The last days of life in hospital and at home
|
|
|
- Amber Quinn
- 5 years ago
- Views:
Transcription

1 The last days of life in hospital and at home Beaumont Multi-disciplinary Palliative Care Study Day 28/9/2017 Dr Sarah McLean Consultant in Palliative Medicine St Francis Hospice Beaumont Hospital

2 Overview What are the priorities? Common symptoms at the end of life How to recognise the dying patient Rapid discharge pathway Community palliative care services Questions

3
4
5
6 What is important at the end of life? Strong consensus amongst seriously ill patients, bereaved family members, physicians, and other HCPs Pain and symptom management Preparation for death Achieving a sense of completion Being involved in decisions about treatment preferences / sense of control Being treated as a whole person Steinhauser et al JAMA 2000

7 Place of care rated least important of 9 attributes by patients

8 Physical care and place of care are important, but only components of overall care No one definition of a good death Quality of care at the end of life means different things to different people Collaborative MDT approach Important for good quality end of life care

9 Dying is a psychological and social phenomenon with a physical dimension, not the other way round


10 How can we achieve this for our patients? Translates into better bereavement outcomes for caregivers too. Pain and symptom management excellent symptom control Preparation for death prognosticating as best can; communication Achieving a sense of completion MSW memory work; life stories Being involved in decisions about treatment preferences / sense of control advance care planning; having conversations to determine patient s goals and wishes Being treated as a whole person person centred care
11 Physical examination Keep to a minimum to avoid unnecessary distress Sites of potential pain Mouth Investigations Only with a clear purpose Tablet burden - review of medications Discontinue non essential oral medications Including prophylactic LMWH, insulin Switch po meds to alternative route if patient is unable to swallow Avoid im route as painful; if buccal medications are used ensure the mouth is moist enough; consider the PR route

12 Advance care planning To ensure patient s wishes and goals are achieved

13 When to refer to palliative care Assess need rather than prognosis Difficult to control symptoms Psychological or social issues Dependent children or elderly vulnerable relatives Difficult ethical question e.g. feeding or hydration
14
15 Common symptoms at the end of life Dying patients tolerate symptoms very poorly due to weakness Important factors: Excellent nursing care Prevention of new symptoms e.g. pressure mattress to prevent bed sores Anticipating future symptoms or needs and putting plans in place
16 Common symptoms in the last 48 hours Noisy moist breathing - secretions Pain Breathlessness Nausea / vomiting Terminal delirium
17 Noisy, moist breathing - secretions Oro-pharyngeal secretions not being coughed or cleared normally + accumulate in the upper airway Exclude acute pulmonary oedema +/- Lasix s/c Hyoscine butylbromide Buscopan 20mgs stat PRN s/c or up to 120mgs / 24 hours s/c infusion Glycopyrronium Robinul mcg PRN s/c or up to 3200mcg / 24hrs s/c infusion Hyoscine hydrobromide crosses blood brain barrier and can exacerbate agitation

18 Pain As per the WHO ladder Via s/c infusion if unable to manage the oral route Ensure breakthrough analgesia prescribed PRN s/c
 Breathlessness Opioids Benzodiazepines Measures such as fan, cool air Oxygen if cooling sensation")
19 Nausea / vomiting Dysmotility Maxalon Chemical causes Cyclizine / Haloperidol If also agitated Levomepromazine (Nozinan) Breathlessness Opioids Benzodiazepines Measures such as fan, cool air Oxygen if cooling sensation helpful
20 Agitation Think list reversible conditions to exclude: Pain Urinary retention Constipation Nausea Cerebral irritability / oedema Anxiety Side effects of medication

21 Delirium - off the ploughed track Common Underrecognised Undertreated Prevalence of 13 42% of patients in palliative care inpatient units Rising to 88% in days and hours before death Hosie A et al Pall Med 2013
22 Medication review Opioid rotation Shown to improve hallucinations and confusion in 29 / 42 patients rotated Parenteral hydration Delirium is the only aspect of terminal symptom control which may benefit from hydration Antibiotics If infective cause is suspected Mercadante et al Cancer Treat Rev 2006 Dev R et al Curr Opin Support Palliat Care 2012
23 Management - combination of a sedating anti-psychotic with a benzodiazpine First line Haloperidol 1-5mgs / 24 hours Midazolam 10 60mgs / 24 hours Second line Levomepromazine 12.5mgs / 24 hours+ Third line Phenobarbitol mgs s/c loading dose; followed by maintenance mgs / 24 hrs s/c
24 Breitbart et al Psychosomatics 2002 Cohen et al J Palliat Care 2009 Helping families understand delirium Distressing Higher levels of distress in spouses and carers who witness the delirium than in the affected patients Evidence demonstrates that distress is lowest in caregivers who were educated about the risk of delirium before it occurred
25 How to recognise the dying patient
26 Nurses, care attendants and family members are better at predicting death than medical staff Physicians more accurate as death draws near Clinician experience may improve accuracy

27 Palliative Prognostic Scale Modified functional score
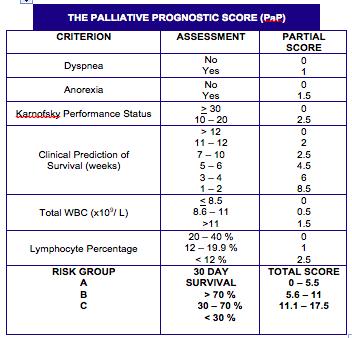
28
29 End of life Day to day deterioration of strength, appetite, and awareness Signs and symptoms of death approaching: Profound weakness / bed bound Gaunt appearance Reduced po intake / difficulty swallowing medication Drowsiness / reduced cognition / difficulty concentrating
30 If end of life care at home is being planned

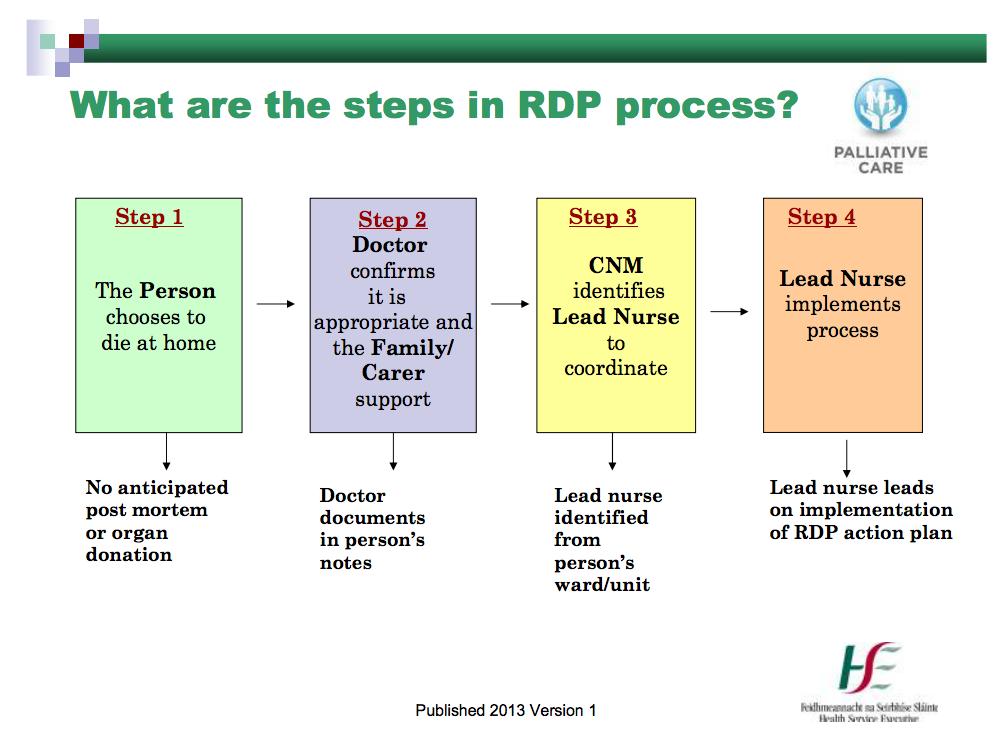
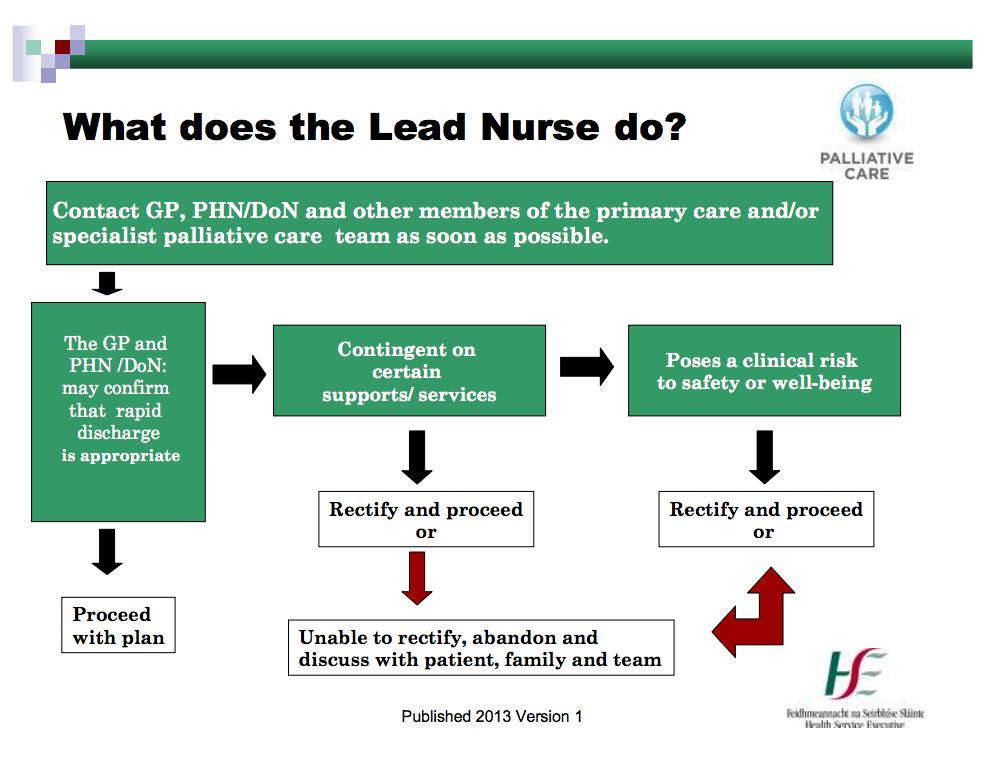
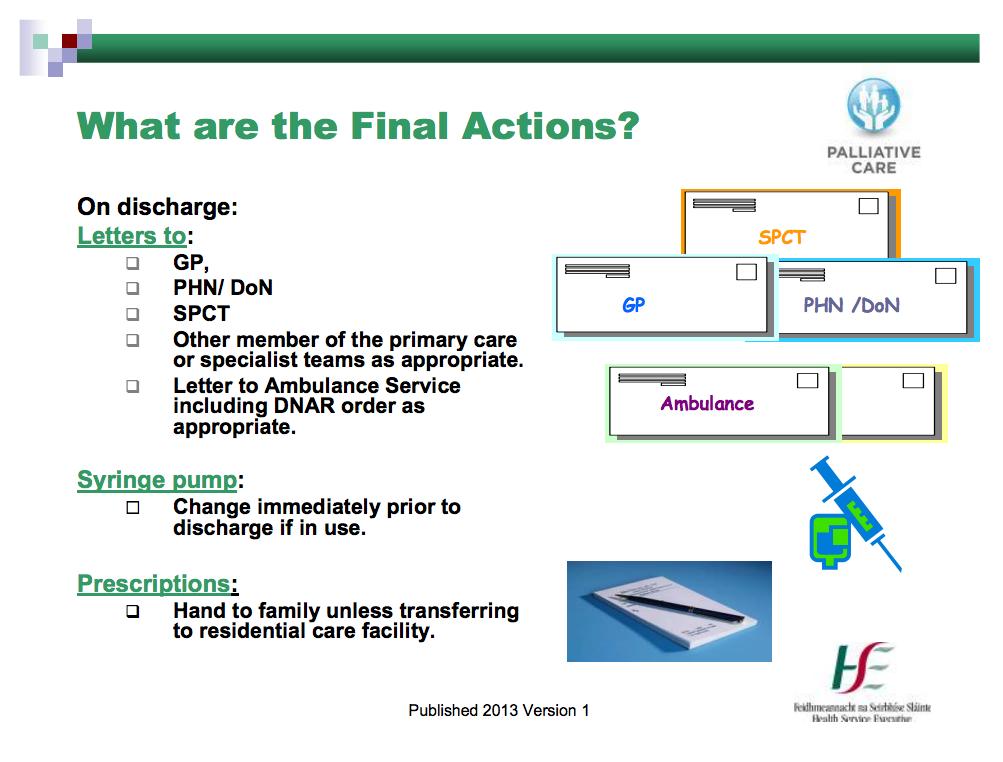
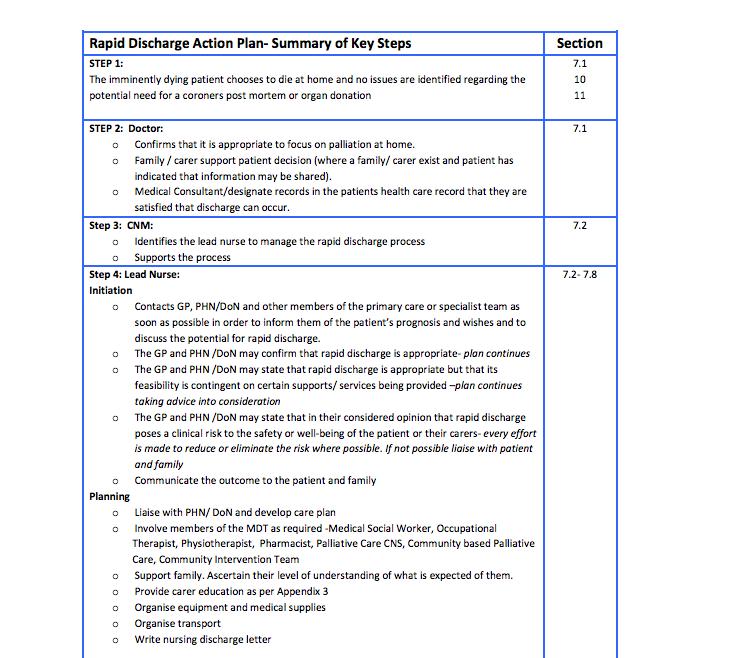
31 Rapid discharge pathway
32
33
34
35
36
37
38

39
40
41
42
43
44 Supports for end of life care at home

45 Community palliative care (CPC) Deluxe dying for the privileged few Increasing recognition of benefit of palliative care input aging population, diagnoses other than cancer, underserved populations 90% of care in the last year of life happens in the home Increasing importance of supporting generalist palliative care provision Douglas, 1991

46 St Francis Hospice Inpatient units 17 beds Raheny 24 beds Blanchardstown

47 Community palliative care patients between east and west teams > 1100 deaths / year Medical social work/ chaplaincy Bereavement services Carer support group Drop in carer support Hospice Day Care Complementary therapy Lymphoedema / MLD Outpatients CT, physiotherapy, nursing Breathlessness / Heart Failure programmes EXHALE Volunteer services Life stories Volunteer bereavement support service

48 Public health nurse Home care package Community Intervention Teams GP Community OT, PT, MSW Irish Cancer Society night nursing service

49 Education and Research Short courses and e- learning Library Kaleidoscope conference TCD / SFH MSc in Palliative Care Community and schools outreach

50 Questions?
Care in the Last Days of Life
 Care in the Last Days of Life Introduction This guideline is an aid to clinical decision making and good practice in person-centred care for patients who are deteriorating and at risk of dying. The patient
Care in the Last Days of Life Introduction This guideline is an aid to clinical decision making and good practice in person-centred care for patients who are deteriorating and at risk of dying. The patient
Renal Palliative Care Last Days of Life
 Renal Palliative Care Last Days of Life Introduction This guideline is an aid to clinical decision-making and good practice for patients with stage 4-5 chronic kidney disease (egfr
Renal Palliative Care Last Days of Life Introduction This guideline is an aid to clinical decision-making and good practice for patients with stage 4-5 chronic kidney disease (egfr
Supporting Last Days of Life Symptom Control Medication Guidance: Algorithm. Agitation & Anxiety
 Agitation & Anxiety (Exclude or treat REVERSIBLE causes*) Patient is anxious / frightened, but lucid Patient is confused, agitated and / or hallucinating MIDAZOLAM 2.5-5mg s/c (Max total 24 hour dose of
Agitation & Anxiety (Exclude or treat REVERSIBLE causes*) Patient is anxious / frightened, but lucid Patient is confused, agitated and / or hallucinating MIDAZOLAM 2.5-5mg s/c (Max total 24 hour dose of
MMG035 Symptom Management Guidelines for a Person thought to be in the Last Few Days and Hours of Life
 MMG035 Symptom Management Guidelines for a Person thought to be in the Last Few Days and Hours of Life The following pages are guidelines for the management of common symptoms for a person thought to be
MMG035 Symptom Management Guidelines for a Person thought to be in the Last Few Days and Hours of Life The following pages are guidelines for the management of common symptoms for a person thought to be
PAIN MANAGEMENT Patient established on oral morphine or opioid naive.
 PAIN MANAGEMENT Patient established on oral morphine or opioid naive. Important; It is the responsibility of the prescriber to ensure that guidelines are followed when prescribing opioids. Every member
PAIN MANAGEMENT Patient established on oral morphine or opioid naive. Important; It is the responsibility of the prescriber to ensure that guidelines are followed when prescribing opioids. Every member
Supportive Care. End of Life Phase
 Supportive Care End of Life Phase Guidelines for Health Care Professionals In the care of patients with established renal failure who are in the last days of life References: Chambers E J (2004) End of
Supportive Care End of Life Phase Guidelines for Health Care Professionals In the care of patients with established renal failure who are in the last days of life References: Chambers E J (2004) End of
PAIN MANAGEMENT Person established taking oral morphine or opioid naive.
 PAIN MANAGEMENT Person established taking oral morphine or opioid naive. Important; it is the responsibility of the prescriber to ensure that guidelines are followed when prescribing opioids. Every member
PAIN MANAGEMENT Person established taking oral morphine or opioid naive. Important; it is the responsibility of the prescriber to ensure that guidelines are followed when prescribing opioids. Every member
Renal Prescribing at End of Life Guidance for Anticipatory prescribing for patients in renal failure (egfr<30) at the end of life
 at the end of life") Guidance for Anticipatory prescribing for patients in renal failure (egfr
Guidance for Anticipatory prescribing for patients in renal failure (egfr
Symptom Management Guidelines for End of Life Care
 Symptom Management Guidelines for End of Life Care The following pages are guidelines for the management of common symptoms in the last few days of life. General principles: 1. Consider how symptoms can
Symptom Management Guidelines for End of Life Care The following pages are guidelines for the management of common symptoms in the last few days of life. General principles: 1. Consider how symptoms can
GUIDELINES FOR PRESCRIBING AT THE END OF LIFE FOR PATIENTS WITH RENAL IMPAIRMENT (estimated glomerular filtration rate<30)
") GUIDELINES FOR PRESCRIBING AT THE END OF LIFE FOR PATIENTS WITH RENAL IMPAIRMENT These guidelines have been produced in collaboration with Dr Lucy Smyth, Consultant in Renal Medicine, Royal Devon and Exeter
GUIDELINES FOR PRESCRIBING AT THE END OF LIFE FOR PATIENTS WITH RENAL IMPAIRMENT These guidelines have been produced in collaboration with Dr Lucy Smyth, Consultant in Renal Medicine, Royal Devon and Exeter
Waterloo Wellington (WW) Symptom Management Guideline for the End of Life (EOL) Medication Order Set for Long Term Care (LTC)
 Symptom Management Guideline for the End of Life (EOL) Medication Order Set for Long Term Care (LTC)") Waterloo Wellington (WW) Symptom Management Guideline for the End of Life (EOL) Medication Order Set for Long Term Care (LTC) May 2018 THE WATERLOO WELLINGTON SYMPTOM MANAGEMENT GUIDELINE FOR THE END OF
Waterloo Wellington (WW) Symptom Management Guideline for the End of Life (EOL) Medication Order Set for Long Term Care (LTC) May 2018 THE WATERLOO WELLINGTON SYMPTOM MANAGEMENT GUIDELINE FOR THE END OF
Palliative care for heart failure patients. Susan Addie
 Palliative care for heart failure patients Susan Addie Treatments The most common limiting and distressing complaint is of fatigue and breathlessness. Optimal treatment strategies relieve symptoms, improves
Palliative care for heart failure patients Susan Addie Treatments The most common limiting and distressing complaint is of fatigue and breathlessness. Optimal treatment strategies relieve symptoms, improves
PRESCRIBING GUIDELINES FOR SYMPTOM MANAGEMENT IN THE DYING PATIENT
 PRESCRIBING GUIDELINES FOR SYMPTOM MANAGEMENT IN THE DYING PATIENT A collaboration between: St. Rocco s Hospice, Bridgewater Community Healthcare NHS Trust, NHS Warrington Clinical Commissioning Group,
PRESCRIBING GUIDELINES FOR SYMPTOM MANAGEMENT IN THE DYING PATIENT A collaboration between: St. Rocco s Hospice, Bridgewater Community Healthcare NHS Trust, NHS Warrington Clinical Commissioning Group,
Implementing the recommendation on medication management and symptom control
 Implementing the recommendation on medication management and symptom control Mike Grocott Professor of Anaesthesia and Critical Care Medicine University of Southampton Consultant in Critical Care Medicine
Implementing the recommendation on medication management and symptom control Mike Grocott Professor of Anaesthesia and Critical Care Medicine University of Southampton Consultant in Critical Care Medicine
Syringe driver in Palliative Care
 Syringe driver in Palliative Care Introduction: Syringe drivers are portable, battery operated devices widely used in palliative care to deliver medication as a continuous subcutaneous infusion over 24
Syringe driver in Palliative Care Introduction: Syringe drivers are portable, battery operated devices widely used in palliative care to deliver medication as a continuous subcutaneous infusion over 24
CLINICAL GUIDELINES FOR END OF LIFE CARE MEDICATIONS IN LONG TERM CARE HOMES
 CLINICAL GUIDELINES F END OF LIFE CARE MEDICATIONS IN LONG TERM CARE HOMES OPENING STATEMENT: Insert Facility Name is committed to providing effective end-of-life symptom management to all residents. Symptom
CLINICAL GUIDELINES F END OF LIFE CARE MEDICATIONS IN LONG TERM CARE HOMES OPENING STATEMENT: Insert Facility Name is committed to providing effective end-of-life symptom management to all residents. Symptom
End of life prescribing guidance
 End of life prescribing guidance Introduction This guidance has been prepared to ASSIST IN DECISION MAKING for the prescribing and monitoring of medicines useful in the management of symptoms commonly
End of life prescribing guidance Introduction This guidance has been prepared to ASSIST IN DECISION MAKING for the prescribing and monitoring of medicines useful in the management of symptoms commonly
Managing Respiratory Symptoms - Breathlessness, Cough and Secretions. Dr Laura Healy. Palliative Medicine Registrar, Beaumont Hospital.
 Managing Respiratory Symptoms - Breathlessness, Cough and Secretions. Dr Laura Healy. Palliative Medicine Registrar, Beaumont Hospital. Things to consider: 1. Very common symptoms. 2. Can occur in any
Managing Respiratory Symptoms - Breathlessness, Cough and Secretions. Dr Laura Healy. Palliative Medicine Registrar, Beaumont Hospital. Things to consider: 1. Very common symptoms. 2. Can occur in any
Approach to symptom control near the end-of-life
 Approach to symptom control near the end-of-life 18 Sept 2011 Dr Alethea Yee Senior Consultant, Department of Palliative Medicine National Cancer Centre,Singapore What is end of life? No precise definition
Approach to symptom control near the end-of-life 18 Sept 2011 Dr Alethea Yee Senior Consultant, Department of Palliative Medicine National Cancer Centre,Singapore What is end of life? No precise definition
For patients and their carers this means smoother symptom control, better support in a crisis, and avoidance of admission if that is their choice.
 Bedfordshire Palliative Care Palliative Care Medicines Guidance This folder has been produced to support professionals providing palliative care in any setting. Its aim is to make best practice in palliative
Bedfordshire Palliative Care Palliative Care Medicines Guidance This folder has been produced to support professionals providing palliative care in any setting. Its aim is to make best practice in palliative
Care of the Dying Management in Severe Renal Failure
 Care of the Dying Management in Severe Renal Failure Clinical Guideline Early recognition of the dying process allows for adequate preparation of the patient, the family and the carers. This clinical guidance
Care of the Dying Management in Severe Renal Failure Clinical Guideline Early recognition of the dying process allows for adequate preparation of the patient, the family and the carers. This clinical guidance
PAIN AND SYMPTOM MANAGEMENT GUIDANCE IN THE LAST DAYS OF LIFE
 PAIN AND SYMPTOM MANAGEMENT GUIDANCE IN THE LAST DAYS OF LIFE Reference: DCM029 Version: 1.1 This version issued: 07/06/18 Result of last review: Minor changes Date approved by owner (if applicable): N/A
PAIN AND SYMPTOM MANAGEMENT GUIDANCE IN THE LAST DAYS OF LIFE Reference: DCM029 Version: 1.1 This version issued: 07/06/18 Result of last review: Minor changes Date approved by owner (if applicable): N/A
Care of the Dying. For dosing in severe renal impairment see separate guidance for care of the dying in severe renal failure.
 Care of the Dying Early diagnosis of the dying process allows for adequate preparation of the patient, the family and the carers. This clinical guidance covers the prescribing and management of patients
Care of the Dying Early diagnosis of the dying process allows for adequate preparation of the patient, the family and the carers. This clinical guidance covers the prescribing and management of patients
Guidelines: EOLC Symptom Control for Patients with Normal Renal Function (in Wandsworth)
") Guidelines: EOLC Symptom Control for Patients with Normal Renal Function (in Wandsworth) Policy Number : DC020 Issue Date: October 2014 Review date: October 2016 Policy Owner: Head Community Services Monitor:
Guidelines: EOLC Symptom Control for Patients with Normal Renal Function (in Wandsworth) Policy Number : DC020 Issue Date: October 2014 Review date: October 2016 Policy Owner: Head Community Services Monitor:
Palliative care in long-term conditions Scottish Palliative Care Pharmacists Association
 Palliative care in long-term conditions 2011 2012 Scottish Palliative Care Pharmacists Association Aims & Objectives To explore symptoms, general management principles and appropriate palliative treatment
Palliative care in long-term conditions 2011 2012 Scottish Palliative Care Pharmacists Association Aims & Objectives To explore symptoms, general management principles and appropriate palliative treatment
SYMPTOM MANAGEMENT GUIDANCE FOR PATIENTS RECEIVING PALLIATIVE CARE AT ROYAL DERBY HOSPITAL
 SYMPTOM MANAGEMENT GUIDANCE FOR PATIENTS RECEIVING PALLIATIVE CARE AT ROYAL DERBY HOSPITAL If a patient is believed to be approaching the end of their life, medication should be prescribed in anticipation
SYMPTOM MANAGEMENT GUIDANCE FOR PATIENTS RECEIVING PALLIATIVE CARE AT ROYAL DERBY HOSPITAL If a patient is believed to be approaching the end of their life, medication should be prescribed in anticipation
 The last days of life Linda Magann CNC Palliative Care St George Hospital I m not afraid of dying, I just don t want to be there when it happens Woody Allen Palliative Care is an approach that improves
The last days of life Linda Magann CNC Palliative Care St George Hospital I m not afraid of dying, I just don t want to be there when it happens Woody Allen Palliative Care is an approach that improves
Care of the Dying Management in Severe Renal Failure
 Care of the Dying Management in Severe Renal Failure Clinical Guideline Early diagnosis of the dying process allows for adequate preparation of the patient, the family and the carers. This clinical guidance
Care of the Dying Management in Severe Renal Failure Clinical Guideline Early diagnosis of the dying process allows for adequate preparation of the patient, the family and the carers. This clinical guidance
Palliative Care Impact Survey
 September 2018 Contents Introduction...3 Headlines...3 Approach...4 Findings...4 Which guideline are used...4 How and where the guidelines are used...6 Alternative sources of information...7 Use of the
September 2018 Contents Introduction...3 Headlines...3 Approach...4 Findings...4 Which guideline are used...4 How and where the guidelines are used...6 Alternative sources of information...7 Use of the
Palliative care for patients with brain cancer
 Palliative care for patients with brain cancer Lyn Cave Clinical Nurse Specialist Palliative Care Hospital2Home (H2H) Dr Jayne Wood Clinical Lead Palliative Care The Royal Marsden and Royal Brompton Palliative
Palliative care for patients with brain cancer Lyn Cave Clinical Nurse Specialist Palliative Care Hospital2Home (H2H) Dr Jayne Wood Clinical Lead Palliative Care The Royal Marsden and Royal Brompton Palliative
SYMPTOM CONTROL IN THE LAST DAYS OF LIFE. Bradford, Airedale, Wharfedale & Craven
 Bradford, Airedale, Wharfedale & Craven Managed Clinical Network SYMPTOM CONTROL IN THE LAST DAYS OF LIFE Guidelines for Healthcare Professionals Bradford, Airedale, Wharfedale & Craven Signs and symptoms
Bradford, Airedale, Wharfedale & Craven Managed Clinical Network SYMPTOM CONTROL IN THE LAST DAYS OF LIFE Guidelines for Healthcare Professionals Bradford, Airedale, Wharfedale & Craven Signs and symptoms
Training in palliative and end-of-life care: Guidance for trainees (and their trainers) in non-palliative medicine training posts
 in non-palliative medicine training posts") Training in palliative and end-of-life care: Guidance for trainees (and their trainers) in non-palliative medicine training posts August 204 Produced by Dr Fiona Hicks onsultant in Palliative Medicine
Training in palliative and end-of-life care: Guidance for trainees (and their trainers) in non-palliative medicine training posts August 204 Produced by Dr Fiona Hicks onsultant in Palliative Medicine
CARE OF THE DYING PATIENT WITH ESKD ELIZABETH JOSLAND - RSC CNC
 CARE OF THE DYING PATIENT WITH ESKD ELIZABETH JOSLAND - RSC CNC OBJECTIVES UNDERSTANDING OF: POTENTIAL COMPLEXITIES OF ESKD PATIENTS IMPORTANCE OF COMMUNICATION CONSIDERATIONS AT END-OF-LIFE END-OF-LIFE
CARE OF THE DYING PATIENT WITH ESKD ELIZABETH JOSLAND - RSC CNC OBJECTIVES UNDERSTANDING OF: POTENTIAL COMPLEXITIES OF ESKD PATIENTS IMPORTANCE OF COMMUNICATION CONSIDERATIONS AT END-OF-LIFE END-OF-LIFE
MND Just in Case kit Information for GPs
 MND Just in Case kit Information for GPs What is the MND Just in Case kit? 2 Motor neurone disease (MND) is a progressive and terminal disease that results in degeneration of the motor neurones in the
MND Just in Case kit Information for GPs What is the MND Just in Case kit? 2 Motor neurone disease (MND) is a progressive and terminal disease that results in degeneration of the motor neurones in the
[Type text] Anticipatory Medication STAT dose and Syringe Driver Guidance [Type text]
![[Type text] Anticipatory Medication STAT dose and Syringe Driver Guidance [Type text]](/thumbs/92/110296570.jpg "[Type text] Anticipatory Medication STAT dose and Syringe Driver Guidance [Type text]") [Type text] Anticipatory Medication STAT dose and Syringe Driver Guidance [Type text] Patients with egfr greater than 30mL/min Patients with egfr less than 30mL/min Symptom Drug Dose Symptom Drug Dose
[Type text] Anticipatory Medication STAT dose and Syringe Driver Guidance [Type text] Patients with egfr greater than 30mL/min Patients with egfr less than 30mL/min Symptom Drug Dose Symptom Drug Dose
Care of dying adults in the last days of life. Improving care at the very end of life.
 Care of dying adults in the last days of life Improving care at the very end of life. Foreword We will all experience death, whether it is our own or that of a loved one. The bereaved person s perception
Care of dying adults in the last days of life Improving care at the very end of life. Foreword We will all experience death, whether it is our own or that of a loved one. The bereaved person s perception
Clatterbridge Centre for Oncology
 Clatterbridge Centre for Oncology CONTENTS 1. Why and when to use a syringe driver 2. Siting the syringe driver 3. Mixing and measuring 4. Setting up the syringe driver 5. Drug information 6. Common problems
Clatterbridge Centre for Oncology CONTENTS 1. Why and when to use a syringe driver 2. Siting the syringe driver 3. Mixing and measuring 4. Setting up the syringe driver 5. Drug information 6. Common problems
End of Life Care in Dementia. Sue Atkins Dignity in Care/Dementia/Learning Disabilities Clinical Nurse Specialist
 End of Life Care in Dementia Sue Atkins Dignity in Care/Dementia/Learning Disabilities Clinical Nurse Specialist Objectives Understanding the decline in people with dementia To recognise when patients
End of Life Care in Dementia Sue Atkins Dignity in Care/Dementia/Learning Disabilities Clinical Nurse Specialist Objectives Understanding the decline in people with dementia To recognise when patients
EAST LANCASHIRE GUIDELINES FOR THE MANAGEMENT OF SYMPTOMS IN THE LAST DAYS OF LIFE
 EAST LANCASHIRE SPECIALIST PALLIATIVE CARE TEAM EAST LANCASHIRE GUIDELINES FOR THE MANAGEMENT OF SYMPTOMS IN THE LAST DAYS OF LIFE Reviewed and updated August 2009 Next review date August 2011 Approved
EAST LANCASHIRE SPECIALIST PALLIATIVE CARE TEAM EAST LANCASHIRE GUIDELINES FOR THE MANAGEMENT OF SYMPTOMS IN THE LAST DAYS OF LIFE Reviewed and updated August 2009 Next review date August 2011 Approved
PENNINE LANCASHIRE GUIDELINES FOR THE MANAGEMENT OF SYMPTOMS IN THE LAST DAYS OF LIFE
 PENNINE LANCASHIRE GUIDELINES FOR THE MANAGEMENT OF SYMPTOMS IN THE LAST DAYS OF LIFE Originally produced: July 2006 First Review: August 2009 Second Review: November 2011 For review November 2013 Approved
PENNINE LANCASHIRE GUIDELINES FOR THE MANAGEMENT OF SYMPTOMS IN THE LAST DAYS OF LIFE Originally produced: July 2006 First Review: August 2009 Second Review: November 2011 For review November 2013 Approved
End Stage Liver Disease Regional Audit Casenote Survey
 1. This questionnaire is an audit of clinical documentation of patients who have died of end stage liver disease. If you have any questions about how this form should be completed please contact Dr Grace
1. This questionnaire is an audit of clinical documentation of patients who have died of end stage liver disease. If you have any questions about how this form should be completed please contact Dr Grace
Conservative Management of Uraemia
 Conservative Management of Uraemia Information for Health Professionals Renal Department The York Hospital and Scarborough Hospital Tel: 01904 725370 For more information, please contact: The Renal Specialist
Conservative Management of Uraemia Information for Health Professionals Renal Department The York Hospital and Scarborough Hospital Tel: 01904 725370 For more information, please contact: The Renal Specialist
ANTICIPATORY PRESCRIBING FOR PATIENTS AT END OF LIFE WITH RENAL IMPAIRMENT
 ANTICIPATORY PRESCRIBING FOR PATIENTS AT END OF LIFE WITH RENAL Doses of opiates must be proptional to current analgesic medication Please refer ALL patients on Methadone Ketamine to SPCT f advice. Patients
ANTICIPATORY PRESCRIBING FOR PATIENTS AT END OF LIFE WITH RENAL Doses of opiates must be proptional to current analgesic medication Please refer ALL patients on Methadone Ketamine to SPCT f advice. Patients
Algorithms for Symptom Management. In End of Life Care
 Algorithms for Symptom Management In End of Life Care The Use of Drugs Beyond Licence (off label) -The Medicines and Healthcare Products Regulatory Agency (MHRA) in the UK regulates the activity of the
Algorithms for Symptom Management In End of Life Care The Use of Drugs Beyond Licence (off label) -The Medicines and Healthcare Products Regulatory Agency (MHRA) in the UK regulates the activity of the
survey Parenteral anti-epileptics What is your experience? May July 2015
 Parenteral anti-epileptics What is your experience? May July 2015 Number of responses = 99 1a) In patients with pre-existing epilepsy controlled by PO medication that are imminently dying (prognosis
Parenteral anti-epileptics What is your experience? May July 2015 Number of responses = 99 1a) In patients with pre-existing epilepsy controlled by PO medication that are imminently dying (prognosis
Delirium. Assessment and Management
 Delirium Assessment and Management Goals and Objectives Participants will: 1. be able to recognize and diagnose the syndrome of delirium. 2. understand the causes of delirium. 3. become knowledgeable about
Delirium Assessment and Management Goals and Objectives Participants will: 1. be able to recognize and diagnose the syndrome of delirium. 2. understand the causes of delirium. 3. become knowledgeable about
INTEGRATED CARE PATHWAY (ICP) FOR THE DYING ADULT
 FOR THE DYING ADULT") INTEGRATED CARE PATHWAY (ICP) FOR THE DYING ADULT PLEASE INFORM THE PALLIATIVE CARE TEAM ON COMMENCEMENT OF THIS ICP (EXT 8958) ICP Start Date Patient s Name. Ward. Consultant.. Named Specialist Nurse
INTEGRATED CARE PATHWAY (ICP) FOR THE DYING ADULT PLEASE INFORM THE PALLIATIVE CARE TEAM ON COMMENCEMENT OF THIS ICP (EXT 8958) ICP Start Date Patient s Name. Ward. Consultant.. Named Specialist Nurse
Care of the dying in End Stage Kidney Disease (ESKD) - Conservative. Elizabeth Josland Renal Supportive Care CNC St George Hospital
 - Conservative. Elizabeth Josland Renal Supportive Care CNC St George Hospital") Care of the dying in End Stage Kidney Disease (ESKD) - Conservative Elizabeth Josland Renal Supportive Care CNC St George Hospital Introduction What does conservative management look like? How does the
Care of the dying in End Stage Kidney Disease (ESKD) - Conservative Elizabeth Josland Renal Supportive Care CNC St George Hospital Introduction What does conservative management look like? How does the
Ventilation/End of Life Neuromuscular Disorders. Dr Emma Husbands Consultant Palliative Medicine
 Ventilation/End of Life Neuromuscular Disorders Dr Emma Husbands Consultant Palliative Medicine Emma.Husbands@glos.nhs.uk Contents Cases NIV and palliation and ethical bits APM guidelines Important bits
Ventilation/End of Life Neuromuscular Disorders Dr Emma Husbands Consultant Palliative Medicine Emma.Husbands@glos.nhs.uk Contents Cases NIV and palliation and ethical bits APM guidelines Important bits
1. GUIDELINES FOR THE MANAGEMENT OF AGITATION IN ADVANCED CANCER
 1. GUIDELINES FOR THE MANAGEMENT OF AGITATION IN ADVANCED CANCER 1.1 GENERAL PRINCIPLES There are many causes of agitation in palliative care patients, which makes recommendations for treatment difficult.
1. GUIDELINES FOR THE MANAGEMENT OF AGITATION IN ADVANCED CANCER 1.1 GENERAL PRINCIPLES There are many causes of agitation in palliative care patients, which makes recommendations for treatment difficult.
Regional Renal Training
 Regional Renal Training Palliative and End of Life Care Dr Clare Kendall North Bristol NHS Trust Advanced Kidney Disease Dialysis/Transplant Conservative Management Deteriorating despite dialysis/failing
Regional Renal Training Palliative and End of Life Care Dr Clare Kendall North Bristol NHS Trust Advanced Kidney Disease Dialysis/Transplant Conservative Management Deteriorating despite dialysis/failing
GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS
 GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS Bristol Palliative Care Collaborative Contact Numbers: Hospital Specialist Palliative Care Teams: North Bristol 0117 4146392 UH Bristol 0117
GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS Bristol Palliative Care Collaborative Contact Numbers: Hospital Specialist Palliative Care Teams: North Bristol 0117 4146392 UH Bristol 0117
SYRINGE DRIVER MEDICATIONS
 SYRINGE DRIVER MEDICATIONS Christine Hull & Anita Webb Staff Nurses, Hospice in the Home 2015 Analgesics:- Groups of Medication used in Syringe Drivers Morphine sulphate Diamorphine Oxycodone Alfentanil
SYRINGE DRIVER MEDICATIONS Christine Hull & Anita Webb Staff Nurses, Hospice in the Home 2015 Analgesics:- Groups of Medication used in Syringe Drivers Morphine sulphate Diamorphine Oxycodone Alfentanil
Anticipatory prescribing and end of life considerations. Dr Stephanie Lippett
 Anticipatory prescribing and end of life considerations Dr Stephanie Lippett contents Pain Restlessness/agitation Nausea/vomiting Secretions Syringe driver Anticipatory prescribing Important things to
Anticipatory prescribing and end of life considerations Dr Stephanie Lippett contents Pain Restlessness/agitation Nausea/vomiting Secretions Syringe driver Anticipatory prescribing Important things to
Anticipatory Medications for End of Life Patients. Doses must be proportional to the current analgesic medication YES NO YES NO
 Anticipatory Medications for End of Life Patients oses must be proportional to the current analgesic medication Please refer ALL patients on Methadone or Ketamine to palliative care team for advice. Patients
Anticipatory Medications for End of Life Patients oses must be proportional to the current analgesic medication Please refer ALL patients on Methadone or Ketamine to palliative care team for advice. Patients
Palliative Care. Anticipatory Prescribing Guidelines & June Gippsland Region Palliative Care Consortium Clinical Practice Group
 Palliative Care Anticipatory Prescribing Guidelines June 2016 Gippsland Region Palliative Care Consortium Clinical Practice Group Policy No. Title Keywords Ratified GRPCC-CPG008_1.1_2016 Anticipatory Prescribing
Palliative Care Anticipatory Prescribing Guidelines June 2016 Gippsland Region Palliative Care Consortium Clinical Practice Group Policy No. Title Keywords Ratified GRPCC-CPG008_1.1_2016 Anticipatory Prescribing
Palliative Care Out-of-hours. A resource pack for West Dorset. Contents:
 Palliative Care Out-of-hours. A resource pack for West Dorset Contents: Section 1 Supply of drugs DCH Pharmacy hours and arrangements How to contact a community pharmacist out of hours Palliative care
Palliative Care Out-of-hours. A resource pack for West Dorset Contents: Section 1 Supply of drugs DCH Pharmacy hours and arrangements How to contact a community pharmacist out of hours Palliative care
Breathlessness in advanced disease. February 2017
 Breathlessness in advanced disease February 2017 Breathlessness Managing breathlessness in primary care Chronic breathlessness Acute exacerbation of breathlessness Breathlessness at end of life Breathlessness
Breathlessness in advanced disease February 2017 Breathlessness Managing breathlessness in primary care Chronic breathlessness Acute exacerbation of breathlessness Breathlessness at end of life Breathlessness
We would like to thank you for completing this audit questionnaire which looks at how you manage nausea and vomiting in palliative care patients.
 We would like to thank you for completing this audit questionnaire which looks at how you manage nausea and vomiting in palliative care patients. The closing date for responses is 19th December The results
We would like to thank you for completing this audit questionnaire which looks at how you manage nausea and vomiting in palliative care patients. The closing date for responses is 19th December The results
Target audience: The target audience for this guidance are: GPs Care home managers and nurses, District nurses, and Specialist Palliative Care teams.
 Anticipatory medication guidance for the last days of life for frail older people being care for in care homes who do not have Specialist Palliative Care needs Purpose of guidance: The purpose of this
Anticipatory medication guidance for the last days of life for frail older people being care for in care homes who do not have Specialist Palliative Care needs Purpose of guidance: The purpose of this
Incidence and aetiology:
 A pilot randomised cross-over double blinded controlled efficacy study of Octreotide versus hyoscine hydrobromide in controlling respiratory secretions at the end of life Katherine Clark, David Currow,
A pilot randomised cross-over double blinded controlled efficacy study of Octreotide versus hyoscine hydrobromide in controlling respiratory secretions at the end of life Katherine Clark, David Currow,
This survey aims to look at individual practice and can be completed by any healthcare professional.
 This survey aims to look at individual practice and can be completed by any healthcare professional. If you have any questions about how this form should be completed please contact Dr Grace Ting (ghlting@doctors.net.uk)
This survey aims to look at individual practice and can be completed by any healthcare professional. If you have any questions about how this form should be completed please contact Dr Grace Ting (ghlting@doctors.net.uk)
Dyspnea: The top things you need to you know! Dr. Megan Sellick & Dr. Lawrence Lee Edmonton Zone Palliative Care Program
 : The top things you need to you know! Dr. Megan Sellick & Dr. Lawrence Lee Edmonton Zone Palliative Care Program Faculty / Presenter Disclosure Faculty: Dr. Lawrence Lee Relationships with commercial
: The top things you need to you know! Dr. Megan Sellick & Dr. Lawrence Lee Edmonton Zone Palliative Care Program Faculty / Presenter Disclosure Faculty: Dr. Lawrence Lee Relationships with commercial
BREATHLESSNESS MANAGEMENT
 Guideline Name: Breathlessness BACKGROUND Breathlessness is a common symptom in patients with cancer, end-stage heart failure and end-stage chronic obstructive pulmonary disease (COPD). There are many
Guideline Name: Breathlessness BACKGROUND Breathlessness is a common symptom in patients with cancer, end-stage heart failure and end-stage chronic obstructive pulmonary disease (COPD). There are many
Symptom Control in the Community Setting. Dr Andrew Tysoe-Calnon
 Symptom Control in the Community Setting Dr Andrew Tysoe-Calnon Lead Consultant t Common symptoms Pain Agitation Shortness of breath Nausea and vomiting Intestinal obstruction Confusion Pain Occurs in
Symptom Control in the Community Setting Dr Andrew Tysoe-Calnon Lead Consultant t Common symptoms Pain Agitation Shortness of breath Nausea and vomiting Intestinal obstruction Confusion Pain Occurs in
National Cancer Action Team. Rehabilitation Care Pathway Brain CNS
 National Cancer Action Team Rehabilitation Care Pathway Brain CNS Rehabilitation Care Pathway Brain CNS Diagnosis & Care Planning Drop Down Pathways Dysphagia Mobility/ loss of function Intervention D1
National Cancer Action Team Rehabilitation Care Pathway Brain CNS Rehabilitation Care Pathway Brain CNS Diagnosis & Care Planning Drop Down Pathways Dysphagia Mobility/ loss of function Intervention D1
Doncaster & Bassetlaw Cancer Locality. Palliative Care Core Formulary
 Doncaster & Bassetlaw Cancer Locality Palliative Core Formulary Approved by Doncaster & Bassetlaw Hospitals NHS Foundation Trust Drugs and Therapeutics Committee. DJ14/2155 Oct 2014 Review date: Oct 2017
Doncaster & Bassetlaw Cancer Locality Palliative Core Formulary Approved by Doncaster & Bassetlaw Hospitals NHS Foundation Trust Drugs and Therapeutics Committee. DJ14/2155 Oct 2014 Review date: Oct 2017
DELIRIUM DR S A R A H A B D E L A T I S A S DR H I L A R Y W O L F E N D A L E S T 4
 DELIRIUM DR S A R A H A B D E L A T I S A S DR H I L A R Y W O L F E N D A L E S T 4 AIMS Define delirium Identify: Different types of delirium Risk factors Preventable causes Screening tools Management
DELIRIUM DR S A R A H A B D E L A T I S A S DR H I L A R Y W O L F E N D A L E S T 4 AIMS Define delirium Identify: Different types of delirium Risk factors Preventable causes Screening tools Management
BACKGROUND Measuring renal function :
 A GUIDE TO USE OF COMMON PALLIATIVE CARE DRUGS IN RENAL IMPAIRMENT These guidelines bring together information and recommendations from the Palliative Care formulary (PCF5 ) BACKGROUND Measuring renal
A GUIDE TO USE OF COMMON PALLIATIVE CARE DRUGS IN RENAL IMPAIRMENT These guidelines bring together information and recommendations from the Palliative Care formulary (PCF5 ) BACKGROUND Measuring renal
Hydration at the End of Life:
 Hydration at the End of Life: A systematic literature review and audit of current practice November 12 th 2015 Dr Alison Coackley- Consultant in Palliative Medicine, Clatterbridge Cancer Centre Dr Catherine
Hydration at the End of Life: A systematic literature review and audit of current practice November 12 th 2015 Dr Alison Coackley- Consultant in Palliative Medicine, Clatterbridge Cancer Centre Dr Catherine
Essential Syringe Driver Training for T 34. Elaine Bird St Luke s Hospice
 Essential Syringe Driver Training for T 34 Elaine Bird St Luke s Hospice Aim For all practitioners to be accountable for their individual competence and capability when caring for a resident with a T34
Essential Syringe Driver Training for T 34 Elaine Bird St Luke s Hospice Aim For all practitioners to be accountable for their individual competence and capability when caring for a resident with a T34
Palliative Approach Toolkit: A framework for a palliative approach to care in residential aged care facilities
 Palliative Approach Toolkit: A framework for a palliative approach to care in residential aged care facilities Professor Liz Reymond MBBS (Hons), MSc, PhD, FRACGP, FAChPM Brisbane South Palliative Care
Palliative Approach Toolkit: A framework for a palliative approach to care in residential aged care facilities Professor Liz Reymond MBBS (Hons), MSc, PhD, FRACGP, FAChPM Brisbane South Palliative Care
Syringe Drivers. Back to top
 Page 1 of 8 Syringe Drivers Introduction Indications for use Advantages Method Siting syringe driver Boost facility Transfer to hospital/hospice syringe driver drugs Drug compatibility P.r.n medication
Page 1 of 8 Syringe Drivers Introduction Indications for use Advantages Method Siting syringe driver Boost facility Transfer to hospital/hospice syringe driver drugs Drug compatibility P.r.n medication
Palliative Care for Primary Care Providers QUYNH BUI, MD MPH DECEMBER 2015
 Palliative Care for Primary Care Providers QUYNH BUI, MD MPH DECEMBER 2015 Objectives Define palliative care and primary palliative care Describe the rationale for providing primary palliative care in
Palliative Care for Primary Care Providers QUYNH BUI, MD MPH DECEMBER 2015 Objectives Define palliative care and primary palliative care Describe the rationale for providing primary palliative care in
Palliative Prescribing - Pain
 Palliative Prescribing - Pain LAURA BARNFIELD 21/2/17 Aims To understand the classes of painkillers available in palliative care To gain confidence in counselling regarding opiates To gain confidence prescribing
Palliative Prescribing - Pain LAURA BARNFIELD 21/2/17 Aims To understand the classes of painkillers available in palliative care To gain confidence in counselling regarding opiates To gain confidence prescribing
Palliative and Hospice Care of the Terminally Ill Introduction
 Palliative and Hospice Care of the Terminally Ill Introduction There has been an increase in life expectancy for men and women of all races to 77.6 years Leading causes of death in older patients are chronic
Palliative and Hospice Care of the Terminally Ill Introduction There has been an increase in life expectancy for men and women of all races to 77.6 years Leading causes of death in older patients are chronic
Palliative Emergencies. Ken Stakiw
 Palliative Emergencies Ken Stakiw Disclosure None to disclose for this lecture Have received honoraria from a number of agencies and companies previously Intend to discuss some off label use of medications
Palliative Emergencies Ken Stakiw Disclosure None to disclose for this lecture Have received honoraria from a number of agencies and companies previously Intend to discuss some off label use of medications
ALLERGIES/ SENSITIVITIES This section must be completed before prescribing/administering any drug
 COMMUNITY PRESCRIPTION CHART All entries should be in CAPITAL letters and in indelible black ink. If medications/ doses are stopped, cross through the relevant line clearly to avoid error. GP: PRESCRIBER
COMMUNITY PRESCRIPTION CHART All entries should be in CAPITAL letters and in indelible black ink. If medications/ doses are stopped, cross through the relevant line clearly to avoid error. GP: PRESCRIBER
PALLIATIVE CARE NEEDS OF PEOPLE WITH DEMENTIA AT END OF LIFE
 PALLIATIVE CARE NEEDS OF PEOPLE WITH DEMENTIA AT END OF LIFE DR. CIARA MCGLADE CONSULTANT GERIATRICIAN MALLOW GENERAL HOSPITAL APRIL 2016 DEMENTIA IN IRELAND 160000 140000 120000 100000 80000 60000 40000
PALLIATIVE CARE NEEDS OF PEOPLE WITH DEMENTIA AT END OF LIFE DR. CIARA MCGLADE CONSULTANT GERIATRICIAN MALLOW GENERAL HOSPITAL APRIL 2016 DEMENTIA IN IRELAND 160000 140000 120000 100000 80000 60000 40000
BRAIN. Tumor byproducts. Autonomic nerves. Somatic nerves. Host immune cells. Cytokines
 Patient s Problems Pain (80%) Fatigue (90%) Weight Loss (80%) Lack of Appetite (80%) Nausea, Vomiting (90%) Anxiety (25%) Shortness of Breath (50%) Confusion-Agitation (80%) Tumor Mass Tumor Function Somatic
Patient s Problems Pain (80%) Fatigue (90%) Weight Loss (80%) Lack of Appetite (80%) Nausea, Vomiting (90%) Anxiety (25%) Shortness of Breath (50%) Confusion-Agitation (80%) Tumor Mass Tumor Function Somatic
Specialist palliative care for patients with heart failure. Dr Katie Taylor Consultant in Palliative Medicine
 Specialist palliative care for patients with heart failure Dr Katie Taylor Consultant in Palliative Medicine Objectives Identify which patients to refer to hospice Review symptom management Think about
Specialist palliative care for patients with heart failure Dr Katie Taylor Consultant in Palliative Medicine Objectives Identify which patients to refer to hospice Review symptom management Think about
Specialist Palliative Care Audit and Guidelines Group (SPAGG)
") Specialist Palliative Care Audit and Guidelines Group (SPAGG) Clinical Guideline for the Prescribing and Administration of Furosemide via continuous subcutaneous infusion (CSCI) for Heart Failure Patients
Specialist Palliative Care Audit and Guidelines Group (SPAGG) Clinical Guideline for the Prescribing and Administration of Furosemide via continuous subcutaneous infusion (CSCI) for Heart Failure Patients
Marie Curie Research Grants Scheme Call for outline applications Themes of call
 Marie Curie Research Grants Scheme 2016 Call for outline applications Themes of call 1. Aim Marie Curie, the Chief Scientist Office (CSO) and the Motor Neurone Disease Association (MND Association) recognise
Marie Curie Research Grants Scheme 2016 Call for outline applications Themes of call 1. Aim Marie Curie, the Chief Scientist Office (CSO) and the Motor Neurone Disease Association (MND Association) recognise
4/10/2018. Preparing for Death. Describe a Recent Death You Have Observed. The Nurse, Dying and Death
 Preparing for Death Core Curriculum FINAL HOURS CARLA JOLLEY MN, ARNP, AOCN, ACHPN WHIDBEYHEALTH PALLIATIVE CARE JOLLEC@WHIDBEYHEALTH.ORG Everyone dies Advance care planning Recognizing the transition
Preparing for Death Core Curriculum FINAL HOURS CARLA JOLLEY MN, ARNP, AOCN, ACHPN WHIDBEYHEALTH PALLIATIVE CARE JOLLEC@WHIDBEYHEALTH.ORG Everyone dies Advance care planning Recognizing the transition
CANCER REHABILITATION PATHWAY - HAEMATOLOGY
 CANCER REHABILITATION PATHWAY - HAEMATOLOGY Statement: To be used in conjunction with Brain and CNS Rehabilitation Care Pathway as appropriate Diagnosis and Care Planning: The following symptom pathways
CANCER REHABILITATION PATHWAY - HAEMATOLOGY Statement: To be used in conjunction with Brain and CNS Rehabilitation Care Pathway as appropriate Diagnosis and Care Planning: The following symptom pathways
In our patients the cause of seizures can be broadly divided into structural and systemic causes.
 Guidelines for the management of Seizures Amalgamation and update of previous policies 7 (Seizure guidelines, ND, 2015) and 9 (Status epilepticus, KJ, 2011) Seizures can occur in up to 15% of the Palliative
Guidelines for the management of Seizures Amalgamation and update of previous policies 7 (Seizure guidelines, ND, 2015) and 9 (Status epilepticus, KJ, 2011) Seizures can occur in up to 15% of the Palliative
Agitation. Susan Emmens Palliative Care Clinical Nurse Specialist
 Agitation Susan Emmens Palliative Care Clinical Nurse Specialist Definitions Restlessness finding or affording no rest, uneasy, agitated. Constantly in motion fidgeting Agitation shaking, moving, mental
Agitation Susan Emmens Palliative Care Clinical Nurse Specialist Definitions Restlessness finding or affording no rest, uneasy, agitated. Constantly in motion fidgeting Agitation shaking, moving, mental
Opioid rotation or switching may be considered if a patient obtains pain relief with one opioid and is suffering severe adverse effects.
 Dose equivalence and switching between opioids Key Messages Switching from one opioid to another should only be recommended or supervised by a healthcare practitioner with adequate competence and sufficient
Dose equivalence and switching between opioids Key Messages Switching from one opioid to another should only be recommended or supervised by a healthcare practitioner with adequate competence and sufficient
Palliative Care for Heart Failure. Service Development in West Hertfordshire
 1 Palliative Care for Heart Failure. Service Development in West Hertfordshire Dr Sharon Chadwick, Medical Director &Consultant in Palliative Medicine Hospice of St Francis, Berkhamsted. Consultant in
1 Palliative Care for Heart Failure. Service Development in West Hertfordshire Dr Sharon Chadwick, Medical Director &Consultant in Palliative Medicine Hospice of St Francis, Berkhamsted. Consultant in
NHS Grampian. Care Plan Palliative & Supportive. Acute Care Settings
 NHS Grampian Palliative & Supportive Care Plan 2013 Acute Care Settings Contents Page 1. Introduction 2. Standards 3. The identification of the palliative patient 4. Assessment of the palliative patient
NHS Grampian Palliative & Supportive Care Plan 2013 Acute Care Settings Contents Page 1. Introduction 2. Standards 3. The identification of the palliative patient 4. Assessment of the palliative patient
Road Blocks in Non-Cancer Palliative Care Obstacles observed from outpatient non-cancer palliative practice.
 Road Blocks in Non-Cancer Palliative Care Obstacles observed from outpatient non-cancer palliative practice. 25th Annual Palliative Education and Research Days, West Edmonton Mall. Edmonton. 2014 Amanda
Road Blocks in Non-Cancer Palliative Care Obstacles observed from outpatient non-cancer palliative practice. 25th Annual Palliative Education and Research Days, West Edmonton Mall. Edmonton. 2014 Amanda
Symptom Management Challenges at End-of-Life
 Symptom Management Challenges at End-of-Life Amanda Lovell, PharmD, BCGP Clinical Pharmacist- Inpatient Units Optum Hospice Pharmacy Services February 15, 2018 Hospice Pharmacy Services Objectives Identify
Symptom Management Challenges at End-of-Life Amanda Lovell, PharmD, BCGP Clinical Pharmacist- Inpatient Units Optum Hospice Pharmacy Services February 15, 2018 Hospice Pharmacy Services Objectives Identify
BJF Acute Pain Team Formulary Group
 Title Analgesia Guidelines for Acute Pain Management (Adults) in BGH Document Type Issue no Clinical guideline Clinical Governance Support Team Use Issue date April 2013 Review date April 2015 Distribution
Title Analgesia Guidelines for Acute Pain Management (Adults) in BGH Document Type Issue no Clinical guideline Clinical Governance Support Team Use Issue date April 2013 Review date April 2015 Distribution
Understanding Parkinson s for health and social care staff. The phases of Parkinson s
 Understanding for health and social care staff The phases of The phases of Diagnosis 11% 1.6 Post diagnosis before symptoms have become significant Maintenance 40.4% 5.9 Symptoms significant but largely
Understanding for health and social care staff The phases of The phases of Diagnosis 11% 1.6 Post diagnosis before symptoms have become significant Maintenance 40.4% 5.9 Symptoms significant but largely
Symptom Management in the Non-Verbal Patient at the End of Life Laura Carmon, ANP-BC
 Symptom Management in the Non-Verbal Patient at the End of Life Laura Carmon, ANP-BC 2017 NPSS Asheville, NC Objectives The learner will recognize non-verbal signs and symptoms commonly seen at the EOL.
Symptom Management in the Non-Verbal Patient at the End of Life Laura Carmon, ANP-BC 2017 NPSS Asheville, NC Objectives The learner will recognize non-verbal signs and symptoms commonly seen at the EOL.
SUBCUTANEOUS AS REQUIRED & SYRINGE PUMP PRESCRIPTION & ADMINISTRATION RECORD (SPAR) Name: Address: Postcode: Date of Birth: NHS Number:
 Name: Address: Postcode: Date of Birth: NHS Number:") FILE IN PATIENT S COMMUNITY HEALTH RECORD FOLDER : SUBCUTANEOUS AS REQUIRED & SYRINGE PUMP PRERIPTION & ADMINISTRATION RECORD (SPAR) Abbreviations used in this document to be listed here with the full
FILE IN PATIENT S COMMUNITY HEALTH RECORD FOLDER : SUBCUTANEOUS AS REQUIRED & SYRINGE PUMP PRERIPTION & ADMINISTRATION RECORD (SPAR) Abbreviations used in this document to be listed here with the full
Diamorphine 4 hour. alfentanil (500microgram/mL) Calculated by dividing 24 hour oral morphine dose by 30
 Calculated by dividing 24 hour oral morphine dose by 30") If more information is required please seek help from specialist palliative care pioid dose conversion chart, syringe driver doses, rescue/prn doses and opioid patches Use the conversion chart to work
If more information is required please seek help from specialist palliative care pioid dose conversion chart, syringe driver doses, rescue/prn doses and opioid patches Use the conversion chart to work
Respiratory Secretions. Care in the last 72 hours of life Paul Tait, pharmacist
 Respiratory Secretions Care in the last 72 hours of life Paul Tait, pharmacist 50% Why? Inability to swallow & clear secretions Ineffective cough Reduced consciousness Pooling of secretions in the throat
Respiratory Secretions Care in the last 72 hours of life Paul Tait, pharmacist 50% Why? Inability to swallow & clear secretions Ineffective cough Reduced consciousness Pooling of secretions in the throat
Restlessness Emotional support Self care
 Comfort Airway Restlessness Emotional support Self care MED 12412 9/12 City of Hope Department of Supportive Care Medicine 1500 Duarte Road Duarte, CA 91010 August 2012 The following are recommendations
Comfort Airway Restlessness Emotional support Self care MED 12412 9/12 City of Hope Department of Supportive Care Medicine 1500 Duarte Road Duarte, CA 91010 August 2012 The following are recommendations
Palliative Care and the Critical Role of the Pharmacist. Arti Thakerar Education/ Palliative Care Peter MacCallum Cancer Centre
 Palliative Care and the Critical Role of the Pharmacist Arti Thakerar Education/ Palliative Care Peter MacCallum Cancer Centre Overview What is palliative care Role of a pharmacist in palliative care Issues
Palliative Care and the Critical Role of the Pharmacist Arti Thakerar Education/ Palliative Care Peter MacCallum Cancer Centre Overview What is palliative care Role of a pharmacist in palliative care Issues