle of Wight NHS Trust November 2016
 Sheena Morgan Parkinson s Disease Nurse Specialist Isle of Wight NHS Trust November 2016") Let s Look at Parkinson s (PD) Sheena Morgan Parkinson s Disease Nurse Specialist Isle of Wight NHS Trust November 2016 What is Parkinson s? Parkinson's is a progressive neurological condition. People
Let s Look at Parkinson s (PD) Sheena Morgan Parkinson s Disease Nurse Specialist Isle of Wight NHS Trust November 2016 What is Parkinson s? Parkinson's is a progressive neurological condition. People
Presented by Meagan Koepnick, Josh McDonald, Abby Narayan, Jared Szabo Mentored by Dr. Doorn
 Presented by Meagan Koepnick, Josh McDonald, Abby Narayan, Jared Szabo Mentored by Dr. Doorn Objectives What agents do we currently have available and what do we ideally need? What biomarkers exist for
Presented by Meagan Koepnick, Josh McDonald, Abby Narayan, Jared Szabo Mentored by Dr. Doorn Objectives What agents do we currently have available and what do we ideally need? What biomarkers exist for
2-The age at onset of PD is variable, usually between 50 and 80 years, with a mean onset of 55 years (1).
.") Parkinson Disease 1-Parkinson disease (PD) is a chronic, progressive movement disorder resulting from loss of dopamine from the nigrostriatal tracts in the brain, and is characterized by rigidity, bradykinesia,
Parkinson Disease 1-Parkinson disease (PD) is a chronic, progressive movement disorder resulting from loss of dopamine from the nigrostriatal tracts in the brain, and is characterized by rigidity, bradykinesia,
PL CE LIVE July 2015 Forum
 July 2015 PL CE LIVE Rachel Maynard, PharmD Associate Editor Pharmacist s Letter/Pharmacy Technician s Letter CE Information Pharmacist's Letter / Therapeutic Research Center is accredited by the Accreditation
July 2015 PL CE LIVE Rachel Maynard, PharmD Associate Editor Pharmacist s Letter/Pharmacy Technician s Letter CE Information Pharmacist's Letter / Therapeutic Research Center is accredited by the Accreditation
Multiple choice questions: ANSWERS
 Multiple choice questions: ANSWERS Chapter 1. Redefining Parkinson s disease 1. Common non-motor features that precede the motor findings in Parkinson s disease (PD) include all of the following except?
Multiple choice questions: ANSWERS Chapter 1. Redefining Parkinson s disease 1. Common non-motor features that precede the motor findings in Parkinson s disease (PD) include all of the following except?
The Ins and Outs of PD Meds. Johanna Hartlein, APRN, MSN Family Nurse Practitoner and Great Hugger Washington University School of Medicine
 The Ins and Outs of PD Meds Johanna Hartlein, APRN, MSN Family Nurse Practitoner and Great Hugger Washington University School of Medicine Words of Caution Just because I list a possible side effect, it
The Ins and Outs of PD Meds Johanna Hartlein, APRN, MSN Family Nurse Practitoner and Great Hugger Washington University School of Medicine Words of Caution Just because I list a possible side effect, it
Margo J Nell Dept Pharmacology
 Margo J Nell Dept Pharmacology 1 The extra pyramidal system Separation of cortico-spinal system (pyramidal system, (PS)) from the basal ganglia (extra pyramidal motor system (EPS)) because they produce
Margo J Nell Dept Pharmacology 1 The extra pyramidal system Separation of cortico-spinal system (pyramidal system, (PS)) from the basal ganglia (extra pyramidal motor system (EPS)) because they produce
Parkinson's Disease Center and Movement Disorders Clinic
 Parkinson's Disease Center and Movement Disorders Clinic 7200 Cambridge Street, 9th Floor, Suite 9A Houston, Texas 77030 713-798-2273 phone pdcmdc@bcm.edu www.jankovic.org Parkinson s Disease Diagnosis
Parkinson's Disease Center and Movement Disorders Clinic 7200 Cambridge Street, 9th Floor, Suite 9A Houston, Texas 77030 713-798-2273 phone pdcmdc@bcm.edu www.jankovic.org Parkinson s Disease Diagnosis
Tremor, Rigidity, Tics and Dystonia: The 4 Most Common Movement Disorders
 Tremor, Rigidity, Tics and Dystonia: The 4 Most Common Movement Disorders VIGNETTE 1: HAND SHAKING 62 YOF tremor of both hands for 6 years FHx: Shaking in mother & maternal cousin PMH: Depression, HTN,
Tremor, Rigidity, Tics and Dystonia: The 4 Most Common Movement Disorders VIGNETTE 1: HAND SHAKING 62 YOF tremor of both hands for 6 years FHx: Shaking in mother & maternal cousin PMH: Depression, HTN,