Improving Healthcare Utilization in Injured Older Adults
|
|
|
- Flora Cole
- 5 years ago
- Views:
Transcription
1 Improving Healthcare Utilization in Injured Older Adults G ERIATRIC T R A U MA I N I T I AT I V E S AT S TA N F O R D H E A LT H C A R E J U LY 12, 2018
2 Objectives Background on Geriatric Trauma Population Needs Aging population Increasing rates of frail, elderly trauma patients Stanford Targeted Geriatric Screening Initiatives Early identification of baseline frailty can guide care with early prediction and proactive interventions Current implementation and Next Steps Integration Geriatrics with routine trauma care Dedicated hospital unit, order sets
3 Why The Elderly Matter Elderly = one of the fastest growing segments in US million over age 65 (25% increase from 2003) will double to 84 million Adults > 65: Up 30% of trauma patients, 25% of trauma mortality Falls, MVCs, burns Older adults hospitalized for injury are high risk for poor outcomes Increased complications and death Prolonged LOS Readmission Discharge to facilities rather than home Geriatric Trauma = High-Risk population

4 Ground Levels Falls Emerging as #1 cause for admission to trauma centers
5 Falls Most common mechanism of injury in elderly 5-10x more EMS calls r/t falls than MVCs 30% >65 y/o fall each year, 50% > 80 y/o 10% result in serious injury- fracture/chi 10-30% multi-trauma Leading cause non-fatal injuries in GT Problem of under-triage 4-7% mortality
6 Mortality From Ground Level Falls Bankey, Journal of Trauma, 2010
7 The Course of Disability before and after a Serious Fall Injury Prospective cohort over 14 yrs in 754 community-living persons age >70 Initially nondisabled in basic ADL 130 participants sustained serious fall 50% lived alone before fall Average age 86, 73% female 67% physically frail Gill et al, JAMA 2013, 173:
8 Results: Rapid recovery observed ONLY for those with no/mild disability before fall ONLY 1/3 with moderate disability recovered NO recovery in those with severe disability before fall Gill et al, JAMA 2013, 173:
9 Physiologic Reserve and Functional Outcomes
10 Results Few post-injury return to baseline status at 1yr. Cognitive impairment predicts functional status at 6-months 25% patients die within one year Age, injury severity, and pre-injury disability predict mortality within one year. Pre-injury physical frailty, as a measure of disability, is the predominant predictor of mortality at 6-months & 1yr.
11 How the frail elderly become disabled Case: 80 year old with emphysema hospitalized with post-ground level fall Perspective 1: Hospital Physician Perspective 2: Daughter Perspective Questions Why might these perspectives differ? Who has it right?
12 Case 1: Physician Perspective 80 yo with HTN, emphysema admitted post-fall, w/ dyspnea, fever, mild kidney impairment Chest Xray: 1 non-displaced rib #, small hemothorax Treatment: supportive Outcome: 5 days later, labs normal, CXR resolving, oxygen normal Disposition: Home Summary: Successful hospitalization
13 Case 2 : Daughter Perspective Mom was getting a little frail but was coping at home Fall leading to hospitalization In hospital: poor mobility, deconditioning,?confused. D/C home required ++ assistance 1 year later: NH. Died 2 years later
14 Summary Physician: Successful Hospitalization Daughter: Everything seemed to fall apart for Mom after she was hospitalized. It was the start of a downward spiral What is the daughter seeing that the physician did not see?
15 Hospitalization Disability Syndrome Hospitalization precipitates disability in older persons! After discharge, elder no longer able to take care of themselves without assistance Generally after hospitalization for medical condition that is not disabling Perception of successful medical treatment VERY common: 1/3 of elders over age 65 Bad prognosis: Over half the time, does NOT improve!!
16 Risk of Hospital Disability Syndrome Increases w/ Age Age % Decline Covinsky KE; JAGS; 2003;51:451
17 Risk Factors For Hospital Acquired Disability: The 3 D s Depression 3 fold higher risk for new ADL disability Dementia Mild Cognitive Impairment 2 fold higher Severe Cognitive Impairment 3 fold higher Delirium 3 fold higher risk Covinsky KE; JAMA; 2011;1575
18 Hospital Processes that Promote Disability Limited Mobility Delirium Inducement Malnutrition
19 The Readmission Circus Hospitals are obsessed with readmission But most efforts to reduce readmission will not succeed Disease management Medicine reconciliation Medical Follow-up Real reasons older patients fail at home Disability Cognitive Impairment Residual Delirium Social Caregiver stress
20 How do we identify early those with underlying frailty who are at greatest risk? 1. Stanford Geriatric Trauma Screen
21 Methods Patient selection: All patients >=65 years of age admitted to the Trauma service (including Trauma/SICU) undergo a geriatric trauma screen as part of the standard tertiary trauma survey conducted by the service APPs or SICU resident/fellow. Compliance with screening and referrals will be monitored and tracked. Screen positive in one or more domains triggers a Geriatrics consultation within 24 hours
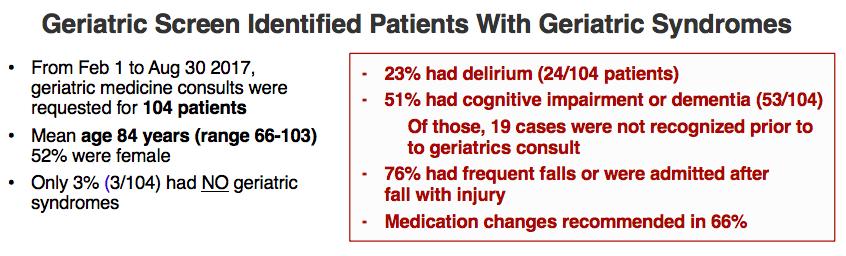
22 GT65 Screen Initiative
23 Summary of Goals Identify and manage geriatric trauma patients at high risk for: Optimize clinical management of geriatric trauma patients Assist trauma managers with registry documentation Empower trauma team and encourages multidisciplinary care Targets: reduce LOS, ICU readmissions, mortality Based on TQIP guidelines (ACS and AGS) and published evidence for early integration of geriatric principles in care of geriatric trauma patients
24

25
26 2. Geriatric Trauma Order sets and protocols IP Gen Surg/ Trauma Admission order sets (65+ version created and integrated to EPIC) Elderly Rib Fracture Pain Protocol (created with combined effort of Trauma, Geriatrics and Pain services)

27 BACKGROUND: Geriatric (>65yrs) patients are especially susceptible to rib fractures due to ground level falls, and have twice the mortality of younger patients MANAGEMENT: *Epidural Placement or Alternatives*: Paravertebral blockade Intercostal nerve blockade Contraindications to Epidural Catheter Placement: Coagulopathy, or anticoagulated with warfarin, apixaban or rivaroxiban Systemic infection Spinal cord injury or spinal fracture near area of catheter placement Delirious, dementia with active behavioral disturbances or noncooperative patient Body habitus (BMI>40) or unable to position the patient Consistent recording of pain scores Non-pharmacologic and pharmacologic treatment De-escalation prior to discharge Multidisciplinary care Family & patient engagement 27
:")


28 28 MANAGEMENT (PHARMACOLOGIC): Special consideration must be given to modulation of pain in elderly (dosing, side effects, risk of polypharmacy)
29 3. Acute Care for Elders Units (ACE Unit) Redesigned system of hospital care Goal: Reduce rate of functional decline in elderly Fits hospital to elderly rather than fit elderly to hospitals Nursing driven interventions Work best if patients and trained nurses colocated because culture driven




30 Key ACE Principles
31 Components of ACE intervention Prepared Environment Carpeting, large clocks, elevated toilet seats Patient Centered Care Daily assessment of functional status Protocols (self-care, nutrition, mobility) Daily rounds by multidisciplinary team Planning to go home Medical care review Daily review of medicines
32 Effects of ACE Unit Intervention Reduced rate of disability at discharge by 33% Reduced discharges to nursing homes by 30% Reduced average length of stay (0.5 days) 67% reduction in restraint use Greater satisfaction with care among patients, nurses, physicians Landefeld CS: NEJM;1995:1338 Counsell SR:JAGS;2000:1572
33 SHC ACE Pilot Phase I - Interventions SHC Surgical Nursing Unit All patients 65 yo and above (October 1 st, 2017 June 30 th, 2018) Admission Nursing Screening Tool (Tool #1 attached SPICES ADMIT) Document as Progress Note in emr and Follow suggested interventions Use information as baseline for patient s cognition/function Daily Team Rounds (Primary Team, Geriatrics APP, Nursing, CM, SW, Rehab) 10-11am, concurrent with other teams Nursing focus on SPICES (Sleep, Pain, Immobility, Cognition/Constipation, Enteral Nutrition, Social Support) Those with positive geriatric syndromes seen by a Geriatric APP. Nursing Hand-off SPICES Tool SPICES Hand-off tool (Tool #2 attached)

34 Nursing Admission Screen (Tool #1)
35 Nursing Hand-off Checklist (Tool #2)
36 SHC ACE Pilot Phase I Outcomes Oct 1 st, June 30 th, ~ 450 patients qualify as ACE patients (65+ discharged from designated nursing unit) Average 70% compliance with nursing interventions. 10% reduction in Delirium Burden (assessed by CAM positivity) Improvement in unit-based nursing - knowledge of and comfort in dealing with geriatric syndromes.
37 Implications For Hospital and Post-Hospital Care Hospitalization traditionally focuses on distinct episode of care Good care of the hospitalized patient demands Detailed understanding of the patient s functional, cognitive, and social context even before admission!
38 Future Geriatric Trauma High Value Clinical Pathway Focus on streamlining care for the geriatric trauma population from presentation to the ED to post-discharge. Proactive and multi-disciplinary approach with standardized pathways.
39 GC Take-Home Messages Better detection/treatment of geriatric specific concerns and conditions GC associated with increased/more thorough advanced planning discussions Possible reduction in ICU LOS and readmission Proof of concept wrt systems integration; GC is sustainable
40 Acknowledgements - Inpatient Geriatric Med Team - Trauma and SICU team - C2 Nursing - SHC Quality/ Safety, High Value team members


41 Q&A? Trauma Critical Care Geriatrics
The Geriatrician in the Trauma Service. Trauma Quality Improvement Program (TQIP) Annual Scientific Meeting and Training 2013
 Annual Scientific Meeting and Training 2013") The Geriatrician in the Trauma Service Trauma Quality Improvement Program (TQIP) Annual Scientific Meeting and Training 2013 Challenges of the Geriatric Trauma Patient Challenges of the Geriatric Patient
The Geriatrician in the Trauma Service Trauma Quality Improvement Program (TQIP) Annual Scientific Meeting and Training 2013 Challenges of the Geriatric Trauma Patient Challenges of the Geriatric Patient
Quality Care for the Hospitalized Older Adult
 Quality Care for the Hospitalized Older Adult Quality Care for the Hospitalized Older Adult Shelley R McDonald, DO, PhD May 19 th, 2018 Objectives To define why the hospital is a dangerous place for older
Quality Care for the Hospitalized Older Adult Quality Care for the Hospitalized Older Adult Shelley R McDonald, DO, PhD May 19 th, 2018 Objectives To define why the hospital is a dangerous place for older
Management of the Frail Older Patients: What Are the Outcomes
 Management of the Frail Older Patients: What Are the Outcomes Professor Edwina Brown Imperial College Renal and Transplant Centre Hammersmith Hospital, London Increasing prevalence of old old on RRT RRT
Management of the Frail Older Patients: What Are the Outcomes Professor Edwina Brown Imperial College Renal and Transplant Centre Hammersmith Hospital, London Increasing prevalence of old old on RRT RRT
There s No Place like Home
 THERE S NO PLACE LIKE HOME There s No Place like Home Regional Advisory Committee for Excellence in Care of Older Adults Elements of the Program TAKE AWAY SERVICES R & G PROGRAM CONSULTATION O SERVICES
THERE S NO PLACE LIKE HOME There s No Place like Home Regional Advisory Committee for Excellence in Care of Older Adults Elements of the Program TAKE AWAY SERVICES R & G PROGRAM CONSULTATION O SERVICES
Evaluating Functional Status in Hospitalized Geriatric Patients. UCLA-Santa Monica Geriatric Medicine Didactic Lecture Series
 Evaluating Functional Status in Hospitalized Geriatric Patients UCLA-Santa Monica Geriatric Medicine Didactic Lecture Series Case 88 y.o. woman was admitted for a fall onto her hip. She is having trouble
Evaluating Functional Status in Hospitalized Geriatric Patients UCLA-Santa Monica Geriatric Medicine Didactic Lecture Series Case 88 y.o. woman was admitted for a fall onto her hip. She is having trouble
Multidisciplinary Geriatric Trauma Care Guideline
 Multidisciplinary Geriatric Trauma Care Background Traumatic injury in the geriatric population is increasing in prevalence and is associated with higher mortality and complication rates comparted to younger
Multidisciplinary Geriatric Trauma Care Background Traumatic injury in the geriatric population is increasing in prevalence and is associated with higher mortality and complication rates comparted to younger
Delirium in the Elderly
 Delirium in the Elderly ELITE 2017 Liza Genao, MD Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity Very much under-recognized
Delirium in the Elderly ELITE 2017 Liza Genao, MD Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity Very much under-recognized
EAST MULTICENTER STUDY DATA COLLECTION TOOL
 EAST MULTICENTER STUDY DATA COLLECTION TOOL Multicenter Study: Effect of Regional Anesthesia on Delirium in Geriatric Trauma Patients with Multiple Rib Fractures Enrolling Center: Enrolling Co-investigators:
EAST MULTICENTER STUDY DATA COLLECTION TOOL Multicenter Study: Effect of Regional Anesthesia on Delirium in Geriatric Trauma Patients with Multiple Rib Fractures Enrolling Center: Enrolling Co-investigators:
Guidelines for Management of the Geriatric & Medically Complex Trauma Patients
 Guidelines for Management of the Geriatric & Medically Complex Trauma Patients Objectives: Provide a framework for consultation of the medical service in medically complex Trauma patients Provide a template
Guidelines for Management of the Geriatric & Medically Complex Trauma Patients Objectives: Provide a framework for consultation of the medical service in medically complex Trauma patients Provide a template
Frailty and Rehabilitation: How We Utilized FIM Data to Develop Risk Models
 Frailty and Rehabilitation: How We Utilized FIM Data to Develop Risk Models User Groups 2015 Orlando, Florida March 19, 2015 Las Vegas, Nevada May 7, 2015 Pam Roberts, PhD, OTR/L, SCFES, FAOTA, CPHQ, FNAP
Frailty and Rehabilitation: How We Utilized FIM Data to Develop Risk Models User Groups 2015 Orlando, Florida March 19, 2015 Las Vegas, Nevada May 7, 2015 Pam Roberts, PhD, OTR/L, SCFES, FAOTA, CPHQ, FNAP
Delirium in the Elderly
 Delirium in the Elderly ELITE 2015 Mamata Yanamadala M.B.B.S, MS Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity
Delirium in the Elderly ELITE 2015 Mamata Yanamadala M.B.B.S, MS Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity
Development of Guidelines to Manage Geriatric Trauma Patients. Kelly Czarnecki MS,FNP
 Development of Guidelines to Manage Geriatric Trauma Patients Kelly Czarnecki MS,FNP No Disclosures Disclosures Project Introduction According to best practice recommendations the geriatric trauma population
Development of Guidelines to Manage Geriatric Trauma Patients Kelly Czarnecki MS,FNP No Disclosures Disclosures Project Introduction According to best practice recommendations the geriatric trauma population
People at the centre of health and care
 People at the centre of health and care Improving Care for Older People in Acute Care F is for Frailty F is for Frailty Identification and co-ordination of care for frail older people Starting point -
People at the centre of health and care Improving Care for Older People in Acute Care F is for Frailty F is for Frailty Identification and co-ordination of care for frail older people Starting point -
Falls Prevention Best Practice
 Falls Prevention Best Practice Prepared by Denise Tomassini Falls Prevention A case study : Mr Tony Topples ISLHD Clinical Quality Manager Clinical Governance Unit November 2011 Falls Prevention Best Practice
Falls Prevention Best Practice Prepared by Denise Tomassini Falls Prevention A case study : Mr Tony Topples ISLHD Clinical Quality Manager Clinical Governance Unit November 2011 Falls Prevention Best Practice
Hospitalization- Associated Disability
 Hospitalization- Associated Disability Deborah Villarreal, MD Assistant Professor Geriatric and Palliative Medicine An Unfortunately Common Scenario Mrs.G 70 y/o BF DM type II, HTN, s/p CVA, OA, OP admitted
Hospitalization- Associated Disability Deborah Villarreal, MD Assistant Professor Geriatric and Palliative Medicine An Unfortunately Common Scenario Mrs.G 70 y/o BF DM type II, HTN, s/p CVA, OA, OP admitted
Evolutions in Geriatric Fracture Care Preparing for the Silver Tsunami
 Evolutions in Geriatric Fracture Care Preparing for the Silver Tsunami James Holstine, DO Medical Director for the Joint Replacement Center, Geriatric Fracture Center, Orthopedic Surgeon PeaceHealth Whatcom
Evolutions in Geriatric Fracture Care Preparing for the Silver Tsunami James Holstine, DO Medical Director for the Joint Replacement Center, Geriatric Fracture Center, Orthopedic Surgeon PeaceHealth Whatcom
Guidelines for Management and Prevention of Delirium In Geriatric Trauma Patients
 Guidelines for Management and Prevention of Delirium In Geriatric Trauma Patients Objectives: Provide a guideline for recognizing and managing delirium in geriatric trauma patients. Provide a template
Guidelines for Management and Prevention of Delirium In Geriatric Trauma Patients Objectives: Provide a guideline for recognizing and managing delirium in geriatric trauma patients. Provide a template
Saman Arbabi M.D., M.P.H., F.A.C.S. Kathleen O'Connell M.D. Bryce Robinson M.D., M.S., F.A.C.S., F.C.C.M
 Form "EAST Multicenter Study Proposal" Study Title Primary investigator / Senior researcher Email of Primary investigator / Senior researcher Co-primary investigator Are you a current member of EAST? If
Form "EAST Multicenter Study Proposal" Study Title Primary investigator / Senior researcher Email of Primary investigator / Senior researcher Co-primary investigator Are you a current member of EAST? If
4/26/2012. Laura Grooms, MD Assistant Professor Geriatric Medicine Department of Family and Geriatric Medicine University of Louisville April 20, 2012
 Laura Grooms, MD Assistant Professor Geriatric Medicine Department of Family and Geriatric Medicine University of Louisville April 20, 2012 Laura Grooms, MD Assistant Professor Geriatric Medicine Department
Laura Grooms, MD Assistant Professor Geriatric Medicine Department of Family and Geriatric Medicine University of Louisville April 20, 2012 Laura Grooms, MD Assistant Professor Geriatric Medicine Department
Why New Thinking is Needed for Older Adults across the Rehabilitation Continuum
 Why New Thinking is Needed for Older Adults across the Rehabilitation Continuum Samir K. Sinha MD, DPhil, FRCPC Director of Geriatrics Mount Sinai and the University Health Network Hospitals Assistant
Why New Thinking is Needed for Older Adults across the Rehabilitation Continuum Samir K. Sinha MD, DPhil, FRCPC Director of Geriatrics Mount Sinai and the University Health Network Hospitals Assistant
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative
 Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Fall Risk Assessment and Prevention in the Post-Acute Setting A Road Map
 Fall Risk Assessment and Prevention in the Post-Acute Setting A Road Map Cora M. Butler, JD, RN, CHC HealthCore Value Advisors, Inc. Juli A. James, RN Primaris Holdings, Inc. Objectives Explore the burden
Fall Risk Assessment and Prevention in the Post-Acute Setting A Road Map Cora M. Butler, JD, RN, CHC HealthCore Value Advisors, Inc. Juli A. James, RN Primaris Holdings, Inc. Objectives Explore the burden
Surgery in Frail Elders. Emily Finlayson, MD, MS Department of Surgery University of California, San Francisco September, 2011
 Surgery in Frail Elders Emily Finlayson, MD, MS Department of Surgery University of California, San Francisco September, 2011 What we re going to cover Mortality after surgery in the elderly Fact v Fantasy
Surgery in Frail Elders Emily Finlayson, MD, MS Department of Surgery University of California, San Francisco September, 2011 What we re going to cover Mortality after surgery in the elderly Fact v Fantasy
TRAUMA ALERT: THE OLDER ADULT TRAUMA PATIENT - FIX ME QUICK
 TRAUMA ALERT: THE OLDER ADULT TRAUMA PATIENT - FIX ME QUICK Alicia Mangram, MD, FACS HonorHealth John C. Lincoln Medical Center Learning Objectives: Prevalence of geriatric trauma. New management strategies.
TRAUMA ALERT: THE OLDER ADULT TRAUMA PATIENT - FIX ME QUICK Alicia Mangram, MD, FACS HonorHealth John C. Lincoln Medical Center Learning Objectives: Prevalence of geriatric trauma. New management strategies.
*GERIATRIC FELLOWSHIP COMPETENCY CHECKLIST EDUCATIONAL GOALS:
 *GERIATRIC FELLOWSHIP COMPETENCY CHECKLIST EDUCATIONAL GOALS: The goal of geriatric fellowship training is to prepare fellows for competency in the following core areas: Check and record date completed
*GERIATRIC FELLOWSHIP COMPETENCY CHECKLIST EDUCATIONAL GOALS: The goal of geriatric fellowship training is to prepare fellows for competency in the following core areas: Check and record date completed
Delirium assessment and management. Dr Kim Jeffs Northern Health
 Delirium assessment and management Dr Kim Jeffs Northern Health What do you need to know? Epidemiology How big is the problem? Who is at risk? Assessment Tools for diagnosis Prevention Evidence base Management
Delirium assessment and management Dr Kim Jeffs Northern Health What do you need to know? Epidemiology How big is the problem? Who is at risk? Assessment Tools for diagnosis Prevention Evidence base Management
Perioperative Care of Older Adults
 Perioperative Care of Older Adults SARAH A. WINGFIELD, MD AND THOMAS O. DALTON, MD UNIVERSITY OF TEXAS SOUTHWESTERN MEDICAL CENTER DIVISION OF GERIATRIC MEDICINE We have no disclosures. Objectives -Recognize
Perioperative Care of Older Adults SARAH A. WINGFIELD, MD AND THOMAS O. DALTON, MD UNIVERSITY OF TEXAS SOUTHWESTERN MEDICAL CENTER DIVISION OF GERIATRIC MEDICINE We have no disclosures. Objectives -Recognize
Perioperative Care of Older Adults
 Perioperative Care of Older Adults SARAH A. WINGFIELD, MD AND THOMAS O. DALTON, MD UNIVERSITY OF TEXAS SOUTHWESTERN MEDICAL CENTER DIVISION OF GERIATRIC MEDICINE We have no disclosures. Objectives -Recognize
Perioperative Care of Older Adults SARAH A. WINGFIELD, MD AND THOMAS O. DALTON, MD UNIVERSITY OF TEXAS SOUTHWESTERN MEDICAL CENTER DIVISION OF GERIATRIC MEDICINE We have no disclosures. Objectives -Recognize
Geriatrics and Cancer Care
 Geriatrics and Cancer Care Roger Wong, BMSc, MD, FRCPC, FACP Postgraduate Dean of Medical Education Clinical Professor, Division of Geriatric Medicine UBC Faculty of Medicine Disclosure No competing interests
Geriatrics and Cancer Care Roger Wong, BMSc, MD, FRCPC, FACP Postgraduate Dean of Medical Education Clinical Professor, Division of Geriatric Medicine UBC Faculty of Medicine Disclosure No competing interests
Early Identification and Reduction of Patient Risk: The Cedars-Sinai Frail Elders Program
 Early Identification and Reduction of Patient Risk: The Cedars-Sinai Frail Elders Program Jeff Borenstein, MD, Medical Director Applied Health Services Research Harriet Aronow, Ph.D., Research Scientist,
Early Identification and Reduction of Patient Risk: The Cedars-Sinai Frail Elders Program Jeff Borenstein, MD, Medical Director Applied Health Services Research Harriet Aronow, Ph.D., Research Scientist,
How to prevent delirium in nursing home. Dr. Sophie ALLEPAERTS Geriatric department CHU-Liège Belgium
 How to prevent delirium in nursing home Dr. Sophie ALLEPAERTS Geriatric department CHU-Liège Belgium 1 CONFLICT OF INTEREST DISCLOSURE I have no potential conflict of interest to report 2 Outline 1. Introduction
How to prevent delirium in nursing home Dr. Sophie ALLEPAERTS Geriatric department CHU-Liège Belgium 1 CONFLICT OF INTEREST DISCLOSURE I have no potential conflict of interest to report 2 Outline 1. Introduction
EMS Subspecialty Certification Review Course. Learning Objectives. Geriatric Patients and EMS Systems
 EMS Subspecialty Certification Review Course Challenges in Geriatric Patient Care 1.4.6 Geriatric Issues Version: 2017 Learning Objectives Upon the completion of this program participants will be able
EMS Subspecialty Certification Review Course Challenges in Geriatric Patient Care 1.4.6 Geriatric Issues Version: 2017 Learning Objectives Upon the completion of this program participants will be able
Frailty. Nicholas Butler MD, MBA Department of Family Medicine University of Iowa
 Frailty Nicholas Butler MD, MBA Department of Family Medicine University of Iowa Doris 84 yo female who comes into your clinic with her daughter. She complains of feeling increasingly fatigued and just
Frailty Nicholas Butler MD, MBA Department of Family Medicine University of Iowa Doris 84 yo female who comes into your clinic with her daughter. She complains of feeling increasingly fatigued and just
Geriatric Grand Rounds
 Geriatric Grand Rounds Prevalence and Risk Factors of Delirium in Older Patients Admitted to a Community Based Acute Care Hospital Tuesday, October 27, 2009 12:00 noon Dr. Bill Black Auditorium Glenrose
Geriatric Grand Rounds Prevalence and Risk Factors of Delirium in Older Patients Admitted to a Community Based Acute Care Hospital Tuesday, October 27, 2009 12:00 noon Dr. Bill Black Auditorium Glenrose
Delirium. Dr. John Puxty
 Delirium Dr. John Puxty Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors, causes and main
Delirium Dr. John Puxty Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors, causes and main
Hospital Transition Management. Barbara Wood, BSN, MBA
 Hospital Transition Management Barbara Wood, BSN, MBA Director, Embedded Care Management Programs OBJECTIVES Improve health care quality for our patients by streamlining care transitions Reduce avoidable
Hospital Transition Management Barbara Wood, BSN, MBA Director, Embedded Care Management Programs OBJECTIVES Improve health care quality for our patients by streamlining care transitions Reduce avoidable
Acute Care for Elders- Improving the Quality and Safety of Older Hospitalized Patients
 Acute Care for Elders- Improving the Quality and Safety of Older Hospitalized Patients Michael L. Malone, M.D. Aurora Health Care University of Wisconsin School of Medicine and Public Health January 14,
Acute Care for Elders- Improving the Quality and Safety of Older Hospitalized Patients Michael L. Malone, M.D. Aurora Health Care University of Wisconsin School of Medicine and Public Health January 14,
EMU A NEW MODEL OF EMERGENCY CARE FOR THE FRAIL & ELDERLY
 EMU A NEW MODEL OF EMERGENCY CARE FOR THE FRAIL & ELDERLY Geriatrics, General practice, Emergency medicine, Interface medicine SUMMARY An integrated, community emergency service specifically designed for
EMU A NEW MODEL OF EMERGENCY CARE FOR THE FRAIL & ELDERLY Geriatrics, General practice, Emergency medicine, Interface medicine SUMMARY An integrated, community emergency service specifically designed for
UND GERIATRIC MEDICINE FELLOWSHIP CURRICULUM ACUTE CARE
 LOCATION SITE Sanford Medical Center Fargo 5225 23rd Avenue S Fargo, ND 58104 CONTACT LEAD FACULTY MEMBER Dr. Darin Lang Darin.lang@sanfordhealth.org PROGRAM CONTACT Dr. Gunjan Manocha gunjan.dhawan@und.edu
LOCATION SITE Sanford Medical Center Fargo 5225 23rd Avenue S Fargo, ND 58104 CONTACT LEAD FACULTY MEMBER Dr. Darin Lang Darin.lang@sanfordhealth.org PROGRAM CONTACT Dr. Gunjan Manocha gunjan.dhawan@und.edu
Hospice and Palliative Care An Essential Component of the Aging Services Network
 Hospice and Palliative Care An Essential Component of the Aging Services Network Howard Tuch, MD, MS American Academy of Hospice and Palliative Medicine Physician Advocate, American Academy of Hospice
Hospice and Palliative Care An Essential Component of the Aging Services Network Howard Tuch, MD, MS American Academy of Hospice and Palliative Medicine Physician Advocate, American Academy of Hospice
HEALTHSTREAM LIVING LABS IN ACTION
 HEALTHSTREAM LIVING LABS IN ACTION A CONVERSATION WITH: Mitchel T. Heflin MD, MHS Associate Professor of Medicine, Duke University School of Medicine Eleanor McConnell PhD, RN, GCNS-BC Associate Professor,
HEALTHSTREAM LIVING LABS IN ACTION A CONVERSATION WITH: Mitchel T. Heflin MD, MHS Associate Professor of Medicine, Duke University School of Medicine Eleanor McConnell PhD, RN, GCNS-BC Associate Professor,
DISCLAIMER: ECHO Nevada emphasizes patient privacy and asks participants to not share ANY Protected Health Information during ECHO clinics.
 DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
Frailty in Geriatric Trauma Pa1ents
 Division of Trauma, Burn, Surgical Critical Care, & Emergency General Surgery Frailty in Geriatric Trauma Pa1ents Zara Cooper, MD, MSc, FACS Elizabeth Bryant, MPH Disclosures NIA R01AG044518 NCI R35CA197730
Division of Trauma, Burn, Surgical Critical Care, & Emergency General Surgery Frailty in Geriatric Trauma Pa1ents Zara Cooper, MD, MSc, FACS Elizabeth Bryant, MPH Disclosures NIA R01AG044518 NCI R35CA197730
Acute Care of Older Surgical Patients. Dr Shane O Hanlon Consultant Geriatrician St Vincent s University Hospital IHFM 8 th Nov 2017
 Acute Care of Older Surgical Patients Dr Shane O Hanlon Consultant Geriatrician St Vincent s University Hospital IHFM 8 th Nov 2017 NCEPOD 2010 overall care % 50 45 40 35 30 25 20 15 10 5 0 Good practice
Acute Care of Older Surgical Patients Dr Shane O Hanlon Consultant Geriatrician St Vincent s University Hospital IHFM 8 th Nov 2017 NCEPOD 2010 overall care % 50 45 40 35 30 25 20 15 10 5 0 Good practice
Rehabilitation - Reducing costs and hospital stay. Dr Elizabeth Aitken Consultant Physician
 Rehabilitation - Reducing costs and hospital stay Dr Elizabeth Aitken Consultant Physician What factors affect outcome? Comorbidities Cardiac Respiratory Neurological Nutritional issues Diabetes Anaemia
Rehabilitation - Reducing costs and hospital stay Dr Elizabeth Aitken Consultant Physician What factors affect outcome? Comorbidities Cardiac Respiratory Neurological Nutritional issues Diabetes Anaemia
What is the shared care model for the Hip fracture patient The Ortho-geriatric Model of Care at St Vincent s Public Hospital Our team and how we make
 What is the shared care model for the Hip fracture patient The Ortho-geriatric Model of Care at St Vincent s Public Hospital Our team and how we make it work! Benefits of a Shared Care Model The Shared
What is the shared care model for the Hip fracture patient The Ortho-geriatric Model of Care at St Vincent s Public Hospital Our team and how we make it work! Benefits of a Shared Care Model The Shared
Palliative Care Consultative Service in Acute Hospital - Impact & Challenges
 Palliative Care Consultative Service in Acute Hospital - Impact & Challenges Dr. Annie Kwok Consultant Palliative Care Unit Department of Medicine & Geriatrics Caritas Medical Centre Contents Aging population
Palliative Care Consultative Service in Acute Hospital - Impact & Challenges Dr. Annie Kwok Consultant Palliative Care Unit Department of Medicine & Geriatrics Caritas Medical Centre Contents Aging population
Palliative Care under a Value Based Reimbursement Model. Janet Bull MD, MBA, FAAHPM CMO Four Seasons
 Palliative Care under a Value Based Reimbursement Model Janet Bull MD, MBA, FAAHPM CMO Four Seasons Objectives o Describe palliative care o Discuss benefits of palliative care o Understand differences
Palliative Care under a Value Based Reimbursement Model Janet Bull MD, MBA, FAAHPM CMO Four Seasons Objectives o Describe palliative care o Discuss benefits of palliative care o Understand differences
How to prevent early & unplanned hospital readmission?
 How to prevent early & unplanned hospital readmission? - after subacute care K. Singler 21th September 2017 CONFLICT OF INTEREST DISCLOSURE I have no potential conflict of interest to report. K. Singler
How to prevent early & unplanned hospital readmission? - after subacute care K. Singler 21th September 2017 CONFLICT OF INTEREST DISCLOSURE I have no potential conflict of interest to report. K. Singler
FALL PREVENTION AND OLDER ADULTS BURDEN. February 2, 2016
 February 2, 2016 FALL PREVENTION AND OLDER ADULTS Each year in Winnipeg, one in three adults over 65 years of age will experience a fall. 1 Approximately one third of people 65 years of age and older and
February 2, 2016 FALL PREVENTION AND OLDER ADULTS Each year in Winnipeg, one in three adults over 65 years of age will experience a fall. 1 Approximately one third of people 65 years of age and older and
The research questions are presented in priority order, and are further elaborated with lay summaries and three-part questions where applicable.
 Top 30 Emergency Medicine Research Priorities 23 January 2017 The rankings were established by consensus at the final prioritisation workshop run by the James Lind Alliance Emergency Medicine Priority
Top 30 Emergency Medicine Research Priorities 23 January 2017 The rankings were established by consensus at the final prioritisation workshop run by the James Lind Alliance Emergency Medicine Priority
20th June Integrated Care in Sunderland: Guide to Risk Stratification
 20th June 2017 Integrated Care in Sunderland: Guide to Risk Stratification Table of Contents Integrated Care in Sunderland:... 1 Guide to Risk Stratification... 1 Table of Contents... 2 Background... 3
20th June 2017 Integrated Care in Sunderland: Guide to Risk Stratification Table of Contents Integrated Care in Sunderland:... 1 Guide to Risk Stratification... 1 Table of Contents... 2 Background... 3
Decreasing Delirium Resolution Times for the Elderly: An Interprofessional Approach
 Decreasing Delirium Resolution Times for the Elderly: An Interprofessional Approach Featuring: Felice Rogers Evans BSN RN BC Ty Breiter MSN RN CNL Tampa General Hospital NICHE exemplar hospital Three time
Decreasing Delirium Resolution Times for the Elderly: An Interprofessional Approach Featuring: Felice Rogers Evans BSN RN BC Ty Breiter MSN RN CNL Tampa General Hospital NICHE exemplar hospital Three time
Do shared care wards work?
 Do shared care wards work? Prof Rowan H. Harwood Nottingham University Hospitals NHS Trust & University of Nottingham rowan.harwood@nuh.nhs.uk This presentation is on independent research funded by the
Do shared care wards work? Prof Rowan H. Harwood Nottingham University Hospitals NHS Trust & University of Nottingham rowan.harwood@nuh.nhs.uk This presentation is on independent research funded by the
The Elusive Frailty Formula: Shining the geriatric light on the 1-5% Dr John Puxty
 The Elusive Frailty Formula: Shining the geriatric light on the 1-5% Dr John Puxty puxtyj@providencecare.ca Health Care use is not uniform by Seniors How common is Frailty? Approximately10% of all individuals
The Elusive Frailty Formula: Shining the geriatric light on the 1-5% Dr John Puxty puxtyj@providencecare.ca Health Care use is not uniform by Seniors How common is Frailty? Approximately10% of all individuals
The National Frailty Opportunity
 Ageing Well Quality Healthcare in Later Life The National Frailty Opportunity Martin Vernon National Clinical Director Older People 1 28thSeptember 2018 Ambition for frailty.. Everybody should know what
Ageing Well Quality Healthcare in Later Life The National Frailty Opportunity Martin Vernon National Clinical Director Older People 1 28thSeptember 2018 Ambition for frailty.. Everybody should know what
Death by Bedrest: The Perils of The Hospital
 Death by Bedrest: The Perils of The Hospital Mindy Fain, MD Professor of Clinical Medicine Director, Arizona Reynolds Program of Applied Geriatrics Section Head, Geriatrics & Gerontology University of
Death by Bedrest: The Perils of The Hospital Mindy Fain, MD Professor of Clinical Medicine Director, Arizona Reynolds Program of Applied Geriatrics Section Head, Geriatrics & Gerontology University of
nicheprogram.org 2016 Annual NICHE Conference Care Across the Continuum 1
 NICHE 101: Resources & Tools: The NICHE Knowledge Center Eugenia Bachaleda, MA Assistant Director, Education and Resources Deirdre M. Carolan, PhD, ANP, BC, GNP, BC Nurse Practitioner, Geriatrics, Clinical
NICHE 101: Resources & Tools: The NICHE Knowledge Center Eugenia Bachaleda, MA Assistant Director, Education and Resources Deirdre M. Carolan, PhD, ANP, BC, GNP, BC Nurse Practitioner, Geriatrics, Clinical
Hospice and Palliative Care: Value-Based Care Near the End of Life
 Hospice and Palliative Care: Value-Based Care Near the End of Life Mary Dittrich, MD, FASN Senior Medical Director, Remedy Partners Joseph W. Shega, MD National Medical Director, VITAS Healthcare 2017
Hospice and Palliative Care: Value-Based Care Near the End of Life Mary Dittrich, MD, FASN Senior Medical Director, Remedy Partners Joseph W. Shega, MD National Medical Director, VITAS Healthcare 2017
5 older patients become delirious every minute
 Management of Delirium: Nonpharmacologic and Pharmacologic Approaches Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley
Management of Delirium: Nonpharmacologic and Pharmacologic Approaches Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley
Acute front door care of frail older people. Simon Conroy Professor of Geriatric Medicine
 Acute front door care of frail older people Simon Conroy Professor of Geriatric Medicine Why is this important for physicians? Type 1 A&E attendances 11% Total Activity (Leicester) Elective admissions
Acute front door care of frail older people Simon Conroy Professor of Geriatric Medicine Why is this important for physicians? Type 1 A&E attendances 11% Total Activity (Leicester) Elective admissions
Geriatric Medicine I) OBJECTIVES
 OBJECTIVES") Geriatric Medicine I) OBJECTIVES 1 To provide a broad training and in-depth experience at a level sufficient for trainees to acquire competence and professionalism required of a specialist in Geriatric
Geriatric Medicine I) OBJECTIVES 1 To provide a broad training and in-depth experience at a level sufficient for trainees to acquire competence and professionalism required of a specialist in Geriatric
Hospice and Palliative Care: Value-Based Care Near the End of Life
 Hospice and Palliative Care: Value-Based Care Near the End of Life Mary Dittrich, MD, FASN Senior Medical Director, Remedy Partners Joseph W. Shega, MD National Medical Director, VITAS Healthcare 2017
Hospice and Palliative Care: Value-Based Care Near the End of Life Mary Dittrich, MD, FASN Senior Medical Director, Remedy Partners Joseph W. Shega, MD National Medical Director, VITAS Healthcare 2017
Why Target Delirium for Surgical Quality Improvement?
 Why Target Delirium for Surgical Quality Improvement? Tom Robinson MD FACS thomas.robinson@ucdenver.edu July 22, 2018 Disclosures Tom Robinson has no disclosures. Who Cares About the Brain? Acute Organ
Why Target Delirium for Surgical Quality Improvement? Tom Robinson MD FACS thomas.robinson@ucdenver.edu July 22, 2018 Disclosures Tom Robinson has no disclosures. Who Cares About the Brain? Acute Organ
Care of older people in surgery (COPS)
") Care of older people in surgery (COPS) Who, what, and does it make a difference Professor Jacqueline Close Geriatrician - POWH Clinical Director Falls, Balance and Injury Research Centre Early Mobilisation
Care of older people in surgery (COPS) Who, what, and does it make a difference Professor Jacqueline Close Geriatrician - POWH Clinical Director Falls, Balance and Injury Research Centre Early Mobilisation
Enhanced Perioperative Management of Older Adults
 Enhanced Perioperative Management of Older Adults Bernardo Reyes, MD Assistant Professor of Geriatrics Charles E. Schmidt College of Medicine Disclosures None Interesting Facts Warhol was a sickly child,
Enhanced Perioperative Management of Older Adults Bernardo Reyes, MD Assistant Professor of Geriatrics Charles E. Schmidt College of Medicine Disclosures None Interesting Facts Warhol was a sickly child,
End of Life Care in Dementia. Dr Rosie Lockwood Consultant Geriatrician Sheffield Teaching Hospitals
 End of Life Care in Dementia Dr Rosie Lockwood Consultant Geriatrician Sheffield Teaching Hospitals Rosie.Lockwood@sth.nhs.uk Agenda Some facts and figures What are the challenges? What is good care? How
End of Life Care in Dementia Dr Rosie Lockwood Consultant Geriatrician Sheffield Teaching Hospitals Rosie.Lockwood@sth.nhs.uk Agenda Some facts and figures What are the challenges? What is good care? How
Critically ill geriatrics. Marianne Kirrane Staff Specialist Intensive Care Royal Brisbane & Women s Hospital
 Critically ill geriatrics Marianne Kirrane Staff Specialist Intensive Care Royal Brisbane & Women s Hospital A typical conundrum at 2330 92F Nancy Alert and orientated Symptoms + signs consistent with
Critically ill geriatrics Marianne Kirrane Staff Specialist Intensive Care Royal Brisbane & Women s Hospital A typical conundrum at 2330 92F Nancy Alert and orientated Symptoms + signs consistent with
Improving Palliative Care Consultation in a Trauma ICU & Step- Down Unit Teresa Hobt-Bingham, MSN, RN, NE-BC
 Improving Palliative Care Consultation in a Trauma ICU & Step- Down Unit Teresa Hobt-Bingham, MSN, RN, NE-BC Learning Objectives Define palliative care and frailty Understand the link between frailty and
Improving Palliative Care Consultation in a Trauma ICU & Step- Down Unit Teresa Hobt-Bingham, MSN, RN, NE-BC Learning Objectives Define palliative care and frailty Understand the link between frailty and
Carolinas HealthCare System Fragility Fracture Program
 Carolinas HealthCare System Fragility Fracture Program Presented By: Monica C. Mowry, MSN, RN, NE-BC, ONC Director, Clinical Program Development Carolinas HealthCare System Charlotte, NC Objectives Expand
Carolinas HealthCare System Fragility Fracture Program Presented By: Monica C. Mowry, MSN, RN, NE-BC, ONC Director, Clinical Program Development Carolinas HealthCare System Charlotte, NC Objectives Expand
Preoperative Assessment Guidelines in the Elderly
 Preoperative Assessment Guidelines in the Elderly How Are They Helping? Mark R. Katlic, M.D., M.M.M. Chairman, Department of Surgery Director, Center for Geriatric Surgery Sinai Hospital Baltimore, Maryland
Preoperative Assessment Guidelines in the Elderly How Are They Helping? Mark R. Katlic, M.D., M.M.M. Chairman, Department of Surgery Director, Center for Geriatric Surgery Sinai Hospital Baltimore, Maryland
The Long-term Prognosis of Delirium
 The Long-term Prognosis of Jane McCusker, MD, DrPH, Professor, Epidemiology and Biostatistics, McGill University; Head, Clinical Epidemiology and Community Studies, St. Mary s Hospital, Montreal, QC. Nine
The Long-term Prognosis of Jane McCusker, MD, DrPH, Professor, Epidemiology and Biostatistics, McGill University; Head, Clinical Epidemiology and Community Studies, St. Mary s Hospital, Montreal, QC. Nine
Goals. Geriatric Trauma. What s the impact Erlanger Trauma Symposium
 Geriatric Trauma William S. Havron III MD Assistant Professor of Surgery University of Oklahoma Goals Realize the impact of injuries in the ageing population Identify the pitfalls associated with geriatric
Geriatric Trauma William S. Havron III MD Assistant Professor of Surgery University of Oklahoma Goals Realize the impact of injuries in the ageing population Identify the pitfalls associated with geriatric
National Frailty Approach
 Ageing Well Quality Healthcare in Later Life National Frailty Approach Martin Vernon National Clinical Director Older People 1 Crawley www.england.nhs.uk 10 th May 2018 Ambition for frailty.. Everybody
Ageing Well Quality Healthcare in Later Life National Frailty Approach Martin Vernon National Clinical Director Older People 1 Crawley www.england.nhs.uk 10 th May 2018 Ambition for frailty.. Everybody
Comprehensive Assessment of the Frail Older Patient
 Comprehensive Assessment of the Frail Older Patient Executive Summary Comprehensive geriatric assessment (CGA) is a multidimensional and usually interdisciplinary diagnostic process designed to determine
Comprehensive Assessment of the Frail Older Patient Executive Summary Comprehensive geriatric assessment (CGA) is a multidimensional and usually interdisciplinary diagnostic process designed to determine
Randomized Controlled Trial of a Prehospital Decision System by Emergency Medical Services to Ensure Optimal Treatment for Older Adults in Sweden
 Track 8: Clinical Geriatrics Randomized Controlled Trial of a Prehospital Decision System by Emergency Medical Services to Ensure Optimal Treatment for Older Adults in Sweden Veronica Vicente 27 oktober
Track 8: Clinical Geriatrics Randomized Controlled Trial of a Prehospital Decision System by Emergency Medical Services to Ensure Optimal Treatment for Older Adults in Sweden Veronica Vicente 27 oktober
Nutrition in the critically ill elderly (geriatric) patient CHRISTINA NIEUWOUDT RD(SA) SASPEN/CCSSA CONGRESS 2017
 patient CHRISTINA NIEUWOUDT RD(SA) SASPEN/CCSSA CONGRESS 2017") Nutrition in the critically ill elderly (geriatric) patient CHRISTINA NIEUWOUDT RD(SA) SASPEN/CCSSA CONGRESS 2017 CONTENT WHO is the critically ill elderly (geriatric) patient? WHY look at the critically
Nutrition in the critically ill elderly (geriatric) patient CHRISTINA NIEUWOUDT RD(SA) SASPEN/CCSSA CONGRESS 2017 CONTENT WHO is the critically ill elderly (geriatric) patient? WHY look at the critically
nicheprogram.org 16th Annual NICHE Conference Forging New Paths and Partnerships 1
 Improving Patient Outcomes in Geriatric Post-Operative Orthopedic Patients: Translating Research into Practice Tripping into The CAM Presented by: Diana LaBumbard, RN, MSN, ACNP/GNP-BC, CWOCN Denise Williams,
Improving Patient Outcomes in Geriatric Post-Operative Orthopedic Patients: Translating Research into Practice Tripping into The CAM Presented by: Diana LaBumbard, RN, MSN, ACNP/GNP-BC, CWOCN Denise Williams,
ASSESS & RESTORE SHARED PROVINCIAL INDICATORS AND TECHNICAL SPECIFICATIONS
 Shared Provincial s & ASSESS & RESTORE SHARED PROVINCIAL INDICATORS AND TECHNICAL SPECIFICATIONS January 2018 0 P a g e J a n u a r y 2 0 1 8 Shared Provincial s & BACKGROUND To evaluate the impact of
Shared Provincial s & ASSESS & RESTORE SHARED PROVINCIAL INDICATORS AND TECHNICAL SPECIFICATIONS January 2018 0 P a g e J a n u a r y 2 0 1 8 Shared Provincial s & BACKGROUND To evaluate the impact of
Bill J. Bryant, MD FAAFP CPPS CMD
 477 Bed Regional Hospital 32 Bed ICU 30 Transitional Care Beds Level III Trauma Center Level III NICU Largest employer west of Louisville in the Commonwealth of Kentucky Owensboro Health Bill J. Bryant,
477 Bed Regional Hospital 32 Bed ICU 30 Transitional Care Beds Level III Trauma Center Level III NICU Largest employer west of Louisville in the Commonwealth of Kentucky Owensboro Health Bill J. Bryant,
ACEing Age Old Issues in the Care of Older Canadians
 ACEing Age Old Issues in the Care of Older Canadians Dr. Samir K. Sinha MD, DPhil, FRCPC Peter and Shelagh Godsoe Chair in Geriatrics and Director of Geriatrics Sinai Health System and the University Health
ACEing Age Old Issues in the Care of Older Canadians Dr. Samir K. Sinha MD, DPhil, FRCPC Peter and Shelagh Godsoe Chair in Geriatrics and Director of Geriatrics Sinai Health System and the University Health
Putting Geriatric Emergency Nursing Education into Practice
 Putting Geriatric Emergency Nursing Education into Practice Disclosure: Marilyn Noettl, MS, RN Senior Associate, Institute for Emergency Nursing Education Meryle Lynn Chamberlain, BA, Marketing Manager
Putting Geriatric Emergency Nursing Education into Practice Disclosure: Marilyn Noettl, MS, RN Senior Associate, Institute for Emergency Nursing Education Meryle Lynn Chamberlain, BA, Marketing Manager
UNTHSC TCOM Geriatric Competencies Curriculum Mapping Document
 INSTRUCTIONS: Place a "B" (Basic), "I" (Intermediate), or "A" (Advanced) in the box next to the Geriatric Competency to indicate the Geraitaric Competency being taught, the corresponding Method of Subject
INSTRUCTIONS: Place a "B" (Basic), "I" (Intermediate), or "A" (Advanced) in the box next to the Geriatric Competency to indicate the Geraitaric Competency being taught, the corresponding Method of Subject
Delirium and dementia: The best of friends, the worst of enemies David Meagher
 Delirium and dementia: The best of friends, the worst of enemies David Meagher Professor of Psychiatry, UL Graduate-Entry Medical School Two Sumo Wrestlers Two great heavyweights Generalised Cognitive
Delirium and dementia: The best of friends, the worst of enemies David Meagher Professor of Psychiatry, UL Graduate-Entry Medical School Two Sumo Wrestlers Two great heavyweights Generalised Cognitive
Falls and Mobility. Katherine Berg, PhD, PT and Arielle Berger, MD. Presented by: Ontario s Geriatric Steering Committee
 Falls and Mobility Katherine Berg, PhD, PT and Arielle Berger, MD Key Learnings Arielle Berger, MD Key Learnings Learn approaches to falls assessment Understand inter-relationship between promoting safe
Falls and Mobility Katherine Berg, PhD, PT and Arielle Berger, MD Key Learnings Arielle Berger, MD Key Learnings Learn approaches to falls assessment Understand inter-relationship between promoting safe
Healthcare, hospitals and the challenges of an ageing population
 Healthcare, hospitals and the challenges of an ageing population Prof David Oliver Vice President, RCP, London Past President, British Geriatrics Society Senior Visiting Fellow, King s Fund Consultant
Healthcare, hospitals and the challenges of an ageing population Prof David Oliver Vice President, RCP, London Past President, British Geriatrics Society Senior Visiting Fellow, King s Fund Consultant
Delirium Pilot Project
 CCU Nurses: Delirium Pilot Project Our unit has been selected to develop and implement a delirium assessment and intervention program. We are beginning Phase 1 with education and assessing for our baseline
CCU Nurses: Delirium Pilot Project Our unit has been selected to develop and implement a delirium assessment and intervention program. We are beginning Phase 1 with education and assessing for our baseline
A END-OF-LIFE PROGRAMME LONG TERM CARE MODEL
 A EVALUATION OF A END-OF-LIFE PROGRAMME EMBEDDED WITHIN A COMMUNITY LONG TERM CARE MODEL IN SINGAPORE PILOT STUDY of COMMUNITY END-OF-LIFE CARE for older non-cancer patients 1 October 2010 30 Sept 2012
A EVALUATION OF A END-OF-LIFE PROGRAMME EMBEDDED WITHIN A COMMUNITY LONG TERM CARE MODEL IN SINGAPORE PILOT STUDY of COMMUNITY END-OF-LIFE CARE for older non-cancer patients 1 October 2010 30 Sept 2012
Sharp HealthCare Hospice and Palliative Care
 Sharp HealthCare Hospice and Palliative Care The Continuum for Advanced Illness and End Stage Disease Management (AAC) Daniel R. Hoefer, MD CMO, Outpatient Palliative Care and Hospice Suzi K. Johnson,
Sharp HealthCare Hospice and Palliative Care The Continuum for Advanced Illness and End Stage Disease Management (AAC) Daniel R. Hoefer, MD CMO, Outpatient Palliative Care and Hospice Suzi K. Johnson,
Romayne Gallagher MD, CCFP Divisions of Residential and Palliative Care Providence Health Care Vancouver, BC
 Romayne Gallagher MD, CCFP Divisions of Residential and Palliative Care Providence Health Care Vancouver, BC My father s memory may be gone but otherwise he is all there Daughter of 92 yr old in wheelchair,
Romayne Gallagher MD, CCFP Divisions of Residential and Palliative Care Providence Health Care Vancouver, BC My father s memory may be gone but otherwise he is all there Daughter of 92 yr old in wheelchair,
Recovery trajectories following critical illness: Can we really modify them? Tim Walsh Professor of Critical Care, Edinburgh University
 Recovery trajectories following critical illness: Can we really modify them? Tim Walsh Professor of Critical Care, Edinburgh University Considerations What is the problem? What is the current evidence
Recovery trajectories following critical illness: Can we really modify them? Tim Walsh Professor of Critical Care, Edinburgh University Considerations What is the problem? What is the current evidence
Post Sepsis Syndrome & Post Sepsis Care. Surviving Sepsis
 Post Sepsis Syndrome & Post Sepsis Care Jennifer Azen, MD, MPH UW Medicine Post Acute Care Service Surviving Sepsis In Hospital Mortality has declined from 35% in 2000 to 18% in 2012 Accounts for 12.2%
Post Sepsis Syndrome & Post Sepsis Care Jennifer Azen, MD, MPH UW Medicine Post Acute Care Service Surviving Sepsis In Hospital Mortality has declined from 35% in 2000 to 18% in 2012 Accounts for 12.2%
Skin Susceptible to injury; longer time Senses of the senses Respiratory system Decreased ability to exchange
 1 Geriatric Review 2 Geriatrics Geriatric patients are individuals older than years of age. In 2000, the geriatric population was almost 35 million. By 2020, the geriatric population is projected to be
1 Geriatric Review 2 Geriatrics Geriatric patients are individuals older than years of age. In 2000, the geriatric population was almost 35 million. By 2020, the geriatric population is projected to be
GRACE Team Care A New Model of Integrated Medical and Social Care for Older Persons
 GRACE Team Care A New Model of Integrated Medical and Social Care for Older Persons Steven R. Counsell, MD Mary Elizabeth Mitchell Professor and Director, Scientist, IU Center for Aging Research E-mail:
GRACE Team Care A New Model of Integrated Medical and Social Care for Older Persons Steven R. Counsell, MD Mary Elizabeth Mitchell Professor and Director, Scientist, IU Center for Aging Research E-mail:
Diagnosis and Treatment of Low Back Pain: A Joint Clinical Practice Guideline from the American College of Physicians and the American Pain Society
 Diagnosis and Treatment of Low Back Pain: A Joint Clinical Practice Guideline from the American College of Physicians and the American Pain Society Annals of Internal Medicine October 2007 Volume 147,
Diagnosis and Treatment of Low Back Pain: A Joint Clinical Practice Guideline from the American College of Physicians and the American Pain Society Annals of Internal Medicine October 2007 Volume 147,
Delirium in the hospitalized patient
 Delirium in the hospitalized patient Jennifer A. Tarin, M.D. Department of Hospital Medicine Geriatric Health Safety Chair Colorado Permanente Medical Group UCLA Reynolds Scholar Delirium Preventing delirium
Delirium in the hospitalized patient Jennifer A. Tarin, M.D. Department of Hospital Medicine Geriatric Health Safety Chair Colorado Permanente Medical Group UCLA Reynolds Scholar Delirium Preventing delirium
Understanding and Assessing for Frailty
 Understanding and Assessing for Frailty Dr Gloria Yu Clinical Head of Bexley Integrated Care Consultant Physician in Elderly, General and Stroke Medicine 8 July 2015 Learning objectives What is frailty?
Understanding and Assessing for Frailty Dr Gloria Yu Clinical Head of Bexley Integrated Care Consultant Physician in Elderly, General and Stroke Medicine 8 July 2015 Learning objectives What is frailty?
Disclosure / Conflict of Interest. None
 Disclosure / Conflict of Interest None Objectives Epidemiology and demographics of injury and emergency surgery in the elderly Anatomic and physiology changes in the context of surgical disease in the
Disclosure / Conflict of Interest None Objectives Epidemiology and demographics of injury and emergency surgery in the elderly Anatomic and physiology changes in the context of surgical disease in the
Interprofessional Care for Elders through 48/5
 Interprofessional Care for Elders through 48/5 Janet E. McElhaney, MD, FRCPC, FACP HSN Volunteer Association Chair in Geriatric Research Professor of Medicine, Northern Ontario School of Medicine Health
Interprofessional Care for Elders through 48/5 Janet E. McElhaney, MD, FRCPC, FACP HSN Volunteer Association Chair in Geriatric Research Professor of Medicine, Northern Ontario School of Medicine Health
Dementia and Primary Care. A Structured Team Approach UNE/MGEC Conference June 2014
 Dementia and Primary Care A Structured Team Approach UNE/MGEC Conference June 2014 First Proviso I have no actual or potential conflict of interest in relation to this program or presentation. Second Proviso
Dementia and Primary Care A Structured Team Approach UNE/MGEC Conference June 2014 First Proviso I have no actual or potential conflict of interest in relation to this program or presentation. Second Proviso