Note: These are abbreviated slides with graphics and other protected content removed for electronic posting purposes with NAPSA.
|
|
|
- Jasper Ross
- 5 years ago
- Views:
Transcription
1

2
3 Note: These are abbreviated slides with graphics and other protected content removed for electronic posting purposes with NAPSA. Please attend the presentation for the full slideshow and information.
4 Attendees will gain an understanding of the County of Ventura s APS multidisciplinary team model, its creation, and day to day functioning. Attendees will learn how psychologists can contribute to APS assessment and intervention efforts. Attendees will learn what neuropsychological assessment is and how it can assist in decision making as part of APS assessment and intervention efforts.
5
6 Prevalence of neurocognitive disorders will grow drastically over the next decades. These adults are at heightened risk for abuse and neglect. 5.7 Million 14 Million $341, Million $232 Billion $277 Billion $1.1 Trillion $7.9 Trillion
7 Case complexity is expected to increase as life expectancy increases Greater medical comorbidities Finances must stretch longer Longer and more intensive caretaking There is and will be a great need for: Effective multidisciplinary teams Standardized practice Evidence-informed practice Objective screening and assessment Integrated approaches to assessment and intervention Culturally informed practice
8
9 Origin of the Ventura County Multidisciplinary Team/Rapid Response Expert Team Funding Team members Function of the team Culture of the team
10
11 Neuropsychological Evaluation
12 A clinical neuropsychologist is a psychologist with special expertise in the applied science of brain-behavior relationships. Clinical neuropsychologists use this knowledge in the assessment, diagnosis, treatment, and/or rehabilitation of patients across the lifespan with neurological medical, neurodevelopmental, and psychiatric conditions, as well as other cognitive and learning disorders.
13 How is this guy s cognition? Is this normal aging or dementia? Would you let him make medical decisions? Does he understand his will? He wants to change it. Should he live alone? Would you let him drive a car? Is this just depression? What impact did the stroke have? Why is he behaving so differently? Is this a reversible problem or not? How can we best improve his current functioning and independence?

14 PROBLEM SOLVING MOOD PSYCHIATRIC SYMPTOMS BEHAVIOR CULTURE MEMORY ENVIRONMENT/SOCIAL SUPPORT SELF-AWARENESS
15 Collateral reports (family) Objective Behavior Rating Scales Provider s observations/ interview Medical Records Client Self-Report Objective Personality & Psychiatric Symptom Assessment Objective Neuropsychological Assessment
16 Starts with a referral question (why is Mr. Smith so forgetful?) Consists of an interview with the patient, family, medical/psych record review, and cognitive/psychological test administration Testing is an objective and standardized measure of what you want to measure (e.g., learning, memory, problem solving) Quantifies behavior or functioning compared to their peers Test data are combined with patient history, context, and observations Creates a cohesive and comprehensive understanding of a person (strengths and weaknesses) Diagnosis, prognosis, tailored recommendations, and referrals


17 Functioning Diagnosis, recommendations, and interventions Neuropsychological Assessment Time
18 Severity of Cognitive Problems? No problems Normal aging Mild Major Problems not due to cognition Course of Problems? Stable Progressive Reversible Improving
19
20 Forgetfulness (appointments, misplacing objects, conversations) Asks the same questions over and over Tip-of-the-tongue moments Learning new information takes more effort Trouble following directions Personality changes Losing independence (managing medications or schedule) Increase in careless errors (forgetting to pay bills) Inappropriate and unusual behavior (e.g., not dressing for the weather, impulsivity) Unexplained weight loss Defer to others to answer questions
21 ADLS and IADLS Toileting and bathing Dressing and grooming Writing checks, paying bills, balancing check book Shopping alone for goods such as groceries Cooking. Turning on/off the stove Keeping track of appointments Managing medications Traveling via bus, car, etc. to various places such as the store and work Emergency procedures
22 1) Evidence of significant cognitive decline from a previous level of performance in one or more cognitive domains based on: Concern of the individual, knowledgeable informant, or clinician that there has been a significant decline in cognitive function, and A substantial impairment in cognitive performance, preferably documented by standardized neuropsychological testing 2) The cognitive deficits interfere with capacity for independence in everyday activities (paying bills, managing medications).
23 1) Evidence of modest cognitive decline from a previous level of performance in one or more cognitive domains based on: Concern of the individual, knowledgeable informant, or clinician that there has been a mild decline in cognitive function, and A modest impairment in cognitive performance, preferably documented by standardized neuropsychological testing 2) The cognitive deficits do not interfere with independence in everyday activities (paying bills, managing medications), but greater effort, compensatory strategies, or accommodation may be required.
24 Alzheimer s disease Frontotemporal lobar degeneration Lewy body disease Cerebrovascular disease Traumatic brain injury Substance/medication use HIV infection Prion disease Parkinson s disease Huntington s disease Another medical condition Multiple etiologies Unspecified
25 Medication Use B 12 deficiency Hypothyroidism Kidney/Liver problems Infections (e.g., UTI) Depression PTSD Sleep apnea Stress Alcohol and drug use
26 Acute decline in brain function A medical condition and emergency Rapid onset Reduced attention and concentration Poor thinking Waxing and waning mental status Behavior changes Emotional disturbance Reversible In older adults often due to medications, infection, medical procedure (anesthesia), metabolic imbalance, exposure to toxin
27 Some subjective symptoms similar to dementia Forgetfulness, poor concentration, inattentive, disoriented, slowed verbal and motor responses, sleep problems, appetite problems May appear sad, irritable, or worried, speech might be flat Often presents with nonspecific physical symptoms Depression is not a normal part of aging Unfortunately, only ~10% of older adults with depression receive treatment. Suicide rates are the highest among older adults Especially men
28 Depression? Delirium? Dementia? Normal Aging? Something Else?
29 Obtain quick sense of global function Identify areas for formal cognitive evaluation Identify mental health/social contributors If repeated, can identify changes over time Cognition Depression Anxiety Alcohol Consumption
30
31 Screening Measures: Patient Health Questionnaire (PHQ-2 or PHQ-9) Geriatric Depression Scale (GDS) - Short Form Beck Depression Inventory-II (BDI-II) Tip: Use the patient s language Gender and age differences in symptom endorsement and language (depression is stigmatized)
32 Screening Measures: Geriatric Anxiety Inventory (GAI) Geriatric Anxiety Scale (GAS-10) Beck Anxiety Inventory (BAI) Tip: Sources of anxiety change with age Social à Work à Financial à Health à Family
33 Use the patient s language (e.g., nerves ) Have you been concerned about/fretting over a number of things? Is there anything going on in your life that is causing you concern? Do you find that you have a hard time putting things out of your mind? If the patient reports physical symptoms: What were you thinking about when you felt your heart start to race? When you can t sleep, what is usually going through your head? Common areas of concern or worry Losing independence, becoming a burden on others Finances Falling Incontinence
34 Screening Measures Short Michigan Alcohol Screening Test-Geriatric Version (S-MAST-G) Cut-Annoyed-Guilty-Eye Opener (CAGE) Alcohol Use Disorders Identification Test (AUDIT or AUDIT-C) Drug Screening Questionnaire (DAST) Tip: Do not assume your patient does not use/abuse Expect to be surprised from time to time (but don t act surprised/shocked)
35 Use a non-judgmental and non-confrontational approach Ask detailed questions about quantity and frequency of drinking, medications, and illicit drugs (yes, cannabis too) Give feedback on screening education on what constitutes low vs. high risk consumption Do not stigmatize or shame Motivational Interviewing Discuss the patient s reasons for drinking, consequences of drinking, and the patient s reasons to cut down or quit Develop realistic goal w/ patient
36 Use appropriate normative samples for objective comparison Interdisciplinary approach Understanding of how symptoms/disorders may present differently across the lifespan Attention to accommodations Length of assessment Time of day Setting Presence of others during assessment
37
38 Female in 70s, with a recent history of memory loss and poor judgment/self-neglect Concerns of opiate medication abuse At risk of losing housing as inadequate income Assessment sought to clarify diagnosis as attempting to help her find housing. Concerns dementia was contributing to difficulties. Findings (seen across several days): impairment in attention, some executive functions, learning ability Normal function in abstract reasoning skills, verbal comprehension, health and safety judgement, and money management Primary issue likely depression and substance abuse
39
40 Male in 90s, living independently, but recent episode of financial abuse Long history of supporting self by making personal loans to others At risk of ongoing financial abuse Assessment sought to clarify diagnosis and extent of impairment as intelligent and presents well, but has history of people taking advantage Findings: Early dementia. Etiology unclear, subcortical in nature and may reflect conditions such as cerebrovascular disease. Impaired attention, speed of information processing, executive functions, initial learning and memory retrieval, and on measures of health and safety judgement and financial management ability Normal functioning in memory retention, abstract reasoning, language skills, and visuospatial skills
41

42 Those referred for neuropsychological assessment: 86% were diagnosed with a neurocognitive disorder Those 86% with a Neurocognitive Disorder: Average 74 years of age 57% Female 73% White/Caucasian Average 12 years of education 9.7% given a co-occurring psychiatric disorder 1.6% given a co-occurring substance-related disorder
43
44 Risk Factors Precursors Live alone Perceived as confused or with evidence of cognitive impairment Biological Indicators Inadequate food/meal supplies Social Indicators Neglect household finances Psychological Indicators None found Interventions Medical evaluation by a physician or nurse In home nursing assessment Tangible support was used to purchase necessary items Outcome Demonstrated selfadvocacy Sought conservatorship/ guardianship Obtained conservatorship/ guardianship APS protective issue reduced or eliminated
45
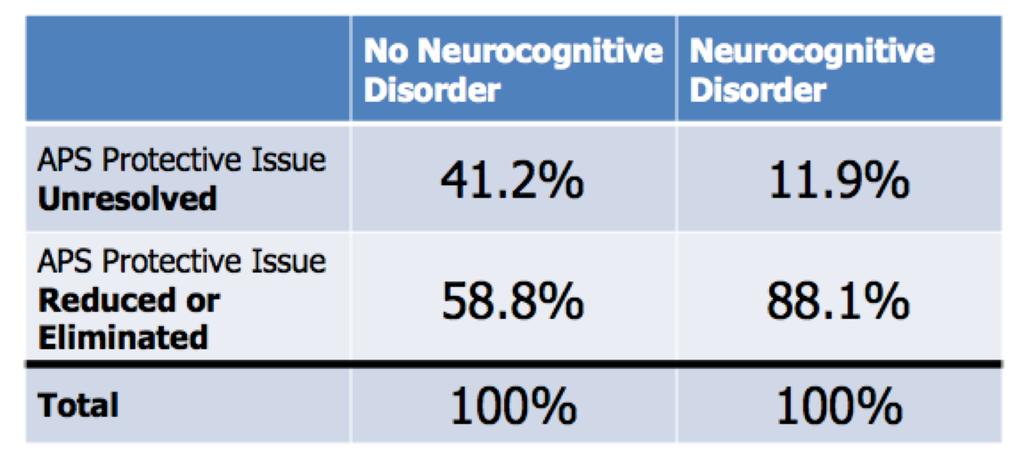
46 Neurocognitive disorders (given at neuropsychological assessment) were significantly predicative of client health and safety and money management abilities. TRIO variables were not predictive Appear to be descriptive Neuropsychological assessment appears to add a unique contribution to understanding APS clients and their functioning.
47 Increasing number of older adults and cognitive impairment in the coming decades Expected increase in use of APS services & case complexity Need for effective multidisciplinary teams Need for assessment standardization and evidence-informed practice Neuropsychology is a specialty that can: Improve objective understanding of a client s cognition Assess decision making capacity Clarify diagnosis Inform prognosis Improve biological, psychological, and social recommendations for intervention Initial research into our model demonstrates neuropsychological assessment provides a unique contribution to APS understanding of clients

48
DISCLAIMER: ECHO Nevada emphasizes patient privacy and asks participants to not share ANY Protected Health Information during ECHO clinics.
 DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
The ABCs of Dementia Diagnosis
 The ABCs of Dementia Diagnosis Dr. Robin Heinrichs, Ph.D., ABPP Board Certified Clinical Neuropsychologist Associate Professor, Psychiatry & Behavioral Sciences Director of Neuropsychology Training What
The ABCs of Dementia Diagnosis Dr. Robin Heinrichs, Ph.D., ABPP Board Certified Clinical Neuropsychologist Associate Professor, Psychiatry & Behavioral Sciences Director of Neuropsychology Training What
DSM-5 MAJOR AND MILD NEUROCOGNITIVE DISORDERS (PAGE 602)
") SUPPLEMENT 2 RELEVANT EXTRACTS FROM DSM-5 The following summarizes the neurocognitive disorders in DSM-5. For the complete DSM-5 see Diagnostic and Statistical Manualof Mental Disorders, 5th edn. 2013,
SUPPLEMENT 2 RELEVANT EXTRACTS FROM DSM-5 The following summarizes the neurocognitive disorders in DSM-5. For the complete DSM-5 see Diagnostic and Statistical Manualof Mental Disorders, 5th edn. 2013,
Overview. Case #1 4/20/2012. Neuropsychological assessment of older adults: what, when and why?
 Neuropsychological assessment of older adults: what, when and why? Benjamin Mast, Ph.D. Associate Professor & Vice Chair, Psychological & Brain Sciences Associate Clinical Professor, Family & Geriatric
Neuropsychological assessment of older adults: what, when and why? Benjamin Mast, Ph.D. Associate Professor & Vice Chair, Psychological & Brain Sciences Associate Clinical Professor, Family & Geriatric
Cognitive Assessment 4/29/2015. Learning Objectives To be able to:
 Supporting the Desire to Age in Place: Important Considerations for the Aging Population AGENDA 8:45 9:00 AM Geriatric Principles Robert L. Kane, MD *9:00 9:55 AM Cognitive Assessments Ed Ratner, MD 10:00
Supporting the Desire to Age in Place: Important Considerations for the Aging Population AGENDA 8:45 9:00 AM Geriatric Principles Robert L. Kane, MD *9:00 9:55 AM Cognitive Assessments Ed Ratner, MD 10:00
DEMENTIA Dementia is NOT a normal part of aging Symptoms of dementia can be caused by different diseases Some symptoms of dementia may include:
 DEMENTIA Dementia is NOT a normal part of aging Symptoms of dementia can be caused by different diseases Some symptoms of dementia may include: 1. Memory loss The individual may repeat questions or statements,
DEMENTIA Dementia is NOT a normal part of aging Symptoms of dementia can be caused by different diseases Some symptoms of dementia may include: 1. Memory loss The individual may repeat questions or statements,
Getting Help for Patients with Dementia and their Caregivers. Erica Salamida Associate Director of Programs and Services Alzheimer s Association-NENY
 Getting Help for Patients with Dementia and their Caregivers Erica Salamida Associate Director of Programs and Services Alzheimer s Association-NENY In this session you will learn about: Symptoms of dementia,
Getting Help for Patients with Dementia and their Caregivers Erica Salamida Associate Director of Programs and Services Alzheimer s Association-NENY In this session you will learn about: Symptoms of dementia,
After the Diagnosis: Rehabilitation & Support Options for Mild Dementia
 After the Diagnosis: Rehabilitation & Support Options for Mild Dementia Dr. Toni Nicholls, Clinical Neuropsychologist Peronne Village, cottage #20, Worthing, Christ Church 621-2022 Say these aloud Dog
After the Diagnosis: Rehabilitation & Support Options for Mild Dementia Dr. Toni Nicholls, Clinical Neuropsychologist Peronne Village, cottage #20, Worthing, Christ Church 621-2022 Say these aloud Dog
What is dementia? What is dementia?
 What is dementia? What is dementia? What is dementia? Dementia is an umbrella term for a range of progressive conditions that affect the brain. It has been identified that there are over 200 subtypes of
What is dementia? What is dementia? What is dementia? Dementia is an umbrella term for a range of progressive conditions that affect the brain. It has been identified that there are over 200 subtypes of
Neurocognitive Impairments in HIV: Natural History, Impacts on Everyday Functioning and Promising Interventions
 Neurocognitive Impairments in HIV: Natural History, Impacts on Everyday Functioning and Promising Interventions Sean B. Rourke, Ph.D. Scientist and Neuropsychologist, St. Michael s Hospital Director, CIHR
Neurocognitive Impairments in HIV: Natural History, Impacts on Everyday Functioning and Promising Interventions Sean B. Rourke, Ph.D. Scientist and Neuropsychologist, St. Michael s Hospital Director, CIHR
Dementia Facts and Resources Dementia Warning Signs Getting a Diagnosis Dementia Communication Tips Dementia Risk Reduction.
 Dementia Facts and Resources Dementia Warning Signs Getting a Diagnosis Dementia Communication Tips Dementia Risk Reduction Intermission Dementia Stages and Behaviors Caregiving and Self-Care Overview
Dementia Facts and Resources Dementia Warning Signs Getting a Diagnosis Dementia Communication Tips Dementia Risk Reduction Intermission Dementia Stages and Behaviors Caregiving and Self-Care Overview
4/11/2017. The impact of Alzheimer s disease. Typical changes. The impact of Alzheimer s disease. Problematic changes. Problematic changes
 The impact of Alzheimer s disease Ron Petersen, MD, PhD, is Director of the Mayo Alzheimer's Disease Research Center. 2 The impact of Alzheimer s disease Typical changes Typical age-related changes involve:
The impact of Alzheimer s disease Ron Petersen, MD, PhD, is Director of the Mayo Alzheimer's Disease Research Center. 2 The impact of Alzheimer s disease Typical changes Typical age-related changes involve:
The Person: Dementia Basics
 The Person: Dementia Basics Objectives 1. Discuss how expected age related changes in the brain might affect an individual's cognition and functioning 2. Discuss how changes in the brain due to Alzheimer
The Person: Dementia Basics Objectives 1. Discuss how expected age related changes in the brain might affect an individual's cognition and functioning 2. Discuss how changes in the brain due to Alzheimer
9/8/2017 OBJECTIVES:
 OBJECTIVES: To help caregivers indentify geriatric conditions by performing a simplified geriatric assessment to better manage these conditions and prevent or delay their complications. Discuss Geriatric
OBJECTIVES: To help caregivers indentify geriatric conditions by performing a simplified geriatric assessment to better manage these conditions and prevent or delay their complications. Discuss Geriatric
Decline in Mental Capacity
 Decline in Mental Capacity Elder Law: Issues, Answers and Opportunities ALI-ABA, February 23-24, 2006 Robert B. Fleming 1 FLEMING & CURTI, P.L.C. 330 N. Granada Ave. Tucson, Arizona 85701 www.elder-law.com
Decline in Mental Capacity Elder Law: Issues, Answers and Opportunities ALI-ABA, February 23-24, 2006 Robert B. Fleming 1 FLEMING & CURTI, P.L.C. 330 N. Granada Ave. Tucson, Arizona 85701 www.elder-law.com
What is dementia? What is dementia?
 What is dementia? What is dementia? What is dementia? Dementia is an umbrella term for a range of progressive conditions that affect the brain. There are over 200 subtypes of dementia, but the five most
What is dementia? What is dementia? What is dementia? Dementia is an umbrella term for a range of progressive conditions that affect the brain. There are over 200 subtypes of dementia, but the five most
Screening for Cognitive Impairment
 Screening for Cognitive Impairment Screening for Cognitive Impairment. Educational Consultant Pearson April 27, 2017 Presentation Title Arial Bold 7 pt 1 Agenda What is Cognitive Impairment? Implications
Screening for Cognitive Impairment Screening for Cognitive Impairment. Educational Consultant Pearson April 27, 2017 Presentation Title Arial Bold 7 pt 1 Agenda What is Cognitive Impairment? Implications
Community Information Forum September 20, 2014
 Community Information Forum September 20, 2014 Dr. David B. Hogan Brenda Strafford Foundation Chair in Geriatrics Medicine University of Calgary Important to note: The slides used during Dr. Hogan's presentation
Community Information Forum September 20, 2014 Dr. David B. Hogan Brenda Strafford Foundation Chair in Geriatrics Medicine University of Calgary Important to note: The slides used during Dr. Hogan's presentation
What APS Workers Need to Know about Frontotemporal, Lewy Body and Vascular Dementias
 What APS Workers Need to Know about Frontotemporal, Lewy Body and Vascular Dementias Presenter: Kim Bailey, MS Gerontology, Program & Education Specialist, Alzheimer s Orange County 1 1 Facts About Our
What APS Workers Need to Know about Frontotemporal, Lewy Body and Vascular Dementias Presenter: Kim Bailey, MS Gerontology, Program & Education Specialist, Alzheimer s Orange County 1 1 Facts About Our
ADRC Dementia Care Training. Module 10: Supporting People with Serious Mental Illness and Dementia: Bipolar Disorders, Dementia, and Delirium
 ADRC Dementia Care Training Module 10: Supporting People with Serious Mental Illness and Dementia: Bipolar Disorders, Dementia, and Delirium 1 Federal definition: Ages 18 and older Serious Mental Illness
ADRC Dementia Care Training Module 10: Supporting People with Serious Mental Illness and Dementia: Bipolar Disorders, Dementia, and Delirium 1 Federal definition: Ages 18 and older Serious Mental Illness
Session outline. Introduction to dementia Assessment of dementia Management of dementia Follow-up Review
 Dementia 1 Session outline Introduction to dementia Assessment of dementia Management of dementia Follow-up Review 2 Activity 1: Person s story Present a person s story of what it feels like to live with
Dementia 1 Session outline Introduction to dementia Assessment of dementia Management of dementia Follow-up Review 2 Activity 1: Person s story Present a person s story of what it feels like to live with
Alzheimer s disease dementia: a neuropsychological approach
 Alzheimer s disease dementia: a neuropsychological approach Dr. Roberta Biundo, PhD Neuropsychology Coordinator at Parkinson s disease and movement disorders unit of San Camillo rehabilitation hospital
Alzheimer s disease dementia: a neuropsychological approach Dr. Roberta Biundo, PhD Neuropsychology Coordinator at Parkinson s disease and movement disorders unit of San Camillo rehabilitation hospital
Dementia and Fall Geriatric Interprofessional Training. Wael Hamade, MD, FAAFP
 Dementia and Fall Geriatric Interprofessional Training Wael Hamade, MD, FAAFP Prevalence of Dementia Age range 65-74 5% % affected 75-84 15-25% 85 and older 36-50% 5.4 Million American have AD Dementia
Dementia and Fall Geriatric Interprofessional Training Wael Hamade, MD, FAAFP Prevalence of Dementia Age range 65-74 5% % affected 75-84 15-25% 85 and older 36-50% 5.4 Million American have AD Dementia
Memory & Aging Clinic Questionnaire
 Memory & Aging Clinic Questionnaire The answers you give to the questions below will assist us with our evaluation. Each section is equally important so please be sure to complete the entire questionnaire.
Memory & Aging Clinic Questionnaire The answers you give to the questions below will assist us with our evaluation. Each section is equally important so please be sure to complete the entire questionnaire.
10/17/2017. Causes of Dementia Alzheimer's Disease Vascular Dementia Diffuse Lewy Body Disease Alcoholic Dementia Fronto-Temporal Dementia Others
 1 Dementia Dementia comes from the Latin word demens, meaning out of mind. It is the permanent loss of multiple intellectual functions. It is progressive deterioration of mental powers accompanied by changes
1 Dementia Dementia comes from the Latin word demens, meaning out of mind. It is the permanent loss of multiple intellectual functions. It is progressive deterioration of mental powers accompanied by changes
P20.2. Characteristics of different types of dementia and challenges for the clinician
 P20.2. Characteristics of different types of dementia and challenges for the clinician, professor Danish Dementia Research Center Rigshospitalet, University of Copenhagen (Denmark) This project has received
P20.2. Characteristics of different types of dementia and challenges for the clinician, professor Danish Dementia Research Center Rigshospitalet, University of Copenhagen (Denmark) This project has received
Understanding the Progression of Alzheimer s and Related Dementias And Planning for Future Changes
 Town Hall Forum Making a Plan: The Smart Approach to Alzheimer s Care Needs May 25, 2017 Understanding the Progression of Alzheimer s and Related Dementias And Planning for Future Changes Daniel D. Sewell,
Town Hall Forum Making a Plan: The Smart Approach to Alzheimer s Care Needs May 25, 2017 Understanding the Progression of Alzheimer s and Related Dementias And Planning for Future Changes Daniel D. Sewell,
Aging: Tools for Assessment
 Aging: Tools for Assessment Eugenia L. Siegler, MD Mason Adams Professor of Geriatric Medicine Weill Cornell Medicine New York, New York San Antonio, Texas: August 21 to 23, 2017 Learning Objectives After
Aging: Tools for Assessment Eugenia L. Siegler, MD Mason Adams Professor of Geriatric Medicine Weill Cornell Medicine New York, New York San Antonio, Texas: August 21 to 23, 2017 Learning Objectives After
Alcohol Use Among Older Adults
 Alcohol Use Among Older Adults Pocket Screening Instruments for Health Care and Social Service Providers U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Substance Abuse and Mental Health Services Administration
Alcohol Use Among Older Adults Pocket Screening Instruments for Health Care and Social Service Providers U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Substance Abuse and Mental Health Services Administration
homeinstead.com Each Home Instead Senior Care franchise office is independently owned and operated Home Instead, Inc.
 Each Home Instead Senior Care franchise office is independently owned and operated. 2010 Home Instead, Inc. homeinstead.com Many of us may joke about having old timers disease, but when cognitive impairment
Each Home Instead Senior Care franchise office is independently owned and operated. 2010 Home Instead, Inc. homeinstead.com Many of us may joke about having old timers disease, but when cognitive impairment
Your aging brain. Contact your local chapter to learn more. Find a chapter near you at or visit alz.org/findus.
 Your aging brain. Being told that additional tests are needed because your inability to remember things or problems with talking or thinking can trigger fear, denial and other worries. You are not alone.
Your aging brain. Being told that additional tests are needed because your inability to remember things or problems with talking or thinking can trigger fear, denial and other worries. You are not alone.
ASHA Comments* (ASHA Recommendations Compared to DSM-5 Criteria) Austism Spectrum Disorder (ASD)
 Austism Spectrum Disorder (ASD)") DSM-5 (Criteria and Major Changes for SLP-Related Conditions) Individuals meeting the criteria will be given a diagnosis of autism spectrum disorder with three levels of severity based on degree of support
DSM-5 (Criteria and Major Changes for SLP-Related Conditions) Individuals meeting the criteria will be given a diagnosis of autism spectrum disorder with three levels of severity based on degree of support
SECTION 1: as each other, or as me. THE BRAIN AND DEMENTIA. C. Boden *
 I read all the available books by other [people with] Alzheimer s disease but they never had quite the same problems as each other, or as me. I t s not like other diseases, where there is a standard set
I read all the available books by other [people with] Alzheimer s disease but they never had quite the same problems as each other, or as me. I t s not like other diseases, where there is a standard set
Cognitive Evaluation in Primary Care. Scott T. Larson, MD Clinical Assistant Professor University of Iowa
 Cognitive Evaluation in Primary Care Scott T. Larson, MD Clinical Assistant Professor University of Iowa scott-larson@uiowa.edu Objectives Understand the subtypes of dementia, and the DSM-5 categorization
Cognitive Evaluation in Primary Care Scott T. Larson, MD Clinical Assistant Professor University of Iowa scott-larson@uiowa.edu Objectives Understand the subtypes of dementia, and the DSM-5 categorization
UNDERSTANDING CAPACITY & DECISION-MAKING VIDEO TRANSCRIPT
 I m Paul Bourque, President and CEO of the Investment Funds Institute of Canada. IFIC is preparing materials to assist advisors and firms in managing effective and productive relationships with their aging
I m Paul Bourque, President and CEO of the Investment Funds Institute of Canada. IFIC is preparing materials to assist advisors and firms in managing effective and productive relationships with their aging
The Basics of Alzheimer s Disease
 2017 Memory Loss Conference The Basics of Alzheimer s Disease Tom Ala, MD Center for Alzheimer s Disease and Related Disorders Southern Illinois University School of Medicine Springfield, Illinois SIU
2017 Memory Loss Conference The Basics of Alzheimer s Disease Tom Ala, MD Center for Alzheimer s Disease and Related Disorders Southern Illinois University School of Medicine Springfield, Illinois SIU
Caregiving for an Individual with Dementia: Beginning the Journey
 Caregiving for an Individual with Dementia: Beginning the Journey Kirsten W. Schwehm, PhD, ABN Institute for Dementia Research and Prevention Getting the Diagnosis Physician Assessment Cognitive Assessment
Caregiving for an Individual with Dementia: Beginning the Journey Kirsten W. Schwehm, PhD, ABN Institute for Dementia Research and Prevention Getting the Diagnosis Physician Assessment Cognitive Assessment
Recognizing Dementia can be Tricky
 Dementia Abstract Recognizing Dementia can be Tricky Dementia is characterized by multiple cognitive impairments that cause significant functional decline. Based on this brief definition, the initial expectation
Dementia Abstract Recognizing Dementia can be Tricky Dementia is characterized by multiple cognitive impairments that cause significant functional decline. Based on this brief definition, the initial expectation
Objectives Gain a better understanding of Alzheimer s disease and other dementias. Enhance ability to detect signs and symptoms of dementia and learn
 Dementia Training provided through a Minnesota Department of Human Services Community Service Development Grant Project Catherine Johnson PsyD LP 1 Objectives Gain a better understanding of Alzheimer s
Dementia Training provided through a Minnesota Department of Human Services Community Service Development Grant Project Catherine Johnson PsyD LP 1 Objectives Gain a better understanding of Alzheimer s
Objectives. 1) Define Dementia and it s symptoms. 2) Review the diagnostic process
 Define Dementia and it s symptoms. 2) Review the diagnostic process") Objectives 1) Define Dementia and it s symptoms 2) Review the diagnostic process 3) Learn about support services for persons with dementia and their families 2 The impact of Alzheimer s disease Ron Petersen,
Objectives 1) Define Dementia and it s symptoms 2) Review the diagnostic process 3) Learn about support services for persons with dementia and their families 2 The impact of Alzheimer s disease Ron Petersen,
Information Gathering Obtaining history is the most critical first step Patient-provided history may not be reliable Need info from relatives, friends
 ASSESSING COMPETENCE Michael A Hill MD UNC Psychiatry 2008 Information Gathering Obtaining history is the most critical first step Patient-provided history may not be reliable Need info from relatives,
ASSESSING COMPETENCE Michael A Hill MD UNC Psychiatry 2008 Information Gathering Obtaining history is the most critical first step Patient-provided history may not be reliable Need info from relatives,
Alzheimer s Disease and Related Disorders: The Public Health Call to Action
 Levine Alzheimer s Disease and Related Disorders: The Public Health Call to Action Jed A. Levine, M.A. Executive Vice President Director of Programs and Services Alzheimer s Association, New York City
Levine Alzheimer s Disease and Related Disorders: The Public Health Call to Action Jed A. Levine, M.A. Executive Vice President Director of Programs and Services Alzheimer s Association, New York City
Certificate in the Principles of Dementia Care
 CACHE Level 2 Certificate in the Principles of Dementia Care LE EQUALITY AND DIVERSITY ACTIVITIES P INTERACTION M PERSON-CENTRED SA MEDICATION Workbook 1 COMMUNICATION In this section, you will learn about
CACHE Level 2 Certificate in the Principles of Dementia Care LE EQUALITY AND DIVERSITY ACTIVITIES P INTERACTION M PERSON-CENTRED SA MEDICATION Workbook 1 COMMUNICATION In this section, you will learn about
Depression: More than just the blues
 Depression: More than just the blues August 2011 Knowing When to Get Help Is it depression? How do you know if you re depressed? That s a good question! Depression can be a byproduct of stress and anxiety.
Depression: More than just the blues August 2011 Knowing When to Get Help Is it depression? How do you know if you re depressed? That s a good question! Depression can be a byproduct of stress and anxiety.
Demystifying the Neuropsychological Evaluation Report. Clinical Neuropsychologist 17 March 2017 Program Director, Neurobehavioral Program
 Demystifying the Neuropsychological Evaluation Report Jennifer R. Cromer, PhD BIAC Annual Conference Clinical Neuropsychologist 17 March 2017 Program Director, Neurobehavioral Program 84% of neuropsychologists
Demystifying the Neuropsychological Evaluation Report Jennifer R. Cromer, PhD BIAC Annual Conference Clinical Neuropsychologist 17 March 2017 Program Director, Neurobehavioral Program 84% of neuropsychologists
Mild cognitive impairment A view on grey areas of a grey area diagnosis
 Mild cognitive impairment A view on grey areas of a grey area diagnosis Dr Sergi Costafreda Senior Lecturer Division of Psychiatry, UCL Islington Memory Service, C&I NHS FT s.costafreda@ucl.ac.uk London
Mild cognitive impairment A view on grey areas of a grey area diagnosis Dr Sergi Costafreda Senior Lecturer Division of Psychiatry, UCL Islington Memory Service, C&I NHS FT s.costafreda@ucl.ac.uk London
ADHD Tests and Diagnosis
 ADHD Tests and Diagnosis Diagnosing Attention Deficit Disorder in Children and Adults On their own, none of the symptoms of attention deficit disorder are abnormal. Most people feel scattered, unfocused,
ADHD Tests and Diagnosis Diagnosing Attention Deficit Disorder in Children and Adults On their own, none of the symptoms of attention deficit disorder are abnormal. Most people feel scattered, unfocused,
Memory Loss, Dementia and Alzheimer's Disease: The Basics
 Memory Loss, Dementia and Alzheimer's Disease: The Basics What is memory loss? What is age-related memory loss? Typical changes Typical age-related changes involve: Making a bad decision once in a while
Memory Loss, Dementia and Alzheimer's Disease: The Basics What is memory loss? What is age-related memory loss? Typical changes Typical age-related changes involve: Making a bad decision once in a while
Department of Geriatric Medicine
 Department of Geriatric Medicine Pre-Visit Questionnaire for Dementia Evaluation Name: MR#: Imprint Area This questionnaire is to be filled out by someone who knows you well. Name of Person completing
Department of Geriatric Medicine Pre-Visit Questionnaire for Dementia Evaluation Name: MR#: Imprint Area This questionnaire is to be filled out by someone who knows you well. Name of Person completing
Our Senior Clients Clinical Issues Treatment Implications Interventions
 Our Senior Clients Clinical Issues Treatment Implications Interventions Presented by Dr. Christine A. Cauffield, CEO, LSF Health Systems Learning Objectives Identify key characteristics of Major Depressive
Our Senior Clients Clinical Issues Treatment Implications Interventions Presented by Dr. Christine A. Cauffield, CEO, LSF Health Systems Learning Objectives Identify key characteristics of Major Depressive
Frontal Behavioural Inventory (FBI)
") This is a Sample version of the Frontal Behavioural Inventory (FBI) The full version of the Frontal Behavioural Inventory (FBI) comes without sample watermark. The full complete version includes Complete
This is a Sample version of the Frontal Behavioural Inventory (FBI) The full version of the Frontal Behavioural Inventory (FBI) comes without sample watermark. The full complete version includes Complete
6800$5< /,)(7,0( ',$*126(6 &+(&./,67 'DWH RI &XUUHQW BBBB BBBB BBBBBB
(7,0( ',$*126(6 &+(&./,67 'DWH RI &XUUHQW BBBB BBBB BBBBBB") Criteria for Probable Diagnosis: 1. Meets criteria for core symptoms of the disorder. 2. Meets all but one, or a minimum of 75% of the remaining criteria required for the diagnosis 3. Evidence of functional
Criteria for Probable Diagnosis: 1. Meets criteria for core symptoms of the disorder. 2. Meets all but one, or a minimum of 75% of the remaining criteria required for the diagnosis 3. Evidence of functional
Dr. W. Dalziel Professor, Geriatric Medicine Ottawa Hospital. November /20/ Safety: Falls/Cooking/Unsafe Behaviour. 2.
 How To Decide if an Elderly Person Can Stay at Home: The Interval of Need Concept Dr. W. Dalziel Professor, Geriatric Medicine Ottawa Hospital November 2013 3 Factors 1. Safety: Falls/Cooking/Unsafe Behaviour
How To Decide if an Elderly Person Can Stay at Home: The Interval of Need Concept Dr. W. Dalziel Professor, Geriatric Medicine Ottawa Hospital November 2013 3 Factors 1. Safety: Falls/Cooking/Unsafe Behaviour
PERSONAL HISTORY QUESTIONNAIRE
 PERSONAL HISTORY QUESTIONNAIRE Here are several pages of questions that we want you to answer about yourself. Please answer them to the best of your ability, as completely and honestly as you can. Completing
PERSONAL HISTORY QUESTIONNAIRE Here are several pages of questions that we want you to answer about yourself. Please answer them to the best of your ability, as completely and honestly as you can. Completing
Talk to your doctor discussion guide
 Talk to your doctor discussion guide Talking openly and honestly with your doctor is the best way to help them understand your symptoms of depression and how they are affecting your daily life. If you
Talk to your doctor discussion guide Talking openly and honestly with your doctor is the best way to help them understand your symptoms of depression and how they are affecting your daily life. If you
Measurement and Classification of Neurocognitive Disability in HIV/AIDS Robert K. Heaton Ph.D University of California San Diego Ancient History
 Measurement and Classification of Neurocognitive Disability in HIV/AIDS Robert K. Heaton Ph.D University of California San Diego Ancient History Group Means for NP and MMPI Variables N=381 Consecutive
Measurement and Classification of Neurocognitive Disability in HIV/AIDS Robert K. Heaton Ph.D University of California San Diego Ancient History Group Means for NP and MMPI Variables N=381 Consecutive
What is dementia? Symptoms of dementia. Memory problems
 What is dementia? What is dementia? What is dementia? Dementia is an umbrella term for a range of progressive conditions that affect the brain. The brain is made up of nerve cells (neurones) that communicate
What is dementia? What is dementia? What is dementia? Dementia is an umbrella term for a range of progressive conditions that affect the brain. The brain is made up of nerve cells (neurones) that communicate
4/26/2012. Laura Grooms, MD Assistant Professor Geriatric Medicine Department of Family and Geriatric Medicine University of Louisville April 20, 2012
 Laura Grooms, MD Assistant Professor Geriatric Medicine Department of Family and Geriatric Medicine University of Louisville April 20, 2012 Laura Grooms, MD Assistant Professor Geriatric Medicine Department
Laura Grooms, MD Assistant Professor Geriatric Medicine Department of Family and Geriatric Medicine University of Louisville April 20, 2012 Laura Grooms, MD Assistant Professor Geriatric Medicine Department
Post-Traumatic Stress Disorder
 Post-Traumatic Stress Disorder Teena Jain 2017 Post-Traumatic Stress Disorder What is post-traumatic stress disorder, or PTSD? PTSD is a disorder that some people develop after experiencing a shocking,
Post-Traumatic Stress Disorder Teena Jain 2017 Post-Traumatic Stress Disorder What is post-traumatic stress disorder, or PTSD? PTSD is a disorder that some people develop after experiencing a shocking,
Know the 10 Signs: Early Detection Matters
 Know the 10 Signs: Early Detection Matters 1 Importance of Early Detection If we could have had a correct diagnosis even two years earlier, it would have given us more time to plan, to do the things that
Know the 10 Signs: Early Detection Matters 1 Importance of Early Detection If we could have had a correct diagnosis even two years earlier, it would have given us more time to plan, to do the things that
DEMENTIA, THE BRAIN AND HOW IT WORKS AND WHY YOU MATTER
 OVERCOMING THE CHALLENGES OF MANAGING CHRONIC DISEASES IN PERSONS WITH DEMENTIA DEMENTIA, THE BRAIN AND HOW IT WORKS AND WHY YOU MATTER LEARNING OBJECTIVES Be familiar with the diagnostic criteria for
OVERCOMING THE CHALLENGES OF MANAGING CHRONIC DISEASES IN PERSONS WITH DEMENTIA DEMENTIA, THE BRAIN AND HOW IT WORKS AND WHY YOU MATTER LEARNING OBJECTIVES Be familiar with the diagnostic criteria for
Recognizing and Managing the Emotional Aspects of Parkinson s. Pamela R. Palmentera, LCSW Coordinator & Clinical Social Worker
 Recognizing and Managing the Emotional Aspects of Parkinson s Pamela R. Palmentera, LCSW Coordinator & Clinical Social Worker Sensory information from the one hemisphere crosses over to the other side
Recognizing and Managing the Emotional Aspects of Parkinson s Pamela R. Palmentera, LCSW Coordinator & Clinical Social Worker Sensory information from the one hemisphere crosses over to the other side
10 WARNING SIGNS OF ALZHEIMER S DISEASE EARLY DETECTION MATTERS
 10 WARNING SIGNS OF ALZHEIMER S DISEASE EARLY DETECTION MATTERS UNDERSTANDING DEMENTIA Your memory often changes as you grow older. Some people recognize changes in themselves before anyone else notices.
10 WARNING SIGNS OF ALZHEIMER S DISEASE EARLY DETECTION MATTERS UNDERSTANDING DEMENTIA Your memory often changes as you grow older. Some people recognize changes in themselves before anyone else notices.
Chapter 7. Screening and Assessment
 Chapter 7 Screening and Assessment Screening And Assessment Starting the dialogue and begin relationship Each are sizing each other up Information gathering Listening to their story Asking the questions
Chapter 7 Screening and Assessment Screening And Assessment Starting the dialogue and begin relationship Each are sizing each other up Information gathering Listening to their story Asking the questions
Forgetfulness: Knowing When to Ask for Help
 National Institute on Aging AgePage Forgetfulness: Knowing When to Ask for Help Maria has been a teacher for 35 years. Teaching fills her life and gives her a sense of accomplishment, but recently she
National Institute on Aging AgePage Forgetfulness: Knowing When to Ask for Help Maria has been a teacher for 35 years. Teaching fills her life and gives her a sense of accomplishment, but recently she
SCREENING FOR COMMON MENTAL DISORDERS DEPRESSIVE AND ANXIETY DISORDERS SUBSTANCE USE DISORDERS
 SCREENING FOR COMMON MENTAL DISORDERS DEPRESSIVE AND ANXIETY DISORDERS SUBSTANCE USE DISORDERS COMMON MENTAL DISORDERS Depressive Disorders Anxiety Disorders Substance use disorders CMD in HIV Twice as
SCREENING FOR COMMON MENTAL DISORDERS DEPRESSIVE AND ANXIETY DISORDERS SUBSTANCE USE DISORDERS COMMON MENTAL DISORDERS Depressive Disorders Anxiety Disorders Substance use disorders CMD in HIV Twice as
USF Mood & Anxiety Disorders Program
 QUICK INVENTORY OF DEPRESSIVE SYMPTOMATOLOGY (SELF-REPORT)(QIDS-SR16) Please circle the one response to each item that best describes you for the past seven days. 1. Falling Asleep: 0 I never take longer
QUICK INVENTORY OF DEPRESSIVE SYMPTOMATOLOGY (SELF-REPORT)(QIDS-SR16) Please circle the one response to each item that best describes you for the past seven days. 1. Falling Asleep: 0 I never take longer
BEHAVIORAL HEALTH SCREENING TOOLS
 BEHAVIORAL HEALTH SCREENING TOOLS FOR THE CO-LOCATION OF BEHAVIORAL HEALTH SERVICES IN A PRIMARY CARESETTING Date: August 29, 2017 Introduction Today s Presenter Jacqueline Delmont, MD, MBA Delmont Healthcare
BEHAVIORAL HEALTH SCREENING TOOLS FOR THE CO-LOCATION OF BEHAVIORAL HEALTH SERVICES IN A PRIMARY CARESETTING Date: August 29, 2017 Introduction Today s Presenter Jacqueline Delmont, MD, MBA Delmont Healthcare
DEMENTIA? 45 Million. What is. WHAT IS DEMENTIA Dementia is a disturbance in a group of mental processes including: 70% Dementia is not a disease
 What is PRESENTS DEMENTIA? WHAT IS DEMENTIA Dementia is a disturbance in a group of mental processes including: Memory Reasoning Planning Learning Attention Language Perception Behavior AS OF 2013 There
What is PRESENTS DEMENTIA? WHAT IS DEMENTIA Dementia is a disturbance in a group of mental processes including: Memory Reasoning Planning Learning Attention Language Perception Behavior AS OF 2013 There
Commi ee Lecture: Neurocogni ve Disorders TBI : Trauma c Brain Disorders. William L. Bograkos, MA, DO, FACOEP
 Commi ee Lecture: Neurocogni ve Disorders TBI : Trauma c Brain Disorders Toxic Brain Disorders William L. Bograkos, MA, DO, FACOEP TBI: Traumatic Brain Injury / Toxic Brain Injury (Trauma and Substance
Commi ee Lecture: Neurocogni ve Disorders TBI : Trauma c Brain Disorders Toxic Brain Disorders William L. Bograkos, MA, DO, FACOEP TBI: Traumatic Brain Injury / Toxic Brain Injury (Trauma and Substance
Cognitive and Behavioral Changes in ALS: A Guide for People with ALS and their Families
 Cognitive and Behavioral Changes in ALS: A Guide for People with ALS and their Families Overview If you had asked doctors about ALS 15 years ago, the majority of providers would have told you that ALS
Cognitive and Behavioral Changes in ALS: A Guide for People with ALS and their Families Overview If you had asked doctors about ALS 15 years ago, the majority of providers would have told you that ALS
Could it be dementia?
 Could it be dementia? Contents Could it be dementia? p1 What can affect memory or thinking skills? p1 Physical Health p1 Mental Health p1 Sensory loss p2 Mild cognitive impairment p2 What is dementia?
Could it be dementia? Contents Could it be dementia? p1 What can affect memory or thinking skills? p1 Physical Health p1 Mental Health p1 Sensory loss p2 Mild cognitive impairment p2 What is dementia?
Understanding Dementia &
 Understanding Dementia & Care Options for Those Suffering with the Disease Paige Landry BSN Hospice Care Consultant SouthernCare New Beacon Hospice Objectives Understand Dementia Understand Common Problems
Understanding Dementia & Care Options for Those Suffering with the Disease Paige Landry BSN Hospice Care Consultant SouthernCare New Beacon Hospice Objectives Understand Dementia Understand Common Problems
Know the 10 Signs: Early Detection Matters
 Importance of Early Detection Know the 10 Signs: Early Detection Matters If we could have had a correct diagnosis even two years earlier, it would have given us more time to plan, to do the things that
Importance of Early Detection Know the 10 Signs: Early Detection Matters If we could have had a correct diagnosis even two years earlier, it would have given us more time to plan, to do the things that
(5) Severe Alzheimer s Disease (SEV):
 Severe Alzheimer s Disease (SEV):") CST MEAN : () Severe Alzheimer s Disease (SEV): The severe AD group shows extreme deficits in all cognitive domains. This group in our database did not show symptoms of anosognosia. Numerous difficulties
CST MEAN : () Severe Alzheimer s Disease (SEV): The severe AD group shows extreme deficits in all cognitive domains. This group in our database did not show symptoms of anosognosia. Numerous difficulties
MANAGING YOUR COGNITIVE SYMPTOMS. Dr. Valerie Suski University of Pittsburgh Medical Center HDSA COE Director
 MANAGING YOUR COGNITIVE SYMPTOMS Dr. Valerie Suski University of Pittsburgh Medical Center HDSA COE Director The information provided by speakers in workshops, forums, sharing/networking sessions and any
MANAGING YOUR COGNITIVE SYMPTOMS Dr. Valerie Suski University of Pittsburgh Medical Center HDSA COE Director The information provided by speakers in workshops, forums, sharing/networking sessions and any
Know the 10 Signs: Early Detection Matters
 Know the 10 Signs: Early Detection Matters 1 Importance of Early Detection If we could have had a correct diagnosis even two years earlier, it would have given us more time to plan, to do the things that
Know the 10 Signs: Early Detection Matters 1 Importance of Early Detection If we could have had a correct diagnosis even two years earlier, it would have given us more time to plan, to do the things that
Cognitive Changes Workshop Outcomes
 HO 4.1 Cognitive Changes Workshop Outcomes At the end of this session, participants should be able to: define Neuropsychology and the role of the Neuropsychologist (optional) recognise normal difficulties
HO 4.1 Cognitive Changes Workshop Outcomes At the end of this session, participants should be able to: define Neuropsychology and the role of the Neuropsychologist (optional) recognise normal difficulties
Alzheimer Disease and Related Dementias
 Alzheimer Disease and Related Dementias Defining Generic Key Terms and Concepts Mild cognitive impairment: (MCI) is a state of progressive memory loss after the age of 50 that is beyond what would be expected
Alzheimer Disease and Related Dementias Defining Generic Key Terms and Concepts Mild cognitive impairment: (MCI) is a state of progressive memory loss after the age of 50 that is beyond what would be expected
Form D1: Clinician Diagnosis
 Initial Visit Packet Form D: Clinician Diagnosis NACC Uniform Data Set (UDS) ADC name: Subject ID: Form date: / / Visit #: Examiner s initials: INSTRUCTIONS: This form is to be completed by the clinician.
Initial Visit Packet Form D: Clinician Diagnosis NACC Uniform Data Set (UDS) ADC name: Subject ID: Form date: / / Visit #: Examiner s initials: INSTRUCTIONS: This form is to be completed by the clinician.
Welcome to the ADHD group
 Welcome to the ADHD group Aims of this group 1. To help you make sense of your diagnosis and how ADHD has affected you 2. To learn strategies to cope with ADHD 3. To meet others with similar experiences
Welcome to the ADHD group Aims of this group 1. To help you make sense of your diagnosis and how ADHD has affected you 2. To learn strategies to cope with ADHD 3. To meet others with similar experiences
AGED SPECIFIC ASSESSMENT TOOLS. Anna Ciotta Senior Clinical Neuropsychologist Peninsula Mental Health Services
 AGED SPECIFIC ASSESSMENT TOOLS Anna Ciotta Senior Clinical Neuropsychologist Peninsula Mental Health Services Issues in assessing the Elderly Association between biological, psychological, social and cultural
AGED SPECIFIC ASSESSMENT TOOLS Anna Ciotta Senior Clinical Neuropsychologist Peninsula Mental Health Services Issues in assessing the Elderly Association between biological, psychological, social and cultural
In-Service Education. workbook 3. by Hartman Publishing, Inc. second edition
 In-Service Education workbook 3 second edition by Hartman Publishing, Inc. Alzheimer s Disease Dignity Diabetes Restraints and Restraint Alternatives Abuse and Neglect Death and Dying Managing Stress Perf
In-Service Education workbook 3 second edition by Hartman Publishing, Inc. Alzheimer s Disease Dignity Diabetes Restraints and Restraint Alternatives Abuse and Neglect Death and Dying Managing Stress Perf
Dementia. Aetiology, pathophysiology and the role of neuropsychological testing. Dr Sheng Ling Low Geriatrician
 Dementia Aetiology, pathophysiology and the role of neuropsychological testing Dr Sheng Ling Low Geriatrician Topics to cover Why is dementia important What is dementia Differentiate between dementia,
Dementia Aetiology, pathophysiology and the role of neuropsychological testing Dr Sheng Ling Low Geriatrician Topics to cover Why is dementia important What is dementia Differentiate between dementia,
HOME HEALTH RE-REGISTRATION/CONCURRENT REVIEW TEMPLATE
 HOME HEALTH RE-REGISTRATION/CONCURRENT REVIEW TEMPLATE Provider EDS/CMAP ID # (Medicaid 9-digit ID) ALL FIELDS WITH * ARE REQUIRED Name of clinician who filled out this form Contact number Facility/Provider
HOME HEALTH RE-REGISTRATION/CONCURRENT REVIEW TEMPLATE Provider EDS/CMAP ID # (Medicaid 9-digit ID) ALL FIELDS WITH * ARE REQUIRED Name of clinician who filled out this form Contact number Facility/Provider
The PD You Don t See: Cognitive Symptoms. Joanne M. Hamilton, PhD, ABPP Clinical Neuropsychologist Division of Neurology Scripps Health
 The PD You Don t See: Cognitive Symptoms Joanne M. Hamilton, PhD, ABPP Clinical Neuropsychologist Division of Neurology Scripps Health OBJECTIVES To understand why cognitive changes occur in a motor disease
The PD You Don t See: Cognitive Symptoms Joanne M. Hamilton, PhD, ABPP Clinical Neuropsychologist Division of Neurology Scripps Health OBJECTIVES To understand why cognitive changes occur in a motor disease
Understanding Alzheimer s Disease What you need to know
 Understanding Alzheimer s Disease What you need to know From the National Institute on Aging For copies of this booklet, contact: Alzheimer s Disease Education and Referral Center P.O. Box 8250 Silver
Understanding Alzheimer s Disease What you need to know From the National Institute on Aging For copies of this booklet, contact: Alzheimer s Disease Education and Referral Center P.O. Box 8250 Silver
Taking an alcohol history
 Taking an alcohol history Dr Tony Rao Consultant Old Age Psychiatrist, SLAM NHS Foundation Trust Visiting Researcher, Institute of Psychiatry, Neurology and Neuroscience Alcohol related brain damage Alcohol
Taking an alcohol history Dr Tony Rao Consultant Old Age Psychiatrist, SLAM NHS Foundation Trust Visiting Researcher, Institute of Psychiatry, Neurology and Neuroscience Alcohol related brain damage Alcohol
Dementia in Independent Senior Housing: Concerns, Barriers and Solutions
 Dementia in Independent Senior Housing: Concerns, Barriers and Solutions LeadingAge NY April 13, 2016 Kelly Papa, MSN, RN Masonicare Corporate Director of Learning The Big Question How can we create systems
Dementia in Independent Senior Housing: Concerns, Barriers and Solutions LeadingAge NY April 13, 2016 Kelly Papa, MSN, RN Masonicare Corporate Director of Learning The Big Question How can we create systems
Kristine Burkman, Ph.D. Staff Psychologist San Francisco VA Medical Center
 Kristine Burkman, Ph.D. Staff Psychologist San Francisco VA Medical Center ASAM Disclosure of Relevant Financial Relationships Content of Activity: ASAM Medical Scientific Conference 2013 Name Commercial
Kristine Burkman, Ph.D. Staff Psychologist San Francisco VA Medical Center ASAM Disclosure of Relevant Financial Relationships Content of Activity: ASAM Medical Scientific Conference 2013 Name Commercial
Pamela S. Klonoff, PhD Clinical Director Center for Transitional Neuro-Rehabilitation Barrow Neurological Institute, Phoenix, Arizona
 Neuropsychology Pamela S. Klonoff, PhD Clinical Director Center for Transitional Neuro-Rehabilitation Barrow Neurological Institute, Phoenix, Arizona Top Ten Ways to Understand and Cope with a Brain Tumor
Neuropsychology Pamela S. Klonoff, PhD Clinical Director Center for Transitional Neuro-Rehabilitation Barrow Neurological Institute, Phoenix, Arizona Top Ten Ways to Understand and Cope with a Brain Tumor
TEN early signs of a Dementia
 TEN early signs of a Dementia 1. Memory loss on a day-to-day basis Memory loss, especially forgetting things that happened only hours or days ago. forgetting important dates or events repeatedly asking
TEN early signs of a Dementia 1. Memory loss on a day-to-day basis Memory loss, especially forgetting things that happened only hours or days ago. forgetting important dates or events repeatedly asking
Dementia. Assessing Brain Damage. Mental Status Examination
 Dementia Assessing Brain Damage Mental status examination Information about current behavior and thought including orientation to reality, memory, and ability to follow instructions Neuropsychological
Dementia Assessing Brain Damage Mental status examination Information about current behavior and thought including orientation to reality, memory, and ability to follow instructions Neuropsychological
Brain-based disorders in children, teens, and young adults: When to know there is a problem and what to do
 Brain-based disorders in children, teens, and young adults: When to know there is a problem and what to do Timothy A. Fratto, Ph.D. Neuropsychology Associates of Fairfax What is Neuropsychology? The study
Brain-based disorders in children, teens, and young adults: When to know there is a problem and what to do Timothy A. Fratto, Ph.D. Neuropsychology Associates of Fairfax What is Neuropsychology? The study
Jacksonville Center for Clinical Research Michael Koren, MD, Erin Doty, MD, Carolyn Tran, MD and Steven Toenjes, MD
 Jacksonville Center for Clinical Research Michael Koren, MD, Erin Doty, MD, Carolyn Tran, MD and Steven Toenjes, MD Is Memory Loss Normal With Aging? There are normal age-related changes with cognitive
Jacksonville Center for Clinical Research Michael Koren, MD, Erin Doty, MD, Carolyn Tran, MD and Steven Toenjes, MD Is Memory Loss Normal With Aging? There are normal age-related changes with cognitive
Chapter 7. Screening and Assessment
 Chapter 7 Screening and Assessment Screening And Assessment Starting the dialogue and begin relationship Each are sizing each other up Information gathering Listening to their story Asking the questions
Chapter 7 Screening and Assessment Screening And Assessment Starting the dialogue and begin relationship Each are sizing each other up Information gathering Listening to their story Asking the questions
We Will Discuss. Dementia and Alzheimer s Disease Basics. Dementia. Developmental Disabilities and Dementia: A Behavior Management Guide
 10/18/2013 1 Dayna Thompson M.S., LMHC Alzheimer s Educator Developmental Disabilities and Dementia: A Behavior Management Guide Alzheimer s Resource Service IU Health Bloomington-Community Health 812-353-9299
10/18/2013 1 Dayna Thompson M.S., LMHC Alzheimer s Educator Developmental Disabilities and Dementia: A Behavior Management Guide Alzheimer s Resource Service IU Health Bloomington-Community Health 812-353-9299
Integrated Care for Depression, Anxiety and PTSD. Introduction: Overview of Clinical Roles and Ideas
 Integrated Care for Depression, Anxiety and PTSD University of Washington An Evidence-based d Approach for Behavioral Health Professionals (LCSWs, MFTs, and RNs) Alameda Health Consortium November 15-16,
Integrated Care for Depression, Anxiety and PTSD University of Washington An Evidence-based d Approach for Behavioral Health Professionals (LCSWs, MFTs, and RNs) Alameda Health Consortium November 15-16,
Seniors Helping Seniors September 7 & 12, 2016 Amy Abrams, MSW/MPH Education & Outreach Manager Alzheimer s San Diego
 Dementia Skills for In-Home Care Providers Seniors Helping Seniors September 7 & 12, 2016 Amy Abrams, MSW/MPH Education & Outreach Manager Alzheimer s San Diego Objectives Familiarity with the most common
Dementia Skills for In-Home Care Providers Seniors Helping Seniors September 7 & 12, 2016 Amy Abrams, MSW/MPH Education & Outreach Manager Alzheimer s San Diego Objectives Familiarity with the most common
Mood Disorders for Care Coordinators
 Mood Disorders for Care Coordinators David A Harrison, MD, PhD Assistant Professor, Dept of Psychiatry & Behavioral Sciences University of Washington School of Medicine Introduction 1 of 3 Mood disorders
Mood Disorders for Care Coordinators David A Harrison, MD, PhD Assistant Professor, Dept of Psychiatry & Behavioral Sciences University of Washington School of Medicine Introduction 1 of 3 Mood disorders